
Submitted:
13 April 2024
Posted:
15 April 2024
You are already at the latest version
Abstract
There are several well-described molecular mechanisms that influence cell growth and are relat-ed to the development of cancer. Chemokines constitute a fundamental element which are not only involved in local growth but also affect angiogenesis, tumor spread and metastatic disease. Among them, the C-X-C motif chemokine ligand 12 (CXCL12) and its specific receptor the chemo-kine C-X-C motif receptor 4 (CXCR4) have been widely studied. The overexpression in cell mem-branes of CXCR4 has been shown to be associated with the development of different kinds of his-tological malignancies, such as adenocarcinomas, epidermoid carcinomas, mesenchymal tumors or neuroendocrine neoplasms (NENs). The molecular synapsis between CXCL12 and CXCR4 leads to the interaction of G proteins and activation of different intracellular signaling pathways in both gastroenteropancreatic (GEP) and bronchopulmonary (BP) NENs conferring greater ca-pacity for locoregional aggressiveness, epithelial-mesenchymal transition (EMT) and the ap-pearance of metastases. Therefore, it has been hypothesized how to design tools that target this receptor. The aim of this review is to focus on current knowledge of the relationship between CXCR4 and NENs, with a special emphasis on diagnostic and therapeutic molecular targets.
Keywords:
CXCR4
; CXCL12
; cancer
; neuroendocrine neoplasm
; radiotracer
1. Introduction
1.1. Role of CXCL12 and CXCR4
Chemokines are a group of small molecules (~8-10k Da) that belong to the cytokine family together with angiogenic factors, growth factors or interferons and are secreted not only by neoplastic cells but also by macrophages, lymphocytes or dendritic cells. Their main function is to stimulate chemotaxis of immune system cells as part of the inflammatory response through the interaction with fibroblasts or endothelial cells, while in neoplastic status they induce angiogenesis and sustain cell growth [1]. This action is exerted by binding the N-terminal domain, which is rich in the aminoacid cysteine, to its specific receptor [2]. Depending on the distribution of this aminoacid, 4 subtypes of cytokines are identified: CXC, CX3C, CC and C [3].
Among the 50 types of chemokines known today, the chemokine CXCL12, which is also recognised as stromal cell-derived factor-1 (SDF-1) [4], has some characteristics that make it different from the rest of its family. Firstly, it is the only cytokine whose mRNA can be subjected to a process known as differential splicing, which is why up to 6 variants of this molecule have been recognized in humans (α to ϕ) [5,6]. Secondly, it is a chemokine with an almost exclusive affinity for a single receptor, nothing to do with the promiscuity of the rest of cytokines [7]. Until a few years ago, CXCR4 was recognized as the only natural receptor for CXCL12, although it has been discovered that it can also mediate its action through interaction with the atypical chemokine receptor type 3 (ACKR3), previously known as chemokine C-X-C motif receptor 7 (CXCR7) [8,9].
1.2. Structure and Signaling Pathway of the CXCL12-CXCR4-ACKR3 Axis
CXCR4 is a molecular structure that has also presented different names throughout history. It was initially called leukocyte-derived seven-transmembrane receptor (LESTR) when it was isolated from a human blood monocyte cDNA library [13] It has also been known as cluster of differentiation 184 (CD184) or fusin. The latter name refers to the ability of the human immunodeficiency virus 1 (HIV-1) to infect human cells by the process of fusion following the binding of its glycoprotein 120 (gp120) [14]. Although its natural ligand is the chemokine CXCL12 (as mentioned before), there is greater evidence that it has a wider spectrum of interactions with other molecules. In fact, it also recognizes as ligands small proteins like ubiquitin or the macrophage migration inhibiting factor (MIF) [15,16]. This receptor belongs to the family of G protein-coupled receptors (GPCRs), which are characterized by the presence of seven membrane-spanning α-helical segments separated by alternating intracellular and extracellular loop regions [17]. The intracytoplasmic domain of the receptor remains in contact with a heterotrimeric G protein that is composed of a Gα, Gβ and Gγ subunits and, when the interaction between CXCL12 and CXCR4 occurs, the exchange of guanosine diphosphate (GDP) for triphosphate (GTP) leads to a complex process in which a GTP-bound Gα monomer and a Gβγ dimer are released [18].
The Gα subunit produces an inhibition of the adenylate cyclase leading to an increase in the intracellular calcium (Figure 1) mediated by the decrease in the concentration of adenosine 3′,5′-cyclic monophosphate (cAMP). It also interacts directly with the Src family of tyrosine kinases and then activates the signaling pathway of MEK1/2-Erk1/2 [19]. The Gβγ subunit activates phosphatidyl-inositol-3-OH kinase (PI3K) and consequently generates an increase in phosphatidylinositol triphosphate (PIP3), while the interaction with phospholipase C generates diacylglycerol (DAG) and inositol-(1,4,5)-triphosphate (IP3). IP3 increases intracellular calcium deposition after outflow from the endoplasmic reticulum (ER), while DAG interacts with protein kinase C and mitogen-activated protein kinase (MAPK) [20].
When CXCL12 binds ACKR3/CXCR7, a different signaling pathway is developed because of the biochemical difference between classical and atypical chemokine receptors, which basically boils down to the fact that atypical cytokine receptors (ACKRs) lack of G proteins and its effects are calcium-independent [21]. The signal pathway through β-arrestin proteins becomes the main way the ACKR3 activation leads to its tumorigenic properties. β-arrestins increase the MEK/ERK axis and the protein kinase B (also known as Akt) activity [22] The binding of CXCR4 to its agonist ligand results in phosphorylation and internalization of the receptor [23,24]. However, once inside the cell it can be recycled and transported back to the plasma membrane or it can be degraded in the cell lysosomes [25]. The first scenario occurs in a PKC-mediated phenomenon [26], whereas the second case takes place after interaction with E3 ubiquitin ligase [27].
2. CXCR4 and Cancer
Firstly, the involvement of CXCR4 as a co-receptor in HIV infection overshadowed its potential as a tumorigenesis-related agent and it was not until 1999 when Burger et al. noticed that this protein favored migration of B cells in chronic lymphocytic leukemia. Since then, the link between CXCR4 and tumoral disease has been analysed and, for instance, it is well known the implication of CXCR4 in more than 23 cancers [28,29,30]. Considering that CXCR4 functions involve the promotion of cell growth, proinflammatory cell recruitment, angiogenesis and cell migration, it is not surprising that the pathological activation of this receptor favors the development of tumoral disease. To be more accurate, the hyperactivation of the CXCL12/CXCR4/AKR3 axis is associated with a bigger size of the tumor, lesser degree of cell differentiation, higher probability of recurrence, worse response to chemotherapy and decresased overall survival [31,32]. The role it plays in cell growth and its different effects on stromal tissue have placed this receptor in the spotlight of the scientific community. CXCR4 has been studied in practically all the different types of cancer because its expression is independently associated with decreased survival [33]. In fact, it is being investigated whether it could be a pan-cancer marker of the microenvironment status [34].
Presence of metastases drastically worsens cancer prognosis and CXCR4 is closely related to this phenomenon in various solid tumors. It is hypothesized that the upward adjustment of the CXCR4/CXCL12 axis occurs in organs on which metastases frequently settle such as liver, lung, brain or bone [5,35,36] and this fact can be ratified if it is taken into account that the blockade of this axis leads to metastatic dissemination in animal studies [37,38]. Regarding the possible underlying mechanisms, the influence on the epithelial-mesenchymal transition (EMT) is postulated. This is a process characterized by the disarticulation of tight junctions and loss of apicobasal polarity [39] that facilitates distant dissemination and invasion of different organs by the acquisition of a mesenchymal phenotype. This process involves interleukin 11 [40] the NF-kB receptor [41] and CXCR4 [42,43].
Lastly, CXCR4 is closely related not only to solid tumors but also to the hematopoietic system [44]. Such is the case that the CXCR4/CXCL12-knockout mice exhibit specific characteristics which consist in heart malformations, abnormal cerebellar development and absence of myelopoiesis and B lymphopoiesis [45,46,47]. This phenomenon can be explained if we take into consideration that CXCL12 is one of the most relevant cytokines involved in the chemotactic response of hematopoietic stem cells (HSCs) [48]. Having this ligand-receptor axis intact results necessary not only for the homing of HSCs through the bone marrow but also to retain them in the hematopoietic microenvironment [49,50] . This knowledge has led to the development of strategies that target this level, such as the CXCR4 antagonist plerixafor, which is used in bone marrow transplant in patients with multiple myeloma or non-Hodgkin lymphoma due to its ability to mobilize HSCs from the bone stroma to the peripheral blood [51].
3. CXCR4 and NENs
3.1. Introduction to Neuroendocrine Neoplasms
NENs are a heterogeneous group of malignant tumors whose origin relies in the cells of the diffuse endocrine system, which are scattered throughout the human body although the most frequent locations are tumors are in the gastrointestinal (GI) tract or in the lung. The incidence of NENs varies substantially according to the location of the primary tumor, being approximately 3.56 new cases per 100,000 in gastroenteropancreatic NENs (GEP-NENs), 1.49/100,000 in bronchopulmonary NENs (BP-NENs) and 0.84/100,000 in unknown primary NENs [52]. It is important to highlight the association of NENs with genetic syndromes such as multiple endocrine neoplasia syndrome type 1 [53]. NENs can be classified depending on whether they produce biologically active substances or not. Currently, it is considered that about 60% of NENs are non-functioning [54]. Carcinoid syndrome is the most common of the many syndromes that can develop due to hormone production [55] (such as insulinoma, glucagonoma, gastrinoma).
The expression of somatostatin receptors (SSTR) on the cell membrane is a typical feature of NENs and it has diagnostic as well as therapeutic approaches [56]. In fact, the ability to diagnose NENs has improved substantially thanks to the incorporation of gallium-68(68Ga)-labeled DOTA tracers, such as DOTA-TOC, DOTA-TATE and DOTA-NOC because of its sensitivity and specificity that reach 97% and 92% respectively [57] compared to Indium-111 scintigraphy (sensitivity 72% and specificity 92%).
Somatostatin analogs (SSA) constitute the first line treatment in NENs due to an antisecretory as well as an antiproliferative effect. In fact, administration of both octreotide [58] or lanreotide [59] has demonstrated increases in progression-free survival (PFS) versus placebo (14.3 vs 6.0 months, HR 0.34 and >27 vs 18 months, HR 0.47 respectively) in GEP-NENs. Regarding BP-NENs, only lanreotide has shown benefits in PFS [60] (16.6 vs 13.6 months, HR 0.90). There are 5 types of SSTRs, although the drugs currently available focus on SSTR2A and SSTR5 agonism. Lanreotide and octreotide mainly stimulate SSTR2 while pasireotide exerts its action after binding to SSTR2 and SSTR5. In general, NENs are indolent and slow-growing tumors. The main prognostic factor for GEP-NENs is the tumor grade according to the latest WHO classification, which takes into account cytologic features, number of mitoses per field and Ki-67 proliferation index [61]. BP-NENs are governed by a similar classification, but this does not take into account the proliferation index but the presence of necrosis on histology [62]. Four variants can be recognized: typical carcinoid (TC), atypical carcinoid (AC), large-cell neuroendocrine carcinoma (LCNC) and small-cell neuroendocrine carcinoma (SCNC).
3.2. Implications of CXCR4 Expression in NENs
The molecular study of NENs involves the detection and evaluation of multiple membrane targets, among which SSTRs are the most important. The more the SSTR are expressed (specially SSTR2A), the lower grade and therefore the better prognosis of NENs [63,64,65,66,67,68]. As with other types of neoplasms, the chemokine receptor CXCR4 is becoming increasingly relevant to researchers in the field of NENs. Circelli et al. demonstrated that the PI3K/Akt/mTOR pathway is enhanced both in GEP-NENs and in BP-NENs cell lines throughout an upregulation of the CXCR4-CXCL12 axis [69]. Indeed, the hyperactivation of this intracellular pathway has led to the development of mTOR inhibitors for the treatment of pancreatic NENs [70,71].
Among the multiple factors that determine the functioning of the CXCL12-CXCR4 axis, the hypoxia phenomenon plays a fundamental role in carcinogenesis [72,73,74] and in the homeostasis of these molecules [75,76]. The hypoxia-inducible factor 1α and 2α (HIF1α and HIF2α) increase the expression of CXCR4, confer greater aggressiveness and result in lower survival in patients with ileal NENs [77,78]. Kaemmerer et al. demonstrated the inverse relationship between CXCR4 expression and overall survival (OS) in GEP-NENs, since those patients with a marked expression of this receptor had a lower, although not significant, OS compared to those with a weak expression (34.0 vs. 50.0 months, p = 0.068). This expression was higher in high grade tumors (differentiating also between grade 3a and 3b) versus low grade tumors. Furthermore, positive correlation was identified between CXCR4 and Ki-67 index (r 0.39; p < 0.001) and with SSTR5 expression (r 0.27; p = 0.003), while SSTR2A expression showed a robust inverse correlation (r -0.50; p < 0.001) [79].
There exists no clear agreement about the relationship between CXCR4 expression and GEP-NENs location. While Mai et al. showed higher expression in those whose primary tumor is located in the appendix or colon (p = 0.024) [80], Popa et al. showed no statistical differences among them, but greater expression in colonic primary tumors but least immunorreactive intensity in appendix ones [81]. Interestingly, no statistical differences were found in both studies between primary tumor and metastases in the intensity of expression. In relation to hormone production, it appears that expression is higher in those non-functioning neoplasms (p = 0.019) [80]. Regarding BP-NENs, it has also been shown an inverse correlation with OS. TC and AT tend to show lower expression of CXCR4 but high and intense in SCLC [82] .The role that CXCR4 plays in the EMT is crucial in the pathogenesis of metastatic disease in both GEP and BP-NENs [83,84,85,86]. It appears that among multiple target organs, bone involvement is intimately influenced by the overexpression of this receptor, both in vitro [87] and in vivo [88] studies.
3.3. CXCR4 as a Target for Imaging Diagnosis on NENs
The use of computed tomography (CT) and magnetic resonance imaging (MRI) scans is essential in the diagnosis and staging of tumoral disease. However, the use of functional imaging techniques through the administration of radiotracers has become a cornerstone in the management of patients with NENs. The main molecular targets in the study of NENs are somatostatin receptors, especially SSTR2 and SSTR5. The first imaging techniques that emerged were 111In-DTPA-Pentetreotide (Octreoscan®) and 99mTC-EDDA-HYNIC-Thr3-octreotide (Tektrotyd®) scintigraphy with improved spatial resolution using single photon emission tomography (SPECT/CT). Diagnostic performance was subsequently increased with the introduction of radiopharmaceuticals suitable for positron emission tomography (PET/CT) such as 68Ga-labeled tracers. However, the expression of SSTRs decreases with the increasing tumor grade and that influences in the 68Ga-PET/CT sensitivity (72,2% in G1 vs 40,8% in G3 NENs) and maximum standardized uptake value (SUVmax) (29,2 in G1 vs 12,8 in G3 NENs) [89], so SSTR targeting may be less useful in the diagnosis and follow-up of dedifferentiated NENs. In this scenario, 18F-fluorodeoxyglucose (18F-FDG) PET/CT provides additional information and provides insight into the metabolic state of the neoplastic lesions [90,91]. However, this technique is not free of interferences that may hinder its correct interpretation [92] and it is therefore necessary to investigate alternative molecular targets for lesions with a lower degree of differentiation.
In 2008, Uy et al. developed the drug plerixafor, (AMD3100) a CXCR4 antagonist that prevents binding of its ligand CXCL12/SDF-1 and is used for stem cell mobilization from bone marrow prior to hematopoietic progenitor transplantation [93]. In 2014 Aghanejad et al. developed a 68Gallium-plerixafor radiotracer that demonstrated its potential utility in the field of Oncology by detecting breast cancer cells in an in vivo mouse model [94]. However, previously Gourni et al. designed a molecule composed of a cyclic peptide CPCR4-2 labeled with 68Ga (cyclo(D-Tyr1-[NMe]-D-Orn2-[4-(aminomethyl) benzoic acid,68Ga-DOTA]-Arg3-2-Nal4-Gly5, also known as pentixafor) which has revealed higher specificity for CXR4 and greater in vivo stability for the study of malignant neoplasms in humans [95,96,97]. 68Ga-Pentixafor seems to be an interesting future tool and therefore studies are being carried out to show the usefulness of this in various types of neoplasms [98].
Regarding NENs, Werner et al. was the first to noninvasively evaluate CXCR4 expression by 68Ga-Pentixafor PET/CT compared with 68Ga-DOTA-TOC and 18F-FDG PET/CT in 12 patients with GEP-NENs. 68Ga-Pentixafor was negative in all G1-NENs while 68Ga-DOTA-TOC and 18F-FDG PET/CT identified lesions in 12/12 and 11/12 patients respectively. In G2-NENs 68Ga-Pentixafor was positive in half of the cases (2/4) whereas both 68Ga-DOTA-TOC and 18F-FDG were positive in all of them and in G3-NENs both 68Ga-Pentixafor and 68Ga-DOTA-TOC confirmed positivity in 4/5 patients when 18F-FDG was positive in 5/5 of the cases. These data agree with what has been published to date on the lower expression of SSTR and the increase in CXCR4 at higher tumor grade. However, the results further support the use of 18F-FDG against direct targeting of CXCR4 with pentixafor. In addition, the number of lesions identified was markedly lower compared to the other radiotracers, both overall (69 lesions for 68Ga-Pentixafor, 127 for 18F-FDG and 245 for 68Ga-DOTA-TOC) and stratified by WHO tumor grading [99]. Interestingly, not only are there differences in the ability to detect lesions in different patients, but intraindividual variability has also been shown in which some G3-NENs lesions may be positive for 18F-FDG and negative for 68Ga-Pentixafor or vice versa. That makes the management of patients with NENs more complex because of the existence of multiple lesions with different molecular behavior [100].
To evaluate the diagnostic potential of CXCR4 labeling in dedifferentiated tumors, Weich et al. confronted 18F-FDG and 68Ga-Pentixafor PET/CT in 11 patients newly diagnosed from GEP-NEC and studied IHC expression of CXCR4. In a per patient analysis 18F-FDG-avid lesions were detected in all patients while 68Ga-Pentixafor was positive in 10/11 patients. In a per lesion analysis, it was shown the ability of 18F-FDG to reveal more lesions in comparison with 68Ga-Pentixafor (102 vs. 42 lesions, p < 0.001). In relation to radiotracer uptake intensity, 18F-FDG showed a higher SUVmax in contrast to 68Ga-Pentixafor (12.8 ± 9.8 vs. 5.2 ± 3.7, p < 0.001) and greater tumor-to-background ratios (TBR) (7.2 ± 7.9 vs. 3.4 ± 3.0, p < 0.001). With respect to IHC, the overall CXCR4 expression was catalogued as low in 7/11 patients and there was no correlation between the intensity of CXCR4 expression and the 68Ga-Pentixafor uptake in biopsies [101].
With regard to BP-NENs, the correlation between the 68Ga-Pentixafor uptake in PET/CT images and the CXCR4 expression by mean fluorescence index and IHC was studied. Although there was an increased uptake in all patients, no correlation was found to both cytologic features [102]. However, a study comparing the usefulness of 68Ga-Pentixafor versus other types of radiotracers in BP-NENs has not yet been developed. In addition, 68Ga-Pentixafor has not shown association with clinical parameters such as OS or PFS both in GP-NENs and SCLC, although it does appear to be related to leukocyte and platelet counts [103].
Among the multiple interrelated processes in CXCR4 homeostasis, the Wnt/β-catenin molecular pathway is fundamental in the correct functioning of the CXCL12-CXCR4 axis [104,105] and is also deregulated in about 25% of patients with GEP, lung or thymus NENs [106]. For this reason, the possibility of modulating the expression density of CXCR4 and its 68Ga-Pentixafor binding capacity in NEN cell lines has been studied, achieving promising results that open the door to future studies with Wnt inhibitors or activators [107].
3.4. CXCR4 Targeting as Treatment of NENs
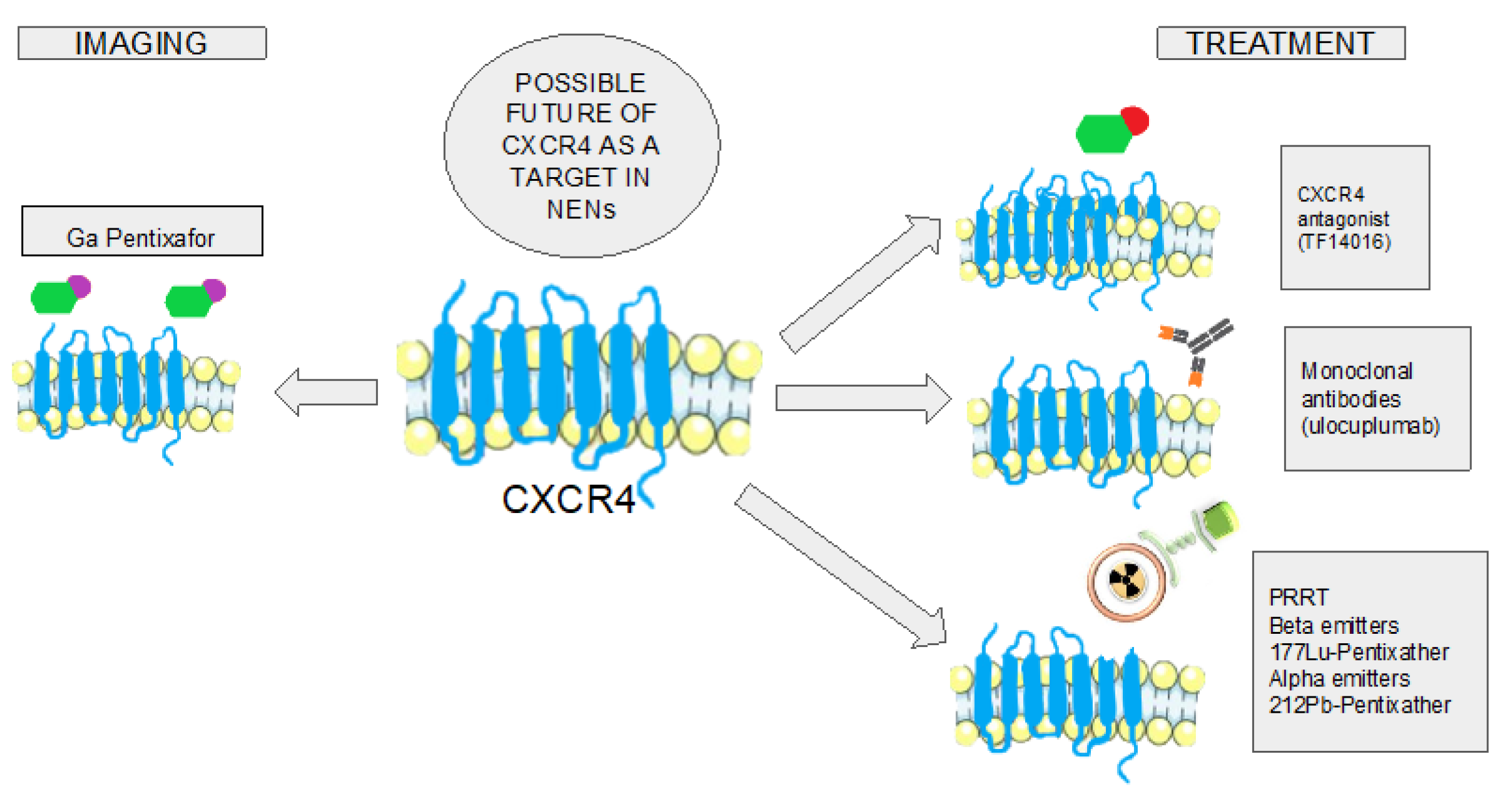
Precision medicine consists of individualizing treatment according to the specific characteristics of each patient and neoplasm. In the case of NENs, a good example is treatment with SSA, which perform their action specifically against neoplastic cells that express SSTR in their plasma membrane. However, sometimes this treatment is not sufficient, and it is necessary to identify new therapeutic targets. CXCR4 emerges as a possible target and the selective approach against it can be carried out using different therapeutic strategies [108] (Figure 2).
Synthetic Peptides
Administration of TF14016, a direct CXCR4 inhibitor, has shown in animal models to decrease the number and size of pulmonary metastases in SCLC. In addition, a lower expression of vascular endothelial cell growth factor was recorded [109]. A cyclic peptide antagonist called LY2510924 was studied in a phase II trial in patients with SCLC added to carboplatin/etoposide but did not show efficacy (PFS 5.88 vs 5.85, p=0.9806) although its toxicity profile was acceptable [110]. Although there is limited information about the treatment of NENs with this type of molecules, there are peptides such as balixafortide, motixafortide or mavorixafor that have been studied in the treatment of solid neoplasms [111,112,113], HSC mobilization prior to bone marrow transplantation [114,115] or even in the rare warts, hypogammaglobulinemia, immunodeficiency and myelokathexis (WHIM) syndrome [116] but not yet neither in GEP nor BP-NENs.
Monoclonal Antibodies
Several antibodies against CXCR4 have been studied, although most trials are in early stages and evidence in NENs is limited [117]. For the time being, no in vivo studies have been developed and the information available comes from in vitro studies. The effect of ulocuplumab (monoclonal antibody that prevents CXCL12 binding) has been studied in pancreatic NENs [118]. Although it has not been shown to exert a cytolytic effect on tumor cells, a reduced migration towards the liver and bone by inhibiting EMT has been observed. Intriguingly, Yingnan Si et al developed dual SSTR2/CXCR4 targeted extracellular vesicles-delivered combined therapy throughout monoclonal antibodies against pancreatic, thyroid and lung NENs [119]. This experimental treatment showed an anticancer efficacy both in vitro and in vivo models and no systemic toxicity was reported.
Peptide Receptor Radionuclide Therapy
Theragnosis is a medical approach combining diagnosis and therapy to tailor treatment strategies for individual patients, primarily used in cancer care to identify specific receptors and then target them with precise radiotracer.
As mentioned above, plerixafor is a CXCR4 antagonist mainly used in haematopoietic stem cell transplant. However, it has also been studied for stem cell collection in patients with a NEN massive bone marrow infiltration, prior to the administration of 177Lu-DOTATATE and initiated after the failure of a granulocyte-colony stimulating factor [120]. NENs are a type of tumor in which peptide receptor radionuclide therapy (PRRT) is being implemented since the publication of the trial NETTER-1 in 2017 [121]. This trial showed the superiority of 177Lu-DOTATATE versus SSA high-dose monotherapy in terms of PFS. Although a non-significant improvement in OS was subsequently identified (36.3 months vs 40 months in the PRRT-Lu arm, p=0.30), this effect was attributed to the high rate (36%) of cross-over of patients in the control arm to PRRT after progression [122].
The role of 68Ga-Pentixafor in the diagnosis of high-grade NENs and dedifferentiated NECs has been investigated. However, due to its altered affinity for CXCR4 when interacting with metal-chelate conjugates and its relatively fast clearance [123], 68Ga-Pentixafor does not appear to be a valid tool for the therapeutic management of malignancies. Thus, Schottelius et al. designed a novel molecule with improved pharmacokinetics called pentixather which was labeled with 177Lu [124]. Most of the available evidence for this novel radiopharmaceutical comes from its endoradiotherapeutic use in hematologic malignancies. It has been shown to elicit high responses and decrease 18F-FDG uptake in multiple myeloma lesions both bound to 177Lu and 90Y [125,126]. It has also demonstrated utility in refractory acute leukemia and diffuse large cell lymphoma [127,128] and may be useful in glioblastoma cells [129]. The available evidence for pentixather in the treatment of NENs comes solely from BP-NENs in animal studies. On the one hand, 177Lu-Pentixather has been shown to decrease tumor growth and increase OS in mice with SCLC [130]. On the other hand, the administration of 212Pb-Pentixather associated with a thioredoxin reductase inhibitor caused a delay in tumor growth in mice with SCLC xenograft [131].
4. Conclusions
CXCR4 and its ligand CXCL12 are essential in the tumorigenesis and development of NENs. It appears that SSTRs and CXCR4 maintain an antagonistic relationship that favors the latter in high-grade, dedifferentiated and metastatic tumors. Consequently, current research is focusing on selectively targeting this membrane receptor. At the moment, it seems that targeted diagnosis using 68Ga-Pentixafor does not provide more information than 18F-FDG although there are mechanisms that may influence its uptake and be relevant in the future. The treatment of NENs with molecules specifically directed against CXCR4 is in preclinical phase, although the data on radiopharmaceuticals such as 177Lu-Pentixather or 212Pb-Pentixather in the theragnosis treatment of BP-NENs are encouraging.
Author Contributions
Conceptualization, D.S-P and M.I.d.O.-G., writing—original draft prepara- tion, D.S-P and M.I.d.O.-G., writing—review and editing, D.S-P, M.I.d.O.-G., S.P.-W., C.Z.R, A.S.H, J.H-G, L.M-B, J.F.M.-T.; supervision, J.F.M.-T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Raman, D.; Baugher, P. J.; Thu, Y. M.; Richmond, A. Role of Chemokines in Tumor Growth. Cancer Lett. 2007, 256, 137–165. [Google Scholar] [CrossRef]
- Le, Y.; Zhou, Y.; Iribarren, P.; Wang, J. Chemokines and Chemokine Receptors: Their Manifold Roles in Homeostasis and Disease. Cell. Mol. Immunol. 2004, 1, 95–104. [Google Scholar]
- Bachelerie, F.; Ben-Baruch, A.; Burkhardt, A. M.; Combadiere, C.; Farber, J. M.; Graham, G. J.; Horuk, R.; Sparre-Ulrich, A. H.; Locati, M.; Luster, A. D.; Mantovani, A.; Matsushima, K.; Murphy, P. M.; Nibbs, R.; Nomiyama, H.; Power, C. A.; Proudfoot, A. E. I.; Rosenkilde, M. M.; Rot, A.; Sozzani, S.; Thelen, M.; Yoshie, O.; Zlotnik, A. International Union of Pharmacology. LXXXIX. Update on the Extended Family of Chemokine Receptors and Introducing a New Nomenclature for Atypical Chemokine Receptors. Pharmacol. Rev. 2014, 66, 1–79. [Google Scholar] [CrossRef]
- Bleul, C. C.; Fuhlbrigge, R. C.; Casasnovas, J. M.; Aiuti, A.; Springer, T. A. A Highly Efficacious Lymphocyte Chemoattractant, Stromal Cell-Derived Factor 1 (SDF-1). J. Exp. Med. 1996, 184, 1101–1109. [Google Scholar] [CrossRef]
- Yu, L.; Cecil, J.; Peng, S.-B.; Schrementi, J.; Kovacevic, S.; Paul, D.; Su, E. W.; Wang, J. Identification and Expression of Novel Isoforms of Human Stromal Cell-Derived Factor 1. Gene 2006, 374, 174–179. [Google Scholar] [CrossRef]
- Righetti, A.; Giulietti, M.; Šabanović, B.; Occhipinti, G.; Principato, G.; Piva, F. CXCL12 and Its Isoforms: Different Roles in Pancreatic Cancer? J. Oncol. 2019, 2019, 9681698. [Google Scholar] [CrossRef] [PubMed]
- Griffith, J. W.; Sokol, C. L.; Luster, A. D. Chemokines and Chemokine Receptors: Positioning Cells for Host Defense and Immunity. Annu. Rev. Immunol. 2014, 32, 659–702. [Google Scholar] [CrossRef] [PubMed]
- Balabanian, K.; Lagane, B.; Infantino, S.; Chow, K. Y. C.; Harriague, J.; Moepps, B.; Arenzana-Seisdedos, F.; Thelen, M.; Bachelerie, F. The Chemokine SDF-1/CXCL12 Binds to and Signals through the Orphan Receptor RDC1 in T Lymphocytes. J. Biol. Chem. 2005, 280, 35760–35766. [Google Scholar] [CrossRef] [PubMed]
- Burns, J. M.; Summers, B. C.; Wang, Y.; Melikian, A.; Berahovich, R.; Miao, Z.; Penfold, M. E. T.; Sunshine, M. J.; Littman, D. R.; Kuo, C. J.; Wei, K.; McMaster, B. E.; Wright, K.; Howard, M. C.; Schall, T. J. A Novel Chemokine Receptor for SDF-1 and I-TAC Involved in Cell Survival, Cell Adhesion, and Tumor Development. J. Exp. Med. 2006, 203, 2201–2213. [Google Scholar] [CrossRef]
- Rajasekaran, D.; Gröning, S.; Schmitz, C.; Zierow, S.; Drucker, N.; Bakou, M.; Kohl, K.; Mertens, A.; Lue, H.; Weber, C.; Xiao, A.; Luker, G.; Kapurniotu, A.; Lolis, E.; Bernhagen, J. Macrophage Migration Inhibitory Factor-CXCR4 Receptor Interactions. J. Biol. Chem. 2016, 291, 15881–15895. [Google Scholar] [CrossRef]
- Tripathi, A.; Saini, V.; Marchese, A.; Volkman, B. F.; Tang, W.-J.; Majetschak, M. Modulation of the CXC Chemokine Receptor 4 Agonist Activity of Ubiquitin through C-Terminal Protein Modification. Biochemistry 2013, 52, 4184–4192. [Google Scholar] [CrossRef]
- Scofield, S. L. C.; Daniels, C. R.; Dalal, S.; Millard, J. A.; Singh, M.; Singh, K. Extracellular Ubiquitin Modulates Cardiac Fibroblast Phenotype and Function via Its Interaction with CXCR4. Life Sci. 2018, 211, 8–16. [Google Scholar] [CrossRef]
- Loetscher, M.; Geiser, T.; O’Reilly, T.; Zwahlen, R.; Baggiolini, M.; Moser, B. Cloning of a Human Seven-Transmembrane Domain Receptor, LESTR, That Is Highly Expressed in Leukocytes. J. Biol. Chem. 1994, 269, 232–237. [Google Scholar] [CrossRef]
- Crump, M. P.; Gong, J. H.; Loetscher, P.; Rajarathnam, K.; Amara, A.; Arenzana-Seisdedos, F.; Virelizier, J. L.; Baggiolini, M.; Sykes, B. D.; Clark-Lewis, I. Solution Structure and Basis for Functional Activity of Stromal Cell-Derived Factor-1; Dissociation of CXCR4 Activation from Binding and Inhibition of HIV-1. EMBO J. 1997, 16, 6996–7007. [Google Scholar] [CrossRef]
- Bernhagen, J.; Krohn, R.; Lue, H.; Gregory, J. L.; Zernecke, A.; Koenen, R. R.; Dewor, M.; Georgiev, I.; Schober, A.; Leng, L.; Kooistra, T.; Fingerle-Rowson, G.; Ghezzi, P.; Kleemann, R.; McColl, S. R.; Bucala, R.; Hickey, M. J.; Weber, C. MIF Is a Noncognate Ligand of CXC Chemokine Receptors in Inflammatory and Atherogenic Cell Recruitment. Nat. Med. 2007, 13, 587–596. [Google Scholar] [CrossRef]
- Saini, V.; Staren, D. M.; Ziarek, J. J.; Nashaat, Z. N.; Campbell, E. M.; Volkman, B. F.; Marchese, A.; Majetschak, M. The CXC Chemokine Receptor 4 Ligands Ubiquitin and Stromal Cell-Derived Factor-1α Function through Distinct Receptor Interactions. J. Biol. Chem. 2011, 286, 33466–33477. [Google Scholar] [CrossRef]
- Rosenbaum, D. M.; Rasmussen, S. G. F.; Kobilka, B. K. The Structure and Function of G-Protein-Coupled Receptors. Nature 2009, 459, 356–363. [Google Scholar] [CrossRef]
- Goldsmith, Z. G.; Dhanasekaran, D. N. G Protein Regulation of MAPK Networks. Oncogene 2007, 26, 3122–3142. [Google Scholar] [CrossRef]
- New, D. C.; Wu, K.; Kwok, A. W. S.; Wong, Y. H. G Protein-Coupled Receptor-Induced Akt Activity in Cellular Proliferation and Apoptosis. FEBS J. 2007, 274, 6025–6036. [Google Scholar] [CrossRef] [PubMed]
- Mellado, M.; Rodríguez-Frade, J. M.; Mañes, S.; Martínez-A, C. Chemokine Signaling and Functional Responses: The Role of Receptor Dimerization and TK Pathway Activation. Annu. Rev. Immunol. 2001, 19. (Volume 19, 2001), 397–421. [Google Scholar] [CrossRef] [PubMed]
- Thelen, M.; Thelen, S. CXCR7, CXCR4 and CXCL12: An Eccentric Trio? J. Neuroimmunol. 2008, 198, 9–13. [Google Scholar] [CrossRef]
- Rajagopal, S.; Kim, J.; Ahn, S.; Craig, S.; Lam, C. M.; Gerard, N. P.; Gerard, C.; Lefkowitz, R. J. β-Arrestin- but Not G Protein-Mediated Signaling by the “Decoy” Receptor CXCR7. Proc. Natl. Acad. Sci. U. S. A. 2010, 107, 628–632. [Google Scholar] [CrossRef]
- Haribabu, B.; Richardson, R. M.; Fisher, I.; Sozzani, S.; Peiper, S. C.; Horuk, R.; Ali, H.; Snyderman, R. Regulation of Human Chemokine Receptors CXCR4: ROLE OF PHOSPHORYLATION IN DESENSITIZATION AND INTERNALIZATION *. J. Biol. Chem. 1997, 272, 28726–28731. [Google Scholar] [CrossRef]
- Signoret, N.; Rosenkilde, M. M.; Klasse, P. J.; Schwartz, T. W.; Malim, M. H.; Hoxie, J. A.; Marsh, M. Differential Regulation of CXCR4 and CCR5 Endocytosis. J. Cell Sci. 1998, 111, 2819–2830. [Google Scholar] [CrossRef]
- Marchese, A.; Chen, C.; Kim, Y.-M.; Benovic, J. L. The Ins and Outs of G Protein-Coupled Receptor Trafficking. Trends Biochem. Sci. 2003, 28, 369–376. [Google Scholar] [CrossRef]
- Signoret, N.; Oldridge, J.; Pelchen-Matthews, A.; Klasse, P. J.; Tran, T.; Brass, L. F.; Rosenkilde, M. M.; Schwartz, T. W.; Holmes, W.; Dallas, W.; Luther, M. A.; Wells, T. N. C.; Hoxie, J. A.; Marsh, M. Phorbol Esters and SDF-1 Induce Rapid Endocytosis and Down Modulation of the Chemokine Receptor CXCR4. J. Cell Biol. 1997, 139, 651–664. [Google Scholar] [CrossRef]
- Marchese, A.; Raiborg, C.; Santini, F.; Keen, J. H.; Stenmark, H.; Benovic, J. L. The E3 Ubiquitin Ligase AIP4 Mediates Ubiquitination and Sorting of the G Protein-Coupled Receptor CXCR4. Dev. Cell 2003, 5, 709–722. [Google Scholar] [CrossRef]
- Burger, J. A.; Burger, M.; Kipps, T. J. Chronic Lymphocytic Leukemia B Cells Express Functional CXCR4 Chemokine Receptors That Mediate Spontaneous Migration beneath Bone Marrow Stromal Cells. Blood 1999, 94, 3658–3667. [Google Scholar] [CrossRef]
- Balkwill, F. Cancer and the Chemokine Network. Nat. Rev. Cancer 2004, 4, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Drury, L. J.; Ziarek, J. J.; Gravel, S.; Veldkamp, C. T.; Takekoshi, T.; Hwang, S. T.; Heveker, N.; Volkman, B. F.; Dwinell, M. B. Monomeric and Dimeric CXCL12 Inhibit Metastasis through Distinct CXCR4 Interactions and Signaling Pathways. Proc. Natl. Acad. Sci. U. S. A. 2011, 108. 17655. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Takeuchi, H.; Lam, S. T.; Turner, R. R.; Wang, H.-J.; Kuo, C.; Foshag, L.; Bilchik, A. J.; Hoon, D. S. B. Chemokine Receptor CXCR4 Expression in Colorectal Cancer Patients Increases the Risk for Recurrence and for Poor Survival. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 2744–2753. [Google Scholar] [CrossRef]
- Scala, S.; Ottaiano, A.; Ascierto, P. A.; Cavalli, M.; Simeone, E.; Giuliano, P.; Napolitano, M.; Franco, R.; Botti, G.; Castello, G. Expression of CXCR4 Predicts Poor Prognosis in Patients with Malignant Melanoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2005, 11, 1835–1841. [Google Scholar] [CrossRef]
- Zhao, H.; Guo, L.; Zhao, H.; Zhao, J.; Weng, H.; Zhao, B. CXCR4 Over-Expression and Survival in Cancer: A System Review and Meta-Analysis. Oncotarget 2014, 6, 5022–5040. [Google Scholar] [CrossRef]
- Marquardt, A.; Hartrampf, P.; Kollmannsberger, P.; Solimando, A. G.; Meierjohann, S.; Kübler, H.; Bargou, R.; Schilling, B.; Serfling, S. E.; Buck, A.; Werner, R. A.; Lapa, C.; Krebs, M. Predicting Microenvironment in CXCR4- and FAP-Positive Solid Tumors—A Pan-Cancer Machine Learning Workflow for Theranostic Target Structures. Cancers 2023, 15. (2), 392. [Google Scholar] [CrossRef]
- Janowski, M. Functional Diversity of SDF-1 Splicing Variants. Cell Adhes. Migr. 2009, 3, 243–249. [Google Scholar] [CrossRef]
- Müller, A.; Homey, B.; Soto, H.; Ge, N.; Catron, D.; Buchanan, M. E.; McClanahan, T.; Murphy, E.; Yuan, W.; Wagner, S. N.; Barrera, J. L.; Mohar, A.; Verástegui, E.; Zlotnik, A. Involvement of Chemokine Receptors in Breast Cancer Metastasis. Nature 2001, 410, 50–56. [Google Scholar] [CrossRef]
- Chow, M. T.; Luster, A. D. Chemokines in Cancer. Cancer Immunol. Res. 2014, 2, 1125–1131. [Google Scholar] [CrossRef]
- Darash-Yahana, M.; Pikarsky, E.; Abramovitch, R.; Zeira, E.; Pal, B.; Karplus, R.; Beider, K.; Avniel, S.; Kasem, S.; Galun, E.; Peled, A. Role of High Expression Levels of CXCR4 in Tumor Growth, Vascularization, and Metastasis. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2004, 18, 1240–1242. [Google Scholar] [CrossRef]
- Thiery, J. P. Epithelial-Mesenchymal Transitions in Tumour Progression. Nat. Rev. Cancer 2002, 2, 442–454. [Google Scholar] [CrossRef]
- Bockhorn, J.; Dalton, R.; Nwachukwu, C.; Huang, S.; Prat, A.; Yee, K.; Chang, Y.-F.; Huo, D.; Wen, Y.; Swanson, K. E.; Qiu, T.; Lu, J.; Park, S. Y.; Dolan, M. E.; Perou, C. M.; Olopade, O. I.; Clarke, M. F.; Greene, G. L.; Liu, H. MicroRNA-30c Inhibits Human Breast Tumour Chemotherapy Resistance by Regulating TWF1 and IL-11. Nat. Commun. 2013, 4, 1393. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.-Y. G.; Chung, L. W. K. RANK-Mediated Signaling Network and Cancer Metastasis. Cancer Metastasis Rev. 2014, 33, 497–509. [Google Scholar] [CrossRef]
- Zhu, Y.; Yang, P.; Wang, Q.; Hu, J.; Xue, J.; Li, G.; Zhang, G.; Li, X.; Li, W.; Zhou, C.; Zhao, M.; Wang, D. The Effect of CXCR4 Silencing on Epithelial-Mesenchymal Transition Related Genes in Glioma U87 Cells. Anat. Rec. Hoboken NJ 2007 2013, 296, 1850–1856. [Google Scholar] [CrossRef]
- Cives, M.; Rizzo, F.; Simone, V.; Bisceglia, F.; Stucci, S.; Seeber, A.; Spizzo, G.; Montrone, T.; Resta, L.; Silvestris, F. Reviewing the Osteotropism in Neuroendocrine Tumors: The Role of Epithelial-Mesenchymal Transition. Neuroendocrinology 2016, 103, (3–4). [Google Scholar] [CrossRef]
- Mehrpouri, M. The Contributory Roles of the CXCL12/CXCR4/CXCR7 Axis in Normal and Malignant Hematopoiesis: A Possible Therapeutic Target in Hematologic Malignancies. Eur. J. Pharmacol. 2022, 920, 174831. [Google Scholar] [CrossRef]
- Nagasawa, T.; Hirota, S.; Tachibana, K.; Takakura, N.; Nishikawa, S.; Kitamura, Y.; Yoshida, N.; Kikutani, H.; Kishimoto, T. Defects of B-Cell Lymphopoiesis and Bone-Marrow Myelopoiesis in Mice Lacking the CXC Chemokine PBSF/SDF-1. Nature 1996, 382, 635–638. [Google Scholar] [CrossRef]
- Ma, Q.; Jones, D.; Borghesani, P. R.; Segal, R. A.; Nagasawa, T.; Kishimoto, T.; Bronson, R. T.; Springer, T. A. Impaired B-Lymphopoiesis, Myelopoiesis, and Derailed Cerebellar Neuron Migration in CXCR4- and SDF-1-Deficient Mice. Proc. Natl. Acad. Sci. U. S. A. 1998, 95, 9448–9453. [Google Scholar] [CrossRef]
- Zou, Y. R.; Kottmann, A. H.; Kuroda, M.; Taniuchi, I.; Littman, D. R. Function of the Chemokine Receptor CXCR4 in Haematopoiesis and in Cerebellar Development. Nature 1998, 393, 595–599. [Google Scholar] [CrossRef]
- Wright, D. E.; Bowman, E. P.; Wagers, A. J.; Butcher, E. C.; Weissman, I. L. Hematopoietic Stem Cells Are Uniquely Selective in Their Migratory Response to Chemokines. J. Exp. Med. 2002, 195, 1145–1154. [Google Scholar] [CrossRef]
- Aiuti, A.; Webb, I. J.; Bleul, C.; Springer, T.; Gutierrez-Ramos, J. C. The Chemokine SDF-1 Is a Chemoattractant for Human CD34+ Hematopoietic Progenitor Cells and Provides a New Mechanism to Explain the Mobilization of CD34+ Progenitors to Peripheral Blood. J. Exp. Med. 1997, 185, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Peled, A.; Grabovsky, V.; Habler, L.; Sandbank, J.; Arenzana-Seisdedos, F.; Petit, I.; Ben-Hur, H.; Lapidot, T.; Alon, R. The Chemokine SDF-1 Stimulates Integrin-Mediated Arrest of CD34(+) Cells on Vascular Endothelium under Shear Flow. J. Clin. Invest. 1999, 104, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, Y. M. Use of Plerixafor for Stem Cell Mobilization in the Setting of Autologous and Allogeneic Stem Cell Transplantations: An Update. J. Blood Med. 2021, 12, 403–412. [Google Scholar] [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J. C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Das, S.; Dasari, A. Epidemiology, Incidence, and Prevalence of Neuroendocrine Neoplasms: Are There Global Differences? Curr. Oncol. Rep. 2021, 23. (4), 43. [Google Scholar] [CrossRef]
- Modlin, I. M.; Moss, S. F.; Chung, D. C.; Jensen, R. T.; Snyderwine, E. Priorities for Improving the Management of Gastroenteropancreatic Neuroendocrine Tumors. JNCI J. Natl. Cancer Inst. 2008, 100, 1282–1289. [Google Scholar] [CrossRef]
- Clement, D.; Ramage, J.; Srirajaskanthan, R. Update on Pathophysiology, Treatment, and Complications of Carcinoid Syndrome. J. Oncol. 2020, 2020, 8341426. [Google Scholar] [CrossRef]
- Del Olmo-Garcia, M. I.; Prado-Wohlwend, S.; Andres, A.; Soriano, J. M.; Bello, P.; Merino-Torres, J. F. Somatostatin and Somatostatin Receptors: From Signaling to Clinical Applications in Neuroendocrine Neoplasms. Biomedicines 2021, 9. (12), 1810. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.; Decristoforo, C.; Kendler, D.; Dobrozemsky, G.; Heute, D.; Uprimny, C.; Kovacs, P.; Von Guggenberg, E.; Bale, R.; Virgolini, I. J. 68Ga-DOTA-Tyr3-Octreotide PET in Neuroendocrine Tumors: Comparison with Somatostatin Receptor Scintigraphy and CT. J. Nucl. Med. 2007, 48, 508–518. [Google Scholar] [CrossRef]
- Rinke, A.; Müller, H.-H.; Schade-Brittinger, C.; Klose, K.-J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.-F.; Bläker, M.; Harder, J.; Arnold, C.; Gress, T.; Arnold, R.; PROMID Study Group. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors: A Report from the PROMID Study Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef]
- Caplin, M. E.; Pavel, M.; Ćwikła, J. B.; Phan, A. T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E. M.; Capdevila, J.; Wall, L.; Rindi, G.; Langley, A.; Martinez, S.; Blumberg, J.; Ruszniewski, P.; CLARINET Investigators. Lanreotide in Metastatic Enteropancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef]
- Baudin, E.; Horsch, D.; Singh, S.; Caplin, M. E.; Ferone, D.; Wolin, E. M.; Capdevila, J.; Buikhuisen, W. A.; Raderer, M.; Dansin, E.; Grohe, C.; Houchard, A.; Thanh, X.-M. T.; Reidy-Lagunes, D. 1096O Lanreotide Autogel/Depot (LAN) in Patients with Advanced Bronchopulmonary (BP) Neuroendocrine Tumors (NETs): Results from the Phase III SPINET Study. Ann. Oncol. 2021, 32, S906. [Google Scholar] [CrossRef]
- Nagtegaal, I. D.; Odze, R. D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K. M.; Carneiro, F.; Cree, I. A.; WHO Classification of Tumours Editorial Board. The 2019 WHO Classification of Tumours of the Digestive System. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Travis, W. D.; Brambilla, E.; Nicholson, A. G.; Yatabe, Y.; Austin, J. H. M.; Beasley, M. B.; Chirieac, L. R.; Dacic, S.; Duhig, E.; Flieder, D. B.; Geisinger, K.; Hirsch, F. R.; Ishikawa, Y.; Kerr, K. M.; Noguchi, M.; Pelosi, G.; Powell, C. A.; Tsao, M. S.; Wistuba, I.; WHO Panel. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Corleto, V. D.; Falconi, M.; Panzuto, F.; Milione, M.; De Luca, O.; Perri, P.; Cannizzaro, R.; Bordi, C.; Pederzoli, P.; Scarpa, A.; Delle Fave, G. Somatostatin Receptor Subtypes 2 and 5 Are Associated with Better Survival in Well-Differentiated Endocrine Carcinomas. Neuroendocrinology 2009, 89, 223–230. [Google Scholar] [CrossRef]
- Zamora, V.; Cabanne, A.; Salanova, R.; Bestani, C.; Domenichini, E.; Marmissolle, F.; Giacomi, N.; O’Connor, J.; Méndez, G.; Roca, E.; Buenos Aires and La Plata Argentina Argentum Working Group. Immunohistochemical Expression of Somatostatin Receptors in Digestive Endocrine Tumours. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2010, 42, 220–225. [Google Scholar] [CrossRef]
- Okuwaki, K.; Kida, M.; Mikami, T.; Yamauchi, H.; Imaizumi, H.; Miyazawa, S.; Iwai, T.; Takezawa, M.; Saegusa, M.; Watanabe, M.; Koizumi, W. Clinicopathologic Characteristics of Pancreatic Neuroendocrine Tumors and Relation of Somatostatin Receptor Type 2A to Outcomes. Cancer 2013, 119, 4094–4102. [Google Scholar] [CrossRef]
- Qian, Z. R.; Li, T.; Ter-Minassian, M.; Yang, J.; Chan, J. A.; Brais, L. K.; Masugi, Y.; Thiaglingam, A.; Brooks, N.; Nishihara, R.; Bonnemarie, M.; Masuda, A.; Inamura, K.; Kim, S. A.; Mima, K.; Sukawa, Y.; Dou, R.; Lin, X.; Christiani, D. C.; Schmidlin, F.; Fuchs, C. S.; Mahmood, U.; Ogino, S.; Kulke, M. H. Association Between Somatostatin Receptor Expression and Clinical Outcomes in Neuroendocrine Tumors. Pancreas 2016, 45, 1386–1393. [Google Scholar] [CrossRef]
- Mehta, S.; de Reuver, P. R.; Gill, P.; Andrici, J.; D’Urso, L.; Mittal, A.; Pavlakis, N.; Clarke, S.; Samra, J. S.; Gill, A. J. Somatostatin Receptor SSTR-2a Expression Is a Stronger Predictor for Survival Than Ki-67 in Pancreatic Neuroendocrine Tumors. Medicine (Baltimore) 2015, 94. (40), e1281.. [Google Scholar] [CrossRef]
- Song, K. B.; Kim, S. C.; Kim, J. H.; Seo, D.-W.; Hong, S.-M.; Park, K.-M.; Hwang, D. W.; Lee, J. H.; Lee, Y.-J. Prognostic Value of Somatostatin Receptor Subtypes in Pancreatic Neuroendocrine Tumors. Pancreas 2016, 45, 187–192. [Google Scholar] [CrossRef]
- Circelli, L.; Sciammarella, C.; Guadagno, E.; Tafuto, S.; Del Basso De Caro, M.; Botti, G.; Pezzullo, L.; Aria, M.; Ramundo, V.; Tatangelo, F.; Losito, N. S.; Ieranò, C.; D’Alterio, C.; Izzo, F.; Ciliberto, G.; Colao, A.; Faggiano, A.; Scala, S. CXCR4/CXCL12/CXCR7 Axis Is Functional in Neuroendocrine Tumors and Signals on mTOR. Oncotarget 2016, 7, 18865–18875. [Google Scholar] [CrossRef] [PubMed]
- Yao, J. C.; Lombard-Bohas, C.; Baudin, E.; Kvols, L. K.; Rougier, P.; Ruszniewski, P.; Hoosen, S.; St Peter, J.; Haas, T.; Lebwohl, D.; Van Cutsem, E.; Kulke, M. H.; Hobday, T. J.; O’Dorisio, T. M.; Shah, M. H.; Cadiot, G.; Luppi, G.; Posey, J. A.; Wiedenmann, B. Daily Oral Everolimus Activity in Patients with Metastatic Pancreatic Neuroendocrine Tumors after Failure of Cytotoxic Chemotherapy: A Phase II Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M. E.; Hainsworth, J. D.; Baudin, E.; Peeters, M.; Hörsch, D.; Winkler, R. E.; Klimovsky, J.; Lebwohl, D.; Jehl, V.; Wolin, E. M.; Öberg, K.; Cutsem, E. V.; Yao, J. C. Everolimus plus Octreotide Long-Acting Repeatable for the Treatment of Advanced Neuroendocrine Tumours Associated with Carcinoid Syndrome (RADIANT-2): A Randomised, Placebo-Controlled, Phase 3 Study. The Lancet 2011, 378, 2005–2012. [Google Scholar] [CrossRef] [PubMed]
- Korbecki, J.; Simińska, D.; Gąssowska-Dobrowolska, M.; Listos, J.; Gutowska, I.; Chlubek, D.; Baranowska-Bosiacka, I. Chronic and Cycling Hypoxia: Drivers of Cancer Chronic Inflammation through HIF-1 and NF-κB Activation: A Review of the Molecular Mechanisms. Int. J. Mol. Sci. 2021, 22. (19), 10701.. [Google Scholar] [CrossRef] [PubMed]
- Albadari, N.; Deng, S.; Li, W. The Transcriptional Factors HIF-1 and HIF-2 and Their Novel Inhibitors in Cancer Therapy. Expert Opin. Drug Discov. 2019, 14, 667–682. [Google Scholar] [CrossRef] [PubMed]
- Wicks, E. E.; Semenza, G. L. Hypoxia-Inducible Factors: Cancer Progression and Clinical Translation. J. Clin. Invest. 2022, 132. (11), e159839. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Xiang, R.; Dai, J.; Wang, Y.; Xu, Z. HIF-1α Mediates CXCR4 Transcription to Activate the AKT/mTOR Signaling Pathway and Augment the Viability and Migration of Activated B Cell-like Diffuse Large B-Cell Lymphoma Cells. Mol. Carcinog. 2023, 62, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Cai, C.; Zhao, G.; Qiu, X.; Zhao, H.; Ma, Q.; Tian, L.; Li, X.; Hu, Y.; Liao, B.; Ma, B.; Fan, Q. Hypoxia Promotes Migration and Induces CXCR4 Expression via HIF-1α Activation in Human Osteosarcoma. PloS One 2014, 9. (3), e90518. [Google Scholar] [CrossRef] [PubMed]
- Arvidsson, Y.; Bergström, A.; Arvidsson, L.; Kristiansson, E.; Ahlman, H.; Nilsson, O. Hypoxia Stimulates CXCR4 Signalling in Ileal Carcinoids. Endocr. Relat. Cancer 2010, 17, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, L.; Bacha, D.; Rebours, V.; Mebarki, M.; Bretagnol, F.; Panis, Y.; Bedossa, P.; Ruszniewski, P.; Couvelard, A. The Expression of the Hypoxia Markers CA9 and CXCR4 Is Correlated with Survival in Patients with Neuroendocrine Tumours of the Ileum. Neuroendocrinology 2012, 95, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Kaemmerer, D.; Träger, T.; Hoffmeister, M.; Sipos, B.; Hommann, M.; Sänger, J.; Schulz, S.; Lupp, A. Inverse Expression of Somatostatin and CXCR4 Chemokine Receptors in Gastroenteropancreatic Neuroendocrine Neoplasms of Different Malignancy. Oncotarget 2015, 6, 27566–27579. [Google Scholar] [CrossRef]
- Mai, R.; Kaemmerer, D.; Träger, T.; Neubauer, E.; Sänger, J.; Baum, R. P.; Schulz, S.; Lupp, A. Different Somatostatin and CXCR4 Chemokine Receptor Expression in Gastroenteropancreatic Neuroendocrine Neoplasms Depending on Their Origin. Sci. Rep. 2019, 9. (1), 4339. [Google Scholar] [CrossRef]
- Discipline of Morphopathology, Department of Microscopic Morphology, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Anapatmol Research Center, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Popa, O. ; Tăban, S. M.; Discipline of Morphopathology, Department of Microscopic Morphology, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Anapatmol Research Center, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Dema, A. L. C.; Discipline of Morphopathology, Department of Microscopic Morphology, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Anapatmol Research Center, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Plopeanu, A. D.; Department of Pathology, Pius Brînzeu Emergency County Hospital, Timişoara, Romania; Barna, R. A.; Anapatmol Research Center, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Discipline of Gastroenterology and Hepatology, Department of Internal Medicine II, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Cornianu, M.; Discipline of Morphopathology, Department of Microscopic Morphology, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Anapatmol Research Center, Victor Babeş University of Medicine and Pharmacy, Timişoara, Romania; Dema, S.; Service of Radiotherapy, Emergency City Hospital, Timişoara, Romania. Immunohistochemical Expression of Chemokine Receptor in Neuroendocrine Neoplasms (CXCR4) of the Gastrointestinal Tract: A Retrospective Study of 71 Cases. Rom. J. Morphol. Embryol. 2021, 62, 151–157. [Google Scholar] [CrossRef]
- Kaemmerer, D.; Reimann, C.; Specht, E.; Wirtz, R. M.; Sayeg, M.; Baum, R. P.; Schulz, S.; Lupp, A. Differential Expression and Prognostic Value of the Chemokine Receptor CXCR4 in Bronchopulmonary Neuroendocrine Neoplasms. Oncotarget 2015, 6, 3346–3358. [Google Scholar] [CrossRef] [PubMed]
- Lambert, A. W.; Pattabiraman, D. R.; Weinberg, R. A. Emerging Biological Principles of Metastasis. Cell 2017, 168, 670–691. [Google Scholar] [CrossRef] [PubMed]
- Galván, J. A.; Astudillo, A.; Vallina, A.; Crespo, G.; Folgueras, M. V.; González, M. V. Prognostic and Diagnostic Value of Epithelial to Mesenchymal Transition Markers in Pulmonary Neuroendocrine Tumors. BMC Cancer 2014, 14. (1), 855. [Google Scholar] [CrossRef] [PubMed]
- Galván, J. A.; Astudillo, A.; Vallina, A.; Fonseca, P. J.; Gómez-Izquierdo, L.; García-Carbonero, R.; González, M. V. Epithelial-Mesenchymal Transition Markers in the Differential Diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Am. J. Clin. Pathol. 2013, 140, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Fendrich, V.; Maschuw, K.; Waldmann, J.; Buchholz, M.; Rehm, J.; Gress, T. M.; Bartsch, D. K.; König, A. Epithelial-Mesenchymal Transition Is a Critical Step in Tumorgenesis of Pancreatic Neuroendocrine Tumors. Cancers 2012, 4, 281–294. [Google Scholar] [CrossRef]
- Cives, M.; Quaresmini, D.; Rizzo, F. M.; Felici, C.; D’Oronzo, S.; Simone, V.; Silvestris, F. Osteotropism of Neuroendocrine Tumors: Role of the CXCL12/CXCR4 Pathway in Promoting EMT in Vitro. Oncotarget 2017, 8, 22534–22549. [Google Scholar] [CrossRef]
- Cives, M.; Pellè, E.; Rinzivillo, M.; Prosperi, D.; Tucci, M.; Silvestris, F.; Panzuto, F. Bone Metastases in Neuroendocrine Tumors: Molecular Pathogenesis and Implications in Clinical Practice. Neuroendocrinology 2021, 111, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Li, N.; Li, J.; Lu, M.; Leal, J. P.; Tan, H.; Su, H.; Fan, Y.; Zhang, Y.; Zhao, W.; Zhu, H.; Pomper, M. G.; Zhou, Y.; Yang, Z. The Correlation Between [68Ga]DOTATATE PET/CT and Cell Proliferation in Patients With GEP-NENs. Mol. Imaging Biol. 2019, 21, 984–990. [Google Scholar] [CrossRef]
- Ezziddin, S.; Adler, L.; Sabet, A.; Pöppel, T. D.; Grabellus, F.; Yüce, A.; Fischer, H.-P.; Simon, B.; Höller, T.; Biersack, H.-J.; Nagarajah, J. Prognostic Stratification of Metastatic Gastroenteropancreatic Neuroendocrine Neoplasms by 18F-FDG PET: Feasibility of a Metabolic Grading System. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2014, 55, 1260–1266. [Google Scholar] [CrossRef]
- Abgral, R.; Leboulleux, S.; Déandreis, D.; Aupérin, A.; Lumbroso, J.; Dromain, C.; Duvillard, P.; Elias, D.; De Baere, T.; Guigay, J.; Ducreux, M.; Schlumberger, M.; Baudin, E. Performance of 18Fluorodeoxyglucose-Positron Emission Tomography and Somatostatin Receptor Scintigraphy for High Ki67 (≥10%) Well-Differentiated Endocrine Carcinoma Staging. J. Clin. Endocrinol. Metab. 2011, 96, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, E. K. J.; Sturm, E. J. C.; Bombardieri, E.; Cleton, F. J.; Stokkel, M. P. M. Positron-Emission Tomography with [18F]Fluorodeoxyglucose. J. Cancer Res. Clin. Oncol. 2000, 126, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Uy, G. L.; Rettig, M. P.; Cashen, A. F. Plerixafor, a CXCR4 Antagonist for the Mobilization of Hematopoietic Stem Cells. Expert Opin. Biol. Ther. 2008, 8, 1797–1804. [Google Scholar] [CrossRef] [PubMed]
- Aghanejad, A.; Jalilian, A. R.; Fazaeli, Y.; Alirezapoor, B.; Pouladi, M.; Beiki, D.; Maus, S.; Khalaj, A. Synthesis and Evaluation of [67Ga]-AMD3100: A Novel Imaging Agent for Targeting the Chemokine Receptor CXCR4. Sci. Pharm. 2014, 82, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Gourni, E.; Demmer, O.; Schottelius, M.; D’Alessandria, C.; Schulz, S.; Dijkgraaf, I.; Schumacher, U.; Schwaiger, M.; Kessler, H.; Wester, H.-J. PET of CXCR4 Expression by a 68Ga-Labeled Highly Specific Targeted Contrast Agent. J. Nucl. Med. 2011, 52, 1803–1810. [Google Scholar] [CrossRef] [PubMed]
- Demmer, O.; Gourni, E.; Schumacher, U.; Kessler, H.; Wester, H.-J. PET Imaging of CXCR4 Receptors in Cancer by a New Optimized Ligand. ChemMedChem 2011, 6, 1789–1791. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Jüttler, S.; Müller, M.; Wester, H.-J. Cationic Eluate Pretreatment for Automated Synthesis of [68Ga]CPCR4.2. Nucl. Med. Biol. 2014, 41, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Diagnostische Leistung und Sicherheit von [68Ga]Ga-PentixaFor zur Erkennung und Lokalisation von Chemokin Rezeptor 4 (CXCR4) positiven Tumoren und Metastasen in einem PAN Cancer Ansatz: eine prospektive, multizentrische, internationale, klinische Phase III Studie, die FORPAN Studie | Cochrane Library. [CrossRef]
- Werner, R. A.; Weich, A.; Higuchi, T.; Schmid, J. S.; Schirbel, A.; Lassmann, M.; Wild, V.; Rudelius, M.; Kudlich, T.; Herrmann, K.; Scheurlen, M.; Buck, A. K.; Kropf, S.; Wester, H.-J.; Lapa, C. Imaging of Chemokine Receptor 4 Expression in Neuroendocrine Tumors - a Triple Tracer Comparative Approach. Theranostics 2017, 7, 1489–1498. [Google Scholar] [CrossRef] [PubMed]
- Werner, R. A.; Weich, A.; Schirbel, A.; Samnick, S.; Buck, A. K.; Higuchi, T.; Wester, H.-J.; Lapa, C. Intraindividual Tumor Heterogeneity in NET – Further Insight by C-X-C Motif Chemokine Receptor 4-Directed Imaging. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 553–554. [Google Scholar] [CrossRef]
- Weich, A.; Werner, R. A.; Buck, A. K.; Hartrampf, P. E.; Serfling, S. E.; Scheurlen, M.; Wester, H.-J.; Meining, A.; Kircher, S.; Higuchi, T.; Pomper, M. G.; Rowe, S. P.; Lapa, C.; Kircher, M. CXCR4-Directed PET/CT in Patients with Newly Diagnosed Neuroendocrine Carcinomas. Diagnostics 2021, 11. (4), 605.. [Google Scholar] [CrossRef]
- Watts, A.; Singh, B.; Singh, H.; Bal, A.; Kaur, H.; Dhanota, N.; Arora, S. K.; Mittal, B. R.; Behera, D. [68Ga]Ga-Pentixafor PET/CT Imaging for in Vivo CXCR4 Receptor Mapping in Different Lung Cancer Histologic Sub-Types: Correlation with Quantitative Receptors’ Density by Immunochemistry Techniques. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 1216–1227. [Google Scholar] [CrossRef]
- Lewis, R.; Habringer, S.; Kircher, M.; Hefter, M.; Peuker, C. A.; Werner, R.; Ademaj-Kospiri, V.; Gäble, A.; Weber, W.; Wester, H.-J.; Buck, A.; Herhaus, P.; Lapa, C.; Keller, U. Investigation of Spleen CXCR4 Expression by [68Ga]Pentixafor PET in a Cohort of 145 Solid Cancer Patients. EJNMMI Res. 2021, 11. (1), 77.. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Behnam Azad, B.; Nimmagadda, S. The Intricate Role of CXCR4 in Cancer. In Advances in Cancer Research; Elsevier, 2014; Vol. 124, pp 31–82. [CrossRef]
- Wang, Z.; Ma, Q. Beta-Catenin Is a Promising Key Factor in the SDF-1/CXCR4 Axis on Metastasis of Pancreatic Cancer. Med. Hypotheses 2007, 69, 816–820. [Google Scholar] [CrossRef] [PubMed]
- Kim, J. T.; Li, J.; Jang, E. R.; Gulhati, P.; Rychahou, P. G.; Napier, D. L.; Wang, C.; Weiss, H. L.; Lee, E. Y.; Anthony, L.; Townsend, C. M.; Liu, C.; Evers, B. M. Deregulation of Wnt/β-Catenin Signaling through Genetic or Epigenetic Alterations in Human Neuroendocrine Tumors. Carcinogenesis 2013, 34, 953–961. [Google Scholar] [CrossRef]
- Weich, A.; Rogoll, D.; Gawlas, S.; Mayer, L.; Weich, W.; Pongracz, J.; Kudlich, T.; Meining, A.; Scheurlen, M. Wnt/β-Catenin Signaling Regulates CXCR4 Expression and [68Ga] Pentixafor Internalization in Neuroendocrine Tumor Cells. Diagnostics 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Mayer, I. A.; Walenkamp, A. M. E.; Lapa, C.; Andreeff, M.; Bobirca, A. At the Bedside: Profiling and Treating Patients with CXCR4-Expressing Cancers. J. Leukoc. Biol. 2021, 109, 953–967. [Google Scholar] [CrossRef] [PubMed]
- Otani, Y.; Kijima, T.; Kohmo, S.; Oishi, S.; Minami, T.; Nagatomo, I.; Takahashi, R.; Hirata, H.; Suzuki, M.; Inoue, K.; Takeda, Y.; Kida, H.; Tachibana, I.; Fujii, N.; Kumanogoh, A. Suppression of Metastases of Small Cell Lung Cancer Cells in Mice by a Peptidic CXCR4 Inhibitor TF14016. FEBS Lett. 2012, 586, 3639–3644. [Google Scholar] [CrossRef] [PubMed]
- Salgia, R.; Stille, J. R.; Weaver, R. W.; McCleod, M.; Hamid, O.; Polzer, J.; Roberson, S.; Flynt, A.; Spigel, D. R. A Randomized Phase II Study of LY2510924 and Carboplatin/Etoposide versus Carboplatin/Etoposide in Extensive-Disease Small Cell Lung Cancer. Lung Cancer Amst. Neth. 2017, 105, 7–13. [Google Scholar] [CrossRef]
- Robinson, T.; Escara-Wilke, J.; Dai, J.; Zimmermann, J.; Keller, E. T. A CXCR4 Inhibitor (Balixafortide) Enhances Docetaxel-Mediated Antitumor Activity in a Murine Model of Prostate Cancer Bone Metastasis. The Prostate 2023, 83, 1247–1254. [Google Scholar] [CrossRef]
- Bockorny, B.; Macarulla, T.; Semenisty, V.; Borazanci, E.; Feliu, J.; Ponz-Sarvise, M.; Abad, D. G.; Oberstein, P.; Alistar, A.; Muñoz, A.; Geva, R.; Guillén-Ponce, C.; Fernandez, M. S.; Peled, A.; Chaney, M.; Gliko-Kabir, I.; Shemesh-Darvish, L.; Ickowicz, D.; Sorani, E.; Kadosh, S.; Vainstein-Haras, A.; Hidalgo, M. Motixafortide and Pembrolizumab Combined to Nanoliposomal Irinotecan, Fluorouracil, and Folinic Acid in Metastatic Pancreatic Cancer: The COMBAT/KEYNOTE-202 Trial. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2021, 27, 5020–5027. [Google Scholar] [CrossRef]
- Andtbacka, R. H. I.; Wang, Y.; Pierce, R. H.; Campbell, J. S.; Yushak, M.; Milhem, M.; Ross, M.; Niland, K.; Arbeit, R. D.; Parasuraman, S.; Bickley, K.; Yeung, C. C.; Aicher, L. D.; Smythe, K. S.; Gan, L. Mavorixafor, an Orally Bioavailable CXCR4 Antagonist, Increases Immune Cell Infiltration and Inflammatory Status of Tumor Microenvironment in Patients with Melanoma. Cancer Res. Commun. 2022, 2, 904–913. [Google Scholar] [CrossRef] [PubMed]
- Karpova, D.; Bräuninger, S.; Wiercinska, E.; Krämer, A.; Stock, B.; Graff, J.; Martin, H.; Wach, A.; Escot, C.; Douglas, G.; Romagnoli, B.; Chevalier, E.; Dembowski, K.; Hooftman, L.; Bonig, H. Mobilization of Hematopoietic Stem Cells with the Novel CXCR4 Antagonist POL6326 (Balixafortide) in Healthy Volunteers-Results of a Dose Escalation Trial. J. Transl. Med. 2017, 15. (1), 2. [Google Scholar] [CrossRef] [PubMed]
- Crees, Z. D.; Rettig, M. P.; Jayasinghe, R. G.; Stockerl-Goldstein, K.; Larson, S. M.; Arpad, I.; Milone, G. A.; Martino, M.; Stiff, P.; Sborov, D.; Pereira, D.; Micallef, I.; Moreno-Jiménez, G.; Mikala, G.; Coronel, M. L. P.; Holtick, U.; Hiemenz, J.; Qazilbash, M. H.; Hardy, N.; Latif, T.; García-Cadenas, I.; Vainstein-Haras, A.; Sorani, E.; Gliko-Kabir, I.; Goldstein, I.; Ickowicz, D.; Shemesh-Darvish, L.; Kadosh, S.; Gao, F.; Schroeder, M. A.; Vij, R.; DiPersio, J. F. Motixafortide and G-CSF to Mobilize Hematopoietic Stem Cells for Autologous Transplantation in Multiple Myeloma: A Randomized Phase 3 Trial. Nat. Med. 2023, 29, 869–879. [Google Scholar] [CrossRef] [PubMed]
- Badolato, R.; Donadieu, J. Results of a Phase 3 Trial of an Oral CXCR4 Antagonist, Mavorixafor, for Treatment of Patients With WHIM Syndrome. Clin. Immunol. 2023, 250, 109349. [Google Scholar] [CrossRef]
- Bobkov, V.; Arimont, M.; Zarca, A.; De Groof, T. W. M.; Van Der Woning, B.; De Haard, H.; Smit, M. J. Antibodies Targeting Chemokine Receptors CXCR4 and ACKR3. Mol. Pharmacol. 2019, 96, 753–764. [Google Scholar] [CrossRef] [PubMed]
- Pellé, E.; Cives, M.; Quaresmini, D.; Lovero, D.; Felici, C.; Cafforio, P.; Palmirotta, R.; Silvestris, F. CXCR4 Inhibition by Ulocuplumab Prevents EMT of pNET Cells in Vitro. Ann. Oncol. 2017, 28, v154–v155. [Google Scholar] [CrossRef]
- Si, Y.; Guan, J.; Xu, Y.; Chen, K.; Kim, S.; Zhou, L.; Jaskula-Sztul, R.; Liu, X. M. Dual-Targeted Extracellular Vesicles to Facilitate Combined Therapies for Neuroendocrine Cancer Treatment. Pharmaceutics 2020, 12. (11), 1079. [Google Scholar] [CrossRef] [PubMed]
- Sabet, A.; Mader, N.; Bittenbring, J. T.; Khreish, F.; Grünwald, F.; Biersack, H. J.; Ezziddin, S. Prophylactic Peripheral Blood Stem Cell Collection in Patients with Extensive Bone-Marrow Infiltration of Neuroendocrine Tumours Prior to Peptide Receptor Radionuclide Therapy with 177Lu-DOTATATE. Pharmaceuticals 2021, 14. (10), 1022.. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P. L.; Kulke, M. H.; Jacene, H.; Bushnell, D.; O’Dorisio, T. M.; Baum, R. P.; Kulkarni, H. R.; Caplin, M.; Lebtahi, R.; Hobday, T.; Delpassand, E.; Van Cutsem, E.; Benson, A.; Srirajaskanthan, R.; Pavel, M.; Mora, J.; Berlin, J.; Grande, E.; Reed, N.; Seregni, E.; Öberg, K.; Lopera Sierra, M.; Santoro, P.; Thevenet, T.; Erion, J. L.; Ruszniewski, P.; Kwekkeboom, D.; Krenning, E.; NETTER-1 Trial Investigators. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Strosberg, J. R.; Caplin, M. E.; Kunz, P. L.; Ruszniewski, P. B.; Bodei, L.; Hendifar, A.; Mittra, E.; Wolin, E. M.; Yao, J. C.; Pavel, M. E.; Grande, E.; Van Cutsem, E.; Seregni, E.; Duarte, H.; Gericke, G.; Bartalotta, A.; Mariani, M. F.; Demange, A.; Mutevelic, S.; Krenning, E. P.; NETTER-1 investigators. 177Lu-Dotatate plus Long-Acting Octreotide versus High-dose Long-Acting Octreotide in Patients with Midgut Neuroendocrine Tumours (NETTER-1): Final Overall Survival and Long-Term Safety Results from an Open-Label, Randomised, Controlled, Phase 3 Trial. Lancet Oncol. 2021, 22, 1752–1763. [Google Scholar] [CrossRef]
- Poschenrieder, A.; Schottelius, M.; Schwaiger, M.; Kessler, H.; Wester, H.-J. The Influence of Different Metal-Chelate Conjugates of Pentixafor on the CXCR4 Affinity. EJNMMI Res. 2016, 6. (1), 36.. [Google Scholar] [CrossRef] [PubMed]
- Schottelius, M.; Osl, T.; Poschenrieder, A.; Hoffmann, F.; Beykan, S.; Hänscheid, H.; Schirbel, A.; Buck, A. K.; Kropf, S.; Schwaiger, M.; Keller, U.; Lassmann, M.; Wester, H.-J. [177Lu]Pentixather: Comprehensive Preclinical Characterization of a First CXCR4-Directed Endoradiotherapeutic Agent. Theranostics 2017, 7, 2350–2362. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, K.; Schottelius, M.; Lapa, C.; Osl, T.; Poschenrieder, A.; Hänscheid, H.; Lückerath, K.; Schreder, M.; Bluemel, C.; Knott, M.; Keller, U.; Schirbel, A.; Samnick, S.; Lassmann, M.; Kropf, S.; Buck, A. K.; Einsele, H.; Wester, H.-J.; Knop, S. First-in-Human Experience of CXCR4-Directed Endoradiotherapy with 177Lu- and 90Y-Labeled Pentixather in Advanced-Stage Multiple Myeloma with Extensive Intra- and Extramedullary Disease. J. Nucl. Med. 2016, 57, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Lapa, C.; Kircher, S.; Schirbel, A.; Rosenwald, A.; Kropf, S.; Pelzer, T.; Walles, T.; Buck, A. K.; Weber, W. A.; Wester, H.-J.; Herrmann, K.; Lückerath, K. Targeting CXCR4 with [68Ga]Pentixafor: A Suitable Theranostic Approach in Pleural Mesothelioma? Oncotarget 2017, 8, 96732–96737. [Google Scholar] [CrossRef] [PubMed]
- Lapa, C.; Hänscheid, H.; Kircher, M.; Schirbel, A.; Wunderlich, G.; Werner, R. A.; Samnick, S.; Kotzerke, J.; Einsele, H.; Buck, A. K.; Wester, H.-J.; Grigoleit, G. U. Feasibility of CXCR4-Directed Radioligand Therapy in Advanced Diffuse Large B-Cell Lymphoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2019, 60, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Habringer, S.; Lapa, C.; Herhaus, P.; Schottelius, M.; Istvanffy, R.; Steiger, K.; Slotta-Huspenina, J.; Schirbel, A.; Hänscheid, H.; Kircher, S.; Buck, A. K.; Götze, K.; Vick, B.; Jeremias, I.; Schwaiger, M.; Peschel, C.; Oostendorp, R.; Wester, H.-J.; Grigoleit, G.-U.; Keller, U. Dual Targeting of Acute Leukemia and Supporting Niche by CXCR4-Directed Theranostics. Theranostics 2018, 8, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S. M.; Wesseling, P.; de Keizer, B.; Tolboom, N.; Ververs, F. F. T.; Krijger, G. C.; Westerman, B. A.; Snijders, T. J.; Robe, P. A.; van der Kolk, A. G. CXCR4 Expression in Glioblastoma Tissue and the Potential for PET Imaging and Treatment with [68Ga]Ga-Pentixafor /[177Lu]Lu-Pentixather. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 481–491. [Google Scholar] [CrossRef] [PubMed]
- Fath, M. A.; Liu, D.; Ewald, J. T.; Robles-Planells, C.; Tomanek-Chalkley, A. M.; Graves, S. A.; Howe, J. R.; O’Dorisio, T. M.; Rastogi, P.; Bellizzi, A. M.; O’Dorisio, M. S.; Menda, Y.; Spitz, D. R. Chemokine Receptor CXCR4 Radioligand Targeted Therapy Using 177Lutetium-Pentixather for Pulmonary Neuroendocrine Cancers. Radiat. Res. 2023, 201, 35–47. [Google Scholar] [CrossRef]
- Fath, M. A.; Liu, D.; Robles-Planells, C.; Ewald, J. T.; Christensen, K. A.; Johnson, S. S.; Graves, S. A.; Spitz, D. R.; Menda, Y.; Sue O’Dorisio, M. Abstract 5034: Targeting CXCR4 and Thioredoxin Reductase in High Grade Neuroendocrine Tumors and Neuroendocrine Carcinomas. Cancer Res. 2023, 83. (7_Supplement),5034. [Google Scholar] [CrossRef]
Figure 1.
Representation of the signaling pathway in the activation of CXCR4 (left) and ACKR3 (right). Blue arrows mean activation while red arrows represent metabolic pathway inhibition. Note that G proteins and calcium do not participate as second messengers after binding CXCL12 to ACKR3. Acronyms: C-X-C motif chemokine ligand 12 (CXCL12), chemokine C-X-C motif receptor 4 (CXCR4), atypical cytokine receptor type 3 (ACKR3), protein kinase C (PKC), adenylate cyclase (AC), adenosine 3′,5′-cyclic monophosphate (cAMP), extracellular signal-regulated kinases (ERK), mitogen-activated protein kinase (MAPK), diacylglycerol (DAG), inositol-(1,4,5)-triphosphate (IP3), phosphatidylinositol triphosphate (PIP3), phospholipase C (PLC), mammalian target of rapamycin (mTOR), endoplasmic reticulum (ER).
Figure 1.
Representation of the signaling pathway in the activation of CXCR4 (left) and ACKR3 (right). Blue arrows mean activation while red arrows represent metabolic pathway inhibition. Note that G proteins and calcium do not participate as second messengers after binding CXCL12 to ACKR3. Acronyms: C-X-C motif chemokine ligand 12 (CXCL12), chemokine C-X-C motif receptor 4 (CXCR4), atypical cytokine receptor type 3 (ACKR3), protein kinase C (PKC), adenylate cyclase (AC), adenosine 3′,5′-cyclic monophosphate (cAMP), extracellular signal-regulated kinases (ERK), mitogen-activated protein kinase (MAPK), diacylglycerol (DAG), inositol-(1,4,5)-triphosphate (IP3), phosphatidylinositol triphosphate (PIP3), phospholipase C (PLC), mammalian target of rapamycin (mTOR), endoplasmic reticulum (ER).
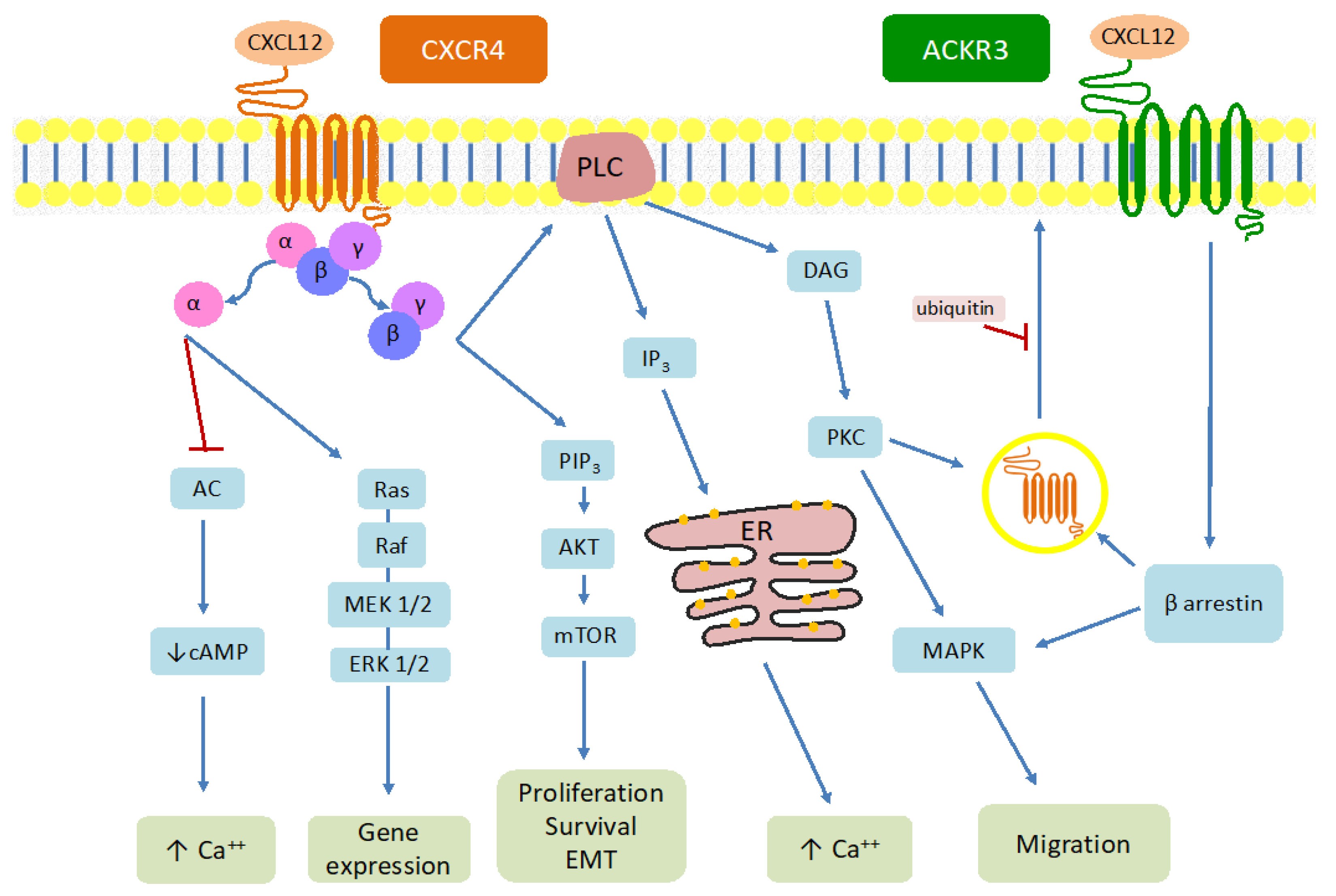
Figure 2.
Schematic representation that summarizes the future of CXCR4 as a target in NENs, both diagnostic and therapeutic approaches. Acronyms: chemokine C-X-C motif receptor 4 (CXCR4), neuroendocrine neoplasms (NENs), peptide receptor radionuclide therapy (PRRT), Gallium (Ga), Plumb (Pb), Lutetium (Lu).
Figure 2.
Schematic representation that summarizes the future of CXCR4 as a target in NENs, both diagnostic and therapeutic approaches. Acronyms: chemokine C-X-C motif receptor 4 (CXCR4), neuroendocrine neoplasms (NENs), peptide receptor radionuclide therapy (PRRT), Gallium (Ga), Plumb (Pb), Lutetium (Lu).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



