
Submitted:
16 April 2024
Posted:
17 April 2024
You are already at the latest version
Abstract
Spinal muscular atrophy (SMA) is an orphan disease characterized by progressive degeneration of spinal alpha motor neurons. In recent years, nusinersen and several other drugs have been approved for the treatment of this disease. Transcutaneous spinal cord stimulation (tSCS) modulates spinal neuronal networks, resulting in changes in locomotion and posture in patients with severe spinal cord injury and stroke. We hypothesize that tSCS can activate motor neurons that are intact and restored by medication, slow the decline in motor activity, and contribute to the development of motor skills in SMA patients. Thirty-seven children and adults with SMA types 2 and 3 participated in the study. The median duration of drug treatment was over 20 months. Application of tSCS was performed during physical therapy for 20-40 minutes per day for ~12 days. Outcome measures were specific SMA motor scales, goniometry of contractured joints, forced vital capacity. Significant increases in motor function, improved respiratory function, and decreased contracture were observed in both types 2 and 3 SMA participants. The magnitude of functional changes was not associated with participants age. Further studies are needed to elucidate the reasons for the beneficial effects of spinal cord electrical stimulation in SMA.
Keywords:
spinal muscular atrophy
; spinal cord stimulation
; physical therapy
; nusinersen
; risdiplam
; onasemnogene abeparvovec
1. Introduction
Spinal muscular atrophy (SMA) is a genetic disease characterized by progressive muscle weakness caused by spinal motor neuron dysfunction. Rehabilitation of patients with SMA aims to slow the loss of motor skills and reduce the burden of the disease. Since 2016, orphan drugs (nusinersen and others) have been used in clinical practice to correct the genes that are directly related to the pathogenesis of SMA. Previously, we demonstrated in a case series that transcutaneous spinal cord stimulation (tSCS) combined with physical therapy is an effective rehabilitation method for patients treated with nusinersen [1]. We now evaluated the effect of tSCS in 37 SMA patients treated with nusinersen and other orphan drugs, and investigated the correlation between SMA severity, patients age, duration of drug therapy and extent of motor changes after tSCS treatment.
1.1. Spinal Muscular Atrophy
SMA is caused by progressive degeneration of spinal alpha motor neurons, resulting in progressive weakness and atrophy of proximal muscles [2,3]. Alpha motor neuron degeneration is caused by deletion or mutation of the SMN1 gene [4]. This gene is responsible for the activity and survival of motor neurons. The paralogous SMN2 gene is similar to the SMN1 gene, except for several single nucleotide substitutions, including one in exon 7, resulting in aberrant pre-mRNA splicing and exon 7 skipping in nearly 90% of the transcripts. The severity of SMA correlates with the copy number of the SMN2 gene carried by patients [2].
There are five SMA phenotypes that differ in age of onset and maximum achievable motor function associated with that age, and three of these are major phenotypes [5]. SMA type 1 manifests in the first 6 months after birth, maximum motor skills are sitting with support. SMA type 2 between the first 6 and 18 months of life, patients with type 2 are able to sit independently. SMA type 3 - after 18 months of age, patients are able to stand upright and walk. Patients with SMA type 1 usually have two or three copies of SMN2, SMA type 2 patients have three copies, and SMA type 3 patients have three or four copies [6]. The classification of SMA into five phenotypes is conditional; in practice, these phenotypes represent a continuum. Clinicians identify additional subtypes, and patients with SMA are characterized by functional status as "non-sitters," "sitters," or "walkers” [5]. In terms of functional abilities, SMA patients are also defined as non-ambulatory patients who are able to sit independently and ambulatory patients [5].
1.2. SMA Orphan Drugs
SMA is an orphan disease with an incidence of less than 5 per 10,000. Drugs used to treat rare diseases are called orphan drugs [7]. Drugs that correct the function of genes directly involved in the pathogenesis of SMA have entered the clinical practice in the last decade [8].
The first disease-modifying drug, nusinersen, was approved for the pharmaceutical market by the U.S. Food and Drug Administration in 2016, and showed good efficacy in the early stages of the disease [9,10]. Nusinersen is an antisense oligonucleotide drug; its activity is based on the correction of the splicing of exon 7 of the endogenous SMN2 pre-mRNA. The drug has no restrictions on age and type of SMA, it is taken for life, maintenance doses are administered intrathecally every 4 months.
1.3. Transcutaneous Spinal Cord Stimulation
In our study, tSCS is the electrical stimulation by rectangular pulses at a frequency of ~30 Hz and modulated with 5-10 kHz pulses. The electrodes were placed on the skin - cathodes over the spinal motor centers, at the level of C3-C5, T11-T12 or L1-L2 vertebrae, and anodes over the iliac crests or clavicles [1]. Many studies with healthy subjects have shown that tSCS modulates spinal neuronal networks, manifested by changes in locomotion and posture [14,15,16,17].
This non-invasive spinal cord stimulation has a clinical impact. In patients paralyzed by spinal cord injury, tSCS induces and improves voluntary movement, muscle strength and function. [18,19,20]. In stroke patients, significant and clinically meaningful differences in walking parameters were achieved after two weeks of tSCS in combination with physical therapy [21]. In children with cerebral palsy, a similar short course of rehabilitation with tSCS resulted in significant and meaningful clinical differences in Gross Motor Function Measure scores [22,23], and acute tSCS improved postural and locomotor skills [24].
1.4. Purpose and Hypothesis of the Study
In all of the above cases where tSCS was used to activate spinal motor centers located in “healthy” areas of the spinal cord, the motor deficits were caused by injury to brain-muscle signaling or abnormal brain activity. In SMA, the alpha motor neurons of the spinal cord are genetically affected, resulting in progressive muscle weakness and the development of muscle atrophy. It has been shown that 18 months of nusinersen treatment in children dramatically increases the number of motor neurons [25], and 10 months of risdiplam treatment in adult patients increases the active motor unit pool [26].
We hypothesized that in patients with SMA, tSCS could activate intact motor neurons and motor neurons that were restored after treatment with pathogenic drugs, leading to a slower decline in motor activity and the development of motor skills. We have obtained encouraging results with stimulation in 5 patients with SMA types 2 and 3 [1]. In this article, we verified these results in a study with a large number of patients and also examined the efficacy of tSCS in relation to SMA type, functional status, age and duration of medication.
2. Materials and Methods
The study was performed at the EirMED Rehabilitation Center (St. Petersburg, Russia) between November 2022 and November 2023. Procedures, training, and outcome measures were performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of EirMED Rehabilitation Center (#22-01, approved on August 12, 2022). Written informed consent was obtained from all adult participants and parents of child participants.
2.1. Participants
Thirty-seven participants with genetically confirmed SMA type 2 or 3 were studied (Table 1, Table S1 and Table S2). Thirty participants were treated with nusinersen, six – with risdiplam and one – with onasemnogene abeparvovec. Treatment with orphan drugs was continued for 23 ± 9 and 28 ± 12 months in SMA type 2 and 3 groups, respectively. Participants had previously received physical therapy aimed to prevent loss of muscle strength and development of joint contractures.
2.2. Procedures
The stimulation of the spinal cord was performed in combination with physical therapy. These interventions aimed to achieve personalized treatment goals. Detailed examples of personalized treatment goals, physical exercises, and tSCS strategy for five SMA type 2 and 3 patients can be found in our previous study [1]. Physical therapy with tSCS took ~1 h per day and carried out 6 days a week. Moreover, physical procedures such as massage and balneotherapy were performed to improve coordination and proprioception. In addition, there were sessions with an ergo therapist and a speech therapist. The intensity of those sessions was adapted to the individual constitution of the participants. All therapies, including tSCS training and other procedures, lasted 3 h per day. The total duration of therapy was ~12 days.
2.2.1. Treatment Goals
The goals were individualized and determined by the SMART (specific, measurable, achievable, realistic/relevant and timed) method because this was an effective method to achieve behavioral change and enhance the quality of life [27]. Individual goals ranged from “turning from supine to lateral position, increasing hand strength, increasing endurance, decreasing joint contracture” (participant 7K14) to “improving stepping pattern, increasing walking speed” (participant 15K48).
2.2.2. Physical Therapy
Physical exercises included passive and active stretching movements in the joints of the upper and lower extremities, passive and active positioning, moving and holding weights, body movements to prevent scoliosis, stepping and kicking movements, breathing exercises, etc. In some cases, to facilitate limb movements, the movements were performed with the limb in a gravity-neutral position, with the participant lying on their side, with the leg or arm supported by a swing [15,28].
2.2.3. Transcutaneous Spinal Cord Stimulation
One, two or three regions of the spinal cord were stimulated, above the cervical and/or lumbar enlargements of the spinal cord and/or above the sacral segments (Table S3 and Table S4). When exposed to the muscles of the upper extremities, stimulation of the neck and upper thoracic region was used. Stimulation of the lower thoracic, lumbar, and coccygeal regions was performed to influence the muscles of the trunk and lower extremities. Stimulation sites were selected depending on the rehabilitation goals, considering the results of all previously published studies [29,30,31,32].
Two adhesive round electrodes (Ø 2.5 cm; ValuTrode® Axelgaard Manufacturing Co., Fallbrook, California, USA) were placed on the skin above the spinous process of either of C5, Th11, L1, and L5 vertebrae or coccyx. These electrodes were independent cathodes. Two adhesive rectangular electrodes (4 × 5 cm2; ValuTrode® Axelgaard Manufacturing Co., Fallbrook, California, USA) above iliac crests were common anodes. Bipolar rectangular pulses of 1 ms duration, ~30 Hz, modulated at 5 kHz, produced by Neostim-5 (Cosyma Ltd., Moscow, Russia).
The intensity of tSCS was determined individually for each participant so that the current amplitude was maximally tolerable without causing unpleasant sensations. The intensity was adjusted by the therapists from session to session to follow this rule.
2.3. Outcome measures
The tests were performed one day before and one day after the treatment course in the absence of tSCS. The outcome measures were specific for SMA patients [33,34]. From the spectrum of all specific tests, invasive tests were selected to assess disability and functional limitations specific to both type 2 and type 3 SMA patients. Efficacy criteria were contracture joint goniometry [35], Revised Upper Limb Module (RULM) [36], modified Hammersmith Function Motor Scale Expanded (HFMSE) [37], and forced vital capacity (FVC) [38]. Participants were allowed to refuse to be tested due to fatigue.
Therapists documented each session. Information on tSCS details, changes in physical exercises, and possible side effects or adverse events was available from session to session.
Therapists, adult participants, and parents of child participants were interviewed on the last day of the course about the significant changes in motor activity and motor skills that they observed during the course of the study.
2.3.1. Joint Goniometry
The ranges of passive motion of the shoulder, elbow, wrist, hip, knee, and ankle were determined and documented for each participant. Knee contracture was more common among contractures of other joints in the participant population. Changes in knee range of motion (ROM) were analyzed in the SMA type 2 and 3 groups. Knee extension was measured in the supine position with the hip extended as well as with the hip flexed to 90 degrees. According to standards [39], a single determination of ROM was performed.
2.3.2. Revised Upper Limb Module
The RULM scale is a robust clinical measure for assessing upper limb motor function in SMA [36]. The scale establishes functional levels covering distal to proximal movements. It is a 20-item scale with a maximum score of 37, with higher scores indicating better upper limb function.
2.3.3. Hammersmith Function Motor Scale Expanded
HFMSE is a standard scale of functional ability in patients with SMA types 2 and 3 [37]. This scale comprises 33 items; the maximum possible score is 66. A limitation of this test is the inability to sit on a chair, couch, or floor (not in a wheelchair) for ~3 seconds without back and hand support.
2.3.4. Forced Vital Capacity
FVC appears to be the most reliable measure among other pulmonary parameters to be used as outcomes in SMA [33,40]. According to the guidelines[38], absolute values of FVC were determined three times. The largest FVC observed from three of the acceptable values was compared with age-matched controls as a percentage predicted for age, which was calculated based on height.
2.4. Statistics
Statistical analysis was performed using Prism 10 for Windows (GraphPad Software, LLC), Excel 2019 (Microsoft Office 2019), and Analyse-it for Microsoft Excel 6.15.4 (Analyse-it Software, Ltd.). The Shapiro-Wilk W test was used to determine whether the data followed a normal distribution. When data were not normally distributed, nonparametric statistics were used.
Values are presented as median [first quartile (Q1), third quartile (Q3)] or as mean ± standard deviation and were calculated depending on values distribution.
Significance of differences between pre- and post-treatment test results was determined using the Wilcoxon or Student t-test. The significance of the differences between the parameters of the SMA type 2 and type 3 groups was calculated using the Mann-Whitney U test. Statistical significance was set at p-value < 0.05. Correlations between test results and demographic and clinical parameters were determined by Spearman’s correlation.
3. Results
3.1. SMA type 2 and type 3 participants
The groups differed in age (Table 1, Figure 1a). The SMA type 2 group was significantly younger than the SMA type 3 group (p=0.006). There was one adult participant in the SMA type 2 group and six adult participants in the SMA type 3 group (Table S1 and Table S2).
Functionally, the participants were “non-sitters”, “sitters”, or “walkers” [5]. Prior to treatment, participants in the SMA type 2 group were more severe than participants in the SMA type 3 group (Table 2, Figure 1). In the SMA type 2 group there were predominantly "non-sitters" and in the SMA type 3 group there were predominantly "sitters". There were two "walkers" in the SMA type 3 group. RULM and HFMSE scores were significantly lower in the SMA type 2 group than in the SMA type 3 group (p=0.0004 and p=0.03, respectively). Pulmonary function, as measured by FVC was also significantly lower in the SMA type 2 group (p=0.01). Knee ROM was less in the SMA type 2 group as a trend (p=0.089).
Funct. status – Functional status; N-S – non-sitters; S – sitters; W – walkers; RULM – Revised Upper Limb Module; HFMSE – Hammersmith Function Motor Scale Expanded; FVC – Forced Vital Capacity
3.2. Transcutaneous Spinal Cord Stimulation
Participants tolerated the stimulation well. No adverse events were observed.
The maximal current intensity, averaged over two or three stimulation sites (Table S3, Table S4), was 22 ± 10 mA and 30 [20; 40] mA in the SMA type 2 and type 3 groups, respectively. The difference between the groups was significant (p=0.01), the current intensity used in sessions with SMA type 2 participants was higher.
Training with tSCS lasted for 20 [20; 40] and 30 [25; 45] minutes in the SMA type 2 and 3 groups, respectively. The difference between the groups was insignificant.
3.3. Revised Upper Limb Module
Nineteen participants in both groups showed an increase in RULM score after the tSCS course (Figure 2 and Figure S1). One participant in the SMA type 2 group and seven in the SMA type 3 group showed the best score of 37 points before and after the tSCS session; these results were not included.
The difference between the post- and pre-treatment RULM scores was 1 [0; 3] and 3 [2; 6] points in the SMA type 2 and 3 groups, respectively. One SMA type 2 participant and seven SMA type 3 participants had a maximum score of 37 before and after the tSCS sessions. Their scores were not included in the RULM difference calculation. Both RULM differences were significantly higher than zero (p=0.001 and p=0.002 in the SMA type 2 and type 3 groups, respectively). The SMA type 3 RULM difference tended to be higher than the SMA type 2 difference (p=0.06).
After tSCS, the RULM score was 22 [16; 29] and 37 [32; 37] in the SMA type 2 and type 3 groups, respectively. The excess of the SMA type 3 group was significant (p=0.0001).
3.4. Hammersmith Function Motor Scale Expanded
Thirteen of the SMA type 2 participants and one SMA type 3 participant were unable to sit for ~3 seconds without back and hand support to begin the HMFSE test or took the opportunity to refuse the test due to fatigue. The results of the other participants are shown in Figure 3, Figure S1.
The difference between post- and pre-treatment HMFSE scores was 2 [0; 2] and 2 [1; 5] points in the SMA type 2 and 3 groups, respectively. The HMFSE difference was significantly greater than zero in the SMA type 3 group (p=0.0006) and different as a trend in the SMA type 2 group (p=0.06).
After the tSCS sessions, the HMFSE score was 26 [17; 38] and 43 ± 13 in the SMA type 2 and type 3 groups, respectively. Inequality between the groups after tSCS was significant (p=0.02).
3.5. Forced Vital Capacity
Six SMA type 2 participants took the opportunity to refuse the breathing test due to fatigue. The results of the others are shown in Figure 4 and Figure S1.
The difference between post- and pre-treatment FVC was 3 ± 5% and 2 [0; 11]% in the SMA type 2 and 3 groups, respectively. The FVC difference was significantly greater than zero in the SMA type 3 group (p=0.005) and different as a trend in the SMA type 2 group (p=0.08).
After the tSCS sessions, the FVC were 58 ± 29% and 86 ± 24% in the SMA type 2 and type 3 groups, respectively. The difference between the groups after tSCS was significant (p=0.007).
3.6. Knee Range of Motion
Knee contracture was observed in eleven of the SMA type 2 participants and eight of the SMA type 3 participants (Table S1 and Table S2). The results for these participants are shown in Figure 5 and Figure S1(d). The right and left knee ROM results are combined.
The differences between post- and pre-treatment ROM were 10 ± 9 degrees and 8 ± 7 degrees in the SMA type 2 and 3 groups, respectively. Both ROM differences were significantly higher than zero (p<0.0001 and p=0.001 in the SMA type 2 and type 3 groups, respectively).
3.7 Motor skills
Opinions of trainers, adult participants and parents of child participants about significant changes in motor activity and acquisition of new skills or restoration of lost skills during the course of tSCS in combination with physical therapy are presented in Table S4 and Table S6. In summary, eleven and ten participants of the SMA type 2 and type 3 groups, respectively, gained motor skills after the tSCS course.
The distribution of these motor skills ranged from elementary skills such as lifting the head in the prone and supine positions (participant 6K12) to more complex skills such as walking up and down stairs with one-hand support (instead of two-hand support) (participant 11K34). Participants 1K2, 10K30, 7K14, 8K19, and 9K28 developed skills to control the position of body parts. Participants 21K53, 9K22, 12K42, 7K15, 4K7 acquired static balance skills. New motor skills related to movement in space were developed by participants 16K50, 3K5, 5K8, 9K26, and 4K7. Participants 8K21 and 15K49 were able to perform coordinated hand movements for self-service.
3.8. Age and Adults
The efficacy of orphan drugs is restricted to older children and adults with SMA [6,9,10]. A multicenter observation on adult SMA patients treated with nusinersen showed that, although half of the patients experienced subjective improvement in function, there were no significant objective changes [41].
We analyzed the correlation between age and main tSCS outcomes (Table 3, Figure S2). No association was found between age and differences in the outcomes.
Adult participants are indicated by dotted lines in Figure 2, Figure 3, Figure 4 and Figure 5 and are shown in gray in Tables S1-S6.
Adult SMA type 2 participant (14K44), 39 years old, is a sitter with peripheral tetraparesis, has contractures of the knee and ankle joints. After tSCS course her knee ROM did not increase, ankle ROM increased by 3-7 deg. Her RULM score increased by 6 points. She could not be tested for HMFSE score due to inability to sit without hands or back support. She refused the breathing study due to fatigue. She did not report significant changes in motor activity and acquisition of new skills after the course.
Six SMA type 3 participants, 20-42 years old, all sitters were in the SMA type 3 group. In the adult participants, after the tSCS course, RULM increased by 3 [2; 3] points, HMFSE - by 3 [1; 5] points, FVC - by 2 [0; 5] %, knee ROM - by 12 [9; 13] degrees. The differences tended to increase above zero in the RULM and HMFSE tests (p=0.06 in both) and were insignificantly different from zero in the other tests. These results and those of children in the SMA type 3 group are shown in Figure 6. All differences in the outcomes between adults and children in the SMA type 3 group are statistically similar. After the tSCS course, three out of six adult participants and seven out of eleven child participants gained or regained motor skills (Table S6), 50% and 60%, respectively.
4. Discussion
This study evaluated the efficacy and safety of non-invasive spinal cord stimulation for motor rehabilitation in type 2 and type 3 SMA patients treated with orphan drugs. No adverse events were observed in the cohort of thirty-seven participants ranging in age from 3 to 42 years, providing safety data for the use of tSCS in SMA patients.
The main finding was that a 2-week physical therapy protocol combining tSCS with the use of a specific orphan drug treatment led to a significant increase in motor function in both SMA type 2 and type 3 participants. Motor scores increased significantly after tSCS. Twenty-one of thirty-seven participants gained new motor skills or regained lost skills. Respiratory function, which correlates strongly with loss of muscle function [42,43], improved significantly in the SMA type 3 group and trended upward in the SMA type 2 group. Joint contractures, which limit the mobility of SMA patients [5,39] decreased significantly after the course.
Reliable improvements in motor function should be associated with the concurrent use of stimulation with physical therapy. In controlled studies involving patients with SMA, physical therapy alone has not been shown to alter muscle strength and motor function [44].
4.1. Minimal Clinically Important Difference and Stimulation Results
In addition to statistical significance, achieving of the minimal clinically important difference (MCID) is meaningful. The MCID is the “smallest change or difference in an outcome measure that is perceived as beneficial and would lead to a change in the patient’s medical management” [45]. The issue of MCID in SMA outcomes is controversial [34,46]. MCIDs for pulmonary and contracture indicators have not been defined for SMA patients.
4.1.1. RULM and HMFSE Scales
In adult SMA patients the MCIDs of the RULM and HMFSE scales are 2.9 and 4.3 points, respectively [46]. These values were obtained from 15 and 36 SMA type 2 and type 3 participants, respectively. The authors of this study pointed out the great heterogeneity of patients' motor functions. MCID values differed between subgroups (SMA type 2 and type 3 participants, ambulatory and non-ambulatory participants). The authors concluded that further studies are needed to adjust the MCID values.
In the study by Pera et al. [47], parents of 149 SMA type 2 and type 3 patients, aged from 17 months to 30 years, considered a 1-point increase in HMFSE score to be meaningful. For pediatric SMA patients, the MCID of the RULM has not been established and a change of 2 to 3 points has been recommended as meaningful [34,48].
We observed that twelve out of twenty-nine participants who did not have a top RULM score of 37 points before the course increased their RULM score by 2 or more points after the tSCS course (Figure S1(a)). Eleven out of twenty-three participants who were tested by HMFSE increased their HMFSE score by 1 point or more (Figure S1(b)).
In addition to the magnitude of the outcome differences, the time period over which these positive differences were achieved is important. In the phase 3 clinical trial of nusinersen in eight-four pediatric SMA type 2 participants (2-9 years old), the average increase in RULM score and HFMSE score was ~1.5 points 3 months after drug treatment (Figure 1 in [10]). In our study, when drug treatment was combined with tSCS and physical therapy for 2 weeks, similar results were obtained. Thus, tSCS accelerates the recovery of drug-induced motor functions.
4.1.2. ROM Results
Minimal hip and knee joint contractures are associated with decreased mobility. Fixed contractures of the knee joint limit the ability to perform functional activities such as rising from a chair, walking up and down stairs, standing, rolling, and comfortable positioning in bed and in a wheelchair [35,39]. In eighty participants with SMA types 2 and 3 (aged 1.1-45.2 years), a decrease in passive knee ROM of 9 degrees or less was shown to correlate with motor deterioration tested by HMFSE [35]. We showed that after tSCS, the mean passive knee ROM increased by more than 8 degrees in both SMA groups. These data are associated with the increase in motor scale scores.
4.1.3. FVC Results
Spinal muscular atrophy affects the respiratory system [43,49]. In the retrospective study of forty-one untreated SMA type 2 and 3 patients, FVC was strongly correlated with muscle strength [50], Spearmen’s correlation coefficient was 0.78. Natural history study of 170 untreated SMA patients showed -1.32 to -0.67% reduction in FVC per year [42]. A study in nineteen adult non-ambulatory SMA patients showed that 10-14 months of nusinersen treatment resulted in stability of outcome measures of FVC, with no increase or decrease in this outcome [51]. In our study FVC increased by 3% as a trend in SMA type 2 group and significantly by 2% in type 3 group. Thus, spinal cord stimulation improves lung function when used in combination with orphan drug treatment.
4.1.4. Motor Skills Results
Motor skills were assessed by researchers using the RULM and HMFSE scales. In addition, we interviewed instructors, adult participants, and parents of pediatric participants to learn about the motor skills they felt emerged after the course. These motor skills are not always captured on standard scales, for example, moving from the floor to the wheelchair or the ability to wash the face with the right hand without supporting the forearm with the left hand. People who spend a lot of time around patients with SMA pay attention to small changes in motor improvement because new motor skills make it easier to manipulate patients and improve the quality of life of patients and their families. Caregivers of patients with SMA have been found to experience significant burdens, including impaired health-related quality of life, reduced work ability and productivity, and financial stress [52].
Twenty-one of thirty-seven participants reported new motor skills after the tSCS course. This is a good result because rehabilitation of patients with SMA is currently aimed not at improving motor activity, but at slowing the process of motor loss and reducing the burden of the disease [5].
4.2. Age Influence
Dysfunction and degeneration of α-motor neurons in the spinal cord occur with age in the natural history of SMA patients [3]. Orphan drug treatment is more effective if started early [6,53]. Therefore, we predicted that stimulation would be more effective in pediatric patients than in adult patients. We analyzed the correlation between age and the magnitude of changes in all the parameters controlled in the study. No association was found between age and differences in outcomes. This is unexpected. This result suggests a complex mechanism of motor function improvement due to the application of stimulation. This mechanism needs to be further investigated.
5. Conclusions
A two-week course of stimulation combined with physical therapy in patients taking nusinersen and other orphan drugs in this group resulted in significant increases in motor function, improved respiratory function, and decreased contracture in both type 2 and type 3 SMA participants. The magnitude of functional changes did not vary with patient age. Further studies are needed to elucidate the reasons for the beneficial effects of spinal cord electrical stimulation in SMA.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Frequency distribution of the difference in RULM, HFMSE, FVC, and ROM before and after tSCS sessions in SMA type 2 and type 3 groups; Figure S2: Difference in RULM, HFMSE and FVC before and after tSCS sessions versus age; Table S1: Demographics and clinical parameters of SMA type 2 participants; Table S2: Demographics and clinical parameters of SMA type 3 participants; Table S3: Spinal stimulation parameters of SMA type 2 participants; Table S4: Spinal stimulation parameters of SMA type 3 participants; Table S5: New motor skills of participants with SMA type 2 after the tSCS training course; Table S6: New motor skills of participants with SMA type 3 after the tSCS training course.
Author Contributions
Conceptualization, N.K. and T.M.; methodology, T.M., A.N. and M.M.; formal analysis, N.S.; investigation, N.S., I.S., E.S. and N.E.; data curation, N.K.; supervision, writing, T.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Ministry of Science and Higher Education of the Russian Federation, agreement No. 075-15-2022-303.
Institutional Review Board Statement
The procedures and investigations were performed in according to Declaration of Helsinki and approved by the Ethics Committee of EirMED Rehabilitation Center (#22-01, date of approval 12 August 2022).
Informed Consent Statement
Parents of all child participants and all adult participants provided informed consent in writing.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors thanked Ekaterina Dudnitskaya for administrative and technical support.
Conflicts of Interest
NK researcher on the study team, hold shareholder interest in EIRMed. TM researcher on the study team, hold shareholder interest in Cosyma. She holds certain inventorship rights on intellectual property licensed by Cosyma. The remaining authors declare no conflicts of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Novikov, A.; Maldova, M.; Shandybina, N.; Shalmiev, I.; Shoshina, E.; Epoyan, N.; Moshonkina, T. First Use of Non-Invasive Spinal Cord Stimulation in Motor Rehabilitation of Children with Spinal Muscular Atrophy. Life 2023, 13, 449. [Google Scholar] [CrossRef] [PubMed]
- Verhaart, I.E.C.; Robertson, A.; Wilson, I.J.; Aartsma-Rus, A.; Cameron, S.; Jones, C.C.; Cook, S.F.; Lochmüller, H. Prevalence, Incidence and Carrier Frequency of 5q–Linked Spinal Muscular Atrophy – a Literature Review. Orphanet J Rare Dis 2017, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, E.; Sumner, C.; Muntoni, F.; Darras, B.T.; Finkel, R.S. Spinal Muscular Atrophy. NATURE REvIEWS 2022. [Google Scholar] [CrossRef]
- Lefebvre, S.; Bürglen, L.; Reboullet, S.; Clermont, O.; Burlet, P.; Viollet, L.; Benichou, B.; Cruaud, C.; Millasseau, P.; Zeviani, M.; et al. Identification and Characterization of a Spinal Muscular Atrophy-Determining Gene. Cell 1995, 1, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, E.; Finkel, R.S.; Muntoni, F.; Wirth, B.; Montes, J.; Main, M.; Mazzone, E.S.; Vitale, M.; Snyder, B.; Quijano-Roy, S.; et al. Diagnosis and Management of Spinal Muscular Atrophy: Part 1: Recommendations for Diagnosis, Rehabilitation, Orthopedic and Nutritional Care. Neuromuscular Disorders 2018, 28, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Nishio, H.; Niba, E.T.E.; Saito, T.; Okamoto, K.; Takeshima, Y.; Awano, H. Spinal Muscular Atrophy: The Past, Present, and Future of Diagnosis and Treatment. International Journal of Molecular Sciences 2023, 24, 11939. [Google Scholar] [CrossRef] [PubMed]
- Sirbu, C.A.; Ivan, R.; Samaha, F.J.; Ionita-Radu, F.; Jianu, D.C.; Vasiliu, O.; Constantin, C.; Tuță, S. Orphan Drugs in Neurology - A Narrative Review. [CrossRef]
- Dangouloff, T.; Botty, C.; Beaudart, C.; Servais, L.; Hiligsmann, M. Systematic Literature Review of the Economic Burden of Spinal Muscular Atrophy and Economic Evaluations of Treatments. Orphanet J Rare Dis 2021, 16, 47. [Google Scholar] [CrossRef] [PubMed]
- Finkel, R.S.; Mercuri, E.; Darras, B.T.; Connolly, N.L.; Kuntz, N.L.; Kirschner, C.A.; Chiriboga, C.A.; Saito, K.; Servais, L.; Tizzano, E. Nusinersen versus Sham Control in Infantile-Onset Spinal Muscular Atrophy. [CrossRef]
- Mercuri, E.; Darras, B.T.; Chiriboga, C.A.; Day, J.W.; Campbell, C.; Connolly, A.M.; Iannaccone, S.T.; Kirschner, J.; Kuntz, N.L.; Saito, K.; et al. Nusinersen versus Sham Control in Later-Onset Spinal Muscular Atrophy. N Engl J Med 2018, 378, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Dangouloff, T.; Servais, L. Clinical Evidence Supporting Early Treatment Of Patients With Spinal Muscular Atrophy: Current Perspectives. TCRM 2019, 15, 1153–1161. [Google Scholar] [CrossRef]
- Mendell, J.R.; Al-Zaidy, S.; Shell, R.; Arnold, W.D.; Rodino-Klapac, L.R.; Prior, T.; Lowes, L.P.; Alfano, L.; Berry, K.; Church, K. Single-Dose Gene-Replacement Therapy for Spinal Muscular Atrophy. [CrossRef]
- Ross, L.F.; Kwon, J.M. Spinal Muscular Atrophy: Past, Present, and Future. NeoReviews 2019, 20, e437–e451. [Google Scholar] [CrossRef]
- Gorodnichev, R.M.; Pivovarova, E.A.; Puhov, A.; Moiseev, S.A.; Gerasimenko, Y.P.; Savochin, A.A.; Moshonkina, T.R.; Chsherbakova, N.A.; Kilimnik, V.A.; Selionov, V.A.; et al. Transcutaneous Electrical Stimulation of the Spinal Cord: A Noninvasive Tool for the Activation of Stepping Pattern Generators in Humans. Human Physiology 2012, 38, 158–167. [Google Scholar] [CrossRef]
- Gerasimenko, Y.; Gorodnichev, R.; Moshonkina, T.; Sayenko, D.; Gad, P.; Reggie Edgerton, V. Transcutaneous Electrical Spinal-Cord Stimulation in Humans. Annals of Physical and Rehabilitation Medicine 2015, 58, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Moshonkina, T.; Grishin, A.; Bogacheva, I.; Gorodnichev, R.; Ovechkin, A.; Siu, R.; Edgerton, V.R.; Gerasimenko, Y. Novel Non-Invasive Strategy for Spinal Neuromodulation to Control Human Locomotion. Available online: https://www.frontiersin.org/articles/10.3389/fnhum.2020.622533/full (accessed on 28 July 2023).
- Shamantseva, N.; Timofeeva, O.; Gvozdeva, A.; Andreeva, I.; Moshonkina, T. Posture of Healthy Subjects Modulated by Transcutaneous Spinal Cord Stimulation. Life 2023, 13, 1909. [Google Scholar] [CrossRef] [PubMed]
- Gerasimenko, Y.P.; McKinney, Z.; Sayenko, D.G.; Gad, P.; Gorodnichev, R.M.; Grundfest, W.; Edgerton, V.R.; Kozlovskaya, I.B. Spinal and Sensory Neuromodulation of Spinal Neuronal Networks in Humans. Hum Physiol 2017, 43, 492–500. [Google Scholar] [CrossRef]
- Megía-García, Á.; Serrano-Muñoz, D.; Taylor, J.; Avendaño-Coy, J.; Comino-Suárez, N.; Gómez-Soriano, J. Transcutaneous Spinal Cord Stimulation Enhances Quadriceps Motor Evoked Potential in Healthy Participants: A Double-Blind Randomized Controlled Study. Journal of Clinical Medicine 2020, 9, 3275. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Lucas, K.; Keller, A.; Martin, R.; Behrman, A.; Vissarionov, S.; Gerasimenko, Y. Transcutaneous Spinal Stimulation From Adults to Children: A Review | Topics in Spinal Cord Injury Rehabilitation. [CrossRef]
- Moshonkina, T.R.; Zharova, E.N.; Ananev, S.S.; Shandybina, N.D.; Vershinina, E.A.; Lyakhovetskii, V.A.; Grishin, A.A.; Shlyakhto, E.V.; Gerasimenko, Y.P. A New Technology for Recovery of Locomotion in Patients after a Stroke | Doklady Biochemistry and Biophysics. Available online: https://link.springer.com/article/10.1134/S1607672922340087 (accessed on 3 February 2024).
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, G. Development and Reliability of a System to Classify Gross Motor Function in Children with Cerebral Palsy - Palisano - 1997 - Developmental Medicine & Child Neurology - Wiley Online Library. Available online: https://doi.org/10.1111/j.1469-8749.1997.tb07414.x (accessed on 3 February 2024).
- Solopova, I.A.; Sukhotina, I.A.; Zhvansky, D.S.; Ikoeva, G.A.; Vissarionov, S.V.; Baindurashvili, A.G.; Edgerton, V.R.; Gerasimenko, Y.P.; Moshonkina, T.R. Effects of Spinal Cord Stimulation on Motor Functions in Children with Cerebral Palsy. Neuroscience Letters 2017, 639, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Gad, P.; Hastings, H.; Zhong, H.; Seth, G.; Kandhari, S.; Edgerton, V.R. Transcutaneous Spinal Neuromodulation Reorganizes Neural Networks in Patients with Cerebral Palsy | SpringerLink. Available online: https://link.springer.com/article/10.1007/s13311-021-01087-6 (accessed on 10 June 2023).
- Kariyawasam, D.; D’Silva, A.; Howells, J.; Herbert, K.; Geelan-Small, P.; Lin, C.S.-Y.; Farrar, M.A. Motor Unit Changes in Children with Symptomatic Spinal Muscular Atrophy Treated with Nusinersen. J Neurol Neurosurg Psychiatry 2021, 92, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Kessler, T.; Sam, G.; Wick, W.; Weiler, M. Evaluation of Risdiplam Efficacy in 5q Spinal Muscular Atrophy: A Systematic Comparison of Electrophysiologic with Clinical Outcome Measures. European Journal of Neurology 2024, 31, e16099. [Google Scholar] [CrossRef]
- Bovend’Eerdt, T.J.; Botell, R.E.; Wade, D.T. Writing SMART Rehabilitation Goals and Achieving Goal Attainment Scaling: A Practical Guide. Clin Rehabil 2009, 23, 352–361. [Google Scholar] [CrossRef]
- Solopova, I.A.; Selionov, V.A.; Zhvansky, D.S.; Gurfinkel, V.S.; Ivanenko, Y.P. Human Cervical Spinal Cord Circuitry Activated by Tonic Input Can Generate Rhythmic Arm Movements. Available online: https://journals.physiology.org/doi/epdf/10.1152/jn.00897.2015 (accessed on 22 March 2024).
- Baindurashvili, A.; Vissarionov, S.; Belianchikov, S.; Kartavenko, K.; Solokhina, I.; Kozyrev, A.; Pukhov, A.; Moshonkina, T.; Gerasimenko, Y. Comprehensive Treatment of a Patient with Complicated Thoracic Spine Injury Using Percutaneous Electrical Spinal Cord Stimulation (Case Report). Genij Ortopedii 2020, 26, 79–88. [Google Scholar] [CrossRef]
- Huang, R.; Nikooyan, A.A.; Moore, L.D.; Zdunowski, S.; Morikawa, E.; Sierro, T.; Sayenko, D.; Gad, P.; Homsey, T.; Le, T. Minimal Handgrip Force Is Needed for Transcutaneous Electrical Stimulation to Improve Hand Functions of Patients with Severe Spinal Cord Injury. Scientific Reports 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Megía García, A.; Serrano-Muñoz, D.; Taylor, J.; Avendaño-Coy, J.; Gómez-Soriano, J. Transcutaneous Spinal Cord Stimulation and Motor Rehabilitation in Spinal Cord Injury: A Systematic Review. Neurorehabil Neural Repair 2020, 34, 3–12. [Google Scholar] [CrossRef]
- Zhang, F.; Momeni, K.; Ramanujam, A.; Ravi, M.; Carnahan, J.; Kirshblum, S.; Forrest, G.F. Cervical Spinal Cord Transcutaneous Stimulation Improves Upper Extremity and Hand Function in People With Complete Tetraplegia: A Case Study. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2020, 28, 3167–3174. [Google Scholar] [CrossRef]
- Iannaccone, S.T. Outcome Measures for Pediatric Spinal Muscular Atrophy. Arch Neurol 2002, 59, 1445. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.W.; Pepler, L.; Maturi, B.; Afonso, A.C.F.; Sarmiento, J.; Haldenby, R. Systematic Review of Motor Function Scales and Patient-Reported Outcomes in Spinal Muscular Atrophy. Am J Phys Med Rehabil 2022, 101, 590–608. [Google Scholar] [CrossRef] [PubMed]
- Salazar, R.; Montes, J.; Dunaway Young, S.; McDermott, M.P.; Martens, W.; Pasternak, A.; Quigley, J.; Mirek, E.; Glanzman, A.M.; Civitello, M.; et al. Quantitative Evaluation of Lower Extremity Joint Contractures in Spinal Muscular Atrophy: Implications for Motor Function. Pediatric Physical Therapy 2018, 30, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, E.S.; Mayhew, A.; Montes, J.; Ramsey, D.; Fanelli, L.; Young, S.D.; Salazar, R.; De Sanctis, R.; Pasternak, A.; Glanzman, A.; et al. Revised Upper Limb Module for Spinal Muscular Atrophy: Development of a New Module. Muscle Nerve 2017, 55, 869–874. [Google Scholar] [CrossRef]
- O’Hagen, J.M.; Glanzman, A.M.; McDermott, M.P.; Ryan, P.A.; Flickinger, J.; Quigley, J.; Riley, S.; Sanborn, E.; Irvine, C.; Martens, W.B.; et al. An Expanded Version of the Hammersmith Functional Motor Scale for SMA II and III Patients. Neuromuscular Disorders 2007, 17, 693–697. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Norkin, C.C.; White D., J. Measurement of Joint Motion: A Guide to Goniometry, Third edition; F.A. Davis Company: Philadelphia, 2004; ISBN 978-0-8036-4566-0. [Google Scholar]
- Iannaccone, S.T.; Hynan, L.S.; Morton, A.; Buchanan, R.; Limbers, C.A.; Varni, J.W. The PedsQLTM in Pediatric Patients with Spinal Muscular Atrophy: Feasibility, Reliability, and Validity of the Pediatric Quality of Life InventoryTM Generic Core Scales and Neuromuscular Module. Neuromuscular Disorders 2009, 19, 805–812. [Google Scholar] [CrossRef]
- Vázquez-Costa, J.F.; Povedano, M.; Nascimiento-Osorio, A.E.; Moreno Escribano, A.; Kapetanovic Garcia, S.; Dominguez, R.; Exposito, J.M.; González, L.; Marco, C.; Medina Castillo, J.; et al. Nusinersen in Adult Patients with 5q Spinal Muscular Atrophy: A Multicenter Observational Cohorts’ Study. European Journal of Neurology 2022, 29, 3337–3346. [Google Scholar] [CrossRef] [PubMed]
- Wijngaarde, C.A.; Veldhoen, E.S.; van Eijk, R.P.A.; Stam, M.; Otto, L.A.M.; Asselman, F.-L.; Wösten-van Asperen, R.M.; Hulzebos, E.H.J.; Verweij-van den Oudenrijn, L.P.; Bartels, B.; et al. Natural History of Lung Function in Spinal Muscular Atrophy. Orphanet J Rare Dis 2020, 15, 88. [Google Scholar] [CrossRef] [PubMed]
- Samaha, F.J.; Buncher, C.R.; Russman, B.S.; White, M.L.; Iannaccone, S.T.; Barker, L.; Burhans, K.; Smith, C.; Perkins, B.; Zimmerman, L. Pulmonary Function in Spinal Muscular Atrophy. J Child Neurol 1994, 9, 326–329. [Google Scholar] [CrossRef] [PubMed]
- Montes, J.; Garber, C.E.; Kramer, S.S.; Montgomery, M.J.; Dunaway, S.; Kamil-Rosenberg, S.; Carr, B.; Cruz, R.; Strauss, N.E.; Sproule, D.; et al. Single-Blind, Randomized, Controlled Clinical Trial of Exercise in Ambulatory Spinal Muscular Atrophy: Why Are the Results Negative? JND 2015, 2, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Beaton, D.; Shea, B.; Boers, M.; Simon, L.; Strand, V.; Brooks, P.; Tugwell, P. Minimal Clinically Important Differences: Review of Methods. The Journal of Rheumatology 2001. [Google Scholar]
- Stolte, B.; Bois, J.-M.; Bolz, S.; Kizina, K.; Totzeck, A.; Schlag, M.; Kleinschnitz, C.; Hagenacker, T. Minimal Clinically Important Differences in Functional Motor Scores in Adults with Spinal Muscular Atrophy. Euro J of Neurology 2020, 27, 2586–2594. [Google Scholar] [CrossRef] [PubMed]
- Pera, M.C.; Coratti, G.; Forcina, N.; Mazzone, E.S.; Scoto, M.; Montes, J.; Pasternak, A.; Mayhew, A.; Messina, S.; Sframeli, M.; et al. Content Validity and Clinical Meaningfulness of the HFMSE in Spinal Muscular Atrophy. BMC Neurology 2017, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Pera, M.C.; Coratti, G.; Mazzone, E.S.; Montes, J.; Scoto, M.; De Sanctis, R.; Main, M.; Mayhew, A.; Muni Lofra, R.; Dunaway Young, S.; et al. Revised Upper Limb Module for Spinal Muscular Atrophy: 12 Month Changes. Muscle & Nerve 2019, 59, 426–430. [Google Scholar] [CrossRef]
- Finkel, R.S.; Mercuri, E.; Meyer, O.H.; Simonds, A.K.; Schroth, M.K.; Graham, R.J.; Kirschner, J.; Iannaccone, S.T.; Crawford, T.O.; Woods, S.; et al. Diagnosis and Management of Spinal Muscular Atrophy: Part 2: Pulmonary and Acute Care; Medications, Supplements and Immunizations; Other Organ Systems; and Ethics. Neuromuscular Disorders 2018, 28, 197–207. [Google Scholar] [CrossRef]
- Chabanon, A.; Seferian, A.M.; Daron, A.; Péréon, Y.; Cances, C.; Vuillerot, C.; De Waele, L.; Cuisset, J.-M.; Laugel, V.; Schara, U.; et al. Prospective and Longitudinal Natural History Study of Patients with Type 2 and 3 Spinal Muscular Atrophy: Baseline Data NatHis-SMA Study. PLoS ONE 2018, 13, e0201004. [Google Scholar] [CrossRef]
- Elsheikh, B.; Severyn, S.; Zhao, S.; Kline, D.; Linsenmayer, M.; Kelly, K.; Tellez, M.; Bartlett, A.; Heintzman, S.; Reynolds, J.; et al. Safety, Tolerability, and Effect of Nusinersen in Non-Ambulatory Adults With Spinal Muscular Atrophy. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Landfeldt, E.; Abner, S.; Pechmann, A.; Sejersen, T.; McMillan, H.J.; Lochmüller, H.; Kirschner, J. Caregiver Burden of Spinal Muscular Atrophy: A Systematic Review. PharmacoEconomics 2023, 41, 275–293. [Google Scholar] [CrossRef] [PubMed]
- Chiriboga, C.A. Pharmacotherapy for Spinal Muscular Atrophy in Babies and Children: A Review of Approved and Experimental Therapies. Pediatr Drugs 2022, 24, 585–602. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pre-treatment demographic and clinical data of the SMA participants. SMA2 and SMA3 – SMA type 2 and 3 participants, respectively. (a) Age; (b) Upper limb function by the Revised Upper Limb Module scale (RULM); (c) Physical abilities by the Hammersmith Function Motor Scale Expanded (HFMSE); (d) Pulmonary function by the Forced Vital Capacity (FVC); (e) Knee range of motion (ROM), left and right leg results combined. *, ** and *** - p<0.05, p<0.01 and p<0.001, respectively, by Mann-Whitney test. # - p<0.05 by Student t-test.
Figure 1.
Pre-treatment demographic and clinical data of the SMA participants. SMA2 and SMA3 – SMA type 2 and 3 participants, respectively. (a) Age; (b) Upper limb function by the Revised Upper Limb Module scale (RULM); (c) Physical abilities by the Hammersmith Function Motor Scale Expanded (HFMSE); (d) Pulmonary function by the Forced Vital Capacity (FVC); (e) Knee range of motion (ROM), left and right leg results combined. *, ** and *** - p<0.05, p<0.01 and p<0.001, respectively, by Mann-Whitney test. # - p<0.05 by Student t-test.
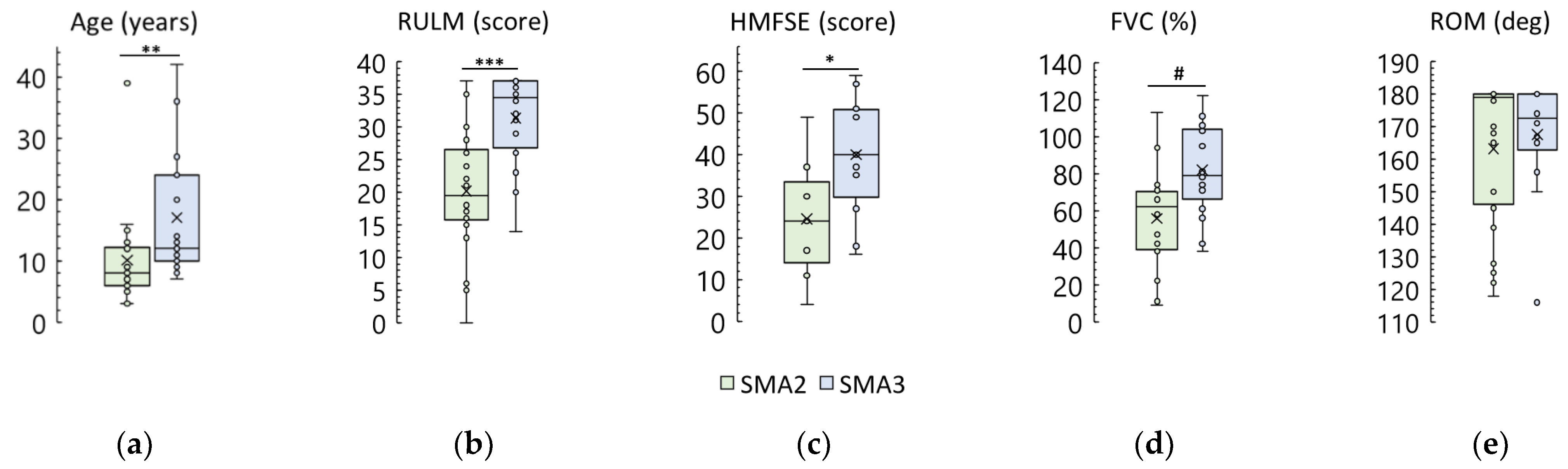
Figure 2.
Change in the Revised Upper Limb Module scale (RULM) score after tSCS course in SMA type 2 and 3 participants ((a) and (b), respectively). Dotted lines – adult patients. One SMA type 2 participant and seven SMA type 3 participants showed a maximum score of 37 before and after tSCS sessions. Their results are not shown because the score does not change after the sessions. (c) – Difference in RULM score after the sessions in SMA type 2 and type 3 groups. ** - p<0.01 by Wilcoxon test.
Figure 2.
Change in the Revised Upper Limb Module scale (RULM) score after tSCS course in SMA type 2 and 3 participants ((a) and (b), respectively). Dotted lines – adult patients. One SMA type 2 participant and seven SMA type 3 participants showed a maximum score of 37 before and after tSCS sessions. Their results are not shown because the score does not change after the sessions. (c) – Difference in RULM score after the sessions in SMA type 2 and type 3 groups. ** - p<0.01 by Wilcoxon test.
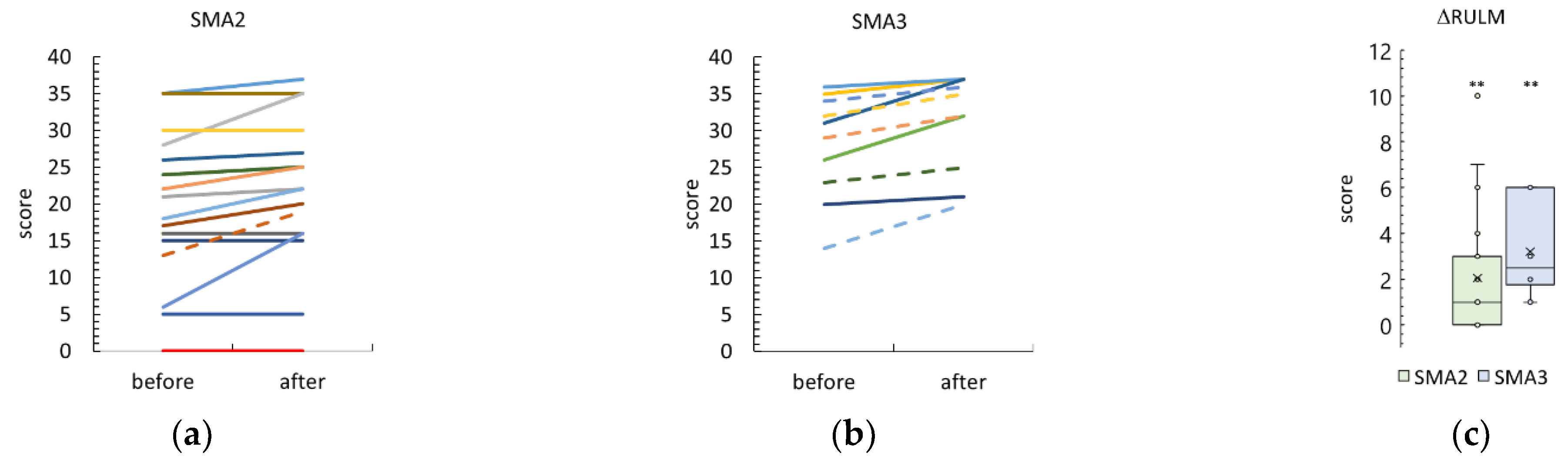
Figure 3.
Change in the Hammersmith Function Motor Scale Expanded (HFMSE) score after tSCS course in SMA type 2 and 3 participants ((a) and (b), respectively). Dotted lines – adult patients. (c) – Difference in the HFMSE score after the sessions in SMA type 2 and type 3 groups. *** - p<0.001 by Wilcoxon test.
Figure 3.
Change in the Hammersmith Function Motor Scale Expanded (HFMSE) score after tSCS course in SMA type 2 and 3 participants ((a) and (b), respectively). Dotted lines – adult patients. (c) – Difference in the HFMSE score after the sessions in SMA type 2 and type 3 groups. *** - p<0.001 by Wilcoxon test.
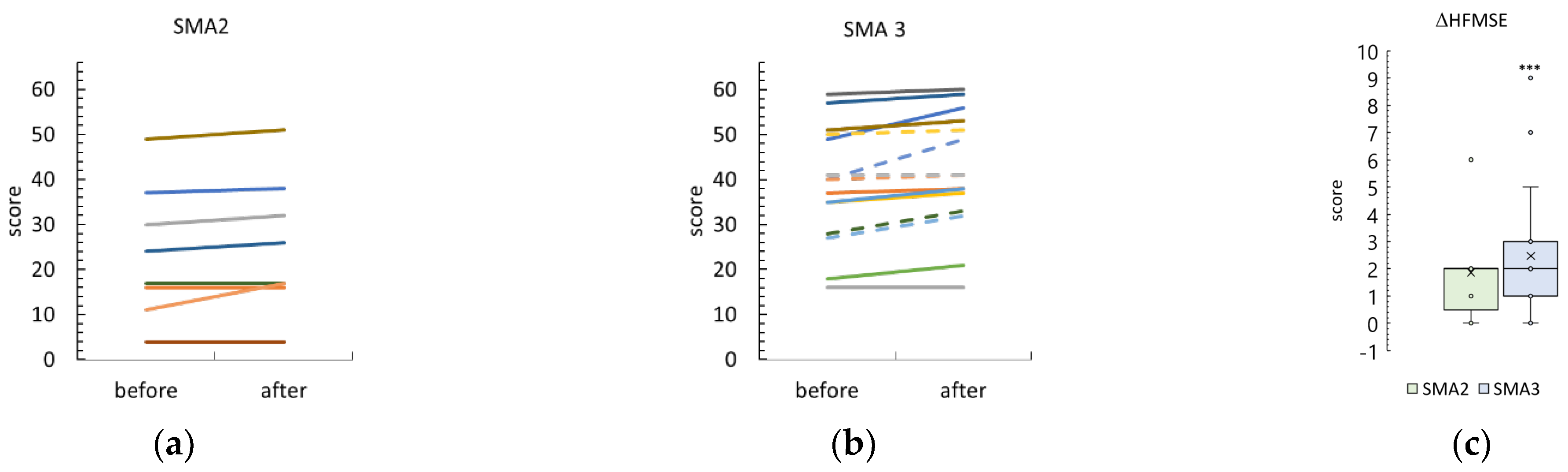
Figure 4.
Change in pulmonary function (Forced Vital Capacity, FVC) after tSCS course in SMA type 2 and 3 participants ((a) and (b), respectively). Dotted lines – adult patients. (c) – Difference of the FVC after the sessions in SMA type 2 and type 3 groups. ** - p<0.01 by Wilcoxon test.
Figure 4.
Change in pulmonary function (Forced Vital Capacity, FVC) after tSCS course in SMA type 2 and 3 participants ((a) and (b), respectively). Dotted lines – adult patients. (c) – Difference of the FVC after the sessions in SMA type 2 and type 3 groups. ** - p<0.01 by Wilcoxon test.
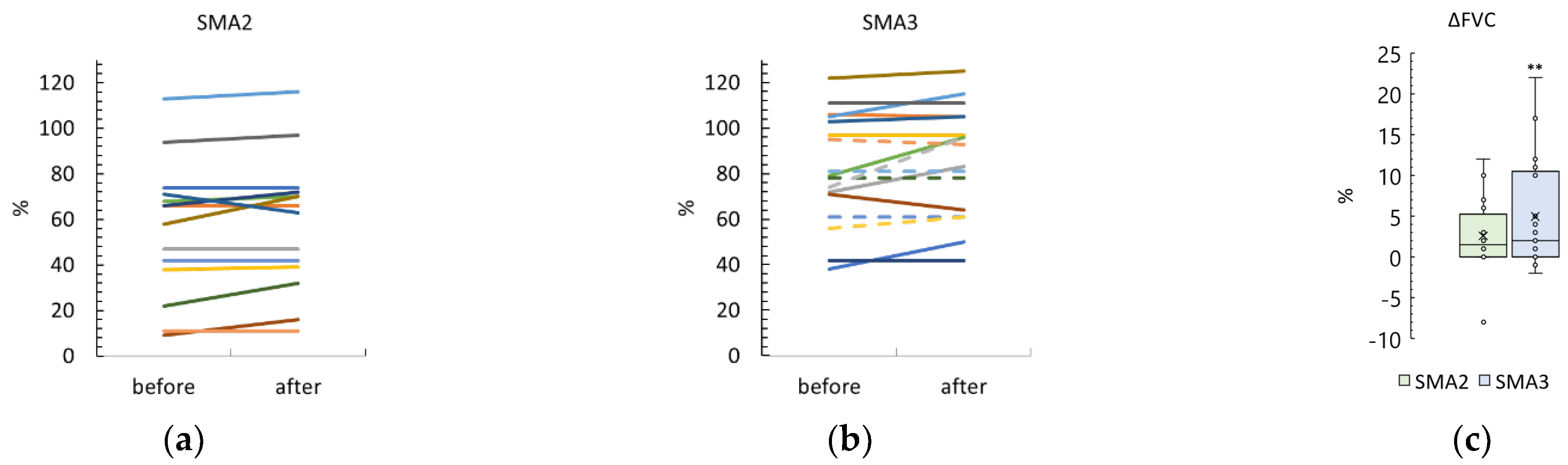
Figure 5.
Change in the knee Range of Motion (ROM) after tSCS treatment in SMA type 2 and 3 participants ((a) and (b), respectively) with pretreatment knee contractures. Right and left knee ROM results are combined. Dotted lines – adult patients. (c) – Difference in ROM after the course in SMA type 2 and type 3 groups. *** and ** - p<0.0001 and p<0.01 by Wilcoxon test, respectively.
Figure 5.
Change in the knee Range of Motion (ROM) after tSCS treatment in SMA type 2 and 3 participants ((a) and (b), respectively) with pretreatment knee contractures. Right and left knee ROM results are combined. Dotted lines – adult patients. (c) – Difference in ROM after the course in SMA type 2 and type 3 groups. *** and ** - p<0.0001 and p<0.01 by Wilcoxon test, respectively.
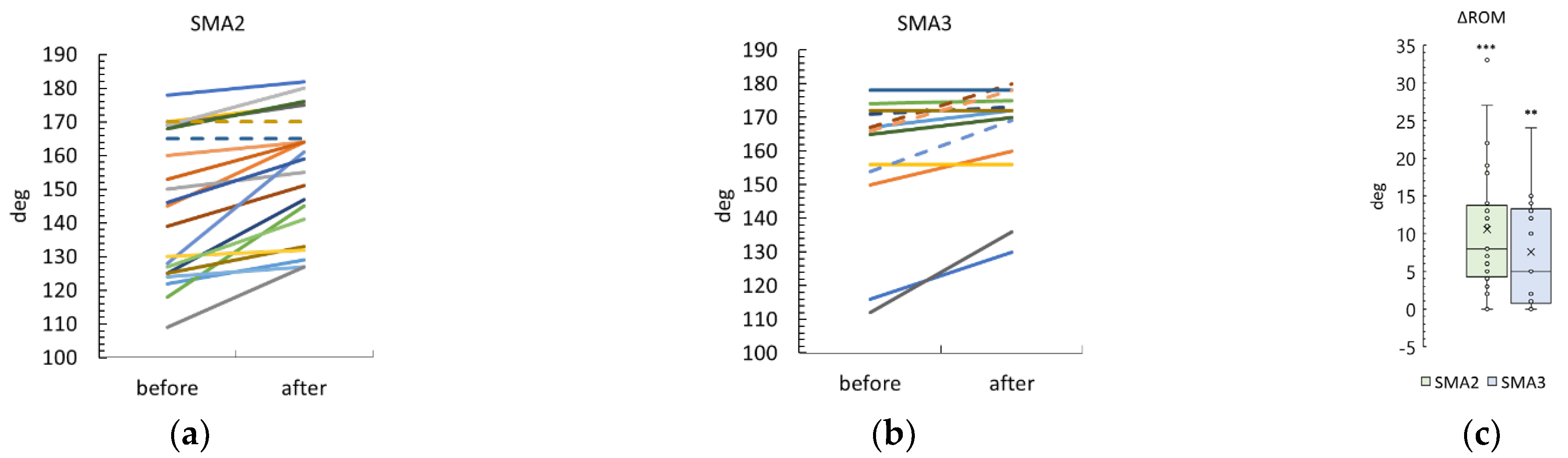
Figure 6.
Comparison of the differences in outcomes between adults and children in the SMA type 3 group. (a) Revised Upper Limb Module scale (RULM); (b) Hammersmith Function Motor Scale Expanded (HFMSE); (c) Forced Vital Capacity (FVC); (d) Knee range of motion (ROM), combined left and right leg results.
Figure 6.
Comparison of the differences in outcomes between adults and children in the SMA type 3 group. (a) Revised Upper Limb Module scale (RULM); (b) Hammersmith Function Motor Scale Expanded (HFMSE); (c) Forced Vital Capacity (FVC); (d) Knee range of motion (ROM), combined left and right leg results.
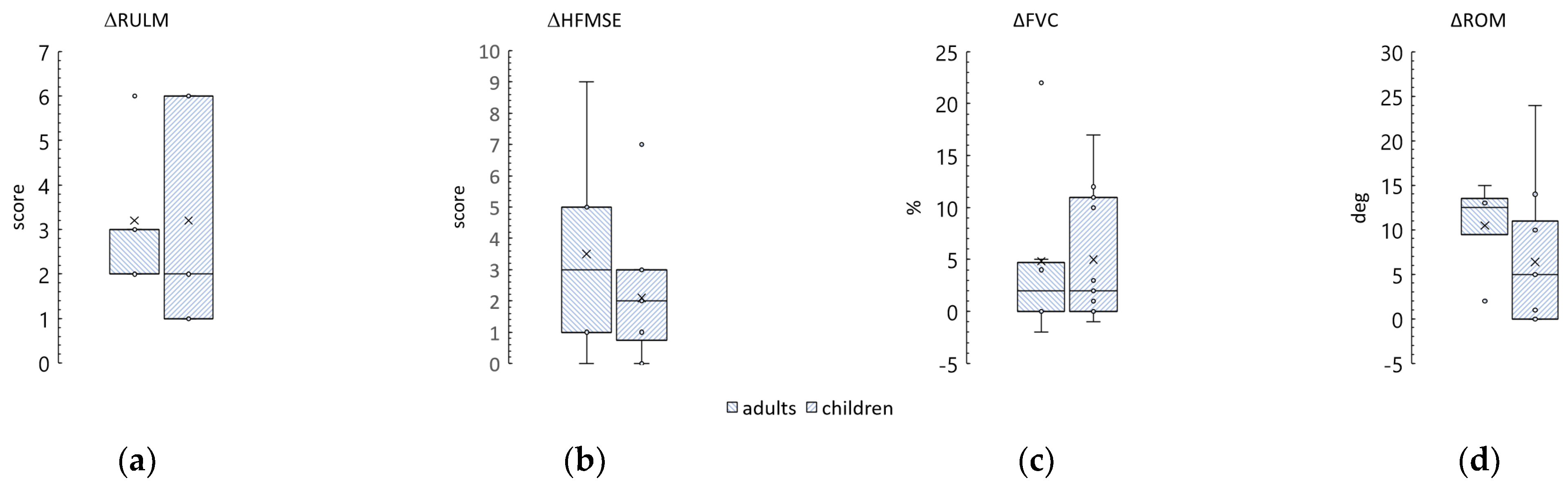

Table 1.
Demographic and clinical parameters of the studied SMA groups
| Group | N | Sex (m/f) |
Age (years) |
Orphan drug (n) | ||
|---|---|---|---|---|---|---|
| Nusinersen | Risdiplam | OA | ||||
| SMA2 | 20 | 11/9 | 8 [6; 13]1 | 13 | 6 | 1 |
| SMA3 | 17 | 10/7 | 12 [10; 24] | 17 | - | - |
1 median [first quartile, Q1; third quartile, Q3]; m – males; f – females; OA – onasemnogene abeparvovec
Table 2.
Clinical parameters of the studied SMA groups
| Group | Funct. status (n) | RULM | HFMSE | FVC | ||
|---|---|---|---|---|---|---|
| N-S | S | W | (score) | (%) | ||
| SMA2 | 12 | 8 | - | 20 ± 101 (20)2 | 24 [11; 37]3 (7) | 56 ± 30 (14) |
| SMA3 | 1 | 14 | 2 | 35 [28; 37] (17) | 40 ± 13 (16) | 82 ± 24 (17) |
1 mean ± standard deviation; 2 (n, number of the tested participants); 3 median [first quartile, Q1; third quartile, Q3].
Table 3.
Spearman's correlation coefficient (r), p-value, and number of pairs (n) for age and tSCS outcome differences
Table 3.
Spearman's correlation coefficient (r), p-value, and number of pairs (n) for age and tSCS outcome differences
| Group | ΔRULM | ΔHFMSE | ΔFVC | ||||||
|---|---|---|---|---|---|---|---|---|---|
| r | p | n | r | p | n | r | p | n | |
| SMA2 | 0.26 | 0.27 | 9 | 0.32 | 0.48 | 7 | 0.11 | 0.71 | 14 |
| SMA3 | 0.49 | 0.16 | 10 | 0.09 | 0.75 | 16 | -0.09 | 0.74 | 17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



