
Submitted:
15 April 2024
Posted:
16 April 2024
You are already at the latest version
Abstract
Uterine Tumor Resembling Ovarian Sex Cord Stromal Tumor (UTROSCT) is a rare uterine mesenchymal neoplasm, which resembles ovarian sex cord tumors of the ovary. Although, in general, UTROSCT exhibits benign behavior with a favorable prognosis, this neoplasm is nonetheless classified as being of an uncertain ma-lignant potential, given its low rate of recurrence and the fact that it rarely pro-duces metastases (lymph nodes, epiploic appendix, omentum, small bowel, subcutaneous, lungs). Its histogenesis too is uncertain. Typically, UTROSCT oc-curs in peri-menopausal or menopausal women but can sometimes be observed in young women. Usually, this neoplasm can be found in the uterine corpus as a nodular intramural lesion, less frequently submucosal, subserosal or poly-poid/intracavitary. UTROSCT can cause abnormal bleeding, pelvic pain, enlarged uterus, mass sensation, but sometimes it is found purely by chance. This neo-plasm can be considered polyphenotypic on morphological, immunohistochem-ical, and genetic analyses. Generally, on microscopic examination, UTROSCT shows a predominant pattern of the cords, nests, and trabeculae typical of sex cord tumors of the ovary while, immunohistochemically, it is characterized by a co-expression of epithelial, smooth muscle, and sex cord markers. The aim of this review is to report clinical and pathological data and genetic alterations to estab-lish its impact on the prognosis and management of patients affected by this rare entity.
Keywords:
Uterine Tumor Resembling Ovarian Sex Cord Stromal Tumor
; Uterine mesenchymal neoplasm
; Polyphenotypic Neoplasm
; Prognosis.
1. Introduction
Uterine Tumor Resembling Ovarian Sex Cord Tumor (UTROSCT) is a rare mesenchymal neoplasm of the uterus, accounting for less than 0.5% of all uterine malignancies and 10 - 15% of mesenchymal uterine malignancies [1]. Morphologically, this neoplasm resembles ovarian sex cord tumors, without a component recognizable as an endometrial stroma. In 1945, Morehead and Bowman first described a case of UTROSCT as a uterine neoplasm resembling a granulosa cell tumor of the ovary [2]. Later, in 1976, Clement and Scully described this entity as a uterine neoplasm characterized by the presence of a component with sex cord differentiation and subdivided it into two groups based on morphological and prognostic features [3]. Group I corresponded to an endometrial stromal tumor with foci of sex cord differentiation (ETSCLE) < 50%, associated with recurrences and metastases. On the contrary, Group II was composed predominantly or exclusively by sex cord-like elements and was named Uterine Tumor Resembling Ovarian Sex Cord Tumor (UTROSCT). According to the current World Health Organization (WHO) classification, UTROSCT is included under “Miscellaneous mesenchymal tumors”, and is still considered a uterine neoplasm with a component that resembles those seen in ovarian sex cord tumors, but without a component recognizable as endometrial stroma [4].
The histogenesis of these rare neoplasms is still unknown. However, many theories about the histogenesis of UTROSCT have been suggested. According to some authors, the neoplasm could arise from ovarian sex cord cells which have been displaced during embryogenesis. Instead, others think that UTROSCTs could arise from an uncommitted mesenchymal stem cell, from overgrowth of sex cord elements within an endometrial stromal neoplasm, adenosarcoma, or within foci of adenomyosis and endometriosis [3,5,6,7,8,9,10]. However, molecular studies have demonstrated that UTROSCTs have no molecular alterations found in endometrial stromal tumors, such as JAZF1-JJAZ1 or PHF1 fusion [7]. In addition, although UTROSCTs have a similar morphology to ovarian adult granulosa cell tumors and sex cord-stromal tumors, they do not present the same mutations, such as DICER1 and FOXL2 mutations, which can be observed in these neoplasms [11,12]. The association with the use of tamoxifen for the treatment of breast carcinoma and UTROSCTs in some cases reported in the literature could suggest a correlation with this drug [13,14,15,16,17,18]. Because of its rarity and peculiar morphological findings, this neoplasm can pose many problems for pathological diagnosis. The aim of this review is to report clinical and pathological data and genetic alterations to establish its impact on the prognosis and management of patients affected by this rare entity.
2. Clinical Data
As regards age, this neoplasm often occurs in perimenopausal or menopausal women [19]. However, in a more recent and large series reported by Boyraz et al, the patients’ age ranged from 21-84 (mean: 52.4; median: 53) years [20], moreover in the literature many cases have been reported in which the patients can be <40 years [16,21,22,23,24,25,26,27,28,29,30,31,32] or are very young [33,34].
The most common symptom found is abnormal vaginal bleeding (67.1%) [35]. Other symptoms observed are pelvic pain (5.1%), palpable pelvic masses (2.5%) [35]. In rare instances extra-uterine symptoms have been observed, due to hormonal alterations. Thus, in a case reported by Dimitriadis, the presence of UTROSCT was associated with hyperprolactinemia and galactorrhea, which resolved after tumor resection [36]. Moreover, in the case described by Suzuki et al a patient with UTROSCT had elevated serum calcium and parathormone (PTH-rP) levels and in this case the tumor production of PTH-rP was demonstrated by normalization of serum PTH-rP after a tumorectomy and by the presence of immunoreactivity for PTH-rP in the tumor cells. [37].
Most tumors exhibit benign behavior. In fact, we have found small case series in which the patients were free of recurrences and metastases. [15,20,32,38]. As a result, there are many examples of UTROSCT being treated with conservative surgery [16,22,23,24,25,26,27,28,29,30,31,32,39,40,41] and in only three of these cases [30,31,41] there was a recurrence observed after conservative surgery, which could well be due to previous incomplete surgery. Thus, as suggested by Watrowski et al and Carbone et al, in young women, fertility-sparing surgery should be offered to patients who wish to preserve their fertility [28,32]. That said, it is important to advise such patients that the neoplasm may recur [25].
In addition, close follow-up should be made after conservative surgery while radical surgery should be considered after a pregnancy [28,32]. In fact, although, UTROSCT usually exhibits benign behavior with a favorable prognosis, this neoplasm is classified as being of uncertain malignant potential, given its low rate of recurrence and the fact that it can sometimes cause metastases. In table 1 we have summarized the cases of UTROSCT which we found in literature from 1986 to 2023, that recurred or caused metastases and occasionally also death [19,20,30,31,36,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61] (Table 1).
From our review we observed that many cases with UTROSCT, which recurred or developed metastases, were observed in single case reports [31,35,42,43,44,46,47,48,49,52,53,54,55,58,59] or sometimes in very small case series [19,30,40,45,50,57] (Table 1). The most frequent sites of recurrences or metastases in these cases were lymph nodes, peritoneum, omentum, vaginal vault, lung, and liver [44,45,46,49,52,53,54,55]. Interestingly, also in these single case reports and in the small series, there are examples in which the recurrences and the metastases were observed many years later when diagnosing lymph nodes [49] in the pelvis, omentum [19] (Table 1).
Death was not reported in any of these cases, although their metastases were in the liver and lung [49,52] (Table 1).
More recently, from 2017 until now, we have found only five studies with larger series and for these it is possible to establish a recurrence or metastasis rate (Table 1) [20,41,51,56,61]. Moore and McCluggage, in their study, found 8/34 tumors which behaved aggressively as defined by either lymph node metastatic disease at diagnosis (n = 1) or recurrence (n = 7) indicating that this rate had reached 23.5%, with a follow-up ranging from 6 to 135 months (mean 39) [51] (Table 1). Moreover, in this study, three patients (23.5%) developed metastases in the liver, vertebra, and clavicle, respectively after 12 and 23 months and died from their disease [51] (Table 1).
In the series of Goebel et al, out of 26 patients, follow-up information was available for eleven of them (42.3%, 11/26), with a mean follow-up interval of 94.4 (range 1-319) months and in only one case did the neoplasm recur in the pelvis 66 months after the initial diagnosis [56] (Table 1). In a study by Boyraz et al only a minority of the cases showed a malignant outcome (5/58, 8.6%). In this work, five out of 58 patients with a follow-up (22 to 192; mean=73.2 mo) had recurrences/metastases from 30 to 144 months, and 2 died from the disease. Out of three cases with metastases, in one case the metastasis was pulmonary, and this was observed at the time of diagnosis. In the remaining two cases, the metastases developed 60 and 48 months after diagnosis and these involved respectively the peritoneum, brain, and femur. In these cases, death occurred respectively 96 and 50 months after diagnosis [20] (Table 1).
In a study by Bi et al, the cases with recurrences or metastases were 7/22 (31.81%) and they involved the pelvic lymph nodes, pelvis, and omentum, and in one case the abdominal aorta. Death was observed in two cases 177 and 44 months after diagnosis and in one of these cases the patient already had pelvic lymph node involvement at diagnosis [41] (Table 1).
Xiong et al in their analysis of 19 cases, observed that 6 patients (31.6%, 6/19) had tumor recurrences with a median follow-up of 40.9 months (range, 1.2-195.3 months) [61]. One case was excluded due to molecular translocation suggesting an endometrial stromal neoplasm (JAZF1-SUZ12) [7,61] (Table 1). The sites of these recurrences and metastases were the peritoneum, pelvis, colon, and lung. Only one patient died 23 years after diagnosis. It is extremely interesting to note that the recurrences were observed in two cases many months after diagnosis, respectively 144 and 195 months from diagnosis [61] (Table 1).
3. Pathological Features
For the diagnosis of UTROSCT there are no specific imaging findings, so it is possible to establish that a uterine lesion corresponds to a UTROSCT exclusively on pathological examination along with an accurate morphological and immunohistochemical analysis.
3.1. Macroscopic Findings
On macroscopic examination, UTROSCT is often located in the uterine corpus and can be an intracavitary polypoid lesion mimicking an endometrial polyp which can be removed by hysteroscopy [23,62] or it can appear as a pale-yellow submucous mass, located within the muscle thickness [15,23,30,31,34,45,46,47,63]. A UTROSCT too can be observed as a yellowish-white intra-myometrial mass, located in the uterine corpus [34,36,41,45,46,48,52,54,55,58,59].
Sometimes the lesion can have hemorrhagic cystic necrotic areas [42] or can be a yellow cystic-solid mass [41,44], and in rare occurrences, can appear as a sub-serosal peduncle solid lesion attached to the uterine fundus [50,64,65] mimicking a sub-serosal leiomyoma. In addition, when the neoplasm shows prominent myxoid features with prominent gelatinous appearance on gross examination, a diagnosis of myxoid leiomyoma or leiomyosarcoma [66] can be suggested. As reported by Liu et al, the lesion can also be located at the isthmus and can protrude through the cervical os [40]. More rarely, a UTROSCT can be observed in the cervix. In fact, in the literature we found only four cases [21,33,37,67] that presented as cervical masses, mimicking a primary cervical carcinoma on instrumental tests, such as Computed Tomography (CT) or pelvic Magnetic Resonance Imaging (MRI), on macroscopic, histologic and cytologic examination. So, as emphasized by Dubruc et al, it is important to keep in mind that UTROSCTs can also be encountered in current cervical screening programs, and in this occurrence, can be responsible for diagnostic pitfalls [67].
3.2. Microscopic Findings
Given the rarity of this tumor, the diagnosis of UTROSCT is usually made post-operatively by histopathological and immunohistochemical analysis. Typically, this neoplasm resembles ovarian sex cord-stromal tumors, with sheets, cords, nests, trabeculae (Figure 1A), or tubules (Figure 1B), [51]. Neoplastic cells are epithelioid with scant eosinophilic cytoplasm, their nuclei are bland with minimal atypia (Figure 1A,B).
Necrosis and mitoses are rare or absent [68]. Sometimes, the neoplasm may show scattered foam cells, consisting of single cells and small or larger aggregates of cells with round, central nuclei and abundant clear to foamy cytoplasm resembling foam cell macrophages or Sertoli cells [34,69,70] (Figure 1C). Glomeruloid structures (Figure 1D), and small nests or micropapillary-like structures [15,16,62,64,70] or micro follicles resembling Call-Exner bodies [20,64] can be observed, too. Another peculiar growth pattern is that of a retiform, with labyrinthine cavities and channels resembling the Rete Ovarii [15,64]. Sometimes this pattern can be prominent, mimicking, on small endometrial biopsy, an adenocarcinoma or myometrial metastasis from a previous breast cancer [15] [Nogales]. Goebel et al also observed microcystic and signet ring cell-like change and retiform patterns [56] [Goebel]. Rhabdoid cells with abundant dense eosinophilic cytoplasm and eccentric nuclei were seen and were diffuse in the example reported by Boyaz et al and Bennett et al [19,20]. Rhabdoid cells with single file growth pattern were found by other authors [55,64].
However, many patterns can be present within the same neoplastic mass causing considerable morphologic heterogeneity [15,56,64,72].
When the neoplasm shows a predominant tubular pattern or gland-like differentiation with few associated stromal, this can frequently pose diagnostic problems, mimicking Sertoliform endometrial adenocarcinoma [73,74,75] or extragenital metastatic carcinoma [76]. In addition, when there is both a tubular pattern and lipid-rich cells, UTROSCT can imitate a Sertoli tumor [42].
On immunohistochemical analysis, UTROSCTs characteristically exhibit polyphenotypic immunophenotypes with co-expression of cytokeratin (Figure 2A), and smooth muscle markers, including muscle actin (Figure 2B), desmin (Figure 2 C), and histone deacetylase 8, hormone receptors [64].
In addition this neoplasm show positivity for markers, which are commonly positive in ovarian sex cord-stromal neoplasms, such as inhibin (Figure 3 A), calretinin (Figure 3B), CD99 Wilm’s tumor protein 1 (WT1), and MART-1, [16,62,64,68] and others markers such as CD10, S100, and CD117 [63,69]. In addition, as reported by Croce et al, characteristically UTROSCT can show nuclear staining with steroidogenic factor-1 (SF-1) (Figure 3D) [55] similarly to ovarian sex cord tumors (Figure 3D).
Moreover, other authors [63,78], in their study inadvertently found in all the cases reported, a strong, diffuse BCL-2 positivity that could be related to peculiar genetic alterations which are translocations on chromosomes t(4; 18) (q21.1; q21.3) and t(x; 6) (p22.3; q23.1) [78] and consequently they suggested that also this marker could have a potential value in the diagnosis of UTROSCT. These peculiar immunohistochemical aspects of this neoplasm are of considerable importance in differentiating an UTROSCT from other uterine neoplasms that could present morphological similarities. The most frequent uterine neoplasms that could mimic an UTROSCT and that should be considered, are some histopathological variants of leiomyomas, such as leiomyoma with tubules, epithelioid leiomyoma, or vascular plexiform leiomyoma. Uterine leiomyoma with tubules is a biphasic neoplasm, composed of epithelial and mesenchymal elements, with intersecting fascicles of smooth muscle, tubular and gland-like structures lined by plump cells with indistinct cytoplasm [79]. Thus, histologically, this lesion simulated uterine tumors resembling ovarian sex cord tumors (UTROSCTs), but the immunophenotype was not consistent with true sex-cord differentiation, in its negativity to inhibin, CD99, CD10 and Melan-A [79]. Epithelioid leiomyoma is a subtype of leiomyoma that macroscopically appears as a well-circumscribed, intramural mass with a soft consistency, and yellow to tan cut surfaces. Microscopically, it is characterized by the presence of more than 50% round-polygonal cells and immunohistochemically shows immunoreactivity to epithelial and smooth muscle markers but negativity to typical sex-cord markers of UTROSCT [80]. Histologically, vascular plexiform leiomyoma is a well-circumscribed, intramural nodule with anastomosing cords and trabeculae of 2 to 3 cell layers with eosinophilic cytoplasm, indistinct cell borders and plump, slightly hyperchromatic nuclei. In addition, cord lumens contain red blood cells. On immunohistochemical analysis, the neoplastic cells in this subtype of leiomyoma are positive to smooth muscle actin (SMA), caldesmon and CD99, but are negative for inhibin-α [81].
Another uterine neoplasm that could mimic a UTROSCT is a low-grade endometrial stromal sarcoma (LGESS) in a biopsy or curettage specimen. This malignancy represents the second most common uterine sarcoma [82] with a wide range of age, but with a predilection for pre-menopausal and peri-menopausal women [83]. Moreover, LGESS, like UTROSCT, may be related to tamoxifen treatment [84]. Histologically, LGESS is composed of permeative tongue-like islands of tumor cells consisting of monotonous oval to spindle cells with minimal cytologic atypia with a whorl pattern of growth around blood vessels. Immunohistochemical analysis is particularly useful since LGESS shows positivity to CD10 and negativity for sex cord markers [85]. Moreover, these endometrial sarcomas along with ESTSCLE, show genetic alterations, such as JAZF1-JJAZ1 or PHF1 fusion that are absent in UTROSCT [7].
Plexiform tumorlets are rare tumors affecting patients with an average age of 48 to 60 years.
A plexiform tumorlet is a rare lesion usually found in the myometrium and is considered to be a variant of epithelioid leiomyoma. Multiple plexiform tumorlets may have an infiltrative pattern and mimic endometrial stromal sarcoma.
Uterine Sertoli form endometrioid adenocarcinoma, this is a rare subtype of an endometrial carcinoma, which can mimic; on morphological [73,74] and immunohistochemical analysis, an UTROSCT due to the presence of tubules and glandular structures and for its positivity to sex cord markers such as inhibin, CD99, (calretinin, WT-1, and Melan-A [75]. In such an occurrence, for a correct differential diagnosis from UTROSCT and Uterine Sertoli form endometrioid adenocarcinoma, it is important to keep in mind that in this subtype of endometrial adenocarcinoma, the remaining endometrium is affected by atypical complex hyperplasia [75] and within the neoplasms can be observed a typical endometrioid component [73].
3.3. Electron Microscopy Findings
In addition, on ultrastructural analysis, UTROSCT exhibits polyphenotypic features, with both epithelial structures such as desmosome-like junctions, tonofilaments, lumina formation, and microvilli and sex-cord-like features including nuclear indentation, abundant intracellular filaments, sparse to moderate rough endoplasmic reticula and abundant intracytoplasmic lipids [86].
4. Impact of Pathological Features on Recurrences or Metastases in UTROSC
Given that, in the literature there are many single case reports of UTROSCT [31,35,36,42,43,44,46,47,48,49,52,53,54,55,58,59] (Table 1) and few small case series [19,20,40,45,50,51,56,57,61], it is extremely difficult to establish which morphological aspects could predict its aggressive behavior, and with a good probability, a poor prognosis.
Moreover, in some cases with recurrences or metastases, morphological findings, which could be signs of malignancy, such as sizes [19,30,45,51,53,58], LVI [19,30,31,36,44,47,50,53,54,55,57,58,59], necrosis [19,30,36,40,43,44,45,47,50,52,53,54,55,56], number of mitoses [19,30,40,41,47,48,50,53,61], nuclear atypia [30,31,35,36,40,44,47,48,50,52,53,54,56,61], these are not always reported (Table 1). In addition, in the small series reported by some authors, it seems that there are cases which recurred or caused metastases, even though they presented benign morphological features such as well-defined margins [30,31,35,36,40,44,47,48,50,52,53,54,56,61], absence of necrosis [19,31,35,41,45,46,51,57,58,61], a low or not significant number of mitoses, [19,20,31,35,41,42,43,44,45,46,49,51,54,55,56,57,58,59,61], absence of nuclear atypia [31,42,43,45,46,49,51,55,57,58,59,61] and absence of LVI [19,40,42,43,46,51,56,61,2035].
Regarding the microscopic appearance, the neoplasms did not show any particular architectural pattern, in fact. the majority of the cases reported in the literature that recurred or developed metastases, revealed the presence of cords, trabeculae, nests or tubules, [20,30,31,36,40,54,56,57,58,59,61] except for one case reported by Croce et al which also presented focal rhabdoid cells [55], or a case observed by Bennett which was characterized by the presence of an extensive rhabdoid component [19].
Although there are no clear criteria to establish a firm prognosis and malignancy level for UTROSCT, more recently, Boyraz et al in their large study with 75 cases, relating all morphological features and follow-up available for 58 women, affirmed that it is important to simultaneously evaluate many features for every neoplasm. In fact, these Authors observed that malignant tumors which developed recurrences/metastases, compared with benign neoplasms, showed > 3 of the following 5 features: size > 5 cm, moderate nuclear atypia, > 3mitoses /10 (High Power Field) HPF, infiltrative border and necrosis and probably also, an extensive rhabdoid component [20]. In addition, Boyraz et al emphasized that sometimes it is impossible to define the prognosis of an UTROSCT since occasionally the entire neoplasm is not examined on microscopic examination, but only some fragments from curettage specimens. Thus, it is perfectly possible that some features of malignancy such as infiltration of myometrial tissue can be missed [20].
5. Molecular Alterations of UTROSC and its Impact on Prognosis
Initially, molecular biology studies for this neoplasm were performed to demonstrate that this entity, although it has similar morphological features to ovarian sex cords tumors, due to its peculiar genetic alterations it must be considered another type of tumor [11,12]. In addition, some authors have demonstrated by molecular analysis that UTROSCTs do not have the molecular alterations found in endometrial stromal tumors, such as JAZF1-JJAZ1 or PHF1 fusion [7,45].
In our review, we also evaluated the presence of other molecular alterations in order to establish whether these could have a prognostic significance. We found a few recent studies which reported that using fluorescence in in situ hybridization (FISH) and RNA- Sequencing validated by RT-PCR [19,41,55,56,58,59,60,61,72,78]. (Table 1).
Wang et al in a single case report, using fluorescence in situ hybridization (FISH) observed, in cultured cells, two balance translocations: t(4;18)(q21.1;q21.3) and t(X;6)(p22.3;q23.1) [78]. The translocations t(4;18)(q21.1;q21.3) are related to gene bcl2 and the development of particular tumors, such as more aggressive squamous cell carcinoma and some forms of acute leukemia or follicular lymphomas. The translocation t(X;6) (p22.3;q23.1) instead involved antigen regulator gene (H-Y R) which is located at p22.3 and is responsible for gonadal organogenesis. However, the molecular results in this study did not provide information on prognostic significance since the patient after a short follow-up of twelve months was well with no signs of disease [78].
On the contrary, Croce et al, in a 70-year-old patient affected by UTROSCT with ruptured uterine serosa and a focal rhabdoid component, which recurred with widespread pelvic nodules seventeen months after surgery and then also one year later developed lung metastases, despite a treatment with aromatase inhibitors, demonstrated a novel translocation t(2;3)(p25;p22) involving the GREB1 (intron 8) and CTNNB1 (exon3), using RNA- Sequencing validated by RT-PCR. This peculiar molecular alteration, observed both in primary and recurrent neoplastic tissue, was responsible for nuclear over-expression of hypo-phosphorylated and truncated beta-Catenin, which, thanks to the involvement of GREB1, was due to a response to estrogens and caused the activation of the Wtn/beta-Catenin signal pathway with a major oncogenic effect [55].
In 2019, Dickson et al, using RNA-Sequencing confirmed by (FISH), in four cases of UTROSCT first observed that this entity presents peculiar genetic alterations [72]. These genetic alterations when identified corresponded to NCOA2/3 gene fusions in 4 cases of UTROSCT, including ESR1-NCOA3 (N=2), ESR1-NCOA2 (N=1), and GREB1-NCOA2 (N=1) [72]. Characteristically, these neoplasms did not reveal conspicuous mitotic activity. On the contrary, one tumor was circumscribed, while the remaining three cases showed myometrial infiltration as a low-grade endometrial stromal sarcoma. The Authors, given the genetic alterations found, suggested that these could be used for an accurate diagnosis of UTROSCT [72].
Although the authors suggested that these genetic alterations may be related to malignant mesenchymal neoplasms, such as mesenchymal chondrosarcoma [87] congenital spindle cell rhabdomyosarcoma [88,89], alveolar rhabdomyosarcoma [90], Ewing sarcoma [91] or human leukemia [92], as well as some uterine sarcoma with variable sex cord differentiation [93,94] they gave no information on the follow-up of patients and consequently their prognostic significance [72].
More recently, it has been demonstrated in some studies that UTROSCTs with Growth Regulating Estrogen Receptor Binding-1 (GREB1) rearrangement may have a more aggressive biological behavior with high risks of recurrence or metastases [56,58]. Likewise, it seems that GREB1 rearranged tumors tend to be larger and more mitotically active [58].
As well as neoplasms with Estrogen Receptor-1 (ESR1)-NCOA2 fusions are more likely related to recurrences and the presence of infiltrative margins and sometimes to the presence of an extensive rhabdoid component, as demonstrated by Bennett et al [19]. In addition, tumors with GREB1-NCOA2 fusion could be more frequently related to recurrences than those with other genetic alterations [41,55].
These data suggest that these gene fusions probably cause aberrant activation of estrogen signaling pathways, with a major oncogenic effect due to the increase in proliferation and activation of neoplastic cells.
In fact, gene fusions involving three nuclear receptor coactivators, such as NCOA1, NCOA2 and NCOA3, have been demonstrated in many cases of UTROSCT [56,59]. The NCOA genes belong to a p160 family of steroid receptor coactivators, which interact with ligand-dependent hormone nuclear receptors, including the estrogen receptor-alpha (ERα), to mediate transcriptional programs, can promote a wide range of signaling pathways including cellular proliferation, metabolism, growth, and survival [92].
Considering that Programmed Cell Death Ligand 1 (PD-L1), which is a trans-membrane protein considered to be a co-inhibitory factor of the immune response and plays an important role in various malignancies, attenuating the host immune response to tumor cells, Xiong et al first correlated the expression of this marker with mitotic activity and NCOA-2 gene alteration in a small series of UTROSCTs [61]. Thus, they discovered that UTROSCT with significant mitotic activity, gene alteration of NCOA2 and a high expression of stromal PDL-1, represents the subset of a neoplasm with aggressive behavior and shorter disease-free survival. [61]. Consequently, from this study, Xiong et al suggested that UTROSCTs with aggressive behavior have a peculiar tumor microenvironment and could be treated with immune therapy in line with other neoplasms [61].
6. Conclusions
In conclusion, through our review of the literature, UTROSCT is rare neoplasm which should be considered in the differential diagnosis of other uterine masses. Similarly, to many uterine intracavitary and intramural lesions, the most common symptom of this neoplasm is abnormal vaginal bleeding. To the best of our knowledge, for pre- or perioperative diagnosis in UTROSCT, there are no studies which have evaluated serum inhibin levels, a marker for sex cord differentiation. Moreover, imaging studies such as MRI cannot be useful to identify this neoplasm because they provide findings, such as cystic degeneration, intra-tumoral hemorrhage and necrosis which are common to leiomyoma [95,96,97] or adenomyosis [32,98].
On the contrary, for a pathological diagnosis many studies over the last few years have contributed to improving pathological diagnosis using immunohistochemical analysis with specific markers, revealing that UTROSCT is a polyphenotypic neoplasm with variable positivity for epithelial, smooth muscle, neuroendocrine, sex cord markers and hormone receptors and with molecular heterogeneity [19,41,55,58,60,61].
Although UTROSCT usually exhibits benign behavior with a favorable prognosis, this neoplasm is classified as being of uncertain malignant potential, given that it has a low rate of recurrence and can sometimes cause metastases. However, close follow-up is required for all patients due to the lack of prognostic biomarkers and a long follow up is needed to evaluate the safety of conservative surgery.
A conservative surgical approach can be offered to young women who wish to preserve their fertility. However, it is important to advise the patients that the neoplasm may recur [25]. In addition, a close follow-up should be made after conservative surgery and radical surgery should be considered after a pregnancy given that, in some instances, the recurrences or metastases were observed many months after diagnosis [40,61].
Although in this rare neoplasm it is extremely difficult to establish which morphological aspects could predict its aggressive behavior, recently some authors have suggested evaluating multiple factors [20]. More recently, some molecular biology studies have revealed that UTROSCTs with GREB1::NCOA1-3 fusions [51,58] and PD-L1 molecule expression appear to be predisposed to more aggressive behavior and recurrences, GREB1::NCOA2 being the most common gene fusion in recurrent tumors [61]. As well as, recently Yin et al observed a case of UTROSC with aggressive histologic features harboring a GREB1-NCOA2 fusion, such as increased mitotic figures (up to 3/10 high power fields), geographic necrosis, and LVI [99].
Thus, it is especially important in the case of this peculiar neoplasm to perform molecular investigations to define the most aggressive forms and to select patients with a higher risk of recurrences or metastases. Additionally, further, more numerous studies should be performed to correlate morphological findings, molecular data and clinical data with long follow up, to identify subtypes with worse prognosis.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, GG. and ET; methodology, DG; validation, GG and DG; formal analysis ET and DG; GGwriting—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The Authors would like to thank Alexander Gillan for his help for English translation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Crum, C.P.; Quick, C.M.; Laury, A.R.; Peters, W.A.; Hirsch, M.S. Uterine tumor resembling sex cord stromal tumor. In Gynecologic and Obstetric Pathology. High Yield Patholog; Elsiever: Philadelphia, 2016; pp. 459–460. [Google Scholar]
- Morehead, R.P.; Bowman, M.C. Heterologous mesenchymal tumors of the uterus: Report of a neoplasm resembling a granulosa cell tumor. Am J Pathol. 1945, 21, 53–61. [Google Scholar] [PubMed]
- Clement, P.B.; Scully, R.E. Uterine tumors resembling ovarian sex-cord tumors: A clinicopathologic analysis of fourteen cases. Am J Clin Pathol. 1976, 66, 512–525. [Google Scholar] [CrossRef] [PubMed]
- Staats, P.N.; Irving, J.A.; McCluggage, W.G. Uterine tumour resembling ovarian sex cord tumour. WHO Classification of Tumours Editorial Board. Female Genital Tumours, 5th ed. International Agency for Research on Cancer, World Health Organization, 2020. [Google Scholar]
- Czernobilsky, B. Uterine tumors resembling ovarian sex cord tumors: An update. Int J Gynecol Pathol. 2008, 27, 229–235. [Google Scholar] [CrossRef] [PubMed]
- De Level, L.; Lim, G.S.; Waltregny, D.; Oliva, E. Diverse phenotypic profile of uterine tumors resembling ovarian sex cord tumors: An immunohistochemical study of 12 cases. Am J Surg Pathol. 2010, 34, 1749–1761. [Google Scholar] [CrossRef] [PubMed]
- Staats, P.N.; Garcia, J.J.; Dias-Santagata, D.C.; Kuhlmann, G.; Stubbs, H.; McCluggage, W.G.; De Nictolis, M.; Kommoss, F.; Soslow, R.A.; Iafrate, A.J.; et al. Uterine tumors resembling ovarian sex cord tumors (UTROSCT) lack the JAZF1-JJAZ1 translocation frequently seen in endometrial stromal tumors. Am J Surg Pathol. 2009, 33, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.; McCluggage, W.G. Uterine tumour resembling ovarian sex cord tumour: First report of a large series with follow-up. Histopathology. 2017, 71, 751–759. [Google Scholar] [CrossRef]
- Stolnicu, S.; Balachandran, K.; Aleykutty, M.A.; Loghin, A.; Preda, O.; Goez, E.; Nogales, F.F. Uterine adenosarcomas overgrown by sex-cord-like tumour: Report of two cases. J Clin Pathol. 2009, 62, 942–944. [Google Scholar] [CrossRef]
- Carleton, C.; Houghton, O.P.; McCluggage, W.G. Juvenile granulosa cell tumour arising in ovarian adenosarcoma: An unusual form of sarcomatous overgrowth. Hum Pathol. 2015, 46, 616–619. [Google Scholar] [CrossRef]
- Croce, S.; de Kock, L.; Boshari, T.; Hostein, I.; Velasco, V.; Foulkes, W.D.; McCluggage, W.G. Uterine Tumor Resembling Ovarian Sex Cord Tumor (UTROSCT) Commonly Exhibits Positivity With Sex Cord Markers FOXL2 and SF-1 but Lacks FOXL2 and DICER1 Mutations. Int J Gynecol Pathol. 2016, 35, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Chiang, S.; Staats, P.N.; Senz, J.; Kommoss, F.; De Nictolis, M.; Huntsman, D.G.; Gilks, C.B.; Oliva, E. FOXL2 mutation is absent in uterine tumors resembling ovarian sex cord tumors. Am J Surg Pathol. 2015, 39, 618–623. [Google Scholar] [CrossRef]
- Oztekin, O.; Soylu, F.; Yigit, S.; Sarica, E. Uterine tumor resembling ovarian sex cord tumors in a patient using tamoxifen: Report of a case and review of literature. Int J Gynecol Cancer. 2006, 16, 1694–1697. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, M.N.; Capellino, P.; Bacigaluppi, A.D.; Cassanello, G.; Guagnini, M.C.F.; Danieli, F.P.; Crivelli, R. Tumor endometrial sìmil tumor de cordones sexuales asociado al uso de tamoxifeno. Revista del HPC, 2008; 11, 22. [Google Scholar]
- Nogales, F.F.; Stolnicu, S.; Harilal, K.R.; Mooney, E.; García-Galvis, O.F. Retiform uterine tumours resembling ovarian sex cord tumours. A comparative immunohistochemical study with retiform structures of the female genital tract. Histopathology. 2009, 54, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Giordano, G.; Lombardi, M.; Brigati, F.; Mancini, C.; Silini, E.M. Clinicopathologic features of 2 new cases of uterine tumors resembling ovarian sex cord tumors. Int J Gynecol Pathol. 2010, 29, 459–467. [Google Scholar] [CrossRef]
- Gutierrez-Pecharroman, A.; Tirado-Zambrana, P.; Pascual, A.; Rubio-Marin, D.; García-Cosío, M.; Moratalla-Bartolomé, E.; Palacios, J. Uterine Tumor Resembling Ovarian Sex Cord Tumor Associated With Tamoxifen Treatment: A Case Report and Literature Review. Int J Gynecol Pathol. 2014, 33, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Segala, D.; Gobbo, S.; Pesci, A.; Martignoni, G.; Santoro, A.; Angelico, G.; Arciuolo, D.; Spadola, S.; Valente, M.; Scambia, G.; et al. Tamoxifen related Uterine Tumor Resembling Ovarian Sex Cord Tumor (UTROSCT): A case report and literature review of this possible association. Pathol Res Pract. 2019, 215, 1089–1092. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.A.; Lastra, R.R.; Barroeta, J.E.; Parilla, M.; Galbo, F.; Wanjari, P.; Young, R.H.; Krausz, T.; Oliva, E. Uterine Tumor Resembling Ovarian Sex Cord Stromal Tumor (UTROSCT): A Series of 3 Cases With Extensive Rhabdoid Differentiation, Malignant Behavior, and ESR1-NCOA2 Fusions. Am J Surg Pathol. 2020, 44, 1563–1572. [Google Scholar] [CrossRef] [PubMed]
- Boyraz, B.; Watkins, J.C.; Young, R.H.; Oliva, E. Uterine Tumors Resembling Ovarian Sex Cord Tumors: A Clinicopathologic Study of 75 Cases Emphasizing Features Predicting Adverse Outcome and Differential Diagnosis. Am J Surg Pathol. 2023, 47, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Kabbani, W.; Deavers, M.T.; Malpica, A.; Burke, T.W.; Liu, J.; Ordoñez, N.G.; Jhingran, A.; Silva, E.G. Uterine tumor resembling ovarian sex-cord tumor: Report of a case mimicking cervical adenocarcinoma. Int J Gynecol Pathol. 2003, 22, 297–302. [Google Scholar] [CrossRef]
- Hillard, J.B.; Malpica, A.; Ramirez, P.T. Conservative management of a uterine tumour resembling an ovarian sex cord-stromal tumour. Gynecol Oncol. 2004, 92, 347–352. [Google Scholar] [CrossRef]
- Anastasakis, E.; Magos, A.L.; Mould, T.; Economides, D.L. Uterine tumor resembling ovarian sex cord tumors treated by hysteroscopy. Int J Gynaecol Obstet. 2008, 101, 194–195. [Google Scholar] [CrossRef]
- Berretta, R.; Patrelli, T.S.; Fadda, G.M.; Merisio, C.; Gramellini, D.; Nardelli, G.B. Uterine tumors resembling ovarian sex cord tumors: A case report of conservative management in young women. Int J Gynecol Cancer. 2009, 19, 808–810. [Google Scholar] [CrossRef] [PubMed]
- Garuti, G.; Gonfiantini, C.; Mirra, M.; Galli, C.; Luerti, M. Uterine tumor resembling ovarian sex cord tumors treated by resectoscopic surgery. J Minim Invasive Gynecol. 2009, 16, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Bakula-Zalewska, E.; Danska-Bidzinska, A.; Kowalewska, M.; Piascik, A.; Nasierowska-Guttmejer, A.; Bidzinski, M. Uterine tumors resembling ovarian sex cord tumors, a clinicopathologic study of six cases. Ann Diagn Pathol. 2014, 18, 329–332. [Google Scholar] [CrossRef]
- Jeong, K.H.; Lee, H.N.; Kim, M.K.; Kim, M.L.; Seong, S.J.; Shin, E. Successful delivery after conservative resectoscopic surgery in a patient with a uterine tumor resembling ovarian sex cord tumor with myometrial invasion. Obstet Gynecol Sci. 2015, 58, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Watrowski, R.; Jäger, C.; Möckel, J.; Kurz, P.; Schmidt, D.; Freudenberg, N. Hysteroscopic treatment of uterine tumor resembling ovarian sex cord-like tumor (UTROSCT). Gynecol Endocrinol. 2015, 31, 856–859. [Google Scholar] [CrossRef] [PubMed]
- De Franciscis, P.; Grauso, F.; Ambrosio, D.; Torella, M.; Messalli, E.M.; Colacurci, N. Conservative Resectoscopic Surgery, Successful Delivery, and 60 Months of Follow-Up in a Patient with Endometrial Stromal Tumor with Sex-Cord-Like Differentiation. Case Rep Obstet Gynecol. 2016, 2016, 5736865. [Google Scholar] [CrossRef]
- Schraag, S.M.; Caduff, R.; Dedes, K.J.; Fink, D.; Schmidt, A.M. Uterine Tumors Resembling Ovarian Sex Cord Tumors - Treatment, recurrence, pregnancy and brief review. Gynecol Oncol Rep. 2017, 19, 53–56. [Google Scholar] [CrossRef]
- Dondi, G.; Tesei, M.; De Crescenzo, E.; Boussedra, S.; Giunchi, S.; Perrone, A.M.; De Iaco, P. Uterine tumor resembling ovarian sex-cord tumor: A case report of recurrence after conservative management and review of the literature. Gynecol Pelvic Med. 2021, 4, 42. [Google Scholar] [CrossRef]
- Carbone, M.V.; Cavaliere, A.F.; Fedele, C.; Vidiri, A.; Aciuolo, D.; Zannoni, G.; Scambia, G. Uterine tumor resembling ovarian sex-cord tumor: Conservative surgery with successful delivery and case series. Eur J Obstet Gynecol Reprod Biol. 2021, 256, 326–332. [Google Scholar] [CrossRef]
- Sahraoui, G.; Sassi, F.; Charfi, L.; Ltaief, F.; Doghri, R.; Mrad, K. Unusual presentation of uterine tumors resembling ovarian sex cord tumor: A rare case report of cervical involvement. Int J Surg Case Rep. 2023, 108, 108477. [Google Scholar] [CrossRef]
- Irving, J.A.; Carinelli, S.; Prat, J. Uterine tumors resembling ovarian sex cord tumors are polyphenotypic neoplasms with true sex cord differentiation. Mod Pathol. 2006, 19, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Cömert, G.K.; Kiliç, Ç.; Çavuşoğlu, D.; Türkmen, O.; Karalok, A.; Turan, T.; Başaran, D.; Boran, N. Recurrence in Uterine Tumors with Ovarian Sex-Cord Tumor Resemblance: A Case Report and Systematic Review. Turk Patoloji Derg. 2018, 34, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, G.K.; Wajman, D.S.; Bidmead, J.; Diaz-Cano, S.J.; Arshad, S.; Bakhit, M.; Lewis, D.; Aylwin, S.J.B. Ectopic hyperprolactinaemia due to a malignant uterine tumor resembling ovarian sex cord tumors (UTROCST). Pituitary 2020, 23, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, C.; Matsumoto, T.; Fukunaga, M.; Itoga, T.; Furugen, Y.; Kurosaki, Y.; Suda, K.; Kinoshita, K. Uterine tumors resembling ovarian sex-cord tumors producing parathyroid hormone-related protein of the uterine cervix. Pathol Int. 2002, 52, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Xia, Y.; Chen, J.; Tang, J.; Shao, Y.; Yu, W. NCOA1/2/3 rearrangements in uterine tumor resembling ovarian sex cord tumor: A clinicopathological and molecular study of 18 cases. Hum Pathol. 2023, 135, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Abdullazade, S.; Kosemehmetoglu, K.; Adanir, I.; Kutluay, L.; Usubutun, A. Uterine tumors resembling ovarian sex cord-stromal tumors: Synchronous uterine tumors resembling ovarian sex cord-stromal tumors and ovarian sex cord tumor. Ann Diagn Pathol. 2010, 14, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Shen, Y.; Zhao, J.G.; Qu, P.P. Clinical experience of uterine tumors resembling ovarian sex cord tumors: A clinicopathological analysis of 6 cases. Int J Clin Exp Pathol. 2015, 8, 4158–4164. [Google Scholar] [PubMed]
- Bi, R.; Yao, Q.; Ji, G.; Bai, Q.; Li, A.; Liu, Z.; Cheng, Y.; Tu, X.; Yu, L.; Chang, B.; et al. Uterine Tumor Resembling Ovarian Sex Cord Tumors: 23 Cases Indicating Molecular Heterogeneity With Variable Biological Behavior. Am J Surg Pathol. 2023, 47, 739–755. [Google Scholar] [CrossRef]
- Kantelip, B.; Cloup, N.; Dechelotte, P. Uterine tumor resembling ovarian sex cord tumors: Report of a case with ultrastructural study. Hum Pathol. 1986, 17, 91–94. [Google Scholar] [CrossRef]
- Biermann, K.; Heukamp, L.C.; Büttner, R.; Zhou, H. Uterine tumor resembling an ovarian sex cord tumor associated with metastasis. Int J Gynecol Pathol. 2008, 27, 58–60. [Google Scholar] [CrossRef]
- O'Meara, A.C.; Giger, O.T.; Kurrer, M.; Schaer, G. Case report: Recurrence of a uterine tumor resembling ovarian sex-cord tumor. Gynecol Oncol. 2009, 114, 140–142. [Google Scholar] [CrossRef]
- Umeda, S.; Tateno, M.; Miyagi, E.; Sakurai, K.; Tanaka, R.; Tateishi, Y.; Tokinaga, A.; Ohashi, K.; Furuya, M. Uterine tumors resembling ovarian sex cord tumors (UTROSCT) with metastasis: Clinicopathological study of two cases. Int J Clin Exp Pathol. 2014, 7, 1051–1059. [Google Scholar]
- Mačák, J.; Dundr, P.; Dvořáčková, J.; Klát, J. Uterine tumors resembling ovarian sex cord tumors (UTROSCT). Report of a case with lymph node metastasis. Cesk Patol. 2014, 50, 46–49. [Google Scholar] [PubMed]
- Jeong, K.H.; Lee, H.N.; Kim, M.K.; Kim, M.L.; Seong, S.J.; Shin, E. Successful delivery after conservative resectoscopic surgery in a patient with a uterine tumor resembling ovarian sex cord tumor with myometrial invasion. Obstet Gynecol Sci. 2015, 58, 418–422. [Google Scholar] [CrossRef]
- Gomes, J.R.; Carvalho, F.M.; Abrão, M.; Maluf, F.C. Uterine tumors resembling ovarian sex-cord tumor: A case-report and a review of literature. Gynecol Oncol Rep 2015, 15, 22–24. [Google Scholar] [CrossRef]
- Endo, D.; Todo, Y.; Okamoto, K.; Suzuki, H. A case of recurrent group II uterine tumor resembling ovarian sex-cord tumors, against which two hormonal agents were ineffective. Taiwan J Obstet Gynecol. 2016, 55, 751–753. [Google Scholar] [CrossRef] [PubMed]
- Viau, M.; Grondin, K.; Grégoire, J.; Renaud, M.C.; Plante, M.; Sebastianelli, A. Clinicopathological features of two cases of uterine tumors resembling ovarian sex-cord tumors (UTROSCTs) and a comprehensive review of literature. Eur. J. Gynaecol. Oncol. 2017, 38, 93–799. [Google Scholar] [CrossRef]
- Moore, M.; McCluggage, W.G. Uterine tumour resembling ovarian sex cord tumour: First report of a large series with follow-up. Histopathology. 2017, 71, 751–759. [Google Scholar] [CrossRef]
- Kuznicki, M.L.; Robertson, S.E.; Hakam, A.; Shahzad, M.M. Metastatic uterine tumor resembling ovarian sex cord tumor: A case report and review of the literature. Gynecol Oncol Rep. 2017, 22, 64–68. [Google Scholar] [CrossRef]
- Kondo, Y.; Sakaguchi, S.; Mikubo, M.; Naito, M.; Shiomi, K.; Ohbu, M.; Satoh, Y. Lung metastases of a uterine tumor resembling ovarian sex-cord tumor: Report of a rare case. Diagn Cytopathol. 2018, 46, 88–91. [Google Scholar] [CrossRef]
- Marrucci, O.; Nicoletti, P.; Mauriello, A.; Facchetti, S.; Patrizi, L.; Ticconi, C.; Sesti, F.; Piccione, E. Uterine Tumor Resembling Ovarian Sex Cord Tumors Type II with Vaginal Vault Recurrence. Case Rep Obstet Gynecol. 2019, 2019, 5231219. [Google Scholar] [CrossRef] [PubMed]
- Croce, S.; Lesluyes, T.; Delespaul, L.; Bonhomme, B.; Pérot, G.; Velasco, V.; Mayeur, L.; Rebier, F.; Ben Rejeb, H.; Guyon, F.; et al. GREB1-CTNNB1 fusion transcript detected by RNA-sequencing in a uterine tumor resembling ovarian sex cord tumor (UTROSCT): A novel CTNNB1 rearrangement. Genes Chromosomes Cancer. 2019, 58, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Goebel, E.A.; Hernandez Bonilla, S.; Dong, F.; Dickson, B.C.; Hoang, L.N.; Hardisson, D.; Lacambra, M.D.; Lu, F.I.; Fletcher, C.D.M.; Crum, C.P.; et al. Uterine Tumor Resembling Ovarian Sex Cord Tumor (UTROSCT): A Morphologic and Molecular Study of 26 Cases Confirms Recurrent NCOA1-3 Rearrangement. Am J Surg Pathol. 2020, 44, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Kaur, K.; Rajeshwari, M.; Gurung, N.; Kumar, H.; Sharma, M.C.; Yadav, R.; Kumar, S.; Manchanda, S.; Singhal, S.; Mathur, S.R. Uterine tumor resembling ovarian sex cord tumor: A series of six cases displaying varied histopathological patterns and clinical profiles. Indian J Pathol Microbiol. 2020, 63, S81–S86. [Google Scholar] [PubMed]
- Chang, B.; Bai, Q.; Liang, L.; Ge, H.; Yao, Q. Recurrent uterine tumors resembling ovarian sex-cord tumors with the growth regulation by estrogen in breast cancer 1-nuclear receptor coactivator 2 fusion gene: A case report and literature review. Diagn Pathol. 2020, 15, 110. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, K.A.; Kertowidjojo, E.; Natale, K.; Ewalt, M.D.; Soslow, R.A.; Hodgson, A. GTF2A1-NCOA2-Associated Uterine Tumor Resembling Ovarian Sex Cord Tumor (UTROSCT) Shows Focal Rhabdoid Morphology and Aggressive Behavior. Am J Surg Pathol. 2021, 45, 1725–1728. [Google Scholar] [CrossRef] [PubMed]
- Bini, M.; Gantzer, J.; Dufresne, A.; Vanacker, H.; Romeo, C.; Franceschi, T.; Treilleux, I.; Pissaloux, D.; Tirode, F.; Blay, J.Y.; et al. ESR1Rearrangement as a Diagnostic and Predictive Biomarker in Uterine Tumor Resembling Ovarian Sex Cord Tumor: A Report of Four Cases. JCO Precis Oncol. 2023, 7, e2300130. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.P.; Luo, R.Z.; Wang, F.; Yang, X.; Lai, J.P.; Zhang, C.; Liu, L.L. PD-L1 expression, morphology, and molecular characteristic of a subset of aggressive uterine tumor resembling ovarian sex cord tumor and a literature review. J Ovarian Res. 2023, 16, 102. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.V.; Phung, H.T.; Dao, L.T.; Ta, D.H.H.; Tran, M.N. Uterine Tumor Resembling Ovarian Sex Cord Tumor: Clinicopathological Characteristics of a Rare Case. Case Rep Oncol. 2020, 13, 807–812. [Google Scholar] [CrossRef]
- Ye, S.; Wu, J.; Yao, L.; He, J. Clinicopathological characteristics and genetic variations of uterine tumours resembling ovarian sex cord tumours. J Clin Pathol. 2022, 75, 776–781. [Google Scholar] [CrossRef]
- Hurrell, D.P.; McCluggage, W.G. Uterine tumour resembling ovarian sex cord tumour is an immunohistochemically polyphenotypic neoplasm which exhibits coexpression of epithelial, myoid and sex cord markers. J Clin Pathol. 2007, 60, 1148–1154. [Google Scholar] [CrossRef]
- Baker, R.J.; Hildebrandt, R.H.; Rouse, R.V.; Hendrickson, M.R.; Longacre, T.A. Inhibin and CD99 (MIC2) expression in uterine stromal neoplasms with sex-cord-like elements. Hum Pathol. 1999, 30, 671–679. [Google Scholar] [CrossRef]
- Ise, K.; Tanei, Z.I.; Oda, Y.; Tanikawa, S.; Sugino, H.; Ishida, Y.; Tsuda, M.; Gotoda, Y.; Nishiwaki, K.; Yanai, H.; et al. A Case of Uterine Tumor Resembling Ovarian Sex Cord Tumor With Prominent Myxoid Features. Int J Gynecol Pathol. 2024, 43, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Dubruc, E.; Alvarez Flores, M.T.; Bernier, Y.; Gherasimiuc, L.; Ponti, A.; Mathevet, P.; Bongiovanni, M. Cytological features of uterine tumors resembling ovarian sex-cord tumors in liquid-based cervical cytology: A potential pitfall. Report of a unique and rare case. Diagn Cytopathol. 2019, 47, 603–607. [Google Scholar] [CrossRef]
- Pradhan, D.; Mohanty, S.K. Uterine tumors resembling ovarian sex cord tumors. Arch Pathol Lab Med. 2013, 137, 1832–1836. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Jungbluth, A.A.; Busam, K.J.; Rosai, J. Uterine tumors resembling ovarian sex-cord tumors have an immunophenotype consistent with true sex-cord differentiation. Am J Surg Pathol. 1998, 22, 1078–1082. [Google Scholar] [CrossRef] [PubMed]
- Fekete, P.S.; Vellios, F.; Patterson, B.D. Uterine tumor resembling an ovarian sex-cord tumor: Report of a case of an endometrial stromal tumor with foam cells and ultrastructural evidence of epithelial differentiation. Int J Gynecol Pathol. 1985, 4, 378–387. [Google Scholar] [CrossRef]
- Sadeh, R.; Segev, Y.; Schmidt, M.; Schendler, J.; Baruch, T.; Lavie, O. Uterine Tumors Resembling Ovarian Sex Cord Tumors: Case Report of Rare Pathological and Clinical Entity. Case Rep Obstet Gynecol. 2017, 2017, 2736710. [Google Scholar] [CrossRef] [PubMed]
- Dickson, B.C.; Childs, T.J.; Colgan, T.J.; Sung, Y.S.; Swanson, D.; Zhang, L.; Antonescu, C.R. Uterine Tumor Resembling Ovarian Sex Cord Tumor: A Distinct Entity Characterized by Recurrent NCOA2/3 Gene Fusions. Am J Surg Pathol. 2019, 43, 178–186. [Google Scholar] [CrossRef]
- Usadi, R.S.; Bentley, R.C. Endometrioid carcinoma of the endometrium with sertoliform differentiation. Int J Gynecol Pathol. 1995, 14, 360–364. [Google Scholar] [CrossRef]
- Eichhorn, J.H.; Young, R.H.; Clement, P.B. Sertoliform endometrial adenocarcinoma: A study of four cases. Int J Gynecol Pathol. 1996, 15, 119–126. [Google Scholar] [CrossRef]
- Liang, S.X.; Patel, K.; Pearl, M.; Liu, J.; Zheng, W.; Tornos, C. Sertoliform endometrioid carcinoma of the endometrium with dual immunophenotypes for epithelial membrane antigen and inhibin alpha: Case report and literature review. Int J Gynecol Pathol. 2007, 26, 291–297. [Google Scholar] [CrossRef]
- Kumar, N.B.; Hart, W.R. Metastases to the uterine corpus from extragenital cancers: A clinicopathologic study of 63 cases. Cancer. 1982, 50, 2163–2169. [Google Scholar] [CrossRef]
- Kumar, A.; Schneider, V. Metastases to the uterus from extrapelvic primary tumors. Int J Gynecol Pathol. 1983, 2, 134–140. [Google Scholar] [CrossRef]
- Wang, J.; Blakey, G.L.; Zhang, L.; Bane, B.; Torbenson, M.; Li, S. Uterine tumor resembling ovarian sex cord tumor: Report of a case with t(X;6)(p22.3;q23.1) and t(4;18)(q21.1;q21.3). Diagn Mol Pathol. 2003, 12, 174–180. [Google Scholar] [CrossRef]
- Pusiol, T.; Parolari, A.M.; Piscioli, F. Uterine leiomyoma with tubules. Int Semin Surg Oncol. 2008, 5, 15. [Google Scholar] [CrossRef]
- Toledo, G.; Oliva, E. Smooth muscle tumors of the uterus: A practical approach. Arch Pathol Lab Med. 2008, 132, 595–605. [Google Scholar] [CrossRef]
- Simon, R.A.; Sung, C.J.; Lawrence, W.D.; Quddus, M.R. Vascular plexiform leiomyoma mimicking uterine tumor resembling ovarian sex cord tumor. Ann Diagn Pathol. 2010, 14, 355–357. [Google Scholar] [CrossRef]
- Abeler, V.M.; Røyne, O.; Thoresen, S.; Danielsen, H.E.; Nesland, J.M.; Kristensen, G.B. Uterine sarcomas in Norway. A histopathological and prognostic survey of a total population from 1970 to 2000 including 419 patients. Histopathology. 2009, 54, 355–364. [Google Scholar] [CrossRef]
- Chan, J.K.; Kawar, N.M.; Shin, J.Y.; Osann, K.; Chen, L.M.; Powell, C.B.; Kapp, D.S. Endometrial stromal sarcoma: A population-based analysis. Br J Cancer. 2008, 99, 1210–1215. [Google Scholar] [CrossRef]
- Beer, T.W.; Buchanan, R.; Buckley, C.H. Uterine stromal sarcoma following tamoxifen treatment. J Clin Pathol. 1995, 48, 596. [Google Scholar] [CrossRef] [PubMed]
- Oliva, E. CD10 expression in the female genital tract: Does it have useful diagnostic applications? Adv Anat Pathol. 2004, 11, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; de Level, L.; Selig, M.; Oliva, E.; Nielsen, G.P. Uterine tumors resembling ovarian sex cord tumors: An ultrastructural analysis of 13 cases. Ultrastruct Pathol. 2010, 34, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Motoi, T.; Khanin, R.; Olshen, A.; Mertens, F.; Bridge, J.; Dal Cin, P.; Antonescu, C.R.; Singer, S.; Hameed, M.; et al. Identification of a novel, recurrent HEY1-NCOA2 fusion in mesenchymal chondrosarcoma based on a genome-wide screen of exon-level expression data. Genes Chromosomes Cancer. 2012, 51, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Mosquera, J.M.; Sboner, A.; Zhang, L.; Kitabayashi, N.; Chen, C.L.; Sung, Y.S.; Wexler, L.H.; LaQuaglia, M.P.; Edelman, M.; Sreekantaiah, C.; et al. Recurrent NCOA2 gene rearrangements in congenital/infantile spindle cell rhabdomyosarcoma. Genes Chromosomes Cancer. 2013, 52, 538–550. [Google Scholar] [CrossRef] [PubMed]
- Alaggio, R.; Zhang, L.; Sung, Y.S.; Huang, S.C.; Chen, C.L.; Bisogno, G.; Zin, A.; Agaram, N.P.; LaQuaglia, M.P.; Wexler, L.H.; et al. A Molecular Study of Pediatric Spindle and Sclerosing Rhabdomyosarcoma: Identification of Novel and Recurrent VGLL2-related Fusions in Infantile Cases. Am J Surg Pathol. 2016, 40, 224–235. [Google Scholar] [CrossRef]
- Sumegi, J.; Streblow, R.; Frayer, R.W.; Dal Cin, P.; Rosenberg, A.; Meloni-Ehrig, A.; Bridge, J.A. Recurrent t(2;2) and t(2;8) translocations in rhabdomyosarcoma without the canonical PAX-FOXO1 fuse PAX3 to members of the nuclear receptor transcriptional coactivator family. Genes Chromosomes Cancer. 2010, 49, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Svoboda, L.K.; Harris, A.; Bailey, N.J.; Schwentner, R.; Tomazou, E.; von Levetzow, C.; Magnuson, B.; Ljungman, M.; Kovar, H.; Lawlor, E.R. Overexpression of HOX genes is prevalent in Ewing sarcoma and is associated with altered epigenetic regulation of developmental transcription programs. Epigenetics. 2014, 9, 1613–1625. [Google Scholar] [CrossRef]
- Moens, C.B.; Selleri, L. Hox cofactors in vertebrate development. Dev Biol. 2006, 291, 193–206. [Google Scholar] [CrossRef]
- Lee, C.H.; Kao, Y.C.; Lee, W.R.; Hsiao, Y.W.; Lu, T.P.; Chu, C.Y.; Lin, Y.J.; Huang, H.Y.; Hsieh, T.H.; Liu, Y.R.; et al. Clinicopathologic Characterization of GREB1-rearranged Uterine Sarcomas With Variable Sex-Cord Differentiation. Am J Surg Pathol. 2019, 43, 928–942. [Google Scholar] [CrossRef]
- Kao, Y.C.; Lee, J.C. An update of molecular findings in uterine tumor resembling ovarian sex cord tumor and GREB1-rearranged uterine sarcoma with variable sex-cord differentiation. Genes Chromosomes Cancer. 2021, 60, 180–189. [Google Scholar] [CrossRef]
- Okada, S.; Uchiyama, F.; Ohaki, Y.; Kamoi, S.; Kawamura, T.; Kumazaki, T. MRI findings of a case of uterine tumor resembling ovarian sex-cord tumors coexisting with endometrial adenoacanthoma. Radiat Med. 2001, 19, 151–153. [Google Scholar]
- Pang, L.; Dai, Y.; Ren, F.; Peng, X.; Guo, Z. Uterine Tumor Resembling Ovarian Sex Cord Tumors (UTROSCT): Two Case Reports of the Rare Uterine Neoplasm with Literature Review. Curr Med Imaging. 2022, 18, 125–1131. [Google Scholar] [CrossRef]
- Vilos, A.G.; Zhu, C.; Abu-Rafea, B.; Ettler, H.C.; Weir, M.M.; Vilos, G.A. Uterine Tumors Resembling Ovarian Sex Cord Tumors Identified at Resectoscopic Endometrial Ablation: Report of 2 Cases. J Minim Invasive Gynecol. 2019, 26, 105–109. [Google Scholar] [CrossRef]
- Hermsen, B.; Bogliatto, F.; Bleeker, M.; Leidi, L.; Trum, H.; Comello, E. Uterine tumour resembling ovarian sex cord tumour (UTROSCT): Experience with a rare disease. Two case reports and overview of the literature. Obstet Gynecol Cases Rev, 2015; 2, 49. [Google Scholar]
- Yin, X.; Wang, M.; He, H.; Ru, G.; Zhao, M. Uterine Tumor Resembling Ovarian Sex Cord Tumor With Aggressive Histologic Features Harboring a GREB1-NCOA2 Fusion: Case Report With a Brief Review. Int J Gynecol Pathol. 2023, 42, 54–62. [Google Scholar] [CrossRef]
Figure 1.
Microscopically, UTROSCT resembles ovarian sex cord-stromal tumors, with sheets, cords, nests, trabeculae, (A: hematoxylin-eosin x 200) or tubules (B: hematoxylin-eosin, Arrows: tubules, x200 ), scattered foam cells, consisting of single cells and small or larger aggregates of cells with round, central nuclei and abundant clear to foamy cytoplasm resembling foam cells macrophages or Sertoli cells (C: hematoxylin-eosin, x100) and glomeruloid structures (D: hematoxylin-eosin, x100).
Figure 1.
Microscopically, UTROSCT resembles ovarian sex cord-stromal tumors, with sheets, cords, nests, trabeculae, (A: hematoxylin-eosin x 200) or tubules (B: hematoxylin-eosin, Arrows: tubules, x200 ), scattered foam cells, consisting of single cells and small or larger aggregates of cells with round, central nuclei and abundant clear to foamy cytoplasm resembling foam cells macrophages or Sertoli cells (C: hematoxylin-eosin, x100) and glomeruloid structures (D: hematoxylin-eosin, x100).
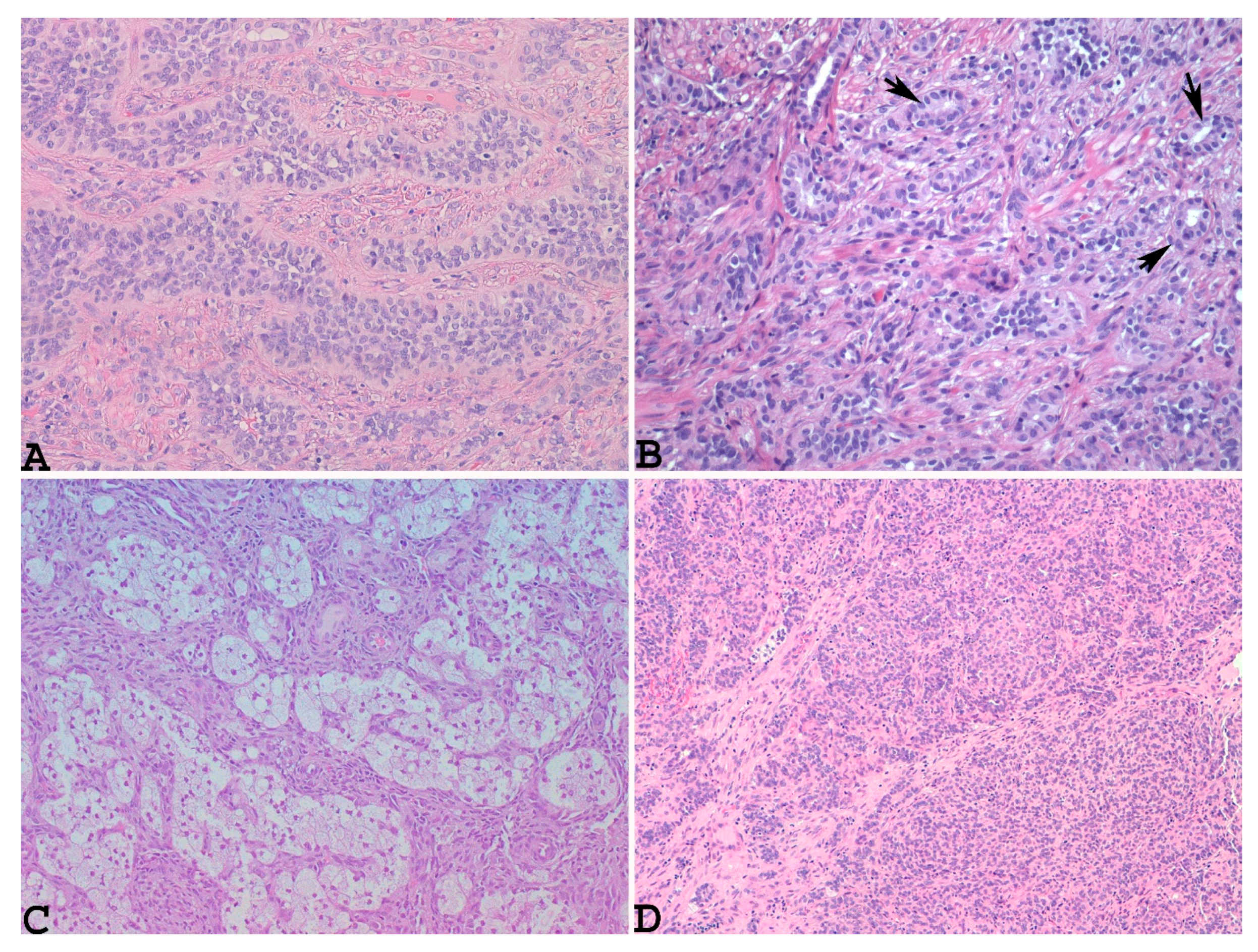
Figure 2.
Example of UTROSCT exhibiting polyphenotypic immunoreactivity with co-expression of cytokeratin (A: x 200), smooth muscle markers, including muscle actin (B: x200) and desmin (C: x200).
Figure 2.
Example of UTROSCT exhibiting polyphenotypic immunoreactivity with co-expression of cytokeratin (A: x 200), smooth muscle markers, including muscle actin (B: x200) and desmin (C: x200).
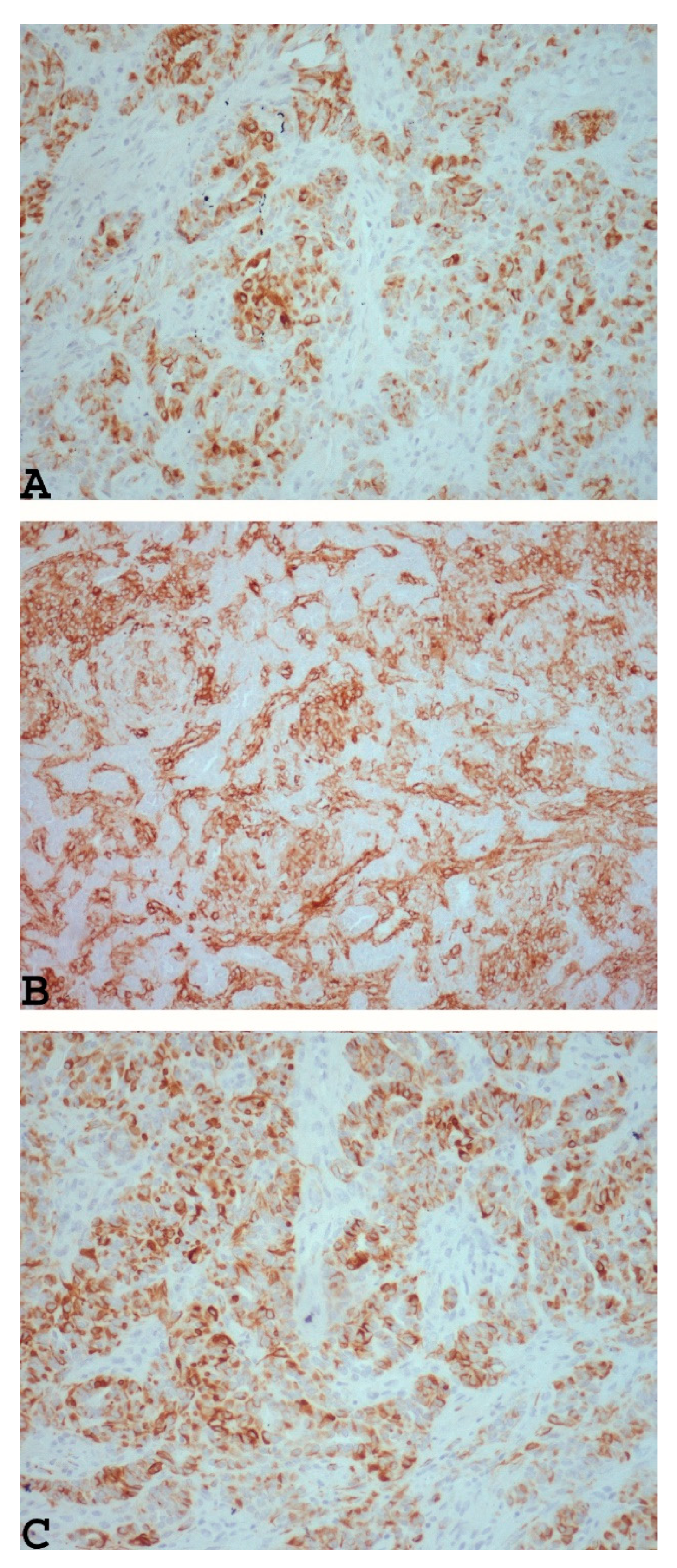
Figure 3.
Example of UTROSCT with positivity for markers, which are commonly positive in ovarian sex cord-stromal neoplasms, such as inhibin (A: x 200), calretinin (B: x 200), CD99 (C: x200) and nuclear staining with steroidogenic factor-1 (SF-1) (D: x200).
Figure 3.
Example of UTROSCT with positivity for markers, which are commonly positive in ovarian sex cord-stromal neoplasms, such as inhibin (A: x 200), calretinin (B: x 200), CD99 (C: x200) and nuclear staining with steroidogenic factor-1 (SF-1) (D: x200).
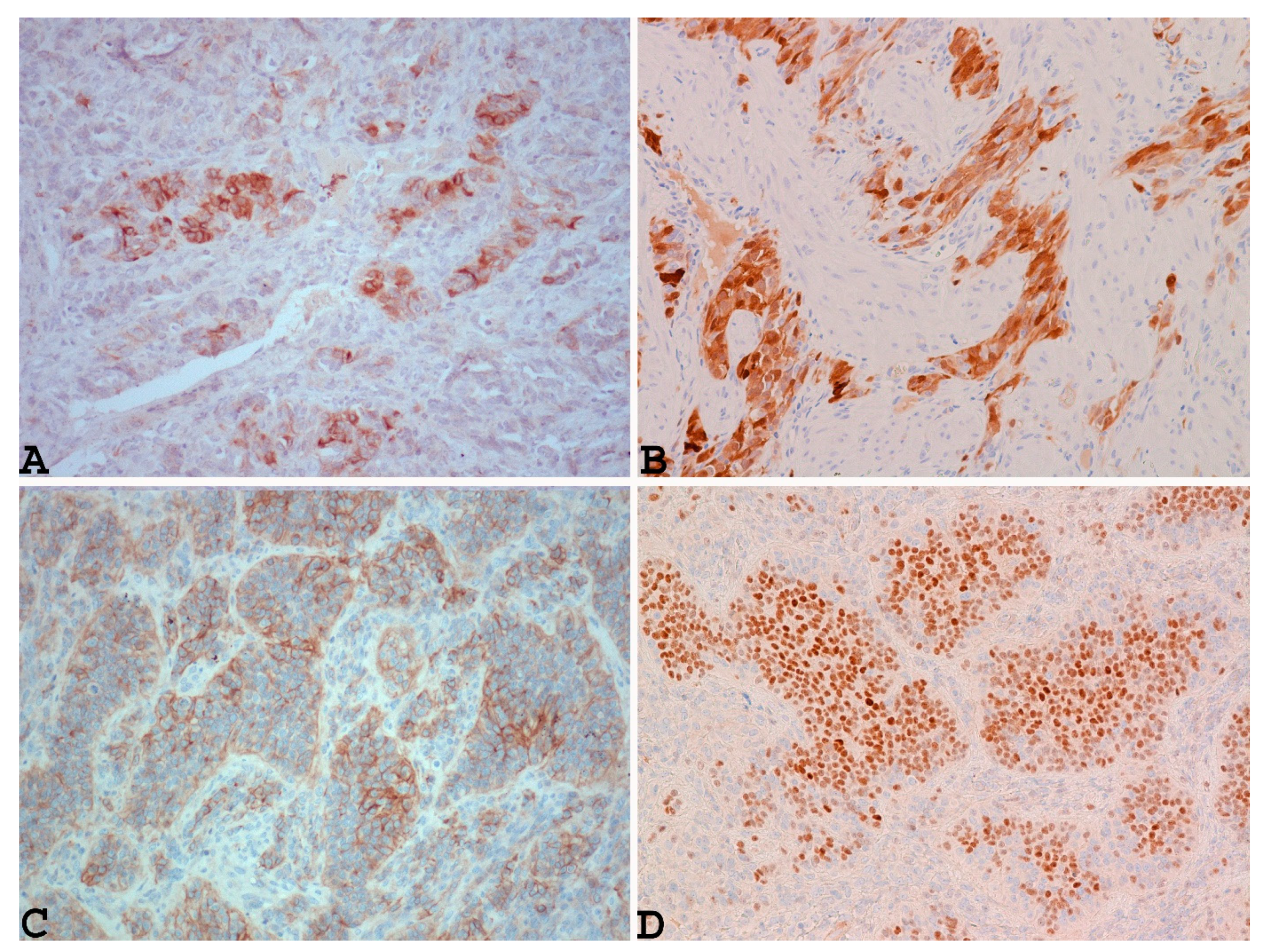

Table 1.
CASES OF UTROSC WITH RECURRENCES AND /OR METASTASES.
| Authors and year (malignant cases/total of cases) |
Age (ys) | Surgery | Gross appearance | Tumor size (cm) | Microscopic appearance (architecture / rhabdoid features) | Nuclear atypia | Mitotic rate | Tumor margins | LVI | Necrosis | Stage | Molecular findings | Site and time of recurrence/ metastasis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Kantelip et al., 1985 (1/1 case) ref (42) |
86 | Total hysterectomy and bilateral salpingo-oophorectomy | Multiple intamyometral cysts filled with hemorragic and necrotic fluid, surrounded by a fibrotic capsule | Ranging from 2 to 10 | Cords, trabeculae, nests, tubules | Not significant | <1/10 HPF | Well circumscribed | Absent | Present | NR | NR | One nodule in the left ovary and two epiploic nodules present at the time of diagnosis |
|
Biermann et al., 2007 (1/1 case) ref (43) |
68 | NR | Graysh-yellow intramyometral nodule | 4.5 | Tubules, pseudorosettes, sheets, cords | Not significant | Ki-67 < 5% | Focally infiltrative | Absent | NR | NR | NR | Mesentery and small bowel (48 mo) |
|
O’Meara et al., 2009 (1/1 case) ref (44) |
35 | Hysterectomy | Soft and partly cystic yellow mass | 9.9 | Sertoliform | NR | Ki-67 = 5% | Expansive /serosal infiltration | NR | NR | NR | NR | Bladder, abdominal and intestinal wall, peritoneum, ovaries, lymph nodes (36 mo) |
|
Umeda et al., 2014 (2/2 cases) ref (45) |
38 | Transvaginal myomectomy followed by total hysterectomy and bilateral salpingo-oophorectomy + LND | Yellowish-white intramyometral mass | 4.5 | Solid, cords, tubules | Not significant | 1/10 HPF | Infiltrative | Present | Absent | NR | NR | Left internal iliac lymph node methastasis present at the time of diagnosis |
| 57 | Total hysterectomy and bilateral salpingo-oophorectomy | Polypoid submucosal mass | 6.4 | Cords, tubules | Not significant | 0/10 HPF | Infiltrative | Present | Absent | NR | NR | Nodule in the epiploic appendix at the time of diagnosis | |
|
Mačák et al., 2014 (1/1 case) ref (46) |
53 | Polyectomy followed by hysteresctomy and bilateral salpingo-oophorectomy | Polypoid mass and intramyometral mass | 1.5 and 1.5 | Solid nests, trabeculae, ribbons | Not significant | <1/10 HPF | NR | Absent | Absent | NR | NR | Pelvic limph node methastatis at the time of diagnosis |
|
Liu et al., 2015 (1/6 cases) ref (40) |
50 | Trans-vaginal submucosal myomectomy | Isthmus mass protruding through cervical os | 4.5 | NR | NR | NR | Well circumscribed | Absent | NR | NR | NR | Local recurrence (10 mo) |
|
Jeong et al., 2015 (1/1 case) ref (47) |
32 | Submucosal resection | Submucosal protruding mass | 3.6 | Cords, tubules and nests | NR | NR | Infiltrative | NR | NR | NR | NR | Local recurrence (17 mo) |
|
Gomes et al., 2015 (1/1 case) ref (48) |
53 | Supracervical hysterectomy followed by bilateral salpingo-oophorectomy, omentectomy, parametrectomy, uterine cervical resection + LND | Myometral mass | 12 | Cords, trabeculae | NR | NR | Infiltrative | Present | Present | NR | NR | Parametrial and right ovarian hilum involvement present at the time of diagnosis |
|
Endo et al., 2016 (1/1 case) ref (49) |
62 | Hysterectomy | NR | NR | Trabeculae, nests, cords | Not significant | Ki-67 < 5% | Myometral infiltration | NR | NR | NR | NR | Pelvic limph-node (23 yr) |
|
Viau et al., 2017 (1/2 cases) ref (50) |
43 | Total hysterectomy and bilateral salpingo-oophorectomy + debulking | Peduncolated solid mass attached to the uterine fundus, with ruptured surface and whitish-yellow colour and solid subserosal mass in the anterior myometrium | 13 and 5.5 | Solid, trabeculae | NR | NR | NR | NR | NR | IIB | NR | Pelvis (40 mo). Sigmoid serosa and peritoneal implants present at the time of diagnosis. |
|
Schraag et al., 2017 (2/3 cases) ref (30) |
24 | Submucosal resection | Submucosal nodule | NR | NR | NR | NR | NR | NR | NR | NR | NR | Local recurrence (9 mo) |
| 28 | Partial resction (due to intraoperative complication) followed by fertility sparing surgery. Hysterectomy + partial bilateral salpingectomy after delivery | Cystic-solid tumor in the anterior uterine wall | 10 | NR | NR | NR | NR | NR | NR | NR | NR | Initial persistence of disease (3 mo). Pelvis, peritoneum, right fallopian tube, ovaries, vagina (39 mo) |
|
|
Moore and McCluggage, 2017 (8/34 cases) ref (51) |
44 | Hysterectomy | NR | 12.5 | NR | Not significant | ≥2/10 HPF |
NR | Absent | Absent | NR | NR | Para-aortic limph nodes, peritoneum (11 mo) |
| 75 | NP | NR | NA | NR | Not significant | ≤1/10 HPF | NR | Absent | Absent | NR | NR | Para-aortic limph nodes, retroperitoneal and sacral metastatis present at the time of diagnosis | |
| 62 | Hysterectomy | NR | 7 | NR | Not significant | ≤1/10 HPF | NR | Absent | Present | NR | NR | Peritoneum, lung (33 mo) |
|
| 43 | Hysterectomy | NR | 1 | NR | Not significant | ≥2/10 HPF |
NR | Absent | Absent | NR | NR | Pelvis, peritoneum (25 mo) |
|
| 47 | Hysterectomy | NR | 6 | NR | Not significant | ≤1/10 HPF | NR | Absent | Present | NR | NR | Vertebra, ovary (78 mo) |
|
| 68 | Hysterectomy | NR | 8 | NR | Significant | ≥2/10 HPF |
NR | Absent | Absent | NR | NR | Death (12 mo) Peritoneum, liver (11 mo) |
|
| 61 | Hysterectomy | NR | 12.5 | NR | Not significant | ≥2/10 HPF |
NR | Present | Present | NR | NR | Death (23 mo) Vertebra, clavicle (12 mo) |
|
| 72 | Hysterectomy | NR | 7 | NR | Not significant | ≥2/10 HPF |
NR | Absent | Absent | NR | NR | Death (23 mo) Liver (23 mo) |
|
|
Kuznicki et al., 2017 (1/1 case) ref (52) |
49 | Cytoreductive surgery post NACT | Intramyometrial mass | 6 | Trabeculae, rosette-like structures, nests, tubules |
NR | High | Myometral invasion / tumor present at 1mm from | Present | NR | NR | NR | Death (15 mo) Liver, peritoneum and pelvis (4 mo). Bilateral ovarian and omental metastasis at the time of diagnosis. |
|
Kondo et al., 2018 (1/1 case) ref (53) |
69 | Hysterectomy | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | Lung (36 mo) |
|
Cömert et al., 2018 (1/1 case) ref (35) |
61 | Total hysterectomy and bilateral salpingo-oophorectomy | Endometrial located tumor, suspect for superficial myometral invasion | 7 | Cords, trabeculae, nests, tubules | NR | 2/10 HPF | Infiltrative | Absent | Absent | NR | NR | Pelvis, omentum and splenic hilum (60 mo) Pelvis, anterior surface of the abdominal wall (75 mo) |
|
Marrucci et al., 2019 (1/1 case) ref (54) |
54 | Total hysterectomy and bilateral salpingo-oophorectomy | Graysh-yellow intramyometral mass with poorly delineated margins | 9 | Trabeculae, alveolar-like structures, tubules | NR | 3/10 HPF | NR | NR | NR | NR | NR | Vaginal vault (59 mo) |
|
Croce et al., 2019 (1/1 case) ref (55) |
70 | Total hysterectomy and bilateral salpingo-oophorectomy | Yellow, well circumscribed myometral mass | 10 | Diffuse, tubules, nests, trabeculae / focal rhadoid cells | Not significant | 1/10 HPF | Well circumscribed, with serosal involmement | NR | NR | NR | GREB1-CTNNB1 fusion | Pelvis (17 mo) Lung and peritoneum (29 mo) |
|
Goebel et al., 2020 (1/26 cases) ref (56) |
74 | Hysterectomy | NA | 13 | Cords, trabeculae, sertoliform, retiform | NR | 1/10 HPF | Infiltrative | Absent | NR | NR | GREB1-NCOA2 fusion | Pelvis (66 mo) |
|
Kaur et al., 2020 (1/6 cases) ref (57) |
47 | Total hysterectomy and bilateral salpingo-oophorectomy | Mass in the uterine body | 9.3 | Cords, nests, trabeculae, sheets | Not significant | 1-3/10 HPF | Infiltrative | NR | Absent | NR | NR | Pelvis, retroperitoneal lymph nodes, lungs (7 mo) |
|
Chang et al., 2020 (1/1 case) ref (58) |
57 | Total hysterectomy and bilateral salpingo-oophorectomy | Intramyometrial, well circumscribed, soft, yellow mass | 10 | Diffuse sheets, nests, cords, trabeculae, glands | Not significant | 3/10 HPF | Infiltrative | NR | Absent | IB | GREB1-NCOA2 fusion | Pelvis (30 mo) |
|
Bennett et al., 2020 (3/3 cases) ref (19) |
37 | Hysterectomy | Yellow white myometral mass | NA | Sheets, cords, trabeculae, occasional pseudopapillary appereance / extensive Rhabdoid component | NR | 0/10 HPF | Infiltrative | Suspect | Absent | I | ESR1-NCOA2 fusion | Pelvis (7 yr) |
| 54 | Supracervical hysterectomy followed by complection trachelectomy and staging | Multiple red brown myometral nodules | Ranging from 1.5 to 6.5 | Sheets, cords, trabeculae, occasional pseudopapillary appereance /extensive rhabdoid component | NR | 4/10 HPF | Infiltrative | Absent | Absent | II | ESR1-NCOA2 fusion | Pelvis (9 yr). Cervical involvement and paratubal soft tissue localization at the time of dagnosis |
|
| 30 | Hysterectomy | NR | NR | NR | NR | NR | NR | NR | NR | NR | ESR1-NCOA2 fusion | Omentum (32 yr and 34 yr) Rectosigmoid nodule (38 yr) |
|
|
Dimitriadis et al., 2020 (1/1 case) ref (36) |
46 | Hysterectomy followed by bilateral salpingo-oophorectomy | Well circumscribed uterine mass | 11 | Sheets, cords, nests, trabeculae | NR | 6/10 HPF | NR | NR | NR | NR | NR | Intra-abdominal receurrence (24 mo) |
|
Devereaux et al., 2021 (1/1 case) ref (59) |
42 | Myomectomy | Myometral based lesion | 8.8 | Clusters, cords | NR | 2/10 HPF | NA | NR | Present | NR | GFT2A1-NCOA2 fusion (in recurrent tumor) | Uterus, bilateral ovarian surfaces, peritoneum, large bowel serosa, anterior abdominal wall (6 mo) |
|
Dondi et al., 2021 (1/1 case) ref (31) |
24 | Myomectomy | Submucosal mass | 3 | NR | NR | 1/10 HPF | NR | NR | Absent | NR | NR | Local recurrence (20 mo) |
|
Boyraz et al., 2023 (5/75 cases) ref (20) |
32 |
Hysterectomy or excision with negative margins |
NA | 11 | Diffuse, cords | Moderate to severe | 6/10 HPF | Infiltrative, with serosal involvement | Absent | Absent | NR | NR | Lung metastasis present at the time of diagnosis |
| 47 | NA | 13 | Diffuse, cords / extensive rhabdoid component. |
Moderate | 7/10 HPF | Infiltrative, with serosal involvement | Absent | Present | NR | NR | Peritoneum (60 mo) |
||
| 58 | NA | 7 | Diffuse, cords | Moderate | 4/10 HPF | Infiltrative | Absent | Absent | NR | NR | Peritoneum (144 mo) | ||
| 68 | NA | 13 | Diffuse, cords | Moderate | 7/10 HPF | Infiltrative, with serosal involvement | Absent | Absent | NR | NR | Death (96 mo) Peritoneum (60 mo) |
||
| 73 | NA | 3 | Diffuse, cords | Moderate to severe | 9/10 HPF | Infiltrative | Absent | Present | NR | NR | Death (50 mo) Brain (30 mo) Femour (48 mo) |
||
|
Bini et al., 2023 (4/4 cases) ref (60) |
NR | NR | NR | NR | NR | NR | 4/50 HPF | NR | NR | NR | NR | ESR1-NCOA2 fusion | All patients had metastatic disease and recived several sistemic treatments. After a median of 13.5 years of follow up (6 to 34 years), 3 patients died of disease. |
| NR | NR | NR | NR | NR | NR | 8/50 HPF | NR | NR | NR | NR | ESR1-NCOA3 fusion |
||
| NR | NR | NR | NR | NR | NR | 5/50 HPF | NR | NR | NR | NR | ESR1-NCOA2 fusion | ||
| NR | NR | NR | NR | NR | NR | 1/50 HPF | NR | NR | NR | NR | NA | ||
|
Bi et al., 2023 (7/22 cases, 1 already reported by Chen et al., 2021) ref (40) |
33 | Total hysterectomy and bilateral salpingo-oophorectomy + LND | Endometrial thickening, intramyometral mass | 2 | Retiform, papillae, nests, diffuse, whorls, sex cords | Not significat | <1/10 HPF | Infiltrative | Absent | Absent | IIIC | GREB1-NCOA2 fusion | Death (177 mo) Retroperitoneal recurrence with abdominal aorta involvement (167 mo) Pelvic lymph nodes involvement presents at the time of diagnosis |
| 48 | Total hysterectomy and bilateral salpingo-oophorectomy | Intramyometral solid mass, partially cystic | 13 | Nests, sex cords, sertoliform trabeculae | Not significat | 1/10 HPF | Well-circumscribed | Absent | Absent | IB | GREB1-NCOA2 fusion | Pelvis and omentum (45 mo) |
|
| 38 | Total hysterectomy and bilateral salpingo-oophorectomy | Intramyometrial solid mass | NA | Nests, diffuse, sex cords / focal rhabdoid cells. |
Not significat | NA | Infiltrative | Absent | Absent | NA | GREB1-NCOA2 fusion | Pelvis and omentum (101 mo) |
|
| 48 | Total hysterectomy and bilateral salpingo-oophorectomy | Protuberant and intramyometral solid mass | 3.5 | Diffuse, focal whorls, pseudopapillae, retiform, few cords | Not significat | <1/HPF | Infiltrative | Absent | Absent | IIB | GREB1-NCOA1 fusion | Pelvis (13 mo). Peritoneal involvement present at the time of diagnosis. |
|
| 65 | Total hysterectomy and bilateral salpingo-oophorectomy | Intramyometrial solid mass | 15 | Diffuse, sex cords, whorls, sertoliform trabeculae | Not significat | 3/10 HPF | Infiltrative | Absent | Absent | IB | GREB1-NCOA1 fusion | Death (44 mo) Pelvis (35 mo) |
|
| 40 | Polypectomy | Polypoid mass | 4 | Sex cords, sertoliform trabeculae / Rhabdoid component | Not significat | <1/10 HPF | Well-circumscribed | Absent | Absent | IA | ESR1-NCOA2 fusion | Local recurrence (21 mo and 64 mo) |
|
| 45 | Hysterectomy | Intramyometral solid mass, partially cystic | 8 | Polypoid mass Diffuse, vague sex cords | Mild to moderate | 1/10 HPF | Well-circumscribed | Absent | Absent | IB | ESR1-NCOA3 fusion | Pelvis (56 mo) |
|
|
Xiong et al., 2023 (6/18 cases) ref. (61) |
41 |
Hysterectomy | NR | 5.5 | Sertoliform, nests, cords |
Not significat | 3/10 HPF | Infiltrative | Absent | Absent | NR | ESR1-NCOA2 fusion | Peritoneum (144.4 mo) |
| 46 | NA | NR | 2.5 | Sertoliform, retiform | Not significant | 2/10 HPF | Infiltrative | Absent | Absent | NR | Negative for NCOA1-3 fusion and JAZF1/SUZ12/PHF1 rearrangement | Death (26.3 mo) Pelvis, colon (2.5 mo) |
|
| 19 | NA | NR | 3 | Cords, trabeculae | Not significant | 2/10 HPF | Infiltrative | Absent | Absent | NR | NA | Metastasis (site NA) (69.9 mo) |
|
| 36 | Hysterectomy | NR | 1.5 | Sertoliform, retiform | Significant | 10/10 HPF | Infiltrative | Absent | Present | NR | Negative for NCOA1-3 fusion and JAZF1/SUZ12/PHF1 rearrangement | Pelvis, lung (56.5 mo) |
|
| 55 | Hysterectomy | NR | 13 | Sertoliform, cords, trabeculae | Significant | 2/10 HPF | Infiltrative | Absent | Absent | NR | GREB1-NCOA2 fusion | Pelvis, colon (195.3 mo) |
|
| 48 | Hysterectomy | NR | 2.2 | Sertoliform, retiform | NA | NA | Infiltrative | Absent | NA | NR | NA | Lung (21.1 mo) |
|
Table Legend: HPF: High Power Field, LVI: lymphovascular invasion, mo: months, NA: Not Avaiable; NR: Not Reported; NOS: Not Otherwise Specified; NP: Not performed, ys: year.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



