
Submitted:
18 April 2024
Posted:
19 April 2024
You are already at the latest version
Abstract
Human epidermal growth factor receptor 2 (HER2) is a major prognostic and predictive marker overexpressed in 15- 20 % of breast cancers. The diagnostic reference standard for selecting patients for HER2-targeted therapy is by analysis of tumor biopsies for HER2 expression and amplification. Previously patients were either defined as HER2-positive or negative, however, with approval of novel treatment options, specifically the antibody-drug conjugate trastuzumab deruxtecan, many breast cancer patients with tumors expressing low levels of HER2 and lacking HER2 amplification have become eligible for HER2-targeted therapy. Such patients will need to be reliably identified by suitable diagnostic methods. Biopsy-based diagnostics are invasive, and repeat biopsies are not always feasible. They cannot visualize heterogeneity of HER2 expression, leading to a substantial number of misdiagnosed patients. An alternative and highly accurate diagnostic method is mo-lecular imaging with radiotracers. In case of HER2, various studies demonstrate the clinical utility and feasibility of such approaches. Affibody-based radiotracers are clinically validated molecules with favorable characteristics for imaging. In this article we summarize the HER2-targeted therapeutic landscape, describe the experience with imaging diagnostics for HER2, and review the currently available clinical data on HER2-Affibody-based molecular imaging as novel diagnostic tool in breast cancer and beyond.
Keywords:
HER2
; breast cancer
; diagnostics
; molecular imaging
; Affibody molecules
; clinical trials
1. Introduction
Human epidermal growth factor receptor 2 (HER2) is overexpressed and/or amplified in around 15-20 % of breast cancer patients and expressed to a lesser degree in a large fraction of the remaining breast cancers [1,2,3]. Many other solid tumors also show high frequencies of HER2 expression, e.g., gastric and gastroesophageal carcinoma, ovarian cancer, pancreatic cancer, and colorectal cancer [4]. The use of HER2-targeted therapies has dramatically improved outcome and survival of HER2-expressing breast cancer patients over the last decades since the approval of the first HER2-targeted antibody, trastuzumab, in 1998 [5]. To date, four tyrosine kinase inhibitors (pyrotinib with approval in China only), three monoclonal antibodies, as well as two antibody-drug conjugates (ADC) directed against HER2 have been approved and implemented in clinical practice primarily for breast cancer, but also for gastric cancer and non-small cell lung cancers (NSCLC) with activating HER2 mutations (Table 1) [6]. Furthermore, several trastuzumab biosimilars, as well as subcutaneous formulations of trastuzumab and pertuzumab, have entered the market. Multiple clinical trials are ongoing in breast cancer and various other HER2-expressing cancers, evaluating promising novel drug formats including (combinations of) HER2-targeted bispecific antibodies, ADCs, radiotherapies, and cancer vaccines among others [7,8]. Notably, the novel ADC trastuzumab deruxtecan has shown efficacy in patients with low HER2 expression in the DESTINY-Breast04 trial [9], thereby opening a new treatment opportunity for a large patient group previously not eligible for HER2-targeted therapies. Notably, trastuzumab deruxtecan demonstrated efficacy in a basket trial investigating therapeutic outcome in a tissue agnostic manner across different HER2-positive indications [10].
The detection of HER2 expression and consequently the decision on whether a patient will receive HER2-targeted therapy is routinely assessed by immunohistochemistry (IHC) and/ or in situ hybridization (ISH) assays on a biopsy of primary tumor or metastases. Hereby, HER2-positive has previously been defined as IHC3+ and IHC2+/ISH+, HER2-negative as IHC2+/ISH-, IHC1+, and IHC0; new research and clinical data suggests that the distinction into HER2-low and true HER2-negative (IHC0) will become more important with the implementation of novel therapeutics into the clinical routine [11]. Heterogeneity of HER2 expression in cancer has been recognized as a major challenge and a plethora of studies have demonstrated the spatial and temporal heterogeneity of HER2 expression and its impact on treatment outcomes [3,12,13,14,15]. Although these limitations have been a topic of debate for over 20 years, no alternative diagnostic methods have been implemented in clinical routines to guide treatment decisions for HER2-targeted agents. In clinical practice patients may not be offered HER2-directed therapies because of false-negative biopsy results. Vice versa, patients whose tumors loose HER2 expression after initial treatment may remain on a therapy that has no or only limited benefit but bears the risk of unnecessary adverse events due to assumed HER2-positivity [14,16,17]. An analysis of more than 21 000 early-stage breast cancer patients in Japan revealed that out of 2811 patients whose tumors were HER2-positive before neoadjuvant chemotherapy, tumors of 601 patients (21.4%) had lost HER2 expression after therapy, while 340 (3.4%) of the 9947 patients with previously HER2-negative tumors had changed to HER2-positive tumors. [18]. In a clinical trial of 164 patients with early-stage breast cancer, tumor heterogeneity was assessed by comparing HER2 expression on biopsy tissue from two locations of the same tumor. Patients with intratumoral heterogeneity of HER2 expression showed no response to neoadjuvant therapy with trastuzumab emtansine plus pertuzumab, while those with HER2-positive tumors without heterogeneity showed a pathological complete response in 55% of cases [17]. These examples highlight the importance of implementing diagnostic tools that allow the assessment of HER2 status before, during or after therapeutic interventions in all tumor lesions. A better understanding of inter- and intratumoral heterogeneity of HER2 expression is crucial for making optimized and personalized treatment decisions, thus maximizing patient benefit. Furthermore, there is an emerging need to better understand the impact of modern HER2-targeted drugs, such as trastuzumab deruxtecan, on patient outcomes, and particularly their role in HER2-low disease. Robust methods that can overcome the shortcomings of biopsy-based determination of HER2 status will need to be developed to characterize HER2-low disease and enable visualization of HER2 heterogeneity [9,14,19].
2. Application of Diagnostic Radiopharmaceuticals in Oncology
Various diagnostic compounds for positron emission tomography (PET) and single-photon emission computed tomography (SPECT) imaging have been approved to date. A prominent tumor agnostic imaging compound is fluorodeoxyglucose F 18 ([18F]FDG) that utilizes the abnormal glucose metabolism of tumors and visualizes areas with increased glucose uptake. In clinical practice [18F]FDG PET is combined with computed tomography (CT) and as such can provide a tool for staging or restaging of tumors, detecting recurrence, and allowing monitoring of treatment responses in some tumor types [20,21,22]. Examples of other radiopharmaceuticals with non-specific accumulation in neoplastic malignancies include gallium-67 citrate, thallium-201 chloride, technetium-99m sestamibi [23].
As opposed to the tumor agnostic detection of metabolically active lesions by, e.g. [18F]FDG PET, many diagnostic radioligands specifically bind and visualize antigens or receptors expressed on tumor cells (see Table 2 for key diagnostic radioligands). Prominent examples are somatostatin receptor (SSTR) targeted radioligands that visualize SSTR-positive neuroendocrine tumors. They are utilized to identify patients who will benefit from treatment with the radiotherapeutic drug lutetium Lu 177 dotatate, which is almost identical to the imaging agent, but radiolabeled with the beta emitter lutetium-177. Similarly, PSMA-targeting radioligands help identify patients eligible for targeted radiotherapy with a second approved radioligand therapy, lutetium Lu 177 vipivotide tetraxetan. These diagnostics are part of a theranostic pair, where the diagnostic imaging compound is closely related to a therapeutic radioligand and can therefore be utilized to stratify patients that will benefit most from such therapy [24].
Targeted radioligands can also be utilized to guide treatment decisions outside of the theranostic context. A prominent example is fluoroestradiol F-18 (FES PET) for the detection of estrogen receptor positive breast cancer lesions by PET imaging in adjunct to biopsy. Among breast cancer patients around 70% have tumors expressing estrogen receptors, which is a major prognostic indicator [25,26]. A key advantage of FES PET imaging in breast cancer is the potential to non-invasively and with high sensitivity and specificity determine the estrogen receptor status throughout the whole body in case of metastatic disease, as recently confirmed in the IMPACT trial. In this trial - including 200 newly diagnosed metastatic breast cancer patients - the clinical validity of FES PET to determine tumor ER status was confirmed [27]. Comparable imaging agents to identify HER2 expression in breast cancer are currently not approved and not routinely used in clinical practice. However, various studies have highlighted the benefits of, for example, trastuzumab-based HER2-imaging agents [28,29,30,31].
The most advanced non-antibody imaging agent directed against HER2 is based on the Affibody class of molecules. In the following sections of the review we will give an overview of the clinical experience in HER2 molecular imaging with a focus on Affibody-based HER2 radioligands and describe the applicability and utility of such ligands as novel diagnostic tools.
3. Assessing HER2 Status in Cancer Patients by Molecular Imaging
Molecular imaging with PET or SPECT for HER2 is a non-invasive diagnostic method that can be used to repeatedly assess whole-body HER2 status. These methods overcome challenges and shortcomings associated with repeat biopsies and lesions not amenable to biopsy. Various radiolabeled biomolecules for imaging of HER2 and other tumor targets have been tested as diagnostics in cancer patients including radiolabeled trastuzumab and pertuzumab, nanobodies, antibody fragments, and other molecules, and are reviewed in detail elsewhere [32,33,34]. Small scale clinical trials have shown a correlation of high uptake values of HER2-imaging tracers with response to HER2-targeted therapy. A pilot study including 10 patients with metastatic HER2-positive breast cancer utilized PET imaging with [18F]FDG PET and [64Cu]Cu-DOTA-trastuzumab before treatment with trastuzumab emtansine. Patients with higher tracer uptake had better response rates and longer duration of response compared to patients under a certain uptake threshold [28]. These results corroborated the outcome of the earlier ZEPHIR trial. Final results of this trial including 90 breast cancer patients were recently published and show the high negative predictive value of [89Zr]Zr-trastuzumab PET alone or in combination with [18F]FDG PET in predicting lesion-based and patient-based response to HER2-targeted therapy with trastuzumab emtansine (T-DM1) [29,35]. The outcome of this study clearly demonstrates that HER2 PET imaging can detect HER2-positive lesions in breast cancer patients and identify patients with a low probability of response to T-DM1.
To increase the accuracy of HER2 assessments during diagnostic workup, an imaging agent should enable high contrast images acquired ideally within a few hours after tracer injection [36]. Full sized monoclonal antibodies (molecular weight ~150 kDa) are not ideal due to their very long plasma half-life, resulting in images being acquired days after tracer administration. Smaller binding molecules such as nanobodies (~14 kDa) can detect HER2 avid metastases in patients on the day of injection [37] but it has been argued that the ideal molecular size would be below 10kDa to allow efficient extravasation and tumor penetration [38]. Affibody molecules are a class of such small (~6.5kDa) engineered affinity proteins that have been extensively investigated for imaging purposes [39,40], including imaging of both HER2 [41] and EGFR [42] expression. Within the Affibody drug class, high affinity binders to a large array of targets have been generated. Of note, safety of this novel drug class has been demonstrated in more than 900 patients receiving different Affibody molecules. These include HER2 imaging tracers, which will be reviewed below, as well as a therapeutic Affibody molecule blocking interleukin 17 (izokibep) that recently demonstrated to be safe and efficacious in more than 750 patients with monthly high dose administrations for up to three years [43]. Together this suggests that the Affibody molecule class can be safe and efficacious for molecular imaging of cancer patients.
4. Clinical Experience of HER2-Affibody Molecular Imaging in HER2-Positive Breast Cancer Patients
ABY-025 (tezatabep matraxetan) is a 7.55 kDa Affibody molecule binding specifically and with picomolar affinity to human HER2 [44]. Its utility for molecular SPECT or PET imaging of HER2 expression has been demonstrated in various preclinical and clinical studies. Notably, ABY-025 binds to a different epitope than the therapeutic antibodies trastuzumab and pertuzumab (see Figure 1) and imaging with this ligand is therefore not impaired by simultaneous HER2-targeted antibody therapy [44,45].
The special technical features resulting in applicability of Affibody ligands as a drug class for molecular imaging are reviewed in detail elsewhere [40].
To date, publications reporting a total of 188 breast cancer patients imaged with either the Affibody tracer ABY-025 or ABY-025-derivatives, or closely related HER2-targeted Affibody molecules have been identified (Table 3). Furthermore, more than 30 patients with gastric or gastroesophageal carcinoma have undergone HER2-Affibody PET imaging, and additional studies in this patient group are ongoing (Table 4). Importantly, no safety issues or adverse events attributed to the imaging compound were reported in any of these studies, demonstrating a favorable benefit-risk profile of this imaging tracer. The first publication about an Affibody imaging tracer with the Affibody ligand ABY-002 labelled with indium-111 or gallium-68, for SPECT or PET imaging, respectively, is to our knowledge also the first report on a non-immunoglobulin-based protein scaffold imaging tracer [46]. In this study, HER2-Affibody imaging was compared to previous [18F]FDG PET results in patients with breast cancer. Nine out of eleven [18F]FDG PET positive lesions could be detected by ABY-002. Already this first study highlighted the potential of the technology: HER2 positive metastases not amenable to biopsy could be identified, whole-body HER2 status could be visualized, and both quantitative and qualitative information not accessible through standard imaging procedures or biopsy analysis could be obtained.
Following up on these promising first in human results Sörensen et al. conducted several imaging trials in metastatic breast cancer patients utilizing ABY-025 initially labeled with indium-111 for SPECT in seven patients and thereafter labeled with gallium-68 for PET, covering a total of 63 ABY-025-imaged breast cancer patients from the same clinical center in Uppsala, Sweden [41,47,48]. In the first seven metastatic breast cancer patients (five HER2-positive and two HER2-negative patients by previous biopsy), analyzed by SPECT imaging utilizing [111In]In-ABY-025, HER2-positive lesions showed clear tracer avidity, while uptake in HER2-negative lesions was of low contrast [47]. In all lesions that were subsequently verified by imaging guided-biopsy, HER2-IHC analyses correlated with either high or low contrast uptake for HER2-positive (defined as IHC3+ or FISH+; IHC2+ and FISH+) or negative (defined as IHC2+/ISH-, IHC1+, or IHC0) biopsy results, respectively. Notably, a brain metastasis not identified by [18F]FDG PET could be visualized with [111In]In-ABY-025 SPECT imaging in one patient, and this lesion was confirmed to be HER2-positive by IHC after surgical removal. No ABY-025 related adverse events were reported in this study, and furthermore up to 6 weeks after tracer injection no anti-drug antibodies could be detected. There was no correlation between tracer organ uptake to shed serum HER2. Despite promising results this study had some limitations: quantification of tracer uptake required dual imaging timepoints, and smaller metastases visualized by [18F]FDG PET could not be detected by HER2-SPECT imaging. These limitations may be due to the lower resolution of SPECT imaging in comparison to PET. Therefore, a follow up trial explored the clinical utility of [68Ga]Ga-ABY-025 PET imaging in 16 breast cancer patients, including both HER2-positive and HER2-negative patients as defined by biopsy [41]. After determining an optimized injected peptide mass in the first 10 patients, five additional patients were imaged two times with a one-week interval as a test-retest of uptake in individual lesions, which showed high correlation between the two tests (r=0.996). Here [68Ga]Ga-ABY-025 PET imaging could discriminate between positive and negative lesions and showed high correlation with corresponding biopsy results. SUV of lesions classified as HER2-positive by histology versus SUV of HER2-negative lesions were significantly different in this study at both peptide doses tested and at all imaging time points. In the high peptide dose group, the mean SUVmax at the 4-hour imaging time point was 5.5-fold higher in HER2-positive versus HER2-negative lesions, and there was a significant correlation between HER2-scoring by biopsy-based IHC and [68Ga]Ga-ABY-025 SUV. Importantly, treating physicians changed therapeutic intervention in three patients in this study based on ABY-025 PET results: two patients with tumors which were defined as HER2-negative by previous biopsies showed very high tracer uptake and the lesions could be confirmed as HER2-positive by additional imaging-guided biopsy analyses. These patients were consequently treated with trastuzumab. A third patient had a primary HER2-positive tumor, but showed very low ABY-025 avidity, and biopsies from two locations confirmed HER2-negative status. As a result, trastuzumab treatment was stopped in this patient. The results gained in this small patient cohort demonstrate the impact HER2-imaging could have if utilized in clinical routine for optimizing patients’ therapy.
To understand if imaging with [68Ga]Ga-ABY-025 PET could predict early response to HER2-targeted therapy, Sörensen and colleagues conducted a phase II study (NCT03655353). Interim results of this study were recently published [48] and report on 40 breast cancer patients with known HER2-positive status. Patients had either primary or metastatic breast cancer and were either treatment-naïve, or had received up to 3, or more than 3 previous therapies. Within the course of the study, they were treated with two cycles of HER2-targeted therapy (trastuzumab plus pertuzumab and chemotherapy in the neoadjuvant setting or at first recurrence, trastuzumab emtansine in case of multiple recurrence). Early response was assessed by comparing metabolic response measured by [18F]FDG PET at baseline and after 2 treatment cycles (see Figure 2). HER2-status was assessed by [68Ga]Ga-ABY-025 PET before the two treatment cycles, and one imaging guided biopsy per patient was taken to reassess HER2 status by IHC/ISH. Strikingly, 12 out of 40 patients showed a mismatch in HER2-expression between biopsy and imaging if a cut-off SUVmax of 6.0 was applied. In the patient group with metastatic breast cancer the same cutoff predicted early metabolic response with a sensitivity of 86% and specificity of 67% in soft tissue lesions, while HER2 status by biopsy showed no predictive value. Significant association between HER2 status by biopsy and [68Ga]Ga-ABY-025 uptake could not be established in this study. The authors concluded that use of [68Ga]Ga-ABY-025 PET can be an adjunct diagnostic to predict the HER2 status required to induce early metabolic tumor remission after HER2-targeted therapy. Further studies are required to establish the clinical utility of ABY-025 PET imaging as diagnostic tool for detection of HER2 status and predictor of response to HER2-targeted therapy.

Table 3.
Affibody-based HER2 molecular imaging clincial trials in breast cancer.
| Affibody ligand | HER2 status | Radioisotope (PET/SPECT) | Number of patients | Reference |
|---|---|---|---|---|
| ABY-002 | pos | 111In (SPECT); 68Ga (PET) | 3 | Baum J Nucl Med 2010 [46] |
| ABY-025 | pos/neg | 111In (SPECT) | 7 | Sörensen J Nucl Med 2014; Sandberg Eur J Nucl Med Mol Imaging 2017 [47,49] |
| ABY-025 | pos/neg | 68Ga (PET) | 16 | Sörensen Theranostics 2016; Sandberg Eur J Nucl Med Mol Imaging 2017; Sandström J Nucl Med 2016 [41,49,50] |
| NOTA-Mal-Cys-MZHer342 | pos/neg | 68Ga (PET) | 2 | Xu Br J Radiol 2019 [51] |
| HEHEHE-ZHER2-GGGC | pos | 99mTc (SPECT) | 30 | Cai Iran J Radiol 2020 [52] |
| NOTA-Mal-Cys-MZHer342 | pos/neg | 68Ga (PET) | 24 | Miao Front Oncol 2022 [53] |
| GE-226 | pos | 18F (PET) | 20 | Kenny JCO 2022 (abstract) [54] |
| RESCA-HER2-BCH / NOTA-HER2-BCH | pos/neg | 18F (PET) | 5 | Liu EJNMMI 2023 [55] |
| ABY-025 | pos | 68Ga (PET) | 40 | Alhuseinalkhudhur J Nucl Med 2023 [48] |
| ABY-025 | low | 68Ga (PET) | 10 | Altena J Nucl Med 2024 [56] |
| ZHER2:41071 | pos/neg | 99mTc (SPECT) | 31 | Bragina Theranostics 2023 [57] |
Another strategy to utilize the HER2 specific Affibody molecule for PET imaging is exemplified by the development of GE-226, in which the Affibody HER2 binder is labeled with 18F [58]. Kenny et al. presented results of 20 breast cancer patients with locally advanced or metastatic disease imaged with this molecule at the Annual Meeting of the American Society of Clincal Oncology (ASCO) 2022. In the meeting abstract, the authors report on a significant difference in tracer uptake measured by SUVmean and SUVmax between biopsy-proven HER2-positive versus HER2-negative tumors. In three out of 20 patients either intertumoral or intratumoral heterogeneity was observed, depicted by varying degrees of tracer avidity. Of note, according to the authors GE-226 imaging allowed to distinguish lymphadenopathy due to sarcoidosis from malignant lesions in one patient and was superior to [18F]FDG PET in this case [54].
Other 18F-labelled HER2-Affibody ligands derived from ABY-025 coupled to two different chelators (NOTA and RESCA) were tested in early clinical trials [55]. In a direct comparison of Affibody-imaging compounds containing either the chelator NOTA or RESCA in five patients the authors concluded on the superiority of the RESCA containing construct. This molecule showed reduced kidney uptake and retention, as well as higher contrast images and performed better in the detection of metastases [55]. Further studies with this compound are warranted to elucidate its full potential.
Lastly, two studies reported on the use of the HER2 Affibody variant [68Ga]Ga-NOTA-MAL-Cys-MZHER2:342. While the first study demonstrated the translatability from preclinical to clinical application and the feasibility of imaging with this tracer in two breast cancer patients [51], the second study highlighted various scenarios in which HER2 imaging can be of clinical utility in the assessment of breast cancer patients. 24 patients with biopsy/IHC confirmed breast cancer participated in the trial. According to the authors of the study treating physicians requested HER2 imaging for the following reasons: 1) to differentiate among metastases of multiple primary tumors, with one confirmed primary HER2-positive breast cancer and additional primary cancers that could be breast cancer with no or low HER2 expression or other primary malignancies; 2) to assess HER2 status of lesions not accessible to biopsy or repeat biopsy; and 3) to assess patients’ inter- and intratumoral heterogeneity of HER2 expression [53]. Intra-patient heterogeneity of tracer uptake was observed, and inter-patient tumor tracer uptake varied greatly (up to 11-fold difference in SUVmax). Nonetheless, when comparing to HER2 status detected on biopsies by IHC/ISH, the Affibody tracer demonstrated high sensitivity and specificity. 22 out of 24 HER2-positive biopsied tumor lesions were also positive by HER2-Affibody-PET imaging. Tumor uptake with the 68Ga-labeled HER2-binding Affibody was considered positive in 16, negative in seven and equivocal in one patient. Strikingly, tumors of five patients previously classified as HER2-negative were reclassified as HER2-positive after imaging. Consequently, these patients showed an overall response rate of 60% after receiving anti-HER2 therapy due to imaging results. Conversely, two patients were reclassified as HER2-negative and received non-HER2 targeting therapy resulting in an objective response in one of them. These results highlight how HER2-binding Affibody imaging can support personalized treatment decisions as well as overcome shortcomings of biopsy-based HER2 assessment.
5. Clinical Experience of HER2-Affibody PET Imaging in HER2-Low Breast Cancer Patients
A first proof-of concept trial utilizing [68Ga]Ga-ABY-025 PET/CT including 10 previously biopsy-verified HER2-low breast cancer patients was conducted as part of the NCT05619016 basket imaging trial for patients with HER2-expressing tumors. Results from this pilot cohort demonstrate that imaging of HER2-low patients with [68Ga]Ga-ABY-025 PET/CT is both safe and feasible [56].
All patients in this cohort showed lesions with [68Ga]Ga-ABY-025 uptake higher than background (Figure 3). After the ABY-025-PET investigation, the HER2-low status was confirmed in 8 of 10 patients by imaging-guided biopsy and subsequent IHC/ISH analysis. Two patients had biopsy results of HER2 0 in tumor lesions, one in a cutaneous lesion with low SUVmax and one in a liver metastasis with high SUVmax (24.9) but a ‘cold’ core due to central necrosis (Figure 4).
Furthermore, substantial heterogeneity in tracer uptake was observed between different lesions within the same patient. The trial is planned to continue with recruitment of new cohorts to validate [68Ga]Ga-ABY-025 PET/CT as diagnostic tool for selecting patients for HER2-targeted therapy. New cohorts will include the HER2-low patient group as well as patients with other tumor types with reported HER2-low expression and HER2-amplification.
6. SPECT Alternative for HER2-Affibody Imaging
PET imaging is mostly available in highly developed countries and may not be available in countries with lower income [59,60]. Therefore, Bragina et al. studied the use of a modified Affibody tracer for SPECT/CT imaging in 31 primary breast cancer patients [61]. The applied tracer utilized GGGC instead of DOTA as chelator for technetium-99m. 99mTc is easily available because of production in generators, much cheaper than 111In, and provides lower absorbed doses and better spatial resolution than 111In. The short half-life of 99mTc makes it suitable to read out already after 3-4 hours when labelled to a small peptide as an Affibody molecule. To define the optimal injected peptide mass, three different mass doses of the Affibody tracer, i.e., 500, 1000 and 1500 g were tested in three treatment groups. A minimum of 5 HER2-positive and 5 HER2-negative patients were enrolled in each group. Patients received a radioactive dose of 451 ± 71 MBq [99mTc]Tc-ZHER2:4107. SPECT/CT imaging was performed at several timepoints up to 24 hours post tracer injection, and planar imaging was conducted at 2, 4, and 6 hours after injection. This study defined 1000 g injected peptide mass as superior to the other doses tested in discriminating between HER2-positive and negative tumor lesions at an optimal imaging time point of 2 hours (see representative images in Figure 5).
All known lymph node metastases could be visualized, and significantly higher uptake in lymph node metastases of patients with HER2-positive lesions versus patients with HER2-low/negative lesions was observed. Further, all liver metastases could be visualized, with some liver metastases exceeding uptake of tracer compared to primary tumor lesions. Kidneys, adrenal glands, and liver were the organs with highest [99mTc]Tc-ZHER2:4107 uptake, followed by breast and lung. Different protein mass doses did not have a major influence on healthy organ uptake of the tracer.
The utility of Affibody-SPECT imaging for HER2-expressing cancers is further supported by a report on 30 breast cancer patients imaged with a [99mTc]Tc-labeled HER2 Affibody [52]. In this study, nine out of 30 patients had to be reclassified based on imaging results as either HER2-positive (six patients), or HER2-negative (three patients). HER2-Affibody SPECT imaging had an overall sensitivity of 80% and specificity of 60%, which increased to 100% sensitivity when a minimum tumor diameter threshold of 12 mm was applied.
These studies, together with the early trial of [111In]In-ABY-025 in breast cancer patients [47], highlight the potential of SPECT/CT imaging for HER2 with Affibody-tracers, which may be a more feasible alternative to PET imaging especially in low-income countries.
7. Affibody-Based HER2 Imaging Outside Breast Cancer
HER2 is not only overexpressed in breast cancer, but to varying degrees also in other cancer types [4]. Most prominently in gastric and gastroesophageal cancer overexpression rates between 9% and 35% have been reported [62] and HER2-targeted therapies are implemented as part of first line (trastuzumab) and second line (trastuzumab deruxtecan) treatment regimens [63]. Other cancer types with known HER2 expression include colorectal cancer, ovarian cancer, bladder cancer, and pancreatic cancer, and clinical trials with HER2-targeted compounds are on the way to evaluate the targetability of HER2 alterations independent of primary indication in a tissue agnostic way [64,65,66]. Notably, the DESTINY-PanTumor-02 trial is currently assessing the efficacy of trastuzumab deruxtecan in HER2-expressing cancers previously not indicated for Enhertu therapy (NCT04482309). Primary results of this Phase 2 trial show promising response rates in several cancer types including endometrial, cervical, ovarian and bladder cancer [67,68].
Similar as for breast cancer, heterogeneity in HER2 expression has been reported in gastric cancer [69,70] and will be an emerging question in many other solid cancer indications with upcoming approvals of HER2-targeted agents. A first study by Zhou and colleagues has indicated the utility of Affibody HER2-imaging in gastric cancer [71], where repeat biopsies to detect changes in HER2 expression may be particularly challenging due to lesion location. Thirty-four patients with advanced gastric cancer were analyzed (23 HER2-positive, 11 HER2-negative on primary lesions). All HER2-positive patients had lesions detectable by the Affibody ligand (68Ga-NOTA-MAL-MZHER2), and tracer uptake was three times higher in the HER2-positive patient group compared to the HER2-negative group. Maximum uptake in HER2-positive regions was highly variable, and dependent on the target organ. Bone and liver metastases showed highest tracer avidity, followed by lymph node metastases and lastly metastases at other sites. Notably, HER2-negative patients showed no site-dependent difference in tracer uptake. A case report on [68Ga]Ga-HER2-Affibody imaging of a 40-year old woman with advanced metastatic gastric cancer published by the same authors was consistent with these results [72] and highlighted the superior ability of Affibody imaging versus [18F]FDG PET in the detection of metastases in this patient. The authors concluded that imaging with the [68Ga]Ga-HER2-Affibody tracer enables a whole-body view of tumor load and HER2 expression and can be an adjunct diagnostic to guide treatment decisions in advanced gastric cancer.
The ongoing clinical trial NCT05619016 described above in the context of HER2-low breast cancer imaging is currently also including a cohort of patients with gastroesophageal cancer with known and unknown HER2-status, for imaging with [68Ga]Ga-ABY-025 PET/CT. This trial will both help increase the understanding of HER2-expression and heterogeneity in this indication as well as validate Affibody HER2-PET imaging as diagnostic tool in gastric cancer.
Table 4.
Affibody-based HER2 molecular imaging clincial trials in gastric cancer.
| Affibody ligand | HER2 status | Radioisotope (PET/SPECT) | Number of patients | Reference |
|---|---|---|---|---|
| NOTA-Mal-Cys-MZHer342 | pos/ neg | 68Ga (PET) | 34 | Zhou EJNMMI 2021 [71] |
| NOTA-Mal-Cys-MZHer342 | pos | 68Ga (PET) | 1 | Zhou Clin Nucl Med 2020 [72] |
| ABY-025 | all | 68Ga (PET) | TBD | NCT05619016 (ongoing) |
8. Future Directions
Molecular imaging for HER2 holds great promise in improving therapeutic decision making and enabling truly personalized medicine through precision imaging. Due to the limitations of the current reference standard for identification of patients with HER2-expressing cancers based on biopsies, several other potential diagnostics are currently under clinical evaluation. Apart from molecular imaging, these comprise analysis of liquid biopsies, where HER2 amplification or expression status is detected in circulating tumor DNA (ctDNA) or on circulating tumor cells [73]. Even though first results of implementing ctDNA into patient selection for HER2-targeted therapy are encouraging, further work needs to be done to prove clinical utility of such approaches [74]. A major draw-back of utilizing liquid biopsies for patient stratification is that although they provide fast, minimally invasive, and cost-effective diagnostic insights, they will not visualize disease localization, tumor heterogeneity and the extent of HER2-expression within patients and are from this aspect inferior to molecular imaging approaches. Another key advantage of molecular imaging for cancer targets is the potential application in a theranostic context [75]. In this context, imaging tracers to define the extent of treatable tumors within a patient before radiotherapeutic intervention will be of great advantage. Affibody imaging tracers may therefore find application in theranostic pairs consisting of an Affibody-imaging agent followed by targeted molecular radiotherapy. The concept of such an Affibody-based radiotherapy has previously been explored preclinically with promising results [76]. Translation of this approach into clinical development of an HER2-targeted radioligand would highly benefit from the HER2-Affibody imaging technology.
9. Conclusions
Based on published data from more than 220 patients, Affibody-based HER2 molecular imaging appears safe and feasible. Considering the possibility to visualize HER2 expression across the whole body, Affibody-HER2 PET or SPECT imaging can become a novel diagnostic entity overcoming the limitations of the current diagnostic standard based on biopsy analysis. Molecular imaging for HER2 could overcome key limitations of biopsies, be an alternative when biopsies are not feasible or cannot be performed safely, and an adjunct or substitute for biopsies when biopsy results are deemed inconclusive or insufficient. This is particularly relevant considering that HER2 heterogeneity cannot be detected by single biopsies. The totality of data available for ABY-025 underline its potential in assessing HER2 receptor status safely and accurately - in breast cancer patients and beyond. Knowing the whole-body status of HER2 expression through molecular imaging as a diagnostic tool will greatly help to meaningfully guide use of HER2-targeted therapies on an individual patient basis.
Acknowledgments
We thank our colleagues for thorough revision of this review article, in particular Lisa Osterling Koskinen, Joshua Gregory, Karin Grünbaum, Camilla Sandell, Therese Söderdahl, and Sven Ohlman. We thank Rezan Güler for creating the image for Figure 1.
References
- Schettini, F.; Chic, N.; Braso-Maristany, F.; Pare, L.; Pascual, T.; Conte, B.; Martinez-Saez, O.; Adamo, B.; Vidal, M.; Barnadas, E. Clinical, pathological, and PAM50 gene expression features of HER2-low breast cancer. NPJ Breast Cancer 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Cronin, K.A.; Harlan, L.C.; Dodd, K.W.; Abrams, J.S.; Ballard-Barbash, R. Population-based estimate of the prevalence of HER-2 positive breast cancer tumors for early stage patients in the US. Cancer Invest 2010, 28, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Yan, M.; Schwaederle, M.; Arguello, D.; Millis, S.Z.; Gatalica, Z.; Kurzrock, R. HER2 expression status in diverse cancers: Review of results from 37,992 patients. Cancer Metastasis Rev 2015, 34, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Harries, M.; Smith, I. The development and clinical use of trastuzumab (Herceptin). Endocr Relat Cancer 2002, 9, 75–85. [Google Scholar] [CrossRef]
- Swain, S.M.; Shastry, M.; Hamilton, E. Targeting HER2-positive breast cancer: Advances and future directions. Nat Rev Drug Discov 2023, 22, 101–126. [Google Scholar] [CrossRef]
- Kunte, S.; Abraham, J.; Montero, A.J. Novel HER2-targeted therapies for HER2-positive metastatic breast cancer. Cancer 2020, 126, 4278–4288. [Google Scholar] [CrossRef] [PubMed]
- Meric-Bernstam, F.; Johnson, A.M.; Dumbrava, E.E.I.; Raghav, K.; Balaji, K.; Bhatt, M.; Murthy, R.K.; Rodon, J.; Piha-Paul, S.A. Advances in HER2-Targeted Therapy: Novel Agents and Opportunities Beyond Breast and Gastric Cancer. Clin Cancer Res 2019, 25, 2033–2041. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med 2022, 387, 9–20. [Google Scholar] [CrossRef]
- Indini, A.; Rijavec, E.; Grossi, F. Trastuzumab Deruxtecan: Changing the Destiny of HER2 Expressing Solid Tumors. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef]
- Gutierrez, C.; Schiff, R. HER2: Biology, detection, and clinical implications. Arch Pathol Lab Med 2011, 135, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Grassini, D.; Cascardi, E.; Sarotto, I.; Annaratone, L.; Sapino, A.; Berrino, E.; Marchio, C. Unusual Patterns of HER2 Expression in Breast Cancer: Insights and Perspectives. Pathobiology 2022, 89, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Seo, A.N.; Kim, E.J.; Jang, M.H.; Suh, K.J.; Ryu, H.S.; Kim, Y.J.; Kim, J.H.; Im, S.A.; Gong, G.; et al. HER2 heterogeneity affects trastuzumab responses and survival in patients with HER2-positive metastatic breast cancer. Am J Clin Pathol 2014, 142, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Nitta, H.; Li, Z. HER2 Intratumoral Heterogeneity in Breast Cancer, an Evolving Concept. Cancers (Basel) 2023, 15, 2664. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, L.S.; Karlsson, E.; Wilking, U.M.; Johansson, U.; Hartman, J.; Lidbrink, E.K.; Hatschek, T.; Skoog, L.; Bergh, J. Clinically used breast cancer markers such as estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 are unstable throughout tumor progression. J Clin Oncol 2012, 30, 2601–2608. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, F.; Carnevale Schianca, A.; Corti, C.; Ivanova, M.; Bianco, N.; Dellapasqua, S.; Criscitiello, C.; Fusco, N.; Curigliano, G.; Munzone, E. Unlocking the Resistance to Anti-HER2 Treatments in Breast Cancer: The Issue of HER2 Spatial Distribution. Cancers (Basel) 2023, 15, 1385. [Google Scholar] [CrossRef] [PubMed]
- Filho, O.M.; Viale, G.; Stein, S.; Trippa, L.; Yardley, D.A.; Mayer, I.A.; Abramson, V.G.; Arteaga, C.L.; Spring, L.M.; Waks, A.G.; et al. Impact of HER2 Heterogeneity on Treatment Response of Early-Stage HER2-Positive Breast Cancer: Phase II Neoadjuvant Clinical Trial of T-DM1 Combined with Pertuzumab. Cancer Discov 2021, 11, 2474–2487. [Google Scholar] [CrossRef] [PubMed]
- Niikura, N.; Tomotaki, A.; Miyata, H.; Iwamoto, T.; Kawai, M.; Anan, K.; Hayashi, N.; Aogi, K.; Ishida, T.; Masuoka, H.; et al. Changes in tumor expression of HER2 and hormone receptors status after neoadjuvant chemotherapy in 21,755 patients from the Japanese breast cancer registry. Ann Oncol 2016, 27, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Viale, G. HER2-Low Breast Cancer-Diagnostic Challenges and Opportunities for Insights from Ongoing Studies: A Podcast. Target Oncol 2023, 18, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Almuhaideb, A.; Papathanasiou, N.; Bomanji, J. 18F-FDG PET/CT imaging in oncology. Ann Saudi Med 2011, 31, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Avril, S.; Muzic, R.F., Jr.; Plecha, D.; Traughber, B.J.; Vinayak, S.; Avril, N. (1)(8)F-FDG PET/CT for Monitoring of Treatment Response in Breast Cancer. J Nucl Med 2016, 57 Suppl 1, 34S–39S. [Google Scholar] [CrossRef]
- Perez-Garcia, J.M.; Gebhart, G.; Ruiz Borrego, M.; Stradella, A.; Bermejo, B.; Schmid, P.; Marme, F.; Escriva-de-Romani, S.; Calvo, L.; Ribelles, N.; et al. Chemotherapy de-escalation using an (18)F-FDG-PET-based pathological response-adapted strategy in patients with HER2-positive early breast cancer (PHERGain): A multicentre, randomised, open-label, non-comparative, phase 2 trial. Lancet Oncol 2021, 22, 858–871. [Google Scholar] [CrossRef] [PubMed]
- Mettler, F.A.J.; Guiberteau, M.J. Essentials of Nuclear Medicine and Molecular Imaging, 7th Edition. Elsevier 2019. [Google Scholar] [CrossRef]
- Bodei, L.; Herrmann, K.; Schoder, H.; Scott, A.M.; Lewis, J.S. Radiotheranostics in oncology: Current challenges and emerging opportunities. Nat Rev Clin Oncol 2022, 19, 534–550. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.H.; Park, Y.; Kang, E.; Kim, E.K.; Kim, J.H.; Kim, S.H.; Suh, K.J.; Kim, S.M.; Jang, M.; Yun, B.; et al. Effect of Estrogen Receptor Expression Level and Hormonal Therapy on Prognosis of Early Breast Cancer. Cancer Res Treat 2022, 54, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Dunnwald, L.K.; Rossing, M.A.; Li, C.I. Hormone receptor status, tumor characteristics, and prognosis: A prospective cohort of breast cancer patients. Breast Cancer Res 2007, 9, R6. [Google Scholar] [CrossRef] [PubMed]
- van Geel, J.J.L.; Boers, J.; Elias, S.G.; Glaudemans, A.; de Vries, E.F.J.; Hospers, G.A.P.; van Kruchten, M.; Kuip, E.J.M.; Jager, A.; Menke-van der Houven van Oordt, W.C.; et al. Clinical Validity of 16alpha-[(18)F]Fluoro-17beta-Estradiol Positron Emission Tomography/Computed Tomography to Assess Estrogen Receptor Status in Newly Diagnosed Metastatic Breast Cancer. J Clin Oncol 2022, 40, 3642–3652. [Google Scholar] [CrossRef] [PubMed]
- Mortimer, J.E.; Bading, J.R.; Frankel, P.H.; Carroll, M.I.; Yuan, Y.; Park, J.M.; Tumyan, L.; Gidwaney, N.; Poku, E.K.; Shively, J.E.; et al. Use of (64)Cu-DOTA-Trastuzumab PET to Predict Response and Outcome of Patients Receiving Trastuzumab Emtansine for Metastatic Breast Cancer: A Pilot Study. J Nucl Med 2022, 63, 1145–1148. [Google Scholar] [CrossRef] [PubMed]
- Gebhart, G.; Lamberts, L.E.; Wimana, Z.; Garcia, C.; Emonts, P.; Ameye, L.; Stroobants, S.; Huizing, M.; Aftimos, P.; Tol, J.; et al. Molecular imaging as a tool to investigate heterogeneity of advanced HER2-positive breast cancer and to predict patient outcome under trastuzumab emtansine (T-DM1): The ZEPHIR trial. Ann Oncol 2016, 27, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Ulaner, G.A.; Hyman, D.M.; Lyashchenko, S.K.; Lewis, J.S.; Carrasquillo, J.A. 89Zr-Trastuzumab PET/CT for Detection of Human Epidermal Growth Factor Receptor 2-Positive Metastases in Patients With Human Epidermal Growth Factor Receptor 2-Negative Primary Breast Cancer. Clin Nucl Med 2017, 42, 912–917. [Google Scholar] [CrossRef] [PubMed]
- Ulaner, G.A.; Hyman, D.M.; Ross, D.S.; Corben, A.; Chandarlapaty, S.; Goldfarb, S.; McArthur, H.; Erinjeri, J.P.; Solomon, S.B.; Kolb, H.; et al. Detection of HER2-Positive Metastases in Patients with HER2-Negative Primary Breast Cancer Using 89Zr-Trastuzumab PET/CT. J Nucl Med 2016, 57, 1523–1528. [Google Scholar] [CrossRef] [PubMed]
- Ge, S.; Li, J.; Yu, Y.; Chen, Z.; Yang, Y.; Zhu, L.; Sang, S.; Deng, S. Review: Radionuclide Molecular Imaging Targeting HER2 in Breast Cancer with a Focus on Molecular Probes into Clinical Trials and Small Peptides. Molecules 2021, 26, 6482. [Google Scholar] [CrossRef] [PubMed]
- Altena, R.; Tzortzakakis, A.; Af Buren, S.; Tran, T.A.; Frejd, F.Y.; Bergh, J.; Axelsson, R. Current status of contemporary diagnostic radiotracers in the management of breast cancer: First steps toward theranostic applications. EJNMMI Res 2023, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Tolmachev, V.; Orlova, A.; Sorensen, J. The emerging role of radionuclide molecular imaging of HER2 expression in breast cancer. Semin Cancer Biol 2021, 72, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Mileva, M.; de Vries, E.G.E.; Guiot, T.; Wimana, Z.; Deleu, A.L.; Schroder, C.P.; Lefebvre, Y.; Paesmans, M.; Stroobants, S.; Huizing, M.; et al. Molecular imaging predicts lack of T-DM1 response in advanced HER2-positive breast cancer (final results of ZEPHIR trial). NPJ Breast Cancer 2024, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Tolmachev, V.; Vorobyeva, A. Radionuclides in Diagnostics and Therapy of Malignant Tumors: New Development. Cancers (Basel) 2022, 14, 297. [Google Scholar] [CrossRef]
- Keyaerts, M.; Xavier, C.; Heemskerk, J.; Devoogdt, N.; Everaert, H.; Ackaert, C.; Vanhoeij, M.; Duhoux, F.P.; Gevaert, T.; Simon, P.; et al. Phase I Study of 68Ga-HER2-Nanobody for PET/CT Assessment of HER2 Expression in Breast Carcinoma. J Nucl Med 2016, 57, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Graff, C.P.; Wittrup, K.D. Theoretical analysis of antibody targeting of tumor spheroids: Importance of dosage for penetration, and affinity for retention. Cancer Res 2003, 63, 1288–1296. [Google Scholar] [PubMed]
- Stahl, S.; Graslund, T.; Eriksson Karlstrom, A.; Frejd, F.Y.; Nygren, P.A.; Lofblom, J. Affibody Molecules in Biotechnological and Medical Applications. Trends Biotechnol 2017, 35, 691–712. [Google Scholar] [CrossRef]
- Tolmachev, V.; Orlova, A. Affibody Molecules as Targeting Vectors for PET Imaging. Cancers (Basel) 2020, 12, 651. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, J.; Velikyan, I.; Sandberg, D.; Wennborg, A.; Feldwisch, J.; Tolmachev, V.; Orlova, A.; Sandstrom, M.; Lubberink, M.; Olofsson, H.; et al. Measuring HER2-Receptor Expression In Metastatic Breast Cancer Using [68Ga]ABY-025 Affibody PET/CT. Theranostics 2016, 6, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Samkoe, K.S.; Sardar, H.S.; Gunn, J.; Feldwisch, J.; Linos, K.; Henderson, E.; Pogue, B.; Paulsen, K. Measuring microdose ABY-029 fluorescence signal in a primary human soft-tissue sarcoma resection. Proc SPIE Int Soc Opt Eng 2019, 10862. [Google Scholar] [CrossRef] [PubMed]
- Klint, S.; Feldwisch, J.; Gudmundsdotter, L.; Dillner Bergstedt, K.; Gunneriusson, E.; Hoiden Guthenberg, I.; Wennborg, A.; Nyborg, A.C.; Kamboj, A.P.; Peloso, P.M.; et al. Izokibep: Preclinical development and first-in-human study of a novel IL-17A neutralizing Affibody molecule in patients with plaque psoriasis. MAbs 2023, 15, 2209920. [Google Scholar] [CrossRef] [PubMed]
- Eigenbrot, C.; Ultsch, M.; Dubnovitsky, A.; Abrahmsen, L.; Hard, T. Structural basis for high-affinity HER2 receptor binding by an engineered protein. Proc Natl Acad Sci U S A 2010, 107, 15039–15044. [Google Scholar] [CrossRef] [PubMed]
- Feldwisch, J.; Tolmachev, V.; Lendel, C.; Herne, N.; Sjoberg, A.; Larsson, B.; Rosik, D.; Lindqvist, E.; Fant, G.; Hoiden-Guthenberg, I.; et al. Design of an optimized scaffold for affibody molecules. J Mol Biol 2010, 398, 232–247. [Google Scholar] [CrossRef] [PubMed]
- Baum, R.P.; Prasad, V.; Muller, D.; Schuchardt, C.; Orlova, A.; Wennborg, A.; Tolmachev, V.; Feldwisch, J. Molecular imaging of HER2-expressing malignant tumors in breast cancer patients using synthetic 111In- or 68Ga-labeled affibody molecules. J Nucl Med 2010, 51, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, J.; Sandberg, D.; Sandstrom, M.; Wennborg, A.; Feldwisch, J.; Tolmachev, V.; Astrom, G.; Lubberink, M.; Garske-Roman, U.; Carlsson, J.; et al. First-in-human molecular imaging of HER2 expression in breast cancer metastases using the 111In-ABY-025 affibody molecule. J Nucl Med 2014, 55, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Alhuseinalkhudhur, A.; Lindman, H.; Liss, P.; Sundin, T.; Frejd, F.Y.; Hartman, J.; Iyer, V.; Feldwisch, J.; Lubberink, M.; Ronnlund, C.; et al. Human Epidermal Growth Factor Receptor 2-Targeting [(68)Ga]Ga-ABY-025 PET/CT Predicts Early Metabolic Response in Metastatic Breast Cancer. J Nucl Med 2023, 64, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, D.; Tolmachev, V.; Velikyan, I.; Olofsson, H.; Wennborg, A.; Feldwisch, J.; Carlsson, J.; Lindman, H.; Sorensen, J. Intra-image referencing for simplified assessment of HER2-expression in breast cancer metastases using the Affibody molecule ABY-025 with PET and SPECT. Eur J Nucl Med Mol Imaging 2017, 44, 1337–1346. [Google Scholar] [CrossRef] [PubMed]
- Sandstrom, M.; Lindskog, K.; Velikyan, I.; Wennborg, A.; Feldwisch, J.; Sandberg, D.; Tolmachev, V.; Orlova, A.; Sorensen, J.; Carlsson, J.; et al. Biodistribution and Radiation Dosimetry of the Anti-HER2 Affibody Molecule 68Ga-ABY-025 in Breast Cancer Patients. J Nucl Med 2016, 57, 867–871. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, L.; Pan, D.; Yu, C.; Mi, B.; Huang, Q.; Sheng, J.; Yan, J.; Wang, X.; Yang, R.; et al. PET imaging of a (68)Ga labeled modified HER2 affibody in breast cancers: From xenografts to patients. Br J Radiol 2019, 92, 20190425. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Li, X.; Mao, F.; Wang, P.; Luo, Y.; Zheng, K.; Li, F.; Zhu, Z. Non-Invasive Monitoring of HER2 Expression in Breast Cancer Patients with 99mTc-Affibody SPECT/CT. Iran J Radiol. 2020. [Google Scholar] [CrossRef]
- Miao, H.; Sun, Y.; Jin, Y.; Hu, X.; Song, S.; Zhang, J. Application of a Novel (68)Ga-HER2 Affibody PET/CT Imaging in Breast Cancer Patients. Front Oncol 2022, 12, 894767. [Google Scholar] [CrossRef]
- Kenny, L.M.; Gilbert, F.J.; Gopalakrishnan, G.; Aravind, P.; Barwick, T.; Patel, N.; Hiscock, D.R.; Boros, I.; Kealey, S.; Aigbirhio, F.I.; et al. The HERPET study: Imaging HER2 expression in breast cancer with the novel PET tracer [18F]GE-226, a first-in-patient study. American Society of Clinical Oncology 2022. [Google Scholar] [CrossRef]
- Liu, J.; Guo, X.; Wen, L.; Wang, L.; Liu, F.; Song, G.; Zhu, H.; Zhou, N.; Yang, Z. Comparison of renal clearance of [(18)F]AlF-RESCA-HER2-BCH and [(18)F]AlF-NOTA-HER2-BCH in mice and breast cancer patients. Eur J Nucl Med Mol Imaging 2023, 50, 2775–2786. [Google Scholar] [CrossRef] [PubMed]
- Altena, R.; Buren, S.A.; Blomgren, A.; Karlsson, E.; Tzortzakakis, A.; Brun, N.; Moein, M.M.; Jussing, E.; Frejd, F.Y.; Bergh, J.; et al. Human Epidermal Growth Factor Receptor 2 (HER2) PET Imaging of HER2-Low Breast Cancer with [(68)Ga]Ga-ABY-025: Results from a Pilot Study. J Nucl Med 2024. [Google Scholar] [CrossRef] [PubMed]
- Chernov, V.; Rybina, A.; Zelchan, R.; Medvedeva, A.; Bragina, O.; Lushnikova, N.; Doroshenko, A.; Usynin, E.; Tashireva, L.; Vtorushin, S.; et al. Phase I Trial of [(99m)Tc]Tc-maSSS-PEG(2)-RM26, a Bombesin Analogue Antagonistic to Gastrin-Releasing Peptide Receptors (GRPRs), for SPECT Imaging of GRPR Expression in Malignant Tumors. Cancers (Basel) 2023, 15, 1631. [Google Scholar] [CrossRef] [PubMed]
- Iveson, P.B.; Glaser, M.; Indrevoll, B.; Shales, J.; Mantzilas, D.; Omtvedt, L.; Luthra, S.K.; Hiscock, D.; Grigg, J. FASTlab Radiosynthesis of the (18) F-labelled HER2-binding Affibody molecule [(18) F]GE-226. J Labelled Comp Radiopharm 2019, 62, 925–932. [Google Scholar] [CrossRef]
- Frija, G.; Blažić, I.; Frush, D.P.; Hierath, M.; Kawookya, M.; Donoso-Bach, L.; Brkljačić, B. How to improve access to medical imaging in low- and middle-income countries ? eClinicalMedicine 2021, 38. [Google Scholar] [CrossRef]
- Hricak, H.; Abdel-Wahab, M.; Atun, R.; Lette, M.M.; Paez, D.; Brink, J.A.; Donoso-Bach, L.; Frija, G.; Hierath, M.; Holmberg, O.; et al. Medical imaging and nuclear medicine: A Lancet Oncology Commission. Lancet Oncol 2021, 22, e136–e172. [Google Scholar] [CrossRef] [PubMed]
- Bragina, O.; Chernov, V.; Larkina, M.; Rybina, A.; Zelchan, R.; Garbukov, E.; Oroujeni, M.; Loftenius, A.; Orlova, A.; Sorensen, J.; et al. Phase I clinical evaluation of (99m)Tc-labeled Affibody molecule for imaging HER2 expression in breast cancer. Theranostics 2023, 13, 4858–4871. [Google Scholar] [CrossRef] [PubMed]
- Gravalos, C.; Jimeno, A. HER2 in gastric cancer: A new prognostic factor and a novel therapeutic target. Ann Oncol 2008, 19, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.L.; He, Y.; Xu, R.H. Gastric cancer treatment: Recent progress and future perspectives. J Hematol Oncol 2023, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Cabel, L.; Fuerea, A.; Lacroix, L.; Baldini, C.; Martin, P.; Hollebecque, A.; Postel-Vinay, S.; Varga, A.; Balheda, R.; Gazzah, A.; et al. Efficacy of histology-agnostic and molecularly-driven HER2 inhibitors for refractory cancers. Oncotarget 2018, 9, 9741–9750. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.Y.; Bang, Y.J. HER2-targeted therapies - a role beyond breast cancer. Nat Rev Clin Oncol 2020, 17, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Tsurutani, J.; Iwata, H.; Krop, I.; Janne, P.A.; Doi, T.; Takahashi, S.; Park, H.; Redfern, C.; Tamura, K.; Wise-Draper, T.M.; et al. Targeting HER2 with Trastuzumab Deruxtecan: A Dose-Expansion, Phase I Study in Multiple Advanced Solid Tumors. Cancer Discov 2020, 10, 688–701. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Makker, V.; Oaknin, A.; Oh, D.Y.; Banerjee, S.N.; Gonzalez Martin, A.; Jung, K.H.; Lugowska, I.A.; Manso, L.; Manzano, A.; et al. Efficacy and safety of trastuzumab deruxtecan (T-DXd) in patients (pts) with HER2-expressing solid tumors: DESTINY-PanTumor02 (DP-02) interim results. American Society of Clinical Oncology 2023. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Makker, V.; Oaknin, A.; Oh, D.Y.; Banerjee, S.; Gonzalez-Martin, A.; Jung, K.H.; Lugowska, I.; Manso, L.; Manzano, A.; et al. Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J Clin Oncol 2024, 42, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Grillo, F.; Fassan, M.; Sarocchi, F.; Fiocca, R.; Mastracci, L. HER2 heterogeneity in gastric/gastroesophageal cancers: From benchside to practice. World J Gastroenterol 2016, 22, 5879–5887. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Yu, T.; Zhao, Z.; Zhang, S.; Huang, Q.; Liu, G. Temporal heterogeneity of HER2 expression in metastatic gastric cancer: A case report. World J Surg Oncol 2022, 20, 157. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Liu, C.; Guo, X.; Xu, Y.; Gong, J.; Qi, C.; Zhang, X.; Yang, M.; Zhu, H.; Shen, L.; et al. Impact of (68)Ga-NOTA-MAL-MZHER2 PET imaging in advanced gastric cancer patients and therapeutic response monitoring. Eur J Nucl Med Mol Imaging 2021, 48, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Guo, X.; Yang, M.; Zhu, H.; Yang, Z. 68Ga-ZHER2 PET/CT Reveals HER2-Positive Metastatic Gastric Cancer With Better Image Quality Than 18F-FDG. Clin Nucl Med 2020, 45, e101–e102. [Google Scholar] [CrossRef] [PubMed]
- Godoy-Ortiz, A.; Alba-Bernal, A.; Pascual, J.; Comino-Mendez, I.; Alba, E. Unveiling the Potential of Liquid Biopsy in HER2-Positive Breast Cancer Management. Cancers (Basel) 2022, 14, 587. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, H.; Yagisawa, M.; Satoh, T.; Kadowaki, S.; Sunakawa, Y.; Nishina, T.; Komatsu, Y.; Esaki, T.; Sakai, D.; Doi, A.; et al. Tissue-agnostic efficacy of trastuzumab deruxtecan (T-DXd) in advanced solid tumors with HER2 amplification identified by plasma cell-free DNA (cfDNA) testing: Results from a phase 2 basket trial (HERALD/EPOC1806). Journal of Clinical Oncology 2023. [Google Scholar] [CrossRef]
- Massicano, A.V.F.; Marquez-Nostra, B.V.; Lapi, S.E. Targeting HER2 in Nuclear Medicine for Imaging and Therapy. Mol Imaging 2018, 17, 1536012117745386. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Xu, T.; Vorobyeva, A.; Loftenius, A.; Bodenko, V.; Orlova, A.; Frejd, F.Y.; Tolmachev, V. Radionuclide Therapy of HER2-Expressing Xenografts Using [(177)Lu]Lu-ABY-027 Affibody Molecule Alone and in Combination with Trastuzumab. Cancers (Basel) 2023, 15, 2409. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
ABY-025 binds with picomolar affinity to the extracellular domain of HER2 (HER2ECD), an epitope distinct to the binding sites of therapeutic antibodies trastuzumab and pertuzumab. Fab: fragment antigen binding region of a monoclonal antibody.
Figure 1.
ABY-025 binds with picomolar affinity to the extracellular domain of HER2 (HER2ECD), an epitope distinct to the binding sites of therapeutic antibodies trastuzumab and pertuzumab. Fab: fragment antigen binding region of a monoclonal antibody.
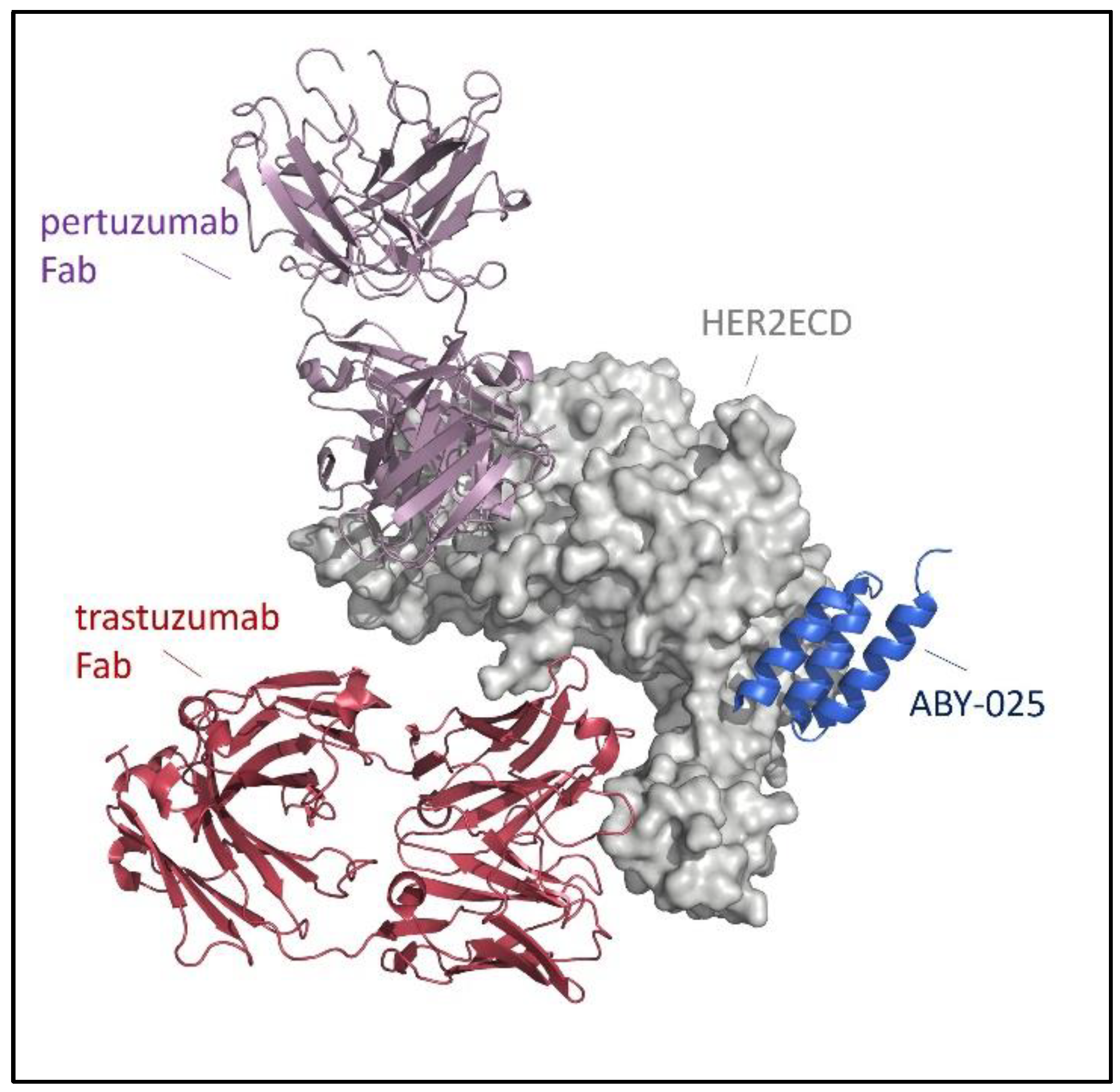
Figure 2.
Representative images of PET scans conducted in the Affibody-3 trial (NCT03655353) by Sörensen and colleagues. A) (pt3): Breast cancer (BC) patient with biopsy confirmed HER2-positive mediastinal metastasis (biopsy results: IHC2+/ISH+), [68Ga]Ga-ABY-025 uptake at baseline was low (SUVmax = 5.2). No metabolic response was observed after receiving 2 cycles of HER2-targeted therapy*. B) (pt5): BC patient with biopsy confirmed HER2-positive lung metastasis (biopsy results: IHC3+/ISH-) with low [68Ga]Ga-ABY-025 uptake at baseline (SUVmax = 5.4). Patient had disease progression despite receiving 3 cycles of HER2-targeted therapy*. C) (pt15): BC patient with biopsy confirmed HER2-negative liver metastasis (biopsy results: IHC1+/ISH-). [68Ga]Ga-ABY-025 PET showed high uptake in tumor lesion (SUVmax = 22.5) and the patient showed good metabolic response after 2 cycles of HER2-targeted therapy*. *Therapies received under study period: Patient 3: epirubicin + cyclophosphamide + trastuzumab + pertuzumab; Patient 5: trastuzumab emtansine (FDG-PET after 3 cycles in this patient); Patient 15: docetaxel + trastuzumab + pertuzumab.
Figure 2.
Representative images of PET scans conducted in the Affibody-3 trial (NCT03655353) by Sörensen and colleagues. A) (pt3): Breast cancer (BC) patient with biopsy confirmed HER2-positive mediastinal metastasis (biopsy results: IHC2+/ISH+), [68Ga]Ga-ABY-025 uptake at baseline was low (SUVmax = 5.2). No metabolic response was observed after receiving 2 cycles of HER2-targeted therapy*. B) (pt5): BC patient with biopsy confirmed HER2-positive lung metastasis (biopsy results: IHC3+/ISH-) with low [68Ga]Ga-ABY-025 uptake at baseline (SUVmax = 5.4). Patient had disease progression despite receiving 3 cycles of HER2-targeted therapy*. C) (pt15): BC patient with biopsy confirmed HER2-negative liver metastasis (biopsy results: IHC1+/ISH-). [68Ga]Ga-ABY-025 PET showed high uptake in tumor lesion (SUVmax = 22.5) and the patient showed good metabolic response after 2 cycles of HER2-targeted therapy*. *Therapies received under study period: Patient 3: epirubicin + cyclophosphamide + trastuzumab + pertuzumab; Patient 5: trastuzumab emtansine (FDG-PET after 3 cycles in this patient); Patient 15: docetaxel + trastuzumab + pertuzumab.
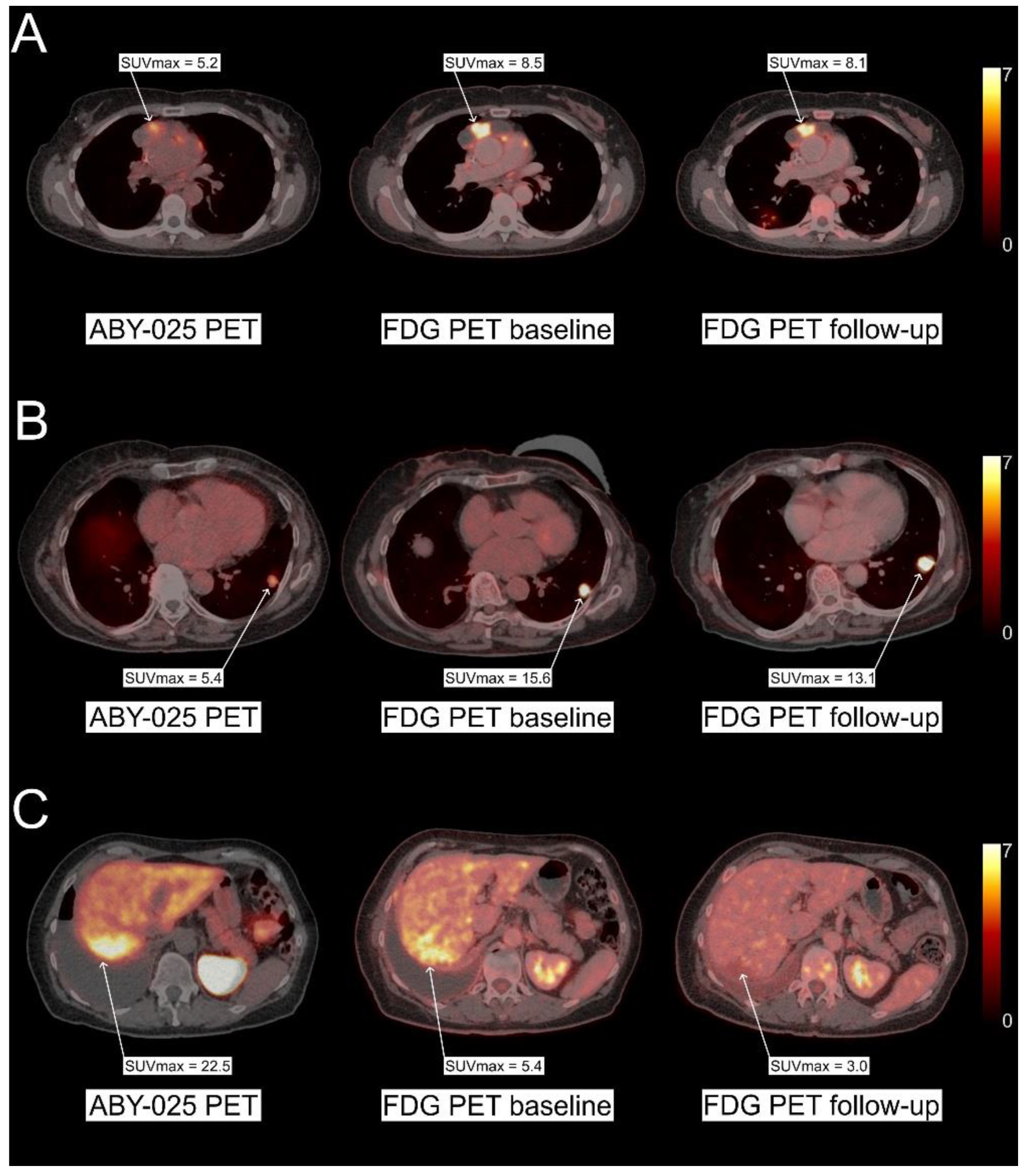
Figure 3.
Overview of the [68Ga]Ga-ABY-025 PET imaging results of all 10 breast cancer patients included in the HER2-low pilot trial visualizing disease heterogeneity. Per patient, the biopsied lesion is depicted with lesion size, SUVmax and organ of origin. The median SUVmax of all the tumor lesions present on HER2-PET are given by a black line. The coloured bars represent the IHC results. Image from Altena et al. J Nucl Med 2024.
Figure 3.
Overview of the [68Ga]Ga-ABY-025 PET imaging results of all 10 breast cancer patients included in the HER2-low pilot trial visualizing disease heterogeneity. Per patient, the biopsied lesion is depicted with lesion size, SUVmax and organ of origin. The median SUVmax of all the tumor lesions present on HER2-PET are given by a black line. The coloured bars represent the IHC results. Image from Altena et al. J Nucl Med 2024.
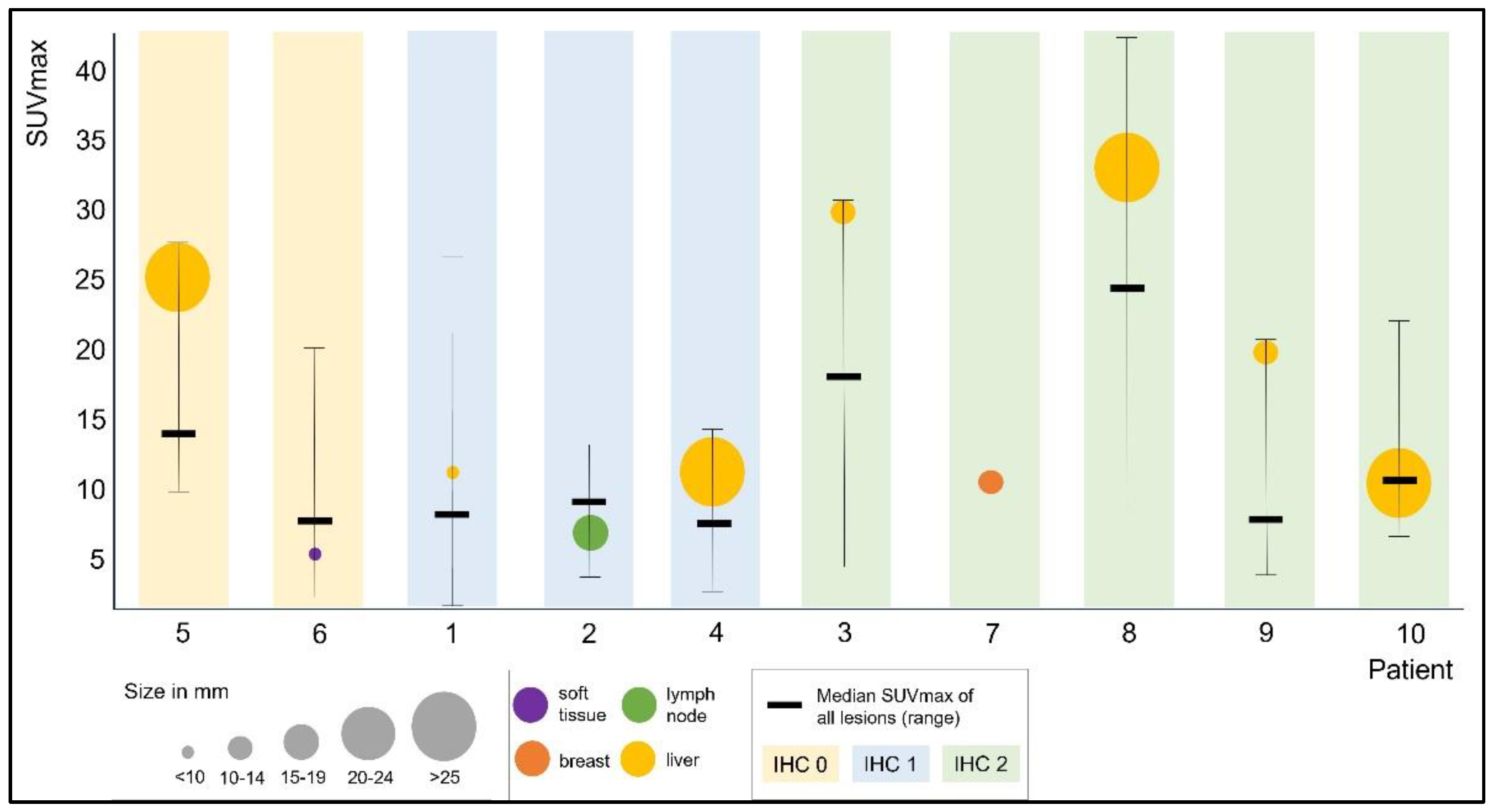
Figure 4.
Representative images from the patient with SUVmax of 24.9 and HER2 IHC 0 in biopsy. The metastatic lesion in segment 3 in the liver shows inhomogeneous intravenous contrast uptake due to central necrosis (arrows). The inhomogeneous nature of the metastatic lesion was verified under ultrasound prior to biopsy. The liver biopsy in the lower right panel shows a HER2 IHC0 status. Image from Altena et al. J Nucl Med 2024.
Figure 4.
Representative images from the patient with SUVmax of 24.9 and HER2 IHC 0 in biopsy. The metastatic lesion in segment 3 in the liver shows inhomogeneous intravenous contrast uptake due to central necrosis (arrows). The inhomogeneous nature of the metastatic lesion was verified under ultrasound prior to biopsy. The liver biopsy in the lower right panel shows a HER2 IHC0 status. Image from Altena et al. J Nucl Med 2024.
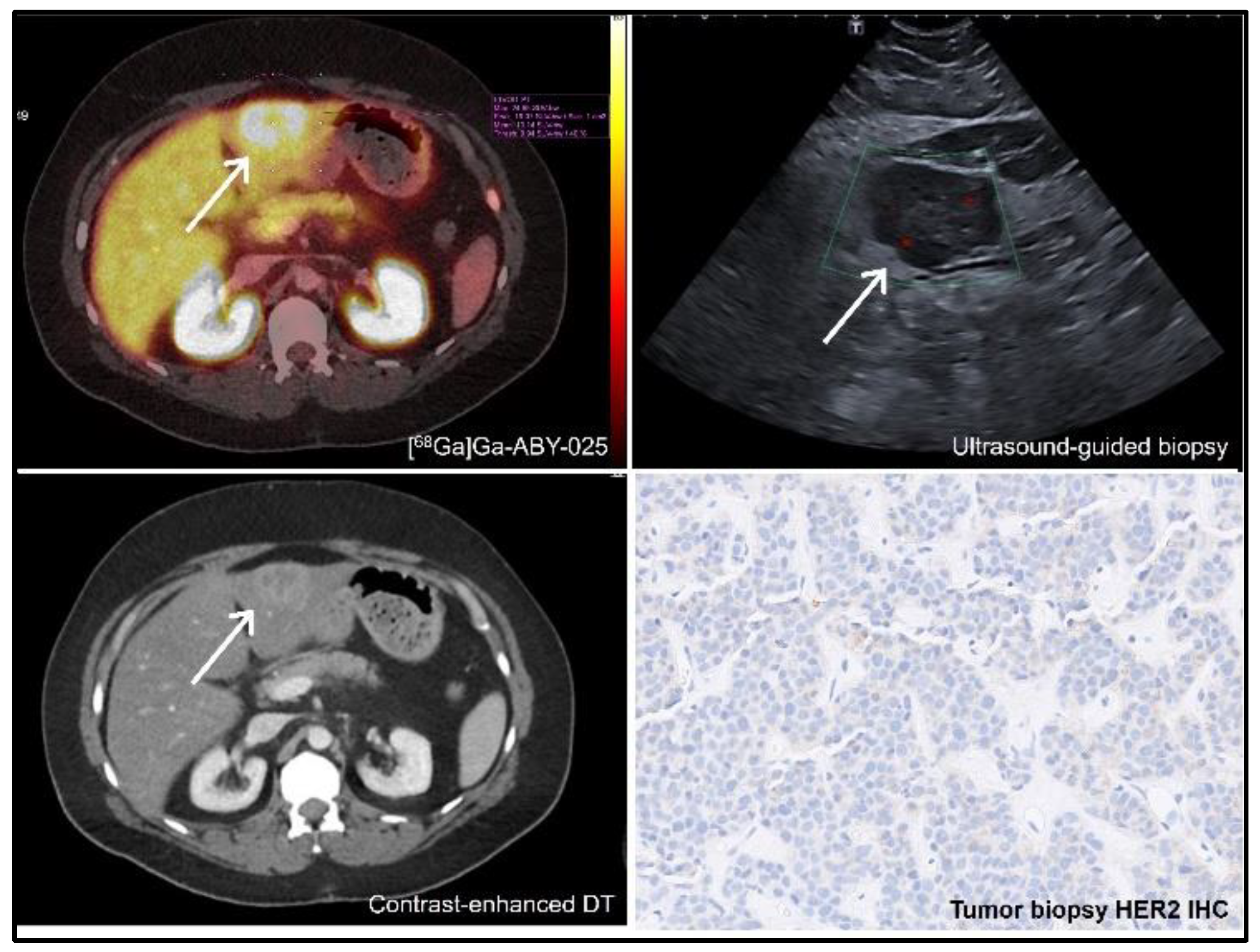
Figure 5.
Representative SPECT images (MIP) at 2, 4, and 6 h after injection of [99mTc]Tc-ZHER2:4107 (Patient 16) visualizing primary breast cancer. Kidney and liver are the normal organs with highest tracer uptake. Imaging was performed after injection of the optimal defined peptide mass of 1000 μg [99mTc]Tc-ZHER2:4107 that showed best discrimination between HER2+ and HER2- tumor lesions. Linear SUV scale from 0 to 15. From Bragina et al. 2023. Phase I clinical evaluation of 99mTc-labeled Affibody molecule for imaging HER2 expression in breast cancer. Image from Bragina et al. Theranostics 2023.
Figure 5.
Representative SPECT images (MIP) at 2, 4, and 6 h after injection of [99mTc]Tc-ZHER2:4107 (Patient 16) visualizing primary breast cancer. Kidney and liver are the normal organs with highest tracer uptake. Imaging was performed after injection of the optimal defined peptide mass of 1000 μg [99mTc]Tc-ZHER2:4107 that showed best discrimination between HER2+ and HER2- tumor lesions. Linear SUV scale from 0 to 15. From Bragina et al. 2023. Phase I clinical evaluation of 99mTc-labeled Affibody molecule for imaging HER2 expression in breast cancer. Image from Bragina et al. Theranostics 2023.
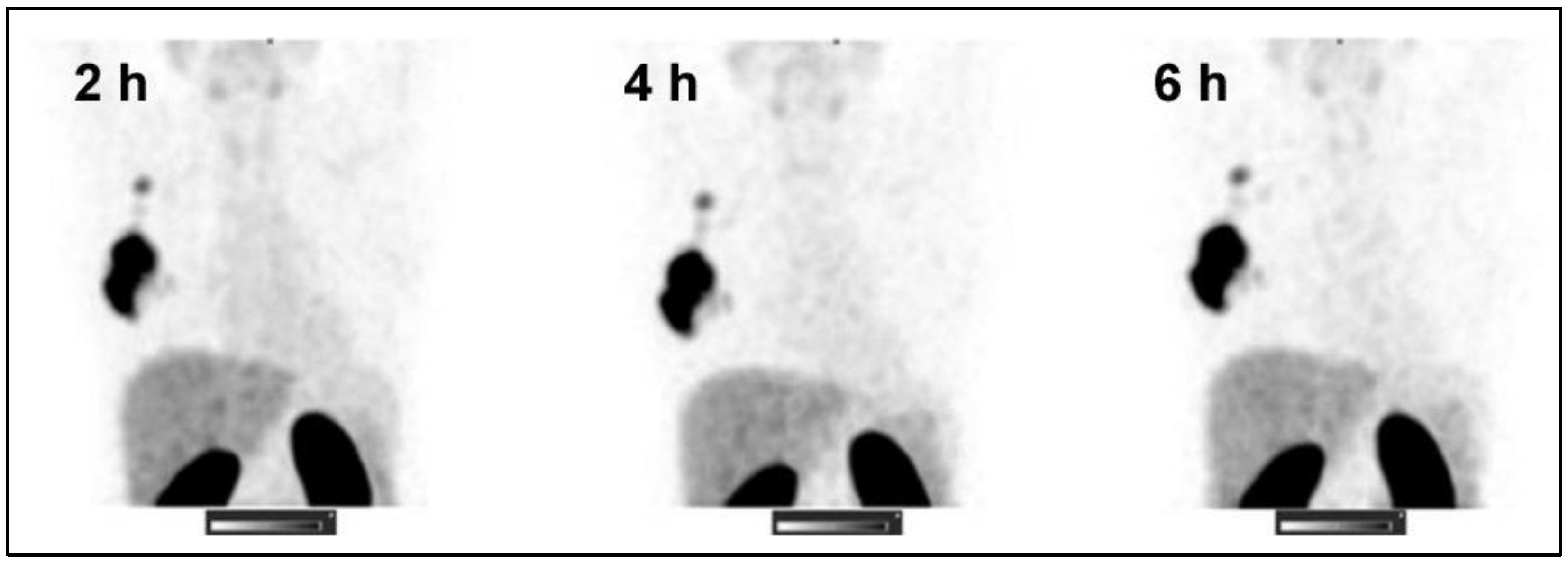
Table 1.
FDA approved HER2-targeted therapeutics.
| Name | Drug type | Indication |
|---|---|---|
| trastuzumab (Herceptin®) | mAB | HER2+ BC (adjuvant, metastatic); HER2+ GC (metastatic) |
| pertuzumab (Perjeta®) | mAB | HER2+ BC (metastatic, locally advanced, inflammatory, or early stage) |
| ado-trastuzumab emtansine (Kadcyla®) | ADC | HER2+ BC (metastatic or early stage) |
| trastuzumab deruxtecan (Enhertu®) | ADC | HER2+ BC (unresectable or metastatic); HER2-mutant NSCLC; HER2+ GC and GEJ carcinoma (locally advanced or metastatic); HER2-low BC (metastatic) |
| margetuximab (Margenza®) | mAB | metastatic HER2+ BC |
| tucatinib (TUKYSA®) | TKI | HER2+ BC (locally advanced or metastatic) |
| lapatinib (Tykerb®) | TKI | HER2+ BC (advanced or metastatic; HR+ metastatic) |
| neratinib (NERLYNX®) | TKI | HER2+ BC (early stage or metastatic) |
Abbreviations: ADC: antibody-drug conjugate; mAB: monoclonal antibody; TKI: tyrosine kinase inhibitor (small molecule); BC: breast cancer; GC: gastric cancer; HR: hormone receptor; NSCLC: non-small cell lung cancer; GEJ: gastroesophageal junction.
Table 2.
Selected FDA or EMA approved PET and SPECT imaging tracers for oncology.
| Name | approval | Active ingredient(s) | Indication |
|---|---|---|---|
| DetectNETTM | FDA | 64Cu dotatate | SSTR+ neuroendocrine tumors |
| NETSPOT® | FDA | 68Ga dotatate | SSTR+ neuroendocrine tumors |
| SomaKit TOC® | EMA | edotreotide (kit for radiolabeling with gallium-68) | SSTR+ neuroendocrine tumors |
| OctreoscanTM | FDA and EU national approvals | pentetreotide (kit for radiolabeling with indium-111) | SSTR+ neuroendocrine tumors |
| LYMPHOSEEK® | FDA and EMA | tilmanocept (kit for radiolabeling with technetium-99m) | Guiding sentinel lymph node biopsy in cancer patients; locate tumor draining lymph nodes in adults and children. |
| LOCAMETZ® | FDA and EMA | gozetotide (kit for radiolabeling with gallium-68) | PSMA+ prostate cancer |
| Illuccix® | FDA | gozetotide (kit for radiolabeling with gallium-68) | PSMA+ prostate cancer |
| PYLARIFY® / PYLCLARY® | FDA and EMA | piflufolastat F-18 | PSMA+ prostate cancer |
| CeriannaTM * | FDA | fluoroestradiol F-18 | ER+ breast cancer |
Abbreviations: EMA: European Medicines Agency; ER: estrogen receptor; FDA: Food and Drug Administration; SSTR: somatostatin receptor; PSMA: prostate-specific membrane antigen; *also known as ESTROTEP in Europe.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



