Submitted:
18 April 2024
Posted:
19 April 2024
You are already at the latest version
Abstract
Drug-induced liver disease represents one of the main problems in the therapeutic field. As with most pathologies, also in this case various risk factors can be recognised, such as age, sex, but also the gut microbiota. Therefore all drugs on the market can, in fact, cause hepatotoxicity of varying degrees. Drugs used in the treatment of IBD can also cause these adverse effects and even lead to DILI. In this review, the various classes of drugs used in the treatment of IBD were taken into consideration and the various adverse effects on the liver were illustrated. In particular, a major role has emerged regarding hepatotoxicity of immunosuppressants. Biological drugs, however, seem to be responsible for these complications to a much lesser extent.
Keywords:
Drug-induced liver injury
; cholestasis
; hepatotoxicity
; liver failure.
1. Introduction
Inflammatory bowel diseases (IBD) are relatively widespread intestinal pathologies with a constantly increasing incidence. Over the decades, several studies have been conducted aimed at developing new pharmacological therapies for these pathologies. To date, commonly used drugs include aminosalicylates, corticosteroids, immunosuppressants, biologics and immunomodulators [1]. In patients with IBD, anomalies in the biohumoral parameters of liver function can be found in percentages ranging from 3% to 50% of cases. The liver diseases that can develop in these cases include hepatic steatosis, primary sclerosing cholangitis (PSC), cholelithiasis, autoimmune hepatitis, cirrhosis, cholangiocarcinoma, and drug induced liver injury (DILI) [2,3].
Today, DILI represents the most common cause of acute liver failure (ALF). It is characterized by an increase in transaminases even above 5 times the normal value, appearance of jaundice, and liver-related coagulopathy [4]. DILI can be direct, indirect or idiosyncratic (Figure 1) (Table 1).
The first case occurs when direct hepatotoxicity occurs from agents intrinsically toxic to the liver. The indirect form is due to the action of the drug and not to its toxic formulation. Idiosyncratic DILI is associated with minimally or not at all toxic drugs and is therefore most likely related to the metabolic characteristics of the liver itself [5].
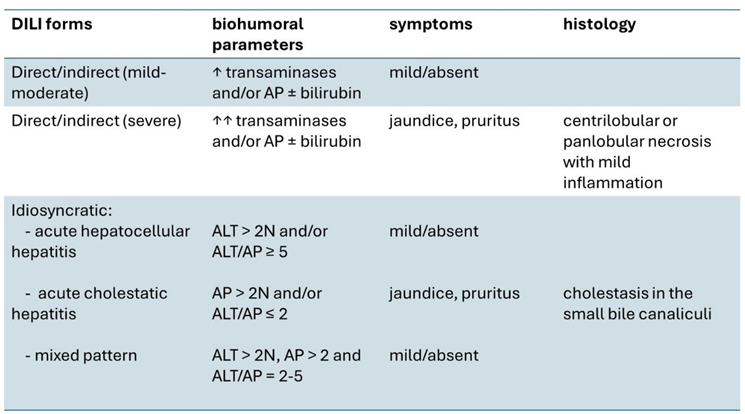
In direct and indirect liver injury, increases in transaminases and/or alkaline phosphatase are generally observed without hyperbilirubinemia. In these cases, symptoms may be mild or even absent [6]. Serum levels of liver function tests decrease when the drug is stopped or the dose is reduced. In some cases these alterations can also be transient and resolve spontaneously without stopping the drug, as an adaptation occurs. If this does not happen and the drug is continued, the damage progresses and jaundice and symptoms may also appear [5]. In severe cases of direct liver injury, acute hepatic necrosis occurs. In particular, histological examination will reveal a centrilobular or panlobular necrosis with mild inflammation, a pattern similar to that of ischemic hepatitis. This condition can also be fatal [7].
The idiosyncratic form is classified into three groups based on serum alanine aminotransferase (ALT) and alkaline phosphatase (AP) values: “acute hepatocellular hepatitis”, if ALT > 2 N or by an ALT⁄AP ≥ 5; “acute cholestatic hepatitis”, with isolated elevation of AP > 2 N or an ALT⁄AP ≤ 2, and “mixed pattern”, defined by simultaneous presentation of both ALT > 2 N and elevation of AP and ALT/AP ratio between 2 and 5 [8].
Idiosyncratic damage associated with acute hepatocellular hepatitis is similar to acute hepatitis of viral origin. Conspicuous increases in transaminases will be observed, while alkaline phosphatase tends to increase to a lesser extent [9].
Acute cholestatic hepatitis is characterized by prominent symptoms of pruritus, jaundice, and moderate-to-severe elevations in AP levels. This form is usually self-limiting. At histological level, lesions of the bile duct can be observed cholestasis in the small bile canaliculi [10].
Finally, the idiosyncratic mixed form is determined by substances that cause both hepatocellular damage and cholestasis. This is the type of damage with better outcomes, which rarely lead to liver failure [11].
Over the last few years, any factors that may be associated with a greater susceptibility towards the development of DILI have been evaluated. For example, some studies have highlighted a higher prevalence of DILI in women (59% women versus 41% men). This is because, for example, there are important differences in various aspects of the pharmacokinetics or pharmacodynamics of drugs between men and women. But not only that, hormones or the immune system can also influence reactions to some drugs [12]
However, the elderly have an almost threefold increase in the incidence of DILI. This has been attributed to the high amount of drugs taken by elderly patients [13].
Another factor that can influence a hepatic adverse drug event is represented by the gut microbiota. The bacteria present in the intestine can, in fact, interfere with the metabolism of drugs and it can, in certain cases, cause an increase in the toxicity of these molecules even at therapeutic doses [14].
For example, it emerged that the Firmicutes/Bacteroidetes ratio is high in subjects who develop DILI, suggesting a probable pathogenetic role of Firmicutes. Instead, other species, such as those of the genus Lactobacillus, were found to be hepatoprotective [15]
Indirect evidence on the influence determined by the gut microbiota is represented by the effectiveness of some probiotics in reducing liver damage. this action is carried out both by maintaining the integrity of the intestinal barrier and by stimulating the secretion of short-chain fatty acids (SCFA) [16].
2. Compounds of 5-aminosalicylic Acid
Among the compounds of 5-aminosalicylic acid (5-ASA) there is sulfasalazine, the use of which has been progressively reduced due to the severe associated adverse effects, including acute hepatitis [17]. In fact, sulfasalazine contains both 5-aminosalicylic acid and sulfapyridine and the latter molecule is responsible for the toxic effects. In particular, it causes a hepatic hypersensitivity reaction which can evolve into various forms of liver damage: granulomatous hepatitis, cholestatic liver disease and, in rare cases, even acute liver failure [18]. A study conducted in mice identified several pathways involved in sulfasalazine-induced liver damage. These include redox processes, the cytochrome p450 pathway, glutathione metabolism, and the cytochrome p450 2C55 pathway [cyp2c55] [19].
Mesalazine is the 5-ASA compound most commonly prescribed to patients with ulcerative colitis (UC) or Crohn's disease for the maintenance of remission and in association with corticosteroids for the induction of remission in mild-moderate active forms. The incidence of mesalazine-associated hepatotoxicity remains low [20,21]. Adverse hepatic effects associated with mesalazine range from a mild asymptomatic increase in hepatic cytolysis rates to idiosyncratic cholestasis and in most cases these events resolve rapidly with discontinuation of the drug [22]. In 0-4% an increase in liver enzymes was detected. In a randomized controlled trial it emerged that 1% of patients taking the lowest daily dosage of mesalazine (1.5 g/day) experienced hypertransaminasemia, which resolved after discontinuation of the drug. Then, upon resumption of treatment 4 weeks later, liver cytolysis enzymes increased again [23].
Serious hepatic complications from 5-ASA are extremely rare in the literature to date. A recent case report by Watanabe et al. presented the case of a patient with UC who, on the 98th day of therapy with mesalazine at a dosage of 2.4 g/day, developed adverse events. In particular, an increase > 5 times the norm of transaminases and a significant increase in cholestasis indices were found. Once 5-ASA was discontinued and all other possible causes of DILI were excluded, it was possible to define 5-ASA-induced DILI and after 24 days from drug suspension a normalization of all liver enzymes was observed [24].
Several studies suggest monitoring liver function tests before and during treatment with sulfasalazine or mesalazine, to diagnose any acute events early [3].
3. Immunosuppressants
Thiopurines used in the treatment of IBD include azathioprine (AZA) and 6-mercaptopurine (MP).
Azathioprine is another immunosuppressant used in the treatment of IBD, particularly Crohn's disease. It has been associated with several forms of hepatotoxicity. This drug is a purine analog that interferes with the cell cycle and inhibits the normal function of leukocytes. In this way its immunosuppressive action is implemented. MP is the active metabolite of azathioprine and is further metabolised to active metabolites including 6-methylmercaptopurine, thioguanine, 6-thioguanine nucleosides and 6-methylmercaptopurine nucleosides [25]. Among the adverse events of these drugs is hepatotoxicity, which can occur in approximately 10% of patients. It does not appear to be dose-related as it can also be observed in patients with low concentrations of 6-methylmercaptopurine [26].
An important step in AZA metabolism includes the involvement of glutathione in hepatocytes, with conversion of AZA to MP and methylnitroimidazole by glutathione S-transferase. Therefore, in patients in whom there is high activity of the hepatic glutathione S-transferase enzyme there is an increased risk of hepatotoxicity induced by the excessive release of methyl-nitroimidazole and MP [27]. The various expressions of hepatotoxicity caused by this category of drugs vary from simple asymptomatic increases in transaminases to real forms of acute hepatitis which can be mainly cholestatic or mixed. Vascular endothelial lesions, peliosis hepatis and sinusoidal syndrome may also be observed expansion [28].
In a study of nearly 4,000 IBD patients, Chaparro et al. have highlighted that hepatotoxicity is one of the most common adverse events of thiopurines, with a frequency of 4% [29].
The high incidence of hepatotoxicity of thiopurines is also demonstrated by the higher rates of dose reduction or interruption of therapy compared to those of other drugs used in IBD. Additionally, patients treated with 6MP had higher dose reduction rates than those treated with AZA, although discontinuation rates were similar in the two groups [30]. Thiopurine-associated liver damage has been related to the activity of thiopurine S-methyltransferase (TPMT), an enzyme involved in the metabolism of both 6-MP and azathioprine [3,22]. In fact, the presence of genetic polymorphisms can decrease the activity level of this enzyme resulting in variable levels of thiopurine metabolites influencing the degree of hepatotoxicity [31].
In several cases, in the early stages of treatment, minimal and transient increases in transaminases can be observed, without liver damage. In other cases, azathioprine can also cause the onset of acute liver damage of a cholestatic type, which manifests itself with jaundice, fatigue, increased transaminases and alkaline phosphatase. This pathological condition usually resolves with discontinuation of azathioprine [32].
The mechanism of hepatotoxicity induced by this drug is not fully known. Azathioprine is a prodrug that is metabolized to 6-mercaptopurine (6-MP). Subsequently, 6-MP can undergo three different metabolic pathways. The first consists of the methylation of 6-MP into 6-methylmercaptopurine, a reaction catalyzed by thiopurine methyltransferase (TPMT). The second pathway involves the conversion of 6-MP to 6-thioinosine 5-monophosphate via hypoxanthine guanine phosphoribosyl transferase and this intermediate is then metabolized in the active nucleotides 6-thioguanine (6-TG). The third pathway consists in the transformation of 6-MP into 6-thiouric acid (6-TA), which is an inactive metabolite, by xanthine oxidase (XO) [33]. It has been observed that some subjects tend to produce more 6-MMP rather than 6-TG and they are more likely to develop hepatotoxicity [34]. The conversion of 6-MP to 6-TA can also be hepatotoxic, as this metabolic pathway is a source of reactive oxygen species (ROS) [33].
Methotrexate (MTX) is a competitive inhibitor of the enzyme dihydrofolate reductase, which participates in the synthesis of purines and pyrimidines, producing antiproliferative and anti-inflammatory effects on cells. It is used in various chronic pathologies with inflammatory pathogenesis, such as rheumatoid arthritis, psoriatic arthritis and also IBD. In fact, it has the aim of inducing and maintaining remission in these types of patients [35]. However, this drug is burdened by several adverse effects that can affect various organs, including the liver. In particular, during long-term therapies with MTX, the accumulation of the polyglutamate metabolite of MTX occurs in the liver cells which, most likely, is responsible for the toxic effects at the liver level [36].
It should be noted that liver damage from MTX occurs more in patients with IBD than in patients with other pathologies. For example, in a study by Fegan et al. it emerged that 17.5% of IBD patients treated with MTX had increased serum aminotransferases [37]. Even Fournier et al. found that 24% of IBD patients developed abnormal liver function with MTX [38]. A similar result was obtained by González-Lama et al., in which at least 20.8% of this type of patients presented liver function abnormalities or even significant liver fibrosis [39]. On the contrary, in various studies the percentage of liver function abnormalities was found to be lower in patients treated with MTX with non-IBD diseases. Lie et al., for example, found an increase in liver enzymes in patients with rheumatoid arthritis (RA) of less than 10% [40].
These peculiar differences can be explained by the mechanism of action of the drug. MTX directly inhibits various enzymes involved in folate metabolism, including the dihydrofolate reductase (DHFR) enzyme. Inhibition of the latter can lead to blocking of DNA replication and consequent cell death [41]. In particular, the rs1650697 (C35T) polymorphism was discovered which concerns the promoter of the DHFR gene which appears to have a protective effect against the hepatotoxicity of MTX. This polymorphism appears to be more frequent in subjects with RA than in those with IBD [42,43].
Other genetic polymorphisms that could be responsible for protective or facilitatory effects against the hepatotoxicity of MTX concern another gene that codes for the MTHFR enzyme. This is the A1298C polymorphism which has been found much more frequently in patients with IBD and appears to be associated with a greater hepatotoxic effect of MTHFR [36].
4. Biologic Therapies
Tumor necrosis factor (TNF) is released by T-cells and macrophages and binds to specific receptors that induce multiple immune responses, including the release of inflammatory cytokines and the migration of leukocytes to organs. TNF inhibitors are Infliximab, Adalimumab, Golimumab, and Certolizumab pegol. They antagonize TNF receptors and induce inhibition of immune responses by TNF, thus inducing recovery and maintenance of remission of CD and UC [44]. Generally, the most common manifestation of anti-TNF hepatotoxicity is acute hepatocellular damage, which occurs on average 13 weeks after the start of therapy. More rarely, mild cholestasis has also been observed. The mechanism by which these drugs cause hepatotoxicity is, however, unknown [45].
Infliximab is the first chimeric monoclonal antibody against TNF produced. It is usually dosed at 5 mg/kg or 10 mg/kg and administered intravenously, with induction therapy at 0, 2, 6 and 8 weeks, followed by maintenance therapy with an infusion every 8 weeks [22]. This drug may cause several adverse effects, including liver damage, which can be represented by a hepatocellular pattern or an autoimmune type [46].
In the autoimmune pattern, positivity for autoantibodies (anti-nucleus antibodies, anti-smooth muscle antibodies, etc.) can be observed, while from a histological point of view the picture is that of interface hepatitis [47].
Immune-mediated liver injury is the most frequent and severe form of Infliximab-induced liver disease. However, direct hepatotoxicity is generally transient and asymptomatic. Severe hypertransaminasemia is highly rare and occurs primarily in individuals taking other hepatotoxic drugs or who already have liver disease at the time of initiation of treatment with Infliximab [48]. This is the case of a young 25-year-old patient undergoing therapy with Infliximab 400 mg IV every 8 weeks and Methotrexate 10 mg once a week. In fact, two months after starting treatment, the woman developed anorexia and weight loss with subsequent suspension of Methotrexate. A few weeks later he then developed pruritus, jaundice and asterixis. Laboratory tests and liver biopsy made it possible to diagnose infliximab-related AIH. In this specific case, the patient experienced a progressive deterioration of her clinical conditions which made an orthotopic liver transplant necessary [49].
Indeed, in a retrospective case-control study of patients with IBD without concomitant liver disease, approximately one third of patients experienced ALT elevations, which however resolved spontaneously in most cases. These biochemical alterations, however, were not significantly associated with the use of infliximab, so it is reasonable to assume that the presence of liver disease prior to the start of therapy with Infliximab could significantly influence the outcome of these patients [50].
Infliximab therapy rarely causes DILI. In most cases only biochemical alterations are present. In a study by Worland et al conducted on 157 patients with IBD treated with Infliximab, one third of them had liver biochemical abnormalities, while only one met the RUCAM criteria for DILI [51]. Infliximab-induced DILI usually develops after several infusions, with an average latency of 14-18 weeks after induction [52].
CT-P13 (Janssen Biotech, Horsham, PA, USA) is a biosimilar drug of anti-TNF alpha Infliximab and has been approved by the European Medicines Agency (EMA) and the US Food and Drug Administration (FDA). Biosimilars do not present significant differences in terms of safety and efficacy compared to the original molecules [53].
Some rare cases of DILI have also been reported for this biosimilar. The first published case involved a 23-year-old woman with CD, who developed DILI after switching from the original IFX to the biosimilar IFX CT-P13. Liver biopsy showed pericentral canalicular cholestasis, with no other findings related to steatosis or sclerosing cholangitis. CT-P13 was discontinued and the patient improved 10 weeks later. The subsequent switch to original Infliximab did not lead to alterations in liver function indices [54].
A similar event was reported by Zachau et al. about a 42 year old patient suffering from Crohn's. Also in his case, the suspension of the biosimilar resulted in an improvement in the clinical picture until normal transaminase values and cholestasis indices were restored and the subsequent switch to the original Infliximab did not cause the appearance of symptoms or biohumoral alterations [53].
Adalimumab is a human monoclonal anti-TNF-alpha antibody that is administered subcutaneously, usually every 2 weeks in the maintenance phase of remission. Compared to infliximab, less hepatotoxicity was detected Adalimumab. Koller et al. observed increases no greater than 2 times normal in transaminases in 135 treated IBD patients Adalimumab [55]. In cases of liver disease related to Adalimumab, it was seen that this resolved without relics when the drug was suspended [56].
Anti-integrin antibodies are molecules capable of blocking integrins, which are surface proteins involved in the migration of leukocytes in the intestinal mucosa, one of the events responsible for the onset of chronic inflammation in the gut [57].
Vedolizumab (VDZ) is a humanized antibody directed against α4β7 integrin. Its efficacy has been demonstrated both in several clinical studies and is approved for the induction and maintenance of remission of moderate-severe ulcerative colitis (UC) and Crohn's disease [58]. Some cases of DILI due to vedolizumab have been reported, but it is a transitory condition that ceases once the drug is discontinued [59]. The final analysis of the GEMINI LTS study found that only 3.2% of patients with UC and 4.7% of MC patients developed a damage to the liver, and in any case in none of these cases was it necessary suspend Vedolizumab [60].
5. Conclusions
Drugs used in the treatment of IBD can cause hepatotoxicity and lead to DILI. In particular, immunosuppressants are more involved in adverse effects on the liver. Biological drugs, however, are responsible for these complications to a much lesser extent. The only exception is represented by anti-TNFs, in particular Infliximab, which are still burdened by a non-negligible percentage of patients who develop hepatotoxicity. The other categories, such as anti-integrin antibodies appear to be better tolerated. For this reason, as well as for the proven effectiveness, it is reasonable to think that in the near future they may be considered first choice drugs in IBD.
Author Contributions
Roberto CATANZARO: drafting the review; Francesco MAROTTA: drafting the review; Azam YAZDANI: bibliographic research and figure creation; Morena SCIUTO: drafting the review and table creation
Conflicts of Interest
None of the authors have conflicts of interest.
References
- Cai, Z.; Wang, S.; Li, J. Treatment of inflammatory bowel disease: a comprehensive review. Front. Med. (Lausanne). 2021, 20, 8:765474. [CrossRef]
- Khan, N.; Abbas, A.M.; Whang, N.; Balart, L.A.; Bazzano, L.A.; Kelly, T.N. Incidence of liver toxicity in inflammatory bowel disease patients treated with methotrexate: a meta-analysis of clinical trials. Inflamm. Bowel. Dis. 2012, 18, 359–67. [Google Scholar] [CrossRef]
- Núñez, F.P.; Quera, R.; Bay, C.; Castro, F.; Mezzano, G. Drug-Induced Liver Injury used in the treatment of inflammatory bowel disease. J. Crohns. Colitis. 2022, 16, 1168–76. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines on the management of acute (fulminant) liver failure. J. Hepatol. 2017, 66, 1047-81.
- Hoofnagle, J.H.; Björnsson, E.S. Drug-Induced Liver Injury - Types and Phenotypes. N. Engl. J. Med. 2019, 381, 264–73. [Google Scholar] [CrossRef]
- Navarro, V.J.; Senior, J.R. Drug-related hepatotoxicity. N. Engl. J. Med. 2006, 354, 731–9. [Google Scholar] [CrossRef]
- Fyfe, B.; Zaldana, F.; Liu, C. The pathology of acute liver failure. Clin. Liver Dis. 2018, 22, 257–68. [Google Scholar] [CrossRef]
- Bermejo, F.; López-Sanromán, A.; Algaba, A.; Van-Domselaar, M.; Gisbert, J.P.; García-Garzón, S.; Garrido, E.; Piqueras, B.; De La Poza, G.; Guerra, I. Mercaptopurine rescue after azathioprine-induced liver injury in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2010, 31, 120–4. [Google Scholar] [CrossRef]
- Chalasani, N.; Bonkovsky, H.L.; Fontana, R.; Lee, W.; Stolz, A.; Talwalkar, J.K.; Reddy, R.; Watkins, P.B.; Navarro, V.; Barnhart, H.; et al. Features and outcomes of 889 patients with drug-induced liver injury: the DILIN Prospective Study. Gastroenterology 2015, 148, 1340–52. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Chalasani, N.P.; Lee, W.M.; Fontana, R.J.; Bonkovsky, H.L.; Watkins, P.B.; Hayashi, P.H.; Davern, T.J.; Navarro, V.; Reddy, R.; et al. Hepatic histological findings in suspected drug-induced liver injury: systematic evaluation and clinical associations. Hepatology 2014, 59, 661–70. [Google Scholar] [CrossRef]
- Martinez, M.A.; Vuppalanchi, R.; Fontana, R.J.; Stolz, A.; Kleiner, D.E.; Hayashi, P.H.; Gu, J.; Hoofnagle, J.H.; Chalasani, N. Clinical and histologic features of azithromycin-induced liver injury. Clin. Gastroenterol. Hepatol. 2015, 13, 369–76. [Google Scholar] [CrossRef]
- Katarey, D.; Verma, S. Drug-induced liver injury. Clin. Med. 2016, 16, s104–s109. [Google Scholar] [CrossRef]
- Chalasani, N.; Bonkovsky, H.L. Fontana, R.; Lee, W.; Stolz, A.; Talwalkar, J.; Reddy, K.R.; Watkins, P.B.; Navarro, V.; Barnhartet, H.; al. Features and outcomes of 899 patients with drug-induced liver injury: the DILIN prospective study. Gastroenterology 2015, 148, 1340–52. [Google Scholar] [CrossRef]
- Sciuto, M.; Catanzaro, R. Composition of gut microbiota and its correlations with neurological, intestinal, cardiovascular and metabolic diseases. Acta Microbiol. Immunol. Hung. 2023, 70, 259–71. [Google Scholar] [CrossRef]
- Chu, H.K.; Ai, Y.; Cheng, Z.L.; Yang, L.; Hou, X.H. Contribution of gut microbiota to drug-induced liver injury. Hepatobiliary Pancreat. Dis. Int. 2023, 22, 458–65. [Google Scholar] [CrossRef]
- Wu, W.; Lv, L.; Shi, D.; Ye, J.; Fang, D.; Guo, F.; Yating, Li.; He, X.; Li, L. Protective effect of Akkermansia muciniphila against immune-mediated liver injury in a mouse model. Front. Microbiol. 2017, 8:1804. [CrossRef]
- Heidari, R.; Rasti, M.; Shirazi Yeganeh, B.; Niknahad, H.; Saeedi, A.; Najibi, A. Sulfasalazine-induced renal and hepatic injury in rats and the protective role of taurine. Bioimpacts 2016, 6, 3–8. [Google Scholar] [CrossRef]
- Núñez, F.P.; Castro, F.; Mezzano, G.; Quera, R.; Diaz, D.; Castro, L. Hepatobiliary manifestations in inflammatory bowel disease: a practical approach. World J. Hepatol. 2022, 14, 319–37. [Google Scholar] [CrossRef]
- Sehgal, P.; Colombel, J.F.; Aboubakr, A.; Narula, N. Systematic review: safety of mesalazine in ulcerative colitis. Aliment. Pharmacol. Ther. 2018, 47, 1597–609. [Google Scholar] [CrossRef]
- D'Haens, G.; Safroneeva, E.; Thorne, H.; Laoun, R. Assessing the clinical and endoscopic efficacy of extended treatment duration with different doses of mesalazine for mild-to-moderate ulcerative colitis beyond 8 weeks of induction. Inflamm. Intest. Dis. 2023, 8, 51–9. [Google Scholar] [CrossRef]
- Shen, M.; Shi, Y.; Ge, Z.; Qian, J. Effects of mesalamine combined with live combined Bifidobacterium, Lactobacillus and Enterococcus capsules on intestinal mucosa barrier function and intestinal microbiota in mildly active Crohn's disease patients. J. Invest. Surg. 2024, 37, 2297565. [Google Scholar] [CrossRef]
- Barnhill, M.S.; Steinberg, J.M.; Jennings, J.J.; Lewis, J.H. Hepatotoxicty of agents used in the management of Inflammatory Bowel Disease: a 2020 update. Curr. Gastroenterol. Rep. 2020, 22, 47. [Google Scholar] [CrossRef]
- Sehgal, P.; Colombel, J.F.; Aboubakr, A.; Narula, N. Systematic review: safety of mesalazine in ulcerative colitis. Aliment. Pharmacol. Ther. 2018, 47, 1597–609. [Google Scholar] [CrossRef]
- Watanabe, A.; Nishida, T.; Osugi, N.; Kitanaka, T.; Minoura, Y.; Okabe, S.; Sakamoto, N.; Fujii, Y.; Sugimoto, A.; Nakamatsu, D.; et al. 5-Aminosalicylic acid-induced liver injury in a patient with ulcerative colitis: a case report. Case Rep. Gastroenterol. 2024, 18, 39–48. [Google Scholar] [CrossRef]
- Ter Horst, P.; Smolders, E.J.; den Besten, D. Mercaptopurine and metabolites in breast milk. Breastfeed Med. 2020, 15, 277–9. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.R.; Coenen, M.J.H.; Derijks, L.J.J.; Vermeulen, S.H.; van Marrewijk, C.J.; Klungel, O.H.; Scheffer, H.; Franke, B.; Guchelaar, H.J.; de Jong, D.J.; et al. Early prediction of thiopurine-induced hepatotoxicity in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2017, 45, 391–402. [Google Scholar] [CrossRef]
- Stocco, G.; Martelossi, S.; Barabino, A.; Decorti, G., Bartoli, F.; Montico, M.; Gotti, A.; Ventura, A. Glutathione-S-transferase genotypes and the adverse effects of azathioprine in young patients with inflammatory bowel disease. Inflamm. Bowel. Dis. 2007, 13, 57–64. [CrossRef]
- Khokhar, O.S.; Lewis, J.H. Hepatotoxicity of agents used in the management of inflammatory bowel disease. Dig. Dis. 2010, 28, 508–18. [Google Scholar] [CrossRef]
- Chaparro, M.; Ordas, I.; Cabre, E.; Garcia-Sanchez, V.; Bastida, G.; Peñalva, M.; Gomollón, F.; García-Planella, E.; Merino, O.; Gutiérrez, A.; et al. Safety of thiopurine therapy in inflammatory bowel disease: long-term follow-up study of 3931 patients. Inflamm. Bowel. Dis. 2013, 19, 1404–10. [Google Scholar] [CrossRef]
- Broekman, M.; Coenen, M.; Marrewijk, C.; Wanten, G.J.A; Wong, D.R. , Verbeek, A.L.M.; Klungel, O.H.; Hooymans, P.M.; Guchelaar, H.J.; Scheffer, H.; et al. More dose-dependent side effects with mercaptopurine over azathioprine in IBD treatment due to relatively higher dosing. Inflamm. Bowel. Dis. 2017, 23, 1873–81. [Google Scholar] [CrossRef]
- Bjornsson, E.; Gu, J.; Kleiner, D.; Chalasani, N.; Hayashi, P.H; Hoofnagle, J.H.; DILIN Investigators. Azathioprine and 6-mercaptopurine induced liver injury: clinical features and outcomes. J. Clin. Gastroenterol. 2017, 51, 63–9.
- Schwartz, B.; Al-Sabti, R.; Reau, N. Late-onset acute liver injury from Azathioprine. ACG Case Rep. J. 2022, 9, e00847. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Sasaki, E.; Higuchi, S.; Takai, S.; Tsuneyama, K.; Fukami, T.; Nakajima, M.; Yokoi, T. Involvement of oxidative stress and immune- and inflammation-related factors in azathioprine-induced liver injury. Toxicol. Lett. 2014, 224, 215–24. [Google Scholar] [CrossRef] [PubMed]
- Munnig-Schmidt, E.; Zhang, M.; Mulder, C.J.; Barclay, M.L. Late-onset rise of 6-MMP metabolites in IBD patients on azathioprine or mercaptopurine. Inflamm. Bowel Dis. 2018, 24, 892–6. [Google Scholar] [CrossRef]
- Pierik, M.; Rutgeerts, P.; Vlietinck, R.; Vermeire, S. Pharmacogenetics in inflammatory bowel disease. World J. Gastroenterol. 2006, 12, 3657–67. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Y.; Liu, Y.; Zhang, Y.; Ke, Z.; Zhang, Y.; Liu, Y. Patients with IBD receiving Methotrexate are at higher risk of liver injury compared with patients with non-IBD diseases: a meta-analysis and systematic review. Front. Med. (Lausanne). 2021, 8, 774824. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; McDonald, J.W.; Panaccione, R.; Enns, R.A.; Bernstein, C.N.; Ponich, T.P., Bourdages, R.; Macintosh, D.G., Dallaire, C.; Cohenet, A.; al.. Methotrexate in combination with infliximab is no more effective than infliximab alone in patients with Crohn's disease. Gastroenterology. 2014, 146, 681–8.
- Fournier, M.R.; Klein, J.; Minuk, G.Y.; Bernstein, C.N. Changes in liver biochemistry during methotrexate use for inflammatory bowel disease. Am. J. Gastroenterol. 2010, 105:1620–6. [CrossRef]
- Gonzalez-Lama, Y.; Taxonera, C.; Lopez-Sanroman, A.; Perez-Calle, J.L.; Bermejo, F.; Pajares, R.; McNicholl, A.G.; Opio, V.; Mendoza, J.L.; López, P.; et al.. Methotrexate in inflammatory bowel disease: a multicenter retrospective study focused on long-term efficacy and safety. The Madrid experience. Euro. J. Gastroenterol. Hepatol. 2012, 24, 1086–91.
- Lie, E.; van der Heijde, D.; Uhlig, T.; Heiberg, M.S.; Koldingsnes, W.; Rodevand, E.; Kaufmann, C.; Mikkelsen, K.; Kvienet, T.K. Effectiveness and retention rates of methotrexate in psoriatic arthritis in comparison with methotrexate-treated patients with rheumatoid arthritis. Ann. Rheumatic. Dis. 2010, 69, 671–6. [Google Scholar] [CrossRef] [PubMed]
- Askari, B.S.; Krajinovic, M. Dihydrofolate reductase gene variations in susceptibility to disease and treatment outcomes. Curr. Genomics. 2010, 11, 578–83. [Google Scholar] [CrossRef] [PubMed]
- Vejnovic, D.; Milic, V.; Popovic, B.; Damnjanovic, T.; Maksimovic, N.; Bunjevacki, V.; Krajinović, M.; Novaković, I.; Damjanov, N.; Jekić, B. Association of C35T polymorphism in dihydrofolate reductase gene with toxicity of methotrexate in rheumatoid arthritis patients. Expert Opin. Drug. Metab. Toxicol. 2019, 15, 253–7. [Google Scholar] [CrossRef] [PubMed]
- Torres, R.P.; Santos, F.P.; Branco, J.C. Methotrexate: Implications of pharmacogenetics in the treatment of patients with Rheumatoid Arthritis. ARP Rheumatol. 2022, 1, 225–9. [Google Scholar] [PubMed]
- Rundquist, S.; Sachs, M.C.; Eriksson, C.; Olén, O.; Montgomery, S.; Halfvarson, J.; SWIBREG Study Group. Drug survival of anti-TNF agents compared with vedolizumab as a second-line biological treatment in inflammatory bowel disease: results from nationwide Swedish registers. Aliment. Pharmacol. Ther. 2021, 53, 471-83. [CrossRef]
- Ghabril, M.; Bonkovsky, H.L.; Kum, C.; Davern, T.; Hayashi, P.H.; Kleiner, D.E.; Serrano, J.; Rochon, J.; Fontana, R.J.; Bonacini, M.; US Drug-Induced Liver Injury Network. Liver injury from tumor necrosis factor-α antagonists: analysis of thirty-four cases. Clin. Gastroenterol. Hepatol. 2013, 11, 558-64. [CrossRef]
- Björnsson, H.K.; Gudbjornsson, B.; Björnsson, E.S. Infliximab-induced liver injury: clinical phenotypes, autoimmunity and the role of corticosteroid treatment. J. Hepatol. 2022, 76, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Parekh, R.; Kaur, N. Liver injury secondary to anti-TNF-alpha therapy in inflammatory bowel disease: a case series and review of the literature. Case Rep. Gastrointest. Med. 2014, 956463. [Google Scholar] [CrossRef] [PubMed]
- Aby, E.S.; Lake, J.R.; Vaughn, B.P. The impact of biologics for the management of inflammatory bowel disease on liver enzymes. Clin. Liver Dis. (Hoboken). 2020, 16, 212–7. [Google Scholar] [CrossRef] [PubMed]
- Alikhan, M.M.; Mansoor, E.; Satyavada, S.; Greer, K.; Xin, W.; Cohen, S.; Cooper, G.; Katz, J. Infliximab-induced acute liver failure in a patient with Crohn’s disease requiring orthotopic liver transplantation. ACG Case Rep. J. 2021, 8, e00586. [Google Scholar] [CrossRef]
- Parisi, I.; O’Beirne, J.; Rossi, R.; Tsochatzis, E.; Manousou, P.; Theocharidou, E.; Hamilton, M.; Murray, C.; Epstein, O.; Burroughs, A.K. Elevated liver enzymes in inflammatory bowel disease: the role and safety on infliximab. Eur. J. Gastroenterol. Hepatol. 2016, 28, 786–91. [Google Scholar] [CrossRef]
- Worland, T.; Chin, K.L.; van Langenberg, D.; Garg, M.; Nicoll, A. Retrospective study of idiosyncratic drug-induced liver injury from infliximab in an inflammatory bowel disease cohort: the IDLE study. Ann. Gastroenterol. 2020, 33, 162–9. [Google Scholar] [CrossRef]
- Björnsson, E.S.; Gunnarsson, B.I.; Gröndal, G.; Jonasson, J.G.; Einarsdottir, R.; Ludviksson, B.R.; Gudbjörnsson, B.; Olafsson, S. Risk of drug-induced liver injury from tumor necrosis factor antagonists. Clin. Gastroenterol. Hepatol. 2015, 13, 602–8. [Google Scholar] [CrossRef] [PubMed]
- Zachou, M.; Pikramenos, K.; Panoutsakou, M.; Lalla, E.; Androutsakos, T. Infliximab (IFX)-Biosimilar induced Drug-Induced Liver Injury (DILI): a case report. Cureus 2022, 14, e32525. [Google Scholar] [CrossRef]
- Kashima, S.; Sawada, K.; Moriichi, K.; Fujiya, M. A case report of drug-induced liver injury due to the infliximab biosimilar CT-P13 on switching from original infliximab in a patient with Crohn's disease. Ther. Adv. Drug. Saf. 2022, 13, 20420986221100118. [Google Scholar] [CrossRef]
- Koller, T.; Galambosova, M.; Filakovska, S.; Kubincova, M.; Hlavaty, T.; Toth, J.; Krajcovicova, A.; Payer, J. Drug-induced liver injury in inflammatory bowel disease: 1-year prospective observational study. World J. Gastroenterol. 2017, 23, 4102–11. [Google Scholar] [CrossRef]
- Hahn, L.; Asmussen, D.; Benson, J. Drug induced-hepatotoxicity with concurrent use of adalimumab and mesalamine for the treatment of Crohn’s disease. Gastroenterology and Hepatology. 2015, 2, 1–4. [Google Scholar] [CrossRef]
- Park, S.C.; Jeen, Y.T. Anti-integrin therapy for inflammatory bowel disease. World J. Gastroenterol. 2018, 24, 1868–80. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas Saraiva, M.; Ribeiro, T.; Dias, E.; Lopes, J.; Cardoso, H.; Macedo, G. Vedolizumab-induced liver injury. GE Port. J. Gastroenterol. 2020, 28, 410–5. [Google Scholar] [CrossRef]
- Parisi, I.; O’Beirne, J.; Rossi, R.E.; Tsochatzis, E.; Manousou, P.; Theocharidou, E.; Hamilton, M.; Murray, C.; Epstein, O.; Burroughs, A.K. Elevated liver enzymes in inflammatory bowel disease: the role and safety of infliximab. Eur. J. Gastroenterol. Hepatol. 2016, 28, 786–91. [Google Scholar] [CrossRef]
- Colombel, J.F.; Sands, B.E.; Rutgeerts, P.; Sandborn, W.; Danese, S.; D'Haens, G.; Panaccione, R.; Loftus Jr, E.V.; Sankoh, S.; Fox, I. The safety of vedolizumab for ulcerative colitis and Crohn’s disease. Gut. 2017, 66, 839–51. [Google Scholar] [CrossRef]
Figure 1.
three types of drug induced liver injury (DILI).
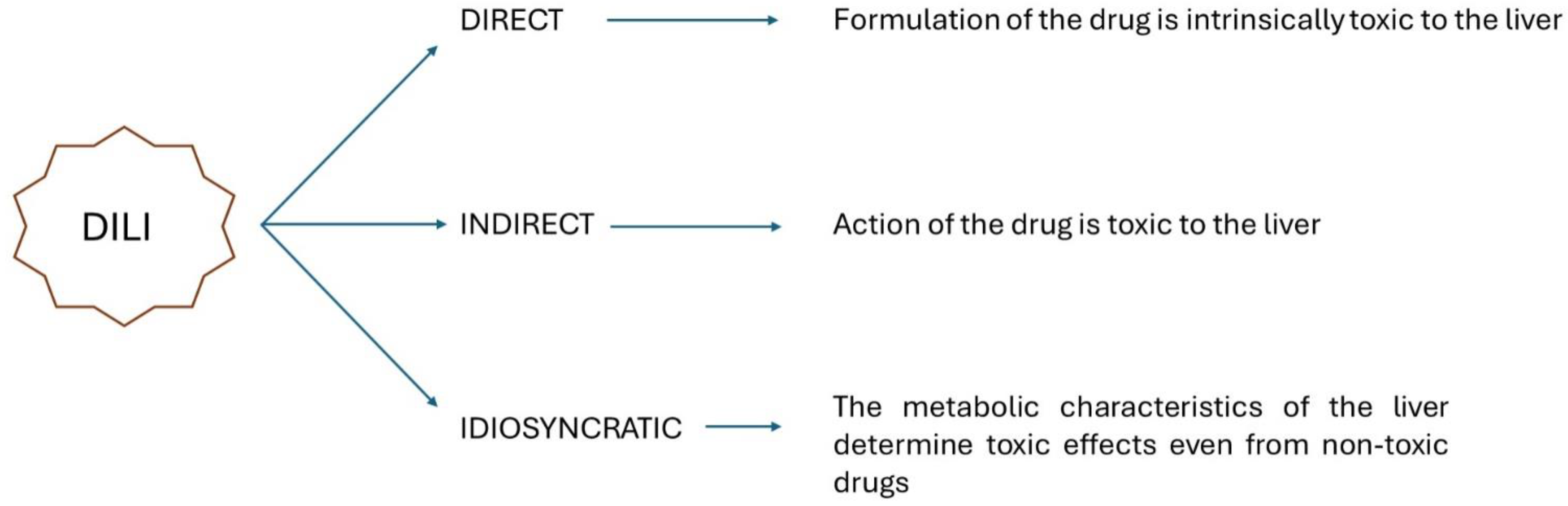

Table 1.
three types of drug induced liver injury (DILI) with respective biohumoral parameters, symptoms and hystology. AP: alkaline phosphatase; ALT: alanine aminotransferase; 2N: twice the norm.
Table 1.
three types of drug induced liver injury (DILI) with respective biohumoral parameters, symptoms and hystology. AP: alkaline phosphatase; ALT: alanine aminotransferase; 2N: twice the norm.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



