
Submitted:
21 April 2024
Posted:
23 April 2024
You are already at the latest version
Abstract
Coronary heart disease (CHD) has become a prevalent issue in Indonesia, resulting in a majority of fatalities and illnesses. The most recent guidelines in the United States for managing patients with chronic coronary syndrome (CCS) have undergone significant changes, with the recommendation for conducting percutaneous coronary intervention (PCI) strictly limited to patients who continue to experience symptoms despite receiving optimal medical treatment (OMT). However, adopting this approach may lead to increased morbidity and mortality due to the presence of vulnerable plaque. Vulnerable plaque is characterized by minimal obstruction during coronary angiography (40-70%) and may not produce ischemia during physiological studies. Identifying vulnerable plaques can be accomplished through several methods, among which computed tomography coronary angiography (CTCA) is the most cost-effective approach. Recently, experts have employed different techniques, either with stents or drug-coated balloons, to manage vulnerable plaques, showing the methods to be safe and effective. The other challenge faced by patients with CCS is the possibility of achieving complete revascularization (CR) to reduce the likelihood of future major adverse cardiac events (MACE) and mortality. Both approaches, identifying and intervening in the vulnerable plaque, are difficult to perform in developing countries due to the limited budget. Studies have shown that plant-based diets (PBD) can reverse atherosclerotic plaque and stabilize vulnerable plaque, possibly leading to CR. PBD is an affordable and effective approach, but it requires healthcare providers skilled in educating and implementing this dietary approach with their patients. Large-scale randomized controlled trials in PBD, specifically aimed at addressing the vulnerable plaque and achieving CR, are necessary before implementing the PBD intervention.
Keywords:
plant based diet
; complete revascularization
; vulnerable plaque
1. Introduction
The prevalence of CHD is growing in Indonesia. CHD is the most widespread form of heart disease and is the primary cause of death and illness in Indonesia. The burden is significantly higher than in other Southeast Asian countries [1]. In the past, it was believed that PCI was the solution to decrease the morbidity and mortality of patients with CHD. Historically, interventional cardiologists typically performed stent procedures for patients with blockage ≥ 70% of patients with CCS, representing the largest proportion of PCI utilization. This practice caused a high burden on the government since the majority of CHD patients utilized government-funded healthcare to cover the cost of their health problems. Recently, the US government recognized the opposition to this practice and has started implementing an alternative approach, i.e., OMT and lifestyle changes, instead of performing PCI as the first indication for patients with CHD.
The most current guidelines [2] suggest that patients with CCS should initially attempt intensive medical treatment or OMT and lifestyle adjustments. The employment of PCI plus OMT ought to be limited to a few specific cases, given that OMT yields the same cardiovascular outcomes as PCI plus OMT. These decisions were based on various studies, including the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial. This trial included 2287 patients diagnosed with severe CHD and a CCS score and were randomly assigned to receive either PCI in combination with OMT or OMT alone [3]. The results showed that stenting in a coronary artery did not reduce the risk of death, myocardial infarction, or other MACE compared to OMT alone, and there were no significant differences in the improvement of anginal symptoms between the two groups. In a double-blind, randomized, placebo-controlled trial known as the Objective Randomized Blinded Investigation with Optimal Medical Therapy of Angioplasty in Stable Angina (ORBITA), 230 patients with ischemic symptoms were randomly assigned to either PCI or OMT. The primary endpoint was exercise tolerance at the end of six weeks. The study authors concluded that PCI did not increase exercise tolerance more than patients who received solely OMT [4]. In 2020, the International Study of Comparative Health Effectiveness with Medical and Invasive Approaches (ISCHAEMIA) trial was published, a randomized controlled trial comparing PCI and OMT for 5179 patients with CCS. This study demonstrated no significant difference in ischemic CV events or mortality between treatment groups over a median of 3.2 years [5]. Therefore, patients with CCS who fit the profile of those in ISCHAEMIA and do not have left main of at least 50%, left ventricular systolic function <35%, New York Heart Association Class III or IV heart failure, and estimated glomerular filtration rate (eGFR) <30ml/min, or have unacceptable angina despite OMT, can be treated with OMT alone. However, according to the ISCHAEMIA study, patients who underwent PCI had better quality of life measures than those in the OMT arm [6]. Recently, Stone et al. conducted a sub-analysis of the ISCHAEMIA trial and concluded that the clinical outcomes of patients in the PCI arm may be improved if complete revascularization (CR), particularly anatomic complete revascularization or ACR, is achieved [7]. The result was not surprising given that various studies have indicated higher survival rates and a decreased incidence of MACE after achieving CR in patients with multivessel disease through either coronary artery bypass graft surgery (CABG) or PCI, as opposed to incomplete revascularization (ICR). However, achieving CR might not always be possible due to the patient’s comorbidities, anatomical constraints, technical limitations, procedural considerations, and financial limitations. According to certain studies, ACR is considered to have been achieved if all coronary vessels larger than 2 mm with stenoses greater than 50% are treated [8]. However, the cost-effectiveness of this approach should be considered, along with its potential risks, such as ISR and ST. Experts assert that incorporating CR is essential to surpass OMT’s accomplishments, particularly in the context of managing vulnerable plaques that may contribute to future cardiac events [7].
One limitation of PCI is the tendency to underestimate low-grade stenosis (less than 50%), which is actually responsible for 68% of myocardial infarctions (MI) [9]. Stenosis of this type may indicate a vulnerable plaque, which is often ignored and may not receive the appropriate treatment. The topic of vulnerable plaque and its significance has recently garnered attention from researchers. A variety of advanced, invasive diagnostic tools are currently available for detecting vulnerable plaques, including IVUS in combination with OCT, or hybrid IVUS-OCT/OFDI, NIRS-IVUS (near-infrared spectroscopy), NIRF-IVUS (near-infrared fluorescence), IVPA-IVUS (molecular imaging intravascular photoacoustics), and TRFS-IVUS (time-resolved fluorescence spectroscopy) [10,11]. However, these highly sophisticated tools are not widely accessible in developing countries like Indonesia due to their high cost. One option is to use CTCA, but interpreting vulnerable plaque with CTCA may require an experienced radiologist.
Recent publications have emphasized the importance of intervening vulnerable plaques to reduce MACE and improve patient survival. It is important to note that vulnerable plaque may not cause clinical ischemia or even show negative results in invasive functional tests, such as FFR. However, it may put the patient at risk for future clinical events. If asymptomatic individuals exhibit stenosis ranging from 40-70%, according to the 2023 ACC/AHA guideline for managing CCS, they should receive OMT rather than undergoing additional testing to identify vulnerable plaque [12]. Evading such testing could compromise certain patients, leading to an increased risk of future MACE or mortality. To add to the situation’s complexity, it has been demonstrated that nearly half of individuals who undergo PCI have remaining vulnerable plaque [13].
Park SJ et al. recently published a noteworthy paper titled “Preventive PCI versus OMT alone for the treatment of vulnerable atherosclerotic coronary plaques (PREVENT).” This study was a multicenter randomized controlled trial that demonstrated that patients with non-flow-limiting vulnerable plaques (angiographic stenosis of 47-66%) experienced a reduction in MACE when they received preventive PCI using stenting, as opposed to the OMT-only approach. Given that PREVENT is the first large trial involving 1606 patients to show the potential effect of the local treatment on vulnerable plaques, these findings support consideration to expand indications for PCI to include non-flow-limiting high-risk vulnerable plaques [14,15]. Unfortunately, we may face other drawbacks associated with stent use, such as in-stent restenosis (ISR) and stent thrombosis (ST). Considering the challenges, various researchers find the technology of drug-coated balloons (DCB) appealing, as it offers the advantage of not leaving anything behind, allowing the endothelium of the coronary vessel to heal properly and retain its vasomotor function. In late 2023, a study conducted by van Veelen et al. (DEBuT-LRP) demonstrated the safety and viability of using DCBs to stabilize vulnerable plaque, thereby preventing future adverse events [16]. However, the study only included a few patients and utilized NIRS-IVUS, a technology not widely available. The full report of this study is expected to be published in the near future. To adequately justify the implementation of PCI using either a stent or DCB, the interventionalist must ensure that the potential risks associated with such procedures are significantly lower than those associated with vulnerable plaques. The long-term risks of such procedures should also be considered when making this determination. Important to note our previous publication has emphasized the substantial reduction in the risk of developing ISR and ST in individuals who have undergone PCI with stenting and adhered to PBD [17]. This finding makes interventions with DCB for vulnerable plaques more appealing.
Managing patients with a substantial coronary plaque burden who are asymptomatic and exhibit intermediate obstruction (40-70%) presents a significant challenge in the field of cardiology. Although these lesions may not cause significant narrowing of the arteries, research has shown that they are a major predictor of cardiovascular events and death [18]. Therefore, it is important to carefully monitor and manage these patients to reduce their risk of adverse outcomes. Remember that guidelines, although beneficial, are not mandatory and are subject to change over time as new ideas emerge from innovative and daring individuals who strive to improve the academic world. If no one were to challenge the status quo, guidelines would remain static and unchanged since their initial release.
2. Discussion
2.1. Plant-Based Diets as the Solution to Treat Vulnerable Plaque in CCS Patients
Numerous studies have underscored the critical significance of PBDs in managing chronic inflammatory diseases, including atherosclerosis, hyperlipidemia, obesity, non-insulin-dependent diabetes mellitus (NIDDM), and hypertension. It has been widely acknowledged that PBD may not only contribute to the prevention of atherosclerosis but may also cause regression of coronary plaques that have occurred [19,20,21,22,23,24,25]. Previous research has indicated that PBDs possess the potential to rectify metabolic abnormalities, restore endothelial function, reduce systemic inflammation, enhance the availability of nitric oxide (NO), anti-thrombotic properties, combat reactive oxygen species (ROS), immune-modulating, foster healthy microbiota, correct mitochondrial dysfunction, and improve telomere as part of epigenetic adjustments. Through these actions, PBDs may regress atherosclerosis and reverse or stabilize the vulnerable plaque [17,26,27,28,29,30,31,32].
Vulnerable plaque, a particularly dangerous form of atherosclerosis, is characterized by a large lipid core, a thin fibrous cap, and neovascularization, all of which exacerbate the plaque’s susceptibility to rupture and increase the likelihood of MACE and death [16]. Pathobiologically, vulnerable plaque is a systemic disease resulting from metabolic dysfunction and chronic inflammation rather than a localized process. It, therefore, should be classified as a metabolic chronic inflammatory condition. Patients who have experienced coronary obstruction due to the vulnerable plaque typically exhibit a state of metabolic disorder and systemic inflammation for an extended period of time. Cardiologists who exclusively employ interventions such as using stent implantation or DCB technology to manage systemic diseases are likely to be disappointed if they do not address these systemic issues. After undergoing coronary interventions, the initial balloon dilatation process causes localized arterial deformation, and the insertion of a foreign substance, such as a stent or the utilization of DCB, triggers the healing process for the resulting injury. This may lead to complications such as ISR or ST. Fortunately, PBDs have been shown to significantly reduce the incidence of ISR and ST [17]. Thus, it is crucial to recognize that even after treating a vulnerable plaque properly with PCI, there is still a possibility that a new vulnerable plaque may develop if we fail to address the systemic issue of our patients.
Results from clinical trials comparing PCI plus OMT versus OMT alone have been disappointing for PCI plus OMT, as interventional cardiologists often disregard the systemic and metabolic issues of their patients, leading to increased MACE and mortality following PCI. Furthermore, they may not be able to perform CR due to intricate, challenging coronary anatomies or high-risk interventions that can only be performed at top centers with minimal complications. Therefore, studies have shown that although CR can potentially reduce MACE and cardiac death, it is achieved in approximately 50% of PCI cases [33,34,35,36,37,38,39]. Moreover, as previously mentioned, these vulnerable plaques are often overlooked.
Eating poor-quality food high in sugar (refined carbohydrate), devoid of fiber-phytonutrients, highly processed, and contains saturated and trans fats, cholesterol, and chemicals that promote chronic inflammation is a major contributor to the development of vulnerable plaque in the first place. The consumption of these unhealthy foods has been demonstrated to increase levels of LDL cholesterol, triglycerides, apolipoprotein (a), apolipoprotein (b), C-reactive protein (CRP), pro-inflammatory mediators, pro-inflammatory chemokines/ cytokines, Trimethylamine N-oxide (TMAO), persistent organic pollutants (POPs), oxidative stress, tumor promotion, and cell proliferation, among other factors will make plaque progress and become more vulnerable [40,41]. On the contrary, eating healthy PBD with adequate supplementation will enhance our body’s ability to fight against inflammation. Healthy foods such as vegetables, fruits, and legumes contain carotenoids, isoflavones, phytoestrogens, and phytosterols, which have been shown to prevent atherosclerosis. These polyphenols and phytochemicals’ role in molecular signaling are anti-inflammatory, antiplatelet aggregation, inhibitor to VSMCs proliferation and migration, and safeguard for lipid oxidation [42,43]. Oxidized LDL (ox-LDL), in addition to its infamous role in causing atherosclerosis, also plays a significant part in developing vulnerable plaque [44]. Healthy PBD can also help improve endothelial function, which is essential to maintaining plaque stability.
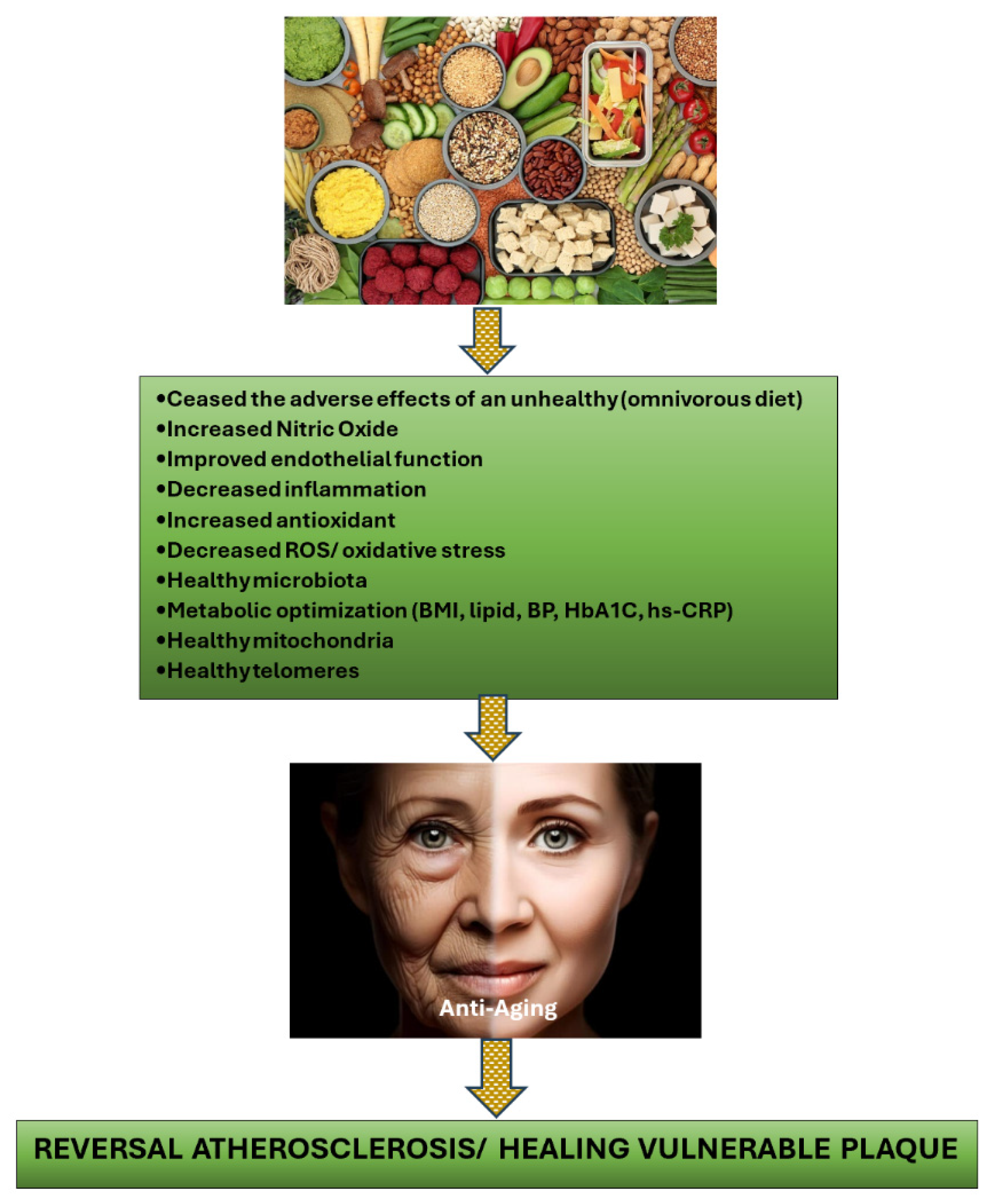
Adopting a diet abundant in PBD can effectively counteract atherosclerotic plaque and bolster vulnerable plaque stability by preventing the consumption of foods that contribute to the formation of vulnerable plaque in the first place. These unhealthy eating habits have also been implicated in dyslipidemia, insulin resistance, hypertension, glucose intolerance, endothelial dysfunction, chronic systemic inflammation, heightened oxidative stress, elevated trimethylamine N-oxide (TMAO), low nitric oxide (NO), gut dysbiosis, mitochondrial damage, and shortened telomeres (accelerating aging) [17,45,46,47,48,49]. All of these factors are widely recognized as risk factors for the development of atherosclerosis and play a crucial role in creating vulnerable plaque. Figure 1 illustrates the various mechanisms through which PBD plays a role in reversing atherosclerosis and hampering vulnerable plaques.
2.2. Supplements Are Compulsory for PBD Followers
It is crucial for individuals who utilize PBD for regressing vulnerable plaque purpose, to pay close attention to their food choices and consume items that possess properties that suppress inflammation, combat oxidative stress, increase NO availability, support healthy microbiota, strengthen mitochondria, heal telomeres, and exhibit anti-thrombotic properties [17]. The precise quantity of these foods must also be determined to prevent nutrient deficiencies (protein, Omega 3, B12, D, K2, Fe, Zn, Cu, and Se), and the food processing method should be carefully considered to ensure maximum benefit. For instance, to obtain the highest NO source from vegetables, consuming them raw rather than cooked is recommended.
Many nutrition experts have specifically emphasized the deficiency of essential nutrients in PBDs, such as vitamins B12 and D, and minerals, like iodine, iron, zinc, selenium, and calcium, which can have detrimental effects, particularly for pregnant individuals [50,51]. In this context, in addition to employing the PBDs program, it is recommended to include supplementations with vitamin C, vitamin D, vitamin K2, vitamin B3/NAD+, zinc, copper, selenium, and natural anti-inflammatory products, such as astaxanthin, curcumin, quercetin, CoQ10, taurine, and multivitamins (containing various small doses of minerals and vitamins as recommended for daily RDA). These supplements ensure no nutrient deficiency occurs when following PBDs and enhance the anti-inflammatory, antioxidant, immunomodulator, repair mitochondria, and strengthen telomere, which will be useful in the anti-aging process, including regressing coronary plaques.
3. Conclusion
Being diagnosed with coronary stenosis of 40-70% on coronary angiography does not necessarily imply that it is benign, as it does not require intervention. However, studies have shown that 68% of acute myocardial infarctions (AMIs) are caused by coronary obstruction less than 50%. This peculiar phenomenon is likely due to a vulnerable plaque [9]. Recent developments have suggested that identifying the presence of a vulnerable plaque and intervening before it causes acute coronary syndrome or mortality is beneficial [15,16]. However, sophisticated diagnostic tools are not available in hospitals in upper-middle-income countries such as Indonesia, and intervening with PCI to treat such plaques may not be cost-effective. Similarly, applying CR may not be possible in Indonesia except for certain patients. The article emphasizes the crucial function of PBDs in decreasing the occurrence of ISR and ST following PCI, regressing atherosclerosis, and stabilizing vulnerable plaques. This approach is cost-effective and successful in decreasing the incidence of MACE and mortality among CCS patients, frequently caused by vulnerable plaques. The PBD approach has demonstrated efficacy in retarding the progression of atherosclerosis, particularly in vulnerable plaques. By inducing regression in all plaques that have the potential to cause MACE and mortality in the future, this method may accomplish CR.
Patients may not find it effective to modify their lifestyle without proper guidance. Medical practitioners must thoroughly understand lifestyle programs, including selecting appropriate foods in the right quantities, optimizing food quality, and knowing the appropriate processing methods. They must also be knowledgeable about avoiding nutrient deficiencies while following the program. Moreover, understanding the role of vitamins, minerals, and nutraceuticals, particularly those that can aid in plaque regression, is crucial.
Author Contributions
D.M.; Conceptualization, and Writing-review and editing.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
References
- Muharram FR, Multazam CECZ, Mustofa A, et al. The 30 Years of Shifting in The Indonesian Cardiovascular Burden- Analysis of The Global Burden of Disease Study. Journal of Epidemiology and Global Health. 2024. [CrossRef]
- Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023 Aug 29;148(9):e9-e119. doi: 10.1161/CIR.0000000000001168. Epub 2023 Jul 20. Erratum in: Circulation. 2023 Sep 26;148(13):e148. Erratum in: Circulation. 2023 Dec 5;148(23):e186. PMID: 37471501.
- Boden WE, O’Rourke RA, Teo KK, et al. COURAGE Trial Research Group. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007 Apr 12;356(15):1503-16. [CrossRef] [PubMed]
- Al-Lamee R, Thompson D, Dehbi HM, et al. ORBITA investigators. Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomized controlled trial. Lancet. 2018 Jan 6;391(10115):31-40. doi: 10.1016/S0140-6736(17)32714-9. Epub 2017 Nov 2. Erratum in: Lancet. 2018 Jan 6;391(10115):30. PMID: 29103656.
- Maron DJ, Hochman JS, Reynolds HR, et al. ISCHEMIA Research Group. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N Engl J Med. 2020 Apr 9;382(15):1395-1407. [CrossRef] [PubMed]
- Kurup R, Wijeysundera HC, Bagur R, et al. Complete Versus Incomplete Percutaneous Coronary Intervention-Mediated Revascularization in Patients With Chronic Coronary Syndromes. Cardiovasc Revasc Med. 2023 Feb;47:86-92. [CrossRef] [PubMed]
- Stone GW, Ali ZA, O’Brien SM, Rhodes G, et al. ISCHEMIA Research Group. Impact of Complete Revascularization in the ISCHEMIA Trial. J Am Coll Cardiol. 2023 Sep 19;82(12):1175-1188. [CrossRef] [PubMed]
- Gaba P, Gersh BJ, Ali ZA, Moses JW, Stone GW. Complete versus incomplete coronary revascularization: definitions, assessment and outcomes. Nat Rev Cardiol. 2021 Mar;18(3):155-168. [CrossRef] [PubMed]
- Doenst T, Haverich A, Serruys P, Bonow RO, Kappetein P, Falk V, Velazquez E, Diegeler A, Sigusch H. PCI and CABG for Treating Stable Coronary Artery Disease: JACC Review Topic of the Week. J Am Coll Cardiol. 2019 Mar 5;73(8):964-976. [CrossRef] [PubMed]
- van Veelen A, van der Sangen NMR, Delewi R, et al. Detection of Vulnerable Coronary Plaques Using Invasive and Non-Invasive Imaging Modalities. J Clin Med. 2022 Mar 1;11(5):1361. [CrossRef] [PubMed]
- Tomaniak M, Katagiri Y, Modolo R, et al. Vulnerable plaques and patients: state-of-the-art. Eur Heart J. 2020 Aug 14;41(31):2997-3004. [CrossRef] [PubMed]
- Virani SS, Newby LK, Arnold SV, et al. Peer Review Committee Members. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023 Aug 29;148(9):e9-e119. doi: 10.1161/CIR.0000000000001168. Epub 2023 Jul 20. Erratum in: Circulation. 2023 Sep 26;148(13):e148. Erratum in: Circulation. 2023 Dec 5;148(23):e186. PMID: 37471501.
- Stone GW, Maehara A, Lansky AJ, et al. PROSPECT Investigators. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011 Jan 20;364(3):226-35. doi: 10.1056/NEJMoa1002358. Erratum in: N Engl J Med. 2011 Nov 24;365(21):2040. PMID: 21247313.
- Stone GW, Maehara A, Ali ZA, et al. PROSPECT ABSORB Investigators. Percutaneous Coronary Intervention for Vulnerable Coronary Atherosclerotic Plaque. J Am Coll Cardiol. 2020 Nov 17;76(20):2289-2301. [CrossRef] [PubMed]
- Park SJ, Ahn JM, Kang DY, et al. Preventive percutaneous coronary intervention versus optimal medical therapy alone for the treatment of vulnerable atherosclerotic coronary plaques (PREVENT): a multicentre, open-label, randomized controlled trial. www.thelancet.com. 2024. [CrossRef]
- van Veelen A, Küçük IT, Fuentes FH, et al. First-in-Human Drug-Eluting Balloon Treatment of Vulnerable Lipid-Rich Plaques: Rationale and Design of the DEBuT-LRP Study. J Clin Med. 2023 Sep 6;12(18):5807. doi: 10.3390/jcm12185807. Erratum in: J Clin Med. 2024 Mar 04;13(5): PMID: 37762747; PMCID: PMC10531515.
- Mulijono, D. Mechanism of How Plant-Based Diet (PBD) Reduces the Risk of In-Stent Restenosis (ISR) and Stent Thrombosis (ST). Preprints 2024, 2024040628. [Google Scholar] [CrossRef]
- Mortensen MB, Dzaye O, Steffensen FH, et al. Impact of Plaque Burden Versus Stenosis on Ischemic Events in Patients With Coronary Atherosclerosis. J Am Coll Cardiol. 2020 Dec 15;76(24):2803-2813. [CrossRef] [PubMed]
- Peña-Jorquera H, Cid-Jofré V, Landaeta-Díaz L, et al. Plant-Based Nutrition: Exploring Health Benefits for Atherosclerosis, Chronic Diseases, and Metabolic Syndrome—A Comprehensive Review. Nutrients 2023, 15, 3244. [Google Scholar] [CrossRef] [PubMed]
- Salehin S, Rasmussen P, Mai S, et al. Plant Based Diet and Its Effect on Cardiovascular Disease. Int J Environ Res Public Health. 2023 Feb 14;20(4):3337. [CrossRef] [PubMed]
- Koutentakis M, Surma S, Rogula S, et al. The Effect of a Vegan Diet on the Cardiovascular System. J Cardiovasc Dev Dis. 2023 Feb 22;10(3):94. [CrossRef] [PubMed]
- Tucci M, Marino M, Martini D, et al. Plant-Based Foods and Vascular Function: A Systematic Review of Dietary Intervention Trials in Older Subjects and Hypothesized Mechanisms of Action. Nutrients. 2022 Jun 24;14(13):2615. [CrossRef] [PubMed]
- Islam SU, Ahmed MB, Ahsan H, et al. Recent Molecular Mechanisms and Beneficial Effects of Phytochemicals and Plant-Based Whole Foods in Reducing LDL-C and Preventing Cardiovascular Disease. Antioxidants (Basel). 2021 May 15;10(5):784. doi: 10.3390/antiox10050784. PMID: 34063371; PMCID: PMC8157003.
- Mehta P, Tawfeeq S, Padte S, et al. Plant-based diet and its effect on coronary artery disease: A narrative review. World J Clin Cases. 2023 Jul 16;11(20):4752-4762. [CrossRef] [PubMed]
- Bruns A, Greupner T, Nebl J, et al. Plant-based diets and cardiovascular risk factors: a comparison of flexitarians, vegans and omnivores in a cross-sectional study. BMC Nutr 10, 29 (2024). [CrossRef]
- Di Sotto A, Vitalone A, Di Giacomo S. Plant-Derived Nutraceuticals and Immune System Modulation: An Evidence-Based Overview. Vaccines (Basel). 2020 Aug 22;8(3):468. [CrossRef] [PubMed]
- Xu K, Kh Al-ani M, Pan X, et al. Plant-Derived Products for Treatment of Vascular Intima Hyperplasia Selectively Inhibit Vascular Smooth Muscle Cell Functions, Evidence-Based Complementary and Alternative Medicine, vol. 2018, Article ID 3549312, 17 pages, 2018. [CrossRef]
- Monsalve B, Concha-Meyer A, Palomo I, et al. Mechanisms of Endothelial Protection by Natural Bioactive Compounds from Fruit and Vegetables. An Acad Bras Cienc. 2017 May;89(1 Suppl 0):615-633. [CrossRef] [PubMed]
- Aquila G, Marracino L, Martino V, et al. The Use of Nutraceuticals to Counteract Atherosclerosis: The Role of the Notch Pathway. Oxid Med Cell Longev. 2019 May 2;2019:5470470. [CrossRef] [PubMed]
- Moss J, Dipak R. (2016). Nutraceutical therapies for atherosclerosis. Nature Reviews Cardiology. 2016; 13(9):513-532. [CrossRef]
- Wei T, Liu J, Zhang D, et al. The Relationship Between Nutrition and Atherosclerosis. Front Bioeng Biotechnol. 2021 Apr 19;9:635504. [CrossRef] [PubMed]
- Mitu O, Cirneala IA, Lupsan AI, et al. The Effect of Vitamin Supplementation on Subclinical Atherosclerosis in Patients without Manifest Cardiovascular Diseases: Never-ending Hope or Underestimated Effect? Molecules 2020, 25, 1717. [Google Scholar] [CrossRef] [PubMed]
- Garcia S, Sandoval Y, Roukoz H, et al. Outcomes after complete versus incomplete revascularization of patients with multivessel coronary artery disease: a meta-analysis of 89,883 patients enrolled in randomized clinical trials and observational studies. J Am Coll Cardiol. 2013 Oct 15;62(16):1421-31. [CrossRef] [PubMed]
- Sandoval Y, Brilakis ES, Garcia S. Completeness of revascularization in multivessel coronary artery disease. J Thorac Dis. 2016 Nov;8(11):E1493-E1496. [CrossRef] [PubMed]
- Hwang D, Kang J, Yang HM, et al. Better Prognosis After Complete Revascularization Using Contemporary Coronary Stents in Patients With Chronic Kidney Disease. Circ Cardiovasc Interv. 2019 Aug;12(8):e007907. [CrossRef] [PubMed]
- Iqbal MB, Moore PT, Nadra IJ, et al. British Columbia Cardiac Registry Investigators. Complete revascularization in stable multivessel coronary artery disease: A real world analysis from the British Columbia Cardiac Registry. Catheter Cardiovasc Interv. 2022 Feb;99(3):627-638. [CrossRef] [PubMed]
- Williams T, Mittal A, Karageorgiev D, et al. e-Ultimaster investigators. Complete revascularization optimizes patient outcomes in multivessel coronary artery disease: Data from the e-Ultimaster registry. Catheter Cardiovasc Interv. 2022 Mar;99(4):961-967. [CrossRef] [PubMed]
- Pham V, Moroni A, Gall E, et al. Revascularization and Medical Therapy for Chronic Coronary Syndromes: Lessons Learnt from Recent Trials, a Literature Review. J Clin Med. 2023 Apr 12;12(8):2833. [CrossRef] [PubMed]
- Giubilato S, Lucà F, Abrignani MG, et al. Management of Residual Risk in Chronic Coronary Syndromes. Clinical Pathways for a Quality-Based Secondary Prevention. J Clin Med. 2023 Sep 15;12(18):5989. [CrossRef] [PubMed]
- Rose, Stewart D. “A Comprehensive Review of the Prevention and Treatment of Heart Disease with a Plant-Based Diet.” Journal of Cardiology & Cardiovascular Therapy (2018): n. pag.
- Bilal M, Ashraf S, Zhao X. Dietary Component-Induced Inflammation and Its Amelioration by Prebiotics, Probiotics, and Synbiotics. Front Nutr. 2022 Jul 22;9:931458. [CrossRef] [PubMed]
- Upadhyay S, Dixit M. Role of Polyphenols and Other Phytochemicals on Molecular Signaling. Oxid Med Cell Longev. 2015;2015:504253. [CrossRef] [PubMed]
- Wu YT, Chen L, Tan ZB, et al. Luteolin Inhibits Vascular Smooth Muscle Cell Proliferation and Migration by Inhibiting TGFBR1 Signaling. Front Pharmacol. 2018 Sep 21;9:1059. [CrossRef] [PubMed]
- Hong CG, Florida E, Li H, Parel PM, Mehta NN, Sorokin AV. Oxidized low-density lipoprotein associates with cardiovascular disease by a vicious cycle of atherosclerosis and inflammation: A systematic review and meta-analysis. Front Cardiovasc Med. 2023 Jan 16;9:1023651. [CrossRef] [PubMed]
- Marchio P, Guerra-Ojeda S, Vila JM, et al. Targeting Early Atherosclerosis: A Focus on Oxidative Stress and Inflammation. Oxid Med Cell Longev. 2019 Jul 1;2019:8563845. [CrossRef] [PubMed]
- Adarsh Ray, Krushna Ch. Maharana, et al. Endothelial dysfunction and its relation in different disorders: Recent update, Health Sciences Review, Volume 7, 2023, 100084, ISSN 2772-6320. [CrossRef]
- Almeida C, Barata P, Fernandes R. The influence of gut microbiota in cardiovascular diseases-a brief review. Porto Biomed J. 2021 Jan 18;6(1):e106. [CrossRef] [PubMed]
- Pollicino F, Veronese N, Dominguez LJ, et al. Mediterranean diet and mitochondria: New findings. Exp Gerontol. 2023 Jun 1;176:112165. [CrossRef] [PubMed]
- Cinegaglia N, Antoniazzi L, Rosa D, et al. Shortening telomere is associated with subclinical atherosclerosis biomarker in omnivorous but not in vegetarian healthy men. Aging (Albany NY). 2019 Jul 19;11(14):5070-5080. [CrossRef] [PubMed]
- Plotnikoff GA, Dobberstein L, Raatz S. Nutritional Assessment of the Symptomatic Patient on a Plant-Based Diet: Seven Key Questions. Nutrients. 2023 Mar 13;15(6):1387. [CrossRef] [PubMed]
- Neufingerl N, Eilander A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients. 2021 Dec 23;14(1):29. [CrossRef] [PubMed]
Figure 1.
Mechanisms of how PBD stabilizes/ regress the vulnerable plaque.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



