
Submitted:
25 April 2024
Posted:
25 April 2024
You are already at the latest version
Abstract
World Health Organization recommends adjusting the salt intake as a part of the nine global targets to reduce premature mortality from non-communicable chronic diseases as priority and most cost-effective intervention. In 2006. the main aim of the Croatian Action on Salt and Health was to decrease salt intake for 16% because of its critical intake and consequences on human health. We have organized educative activities for increasing awareness on salt harmfulness, defined food categories of prime interest, collaborate with industries and determine salt intake (24h urine-sodium excretion). It was determined that the proportion of salt in ready-to-eat baked bread should not exceed 1.4%. In the period 2014 –2022, salt in the semi-white bread was reduced 14%, in bakery 22% and in largest meat industry in Croatia 25%. Awareness of the harmfulness of salt on health increased from 65.3% in 2008 to 96.9% in 2023 and salt intake was reduced 15.9%-1.8 grams/day (22.8% men, 11.7% women). In last 18 years a significant decrease in salt intake was achieved in Croatia, awareness of its harmfulness increased, collaboration with food industry established and regulatory documents launched. However, salt intake is still very high underlying the need for continuation of efforts and even stronger activities.
Keywords:
salt
; sodium
; potassium
; iodine
; epidemiology
; public health
; blood pressure
; hypertension
; cardiovascular mortality
; non-communicable diseases
1. Introduction
The average sodium intake worldwide is estimated at 4,310 mg/day (10.78 g salt per day), which is significantly higher than physiological needs (500 mg/day) and more than double the World Health Organization (WHO) recommends (2,000 mg/day) [1]. Non-communicable diseases (NCDs) are the leading cause of death worldwide, responsible for 41.5 million deaths in 2016 (71% of the 57 million deaths), more than all the other causes combined [2]. Cardiovascular diseases (CVDs) account for most deaths and raised blood pressure (BP) is the leading risk factor for CVDs. The recent Global Burden of Disease Study (GBDS) showed that high BP accounted for 10.4 million deaths and 218 million disability-adjusted life years (DALYs) in 2017 [3]. According to the meta-analysis, the number of people with arterial hypertension (AH) doubled between 1990 and 2019 and currently is approximately 1.3 billion [4]. Even a small increase in BP is associated with an increase in CV risk, including stroke, myocardial infarction, coronary heart disease and heart failure [5]. The WHO 2023 Global report on AH stated that elevated BP is one of the most important risk factors for disability and death worldwide [6]. High salt intake which is a well-established cause of high BP was responsible for 3.2 million deaths and 70 million DALYs [7,8,9,10,11,12,13]. According to the GBDS from 2019, the number of deaths from CVDs associated with high salt intake is 41.08% higher than it was in 1990 [14]. A reduction of 100 mmol/day in 24-hour urinary sodium excretion is associated with systolic BP reduction of 5.56 mmHg [15]. While the primary health effect associated with a diet high in sodium is raised BP, there is a growing body of evidence documenting the impact of high sodium intake on various health outcomes, including gastric cancer [16,17], obesity [18,19,20,21,22] osteoporosis [23] etc. Based on the analysis of the GBDS data, it was concluded that the total number of deaths from chronic kidney disease (CKD) associated with increased salt intake was 45,530, while the number of DALYs was 1.32 million [24]. In a prospective study, we found that in our population with low potassium intake, increased salt intake is a significant risk factor for new-onset CKD [25]. A 2021 Cochrane review concluded that reducing high salt intake in patients in the early stages of CKD and with albuminuria is associated with a reduction in BP, which may lead to a slowing of CKD progression and a reduction in CV risk [26]. Recently published research has confirmed that high salt intake increases the risk of type 2 diabetes [27], and a Cochrane review published in 2023 concluded that reducing salt intake in patients with diabetes can significantly lower BP, preventing the onset and slowing the progression of diabetic kidney disease and that salt intake in patients with diabetes, whether or not they have AH and whether or not they already have signs of CKD, must be less than 5 g per day (less than 2 g of sodium) [28]. In 2013, the WHO recommended to all Member States to reduce population salt intake by 30%, as a part of the 9 global targets to reduce premature mortality from NCDs by 25% by 2025 [29]. Reducing salt intake in populations is among the most cost-effective interventions to reduce the burden of NCDs and is therefore considered a priority action for all countries (an average cost-effectiveness ratio of ≤ I$100/DALY averted in low- and lower middle-income countries) [30,31,32,33]. The Sodium Country Score Card was established as part of a WHO's efforts primarily to reduce dietary sodium intake, but this system will continuously monitor countries' performance and continue to be enhanced with additional features [34,35]. In 2016, the WHO published the SHAKE Technical Package for Salt Reduction, to further stimulate Member States in carrying out salt reduction strategies through 5 key action areas: surveillance, harnessing industry, adopting standards for labeling, knowledge, and environment [36]. In 2017, WHO recommended several sodium-related best buys policies and other measures as practical actions that should be undertaken immediately, to prevent CVD [37]. In 2023, WHO launched the first Global Report on Sodium Intake Reduction investigating the progress of countries which are implementing sodium reduction policies and their impact on population and CVD [38]. Finally, salt reduction recommendation is an essential part of all relevant guidelines [39,40,41,42,43].
Since it is obvious that the primary goal of decreasing salt consumption for 30% by 2025 will not be achieved WHO called for accelerated actions in scaling up efforts to reduce populations’ sodium intake.
2. Prevalence of Hypertension and Cardiovascular Mortality in Croatia
According to recent data, in 2022 CVDs were the leading cause of death in Croatia (39.1%), of which more women died from CVDs than men (43.8% vs. 39.1%) [44]. The age-standardized death rate in Croatia is significantly higher than the EU average (591/100,000 vs. 344/100,000). It is particularly worrying that the age-standardized death rate in people under 65 (57/100,000 vs. 41/100,000) is higher in Croatia compared to the EU average. Ischemic heart disease is the leading cause of death (12.2% or 6925 deaths), and hypertensive disease is in the second place (9.2% or 5231 deaths), which indicates that AH is the main cause of death in Croatia. Elevated BP ranks second after smoking as an important risk factor for DALYs in Croatia [45]. Today's data are better than in 2009, the year when 49,2% of people died from CVDs, but since 2019, a decrease in the reduction of CVD mortality has been observed, which is mostly the consequence of the high prevalence of AH (50.9%). However, there are still many untreated patients with AH (23%), and control is achieved in only 50.1% of treated subjects with AH [46]. All these data undoubtedly confirm that AH is the main public health problem in Croatia. This is significantly contributed by the large intake of salt in Croatia, which was recognized as early in 2006 [47].
3. Brief History of Eighteen Years Old Salt War in Croatia
3.1. First Period 2005 – 2014
One year after the announcement of the World Action on Salt and Health (WASH) program, a Declaration on the importance of starting a national campaign to reduce salt intake in Croatia was accepted at the Congress of the Croatian Society for Hypertension in 2006, and in 2007 the Croatian initiative (Croatian Action on Salt and Health - CRASH) and the national program were presented at the Congress of the Croatian Atherosclerosis Society [47,48,49,50,51,52]. The motto of the CRASH program is "Less salt, more health". The chronology of activities is shown in Figure 1.
In the initial period from 2005 to 2014, the following was done: 1) The average intake of salt in gram/day was determined based on the determination of sodium in 24-hour urine in mmol/day, which is today the "gold standard" for salt intake estimation. The average intake of salt was 11.6 grams per day (men 13.3 grams, women 10.2 grams) (Table 1) [53]; 2) The relationship between the amount of consumed salt and BP values in the Croatian population was established (Figure S1) [54,55]; 3) It was found that there was insufficient awareness of the general population about the harmfulness of excessive intake of salt (Table 2) [56]; 4) The proportion of salt in bakery products has been determined, ranging from 1.56% in some types of bread to an average of 2.0% (Table S1) [57,58,59]; 5) The proportion of daily salt intake from bread, bakery, meat and dairy products, and snacks was determined in a national, representative sample (Table S2 and Table S3) [60]. The average total intake of salt from bread and bakery products was 2,46 grams per day, which is half of the recommended value of WHO. Moreover, only because consuming bread and bakery products, 7.8% of respondents consumed larger amounts of salt than the recommended daily intake [61,62]; 6) Education was organized by symposia for health workers, as well as public health actions and the preparation of popular educational brochures, leaflets and posters for patients and the general population; 7) Negotiations with the food industry, restaurants and catering facilities have begun; 8) A document - Scientific opinion on the harmfulness of excessive intake of salt was prepared [47]. These first steps have already led to initial results. Public awareness of the harmful effects of excessive salt intake and the importance of reducing it increased, and parts of the industry have started to voluntarily reduce the NaCl content in their products (e.g. Lipički Studenac mineral water, Čakovečki Mlinovi bakery industry).
3.2. Action Plan for Salt Reduction in Croatia, Ministry of Health 2014 – 2019
These initial steps were the basis for the Action plan for salt reduction in Croatia 2014 – 2019, and it was prepared according to the WHO recommendations for reducing the intake of salt in the population: 1) To decrease salt intake for 16% over 4 years (4% per year in period of 2014 – 2019); 2) To increase awareness on salt harmfulness; 3) To define food categories of prime interest; 4) To determine salt intake by measuring 24h urine sodium excretion; 5) To develop new recipes in collaboration with food industry; 6) To monitor salt intake, collaboration with food industry and analyze trends in awareness. In this period, the following was achieved: 1) In 2015, the Ministry of Agriculture adopted the Ordinance on Cereals and Cereal Products (OG 81/2016), which determined that the proportion of salt in ready-to-eat baked bread should not exceed 1.4% and in 2022, as second step, which determined that the salt content of ready-to-eat baked bread, as well as the baked pastry, may not exceed 1.3 % [63]. With this Ordinance, Croatia joined a small number of European countries with such an advanced regulation (Table S4); 2) After years of negotiations, the largest meat industry in Croatia, PIK Vrbovec, made a reformulation of meat products and in 2016 reduced the proportion of salt in all its products by an average of 25%. We have continued with educative public health actions that increased awareness about salt (Table 2) [64]; 3) The control of the implementation of the project was done by analyzing the share of salt in bakery products. In the analyzed bread samples, the amount of salt was on average 1.34% (0.9% to 1.8%) and in the bakery products 1.21% (0.7% to 1.7%). In semi-white bread the amount of salt was reduced by about 14%, while in bakery products this reduction was about 22% (Figure 2) [61].
These results are consistent with another analysis, according to which the intake of salt by eating bread decreased by about 14% in the population, while this reduction in bakery products amounts to 28% [61]. According to the Croatian Institute of Public Heath (CIPH) study during 2019, the majority of the bakery industry was found to be compliant with the regulation (72% of breads and 66% of bakery products had a salt content < 1.4%), which is consistent with data from the State Inspectorate and the Ministry of Agriculture, which found that the salt content in 89% of analyzed bread samples was compliant [61]. In contrast, study of the Faculty of Food Technology has shown that a significant number of small bakeries still do not comply with the regulations. Bread from large shopping centers, which is usually imported as a frozen form from other countries, which is not subject to the regulation, also contained a high content of salt [66]. 4) The success of the project implementation was analyzed by determining the urine salt excretion in 2008 and 2015. Unfortunately, the data obtained showed that the intake of salt had not decreased [67]. It should be noted that the study was conducted in a part of the rural population and that salt intake was estimated using spot morning urine samples, which is not the gold standard. Nevertheless, using the same method in the same population sample, we could conclude that, at least in this part of the population, there was no decrease in salt intake during this phase of the CRASH program, suggesting the need for a more intensive continuation of the program [52].
3.3. Third Period 2020 – 2024
Although officially the Action Plan of the Ministry of Health has not been continued, the Croatian Society for Hypertension, the Croatian Hypertension League, the Croatian Institute of Public Health (CIPH), the Croatian Agency for Agriculture and Food (CAAF), together with the Ministry of Agriculture, have continued with all previously planned activities. 1). In 2020, the Ministry of Agriculture adopted the Ordinance on Cereals and Cereal Products (OG 101/2022), which stated that the quantity of the salt in baked bread and bakery products ready for consumption should not exceed 1.3%; 2) The CAAF published two scientific reports: Scientific report on the intake of salt by the consumption of bread and bakery products, and Scientific report on the intake of salt by the consumption of meat products [61,68]; 3) The CIPH analyzed school meals.
The results showed that elementary school students still consume, only by eating at school, an excessive amount of salt (range 5.2 to 10.2 grams per day); 4) Croatian Hypertension League and CIPH continued with numerous activities that increased the awareness of the general population. In this period the Croatian Hypertension League further expanded these actions by launching the digital educational platform Hunting for the Silent Killer, where citizens are provided with various useful, important and practical information, which resulted in a significant increase in health literacy for this important segment of human health. Awareness of the harmful effects of excessive salt intake on human health increased from 65.3% in 2008 to 96.9%, and the number of people who believe that they could reduce their intake of salt increased from 69.4% to 87.9% (Table 2); 5) The intake of salt in the general population was determined by the "gold standard" method as a part of the Croatian Science Foundation project (Epidemiology of arterial hypertension and salt intake in Croatia - EH-UH 2) and public health actions organized by the Croatian Hypertension League and CIPH. According to the preliminary results, the intake of salt in the general population was reduced by an average of 15.9% for the total population, 22.8% for men and 11.7% for women (Table 1) [46]; 6) The CIPH conducted a project to analyze iodine in household salt, according to which 10% of salt samples did not contain the appropriate, prescribed amount of iodine (18 – 33 mg/kg as KI), in accordance with regulations [69]. The biochemical marker for assessing iodine is urinary iodine concentration (µg/L). According to the preliminary results of the EH-UH 2 project, where iodine intake was assessed by determining it in 24-hour urine, the largest number of the adult population (54.5%) had adequate iodine intake (100 – 200 µg/L), insufficient intake (<100 µg/L) was found in 26.6% of the population, and 17.3% had an intake above the recommended level (>200 µg/L), which reflects the data of the CIPH on insufficiently adequate iodization or storage of salt, and possibly it also reflects the use of non-iodized salt, which is still preferred by a part of population [46].
4. Future Plans and Strategies – Decrease Salt and Increase Potassium Intake
During 2024, the Ministry of Health, together with partners who have been active all along, prepared a proposal for a Croatian National Prevention Program for reduction of excessive intake of salt with adequate iodine intake, stressing the importance of increasing potassium intake. A meta-analysis by Ma et al. showed that an increase in potassium excretion in 24-hour urine for every 1000 mg was associated with an 18% lower CV risk [70]. Based on this and numerous other results, the WHO recommends that the minimum intake of potassium estimated by 24-hour excretion should not be less than 90 mmol per day, which is equivalent to an approximate intake of potassium of 3.50 grams per day. WHO recommends increasing dietary potassium intake to reduce the risk of AH, CVDs and stroke [71–73]. According to the preliminary results of the EH-UH 2 project, the average intake of potassium in the general adult Croatian population is 2.98 grams per day (men 3.17 grams per day; women 2.86 grams per day), which is below the WHO recommendation. The recommended intake of potassium estimated by a 24-hour urine potassium excretion (≥ 90 mmol per day) was observed in 8.9% of subjects (10.9% of men and 7.8% of women). The average Na-to-K ratio was 3.1 (men 3.4 and women 3.0), which best reflects an unfavorable dietary pattern regarding the intake of salt and potassium. The percentage of people with a Na-to-K ratio ≤ 1, which is the WHO recommendation, was determined in a very small proportion of general population 3.2% (3.3% in men and 3.1% in women) [46]. A study on the quality of the diet of pregnant women found that Na-to-K ratio of 2.68 (1.11 – 5.24) does not meet nutrition quality due to high sodium and insufficient potassium intake [74]. In our prospective study conducted in the general rural population, we found that the intake of salt above 10 grams per day was present in 56.5% of respondents, and an intake of potassium > 3.5 grams per day in 3.2% with an extremely poor Na-to-K ratio of average 4.3 [75]. During an average of 7.5 years of follow-up, we observed that the Na-to-K ratio is a more important risk factor for new-onset AH than the intake of salt [76]. Based on all the evidence, the Guidelines of the European Society for Hypertension recommend non-pharmacological treatment of subjects with AH: 1) In subjects with AH who consume a high salt diet, it is recommended to use substitute salts in which NaCl is replaced by KCl (evidence level I A); Increased intake of potassium, primarily through dietary changes, is recommended for all adults with elevated BP, except for patients in advanced stages of CKD [77].
These were the reasons for adding importance of increase of potassium intake in addition to reducing the excessive intake of salt to the Croatian National Program. The new Croatian National Program continues to follow the SHAKE recommendations of the WHO [36] with the basic tasks: 1) the reformulation of food products to contain less salt and the setting of target levels for the amount of salt in foods and meals; 2) the establishment of a supportive environment in public institutions (hospitals, schools, kindergartens, workplaces, nursing homes) to enable lower sodium options to be provided; 3) a behavior change communication and mass media campaign; 4) the implementation of front-of-pack labelling. The Croatian National Program will have two arms - one aimed at increasing health literacy, which will be organized using classic public health methods, but also using digital technology (educational web platforms, social networks), and the other arm, which will be aimed at the food industry, restaurants, and catering.
5. Conclusion
In the last 18 years a significant decrease in salt intake was achieved in Croatia (15.9 % - 1.8 gram per day). Awareness of harmful effects of excessive salt intake on health substantially increased. Good collaboration with the food industry (bakery, meet) was established, and regulatory documents were prepared and launched. However, salt intake is still very high in Croatia stressing the need for continuation of efforts, even more intensive activities aimed not only for salt reduction, and appropriate iodine intake, but also to increase the potassium consumption which are important elements of the new Croatian National Program.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Huang, L.; Trieu, K.; Yoshimura, S.; Neal, B.; Woodward, M.; Campbell, N. R. C.; Li, Q.; Lackland, D. T.; Leung, A. a. C.; Anderson, C. A. M. et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: systematic review and meta-analysis of randomised trials. BMJ 2020, m315. [CrossRef]
- Bennett, J. L.; Stevens, G. A.; Mathers, C.; Bonita, R.; Rehm, J.; Kruk, M. E.; Riley, L.; Dain, K.; Kengne, A. P.; Chalkidou, K. et al. NCD Countdown 2030: worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. Lancet 2018, 392 (10152), 1072–1088. [CrossRef]
- Global Burden of Disease 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioral, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392 (10159), 1923–1994. [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398 (10304), 957–980. [CrossRef]
- Cook, N. R.; He, F. J.; MacGregor, G. A.; Graudal, N. Sodium and health—concordance and controversy. BMJ. (Clinical Research Ed.) 2020, m2440. [CrossRef]
- World Health Organization. Management-Screening, Diagnosis and Treatment (MND). Global report on hypertension: the race against a silent killer. Available online: https://www.who.int/publications/i/item/9789240081062 (accessed on 2 February 2024).
- Elliott, P.; Stamler, J.; Nichols, R.; Dyer, A. R.; Stamler, R.; Kesteloot, H.; Marmot, M. Intersalt revisited: further analyses of 24-hour sodium excretion and blood pressure within and across populations. BMJ. 1996, 312 (7041), 1249–1253. [CrossRef]
- Aburto, N.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F. P.; Meerpohl, J. J. Effect of lower sodium intake on health: systematic review and meta-analyses. BMJ. 2013, 346 (apr03 3), f1326. [CrossRef]
- He, F. J.; Li, J.; MacGregor, G. A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ. 2013, 346 (apr03 3), f1325. [CrossRef]
- Act, A.; Mozaffarian, D.; Fahimi, S.; Singh, G.; Khatibzadeh, S.; Engell, R. E.; Lim, S. S.; Danaei, G.; Ezzati, M.; Powles, J. Global Sodium Consumption and Death from Cardiovascular Causes. N Engl J Med. 2014, 371 (7), 624–634. [CrossRef]
- Huang, L.; Trieu, K.; Yoshimura, S.; Neal, B.; Woodward, M.; Campbell, N. R. C.; Li, Q.; Lackland, D. T.; Leung, A. a. C.; Anderson, C. A. M.; MacGregor, G. A. et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: systematic review and meta-analysis of randomised trials. BMJ. 2020, m315. [CrossRef]
- World Health Organization. WHO global report on sodium intake reduction. Available online: https://iris.who.int/bitstream/handle/10665/366393/9789240069985-eng.pdf (accessed on 13 March 2024).
- Filippini, T.; Malavolti, M.; Whelton, P.K.; Naska, A.; Orsini, N.; Vinceti, M. Blood pressure effects of sodium reduction. Circulation. 2021, 143 (16), 1542–1567. [CrossRef]
- Wang, K.; Jin, Y.; Wang, M.; Liu, J.; Bu, X.; Mu, J.; Lu, J. Global cardiovascular diseases burden attributable to high sodium intake from 1990 to 2019. J. Clin. Hypertens. 2023, 25 (9), 868–879. [CrossRef]
- Filippini, T.; Malavolti, M.; Whelton, P. K.; Naska, A.; Orsini, N.; Vinceti, M. Blood pressure effects of sodium reduction. Circulation. 2021, 143 (16), 1542–1567. [CrossRef]
- D’Elia, L.; Galletti, F.; Strazzullo, P. Dietary Salt Intake and Risk of Gastric Cancer. In: Zappia, V., Panico, S., Russo, G., Budillon, A., Della Ragione, F. (eds) Advances in Nutrition and Cancer, Cancer Treatment and Research. 2014, vol 159. Springer, Berlin, Heidelberg. [CrossRef]
- D’Elia, L.; Rossi, G.; Ippolito, R.; Cappuccio, F. P.; Strazzullo, P. Habitual salt intake and risk of gastric cancer: A meta-analysis of prospective studies. Clin Nutr. 2012, 31 (4), 489–498. [CrossRef]
- Bolhuis, D. P.; Costanzo, A.; Newman, L. P.; Keast, R. Salt promotes passive overconsumption of dietary fat in humans. J Nutr. 2016, 146 (4), 838–845. [CrossRef]
- Moosavian, S. P.; Haghighatdoost, F.; Surkan, P. J.; Azadbakht, L. Salt and obesity: a systematic review and meta-analysis of observational studies. Int J Food Sci Nutr. 2016, 68 (3), 265–277. [CrossRef]
- Teucher, B.; Dainty, J.; Spinks, C. A.; Majsak-Newman, G.; Berry, D. J.; Hoogewerff, J.; Foxall, R. J.; Jakobsen, J.; Cashman, K. D.; Flynn, A.; Fairweather-Tait, S. Sodium and bone health: Impact of moderately high and low salt intakes on calcium metabolism in postmenopausal women. J Bone Miner Res. 2008, 23 (9), 1477–1485. [CrossRef]
- Pećin, I.; Premužić, V.; Čvorišćec, D.; Erceg, I.; Fuček, M.; Jelaković M, Jovanović A, Kaić-Rak A, Laganović M, Lederer P, Perković M, Reiner Ž, Sertić J, Špišić T, Jelaković B: Salt Intake and the metabolic syndrome. Croatian Action on Salt and Health (CRASH). Kidney and Blood Pressure Research, 2009; 32:324.
- Kos, M.; Nađ, T.; Stanojević, L.; Lukić, M.; Stupin, A.; Drenjančević-Perić, I.; Pušeljić, S.; Cvetko, E. D.; Mihaljević, Z.; Dumančić, D.; Jukić, I. Estimation of salt intake in normotensive and hypertensive children: The role of body weight. Nutrients 2023, 15 (3), 736. [CrossRef]
- Cappuccio, F.P.; Kalaitzidis, R.; Duneclift, S.; Eastwood, J.B. Unravelling the links between calcium excretion, salt intake, hypertension, kidney stones and bone metabolism. J Nephrol. 2000;13(3):169–77. https://pubmed.ncbi.nlm.nih.gov/10928292/.
- Liu, W.; Zhou, L.; Yin, W.; Wang, J.; Zuo, X. Global, regional, and national burden of chronic kidney disease attributable to high sodium intake from 1990 to 2019. Front. Nutr. 2023, 10. [CrossRef]
- Premužić, V.; Miličić, B.; Krtalić, B.; Gellineo, L.; Knežević, T.; Jelaković, A.; Dapić, K.; Matašin, M.; Ivković, V.; Fuček, M.; Josipović, J.; Dika, Ž.; Kos, J.; Karanović, S.; Jelaković, B. New onset chronic kidney disease is associated with high sodium intake in population with low potassium consumption. J. Hypertens. 2019, 37, e249. [CrossRef]
- McMahon, E.; Campbell, K. L.; Bauer, J.; Mudge, D. W.; Kelly, J. Altered dietary salt intake for people with chronic kidney disease. Cochrane Library 2021, 2021 (6). [CrossRef]
- Wang, X.; Ma, H.; Kou, M.; Tang, R.; Xue, Q.; Li, X.; Harlan, T. S.; Heianza, Y.; Qi, L. Dietary sodium intake and risk of incident type 2 diabetes. Mayo Clinic Proceedings 2023, 98 (11), 1641–1652. [CrossRef]
- Hodson, E. M.; Cooper, T. E. Altered dietary salt intake for preventing diabetic kidney disease and its progression. Cochrane Library 2023, 2023 (1). [CrossRef]
- World Health Organization. Noncommunicable Diseases, Rehabilitation and Disability (NCD). Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Available online: https://www.who.int/publications/i/item/9789241506236 (accessed on 15 February 2024).
- Cobiac, L.; Vos, T.; Veerman, L. Cost-effectiveness of interventions to reduce dietary salt intake. Heart 2010, 96 (23), 1920–1925. [CrossRef]
- Webb, M.; Fahimi, S.; Singh, G.; Khatibzadeh, S.; Micha, R.; Powles, J.; Mozaffarian, D. Cost effectiveness of a government supported policy strategy to decrease sodium intake: global analysis across 183 nations. BMJ. 2017, i6699. [CrossRef]
- Trieu, K.; Neal, B.; Hawkes, C.; Dunford, E.; Campbell, N. R. C.; Rodríguez-Fernández, R.; Legetić, B.; McLaren, L.; Barberio, A. M.; Webster, J. Salt Reduction Initiatives around the World – A Systematic Review of Progress towards the Global Target. PloS One 2015, 10 (7), e0130247. [CrossRef]
- Webster, J.; Dunford, E.; Hawkes, C.; Neal, B. Salt reduction initiatives around the world. J. Hypertens. 2011, 29 (6), 1043–1050. [CrossRef]
- McLaren, L.; Sumar, N.; Barberio, A. M.; Trieu, K.; Lorenzetti, D.; Tarasuk, V.; Webster, J.; Campbell, N. R. C. Population-level interventions in government jurisdictions for dietary sodium reduction. Cochrane Library 2016, 2017 (3). [CrossRef]
- Santos, J. A.; Tekle, D. Y.; Rosewarne, E.; Flexner, N.; Cobb, L. K.; Al-Jawaldeh, A.; Kim, W.; Breda, J.; Whiting, S.; Campbell, N. R. C. et al. A Systematic Review of Salt Reduction Initiatives around the world: A midterm evaluation of progress towards the 2025 Global Non-Communicable Diseases Salt Reduction Target. Adv Nutr. 2021, 12 (5), 1768–1780. [CrossRef]
- World Health Organization. Food & Nutrition Action in Health Systems (AHS). SHAKE the salt habit. Available online: https://www.who.int/publications/i/item/WHO-NMH-PND-16.4 (accessed on 19 January 2024).
- World Health Organization. Noncommunicable Diseases, Rehabilitation and Disability (NCD). Tackling NCDs: 'best buys' and other recommended interventions for the prevention and control of noncommunicable diseases. Available online: https://www.who.int/publications/i/item/WHO-NMH-NVI-17.9 (accessed 18 January 2024).
- Tang, N.; Huang, S.; Yang, Y.; Hu, A.; Wang, J.; Cheng, Z.; Liu, W. A review of the world’s salt reduction policies and strategies – preparing for the upcoming 2025. Food & Function 2023. [CrossRef]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; De Jesus, J.; Miller, N.H.; Hubbard, V.S.; Lee, I.-M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E. et al. Z. 2013 AHA/ACC Guideline on Lifestyle Management to Reduce Cardiovascular Risk. Circulation 2014, 129 (25_suppl_2). [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.S.; Jamerson, K.; Jones, D.W. et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation (New York, N.Y.) 2018, 138 (17). [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clément, D.; Coca, A.; De Simone, G.; Dominiczak, A. F. bet al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. J. Hypertens. 2018, 36 (10), 1953–2041. [CrossRef]
- Board, N.; Potassium; Oria, M.; Harrison, M.; Stallings, V. A. Dietary reference intakes for sodium and potassium; 2019. [CrossRef]
- Turck, D.; Castenmiller, J.; De Henauw, S.; Hirsch-Ernst, K.; Kearney, J.; Knutsen, H. K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H. J.; Peláez, C. et al. Dietary reference values for chloride. EFSA Journal 2019, 17 (9). [CrossRef]
- Croatian Institute of Public Health. Epidemiological data on cardiovascular diseases. Available online:https://www.hzjz.hr/aktualnosti/epidemioloski-podaci-o-kardiovaskularnim-bolestima/ (accessed on 10 January 2024).
- Murray, C. J. L.; Aravkin, A. Y.; Zheng, P.; Abbafati, C.; Abbas, K.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I. et al.Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396 (10258), 1223–1249. [CrossRef]
- EH-UH | HDH. HDH. https://hdh.healthmed.hr/projekti/eh-uh (accessed on 20 February 2024).
- Jelaković, B.; Reiner, Ž.; Kusić, Z.; Ugarčić, Ž.; Drenjančević, I. Scientific opinion on the effect of reduced intake of salt in human nutrition. 2014. Zagreb. Available online: file:///C:/Users/mihaela/Downloads/HAH-Z-2014-1%20(9).pdf (accessed on 5 January 2024).
- Reiner, Ž.; Skupnjak B.; Jelaković, B. Launch of a promising national campaign to reduce salt intake in Croatia. Oral communication. Sixth Congress on Atherosclerosis, Rovinj, 2007.
- Less salt -- more health. Croatian action on salt and health (CRASH). PubMed. https://pubmed.ncbi.nlm.nih.gov/19514255/.
- Salt--hidden poison in everyday meal. PubMed. https://pubmed.ncbi.nlm.nih.gov/19642535/.
- Less salt--more health: possibilities of prevention in Croatia. PubMed. https://pubmed.ncbi.nlm.nih.gov/20649071/.
- Jelaković, B.; Vrdoljak, A.; Pećin, I.; Buzjak, V.; Karanović, S.; Ivković, V.; Dapić, K.; Domislović, V.; Reiner, Z. Less salt – more health. Croatian Action on Salt and Health (46). J Hypertens Res 2016, 2 (2), 61-68. Available online: http://hypertens.org/contents/pdfs/jhr-201606-020203.pdf (accessed on 5 February 2024).
- Jelaković, B.; Premužić, V.; Čvorišćec, D.; Erceg, I.; Fuček, M.; Jelaković, M.; Jovanović, A.; Kaić-Rak, A.; Laganović, M.; Lederer, P. et al. Salt Mapping in Croatia. Croatian Action on Salt and Health (CRASH). Kidney and Blood Press Research, 2009; 32:323, 2009.
- Sović, S.;Vitale, K.;Keranović, A;Dražić;Džakula, A.; Jelaković, B. Prevalence, awareness, treatment and control of hypertension and salt intake in some rural area of Sisak – Moslavina county, Croatia. Period. Biol. 2011. Vol. 113, No 3, 321 – 326.
- Pezo-Nikolić, B. Clinical benefit of continuous arterial pressure measurement in the early phase of essential hypertension. Master's thesis (mentor B. Jelaković). School of Medicine, University of Zagreb, Zagreb, Croatia. 2009.
- Salt and hypertension--silent killers. Inform yourself and live longer. World day of hypertension 2009 in Croatia]. PubMed. https://pubmed.ncbi.nlm.nih.gov/19642537/ .
- Ugarčić-Hardi, Ž.; Dumančić, G.; Pitlik, N.; Koceva Komlenić, D.; Jukić, M.; Kuleš, A.; Sabo, M. The salt content in bakery products in Osječko-baranjska County. At Proceedings of 5th International Congress „Flour-Bread ̀09“ and 7th Croatian Congress of Cereal Technologists, 551-556. Faculty of Food Technology, Osijek, 2010.
- Ugarčić-Hardi, Ž. Importance of salt content reduction in bakery products. U Annual 2010/2011 of the Croatian Academy of Engineering, 213-219. Croatian Academy of Engineering, Zagreb, 2012.
- Jurković, M.; Marijanović-Vincetić, D.; Jurković, Z.; Mandić, M.L.; Sokolić-Mihalak D. Salt intake through bakery products in Slavonia region. 7th International Congress "Flour-Bread '13" and 9th Croatian Congress of Cereal Technologists "Brašno-Kruh '13", 42-49, Faculty of Food Technology, Osijek, 2013.
- Pleadin, J.; Koprivnjak, O.; Krešić, G.; Gross-Bošković, A.; Buzjak Služek, V.; Tomljanović, A.; Kovačević, D. Daily salt intake through traditional meat products in Croatia. 2015; 17(6): 566-571.
- Hrvatska agencija za poljoprivredu i hranu, HAPIH (Croatian Agency for Agriculture and Food, CAAF), 2020. Scientific report on the intake of salt through the consumption of bread and bakery products. Ad hoc. Task force of the Center for Food Safety. Available online: https://www.hapih.hr/wp-content/uploads/2021/01/Znanstveno-izvjesce-o-unosu-kuhinjske-soli-konzumacijom-kruha-i-pekarskih-proizvoda_compressed.pdf (accessed on 15 January 2024).
- Hrvatska agencija za hranu, HAH (Croatian Food agency). Less salt – more health. 2014. ISBN: 978-953-55680-3-2. Available online: https://www.hah.hr/pdf/brosura-manje-soli-2014.pdf (accessed on 11 January 2024).
- Ordinance on cereals and cereal products (NN 101/2022.) Available online: https://narodne-novine.nn.hr/clanci/sluzbeni/2016_09_81_1823.html (accessed on 5 February 2024).
- Domislović, V.; Dapić, K.; Miličić, B.; Matašin, M.; Bukal, N.; Capak, K.; Drenjančević, I.; Gulin, M.; Herceg-Cavrak; Jelaković, A. et al. Positive trends in awareness of harmful effects of high salt intake - 10 years Croatian action on salt and health (CRASH). Data from 2008 and 2017 World hypertension days. J. Hypertens. 2018, 36 (Supplement 1), e130. [CrossRef]
- Croatian national programme for reduction of excessive salt intake. PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/25632778/ (accessed on 10 February 2024).
- Aždajić, M.D.; Delaš, I.; Aždajić, S.; Grbić, D. Š.; Vahčić, N. A cross sectional study of salt content in bakery bread in Zagreb, Croatia. Archives for Occupational Hygiene and Toxicology. 2019, 70 (3), 219–223. [CrossRef]
- Karanović, S.; Vrdoljak, A.; Ivković, V.; Dika, Ž.; Domislović, V.; Dapic, K.; Gallineo, L.; Ivandić, E.; Josipović, J.; Vuković, I.; Kos, J.; Laganović, M.; Vrkić, T. Ž.; Fodor, Lj.; Matijević, V.; Fuček, M.; Čulig, J.; Stevanović, R.; Jelaković, B. [PP.30.14] salt consumption in Croatian continental rural population. Journal of Hypertension 2016, 34 (Supplement 2), e311. [CrossRef]
- Croatian Agency for Agriculture and Food, Ad hoc Working Group, Jelaković, B.; Pollak, L.;, Medić, H.; Čačić Kenjerić, D.; Šimundić, T.; Stražanac, D.; Gross - Bošković, A.: Scientific report on the intake of table salt through the consumption of meat products. in 2020.
- Ordinance on salt (NN 89/11), 2011. Available online: https://www.zakon.hr/cms.htm?id=12012 (accessed on 2 March 2024).
- Ma, Y.; He, F. J.; Sun, Q.; Yuan, C.; Kieneker, L. M.; Curhan, G. C.; MacGregor, G. A.; Bakker, S. J. L.; Campbell, N. R. C.; Wang, M. et al. 24-Hour urinary sodium and potassium excretion and cardiovascular risk. N Engl J Med. 2022, 386 (3), 252–263. [CrossRef]
- World Health Organization. Effect of increased potassium intake on blood pressure, renal function, blood lipids and other potential adverse effects. Available online: https://www.who.int/publications/i/item/9789241504881 (accessed on 10 January 2024).
- D’Elia, L.; Barba, G.; Cappuccio, F. P.; Strazzullo, P. Potassium intake, stroke, and cardiovascular disease. J Am Coll Cardiol. 2011, 57 (10), 1210–1219. [CrossRef]
- World Health Organization. Guidelines Review Committee. Guideline: potassium intake for adults and children. Available online: https://www.who.int/publications/i/item/9789241504829 (accessed on 21 February 2024).
- Vulin, M.; Magušić, L.; Metzger, A.-M.; Muller, A.; Drenjančević-Perić, I.; Jukić, I.; Šijanović, S.; Lukić, M.; Stanojević, L.; Cvetko, E. D. et al. Sodium-to-Potassium ratio as an indicator of diet quality in healthy pregnant women. Nutrients 2022, 14 (23), 5052. [CrossRef]
- Miličić, B.; Krtalić, B.; Gellineo, L.; Knežević, T.; Jelaković, A.; Premužić, V.; Dapić, K.; Ivković, V.; Matašin, M.; Fuček, M. et al. Sodium and potassium intake in rural population. J. Hypertens. 2019, 37, e315–e316. [CrossRef]
- Jelaković, A.; Miličić, B.; Krtalić, B.; Gellineo, L.; Knežević, T.; Premužić, V.; Abramović, M.; Domislović, V.; Ivković, V.; Fuček, M. et al. Sodium-to-potassium ratio and new onset hypertension. J. Hypertens. 2019, 37, e121. [CrossRef]
- Chairperson, G.M.; Co-Chair, R.K.; Brunström, M.; Burnier, M.; Grassı, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, C.; Agabiti-Rosei, E.; Algharably, E. et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension. Journal of Hypertension 2023, 41 (12), 1874–2071. [CrossRef]
Figure 1.
Chronology of the CRASH program in Croatia.
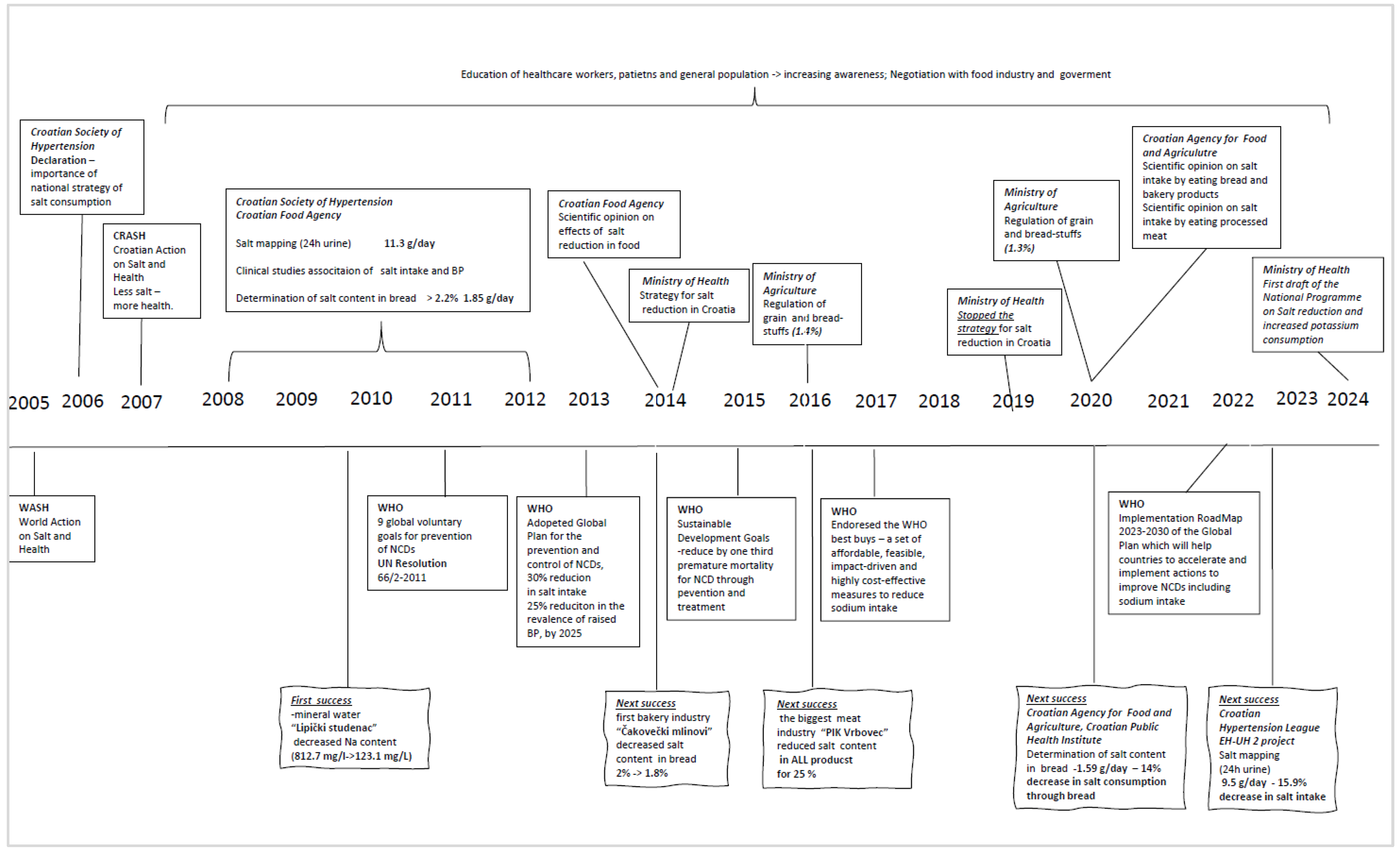
Figure 2.
Decrease in daily intake of table salt through bread and bakery products at the beginning and the end of the third phase of the CRASH program.
Figure 2.
Decrease in daily intake of table salt through bread and bakery products at the beginning and the end of the third phase of the CRASH program.
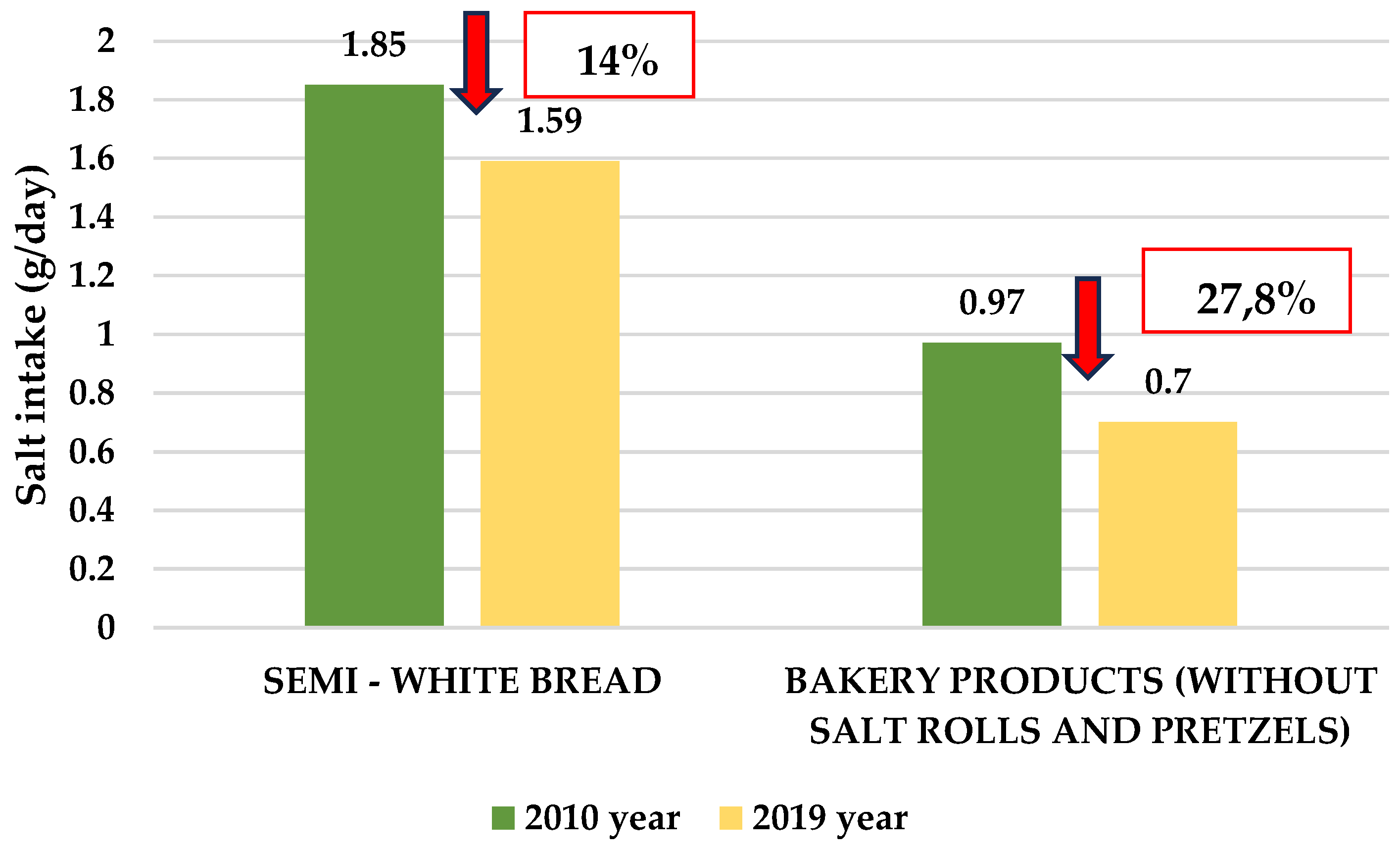

Table 1.
Salt intake (NaCl g/day) before the start of the CRASH program and at the end of the follow-up.
Table 1.
Salt intake (NaCl g/day) before the start of the CRASH program and at the end of the follow-up.
| 2008 | 2020 | Difference in the salt intake | % of change |
|
|---|---|---|---|---|
| Whole group | 11.3 (4.5) | 9.5 (4.1) | -1.8 | 15.9 % |
| Men | 13.3 (4.3) | 10.3 (4.4) | -3.0 | 22.8 % |
| Women | 10.2 (4.2) | 9.0 (3.3) | -1.2 | 11.7 % |
Values are expressed as mean (standard deviation).
Table 2.
Awareness of the harmful effects of excessive salt intake.
| World Hypertension Day, 2008 (%) |
World Hypertension Day, 2017 (%) | May Measurement Month, 2023 (%) | ||
|---|---|---|---|---|
| N | 1076 | 2175 | 10 480 | |
| Questions | Do you know that high salt intake is harmful for your health ? Yes. | 65.3 | 95.8 | 96.9 |
| Have you got this information from physician ? Yes. | 48.9 | 89.1 | 33.8 | |
| Are you eating to salty? Yes | 27 | 36.1 | 36.2 | |
| If advised, would you be able to reduce salt intake ? Yes. | 69.4 | 77.8 | 87.9 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



