Submitted:
21 April 2024
Posted:
22 April 2024
You are already at the latest version
Abstract
The use of antibiotics in neonatal units worldwide varies significantly. We included data from 2015-2022 from the EpicLatino database, which comprises a network of 32 units in Latin America and the Caribbean with gestational age at birth (GA) of ≤ 32 weeks. A questionnaire was sent to the EpicLatino units, to correlate practice with outcomes. Negative binomial regression with standard errors and confidence intervals computed for incidence-rate ratios (IRRs) was used for comparative statistics on antibiotic days per 1000 patient-days between units. All units that responded had 1-6 differences with the reference unit (Unit 2) with the best results, but there was no clear association with the IRR. Each EpicLatino unit should review its statistics to explore possibilities for reducing antibiotic usage.
Keywords:
Antibiotic use in neonatal units
; preterm infants
; EpicLatino database
Introduction
Materials and Methods:
We included data from 2015-2022 from the EpicLatino database, which comprises a network of 32 units in Latin America and the Caribbean (Table 1), with gestational age at birth (GA) of ≤ 32 weeks. A questionnaire was sent to the EpicLatino units, to correlate practice with outcomes (Table 2).
Negative binomial regression with standard errors and confidence intervals computed for incidence-rate ratios[3,4] (IRRs) was used for comparative statistics on antibiotic days per 1000 patient-days between units. We used for the statistics Stata 18, StataCorp LLC, Texas, USA. The variables used to adjust the regression analysis were necrotizing enterocolitis (NEC), GA, infected patients (positive blood or cerebrospinal fluid cultures), length of stay, time period (before/after 2020) and mortality.

Table 2.
Questionnaire sent to the EpicLatino units, to correlate practice with outcomes.
|
| A) Initiate antibiotics in all or almost all premature infants[5] ≤ 32 weeks gestational age after birth due to the risk of infection? |
| B) Select premature infants ≤ 32 weeks gestation for antibiotic administration based on risk factors or laboratory tests. |
|
| A) Yes |
| B) No |
|
| A) Yes |
| B) No |
|
| A) Yes |
| B) No |
|
| A) Select premature infants based on risk factors. |
| B) Select premature infants based on laboratory results obtained within the first 24 hours. |
| C) Do not perform tests and rely on clinical follow-up. |
| D) Both A and B. |
|
| A) If the premature infant is stable and the blood cultures are negative, antibiotics are discontinued within 24 to 72 hours. |
| B) Despite negative results, antibiotics are often continued for 5 to 10 days due to a lack of confidence in the results. |
|
| A) Complete blood count |
| B) C-reactive protein |
| C) A and B, or A and D |
| D) Procalcitonin |
| E) No tests are used to make this decision |
| F) Other tests not listed |
| Antibiotics initiated after the second day of life: |
|
| A) Blood cultures are taken, and antibiotics are initiated regardless of the results of other tests, if performed. |
| B) Blood cultures and other tests are taken, and antibiotics are initiated based on the results of the other tests. |
| C) Antibiotics are initiated before taking blood cultures or other tests, if performed. |
|
| A) If the premature infant is stable, there have been no changes in the laboratory findings, and blood cultures are negative, antibiotics are discontinued within 24 to 72 hours. |
| B) Despite negative blood cultures, antibiotics are often continued for more than 72 hours due to a lack of confidence in the results. |
|
| A) Antibiotics are discontinued when symptoms resolve or 2-3 days later, regardless of the treatment duration. |
| B) Antibiotics are only discontinued if a new blood culture is negative and/or the previously positive laboratory tests completely normalize, regardless of symptoms. |
| C) The duration depends on the type of organism. |
| D) The established treatment duration in the unit is always completed (7, 10, 14, 21 days). |
| E) Options C and D include our management in the unit. |
|
| A) It is common to complete the antibiotic course, even if blood cultures are negative due to a lack of confidence in them. |
| B) It is uncommon to continue antibiotics with negative blood cultures, only in highly symptomatic patients or in conditions such as enterocolitis. |
| C) All premature infants at a predetermined gestational age (< 30, < 28, or < 26 weeks gestation) receive antibiotic regimens of 7, 10, 14, or 21 days regardless of symptoms or laboratory tests. |
| Use of antibiotics in your unit: |
|
| A) Antibiotics are used excessively. |
| B) Antibiotics are used sparingly. |
Results
Figure 1 illustrates the units compared to Unit 2, which serves as the baseline due to having the lowest number of antibiotic days per 1000 patient-days and enough cases. The light blue color on the graph indicates the number of cases in each unit. The two numbers next to each dot represents the number of antibiotic days per 1000 patient-days next to the adjusted IRR and its 95% confidence interval (CI) adjusted with the mentioned variables.
Table 3 presents the parameters used by unit 2 to reduce the use of antibiotics. All units that responded the questionnaire (representing 99.5% of records) showed 1-6 differences compared to the baseline unit. There was no clear relationship between the responses and the IRR of each unit. Notably, among units that perceived themselves as using few antibiotics (as indicated in the last question), the average IRR for these units was 2.4, and three of them had an IRR above 3.
Discussion
To understand the practices leading to this marked difference, the questionnaire on antibiotic use practices showed some differences, but there was no clear association with the IRR. Units that believed they used few antibiotics may not be fully aware of their higher antibiotic usage.
It is noteworthy that a significant number of units claim to comply with most internationally recognized concepts of good antibiotic usage practices. However, it is possible that some units may report what they would like to happen in their facilities rather than the actual practices. Based on international literature, there is always some variables that were not considered. Each EpicLatino unit should review its statistics to explore possibilities for reducing antibiotic usage.
Acknowledgment is given to the units in EpicLatino for their efforts in maintaining this database, which allows us to improve quality and to Pablo Vasquez-Hoyos for the help in statistics.
EpicLatino Database 2015-2022, Premature Infants ≤ 32 Weeks GA, Actual Value (days of antibiotics per 1000 patient-days [DA/P]) and Adjusted Incidence Rate Ratio (IRR) (95% CI) on Logarithmic Scale Adjusted for Gestational Age, Positive Blood/CSF cultures, Length of Stay, NEC, time period and Death
References
- Z. Willis and A. de St Maurice, "Strategies to improve antibiotic use in the neonatal ICU," (in eng), Curr Opin Pediatr, vol. 31, no. 1, pp. 127-134, Feb 2019. [CrossRef]
- EpicLatino, "Epiclatino Repport 2021," https://www.epiclatino.co/reports-2021, 2021. [Online]. Available: https://www.epiclatino.co/reports. 2021.
- M. Ibáñez-Pinilla, S. Villalba-Niño, and N. N. Olaya-Galán, "Negative log-binomial model with optimal robust variance to estimate the prevalence ratio, in cross-sectional population studies," (in eng), BMC Med Res Methodol, vol. 23, no. 1, p. 219, Oct 04 2023. [CrossRef]
- J. A. Grembi and E. T. Rogawski McQuade, "Introducing riskCommunicator: An R package to obtain interpretable effect estimates for public health," (in eng), PLoS One, vol. 17, no. 7, p. e0265368, 2022. [CrossRef]
- S. Mukhopadhyay, S. Sengupta, and K. M. Puopolo, "Challenges and opportunities for antibiotic stewardship among preterm infants," (in eng), Arch Dis Child Fetal Neonatal Ed, vol. 104, no. 3, pp. F327-F332, May 2019. [CrossRef]
- Viel-Thériault, A. Agarwal, E. Bariciak, N. Le Saux, and N. Thampi, "Antimicrobial Prophylaxis Use in the Neonatal Intensive Care Unit: An Antimicrobial Stewardship Target That Deserves Attention!," (in eng), Am J Perinatol, vol. 39, no. 12, pp. 1288-1291, Sep 2022. [CrossRef]
- Katz S, Banerjee R, Schwenk H. Antibiotic Stewardship for the Neonatologist and Perinatologist. Clin Perinatol. 2021 Jun;48(2):379-391. [CrossRef] [PubMed]
- Morowitz MJ, Katheria AC, Polin RA, Pace E, Huang DT, Chang CH, Yabes JG. The NICU Antibiotics and Outcomes (NANO) trial: a randomized multicenter clinical trial assessing empiric antibiotics and clinical outcomes in newborn preterm infants. Trials. 2022 May 23;23(1):428. PMCID: PMC9125935. [CrossRef] [PubMed]
Figure 1.
Statistics of EpicLatino units, numbered for confidentiality. The number of cases is indicated in light blue. Unit 2 (highlighted in green) was used as the base due to its lowest statistic value in DA/P and an adequate number of cases. Units with a significant difference, indicated in red and confidence intervals for the incidence-rate ratio (IRR) (see text). NEC: Necrotizing Enterocolitis, CSF: cerebrospinal fluid. Unit 1 was excluded due to only 1 case of infants of ≤ 32 Weeks GA
Figure 1.
Statistics of EpicLatino units, numbered for confidentiality. The number of cases is indicated in light blue. Unit 2 (highlighted in green) was used as the base due to its lowest statistic value in DA/P and an adequate number of cases. Units with a significant difference, indicated in red and confidence intervals for the incidence-rate ratio (IRR) (see text). NEC: Necrotizing Enterocolitis, CSF: cerebrospinal fluid. Unit 1 was excluded due to only 1 case of infants of ≤ 32 Weeks GA
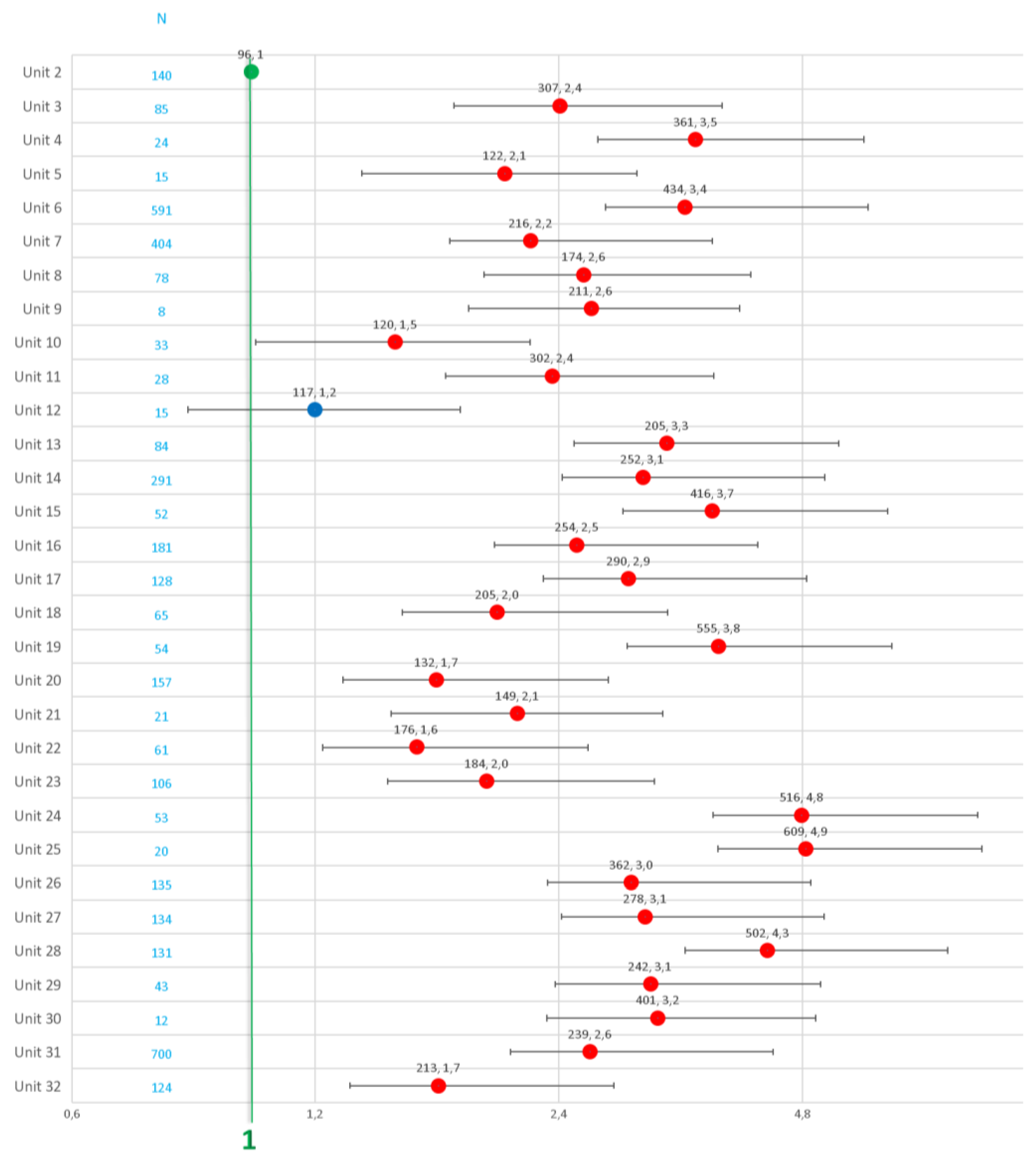
Table 1.
Units belonging to the EpicLatino network.
| UNITS | CITY/COUNTRY |
| Centenario H. de Esp. Miguel Hidalgo | Aguascalientes, Mexico |
| Clínica Dávila | Santiago, Chile |
| Clínica de Santa María de Santiago | Santiago, Chile |
| Clínica del Country | Bogotá, Colombia |
| Clínica la Colina | Bogotá, Colombia |
| Clínica Materno Infantil San Luis | Bucaramanga, Colombia |
| Clínica San Felipe | Lima, Perú |
| Clínica Santa Bárbara | Quito, Ecuador |
| Clínica Somer | Rio Negro, Colombia |
| Clínica Universitaria Colombia | Bogotá, Colombia |
| Clínica Vespucio | Santiago, Chile |
| Colsanitas – Clínica Pediátrica UCI Neonatal | Bogotá, Colombia |
| Curaçao Medical Center | Willemstad, Curaçao |
| H Regional DR Rafael Pascacio Gamboa | Tuxtla Gutiérrez, México |
| Hospital Central Dr. Ignacio Morones Prieto | San Luis Potosí, México |
| Hospital Civil de Ipiales E.S.E | Ipiales, Colombia |
| Hospital de los Valles | Quito, Ecuador |
| Hospital Departamental San Vicente de Paul | Garzón, Huila, Colombia |
| Hospital Dr. Florencio Escardó | Tigre, Argentina |
| Hospital Español de Mendoza | Mendoza, Argentina |
| Hospital General EISS de Manta | Manta, Ecuador |
| Hospital Italiano de La Plata | La Plata, Argentina |
| Hospital Luis Lagomaggiore | Mendoza, Argentina |
| Hospital Metropolitano | Quito, Ecuador |
| Hospital Militar Central | Bogotá, Colombia |
| Hospital Regional Universitario de Colima | Colima, México |
| Hospital San Francisco de Quito | Quito, Ecuador |
| Hospital San José | Bogotá, Colombia |
| Hospital Santísima Trinidad | Asunción, Paraguay |
| Los Cobos Medical Center | Bogotá, Colombia |
| Maternidad Nuestra Sra. de las Mercedes | Tucumán, Argentina |
| S.E.S. Hospital de Caldas | Manizales, Colombia |
Table 3.
The base unit (Unit 2 for statistical calculation) uses the following criteria to minimize antibiotic use, which served as the basis for the comparison:.
Table 3.
The base unit (Unit 2 for statistical calculation) uses the following criteria to minimize antibiotic use, which served as the basis for the comparison:.
|
|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



