
Submitted:
16 April 2024
Posted:
17 April 2024
You are already at the latest version
Abstract
This is a single tertiary center in southwest Romania, population-based, study. We retrospectively compared data obtained in two periods: January 2008 - December 2013 and January 2018 - De-cember 2023, respectively. The global incidence of transposition of great arteries (TGA) - the ter-minated cases added to the ones resulting in live-born pregnancies, remained almost constant. The live-born incidence of TGA decreased (0.34% to 0.013%). The prenatal detection rate increased slightly (71.42% to 87.5%). The median gestational age at the diagnosis decreased, from 29.3 ges-tational weeks (mean 25.4) to 13.4 weeks (mean 17.2). The proportion of terminated pregnancies significantly increased (14.28% to 75%, p = 0.019).
Keywords:
transposition of great arteries
; ultrasound
; prenatal diagnosis
; termination of pregnancy
; live-birth incidence
; counseling
1. Introduction
The reported prevalence of major congenital heart disease (MCHDs) varies from 0.8% to 1.5% (close to 1%) [1,2]. Dextro-transposition of the great arteries (D-TGA) is the second-most common cyanotic congenital heart defect, accounting for 4-5% of all congenital heart defects [3,4], with an incidence of 0.02–0.05% of live births [3]. It was reported a 2:1 male predominance [4].
Although a major defect, D-TGA is seen as a surgically correctable disease. The most common surgical procedure used is Jatene arterial switch operation (ASO) [5], with a perioperative mortality about 2–4% [6,7,8,9], long-term benefits [7], and a high long-term survival rate [6,10] (10-year survival rate 88–97% [6], 20-year survival rate - nearly 90% [10]. However, neurodevelopmental dysfunctions are frequently reported (reduced performance in attention, visual-spatial skills, and executive functions, anxiety disorders) [6,11]. It was hypothesized that delayed brain development in utero heightens the postnatal susceptibility to acquired white matter injury [12,13]. These symptoms may be results of TGA per se or results of ASO complications. More studies are needed to confirm if the appropriate perinatal management is enough in isolated D-TGA to reach a good long-term prognosis.
Routine obstetric ultrasound (US) aims to identify suspected cases of CHD so these women can be referred for full fetal echocardiography. Currently, the question of whether the detection rate (DR) of MCHDs is acceptably high if screening in low-risk pregnancies or not, has remained unanswered. Previously published studies included populations and techniques that differed considerably. Thus, the reported DRs of MCHDs have huge variations.
TGA is the most representative CHD for the ductal-dependent group. According to some researchers, prenatal diagnosis (PND) is paramount in ductal-dependent CHDs because morbidity and mortality may be reduced [14,15,16]. Yet, the PND role in reducing mortality and long-term morbidity in TGA (doctors’ awareness, emergent neonatal management strategies, balloon atrial septostomy, short interval ASO) is still debated [8,10,14,17,18,19]. Thus, the benefits of routine screening are still to be proven, and even more so – those of the diagnosis of TGA in early pregnancy.
In TGA also, DRs range widely: 3% [20], 6.9% [21], 20% ”in many first world centers” [22], 54% [23] and very high – 72% [24]. Despite advances in fetal echocardiography and the technological impressive improvement, the PND of TGA is reported as low in general [25,26].
Different approaches to prenatal screening exist in Romania also, and access to routine scans varies within our country, due to geographical, social, and economic limitations. We hypothesize that PND rates for all CHD vary, thus it will induce various rates in TOPs. There are no nationwide population-based studies examining the incidence of CHDs or TOPs for CHD in Romania.
The fetal cardiac scan at the late first trimester (FT) anomaly scan (FTAS) at 11-13 GW was introduced progressively in the prenatal diagnosis unit (PDU) of Emergency University County Hospital (EUCH) of Craiova since 2010, and became mandatory at the end of 2013 [27,28]. The internal policy changed, and the simplified cardiac sweep [29,30,31] was attempted universally, in every case scanned. The standardized cardiac sweep was obtained afterward in more than 95% of women. The PDU team comprises 6 maternal-fetal specialists with experience in the field (more than 20 years) and we benefit from periodic multidisciplinary meetings including pediatric cardiologists.
We aimed to evaluate the incidence, DRs, gestational age at diagnosis and TOP of isolated D-TGA and assess their trends over time in our unit.
2. Materials and Methods
We conducted a retrospective study including all newborns with TGA in the EUCH, as well as fetuses diagnosed with TGA leading to TOP, in two different periods: 1st January 2008 - 31st December 2013, and 1st January 2018 - 31st December 2023. We aimed for the isolated (uncorrected, D-type) TGA cases. We considered ”isolated TGA” (iTGA) all cases without major cardiac and extracardiac defects, but we included cases with the common association of ventricular septal defect (VSD). TGA was considered ”complex” when associated with any other major cardiac/extracardiac malformations and these cases were excluded from the analysis.
Inclusion criteria for prenatally diagnosed cases were typical images of D-TGA [22,32,33,34] and absence of associated major cardiac anomalies (other than small trabecular below 3 mm VSDs). Although the complete diagnosis was considered accessible in the prenatal life only in fetuses scanned later than 22 gestational weeks (GW), we included all cases reaching the consensus from at least 3 consultants in maternal-fetal medicine (highly experienced specialists).
Inclusion criteria for the postnatally diagnosed cases were relevant clinical features and the description of the neonatal echocardiography, as noted in the file by the pediatric cardiologist, in cases managed peripartum in the EUCH. Pulse oximetry screening was initiated before 2008 and has been fully operational in the second period of the study. In the EUCH neonatal surgery is not available; all cases were treated with prostaglandins and air transportation was arranged to the Pediatric Intensive Care Unit, Emergency Institute for Cardiovascular Diseases and Transplantation, Targu Mures, Romania (EICVDT). The treatment target saturation before referral was >80% (measured from the right upper arm).
At the first search, nineteen cases met the inclusion criteria and were investigated for entering the study. Four patients were excluded: one had a major associated cardiac anomaly (pulmonary stenosis), one was subsequently diagnosed with double outlet right ventricle (DORV); one patient was excluded because the delivery took place in a private foreign institution, and the peripartum data were not accessible; in one case we found the US data not suitable for the enrollment.
We included 15 cases: 7 in the historical cohort, and 8 in the recent one. Data were extracted from the patients’ hard-copy and electronic files, the intranet network Hipocrate used by the EUCH of Craiova, the electronic registries Natalcare (Operational Program Human Capital—Complex Program—Information and Care for Mother and Child—Project Code 142081 (the European Social Fund) and Materna clinic. All these registries prospectively record the diagnoses made during outpatient visits and hospital admissions. In the Hipocrate database, the search was undertaken for diagnoses code Q24-26 and Q20-28 for newborns with TGA diagnosis in the study period. A separate list of cases was created from the database of patients suspected of TGA in prenatal life. Medical and US files were then reviewed, and relevant data was extracted. This comprised clinical information only, to ensure anonymity and to comply with information governance; no patient identifiers were recorded. All US files of cases resulting in TOPs were reviewed by 3 maternal-fetal specialists. Photographic files of cases with autopsy performed were reviewed. The postoperative outcome was obtained in cases referred for neonatal surgery.
The minimum and maximum follow-up periods for the 8 children with ASO were 2 days and 12 years respectively. The median follow-up was 45 months (IQR 92).
2.1. Study Size
As a local population-based study, it was limited by the number of fetuses scanned and registered by the institutions involved and by the number of cases of TGA born within the two periods of data collection. If data items were missing from the notes or the US file, cases were excluded from the specific outcome analysis between cohorts.
2.2. Approval
The study was conducted according to the guidelines of the Declaration of Helsinki. This is an observational and retrospective study, implying almost exclusively registries research. No patients’ details are included in the manuscript and all patients were undergoing scans and medical care as part of routine clinical practice and not for research. Therefore, this study did not require registration, approval from the research ethics committee, or informed consent.
2.3. Screening Ultrasound (US) Protocol
Ultrasound examinations were performed using Voluson E8 and E10 (GE Medical Systems) ultrasound machines, equipped with a 4 – 8 MHz curvilinear transducer and a 5-9 MHz transvaginal probe.
The nuchal translucency (NT) scan at 11-13 WG was introduced in our unit since 2008. We used a US scan at this gestational to establish the risk of aneuploidy using the combined test [35,36,37].
The standard prenatal care included back then a second trimester (ST) anomaly scan, between 18-23 WG. Views of the left and right ventricular outflow tracts (LVOT and RVOT) were attempted as an integral part of the fetal cardiac screening examination in the ST, in both periods of the study [38,39,40].
Between 2008 and 2013, prenatal screening for CHDs was not offered routinely at the end of the FT. Since 2013, in line with the general shift to the late FTAS [28,41,42,43,44], the aim of the ”nuchal scan” widened, and we targeted all major structural abnormalities. As a major advantage, FTAS was seen as an excellent tool for early reassurance, very important in selected cases (advanced maternal age, positive history for major structural/chromosomal anomalies, pregnancies after assisted reproductive techniques and others). Subsequently, the FT fetal cardiac scan became routine. The simplified cardiac sweep [30,31,45,46] was attempted universally, in every case scanned at 11-13 WG in our unit (Figure 1). We commonly use the duplex (2D-2D Doppler color). At the FTAS, all ST features recommended for the TGA diagnosis were searched. [28,47,48]. When using color Doppler/power Doppler, the mechanical and thermal indices were kept as low as possible (ALARA principle) [49] and current guidelines were followed [50].
The cardiac sweep at the FTAS contains two planes considered mandatory in the PDU (a and b). The second (the 3VT view plane) is severely distorted in all malposed aorta cases, and is typical (not pathognomonic) in TGA.
- normal 4-chamber view, normal equal ventricular inflows, in a normal case
- b. confluence of the arches on the left (”the V-sign” in the 3VT view) in a normal case
- c. the ”reverse boomerang sign” - the reverse curvature of right ventricle outflow tract (RVOT) at level of the 3VT view in a TGA case
Since 2013, all pregnant women cared for in the PDU of EUCH were offered at least two anomaly scans: the FTAS (at 11-13 WG) and the STAS (at 18-23 weeks) (Figure 2). The third trimester (TT) scan remained optional, at the attending physician’s convenience. Yet, the TT scan was commonly recommended in our unit during both periods assessed.
We included all cases with suspected or confirmed TGA diagnosis in which a complete consensus about the diagnosis was reached. These cases were included regardless of the gestational age and regardless of the outcome: resulting in live birth or TOPs, TOP followed by an informative/documented autopsy or not.
The population scanned in the PDU is generally low-risk and unselected. Yet approximately 20-22% of cases are referred, due to the tertiary status of the unit. Usually, if any CHD is suspected at US eexamination in counties surrounding ours, the patient is referred to a specialist in fetal medicine for fetal echocardiography in our unit.
All couples with suspicion of TGA were offered genetic counseling and testing: quantitative fluorescence-polymerase chain reaction (QF-PCR), conventional karyotyping, and array-CGH.
If the PDU team anticipates the necessity of surgical or complex multidisciplinary treatment shortly after birth, the delivery is set to take place in another tertiary center. Our cases were referred (both prenatally and postnatally) to the most representative public tertiary center for the surgical treatment of CHD in Romania, the EICVDT, Targu Mures.
2.4. Live Births
In the Hipocrat Network, patients who at any time had been given a Q24-26 and Q20-28 code (corresponding to congenital malformations of cardiac chambers, great vessels, cardiac valves, septae and venous system) were searched. CHDs were identified. Extracted data included identification number, neonate sex, weight, Apgar score, and all procedural codes given.
We identified patients with TGA based on the Q25 code. In EUCH neonatal surgery being unavailable, we followed the cases after referral at the EICVDT. Patients’ postnatal US records were examined, and cases with an outcome available for verification postnatally were included. In TGA cases, routine management is continuous pulse oximetry and daily US exam to document the ductus arteriosus diameter, and continuous infusion of prostaglandin E1 (PGE1) to maintain its patency, when needed. After excluding patients with incomplete medical records, we included 8 pregnancies ending at term, among them 3 cases being diagnosed postnatally. We referred all cases (5 were transported in utero, 3 after birth).
One newborn died before the emergency intervention was possible, and one newborn was lost immediately after the Raskind procedure. All 6 remaining babies were subjected to ASO, at intervals between 2 days and 8 days. Among these, 2 were genetically tested, and the molecular karyotype showed no significant changes. They all evolved uneventfully after surgery, but 3 of them have suboptimal long-term neurodevelopment. No differences in long-term outcomes were identified between the children diagnosed prenatally and the ones diagnosed postnatally.
2.5. Termination of Pregnancy
We searched for O04.0 - O04.5 and O35.8 - O35.9 codes related to TOP for congenital abnormalities. We searched for all iatrogenic TOPs after 12 weeks of gestation and selected for inclusion the ones diagnosed with TGA. We included the woman’s identification number, place, gestational age, and date of the TOP. We reviewed the records and the autopsy files following TOPs. TOPs not followed by autopsy or followed by non-informative autopsy were not excluded from the study.
2.6. Analyses
Rates were calculated as follows:
- incidence of TGA as the number of TGA (live-born and terminated) divided by the total number of fetuses scanned.
- live-birth incidence of TGA as the number of TGA in live-born children divided by the total number of live births.
DRs for TGA were calculated as the number of prenatally diagnosed TGA divided by the total number of fetuses (live-born and terminated) with TGA. The TOP rates were calculated as the number of terminated fetuses with TGA divided by the total number of fetuses with TGA (live-born and terminated).
Categorical data are presented as frequencies and percentages along with their respective 95% confidence intervals. Differences in proportions were evaluated using z-tests, and logistic regression was employed to investigate the influence of factors such as BMI on PND of TGA. The analyses were performed using Python, which facilitated data manipulation and calculation of confidence intervals and p-values, and IBM SPSS Statistics, version 26, for logistic regression modeling. All hypothesis testing was two-sided, and a P value of less or equal to 0.05 was considered indicative of statistical significance.
3. Results
A flow chart is shown in Figure 3.
In total, we had 32320 births in our institution during the two intervals selected for the study. 5 fetuses were referred to be born in EICVDT, and 3 neonates were referred postnatally.
13 fetuses with TGA were identified in prenatal life and we had 7 terminated pregnancies after 12 weeks of gestation. 6 of them belong to the recent cohort.
3.1. Incidence
During the first period of the study, 17522 children were born, resulting in a live-birth incidence of TGA of 0.034% (95% CI, 0.00685% - 0.06164%). During the second period of the study, 14798 children were born, resulting in a live-birth incidence of TGA of 0.013% (95% CI, 0.000% - 0.03225%).
This doesn’t represent a significant change comparing the two periods throughout the study (p = 0.238).
The live-birth incidence of TGA decreased from 0.034% to 0.013% (OR = 0.395, 95% CI, 0.080 – 1.1955; P = 0.238)
The influence of general prenatal screening was not confirmed (OR=2.8, 95% CI 0.196 – 40.059, P = 0.438)
In our case series, TGA was not significantly more common in males than in females (OR = 1.5, 95% CI 0.353 – 0.812, P = 0.273)
When including TOPs, the incidence of TGA in all fetuses was 0.062% (95% CI, 0.0104% - 0.0695%) during the first period and 0.060% (95% CI, 0.0166% - 0.0915%), with no significant changes over time.
3.2. Detection Rates
The individual gestational age at the diagnosis of TGA is shown in Figure 4.
During the two study periods, 12/15 (80%) fetuses with TGA (95% CI, 0.53 – 0.94) were diagnosed prenatally, without sex-specific differences. The overall increase in DRs was not statistically significant if comparing the two periods (71.42% vs 87.5%) (p = 0.438).
The increase was statistically significant in the FT (p = 0.05) and didn’t reach statistical significance in the ST (OR = 1.5; 95% CI, 0.071-31.575; P = 0.793).
In the historical cohort, one case only was diagnosed in the FT, whereas in the third trimester (TT) 42.85% cases were detected.
In the second period of the study, there was a significant difference in detection rates between the first and second trimesters (71.43% vs 14.29%; p = 0.031).
In the prenatally diagnosed group (PND+ group) of 12 patients, TGA was diagnosed at a median gestational age of 29.3 gestational weeks (mean 25.4) in the historical cohort, and at a median of 13.4 weeks (mean 17.2) in the recent one.
In the global population studied, TGA was diagnosed prenatally at an average of 20.65 weeks GA, with 50 % diagnosed during the FT, 17% in the ST, and 33% in the TT.
There was no significant difference in DRs considering the type of practice, whether public or private (p = 0.736).
The body mass index (BMI) did not influence the PND of TGA. The BMI coefficient is negative (B = -0.489), but its p-value is 0.068, which is above the conventional threshold for significance (0.05). Thus, higher BMI is associated with a lower likelihood of PND+, but this result is not statistically significant. There was a suggestive but not statistically significant increased risk of missed PND for overweight and obese patients (BMI >25 kg/m2).
3.3. Characteristics of TGA Liveborn in EUCH

Table 1.
Characteristics of TGA liveborn in EUCH.
| Prenatal vs Postnatal Diagnosis, No./Total No. (%) | P Value | ||
|---|---|---|---|
| 2008 – 2013 (No universal FT Screening) |
2018 – 2023 (universal FT Screening) |
||
| TGA FT | 1/7 (14.28%) | 5/8 (62.5%) | 0.34 |
| TGA ST | 1/7 (14.28%) | 1/8 (12.5%) | 1.0 |
| TGA TT | 3/7 (42.85%) | 1/8 (12.5%) | 0.58 |
| Prenatal Dx TGA overall | 4/7 (57.14%) | 7/8 (87.5%) | 0.7 |
| Postnatal Dx TGA | 2/7 (28.57%) | 1/8 (12.5%) | 1.0 |
3.4. Termination of Pregnancy
During the study periods, 7/15 (46.66%) (CI 95% = 0.73% - 55.42%) of all pregnancies with TGA were iatrogenic terminated, on parental request. In other words, 7 cases ended in TOPs among the 12 cases diagnosed prenatally (58.33%). In the two cohorts presented, all TOPs were medically performed, we had no surgically terminated cases.
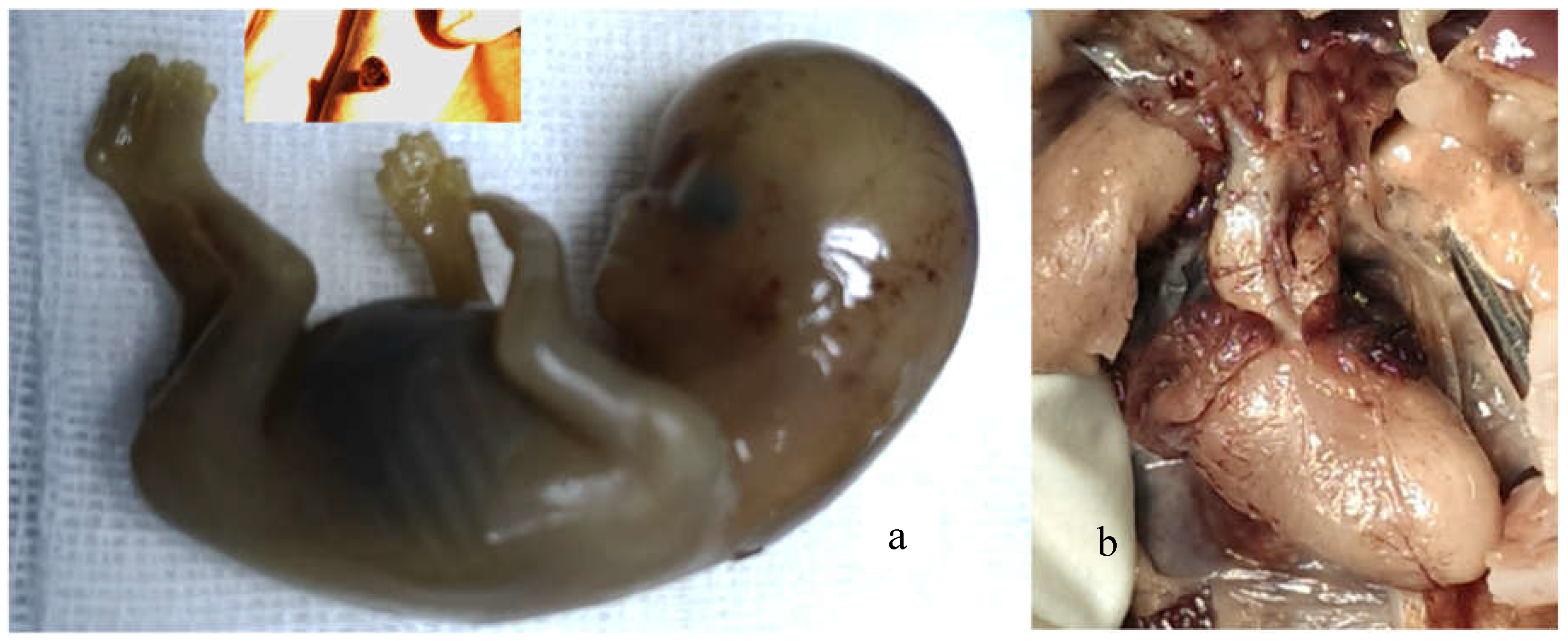
Autopsy was performed in both fetuses terminated in the ST. The autopsies files were found relevant. Although intact specimens were obtained in 4 out of 5 fetuses terminated after the FT diagnosis, informative images from the fetal conventional autopsy were lacking (Figure 5), and we had one case confirmed postmortem using a non-conventional method.
For pregnancies with prenatally diagnosed TGA, the proportion of TOPs changed over time.
TOPs increased from 1 case/7 - 14.29% in the historical cohort to 6/8 - 75% (CI 95% = 36.46% - 95.36%) in the recent cohort (p = 0.0187)
4. Discussion
This is the first study to describe the time trends in the incidence, detection rates, and TOP rates for iGAT in a tertiary center in Romania. Two periods separated by a 10-year interval are presented.
The overall incidence was 0.79% for all CHD and 0.04% for TGA. The figures are in line with most estimates [1,51,52,53,54]. There are controversies about time trends of the incidence of CHD [55,56]. We did not find significant changes over time in the overall incidence of MCHD or TGA.
We chose iTGA for investigation due to cases homogeneity, and due to the reported excellent postsurgical prognosis among ductal-dependent CHDs. Moreover, this critical CHD have a notorious negative correlation with chromosomal abnormalities [57], thus we considered most worthwhile searching.
The main findings are that while the general incidence of TGA was stationary, the live-birth incidence decreased significantly – by 66.66%. Furthermore, comparing the two periods, we found a 5-fold increase in TOP rates. Similar results, showing that the decrease in live-birth incidence of MCHD follows increased TOP rate, were previously reported for univentricular heart [58].
Generalizing the cardiac sweep is both ethical and rational, as it is known that most CHD occurs in pregnancies with no risk factors [59] and all parents that choose to be tested by US scan have the right to find out as early as possible about suspected structural abnormalities [60,61].
It was previously found that TOP rates for structural abnormalities are higher in fetuses diagnosed in the FT compared with those diagnosed in the ST [62]. In our study also, increased TOP rate is associated with higher DRs of TGA prenatally, especially in early pregnancy. In the second period of the study, DRs were higher in both the FT and the ST. Our DRs are consistent with recent conducted studies [63,64].
This may be explained by the increase in doctors’ skills and awareness and may be partially attributed to the development in obstetric US equipment. Also, the change in internal policy, with introducing the routine cardiac sweep (implementation of the 3-vessel and trachea view) at the FTAS and the sustained effort to implement published guidelines may be considered. Additionally, the number of malformation scans performed at the end of FT in the PDU was much higher in the recent cohort: on average – 6 FTAS/day (compared with an average of 2 FTAS/day in the historical cohort). The phenomenon was previously reported [65], and our results confirm it.
Most probably, it is not feasible to reach a 100% detection rate of TGA. Yet, in our recent cohort, all fetuses presented in the unit for FTAS and for STAS were detected, but one (7/8). Characteristic US features were present in all fetuses. The missed case was related to a relevant scan, and iTGA should have been readily detected. Unfortunately, the images were misinterpreted by a less experienced operator. Our findings, as well of those of others [2] confirm that clinical experience of the sonographer influences prenatal detection.
We found no significant difference in terms of type of medical practice - public versus private [66]. Unlike other reports [66],we found no higher risk for missing the PND of TGA in overweight and obese patients (BMI >25 kg/m2).
In our case series, all 3 cases diagnosed postnatally have had US examinations during pregnancy, in low range hospitals. Our unit had the highest DR in first-time scanned fetuses than all referral hospitals. It is desirable to ensure training and adequate examinations across hospitals. The complete implementation of 3-VTv and outflow tracts views enhances the detectability of iGAT, but further centralization of malformation scans may improve DRs.
The prenatal diagnosis of any major CHD always raises the question to terminate or to continue the pregnancy, and this decision will depend on a variety of factors [24,61,67,68].
Currently, TOP is performed in 50-60% of all fetuses with MCHD diagnosed prenatally [65]. TOP for TGA also vary largely from roughly 12 [52] to 21%[65] and to 72% [69]. In certain countries, a decrease in TOPs of TGA is registered [65].
The ethics of TOPs in TGA is beyond the aim of this manuscript. But it’s worthwhile mentioning that in Romania, the on-parents-request TOP is regulated until 14 weeks GA [70]. If major or suboptimal repair congenital abnormalities are detected later, it is customary that an ethics board is gathered, to adjudge the opportunity to continue the pregnancy. Medically indicated terminations are permitted until 24 weeks GA.
We must highlight that TGA (as tetralogy of Fallot, pulmonary atresia, interrupted aortic arch, coarctation of aorta, and anomalous pulmonary venous return) can be repaired in a biventricle manner. The improvements in management, the BAS [71] and the ASO procedures have altered dramatically outcomes for TGA neonates. Currently, the 25-year postoperative survival rate after arterial switch surpasses 96% [72]. Yet, the reported 1-year mortality after ASO less than 5% [73] has at times a huge emotional impact on parents.
In our experience, the optimism in counselling is often futile and rarely influence the parents’ decision to terminate a perceived as severely affected fetus. The limited access to high-quality neonatal surgery, difficulties faced by the parents engaged in long-term care of a child born with TGA may be considered also.
On longer term, maintained increased TOP rates will lead to decreased live-birth incidence of TGA, and subsequently - to lower patient flow in tertiary centers with neonatal surgery availability. This underlines again the importance of PND and raises the discussion of centralization (even for more than one country) for the surgical treatment. Eventually, we may face the balance between the high procedural experience, crucial for the invasive treatment of TGA, and longer distances needed for in utero/ neonatal transportation.
In our view, the current performance in FT prenatal screening still implies two important disadvantages: uncertain results in estimating the actual postnatal severity and the risk of on-parental-request TOP. In the latter group, the accurate follow-up diagnostic is absent due to fetal size restriction [74], not widely accepted or difficult to perform [75,76,77]. Conversely, the ST scan is more accurate and safer, having though the disadvantage of inflict the time interval of waiting.
The counseling after US screening scan should remain evidence-based and non-directive. Yet, parents should be advised in a respectful, considerate, and empathic manner, to postpone the TGA suspected fetuses’ termination, at least util the US technology is able to provide a complete prenatal diagnosis. Couples should be offered follow-up US scans without the fear of losing a narrow window of opportunity due to law issues.
Similar shift in trend is to be expected in other congenital pathologies: the DRs will increase, due to both - technological improvement and the current guidelines [50]. For example, in open spina bifida, the highly suspicion may already be achieved extremely early in pregnancy [78], yet the accurate localization/height, the dimensions and the structure of the spinal defect remains fully unknown at the FTAS. Thus, the counseling will be incomplete or incorrect at the end of the FT. In other -highly evolving- fetal systems, the counselling following the FTAS will remain suboptimal also [45,79].
In all early diagnosed cases, the parents will face difficult dilemmas. Moreover, the professionals’ tasks will be increasingly difficult also because they will struggle to weigh different ethical principles: the autonomy of the parents on one hand, and the principles of beneficence, nonmaleficence, and justice – on the other. An impaired neonate leads to moral distress and posttraumatic stress reactions in parents. Thus, at times, physicians are tempted to exercise defensive medicine and allow easier incompletely justified medical TOPs.
In the ECUH neonatal cardiac surgery being not available, we present a rather homogenous cohort, identifying cases from a geographically defined population, opposite to a population of fetuses/neonates referred to a single tertiary center committed to treat and operate the TGA cases. To some extent, the results of the study are descriptive for both the advances in the PND and for the limits of surgical correction in our country.
This study has several important limitations.
The paramount ones are related to the active management following the FT scan information, ending in TOPs. This limited both US and pathological investigation. All predictors for urgent BAS and long-term outcome are still controversial [8,80,81,82] and the most important ones for the neonatal outcome are reachable later in pregnancy: the VSD presence and dimensions, the physiological shunts, like foramen ovale (FO) anatomy and diameters [83,84,85], ductus arteriosus. [85,86], findings of increased pulmonary venous blood flow, association of aortic coarctation/obstruction of right ventricular outflow tract, volume of intracranial structures [87], US features of cavum septi pellucidi [88] - all cannot be assessed in early pregnancy. Although the favorable counseling at the diagnosis remains appropriate, cautious must be exercised by counselors. All cardiac parameters (physiological shunts) may change late in pregnancy. In some cases, neonatal death occurs, despite adequate management and appropriate resuscitation measures [85].
Also, the coronary anatomy [89,90] a key determinant of both short- and long-term outcomes following ASO was not investigated in our study. Coronary arterial abnormalities are related to the spatial relationships of arterial trunks [91,92]. Thus, efforts have been made to define them using 4DUS with color Doppler, to predict the likelihood of abnormal coronary arterial distribution [93].
Additionally, we may hypothesize that some of the FT diagnosed cases had either an incomplete, or a wrong diagnosis [66,94,95]. Still, we involved all specialists in maternal-fetal medicine in difficult to interpret cases, and included only cases that reached a definitive consensus.
In a recent systematic review and metanalysis [96], associations were found between high DR and structured anatomical assessment, the latter improving sensitivity. According to this research, the FT scan yield similar figures in DRs with the ST scan (over half of fetuses affected by major cardiac pathology). Recently, the most important professional society in prenatal US published GLs supporting this vision [50]. We previously published [27,30,97] our standardized technique to assess the FT heart, by adding the visualization of the outflow tracts and color-flow Doppler imaging to the 4CV assessment.
In this study, not all fetuses were genetically tested, although chromosomal microarray analysis (arrayCGH) is seen as a valuable tool to detect chromosomal copy number variation in TGA and may improve prenatal counseling [3,98,99]. In our case series, all parents with the suspicion/diagnosis of TGA at the end of the FT declined the invasive procedure after counseling. We tested two fetuses by amniocentesis and conventional karyotype and two neonates were tested by means of arrayCGH. As expected, no significant changes were found.
Miscarriages were not included in this study. Therefore, we may have missed some fetuses with iGAT.
Surgical and follow-up data could not be obtained for one neonate operated elsewhere than EICVDT, which could limit the interpretation of the long-term outcomes.
The relatively small number of patients included hampered any demonstration of the effect on long term outcome. According to published literature, rates of adverse neurodevelopmental outcome in children TGA disease remain relatively high. Further investigation is needed to understand whether the antenatal diagnosis has the potential to improve longer term outcome [100].
5. Conclusions
This study, based on a geographically defined population, showed that incidences of fetuses with TGA have not changed significantly from 2008-2013 to 2018-2023. Prenatal detection of TGA has increased, currently approximating 80% in our unit. The gestational age at the diagnosis significantly decreased. Therefore, terminations of pregnancy in TGA reached 85.7% of all fetuses diagnosed prenatally in our case series. TOP rates increased from 14.28 % to 75 % (p = 0.019 < 0.05) and we registered a subsequent 0.327% decrease in the live-birth incidence of TGA. Most probably, this population-based study results are related to the introduction of routine FT fetal heart scan in the prenatal screening in our unit, in 2013.
Centralization of anomaly scans, training, and technological advances, added to the relatively easy early diagnosis, will most probably further improve prenatal detection rates in TGA and other major structural abnormalities. Multicentric studies are needed to prevent early and/or unnecessary terminations in cases with a favorable prognosis.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Video S1: FT_TGA, Video S2: ST_TGA.
Author Contributions
Conceptualization, S.C.A.F. and S.T.; methodology, A.C.V.; software, M.R.R.; validation, M.D.; S.O.C., R.C.P. and F.T.; formal analysis, F.G.D.; investigation, S.C.A.F.; M.A.P; R.G.C.; M.G.; writing—original draft preparation, S.C.A.F.; writing—review and editing, S.T.; visualization, F.T.; supervision, M.D.; A.C.V.; project administration, R.G.C.; funding acquisition, S.C.A.F. All authors have read and agreed to the published version of the manuscript.
Funding
The Article Processing Charges were funded by the Doctoral School of the University of Medicine and Pharmacy of Craiova, Romania.
Institutional Review Board and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki. This is an observational and retrospective study, implying almost exclusively registries research. No patients’ details are included in the manuscript and all patients were undergoing scans and medical care as part of routine clinical practice and not for research. Therefore, this study did not require registration, approval from the research ethics committee, or informed consent.
Data Availability Statement
All ultrasound files, neonates’ files and autopsy files are available and will be provided upon reasonable request.
Acknowledgments
This work benefited from administrative and technical support through the Operational Program Human Capital (POCU) NATALCARE—Complex Program—Information and Care for Mother and Child—Project Code 142081 (the European Social Fund).
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Sainz, J.A.; Zurita, M.J.; Guillen, I.; Borrero, C.; Garcia-Mejido, J.; Almeida, C.; Turmo, E.; Garrido, R. [Prenatal screening of congenital heart defects in population at low risk of congenital defects. A reality today]. An Pediatr (Barc) 2015, 82, 27–34. [Google Scholar] [CrossRef]
- Tegnander, E.; Williams, W.; Johansen, O.J.; Blaas, H.G.; Eik-Nes, S.H. Prenatal detection of heart defects in a non-selected population of 30,149 fetuses--detection rates and outcome. Ultrasound Obstet Gynecol 2006, 27, 252–265. [Google Scholar] [CrossRef]
- Hu, Q.; Deng, C.; Zhu, Q.; Yang, X.; Liu, H.; Liao, H.; Wang, X.; Yu, H. Dextro-transposition of the great arteries in one twin: Case reports and literature review. Transl Pediatr 2022, 11, 601–609. [Google Scholar] [CrossRef]
- Baumgartner, H.; Bonhoeffer, P.; De Groot, N.M.; de Haan, F.; Deanfield, J.E.; Galie, N.; Gatzoulis, M.A.; Gohlke-Baerwolf, C.; Kaemmerer, H.; Kilner, P.; et al. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010). Eur Heart J 2010, 31, 2915–2957. [Google Scholar] [CrossRef] [PubMed]
- Jatene, A.D.; Fontes, V.F.; Paulista, P.P.; Souza, L.C.; Neger, F.; Galantier, M.; Sousa, J.E. Anatomic correction of transposition of the great vessels. J Thorac Cardiovasc Surg 1976, 72, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Moe, T.G.; Bardo, D.M. E. Long-term Outcomes of the Arterial Switch Operation for d-Transposition of the Great Arteries. Prog Cardiovasc Dis 2018, 61, 360–364. [Google Scholar] [CrossRef]
- Devlin, P.J.; Jegatheeswaran, A.; Williams, W.G.; Blackstone, E.H.; DeCampli, W.M.; Lambert, L.M.; Mussatto, K.A.; Prospero, C.J.; Bondarenko, I.; McCrindle, B.W. Late Survival and Patient-Perceived Health Status of the Congenital Heart Surgeons' Society dextro-Transposition of the Great Arteries Cohort. Ann Thorac Surg 2019, 108, 1447–1455. [Google Scholar] [CrossRef]
- Zhang, X.; Haneishi, H.; Liu, H. Impact of ductus arteriosus constriction and restrictive foramen ovale on global hemodynamics for term fetuses with d-TGA. Int J Numer Method Biomed Eng 2021, 37, e3231. [Google Scholar] [CrossRef]
- Soongswang, J.; Adatia, I.; Newman, C.; Smallhorn, J.F.; Williams, W.G.; Freedom, R.M. Mortality in potential arterial switch candidates with transposition of the great arteries. J Am Coll Cardiol 1998, 32, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Villafane, J.; Lantin-Hermoso, M.R.; Bhatt, A.B.; Tweddell, J.S.; Geva, T.; Nathan, M.; Elliott, M.J.; Vetter, V.L.; Paridon, S.M.; Kochilas, L.; et al. D-transposition of the great arteries: The current era of the arterial switch operation. J Am Coll Cardiol 2014, 64, 498–511. [Google Scholar] [CrossRef]
- Paladini, D.; Alfirevic, Z.; Carvalho, J.S.; Khalil, A.; Malinger, G.; Martinez, J.M.; Rychik, J.; Ville, Y.; Gardiner, H.; Committee, I.C. S. ISUOG consensus statement on current understanding of the association of neurodevelopmental delay and congenital heart disease: Impact on prenatal counseling. Ultrasound Obstet Gynecol 2017, 49, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Peyvandi, S.; Lim, J.M.; Marini, D.; Xu, D.; Reddy, V.M.; Barkovich, A.J.; Miller, S.; McQuillen, P.; Seed, M. Fetal brain growth and risk of postnatal white matter injury in critical congenital heart disease. J Thorac Cardiovasc Surg 2021, 162, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Park, C.S.; Lee, J.R.; Lim, H.G.; Kim, W.H.; Kim, Y.J. The long-term result of total repair for tetralogy of Fallot. Eur J Cardiothorac Surg 2010, 38, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, D.; Coltri, A.; Butera, G.; Fermont, L.; Le Bidois, J.; Kachaner, J.; Sidi, D. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation 1999, 99, 916–918. [Google Scholar] [CrossRef] [PubMed]
- van Velzen, C.L.; Haak, M.C.; Reijnders, G.; Rijlaarsdam, M.E.; Bax, C.J.; Pajkrt, E.; Hruda, J.; Galindo-Garre, F.; Bilardo, C.M.; de Groot, C.J.; et al. Prenatal detection of transposition of the great arteries reduces mortality and morbidity. Ultrasound Obstet Gynecol 2015, 45, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Raboisson, M.J.; Samson, C.; Ducreux, C.; Rudigoz, R.C.; Gaucherand, P.; Bouvagnet, P.; Bozio, A. Impact of prenatal diagnosis of transposition of the great arteries on obstetric and early postnatal management. Eur J Obstet Gynecol Reprod Biol 2009, 142, 18–22. [Google Scholar] [CrossRef]
- Donofrio, M.T. Images in cardiovascular medicine. Premature closure of the foramen ovale and ductus arteriosus in a fetus with transposition of the great arteries. Circulation 2002, 105, e65–e66. [Google Scholar] [CrossRef] [PubMed]
- Lara, D.A.; Fixler, D.E.; Ethen, M.K.; Canfield, M.A.; Nembhard, W.N.; Morris, S.A. Prenatal diagnosis, hospital characteristics, and mortality in transposition of the great arteries. Birth Defects Res A Clin Mol Teratol 2016, 106, 739–748. [Google Scholar] [CrossRef]
- Slodki, M.; Respondek-Liberska, M.; Pruetz, J.D.; Donofrio, M.T. Fetal cardiology: Changing the definition of critical heart disease in the newborn. J Perinatol 2016, 36, 575–580. [Google Scholar] [CrossRef]
- Bull, C. Current and potential impact of fetal diagnosis on prevalence and spectrum of serious congenital heart disease at term in the UK. British Paediatric Cardiac Association. Lancet 1999, 354, 1242–1247. [Google Scholar] [CrossRef]
- Blyth, M.; Howe, D.; Gnanapragasam, J.; Wellesley, D. The hidden mortality of transposition of the great arteries and survival advantage provided by prenatal diagnosis. BJOG 2008, 115, 1096–1100. [Google Scholar] [CrossRef] [PubMed]
- Skinner, J.; Hornung, T.; Rumball, E. Transposition of the great arteries: From fetus to adult. Heart 2008, 94, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Landis, B.J.; Levey, A.; Levasseur, S.M.; Glickstein, J.S.; Kleinman, C.S.; Simpson, L.L.; Williams, I.A. Prenatal diagnosis of congenital heart disease and birth outcomes. Pediatr Cardiol 2013, 34, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Khoshnood, B.; De Vigan, C.; Vodovar, V.; Goujard, J.; Lhomme, A.; Bonnet, D.; Goffinet, F. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983-2000: A population-based evaluation. Pediatrics 2005, 115, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Escobar-Diaz, M.C.; Freud, L.R.; Bueno, A.; Brown, D.W.; Friedman, K.G.; Schidlow, D.; Emani, S.; Del Nido, P.J.; Tworetzky, W. Prenatal diagnosis of transposition of the great arteries over a 20-year period: Improved but imperfect. Ultrasound Obstet Gynecol 2015, 45, 678–682. [Google Scholar] [CrossRef] [PubMed]
- Slodki, M. Dextro-transposition of great vessels: Difficult to detect prenatally, one of the most dangerous and one of the best prognosed. Transl Pediatr 2022, 11, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Tudorache, S.; Cara, M.; Iliescu, D.G.; Novac, L.; Cernea, N. First trimester two- and four-dimensional cardiac scan: Intra- and interobserver agreement, comparison between methods and benefits of color Doppler technique. Ultrasound Obstet Gynecol 2013, 42, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, D.; Tudorache, S.; Comanescu, A.; Antsaklis, P.; Cotarcea, S.; Novac, L.; Cernea, N.; Antsaklis, A. Improved detection rate of structural abnormalities in the first trimester using an extended examination protocol. Ultrasound Obstet Gynecol 2013, 42, 300–309. [Google Scholar] [CrossRef]
- Ştefania Tudorache, A.U. , Roxana Cristina Drăguşin, Florea Maria Şorop, Monica Laura Cara, D.G. Iliescu. FIRST TRIMESTER DIAGNOSTIC ACCURACY OF A TWO- DIMENSIONAL SIMPLIFIED ULTRASOUND TECHNIQUE IN CONGENITAL HEART DISEASES AND GREAT ARTERIES ANOMALIES. Obstetrica & Ginecologia, 2016; LXIV, 165–176. [Google Scholar]
- Tudorache, S.; Florea, M.; Dragusin, R.; Patru, C.; Zorila, L.; Iliescu, D.G. OP15.03: First trimester fetal heart assessment learning curve. Ultrasound in Obstetrics & Gynecology 2016, 48, 97. [Google Scholar]
- Tudorache, S.; M, F.; R, D.; Zorila, L.; Cl, P.; Alexandru, D.; Cara, M.; Iliescu, D. Learning Curve for Ultrasound Assessment of the Fetal Heart at Nuchal Scan. JBR Journal of Clinical Diagnosis and Research 2017, 05. [Google Scholar] [CrossRef]
- Vinals, F.; Medina, L.; Guerra, F.A.; Naveas, R.; Giuliano, A. OC134: Accuracy of prenatal diagnosis of congenital heart defects evaluating the STIC sweep of the acquisition plane. Ultrasound in Obstetrics & Gynecology 2006, 28, 398. [Google Scholar]
- Bravo-Valenzuela, N.J.; Peixoto, A.B.; Araujo Junior, E. Prenatal diagnosis of congenital heart disease: A review of current knowledge. Indian Heart J 2018, 70, 150–164. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Valenzuela, N.J.; Peixoto, A.B.; Araujo Junior, E. Prenatal diagnosis of transposition of the great arteries: An updated review. Ultrasonography 2020, 39, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Bindra, R.; Heath, V.; Liao, A.; Spencer, K.; Nicolaides, K.H. One-stop clinic for assessment of risk for trisomy 21 at 11-14 weeks: A prospective study of 15 030 pregnancies. Ultrasound Obstet Gynecol 2002, 20, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, K.H. Screening for fetal aneuploidies at 11 to 13 weeks. Prenat Diagn 2011, 31, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Cicero, S.; Bindra, R.; Rembouskos, G.; Spencer, K.; Nicolaides, K.H. Integrated ultrasound and biochemical screening for trisomy 21 using fetal nuchal translucency, absent fetal nasal bone, free beta-hCG and PAPP-A at 11 to 14 weeks. Prenat Diagn 2003, 23, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.S.; Mavrides, E.; Shinebourne, E.A.; Campbell, S.; Thilaganathan, B. Improving the effectiveness of routine prenatal screening for major congenital heart defects. Heart 2002, 88, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Chaoui, R.; McEwing, R. Three cross-sectional planes for fetal color Doppler echocardiography. Ultrasound Obstet Gynecol 2003, 21, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Cardiac screening examination of the fetus: Guidelines for performing the 'basic' and 'extended basic' cardiac scan. Ultrasound Obstet Gynecol 2006, 27, 107–113. [CrossRef]
- Salomon, L.J.; Alfirevic, Z.; Bilardo, C.M.; Chalouhi, G.E.; Ghi, T.; Kagan, K.O.; Lau, T.K.; Papageorghiou, A.T.; Raine-Fenning, N.J.; Stirnemann, J.; et al. ISUOG practice guidelines: Performance of first-trimester fetal ultrasound scan. Ultrasound Obstet Gynecol 2013, 41, 102–113. [Google Scholar] [CrossRef]
- Syngelaki, A.; Chelemen, T.; Dagklis, T.; Allan, L.; Nicolaides, K.H. Challenges in the diagnosis of fetal non-chromosomal abnormalities at 11-13 weeks. Prenat Diagn 2011, 31, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Becker, R.; Wegner, R.D. Detailed screening for fetal anomalies and cardiac defects at the 11-13-week scan. Ultrasound Obstet Gynecol 2006, 27, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.M.; Bellotti, M.; Fesslova, V.; Cappellini, A. Fetal echocardiography at the time of the nuchal translucency scan. Ultrasound Obstet Gynecol 2007, 29, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Tudorache, S.; Cara, M.; Iliescu, D.G.; Stoica, A.; Simionescu, C.; Novac, L.V.; Cernea, D. Fetal Kidneys Ultrasound Appearance in the First Trimester - Clinical Significance and Limits of Counseling. Curr Health Sci J 2016, 42, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Quarello, E.; Lafouge, A.; Fries, N.; Salomon, L.J.; Cfef. Basic heart examination: Feasibility study of first-trimester systematic simplified fetal echocardiography. Ultrasound Obstet Gynecol 2017, 49, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Vayna, A.M.; Veduta, A.; Duta, S.; Panaitescu, A.M.; Stoica, S.; Buinoiu, N.; Nedelea, F.; Peltecu, G. Diagnosis of Fetal Structural Anomalies at 11 to 14 Weeks. J Ultrasound Med 2018, 37, 2063–2073. [Google Scholar] [CrossRef] [PubMed]
- Menahem, S.; Rotstein, A.; Meagher, S. Rightward convexity of the great vessel arising from the anterior ventricle: A novel fetal marker for transposition of the great arteries. Ultrasound Obstet Gynecol 2013, 41, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Salvesen, K.; Abramowicz, J.; Ter Haar, G.; Miloro, P.; Sinkovskaya, E.; Dall'Asta, A.; Marsal, K.; Lees, C.; Board of the International Society of Ultrasound in, O.; Gynecology. ISUOG statement on the safe use of Doppler for fetal ultrasound examination in the first 13 + 6 weeks of pregnancy (updated). Ultrasound Obstet Gynecol 2021, 57, 1020. [Google Scholar] [CrossRef]
- International Society of Ultrasound in, O.; Gynecology; Bilardo, C. M.; Chaoui, R.; Hyett, J.A.; Kagan, K.O.; Karim, J.N.; Papageorghiou, A.T.; Poon, L.C.; Salomon, L.J.; et al. ISUOG Practice Guidelines (updated): Performance of 11-14-week ultrasound scan. Ultrasound Obstet Gynecol 2023, 61, 127–143. [Google Scholar] [CrossRef] [PubMed]
- Oster, M.E.; Kim, C.H.; Kusano, A.S.; Cragan, J.D.; Dressler, P.; Hales, A.R.; Mahle, W.T.; Correa, A. A population-based study of the association of prenatal diagnosis with survival rate for infants with congenital heart defects. Am J Cardiol 2014, 113, 1036–1040. [Google Scholar] [CrossRef]
- Garne, E.; Stoll, C.; Clementi, M.; Euroscan, G. Evaluation of prenatal diagnosis of congenital heart diseases by ultrasound: Experience from 20 European registries. Ultrasound Obstet Gynecol 2001, 17, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.I.; Kaplan, S. The incidence of congenital heart disease. J Am Coll Cardiol 2002, 39, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, D.E.; Vejlstrup, N.; Jorgensen, C.; Maroun, L.L.; Steensberg, J.; Hessellund, A.; Jorgensen, F.S.; Larsen, T.; Shalmi, A.C.; Skibsted, L.; et al. Prenatal detection of congenital heart disease in a low risk population undergoing first and second trimester screening. Prenat Diagn 2015, 35, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Oyen, N.; Poulsen, G.; Boyd, H.A.; Wohlfahrt, J.; Jensen, P.K.; Melbye, M. National time trends in congenital heart defects, Denmark, 1977-2005. Am Heart J 2009, 157, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Egbe, A.; Uppu, S.; Lee, S.; Ho, D.; Srivastava, S. Changing prevalence of severe congenital heart disease: A population-based study. Pediatr Cardiol 2014, 35, 1232–1238. [Google Scholar] [CrossRef]
- Vedel, C.; Hjortshoj, T.D.; Jorgensen, D.S.; Tabor, A.; Rode, L.; Sundberg, K.; Ekelund, C.K.; Petersen, O.B. Prevalence of chromosomal disorders in cases with congenital heart defect: Registry-based study from Denmark between 2008 and 2018. Ultrasound Obstet Gynecol 2023, 61, 40–48. [Google Scholar] [CrossRef]
- Idorn, L.; Olsen, M.; Jensen, A.S.; Juul, K.; Reimers, J.I.; Sorensen, K.; Johnsen, S.P.; Sondergaard, L. Univentricular hearts in Denmark 1977 to 2009: Incidence and survival. Int J Cardiol 2013, 167, 1311–1316. [Google Scholar] [CrossRef]
- Stumpflen, I.; Stumpflen, A.; Wimmer, M.; Bernaschek, G. Effect of detailed fetal echocardiography as part of routine prenatal ultrasonographic screening on detection of congenital heart disease. Lancet 1996, 348, 854–857. [Google Scholar] [CrossRef]
- Becker, R.; Schmitz, L.; Kilavuz, S.; Stumm, M.; Wegner, R.D.; Bittner, U. 'Normal' nuchal translucency: A justification to refrain from detailed scan? Analysis of 6858 cases with special reference to ethical aspects. Prenat Diagn 2012, 32, 550–556. [Google Scholar] [CrossRef]
- Bonnet, D. Impacts of prenatal diagnosis of congenital heart diseases on outcomes. Transl Pediatr 2021, 10, 2241–2249. [Google Scholar] [CrossRef]
- Jicinska, H.; Vlasin, P.; Jicinsky, M.; Grochova, I.; Tomek, V.; Volaufova, J.; Skovranek, J.; Marek, J. Does First-Trimester Screening Modify the Natural History of Congenital Heart Disease? Analysis of Outcome of Regional Cardiac Screening at 2 Different Time Periods. Circulation 2017, 135, 1045–1055. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, H.M.; Kovacevic, A.; van der Heijden, L.B.; Pfeiffer, P.W.; Franklin, R.C.; Gibbs, J.L.; Averiss, I.E.; Larovere, J.M. Prenatal screening for major congenital heart disease: Assessing performance by combining national cardiac audit with maternity data. Heart 2014, 100, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Galindo, A.; Herraiz, I.; Escribano, D.; Lora, D.; Melchor, J.C.; de la Cruz, J. Prenatal detection of congenital heart defects: A survey on clinical practice in Spain. Fetal Diagn Ther 2011, 29, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Lytzen, R.; Vejlstrup, N.; Bjerre, J.; Petersen, O.B.; Leenskjold, S.; Dodd, J.K.; Jorgensen, F.S.; Sondergaard, L. Live-Born Major Congenital Heart Disease in Denmark: Incidence, Detection Rate, and Termination of Pregnancy Rate From 1996 to 2013. JAMA Cardiol 2018, 3, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Bertagna, F.; Rakza, T.; Vaksmann, G.; Ramdane-Sebbane, N.; Devisme, L.; Storme, L.; Francart, C.; Vaast, P.; Houfflin-Debarge, V. Transposition of the great arteries: Factors influencing prenatal diagnosis. Prenat Diagn 2014, 34, 534–537. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Li, Y.; Tang, Y.; Qu, X.; Wang, F.; Song, H.; Xu, Y. Clinical analysis of prenatal ultrasound diagnosis of fetal cardiovascular malformations in the first and second trimesters of pregnancy: A CARE-compliant article. Medicine (Baltimore) 2019, 98, e16822. [Google Scholar] [CrossRef] [PubMed]
- Dolk, H.; Loane, M.; Garne, E. ; European Surveillance of Congenital Anomalies Working, G. Congenital heart defects in Europe: Prevalence and perinatal mortality, 2000 to 2005. Circulation 2011, 123, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Wen, S.; Liu, X.; Pan, W.; Han, F.; Mai, J.; Ou, Y.; Nie, Z.; Gao, X.; Wu, Y.; et al. Perinatal and early postnatal outcomes for fetuses with prenatally diagnosed d-transposition of the great arteries: A prospective cohort study assessing the effect of standardised prenatal consultation. Cardiol Young 2018, 28, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Termination of pregnancy. Aggression towards the fetus New Penal Code, 2009.
- Thomas, C.; Yu, S.; Lowery, R.; Zampi, J.D. Timing of Balloon Atrial Septostomy in Patients with d-TGA and Association with Birth Location and Patient Outcomes. Pediatr Cardiol 2023, 44, 1333–1341. [Google Scholar] [CrossRef]
- Khairy, P.; Clair, M.; Fernandes, S.M.; Blume, E.D.; Powell, A.J.; Newburger, J.W.; Landzberg, M.J.; Mayer, J.E., Jr. Cardiovascular outcomes after the arterial switch operation for D-transposition of the great arteries. Circulation 2013, 127, 331–339. [Google Scholar] [CrossRef]
- Wernovsky, G.; Mayer, J.E., Jr.; Jonas, R.A.; Hanley, F.L.; Blackstone, E.H.; Kirklin, J.W.; Castaneda, A.R. Factors influencing early and late outcome of the arterial switch operation for transposition of the great arteries. J Thorac Cardiovasc Surg 1995, 109, 289-301; discussion 301-282. [Google Scholar] [CrossRef] [PubMed]
- Maria Sorop-Florea, R.N. C., Mihai Ioana, Alex Emilian Stepan, George Alin Stoica, Florentina Tanase, Maria Cristina Comanescu, Marius-Bogdan Novac, Ioana Dragan, Ciprian Laurentiu Patru, Roxana Cristina Dragusin, George Lucian Zorila, Ovidiu Marian Carbunaru, Nuti Daniela Oprescu, Iuliana Ceausu, Simona Vladareanu, Stefania Tudorache, Dominic Gabriel Iliescu. The importance of perinatal autopsy. Review of the literature and series of cases. Romanian Journal of Morphology and Embryology 2017, 58.
- Ruican, D.; Petrescu, A.M.; Istrate-Ofiteru, A.M.; Iliescu, D.G. Postmortem Evaluation of First Trimester Fetal Heart. Curr Health Sci J 2022, 48, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Staicu, A.; Albu, C.; Popa-Stanila, R.; Chiriac, L.; Boitor-Borza, D.; Bondor, C.; Kovacs, T.; Caracostea, G.; Rotar, I.C.; Turcu, R.V. F.; et al. Potential clinical benefits and limitations of fetal virtopsy using high-field MRI at 7 Tesla versus stereomicroscopic autopsy to assess first trimester fetuses. Prenat Diagn 2019, 39, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Zhang, Y.; Dai, C.; Ru, T.; Li, J.; Chen, J.; Zhang, B.; Zhou, K.; Lv, P.; Liu, R.; et al. Postmortem 9.4-T MRI for Fetuses With Congenital Heart Defects Diagnosed in the First Trimester. Front Cardiovasc Med 2021, 8, 764587. [Google Scholar] [CrossRef]
- Ushakov, F.; Sacco, A.; Andreeva, E.; Tudorache, S.; Everett, T.; David, A.L.; Pandya, P.P. Crash sign: New first-trimester sonographic marker of spina bifida. Ultrasound Obstet Gynecol 2019, 54, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Ungureanu, D.R.; Dragusin, R.C.; Capitanescu, R.G.; Zorila, L.; Ofiteru, A.M. I.; Marinas, C.; Patru, C.L.; Comanescu, A.C.; Comanescu, M.C.; Sirbu, O.C.; et al. First Trimester Ultrasound Detection of Fetal Central Nervous System Anomalies. Brain Sci 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Tuo, G.; Paladini, D.; Montobbio, G.; Volpe, P.; Cheli, M.; Calevo, M.G.; Marasini, M. Prenatal Echocardiographic Assessment of Foramen Ovale Appearance in Fetuses with D-Transposition of the Great Arteries and Impact on Neonatal Outcome. Fetal Diagn Ther 2017, 42, 48–56. [Google Scholar] [CrossRef]
- Masci, M.; Pasquini, L.; Alsaied, T.; Di Chiara, L.; Formigari, R.; Galletti, L.; Campanale, C.M.; Romiti, A.; Bonito, M.; Bagolan, P.; et al. Reliability of Fetal Echocardiography in Predicting Postnatal Critical Hypoxia in Patients with Transposition of Great Arteries and Intact Ventricular Septum. Pediatr Cardiol 2021, 42, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- Buca, D.; Winberg, P.; Rizzo, G.; Khalil, A.; Liberati, M.; Makatsariya, A.; Greco, F.; Nappi, L.; Acharya, G.; D'Antonio, F. Prenatal risk factors for urgent atrial septostomy at birth in fetuses with transposition of the great arteries: A systematic review and meta-analysis. J Matern Fetal Neonatal Med 2022, 35, 598–606. [Google Scholar] [CrossRef]
- Gottschalk, I.; Walter, A.; Menzel, T.; Weber, E.C.; Wendt, S.; Sreeram, N.; Gembruch, U.; Berg, C.; Abel, J.S. D-Transposition of the great arteries with restrictive foramen ovale in the fetus: The dilemma of predicting the need for postnatal urgent balloon atrial septostomy. Arch Gynecol Obstet 2024, 309, 1353–1367. [Google Scholar] [CrossRef] [PubMed]
- Slodki, M.; Axt-Fliedner, R.; Zych-Krekora, K.; Wolter, A.; Kawecki, A.; Enzensberger, C.; Gulczynska, E.; Respondek-Liberska, M.; International Prenatal Cardiology Collaboration, G. New method to predict need for Rashkind procedure in fetuses with dextro-transposition of the great arteries. Ultrasound Obstet Gynecol 2018, 51, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Jouannic, J.M.; Gavard, L.; Fermont, L.; Le Bidois, J.; Parat, S.; Vouhe, P.R.; Dumez, Y.; Sidi, D.; Bonnet, D. Sensitivity and specificity of prenatal features of physiological shunts to predict neonatal clinical status in transposition of the great arteries. Circulation 2004, 110, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Rychik, J.; Liu, L.; Tian, Z. OC17.07: Relationship between foramen ovale restriction and flow characteristics of the ductus arteriosus in the fetus with transposition of the great arteries. Ultrasound in Obstetrics & Gynecology 2019, 54, 43–44. [Google Scholar] [CrossRef]
- Zeng, S.; Zhou, Q.C.; Zhou, J.W.; Li, M.; Long, C.; Peng, Q.H. Volume of intracranial structures on three-dimensional ultrasound in fetuses with congenital heart disease. Ultrasound Obstet Gynecol 2015, 46, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Saadeh, M.; Zhao, Y.; Galadima, H.; Chaoui, R.; Sinkovskaya, E.; Abuhamad, A. Relationship Between Cavum Septi Pellucidi Measurements and Fetal Hypoplastic Left Heart Syndrome or Dextro-Transposition of the Great Arteries. J Ultrasound Med 2018, 37, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- Haligheri, G.; Patel, C.R.; Komarlu, R. Prenatal Delineation of Coronary Anatomy in Dextro-Transposition of Great Arteries. J Cardiovasc Echogr 2021, 31, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Kaji, T.; Hayabuchi, Y.; Maeda, K.; Nakayama, S.; Irahara, M. Prenatal assessment of coronary artery anatomy using color Doppler in cases of D-transposition of the great arteries: Case reports. J Obstet Gynaecol Res 2017, 43, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Pasquini, L.; Sanders, S.P.; Parness, I.A.; Colan, S.D.; Van Praagh, S.; Mayer, J.E., Jr.; Van Praagh, R. Conal anatomy in 119 patients with d-loop transposition of the great arteries and ventricular septal defect: An echocardiographic and pathologic study. J Am Coll Cardiol 1993, 21, 1712–1721. [Google Scholar] [CrossRef]
- Massoudy, P.; Baltalarli, A.; de Leval, M.R.; Cook, A.; Neudorf, U.; Derrick, G.; McCarthy, K.P.; Anderson, R.H. Anatomic variability in coronary arterial distribution with regard to the arterial switch procedure. Circulation 2002, 106, 1980–1984. [Google Scholar] [CrossRef]
- Paladini, D.; Bottelli, L.; Lops, G.; Tuo, G. Color Doppler visualization of fetal coronary arteries is enhanced by high resolution and Radiantflow. Ultrasound Obstet Gynecol 2022, 60, 432–434. [Google Scholar] [CrossRef] [PubMed]
- Wiechec, M.; Nocun, A.; Stettner, D.; Knafel, A. OC02.02: Conotruncal anomalies: How effective is first trimester diagnosis? Ultrasound in Obstetrics & Gynecology 2014, 44, 3. [Google Scholar]
- Nocuń, A.; Wiecheć, M.; Dudzik, M.; Serafin, K. The role of first-trimester single arterial vessel sign instead of a V-sign at the level of the three-vessel and tracheal view in screening for congenital heart diseases. Prenatal Cardiology 2023, 1–12. [Google Scholar] [CrossRef]
- Karim, J.N.; Bradburn, E.; Roberts, N.; Papageorghiou, A.T.; study, A. First-trimester ultrasound detection of fetal heart anomalies: Systematic review and meta-analysis. Ultrasound Obstet Gynecol 2022, 59, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Rotar, I.C.; Muresan, D.; Marginean, C.; Marginean, C.; Iliescu, D.G.; Iliescu, D.G.; Tudorache, S.; Tudorache, S. First trimester fetal heart evaluation. A pictorial essay. Med Ultrason 2020. [CrossRef]
- Lee, M.Y.; Won, H.S.; Han, Y.J.; Ryu, H.M.; Lee, D.E.; Jeong, B.D. Clinical value of chromosomal microarray analysis in prenatally diagnosed dextro-transposition of the great arteries. J Matern Fetal Neonatal Med 2020, 33, 1480–1485. [Google Scholar] [CrossRef] [PubMed]
- Skoric-Milosavljevic, D.; Tadros, R.; Bosada, F.M.; Tessadori, F.; van Weerd, J.H.; Woudstra, O.I.; Tjong, F.V. Y.; Lahrouchi, N.; Bajolle, F.; Cordell, H.J.; et al. Common Genetic Variants Contribute to Risk of Transposition of the Great Arteries. Circ Res 2022, 130, 166–180. [Google Scholar] [CrossRef]
- Peake, L.K.; Draper, E.S.; Budd, J.L.; Field, D. Outcomes when congenital heart disease is diagnosed antenatally versus postnatally in the UK: A retrospective population-based study. BMC Pediatr 2015, 15, 58. [Google Scholar] [CrossRef]
Figure 1.
Details at the FT cardiac sweep, in a normal (a and b) and in a TGA case (c).
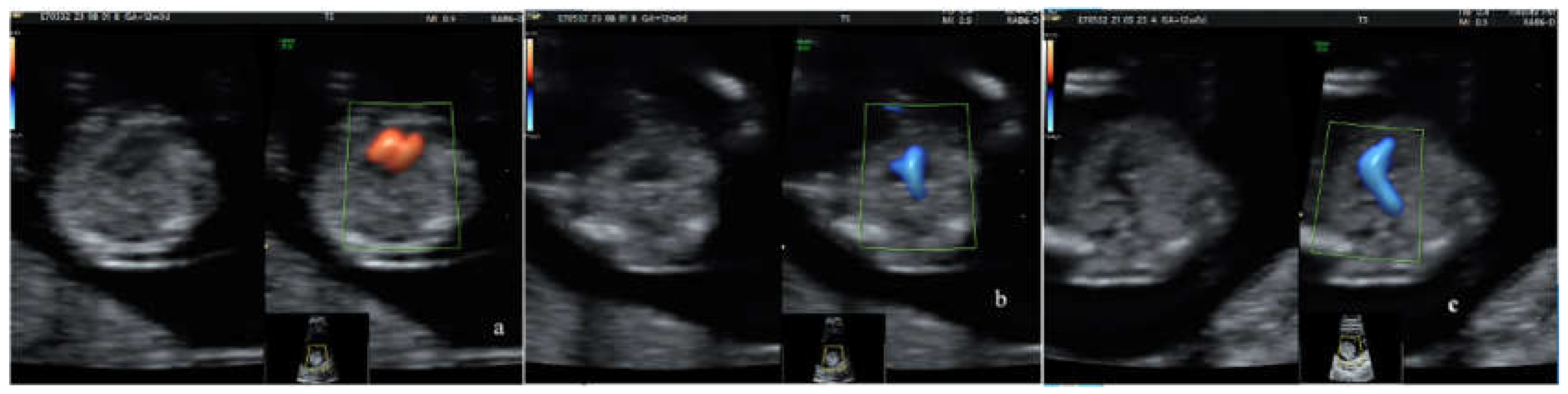
Figure 2.
TGA cases: the right ventricle outflow tract (RVOT) at level of the three-vessel with trachea (3VT) view (A) and parallel arterial trunks (B).
Figure 2.
TGA cases: the right ventricle outflow tract (RVOT) at level of the three-vessel with trachea (3VT) view (A) and parallel arterial trunks (B).
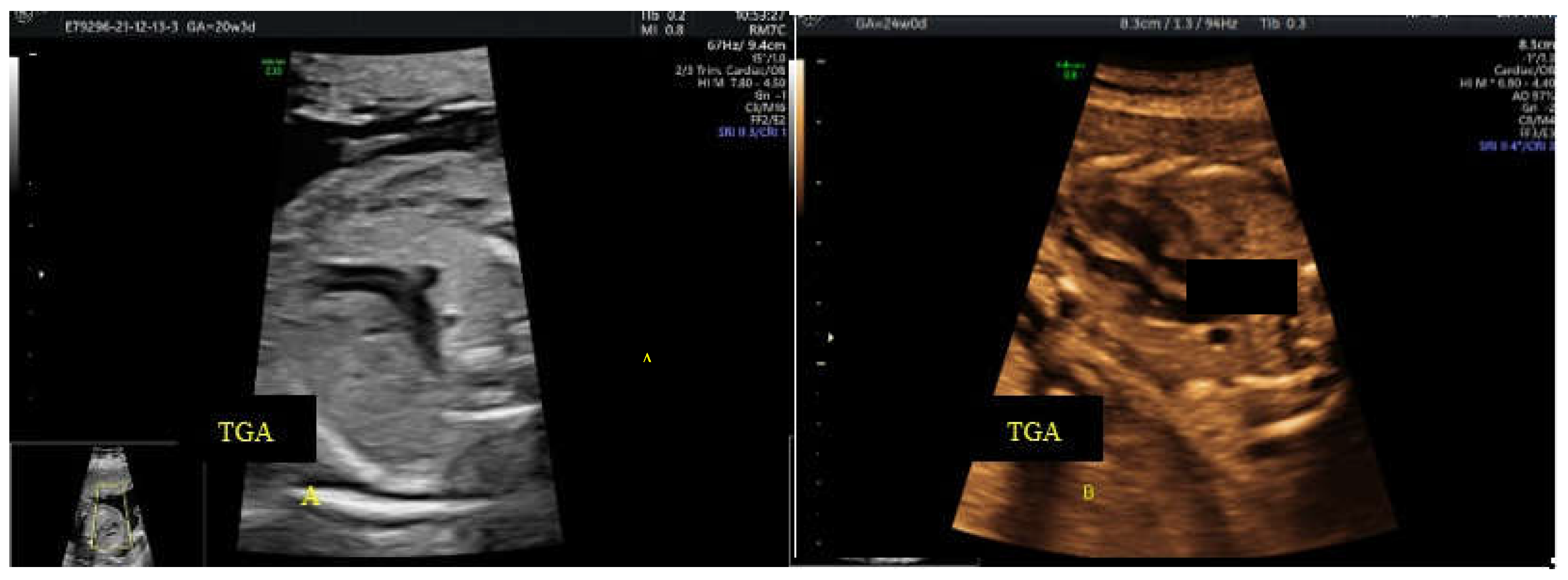
Figure 3.
Flowchart presenting the selected study population.
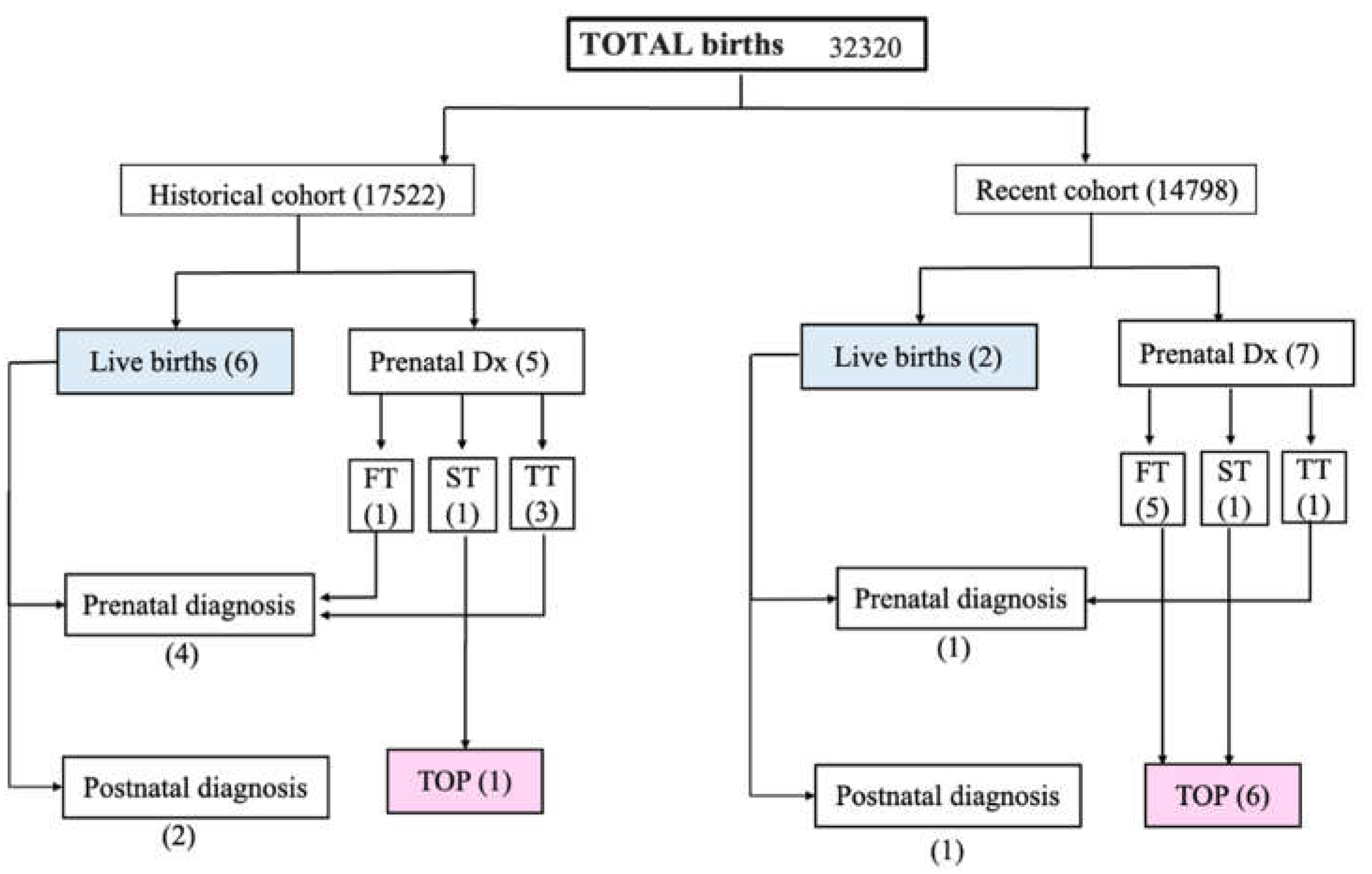
Figure 4.
Graphic representation of gestational age at diagnosis (in blue dots – the historical cohort, in pink dots – the recent cohort, trends are represented by dotted lines).
Figure 4.
Graphic representation of gestational age at diagnosis (in blue dots – the historical cohort, in pink dots – the recent cohort, trends are represented by dotted lines).
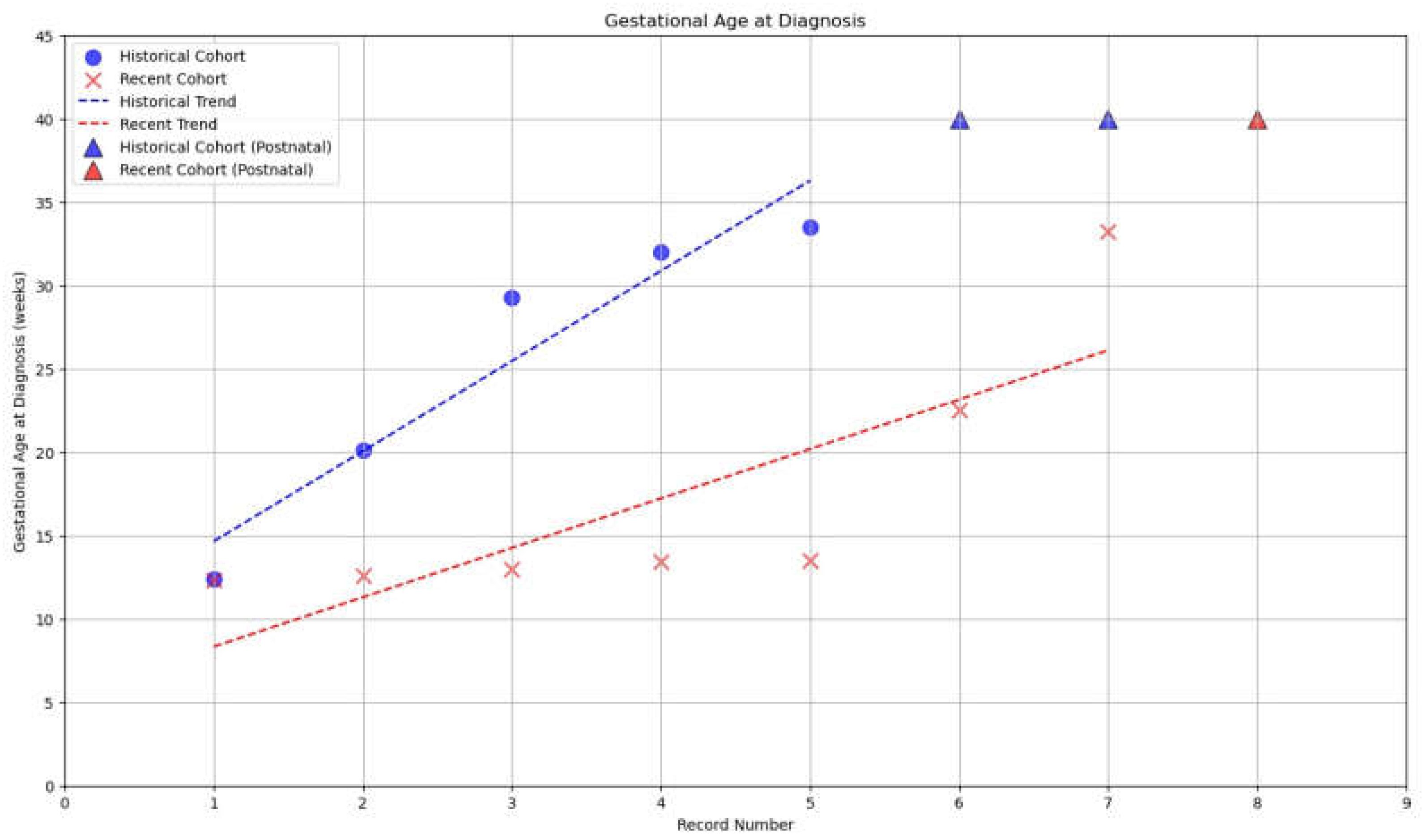
Figure 5.
Postabortum conventional autopsy details: a. specimen after first trimester medical TOP – CRL (Crown-rump length) 68 mm; in the upper window – the fetal heart is shown in transverse section on the operator’s fingers; the comparative size may be appreciated. b. specimen after second trimester medical TOP; the accurate diagnosis of TGA is reachable.
Figure 5.
Postabortum conventional autopsy details: a. specimen after first trimester medical TOP – CRL (Crown-rump length) 68 mm; in the upper window – the fetal heart is shown in transverse section on the operator’s fingers; the comparative size may be appreciated. b. specimen after second trimester medical TOP; the accurate diagnosis of TGA is reachable.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



