
Submitted:
14 April 2024
Posted:
15 April 2024
You are already at the latest version
Abstract
Same-day desensitization (SDD) is a procedure in which desensitization to the drug suspected of causing the hypersensitivity reaction (HR) is performed on the same day as the patient's reaction. In rapid drug desensitization (RDD), desensitization to the suspected drug is performed after an allergological study. The aim of the study was to analyze the diagnostic capacity of the allergist in Oncology Day Hospital (ODH) to establish the phenotype of the HR, in the context of SDD, based exclusively on clinical biomarkers. This is a study of patients treated with desensitization on the same day they had a HR. Later an allergological study (clinical history, skin test, risk assessment, serological biomarkers, drug provocation test if applicable) was performed prior to the following administrations. A total of 35 successful SDDs were performed. A high concordance (91.5% of patients) was found between the phenotype suspected by the allergist after the initial assessment of the patient prior to SDD and the final phenotype after subsequent allergological study performed in the Allergy Department. The presence of the allergist at the ODH allows, in addition to initial treatment according to phenotype, desensitization on the day of the reaction. This will lead to personalized and precision allergology.
Keywords:
drug allergy
; rapid drug desensitization
; same‐day desensitization
; chemotherapy allergy
; personalized & precision medicine
Introduction
The last years have witnessed the birth of precision oncology due to greater knowledge of tumor biology and the development of new antineoplastic drugs. This has provided greater benefits for oncology patients, duplicating their survival compared to that of classic drugs [1,2]. One of the main problems that arise during this pharmacological evolution are treatment toxicities [3], among in which it could be included hypersensitivity reactions (HRs). The oncologic patient who interrupts the treatment regimen because of a HR is likely to experience a reduction in survival. In many cases, this "failure" is an added condition to their disease, with the negative clinical and emotional repercussions that this entails [4].
The mechanisms of HR are very heterogeneous and complex and require an acute diagnosis for correct phenotyping and endotyping, which is important for the management of HR patients [5]. The synergic work between oncology and allergology is essential to achieve adequate diagnosis and treatment of patients with HRs to antineoplastic and biologic drugs [6,7,8].
Rapid Drug Desensitization (RDD) is a safe procedure that allows the re-administration of a antineoplastic or biologic drugs in a patient after suffering a HR [9,10,11]. It is performed in a highly controlled manner using a multi-step system in which the drug dose is gradually increased (which may be in both concentration and volume) [12]. There are numerous publications of RDD protocols designed by different groups therefore the choice of protocol will depend on the patient´s allergological study and risk stratification [13,14,15,16,17]. In addition, in relation to platinum salts, the survival outcomes of patients who received oxaliplatin through RDD did not differ significantly from those who received it as standard [18].
Recently, a novel RDD procedure was introduced with the aim of improving the patient's quality of life and reducing the emotional burden after the possible loss or delay of a treatment cycle following a hypersensitivity reaction. This procedure, called Same-Day Desensitization (SDD), allows drug administration to continue the same day as the patient's reaction [6]. In this way, both delay and/or discontinuation of the drug are avoided and maintaining therapeutic schedule [4,19].
SDD consists in the reintroduction and administration of the full dose of chemotherapy in patients with suspected HR to an antineoplastic or biologic agent, on the same day of the reaction once it has been adequately treated and resolved. SDD takes advantage of the cellular refractory period commonly referred to as post-anaphylactic mast cell anergy or "mast cell emptying syndrome" [20].
This requires a multidisciplinary team, highly qualified personnel, and the presence of an allergist in the Oncology Day Hospital (ODH). Once the SDD is completed, to continue the study and management, the patient is referred to an allergy consult to study and confirm the phenotype of the HR [6].
One of the main limitations of the SDD procedure could be the fact that the treatment of the patient with a HR is performed without knowing the exact diagnosis and the underlying mechanism of the presenting HR. This is because the diagnosis of the HR and the phenotyping of the HR is done in a second step, with the usual in vivo and in vitro biomarkers [5]. However, the presence of the allergist in ODH makes it possible not only to treat the initial reaction and establish desensitization treatment, but also to reach a correct diagnosis and identify the mechanisms involved in HR based solely on clinical markers.
This study, in the context of SDD, aims to analyze the diagnostic capacity of the allergist in an ODH after a HR has occurred, using only clinical biomarkers.
During the SDD procedure, no complementary test results are available to support the definitive diagnosis. Thus, SDD is performed exclusively based on the phenotype suggested by the signs and symptoms presented by the patient and witnessed by the allergist and the type of drug implicated in the HR.
The presence of the allergist at the ODH allows both the initial diagnosis and treatment of infusion reactions in oncology patients who have developed RH to antineoplastic drugs.
Methods
Ethics Approval Statement
The Castellon Provincial Hospital Consortium Ethics Committee approved the study protocol and informed consents. The patients/participants provided their written informed consent to participate in this study.
Study Population and Design
Study with 35 patients who presented HRs to antineoplastic or biologic agents at the ODH during a period of one and a half years (between February 2021 and July 2022) and underwent SDD. The study was prospective, observational and longitudinal. Patients were distributed according to sex, mean age and diagnosis of neoplastic disease.
Initial Reaction
The reactions were classified according to their phenotype into Type I reactions (IgE-mediated or non-IgE-mediated), infusional reactions, cytokine release reactions (CRR) and mixed reactions [17].
The severity of the reactions was established using Brown's severity scale (1, 2 and 3) [21] for Type I HRs and the Common Terminology Criteria for Adverse Events (CTCAE) - National Cancer Institute (NCI) [22] for infusional reaction/CRR.
Patients were classified according to the suspected drug of the initial reaction (oxaliplatin, carboplatin, paclitaxel, doxorubicin and cetuximab) and whether it was an initial treatment or retreatment after a disease-free period.
Candidate Patients for SDD
Patients who met the following inclusion criteria were considered candidates for SDD: (1) HR during drug infusion; (2) clinical presentation witnessed and treated by the allergist; (3) confirmation of the need for treatment with the culprit drug as first choice by the oncologist responsible for the patient; (4) clinical stabilization of the patient after treatment; and (5) signed informed consent.
Patients who, after suffering a HR at the ODH witnessed and treated by the allergist, did not meet the rest of the criteria for an SDD (absence of criteria 3, 4 or 5), the suspected drug was discontinued and they were referred to the Allergy Department for further study and management.
The SDD Protocol
The standard SDD protocol is designed to last approximately 3.6 - 4 hours (Table 1) [6]. Tolerance to the culprit drug in the SDD procedure, as in normal desensitization, is achieved with 2 to 2.5 fold dose increments of the drug with fixed time intervals of 15 minutes. While the rationale for RDD is based on in vitro models of IgE/antigen mast cell desensitization [23], in SDD it could be justified by a combination of the previous rationale and by the likely anergic state in which the degranulated mast cells are found [20].
SDD Premedication and Concomitant Drugs
The patient undergoing SDD receives, like any oncology patient, the standard premedication for each drug (according to the manufacturer's prescription information and the center's own protocols). Prior to the onset of SDD, the patient receives the acute treatment used by the allergist to resolve RH.
For patients undergoing SDD routinely treated with beta-blockers, caution should be considered to ensure the availability of alternative drugs to epinephrine, such as glucagon, to address possible ineffectiveness of epinephrine in the treatment of anaphylaxis.
After SDD, patients received their additional treatment (other antineoplastics or adyuvants) as prescribed by the responsible oncologist.
SDD Location
All the SDDs were performed in the ODH. This area has specific facilities to perform the procedure: nurses trained in the management of anaphylaxis, physical and continuous presence of an allergist, measures for handling dangerous drugs, constant monitoring of patients, material for cardiorespiratory arrest management and quick access to the medical intensive care unit.
SDD Breakthrough Reactions
The management of the breakthrough reactions (BTR) produced during SDD did not differ from those produced during RDD [24,25] (Figure 1). The average waiting time to restart drug administration after BTR during SDD is 20 minutes. This parameter can be influenced by the severity of BTR and the speed of response to treatment.
Diagnostic Protocol: Skin Test, Serological Biomarkers and Drug Provocation Test (DPT)
The patients were referred to the Allergy Department to complete the allergological study after SDD.
Skin testing was performed: skin prick test (SPT) and intradermal test (IDT), according to international methodology [26]. Skin tests were performed with all the drugs involved (Table 2) [27,28] except in the case of doxorubicin due to its vesicant nature. Skin tests were also performed with other drugs such as premedications, concomitant drugs or additional antineoplastic or biological agents possibly involved in the initial reactions.
Serological biomarkers were determined: total IgE (ImmunoCAPTM Total IgE. Uppsala, Sweden), Interleukin 6 (Human IL-6 - Immunoassay Quantikine® ELISA. Minneapolis, USA) and tryptase (ImmunoCAPTM Tryptase. Uppsala, Sweden) post-reaction (90 minutes after HR onset) and baseline (2 weeks after HR).
Those patients in whom a diagnosis was not concluded by skin tests and serological biomarkers were subjected to a drug provocation test (DPT) [29]. Subsequently, we analyzed whether the initial suspected phenotype prior to SDD was finally confirmed after allergological study.
We also recorded the number of RDD performed after SDD and whether, or not, there were BTR.
Results
Patient Characteristics
Seventeen (49%) patients were female and 18 (51%) were male. The mean age was 58 with a range of 37 to 79 years. Eighteen patients (51%) were diagnosed colorectal cancer, 8 patients (23%) gastric cancer, 4 patients (11%) ovarian cancer, 1 patient (3%) breast cancer, 1 patient (3%) lung cancer, 1 patient (3%) esophageal cancer, 1 patient (3%) pancreatic cancer and 1 patient (3%) urologic cancer.
The most frequently implicated drug was oxaliplatin, followed by carboplatin and paclitaxel. Doxorubicin and cetuximab were also implicated (Table 3).
SDD Outcomes
According to the initial reaction phenotype, 31 patients (88%) had type 1 HR, 2 patients (6%) presented a mixed reaction, and 2 patients (6%) were classified as infusional reactions.
From the 31 patients with type I reaction, 23 patients were grade 1, 7 patients were grade 2, and 1 patient was grade 3 [21]. As for infusional and mixed reactions, two patients presented a grade 1 reaction and two patients presented a grade 2 reaction [22] (Table 4).
A high number of patients (77%) had a positive skin test, 14% had a negative skin test and in 9% of patients a skin test was not performed because of various circumstances. Within the percentage of patients with positive skin test, the results are as following: 11% positive in SPT, 29% positive in IDT at 1/100 concentration, 31% positive in IDT at 1/10 and 6% positive in IDT at 1/1 (Table 5). Tests were performed two weeks after the initial reaction to avoid false negatives, except in specific cases due to clinical needs (weekly therapeutic regimens).
The mean post-reaction tryptase was 8.5 ng/ml (1 - 39.8 ng/ml) and the mean IL-6 was 93.15 pg/ml (1.2 – 2370 pg/ml). The mean total IgE level was 418 IU/ml (Table 5).
The initial suspected phenotype prior to SDD was confirmed in 91.5% of patients (32 patients) after performing the allergological study. In 3 patients (8.5%) the IgE-mediated reaction phenotype suspected before performing SDD were diagnosed as an infusional reaction after finishing the allergological study. The first and second patient had a change of treatment regimen by decision of their oncologist and for clinical reasons respectively. In the third patient, DPT was performed, and it was negative, therefore he was discharged to regular infusion.
Furthermore, in this study we present two cases of patients who were phenotyped at first as type I HR but a final diagnosis of mixed reaction (type I and cytokine release) was confirmed.
The first of these patients, with pre-SDD clinical features of type I HR to oxaliplatin (Brown's grade 1), developed symptoms of CRR 45 minutes after the end of SDD. The patient remained under observation for 24 hours. After further allergological study, the oxaliplatin SPT was positive, post-reaction tryptase was non-significant compared to baseline, and IL-6 was 219.6 pg/ml with a baseline of 12.6 pg/ml. The final diagnosis of this patient was a mixed reaction and he continued to receive oxaliplatin by RDD. This patient received a total of 2 RDD presenting a BTR consisting of immediate clinical type I in the first one.
The second patient, who presented initial clinical manifestations prior to SDD compatible with type I HR to oxaliplatin (Brown grade 1, exclusively palmar itching), completed SDD without incident and skin testing was negative. In view of these results, and to complete the allergological study within the therapeutic scheme of the patient, a DPT was proposed with oxaliplatin (the determination of tryptase and IL-6 postreaction were unknown at that time). Forty-five minutes after completion of DPT, the patient presented symptoms of CRR (CTCAE-NCI grade 2) together with symptoms compatible with type I reaction (palpebral angioedema and hypoxia, Brown grade 2). The patient required observation for 24 hours in a normal hospitalization setting and was discharged with full recovery. Finally, the post-reaction IL-6 determination obtained after the initial reaction was 2370 pg/ml (basal IL-6 2 pg/ml) and tryptase was 14,3 ng/ml (basal tryptase 10 ng/ml). So, the mixed phenotype was confirmed. Taking in account the possibility of the cutaneous test was performed only eleven days after the initial reaction, which could have led to a false negative skin test, it was decided to repeat them 2 weeks later, presenting a positive IDT at 1/1. Afterwards, the patient continued to receive his chemotherapy regimen by RDD.
All SDD performed in the 35 patients ended successfully but 14% of patients presented BTR during the SDD, all of them being mild (Brown grade 1, CTCAE-NCI grade 1). One hundred percent of the patients with BTRs during SDD responded to the treatment administered and completed the procedure without new incidences.
All patients were treated and stabilized at the ODH after suffering the initial reaction and all SDD were similarly performed at ODH. All reactions were treated with intravenous and/or intramuscular medication at the discretion of the specialist who performed the initial assessment. Three patients (9%) received intravenous antihistamine (dexchlorpheniramine 5 mg), 3 patients (9%) received intravenous corticosteroid (methylprednisolone 1-2 mg/kilogram of body weight or hydrocortisone 100-500 mg), 27 patients (77%) received a combination of intravenous antihistamine and corticosteroid and 2 patients (6%) received intravenous antihistamine, corticosteroid and intramuscular epinephrine (0,5 mg). After completion of SDD all patients were referred home after completing one hour of observation, except for the patient who presented with clinical signs of cytokine release after completion of the SDD, who remained under observation for 24 hours. In cases with severe initial HR and/or BTR during SDD, oral treatment with antihistamines was prescribed for 48 hours at home.
After SDD, 29 patients (82.8%) returned to receive their same chemotherapy schedule using the RDD procedure. A total of 118 RDD were performed on a scheduled basis after drug administration by SDD. Of these, 107 RDD were performed without incident and 11 RDD had BTR during the procedure. In our series, none of the patients developed a converting phenotype in subsequent RDD [30].
Discussion
This work shows that the presence of the allergist in the ODH is vital for the proper management of HR. An approximation of the phenotype of the initial reaction is particularly relevant as it will help to predict the outcome of desensitization and to personalize future treatment plans [31].
At present, there is only one previous publication describing the SDD procedure. The current publication solves one of the main problems with RDD, namely the loss of the treatment cycle in which the HR occurs [6]. SDD procedure is more cost-effective than RDD because the dose is not missed on the day the patient presents his first HR. In this manner, patient anxiety is also reduced and the therapeutic schedule established by the oncologist is adhered to without delay, which is essential for patient survival [4,8].
SDD procedure is shown to be a safe and highly effective procedure in patients who present HRs during drug administration. This study confirms that SDD does not increase the risk to which the patient is exposed with a HR, even in initial severe reactions (grade 3 Brown and grade 2 CTCAE-NCI). Thus, it confirms that SDD does not pose a greater risk than delayed RDD.
Based on the safety observed in the previous publication [6], describing 9 patients undergoing SDD all of whom were initiated in step 1, in this study, it was initiated in most patients in step 4 or 5 of the 1/1 bag (Table 1). However, caution must be observed in extremely reactive patients who present reactions with few milliliters of infusion, especially in platinum salts. In these patients it would be advisable, until more data is available, to initiate the SDD procedure with a 1/100 bag (4 steps) and then continue with the initial bag with 10 steps.
In 3 patients (8.5%) with an initial clinical phenotype of type 1 reaction, the phenotype could not be confirmed after allergological study. These were three patients who managed to complete treatment using SDD and were finally diagnosed as having an infusional reaction. All of them had negative skin tests and non-significant post-reaction tryptase levels. The drugs involved in these 3 patients were paclitaxel, oxaliplatin and cetuximab. However, we have found that the suspected phenotype in 91.5% of patients treated with SDD was subsequently confirmed.
Previous publications highlight that, in the case of oxaliplatin, almost 40% of patients with initial type I HR converted to another endophenotype (most often CRR or mixed reaction) during RDD [31]. This situation may have occurred in both patients finally diagnosed with mixed reaction to oxaliplatin. Another possibility is that the rapid recognition of symptoms by the allergist present at the ODH, might make these patients, with incipient reactions suggestive of type I reaction, do not develop the florid picture of signs and symptoms of CRR at the same time they present the initial reaction prior to SDD. Therefore, a diagnostic correlation is confirmed since type I HR is included in mixed HR.
Regarding serum biomarkers according to phenotype, tryptase determination during the acute phase of HR is a useful method to confirm mast cell involvement, with higher tryptase values being obtained in more severe clinical drug reactions [5,32]. We have observed that patients with low clinical severity (exclusively cutaneous) that could go unnoticed, have significantly elevated post-reaction tryptase levels. These figures should correspond to clinical phenotypes of greater severity than those observed. We have observed seen that the post-reaction serum tryptase level is not always directly related to the degree of clinical severity. We think this is likely related to the allergist's quick action at ODH at the onset of the reaction.
Regarding IL-6 levels, previous publications have found that an average elevation of about 40 times the normal serum IL-6 concentration helps define the oxaliplatin CRR endophenotype [31]. We observed that levels below 50 pg/ml are not usually correlated with clinical cytokine release. All patients who presented clinical symptoms compatible with cytokine release had IL-6 levels equal to or higher than 100 pg/ml. IL-6 is particularly useful as a biomarker to identify CRRs [31,33].
To correctly make the final diagnosis of patients, we must consider a series of biomarkers whose results we do not know at the time it is decided to perform SDD after the initial HR. However, we should not underestimate in any case the clinical markers that remain of utmost importance to phenotype a HR. For this reason, we believe that the presence of the allergist in ODH is essential.
Sometimes, the presence of different endotypes simultaneously in the same patient, could induce a reaction by different mechanisms. It is important to keep in mind that patients may present reactions in which more than one mechanism of cell degranulation is involved e.g., immunologically mediated (IgE or IgG) or non-immunologically mediated mechanisms (MAS related G protein-coupled receptor X2 in mast cell, MRGPRX2) This may generate a synergistic effect rather than an exclusionary effect [5,32,34].
Another issue to consider regarding the presence of the allergist in the ODH, is that during SDD we are not exempt from presenting breakthrough reactions, in the same way that they appear in RDD. We have found that these breakthrough reactions are, in their majority, mild. All patients who underwent SDD, including those who presented breakthrough reactions during the procedure, completed the SDD successfully with complete administration of the dose of antineoplastic prescribed by the oncologist.
Some publications have found that the presence of a positive skin test (especially positive SPT) result is an important predictor of reaction during desensitization, as corroborated in this study, where all patients who presented breakthrough reactions during subsequent RDD had positive skin tests [11,25].
The presence of the allergist at ODH facilitates the rapid and adequate diagnosis of patients presenting a HR. The fact that these patients are treated in the first instance by specialists in allergology means that the diagnosis issued has a greater correlation with the initial reaction phenotype presented, as we have shown in this study. On the other hand, it guarantees the complete request for complementary explorations at the time of the HR.
A recent consensus document published by the World Allergy Organization [35] devotes an extensive section to explaining how to redesign an allergy department that successfully addresses pharmacologic desensitization. We should consider SDD as a procedure as important as RDD, so it is essential to learn how to organize allergy department to be able to implement this technique.
The most outstanding advantage of SDD is the maintenance of the first-line therapeutic regimen in the oncology patient without producing losses or delays in its administration. This has both clinical and emotional benefits for the patient.
SDD is therefore confirmed as a cost-effective, safe, efficient, and facilitating procedure towards personalized precision medicine. The path towards this precision medicine necessarily involves knowledge of the endotypes underlying HRs [36]. This will make it possible to update new classifications of hypersensitivity reactions, which will be key in the future, for the establishment of new therapeutic targets.
Conclusions
The presence of the allergist during SDD is considered necessary for the success of the procedure [37]. From our point of view, we believe that the presence of the allergist is not only vital during SDD, but also prior to it, that is, in the HDO where the administration of oncologic treatments takes place. This statement is based on the high degree of diagnostic concordance found in this study. The fact of witnessing the HR in the HDO allows allergists, on one hand, to desensitize the patient on the same day and, on the other hand, and no less important, to accurately phenotype the HR.
Accurate phenotyping and endotyping is essential as it allows risk stratification of the HR patient and the development of RDD protocols within personalized medicine [38].
So, and in agreement with researchers such as Madrigal-Burgaleta and Castells [39], more resources are needed to continue working along these lines and to create multidisciplinary teams to incorporate these techniques as a fundamental part of the integral treatment of the oncology patient.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, X.X. and Y.Y.; methodology, X.X.; software, X.X.; validation, X.X., Y.Y. and Z.Z.; formal analysis, X.X.; investigation, X.X.; resources, X.X.; data curation, X.X.; writing—original draft preparation, X.X.; writing—review and editing, X.X.; visualization, X.X.; supervision, X.X.; project administration, X.X.; funding acquisition, Y.Y. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Doroshow JH, Kummar S. Translational research in oncology-10 years of progress and future prospects. Nat Rev Clin Oncol. 2014, 11, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Desmond-Hellmann S, Sawyers CL, Cox DR et al. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease. Washington, DC: The National Academies Press; 2011.
- Rosell R, Monzó M, Alberola V, Taron M, Barnadas A, Sánchez JM, et al. Determinants of response and resistance to cytotoxics. Semin Oncol. 2002, 29, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Matzka M, Köck-Hódi S, Jahn P, Mayer H. Relationship among symptom clusters, quality of life, and treatment-specific optimism in patients with cancer. Support Care Cancer. 2018, 26, 2685–2693. [Google Scholar] [CrossRef] [PubMed]
- Mayorga C, Ariza A, Muñoz-Cano R, Sabato V, Doña I, Torres MJ. Biomarkers of immediate drug hypersensitivity. Allergy. 2024, 79, 601–612. [Google Scholar] [CrossRef]
- Borrás J, Farzanegan R, Torres MC, Germán A et al. Same-Day Desensitization in Patients Who Experience Their First Reaction to a Platin Agent at the Oncology Day Unit: A Pilot Study to Safely Include This Technique Within the Multidisciplinary Pathways for the Diagnosis & Management of Hypersensitivity to Platin Agents. Front Allergy. 2022, 3, 1–7. [Google Scholar]
- Cernadas JR, Brockow K, Romano A, Aberer W, Torres MJ, Bircher A, et al. General considerations on rapid desensitization for drug hypersensitivity - a consensus statement. Allergy. 2010, 65, 1357–1366. [Google Scholar] [CrossRef]
- Jensen-Jarolim E, Bax HJ, Bianchini R, Capron M, Corrigan C, Castells M, et al. AllergoOncology - the impact of allergy in oncology: EAACI position paper. Allergy. 2017, 72, 866–887. [Google Scholar] [CrossRef]
- Gastaminza G, de la Borbolla JM, Goikoetxea MJ, Escudero R, Antón J, Espinós J, et al. A new rapid desensitization protocol for chemotherapy agents. J Investig Allergol Clin Immunol. 2011, 21, 108–112. [Google Scholar]
- Borras J, El-Qutob D. Experience With Rapid Desensitization to Chemotherapy in a Type B Hospital. J Investig Allergol Clin Immunol. 2016, 26, 271–273. [Google Scholar] [CrossRef]
- Madrigal-Burgaleta R, Bernal-Rubio L, Berges-Gimeno MP, Carpio-Escalona LV, Gehlhaar P, Alvarez-Cuesta E. A large single-hospital experience using drug provocation testing and rapid drug desensitization in hypersensitivity to antineoplastic and biological agents. J Allergy Clin Immunol Pract. 2019, 7, 618–632. [Google Scholar] [CrossRef]
- Broyles AD, Banerji A, Castells M. Practical guidance for the evaluation and management of drug hypersensitivity: general concepts. J Allergy Clin Immunol Pract. 2020, 8, S3–S15. [Google Scholar] [CrossRef]
- Lee JH, Moon M, Kim YC, Chung SJ, Oh J, Kang D-Y, et al. A one-bag rapid desensitization protocol for paclitaxel hypersensitivity: a noninferior alternative to a multi-bag rapid desensitization protocol. J Allergy Clin Immunol Pract. 2020, 8, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Vidal C, Méndez-Brea P, López-Freire S, Bernárdez B, Lamas MJ, Armisén M, et al. A modified protocol for rapid desensitization to chemotherapy agents. A modified protocol for rapid desensitization to chemotherapy agents. J Allery Clin Immunol Pract. 2016, 4, 1003–1005. [Google Scholar]
- Sala-Cunill A, Molina-Molina G, Verdesoto J, Labrador-Horrillo M, Luengo O, Galvan-Blasco P, et al. One-dilution rapid desensitization protocol to chemotherapeutic and biological agents: a five-year experience. J Allergy Clin Immunol Pract. 2021, 9, 4045–4054. [Google Scholar] [CrossRef]
- Vázquez-Revuelta P, Lleonart-Bellfill R, Molina-Mata K, Múñoz-Sánchez C, Rey-Salido M, Madrigal-Burgaleta R, et al. A Pilot Experience Using a 1-Bag Intravenous Rapid Desensitization Protocol for Chemotherapy and Biologics in a Cohort of Patients With Access to a Delabeling Pathway. J Investig Allergol Clin Immunol. 2023, 33, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Yang BC, Castells MC. The Who, What, Where, When, Why, and How of Drug Desensitization. Immunol Allergy Clin North Am. 2022, 42, 403–420. [Google Scholar] [CrossRef]
- Berges-Gimeno MP, Carpio-Escalona LV, Longo-Muñoz F, Bernal-Rubio L, López-Gónzalez P, Gehlhaar P, et al. Does Rapid Drug Desensitization to Chemotherapy Affect Survival Outcomes? J Investig Allergol Clin Immunol. 2020, 30, 254–263. [Google Scholar] [CrossRef]
- Castells M, Matulonis U, Horton T. Infusion reactions to systemic chemotherapy. UpToDate. O: Version 23 (Accessed, 20 January 2023.
- Mohamed OE, Baretto RL, Walker I, Melchior C, Heslegrave J, Mckenzie R, et al. Empty mast cell syndrome: fallacy or fact? J Clin Pathol. 2020, 73, 250–256. [Google Scholar] [CrossRef]
- Brown SGA. Clinical features and severity grading of anaphylaxis. J Allergy Clin Immunol. 2004, 114, 371–376. [Google Scholar] [CrossRef]
- Roselló S, Blasco I, García Fabregat L, Cervantes A, Jordan K. Management of infusion reactions to systemic anticancer therapy: ESMO Clinical Practice Guidelines. Ann Oncol. 2017, 28, iv100–iv118. [Google Scholar]
- Adnan A, Acharya S, Alenazy LA, de las Vecillas L, Giavina Bianchi P, Picard M, et al. Multistep IgE Mast Cell Desensitization Is a Dose- and Time-Dependent Process Partially Regulated by SHIP-1. J Immunol. 2023, 210, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Vega A, Jiménez-Rodríguez T-W, Barranco R, Bartra J, Diéguez MC, Doña I, et al. Hypersensitivity Reactions to Cancer Chemotherapy: Practical Recommendations of ARADyAL for Diagnosis and Desensitization. J Investig Allergol Clin Immunol. 2021, 31, 364–384. [Google Scholar] [CrossRef] [PubMed]
- Gorgulu Akin B, Erkoc M, Korkmaz ET, Ozdel Ozturk B, Colak S, Ozalp Ates FS, et al. Rapid drug desensitization with platin-based chemotherapy: Analysis of risk factors for breakthrough reactions. World Allergy Organ J. 2021, 15, 1–12. [Google Scholar]
- Broyles AD, Banerji A, Bermettler S, Biggs CM, Blumenthal K, Brennan PJ, et al. Practical Guidance for the Evaluation and Management of Drug Hypersensitivity: Specific Drugs. J Allergy Clin Immunol Pract. 2020, 8, S16–S116. [Google Scholar] [CrossRef] [PubMed]
- García JC, Rodríguez E. Capítulo 12: Técnicas diagnósticas in vivo, En: Dávila I, Jáuregui I, eds. Tratado de Alergología. TOMO I. 2da Edición. Madrid (2015): 151-160.
- Pagani M, Bavbek S, Alvarez-Cuesta E, Berna Dursun A, Bonadonna P, Castells M, et al. Hypersensitivity reactions to chemotherapy: an EAACI Position Paper. Allergy 2022, 77, 388–403. [Google Scholar] [CrossRef] [PubMed]
- Madrigal-Burgaleta R, Vázquez-Revuelta P, Martí-Garrido J, Lleonart R, Ali MBBS FR, Alvarez-Cuesta E, et al. Importance of Diagnostics Prior to Desensitization in New Drug Hypersensitivity: Chemotherapeutics and Biologicals. Curr Treat Options Allergy. 2020, 7, 1–13. [Google Scholar] [CrossRef]
- Jiménez-Rodríguez T-W, Marco de la Calle F-M, Lozano-Cubo I, Montoyo-Anton R-A, Soriano-Gomis V, González-Delgado P, et al. Converter Phenotype: A New Profile That Is Not Exclusive to Taxanes. Front Allergy. 2022, 12, 785259. [Google Scholar]
- Silver J, Garcia-Neuer M, Lynch DM, Pasaoglu G, Sloane DE, Castells M. Endophenotyping oxaliplatin hypersensitivity: personalizing desensitization to the atypical platin. J Allergy Clin Immunol Pract. 2020, 8, 1668–1680. [Google Scholar] [CrossRef] [PubMed]
- Mayorga C, Celik G, Rouzaire P, Whitaker P, Bonadonna P, Rodrígues-Cernadas J, et al. In vitro tests for drug hypersensitivity reactions: an ENDA/EAACI Drug Allergy Interest Group position paper. Allergy. 2016, 71, 1103–1134. [Google Scholar] [CrossRef]
- Jakubovic BD, Sanchez-Sanchez S, Hamadi S, Lynch D, Castells M. Interleukin-6: a novel biomarker for monoclonal antibody and chemotherapy-associated hypersensitivity confirms a cytokine release syndrome phenotype-endotype association. Allergy. 2021, 76, 1571–1573. [Google Scholar] [CrossRef]
- Sabato V, Ebo DG, Van Der Poorten MM, Toscano A, Van Gasse AL, Mertens C et al. Allergenic and mas-related G protein-coupled receptor X2-activating properties of drugs: resolving the two. J Allergy Clin Immunol Pract. 2023, 11, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Cuesta E, Madrigal-Burgaleta R, Broyles AD, Cuesta-Herranz J, Guzman-Melendez MA, Maciag MC, et al. Standards for practical intravenous rapid drug desensitization & delabeling: A WAO committee statement. World Allergy Organ J. 2022, 15, 100640.
- Jutel M, Agache I, Zemelka-Wiacek M, Akdis M, Chivato T, Del Giacco S, et al. Nomenclature of allergic diseases and hypersensitivity reactions: Adapted to modern needs: An EAACI position paper. Allergy. 2023, 78, 2851–2874. [Google Scholar] [CrossRef] [PubMed]
- Madrigal-Burgaleta R, Guzman-Melendez MA, Alvarez-Cuesta E. New Technical Aspects Used in the Management of Desensitization to Antineoplastic Drugs. Curr Treat Options Allergy. 2022, 9, 204–218. [Google Scholar] [CrossRef]
- Jimenez-Rodriguez TW, Garcia-Neuer M, Alenazy LA, Castells M. Anaphylaxis in the 21st century: phenotypes, endotypes, and biomarkers. J Asthma Allergy. 2018, 20, 121–142. [Google Scholar]
- Madrigal-Burgaleta R and Castells, M. Editorial: Diagnosis and management of allergy to chemotherapy and biologics. Front Allergy. 2023, 11, 1205345. [Google Scholar] [CrossRef]
Figure 1.
Management of the breakthrough reactions during SSD-RDD. Adapted from Vega et al 24.
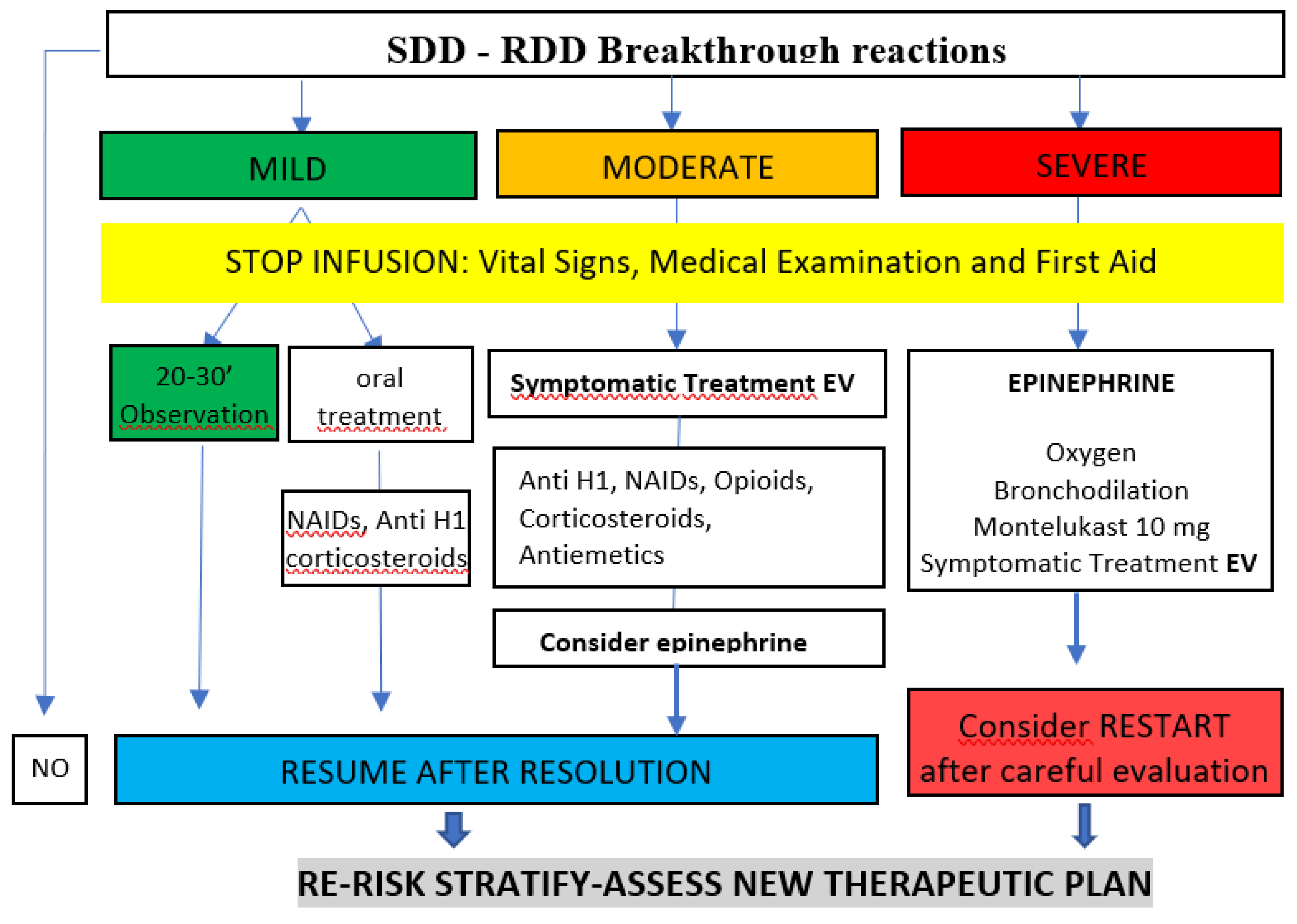

Table 1.
Example of the protocol used for the Same-day desensitization, using a non-diluted 1 bag/10 step protocol.6 Example of dosing for 100 mg of oxaliplatin.
Table 1.
Example of the protocol used for the Same-day desensitization, using a non-diluted 1 bag/10 step protocol.6 Example of dosing for 100 mg of oxaliplatin.
|
5 mg/ml | |||||
|
100 mg (20 ml) | |||||
|
270 ml | |||||
|
0.37 mg/ml | |||||
| Example when the reaction appears at 40 ml of volume infused: | 14.8 mg (40 ml) | |||||
|
85.2mg (230ml) | |||||
| STEP | Rate ml/hour | Time (min) | Administered volumen (ml) | Administered dose (mg) | Cumulative dose infused (mg) | |
| 1 | 0.6 | 15 | 0.15 | 0.06 | 0.06 | |
| 2 | 1.2 | 15 | 0.3 | 0.11 | 0.17 | |
| 3 | 2.4 | 15 | 0.6 | 0.22 | 0.39 | |
| 4 | 4.8 | 15 | 1.2 | 0.44 | 0.83 | |
| 5 | 9.6 | 15 | 2.4 | 0.89 | 1.72 | |
| 6 | 19.2 | 15 | 4.8 | 1.78 | 3.50 | |
| 7 | 38.4 | 15 | 9.6 | 3.56 | 7.06 | |
| 8 | 76.8 | 15 | 19.2 | 7.11 | 14.17 | |
| 9 | 100 | 15 | 25 | 9.26 | 23.43 | |
| 10 | 120 | 83.37 | 166.75 | 61.76 | 85.19 | |
| TOTAL (SDD) | 218.4 | 230 | 85.20 | 85.20 | ||
| Previous to reaction: | 40 ml | 14.8 mg | ||||
| TOTAL (Administered) | 270 ml | 100 mg | ||||
Table 2.
Concentrations used for SPT and IDT 27,28.
| Drug | SPT | IDT |
|---|---|---|
| Paclitaxel 6 mg/mL |
1/10: 0.1 - 0.6 mg/mL 1/1: 1 - 6 mg/mL |
1/1000: 0.001- 0.006 mg/mL 1/100: 0.01 - 0.06 mg/mL 1/10: 0.6 mg/mL |
| Carboplatin 10 mg/mL |
1/1: 10 mg/mL | 1/100: 0.1 mg 1/10: 1 mg |
| Oxaliplatin 5 mg/mL |
1/1: 5 mg/mL | 1/100: 0.05 mg 1/10: 0.5 mg 1/1: 5 mg |
| Cetuximab 5 mg/mL |
1/1: 5 mg/mL | 1/10: 0.5 mg/mL 1/1: 5 mg/mL |
| Doxorubicin | unrealized | unrealized |
Table 3.
Demographic and clinical characteristics of the patients.
| Total n=35 | ||
|---|---|---|
| Sex | ||
| Male | 18 | (51%) |
| Female | 17 | (49%) |
| Age | ||
| Average | 58 | |
| Range | 37-79 | |
| Diagnosis | ||
| Colorectal | 18 | (51%) |
| Gastric | 8 | (23%) |
| Ovarian | 4 | (11%) |
| Breast | 1 | (3%) |
| Lung | 1 | (3%) |
| Esophagus | 1 | (3%) |
| Pancreas | 1 | (3%) |
| Urologic | 1 | (3%) |
| TNM staging | ||
| T2 | 2 | (6%) |
| T3 | 11 | (31%) |
| T4 | 22 | (63%) |
| Associated mutations | ||
| BRCA | 0 | |
| BRAF | 6 | |
| RAS | 2 | |
| HER2 | 2 | |
| Drug | ||
| Oxaliplatin | 28 | (80%) |
| Carboplatin | 3 | (9%) |
| Paclitaxel | 2 | (6%) |
| Doxorubicin | 1 | (3%) |
| Cetuximab | 1 | (3%) |
| Cycle in which the reaction was presented | ||
| Average | 4 | |
| Range | 1-12 | |
| Periordicity of cycles | ||
| weekly (7) | 1 | (3%) |
| every 15 days | 13 | (37%) |
| every 21 days | 20 | (57%) |
| every 28 days | 1 | (3%) |
| Retreatment | ||
| Yes | 24 | (69%) |
| No | 11 | (31%) |
| Volume infused (in the initial HR) | ||
| Average | 76,57 | ml |
| Range | 7-256 | ml |
| Type of infusion (according to oncological prescription) | ||
| Normal | 13 | (37%) |
| Slow | 22 | (63%) |
| Suspected phenotype | ||
| Type 1 reaction | 31 | (88%) |
| Infusional reaction | 2 | (6%) |
| Cytokine release reaction | 0 | |
| Mixed reaction | 2 | (6%) |
| Final diagnosis | ||
| Type 1 reaction | 27 | (77%) |
| Infusional reaction | 5 | (14%) |
| Cytokine release reaction | 0 | |
| Mixted reaction | 3 | (9%) |
Table 4.
Clinical presentation and severity according to drug.
| Oxaliplatin (n=28) | Carboplatin (n =3) | Paclitaxel(n=2) | Doxorubicin(n=1) | Cetuximab(n=1) | |
|---|---|---|---|---|---|
| Symptomatology | |||||
| Shivering | 1 | 0 | 0 | 0 | 0 |
| Hypertension | 4 | 0 | 2 | 0 | 0 |
| Flushing | 5 | 0 | 1 | 0 | 0 |
| Cutaneous | 22 | 3 | 1 | 1 | 1 |
| Digestive | 6 | 1 | 0 | 0 | 1 |
| Respiratory | 4 | 2 | 0 | 1 | 1 |
| Cardiac | 0 | 1 | 0 | 1 | 0 |
| Hemodynamic inestability* | 2 | 0 | 1 | 1 | 1 |
| Severity according to Brown's scale | |||||
| Grade 1 | 21 (75%) | 1 (33%) | 1 (50%) | ||
| Grade 2 | 5 (18%) | 2 (67%) | |||
| Grade 3 | 1 (100%) | ||||
| Severity according to NCI | |||||
| Grade 1 | 2 (7%) | ||||
| Grade 2 | 1 (50%) | 1 (100%) | |||
| Grade 3 | |||||
| Grade 4 | |||||
| Grade 5 | |||||
*Hemodynamic instability including desaturation, hypotension or tachycardia.
Table 5.
Allergological explorations.
| Positive skin tests | N=35 | |
|---|---|---|
| Prick | 4 | (11%) |
| ID 1/100 | 10 | (29%) |
| ID 1/10 | 11 | (31%) |
| ID 1/1 | 2 | (6%) |
| Negative | 5 | (14%) |
| not performed | 3 | (9%) |
| Post reaction tryptase (ng/ml) | ||
| Average | 8,5 | |
| Range | 1-39,8 | |
| Basal tryptase (ng/ml) | ||
| Average | 5,9 | |
| Range | 2,3-11,9 | |
| Post reaction IL-6 (pg/ml) | ||
| Average | 93 | |
| Range | 1,2-2370 | |
| IL-6 Basal (pg/ml) | ||
| Average | 14,25 | |
| Range | 0,9-61 | |
| IgE total (IU/ml) | ||
| Average | 418 | |
| Range | 2,8-3891 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



