
Submitted:
16 April 2024
Posted:
17 April 2024
You are already at the latest version
Abstract
This interdisciplinary investigation of the human remains of Balduin Helm, one of the most important abbots of Fürstenfeld monastery, provides novel information on that historic individual. This is particularly interesting since Balduin, during early 18th century, was involved in the renovation of this large Bavarian monastery. Metastatic prostate cancer was found as evidenced by multiple mixed osteolytic-osteoblastic bone lesions in all available vertebral bodies, fragments of both hemipelvises and isolated metastases in skull bones. Distribution, radio- and histomorphology, and especially the immunohistochemical detection of prostate-specific antigen in those metastases, definitively confirm this diagnosis. Further investigation, especially by stable isotope analysis, showed a balanced high-level diet with considerable contribution from animal protein and significant freshwater fish. These additional findings suggest a significant radiocarbon reservoir effect as an explanation for a “too old” radiocarbon dating. Finally, the obviously high-level protein diet may have contributed to the tumorigenesis which caused the death of the abbot at an advanced age.
Keywords:
cancer
; skeleton
; stable isotope
; radiocarbon
; immunohistochemistry
1. Introduction
The interdisciplinary investigation of human remains offers a unique opportunity to identify specific information about the life and disease in historic individuals. These data are of even greater value when the individual is known so that bioarcheological data may be correlated with biographic information. Besides this, the identification of specific diseases, such as in malignant tumours, offers new insight, not only into an individual’s medical history, but also into specialised medical disciplines, such as paleo-oncology.
Oncological diseases are widespread in modern times, but relatively rare in studies of the osseous remains of ancient populations [1,2,3,4]. There are several reasons which include low level of tumour detection in dry bone, incomplete preservation of historic skeletons, lower life expectancy in previous populations than today, and, perhaps, reduced environmental factors for tumorigenesis. While the exact influence of these factors on any real tumour rate remains unknown, every well-documented case of malignant skeletal tumour, both of primary or secondary (metastatic) cause, is of interest [2,3]. This holds particularly true in those cases where an historic individual can be identified. The identification of malignant tumoral growth in an historic person of particular interest, since the diagnosis of a malignancy may be correlated with its potential impact on the life and living conditions in a past setting. To date few such examples of paleopathologically identified malignant tumours in specific persons exist [5,6,7]. This report adds to the literature with particular emphasis on the potential influence of a metastatic cancer on the life of a South German abbot of the early 18th century who played an important role in regional history, and provides some insight into his living conditions before death.
2. Material and Methods
2.1. The Individual´S History
Balduin Helm (1645-1720 CE) was abbot of one of the most eminent monasteries of Southern Bavaria, the monastery of Fürstenfeld located close to the small town of Fürstenfeldbruck, which is about 25km from the Bavarian capital city of Munich. The abbey was founded in 1263 by the Bavarian Duke Ludwig II, who had initially designated the monastery as the burial place for his family, and had gifted the convent with a large land and property holding [8,9,10].
Following serious decay during the Thirty Years War in 1632, the monastery returned to some of its previous economic wealth during the post-war decades such that, by the end of the 17th century, it was decided to rebuild the whole monastery. The church was considerably enlarged and decorated in the in vogue baroque style. This was started under the leadership of Abbot Balduin Helm.
Balduin Helm was born in Munich in 1645 with the Christian names Christoph Ferdinand. He was the son of the Munich court musician Elias Helm and his wife Anna Maria [10]. According to the baptismal register he was the youngest son with two elder brothers and two sisters, one of each becoming a monk and a nun respectively. He was later named Balduin. In 1663 CE, following an extended school education, he entered the monastery at the age of 18 years. This was followed by 3 years of studying theology at the University of Dillingen (Bavaria). In 1669 CE he not only received his final consecration but he also graduated as Doctor of Theology [10].
Following his return to the monastery he served as parochial curate between 1671 and 1690 in the parish of St. Magdalena in Bruck (which is a part of Fürstenfeldbruck) [10]. These services were interrupted by periods of residence in the monastery. While serving in the monastery, he also was engaged in administrative work, mainly as the secretary of the abbot Martin Dallmayr. In 1690 abbot Martin Dallmayr unexpectedly died and the convent unanimously elected Balduin Helm to replace him [9].
During his appointment he was described as being “calm, steady, humble, tolerant and of superior character associated with ample learnedness”. There exists one painting in which Abbot Balduin has been identified with him as a member of an important ceremony (Figure 1). Beyond his work as an abbot, Balduin authored several theological oeuvres which were widely viewed. Additionally, he was frequently invited to perform church services in Munich. Apart from the theological services, he was, by virtue of his ecclesiastical duties, a member of the Bavarian Diet. All these obligations required frequent travelling. A compilation of his travel itinerary shows a list of 75 journeys in 15 years of duty [10].
The most important event during Balduin´s abbacy was the renovation and restructuration of the monastery and particularly the new church. Balduin planned the erection of an up-to-date building of enormous dimensions. The economic conditions favoured his plans since the monastery had considerable revenues from several endowments that were obliged to pay taxes to the monastery [8].
The construction works started soon after Balduin´s election in 1691 and lasted until 1701 when numerous offices and service buildings had been finished. The renovation of the church, however, though already started, remained unfinished at that time. Despite this, the enormous amount of 120.000 florins had been spent (equivalent to about 12 million Euros today). But the political conditions had dramatically changed. The War of the Spanish Succession (1701 – 1714) had begun and the Bavarian Elector Maximilian II. Emmanuel (1662-1726) had been defeated by the Holy Roman Emperor forcing him to flee from his home state Bavaria. Since the Elector had protected the monastery, and, in particular, supported Abbot Balduin, the loss of this support led to the latter’s resignation on the 29th May 1705 [10].
The church was not finished until 1741 (Figure 2 and Figure 3), a date that Abbot Balduin did not live to see [8]. He had died on the 8th May 1720, having spent another 15 years as a titular abbot in Fürstenfeld abbey being mainly devoted to theological studies. During this period Balduin authored five tomes on theological issues [10]. He lived withdrawn from all official duties. No report exists about his physical abilities or any ill health.
Abbot Balduin presumably was buried in the monastery´s cemetery. It is mentioned that his grave was decorated with a large tombstone [10]. However during renovation works in 1847, his skeletal remains were removed from his tomb and transferred into a large clay pot (Figure 4A). This was transported into the monastery´s crypt. In 2019 his skeletal remains were inspected by the authoring team at the request of the local parish (Figure 4B).
2.2. Methods for Analysis of the Skeletal Remains
All material that was contained in the pot was removed and sorted. Besides the human remains the pot contained several distorted and corroded metal objects, most likely to be clasps. Wood particles were identified as remnants of a wooden coffin. The bones were found to comprise major parts of a skeleton including the skull and mandible, most of the long bones, fragments of both hemipelvises, several vertebral bodies, and several small bones of the feet. Surprisingly, there were only three small pieces of mid-shaft ribs. Some of those bones had minor soil residues on the surface which were partly of a reddish colour.
All bones were cleaned, registered and evaluated according to the presence of the skeletal elements (termed “representativity”) and the condition of the bone matrix (“preservation”). For standardisation a previously developed and applied scheme was used. This covers 42 regions of the human skeleton and evaluates the presence of the respective skeletal material (0 – 42 points) and the condition of the bone (0 – max. 126 points) with low figures indicating an absent or very fragmented skeleton and extremely poorly conserved bone matrix respectively [11]. In contrast, high figures indicate the presence of all/most skeletal elements and good/excellent bone preservation respectively. This system has previously been successfully applied to other small skeletal series [12].
Furthermore, the anthropological investigation comprised of a determination of individual age (skull sutures, symphysis and cancellous bone of several long bones) and individual sex (pelvis and skull) [13,14]. Body height was estimated from long bone measurements wherever possible [15]. Physical properties, such as handedness, mobility pattern and development of skeletal musculature were determined from bone measurement ratios and the extent of muscular insertion zones on long bones, as previously described in detail [16,17]. Subsequently, all bones were subjected to a CT-scan (Siemens Somatom, 120V, slice thickness 0.6 cm; [18]).
Finally, some small tissue samples were obtained for radiocarbon testing and stable isotope analysis, as well as selected bone tissue histomorphology analysis. For radiocarbon and stable isotope analysis, the tissue samples were taken from compact bone of the left femur diaphysis. The extraction of collagen and stable isotope analyses of the ratios of carbon, nitrogen, sulfur and hydrogen isotopes followed the usual protocols [19].
The radiocarbon dating was performed on the femoral collagen following established extraction protocols [20]. Thereby 3.2 mg material was analysed by accelerator mass spectrometry (AMS) at the Leibniz-Laboratory for Radiometric Dating and Isotope Research, Kiel University (Germany) (AMS Type HVE 3MV Tandetron 4130) using the calibration data by Reimers et al. [21].
3. Results
3.1. Anthropological Evaluation of the Skeletal Remains
Within the clay pot, an incomplete skeleton was found of an old male individual; several skeletal elements were absent (Figure 5). The estimation of the skeleton´s completeness was 17 points out of 42 possible points (40.5%) and the value for bone structure was 58 out of 72 possible points (80.6%). In summary, roughly half of an adult skeleton was preserved and the bone matrix was fairly well preserved.
Using the typical criteria for sex typing, both the preserved right hemipelvis fragment and the skull strongly suggested a male individual (see Figure 6). The complete closure of skull sutures (Figure 6D) suggested old age of more than 60 years which was confirmed by the flat surface of the symphysis without retained grooves (grade V). Since almost all teeth were lost, this feature is also consistent with advanced age (Figure 6B, C). The spongy bone structure of the long bones was moderately reduced which is also in agreement with old age. In summary, these are the skeletal remains of an elderly male consistent with Balduin Helm’s historical record.
Bone length measurements of the left femur and tibia, as well as the humeri, ulnae and radii indicate a body height of 167 cm +/- 2 cm (mean +/- 1 SD). The determination of several osteometric indices provided evidence for right handedness. The mobility index (index platycnemius) reveals low mobility ratios (stenomeric). The muscular insertion zones in all long bones were not significantly prominent and confirmed low physical activity profiles.
3.2. Paleopathological Analysis
The most prominent finding was the presence of numerous small mixed osteolytic-osteoblastic lesions affecting several bones. This was seen in all available vertebral bodies, the fragments of both hemipelvises and occasionally in the inner table of the skull (Figure 7). Besides the bone defects a tiny network of newly formed bone matrix can be seen. Furthermore a section through a lumbar vertebral body showed central irregular osteolysis with considerable osteoblastic bone reaction at the margins (Figure 7C). The skull showed few and mainly osteolytic defects that were primarily affecting the inner skull bone table (Figure 7D).
Beyond these clearly pathological features, the only minor additional pathology was the lost teeth. On visual inspection, there were no signs of trauma, no evidence for metabolic deficiency (e.g. vitamin deficiency or chronic anaemia) and the available joints did not show any significant wear or tear such as seen in chronic biomechanical overload, e.g. by specific activities such as dominant handed work load.
3.3. CT-scans
The scanning of all available bones confirmed the macroscopic observations. All preserved vertebral bodies and the fragments of both hemipelvises showed widespread mixed osteolytic-osteoblastic bone defects highly suggestive of multiple osseous metastases (Figure 8A, B). Additionally, isolated, mostly osteolytic lesions were seen in the skull, mainly lacking the osteoblastic component (Figure 8C). In addition, the CT scans showed additional metastatic infiltration in the left temporo-mandibular joint which was macroscopically unremarkable (Figure 8D). In contrast, long bones and the few small bones of the feet remain free of abnormal lesions. In general, the mineralisation of the skeleton was fairly well preserved with no signs of significant generalised osteopenia.
In the jaws, the CT scans also confirmed the presence of old-healed tooth loss in the whole maxilla, and several “younger” tooth losses in the central mandible with still partly preserved dental alveoli. Only the tooth of region 47 was present (Figure 9A). In the paranasal sinuses, the scans show almost complete filling by external soil material (Figure 9A). Finally, the distal right radius shows an oblique bone bar in the distal metaphysis (Figure 9C).
3.4. Radiocarbon Determination and Stable Isotope Testing
A sample from the right femur was used for radiocarbon and stable isotope analysis. The calibrated 14C value matched with three time periods (Figure 10) which covered the time frames (95%-probability) of 1508-1593 CE, 1618-1661 CE and 1788-1792 CE. These ranges have to be adjusted for the effect of metabolism in the cortical femoral bone of approximately 29 years [23]. All three ranges do not match with Abbot Balduin’s known date of death (1720) and have to be considered in combination with stable isotope values and the general discussions below.
For the stable isotope values sufficient bone collagen was extracted with a yield 16.5%. The ratio of carbon to nitrogen (C:N-ratio) ranges at 3,14 and indicated excellent collagen quality. The detailed results were:
δ13
C [‰]: -20,0
δ15
N [‰]: 12,5
δ34
S [‰]: 6,6
δ2
H [‰]: -2,3
Accordingly, Abbot Balduin’s diet mainly contained food products based on C3-plants. The nitrogen value indicates a considerable proportion of animal protein, both from terrestrial animals and also freshwater fish. There was no evidence for marine fish consumption. A further evaluation is given below.
3.5. Bone histology and Immunohistochemistry
Bone material was taken from one of the macroscopically and radiologically suspicious mixed osteolytic-osteoblastic lesions of a vertebral body. Following fixation and decalcification histological sections were routinely stained. The resulting pattern shows appositional irregular woven bone trabeculae (Figure 11A) which is consistent with an osteoblastic bone reaction. Subsequent sections were stained immunohistochemically using monospecific antibodies against a surface protein which is highly selective for prostate-specific antigens (PSA). Small residues in the marrow cavities showed positive staining consistent with prostatic origin of the tumour infiltration (Figure 11B).
4. Discussion
This paper describes the interdisciplinary findings in an aged male skeleton of an historic person. Abbot Balduin was a prominent leader of one of the most important monasteries in late 17th to early 18th century Bavaria; accordingly, he can be regarded as an eminent local person. The detection of numerous osseous metastases, mainly in his axial skeleton, and the immunohistochemically verified origin of prostate carcinoma make this case interesting both for the history of early modern era, and for paleo-oncology.
4.1. Authentication of the Skeletal Material
The skeletal material found in the clay pot contained nearly half of the skeleton of an old male. The written information indicated that Abbot Balduin died at the age of 75 years which is in keeping with the skeletal findings. Further information reported that the body of Abbot Balduin obviously had first been buried in a tomb in the monastery´s cemetery [10]. In 1847, his remains were exhumed and transferred into the church´s crypt. Although there is no written report about this transfer, it can be assumed that this happened during a renovation of the church’s crypt providing additional loculi, and the remains of the Abbot were transported there. Furthermore, considerable soil material was found, for instance the paranasal sinuses, with staining of the bone surface from red bricks, as well as small fragments of wood from the coffin. This is consistent with a previous burial in a cemetery with subsequent exhumation of the remains into a pot and transference to the crypt.
The discrepancy in the radiocarbon data suggests that these remains were of a skeleton that predeceased Abbot Balduin´s death by a number of decades. Taking the calibrated 14C-values into account, only the two earlier date ranges can be considered, 1508-1593CE and 1618-1661CE. Even including the fact that bone collagen turnover of 29 years occurs in compact femoral bone in the elderly [23] and using the second time period, the results suggest the skeletal remains date of death is no later than 1691 CE, 29 years earlier than the true one. However, the reason may be the radiocarbon reservoir effect of considerable amounts of dietary protein coming from fish. In the aquatic food chain, “old” carbon from calcareous sediments may be incorporated into the body tissues of the consumer [24,25]. A radiocarbon reservoir effect has been documented in several lakes and its effect is highly variable. It may result in a time lag of around 1,000 years as in Lake Tegernsee (Bavaria) [26]. This means that the consumption of fish from waters in the foothills of the Alps may have a considerable influence on the radiocarbon age and leading to an erroneous older 14C-dating. Considering the fasting rules in Catholic monasteries with, every Friday, long periods of fasting following, for example on feast days, an increase in fish consumption, that could then account for the early date of death for this skeleton. Unfortunately, there is no information on where the Fürstenfeld monastery received their fish supply. Also, as yet, there does not exist radiocarbon reservoir effect data on nearby lakes, such as Lake Ammersee, or other smaller lakes or fish ponds. The sulfur isotope value exclude a major marine fish consumption which might have occurred as with dried fish (stockfish or dried cod).
On balance the probability is that the skeleton is that of Abbot Balduin Helm.
4.2. Metastatic Carcinoma
The most prominent pathological findings were multiple mixed osteolytic-osteoblastic tumoral lesions in the axial parts of the skeleton comprising all of the few available intervertebral bodies and pelvic bone fragments, and a few lesions in the skull, whereas none were found in the available long bones. This distribution pattern suggests metastatic carcinoma [2,3,4,6,7] which was confirmed by the immunohistochemical detection of a prostate-specific antigen in the tumour residues in the lesions. Accordingly, the diagnosis of a metastatic prostate cancer was established. Prostatic carcinoma is the most common malignant tumour in modern elderly males [27]. This diagnosis also clarified Balduin Helm’s cause of death, namely cachexia from disseminated metastatic prostate carcinoma. Assuming a similar clinical course to modern populations in historic ones, and the absence of effective therapies, it can be assumed that the time course for the malignancy was at least several months to many years [27]. The extensive involvement of the vertebra and pelvic bones must have almost certainly led to significant pain symptoms in the later stages, with the final one being a wasting disorder [28]. This would be in line with the loss of several teeth in the front of the mandible that should have occurred not long before Balduin´s death, noting that the reason for loss of many more teeth (all of maxillary and a few of the mandibular teeth) long before his death. The latter would have been independent of his malignancy.
4.3. Further Pathological Findings
Besides the multiple metastases and the tooth loss, this investigation showed only a few additional disorders; most cases of intra vitam tooth loss in historic populations is due to poor dental health e.g. extensive chronic periodontitis or lack of dental hygiene [11], but remains unproven in this case.
There was no evidence for bony trauma either macroscopically or on CT-scanning. The right radius showed an oblique hyperdense bone line, which is an unusual finding and is also called a reinforcement bar. The pathogenesis is uncertain. It is considered to be similar to a Harris growth arrest line although this is typically perpendicular to the bone cortex and associated with illness in children. When found in the elderly, it is usually associated with chronic osteopenia [29,30]. Here the reduction in size and lost trabeculae reveals the bone bar which is presumed to develop due to bone remodelling in response to mechanical stresses (Wolff’s Law [31]).
Finally, we have no evidence for further osteopathology; no sign of significant wear or tear of joint surfaces in keeping with the abbot not have heavy physical duties.
4.4. Balduin´s Diet and Nutrition
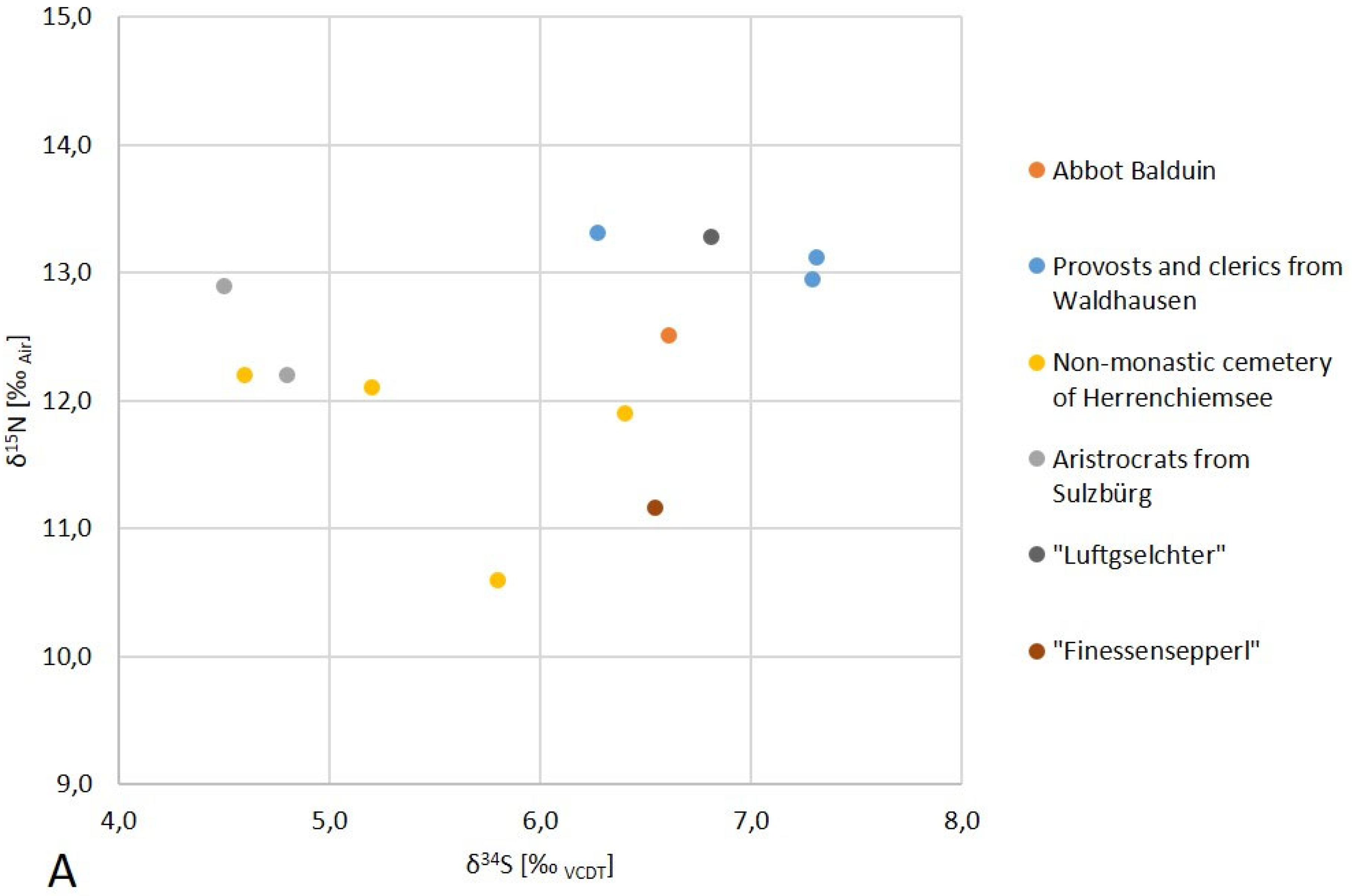
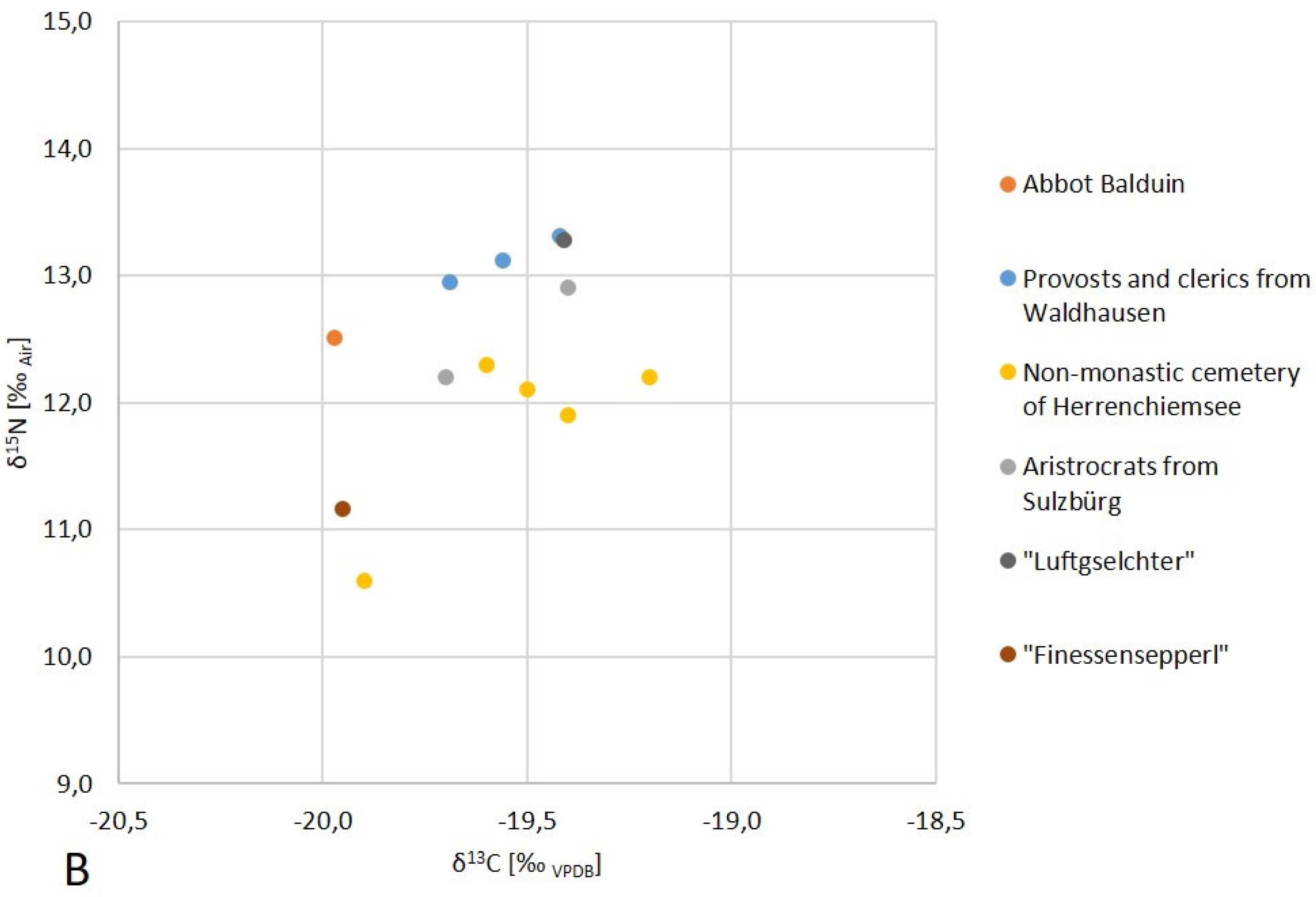
There was good evidence that Abbot Balduin’s diet contained considerable amounts of freshwater fish, presumably from local waters. The isotope data provided further information that showed, in general, he ate well. Although there are no directly comparable data from the Fürstenfeld monastery or a nearby contemporary site, there do exist data on contemporaneous or socially comparable individuals in the literature. Skeletal remains from a non-monastic cemetery of the monastery of Herrenchiemsee (a convent on an island of Lake Chiemsee, Bavaria; [32]), as well as several provosts and clerics of Waldhausen monastery (Upper Austria; including the so-called “Luftgselchter Pfarrer” [33,34], and finally contemporaneous aristocrats from Sulzbürg (the Counts of Wolfstein, [3[[M1] 5]). These show comparable levels of isotope values and thus a very high-quality nutrient supply (see Figure 12). The carbon isotope value also indicates a diet based on C3 plants as is common in Southern Germany and a high content of animal protein.
In summary, it can be assumed that the abbott had a high-quality diet in adequate amounts. Since the stable isotope values are the accumulated results over a long period of time (around 30 years), any final wasting secondary to the malignant cannot be expected to show up in those data.
A high consumption of inland fish could be the cause of the shift between the radiocarbon date for Balduin’s death compared with the known one. The ingestion of "old" carbon from calcareous sediments in lakes and rivers via the aquatic food chain can lead to the body tissues of consumers being estimated to be older than they actually are. This freshwater reservoir effect can be very variable with an inaccuracy of more than 1000 years. A possible radiocarbon reservoir effect may have led to a temporal shift in the radiocarbon age of Balduin by more than 100 years.
4.5. Scenario of the Life of Abbot Balduin
Combining historical information and biomedical data supplements the biography of this individual. The diagnosis of a metastatic prostate carcinoma adds to paleo-oncological knowledge [1,2,3,4]. Therefore Balduin Helm’s life can be summarised as that he was born in a middle-class family of the mid-17th century. Early in his life he decided to enter the monastery of Fürstenfeld, one of the most important in Central Bavaria at that time. There he rapidly advanced by virtue of his ecclesiastical activities to the position of abbot at a time when, not only the scars of the Thirty-Years-War had healed, but monasteries regained economic activity and gained considerable wealth. In this position he initiated the complete rebuilding of the monastery. Political interference by the upcoming War of the Spanish Succession, and the temporary flight of the Bavarian Elector to the Spanish Netherlands, interrupted his career and, in 1705, very abruptly ended his service as an abbot. His final 15 years were spent he living quietly in the monastery.
He was, by virtue of his high social rank by becoming an abbot, very well supplied with food likely to comprise of entrails, meat, fish, and also alcohol. In excess these can be unhealthy. Otherwise, during the first decades of his life, he did not suffer from obvious major disorder, at least that manifested in his skeleton, except for the complete loss of teeth of the maxilla and several teeth of the mandible. This, however, was quite a frequent occurrence in advanced aged individuals at this time and included monastic communities, probably due to poor dental health care and lack of oral hygiene [11]. Beyond this, his most important health problem was the development of prostatic cancer which may have affected him symptomatically in his very final years or even only for his final months of life. This final period must have been difficult for him, despite all possible support in the well-supplied monastery. It can be assumed that he suffered from significant back pain from bone metastases, a frequent complication of spread to the vertebrae and pelvic [29]. In addition he seems to have lost most of his remaining frontal teeth, possibly from periodontitis, which frequently occurs in the wasting-associated complications of untreated or poorly managed cancer patients in the modern era [29].
Finally, this is not only an interesting interdisciplinary biography of a high-ranked 17th century individual, but also a further case of historical metastatic cancer. In this regard, the observation continues previous discussions about the presence and absence of cancer in human history. In this case, the relative longevity of this otherwise very well resourced person may have contributed to his cancer risk. This supports the previous notion that the relatively low numbers of documented cancer cases in history may have mainly been influenced by the short life expectancy [34]. A further interesting aspect of the present case is that the high level of protein rich nourishment may have even increased his individual cancer risk [27], although this requires several more comparable cases to strengthen the argument.
Acknowledgments
We are very grateful to pastor Otto Gäng, Pfarrverband Fürstenfeld, Fürstenfeldbruck, and Dr. Birgitta Klemenz, Fürstenfeldbruck, for the permission to study the skeletal remains of abbot Balduin and their generous and lasting support with this study and finally the permission for image reproduction.
References
- Waldron T (1996) What was the prevalence of malignant disease in the past? Int. J. Osteoarcheol. 6: 463 – 470.
- David AR, Zimmerman MR (2010) Cancer: an old disease, a new disease or something in between? Nature Rev. Cancer 10: 728-733. [CrossRef]
- Hunt KJ, Roberts C, Kirkpatrick C (2018) Taking stock: A systematic review of archaeological evidence of cancers in human and early hominin remains. Int. J. Paleopathol. 21: 12-26. [CrossRef]
- Nerlich AG (2018) Molecular paleopathology and paleo-oncology–State of the art, potentials, limitations and perspectives. Int. J. Paleopathol. 21: 77–82. [CrossRef]
- Marchetti A, Pellegrini S, Bevilacqua G, Fornaciari G. (1996) K-ras mutation in the tumor of Ferrante I of Aragon, King of Naples. Lancet 347: 1272. [CrossRef]
- Schultz M, Parzinger H, Posdnjakov DV, Chikisheva TA, Schmidt-Schultz T (2007) Oldest known case of metastasizing prostate carcinoma diagnosed in the skeleton of a 2,700-year-old Scythian King from Arzhan (Siberia, Russia). Int. J. Cancer 121: 2591 – 2595. [CrossRef]
- Prates C, Sousa S, Oliveira C, Ikram S (2011) Prostate metastatic bone cancer in an Egyptian Ptolemaic mummy, a proposed radiological diagnosis. Int. J. Paleopathol. 1 (2011), 98-103. [CrossRef]
- Bauer H, Bauer E (1993) Klöster in Bayern. 2. Ed. Munich, Beck, pp.107-110.
- Klemenz B (1997) Das Zisterzienserkloster Fürstenfeld zur Zeit von Abt Martin Dallmayr 1640-1690. Weissenhorn, Anton.
- Trinkl S (2015) Das Zisterzienserkloster Fürstenfeld unter Abt Balduin Helm. München.
- Nerlich AG, Riepertinger A, Gillich R, Panzer S (2015) Paleopathology and nutritional analyis of a South German monastery population. BioMed Res. Intl. Article ID 486467, 8 p. [CrossRef]
- Nerlich AG (2022) Ancient Egyptian paleopathology – The population of the tomb of IPI, necropolis of Dahshur-South. Ital. J. Anat. Embryol. 126: 61-79. [CrossRef]
- Buikstra JE, Ubelaker DH (1996) Standards for data collection from human skeletal remains. Proceedings of a seminar at the field museum of natural history. Arkansas Archaeological Survey Research Series 44.
- Rösing FW, Graw M, Marre B, Ritz-Timme S, Rothschild MA, Rötzscher K, Schmeling A, Schröder I, Geserick G (2007) Recommendations for the forensic diagnosis of sex and age from skeletons. Homo 58: 75-89. [CrossRef]
- Breitinger E (1938) Zur Berechnung der Körperhöhe aus den langen Gliedmaßenknochen. Anthropol. Anz. 14: 249-274.
- Nerlich AG, Zink A, Rohrbach H (2002) Paläopathologie altägyptischer Mumien und Skelette. Untersuchungen über Auftreten und Häufigkeit spezifischer Erkrankungen in verschiedenen Zeitperioden der Nekropole von Theben-West. Pathologe 23: 379-385.
- Nerlich A, Zink A, Hagedorn HG, Szeimies U, Weyss C (2000) Anthropological and palaeopathological analysis of the human remains from three „Tombs of the Nobles“ of the necropolis of Thebes-west, upper Egypt. Anthropol. Anz. 58: 321-343.
- Panzer S, Ketterl S, Bicker R, Schoske S, Nerlich AG (2019) How to CT scan human mummies: Theoretical considerations and examples of use. Int. J. Paleopathol. 26: 122-134. [CrossRef]
- Lehn C, Rossmann A, Mayr C (2020) Stable isotope relationships between apatite phosphate (δ18O), structural carbonate (δ18O, δ13C), and collagen (δ2H, δ13C, δ15N, δ34S) in modern human dentine. Rapid Comm. Mass Spect. 34: e8674. [CrossRef]
- Longin R (1971) New method of collagen extraction for radiocarbon dating. Nature 230: 241–242. [CrossRef]
- Reimer PJ, Bard E, Bayliss A, Beck JW, Blackwell PG, Ramsey CB, Buck CE, Cheng H, Edwards RL, Friedrich M, Grootes PM, Guilderson TP, Haflidason H, Hajdas I, Hatté C, Heaton TJ, Hoffmann DL, Hogg AG, Hughen KA, Kaiser KF, Kromer B, Manning SW, Niu M, Reimer RW, Richards DA, Scott EM, Southon JR, Staff RA, Turney CSM, van der Plicht J (2013) IntCal13 and Marine13 Radiocarbon Age Calibration Curves 0–50,000 Years cal BP. Radiocarbon 55, 1869–1887. [CrossRef]
- Nerlich AG, Parsche F, Kirsch T, Wiest I, von der Mark K (1993) Immunohistochemical detection of interstitial collagens in bone and cartilage tissue remnants in an infant Peruvian mummy. Am. J. Phys. Anthropol. 91:279-285. [CrossRef]
- Quinn RL (2024). Bomb pulse 14C evidence for consistent remodeling rates of cortical femur collagen in middle-late adulthood. Am. J. Biol. Anthropol. 183:e24887. [CrossRef]
- Siani G, Paterne M, Arnold M, Bard E, Metivier B, Tisnerat N, Bassinot F (2000) Radiocarbon reservoir ages in the Mediterranean Sea and Black Sea. Radiocarbon 42, 271–280. [CrossRef]
- Fernandes R, Rinne C, Nadeau MJ, Grootes P (2016) Towards the use of radiocarbon as a dietary proxy: establishing a first wide-ranging radiocarbon reservoir effects baseline for Germany. Environ Archaeol 21: 285 – 294. [CrossRef]
- Lehn C, Graw M (2017) Haare, Zähne und Knochen – Über Isotopenanalysen zu Lebensdaten. In: Rosendahl W, Madea B (Eds.) Tatorte der Vergangenheit. Darmstadt: Theiss Verl. pp. 85-91.
- Rawla P (2019) Epidemiology of prostate cancer. World J. Cancer 10: 63-89. [CrossRef]
- Espinosa-Marrón A, Rubio-Blancas A, Quiñones-Capistran CA, Camacho-Zamora A, Salcedo-Grajales I, Bravo-García AP, Bourlon MT, Castillejos-Molina RA, Dias JA, Milke-García MP (2022) Muscle wasting assessment tools for prostate cancer. Sci Rep. 12: 4662. [CrossRef]
- Kursunoglu S, Pate D, Resnick D, Haghighi P, Tyson R, Pitt M (1986) Bone reinforcement lines in chronic adult osteopenia: a hypothesis. Radiology 158: 409-415. [CrossRef]
- Pitt MJ, Morgan SL, Lopez-Ben R, Steelman RE, Nunnally N, Burroughs L, Fineberg N (2011) Association of the presence of bone bars on radiographs and low bone mineral density. Skeletal Radiol 40:905-11. [CrossRef]
- Rowe P, Koller A, Sharma S (2023) Physiology, Bone remodelling. StatPearls [Internet]. www.ncbi.nlm.nih.gov/books/NBK499863 [Accessed 29/Feb/2024].
- Lehn C (2022) Stabilisotopenanalysen – Ermittlung der Ernährungsweisen und Lebensumstände auf der Herreninsel im Chiemsee vom Frühmittelalter bis zur Barockzeit (7. bis 18. Jahrhundert). In: H. Dannheimer (Ed.), Kloster und Stift Herrenchiemsee – Archäologie und Geschichte (um 620–1803). Vol. 148 (New Series). München: Bay. Akademie Wiss. pp. 251-278.
- Lehn C, Nerlich A (2019) Braten oder Brei? – Feststellung der Ernährungsweise durch Stabilisotopenanalyse. In: Nerlich A, Peschel O, Wimmer J (Eds.) Berührt von der Majestät des Todes. Die Mumie in der Kirchengruft von St. Thomas am Blasenstein. Wagner Linz, pp. 70-78.
- Wimmer J, Nerlich A, Peschel O (2022) Dieser Zeitlichkeit entrissen. Die Mumien in der Gruft der ehemaligen Stiftskirche Waldhausen. Wagner Linz, pp. 65-87.
- Lösch S, Bunzel M, Lehn C, Struck U, Peschel O, Graw M (2011). Die Wolfstein Mumien (16.-18. Jhdt). Untersuchungen an mumifizierten Körpern einer Gruft in Süddeutschland. In: Sörries R, Füldner K, Rosendahl W (Eds.) Geschichte und Tradition der Mumifizierung in Europa. Kassler Studien zur Sepulkralkultur Bd. 18, AG Friedhof Denkmal, Kassel, 2011, pp. 113-120.
- Stelter R, de la Croix D, Myrskylä M (2021) Leaders and Laggards in Life Expectancy Among European Scholars from the Sixteenth to the Early Twentieth Century. Demography 58: 111–135. [CrossRef]
Figure 1.
Part of the so-called “Hagnau portrait”: This shows a consecration scene of 1701 at which Abbot Balduin took part. Due to available evidence, Balduin was definitely identified as the person on the right (circle) (Kath. Kirchenstiftung St. Magdalena Fürstenfeldbruck, with permission).
Figure 1.
Part of the so-called “Hagnau portrait”: This shows a consecration scene of 1701 at which Abbot Balduin took part. Due to available evidence, Balduin was definitely identified as the person on the right (circle) (Kath. Kirchenstiftung St. Magdalena Fürstenfeldbruck, with permission).

Figure 2.
Fürstenfeld monastery in 1701. This lithography by Michael Wenig shows a sketch of the planned new church; the surrounding service and office buildings had already been erected under Balduin Helm´s leadership (Bay. Vermessungsamt, München, with permission).
Figure 2.
Fürstenfeld monastery in 1701. This lithography by Michael Wenig shows a sketch of the planned new church; the surrounding service and office buildings had already been erected under Balduin Helm´s leadership (Bay. Vermessungsamt, München, with permission).

Figure 3.
Fürstenfeld monastery in 1748 (Kath. Kirchenstiftung St. Magdalena Fürstenfeldbruck, with permission)).
Figure 3.
Fürstenfeld monastery in 1748 (Kath. Kirchenstiftung St. Magdalena Fürstenfeldbruck, with permission)).

Figure 4.
The clay pot containing the skeletal remains of Abbot Balduin Helm: A) left: external appearance; B) right: view into the content of the pot (images: A. Nerlich).
Figure 4.
The clay pot containing the skeletal remains of Abbot Balduin Helm: A) left: external appearance; B) right: view into the content of the pot (images: A. Nerlich).

Figure 5.
The skeleton of Balduin Helm following opening of the clay pot (image: A. Nerlich).

Figure 6.
The skull of Balduin Helm. A) Frontal view of the skull showing complete loss of all maxillary teeth. B) View at the skull base showing some post-mortem defects and some minor soil residues. C) View at the mandibula with only one retained tooth. Numerous frontal teeth must have gone lost intra-vitam since the dental alveoli are already closed. D) View at the skull surface: all sutures are closed (images: A. Nerlich).
Figure 6.
The skull of Balduin Helm. A) Frontal view of the skull showing complete loss of all maxillary teeth. B) View at the skull base showing some post-mortem defects and some minor soil residues. C) View at the mandibula with only one retained tooth. Numerous frontal teeth must have gone lost intra-vitam since the dental alveoli are already closed. D) View at the skull surface: all sutures are closed (images: A. Nerlich).

Figure 7.
Bone defects in skeletal elements: A) Fragment of a thoracic vertebral body with significant osteolytic defects with minor osteoblastic reaction. B) Fragment of a lumbar vertebral body with mainly osteoplastic reaction. C) Cut surface through the vertebral body of B showing central osteolysis with peripheral major new bone formation (arrows). D) Osteolytic defect in the inner table of the skull (arrows) (images: A. Nerlich).
Figure 7.
Bone defects in skeletal elements: A) Fragment of a thoracic vertebral body with significant osteolytic defects with minor osteoblastic reaction. B) Fragment of a lumbar vertebral body with mainly osteoplastic reaction. C) Cut surface through the vertebral body of B showing central osteolysis with peripheral major new bone formation (arrows). D) Osteolytic defect in the inner table of the skull (arrows) (images: A. Nerlich).
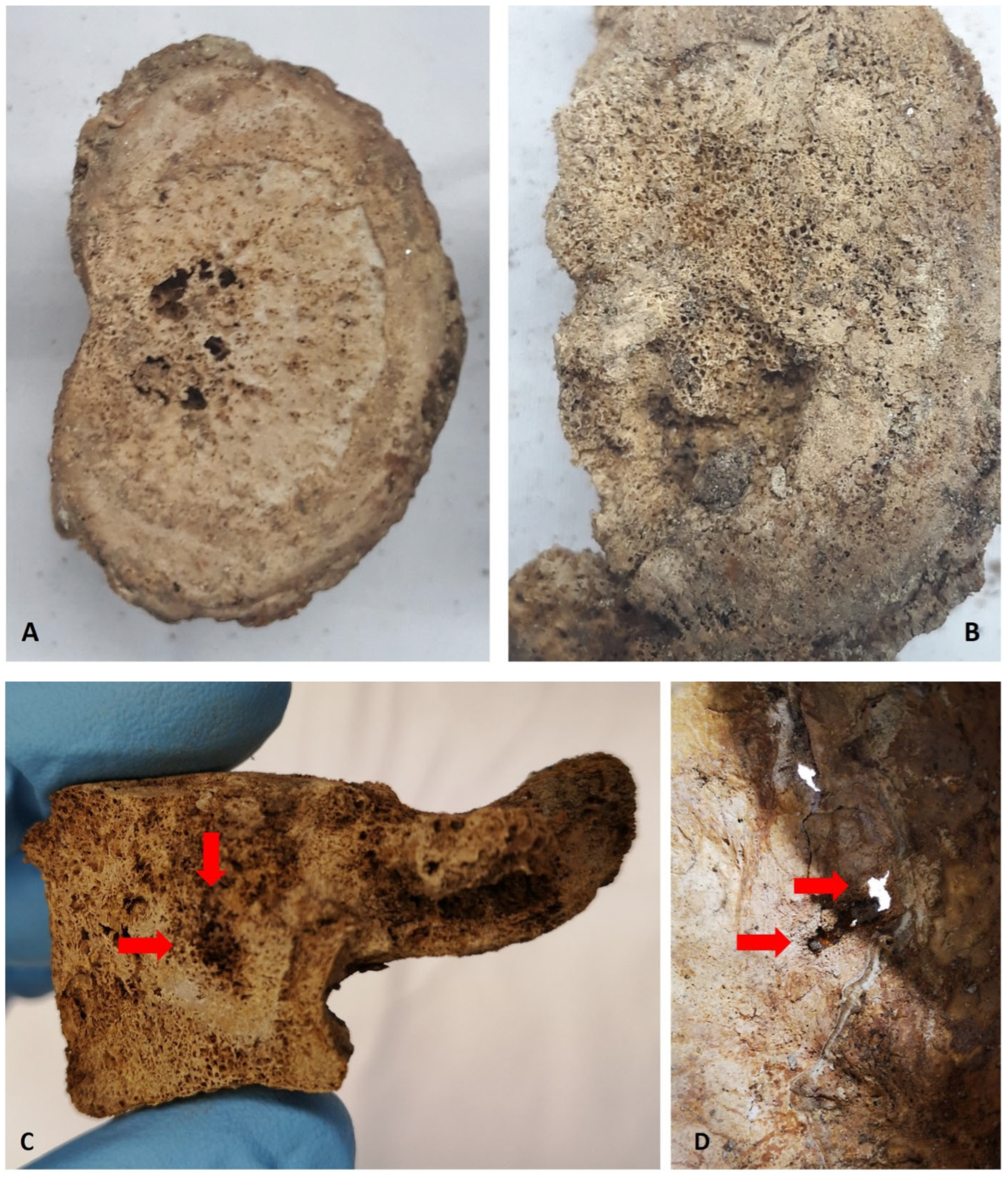
Figure 8.
CT scans of the osteolytic-osteoblastic lesions of the skeleton: A) Sagittal reconstruction through several vertebral bodies showing the extensive mixed osteolytic-osteoblastic bone reaction (arrows). B) Paracoronal reconstruction through the right pelvic bone fragment also showing extensive mixed bone infiltration (arrows). C) Parasagittal reconstruction through the skull with a circumscribed osteolysis, mainly of the inner skull bone table (arrows). D) Axial reconstruction through the skull showing an additional presumed metastasis in the left temporomandibular joint (circle); note the soil residues in the maxillary sinus (arrows) (images: S. Panzer).
Figure 8.
CT scans of the osteolytic-osteoblastic lesions of the skeleton: A) Sagittal reconstruction through several vertebral bodies showing the extensive mixed osteolytic-osteoblastic bone reaction (arrows). B) Paracoronal reconstruction through the right pelvic bone fragment also showing extensive mixed bone infiltration (arrows). C) Parasagittal reconstruction through the skull with a circumscribed osteolysis, mainly of the inner skull bone table (arrows). D) Axial reconstruction through the skull showing an additional presumed metastasis in the left temporomandibular joint (circle); note the soil residues in the maxillary sinus (arrows) (images: S. Panzer).
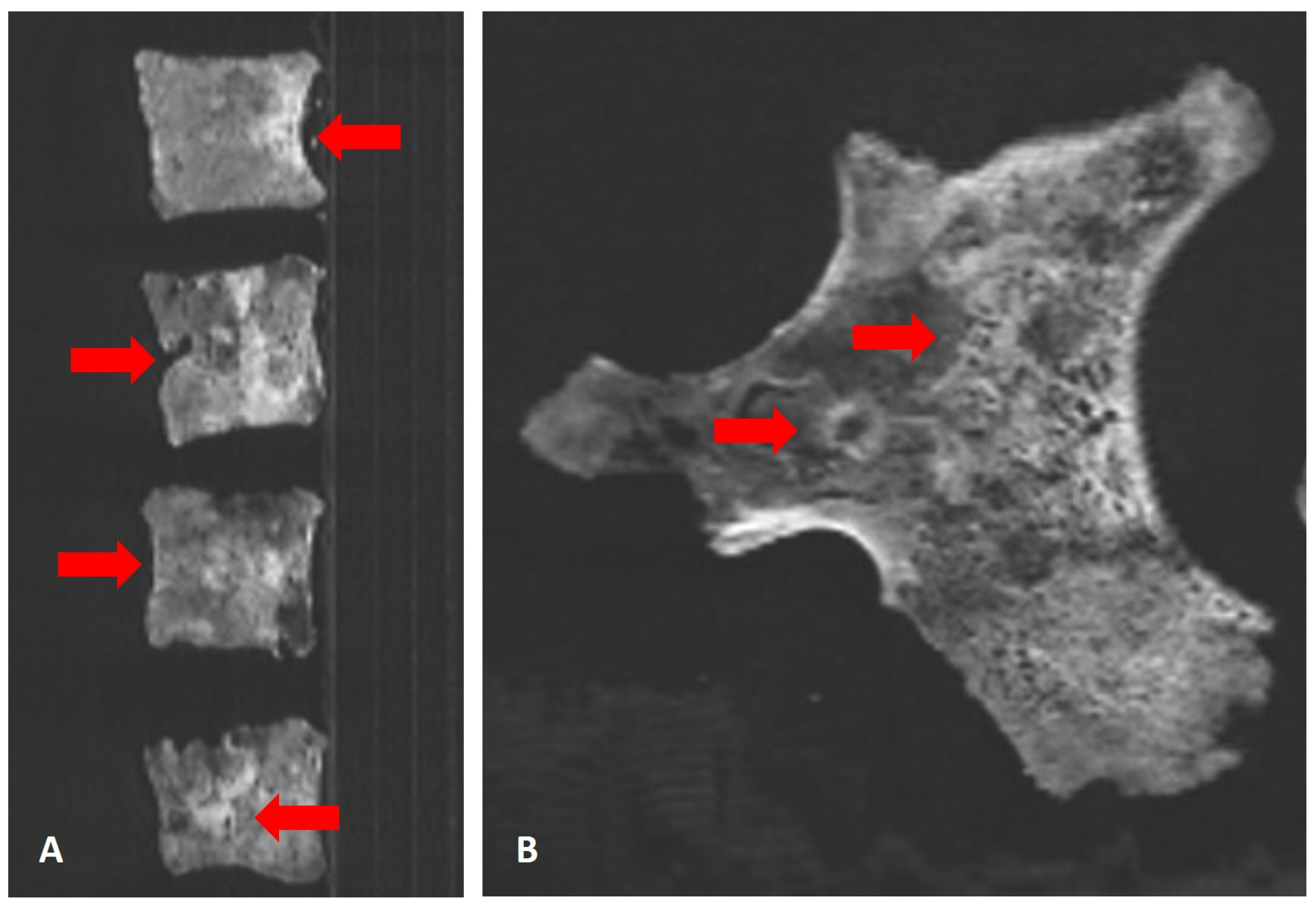

Figure 9.
Further CT-scan features: A) Coronal reconstruction through the skull showing soil in the paranasal sinuses (arrow). Note the single preserved tooth in region 47 (circle). B) Coronal reconstruction of the right radius showing an oblique bone bar in the distal radial metaphysis (circle) (images: S. Panzer).
Figure 9.
Further CT-scan features: A) Coronal reconstruction through the skull showing soil in the paranasal sinuses (arrow). Note the single preserved tooth in region 47 (circle). B) Coronal reconstruction of the right radius showing an oblique bone bar in the distal radial metaphysis (circle) (images: S. Panzer).
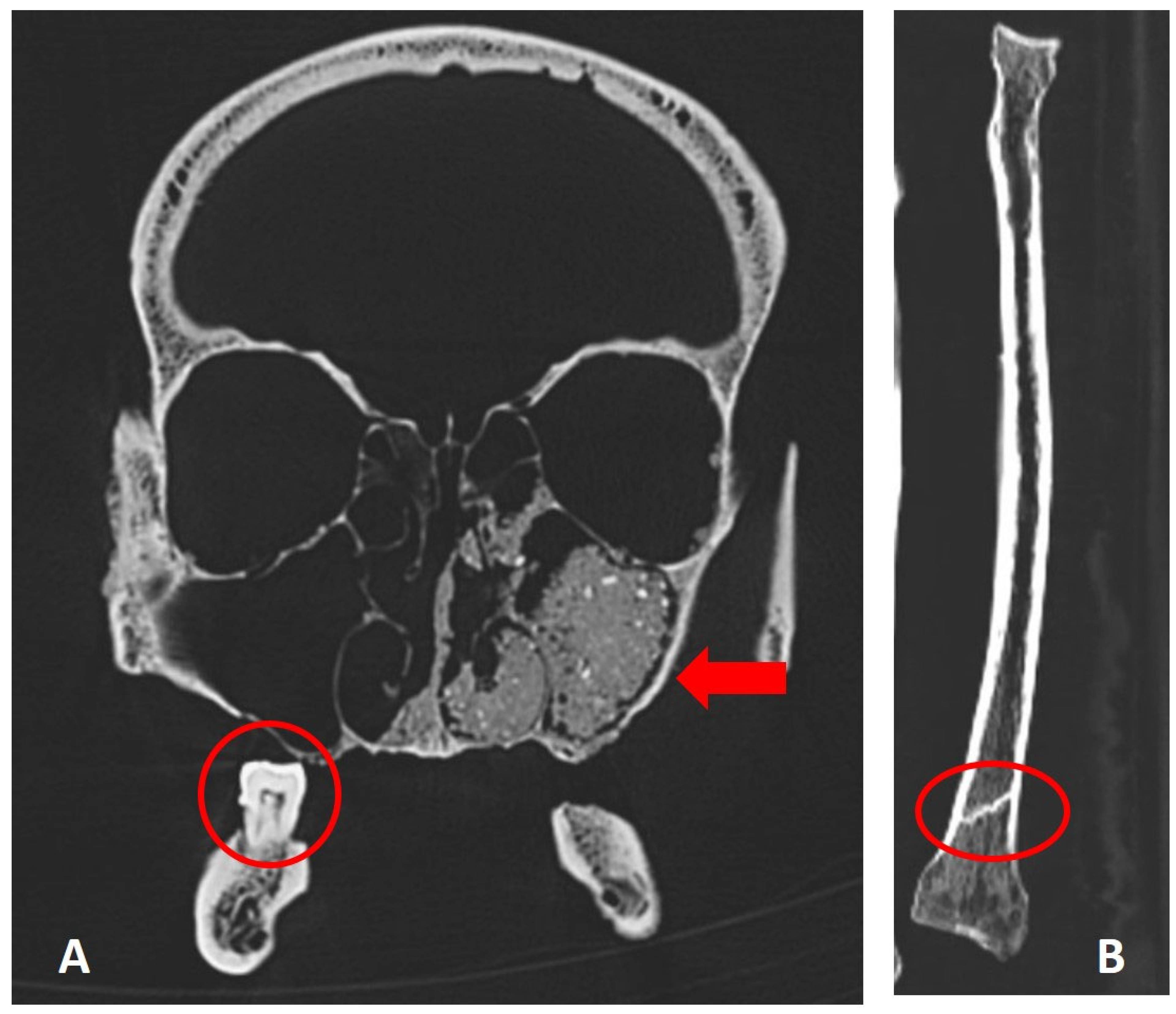
Figure 10.
Calibrated radiocarbon date profile of a femur sample (image: Ch. Hamann).
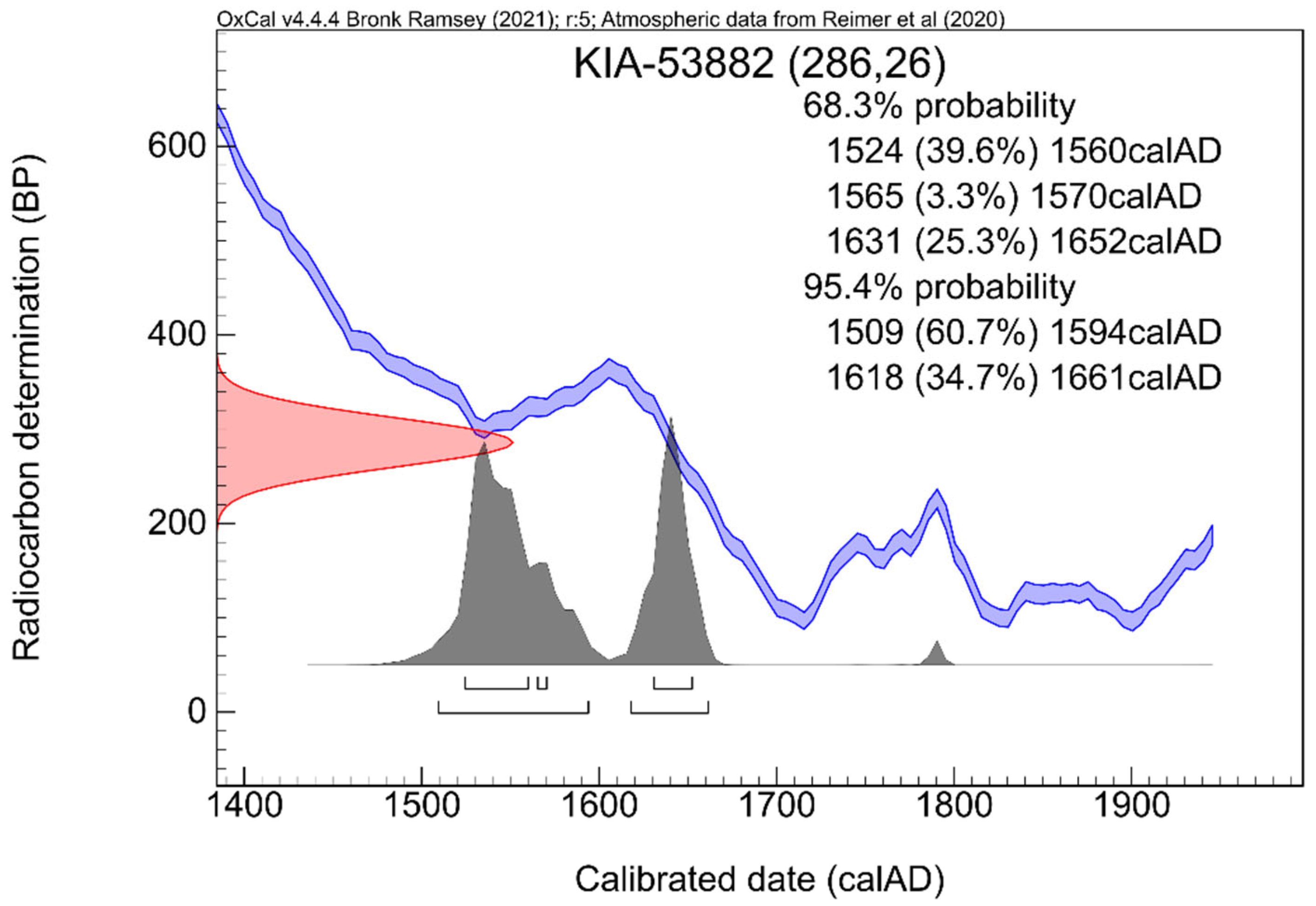
Figure 11.
Histomorphology of tumour tissue found in a vertebral body: A) Routine staining (H&E stain) showing irregular newly built tumour bone enclosing small residues of tumour tissue in the marrow. B) Immunohistochemical detection of PSA-specific antigen (red colour; circles) indicating a prostate metastasis (images: A. Nerlich).
Figure 11.
Histomorphology of tumour tissue found in a vertebral body: A) Routine staining (H&E stain) showing irregular newly built tumour bone enclosing small residues of tumour tissue in the marrow. B) Immunohistochemical detection of PSA-specific antigen (red colour; circles) indicating a prostate metastasis (images: A. Nerlich).
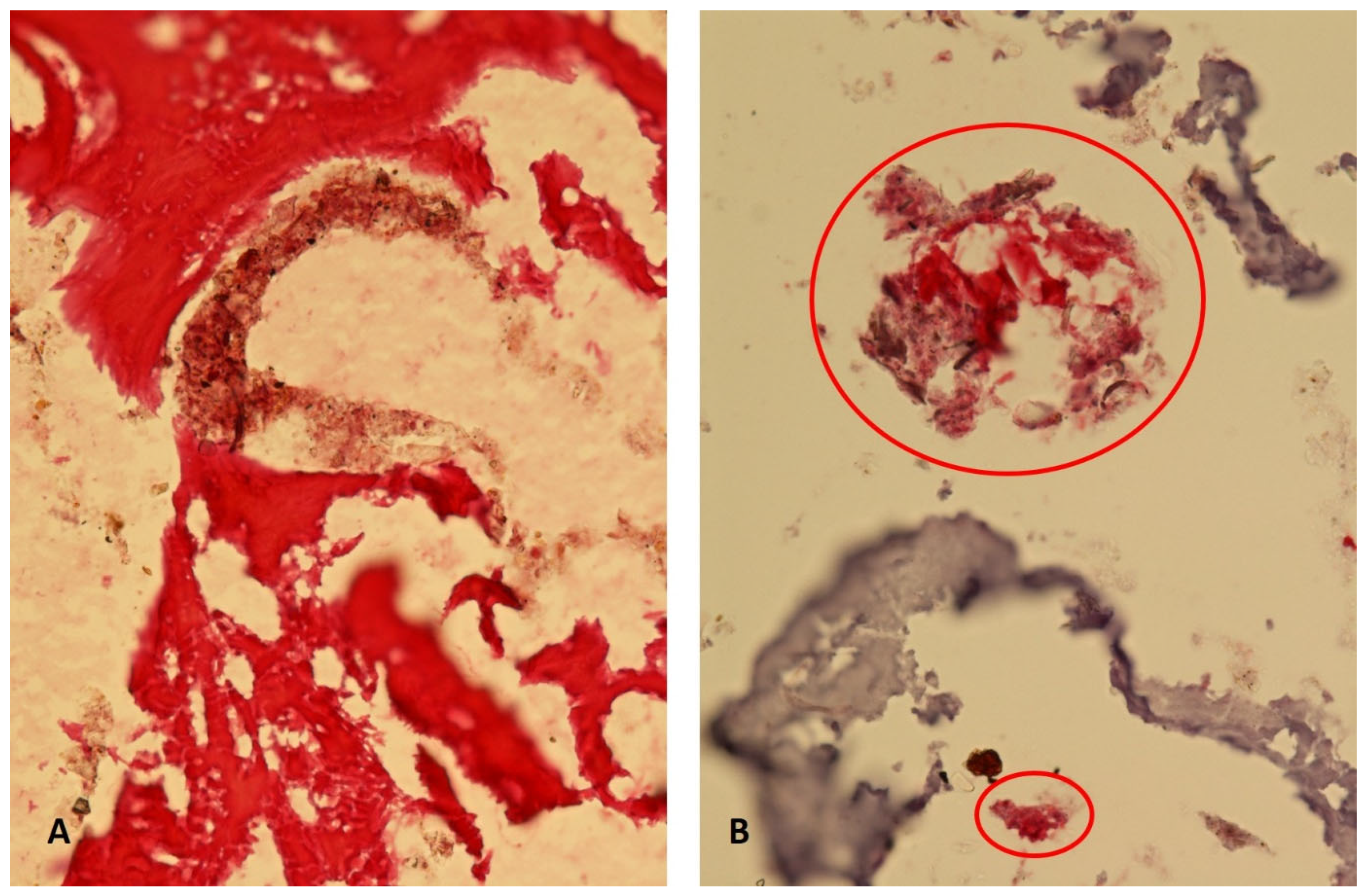
Figure 12.
Isotope levels of A) nitrogen vs. carbon stable isotope ratios and B) nitrogen vs. sulfur stable isotope ratios for abbot Balduin and comparable individuals (for refs. see also the text) (image: Ch. Lehn).
Figure 12.
Isotope levels of A) nitrogen vs. carbon stable isotope ratios and B) nitrogen vs. sulfur stable isotope ratios for abbot Balduin and comparable individuals (for refs. see also the text) (image: Ch. Lehn).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



