
Submitted:
19 April 2024
Posted:
23 April 2024
You are already at the latest version
Abstract
The development in the field of ceramics has been increasing over the past several decades. Among all of the dental ceramics, zirconia ceramics show very good mechanical properties and a significant improvement in mechanical function. However, it is properly established that each step of the fabrication process of zirconia ceramics must be controlled to achieve the expected mechanical properties. These steps include the block constructing, sintering process, machining and surface processing. Recent advances have focused on zirconia ceramics in forming and sintering processes, mechanical properties, combining with various materials, and on surface processing. All these items provide conceptions about the formability and machinability of the zirconia. Until now, very excellent studies have been done to specify the evolution of microstructures, phase and mechanical properties of zirconia ceramics during the sintering process. However, more studies are required in this field. This paper aims to demonstrate general views and various studies in the field of zirconia ceramics. The properties, applications and tests performed and the recent developments in the field of zirconia bioceramics are discussed.
Keywords:
Zirconia ceramics
; Mechanical characteristics
; Machining
; Sintering process
1. Introduction
Breaking and teeth loss are the most common problems of the oral cavity. They not only affect the beauty of the teeth, but also affect the chewing function. In this case, tooth restoration is the only solution to these problems. To restore the natural function of teeth, artificial materials are often used, and they are known as dental materials. A wide range of materials are used in dentistry for the restoration purpose, which include metals, ceramic materials, alloys and etc. Among dental restorative materials, metals are competitive with other materials because of the high strength. But due to the adverse reactions of metal prostheses, like limited chemical ability, low biocompatibility, and toxic to the surrounding tissues of the teeth and lack of the appearance beauty, the current trend in dental materials has gone towards the development of metal-ceramic or metal-free systems. In 2005, it was estimated that more than 50% of all dental restorations are made of metal-ceramic materials, and the Appearance beauty is obtained by expert technicians. Therefore, in addition to functional and structural problems related to the metal part of the restoration, the skill of a technician is also required for manufacturing. But with the development of dental materials, the use of dental restorative materials has changed from metals to ceramics due to the need to improve clinical performance and physical features and biocompatibility characteristics. Over the past thirty years, the advancement of ceramics in dental applications has been remarkable. Dental ceramics include alumina, zirconia, sanidine and etc., which have become promising substitutes in the dental market. Among these dental ceramics, zirconia has become the most usable material in clinical applications which has many advantages over other ceramic materials [1-8].
Zirconium oxide (ZrO2), which is also known as zirconia and zirconium dioxide, is a white powder with a melting point of 2710⁰c, which is sensitive to temperature, and the structure changes with temperature. Due to this feature, it has 3 structural phases According to temperature, it finds the monoclinic phase at room temperature up to 1170⁰c, tetragonal phase from 1270⁰c-2370⁰c and the cubic phase at temperatures above 2370⁰c. During the cooling of zirconia, the tetragonal structure turns into a monoclinic. The transformation of tetragonal to monoclinic is associated with an increase in volume. This volume change causes non-uniformity, crack and finally failure. For this reason to stabilize zirconia, it must be combined with various oxides, for example: magnesium oxide, yttrium oxide, sodium oxide, lanthanum oxide, etc. But among these oxides, yttria is the most common. Phase stabilization is usually done in three general ways: 1) partially stabilized zirconia (PSZ), that zirconia is doped with substances like magnesium (Mg-PSZ) or calcium (Ca-PSZ). 2) Tetragonal zirconia polycrystal (TZP), which is transformed into stabilized tetragonal form by including materials like yttria (Y-TZP) or cerium (Ce-TZP) to stabilized zirconium dioxide. 3) Fully stabilized zirconia (FSZ) refers to the state in which zirconia is completely stabilized in cubic phase [9-11].
Natural zirconia is significantly different from teeth respect to color, and translucency and this feature may limit the exclusive use of this material in dental restoration. This problem was solved by veneering the external surface of the zirconia framework with feldspar-based ceramics. But it has limitations such as high fracture risk, less strength and being more vulnerable to fracture. In addition, veneering porcelain requires the expertise of dental technicians and more time. Therefore, the monolithic zirconia restorations were considered. Monolithic restorations are fixed prostheses made of pure zirconia and have advantages like reduced fabrication time, cost-effectiveness, better mechanical properties, and elimination of the interface between zirconia and veneer. Monolithic zirconia is available in two forms, opaque and translucent. Opaque zirconia has more strength and is usually used for posterior restorations, whereas translucent zirconia offers a more natural appearance and is more often used in anterior restorations. Of course, to solve the problem of matching the color of zirconia with natural teeth, metal oxide (Fe2O3) is added to zirconia with a certain percentage [12-19].
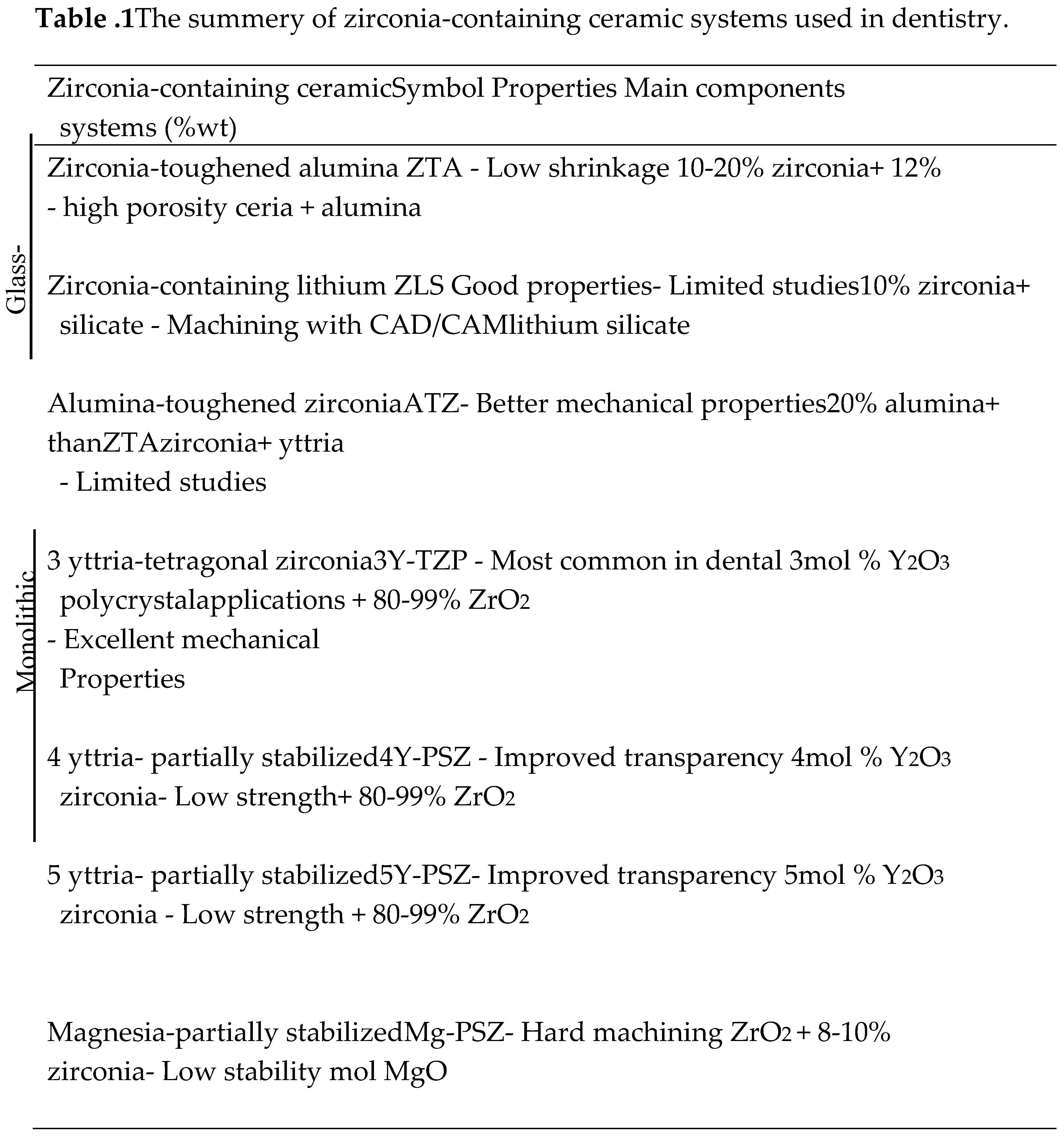
Generally, zirconia-containing ceramic systems used in dentistry are summarized in Table 1. Nowadays, mostly three types of them are employed in dentistry, including yttria-stabilized tetragonal zirconia polycrystal (3Y-TZP), magnesium-partially stabilized zirconia (Mg-PSZ), and zirconia-toughened alumina (ZTA) which includes glass-infiltrated zirconia-oughened [20]. In clinical applications, especially dental restorations, zirconia stabilized with yttria (3Y-TZP) is more common. This system is used in most studies, which is due to the unique and sufficient properties of zirconia. It seems that it does not need to be combined with another material to improve properties and it is better to optimize the manufacturing and processing steps. Naturally, zirconia contains some limitations, but these limitations can be controlled in the processing stages of zirconia.
1.1. Properties
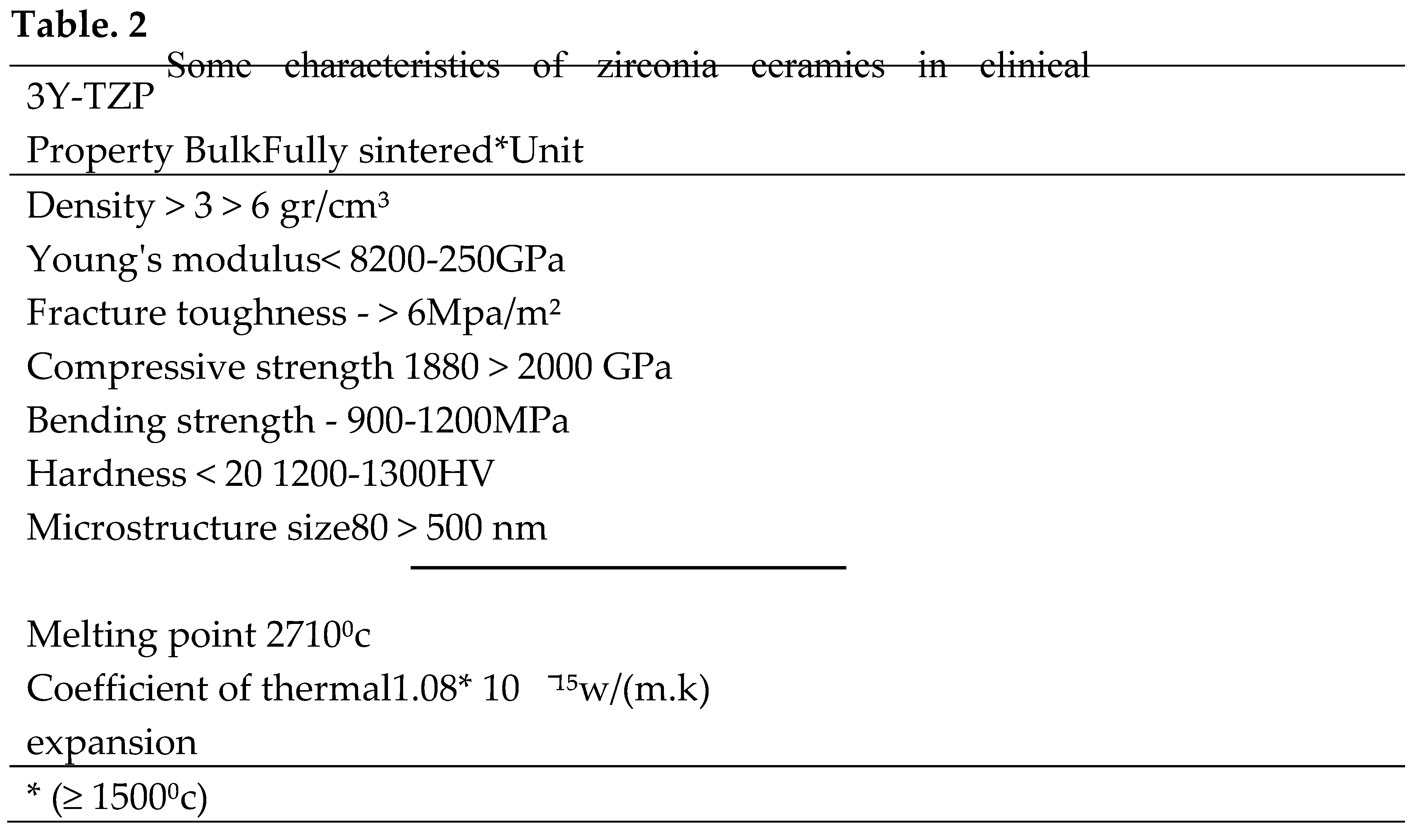
The choice of material in clinical applications is very critical. In choosing a material, factors like corrosion behavior, mechanical properties, manufacturability and cost, biocompatibility and Physical features should be considered [5]. Among the all-ceramic systems, zirconia is the most suitable material for tooth restoration. This is refer to the unique properties of zirconia, including high fracture toughness and good corrosion and wear resistance, excellent mechanical properties and high strength [4, 10]. In the first medical application of zirconia presented by Helmer [21], to manufacture ball heads for total hip replacements, no adverse reactions were observed. This issue is related to the biocompatibility of zirconia, which is one of the most significant advantages of zirconium-based ceramics. The thermal shock resistance of the zirconia is low, especially at temperatures above 1000⁰c due to phase transformation. The hardness of monoclinic zirconia is 9.2 GPA, which reaches 11 GPA for yttria stabilized zirconia [22]. Other characteristics of zirconia ceramics include good chemical resistance, high hardness, resistance to cracking and mechanical stress, high toughness and good ionic conductivity. Some salient features of zirconia are determined in Table 2.
Posterior zirconia bridges have been shown to comparable life time to metal-based restorations. The life time of zirconia is more than 20 years in moist conditions, and this is a sign of high initial mechanical strength of zirconia [23].
1.2. Other applications
Zirconia is a very versatile ceramic. This makes them appropriate candidate for a diverse range of applications in modern industries, engineering, medicine and dentistry because of excellent properties. Including optical fiber connectors, sensors, environmental filters, mechanical components, electronics are used. For example, due to its high biocompatibility, it allows use in the field of biomedicine, like teeth, body prostheses, and tissue engineering. For example, it used in orthopedic joints and bones, surgical and dental prostheses, including making dental veneers, crowns, fixed partial prostheses, inlays, implant bases, and orthodontic brackets. Also, due to the low price, high strength and appearance similarity to diamond, it has been the main competitor for diamond in the jewelry industry since 1976 (the time of economic industrial production). Because of their high melting point (2710°C), zirconia ceramics are highly refractory, so they can be operated for significant structural applications up to very high temperatures. Zirconia ceramics have been used for coating applications due to having the same thermal expansion coefficient as iron alloys, high toughness and cost-effectiveness [24-27].
2. Processing methods of zirconia
Blank manufacturing comprise the first stage of the zirconia production process. In this way, zirconia powder is combined with specific amounts of other materials (according to the Producer Company) and compressed with an isostatic pressure. Two methods are available for compressing zirconia: cold isostatic pressure and hot isostatic pressure. In the first method, zirconia powder is compressed with a cold isostatic press with a pressure of 200-300 MPa. In another method, zirconia powder is first compressed under a dry condition with a pressure of 90 Mpa, then hot-pressed at a 300⁰c temperature with a pressure of 240 MPa. After the compression is shaped into a disk which is known as green state zirconia. Then it is cut into desired dimensions and sintered at different temperatures. After that, it is machined and various tests are performed on zirconia samples. Usually, the phase transformation of zirconia at each stage of sintering is determined by X-ray diffraction (XRD) and scanning electron microscope (SEM) is used to analyze the surface morphology.
2.1. Sintering process
Sintering is one of the methods of shaping metal and ceramic materials. Although there are many laboratory methods for production fully dense zirconia: like Laser, microwave, hot press, sintering, spark plasma and high temperature isostatic press, but sintering remain the most suitable and economical method for industrial applications. Sintering represent the growth and expansion and sticking of material particles through surface melting under suitable temperature conditions so that it becomes a solid mass. The overall purpose of sintering is to produce a coherent body under appropriate temperature conditions. Recently, a method called two-step sintering (TSS) has been developed, at first the ceramic is pre-sintered at a low-temperature and machined, then sintered at a higher temperature [28-30]. The quality of the prosthesis surface depends on the sintering process not only on the machining process. Therefore, the sintering process serves as the technical basis for improving the machinability of zirconia.
2.1.1. Deformation behavior of zirconia during sintering process
The size of zirconia microstructures significantly depends on the sintering temperature [1]. So that with increasing the sintering temperature, the microstructures of zirconia become larger and the pores between them decrease, so it becomes denser [31]. The porosity of zirconia reaches 1.4% after the sintering temperature of 1400⁰c. The maximum achievable density for zirconia used in clinical applications is about 6.1 gr/cm³ [8]. Zirconia approaches this density from the sintering temperature above 1300⁰c. Therefore, the density of the material is affected by changing the porosity distribution [32]. Generally, in the sintering process, zirconia is brittle in the range of 800⁰c-1000⁰c, most of the condensation of materials is done in the temperature range of 1000⁰c-1300⁰c and in the temperature range of 1300⁰c-1500⁰c, the sintering process is completed and the hardness is stable. [30].Most of the densification of zirconia occurs from temperature above 1300⁰c, and the densification is almost completed at 1700⁰c. Grain growth has two types of behavior. The first behavior indicates slow grain growth for low temperatures, and the second behavior is related to grain growth for temperatures higher than 1550⁰c, in which zirconia-forming fine grains grow faster [33]. Danilenko et al. [28] pointed out that the microstructure and shrinkage characteristics can be controlled by sintering, so sintering remain a significant step in the production of ceramic materials.
2.2. Machining
Zirconia restorations need processing and surface modification after the sintering process and are usually done by mechanical operations, the best of which is machining [34]. Currently, various types of machining processes are carried out, like micromachining, lithography, engraving, and laser machining [4]. Among all of them, the laser machining process is better because of non-contact features and high efficiency in terms of creating microtextures on the surface [35]. But this modern technology require more equipment and cost [36]. Recently, computer-aided design and manufacturing technology (CAD/CAM) are used as a new approach that reduces the number of prosthetic manufacturing steps. This process allows the formation of zirconia with complex shape and eliminates the manual methods of the dental technician [37]. Generally, two main processing techniques are defined for zirconia machining: 1) hard machining 2) soft machining [20]. Hard machining involves direct machining on the material after complete sintering. Soft machining refers to a technique in which ceramics are pre-sintered at a certain temperature and machined, then completely sintered at a high temperature [31]. Zhang et al. [36] proposed an ultrasonic vibration assisted milling process as a new technology in hard machining. This technology partially solved the impact of hard machining on the fabrication of ceramic prostheses, but resulted higher costs for manufacturers. Soft machining produces less friction, and the tool wear during milling, so soft machining is more desirable [20].
By examining three different machining methods (conventional machining, polishing or rough polishing, and micro-machining) on zirconia, Traini et al. [34] found out the highest hardness, and fracture strength is for samples that have been conventionally machined, so it is better to use conventional machining. Also, the machining results in Min Ji and Jinyang study showed that before the sintering temperature of 1100⁰c, the material removal process is in the form of chip and typically fails, but after the temperature of 1100⁰c, it is in the form of cracking [38].The researchers have focused on the machining science studies for understanding the basic responses of sintered zirconia and high quality restorations.
3. Limitations
3.1. Shrinkage
Zirconia experiences approximately 20-25% shrinkage during the sintering process. Therefore, the shrinkage rate should be predicted before milling and it is an important factor to achieve an accurate fit of the prosthetic veneers. According to Amat et al., zirconia has a 48% shrinkage at a sintering temperature of 900⁰c and a 9% shrinkage at a temperature of 1200⁰c. Which means with increasing the temperature, the shrinkage decreases. It should be noted that during the compression of zirconia, there may be blank in some parts, in which case, it may have non-uniform shrinkage due to non-uniform compression of particles during the sintering process of zirconia. So, if zirconia sintering at high temperature it will be uniform. Also, for dental applications, it is better to use monolithic zirconia because the addition of metal oxide (to match the tooth) increases the rate of shrinkage [39-42]. A sample with less shrinkage is more suitable because it is closer to the real dimensions of the tooth.
3.2. Aging
Yttria is used as a stabilizer in zirconia to achieve phase stability, but in the oral environment, it is exhausted through reaction with water in the presence of moisture. So, it transforms from tetragonal to the monoclinic phase (t-m). This spontaneous degradation mechanism is called low temperature degradation (LTD), which is also known as aging. The most critical temperature range for zirconia aging process is 200°C-300°C according to Swab. This process happens with long-term use of zirconia in a hydrothermal environment like the mouth, in fact, the linkage of zirconia are disrupted by water. This phase transformation is associated with microcracks, surface roughness and 4.5% increase in volume [43-47]. This issue can affect the mechanical properties over time.
In a comparative study to modify the surface of dental zirconia ceramics to improve aging, the low temperature degradation textured zirconia ceramic surfaces is affected by the depth and width of the groove. And proposed to consider the minimum width of the groove and the depth of the groove corresponding to natural teeth [1].
It is necessary the LTD of zirconia occurs only on the surface of the sample, and this is a positive event because it takes many times for water to penetrate the main part of the restoration, so this process does not shorten the life of the restoration. On the other hand, prevent further propagation of cracks with increasing the volume of the zirconia. It should be noted that low temperature degradation is related to factors such as microstructural properties and density, sintering temperature and manufacturing method, type and amount of stabilizer, surface milling. With changing in these parameters can be improved the LTD of zirconia [48-51]. Generally, the low temperature degradation of zirconia can be summarized as follows:
1) loss of yttria through reaction with water, 2) transition of tetragonal phase to monoclinic (t-m), 3) increase volume and appearance of microcracks on the surface of the dental restoration, 4) progress of phase transition from the surface to the inner part of the restoration.
4. Basic researches on zirconia
Zirconia was identified in 1789 by the German chemist Martin Heinrich Klaprot and was used as a pigment in combination with other materials for a long time [3]. The first suggestion to use zirconia for medical purposes in vivo was made by Helmer [21] in 1969. Zirconia was introduced as an alternative for femoral heads instead of titanium or alumina prostheses. The result after implanting zirconia was evaluated and no adverse reactions were observed and they related to the biocompatibility of zirconia. This was one of the first in vivo studies. But the first study on the use of zirconia for the construction of the femoral head prosthesis with the current application was conducted by Christel et al. [52], More than three hundred thousand zirconia hip prostheses have been implanted [53]. Just two failures have been reported [54] that the reason was steam sterilization and phase transformation [33].
In 1975, Garvie [55] called the zirconia "ceramic steel" to rationalize the good mechanical properties of it. Since 1990, in vitro studies have been conducted to evaluate zirconia cellular behavior. In laboratory evaluations, it was confirmed that zirconia does not cause any toxicity. In a test conducted by Ichikaw et al. [56], the zirconia ceramic bonded well to the tissue and it was shown that the zirconia possessed mechanical stability during the 1-year experimental period. Also, in 3-year study by Suarez et al. [57] on dental restorations, no negative effects were observed in terms of compatibility. And based on the findings of this study, zirconium oxide restorations can be considered reliable for clinical application.
Although there are no long-term clinical experiment to prove the positive effects of zirconia and long-term evaluations are needed to conclude the reliability of zirconia. But the studies carried out to date indicate that zirconia restorations are accepted by the tissue, do not cause destructive effects and are sufficiently resistant.
5. Mechanical properties
The mechanical properties reviewed on zirconia ceramics include hardness, fracture toughness, bending Strength, Young's modulus, Elastic and plastic deformation, compressive strength, etc. Zirconia ceramics are used for many clinical applications like dental restorations, body prostheses and tissue engineering. The materials employed in the medical applications must possess appropriate mechanical properties. For example, for load-bearing structures, the material must have mechanical stability equal to or greater than of natural tissue. Various studied have been conducted on the mechanical properties of zirconia ceramics.
The mechanical properties of zirconia structures are significantly affected by the machining quality [58]. Therefore understanding the mechanical behavior of zirconia is very important because it determines the machinability and wear behavior of the material [59]. It is substantial measuring the mechanical properties of pure zirconia is very difficult because the properties of zirconia are determined at high sintering temperatures. Generally, if for evaluating mechanical properties, complete densification is expected, the material should be sintered to a temperature higher than the monoclinic to tetragonal transformation (i.e. at temperature of 1200°C). It is difficult to measure the toughness of monoclinic zirconia due to problems during sintering. However, in many studies the mechanical properties of zirconia have been determined, but more studies are needed because of the importance in engineering applications [23]. Nowadays, many researches are based on the Sakai [60] model that was presented in 1999. In this technique, by creating a single indention on the surface of the ceramic, resistance to plasticity and deformation was analyzed. This test called nanoscratch and its an effective method for analyzing mechanical properties. This test determines the deformation of the surface, the amount of displacement and the indention depth. Also, to obtain the contact hardness, Young's modulus and the deformation behaviors of the materials if combined with the electron microscope are suitable [61, 62]. All of which provide insights into the plasticity and machinability of materials.
With increasing the sintering temperature, the hardness of the zirconia increases [31]. The standard hardness value for zirconia used in dental applications is 1200-1300 HV. Zirconia shows good hardness properties in the temperature range of 1400⁰c-1600⁰c [36]. In fact, it reaches the desired standard value in this temperature range. Furthermore, no significant difference was observed by examining the hardness of the zirconia in aging and normal conditions. Because these mechanical properties are related to the nature of zirconia ceramics [62]. The strength and hardness of zirconia is enough to stand the chewing process, even if the impacting agent has a very high hardness [7].
At temperatures where the material is porous, the sample shows little resistance to bending and fracture [63]. So, with increasing the hardness of the material, the bending strength also increases [64]. The flexural strength of sintered zirconia for clinical applications is 836 MPa. Stawarczyk et al. [65] proposed that sintering temperature should not exceed 1550⁰c to have a suitable bending strength and mechanical properties. In the study of fully sintered zirconia (1300⁰c- 1700⁰c), the highest bending strength was in the temperature range of 1400⁰c- 1550⁰c and the lowest bending strength was at 1700⁰c.
According to the studies of Haixin et al., the compressive strength of green zirconia is 1886.38 GPA. This value reaches 2025.9 GPA at the sintering temperature of 1100⁰c. In another study, the value of compressive strength at sintering temperature of 1550⁰c, 1988.27 GPA has been evaluated [66]. The compressive strength of zirconia in the green state is also significant. But the sintering process also has an effect, and increasing the sintering temperature improves this property. Although the results show that there is no specific trend.
The studies of Tateishi and Yunoki [67] showed that with increasing sintering temperature, the impact resistance of the zirconia increases. The fracture toughness of sintered 3Y-TZP is 6 Mpa/m². Zirconia reaches this range of fracture toughness from the sintering temperature of 1300⁰c. This value reaches almost 8 Mpa/m² at the sintering temperature of 1500⁰c [29].
An understanding of the elastic/plastic deformation caused by the machining of pre-sintered zirconia is needed to predict the machinability [68]. Nano-indentation tests are very useful for characterizing mechanical properties and elastic deformation at the nanoscale. The contact hardness of zirconia is dependent on the loading rate according to Alao and Yin's research [58]. Resistance to plasticity decreases with increasing loading rate if the elastic displacement is independent of loading rate. As the temperature increases, the plastic properties of the material increase and the zirconia tends to crack [31]. If the elastic deformation of the material is more significant, the material can be less resistant to failure [58]. According to Gregorova et al. [27] the elastic modulus does not demonstrate a specified trend with increasing temperature, but it is expected to decrease. Although there is an increasing trend in some of the studies. The expected Young's modulus for zirconia is 250 GPA, which is obtained at temperatures above 1400⁰c.
In comparison of different temperatures of complete curing of zirconia, the Weibull module has the highest value at 1400⁰c temperature and the lowest value at 1700⁰c temperature [8]. The Weibull modulus describes the dispersion in the mechanical properties of ceramics. Therefore, at higher temperatures, this amount of dispersion is less, and the material has reached greater stability.
6. Tool wear in machining
Generally, the life of machining tools ends with the tool wear, cracking and fraction. Tool wear attends the deformation of the cutting part proper to the gradual loss of tool material during cutting process. There are two forms of tool wear, surface and lateral. Wear is caused by friction and heat during machining. Usually, the most failures occur on the marginal edges of the tool. In applicatory situations, when the tool does not produce workpiece of the expected quality, the end of the effective life of the tool [69-74]. Usually, the factors that affect the tool life include the type and properties of the machined material, the material and geometry of the tool, and the cutting speed and depth of the machining [69]. Testers usually determine the material of the tool. However, according to the standard, the use of uncoated steel and cobalt alloy is recommended [73, 74]. Malkin and Huang [75] realized that milling of the material surface accounts for almost 80% of the total cost of manufacturing ceramic workpiece, which is due to the cost of replacing tools that are excessively wearing or broken. Therefore, the study of wear behavior is important to achieve machining results with high efficiency and high quality [76].
Zirconia ceramics are naturally brittle, therefore, they are highly exposed to surface damage during machining [77]. A good and undamaged surface is required in clinical applications to avoid tissue damage and infection. Many suggestions have been made to reduce the damage caused by machining. There are many theories for surface modification of zirconia, such as addition of conditioner during machining that destroys mechanical properties [78], or changing the position of the tool with the workpiece that does not affect the surface [79]. Machining at higher speed or higher loading force, which causes degradation of strength and tool wear and the surface damage. Increasing these parameters removes more material from the surface and increases tool wear. In the pre-sintering state, the cracking resistance against machining in this material is equal to 132.74 Mpa. This low value causes energy to be absorbed into the pores and increases the possibility of damage to the surface [80]. Anandita et al. [77] machining characteristics are influenced by process parameters and tool geometry. If the cutting depth is less than the critical depth and the material is in a formable state and subjected to cutting with a microscopic tool, it leads to the creation of a crack-free surface. In the part where the hardness is lower or the porosity is higher, occurs more fracture. But in the part of the sample where the hardness is higher, more cracking occurs, and in this area, tool wear is more concentrated [38, 81].
Wear represent the gradual reduction of material from the surface of an object moves relative to another object. In fact, during machining, when the milling tool enters contact with a sample material, it may suffer erosion or loss. The tool wear on the machined surface and stresses created during the machining process affect the finished product of dental restorations. The tool wear is inevitable and not considered a negative process. But the amount, type and occurrence time of the tool wear should be checked that it can controlled by zirconia processing methods like sintering.
7. Suggestions
In the field of improving of zirconia ceramics, many suggestions have been proposed in various studies. Some suggestions are effective and nowadays have been used in scientific literature.
Combination with other materials: To improve the properties of zirconia, there are many studies in the form of combining this material with other materials, for example silicon carbide (as a conditioner to improvement surface roughness) [82], silica (Sio2: for a smoother surface) [83], methacrylate (to increase hardness) [41] and alumina (to improve mechanical properties) [84]. The results of these studies are consistent with the previous results for zirconia ceramics. So it should be accepted that these results are related to the nature of zirconia ceramics and because of the excellent properties combined with any material the characteristic features retain and improve.
Two-step sintering: In this method, initially, the zirconia ceramic is pre-sintered at a lower temperature and machined, then it is fully sintered at a higher temperature. This method allows resisting cracking during machining [85]. It also reduces milling time and wear of cutting tools [86]. The purpose of two-step sintering is to control the grain growth rate [87]. According to Mazaheri et al. [88] by examining the effects of sintering paths on grain growth behavior, two-stage sintering reduces the rate of grain growth during final sintering compared to single-stage sintering. However, there is additionally an opposing theory that related the control of grain growth rate to the increase of heating rate. According to Irvine et al. [81], the hardness of pre-sintered zirconia is about 66 Vickers, but its hardness increases to 1600 Vickers with full sintering. In the pre-sintering state, the cutting length reaches up to 1400 mm, but in the full sintering state, it finally reaches 350 mm [76]. In the full-sintered state, a tool wear increases, tool life and cutting depth decreases. As a result, two-stage sintering is suggested. This method has been employed in the last few decades as a very efficient method to improve the mechanical properties and machining of zirconia.
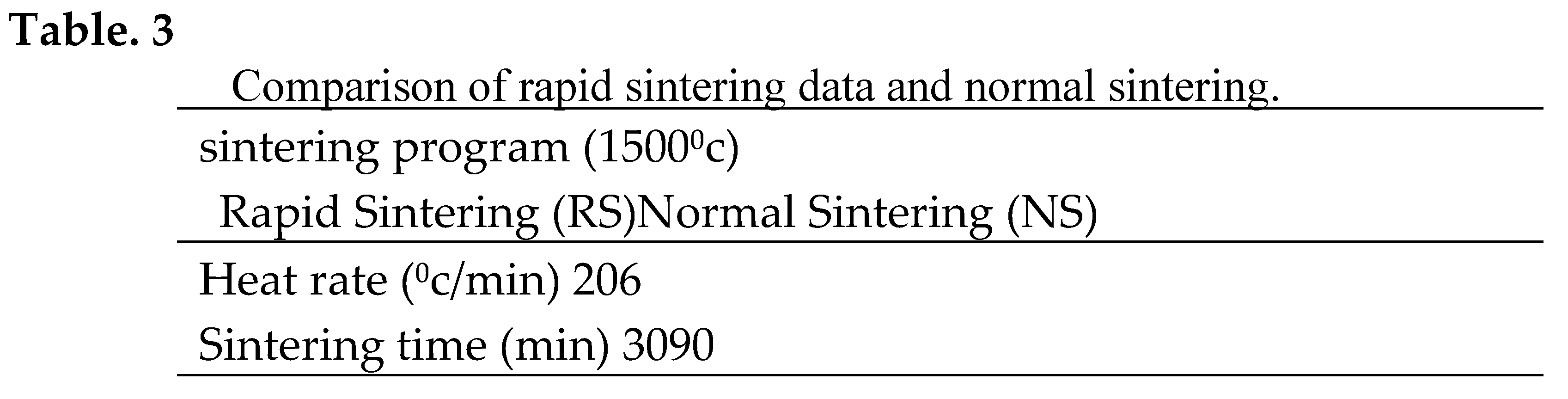
Rapid sintering (RS): Sintering endures 6-8 hours for heating, cooling and dwell time. If the sintering process takes more than 8 hours, it is uneconomical. This has encouraged manufacturers to use fast firing ovens. This method with increasing heat rate, reduces the processing time from hours to minutes. This matter leads manufacturers to use ovens with rapid sintering. This method reduces the processing time from hours to minutes. A comparison of the data of rapid sintering and conventional sintering is reported in Table 3. This process saves time and energy in zirconia ceramics and thus increases productivity. By comparing the rapid and normal sintering of zirconia, a similar behavior has been observed in the mechanical properties. This method is particularly useful for sintering dental restorations in minutes, which can result in the fabrication of the restoration while the dental patient is waiting. However, this method has limited reliability, actually the consequences of zirconia on different generations have been uninvestigated, and so more research is required in this field [89-92].
Increasing sintering time: Increasing the sintering time is recommended to increase the fracture resistance, but may decrease the strength of zirconia, also, it does not affect the phase change of zirconia. Sintering in a shorter time does not weaken zirconia. Although it is significant that to obtain transparent dental restorations, more brief sintering time should be considered [93-96]. As a result the authors proposed normal sintering.
Heating machining: This method was proposed by Ito et al. [97]. According to this study, if the machining speed increases, the heat is more produced. Therefore, the milling temperature increases, and the hardness of the zirconia surface decreases and becomes flexible. Due to this issue, machining becomes easier, an accurate surface is obtained and tool wear is reduced.
Sandblasting: Sandblast was suggested by Monaco et al. [37]. This machining method is for polishing and preparing surfaces. In pre-sintered samples, sandblasting produces more irregular surfaces than full-sintered samples. Consequently it is better to sandblast the samples after complete sintering.
Extrinsic coating technique: In the study of Shui et al. [98], this technique was presented. This model refers to coating the surface of zirconia by immersion in sodium-rich feldspar or brushing the surface of the sample before the final sintering process. Due to the appearance color of zirconia, it has a limited use in anterior restorations. This method is more suitable for fabricating transparency and natural color of zirconia, if it does not affect the mechanical properties.
8. Discussion
The mechanical properties of zirconia are similar to stainless steel. The extension strength of zirconia is 1200-900 MPa and its compressive strength is about 2000 MPa [66]. Other ceramic technologies only allow the fabrication of structures that are resistant to chewing on anterior teeth. But zirconia ceramic restorations can also be used on posterior teeth [99]. Posterior zirconia restorations have been shown to have comparable longevity (more than 20 years) to metal-based restorations. Luthy [100] reported an average load-bearing capacity of 518 N for alumina restorations, 282 N for lithium disilicate restorations, and 755 N for zirconia restorations. Therefore, zirconia is a good choice for dental restorations.
Brittle materials must be machined in a ductile state. Formative mode machining is a method to achieve high surface quality workpiece. Machining at high temperature is not suitable for obtaining flawless workpiece [101]. Surface quality is important in mechanical behavior such as wear and fatigue of dental restorations. Which include surface roughness and morphology and phase transformation [86]. Also, the material removal process shows that any material can be machined without damage on a small scale and in a formable mode [102].
Understanding the mechanical behavior of zirconia can provide scientific insights into the machining mechanisms of the material's ductile state, which can be simulated by an indentation. That the mechanical contact conditions for indentation are similar to the machining conditions. Machining forces, speed, and tool geometry can be simplified by indentation loads, loading rates, and indentation tool geometry [61]. The response of materials to machining and functional processes can be predicted, but not exactly. As a result, direct machining is better than creating an indention [58].
Zirconia ceramics have many advantages over the other ceramic materials due to the transformation hardening mechanisms of microstructure. Which can give them very good mechanical properties. These mechanical properties depend on the process in sintering and manufacturing and processing the workpieces. The production of zirconia biological materials requires the use of high purity, because high purity materials can only have the required stability, especially when they are used in the body [3]. And because long-term human tests to prove clinical success are still lacking [103]. So a long experimental research study is usually needed to improve the results.
Zirconia ceramics show the highest fracture toughness among all dental ceramics [6]. Fracture toughness represents the resistance of a ceramic material to crack growth, which is mainly controlled by the transformation resistance mechanism, depending on grain size, sintering temperature, and yttrium content [92]. Furthermore recent advances in the processing of high-transparency zirconia materials can significantly increase the clinical indications of monolithic zirconia restorations to prevent interface fractures in veneer-core structures [86]. Therefore, to receive a restoration with high fracture tolerance, it is better to use monolithic zirconia without impurities. And used the appropriate sintering temperature to achieve the expected mechanical properties and appropriate microstructure size.

9. Conclusion
Ceramics used in the medical field are known as bioceramics. Bioceramics should be biocompatible. That is, it should be not recognized as a foreign substance in the body. It should also be biodegradable. Biodegradability means that the substance is destroyed or dissolved without harming the tissue. And it should be suitable in terms of mechanical properties and retain mechanical stability as much or more than natural tissue. In the clinical applications of zirconia, the results show no toxicity and adverse reactions have been detected, and because of the high biocompatibility of this material. In addition, zirconia ceramics have many advantages over other ceramic materials due to the transformation hardening mechanisms that occur in its microstructure and obtain very exceptional mechanical properties. As a result, zirconia belongs to the group of bioceramics.
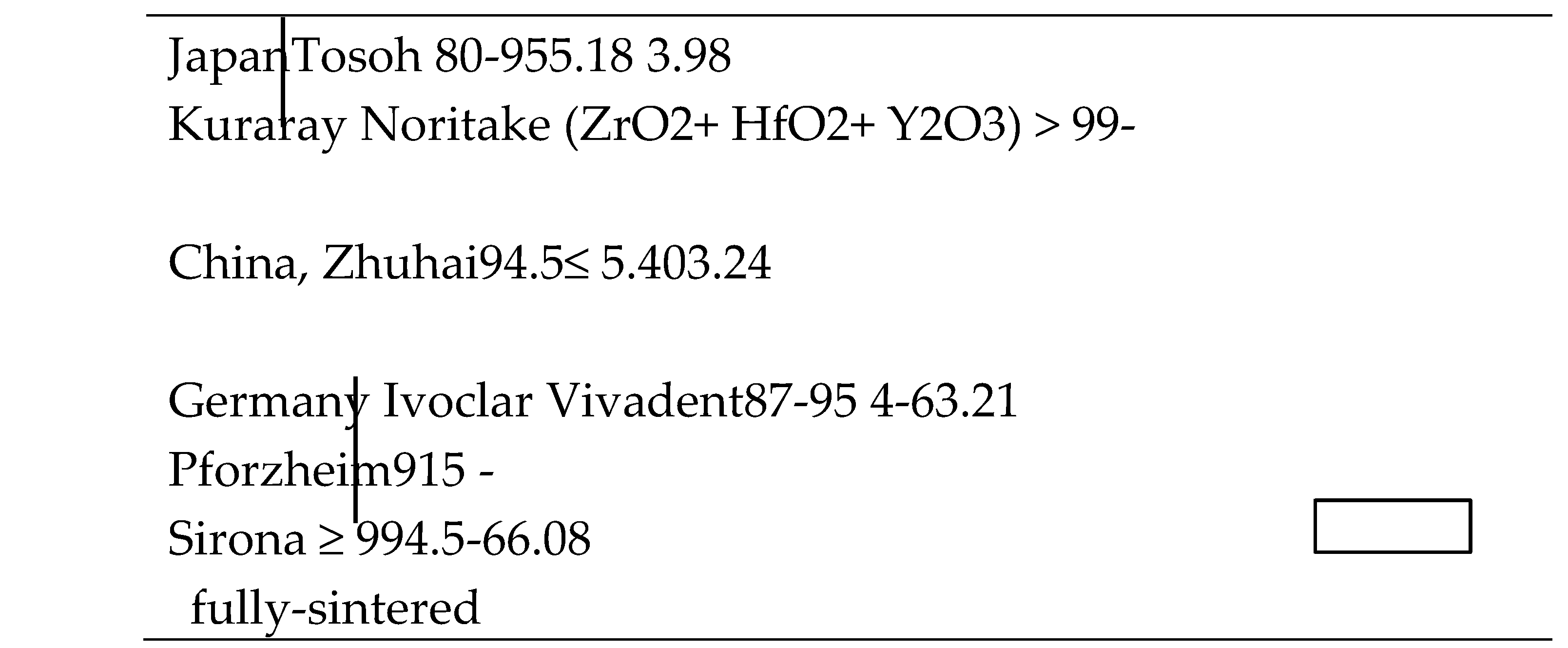
Zirconia bioceramics are materials with excellent strength, high fracture resistance and good chemical properties widely used in clinical applications like orthopedics, dentistry, etc. The structure of this material changes with temperature. They use stabilizing oxides to prevent structure from changing. In dental applications, tetragonal zirconia stabilized with 3 mole % of yttria (3Y-TZP) is usually used. The most common zirconia (3Y-TZP) is reported in Table. 3 in terms of constituent content and country of manufacture. Several generations of zirconia have been created with different compositions to improve transparency and mechanical properties. In the structural zirconia applications, it is necessary to employ chemical structures with high purity, because high purity materials can gain the required stability, especially when they are used in the body. This means that the higher the impurity in the raw materials, the lower the stability. For example, zirconia with yttria content of more than 4% wt provides more transparency, but reduces mechanical properties. As a result, the constituent contents of zirconia are significant and should be investigated.
To use zirconia in structural applications, it is necessary to sinter this material at a suitable temperature. Sintering is a process in which ceramics are baked and during which the properties of the material are constantly changing. Including grain size, structural phase, mechanical properties, etc. Of course, the machinability also changes with Sintering process. It is better to sinter zirconia for machining at a lower temperature and then complete the sintering process at higher temperatures to achieve the desired mechanical properties. Full sintering improves the mechanical properties of ceramics but reduces machinability, leading to long machining times and tool wear. Accordingly the sintering process affects the quality of the material and the final precision of machining. Additionally, the heating rate is important in sintering. The lower the heating rate, the better the material densification behavior. However, this difference does not affect the final sintering results.
The density of raw zirconia is between 3-4 g/cm³. And this value in sintered zirconia used in dental applications (the maximum density desired for using zirconia in dentistry) reaches 6.04 g/cm³. From the sintering temperature above 1300⁰c, the density of zirconia crosses the border of 5.73 g/cm³ and reaches 5.98 g/cm³ at the 1500⁰c sintering temperature. It can be concluded that a temperature above 1300⁰c represent the full sintering temperature for zirconia. And at the final temperature of 1600⁰c, it achieves the desired maximum density. The density is 4.11 g/cm³ at 1100⁰c sintering temperature and 5.13 g/cm³ at 1200⁰c sintering temperature. In view of this issue, it can be concluded the pre-sintering temperature should be up to 1200⁰c. So zirconia machining should be in these temperature ranges. On the other hand, the temperature above 1300⁰c was considered unsuitable for machining. Achieving the desired maximum density without grain growth is one of the main goals of sintering optimization in materials. Obviously, to improve these sintering results, a long experimental exploratory study is usually required. However, the two-step sintering method is suitable for optimizing the sintering path and controls the process of microstructure growth. The rate of contraction of zirconia decreases with increasing temperature and stops at 1500⁰c sintering temperature. Therefore, the shrinkage rate of zirconia can also be controlled by the sintering process. Two-step sintering is also useful for zirconia shrinkage due to grain growth rate control. Because the shrinkage rate is lower at the initial sintering temperature.
The values of the mechanical properties of zirconia (Table. 2) show that this material achieves desirable mechanical properties for use in high tolerance structures at high sintering temperatures. Zirconia is more formable at pre-sintering temperature. For this reason, it is recommended to be machined at pre-sintering temperatures. Definitely, many factors affect the mechanical properties. The loading rate also affects the mechanical properties. According to some authors, hardness and resistance to cracking and Young's modulus are independent of loading rate. There is also an opposite theory. Of course, it can be due to the range of selected loading rates in each research. However, it can be express it is difficult to predict the behavior of zirconia. It has been well established that zirconia has excellent properties in various fields. However, these properties depend on the selective process in the fabrication and processing of zirconia. In different researches, each of them introduced a different temperature as the optimal temperature for zirconia sintering. It is difficult to predict the behavior of zirconia from its mechanical properties and more studies are required. To provide valuable information, tests in the oral environment about the long-term performance of zirconia ceramics are needed. Zirconia must be carefully checked in the environment of use and failures and problems analyzed. It is expected that there will be significant improvements in the field of ceramics in the future.
References
- Min Ji, Jinyang Xu, Ming Chen, Mohamed El Mansori. Enhanced hydrophilicity and tribology behavior of dental zirconia ceramics based on picosecond laser surface texturing. Journal Pre-proof. [CrossRef]
- Deepti Upadhyay, Manoj A. Panchal, R.S. Dubey, V.K. Srivastava. Corrosion of alloys used in dentistry: A review. Materials Science and Engineering A 432 (2006) 1–11.
- Holand, W.; Schweiger, M.; Rheinberger, V.M.; Kappert, H. Bioceramics and their application for dental restoration. Adv. Appl. Ceram. 2009, 108, 373–380. [Google Scholar] [CrossRef]
- Min Ji, Heng Zhang, Jinyang Xu, Chao Li, Dedong Yu, Ming Chen, Mohamed El Mansori. Toward the mechanisms of surface texturing on the wear behavior of dental zirconia ceramics under dry and saliva lubricated conditions. [CrossRef]
- Isabelle Denry and Julie, A. Holloway. Ceramics for Dental Applications: A Review. Materials 2010, 3, 351–368; [Google Scholar] [CrossRef]
- Denry and, J.R. Kelly. Emerging Ceramic-based Materials for Dentistry. Journal of Dental Research (2014). [CrossRef]
- S. Zinelis, A. S. Zinelis, A. Thomas, K. Syres, N. Silikas, G. Eliades. Surface characterization of zirconia dental implants. Dental materials 26 (2010) 295–305.
- C. Piconi, G. C. Piconi, G. Maccauro. Zirconia as a ceramic biomaterial. (1997) Biomaterials 20 (1999) 1—25.
- H. G. Scott, “Phase Relationships in the Zirconia–Yttria System,” J. of Materials Science, Vol.10, No.9, pp. 1527-1535, 1975.
- David Grossin, Alejandro Monton, Pedro Navarrete-Segado, Eren O€zmen, GiovanniUrruth, Francis Maury, Delphine Maury, Christine Frances, Mallorie Tourbin, Pascal Lenormand,Ghislaine Bertrand. A review of additive manufacturing of ceramics by powder bed selective laser processing (sintering / melting): Calcium phosphate, silicon carbide, zirconia, alumina, and their composites. Open Ceramics 5 (2021) 100073.
- Graeve, O.A. (2008). Zirconia. In: Shackelford, J.F., Doremus, R.H. (eds) Ceramic and Glass Materials. Springer, Boston, MA. [CrossRef]
- Baldissara, P. , Llukacej, A., Ciocca, L., Valandro, F.L., Scotti, R., 2010. Translucency of zirconia copings made with different CAD/CAM systems School of Dentistry. J. Prosthet. Dent 104, 6–12.
- Guazzato, M. , Quach, L., Albakry, M., Swain, M.V., 2005. Influence of surface and heat treatments on the flexural strength of Y-TZP dental ceramic. J. Dent. 33, 9–18.
- Stawarczyk, B. , O ̈zcan, M., Roos, M., Trottmann, A., Sailer, I., Ha ̈mmerle, C.H.F., 2011. Load-bearing capacity and failure types of anterior zirconia crowns veneered with over pressing and layering techniques. Dent. Mater. 27, 1045–1053. [CrossRef]
- Tong, H. , Tanaka, C.B., Kaizer, M.R., Zhang, Y., 2016. Characterization of three commercial Y-TZP ceramics produced for their high-translucency, high-strength and high-surface area. Ceram. Int. 42, 1077–1085.
- Raigrodski AJ, Hillstead MB, Meng GK, Chung K-H. Survival and complications of zirconia-based fixed dental prostheses: A systematic review. J Prosthet Dent 2012; 107:170-7.
- Lameira DP, De Souza GM. Fracture strength of aged monolithic and bilayer zirconia-based crowns. BioMed Res Int 2015; 2015:418641.
- Jiang L, Liao Y, Wan Q, Li W. Effects of sintering temperature and particle size on the translucency of zirconium dioxide dental ceramic. Journal of materials science Materials in medicine 2011; 22:2429-35.
- Zhang Y, Lee JJ, Srikanth R, Lawn BR. Edge chipping and flexural resistance of monolithic ceramics. Dent Mater 2013; 29:1201-8.
- Isabelle Denry, J. Robert Kelly. State of the art of zirconia for dental applications. Dental materials 24 (2008) 299–307.
- Helmer JD, Driskell TD. Research on bioceramics. Symp. On Use of Ceramics as Surgical Implants. South Carolina (USA): Clemson University, 1969.
- Ossama Saleh Abd El-Ghany, Ashraf Husein Sherief. Zirconia based ceramics, some clinical and biological aspects: Review. Future Dental Journal 2 (2016) 55-64.
- F. Filser, P. Kocher, L.J. Gauckler. In vitro lifetime of dental ceramics under cyclic loading in water. Biomaterials. June 2007, Pages 2695-2705.
- Yin, L. , Huang, H., 2004a. Ceramic response to high speed grinding. Mach. Sci. Technol. 8 (1), 21–37.
- Chintapalli, R.K. , Jimenez-Pique, E., Marro, F.G., Yan, H., Reece, M., Anglada, M., 2012. Spherical instrumented indentation of porous nanocrystalline zirconia. J. Eur. Ceram. Soc. 32, 123–132.
- Z. Chen, Z. Li, J. Li, C. Liu, C. Lao, Y. Fu, C. Liu, Y. Li, P. Wang, Y. He, 3D printing of ceramics: a review, J. Eur. Ceram. Soc. 39 (2019) 661–687. [CrossRef]
- Eva Gregorová, Vojtěch Nečina, Soňa Hříbalová, Willi Pabst. Temperature dependence of Young’s modulus and damping of partially sintered and dense zirconia ceramics. Journal of the European Ceramic Society.
- Igor Danilenko, Marharyta Lakusta, Larisa Loladze, Galina Volkova, Inna Popov, Valentina Glazunova, Leonid Akhkozov, Andrii Shut, Tetyana Konstantinov. Paradoxes of the initial stages of sintering of zirconia nanoparticles. Results in Physics 42 (2022) 106027.
- Rajendra, K. Bordia, Suk-Joong L. Kang and Eugene A. Olevsky. CURRENT UNDERSTANDING AND FUTURE RESEARCH DIRECTIONS AT THE ONSET OF THE NEXT CENTURY OF SINTERING SCIENCE AND TECHNOLOGY. 10.1111/jace.14919.
- Min Ji, Jinyang Xu, Dedong Yu, Ming Chen, Mohamed El Mansori. Influence of sintering temperatures on material properties and corresponding milling machinability of zirconia ceramics. Journal of Manufacturing Processes 68 (2021) 646–656.
- Min Ji, Jinyang Xu, Linfeng Li, Dedong Yu, Ming Chen, Mohamed El Mansori. Nano-scale mechanical behaviors and material removal mechanisms of zirconia ceramics sintered at various temperatures. Ceramics International 47 (2021) 32588–32598.
- Filser, FT. Direct ceramic machining of ceramic dental restorations: ETH Zurich. 2001.
- Charles Maniere, Geuntak Lee, Joanna McKittrick, Shirley Chan, Eugene A. Olevsky. Modeling zirconia sintering trajectory for obtaining translucent submicronic ceramics for dental implant applications. Acta Materialia 188 (2020) 101107.
- Tonino Traini & Enrico Gherlone & Stefano Ferrari Parabita & Sergio Caputi & Adriano Piattelli. Fracture toughness and hardness of a Y-TZP dental ceramic after mechanical surface treatments. Clin Oral Invest (DOI 10.1007/s00784-013-1018-z).
- Hao L, Lawrence J, Chian KS, Osteoblast cell adhesion on a laser modified zirconia based bioceramics, J. Mater. Sci. Mater. M. 16 (2005) 719-726.
- Zheng K, Li Z, Liao W, Xiao X. Friction and wear performance on ultrasonic vibration assisted grinding dental zirconia ceramics against natural tooth. J Braz Soc Mech Sci Eng 2017;39(3):833–43.
- Carlo Monaco, Antonella Tucci, Leonardo Esposito, Roberto Scotti. Microstructural changes produced by abrading Y-TZP in presintered and sintered conditions. Journal of dentistry 41 (2013) 121–126.
- Min Ji, Jinyang Xu, Linfeng Li, Dedong Yu, Ming Chen, Norbert Geier, Mohamed El Mansori. Investigation of material removal mechanisms and ductile-brittle transition zone of zirconia ceramics sintered at various temperatures. Journal of the mechanical behavior of biomedical materials 125 (2022) 104944.
- Sachs, C. , Groesser, J., Stadelmann, M., Schweiger, J., Erdelt, K., Beuer, F., 2014. Full- arch prostheses from translucent zirconia: accuracy of fit. Dent. Mater. 30, 817–823.
- Noor Faeizah Amat, Andanastuti Muchtar, Hsu Zenn Yew, Muhammad Sufiyan Amril, Rahimi L. Muhamud. Machinability of a newly developed pre-sintered zirconia block for dental crown applications. [CrossRef]
- Jaroslav Kastyl, Zdenek Chlup, Premysl Stastny, Martin Trunec. Machinability and properties of zirconia ceramics prepared by gelcasting method. Advances in Applied Ceramics on 11 Oct 2019. [CrossRef]
- Mizuho Hirano, Syuntaro Nomoto, Toru Sato, Mamoru Yotsuya, Ryuichi Hisanaga, Hideshi Sekine. Sintering distortion of monolithic zirconia in 4-unit fixed partial denture: Effect of layered structure and vertical milling area. Journal of the mechanical behavior of biomedical materials 128 (2022) 105078.
- Pereira GKR, Silvestri T, Amaral M, Rippe MP, Kleverlaan CJ, Valandro LF. Fatigue limit of polycrystalline zirconium oxide ceramics: Effect of grinding and low-temperature aging. J Mechanic Behav Biomed Mater 2016; 61: 45-54.
- J. Chevalier, L. J. Chevalier, L. Gremillard, S. Deville, Low-temperature degradation of zirconia and implications for biomedical implants, Annu. Rev. Mater. Res. 37 (2007) 1–32.
- Chevalier J, Cales B, Drouin JM. Low-temperature aging of Y-TZP ceramics. J Am Ceram Soc 1999; 54:2150–4. [CrossRef]
- Garvie RC, Nicholson PS (1972). Phase analysis in zirconia systems. J Am Ceram Soc 55:303-305.
- Swab, JJ. Low temperature degradation of Y-TZP materials. J Mater Sci 1991; 26:6706—14.
- F. Filser, P. Kocher, L.J. Gauckler. In vitro lifetime of dental ceramics under cyclic loading in water. Biomaterials. June 2007, Pages 2695-2705.
- Lucas TJ, Lawson NC, Janowski GM, Burgess JO. Effect of grain size on the monoclinic transformation, hardness, roughness, and modulus of aged partially stabilized zirconia. Dent Mater 2015; 1:1487–92. 1. [CrossRef]
- Camposilvan E, Marro FG, Mestra A, Anglada M. Enhanced reliability of yttria-stabilized zirconia for dental applications. Acta Biomater 2015; 17:36–46. [CrossRef]
- Noor Faeizah Amat, Andanastuti Muchtar, Muhammad Sufiyan Amril, Mariyam Jameelah Ghazali, Norziha Yahaya. Effect of sintering temperature on the aging resistance and mechanical properties of monolithic zirconia. [CrossRef]
- Christel P, Meunier A, Dorlot J-M et al. Biomechanical compatibility and design of ceramic implants for orthopedic surgery. Bioceramics: material characteristics versus in vivo behavior. Ann NY Acad Sci 1988; 523:234—56.
- Chevalier J, Drouin JM, Cale ́ s B. Low temperature ageing behavior of zirconia hip joint heads. In: Sedel L, Rey C, editors. Bioceramics 10, Amsterdam, Elsevier, 1977:135—7.
- Hummer CD, Rothman RH, Hozack WJ. Catastrophic failure of modular zirconia ceramic femoral head components after total hip arthroplasty. J Arthr 1995; 10(6):848—50.
- Garvie RC, Hannink RH, Pascoe RT. Ceramic steel? Nature 1975; 258:703–4.
- Yoichiro Ichikaw, DDS, Yasumas, Akagaw, DDS, PhD, Hirosama Nikai, DDS, PhD, and Hiromichi Tsuru, DDS, PhD. Tissue compatibility and stability of a new zirconia ceramic in vivo. THE JOURNAL OF PROSTHETIC DENTISTRY. AUGUST 1992 VOLUME 68 NUMBER 2. 10/l/36697.
- Suarez MJ, Lozano JF, Paz Salido M, Martinez F. Three-year clinical evaluation of In-Ceram Zirconia posterior FPDs. International Journal of Prosthodontic 2004;17:35–8.
- Abdur-Rasheed Alao, Ling Yin. Nanoindentation characterization of the elasticity, plasticity and machinability of zirconia. [CrossRef]
- Abdur-Rasheed Alao, Ling Yin. Nano-scale mechanical properties and behavior of pre-sintered zirconia. Journal of the mechanical behavior of biomedical materials 36 (2014) 21–31.
- M. Sakai, Meyer hardness: a measure for plasticity? J. Mater. Res. 14 (9) (1999) 3630–3639.
- Abdur-Rasheed Alao, Ling Yin. Loading rate effect on the mechanical behavior of zirconia in nanoindentation. Materials Science & Engineering A 619 (2014) 247–255.
- Eleftheria Tsalouchou, Mike J. Cattell, Jonathan C. Knowles, Piyapanna Pittayachawan, Ailbhe McDonald. Fatigue and fracture properties of yttria partially stabilized zirconia crown systems. Dental materials 24 (2008) 308–318.
- Haixin QIAN, Chang CUI, Tingshu SU, Fuqiang ZHANG and Jian SUN. Exploring the optimal pre-sintering temperature on compressive strength and anti-fatigue property of graded zirconia-based glass/zirconia structure. Dental Materials Journal 2016; 35(3): 341–344.
- Mina Mohaghegh, Sajad Baseri, Mohammad Hassan Kalantari, Rashin Giti, Seyed Ahmad Ghoraishian. Influence of Sintering Temperature on the Marginal Fit and Compressive Strength of Monolithic Zirconia Crowns. J Dent Shiraz Univ Med Sci.
- Bogna Stawarczyk & Mutlu Özcan & Lubica Hallmann & Andreas Ender & Albert Mehl & Christoph H. F. Hämmerlet. The effect of zirconia sintering temperature on flexural strength, grain size, and contrast ratio. Clin Oral Invest (2013) 17:269–274.
- Paolo Francesco Manicone, Pierfrancesco Rossi Iommetti, Luca Raffaelli. An overview of zirconia ceramics: Basic properties and clinical applications. Journal of dentistry 35 (2007) 819–826.
- Tateishi T, Yunoki H. Research and development of alumina and zirconia artificial hip joint. Clin Mater 1993; 12:219—25.
- Abdur-Rasheed Alao, Ling Yin. Assessment of Elasticity, Plasticity and Resistance to Machining-induced Damage of Porous Pre-sintered Zirconia Using Nanoindentation Techniques. Journal of Materials Science & Technology 32 (2016) 402–410.
- M. Alauddin, M.A. El Baradie, M.S.J. Hashmi. Tool-life testing in the end milling of Inconel 718. Journal of Materials Processing Technology 55 (1995) 321-330.
- ISO 8688-1, Tool life testing in milling - Part 1: Face milling, 1989 (E).
- Suh, M. , Chae, Y. and Kim, S. (2008) Friction and wear behavior of structural ceramics sliding against zirconia. Wear. 264 (9-10), pp. 800-806.
- Nasrin, S. , Katsube, N., Seghi, R. and Rokhlin, S. (2016) 3D statistical failure analysis of monolithic dental ceramic crowns. Journal of Biomechanics. 49 (10), pp. 2038-2046.
- ISO 8688-2, Tool life testing in milling - Part 2: End milling, 1989 (E) z.
- Tamizharasan, T. , Selvaraj, T. and Noorul Haq, A. (2005) Analysis of tool wear and surface finish in hard turning. The International Journal of Advanced Manufacturing Technology. 28 (7-8), pp. 671-679.
- S. Malkin (1). T. W. Hwang, Department of Mechanical b Industrial Engineering, Engineering Lab Building, University of Massachusetts, Amherst, MA, USA. Grinding Mechanisms for Ceramics. Annals of the ClRP Vol. 45/2/7996.
- Jinyang Xu, Min Ji, Linfeng Li, and Ming Chen. Evaluation of Polycrystalline Diamond Tools in Milling of Pre-Sintered and Fully-Sintered Zirconia Ceramics. Journal of Superhard Materials, 2022, Vol. 44, No. 1, pp. 62–69.
- Anandita Singh, Divyanshu Solanki, Rohit Sencha, Ritesh K. Singh, Rakesh G. Mote, Ramesh K. Singh. Study and characterization of the ductile-brittle transition zone in sintered zirconia. Journal of Manufacturing Processes 58 (2020) 749–762.
- Suya Prem Anand P, Arunachalam N, Vijayaraghavan L. Effect of grinding on subsurface modifications of pre-sintered zirconia under different cooling and lubrication conditions. J Mech Behav Biomed Mater 2018;86:122–30.
- Diniz, A. and Filho, J. (1999) Influence of the relative positions of tool and workpiece on tool life, tool wear and surface finish in the face milling process. Wear. 232 (1), pp. 67-75.
- Ha SJ, Shin BC, Cho MW, Lee KJ, Won-Seung C. High speed end milling characteristics of pre-sintered Al2O3/Y-TZP ceramic composites for dental applications. J Ceram So JPN 2010;118:1053–6.
- David Irvine, Wan Tsin Goh, Farid Dailami & Jason Matthews. The analysis of tool wear mechanisms in the machining of pre-sintered zirconia dental crowns. Procedia Manufacturing 38 (2019) 1026–1033.
- Tomofumi Sawada, Christine Schille, Judit Zöldföldi, Ernst Schweizer, Jürgen Geis-Gerstorfer, Sebastian Spintzyk. Influence of a surface conditioner to pre-sintered zirconia on the biaxial flexural strength and phase transformation. [CrossRef]
- Dalia, I. El-korashy, Dina A. El-Refai. Mechanical Properties and Bonding Potential of Partially Stabilized Zirconia Treated with Different Chemo mechanical Treatments. J Adhes Dent 2014; 16: 365-376.
- Eva Gregorova ́, Linda Semradova, Ivona Sedlarova ́, Vojtech Necina, Sona Hríbalova ́, Willi Pabst. Microstructure and Young’s modulus evolution during re-sintering of partially sintered alumina-zirconia composites (ATZ ceramics). Journal of the European Ceramic Society 41 (2021) 3559-3569.
- Alao, A. and Yin, L. (2014) Prediction of the resistance to machining-induced cracking in zirconia by Nano indentation. Recent Advances in Structural Integrity Analysis - Proceedings of the International Congress (APCF/SIF-2014). pp. 580-584.
- Abdur-Rasheed Alao, Richard Stoll, Xiao-Fei Song, Takashi Miyazaki, Yasuhiro Hotta, Yo Shibata, Ling Yin. Surface quality of yttria-stabilized tetragonal zirconia polycrystal in CAD/CAM milling, sintering, polishing and sandblasting processes. Journal of the mechanical behavior of biomedical materials 65 (2017) 102–116.
- Jonathan Grech, Elsa Antunes. Optimization of two-step sintering conditions of zirconia blanks for dental restorations. Ceramics International 46 (2020) 24792–24798.
- Mazaheri M, Simchi A, Golestani-Fard F. Densification and grain growth ofnanocrystalline 3Y-TZP during two-step sintering. J Eur Ceram Soc 2008;28(15):2933–9.
- Stevan, M. Cokic, Jef Vleugels, Bart Van Meerbeek, Bernardo Camargo, Evita Willems, Maoyin Li,Fei Zhang. Mechanical properties, aging stability and translucency of speed-sintered zirconia for chairside restorations. Dental materials. [CrossRef]
- Maginnis S, Carden R, Szeremeta A, Paskalov G. Method of rapid sintering of ceramics. US Patent US8845951B2 (2014).
- Chun-Chuan Yang, Shinn-Jyh Ding, Tzu-Hao Lin, Min Yan. Mechanical and optical properties evaluation of rapid sintered dental T zirconia. Ceramics International 46 (2020) 26668–26674.
- Andrea Ordoñez Balladares, Cristian Abad-Coronel, Joao Carlos Ramos and Benjamín José Martín Biedma. Fracture Resistance of Sintered Monolithic Zirconia Dioxide in Different Thermal Units. Materials 2022, 15, 2478. [CrossRef]
- Perihan Oyar, PhD, Rukiye Durkan, PhD, and Gonca Deste, PhD. Effects of sintering time and hydrothermal aging on the mechanical properties of monolithic zirconia ceramic systems. THE JOURNAL OF PROSTHETIC DENTISTRY. [CrossRef]
- Rukiye Durkan, DDS, PhD, Gonca Deste Gökay, DDS, MS, Hatice S ̧ims ̧ek, DDS, MS, and Burak Yilmaz, DDS, PhD. Biaxial flexural strength and phase transformation characteristics of dental monolithic zirconia ceramics with different sintering durations: An in vitro study. THE JOURNAL OF PROSTHETIC DENTISTRY. [CrossRef]
- Jenni Hjerppe, Pekka K. Vallittu, Kaj Fröberg, Lippo V.J. Lassila. Effect of sintering time on biaxial strength of zirconium dioxide. Dental materials 25 (2009) 166–171.
- Mi-Jin Kim, DT, MS, Jin-Soo Ahn, DDS, PhD, Ji-Hwan Kim, MPH, PhD, Hae-Young Kim, DDS, PhD, Woong-Chul Kim, MPH, PhD. Effects of the sintering conditions of dental zirconia ceramics on the grain size and translucency. J Adv Prosthodont 2013; 5:161-6.
- Yusuke Ito, Naohiko Sugita, Tatsuya Fujii, Toru Kizaki, and Mamoru Mitsuishi. Precision Machining of Sintered Zirconia Ceramics by High-Speed Milling. Int. J. of Automation Technology Vol.11 No.6, 2017.
- Yusen Shui, Yuqiang Zhang, Tian Luo, Manlin Sun, Tinglu Fang, Qin Wu, Jikui Sun, Haiyang Yu.The mechanical properties, tribological behaviors and color stability of a feldspar Nano ceramics strengthening extrinsic stain for high-translucent zirconia. Journal of the Mechanical Behavior of Biomedical Materials. April 2023, 105698.
- Raigrodski, AJ. Contemporary materials and technologies for all-ceramic fixed partial dentures: a review of the literature. Journal of Prosthetic Dentistry 2004; 92:557–62.
- Luthy H, Filser F, Loeffel O, Schumacher M, Gauckler LJ, Hammerle CH. Strength and reliability of four-unit all- ceramic posterior bridges. Dental Materials 2005; 21: 930–7.
- Muhammad Arif, Zhang Xinquan, Mustafizur Rahman, Senthil Kumar. A predictive model of the critical undeformed chip thickness for ductile–brittle transition in nano-machining of brittle materials. International Journal of Machine Tools & Manufacture 64 (2013) 114–122.
- Shoichi Shimada (2), Naoya lkawa (I), Dept. of Precision Engineering, Osaka University Toyoshiro Inamura, Nobuhiro Takezawa, Nagoya Institute of Technology Hitoshi Ohmori, RlKEN Institute of Physical and Chemical Research Toshio Sata ( I ). Brittle-Ductile Transition Phenomena in Micro indentation and Micromachining. Annals of the ClRP Vol. 44/1/1995.
- Wenz HJ, Bartsch J, Wolfart S, Kern M. Osseointegration and clinical success of zirconia dental implants: a systematic review. Int J Prosthodont 2008; 21:27–36.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



