
Submitted:
12 April 2024
Posted:
17 April 2024
You are already at the latest version
Abstract
Abstract Precision medicine is essentially based on reliable and non-invasive biomarkers. Aim of this review has been to describe the newest biomarkers in the field of kidney transplantation and the kidney rejection, one of the commonest and severe complications. Standard of care tools to identify acute rejection are largely full of errors and of drawbacks. In recent years new and reliable biomarkers have been found. They are avoid of risks, non-invasive and able to detect rejection even in those frequent cases in which acute rejection are clinically asymptomatic and not otherwise identifiable. In recent years several biomarkers have been identified. Very recently have been found new relevant biomarkers able to diagnose rejection with high positive predictive value and low negative predictive value. These are the donor derived cell free DNA found in the recipient, the gene expression profile of the donor found in the recipient and the urinary cytokines that express modification in the graft tissue. The aim of this study has been to find the most recent findings in the literature on this topic and to describe the utility and possible limitation of such new biomarkers on kidney rejection.
Keywords:
Kidney rejection
; biomarkers
; subclinical rejection
; donor derived cell free DNA
; gene expression profile
; urinary cytokines
Introduction and Definitions
Transplant medicine is slowly translating from the “evidence based medicine” to the “precision medicine”. This fact is due to several factors and novel technologies among which biomarkers have a relevant role [1]. Since a long time several papers have been describing the role of biomarkers in renal transplantation [2].
Immunosuppression is a cornerstone in transplantation, but this therapy has to balance from insufficient drug therapy leading to acute or chronic rejection and excessive drug therapy leading to infections or malignancies. We have been delivering our immunosuppressive treatment with indiscriminate monitoring tools for decades in the past waiting for either clinically evident rejection to occur or clinically evident infection or malignancy to develop. The standard-of-care management to monitoring clinical events is shown in Table 1. These have several deficiencies or drawbacks.
Serum creatinine testing is a lagging and not specific marker of injury as well as urine standard testing.
Screening and monitoring donor specific antibodies (DSAs) does not consider that not all DSAs are overtly pathogenic and that there are many unknown non-HLA antibodies.
Drug level monitoring is helpful but non-specific in the absence of other relevant signs.
Renal biopsy has always been considered the gold standard, but is expensive and not without risks/complications. In addition, it is subject to sampling errors and interpreter variability. Finally, the histologic assessment has several limitations, principally if conducted in not expert centers.
As a consequence, there is the need of non-invasive biomarkers that may be distinguished in diagnostic biomarkers, prognostic biomarkers, monitoring biomarkers and pharmacodynamics/response biomarkers, as shown in Table 2 [3,4,5,6,7,8,9,10,11].
In the story of a transplant, before than any disease activity is present risk/susceptibility biomarkers will facilitate the identification of high-risk patients who require closer follow up examinations, which are typically, performed using noninvasive diagnostic biomarkers. After a disease process is diagnosed, a prognostic biomarker estimates the erect of the disease and the chance of spontaneous resolution. A prognostic biomarker should be able to identify those patients who need treatment and those patients who will have a spontaneous disease resolution. If a patient with disease would have a poor outcome, the research for the best appropriate therapy will be based not only based on diagnosis and prognosis, but also based on predictive biomarkers and of safety/pharmacodynamics/response biomarkers and monitoring biomarkers, ideally noninvasive [1].
In this study, several evolving biomarkers in kidney transplantation will be treated as Donor-derived cell-free DNA (dd-cf DNA), Blood gene expression profiles (Trugraf study), Urine biomarkers (CXCL9, gene expression profiles).
Donor-Derived Cell-Free DNA (dd-cfDNA)
This biomarker is based on the fact that allograft cell injury leads to increase of dd-cfDNA in the bloodstream of the recipient [12]. It is a reliable marker of endothelial cell injury and can be elevated in rejection, infection and drug induced kidney injury [13,14,15,16]. It should be considered that there is a possible release of recipient-derived cfDNA by recipient’s immunologic effector cells activated during rejection [15].
In addition, urinary cfDNA (so-called Transrenal DNA) is important. These molecules cross the kidney barrier and appear in the urine [17]. They reflect an increased burden of tissue injury and apoptosis [16]. May be both donor derived and recipient derived.
Overall, there are three clinically available assays:
Allosure (Care Dex)
Prospera (Natera)
TRAC (Virecor Eurofils)
Several questions are still open in understanding the significance of dd-cfDNA in kidney transplant recipients.
There is ongoing debate on whether relative or absolute quantification of dd-cfDNA is more reliable to detect acute transplant injury.
In a recent study from Osmadodja et al. [18], 22 kidney transplant patients underwent dd-cfDNA measurement either as percentage or as absolute. The study concludes that relative dd-cfDNA alone can lead to false negative and false positive results. The use of both absolute and relative dd-cfDNA is better to assure a higher reliability and interindividual comparability.
In a different study, Graver et al. [19] states that the potential benefits and pitfalls of dd-cfDNA are as shown in Table 3. In the same study the authors highlighted that dd-cfDNA are released by allograft into the bloodstream, the level is dependent on allograft health and that level < 0.5% are present in kidney transplant recipients without allograft injury. On the other hand, modification of dd-cfDNA is probably due to injury or rejection. Biopsy is still required to confirm pathological diagnosis.
In a study from Sigdel et al. [20] from the UCSF, the dd-cfDNA was assessed via massively multiplex PCR in 193 kidney transplant patients. All patients were biopsy matched: 38 had active rejection, 72 borderline rejection, 82 had a stable allograft and 25 with different types of injuries. The dd-cfDNA analyzed by the single nucleotide polymorphism (SNP) differentiated patients with active rejection from patients affected by all other conditions (p<0.0001) with high sensitivity (88.7%) and high specificity (77.6%) (Table 4). In this study, dd-cfDNA was not able to differentiate antibody mediated rejection (ABMR) from T cell mediated rejection (TCMR) (p=0.855). This is in contrast with the study of Bloom et al. [21]. In this study dd-cfDNA, levels are higher in ABMR (both chronic and acute) respect to TCMR (2.9% versus 1.2%). This study from the Circulating Donor Derived Cell-Free DNA in Blood for Diagnosing Acute Rejection in Kidney Transplant Recipients (DART) highlights that plasma levels of dd-cfDNA discriminate the active rejection pathogenesis.
Two recent meta-analyses using the existing data, documented the relevance of dd-cfDNA in the diagnosis of kidney rejection [22,23].
The first one analyzed seven studies [24,25,26,27,28] and used the “Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines [29].
The median dd-cfDNA level was significantly higher in patients with ABMR respect to stable patients, while patients with TCMR did not have a different median dd-cfDNA compared to stable patients. Similar results were reported in the other meta-analysis [23], who analyzed nine studies.
In conclusion, dd-cfDNA can be a helpful marker for the diagnosis of ABMR in patients with suspected renal dysfunction, but not probably for patients with TCMR. An explanation of this fact is that ABMR results in a microvascular injury [30], with a release of free DNA after endothelial damage, while TCMR is essentially an interstitial injury that only rarely is associated with endovasculitis [31].
dd-cfDNA may also act as a prognostic tool. Even if several already cited studies documented that high levels of dd-cfDNA are diagnostic for ABMR rejections and not always distinguish TCMR rejection from stable kidneys, a recent study from Stites et al. [32]. This important study documents that high levels of dd-cfDNA identifies patients with TCMR1A and borderline allograft rejection at elevated risk of graft injury. The impact of any acute rejection on the risk of late allograft failure has been also documented by other studies [33,34]. Risk for a poor outcomes of kidney recipients with early posttransplant donor specific anti-HLA antibodies and high dd-cfDNA levels was documented also by the study of Cooper et al. [35].
In the study of Stites [32] were evaluated 79 patients with TCMR1A or borderline rejection. Rejections were evaluated with kidney biopsies, for cause, or for surveillance. Patients were stratified by dd-cfDNA >0.5% or dd-cfDNA < 0.5%. The % change in estimated glomerular filtration rate (eGFR) was measured 3-6 months after evaluation of dd-cfDNA levels and kidney biopsies. The decrease of eGFR, the presence of DSAs and the recurrence of rejection were statistically significant in patients with dd-cfDNA <0.5% respect to patients with dd-cfDNA >0.5%. The results are shown in Table 5.
dd-cfDNA is also important in determining the clinical outcomes of a transplant as determined by monitoring the kidney allografts with a longitudinal surveillance study. The study is called ADMIRAL and s reported by a paper from Bu et al. [36].
The study reports the data of 1094 patients from seven transplant centers. All patients received a single adult kidney, most of them from a deceased donor. The control of dd-cfDNA lasted 3 years posttransplant. In particular was performed an analysis of de novo DSA, of eGFR trajectories and of allograft rejections. Two previous studies [37,38] have already reported that a decline in eGFR is superior to other surrogate measures of long-term kidney transplant outcomes. The ADMIRAL study confirmed that persistently elevated dd-cfDNA (above 0.5%) predicted a >25% decline in eGFR over 3 years. Similarly, dd-cfDNA values >0.5% were associated with a nearly 3-fold increase in the risk of development of de novo donor specific antibody (DSA). Finally, significant elevations in dd-cfDNA were observed during rejection ahead of changes in serum creatinine. In conclusion, the ADMIRAL study demonstrates a broad utility of dd-cfDNA as a leading indicator ahead of clinical presentations of allograft injury, formation of dnDSA, eGFR decline and subclinical rejection.
Treating of dd-cfDNA we have already highlighted the importance of diagnosing subclinical rejection by biomarkers in the absence of clinical signs.
Several studies document the importance of early recognizing the occurrence of early inflammation and sub-clinical rejection.
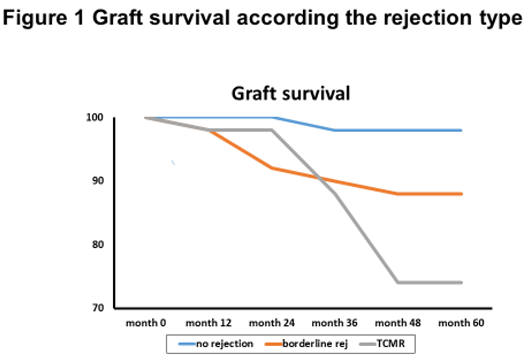
Nankivell et al. [39] evaluated in 551 renal transplant recipients, the clinical and pathological significance of borderline T cell mediated rejection against normal controls and acute TCMR.
The group of patients was followed for 60 months and borderline rejection was associated to renal dysfunction, acute tubular necrosis and chronic tubular atrophy. Additionally, patients with borderline rejection were associated to a reduced graft survival (Figure 1).
Similarly, subclinical inflammation phenotypes and worse long-term renal outcomes have been observed in some group of patients as pediatric kidney transplantation [40] and kidney transplant recipients with a rapid steroid withdrawal protocol [41]. Hence the importance of new biomarkers in addition to dd-cfDNA.
Several studies recognize the importance of gene profile in the diagnosing of early inflammation and subclinical rejection after kidney transplantation.
Gene Expression Profile as Biomarkers
Fridewald et al. [42] documented the development and clinical validity of a novel blood-based molecular biomarker for the diagnosis of subclinical acute rejection following kidney transplantation.
Several previous studies had documented that the gene expression profiles (GEPs) in both urine and blood could detect kidney transplant rejection. The CTOT-04 study [4] documented that a 3-gene signature in urine samples was able to detect kidney rejection. In a similar way, the CTOT-01 study [43] documented that urine CXCL9 protein revealed the existing of rejection. In the CTOT-08 study [42], Fridewald et al. demonstrated the clinical validity of the clinical significance of both the clinical phenotype (CP) and GEP of subclinical acute rejection within the first 12 months on the composite clinical endpoint. The same study documented in these subjects the development of de novo DNAs by the 24 months. In particular, in the CTOT-08 study, the gene expression profile consisted of 120 genes that are up and down regulated and specifically chosen to distinguish stable normal biopsy from subclinical rejection.
In a different study, Zhang et al. [44], examined 191 kidney transplant patients from the prospective Genomic of Chronic Allograft Rejection (GoCAR) study [45], who underwent surveillance biopsies over 2 years and identified patients with subclinical or borderline acute cellular rejection (ACR) at three months (ACR-3) post transplant. These patients had a subsequent worse outcome with decline in renal function and decreased graft survival. Using a RNA sequencing analysis, the authors identified a 17-gene signature (Table 6). This TREx assay based on the 17-gene set achieved PPV of 0.79 and NPV of 0.98 for subclinical ACR diagnosis.This set was validated and represents a peripheral blood gene expression signature to diagnose subclinical acute rejection and to risk stratify kidney transplant recipients.
An important blood gene expression classifier in the field of kidney transplantation is the TruGraf. It represents a novel molecular biomarker for managing kidney transplant recipients with stable renal function [46]. The TruGraf algorithm is a DNA microarray-based gene expression algorithm that analyzes the gene expression profile of 120 genes. In the original study it was designed to avoid surveillance biopsies and was validated in multiple cohorts. Simultaneous blood tests and clinical assessments have been performed on 192 patients from seven transplant centers [46]. Evaluating the results of TruGraf blood test and compared with clinical phenotype in 99 kidney transplant recipients with stable renal function and biopsy confirmed phenotypes and in 63 kidney transplant patients with stable renal function but with per protocol biopsy documenting subclinical rejection, the accuracy was 74% in patients without rejection and 80% in patients with rejection. The overall negative predictive value was 89% and the positive predictive value 48% with sensitivity of 71% and specificity of 75%. The conclusion of the study was in favor of a clinical decision without unnecessary surveillance biopsies basing on an accurate gene expression profile (GEP).
Basing on TruGraf method Heilman et al. [47] conducted a prospective study obtaining peripheral blood at five time points in the first year post transplant to obtain GEP. Overall, 240 kidney transplant patients have been enrolled and stratified into three groups according the absence or presence of one or more GEP. Presence of multiple GEP correlated with a poorer histological aspects, lower eGFR and higher death censored graft loss.
We have described the relevance in diagnosing subclinical rejection of dd-cfDNA and the gene expression profile. A question is whether blood gene expression assays and donor-derived cell free DNA may be used together to diagnose subclinical rejection. Park et al. [48] have provided an answer to this question recently.
In this study, the authors enrolled 208 subjects for a total of 428 biopsies samples. The study was a post hoc analysis of the clinical Trial in Organ Transplantation 08. Surveillance biopsies have been performed from month 2 to month 6 post-transplant and at month 12 and 24.
Patients were simultaneously followed by gene expression profile assay (TruGraf method); donor derived cfDNA and combined tests. Observing the diagnosis of subclinical rejection, the authors reported a PPV of 47% with gene profile, of 56% with dd-cfDNA, of 81% with the combined tests.
A NPV was 82% with gene profile, 84% with dd-cfDNA and 88% with combined tests. The area under the receiver operating characteristic curve (AUROC) values was similar with each method. Overall, the GEP was better at detecting cellular rejection and dd-cfDNA was better in detecting antibody rejection.
In conclusion, donor derived cell free DNA and gene expression profiles provide a less invasive monitoring strategy for subclinical rejection with different detection of antibody and cell mediated rejection.
Urinary RNA Profile for the Diagnosis of Rejection
Independently from the information on clinical or subclinical rejection that can be drawn from the blood, the urine too may allow the rejection diagnosis of a kidney graft in a non-invasive method.
Li et al. [49] comparing the urine specimen from 22 kidney graft with a biopsy confirmed acute rejection with 63 grafts without biopsy-confirmed acute rejection found higher levels of perforin mRNA and granzyme B mRNA in patients with biopsy confirmed acute rejection. Both mRNA encode the cytotoxic proteins.
The authors divided the patients in four groups (acute rejection, stable graft function, other pathological findings not rejection related, and chronic rejection). The levels of perforin mRNA were significantly higher in patients with acute rejection than patients with stable renal function (p<0.001), patients with other findings (p<0.001) and patients with chronic rejection (p=0.03).
This was not the case of granzyme B mRNA levels, which were not able to distinguish patients with acute rejection from patients with chronic rejection (p =0.12).
The authors conclude that urinary mRNA levels of perforin and granzyme B are a useful noninvasive tool for the diagnosis of acute rejection, but levels of granzyme B mRNA were not able to distinguish acute rejection from chronic rejection.
We have already cited the study of Suthanthiran et al. [4]. One year later the same authors published another more extensive study on the urinary mRNA profile and acute rejection in kidney transplant recipients [50]. Overall, a total of 4300 urine samples were collected from 485 patients for urinary-cell messenger RNA (mRNA) repeatedly after transplantation and at the time of kidney allograft biopsy. Urinary mRNA has been examined for CD3 ε perforin, granzyme B, interferon-inducible protein 10 (IP-10), CXCR3, CD103, transforming growth factor β (TGF β) and proteinase inhibitor 9. Patients were divided into three groups (acute cellular rejection, No rejection; and stable function in patients which did not receive renal biopsy). The mRNA levels of CD ε perforin, granzyme B, and IP-10 differed significantly among the three groups (p< =.001), but not the levels of CXCR3 (p = 0.06), CD 103 (p = 0.13), TGFβ (p = 0.11), and proteinase inhibitor 9 (p = 0.38).
The authors conclude that CD3 εmRNA, IP-10 mRNA and 18S rRNA levels in urinary cells appear to be diagnostic of acute rejection in kidney allografts.
In another study [51], messenger RNA (mRNA) for FOXP3, a specification and functional factor for regulatory T lymphocytes, and mRNA for CD25, CD3εperforin, and 18S ribosomal RNA (rRNA) were examined in urine specimen of patients with acute rejection, with chronic allograft nephropathy and in patients with a normal renal biopsy. In particular, was examined the relationship of these mRNA levels and acute rejection, rejection reversal and graft failure. mRNA levels for all the factors studied were significantly higher in acute rejection than chronic rejection and stable graft function (p<0.001). FOXP3 mRNA was the only one factor that related with reversibility. Patients with higher FOXP3 mRNA had lower possibility to have a reversible rejection. Similarly, patients with higher FOXP3 mRNA had higher risk of graft loss. On the contrary, mRNA for CD25, CD3εperforin, and 18S ribosomal RNA (rRNA) did not had relationship with rejection reversibility and risk of graft loss.
In the already cited study from Hricik et al. [43], have been enrolled 280 kidney transplant patients, principally from living donors to evaluate and compare urinary biomarkers useful for a sure diagnosis of acute rejection. At the time of collecting urine, all patients received a for-cause renal biopsy. Urinary samples were examined for sediment RNA already known to be elevated for acute rejection as CCR1, CCR5, CXCR3, CCL5, CXCL9 (cytokine induced by interferon gamma), CXCL10, IL-8, perforin and granzyme B [52,53,54].
Using a correlation analysis, many of these substances highly correlated and showed interdependence. CXCL9 and CXCL10 documented the higher significant in diagnosing acute rejection. CXCL 10 was higher in patients with acute rejection and in patients with infections. Therefore, in the author’s opinion CXCL9 is the protein with the higher significance in diagnosing acute rejection and in distinguishing acute rejection from other renal injuries. In detail, CXCL9 in acute rejection diagnosis had an area under the curve (AUC) of 0.856, a PPV of 67.6% and a NPV of 92%. The addition of CXCL10 did not modified the results.
However, the utility on the use of urinary cytokines as noninvasive biomarkers is the diagnosis of acute rejection is discussed by other studies, which found several controversies. In a French retrospective study [55], reviewing 329 transplanted patients, the utility of urinary CXCL9 and CXCL10 is discussed as a noninvasive method to diagnosing allograft rejection. To be considered in the retrospective study, all patients should have an allograft biopsy specimen, concomitant urine samples and blood research for BKV infection. Indeed, the study documented that a similar elevation of these urinary cytokines is found in the case of acute rejection as well as in the case of BKV infection and in the case of urinary tract infection frequently observed in kidney transplant subjects.
In a different and very, recent study [56] was evaluated the utility of urinary CXCL 10 to monitoring the renal allograft. In the study, patients were divided in two arms. The intervention arm (120 patients) and the control arm (121 patients. In both arms urine for detecting CXCL 10 were collected at month 1, 3 and 6. If elevated, renal biopsy was made and the subsequent treatment of rejection in intervention arm. In the control arm, the results were concealed. At 1 year were evaluated the death censored graft loss, the existence of an acute rejection, the presence of de novo DSA and the presence of an eGFR < 25 ml/min. Considering the combined endpoint at 1 year, the intervention arm and the control arm did not differ (51% vs 49%) and the study could not demonstrate the beneficial effect of urine CXCL 10 monitoring.
On the other hand, another study from Hricik et al. for the Clinical Trials in Organ Transplantation-09 Consortium [57] documented the usefulness of cytokines and other tools in predicting high-risk patients. The study had the aim of analyzing the safety of Tacrolimus withdrawal in immune-quiescent kidney transplant recipients. Overall, were randomized 21 patients, 14 in the tacrolimus withdrawal group, 7 in the control group. The study was terminated prematurely because of the high risk of acute rejection in the tacrolimus withdrawal group. High mismatches pretransplant, donor-reactive IFN-γ ELISPOT assay and high levels of urinary CXCL9 were all predictive of the development of acute rejection or/and development of DSAs in the tacrolimus withdrawal arm.
Table 7 highlights the main challenges in the field of finding new biomarkers.
Conclusions
In conclusion, multiple new non-invasive and invasive biomarkers are changing the paradigm of rejection diagnosis and immunosuppression management.
Further refinement of the proper context of use and interpretation of these tests will shape patient care as transplantation moves further into the field of personalized medicine.
Well designed, interventional clinical trials using these tools are the next logical step in development.
Author Contributions
Salvadori M, Rosati A and Rosso G contributed equally to the manuscript; Salvadori M designed the study. Rosso G collected the data from the literature; Salvadori M and Rosatin A analyzed the collected data; Salvadori M, Rosati A and Rosso G wrote the manuscript. All the authors performed and approved the last revision.
Conflict of interest statement
Maurizio Salvadori, Alberto Rosati and Giuseppina Rosso do not have any conflict of interest in relation with the manuscript.
References
- Naesens, M.; Anglicheau, D. Precision Transplant Medicine: Biomarkers to the Rescue. J Am Soc Nephrol. 2018, 29, 24–34. [Google Scholar] [CrossRef]
- Salvadori, M.; Tsalouchos, A. Microbiota, renal disease and renal transplantation. World J Transplant. 2021, 11, 16–36. [Google Scholar] [CrossRef] [PubMed]
- Anglicheau, D.; Naesens, M.; Essig, M.; Gwinner, W.; Marquet, P. Establishing Biomarkers in Transplant Medicine: A Critical Review of Current Approaches. Transplantation. 2016, 100, 2024–2038. [Google Scholar] [CrossRef]
- Suthanthiran, M.; Schwartz, J.E.; Ding, R.; Abecassis, M.; Dadhania, D.; Samstein, B.; Knechtle, S.J.; Friedewald, J.; Becker, Y.T.; Sharma, V.K.; Williams, N.M.; Chang, C.S.; Hoang, C.; Muthukumar, T.; August, P.; Keslar, K.S.; Fairchild, R.L.; Hricik, D.E.; Heeger, P.S.; Han, L.; Liu, J.; Riggs, M.; Ikle, D.N.; Bridges, N.D.; Shaked, A. Clinical Trials in Organ Transplantation 04 (CTOT-04) Study Investigators. Urinary-cell mRNA profile and acute cellular rejection in kidney allografts. Transplantation. 2012, 93, 1136–1146. [Google Scholar]
- Roedder, S.; Sigdel, T.; Salomonis, N.; Hsieh, S.; Dai, H.; Bestard, O.; Metes, D.; Zeevi, A.; Gritsch, A.; Cheeseman, J.; Macedo, C.; Peddy, R.; Medeiros, M.; Vincenti, F.; Asher, N.; Salvatierra, O.; Shapiro, R.; Kirk, A.; Reed, E.F.; Sarwal, M.M. The kSORT assay to detect renal transplant patients at high risk for acute rejection: results of the multicenter AART study. PLoS Med. 2014, 11, e1001759. [Google Scholar] [CrossRef] [PubMed]
- Kurian, S.M.; Williams, A.N.; Gelbart, T.; Campbell, D.; Mondala, T.S.; Head, S.R.; Horvath, S.; Gaber, L.; Thompson, R.; Whisenant, T.; Lin, W.; Langfelder, P.; Robison, E.H.; Schaffer, R.L.; Fisher, J.S.; Friedewald, J.; Flechner, S.M.; Chan, L.K.; Wiseman, A.C.; Shidban, H.; Mendez, R.; Heilman, R.; Abecassis, M.M.; Marsh, C.L.; Salomon, D.R. Molecular classifiers for acute kidney transplant rejection in peripheral blood by whole genome gene expression profiling. Am J Transplant. 2014, 14, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Lefaucheur, C.; Vernerey, D.; Prugger, C.; Duong van Huyen, J.P.; Mooney, N.; Suberbielle, C.; Frémeaux-Bacchi, V.; Méjean, A.; Desgrandchamps, F.; Anglicheau, D.; Nochy, D.; Charron, D.; Empana, J.P.; Delahousse, M.; Legendre, C.; Glotz, D.; Hill, G.S.; Zeevi, A.; Jouven, X. Complement-binding anti-HLA antibodies and kidney-allograft survival. N Engl J Med. 2013, 369, 1215–1226. [Google Scholar] [CrossRef]
- Sicard, A.; Ducreux, S.; Rabeyrin, M.; Couzi, L.; McGregor, B.; Badet, L.; Scoazec, J.Y.; Bachelet, T.; Lepreux, S.; Visentin, J.; Merville, P.; Fremeaux-Bacchi, V.; Morelon, E.; Taupin, J.L.; Dubois, V.; Thaunat, O. Detection of C3d-binding donor-specific anti-HLA antibodies at diagnosis of humoral rejection predicts renal graft loss. J Am Soc Nephrol. 2015, 26, 457–467. [Google Scholar] [CrossRef]
- Einecke, G.; Reeve, J.; Sis, B.; Mengel, M.; Hidalgo, L.; Famulski, K.S.; Matas, A.; Kasiske, B.; Kaplan, B.; Halloran, P.F. A molecular classifier for predicting future graft loss in late kidney transplant biopsies. J Clin Invest. 2010, 120, 1862–1872. [Google Scholar] [CrossRef]
- Loupy, A.; Lefaucheur, C.; Vernerey, D.; Chang, J.; Hidalgo, L.G.; Beuscart, T.; Verine, J.; Aubert, O.; Dubleumortier, S.; Duong van Huyen, J.P.; Jouven, X.; Glotz, D.; Legendre, C.; Halloran, P.F. Molecular microscope strategy to improve risk stratification in early antibody-mediated kidney allograft rejection. J Am Soc Nephrol. 2014, 25, 2267–2277. [Google Scholar] [CrossRef]
- O‘Connell, P.J.; Zhang, W.; Menon, M.C.; Yi, Z.; Schröppel, B.; Gallon, L.; Luan, Y.; Rosales, I.A.; Ge, Y.; Losic, B.; Xi, C.; Woytovich, C.; Keung, K.L.; Wei, C.; Greene, I.; Overbey, J.; Bagiella, E.; Najafian, N.; Samaniego, M.; Djamali, A.; Alexander, S.I.; Nankivell, B.J.; Chapman, J.R.; Smith, R.N.; Colvin, R.; Murphy, B. Biopsy transcriptome expression profiling to identify kidney transplants at risk of chronic injury: a multicentre, prospective study. Lancet. 2016, 388, 983–993. [Google Scholar] [CrossRef] [PubMed]
- Gielis, E.M.; Ledeganck, K.J.; De Winter, B.Y.; Del Favero, J.; Bosmans, J.L.; Claas, F.H.; Abramowicz, D.; Eikmans, M. Cell-Free DNA: An Upcoming Biomarker in Transplantation. Am J Transplant. 2015, 15, 2541–2551. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Bierau, S.; Balzer, S.; Andag, R.; Kanzow, P.; Schmitz, J.; Gaedcke, J.; Moerer, O.; Slotta, J.E.; Walson, P.; Kollmar, O.; Oellerich, M.; Schütz, E. Digital droplet PCR for rapid quantification of donor DNA in the circulation of transplant recipients as a potential universal biomarker of graft injury. Clin Chem. 2013, 59, 1732–1741. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Tong, K.L.; Li, P.K.; Chan, A.Y.; Yeung, C.K.; Pang, C.C.; Wong, T.Y.; Lee, K.C.; Lo, Y.M. Presence of donor- and recipient-derived DNA in cell-free urine samples of renal transplantation recipients: urinary DNA chimerism. Clin Chem. 1999, 45, 1741–1746. [Google Scholar] [CrossRef] [PubMed]
- García Moreira, V.; Prieto García, B.; Baltar Martín, J.M.; Ortega Suárez, F.; Alvarez, F.V. Cell-free DNA as a noninvasive acute rejection marker in renal transplantation. Clin Chem. 2009, 55, 1958–1966. [Google Scholar] [CrossRef] [PubMed]
- Sigdel, T.K.; Vitalone, M.J.; Tran, T.Q.; Dai, H.; Hsieh, S.C.; Salvatierra, O.; Sarwal, M.M. A rapid noninvasive assay for the detection of renal transplant injury. Transplantation. 2013, 96, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Botezatu, I.; Serdyuk, O.; Potapova, G.; Shelepov, V.; Alechina, R.; Molyaka, Y.; Ananév, V.; Bazin, I.; Garin, A.; Narimanov, M.; Knysh, V.; Melkonyan, H.; Umansky, S.; Lichtenstein, A. Genetic analysis of DNA excreted in urine: a new approach for detecting specific genomic DNA sequences from cells dying in an organism. Clin Chem. 2000, 46, 1078–1084. [Google Scholar] [CrossRef]
- Osmanodja, B.; Akifova, A.; Budde, K.; Choi, M.; Oellerich, M.; Schütz, E.; Beck, J. Absolute or Relative Quantification of Donor-derived Cell-free DNA in Kidney Transplant Recipients: Case Series. Transplant Direct. 2021, 7, e778. [Google Scholar] [CrossRef]
- Graver, A.S.; Lee, D.; Power, D.A.; Whitlam, J.B. Understanding Donor-derived Cell-free DNA in Kidney Transplantation: An Overview and Case-based Guide for Clinicians. Transplantation. 2023, 107, 1675–1686. [Google Scholar] [CrossRef]
- Sigdel, T.K.; Archila, F.A.; Constantin, T.; Prins, S.A.; Liberto, J.; Damm, I.; Towfighi, P.; Navarro, S.; Kirkizlar, E.; Demko, Z.P.; Ryan, A.; Sigurjonsson, S.; Sarwal, R.D.; Hseish, S.C.; Chan-On, C.; Zimmermann, B.; Billings, P.R.; Moshkevich, S.; Sarwal, M.M. Optimizing Detection of Kidney Transplant Injury by Assessment of Donor-Derived Cell-Free DNA via Massively Multiplex PCR. J Clin Med. 2018, 8, 19. [Google Scholar] [CrossRef]
- Bloom, R.D.; Bromberg, J.S.; Poggio, E.D.; Bunnapradist, S.; Langone, A.J.; Sood, P.; Matas, A.J.; Mehta, S.; Mannon, R.B.; Sharfuddin, A.; Fischbach, B.; Narayanan, M.; Jordan, S.C.; Cohen, D.; Weir, M.R.; Hiller, D.; Prasad, P.; Woodward, R.N.; Grskovic, M.; Sninsky, J.J.; Yee, J.P.; Brennan, D.C. Circulating Donor-Derived Cell-Free DNA in Blood for Diagnosing Active Rejection in Kidney Transplant Recipients (DART) Study Investigators. Cell-Free DNA and Active Rejection in Kidney Allografts. J Am Soc Nephrol. 2017, 28, 2221–2232. [Google Scholar] [CrossRef]
- Wijtvliet, V.P.W.M.; Plaeke, P.; Abrams, S.; Hens, N.; Gielis, E.M.; Hellemans, R.; Massart, A.; Hesselink, D.A.; De Winter, B.Y.; Abramowicz, D.; Ledeganck, K.J. Donor-derived cell-free DNA as a biomarker for rejection after kidney transplantation: a systematic review and meta-analysis. Transpl Int. 2020, 33, 1626–1642. [Google Scholar] [CrossRef]
- Xiao, H.; Gao, F.; Pang, Q.; Xia, Q.; Zeng, X.; Peng, J.; Fan, L.; Liu, J.; Wang, Z.; Li, H. Diagnostic Accuracy of Donor-derived Cell-free DNA in Renal-allograft Rejection: A Meta-analysis. Transplantation. 2021, 105, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Oellerich, M.; Shipkova, M.; Asendorf, T.; Walson, P.D.; Schauerte, V.; Mettenmeyer, N.; Kabakchiev, M.; Hasche, G.; Gröne, H.J.; Friede, T.; Wieland, E.; Schwenger, V.; Schütz, E.; Beck, J. Absolute quantification of donor-derived cell-free DNA as a marker of rejection and graft injury in kidney transplantation: Results from a prospective observational study. Am J Transplant. 2019, 19, 3087–3099. [Google Scholar] [CrossRef]
- Whitlam, J.B.; Ling, L.; Skene, A.; Kanellis, J.; Ierino, F.L.; Slater, H.R.; Bruno, D.L.; Power, D.A. Diagnostic application of kidney allograft-derived absolute cell-free DNA levels during transplant dysfunction. Am J Transplant. 2019, 19, 1037–1049. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zheng, C.; Li, X.; Fu, Q.; Li, J.; Su, Q.; Zeng, L.; Liu, Z.; Wang, J.; Huang, H.; Xu, B.; Ye, M.; Liu, L.; Wang, C. Diagnostic Performance of Donor-Derived Plasma Cell-Free DNA Fraction for Antibody-Mediated Rejection in Post Renal Transplant Recipients: A Prospective Observational Study. Front Immunol. 2020, 11, 342. [Google Scholar] [CrossRef]
- Bromberg, J.S.; Brennan, D.C.; Poggio, E.; Bunnapradist, S.; Langone, A.; Sood, P.; Matas, A.J.; Mannon, R.B.; Mehta, S.; Sharfuddin, A.; Fischbach, B.; Narayanan, M.; Jordan, S.C.; Cohen, D.J.; Zaky, Z.S.; Hiller, D.; Woodward, R.N.; Grskovic, M.; Sninsky, J.J.; Yee, J.P.; Bloom, R.D. Biological Variation of Donor-Derived Cell-Free DNA in Renal Transplant Recipients: Clinical Implications. J Appl Lab Med. 2017, 2, 309–321. [Google Scholar] [CrossRef]
- Huang, E.; Sethi, S.; Peng, A.; Najjar, R.; Mirocha, J.; Haas, M.; Vo, A.; Jordan, S.C. Early clinical experience using donor-derived cell-free DNA to detect rejection in kidney transplant recipients. Am J Transplant. 2019, 19, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Loupy, A. Antibody-Mediated Rejection of Solid-Organ Allografts. N Engl J Med. 2018, 379, 2580–2582. [Google Scholar]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; Alachkar, N.; Bagnasco, S.; Bouatou, Y.; Becker, J.U.; Cornell, L.D.; Duong van Huyen, J.P.; Gibson, I.W.; Kraus, E.S.; Mannon, R.B.; Naesens, M.; Nickeleit, V.; Nickerson, P.; Segev, D.L.; Singh, H.K.; Stegall, M.; Randhawa, P.; Racusen, L.; Solez, K.; Mengel, M. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am J Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Stites, E.; Kumar, D.; Olaitan, O.; John Swanson, S.; Leca, N.; Weir, M.; Bromberg, J.; Melancon, J.; Agha, I.; Fattah, H.; Alhamad, T.; Qazi, Y.; Wiseman, A.; Gupta, G. High levels of dd-cfDNA identify patients with TCMR 1A and borderline allograft rejection at elevated risk of graft injury. Am J Transplant. 2020, 20, 2491–2498. [Google Scholar] [CrossRef]
- Pallardó Mateu, L.M.; Sancho Calabuig, A.; Capdevila Plaza, L.; Franco Esteve, A. Acute rejection and late renal transplant failure: risk factors and prognosis. Nephrol Dial Transplant, 2004; 19, (Suppl. 3), iii38–42. [Google Scholar]
- Jevnikar, A.M.; Mannon, R.B. Late kidney allograft loss: what we know about it, and what we can do about it. Clin J Am Soc Nephrol. 2008, 3 (Suppl. 2), S56–S67. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.E.; Gralla, K.; Chan, K. Clinical significance of post kidney transplant de novo DSA in otherwise stable grafts. Clin Transpl 2011, 35, 359–364. [Google Scholar]
- Bu, L.; Gupta, G.; Pai, A.; Anand, S.; Stites, E.; Moinuddin, I.; Bowers, V.; Jain, P.; Axelrod, D.A.; Weir, M.R.; Wolf-Doty, T.K.; Zeng, J.; Tian, W.; Qu, K.; Woodward, R.; Dholakia, S.; De Golovine, A.; Bromberg, J.S.; Murad, H.; Alhamad, T. Clinical outcomes from the Assessing Donor-derived cell-free DNA Monitoring Insights of kidney Allografts with Longitudinal surveillance (ADMIRAL) study. Kidney Int. 2022, 101, 793–803. [Google Scholar] [CrossRef]
- Clayton, P.A.; Lim, W.H.; Wong, G.; Chadban, S.J. Relationship between eGFR Decline and Hard Outcomes after Kidney Transplants. J Am Soc Nephrol. 2016, 27, 3440–3446. [Google Scholar] [CrossRef] [PubMed]
- Faddoul, G.; Nadkarni, G.N.; Bridges, N.D.; Goebel, J.; Hricik, D.E.; Formica, R.; Menon, M.C.; Morrison, Y.; Murphy, B.; Newell, K.; Nickerson, P.; Poggio, E.D.; Rush, D.; Heeger, P.S. CTOT-17 consortium. Analysis of Biomarkers Within the Initial 2 Years Posttransplant and 5-Year Kidney Transplant Outcomes: Results From Clinical Trials in Organ Transplantation-17. Transplantation. 2018, 102, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Nankivell, B.J.; Agrawal, N.; Sharma, A.; Taverniti, A.; P‘Ng, C.H.; Shingde, M.; Wong, G.; Chapman, J.R. The clinical and pathological significance of borderline T cell-mediated rejection. Am J Transplant. 2019, 19, 1452–1463. [Google Scholar] [CrossRef] [PubMed]
- Seifert, M.E.; Yanik, M.V.; Feig, D.I.; Hauptfeld-Dolejsek, V.; Mroczek-Musulman, E.C.; Kelly, D.R.; Rosenblum, F.; Mannon, R.B. Subclinical inflammation phenotypes and long-term outcomes after pediatric kidney transplantation. Am J Transplant. 2018, 18, 2189–2199. [Google Scholar] [CrossRef]
- Mehta, R.; Bhusal, S.; Randhawa, P.; Sood, P.; Cherukuri, A.; Wu, C.; Puttarajappa, C.; Hoffman, W.; Shah, N.; Mangiola, M.; Zeevi, A.; Tevar, A.D.; Hariharan, S. Short-term adverse effects of early subclinical allograft inflammation in kidney transplant recipients with a rapid steroid withdrawal protocol. Am J Transplant. 2018, 18, 1710–1717. [Google Scholar] [CrossRef]
- Friedewald, J.J.; Kurian, S.M.; Heilman, R.L.; Whisenant, T.C.; Poggio, E.D.; Marsh, C.; Baliga, P.; Odim, J.; Brown, M.M.; Ikle, D.N.; Armstrong, B.D.; Charette, J.I.; Brietigam, S.S.; Sustento-Reodica, N.; Zhao, L.; Kandpal, M.; Salomon, D.R.; Abecassis, M.M. Clinical Trials in Organ Transplantation 08 (CTOT-08). Development and clinical validity of a novel blood-based molecular biomarker for subclinical acute rejection following kidney transplant. Am J Transplant. 2019, 19, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Hricik, D.E.; Nickerson, P.; Formica, R.N.; Poggio, E.D.; Rush, D.; Newell, K.A.; Goebel, J.; Gibson, I.W.; Fairchild, R.L.; Riggs, M.; Spain, K.; Ikle, D.; Bridges, N.D.; Heeger, P.S. CTOT-01 consortium.Multicenter validation of urinary CXCL9 as a risk-stratifying biomarker for kidney transplant injury. Am J Transplant. 2013, 13, 2634–2644. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Yi, Z.; Keung, K.L.; Shang, H.; Wei, C.; Cravedi, P.; Sun, Z.; Xi, C.; Woytovich, C.; Farouk, S.; Huang, W.; Banu, K.; Gallon, L.; Magee, C.N.; Najafian, N.; Samaniego, M.; Djamali, A.; Alexander, S.I.; Rosales, I.A.; Smith, R.N.; Xiang, J.; Lerut, E.; Kuypers, D.; Naesens, M.; O‘Connell, P.J.; Colvin, R.; Menon, M.C.; Murphy, B. A Peripheral Blood Gene Expression Signature to Diagnose Subclinical Acute Rejection. J Am Soc Nephrol. 2019, 30, 1481–1494. [Google Scholar] [CrossRef] [PubMed]
- Yazdani, S.; Naesens, M. Foretelling Graft Outcome by Molecular Evaluation of Renal Allograft Biopsies: The GoCAR Study. Transplantation. 2017, 101, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Marsh, C.L.; Kurian, S.M.; Rice, J.C.; Whisenant, T.C.; David, J.; Rose, S.; Schieve, C.; Lee, D.; Case, J.; Barrick, B.; Peddi, V.R.; Mannon, R.B.; Knight, R.; Maluf, D.; Mandelbrot, D.; Patel, A.; Friedewald, J.J.; Abecassis, M.M.; First, M.R. Application of TruGraf v1: A Novel Molecular Biomarker for Managing Kidney Transplant Recipients With Stable Renal Function. Transplant Proc. 2019, 51, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Heilman, R.L.; Fleming, J.N.; Mai, M.; Smith, B.; Park, W.D.; Holman, J.; Stegall, M.D. Multiple abnormal peripheral blood gene expression assay results are correlated with subsequent graft loss after kidney transplantation. Clin Transplant. 2023, 37, e14987. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Guo, K.; Heilman, R.L.; Poggio, E.D.; Taber, D.J.; Marsh, C.L.; Kurian, S.M.; Kleiboeker, S.; Weems, J.; Holman, J.; Zhao, L.; Sinha, R.; Brietigam, S.; Rebello, C.; Abecassis, M.M.; Friedewald, J.J. Combining Blood Gene Expression and Cellfree DNA to Diagnose Subclinical Rejection in Kidney Transplant Recipients. Clin J Am Soc Nephrol. 2021, 16, 1539–1551. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Hartono, C.; Ding, R.; Sharma, V.K.; Ramaswamy, R.; Qian, B.; Serur, D.; Mouradian, J.; Schwartz, J.E.; Suthanthiran, M. Noninvasive diagnosis of renal-allograft rejection by measurement of messenger RNA for perforin and granzyme B in urine. N Engl J Med. 2001, 344, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Suthanthiran, M.; Schwartz, J.E.; Ding, R.; Abecassis, M.; Dadhania, D.; Samstein, B.; Knechtle, S.J.; Friedewald, J.; Becker, Y.T.; Sharma, V.K.; Williams, N.M.; Chang, C.S.; Hoang, C.; Muthukumar, T.; August, P.; Keslar, K.S.; Fairchild, R.L.; Hricik, D.E.; Heeger, P.S.; Han, L.; Liu, J.; Riggs, M.; Ikle, D.N.; Bridges, N.D.; Shaked, A. Clinical Trials in Organ Transplantation 04 (CTOT-04) Study Investigators. Urinary-cell mRNA profile and acute cellular rejection in kidney allografts. N Engl J Med. 2013, 369, 20–31. [Google Scholar] [CrossRef]
- Muthukumar, T.; Dadhania, D.; Ding, R.; Snopkowski, C.; Naqvi, R.; Lee, J.B.; Hartono, C.; Li, B.; Sharma, V.K.; Seshan, S.V.; Kapur, S.; Hancock, W.W.; Schwartz, J.E.; Suthanthiran, M. Messenger RNA for FOXP3 in the urine of renal-allograft recipients. N Engl J Med. 2005, 353, 2342–2351. [Google Scholar] [CrossRef]
- Ho, J.; Wiebe, C.; Gibson, I.W.; Rush, D.N.; Nickerson, P.W. Immune monitoring of kidney allografts. Am J Kidney Dis. 2012, 60, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Panzer, U.; Reinking, R.R.; Steinmetz, O.M.; Zahner, G.; Sudbeck, U.; Fehr, S.; Pfalzer, B.; Schneider, A.; Thaiss, F.; Mack, M.; Conrad, S.; Huland, H.; Helmchen, U.; Stahl, R.A. CXCR3 and CCR5 positive T-cell recruitment in acute human renal allograft rejection. Transplantation. 2004, 78, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Rottman, J.B.; Myers, P.; Kassam, N.; Weinblatt, M.; Loetscher, M.; Koch, A.E.; Moser, B.; Mackay, C.R. The chemokine receptors CXCR3 and CCR5 mark subsets of T cells associated with certain inflammatory reactions. J Clin Invest. 1998, 101, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Tinel, C.; Devresse, A.; Vermorel, A.; Sauvaget, V.; Marx, D.; Avettand-Fenoel, V.; Amrouche, L.; Timsit, M.O.; Snanoudj, R.; Caillard, S.; Moulin, B.; Olagne, J.; Essig, M.; Gwinner, W.; Naesens, M.; Marquet, P.; Legendre, C.; Terzi, F.; Rabant, M.; Anglicheau, D. Development and validation of an optimized integrative model using urinary chemokines for noninvasive diagnosis of acute allograft rejection. Am J Transplant. 2020, 20, 3462–3476. [Google Scholar] [CrossRef] [PubMed]
- Hirt-Minkowski, P.; Handschin, J.; Stampf, S.; Hopfer, H.; Menter, T.; Senn, L.; Hönger, G.; Wehmeier, C.; Amico, P.; Steiger, J.; Koller, M.; Dickenmann, M.; Schaub, S. Randomized Trial to Assess the Clinical Utility of Renal Allograft Monitoring by Urine CXCL10 Chemokine. J Am Soc Nephrol. 2023, 34, 1456–1469. [Google Scholar] [CrossRef]
- Hricik, D.E.; Formica, R.N.; Nickerson, P.; Rush, D.; Fairchild, R.L.; Poggio, E.D.; Gibson, I.W.; Wiebe, C.; Tinckam, K.; Bunnapradist, S.; Samaniego-Picota, M.; Brennan, D.C.; Schröppel, B.; Gaber, O.; Armstrong, B.; Ikle, D.; Diop, H.; Bridges, N.D.; Heeger, P.S. Clinical Trials in Organ Transplantation-09 Consortium. Adverse Outcomes of Tacrolimus Withdrawal in Immune-Quiescent Kidney Transplant Recipients. J Am Soc Nephrol. 2015, 26, 3114–3122. [Google Scholar] [CrossRef]

Table 1.
Standard-of-care management to monitoring clinical events and their drawbacks.
| Serum creatinine testing | Creatinine is a lagging and non-specific marker of injury |
| Urine testing | Non-specific |
| Transplant ultrasonography | Non-specific |
| Screening and monitoring donor specific antibodies (DSA) | Not all DSAs are overtly pathogenic, many unknown non-HLA Abs |
| Drug level monitoring | Non-specific |
| Renal biopsy | Expensive and not without complications Subject to sampling error and interpreter variability Histologic assessment has limitations |
Table 2.
Overview of biomarker subtypes and assessment of kidney allografts.
| Biomarker Type | Biomarker Definition | Established Examples in Transplantation | Potential new Examples in Transplantation |
|---|---|---|---|
| Diagnostic biomarker | A biomarker used to identify individuals with the disease or condition of interest or define a subset of the disease | Serum creatinine Proteinuria Hematuria DSA Signs of hemolysis Renal ultrasound examination Protocol or for cause biopsy histology |
Urinary three gene mRNA expression signature and wide range of other suggested molecules [3,4] Wide range of urinary target proteins, like CXCL10 and CXCL9 [3] Blood 17-gene mRNA expression “kSORT” [5] Blood 200-gene mRNA expression “TruGraf” [6] Several blood and urine mRNAs [3] Molecular microscope for allograft pathology |
| Prognostic biomarker | A biomarker used to identify likelihood of a clinical event, disease recurrence, or progression | Serum creatinine Proteinuria DSA Protocol or for cause biopsy histology |
Complement-fixing characteristics of DSA [7,8] Edmonton classifier for graft loss [9] Edmonton ABMR molecular score [10]GOCAR 13-gene set [11] |
| Monitoring biomarker | A biomarker measured serially and used to detect a change in the degree or extent of disease; monitoring biomarkers may also be used to indicate toxicity, assess safety, or provide evidence of exposure, including exposures to medical products | Serum creatinine Proteinuria Hematuria Immunosuppressive drug levelsBKV/PCR Signs of hemolysis |
There are currently no new monitoring biomarkers proposed in kidney transplantation |
| Pharmacodynamics/response biomarker | A biomarker used to show that a biologic response has occurred in an individual who has received an intervention or exposure | CD19/CD20 count with rituximab treatment DSA mean fluorescence index after AMMR treatment Post-treatment control biopsy histology |
There are currently no new pharmacodynamics/response biomarkers proposed in kidney transplantation |
Table 3.
Benefits and pitfalls of the use of dd-cfDNA.
| Potential Benefits | Pitfalls |
|---|---|
| Noninvasive blood biomarker | Fractional quantification affected by changes in rdcfDNA |
| Applicable to all solid organ transplantation | Does not exclude TCMR (if ddcfDNA normal) |
| Elevations may occur up to 30 days before histologic changes | Elevated in nonrejection pathologies associated with tissue injury (BKV, CVNI toxicity) |
| Absolute quantification of ddcfDNA not affected by changes in rdcfDNA | Not recommemded for use in early posttransplant period |
| Avoidance of protocol biopsy | No recommended flor use for 24 h post-biopsy |
| Avoidance of unnecessary biopsies | Confounded in pregnancy |
| Noninvasive diagnosis of AMR | Confounders in some repeat and multiorgan transplants |
| Assessment of response to rejection treatment | |
| Indicator for treatment of chronic active AMR |
Table 4.
dd_cfDNA and diagnosis of rejection.
| Acute rejection median | 2,32% |
| Non-acute rejection median | 0.47% |
| |
Table 5.
Patients with dd-cfDNA >0.5 were at increased risk of recurrent rejection, DSA detection, and eGFR decline over the following 3-6 months.
Table 5.
Patients with dd-cfDNA >0.5 were at increased risk of recurrent rejection, DSA detection, and eGFR decline over the following 3-6 months.
| Statistics | Low (dd-cfDNA <0.5% | Hgh (dd-cfDNA > 0.5% | p-value | |
|---|---|---|---|---|
| dd-cfDNA value (%) | Mean (SD) | 0.25 (0.087) | 1.76 (1.40) | - |
| Median | 0.21 (0.19, 0,29) | 1.40 (0.87, 2.02) | - | |
| Min, Max | 0.19, 0.49 | 0.52, 6.70 | - | |
|
% Change in eGFR |
Mean (SD) | -0.40 (18.149) | -8.64 (11.98) | 0.0040 |
| Median | 0.00 (-0.92, 4,76 | -7.50 (-16.22, -1.39) | ||
| Min, Max | -70.73, 33,.33 | -37-50, 32.65 | ||
| Presence of DSAs | 1/37 (2.7%) | 17/42 (40.5%) | <0.0001 | |
| Recurrent Rejection | 0/37 (0.0%) | 9/42 (21.4%) | 0.0028 |
Table 6.
Seventeen –gene set for 3-month ACR diagnosis.
| Symbol | RefSeq | Name | P-value |
|---|---|---|---|
| ZMAT1 | NM_001011657 | Zinc finger, matrin type 1 | 0.01 |
| ETAA1 | NM_019002 | Ewing tumor.associated antigen 1 | 0.04 |
| ZNF493 | NM_001076678 | Zinc finger protein 493 | 0.002 |
| CCDC82 | NM_024725 | Coiled-coil domain containing 82 | 0.02 |
| NFYB | NM_006166 | Nuclear transcription factor Y, β | 0.03 |
| SENP7 | NM_001077203 | SUMO1/sentrin specific peptidase 7 | <0.001 |
| CLK1 | NM_001162407 | CDC-like kinase 1 | 0.01 |
| SENP6 | NM_001100409 | SUMO1/sentrin specific peptidase 6 | 0.01 |
| C1GALT1C1 | NM_001011551 | C1GALT1-specific chaperone 1 | 0.01 |
| SPCS3 | NM_021928 | Signal peptidase complex subunit 3 homolog (S,. cerevisiae) | 0.03 |
| MAP1A | NM_002373 | Microtubule-associated protein 1A | 0.01 |
| EFTUD2 | NM_001142605 | Elongation factor Tu GTP binding domain containing 2 | 0.001 |
| AP1M1 | NM_001130524 | Adaptor-related protein complex 1, mu 1 subunit | <0001 |
| ANXA5 | NM_001154 | Annexin A5 | <0.001 |
| TSC22D1 | NM_001243797 | TSC22 domain family, member 1 | 0.01 |
| F13A1 | NM_000129 | Coagulation factor XIII, A1 polypeptide | 0.02 |
| TUBB1 | NM_030773 | Tubulin, β1 class VI | 0.03 |
Table 7.
Main challenges in finding new biomarkers.
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



