
Submitted:
25 April 2024
Posted:
25 April 2024
You are already at the latest version
Abstract
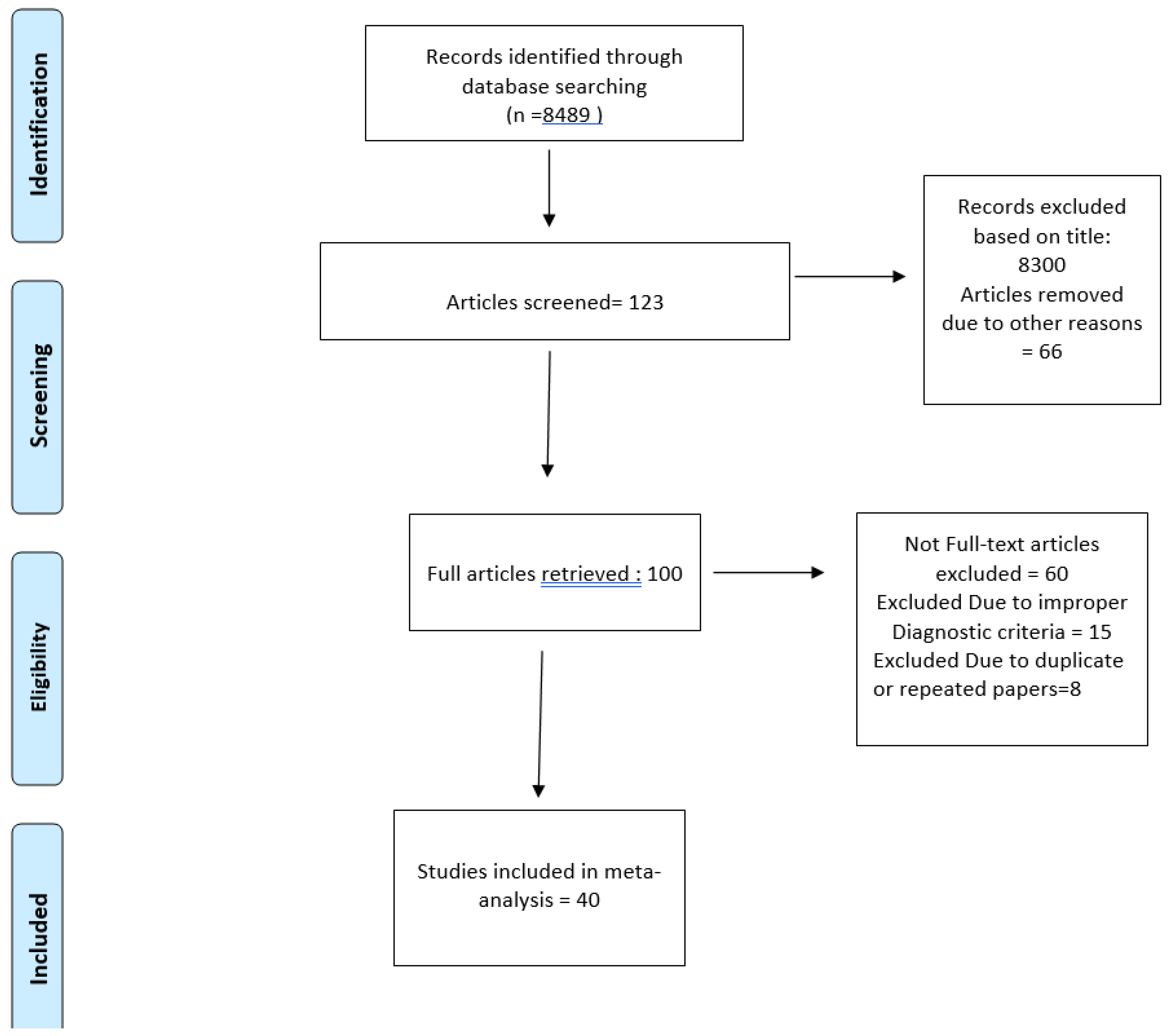
Introduction: Biliary Atresia (BA) is a common cause of neonatal cholestatic jaundice which, if recognized and treated early, can be life-saving for the infant. If the liver biopsy suggests the presence of BA, exploratory laparotomy is then carried out to confirm the diagnosis, along with the Kasai procedure to provide drainage to the bile secreted by the liver. The purpose of this study is to get a deep dive into all the various imaging modalities that can diagnose BA more effectively and with absolute certitude, thus helping prevent several children from a grave prognosis.Methodology: For the collection of the data, a search was done by two individuals using PubMed, Google Scholar, and Cochrane Library databases for all relevant literature. Each qualifying paper was evaluated independently by two reviewers. Each article was analyzed for the number of patients, their age, procedure modality, complexity of ethology, and incidence of the pre-decided complications. The statistical software packages RevMan (Review Manager, version 5.3), SPSS (Statistical Package for the Social Sciences, version 20), Google Sheets, and Excel in Stata 14 were used to perform the statistical analyses. The data was obtained and entered into analytic software.Results: A total of 39 studies with 3,679 subjects were selected for the study, out of which 7 studies showed sensitivity above or equal to 95%, and an astounding 14 studies showed specificity above 95%. The value of True Positive (TP) was 1280, that of True Negative (TN) was 1817, that of False Positive (FP) was 239, and that of False Negative (FN) was 343. With a confidence interval of 95%, sensitivity, specificity, and positive predictive values were calculated. The sensitivity of Ultrasonography for Biliary Atresia is 0.79, with a CI of 95% in a range of 0.77 to 0.81. The specificity of Ultrasonography for Biliary Atresia is 0.88, with a CI of 95% in a range of 0.87 to 0.90. Conclusion: Even though several radiological techniques at present help to detect BA, USG of the abdomen proves to be an effective diagnostic and a modest screening test for the detection of BA.
Keywords:
biliary atresia
; USG
; diagnosis
; meta-analysis
; Index test
; Reference standard
Introduction
Biliary Atresia (BA) is an idiopathic, localized, complete obliteration, or discontinuation, of the hepatic or common bile ducts at any point from the porta hepatis to the duodenum. It is a common cause of neonatal cholestatic jaundice which, if recognized and treated early, can be life-saving for the infant. However, in 70% of the cases, the exact cause of neonatal jaundice is difficult to pinpoint; with idiopathic neonatal hepatitis (NH) and biliary atresia (BA) being the two highly ambiguous diagnoses. Patients with signs of BA usually undergo percutaneous liver biopsy. If the liver biopsy suggests the presence of BA, exploratory laparotomy is then carried out to confirm the diagnosis, along with the Kasai procedure to provide drainage to the bile secreted by the liver. However, the kasai procedure, just like getting used to daylight savings, is more effective when done earlier in life.
This puts forward the need to establish diagnostic procedures that can, with certainty, aid in this time-sensitive diagnosis.
Triangular cord sign, commonly seen during ultrasonographic evaluation, is denoted by a cone-shaped fibrotic mass superior to the bifurcation of the portal vein in BA patients, and is very useful in the diagnosis of BA [1]. Additional strong predictors in a USG for biliary atresia include absence or abnormal gallbladder morphology and enlarged hepatic artery [2].
However other imaging modalities can also be used in the diagnosis of BA. MR cholangiography may not help look at the intrahepatic bile ducts effectively, but it can show a normal extrahepatic bile duct, a dilated common bile duct, and the presence of a choledochal cyst. In this way, it can be used to exclude biliary atresia as the cause of neonatal cholestasis when the extrahepatic bile duct is observed. We discovered in certain studies, a triangular area of high signal intensity on T2-weighted images that was confined to the porta hepatis during the initial period of single shot MR cholangiography [3].
Ultrasound shear wave elastography (SWE) is based on measuring the speed of shear waves generated within the liver. It can help differentiate biliary atresia from other causes of neonatal cholestasis, with higher shear wave speeds suggesting the presence of biliary atresia [4].
An important imaging criterion of biliary patency and biliary atresia has been the presence or absence of bowel radioactivity within 24 h without impaired hepatocellular uptake of the radiotracer. Certain studies showed a fair hepatic uptake but a scintigraphy scan failed to detect bowel radioactivity. As a result, biliary atresia was extraneously diagnosed, and those patients could have been subjected to unnecessary laparotomy. This signifies the need to investigate more in the realm of radiotracer uptake imaging methods [5].
The purpose of this study is to get a deep dive into all the various imaging modalities that can diagnose BA more effectively and with absolute certitude, thus helping prevent several children from a grave prognosis.
Methodology
Data Collection
For the collection of the data, a search was done by two individuals using PubMed, Google Scholar, and Cochrane Library databases for all relevant literature. Full - Text Articles written only in English were considered.
The medical subject headings (MeSH) and keywords ‘Biliary Atresia, ‘Ultrasonography’, ‘Triple Cord Sign’, and ‘Diagnosis’ were used. References, reviews, and meta-analyses were scanned for additional articles.
Inclusion and Exclusion Criteria
Screening of titles and abstracts was carried out, wherein duplicates and citations were filtered out of consideration. Reviewing references of papers found to be relevant was carried out further for underlying additional articles, following which papers with detailed and reliable patient information and results with a strong statistical base were selected.
We searched for papers showing more accurate diagnoses, wherein the modality considered was Ultrasonography for Biliary Atresia for diagnosis of Biliary Atresia.
The inclusion criteria were as follows: (1) studies that provided information about the accurate diagnosis of Biliary Atresia with Ultrasonography for Biliary Atresia; (2) studies published in English; (3) Studies comparing Ultrasonography for Biliary Atresia to the Gold Standard (Surgery) as a diagnostic modality for cases of Biliary Atresia.
The exclusion criteria were: (1) articles that were not full text, (2) unpublished articles, and (3) articles in other languages.
Data Extraction
Each qualifying paper was evaluated independently by two reviewers. Each article was analyzed for the number of patients, their age, procedure modality, complexity of ethology, and incidence of the pre-decided complications. Further discussion or consultation with the author and a third party was used to resolve conflicts. The study’s quality was assessed using the modified Jadad score. In the end, According to PRISMA, a total of 39 studies about the use of Ultrasonography for Biliary Atresia with a total of 3,679 patients were selected for further analysis.
Assessment of Study Quality
Using the QualSyst tool, two writers independently assessed the caliber of each included study. This test consists of 10 questions, each with a score between 0 and 2, with 20 being the maximum possible overall score. Two authors independently rated each article based on the above criteria. The weighted Cohen’s Kappa coefficient (K) was used to determine the interobserver agreement for the study selection. For evaluating the bias risk of the studies, we also employed the Cochrane tool. No assumptions were made about any missing or unclear information. Neither the collection nor the review of data were funded.
Statistical Analysis
The statistical software packages RevMan (Review Manager, version 5.3), SPSS (Statistical Package for the Social Sciences, version 20), Google Sheets, and Excel in Stata 14 were used to perform the statistical analyses. The data was obtained and entered into analytic software [21]. Fixed- or random-effects models were used to estimate Sensitivity, Specificity, positive predictive value (PPV), diagnostic odds ratios (DOR), and relative risk (RR) with 95 percent confidence intervals to examine critical clinical outcomes (CIs). Diagnosis accuracy and Younden Index were calculated for each result. Individual study sensitivity and specificity were plotted on Forest plots and in the receiver operating characteristic (ROC) curve. The forest plot and Fagan’s Nomogram were used to illustrate the sensitivity and specificity of different papers.
Bias Study
Result
Ultrasonography for Biliary Atresia vs Gold Standard
Here, Table 1 describes all the descriptions of papers used for the study regarding the use of Ultrasonography for Diagnosing Biliary Atresia. In Figure 2, the Pooled Sensitivity Values for all papers being considered can be observed and compared amongst each other, while Figure 3 serves the same purpose in the context of Pooled Specificity Values. Figure 4 denotes the pooled Diagnostic Odds Ratio for the application of Ultrasonography for Biliary Atresia. The same is illustrated in the SROC curve. (Figure 5). Figure 6 represents Deek’s Funnel Plot. A total of 39 studies with 3,679 subjects were selected for the study, out of which 7 studies showed sensitivity above or equal to 95%, and an astounding 14 studies showed specificity above 95%. The value of True Positive (TP) was 1280, that of True Negative (TN) was 1817, that of False Positive (FP) was 239, and that of False Negative (FN) was 343. With a confidence interval of 95%, sensitivity, specificity, and positive predictive values were calculated. The sensitivity of Ultrasonography for Biliary Atresia is 0.79, with a CI of 95% in a range of 0.77 to 0.81. The specificity of Ultrasonography for Biliary Atresia is 0.88, with a CI of 95% in a range of 0.87 to 0.90.
Figure 5 shows the summary of the ROC curve. It shows that the area under the curve for Ultrasonography for Biliary Atresia was 0.9395 and the overall diagnostic odds ratio (DOR) was 63.13 with Younden Index being 0.67.
Figure 7 describes the summary of Fagan plot analysis for all the studies considered for Ultrasonography for Biliary Atresia, showing a prior probability of 44% (0.8); a Positive Likelihood Ratio of 6.78; a probability of post-test 84% (5.4); a Negative likelihood ratio of 0.24, and a probability of post-test 16% (0.2).
Discussion
In this Systematic review and meta-analysis including 48 studies, we found that Ultrasonography(USG) is an important and valuable diagnostic test to confirm the presence of Biliary atresia (BA) in neonates and children suffering from cholestatic jaundice. The results show that the pooled sensitivity and specificity of USG, and the various signs we can see with it in biliary atresia, come out to be approximately 79% and 88% respectively. The pooled Odds ratio was found to be about 63.13 and further calculations help us derive the Younden index to be 0.67. Therefore using this test would help us get a relatively lower number of false positive cases, thus helping reduce the incessant need for laparotomy and biopsy for diagnosis. However, other diagnostic modalities that can also help in the diagnosis of BA do exist. This study helped us get a clear representation of each of these methods functions as well as their various advantages and disadvantages to consider when talking about a prompt and certain diagnosis of BA.
The initial evaluation and management of infants presenting with conjugated cholestasis must be rapid and decisive. It is of utmost importance to diagnose surgically correctable disorders, such as BA, promptly to halt the progressive damage to the liver. The success rate for establishing good bile flow after hepatoportoenterostomy (kasai procedure) is much higher if the procedure is done before 2 months of age; the chances of obtaining adequate flow are much lower when the procedure is performed in infants older than 90 days [1].
Ultrasonography is a preferred tool for the visualization of hepatobiliary trees and has several advantages over other imaging methods, notably being non-ionizing, noninvasive, and convenient. However, abdominal ultrasound with a frequency less than 5 MHz is not sufficient enough to evaluate the hepatobiliary tree in infants and neonates. With advances in the technologies behind an ultrasound apparatus, such as the application of the high-frequency detecting probe in the 7 to 12 MHz range, hepatic USG has transformed the screening and diagnosis of BA [39].
Percutaneous biopsy is one of the most reliable methods that can diagnose BA. However, because the procedure is invasive and thus comes with a roster of unwanted but sometimes unavoidable complications such as bleeding and bile leakage, many parents are reluctant to have their infants undergo the anesthesia that is required for this procedure. Thus making it difficult to diagnose or exclude BA preoperatively [35].
When screening infants with cholestatic jaundice, especially to differentiate BA from NH and other causes of infantile cholestasis, length and contractility of the gallbladder, as seen during USG, were used to be reliable findings. An uncontracted bladder or a reduced size is diagnostic of BA. However, both of these findings are seen in both BA and neonatal hepatitis. It should be noted that gall bladder contractility can also sometimes be observed in patients with BA, particularly in patients with a patent common bile duct.
The Triangular Cord Sign (TCS) as defined in 1996, is a triangular or conical-shaped echogenic density representing a fibrous remnant of the extrahepatic bile duct at the porta hepatis observed superior to the portal bifurcation. Triangular cord sign offers a reliable sign in the diagnosis of BA. However, to further improve the accuracy of ultrasonographic imaging in the diagnosis of BA, studies proposed combining TCS findings with gallbladder imaging. Positive TCS coupled with abnormal gallbladder (length <1.5 cm, identifiable but no lumen [“non visualized”] or not identifiable) improves the diagnostic parameters. It should be noted that a gallbladder is considered to be abnormal when it is small (length <1.5 cm or not identifiable) or uncontracted [31]. Triangular cord sign comes with the bane of being operator-dependent which sullies its usefulness and questions its reliability in all cases and scenarios, especially in the early stages of the disease or when the operator is not experienced enough to localize this sign.
Doppler studies help improve the accuracy of USG. The use of an EARPV(echogenic anterior wall of the right portal vein) with 4-mm thickness as a criterion for identifying the TC sign in the diagnosis of BA is considered a standard with fairly high sensitivity and specificity. According to some studies, the fibrotic cord can be easily masked by diffuse periportal echogenicity when there is nonspecific inflammation or cirrhosis. Thus, the TC sign is supportive but not as sensitive when either cirrhosis or widespread periportal inflammation is present.
In patients with BA, the diameter of the hepatic artery is considerably higher, as compared to patients without BA. Multiple studies show that the diameter of the hepatic artery was significantly higher in patients with BA as compared to patients with non-BA and control subjects [35].
BA leads to hyperplastic and hypertrophic changes in the hepatic artery, which has been well documented in several studies. Although the definitive pathogenesis of RHA enlargement is still unclear, it has been theorized that this may be due to a compensatory change to maintain the blood supply to the hepatobiliary tree, which is considered a compensatory change to hepatic fibrosis. Studies have also suggested that the presence of hepatic subcapsular flow was useful for differentiating BA from other causes of neonatal jaundice [37].
Hepatobiliary scintigraphy with technetium labeled iminodiacetic acid derivatives, followed by the measurement of radioactivity in the bowel, can also be used in the diagnosis of BA and helps to distinguish it from other causes of cholestatic jaundice. In BA, the hepatic uptake of the agent is unimpaired, while its excretion into the intestine is absent. However, by contrast, the uptake may be impaired in Neonatal Hepatitis (NH) but excretion into the bowel will eventually occur. Therefore, obtaining a follow-up scan will be important in determining the patency of the extrahepatic biliary tree. The administration of phenobarbital (5 mg/kg/d), 5 days before the scan, may amplify biliary excretion of the isotope. Certain drawbacks such as the need to wait for 5 days and the decreased specificity of the test make it less practical and its usefulness is limited for most children and neonates suspected to have BA [31].
In recent years, multiple studies have come up with a new imaging technique that has the advantage of being a novel sonographic method that is not only non-invasive but is also low-cost and a well-tolerated approach to evaluate and diagnose liver fibrosis by quantifying liver stiffness, a very common finding in BA [35].
Based on these studies, the approximated normal SWS (shear wave speed) is 1.15 m/s, ranging from 1.12 m/s to 1.19 m/s. Additional small cohort studies have shown the utility of SWE in quantifying liver fibrosis in children, ensuring its place in the array of diagnostic tests used for disease entities with hepatic fibrosis as a major culprit for their pathology.
It should be noted that despite its reliability, SWE as a sole diagnostic tool for biliary atresia was not as sensitive or specific as the majority of objective individual grey-scale US findings
The SWS values correspond significantly with the infant’s age as well as the stage of hepatic fibrosis, implying that the increase of SWS in older infants could very well be confounded by progressive fibrosis seen in later stages of the disease. However, in multiple studies, these variables were considered equivalent because increased fibrosis staging is expected in older infants.
The median SWE SWS value for infants with biliary atresia was 2.1 m/s ranging from 1.7–2.4 m/s, significantly higher than non-biliary-atresia infants, 1.5 m/s.
Overall, considering the current advances in US technology, SWE as a sole diagnostic method was not highly accurate for differentiating biliary atresia from other causes of neonatal jaundice.
A grey-scale US evaluation of the child should be performed first, and if the triangular cord sign is present, irrespective of additional findings, BA can be diagnosed with certainty. If the triangular cord sign is not present or if the results are equivocal, further evaluation for gallbladder abnormality and CBD visualization should be done. If both are normal, and there is no hepatic artery enlargement, then biliary atresia is most likely ruled out. If the gallbladder and CBD are both abnormal/absent and hepatic artery enlargement is seen, then biliary atresia is most certainly present.
The likelihood of BA remains indeterminate in all other cases. In this situation, SWE is a helpful tool to predict the likelihood of biliary atresia, With a direct correlation between higher SWS values and the probability of BA. The recommended high SWS cutoff in a 2-month-old infant is 2.2 m/s and low SWS cutoff is 1.5 m/s. A value of SWS in between these would be considered indeterminate, requiring additional tests [2].
Additionally, it was found that the mean SWE values between normal infants and those with infantile hepatitis syndrome were not statistically different. Thus the liver stiffness in infantile hepatitis syndrome is equal to that in normal infants. Hence SWE measurement of increased liver stiffness can be helpful to differentiate BA from infantile hepatitis syndrome Furthermore, some studies point out the fact that in a lot of infants with BA, the histologic examination may not be evident of the classic findings of BA, especially during the early onset of disease (i.e., before 6 weeks of age).
We can also correlate the SWS values with the degree of liver stiffness, and indirectly the progress of BA. It is especially useful in the sonographic screening of liver fibrosis progression over time after the kasai procedure [37].
Thus SWS elastography could be an important adjunctive test to not only aid in the diagnosis of BA but also help in further prognostication of the disease after a curative surgery.
In several preliminary studies, MR cholangiography has been used to detect Biliary atresia in infants. The presence of the complete extrahepatic biliary tree on MR cholangiography can very well be used to rule out BA. However, in the case of MR cholangiography, visualization of the biliary tree depends on the production and secretion of bile. Therefore, the insufficient production or secretion of bile due to other severe cholestatic diseases can result in a false-positive result. In addition, the spatial resolution of images obtained in neonates with shallow respiration allows visualization of abnormal dilated ducts But in infants who cannot hold their breaths, MR cholangiography cannot reliably confirm the absence of ducts because of the image degradation that occurs in these infants.
Several previous studies have indicated that MR cholangiography is a noninvasive, reliable as well as accurate imaging technique that helps to define the architecture of major biliary structures in neonates and small infants, thus excluding biliary atresia as the cause of neonatal cholestasis However, in contrast to these reports, some studies reported both false positive and false negative findings and an overall accuracy of only 82% when they used MR cholangiography. The basic principle of MR cholangiography lies in its ability to detect fibrosis, especially periportal fibrosis. However, periportal fibrosis is not specific to biliary atresia and can also be seen with other conditions such as severe neonatal hepatitis. These characteristics of MR cholangiography make it a reliable technique to diagnose BA but with the caveat of considering it with a grain of salt when dealing with diseases with a similar pathology to that of BA [30].
Conclusion
The concluding statement of this article would likely point out the disappearing ambiguity in the diagnostic tests used in BA, akin to the fate of the biliary system in this dreadful yet treatable condition. As more and more diseases pivot towards a worsening prognosis if treated at a later stage, diagnostic tests that are less invasive, cheaper, easier to operate, and simplified in their interpretation, are a welcome introduction in the cohort of treatment plans that improve the survival of the patient. Even though several radiological techniques at present help to detect BA, USG of the abdomen proves to be an effective diagnostic and a modest screening test for the detection of BA. Other imaging techniques, while requiring certain prerequisites and prior preparations, certainly help to make up a diagnostic algorithm that can be relied upon to make sure that the various differential diagnoses for cholestatic jaundice in neonates and newborns can be demarcated with precision and accuracy.
Funding and Sponsorship
None of the authors are financially interested in any of the products, devices or drugs mentioned in this manuscript.
Ethical Statement
Being Meta analysis, there were no ethical issues and the IRB permission is not required.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kotb MA, Kotb A, Sheba MF, El Koofy NM, El-Karaksy HM, Abdel-Kahlik MK, Abdalla A, El-Regal ME, Warda R, Mostafa H, Karjoo M, A-Kader HH. Evaluation of the triangular cord sign in the diagnosis of biliary atresia. Pediatrics. 2001 Aug;108(2):416-20. [CrossRef] [PubMed]
- Sandberg JK, Sun Y, Ju Z, Liu S, Jiang J, Koci M, Rosenberg J, Rubesova E, Barth RA. Ultrasound shear wave elastography: does it add value to gray-scale ultrasound imaging in differentiating biliary atresia from other causes of neonatal jaundice? Pediatr Radiol. 2021 Aug;51(9):1654-1666. Epub 2021 Mar 27. [CrossRef] [PubMed]
- Zhou LY, Jiang H, Shan QY, Chen D, Lin XN, Liu BX, Xie XY. Liver stiffness measurements with supersonic shear wave elastography in the diagnosis of biliary atresia: a comparative study with grey-scale US. Eur Radiol. 2017 Aug;27(8):3474-3484. Epub 2017 Jan 12. [CrossRef] [PubMed]
- Wongsawasdi L, Ukarapol N, Visrutaratna P, Singhavejsakul J, Kattipattanapong V. Diagnostic evaluation of infantile cholestasis. J Med Assoc Thai. 2008 Mar;91(3):345-9. [PubMed]
- Dong B, Weng Z, Lyu G, Yang X, Wang H. The diagnostic performance of ultrasound elastography for biliary atresia: A meta-analysis. Front Public Health. 2022 Oct 26;10:973125. PMCID: PMC9643747. [CrossRef] [PubMed]
- Aziz S, Wild Y, Rosenthal P, Goldstein RB. Pseudo gallbladder sign in biliary atresia--an imaging pitfall. Pediatr Radiol. 2011 May;41(5):620-6; quiz 681-2. Epub 2011 Mar 16. PMCID: PMC3076559. [CrossRef] [PubMed]
- Boo YA, Chang MH, Jeng YM, Peng SF, Hsu WM, Lin WH, Chen HL, Ni YH, Hsu HY, Wu JF. Diagnostic Performance of Transient Elastography in Biliary Atresia Among Infants With Cholestasis. Hepatol Commun. 2021 Feb 26;5(5):882-890. PMCID: PMC8122382. [CrossRef] [PubMed]
- Dillman JR, DiPaola FW, Smith SJ, Barth RA, Asai A, Lam S, Campbell KM, Bezerra JA, Tiao GM, Trout AT. Prospective Assessment of Ultrasound Shear Wave Elastography for Discriminating Biliary Atresia from Other Causes of Neonatal Cholestasis. J Pediatr. 2019 Sep;212:60-65.e3. Epub 2019 Jun 26. [CrossRef] [PubMed]
- Donia AE, Ibrahim SM, Kader MS, Saleh AM, El-Hakim MS, El-Shorbagy MS, Mansour MM, Gibriel MA. Predictive value of assessment of different modalities in the diagnosis of infantile cholestasis. J Int Med Res. 2010;38(6):2100-16. [CrossRef] [PubMed]
- Duan X, Peng Y, Liu W, Yang L, Zhang J. Does Supersonic Shear Wave Elastography Help Differentiate Biliary Atresia from Other Causes of Cholestatic Hepatitis in Infants Less than 90 Days Old? Compared with Grey-Scale US. Biomed Res Int. 2019 Jun 2;2019:9036362. PMCID: PMC6582890. [CrossRef] [PubMed]
- Duan X, Peng Y, Liu W, Yang L, Zhang J. Does Supersonic Shear Wave Elastography Help Differentiate Biliary Atresia from Other Causes of Cholestatic Hepatitis in Infants Less than 90 Days Old? Compared with Grey-Scale US. Biomed Res Int. 2019 Jun 2;2019:9036362. PMCID: PMC6582890. [CrossRef] [PubMed]
- El-Guindi MA, Sira MM, Sira AM, Salem TA, El-Abd OL, Konsowa HA, El-Azab DS, Allam AA. Design and validation of a diagnostic score for biliary atresia. J Hepatol. 2014 Jul;61(1):116-23. Epub 2014 Mar 18. Erratum in: J Hepatol. 2015 Jul;63(1):289. [CrossRef] [PubMed]
- Farrant P, Meire HB, Mieli-Vergani G. Improved diagnosis of extrahepatic biliary atresia by high-frequency ultrasound of the gall bladder. Br J Radiol. 2001 Oct;74(886):952-4. [CrossRef] [PubMed]
- Hanquinet S, Rougemont AL, Courvoisier D, Rubbia-Brandt L, McLin V, Tempia M, Anooshiravani M. Acoustic radiation force impulse (ARFI) elastography for the noninvasive diagnosis of liver fibrosis in children. Pediatr Radiol. 2013 Mar;43(5):545-51. Epub 2012 Dec 28. [CrossRef] [PubMed]
- Humphrey TM, Stringer MD. Biliary atresia: US diagnosis. Radiology. 2007 Sep;244(3):845-51. [CrossRef] [PubMed]
- Imanieh MH, Dehghani SM, Bagheri MH, Emad V, Haghighat M, Zahmatkeshan M, Forutan HR, Rasekhi AR, Gheisari F. Triangular cord sign in detection of biliary atresia: is it a valuable sign? Dig Dis Sci. 2010 Jan;55(1):172-5. Epub 2009 Feb 20. [CrossRef] [PubMed]
- Jiang LP, Chen YC, Ding L, Liu XL, Li KY, Huang DZ, Zhou AY, Zhang QP. The diagnostic value of high-frequency ultrasonography in biliary atresia. Hepatobiliary Pancreat Dis Int. 2013 Aug;12(4):415-22. [CrossRef] [PubMed]
- Kanegawa K, Akasaka Y, Kitamura E, Nishiyama S, Muraji T, Nishijima E, Satoh S, Tsugawa C. Sonographic diagnosis of biliary atresia in pediatric patients using the “triangular cord” sign versus gallbladder length and contraction. AJR Am J Roentgenol. 2003 Nov;181(5):1387-90. [CrossRef] [PubMed]
- Kim WS, Cheon JE, Youn BJ, Yoo SY, Kim WY, Kim IO, Yeon KM, Seo JK, Park KW. The hepatic arterial diameter was measured with the US: adjunct for US diagnosis of biliary atresia. Radiology. 2007 Nov;245(2):549-55. Epub 2007 Sep 21. [CrossRef] [PubMed]
- Kim MJ, Park YN, Han SJ, Yoon CS, Yoo HS, Hwang EH, Chung KS. Biliary atresia in neonates and infants: triangular area of high signal intensity in the porta hepatis at T2-weighted MR cholangiography with US and histopathologic correlation. Radiology. 2000 May;215(2):395-401. [CrossRef] [PubMed]
- Lee CH, Wang PW, Lee TT, Tiao MM, Huang FC, Chuang JH, Shieh CS, Cheng YF. The significance of functioning gallbladder visualization on hepatobiliary scintigraphy in infants with persistent jaundice. J Nucl Med. 2000 Jul;41(7):1209-13. [PubMed]
- Lee HJ, Lee SM, Park WH, Choi SO. Objective criteria of triangular cord sign in biliary atresia on US scans. Radiology. 2003 Nov;229(2):395-400. [CrossRef] [PubMed]
- Lee MS, Kim MJ, Lee MJ, Yoon CS, Han SJ, Oh JT, Park YN. Biliary atresia: color Doppler US findings in neonates and infants. Radiology. 2009 Jul;252(1):282-9. Erratum in: Radiology. 2011 Dec;261(3):1003. [CrossRef] [PubMed]
- Lee SM, Cheon JE, Choi YH, Kim WS, Cho HH, Kim IO, You SK. Ultrasonographic Diagnosis of Biliary Atresia Based on a Decision-Making Tree Model. Korean J Radiol. 2015 Nov-Dec;16(6):1364-72. Epub 2015 Oct 26. Erratum in: Korean J Radiol. 2016 Jan-Feb;17(1):173. PMCID: PMC4644760. [CrossRef] [PubMed]
- Liu YF, Ni XW, Pan Y, Luo HX. Comparison of the diagnostic value of virtual touch tissue quantification and virtual touch tissue imaging quantification in infants with biliary atresia. Int J Clin Pract. 2021 Apr;75(4):e13860. Epub 2020 Dec 22. [CrossRef] [PubMed]
- Dong B, Weng Z, Lyu G, Yang X, Wang H. The diagnostic performance of ultrasound elastography for biliary atresia: A meta-analysis. Front Public Health. 2022 Oct 26;10:973125. PMCID: PMC9643747. [CrossRef] [PubMed]
- Mittal V, Saxena AK, Sodhi KS, Thapa BR, Rao KL, Das A, Khandelwal N. Role of abdominal sonography in the preoperative diagnosis of extrahepatic biliary atresia in infants younger than 90 days. AJR Am J Roentgenol. 2011 Apr;196(4):W438-45. [CrossRef] [PubMed]
- Park WH, Choi SO, Lee HJ, Kim SP, Zeon SK, Lee SL. A new diagnostic approach to biliary atresia with emphasis on the ultrasonographic triangular cord sign: comparison of ultrasonography, hepatobiliary scintigraphy, and liver needle biopsy in the evaluation of infantile cholestasis. J Pediatr Surg. 1997 Nov;32(11):1555-9. [CrossRef] [PubMed]
- Rouzrokh, Mohsen & Sobhiyeh, Mohammad & Heibatollahi, Motahare. (2009). The Sensitivity, Specificity, Positive and Negative Predictive Values of Stool Color test, Triangular Cord Sign, and Hepatobiliary Scintigraphy in Diagnosis of Infantile Biliary Atresia. Iranian Red Crescent Medical Journal. 11.
- Ryeom HK, Choe BH, Kim JY, Kwon S, Ko CW, Kim HM, Lee SB, Kang DS. Biliary atresia: feasibility of mangafodipir trisodium-enhanced MR cholangiography for evaluation. Radiology. 2005 Apr;235(1):250-8. Epub 2005 Mar 4. [CrossRef] [PubMed]
- Shen Q, Tan SS, Wang Z, Cai S, Pang W, Peng C, Chen Y. Combination of gamma-glutamyl transferase and liver stiffness measurement for biliary atresia screening at different ages: a retrospective analysis of 282 infants. BMC Pediatr. 2020 Jun 4;20(1):276. PMCID: PMC7271542. [CrossRef] [PubMed]
- Shima H, Igarashi G, Wakisaka M, Hamano S, Nagae H, Koyama M, Kitagawa H. Noninvasive acoustic radiation force impulse (ARFI) elastography for assessing the severity of fibrosis in the post-operative patients with biliary atresia. Pediatr Surg Int. 2012 Sep;28(9):869-72. [CrossRef] [PubMed]
- Sun Y, Zheng S, Qian Q. Ultrasonographic evaluation in the differential diagnosis of biliary atresia and infantile hepatitis syndrome. Pediatr Surg Int. 2011 Jul;27(7):675-9. Epub 2011 Jan 5. [CrossRef] [PubMed]
- Takamizawa S, Zaima A, Muraji T, Kanegawa K, Akasaka Y, Satoh S, Nishijima E. Can biliary atresia be diagnosed by ultrasonography alone? J Pediatr Surg. 2007 Dec;42(12):2093-6. [CrossRef] [PubMed]
- Tan Kendrick AP, Phua KB, Ooi BC, Tan CE. Biliary atresia: making the diagnosis by the gallbladder ghost triad. Pediatr Radiol. 2003 May;33(5):311-5. Epub 2003 Mar 6. [CrossRef] [PubMed]
- Visrutaratna P, Wongsawasdi L, Lerttumnongtum P, Singhavejsakul J, Kattipattanapong V, Ukarapol N. Triangular cord sign and ultrasound features of the gall bladder in infants with biliary atresia. Australas Radiol. 2003 Sep;47(3):252-6. [CrossRef] [PubMed]
- Wang X, Qian L, Jia L, Bellah R, Wang N, Xin Y, Liu Q. Utility of Shear Wave Elastography for Differentiating Biliary Atresia From Infantile Hepatitis Syndrome. J Ultrasound Med. 2016 Jul;35(7):1475-9. Epub 2016 May 26. [CrossRef] [PubMed]
- Wu JF, Lee CS, Lin WH, Jeng YM, Chen HL, Ni YH, Hsu HY, Chang MH. Transient elastography is useful in diagnosing biliary atresia and predicting prognosis after hepatoportoenterostomy. Hepatology. 2018 Aug;68(2):616-624. Epub 2018 May 24. [CrossRef] [PubMed]
- Zhou LY, Wang W, Shan QY, Liu BX, Zheng YL, Xu ZF, Xu M, Pan FS, Lu MD, Xie XY. Optimizing the US Diagnosis of Biliary Atresia with a Modified Triangular Cord Thickness and Gallbladder Classification. Radiology. 2015 Oct;277(1):181-91. Epub 2015 May 6. [CrossRef] [PubMed]
Figure 2.
The forest chart summary for pooled sensitivity values of Ultrasonography for Diagnosing Biliary Atresia.
Figure 2.
The forest chart summary for pooled sensitivity values of Ultrasonography for Diagnosing Biliary Atresia.
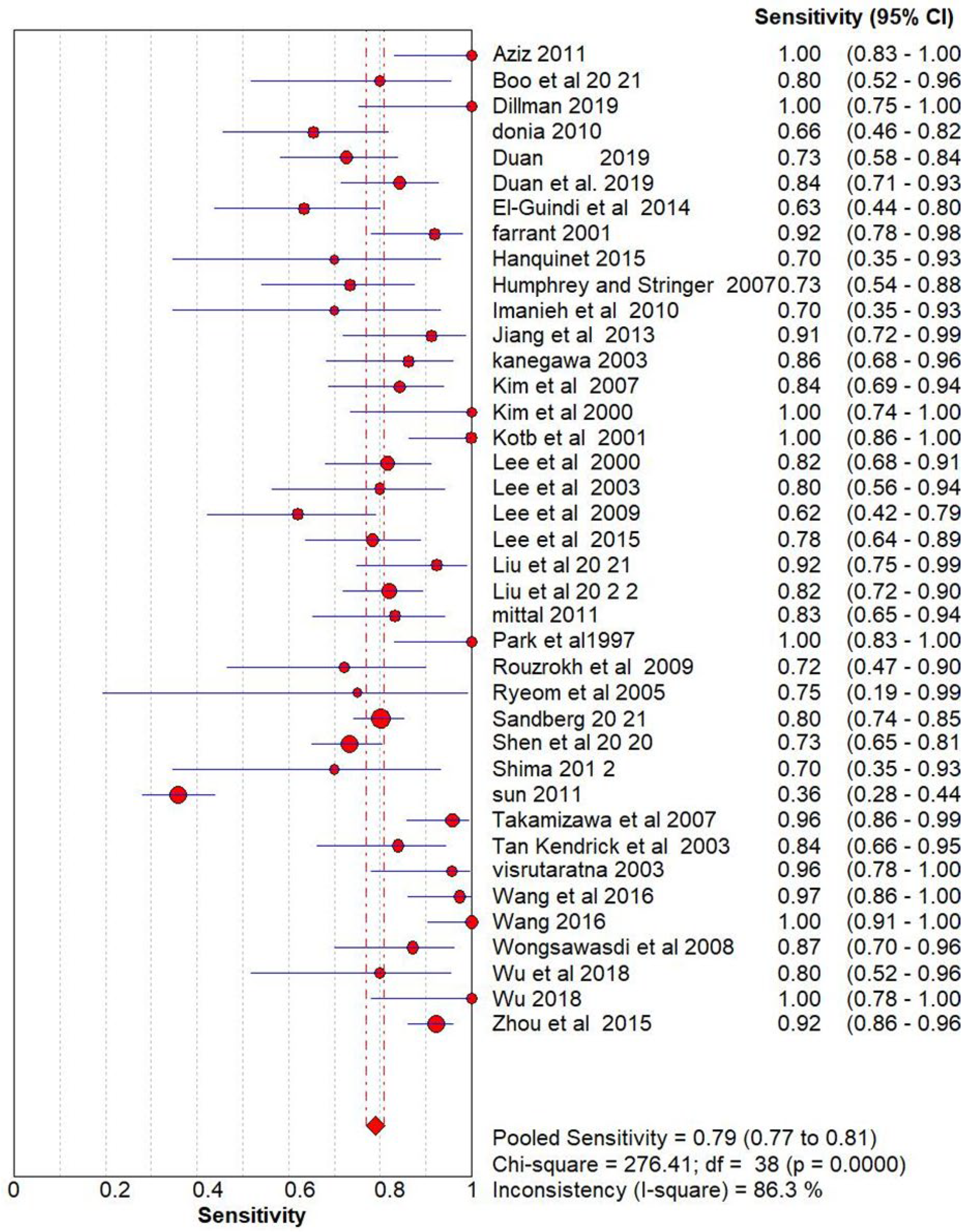
Figure 3.
The forest chart summary for pooled specificity values for Ultrasonography for Diagnosing Biliary Atresia.
Figure 3.
The forest chart summary for pooled specificity values for Ultrasonography for Diagnosing Biliary Atresia.
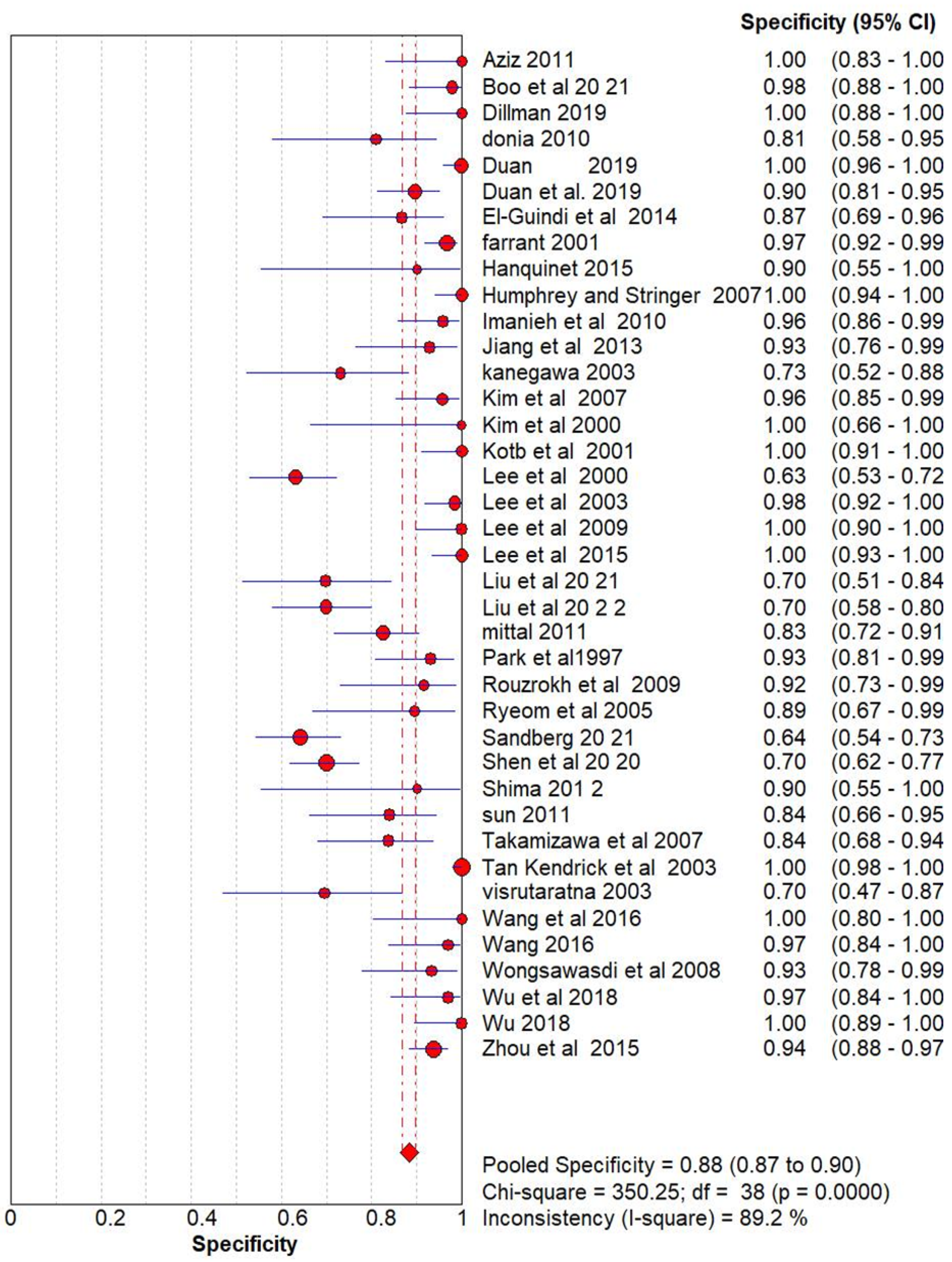
Figure 4.
The forest chart summary for pooled Diagnostic Odds Ratio for Ultrasonography for Diagnosing Biliary Atresia.
Figure 4.
The forest chart summary for pooled Diagnostic Odds Ratio for Ultrasonography for Diagnosing Biliary Atresia.
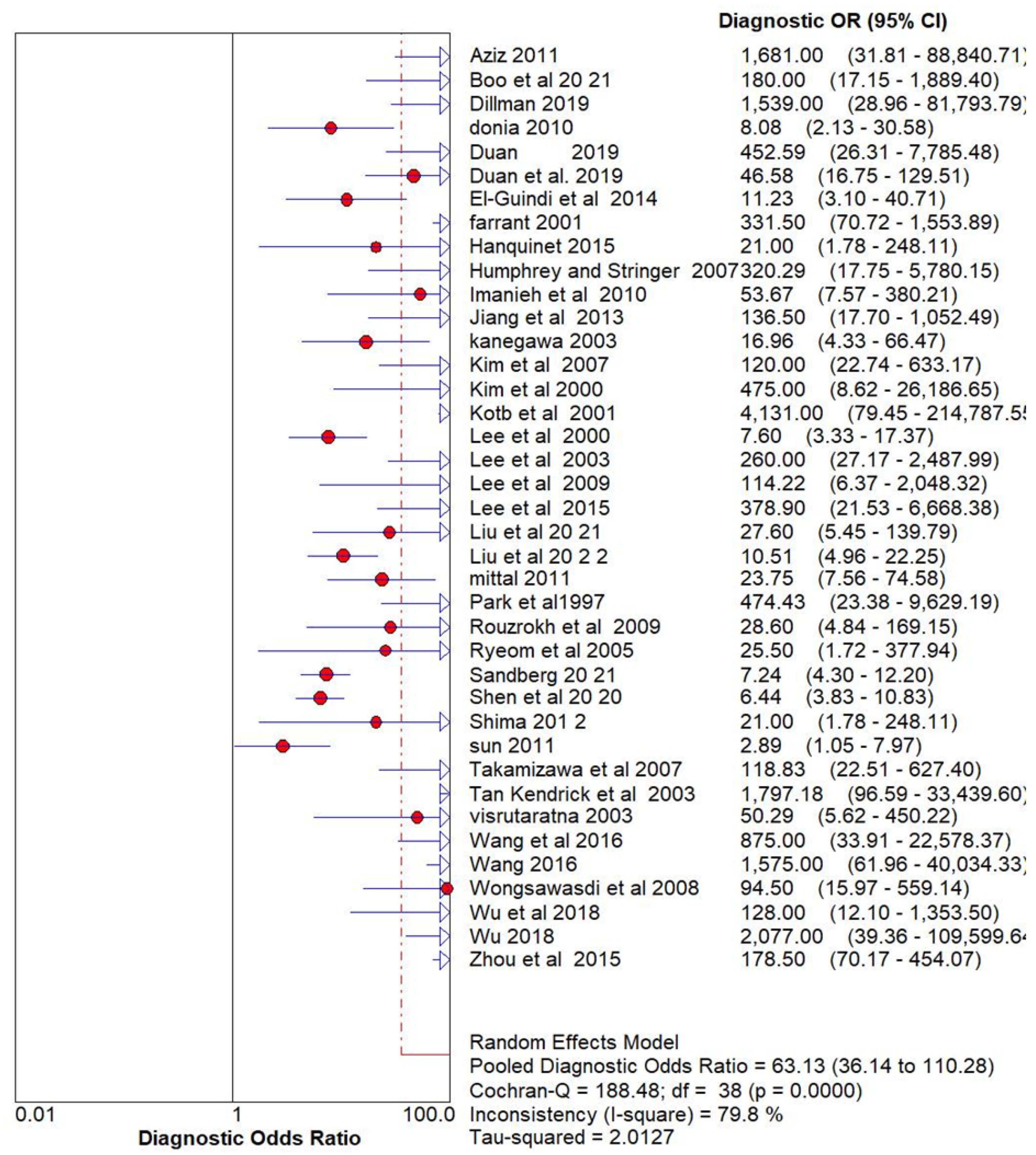
Figure 5.
The SROC plot summary for Ultrasonography for Diagnosing Biliary Atresia.
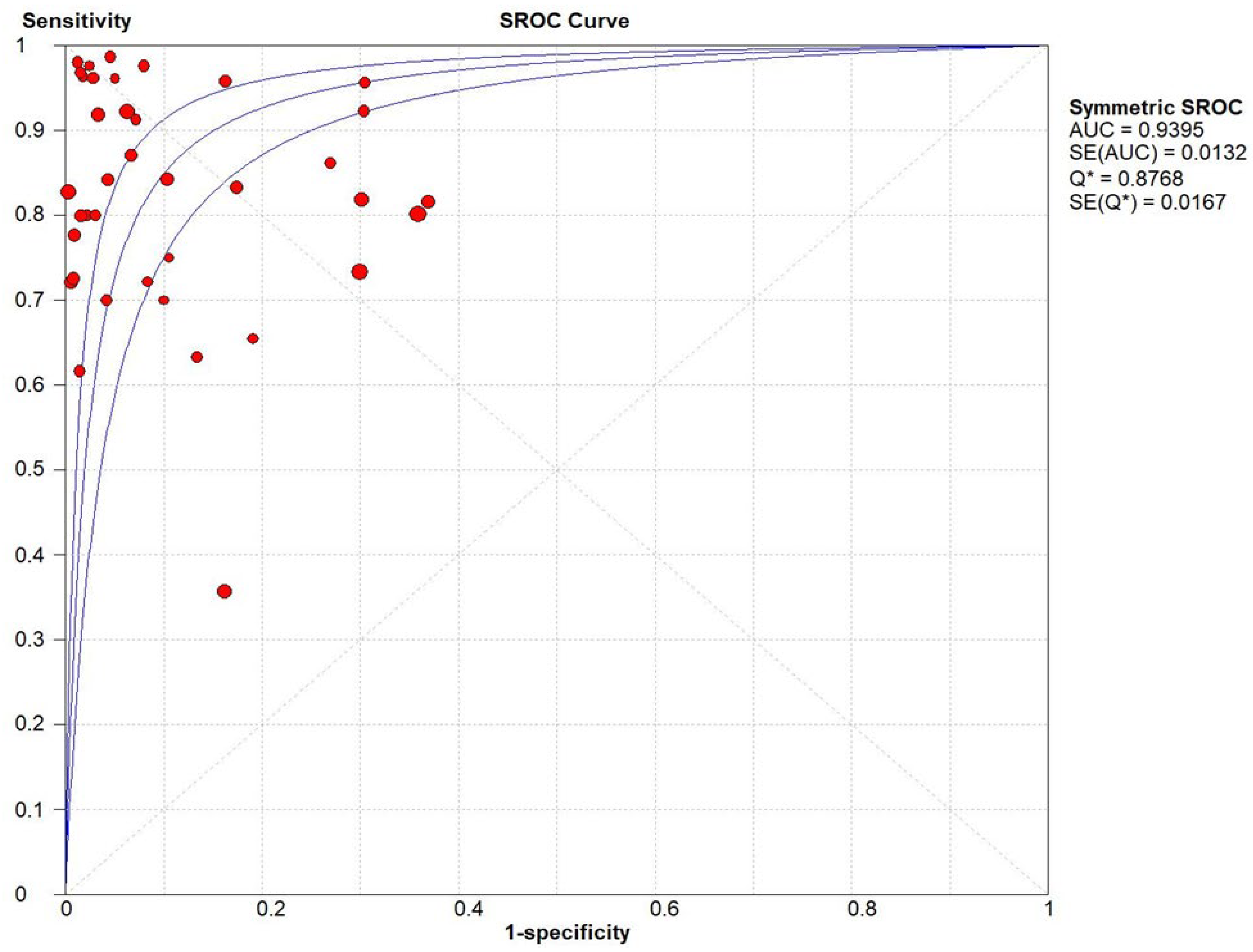
Figure 6.
Funnel Plot for Ultrasonography for Diagnosing Biliary Atresia.
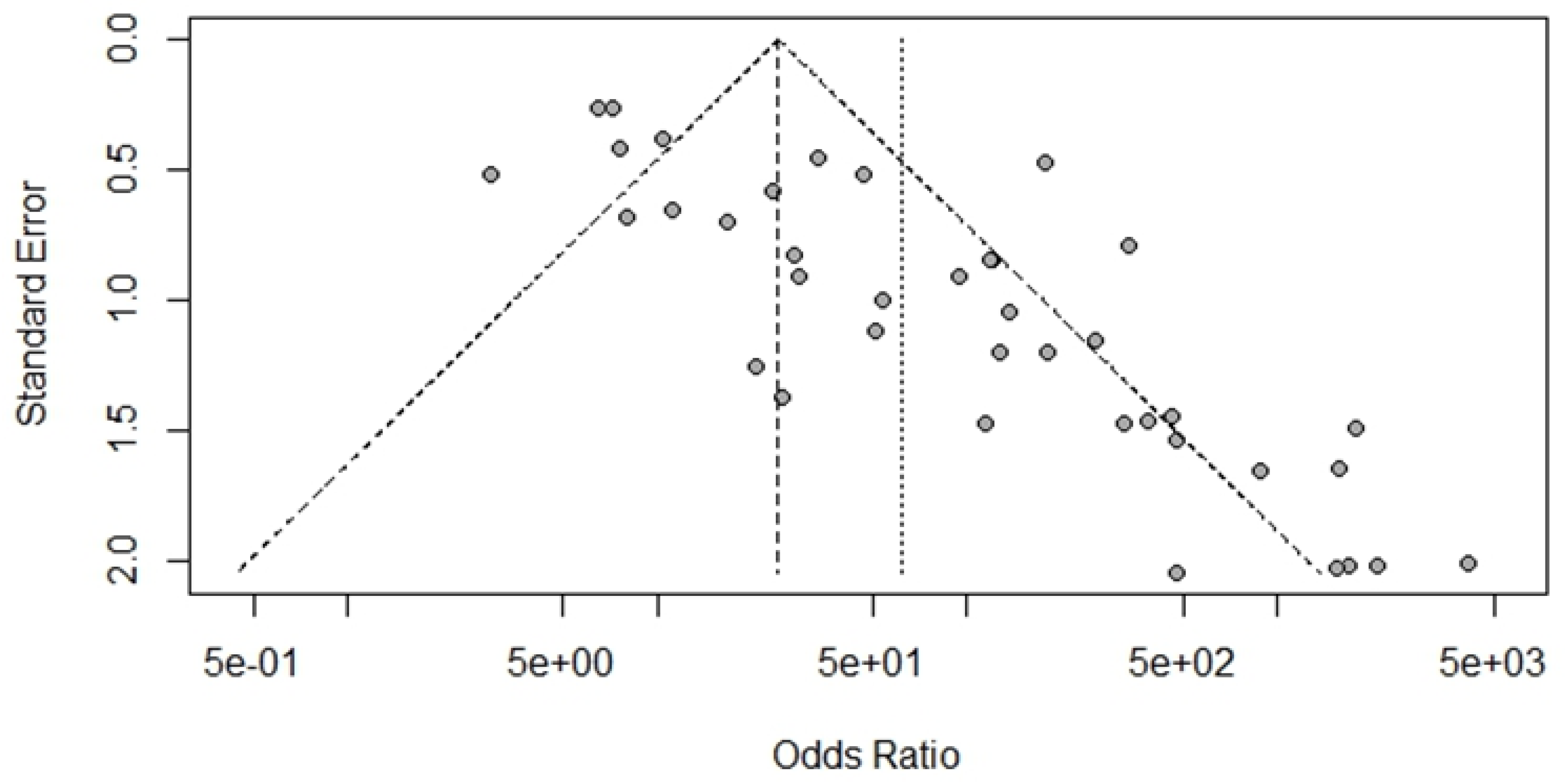
Figure 7.
Fagan’s Analysis for Ultrasonography for Diagnosing Biliary Atresia. Prior Probability (Odds): 44% (0.8).
Figure 7.
Fagan’s Analysis for Ultrasonography for Diagnosing Biliary Atresia. Prior Probability (Odds): 44% (0.8).
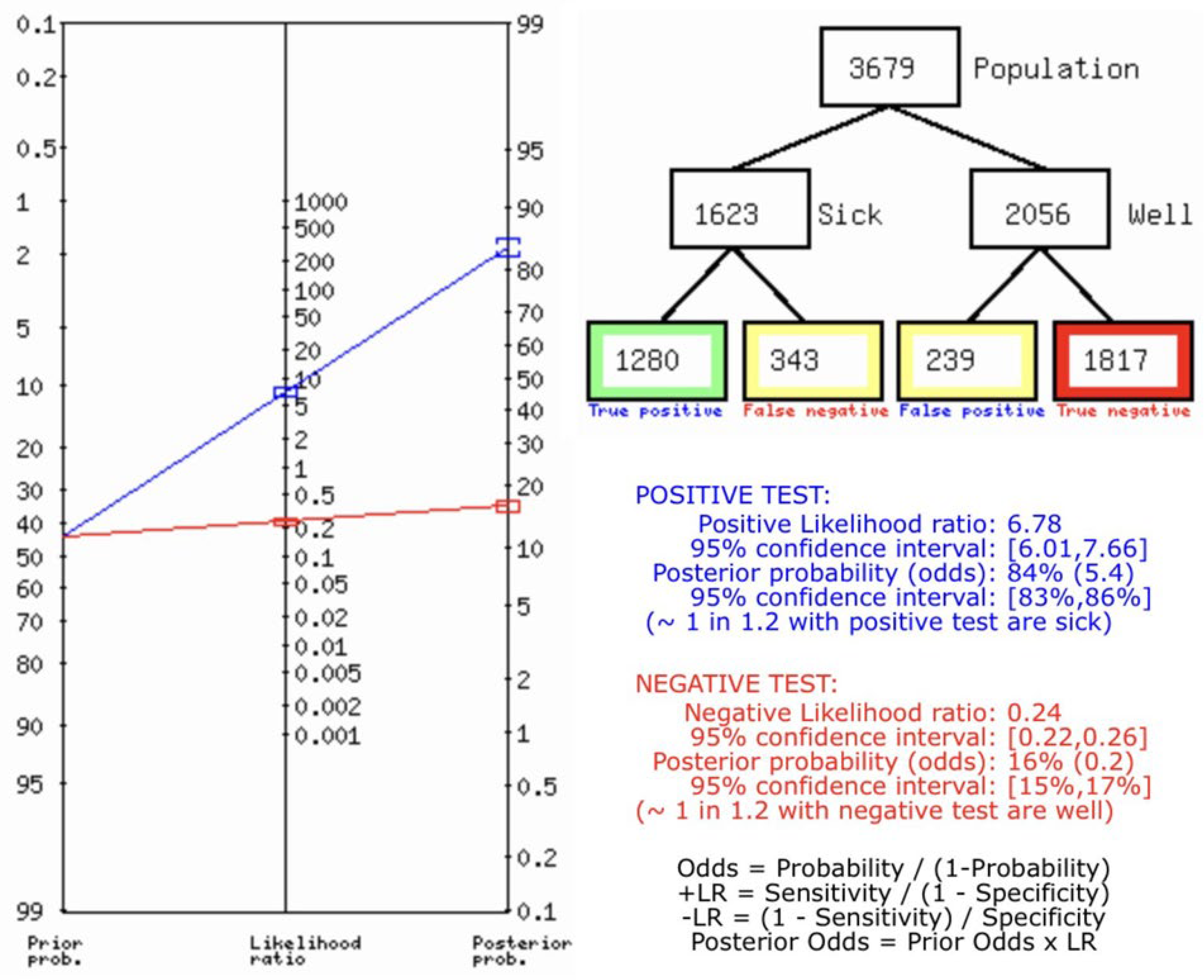
Figure 8.
Bias study.
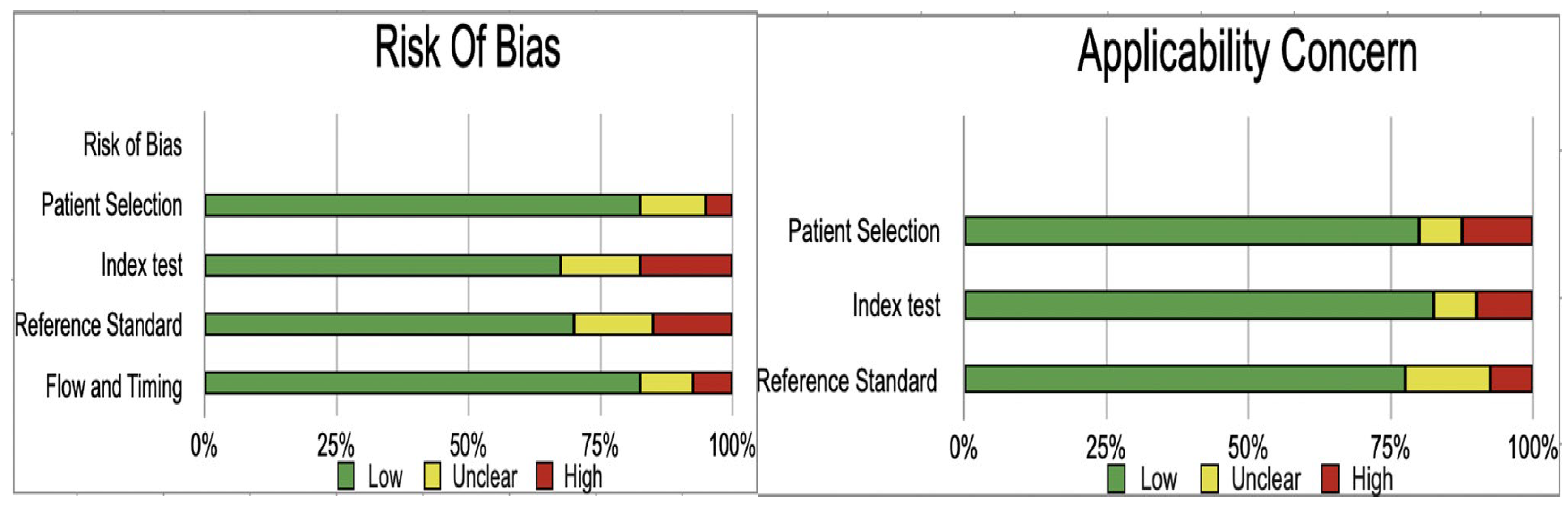

Table 1.
characteristics of the study.
| Name | Methodology | True Positive (Tp) | False positive (FP) | False Negative (FN) | True Negative (TN) |
|---|---|---|---|---|---|
| Aziz 2011 [6] | USG | 20 | 0 | 0 | 20 |
| Boo et al. 20 21 [7] | USG | 12 | 1 | 3 | 45 |
| Dillman 2019 [8] | USG | 13 | 0 | 0 | 28 |
| donia 2010 [9] | USG | 19 | 4 | 10 | 17 |
| Duan 2019 [10] | USG | 37 | 0 | 14 | 87 |
| Duan et al. 2019 [11] | USG | 43 | 9 | 8 | 78 |
| El-Guindi et al. 2014 [12] | USG | 19 | 4 | 11 | 26 |
| farrant 2001 [13] | USG | 34 | 4 | 3 | 117 |
| Hanquinet 2015 [14] | USG | 7 | 1 | 3 | 9 |
| Humphrey and Stringer 2007 [15] | USG | 22 | 0 | 8 | 60 |
| Imanieh et al. 2010 [16] | USG | 7 | 2 | 3 | 46 |
| Jiang et al. 2013 [17] | USG | 21 | 2 | 2 | 26 |
| kanegawa 2003 [18] | USG | 25 | 7 | 4 | 19 |
| Kim et al. 2007 [19] | USG | 32 | 2 | 6 | 45 |
| Kim et al. 2000 [20] | USG | 12 | 0 | 0 | 9 |
| Kotb et al. 2001 [1] | USG | 25 | 0 | 0 | 40 |
| Lee et al. 2000 [21] | USG | 40 | 38 | 9 | 65 |
| Lee et al. 2003 [22] | USG | 16 | 1 | 4 | 65 |
| Lee et al. 2009 [23] | USG | 18 | 0 | 11 | 35 |
| Lee et al. 2015 [24] | USG | 36 | 0 | 10 | 54 |
| Liu et al. 20 21 [25] | USG | 24 | 10 | 2 | 23 |
| Liu et al. 20 2 2 [26] | USG | 68 | 22 | 15 | 51 |
| mittal 2011 [27] | USG | 25 | 12 | 5 | 57 |
| Park et al.1997 [28] | USG | 20 | 3 | 0 | 40 |
| Rouzrokh et al. 2009 [29] | USG | 13 | 2 | 5 | 22 |
| Ryeom et al. 2005 [30] | USG | 3 | 2 | 1 | 17 |
| Sandberg 2021 [2] | USG | 170 | 38 | 42 | 68 |
| Shen et al. 2020 [31] | USG | 99 | 44 | 36 | 103 |
| Shima 2012 [32] | USG | 7 | 1 | 3 | 9 |
| sun 2011 [33] | USG | 54 | 5 | 97 | 26 |
| Takamizawa et al. 2007 [34] | USG | 46 | 6 | 2 | 31 |
| Tan Kendrick et al. 2003 [35] | USG | 26 | 0 | 5 | 186 |
| visrutaratna 2003 [36] | USG | 22 | 7 | 1 | 16 |
| Wang et al. 2016 [37] | USG | 37 | 0 | 1 | 17 |
| Wang 2016 [37] | USG | 37 | 1 | 0 | 31 |
| Wongsawasdi et al. 2008 [4] | USG | 27 | 2 | 4 | 28 |
| Wu et al. 2018 [5] | USG | 12 | 1 | 3 | 32 |
| Wu 2018 [38] | USG | 15 | 0 | 0 | 33 |
| Zhou et al. 2015 [39] | USG | 119 | 9 | 10 | 135 |
| Zhou 2017 [3] | USG | 109 | 12 | 11 | 40 |
Table 2.
Bias study.
| Author and Year | Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | |
|---|---|---|---|---|---|---|---|---|
| Aziz 2011 | low | low | unclear | low | low | low | low | |
| Boo et al. 20 21 | unclear | high | low | low | low | low | low | |
| Dillman 2019 | low | low | high | low | high | low | low | |
| donia 2010 | low | low | low | low | unclear | low | unclear | |
| Duan 2019 | low | high | high | unclear | low | unclear | low | |
| Duan et al. 2019 | low | unclear | low | low | low | low | low | |
| El-Guindi et al. 2014 | unclear | low | unclear | low | high | low | low | |
| farrant 2001 | low | low | high | low | low | low | low | |
| Hanquinet 2015 | low | low | unclear | low | low | unclear | low | |
| Humphrey and Stringer 2007 | low | unclear | low | unclear | low | low | low | |
| Imanieh et al. 2010 | low | low | high | low | low | low | low | |
| Jiang et al. 2013 | low | low | low | low | low | low | high | |
| kanegawa 2003 | low | high | low | low | low | high | low | |
| Kim et al. 2007 | low | high | low | unclear | low | low | low | |
| Kim et al. 2000 | unclear | low | low | low | high | low | high | |
| Kotb et al. 2001 | low | unclear | low | low | low | low | low | |
| Lee et al. 2000 | high | low | low | low | high | low | low | |
| Lee et al. 2003 | low | unclear | low | high | low | high | low | |
| Lee et al. 2009 | low | low | low | low | unclear | low | unclear | |
| Lee et al. 2015 | low | high | low | low | low | low | low | |
| Liu et al. 20 21 | low | low | unclear | low | low | high | low | |
| Liu et al. 20 2 2 | high | low | low | low | low | low | low | |
| mittal 2011 | low | unclear | low | high | low | low | unclear | |
| Park et al.1997 | low | low | unclear | low | high | low | low | |
| Rouzrokh et al. 2009 | low | low | high | low | low | low | low | |
| Ryeom et al. 2005 | low | low | low | low | low | low | low | |
| Sandberg 20 21 | unclear | high | low | low | low | unclear | low | |
| Shen et al. 20 20 | low | unclear | low | low | low | low | low | |
| Shima 201 2 | low | low | low | low | low | low | low | |
| sun 2011 | low | low | low | unclear | low | low | low | |
| Takamizawa et al. 2007 | low | low | unclear | low | low | high | low | |
| Tan Kendrick et al. 2003 | unclear | low | low | low | low | low | low | |
| visrutaratna 2003 | low | low | low | low | low | low | unclear | |
| Wang et al. 2016 | low | low | low | low | low | low | low | |
| Wang 2016 | low | high | low | high | low | low | unclear | |
| Wongsawasdi et al. 2008 | low | low | low | low | low | low | low | |
| Wu et al. 2018 | low | low | low | low | low | low | low | |
| Wu 2018 | low | low | high | low | low | low | low | |
| Zhou et al. 2015 | low | low | low | low | low | low | high | |
| Zhou 2017 | low | low | low | low | unclear | low | unclear |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



