
Submitted:
25 April 2024
Posted:
26 April 2024
You are already at the latest version
Abstract
Background: The accurate diagnosis of regional lymph node metastasis is critical for guiding treatment decisions in head and neck cancer patients. Despite advances in imaging techniques, detecting nodal metastasis remains challenging, leading to potential undertreatment or overtreatment. This systematic review aims to identify molecular markers associated with occult metastasis in Head and Neck Squamous Cell Carcinoma (HNSCC) patients. Methods: The present research was conducted following PRISMA guidelines. Prospero registration nr. CRD42024522985. Results: Through a comprehensive literature search and review process, 634 articles were considered, 103 of them were finally included. Conclusions: Several promising markers were identified, including miR-205, DSG3, pan-CK AE1/AE3, HPV-16, Activin-A, Cyclin D1, and NPL that demonstrated effectiveness across multiple studies. Future research should focus on exploring combination scoring systems to improve diagnostic precision and optimize treatment selection in HNSCC patients.
Keywords:
Head and neck squamous cell carcinoma
; Meastasis
; Lymp Node
; Regional Metastasis
; Cancer Marker
; Occult Metastasis
1. Introduction
Head and Neck Squamous Cell Carcinoma (HNSCC) has an annual incidence of 600,000 new cases globally. [1] Lymph node metastasis profoundly impacts patient outcomes, drastically reducing 5-year overall survival (OS) rates from 63-86% to 20-36%, making it the paramount prognostic indicator. [2,3,4,5] Regrettably, existing imaging techniques often fail to detect occult nodal metastasis smaller than 2 mm, complicating accurate diagnosis and treatment planning. [6,7]
Therapeutic approaches for HNSCC typically involve prophylactic neck dissection followed by radiotherapy with or without chemotherapy for clinically positive lymph nodes. [8,9] However, 15-20% of cases present with occult metastasis in clinically negative (cN0) lymph nodes, challenging treatment decisions. [10] Failure to detect such metastases may lead to suboptimal therapeutic strategies, potentially resulting in cancer recurrence and compromised patient outcomes. [11]
The National Comprehensive Cancer Network (NCCN) Guidelines underscore the importance of neck dissection for high-risk or clinically positive nodal metastasis. Moreover, histological confirmation of nodal metastasis warrants adjuvant therapy. [12] Detection of occult metastasis is pivotal, as it informs tailored treatment strategies, sparing patients unnecessary systemic chemotherapy while ensuring adequate management of distal metastases. [12]
Identifying occult metastasis remains a daunting task, with significant implications for treatment decisions and patient prognosis. This systematic review aims to comprehensively survey the literature to identify molecular markers associated with occult metastasis in HNSCC patients. By elucidating these markers, we aim to enhance diagnostic precision, optimize therapeutic selection, and ultimately improve patient outcomes in this challenging clinical scenario.
2. Materials and Methods
The systematic review adhered to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure methodological rigor and transparency. A comprehensive search of PubMed, Embase, Google Scholar, and Scopus databases was performed to identify relevant articles pertaining to occult metastasis markers in Head and Neck Squamous Cell Carcinoma (HNSCC). Only randomized and non-randomized clinical trials, encompassing both prospective and retrospective designs, were included in the review, with no restrictions on publication dates. The search was confined to English-language articles. In vitro and animal-based studies were excluded. Duplicate articles were initially identified and removed using the Mendeley platform, which also facilitated bibliographic management. Subsequently, the remaining articles underwent screening based on title and abstract by the authors collectively. Full-text analysis was conducted for selected manuscripts, with exclusion criteria applied to trials not involving human subjects or lacking assessment of secondary primary carcinomas among their outcomes. The selected articles were summarized within the manuscript and presented in Table 1. The article screening and selection process is depicted in a PRISMA flow chart (Figure 1), providing a visual representation of the review process. Furthermore, the literature analysis, including final review considerations, informed the discussion section of the manuscript. Critical issues pertaining to the identified markers were deliberated by the research team and synthesized within the article’s discussion. The PRISMA checklist was completed post-manuscript composition.
The review protocol was registered in the PROSPERO International prospective register of systematic reviews (CRD42024522985) to enhance transparency and facilitate reproducibility of the study methodology.
3. Results
Following extensive individual searches conducted by the first two authors (M.P.G. and P.S.), a total of 771 articles were initially retrieved (PubMed = 145 results; Embase = 482 results; Scopus = 72 results; Cochrane = 3; Google Scholar = 69 results). Employing Mendeley Software, an automated duplicate removal process validated by human check for each article identified and eliminated 137 duplicates, resulting in 634 unique manuscripts. Subsequently, a meticulous screening phase based on title and abstract led to the exclusion of 412 articles, leaving 222 for further evaluation. Comprehensive scrutiny of the entire manuscripts was undertaken, followed by group discussions to ensure consensus on inclusion criteria. Additionally, the bibliographies of selected articles were scrutinized to identify any missed manuscripts, leading to the inclusion of one additional article. Ultimately, 103 articles met the predefined criteria and were included in the review, with the remaining excluded for specific reasons detailed as follows: Not regarding HNSCC (n = 33); Occult carcinoma (n = 22); Article in Japanese (n = 2); Article in Chinese (n = 3); Article in German (n = 1); Article in Polish (n = 1); HNSCC not regarding marker of occult metastasis (n = 35); Abstract only (n = 1); Reviews (n = 16); Congress abstract with unavailable full text (n = 1); Case report (n = 1); Post neoadjuvant CT PET/CT (n = 1); Reply letter (n = 1). The entire selection process is summarized in a PRISMA flow-chart (Figure 1) for transparency and reproducibility. All the selected articles are summarised in Table 1.
3.1. Lymph Nodes Analysis
3.1.1. Micro-RNA in Lymph Nodes
Micro-RNAs (miRNA, miR) are non-coding RNA molecules that regulate gene expression by interacting with messenger RNA (mRNA). [13,14] Specific miRNAs play pivotal roles in orchestrating gene expression patterns in various tumors, including HNSCC. [15,16,17,18,19] For instance, Fletcher et al. observed tumor-specific expression of miR-205 in metastatic HNSCC lymph nodes, demonstrating significant differential expression compared to benign mucosal samples (p < 0.05). While miR-205 levels may not serve as a marker for cancer transformation in epithelial tissues, they show promise in detecting lymph node metastasis. In their study, miR-205 expression was significantly different in histologically metastatic lymph nodes compared to non-metastatic ones (p < 0.01), indicating its potential as a marker for micro-metastatic disease. Additionally, quantitative real-time polymerase chain reaction (qRT-PCR) analysis demonstrated acceptable sensitivity in identifying metastatic HNSCC within lymph nodes, suggesting the utility of miR-205 as a diagnostic marker. [20]
The pooled analysis of miRNA expression profiles in HNSCC lymph nodes revealed a spectrum of potential markers, encompassing miR-200a, miR-200c, miR-203, miR-205, miR-382, miR-628-5p, and miR-758. Notably, miR-628-5p, miR-758, and miR-382 exhibited limited sensitivity, detecting only 26.3%, 31.6%, and 52.6% of metastatic samples, respectively, underscoring their suboptimal diagnostic utility. Conversely, miR-200a, miR-200c, miR-203, and miR-205 demonstrated maximal specificity (100%) and high sensitivity levels (84.2%, 94.7%, 100%, and 100%, respectively), indicative of their potential as robust diagnostic markers. The expression profiles of these miRNAs were significantly associated with the presence of metastatic disease. However, miR-200a and miR-200c exhibited limited efficacy in detecting micrometastases, identifying only 40% and 80%, respectively, of such cases and failing to detect isolated tumor cells. In contrast, miR-203 and miR-205 displayed exceptional sensitivity, accurately classifying lymph nodes containing macrometastases, micrometastases, or isolated tumor cells with 100% sensitivity. The diagnostic accuracy of miR-200a was 84.2% (95% CI, 68.1–93.4%), with a positive predictive value of 100% and a negative predictive value of 68.4% (95% CI, 43.5–87.3%). Similarly, miR-200c exhibited an accuracy of 92.1%, with positive and negative predictive values of 100% and 81.2% (95% CI, 77.5–97.9%), respectively. For miR-203 and miR-205, both positive and negative predictive values, along with accuracy levels, were 100%, with an area under the curve (AUC) of 1.0. Given their high accuracy, miR-203 and miR-205 were further evaluated by comparing fine needle aspiration biopsies (FNAs) with cytological assessments, revealing complete concordance between molecular and cytological approaches. Notably, both markers exhibited 100% sensitivity, specificity, negative predictive value, and positive predictive value. Furthermore, the diagnostic accuracy of miR-203 and miR-205 in distinguishing positive and negative FNAs was remarkably high, with AUC values of 0.963 and 0.966, respectively, and accuracy levels of 97.3% (95% CI, 92.1–99.4%). Moreover, the negative predictive values were 95.9% (95% CI, 88.6–99.1%), and the positive predictive values were 100% (95% CI, 90.9–100%) for both miRNAs. These findings underscore the clinical potential of miR-203 and miR-205 as reliable diagnostic markers for HNSCC lymph node metastasis, offering enhanced accuracy and precision in patient management. [21]
miR-145 and MYO5A are implicated in the development and metastasis of laryngeal squamous cell carcinoma (LSCC). In a study involving 132 LSCC patients and 52 healthy individuals, the expression levels of miR-145 and MYO5A were examined. It was observed that miR-145 expression was significantly diminished in the LSCC group compared to the healthy mucosa group (4.05±2.82 vs. 10.00±2.44, p = .002). Conversely, the relative expression value of MYO5A in LSCC tissue was markedly elevated relative to healthy tissue (64.52±15.20 vs. 31.81±8.30, p = .007). Furthermore, the serum concentrations of MYO5A in the N+ and N0+ groups were notably higher than those in the N- group (294.2±62.0 pg/mL vs. 199.3±71.1 pg/mL, p = .003; 276.3±73.5 pg/mL vs. 199.3±71.1 pg/mL, p = 0.009), with no significant disparities between the N+ and N0+ groups. These findings underscore the potential of MYO5A as a presurgical biomarker, as its levels in both primary tumor tissue and serum exhibit significant elevation in conjunction with neck lymph node or occult metastasis. In conclusion, the altered expression patterns of miR-145 and MYO5A in LSCC tissues and serum suggest their involvement in the pathogenesis and metastatic progression of LSCC. The observed dysregulation of these molecules highlights their potential as biomarkers for prognostic and diagnostic purposes in LSCC, offering insights into the disease mechanisms and paving the way for the development of targeted therapeutic strategies. [22]
3.1.2. REEP1, RNF145, CTONG2002744, MYO5A, and FBXO32
In the investigation of oral squamous cell carcinoma (OSCC), the disparity in gene expression profiles between metastatic and non-metastatic lymph nodes was scrutinized, with 73 positive and 40 negative nodes compared. Utilizing multivariate linear regression analysis, researchers pinpointed several genes—REEP1, RNF145, CTONG2002744, MYO5A, and FBXO32—that exhibited differential expression between node-positive and node-negative OSCCs. Subsequently, employing stepwise logistic regression, a predictive model based on four of these genes—MYO5A, RNF145, FBXO32, and CTONG2002744—was identified. Comparison of this gene-based predictive model with tumor size—a conventional predictor of locoregional metastasis—revealed a significantly superior AUC at the Receiver Operating Characteristic (ROC) curve (AUC= 0.85 vs. 0.61, respectively; p < .011). Interestingly, the incorporation of tumor size into the gene-based model did not enhance its predictive value. Notably, this investigation was conducted using the Affymetrix Platform, with quantitative PCR (qPCR) subsequently employed on a separate set of 31 metastatic vs. 13 non-metastatic lymph nodes. Observations from qPCR analysis indicated a correlation between CTONG2002744 and FBX032 only. However, it’s noteworthy that statistical power analysis revealed sufficient power (at alpha = 0.05) for CTONG2002744 exclusively. These findings underscore the potential significance of CTONG2002744 as a key gene associated with metastatic processes in OSCC. Further validation studies are warranted to consolidate and expand upon these preliminary findings, shedding more light on the role of CTONG2002744 and other implicated genes in the metastatic cascade of OSCC. [23]
3.1.3. CK14, eIF4E, and DSG3
qPCR was employed to assess the expression levels of CK14, eIF4E, and DSG3 in 44 patients with oral tongue squamous cell carcinoma (SCC). Subsequently, these results were compared with histological and immunohistochemical analyses. The sensitivity of each marker as a diagnostic tool for lymph node cancer involvement varied: CK14: 0.6, eIF4E: 0.92, and DSG3: 0.88. Regarding specificity, CK14 exhibited a specificity of 0.9, eIF4E had a specificity of 0.74, and DSG3 showed a specificity of 0.8. Interestingly, combining more than one marker led to an increase in diagnostic capacity. Specifically, the combination of CK14 and DSG3 demonstrated a sensitivity of 0.88 and a specificity of 0.85. Furthermore, a comprehensive evaluation incorporating all markers achieved the highest sensitivity possible (sensitivity = 1). Notably, immunohistochemical investigation of DSG3 alone surpassed cytokeratin in terms of sensitivity (0.9 vs. 0.7, respectively). In conclusion, the authors advocated for the use of multiple markers to facilitate an accurate diagnosis of occult metastasis in patients with HNSCC. Such a comprehensive approach enhances the sensitivity and specificity of intraoperative staging of the pN0 neck, thereby potentially improving clinical outcomes and patient management strategies. [5]
James et al. utilized a microfluidics-based molecular assay system for the intraoperative detection of nodal metastasis, selecting markers based on meta-analysis. They developed both polyclonal and monoclonal antibodies, establishing a lateral flow assay system to screen lymph nodes from patient samples—both positive and negative for metastasis—to determine sensitivity and specificity. In their preliminary study focusing on DSG3, five monoclonal and one polyclonal antibodies were developed and validated in positive (17) and negative (7) lymph nodes. The marker demonstrated a sensitivity above 80% and specificity above 71%. Subsequently, a sandwich ELISA indicated the optimal combination of antibodies, and the Lateral Flow test (LFT) assays developed with this combination for DSG-3 exhibited a sensitivity of 72.5% and specificity of 55.6% in detecting positive lymph node samples (11 positive & 9 negative lymph nodes). Moving forward, DSG3, along with the newly identified markers, will undergo validation in larger patient cohorts, with the aim of selecting the best combination of markers for developing the diagnostic assay. The authors concluded that incorporating multiple markers on a proficient platform like microfluidics holds the potential to enhance the clinical utility of the assay system, offering improved accuracy and reliability in the intraoperative detection of nodal metastasis. [24]
3.1.4. The Loss of Heterozygosity at D9S 171 (9p21)
The loss of heterozygosity at D9S 171 microsatellite locus on the 9th chromosome (9p21) was studied as a potential marker for lymph node micro metastasis. The authors used 20 supraglottic cancer samples and 182 lymph nodes and examined loss of heterozygosity at D9S 171 with the outcomes of immunohistochemistry for CK19 and histology. They observed significantly different outcomes between those three techniques (34.4%, 23.6%, and 16.5%, respectively) with 45% of the population had micro metastasis. [25]
3.1.4. Squamos Cell Carcinoma Antigen and Cytokeratins
In 2004, Onishi et al. conducted a study aimed at identifying occult metastasis in cervical lymph nodes of patients with oral cancer utilizing polymerase chain reaction (PCR). Their investigation focused on assessing the expression of squamous cell carcinoma antigen (SCCA) and cytokeratin 13 (CK13) as potential markers. While CK13 was initially considered as a candidate marker for occult metastasis detection, its expression was found in control lymph nodes, rendering it unsuitable for this purpose. Conversely, SCCA demonstrated promising results, with expression observed in 4 out of 30 control lymph nodes and significantly elevated levels detected in metastatic lymph nodes. Based on their findings, the authors concluded that SCCA mRNA expression, detected through real-time quantitative PCR, holds clinical utility for the detection of occult tumor cells in cervical lymph nodes. This underscores the potential of molecular techniques, such as PCR, in improving the accuracy and sensitivity of lymph node metastasis detection in oral cancer patients, thereby informing treatment decisions and enhancing patient outcomes. [26]
Cytokeratin 14 (CK14) expression was investigated using real-time (RT) PCR in 153 cervical lymph nodes obtained from 13 patients with HNSCC. These lymph nodes were also subjected to semi-step sectioning and immunohistochemistry for CK14 analysis. A cutoff value of 50 molecules of CK14-RNA per nanogram was utilized for the RT-PCR analysis. The results indicated that CK14-RNA was detected in a total of 33 nodes, 14 of which were found to have nodal metastasis upon pathological examination. Interestingly, among these, 2 metastatic nodes with occult metastasis tested positive for CK14-RNA, and an additional 2 nodes without micro-metastasis exhibited CK-14 levels above the predetermined cutoff value. In conclusion, the authors noted that RT-PCR for CK-14 RNA in lymph nodes demonstrated sensitivity in detecting micro-metastasis. However, they also observed a relatively high false-positive rate associated with this method. These findings underscore the need for cautious interpretation of RT-PCR results for CK14-RNA in lymph node evaluation, emphasizing the importance of corroborating findings with other diagnostic modalities to minimize the risk of misdiagnosis and ensure accurate clinical management of HNSCC patients. [27]
Cytokeratin 19 (CK19) has been found to be an inadequate marker for occult lymph node metastasis in oral squamous cell carcinoma (OSCC), as well as lacking specificity for SCC. This conclusion was drawn based on observations that glandular tissue adjacent to the analyzed lymph nodes exhibited positive expression of CK19. In a study involving tissue microarrays from 212 patients, the authors investigated the correlation between CK19 expression in tumors and lymph nodes. They found that in 65 cases, there was a correlation between tumor and lymph node CK19 expression, albeit this correlation was deemed only “fair” (kappa 0.391; p = .001). Notably, for early-stage OSCC, this correlation was not statistically significant (kappa 0.422; p = .064). Furthermore, CK19 was also evaluated through CK19 mRNA expression in cervical lymph nodes. Amplification of CK19 mRNA, as demonstrated by RT-PCR, was associated with the presence of carcinoma cells in lymph nodes, with significantly higher values observed in metastatic nodes (p < .0001). This approach exhibited higher sensitivity for nodal involvement compared to histology alone (16.3% vs. 36%; p < .0001). In summary, CK19 has limitations as a marker for occult lymph node metastasis in OSCC, with its expression not being specific to SCC. However, CK19 mRNA expression analysis via RT-PCR shows promise as a more sensitive method for detecting nodal involvement, highlighting the importance of employing advanced molecular techniques in clinical practice for improved diagnostic accuracy and patient management. [28]
Pan-cytokeratin (pan-CK) (AE1/AE3) was evaluated in 133 lymph nodes obtained from 10 patients diagnosed with OSCC. In addition to pan-CK analysis, these lymph nodes underwent serial sectioning at 100 μm intervals to detect micro-metastases or single cancer cells. The analysis resulted in the upstaging of 3 out of 10 patients (3.33%), with cancer positivity detected in 2.25% of the examined lymph nodes. [29]
Similarly, Barrera et al. utilized pan-CK AE1/AE3 in a study involving 1012 lymph nodes from 50 patients with HNSCC. They compared the efficacy of metastasis detection using serial sectioning at 5-to 6-μm interval specimens. Notably, unexpected micro-metastases were identified through pan-CK AE1/AE3 immunohistochemistry, leading to an upstaging in 29% of N0 patients and 45% of N1 patients. The authors observed that in 8 cases where serial sectioning analysis yielded negative results, immunohistochemical analysis with pan-CK AE1/AE3 revealed positive findings, while the opposite occurred in 3 cases. Consequently, they concluded that the combined utilization of serial sectioning and immunohistochemistry employing pan-CK AE1/AE3 could enhance the detection of micro-metastases. This approach holds promise for improving the accuracy of nodal staging in patients with HNSCC, potentially leading to more tailored and effective treatment strategies. [30]
In a study involving 26 cases of laryngeal and hypopharyngeal carcinoma, classic hematoxylin and eosin (H&E) histology and cytokeratin immunostaining were employed for analysis. Interestingly, the cytokeratin immunostaining revealed micro-metastases in 5 out of the 26 cases, representing 19.2% of the specimens that tested negative via conventional histology (p = .001). This finding underscores the enhanced sensitivity of cytokeratin immunostaining in detecting micro-metastases, thereby highlighting its potential utility as a complementary diagnostic tool alongside traditional histological examination. The ability to identify these occult metastases can have significant implications for patient prognosis and treatment planning, emphasizing the importance of incorporating advanced immunostaining techniques into routine pathological assessment protocols for improved clinical outcomes. [31]
CK19 mRNA was investigated utilizing a one-step nucleic acid amplification method to identify occult metastasis from OSCC, achieving an impressive accuracy of 95%. Oka et al. conducted an analysis of gene expression profiles from metastatic lymph nodes, identifying 36 genes, including annexin A8-like 2 (ANXA8L2) and desmoglein 3 (DSG3), which were consistently detected at significantly higher levels in metastatic lymph nodes compared to benign lymph nodes. Subsequently, a retrospective analysis of 330 lymph nodes was performed, with 62 of them testing positive for metastatic involvement. The individual accuracy of each marker—CK19, ANXA8L2, and DSG3—was approximately 90%. Remarkably, the combination of these markers substantially improved sensitivity to 96-100%. Furthermore, the expression of ANXA8L2 and DSG3 was detected in approximately 3% of histopathologically metastasis-negative lymph nodes. These findings suggest that ANXA8L2 and DSG3 hold promise as molecular markers for enhancing the detection rate of occult metastasis in OSCC. By utilizing a combination of these markers, clinicians may achieve higher sensitivity in identifying metastatic involvement, thereby facilitating more accurate staging and treatment planning for patients with OSCC. [32]
Three immunohistochemistry assays utilizing antibodies against CK5/14, a broad spectrum of cytokeratins (CK 1–8, 10, 14–16, and 19), and CD44v6 were employed for investigating regional lymph node metastasis. Among 50 cN0 subjects with head and neck squamous cell carcinoma (HNSCC), the authors detected 7 micrometastases in 5 patients and 31 disseminated tumor cells in 12 patients. Sentinel lymph node biopsy is recommended by NCCN guidelines for HNSCC. Similarly, in breast cancer, the one-step nucleic acid amplification (OSNA) method has demonstrated enhanced reliability. In a study involving 26 cN0 HNSCC patients, 157 lymph nodes were analyzed using immunohistochemistry for CK19, RT-qPCR for CK19 (the target of OSNA assay), and two additional markers, EPCAM and PVA. OSNA provided intraoperative results for all patients, detecting 21 metastases. Of the 157 lymph nodes, 139 were concordant (88.5%). There were 18 initially discordant lymph nodes (11.5%), with 13 (8.3%) being OSNA positive but pathologically negative, and 5 (3.2%) being OSNA negative but pathologically positive. After the elimination of allocation bias, the false-negative rate was reduced to 1.3%, with a sensitivity and specificity of 90% and 95.6%, respectively. The positive predictive value and negative predictive value were calculated at 75% and 98.5%, respectively. These findings underscore the potential utility of OSNA as an effective intraoperative diagnostic tool for assessing lymph node metastasis in HNSCC patients, providing valuable insights for treatment decision-making and patient management. [33]
Rhee et al. utilized a monoclonal antibody cocktail AE1/AE3 for cytokeratin in their investigation of occult nodal metastasis. Their study uncovered 5 micrometastases among 10 patients that were not detected by standard analysis methods. This underscores the potential of utilizing monoclonal antibody cocktails for enhancing the sensitivity of nodal metastasis detection, providing valuable insights into the presence of micrometastases that may otherwise go undetected using conventional approaches. [34]
3.1.5. Tumour Budding Score
In a study involving 97 patients with cT2N0 tongue SCC, researchers investigated the potential of tumour budding score and the AE1/AE3 cocktail as predictors of occult nodal metastasis. Their findings confirmed the significance of both markers in predicting the occurrence of occult neck metastasis. Specifically, a tumor budding score of ≥4 emerged as a significant independent predictive factor for occult neck metastasis. This underscores the importance of incorporating tumor budding assessment into clinical evaluations for identifying patients at higher risk of nodal metastasis, thereby facilitating more informed treatment decisions and improved patient outcomes. [35,36]
3.1.6. Desmoglein 3
In the investigation of antibodies to Desmoglein-3 (DSG3) within lymph nodes using the Lateral Flow Test assay system, researchers observed a sensitivity of 72.5% and specificity of 55.6% in the detection of nodal metastasis. These findings suggest that while the assay system demonstrates moderate sensitivity in identifying nodal metastasis, its specificity is relatively lower. This underscores the need for further refinement or complementary approaches to improve the accuracy of nodal metastasis detection, ensuring more reliable clinical assessments and treatment decisions for patients. [7] DSG3 immunohistochemical analysis was also conducted by Nagvekar et al. in a study involving 47 lymph nodes from 10 patients with OSCC. The researchers identified positivity for DSG3 in 6 nodes upon histological examination with 3 µm sections. However, the identification of additional micrometastatic deposits was challenging due to the presence of a considerable number of activated macrophages exhibiting DSG3 immunoreactivity. These DSG3-positive macrophages were distributed throughout various regions, including the subcapsular sinuses, interfollicular areas, medullary sinuses, and lymphoid follicles. Importantly, further characterization revealed that these DSG3-positive cells expressed CD68, confirming their macrophage phenotype. Based on these observations, the authors concluded that while DSG3 is indeed overexpressed, its utility as a marker for detecting micrometastasis is limited due to the confounding presence of DSG3-positive macrophages. This highlights the complexity of interpreting DSG3 immunoreactivity in lymph nodes and underscores the importance of considering potential cellular heterogeneity and non-neoplastic expression patterns when assessing its diagnostic significance in OSCC metastasis detection. [37]
Patel et al. introduced a ground-breaking nanostructured immunoarray system tailored for the ultrasensitive detection of DSG3 in lymph node tissue lysates. Through their research, they made a significant observation: DSG3 exhibits high expression levels in all head and HNSCC lesions and their corresponding metastatic cervical lymph nodes, while being conspicuously absent in non-invaded lymph nodes. This finding underscores the potential of DSG3 as a discriminatory biomarker for metastatic disease in HNSCC. Utilizing a straightforward microfluidic immunoarray platform, Patel et al. demonstrated the rapid and remarkably sensitive detection of DSG3. Their innovative approach enabled the detection of DSG3 even in human tissue sections containing minimal HNSCC-invading cells, thus enabling the clear differentiation between positive and negative lymph nodes. This advancement represents a significant leap forward in the field of HNSCC diagnosis, offering a promising avenue for the early and accurate detection of metastatic disease using DSG3 as a key molecular indicator. [38]
3.1.7. HPV-DNA in Lymph Nodes
In a study investigating HPV-16 positivity in cervical lymph node metastases of HPV16+ oropharyngeal SCC, researchers conducted RT-PCR analysis on cervical lymph nodes from 11 patients with oropharyngeal SCC and 3 controls with HPV-negative oropharyngeal SCC. The results revealed a significantly higher viral load in metastatic lymph nodes compared to tumor-free nodes in the experimental group (p < .01). Among the tumor-free lymph node samples, 16 had undetectable viral load values, 8 showed low or medium levels (<105 copies per million cells), and 3 exhibited high levels (>105 copies per million cells). This finding led the researchers to conclude that the detection of HPV-16 DNA in lymph nodes of patients with HPV-16(+) oropharyngeal cancer is indicative of metastatic involvement. Moreover, they suggested that tumor-free lymph nodes with a high viral load value may signify the presence of occult lymph node metastasis, thereby proposing HPV-16 DNA as a potential marker for metastasis in these cases.[39]
In a study by Mirghani et al., RT-PCR for HPV16 identification was evaluated as a potential marker of occult metastasis. The study included 11 patients with HPV16+ oropharyngeal SCC and 3 patients with HPV16- OSCC. Notably, HPV16 was not identified in the HPV16- patients, while metastatic lymph nodes from HPV16 oropharyngeal SCC exhibited a high viral load. Among 27 pathologically tumor-free lymph node (PTFLN) samples, 16 had no detectable viral load, while the viral load was low or medium (<105 copies/million cells) in 8 samples and high (>105 copies/million cells) in 3 samples. Interestingly, in the latter group where high viral load was detected in PTFLN, no metastatic cells were identified, and the viral DNA was found to be located in immune cells. Based on these findings, the authors concluded that HPV16 detection in lymph nodes can be attributed to its presence within either metastatic cells or immune cells. Furthermore, they suggested that HPV16 detection in PTFLN may not necessarily correlate with occult lymph node metastases. [40]
3.1.8. Tumor Infiltrating Lymphocytes and Immunohistochemistry
In a study involving 14 patients treated with transoral robotic surgery and neck dissection for HPV+ oropharyngeal SCC, tumor infiltrating lymphocytes (TILs) were investigated. Immunohistochemistry targeting CD3, CD8, FOXP3, PD-L1, and CTLA-4 was conducted. The analysis revealed that occult primary tumors exhibited a higher percentage of CD3+ and CD8+ TILs compared to tumor in lymph nodes. Specifically, the percentage of CD3+ T cells was 61% in occult primary tumors versus 42% in nodal tumors (p = 0.006), and the percentage of CD8+ T cells was 36% versus 23%, respectively (p = 0.01). Additionally, there was a higher concentration of FOXP3+ TILs in primary tumors compared to nodal tumors, with percentages of 8% and 5%, respectively (p = 0.01). Although not statistically significant, there was a trend towards a higher percentage of CTLA-4+ cells in primary tumors compared to nodal tumors (52% versus 34%, p = 0.09). Based on these findings, the authors concluded that occult primary HPV+ oropharyngeal SCC tumors tend to have a higher concentration of CD3+ and CD8+ TILs compared to their associated regional lymph node metastases. This observation may potentially contribute to the clinical presentation observed in these patients. [41]
3.1.9. Histological Techniques for Sentinel Lymph Node Analysis
In stage I (T1-2cN0) tongue cancer patients, sentinel lymph nodes were pathologically evaluated using various analysis techniques, including frozen section, imprint cytology, hematoxylin-eosin staining, serial step sectioning (SSS) with hematoxylin-eosin, and immunohistochemistry (IHC). Metastases were classified based on size: macrometastasis (>2.0 mm), micrometastasis (0.2 mm-2.0 mm), and isolated tumor cells (<0.2 mm). Out of 80 patients, occult metastasis was detected in 20. Frozen section and imprint cytology identified metastasis in 10 patients, while hematoxylin-eosin stain detected it in 13 patients. SSS further upstaged the disease in 7 additional patients (9%). While frozen section successfully detected macrometastasis in 7 out of 8 cases, it missed micrometastasis in 4 out of 7 cases and isolated tumor cells in all 5 cases. SSS was particularly effective, upstaging the disease by 10%, with a sensitivity and negative predictive value of 90% and 97%, respectively, when combined with hematoxylin-eosin stain. The authors concluded that frozen section and imprint cytology are inadequate for identifying occult metastasis, while IHC and SSS are necessary to detect micrometastasis and isolated tumor cells. [42]
3.1.10. Single Fiber Reflectance Spectroscopy
In a cohort of nine patients, intraoperative single-fiber reflectance (SFR) spectroscopy was conducted to assess its predictive capability for nodal metastasis. The study revealed three parameters—blood volume fraction (BVF), microvascular saturation (StO(2)), and Rayleigh amplitude—that were significantly lower in positive lymph nodes. These parameters were consolidated into a single score termed “delta” using discriminant analysis. The “delta” score exhibited a substantial decrease in positive lymph nodes, with remarkable sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) (p = .0006, 90.0%, 88.9%, 90.0%, and 88.9%, respectively). Moreover, the area under the ROC curve was an impressive 96.7% (95% confidence interval 89.7-100.0%). [43]
3.1.11. PET/MRI
cN0 HNSCC cases are typically identified following clinical and radiological assessments. The combination of positron emission tomography and magnetic resonance imaging (PET/MRI) has shown superior performance compared to PET or MRI alone. Specifically, PET/MRI demonstrated higher sensitivity, specificity, negative predictive value, positive predictive value, and accuracy when compared to PET or MRI alone. These values were as follows: 83.3%, 92.1%, 97.2%, 62.5%, and 90.9% for PET/MRI, 50%, 89.5%, 91.8%, 42.8%, and 84% for PET alone, and 83.3%, 68.4%, 96.2%, 29.4%, and 70.4% for MRI alone, respectively. [44]
3.1.12. PET/CT
The sensitivity of PET-CT in detecting nodal disease in recurrent laryngeal cancer was found to be 16.7% (95% CI, 3.5% to 46.0%), with a specificity of 97.1% (95% CI, 83.8% to 99.9%). The PPV was calculated at 66.7% (95% CI, 20.2% to 94.4%), while the NPV stood at 76.7% (95% CI, 62.1% to 87.0%). These findings suggest that PET-CT exhibits poor sensitivity and NPV, indicating its limitations as a predictor of nodal disease in recurrent laryngeal cancer. [45]
3.2. Tumour Tissue Analysis
3.2.1. Activin A and Carcinoma-Associated Fibroblasts
In oral tongue SCC, researchers have investigated the expression of Activin A and its association with carcinoma-associated fibroblasts (CAF). Activin A, a member of the transforming growth factor beta family, is produced by CAF and has been implicated in various aspects of cancer progression. Studies have shown that Activin A enhances cell proliferation and increases xenograft tumor volume in oral tongue SCC. Furthermore, it has been found to promote cancer cell migration, invasion, and epithelial-mesenchymal transition, thereby potentially contributing to the aggressive nature of the disease. Its high expression was significantly associated regional recurrence, regional metastasis and occult lymph node metastasis (p = .01, p = 0.034 and p = .006, respectively). [46] Additionally, multivariate analysis has revealed that activin A overexpression serves as an independent marker for overall survival in early-stage oral tongue SCC. When comparing populations with Activin A overexpression to those with low levels, the 5-year overall survival rates were 76.5% versus 89.7%, respectively (HR: 2.44, 95% CI: 1.55-3.85, p = 0.012). [47,48]
3.2.2. Cyclins
3.2.2.1. Cyclin D1
Cyclin D1 expression has been found to correlate with occult nodal metastasis in a cohort of 158 patients with early-stage tongue or floor of mouth cancers clinically negative for neck lymph node metastasis. Specifically, Cyclin D1 amplification and immunohistochemical positivity were significantly correlated with occult nodal metastasis in early floor of mouth SCC (p = .020). [6]
The predictive value of Cyclin D1 as a marker of occult lymph node metastasis has been consistently confirmed in various studies, including the trial conducted by Capaccio et al. In their study, which involved 96 cN0 HNSCC patients, 32 of whom were found to have pN+ status while 64 were pN0, Cyclin D1 expression was observed in 42 patients (43.7%) via immunofluorescence. Univariate regression analysis demonstrated a significant correlation between Cyclin D1 expression and occult lymph node metastasis (p = .007). This correlation remained significant in the multivariate regression analysis, where Cyclin D1 emerged as an independent predictor of occult metastasis (p = .0059). [49]
Numerical aberrations of the Cyclin D1 gene were found to be associated with occult lymph node metastasis in a study involving 45 patients with OSCC. These patients underwent primary tumor surgical excision without neck dissection. Fluorescence in situ hybridization (FISH) was utilized to detect numerical aberrations in the Cyclin D1 gene from fine-needle aspiration biopsies of cN0 patients. Among the cohort, 15 patients exhibited CCND1 aberrations, accounting for 33.3% of the sample. Remarkably, 12 out of these 15 patients (80%) developed cervical lymph node metastases within 2 years. Multivariate analysis underscored that the numerical aberration of the CCND1 gene independently predicted late cervical lymph node metastasis (RR = 8.685%, 95% CI = 2.232-33.802, p = .002). [50]
In a study involving 75 cases of laryngeal SCC, Cyclin D1 and E-Cadherin were assessed via immunohistochemistry to predict various outcomes, including lymph node metastasis. Cyclin D1 emerged as a significant independent prognostic factor for lymph node metastasis (p = 0.000). Consequently, the researchers concluded that Cyclin D1 could serve as an independent prognostic marker for lymph node metastasis in patients with laryngeal SCC. Furthermore, they suggested that Cyclin D1 expression could aid in identifying patients with clinically negative lymph nodes who may still harbour a considerable risk for occult metastasis. [51]
3.2.2.2. Cyclin L1
Cyclin L1 amplification has been associated with higher stage in HNSCC. Through logistic regression analysis based on tissue microarray analysis using fluorescence in situ hybridization in 280 cases of HNSCC, a correlation between CCNL1 gain and lymph node metastasis was observed, independent of stage or subsite (p = .049). Additionally, this amplification was linked to shorter overall survival, as evidenced by the log-rank test (p = .006). These findings underscore the potential prognostic significance of Cyclin L1 amplification in HNSCC, particularly regarding lymph node involvement and overall survival. [52]
3.2.2.3. Cyclin B
Cyclin B1 expression in the cytoplasm of tumor cells has been associated with occult cervical lymph node metastasis in a case series involving 40 patients with oral tongue SCC. Moreover, the levels of Cyclin B1 were found to be positively correlated with Ki67 levels in cancer cells. This suggests that Cyclin B1 expression may serve as a potential marker for predicting occult lymph node metastasis in oral tongue SCC patients, highlighting its potential role in assessing tumor aggressiveness and metastatic potential. [53]
3.2.3. β-catenin
The expression of β-catenin in OSCC has been found to be significantly associated with nodal stage (p = 0.02), suggesting its potential role as a marker for identifying occult metastases in patients with OSCC. This finding underscores the importance of β-catenin as a potential biomarker for assessing the metastatic potential and disease progression in OSCC. Further research is needed to validate its utility in clinical practice for identifying occult lymph node metastases in OSCC patients. [54]
3.2.4. Histopathological Characteristics
The proliferative activity of cancer, measured through immunohistochemical assessment of PCNA and Ki67, as well as mitotic counting in laryngeal SCC, was investigated as a potential predictive factor for occult nodal metastasis. However, the researchers found that proliferative markers were not reliable indicators for diagnosing occult neck metastasis. This suggests that other factors or markers may need to be explored for more accurate prediction of occult nodal metastasis in laryngeal SCC. Further research is warranted to identify novel biomarkers or predictive factors that can improve the detection of occult metastasis in this context. [55]
PCNA and p53 were investigated as potential markers of occult metastasis in a population of 37 patients with oral tongue SCC. However, the study found that neither PCNA nor p53 had predictive value for detecting occult metastasis. This underscores the need for further research to identify more reliable markers or predictive factors for occult metastasis in oral tongue SCC. [56]
3.2.5. Genetic Amplifications
Genetic amplification of the 11q13 region, including genes such as CCND1, FGF4, FADD, and CTTN, as well as loss of CSMD1, showed significant correlation with lymph node metastasis in a cohort of 355 patients with oropharyngeal SCC and OSCC. When analyzing a clinically relevant subgroup, 11q13 amplification was the only factor that retained the ability to detect occult metastasis (p = .002), with a negative predictive value of 81%. This suggests that 11q13 amplification may serve as a useful marker for identifying occult lymph node metastasis in patients with oropharyngeal SCC and OSCC. [57]
Thangaraj et al. investigated a cohort of 100 patients with oral tongue SCC using RT-PCR and found that the upregulation of Tanancin C and Podoplanin genes was associated with occult lymph nodal metastasis (p = .049, F = 6.76; p = .049, F = .5). [58]
3.2.6. DNA Methylation
Clausen et al. explored the potential application of DNA methylation analysis of cancer cells as a predictor of nodal metastasis. They compared methylation levels from 6 cases of OSCC with nodal metastasis (N+) and 6 cases without nodal metastasis (N0) using MethlCap-Seq. Subsequently, they sequenced the isolated methylated DNA fragments using Illumina GA II and computationally mapped them back to the genome. Their next step involves validating the most promising methylation markers identified in this study in a larger cohort of 463 cases, pending completion of follow-up data collection. [59]
3.2.7. Ecotropic Viral Integration Site 1
EVI1 (Ecotropic Viral Integration Site 1) expression has emerged as a prognostic marker in various solid cancers and leukaemia. In HNSCC, EVI1 expression has been associated with poor survival and the presence of lymph node metastatic disease. A study conducted on a cohort of 389 HNSCC patients, of whom 57.2% had locoregional metastasis, revealed a correlation between EVI1 expression and these adverse outcomes. As a result, there is a hypothesis suggesting the potential utility of EVI1 as a marker for occult lymph node metastasis in patients clinically negative for lymph node involvement (cN0) with HNSCC. [60]
3.2.8. CC-Chemokine Receptor 7
The expression of CC-chemokine receptor 7 (CCR7) and its ligand, CCL21, plays a crucial role in tumor cell chemotaxis, particularly in the context of lymph node metastasis. In OSCC, the expression of CCR7 has been investigated in relation to cervical lymph node metastasis. Analyzing paraffin-embedded samples from previous patients using hematoxylin and eosin staining and anti-cytokeratin AE1/AE3 antibodies, researchers found that CCR7 expression in tumors was not significantly associated with cervical metastasis (p = .058). However, they concluded that lymph node sectioning combined with pan-CK AE1/AE3 staining remains an important complementary tool in detecting lymph node metastasis. Despite the lack of a significant correlation, the authors stated that the higher immunoexpression of the chemokine CCR7 in tumors of patients with cervical metastasis suggests its potential role as a prognostic biomarker, which warrants further investigation. [61]
3.2.9. Connexins, Pannexin 1 and Vimentin
In a study involving 32 patients with SCC, Connexins (Cx) 37, Cx40, Cx45, Pannexin 1 (Panx1), and Vimentin expression in cancer tissue were investigated using immunofluorescence. The findings revealed significant associations between certain markers and neck metastatic status. Specifically, the median Immunoreactive Score (IRS) of Panx-1 was notably higher in patients with a negative neck status compared to those with metastatic neck disease, with values of 4.5 and 2, respectively (p = .045). Additionally, Vimentin expression was observed to be higher in patients with a positive neck status, with a median of 7.65 compared to 3.83 in those with negative neck status (p = .048). Moreover, according to the logistic regression model, Panx-1 emerged as an independent prognostic factor for regional metastatic disease in LSCC (p = .049, 95% CI: .563–.980, OR: .76; regression coefficient −.271). Other identified risk factors for positive neck disease included higher histological grade, higher T stage, and positive lymphovascular invasion, all of which were statistically significant (all p < .05). [62]
3.2.10. E-Cadherin
In their 2002 publication, Rodrigo et al. conducted research on the quantification of E-cadherin in supraglottic laryngeal SCC and its association with various outcomes, including nodal metastasis. They found that low levels of E-cadherin in SCC of the supraglottic larynx were significantly correlated with nodal metastases (p = .007). Based on their findings, the authors concluded that E-cadherin serves as an independent predictor of nodal metastases in supraglottic squamous cell carcinomas. [63]
3.2.11. Melanoma Associated-A Antigens
Melanoma-associated antigens (MAGE-A) are typically silent in normal tissues except for the testis, but their expression in other tissues is characteristic of tumor cells. In a study on OSCC, RT-PCR analysis for MAGE-A12 revealed expression of the gene in 49.1% of the 57 cancer tissue samples, while no expression was detected in normal tissues. Based on these findings, the authors hypothesized that MAGE-A12 could serve as a diagnostic marker for occult metastasis. [64]
3.2.12. Vascular Endothelial Growth Factor - C
In a study involving 87 patients with OSCC and T1-2cN0M0 tumors, the expression of Vascular Endothelial Growth Factor – C (VEGF-C) was analysed. The researchers compared the VEGF-C expression with the incidence of occult metastasis after elective neck dissection, which was found to be 22%. Surprisingly, the authors discovered that VEGF-C expression was not related to lymph node metastasis in this cohort of patients. [65]
3.2.13. Panitumumab and Epidermal Growth Factor Receptor
Panitumumab is an antibody that targets the epidermal growth factor receptor (EGFR), which is commonly expressed in up to 90% of HNSCC cases. In a study involving six patients, intravenous injection of panitumumab-IRDye800 was administered, followed by evaluation using a high-sensitivity fluorescence system. The correlation between fluorescence intensity and tumor location, as defined by pathologists, was examined. During neck dissections, a total of 172 lymph nodes were extracted, with eight of them found to be positive for cancer metastasis. Fluorescence imaging of panitumumab-IRDye800 accurately predicted the lymph node status in all cases. Specifically, there were 164 true negative nodes (i.e., not fluorescent and not tumor-positive), eight true positive nodes (i.e., fluorescent and tumor-positive), and no false-positive or false-negative nodes. These findings yielded a sensitivity, specificity, positive predictive value, and negative predictive value of 100%. Therefore, the authors concluded that panitumumab-IRDye800 can effectively identify HNSCC lymph node metastasis with high specificity and negative predictive value.[66]
In 2021, researchers investigated a novel technique for sentinel lymph node biopsy (SLNB) in 27 patients with OSCC, 18 of whom were cN0. The study involved the intravenous administration of Panitumumab-IRDye800CW before surgical resection of the primary tumor with neck dissection and/or SLNB. A total of 960 lymph nodes were analyzed, of which 34 (3.5%) contained metastatic disease. Panitumumab-IRDye800CW demonstrated preferential localization to metastatic and sentinel lymph nodes, exhibiting a higher fluorescent signal compared to others. The median fluorescent intensity (MFI) of metastatic lymph nodes was significantly higher than that of benign ones (0.06 versus 0.02, p < 0.05). Furthermore, selecting the five lymph nodes with the highest fluorescence intensity from individual specimens resulted in 100% sensitivity, 85.8% specificity, and 100% NPV for the detection of occult metastases, and 100% accuracy for clinically staging the neck. In the cN+ cohort, assessment of the highest five fluorescence lymph nodes per patient achieved 87.5% sensitivity, 93.2% specificity, and 99.1% NPV for the detection of metastatic nodes. These findings suggest that Panitumumab-IRDye800CW-enhanced SLNB may offer high sensitivity and accuracy in detecting occult metastases and clinically staging the neck in patients with OSCC. [67]
3.2.14. Cornulin and Total Protein Analysis
The study utilized a sophisticated approach to analyze protein expression in snap-frozen tumor tissue and adjacent normal tissue from patients with HNSCC, aiming to identify potential biomarkers associated with occult nodal metastases. Total protein analysis was performed using laser microdissection and saturation-labeling 2D difference in-gel electrophoresis (2D-DIGE). Significance analysis of Microarray (SAM) method was utilized to evaluate differential protein expression. Protein spots meeting specific criteria were further analysed by liquid chromatography and tandem mass spectrometry to identify proteins. In tumor tissue, no significant differences in protein expression were observed between patients with and without occult nodal metastases. However, considerable differences in protein expression were detected in normal adjacent tissue: 60 protein spots showed significant differences between patients with and without occult metastases; Among these, 31 proteins were underexpressed and 29 were overexpressed in patients with occult metastases; The top candidate among the underexpressed proteins was found to be 11.9-fold lower in the occult metastasis group, while the top candidate among the overexpressed proteins was 6.6-fold higher; Cornulin, a 53 kDa calcium-binding protein of the S100 family, emerged as a significant protein overexpressed in the occult metastasis group. Cornulin, previously identified as a novel biomarker for HNSCC, was found to be overexpressed in the adjacent normal tissue of patients with occult nodal metastases. Elevated cornulin levels in normal adjacent tissue may indicate ongoing epithelial injury, potentially predisposing developing tumors to aggressive behavior. The findings suggest that overexpression of cornulin in adjacent normal tissue could serve as a novel biomarker for tumors with occult metastases in cN0 HNSCC patients. Additionally, the study underscores the importance of tumor-stroma interactions in the development of early nodal metastases.
Overall, this study provides valuable insights into the molecular mechanisms underlying occult nodal metastases in HNSCC and highlights the potential utility of cornulin as a biomarker for identifying high-risk patients. Further research is warranted to validate these findings and explore the clinical implications of cornulin expression in HNSCC. [68]
3.2.15. Markers of Cancer Stem Cells CD133, NANOG and NOTCH1
The study investigated the association between cancer stem cell markers (CD133, NANOG, and NOTCH1) and lymph node metastasis in 144 T1-2cN0 OSCC patients. High expression levels of CD133, NANOG, and NOTCH1 were observed in 72.91%, 59.02%, and 56.94% of the tumor samples, respectively. Significant associations were found between the expression of these markers and lymph node metastasis in early-stage OSCC (CD133: p = 0.035; NANOG: p = .024; NOTCH1: p = .043). These findings suggest that CD133, NANOG, and NOTCH1 may serve as potential indicators of lymph node metastasis in early-stage OSCC. Further research is needed to validate these findings and explore the underlying mechanisms. Top of FormBottom of Form[69]
3.2.16. Metastasis-Associated Protein 1
In a study involving 43 patients with tonsillar squamous cell carcinoma (SCC), overexpression of Metastasis-associated protein (MTA) 1 was found to be a predictor of occult nodal metastasis. Among the population, 41.9% of patients expressed MTA1, and its presence was significantly associated with lymph node metastasis (p = .034). The sensitivity and specificity for diagnosing occult metastasis were reported as 53.3% and 84.6%, respectively. These findings suggest that MTA1 expression could serve as a potential marker for identifying occult nodal metastasis in tonsillar SCC patients. [70]
3.2.17. SFN, TCTP and 14-3-3-Zeta
A proteomic approach was employed to analyze lymph nodes and identify predictors of occult metastasis in early-stage buccal mucosa SCC involving 90 patients. Among the molecules considered, higher expression of SFN was associated with a lower risk of nodal metastasis (p = .03), while higher expression of TCTP was also linked to a lower risk of nodal metastasis (p = .003). Additionally, these markers, along with 14-3-3-zeta, exhibited significant differences in expression between well-differentiated tumors and others. These findings highlight the potential utility of SFN and TCTP as markers for identifying occult nodal metastasis in early-stage buccal mucosa SCC. [71]
3.2.18. E-Cadherin and Focal Adhesion Kinase
In a study involving 95 patients with supraglottic laryngeal cancer, E-cadherin and Focal Adhesion Kinase (FAK) were investigated as markers for nodal metastasis. Reduced E-cadherin expression was found to be associated with the presence of nodal metastases (P = .006). Furthermore, combining the assessment of E-cadherin and FAK expression resulted in improved accuracy in detecting nodal metastasis (P = .001). Histological grade also showed an association with nodal metastases (P = .005). Multivariate analysis confirmed that these parameters were independent predictors of nodal metastases. [72]
3.2.19. p-EMT and SPRR1B
Parikh et al. conducted a study involving 99 patients with OSCC, where they examined tumor tissues using three validated markers of partial epithelial-mesenchymal transition (p-EMT) (PDPN, LAMB3, LAMC2), as well as one marker of well-differentiated epithelial cells (SPRR1B). They found that the p-EMT score was associated with node positivity (2.09 vs. 1.87, p = 0.02), including occult node positivity (56% vs. 19%, p = 0.005). In a multivariate analysis, p-EMT was independently associated with nodal metastasis (OR 3.12, p = 0.039). [73]
3.2.20. NKX3-1 and DNA Copy Number Aberrations
In a study involving 60 patients with OSCC, Affymetrix mapping arrays were utilized to analyze DNA copy number aberrations (CNAs) as a potential marker for occult nodal metastasis. Through correlation analysis between CNA data for genes and the presence of occult metastasis using Fisher’s exact test, several gene clusters with loss/deletion or gain/amplification of genes were found to be significantly associated with occult metastasis (p < .05). Among these clusters, the authors focused on the loss of NKX3-1 (8p21.2), a homeodomain-containing transcription factor, based on findings from a literature review. Further analysis through quantitative RT-PCR and immunohistochemistry (IHC) confirmed significantly lower expression of NKX3-1 in cases with occult nodal metastasis. This observation was validated by IHC analysis in independent cases, where the Wilcoxon rank sum test revealed a significant difference in average positive rates between OSCC cases with and without occult LNM (p<.001). Additionally, the Wilcoxon rank sum test applied to the IHC results in the independent OSCC cases further confirmed the significance (p= .004). Thus, the authors concluded that loss of NKX3-1 may serve as a potential biomarker for occult LNM in OSCC. [74]
3.2.21. MFAP5, TNNC1, MGP, FBFBP1 and FBXO32
Tissue samples from patients with tongue squamous cell carcinoma (TSCC) were analyzed using the Affymetrix HTA2.0 high-density oligonucleotide array to identify differentially expressed genes associated with cervical lymph node metastasis (CLNM). A total of 107 genes were found to be differentially expressed (p < 0.05) in TSCC samples with CLNM (n = 6) compared to those without CLNM (n = 6). Further analysis using Gene Ontology and Kyoto Encyclopedia of Genes and Genomes revealed that these genes were involved in cell-matrix adherens junction and migration functions. Five genes, namely MFAP5, TNNC1, MGP, FBFBP1, and FBXO32, implicated in these pathways were selected and validated using RT-PCR in TSCC samples from a larger cohort (n = 32). Among them, MFAP5 and TNNC1 expressions were further confirmed using immunohistochemistry in additional TSCC samples (n = 61). A significant positive correlation between MFAP5 and TNNC1 expression (p<.001) was observed. Notably, overexpression of MFAP5 and TNNC1 was associated with CLNM, metastasis relapse-free survival, and overall survival. These findings suggest that MFAP5 and TNNC1 may serve as potential markers for predicting occult cervical lymphatic metastasis and prognosis in patients with oral tongue carcinoma. [75]
3.2.22. Homo Sapiens Fatty Acid Binding Protein 5
Ramanathan et al. conducted a study on gene expression in 30 samples of tongue cancers using the mRNA Differential Display system (DD-PCR). Among the 30 cases, 15 signals that showed differential expression between the tumor and metastatic samples were selected after DD-PCR. Out of these 15 signals, only two were successfully reamplified to obtain a single band using primer pair AP18 and T12MC, with a band size of 180 bp. The expressions of these signals were found to be higher in the primary tumors compared to the metastasis. Further analysis revealed that the sequences of these signals showed 100% homology to the gene for Homo sapiens fatty acid binding protein 5 (psoriasis-associated) (FABP5). Northern blot analysis was performed, which indicated that the primary tumors had up to four times higher expression of FABP5 compared to the metastasis. In three cases, the metastatic samples showed complete absence of expression, while in one case, the expression of FABP5 was similar in both the tumor and metastatic samples. A t-test for paired samples comparing the expression between primary tumors and metastases showed a significant difference (p = .011). The mean expression value for primary tumor samples was 0.8741, while the value for metastatic samples was 0.5309. [76]
3.2.23. B cell-Specific Moloney Murine Leukemia Virus Integration Site 1
In a study involving 64 laryngeal SCC patients, the expression of B cell-specific Moloney murine leukemia virus integration site 1 (BMI-1) was examined immunohistochemically on formalin-fixed paraffin-embedded primary tissue specimens. It was found that high expression of nuclear BMI-1 served as an independent prognostic factor for lymph node metastasis (p = .0002). Additionally, high BMI-1 expression correlated significantly with distant metastasis (p < .05), while negative or low BMI-1 expression correlated with negative lymph nodes (p < .05). [77]
3.2.24. Podoplanin
In a prospective clinical trial involving 120 patients with early HNSCC of the oral cavity and oropharynx undergoing sentinel lymph node (SLN) biopsy, the value of cancer cell-expressed podoplanin as a predictive marker for SLN metastasis was assessed. Podoplanin expression by cancer cells was determined using immunohistochemistry on tissue microarrays, with expression quantified by the intensity reactivity score and categorized into expression and nonexpression. Occult metastasis was found in 45 patients (37.5%) upon SLN examination, while 29 out of 120 (24.2%) primary HNSCC tumors showed podoplanin expression. Podoplanin expression significantly correlated with SLN metastasis (p = .029) and remained a significant predictor for lymph node status even after adjusting for tumor stage (p = .028). However, as a predictive marker for SLN metastasis, podoplanin expression demonstrated low sensitivity (36%) and moderate specificity (83%). [78]
3.2.25. p53, Bcl-2, EGFR, Ki67, Cyclin D1 and Cox-2
In laryngeal squamous cell carcinoma (SCC), various molecules were investigated as potential markers of nodal positivity. Among these were apoptotic markers such as p53 and Bcl-2, proliferation markers including EGFR, Ki67, and Cyclin D1, as well as the inflammatory marker Cox-2. Cox-2 was found to be significantly associated with nodal positivity, suggesting its potential utility as a marker for occult nodal metastasis. Additionally, the expression of Cyclin D1 or Ki67 in node-negative patients may indicate the need for neck dissection or irradiation to manage the risk of occult nodal metastasis. [79]
3.2.26. Semaphorin-3F and Neuropilin-2
In 53 patients with cN0 (clinically node-negative) HNSCC, the expression levels of semaphorin-3F (SEMA3F) and neuropilin-2 (NRP2) were investigated. It was found that SEMA3F expression was significantly lower in patients with lymph node involvement compared to those without (cN0/pN0). Based on these findings, patients were categorized into two groups based on their risk of occult nodal metastasis: Group 1 (n = 34): This group exhibited high SEMA3F expression and low NRP2 expression. They demonstrated a low risk of occult nodal involvement, with only 14.7% of patients in this group progressing from cN0 to pN+ (pathologically node-positive). Group 2 (n = 19): Patients in this group had either low SEMA3F expression or high SEMA3F expression along with high NRP2 expression. They showed a significantly higher risk of occult nodal involvement, with 78.9% of patients progressing from cN0 to pN+. Multivariate analysis further confirmed that patients in Group 2 had a substantially higher risk (26.2 times higher) of lymph node involvement compared to those in Group 1. These findings suggest that SEMA3F-NRP2 expression levels may serve as a potential predictive marker for occult nodal metastasis in HNSCC. [80]
3.2.27. Histologic Features
In their study, Sparano et al. examined histologic and staging characteristics in early-stage (T1-2cN0) oral tongue cancers and explored their association with occult metastasis. They found that several factors were significantly linked to occult metastasis, including greater tumor thickness, deeper muscle invasion, T2 stage, poorly differentiated tumors, an infiltrating-type invasion front, presence of perineural invasion, and presence of angiolymphatic invasion. Using a multivariate analysis, they constructed a model to predict the likelihood of occult neck disease, which incorporated greater tumor thickness, presence of perineural invasion, infiltrating-type invasion front, poorly differentiated tumors, and T2 stage. These findings suggest that these histologic and staging characteristics may be valuable indicators for identifying patients at heightened risk of occult neck disease in early-stage oral tongue cancers. [81]
In a study comparing skeletal muscle invasion and depth of invasion (DOI) in oral tongue squamous cell carcinoma (SCC), 61 T1N0 cases served as a reference group for assessing their predictive value for occult metastasis over a 2-year follow-up period. Among cases with muscle invasion, there was a 23.3% positive predictive value (PPV) for occult lymph node metastasis. Similarly, cases with a DOI greater than 3 mm exhibited a 29.7% PPV for occult lymph node metastasis. These findings highlight the potential of both skeletal muscle invasion and DOI as predictive factors for identifying cases at risk of occult lymph node metastasis in oral tongue SCC. [82]
In a retrospective review of 48 patients with early oral tongue squamous cell carcinoma (SCC), histopathological factors such as depth of tumor, differentiation, blood vessel invasion, lymphatic invasion, and tumor budding were examined for their association with late lymph node metastasis. Univariate analysis revealed that blood vessel invasion, lymphatic invasion, and high-grade tumor budding were predictive factors for neck recurrence (p < .001). However, the Cox proportional hazards model identified high-grade tumor budding as an independent predictive factor (p < .01). Notably, the combination of a tumor depth ≥ 3 mm and high-grade tumor budding showed high diagnostic accuracy. These findings underscore the significance of tumor depth and budding grade as histopathological risk factors for late neck recurrence in clinical N0 early oral tongue carcinoma. [83]
In patients with cT1/2N0 oral tongue squamous cell carcinoma (SCC), the pathomorphological evaluation of tumor budding grade (TBG) and tumor–stroma ratio (TSR) has been shown to predict lymph-node metastases. Among 70 patients, 35 had positive neck lymph node metastasis. Univariate analysis revealed correlations between lymph node metastasis and pathological depth of invasion (pDOI) (p < 0.001), TBG (p = 0.008), and TSR (p < 0.001). In multivariate analysis, pDOI (p = 0.01) and TSR (p = 0.02) remained significant predictors of lymph node metastasis. [84]
In a study involving 152 patients with cT1-T3N0 oral squamous cell carcinoma (OSCC), the presence of stromal myofibroblasts was examined as a potential marker for occult nodal metastasis. Immunohistochemical analysis of surgical resection specimens revealed that 84.2% of OSCC cases (n=128) were positive for myofibroblasts in the tumor stroma. Importantly, an increased presence of myofibroblasts in the tumor stroma was significantly correlated with the presence of occult neck metastasis (P<0.001). [85]
The Modified Polsby-Popper (MPP) score, implemented as a semi-automated image analysis workflow, was explored as a potential predictor of cervical lymph node metastases in tongue cancer. Machine learning models were constructed to forecast both survival outcomes and the likelihood of occult cervical metastases. The findings indicated that higher MPP scores correlated with an elevated incidence of distant metastasis, particularly in early-stage tongue cancer. [86]
Digital analysis of tumor budding (TB) and minimal cell nest size (MCNS) was conducted in 331 cases of HNSCC, both HPV-positive and HPV-negative. The analysis encompassed 1 and 10 high-power fields (HPF). High cellular dissociation grading was found to be linked with clinically occult lymph-node metastases. [87]
In a study involving 323 patients with stage I OSCC (cT1-2N0), the Worst Pattern of Invasion-type 5 (WPOI-5) was evaluated as a risk model outcome. High-risk classification according to WPOI-5 was associated with regional metastasis (p = .052; HR, 3.27; 95% CI, 1.42-7.5). Moreover, WPOI-5 was found to be significantly predictive of occult cervical metastases (p < .0001). [88]
3.2.28. Cellular Dissociation Grade
In an article published in the British Journal of Cancer, a novel grading system termed Cellular Dissociation Grade (CDG), based on Tumour Budding and Cell Nest Size, was proposed as a predictor of occult metastasis. In a subgroup of HNSCC patients with clinically negative cervical lymph nodes (cN0 necks; n = 40), occult metastases were detected by pathological evaluation of neck dissection specimens in 8 out of 40 cases (20.0%). All cases with occult metastases had a histopathological grading of nG2/3, while none of the nG1 cases showed presence of lymph node metastases. This finding suggested a positive predictive value (PPV) of 100% for nG1 grading in predicting nodal negativity upon pathological examination in cN0 necks. [89]
3.2.29. MRI Size for Oral Tongue SCC
Kwon et al. investigated the tumor contrast MRI thickness measured in axial (mediolateral direction), coronal (superoinferior direction), and sagittal (anteroposterior direction) views of oral tongue SCC as a predictor of occult lymph node metastasis in 53 patients. Among the 39 patients classified as cN0, 15 were found to have occult metastasis (38.5%). Using ROC curves, the authors developed a predictive model for occult lymph node metastasis, yielding an area under the curve (AUC) of 0.750 in the medial-lateral direction on the axial view, 0.753 for tumor thickness (TT) in the superior-inferior direction on the coronal view, and 0.750 for TT in the anterior-inferior direction on the sagittal view. They found that cutoff values of 6.7 mm, 7.2 mm, and 12.3 mm in axial, coronal, and sagittal planes, respectively, were predictors of occult lymph node metastasis (p < .05). [90]
3.2.30. Prospero Homeobox Protein 1
Mermod et al. investigated lymphatic vessel density as a predictor of occult lymph node metastasis, using a specific antibody against the transcription factor Prospero homeobox protein 1 (PROX1) as an indicator. They retrospectively included 42 cN0 HNSCC and 10 cN+ HNSCC patients. A PROX1 nuclei cutoff >31.33 showed a sensitivity of 0.6 (95% CI 0.26–0.88), specificity of 0.98 (95% CI 0.87–0.99), positive predictive value (PPV) of 0.86 (95% CI 0.42–0.99), negative predictive value (NPV) of 0.91 (95% CI 0.79–0.98), and overall accuracy of 0.88 (95% CI 0.76–0.96). Reliability analysis assessing agreement between authors resulted in an ICC of 0.83 (p = .005). Consequently, the authors concluded that PROX1 could be an independent predictor of occult metastasis. [11]
3.2.31. SPECT/CT
SPECT/CT, a radiological imaging technique for lymphatic metastasis detection, was evaluated in 44 cases of OSCC, including 13 with occult nodal disease confirmed by histopathology and elective neck dissection (END). Occult nodal disease was present in 29.5% (n=13) of patients based on END histopathology. Sentinel node biopsy (SNB) demonstrated sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) of 76%, 100%, 91%, and 100% respectively. A total of 183 sentinel nodes were identified, with a mean of 8.13 per patient. Planar lymphoscintigraphy (PL) and SPECT revealed ipsilateral neck hotspots in 95% (n=42) of patients and contralateral neck hotspots in 9% (n=4). PL identified 77 hotspots (mean 1.75 per patient) and SPECT identified 92 hotspots (mean 2.5 per patient). SPECT/CT detected additional hotspots in 8 patients, including 3 where PL failed to detect any nodes. In 2 patients, both PL and SPECT were negative. Detection rates by PL, SPECT, and gamma probe were 93%, 95%, and 97% respectively. Good concordance was observed between anatomical localization on SPECT/CT and gamma probe findings. Although SPECT/CT allowed better anatomical characterization, the authors concluded that given the excellent accuracy of combined planar imaging and intra-operative gamma probe, SPECT/CT did not offer clear advantages. [91]
3.2.32. SUV PET/CT
Xu et al. investigated whether the maximum standardized uptake value (SUVmax) measured on PET/CT could serve as a predictor of occult nodal metastasis in stage I (cT1-2N0) tongue SCC. The study included 120 patients for analysis. Among 60 patients with an SUVmax of ≤9.7, 5 patients had occult metastasis. In contrast, among 60 patients with an SUVmax of >9.7, 13 patients had occult metastasis. This difference was found to be statistically significant (p=0.041). [92] While Kuźmińska et al. considered PET/CT alone as a potential tool for detecting occult metastasis. [93]
3.2.33. Ultrasonography
Norling et al. investigated the benefits of incorporating ultrasonography into the standard imaging protocol for OSCC. They found that the short axial diameter was the most effective size criterion for metastasis detection. However, they observed that sonographic characteristics were better predictors than size alone. Specifically, the presence of at least four sonographic characteristics—hypoechoic or heterogeneous appearance, irregular border, spherical shape, absence of nodal hilum, and peripheral nodal blood flow—yielded a sensitivity of 43.8%, specificity of 91.4%, positive predictive value (PPV) of 70.0%, and negative predictive value (NPV) of 78.0%. With this approach, the number of patients with occult metastases decreased from 16 out of 51 (31%) to nine out of 51 (18%). [94]
Ultrasonography assessment of cervical lymph nodes was conducted in 60 patients with laryngeal SCC who had negative neck nodes on CT scan. The respective values for ultrasound-guided fine needle aspiration cytology (USg FNAC) demonstrated high sensitivity, specificity, positive predictive value, negative predictive value, and accuracy (92%, 100%, 100%, 96%, and 97%, respectively). However, the size, shape, and vascularity showed significantly lower values for these statistical parameters. [95]
3.2.34. E-Cadherin
The E-Cadherin glycoprotein plays a crucial role in establishing and maintaining intercellular connections. In an analysis of 120 patients with HNSCC affecting the oral cavity or oropharynx, the Intensity Reactivity Score for E-Cadherin expression was quantified and compared to lymph node status obtained by sentinel lymph node biopsy. The study revealed a significant correlation between the differentiation grade and E-cadherin expression with positive lymph node status (p = .018 and p = .005, respectively). [96]
3.2.35. Ki-67, PARP, BAD, Caspase-9, VEGF-A
Researchers utilized a targeted spatial proteomic approach to analyze lymph node metastasis. Their observations revealed higher expression levels of Ki-67, PARP, BAD, and cleaved Caspase 9 within metastatic cells compared to primary cancer cells. [97]
Ki-67 and vascular endothelial growth factor A (VEGF-A) expression were investigated in pharyngeal and laryngeal SCC. The study revealed that Ki-67 expression was a significant risk factor for nodal involvement (N+) across all tumors (P ≤ .009). Conversely, VEGF-A expression was associated with nodal involvement in oral and pharyngeal SCC exclusively (P < .03). Specifically, Ki-67 expression alone in oral and pharyngeal SCC was linked to a relative risk of nodal involvement of 3.83 (95% confidence interval, 1.22-11.99; P = .009), and the additional expression of VEGF-A increased this value to 6.12 (2.09-17.93; P < .001). Furthermore, the combined expression of both markers was 3.25 times more effective in predicting nodal involvement for T1,2 tumors compared to T3,4 tumors. [98]
3.2.36. HPV and p16
In a study of 93 cases of nodal metastatic (N+) SCC, researchers employed in situ hybridization for high-risk HPV and immunostaining for p16 in both nodal tissues and primary tumors. The cohort comprised 32 cases of oropharyngeal cancer, 35 cases of oral cancer, and 26 cases from the larynx or hypopharynx. Of the total cases, 23 were found to be HPV-positive, with 22 of them originating from the oropharynx. The findings suggested that lymph node metastasis could be assessed using in situ hybridization and p16 immunoreactivity in conjunction with histomorphological evaluation. [99]
3.2.37. Methylation Status of Long INterspersed Element 1 (LINE-1) and Alu Elements (Alu)
Epigenomic analysis was conducted on lymph node tissues to explore their potential as markers for cancer metastasis. Hypomethylation of Long INterspersed Element 1 (LINE-1) and Alu elements (Alu) was investigated using the Combine Bisulfite Restriction Analysis (COBRA) technique. A total of 61 nodes were analyzed. LINE-1 and Alu loci were classified based on the methylation statuses of two CpG dinucleotides in each allele, including hypermethylation (mCmC), hypomethylation (uCuC), and two forms of partial methylation (mCuC and uCmC). The results showed altered LINE-1 methylation, with lower LINE-1 methylation levels observed (p < 0.001). Additionally, there was a higher percentage of mCuC (p < 0.01), a lower percentage of uCmC (p < 0.001), and a higher percentage of uCuC (p < 0.001) in the analyzed samples. Receiver operating characteristic (ROC) curve analysis revealed that %uCmC and %mCuC values had high areas under the curve (AUC) of 0.806 and 0.716, respectively, in distinguishing lymph node (LN) from non-metastatic (NM) cases. Based on these findings, the authors concluded that the LINE-1 methylation changes in LN exhibited a similar pattern to that in primary tumors. This epigenomic alteration may be indicative of the presence of occult metastatic tumor cells in the lymph nodes analyzed.[100]
3.2.38. MET
In a study involving 151 lymph nodes from 20 cases of squamous cell carcinomas, both in-depth histology and end-point and real-time quantitative RT-PCR techniques were used. MET-encoding sequences were detected in 61 out of 151 nodes (40%), with 24 nodes (16%) found to be metastatic by in-depth histopathology. In comparison, routine histopathologic analysis of 654 lymph nodes from the same cases identified only 36 metastases (5%). Real-time quantitative RT-PCR was employed to measure MET gene-specific mRNA levels in normal tissues, primary tumors, and lymphatic metastases. The study concluded that the MET gene product serves as a valuable marker for the detection of occult tumor cells in lymph nodes due to its high expression in metastatic cells. [101]
3.2.39. Gene Expression Analyses and Molecular Subtypes
In a retrospective cohort study, gene expression subtypes in oral squamous cell carcinoma (OSCC) and laryngeal squamous cell carcinoma (SCC) were examined to determine their predictive value for nodal metastasis. The study identified four molecular subtypes: basal (BA), mesenchymal (MS), atypical (AT), and classical (CL). In OSCC, the mesenchymal (MS) subtype was significantly associated with a higher risk of nodal metastasis. Furthermore, it was predictive of occult nodal metastasis in a subset of T1-2cN0M0 patients, with a relative risk of 3.38 (95% confidence interval [CI]: 1.08-10.69).[102]
3.3. Blood Markers
3.3.1. Indexes and Rations from Standard Blood Analysis
In a multicentric retrospective analysis by Gaudioso et al. involving 472 patients with cN0 neck, various baseline blood parameters including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), systemic inflammatory marker (SIM), and systemic immune-inflammation index (SII) were evaluated, along with stage and differentiation grade. The study focused on oral, oropharyngeal, and hypopharyngeal cancers, which were found to have a greater risk of occult metastasis compared to other head and neck subsites. Additionally, locally advanced stages and moderate to poor differentiation grades (G2 and 3) were associated with a higher risk of lymph node involvement. Multivariate analysis revealed a significant association between NLR, LMR, PLR, SIM, and SII, with NLR greater than 2.12 emerging as the most reliable parameter (OR = 5.22; 95% CI 2.14 – 12.75) for predicting lymph node metastasis. Based on these findings, the authors developed a predictive score for lymph node metastasis incorporating cancer subsite, local stage, and NLR value. [10]
In a retrospective analysis of 108 patients with laryngeal squamous cell carcinoma (SCC), the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were assessed as predictors of occult metastasis (OM). High values of NLR, but not PLR, were found to significantly correlate with the probability of OM. Through an iterative algorithm, an NLR value of 2.26 was determined to correspond to a probability of OM of 20%. As a result, the authors concluded that there is a statistical correlation between high pre-treatment NLR values and occult metastasis in patients with laryngeal SCC. [103]
In a retrospective study involving 110 patients with early-stage oral tongue squamous cell carcinoma (SCC) (T1-2cN0), the neutrophil-to-lymphocyte ratio (NLR) was investigated as a predictor of occult metastasis. The analysis revealed a statistically significant relationship between high levels of pre-treatment NLR and the probability rate for neck occult metastases (p = 0.000496). A cutoff value of NLR > 2.93 was determined, above which the probability of finding metastasis in a clinically negative neck increased exponentially according to their model. [104]
In a recent study by Yamagata et al., the neutrophil-to-lymphocyte ratio (NLR) was confirmed as a predictor of occult metastasis. Similarly, Ventura et al. found a significant association between NLR (p = 0.001) and monocyte-lymphocyte ratio (p = 0.011) with neck status on univariate analysis. However, multivariate analysis revealed that only NLR (p = 0.02) was an independent risk factor for occult metastasis among inflammatory blood markers. [105]
In a cohort of 110 patients with oral tongue SCC, the neutrophil-to-lymphocyte ratio (NLR) and depth of invasion (DOI) were analyzed as predictors of occult nodal metastasis using a logistic regression model. The study found that a DOI greater than 5.4 mm and an NLR greater than 2.93 are associated with an increased risk of presenting occult cervical metastases. Additionally, a positive correlation was observed between the variables NLR and DOI, as indicated by Spearman’s rank correlation coefficient rho of 0.64. Specifically, a unitary increase in the DOI of 1 mm was directly associated with an increase of 0.47 in the NLR. [106]
3.3.2. Circulating Tumour Cells
In a study involving 152 patients using the OncoDiscover technique for circulating tumor cells (CTCs), comparisons were made with 40 non-HNSCC controls. Among several outcomes measured, including the presence of nodal metastasis, the results suggested that CTC counts above 20.5 were indicative of nodal metastasis (p < .0001). Additionally, there was a linear trend observed for detecting occult metastasis (p = .061). [107]
3.3.3. Circulating Tumour Cells
Circulating hybrid cells (CHCs) are characterized by their fusion of genetic material from cancer cells and host leukocytes. These hybrid cells exhibit increased tumorigenic potential compared to standard circulating tumor cells and have been found to correlate with disease stage and progression in cancer. [108,109] In a study involving 20 patients with clinically node-negative oral squamous cell carcinoma (OSCC), researchers investigated circulating hybrid cell (CHC) levels. They compared these levels with the pathological nodal status and also included positive controls (patients with clinically positive nodal metastasis, cN+) and negative controls (volunteers without cancer, T0). The findings revealed a significant difference in CHC levels between patients with cN0 OSCC who later developed positive nodes and those who remained negative (p = .005). [108] Henn et al. also found a significant relationship between circulating hybrid cells (CHC) and occult nodal metastasis (p = .006) in patients with clinically node-negative oral squamous cell carcinoma (OSCC). [109]
3.3.4. Circulating HPV DNA
Circulating human papillomavirus (HPV) DNA in the serum of patients with HPV-positive head and neck squamous cell carcinoma (HNSCC) was investigated using conventional PCR, real-time quantitative assay, and Southern blotting for confirmation in case of positivity. Among the patients tested, conventional PCR using E7 primers and Southern blot hybridization detected circulating HPV DNA in 6 patients. Strikingly, 4 of these patients subsequently developed distant metastasis. This finding led the authors to hypothesize a potential relationship between circulating HPV DNA and tumor cells, suggesting a possible role in metastatic dissemination. [110]
3.3.5. CD31
The density of the panvascular endothelial antibody CD31 was evaluated as a potential predictor of occult metastasis in patients with clinically node-negative (cN0) oral cavity and oropharyngeal squamous cell carcinoma (SCC). A total of 56 cases of oral cavity SCC and 6 cases of oropharyngeal SCC were included in the analysis. The results revealed a significant correlation between CD31 density and occult lymph node metastasis (p < 0.01). Using recursive partitioning analysis, a cutoff value of 19.33 for CD31 density was determined, which demonstrated a sensitivity of 91%, a specificity of 65%, a positive predictive value of 40%, a negative predictive value of 97%, and an overall diagnostic accuracy of 71% for identifying occult lymph node metastasis. [111]
3.3.6. Bone Marrow
In 2004, Wollenberg et al. conducted a study investigating the predictive value of detecting free tumor cells in bone marrow aspirates of patients with head and neck squamous cell carcinoma (HNSCC). They utilized monoclonal KS 19.1 antibodies to detect cytokeratin 19 (CK19) expression in bone marrow aspirates obtained from the iliac crest of 176 HNSCC patients. Among them, 54 patients tested positive for CK19 expression in bone marrow cells. Over a 60-month follow-up period, 60 patients (34.09%) experienced disease recurrence, with 34 cases (56.67%) involving locoregional recurrences and 26 cases (43.33%) involving distant metastases. Among the 54 patients with CK19-positive cells in the bone marrow, 27 (50%) had tumor recurrence, compared to 33 out of 122 patients (27.05%) in the CK19-negative group. This difference demonstrated a significant correlation between CK19 positivity in bone marrow aspirates and tumor recurrence (p < 0.05). [112]
4. Discussion
The accurate diagnosis of regional lymph node metastasis is critical for determining the appropriate treatment strategy in patients with head and neck cancer. Clinical staging, based on physical examination and imaging modalities, may not always accurately detect occult metastasis. Therefore, elective neck dissection is often recommended for N0 patients with a calculated risk of locoregional metastasis exceeding 20%, especially in high-risk cases or when imaging results are inconclusive. This approach helps ensure that occult metastases are detected and appropriately managed, ultimately improving patient outcomes. [12,113] Indeed, postoperative histological analysis often reveals that a significant proportion of patients who undergo elective neck dissection do not harbor metastatic disease in their lymph nodes. Studies have reported rates ranging from 50% to 80% of patients with clinically node-negative necks who ultimately have no evidence of metastasis in the dissected lymph nodes. This highlights the potential for over-treatment and the associated morbidity of unnecessary surgical intervention in these patients. As such, there is a growing interest in refining the selection criteria for elective neck dissection to minimize unnecessary procedures and reduce associated morbidity while still ensuring appropriate management for those at risk of occult metastasis. [108,114,115,116,117] Exactly, the sensitivity of conventional pathologic evaluation, which typically involves the examination of hematoxylin and eosin (H&E)-stained tissue sections under a microscope, is limited in detecting small metastatic deposits within lymph nodes. This limitation can lead to false-negative results, where small metastases are missed during routine histopathological examination. As a result, patients with occult metastasis may be incorrectly classified as node-negative based on conventional pathological evaluation, leading to potential undertreatment. This underscores the need for more sensitive diagnostic approaches to accurately identify occult metastases in lymph nodes, especially in patients with clinically node-negative necks. [118] Absolutely, identifying reliable markers of locoregional or distal metastasis is crucial for several reasons. Firstly, it helps avoid subjecting patients to unnecessary and potentially harmful treatments, such as elective neck dissection or adjuvant therapy, if they do not have metastatic disease. This reduces the risk of treatment-related morbidity and improves patients’ quality of life. Secondly, accurate identification of metastasis allows for more tailored and precise treatment strategies, ensuring that patients receive appropriate therapy based on their disease stage and prognosis. Lastly, early detection of metastasis enables timely intervention and monitoring, which can improve outcomes and overall survival rates for patients with head and neck cancer. Therefore, finding reliable markers of metastasis is essential for optimizing patient care and treatment outcomes in this population.Furthermore, clinical staging of lymph nodes is far less accurate than pathological staging. Pathological staging also suffers limitations because it fails to detect micrometastasis in a subset of nodal specimens. [20] Therefore, the use of microRNA for metastasis detection could also help identifying occult metastasis in cases of apparent negative neck dissections improving accuracy of post operative neck dissection specimens analysis.
Fletcher et al. highlight the importance of defining the threshold value for metastasis markers. This value separates patients into positive and negative groups, guiding treatment decisions. Determining the optimal threshold requires balancing sensitivity and specificity. Further studies are needed to establish accurate cutoff values, improving clinical utility and patient outcomes. [20]
The investigation into metastasis markers presents several considerations. Blood markers offer a less invasive approach, allowing surgeons to plan operations and conduct concurrent procedures like neck dissection and tumor excision. However, analyzing markers from the initial biopsy of the cancer specimen, rather than post-surgery specimens, is crucial. This is because suspected nodal metastasis may necessitate a second surgery, leading to treatment delays and increased risks due to repeated anesthesia exposure.
Moreover, it’s important to note that many studies included in this systematic review focused solely on neck nodal metastasis. However, paratracheal lymph nodes should also be considered. For example, in a cohort of laryngeal cancer patients undergoing salvage laryngectomy, 14% had paratracheal involvement, with 55% showing no lateral neck disease. Neglecting to consider lateral neck disease may result in incomplete evaluation and mismatches in identifying molecular markers. [119]
Identifying micro-metastases through molecular techniques in lymph node specimens may seem inconsequential unless we consider its impact on post-surgical therapy. A positive lymph node status (pN+) typically prompts healthcare providers to recommend adjuvant chemotherapy or radiotherapy to the patient. [12] Hence, investigating micro-metastases preoperatively through blood markers aids in surgery planning, while examining nodal specimens post-neck dissection is pivotal for adjuvant therapy planning. In our review, we noted various potential markers of occult metastasis. Although the concept of identifying a single powerful marker to predict occult nodal involvement is appealing, it may overlook the influence of other factors. Combining multiple markers could enhance predictive accuracy. [5,7,24] Indeed, the concept of devising a scoring system that incorporates multiple factors, similar to the approaches taken by Gaudioso et al. and James et al., enhances predictive capability. [7,10,24] Integrating the various molecules and markers discussed could pave the way for the development of a novel scoring system with enhanced predictive value for occult lymph node metastasis. [5,24]
Advancements in imaging technology are inherently tied to technological progress. As new imaging techniques enhance their diagnostic capabilities, it becomes essential to correlate molecular findings with the latest radiological insights. However, a significant challenge lies in the slow dissemination of costly equipment. Despite the promising outcomes of new imaging modalities, their widespread adoption, like PET/MRI, remains limited due to cost and accessibility issues. [44]
While numerous researchers have explored promising markers, the limited sample sizes often hinder conclusive findings. For instance, in the case of HPV DNA research as a marker for circulating tumor cells, only six patients tested positive, with four of them later developing distant metastasis. Such small sample sizes underscore the need for larger, more comprehensive studies to draw meaningful conclusions about these markers. [110] Indeed, with such a small sample size, generalizing the findings becomes challenging. However, these preliminary results can serve as a valuable starting point for larger-scale clinical trials, providing a foundation for further investigation and potentially uncovering more robust associations between the marker and metastasis.
Indeed, some of the techniques mentioned could prove useful intraoperatively, aiding surgeons in making clinical decisions regarding neck dissection during surgery. For instance, light reflectance spectroscopy has shown promise as a predictor of nodal metastasis, offering real-time information that can guide surgical interventions. [43] It’s crucial to critically analyze the practical impact of such promising results on clinical practice. While techniques like light reflectance spectroscopy offer real-time guidance during surgery, it’s important to consider their limitations. Since neck dissection already exposes patients to significant morbidity, the decision to perform it should be carefully weighed. While predictive models may not achieve 100% accuracy in detecting metastasis, factors like depth of invasion (DOI) remain important predictors for occult lymph node metastasis in oral squamous cell carcinoma (OSCC). [120,121,122] Indeed, indicators like a DOI exceeding 2.5 mm or the presence of poorly differentiated OSCC are strong signals for considering elective neck dissection. These factors provide valuable guidance in determining the appropriate course of action to manage potential occult lymph node metastasis. [123] The adoption of this marker, as endorsed by NCCN guidelines, establishes it as the current gold standard in clinical practice. [12] Hence, we contend that any novel marker should undergo comparison with DOI or be integrated with it before being incorporated into any clinical protocol.
Méndez et al. compared their model with tumor size, which is a distinctly different parameter compared to DOI. [23] Indeed, the relationship between tumor size and DOI can vary significantly. Hence, it’s crucial to compare these parameters alongside DOI for a more comprehensive understanding of their predictive value.
Several of the aforementioned markers have been tested in multiple studies, consistently showing efficacy as predictors of occult cervical lymph node metastasis. However, the studies reviewed here often involve small populations, limiting their statistical power. We advocate for large multicenter trials that focus on markers demonstrating effectiveness across multiple studies. Promising candidates for such validation trials include microRNAs, notably miR-205, as well as DSG3, pan-CK AE1/AE3, HPV-16, Activin-A, Cyclin D1, and NPL.
5. Conclusions
The accurate diagnosis of regional lymph node metastasis is pivotal for guiding treatment decisions in head and neck cancer patients. Markers serving as diagnostic tools hold promise in averting overtreatment of negative necks and ensuring appropriate treatment for metastatic patients. To solidify their efficacy, future research efforts should involve larger populations. This validation process is particularly crucial for markers like miR-205, DSG3, pan-CK AE1/AE3, cytokeratins, HPV-16, Activin-A, Cyclin D1, and NPL, which have demonstrated effectiveness across multiple studies. Combining multiple markers into a scoring system could enhance their predictive accuracy.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of Worldwide Burden of Cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef]
- Dias, F.L.; Kligerman, J.; Matos De Sá, G.; Arcuri, R.A.; Freitas, E.Q.; Farias, T.; Matos, F.; Lima, R.A. Elective Neck Dissection versus Observation in Stage I Squamous Cell Carcinomas of the Tongue and Floor of the Mouth. Otolaryngol. - Head Neck Surg. 2001, 125, 23–29. [Google Scholar] [CrossRef]
- Ferlito, A.; Silver, C.E.; Rinaldo, A. Neck Dissection: Present and Future? Eur. Arch. Oto-Rhino-Laryngology 2008, 265, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.C.; Zhang, S.; Ishii, G.; Endoh, Y.; Kodama, K.; Miyamoto, S.; Hayashi, R.; Ebihara, S.; Cho, J.S.; Ochiai, A. Predictive Markers for Late Cervical Metastasis in Stage I and II Invasive Squamous Cell Carcinoma of the Oral Tongue. Clin. Cancer Res. 2004, 10, 166–172. [Google Scholar] [CrossRef]
- Suresh, A.; Jeevan, M.; Trivedi, N.; Hiran, K.R.; Kekatpure, V.; Kuriakose, M.A. Detection of Occult Lymph Node Metastasis in Oral Tongue Squamous Cell Carcinoma. Oral Oncol. 2011, 47, S89. [Google Scholar] [CrossRef]
- Noorlag, R.; Boeve, K.; Witjes, M.J.H.; Koole, R.; Peeters, T.L.M.; Schuuring, E.; Willems, S.M.; van Es, R.J.J. Amplification and Protein Overexpression of Cyclin D1: Predictor of Occult Nodal Metastasis in Early Oral Cancer. Head Neck 2017, 39, 326–333. [Google Scholar] [CrossRef]
- Kothandaraman, S.; James, B.L.; Raghavan, N.; Suresh, A.; Kuriakose, M.A. Clinical Application of Bio-Markers for Detection of Nodal Metastasis in Head and Neck Squamous Cell Carcinoma. Head Neck 2017, 39, E96. [Google Scholar]
- Ferlito, A.; Rinaldo, A.; Robbins, K.T.; Silver, C.E. Neck Dissection: Past, Present and Future? J. Laryngol. Otol. 2006, 120, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.I.; Ferlito, A.; Rinaldo, A.; Gourin, C.G.; Lowry, J.; Ho, W.K.; Leemans, C.R.; Shaha, A.R.; Suárez, C.; Clayman, G.L.; et al. Management of the N0 Neck - Reference or Preference. Oral Oncol. 2006, 42, 115–122. [Google Scholar] [CrossRef]
- Gaudioso, P.; Borsetto, D.; Polesel, J.; Tirelli, G.; Emanuelli, E.; Menegaldo, A.; Molteni, G.; Nicolai, P.; Tomasoni, M.; Montenegro, C.; et al. Blood Markers Predicting Clinically Occult Lymph Node Metastasis in Head and Neck Squamous Cell Carcinoma. ORL. J. Otorhinolaryngol. Relat. Spec. 2024, 86, 32–40. [Google Scholar] [CrossRef]
- Mermod, M.; Bongiovanni, M.; Petrova, T.V.T.V.; Dubikovskaya, E.A.E.A.; Simon, C.; Tolstonog, G.; Monnier, Y. Prediction of Occult Lymph Node Metastasis in Squamous Cell Carcinoma of the Oral Cavity and the Oropharynx Using Peritumoral Prospero Homeobox Protein 1 Lymphatic Nuclear Quantification. Head Neck 2016, 38, 1407–1415. [Google Scholar] [CrossRef] [PubMed]
- Network, N.C.C. NCCN Clinical Practice Guidelines in Oncology - Head and Neck Cancers Version 2.2022. NCCN 2022. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. MicroRNAs: Genomics, Biogenesis, Mechanism, and Function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Hannon, G.J. MicroRNAs: Small RNAs with a Big Role in Gene Regulation. Nat. Rev. Genet. 2004, 5, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Nagadia, R.; Pandit, P.; Coman, W.B.; Cooper-White, J.; Punyadeera, C. MiRNAs in Head and Neck Cancer Revisited. Cell. Oncol. 2013, 36, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Childs, G.; Fazzari, M.; Kung, G.; Kawachi, N.; Brandwein-Gensler, M.; McLemore, M.; Chen, Q.; Burk, R.D.; Smith, R. V.; Prystowsky, M.B.; et al. Low-Level Expression of MicroRNAs Let-7d and MiR-205 Are Prognostic Markers of Head and Neck Squamous Cell Carcinoma. Am. J. Pathol. 2009, 174, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Hui, A.B.Y.; Lenarduzzi, M.; Krushel, T.; Waldron, L.; Pintilie, M.; Shi, W.; Perez-Ordonez, B.; Jurisica, I.; O’Sullivan, B.; Waldron, J.; et al. Comprehensive MicroRNA Profiling for Head and Neck Squamous Cell Carcinomas. Clin. Cancer Res. 2010, 16, 1129–1139. [Google Scholar] [CrossRef] [PubMed]
- Salazar, C.; Calvopiña, D.; Punyadeera, C. MiRNAs in Human Papilloma Virus Associated Oral and Oropharyngeal Squamous Cell Carcinomas. Expert Rev. Mol. Diagn. 2014, 14, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Salazar, C.; Nagadia, R.; Pandit, P.; Cooper-White, J.; Banerjee, N.; Dimitrova, N.; Coman, W.B.; Punyadeera, C. A Novel Saliva-Based MicroRNA Biomarker Panel to Detect Head and Neck Cancers. Cell. Oncol. 2014, 37, 331–338. [Google Scholar] [CrossRef]
- Fletcher, A.M.; Heaford, A.C.; Trask, D.K. Detection of Metastatic Head and Neck Squamous Cell Carcinoma Using the Relative Expression of Tissue-Specific Mir-205. Transl. Oncol. 2008, 1, 202–208. [Google Scholar] [CrossRef]
- de Carvalho, A.C.A.C.; Scapulatempo-Neto, C.; Maia, D.C.C.D.C.C.; Evangelista, A.F.A.F.; Morini, M.A.M.A.; Carvalho, A.L.A.L.; Vettore, A.L.A.L. Accuracy of MicroRNAs as Markers for the Detection of Neck Lymph Node Metastases in Patients with Head and Neck Squamous Cell Carcinoma. BMC Med. 2015, 13, 108. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Zhang, W.; Ji, W. MYO5A Inhibition by MiR-145 Acts as a Predictive Marker of Occult Neck Lymph Node Metastasis in Human Laryngeal Squamous Cell Carcinoma. Onco. Targets. Ther. 2018, 11, 3619–3635. [Google Scholar] [CrossRef]
- Méndez, E.; Lohavanichbutr, P.; Fan, W.; Houck, J.R.; Rue, T.C.; Doody, D.R.; Futran, N.D.; Upton, M.P.; Yueh, B.; Zhao, L.P.; et al. Can a Metastatic Gene Expression Profile Outperform Tumor Size as a Predictor of Occult Lymph Node Metastasis in Oral Cancer Patients? Clin. cancer Res. an Off. J. Am. Assoc. Cancer Res. 2011, 17, 2466–2473. [Google Scholar] [CrossRef]
- James, B.L.; Kontharaman, S.; Kumar, M.; Ravindra, D.R.; Mitha, S.; Dwivedi, N.; Nisheena, R.; Pillai, V.; Hedne, N.; Suresh, A.; et al. Molecular Marker Based Intra-Operative Diagnostic Assay for Detection of Lymph Node Metastasis in Hnscc. Head Neck 2017, 39, E108. [Google Scholar]
- Wang, Q.; Takashima, S.; Takayama, F.; Wang, J.C.; Kawakami, S.; Saito, A.; Matsushita, T.; Sone, S. Detection of Occult Metastatic Lymph Nodes in the Neck with Gray-Scale and Power Doppler US. Acta Radiol. 2001, 42, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Onishi, A.; Nakashiro, K.-I.; Mihara, M.; Sumida, T.; Kawamata, H.; Shintani, S.; Aida, T.; Tachikawa, T.; Hamakawa, H. Basic and Clinical Studies on Quantitative Analysis of Lymph Node Micrometastasis in Oral Cancer. Oncol. Rep. 2004, 11, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Shores, C.G.; Yin, X.; Funkhouser, W.; Yarbrough, W. Clinical Evaluation of a New Molecular Method for Detection of Micrometastases in Head and Neck Squamous Cell Carcinoma. Arch. Otolaryngol. - Head Neck Surg. 2004, 130, 937–942. [Google Scholar] [CrossRef]
- Tao, L.; Lefèvre, M.; Ricci, S.; Saintigny, P.; Callard, P.; Périé, S.; Lacave, R.; Bernaudin, J.-F.; Lacau, St. Guily, J. Detection of Occult Carcinomatous Diffusion in Lymph Nodes from Head and Neck Squamous Cell Carcinoma Using Real-Time RT-PCR Detection of Cytokeratin 19 MRNA. Br. J. Cancer 2006, 94, 1164–1169. [Google Scholar] [CrossRef]
- Dhawan, I.; Sandhu, S. V; Bhandari, R.; Sood, N.; Bhullar, R.K.; Sethi, N. Detection of Cervical Lymph Node Micrometastasis and Isolated Tumor Cells in Oral Squamous Cell Carcinoma Using Immunohistochemistry and Serial Sectioning. J. Oral Maxillofac. Pathol. 2016, 20, 436–444. [Google Scholar] [CrossRef]
- Barrera, J.E.; Miller, M.E.; Said, S.; Jafek, B.W.; Campana, J.P.; Shroyer, K.R. Detection of Occult Cervical Micrometastases in Patients with Head and Neck Squamous Cell Cancer. Laryngoscope 2003, 113, 892–896. [Google Scholar] [CrossRef]
- Hamed, M.; Samir, M.; Hamid, O.A.; El-Maraghy, M. Evaluation of Cytokeratin Tissue Marker in Detection of Metastatic Lymph Nodes in Cases of Laryngeal and Hypopharyngeal Carcinoma. Cancer Mol. Biol. 1996, 3, 955–960. [Google Scholar]
- Oka, R.; Nakashiro, K.-I.; Goda, H.; Tanaka, H.; Hamakawa, H. Identification of Novel Molecular Markers for Detecting Lymph Node Metastasis of Oral Squamous Cell Carcinoma. Cancer Res. 2012, 72. [Google Scholar] [CrossRef]
- Peigné, L.; Godey, F.; Le Gallo, M.; Le Gall, F.; Fautrel, A.; Morcet, J.; Jégoux, F. One-Step Nucleic Acid Amplification for Detecting Lymph Node Metastasis of Head and Neck Squamous Cell Carcinoma. Oral Oncol. 2020, 102. [Google Scholar] [CrossRef] [PubMed]
- Rhee, D.; Wenig, B.M.; Smith, R. V. The Significance of Immunohistochemically Demonstrated Nodal Micrometastases in Patients with Squamous Cell Carcinoma of the Head and Neck. Laryngoscope 2002, 112, 1970–1974. [Google Scholar] [CrossRef] [PubMed]
- Sakata, J.; Yamana, K.; Yoshida, R.; Matsuoka, Y.; Kawahara, K.; Arita, H.; Nakashima, H.; Nagata, M.; Hirosue, A.; Kawaguchi, S.; et al. Tumor Budding as a Novel Predictor of Occult Metastasis in CT2N0 Tongue Squamous Cell Carcinoma. Hum. Pathol. 2018, 76, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yamana, K.; Sakata, J.; Yoshida, R.; Gohara, S.; Kawaguchi, S.; Nagao, Y.; Arita, H.; Nakashima, H.; Matsuoka, Y.; Kawahara, K.; et al. Tumor Budding Is a Predict Marker of Occult Node Metastasis and Prognosis in Patients with CT2N0 TSCC. Cancer Sci. 2018, 109. [Google Scholar]
- Nagvekar, S.; Spadigam, A.; Dhupar, A. Determining the Potential of Desmoglein 3 as a Sensitive and Specific Immunohistochemical Marker for the Detection of Micrometastasis in Patients with Primary Oral Squamous Cell Carcinoma. Contemp. Oncol. (Poznan, Poland) 2016, 20, 374–380. [Google Scholar] [CrossRef]
- Patel, V.; Martin, D.; Malhotra, R.; Marsh, C.A.; Doçi, C.L.; Veenstra, T.D.; Nathan, C.-A.O.; Sinha, U.K.; Singh, B.; Molinolo, A.A.; et al. DSG3 as a Biomarker for the Ultrasensitive Detection of Occult Lymph Node Metastasis in Oral Cancer Using Nanostructured Immunoarrays. Oral Oncol. 2013, 49, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, H.; Moreau, F.; Lefèvre, M.; Tam, C.; Périé, S.; Soussan, P.; St Guily, J.L. Human Papillomavirus Type 16 Oropharyngeal Cancers in Lymph Nodes as a Marker of Metastases. Arch. Otolaryngol. Head. Neck Surg. 2011, 137, 910–914. [Google Scholar] [CrossRef]
- Mirghani, H.; Ferchiou, M.; Moreau, F.; Vourexakis, Z.; Amen, F.; Breuskin, I.; Lefèvre, M.; Casiraghi, O.; Drusch, F.; Soussan, P.; et al. Oropharyngeal Cancers: Significance of HPV16 Detection in Neck Lymph Nodes. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2013, 57, 120–124. [Google Scholar] [CrossRef]
- Lukens, J.N.; Pustylnikov, S.; Montone, K.; Lin, A.; Swisher-McClure, S.D.; Ghiam, A.F.; Weinstein, G.S.; Cohen, R.; Facciabene, A. Tumor Infiltrating Lymphocytes in Occult Primary HPV+ Oropharyngeal Squamous Cell Carcinoma (OPSCC): Comparison of the Primary Tumor and Regional Lymph Node Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, E425–E426. [Google Scholar] [CrossRef]
- Trivedi, N.P.; Ravindran, H.K.; Sundram, S.; Iyer, S.; Kekatpure, V.; Durah, S.; Kuriakose, M.A. Pathologic Evaluation of Sentinel Lymph Nodes in Oral Squamous Cell Carcinoma. Head Neck 2010, 32, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Bugter, O.; Aaboubout, Y.; Algoe, M.; de Bruijn, H.S.; Keereweer, S.; Sewnaik, A.; Monserez, D.A.; Koljenović, S.; Hardillo, J.A.U.; Robinson, D.J.; et al. Detecting Head and Neck Lymph Node Metastases with White Light Reflectance Spectroscopy; a Pilot Study. Oral Oncol. 2021, 123, 105627. [Google Scholar] [CrossRef] [PubMed]
- Cebeci, S.; Aydos, U.; Yeniceri, A.; Pula, D.; Duzlu, M.; Atay, L.O.; Yilmaz, M. Diagnostic Performance of FDG PET/MRI for Cervical Lymph Node Metastasis in Patients with Clinically N0 Head and Neck Cancer. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 4528–4535. [Google Scholar] [CrossRef] [PubMed]
- Rosko, A.; Birkeland, A.; Shuman, A.; Prince, M.; Bradford, C.; Wolf, G.; Worden, F.; Eisbruch, A.; Srinivasan, A.; Wong, K.K.; et al. Positron Emission Tomography-CT Prediction of Occult Nodal Metastasis in Recurrent Laryngeal Cancer. Head Neck 2017, 39, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Coletta, R.D.; Bufalino, A.; Sobral, L.M.; Rodrigues, P.C.; Graner, E.; Kowalski, L.P.; Salo, T. Activin A Regulates Cell Interactions in the Microenvironment of Oral Squamous Cell Carcinomas. Cancer Res. 2015, 75. [Google Scholar] [CrossRef]
- Kelner, N.; Rodrigues, P.C.P.C.; Bufalino, A.; Fonseca, F.P.F.P.; Santos-Silva, A.R. dos; Miguel, M.C.C.M.C.C.; Pinto, C.A.L.C.A.L.; Leme, A.F.P.A.F.P.; Graner, E.; Salo, T.; et al. Activin A Immunoexpression as Predictor of Occult Lymph Node Metastasis and Overall Survival in Oral Tongue Squamous Cell Carcinoma. Head Neck 2015, 37, 479–486. [Google Scholar] [CrossRef]
- Coletta, R.; Rodrigues, P.; Kelner, N.; Bufalino, A.; Fonseca, F.; Santos- Silva, A.; Kowalski, L.P.; Salo, T.; Graner, E. Activin A Immunoexpression Is Useful to Predict Occult Lymph Node Metastasis and Overall Survival in Oral Tongue Squamous Cell Carcinoma. Virchows Arch. 2013, 463, 116. [Google Scholar] [CrossRef] [PubMed]
- Capaccio, P.; Pruneri, G.; Carboni, N.; Pagliari, A.V.; Quatela, M.; Cesana, B.M.; Pignataro, L. Cyclin D1 Expression Is Predictive of Occult Metastases in Head and Neck Cancer Patients with Clinically Negative Cervical Lymph Nodes. Head Neck 2000, 22, 234–240. [Google Scholar] [CrossRef]
- Myo, K.; Uzawa, N.; Miyamoto, R.; Sonoda, I.; Yuki, Y.; Amagasa, T. Cyclin D1 Gene Numerical Aberration Is a Predictive Marker for Occult Cervical Lymph Node Metastasis in TNM Stage I and II Squamous Cell Carcinoma of the Oral Cavity. Cancer 2005, 104, 2709–2716. [Google Scholar] [CrossRef]
- Ahmed, R.A.; Shawky, A.E.-A.; Hamed, R.H. Prognostic Significance of Cyclin D1 and E-Cadherin Expression in Laryngeal Squamous Cell Carcinoma. Pathol. Oncol. Res. 2014, 20, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Sticht, C.; Hofele, C.; Flechtenmacher, C.; Bosch, F.X.X.; Freier, K.; Lichter, P.; Joos, S. Amplification of Cyclin L1 Is Associated with Lymph Node Metastases in Head and Neck Squamous Cell Carcinoma (HNSCC). Br. J. Cancer 2005, 92, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Harada, H.; Omura, K.; Nakajima, Y.; Hasegawa, S.; Mogi, S. Cyclin B1 Is Useful to Predict Occult Cervical Lymph Node Metastases in Tongue Carcinoma. J. Exp. Clin. Cancer Res. 2006, 25, 351–356. [Google Scholar] [PubMed]
- Rosado, P.; Lequerica-Fernández, P.; Fernández, S.; Allonca, E.; Villallaín, L.; De Vicente, J.C. E-Cadherin and β-Catenin Expression in Well-Differentiated and Moderately-Differentiated Oral Squamous Cell Carcinoma: Relations with Clinical Variables. Br. J. Oral Maxillofac. Surg. 2013, 51, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Bayazit, Y.; Bakir, K.; Ucak, R.; Mumbuc, S.; Ozer, E.; Kanlikama, M. Clinical and Histopathological Correlates of the Proliferative Activity in Squamous Cell Laryngeal Carcinoma. Rev. Laryngol. Otol. Rhinol. (Bord). 2002, 123, 43–46. [Google Scholar]
- Keum, K.C.K.C.; Chung, E.J.E.J.; Koom, W.S.W.S.; Cho, J.H.J.H.; Cho, S.H.S.H.; Choi, E.C.E.C.; Lee, C.G.C.G.; Suh, C.O.C.O.; Kim, G.E.G.E. Predictive Value of P53 and PCNA Expression for Occult Neck Metastases in Patients with Clinically Node-Negative Oral Tongue Cancer. Otolaryngol. neck Surg. Off. J. Am. Acad. Otolaryngol. Neck Surg. 2006, 135, 858–864. [Google Scholar] [CrossRef] [PubMed]
- van Kempen, P.M.W.; Noorlag, R.; Braunius, W.W.; Moelans, C.B.; Rifi, W.; Savola, S.; Koole, R.; Grolman, W.; van Es, R.J.J.; Willems, S.M. Clinical Relevance of Copy Number Profiling in Oral and Oropharyngeal Squamous Cell Carcinoma. Cancer Med. 2015, 4, 1525–1535. [Google Scholar] [CrossRef] [PubMed]
- Thangaraj, S.V.S.V.; Shyamsundar, V.; Krishnamurthy, A.; Ramshankar, V. Deregulation of Extracellular Matrix Modeling with Molecular Prognostic Markers Revealed by Transcriptome Sequencing and Validations in Oral Tongue Squamous Cell Carcinoma. Sci. Rep. 2021, 11, 250. [Google Scholar] [CrossRef]
- Clausen, M.J.A.M.; Melchers, L.J.; De Bruin, L.B.; Mastik, M.F.; Slagter-Menkema, L.; Groen, H.J.M.; Van Der Vegt, B.; Van Der Laan, B.F.A.M.; De Meyer, T.; Van Criekinge, W.; et al. Discovery of DNA Methylation Markers That Predict Nodal Metastases in Oral Squamous Cell Carcinoma. Oral Oncol. 2013, 49, S5. [Google Scholar] [CrossRef]
- Idel, C.; Ribbat-Idel, J.; Kuppler, P.; Krupar, R.; Offermann, A.; Vogel, W.; Rades, D.; Kirfel, J.; Wollenberg, B.; Perner, S. EVI1 as a Marker for Lymph Node Metastasis in HNSCC. Int. J. Mol. Sci. 2020, 21. [Google Scholar] [CrossRef]
- Lourenc¸o, S.; Silami, M.; Camisasca, D.; Diblasi, E.; Fonseca, E.; Faria, P.; Dias, F. Expression of Chemokine Receptor CCR7 in Oral Squamous Cell Carcinoma with and without Cervical Metastasis. Eur. J. Cancer 2012, 48, S266. [Google Scholar] [CrossRef]
- Mizdrak, I.; Mizdrak, M.; Racetin, A.; Bošković, B.; Benzon, B.; Durdov, M.G.; Vukojević, K.; Filipović, N. Expression of Connexins 37, 40 and 45, Pannexin 1 and Vimentin in Laryngeal Squamous Cell Carcinomas. Genes (Basel). 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, J.P.; Domínguez, F.; Alvarez, C.; Manrique, C.; Herrero, A.; Suárez, C. Expression of E-Cadherin in Squamous Cell Carcinomas of the Supraglottic Larynx with Correlations to Clinicopathological Features. Eur. J. Cancer 2002, 38, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Mollaoglu, N.; Vairaktaris, E.; Nkenke, E.; Neukam, F.W.; Ries, J. Expression of MAGE-A12 in Oral Squamous Cell Carcinoma. Dis. Markers 2008, 24, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Faustino, S.E.S.; Oliveira, D.T.; Nonogaki, S.; Landman, G.; Carvalho, A.L.; Kowalski, L.P. Expression of Vascular Endothelial Growth Factor-C Does Not Predict Occult Lymph-Node Metastasis in Early Oral Squamous Cell Carcinoma. Int. J. Oral Maxillofac. Surg. 2008, 37, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Van Den Berg, N. Feasibility of Panitumumab-IRDye800 for Metastatic Lymph Node Identification in Patients with Head-and-Neck Squamous Cell Carcinoma. Mol. Imaging Biol. 2017, 19, S515. [Google Scholar] [CrossRef]
- Krishnan, G.; van den Berg, N.S.; Nishio, N.; Juniper, G.; Pei, J.; Zhou, Q.; Lu, G.; Lee, Y.-J.; Ramos, K.; Iagaru, A.H.; et al. Metastatic and Sentinel Lymph Node Mapping Using Intravenously Delivered Panitumumab-IRDye800CW. Theranostics 2021, 11, 7188–7198. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, P.M.; Merkley, M.; Jackson, L.; Dynan, W.S. Overexpression of Cornulin in Histologically Normal Adjacent Tissue Predicts Occult Nodal Metastases in Head and Neck Cancer Patients. Cancer Res. 2010, 70. [Google Scholar] [CrossRef]
- Wang, S.; Fan, H.; Xu, J.; Zhao, E. Prognostic Implication of NOTCH1 in Early Stage Oral Squamous Cell Cancer with Occult Metastases. Clin. Oral Investig. 2018, 22, 1131–1138. [Google Scholar] [CrossRef]
- Park, J.-O.; Jung, C.-K.; Sun, D.-I.; Joo, Y.-H.; Kim, M.-S. Relationships between Metastasis-Associated Protein (MTA) 1 and Lymphatic Metastasis in Tonsil Cancer. Eur. Arch. oto-rhino-laryngology Off. J. Eur. Fed. Oto-Rhino-Laryngological Soc. Affil. with Ger. Soc. Oto-Rhino-Laryngology - Head Neck Surg. 2011, 268, 1329–1334. [Google Scholar] [CrossRef]
- Nair, S.; Malgundkar, S.; Patil, A.; Kane, S.; Sadhana, K.; D’Cruz, A.; Zingde, S. Proteomic Markers in Early Buccal Mucosa Squamous Cell Cancers. Eur. J. Cancer 2013, 49, S26. [Google Scholar] [CrossRef]
- Rodrigo, J.P.; Dominguez, F.; Suárez, V.; Canel, M.; Secades, P.; Chiara, M.D. Focal Adhesion Kinase and E-Cadherin as Markers for Nodal Metastasis in Laryngeal Cancer. Arch. Otolaryngol. Head. Neck Surg. 2007, 133, 145–150. [Google Scholar] [CrossRef]
- Parikh, A.S.A.S.; Puram, S.V.S. V; Faquin, W.C.W.C.; Richmon, J.D.J.D.; Emerick, K.S.K.S.; Deschler, D.G.D.G.; Varvares, M.A.M.A.; Tirosh, I.; Bernstein, B.E.B.E.; Lin, D.T.D.T. Immunohistochemical Quantification of Partial-EMT in Oral Cavity Squamous Cell Carcinoma Primary Tumors Is Associated with Nodal Metastasis. Oral Oncol. 2019, 99, 104458. [Google Scholar] [CrossRef]
- Miyaguchi, K.; Uzawa, N.; Mogushi, K.; Takahashi, K.-I.; Michikawa, C.; Nakata, Y.; Sumino, J.; Okada, N.; Mizushima, H.; Fukuoka, Y.; et al. Loss of NKX3-1 as a Potential Marker for an Increased Risk of Occult Lymph Node Metastasis and Poor Prognosis in Oral Squamous Cell Carcinoma. Int. J. Oncol. 2012, 40, 1907–1914. [Google Scholar] [CrossRef]
- Yang, X.; Wu, K.; Li, S.; Hu, L.; Han, J.; Zhu, D.; Tian, X.; Liu, W.; Tian, Z.; Zhong, L.; et al. MFAP5 and TNNC1: Potential Markers for Predicting Occult Cervical Lymphatic Metastasis and Prognosis in Early Stage Tongue Cancer. Oncotarget 2017, 8, 2525–2535. [Google Scholar] [CrossRef]
- Uma, R.S.R.S.; Naresh, K.N.K.N.; D’Cruz, A.K.A.K.; Mulherkar, R.; Borges, A.M.A.M. Metastasis of Squamous Cell Carcinoma of the Oral Tongue Is Associated with Down-Regulation of Epidermal Fatty Acid Binding Protein (E-FABP). Oral Oncol. 2007, 43, 27–32. [Google Scholar] [CrossRef]
- Allegra, E.; Puzzo, L.; Zuccalà, V.; Trapasso, S.; Vasquez, E.; Garozzo, A.; Caltabiano, R. Nuclear BMI-1 Expression in Laryngeal Carcinoma Correlates with Lymph Node Pathological Status. World J. Surg. Oncol. 2012, 10, 206. [Google Scholar] [CrossRef]
- Huber, G.F.G.F.; Fritzsche, F.R.F.R.; Züllig, L.; Storz, M.; Graf, N.; K. Haerle, S.; Jochum, W.; Stoeckli, S.J.S.J.; Moch, H.; Haerle, S.K.; et al. Podoplanin Expression Correlates with Sentinel Lymph Node Metastasis in Early Squamous Cell Carcinomas of the Oral Cavity and Oropharynx. Int. J. cancer 2011, 129, 1404–1409. [Google Scholar] [CrossRef]
- Iype, E.M.; Balakrishnan, L.S.R. Selected Molecular Markers as Indicators of Clinical Profile, Tumor Characteristics and Treatment Outcome in Squamous Cell Carcinoma of the Larynx. J. Clin. Oncol. 2019, 37. [Google Scholar] [CrossRef]
- Meler-Claramonte, C.; Avilés-Jurado, F.X.; Vilaseca, I.; Terra, X.; Bragado, P.; Fuster, G.; Vintró, X.L.; Camacho, M. Semaphorin-3F/Neuropilin-2 Transcriptional Expression as a Predictive Biomarker of Occult Lymph Node Metastases in HNSCC. Cancers (Basel). 2022, 14. [Google Scholar] [CrossRef]
- Sparano, A.; Weinstein, G.; Chalian, A.; Yodul, M.; Weber, R. Multivariate Predictors of Occult Neck Metastasis in Early Oral Tongue Cancer. Otolaryngol. - Head Neck Surg. 2004, 131, 472–476. [Google Scholar] [CrossRef]
- Chandler, K.; Vance, C.; Budnick, S.; Muller, S. Muscle Invasion in Oral Tongue Squamous Cell Carcinoma as a Predictor of Nodal Status and Local Recurrence: Just as Effective as Depth of Invasion? Head Neck Pathol. 2011, 5, 359–363. [Google Scholar] [CrossRef]
- Hori, Y.; Kubota, A.; Yokose, T.; Furukawa, M.; Matsushita, T.; Takita, M.; Mitsunaga, S.; Mizoguchi, N.; Nonaka, T.; Nakayama, Y.; et al. Predictive Significance of Tumor Depth and Budding for Late Lymph Node Metastases in Patients with Clinical N0 Early Oral Tongue Carcinoma. Head Neck Pathol. 2017, 11, 477–486. [Google Scholar] [CrossRef]
- Sakai, T.; Saito, Y.; Tateishi, Y.; Yamazawa, S.; Fukuoka, O.; Kobayashi, K.; Omura, G.; Akashi, K.; Yoshida, M.; Ando, M.; et al. Tumor–Stroma Ratio Can Predict Lymph-Node Metastasis in CT1/2N0 Oral Tongue Squamous Cell Carcinoma Independent of Tumor Budding Grade. Int. J. Clin. Oncol. 2022, 27, 1818–1827. [Google Scholar] [CrossRef]
- Luksic, I.; Suton, P.; Manojlovic, S.; Virag, M.; Petrovecki, M.; Macan, D. Significance of Myofibroblast Appearance in Squamous Cell Carcinoma of the Oral Cavity on the Occurrence of Occult Regional Metastases, Distant Metastases, and Survival. Int. J. Oral Maxillofac. Surg. 2015, 44, 1075–1080. [Google Scholar] [CrossRef]
- Choi, K.; Park, S.; Kim, J.; Medicine, D.L.-; 2021, undefined The Occult Nodal Metastasis Rate of Early Tongue Cancer (T1–T2): A Protocol for a Systematic Review and Meta-Analysis. journals.lww.com.
- Stögbauer, F.; Beck, S.; Ourailidis, I.; Hess, J.; Poremba, C.; Lauterbach, M.; Wollenberg, B.; Buchberger, A.M.S.; Jesinghaus, M.; Schirmacher, P.; et al. Tumour Budding-Based Grading as Independent Prognostic Biomarker in HPV-Positive and HPV-Negative Head and Neck Cancer. Br. J. Cancer 2023, 128, 2295–2306. [Google Scholar] [CrossRef]
- Velosa, C.; Shi, Q.; Stevens, T.M.; Chiosea, S.I.; Purgina, B.; Carroll, W.; Rosenthal, E.; Morlandt, A.; Loree, T.; Brandwein-Weber, M.S. Worst Pattern Of Invasion and Occult Cervical Metastases for Oral Squamous Carcinoma. Head Neck 2017. [Google Scholar] [CrossRef]
- Jesinghaus, M.; Steiger, K.; Stögbauer, F.; Haller, B.; Kolk, A.; Straßen, U.; Pickhard, A.; Wirth, M.; Silva, M.; Budczies, J.; et al. Pre-Operative Cellular Dissociation Grading in Biopsies Is Highly Predictive of Post-Operative Tumour Stage and Patient Outcome in Head and Neck Squamous Cell Carcinoma. Br. J. Cancer 2020, 122, 835–846. [Google Scholar] [CrossRef]
- Kwon, M.; Moon, H.; Nam, S.Y.; Lee, J.H.; Kim, J.W.; Lee, Y.-S.; Roh, J.-L.; Choi, S.-H.; Kim, S.-Y. Clinical Significance of Three-Dimensional Measurement of Tumour Thickness on Magnetic Resonance Imaging in Patients with Oral Tongue Squamous Cell Carcinoma. Eur. Radiol. 2016, 26, 858–865. [Google Scholar] [CrossRef] [PubMed]
- Chandra, P.; Dhake, S.; Agrawal, A.; Shah, S.; Purandare, N.; Rangarajan, V.; Dutta, S.; Chaturvedi, P. Does SPECT/CT Offer Incremental Benefit over Planar Lympho-Scintigraphy in Sentinel Node Biopsies in Oral Cavity Squamous Cell Carcinomas? Indian J. Nucl. Med. 2015, 30, S19. [Google Scholar]
- Xu, C.; Li, H.; Seng, D.; Liu, F. Significance of SUV Max for Predicting Occult Lymph Node Metastasis and Prognosis in Early-Stage Tongue Squamous Cell Carcinoma. J. Oncol. 2020, 2020, 6241637. [Google Scholar] [CrossRef]
- Kuźmińska, M.; Osuch-Wójcikiewicz, E.; Fronczewska-Wieniawska, K.; Królicki, L.; Niemczyk, K. Usefulness of 18F-FDG PET/CT examination in the diagnosis of head and neck cancer - Preliminary results. Otolaryngol. Pol. 2011, 65, 17–21. [Google Scholar] [CrossRef]
- Norling, R.; Buron, B.M.D.; Therkildsen, M.H.; Henriksen, B.M.; Von Buchwald, C.; Nielsen, M.B. Staging of Cervical Lymph Nodes in Oral Squamous Cell Carcinoma: Adding Ultrasound in Clinically Lymph Node Negative Patients May Improve Diagnostic Work-Up. PLoS One 2014, 9. [Google Scholar] [CrossRef]
- Cvorović, L.; Milutinović, Z.; Strbac, M.; Markovski, S. What Is Important for Ultrasound Evaluation of Occult Metastatic Lymph Nodes in Laryngeal Cancer: Size, Shape, Vascularity or Cytological Findings? ORL. J. Otorhinolaryngol. Relat. Spec. 2007, 69, 172–175. [Google Scholar] [CrossRef]
- Huber, G.F.G.F.; Züllig, L.; Soltermann, A.; Roessle, M.; Graf, N.; Haerle, S.K.S.K.; Studer, G.; Jochum, W.; Moch, H.; Stoeckli, S.J.S.J. Down Regulation of E-Cadherin (ECAD) - a Predictor for Occult Metastatic Disease in Sentinel Node Biopsy of Early Squamous Cell Carcinomas of the Oral Cavity and Oropharynx. BMC Cancer 2011, 11, 1–8. [Google Scholar] [CrossRef]
- Sadeghirad, H.; Monkman, J.; Mehdi, A.M.; Ladwa, R.; O’Byrne, K.; Hughes, B.G.M.B.G.M.; Kulasinghe, A.; O’Byrne, K.; Hughes, B.G.M.B.G.M.; Kulasinghe, A. Dissecting Tissue Compartment-Specific Protein Signatures in Primary and Metastatic Oropharyngeal Squamous Cell Carcinomas. Front. Immunol. 2022, 13, 895513. [Google Scholar] [CrossRef]
- Boonkitticharoen, V.; Kulapaditharom, B.; Leopairut, J.; Kraiphibul, P.; Larbcharoensub, N.; Cheewaruangroj, W.; Chintrakarn, C.; Pochanukul, L. Vascular Endothelial Growth Factor a and Proliferation Marker in Prediction of Lymph Node Metastasis in Oral and Pharyngeal Squamous Cell Carcinoma. Arch. Otolaryngol. Head. Neck Surg. 2008, 134, 1305–1311. [Google Scholar] [CrossRef]
- El-Mofty, S.K.; Zhang, M.Q.; Davila, R.M. Histologic Identification of Human Papillomavirus (HPV)-Related Squamous Cell Carcinoma in Cervical Lymph Nodes: A Reliable Predictor of the Site of an Occult Head and Neck Primary Carcinoma. Head Neck Pathol. 2008, 2, 163–168. [Google Scholar] [CrossRef]
- Kitkumthorn, N.; Keelawat, S.; Rattanatanyong, P.; Mutirangura, A. LINE-1 and Alu Methylation Patterns in Lymph Node Metastases of Head and Neck Cancers. Asian Pacific J. Cancer Prev. 2012, 13, 4469–4475. [Google Scholar] [CrossRef]
- Cortesina, G.; Martone, T.; Galeazzi, E.; Olivero, M.; De Stefani, A.; Bussi, M.; Valente, G.; Comoglio, P.M.M.; Di Renzo, M.F.F. Staging of Head and Neck Squamous Cell Carcinoma Using the MET Oncogene Product as Marker of Tumor Cells in Lymph Node Metastases. Int. J. cancer 2000, 89, 286–292. [Google Scholar] [CrossRef]
- Zevallos, J.P.J.P.; Mazul, A.L.A.L.; Walter, V.; Hayes, D.N.D.N. Gene Expression Subtype Predicts Nodal Metastasis and Survival in Human Papillomavirus-Negative Head and Neck Cancer. Laryngoscope 2019, 129, 154–161. [Google Scholar] [CrossRef]
- Salzano, G.; Perri, F.; Maglitto, F.; Togo, G.; De Fazio, G.R.; Apolito, M.; Calabria, F.; Laface, C.; Vaira, L.A.; Committeri, U.; et al. Pre-Treatment Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios as Predictors of Occult Cervical Metastasis in Clinically Negative Neck Supraglottic and Glottic Cancer. J. Pers. Med. 2021, 11. [Google Scholar] [CrossRef]
- Abbate, V.; Dell’Aversana Orabona, G.; Salzano, G.; Bonavolontà, P.; Maglitto, F.; Romano, A.; Tarabbia, F.; Turri-Zanoni, M.; Attanasi, F.; Di Lauro, A.E.; et al. Pre-Treatment Neutrophil-to-Lymphocyte Ratio as a Predictor for Occult Cervical Metastasis in Early Stage (T1-T2 CN0) Squamous Cell Carcinoma of the Oral Tongue. Surg. Oncol. 2018, 27, 503–507. [Google Scholar] [CrossRef]
- Ventura, E.; Barros, J.; Salgado, I.; Millán, A.; Vilares, M.; Zagalo, C.; Gomes, P. Pretreatment Blood Markers in the Prediction of Occult Neck Metastasis: A 10-Year Retrospective Study. Cureus 2021, 13, e16641. [Google Scholar] [CrossRef]
- Salzano, G.; Dell’Aversana Orabona, G.; Abbate, V.; Vaira, L.A.; Committeri, U.; Bonavolontà, P.; Piombino, P.; Maglitto, F.; Russo, C.; Russo, D.; et al. The Prognostic Role of the Pre-Treatment Neutrophil to Lymphocyte Ratio (NLR) and Tumor Depth of Invasion (DOI) in Early-Stage Squamous Cell Carcinomas of the Oral Tongue. Oral Maxillofac. Surg. 2022, 26, 21–32. [Google Scholar] [CrossRef]
- Qayyumi, B.; Bharde, A.; Aland, G.; D’Souza, A.; Jayant, S.; Singh, N.; Tripathi, S.; Badave, R.; Kale, N.; Singh, B.; et al. Circulating Tumor Cells as a Predictor for Poor Prognostic Factors and Overall Survival in Treatment Naïve Oral Squamous Cell Carcinoma Patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2022, 134, 73–83. [Google Scholar] [CrossRef]
- Anderson, Y.; Wong, M.H.; Clayburgh, D. Circulating Hybrid Cells as a Marker of Nodal Metastases in Oral Cavity Squamous Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 1125–1126. [Google Scholar] [CrossRef]
- Henn, T.E.; Anderson, A.N.; Hollett, Y.R.; Sutton, T.L.; Walker, B.S.; Swain, J.R.; Sauer, D.A.; Clayburgh, D.R.; Wong, M.H. Circulating Hybrid Cells Predict Presence of Occult Nodal Metastases in Oral Cavity Carcinoma. Head Neck 2021, 43, 2193–2201. [Google Scholar] [CrossRef]
- Capone, R.B.B.; Pai, S.I.I.; Koch, W.M.M.; Gillison, M.L.L.; Danish, H.N.N.; Westra, W.H.H.; Daniel, R.; Shah, K.V. V; Sidransky, D. Detection and Quantitation of Human Papillomavirus (HPV) DNA in the Sera of Patients with HPV-Associated Head and Neck Squamous Cell Carcinoma. Clin. cancer Res. an Off. J. Am. Assoc. Cancer Res. 2000, 6, 4171–4175. [Google Scholar]
- Mermod, M.; Bongiovanni, M.; Petrova, T.; Goun, E.; Simon, C.; Tolstonog, G.; Monnier, Y. Prediction of Occult Lymph Node Metastasis in Head and Neck Cancer with CD31 Vessel Quantification. Otolaryngol. neck Surg. Off. J. Am. Acad. Otolaryngol. Neck Surg. 2019, 160, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Wollenberg, B.; Walz, A.; Kolbow, K.; Pauli, C.; Chaubal, S.; Andratschke, M. Clinical Relevance of Circulating Tumour Cells in the Bone Marrow of Patients with SCCHN. Onkologie 2004, 27, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Elsheikh, M.N.; Rinaldo, A.; Hamakawa, H.; Mahfouz, M.E.; Rodrigo, J.P.; Brennan, J.; Devaney, K.O.; Grandis, J.R.; Ferlito, A. Importance of Molecular Analysis in Detecting Cervical Lymph Node Metastasis in Head and Neck Squamous Cell Carcinoma. Head Neck 2006, 28, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Rhee, D.; Wenig, B.M.; Smith, R. V The Significance of Immunohistochemically Demonstrated Nodal Micrometastases in Patients with Squamous Cell Carcinoma of the Head and Neck. Laryngoscope 2002, 112, 1970–1974. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, J.P.; Shah, J.P.; Silver, C.E.; Medina, J.E.; Takes, R.P.; Robbins, K.T.; Rinaldo, A.; Werner, J.A.; Ferlito, A. Management of the Clinically Negative Neck in Early-Stage Head and Neck Cancers after Transoral Resection. Head Neck 2011, 33, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, J.B.; Christensen, R.K.; Sørensen, J.A.; Krogdahl, A. Sentinel Lymph Nodes in Cancer of the Oral Cavity: Is Central Step-Sectioning Enough? J. Oral Pathol. Med. 2007, 36, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Kligerman, J.; Lima, R.A.; Soares, J.R.; Prado, L.; Dias, F.L.; Freitas, E.Q.; Olivatto, L.O. Supraomohyoid Neck Dissection in the Treatment of T1/T2 Squamous Cell Carcinoma of Oral Cavity. Am. J. Surg. 1994, 168, 391–394. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, A.C.; Maia, D.C.C.; Horst, M.A.; Carvalho, A.L.; Scapulatempo-Neto, C.; Vettore, A.L. Concord Ance of Pathologic Examination and QRT-PCR for MicroRNA Expressi on in Lymph Nodes from Oral Squamous Cell Carcinoma Patients. Oral Oncol. 2013, 49, S104–S105. [Google Scholar] [CrossRef]
- Farlow, J.L.; Birkeland, A.C.; Rosko, A.J.; VanKoevering, K.; Haring, C.T.; Smith, J.D.; Brenner, J.C.; Shuman, A.G.; Chinn, S.B.; Stucken, C.L.; et al. Elective Paratracheal Lymph Node Dissection in Salvage Laryngectomy. Ann. Surg. Oncol. 2019, 26, 2542–2548. [Google Scholar] [CrossRef] [PubMed]
- Shih, H.; Khanna, M.; Thomas, J.; Gazala, F.; El-Hakim, M. DEPTH OF INVASION CUTOFF FOR RECOMMENDING ELECTIVE NECK DISSECTION IN ORAL SQUAMOUS CELL CARCINOMA. Int. J. Oral Maxillofac. Surg. 2024, 52, 185. [Google Scholar] [CrossRef]
- Masood, M.M.; Farquhar, D.R.; Vanleer, J.P.; Patel, S.N.; Hackman, T.G. Depth of Invasion on Pathological Outcomes in Clinical Low-Stage Oral Tongue Cancer Patients. Oral Dis. 2018, 24, 1198–1203. [Google Scholar] [CrossRef]
- Aaboubout, Y.; van der Toom, Q.M.Q.M.; de Ridder, M.A.J.M.A.J.; De Herdt, M.J.M.J.; van der Steen, B.; van Lanschot, C.G.F.C.G.F.; Barroso, E.M.E.M.; Nunes Soares, M.R.; ten Hove, I.; Mast, H.; et al. Is the Depth of Invasion a Marker for Elective Neck Dissection in Early Oral Squamous Cell Carcinoma? Front. Oncol. 2021, 11, 628320. [Google Scholar] [CrossRef] [PubMed]
- Chien, C.-Y.; Wang, C.P.; Lee, L.-Y.; Lee, S.-R.; Ng, S.-H.; Kang, C.-J.; Lin, J.-C.; Terng, S.-D.; Hua, C.-H.; Chen, T.-M.; et al. Indications for Elective Neck Dissection in CT1N0M0 Oral Cavity Cancer According to the AJCC Eight Edition: A Nationwide Study. Oral Oncol. 2023, 140. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA Flow diagram.
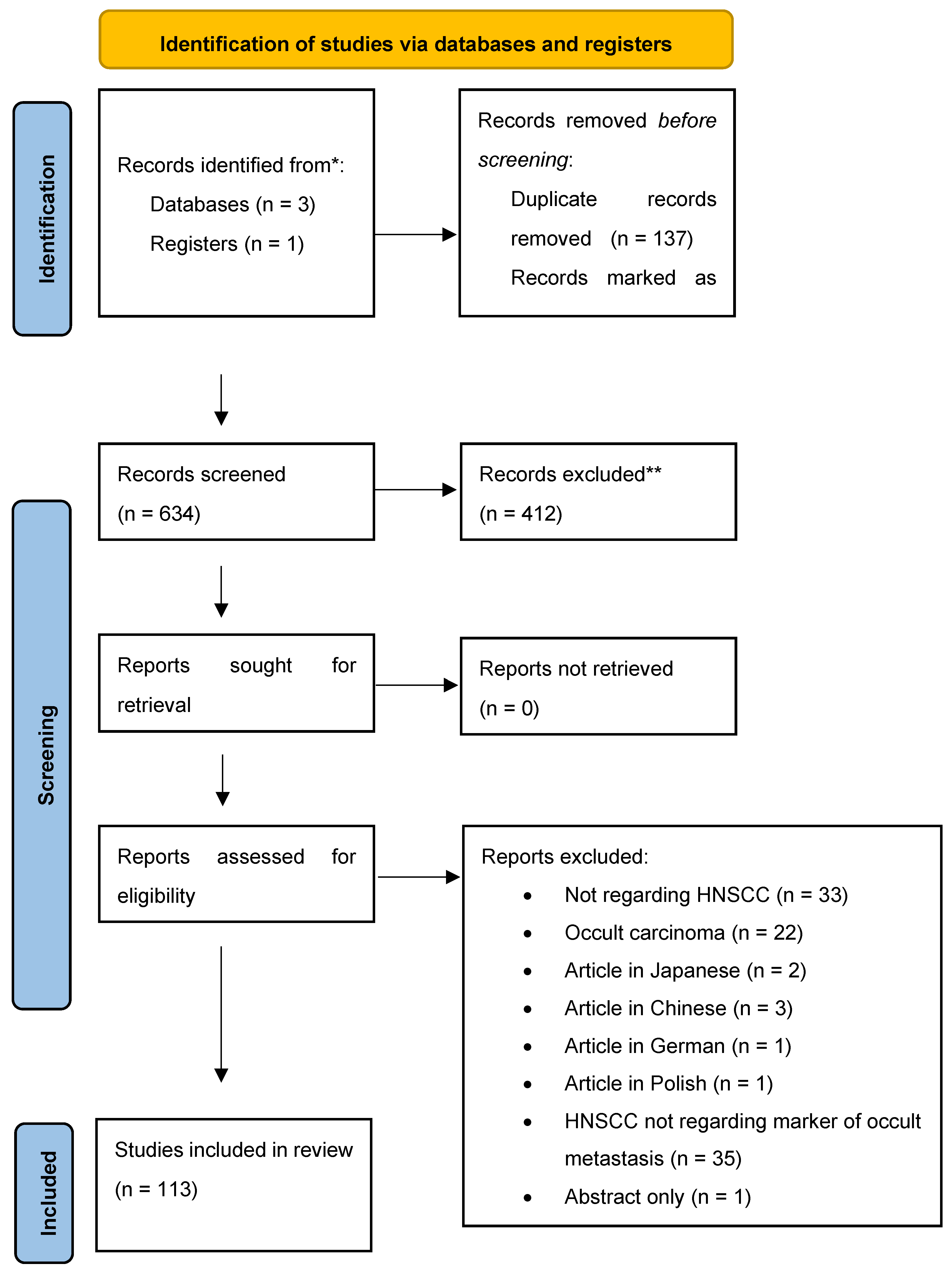

Table 1.
Articles considered for review.
| Title | Year | Authors | Journal | Doi | Population | Subsites | Material | Results | P Value |
|---|---|---|---|---|---|---|---|---|---|
| Evaluation of cytokeratin tissue marker in detection of metastatic lymph nodes in cases of laryngeal and hypopharyngeal carcinoma | 1996 | Hamed M, Samir M, Hamid O et al. | Cancer Molecular Biology | 51 cases of laryngeal and hypopharyngeal carcinoma. | Laryngeal and hypopharyngeal carcinoma | Nodal specimens | Analysis of the percentage of occult metastases cases detected by cytokeratin immunostaining and missed by Haematoxilin and Eosin gave significant value | p > 0.001 | |
| Staging of head and neck squamous cell carcinoma using the MET oncogene product as marker of tumor cells in lymph node metastases. | 2000 | Cortesina G, Martone T, Galeazzi E et al. | International journal of cancer | 10.1002/1097-0215(20000520)89:3<286::AID-IJC12>3.0.CO;2-U | 20 patients with HNSCC | HNSCC | Nodal specimens | MET- encoded sequences were found in 61 of 151 nodes (40%), of which 24 (16%) were found metastatic by in-depth histopathology. Western blot analysis demonstrated the presence of the full-size MET receptor in primary tumors and lymph node metastases: immunohistochemistry showed receptor localization in tumor cells. | |
| Detection and quantitation of human papillomavirus (HPV) DNA in the sera of patients with HPV-associated head and neck squamous cell carcinoma. | 2000 | Capone R, Pai S, Koch W et al. | Clinical cancer research | 70 patients with HNSCC | HNSCC | Serum DNA extracts | Four of these patients with HPV-positive tumors later developed distant metastases, suggesting that HPV DNA in serum may represent occult hematogenous spread of cancer cells in this subset of patients. | ||
| Cyclin D1 expression is predictive of occult metastases in head and neck cancer patients with clinically negative cervical lymph nodes | 2000 | Capaccio P, Pruneri G, Carboni N et al. | Head and Neck | 10.1002/(SICI)1097-0347(200005)22:3<234::AID-HED5>3.0.CO;2-3 | 32 HNSCC patients with clinically and radiologically negative lymph nodes in whom metastatic involvement was subsequently demonstrated at histologic examination (pN+);Group of 64 head and neck cancer patients with histologically negative laterocervical lymph nodes (pN0) was used as control | HNSCC | Biopsy samples of lymph nodes | Cyclin D1 expression significantly correlated with the presence of occult lymph node metastases | p =0 .0007 |
| Detection of occult metastatic lymph nodes in the neck with gray-scale and power Doppler US. | 2001 | Wang Q, Takashima S, Takayama F et al. | Acta radiologica | 10.1080/028418501127346701 | 57 patients without wide echogenic hilum on GSUS that measured less than 10 mm in minimal axial diameter were prospectively studied | HNSCC | Findings of 69 pathologically verified cervical nodes (38 benign, 31 malignant) | Of the vascularity patterns, spotted or peripheral pattern had the highest accuracy (80%) with 61% sensitivity and 93% specificity. A combined criterion of the minimal axial diameter larger than 8 mm and spotted or peripheral pattern increased the accuracy to 82% and sensitivity to 77% but specificity decreased to 86%. | |
| The significance of immunohistochemically demonstrated nodal micrometastases in patients with squamous cell carcinoma of the head and neck | 2002 | Rhee D, Wenig B, Smith R | Laryngoscope | 10.1097/00005537-200211000-00011 | 10 patients with squamous cell carcinoma of the head and neck without conventional histological evidence of nodal metastases | HNSCC | Nodal specimens | Occult micrometastases were found in the lymph nodes 5 of 10 patients examined. There was no association between the site of primary tumor, or T stage, and the presence of occult metastases. | |
| Expression of E-cadherin in squamous cell carcinomas of the supraglottic larynx with correlations to clinicopathological features | 2002 | Rodrigo J, Domínguez F, Alvarez C et al. | European Journal of Cancer | 10.1016/S0959-8049(01)00399-9 | 101 primary carcinomas | Squamous cell carcinomas of the supraglottic larynx | Tissue samples | There was a significant correlation between decreased E-cadherin expression and the presence of nodal metastases | P=0.007 |
| Clinical and histopathological correlates of the proliferative activity in squamous cell laryngeal carcinoma. | 2002 | Bayazit Y, Bakir K, Ucak R et al. | Revue de laryngologie - otologie - rhinologie | 28 patients who were treated for LSCC | Laryngeal squamous cell carcinoma | Tissue samples | There was no association between the mean values of the proliferative markers, and N stage and T stage of the patients as well as laryngeal site of involvement | p > 0.05 | |
| Detection of occult cervical micrometastases in patients with head and neck squamous cell cancer | 2003 | Barrera J, Miller M, Said S et al. | Laryngoscope | 10.1097/00005537-200305000-00022 | 50 patients treated between 1992 and 2001 | HNSCC | 1012 lymph nodes | H&E-stained and cytokeratin-stained sections revealed occult nodal micrometastases in 3.8% of NO and 5% of N1 cases. Overall, 26 micrometastases were identified in NO and N1 patients, causing 29% of N0 patients and 45% of N1 patients to be upstaged. | |
| Multivariate Predictors of Occult Neck Metastasis in Early Oral Tongue Cancer | 2004 | Sparano A, Weinstein G, Chalian A et al. | Otolaryngology - Head and Neck Surgery | 10.1016/j.otohns.2004.04.008 | 45 clinically determined N0 patients (T1/T2) | Oral tongue cancer | Tissue samples | Independent correlates of positive occult neck metastasis included greater tumor thickness, greater depth of muscle invasion, T2 stage, poorly differentiated tumors, infiltrating-type invasion front, presence of perineural invasion, and presence of angiolymphatic invasion. | Greater tumor thickness (P = 0.01)Depth of muscle invasion (P = 0.01) T2 stage (P = 0.01)Poorly differentiated tumors (P = 0.007),Infiltrating-type invasion front (P = 0.03)Presence of perineural invasion (P = 0.001)Presence of angiolymphatic invasion (P = 0.005) |
| Clinical relevance of circulating tumour cells in the bone marrow of patients with SCCHN | 2004 | Wollenberg B, Walz A, Kolbow K et al. | Onkologie | 10.1159/000079088 | 176 patients suffering from SCCHN | HNSCC | Bone marrow aspirates | Single CK19-expressing tumour cells could be detected in the bone marrow of 30.7% of the patients. | |
| Clinical evaluation of a new molecular method for detection of micrometastases in head and neck squamous cell carcinoma | 2004 | Shores C, Yin X, Funkhouser W et al. | Archives of Otolaryngology - Head and Neck Surgery | 10.1001/archotol.130.8.937 | 35 consecutive patients | HNSCC | 153 cervical lymph nodes | Of 35 HNSCCs, 33 expressed CK 14 RNA, and 15 lymph nodes with routine pathologically positive metastasis were also positive for CK 14 RNA. 4 lymph nodes that were pathologically negative nodes were positive for CK 14 RT-PCR, with 2 containing metastases detected by semi-step sectioning. | |
| Basic and clinical studies on quantitative analysis of lymph node micrometastasis in oral cancer. | 2004 | Onishi A, Nakashiro K, Mihara M et al. | Oncology reports | 10 patients with oral cancer | Oral squamous cell carcinoma | 115 lymph nodes using real-time quantitative polymerase chain reaction (PCR) based on the expression of squamous cell carcinoma antigen (SCCA) and cytokeratin 13 (CK13) | Of 108 histologically metastasis-negative LNs, 19 (17.6%) expressed SCCA mRNA levels higher than the cut-off value. CK13 mRNA is not a suitable marker for the real-time PCR since it was detected frequently even in the control LNs | ||
| Cyclin D1 gene numerical aberration is a predictive marker for occult cervical lymph node metastasis in TNM Stage I and II squamous cell carcinoma of the oral cavity | 2005 | Myo K, Uzawa N, Miyamoto R et al. | Cancer | 10.1002/cncr.21491 | 45 patients with previously untreated TNM Stage I and II (T1-2N0M0) disease who had not undergone elective cervical lymph node dissection | Oral squamous cell carcinoma | Fluorescence in situ hybridization (FISH), using a BAC clone specific for CCND1, was performed on OSCC specimens obtained by fine-needle aspiration (FNA) biopsy | CCND1 numerical aberrations were observed in 15 of the 45 patients and were significantly associated with the presence of occult lymph node metastases | P < 0.001 |
| Amplification of Cyclin L1 is associated with lymph node metastases in head and neck squamous cell carcinoma (HNSCC). | 2005 | Sticht C, Hofele C, Flechtenmacher C et al. | British journal of cancer | 10.1038/sj.bjc.6602400 | 280 primary paraffin-embedded HNSCC | 124 oral squamous cell carcinomas (OSCC);96 pharyngeal squamous cell carcinomas (PSCC);60 laryngeal squamous cell carcinomas (LSCC) | HNSCCs biopsies mounted on a tissue microarray were analysed for copy number changes of CCNL1, SNO, PIK3CA and TP73L by fluorescence in situ hybridisation (FISH). | A significant association of CCNL1 gains and the presence of lymph node metastases was found, which was independent of anatomical site and T-stage of the primary tumour. | P=0.049 |
| Predictive value of p53 and PCNA expression for occult neck metastases in patients with clinically node-negative oral tongue cancer | 2006 | Keum K, Chung E, Koom W et al. | Otolaryngology–head and neck surgery | 10.1016/j.otohns.2006.02.011 | 37 clinically N0 patients who underwent neck dissection | Oral tongue cancer | p53 or proliferating cell nuclear antigen (PCNA) immunoreactivities on deparaffinized sections of the primary tumor | Although tumor differentiation and tumor size were significantly correlated with occult neck metastases of oral tongue cancer by univariate analysis, no correlation was found between p53 or PCNA and the presence of occult neck metastasis | P = 0.03 |
| Detection of occult carcinomatous diffusion in lymph nodes from head and neck squamous cell carcinoma using real-time RT-PCR detection of cytokeratin 19 mRNA | 2006 | Tao L, Lefèvre M, Ricci S et al. | British Journal of Cancer | 10.1038/sj.bjc.6603073 | 31 patients treated between 2004 and 2005 | HNSCC | A total of 1328 lymph nodes were prospectively evaluated by routine haematoxylin-eosin-safran (HES) staining, immunohistochemistry (IHC) and real-time Taqman reverse-transcriptase polymerase chain reaction (real-time RT-PCR) assay. Amplification of cytokeratin 19 (CK19) mRNA transcripts using real-time RT-PCR was used to quantify cervical micrometastatic burden | The cervical lymph node metastatic rates determined by routine HES staining and real-time RT-PCR assay were 16.3 and 36.0%, respectively,Moreover, CK19 mRNA expression values in histologically positive lymph nodes were significantly higher than those observed in histologically negative lymph nodes. | P<0.0001 |
| Cyclin B1 is useful to predict occult cervical lymph node metastases in tongue carcinoma. | 2006 | Harada H, Omura K, Nakajima Y et al. | Journal of experimental & clinical cancer research | 40 oral tongue squamous cell carcinomas | Oral tongue squamous cell carcinomas | immunohistochemical expression of cyclin B1 in a series of tissue samples | Cyclin B1 overexpression was positively correlated with occult cervical lymph node metastases and the number of mitotic cells. In addition, there was a positive relationship between labeling indices of cyclin B1 and Ki-67. | ||
| What is important for ultrasound evaluation of occult metastatic lymph nodes in laryngeal cancer: size, shape, vascularity or cytological findings? | 2007 | Cvorović L, Milutinović Z, Strbac M et al. | ORL; journal for oto-rhino-laryngology and its related specialties | 10.1159/000099227 | 60 patients with laryngeal squamous cell carcinoma without enlarged neck nodes on CT scan. | Laryngeal squamous cell carcinoma | 144 lymph nodes | Fifty-two of 144 lymph nodes were involved with metastasis on histopathological examination. Respective values for ultrasound-guided fine needle aspiration cytology (USg FNAC) showed high sensitivity, specificity, positive and negative predictive values and accuracy | |
| Metastasis of squamous cell carcinoma of the oral tongue is associated with down-regulation of epidermal fatty acid binding protein (E-FABP). | 2007 | Uma R, Naresh K, D’Cruz A et al. | Oral oncology | 10.1016/j.oraloncology.2005.12.024 | 54 cases of squamous carcinoma of the oral tongue; stages: T1, T2 or T3 | Oral tongue carcinoma | About 100 mg of fresh tissue from the primary tumour, a grossly metastatic lymph node and a non-metastatic lymph node were collected from each surgical procedure. | Gene FABP5, coding for Epidermal fatty acid binding protein (E-FABP) expression was up to 4-fold higher in the primary tumours (67%) as compared to the corresponding metastatic lymph nodes by northern blot analysis. | |
| Focal adhesion kinase and E-cadherin as markers for nodal metastasis in laryngeal cancer | 2007 | Rodrigo J, Dominguez F, Suárez V et al. | Archives of otolaryngology–head & neck surgery | 10.1001/archotol.133.2.145 | 95 previously untreated men with squamous cell carcinoma of the supraglottic larynx. | Squamous cell carcinoma of the supraglottic larynx. | Samples of tissue from surgical resection of the tumor and bilateral neck dissection | Decreased E-cadherin expression was correlated with the presence of nodal metastases. The combination of E-cadherin and FAK expression resulted in a superior accuracy in assessing nodal metastasis. | P=0.006P=0.001 |
| Determination of lymph node micrometastases in patients with supraglottic carcinoma | 2007 | Xu Y, Zhao X, Guan M et al. | Acta Oto-Laryngologica | 10.1080/00016480701200327 | 20 patients with supraglottic cancer | Supraglottic cancer | Twenty samples from supraglottic cancer and 182 lymph nodes from neck dissections were examined by LOH comparing immunohistochemical (IHC) staining using cytokeratin 19 (CK19), and hematoxylin and eosin (H&E) staining. | The frequency of LOH was 37.4% of lymph nodes and all of the primary tumors. Occult micrometastases were present in 9 of 20 cases; 23.6% of lymph nodes were positive for CK19 by IHC; 16.5% of lymph nodes were positive by H&E. | |
| Vascular endothelial growth factor a and proliferation marker in prediction of lymph node metastasis in oral and pharyngeal squamous cell carcinoma | 2008 | Boonkitticharoen V, Kulapaditharom B, Leopairut J et al. | Archives of Otolaryngology - Head and Neck Surgery | 10.1001/archotol.134.12.1305 | A total of 147 previously untreated patients with different stages of HNSCC | Oral cavity SCC; Pharyngeal SCC;Laryngeal SCC | Lymph nodes samples | Regarding nodal status, Ki-67 expression was a significant risk factor for N+ in all tumors, whereas VEGF-A expression was related to N+ in oral and pharyngeal SCC only. Analytically, Ki-67 expression alone in oral and pharyngeal SCC was associated with a relative risk of N+ of 3.83,and additional expression of VEGF-A raised the value to 6.12. Moreover, the combined expression of both markers was 3.25 times more effective in predicting N+ for T1,2 tumor compared with T3,4 tumor. | Ki-67 expression in all tumors (P< 0,009);Ki-67 expression alone in oral and pharyngeal SCC (P=0.009);VEGF-A expression was related to N+ in oral and pharyngeal SCC only (P<0.03);Ki-67 associated with VEGF-A expression in oral and pharyngeal SCC (P<0,001) |
| Histologic identification of human papillomavirus (HPV)-related squamous cell carcinoma in cervical lymph nodes: A reliable predictor of the site of an occult head and neck primary carcinoma | 2008 | El-Mofty S, Zhang M, Davila R | Head and Neck Pathology | 10.1007/s12105-008-0066-1 | 93 cases of SCC metastatic to the neck from known primary tumors were classified morphologically into conventional keratinizing SCC (KSCC) and non-keratinizing SCC (NKCa) | 32 oropharyngeal, 35 oral, and 26 arose in the laryx/hypopharynx | In situ hybridization (ISH) for high risk HPV as well as immunostaining for p16 were performed on all metastsatic and primary tumors | Twenty-three cases were found to be HPV+ by ISH, of which 22/23 had oropharyngeal origin, with 95.7% sensitivity and 85.7% specificity. Twenty-one of these HPV+ oropharyngeal tumors were NKCa. The remaining case showed overlapping NKCa/KSCC hybrid morphology. All NKCa were HPV+ and stained diffusely and strongly with p16 antibodies. | P<0.0001 |
| Expression of vascular endothelial growth factor-C does not predict occult lymph-node metastasis in early oral squamous cell carcinoma. | 2008 | Faustino S, Oliveira D, Nonogaki S et al. | International journal of oral and maxillofacial surgery | 10.1016/j.ijom.2007.11.021 | 87 patients with primary OSCC arising in the tongue or floor of mouth, clinically T1N0M0 or T2N0M0, with (pN+) and without (pN0) occult lymph-node metastases | Oral squamous cell carcinoma | Occult lymph-node metastases were analyzed for VEGF-C expression by malignant cells | Independently of VEGF-C expression, lymph-node metastasis (pN+) was the most significant prognostic factor for overall survival of patients with OSCC | P=0.030 |
| Expression of MAGE-A12 in oral squamous cell carcinoma. | 2008 | Mollaoglu N, Vairaktaris E, Nkenke E et al. | Disease markers | 10.1155/2008/359840 | Total of 57 specimens from OSCC | Oral squamous cell carcinoma | Total of 57 tissue samples obtained from patientswith OSCC and 20 normal oral mucosal (NOM) probesof otherwise healthy volunteers | No expression of MAGE-A12 was observed in the non-neoplasticNOM tissues. MAGE-A12 was expressed in 49.1% of the investigated tumor samples. The correlation between malignant lesion and MAGE-A12 detection was significant | P<0.001 |
| Detection of metastatic head and neck squamous cell carcinoma using the relative expression of tissue-specific mir-205 | 2008 | Fletcher A, Heaford A, Trask D | Translational Oncology | 10.1593/tlo.08163 | 12 patients with primary HNSCC | HNSCC | Snap-frozen tissue from 12 surgically removed, pathologically confirmed, primary HNSCC samples from various subsites in the head and neck and 7 benign mucosal tissue samples derived from the oral cavity or oropharynx were collected. A total of eight histologicallydetermined HNSCC-positive lymph nodes were included in thisstudy. Using a quantitative reverse transcription-polymerase chain reaction-based assay, we examined the expression of microRNA-205 (mir-205) across tissues. | mir-205 is abundantly expressed in squamous epithelial cells and that this expression remains relatively constant as these tissues transition from normal to neoplastic. Significantly, mir-205 is not expressed in normal lymph node tissue, allowing for the use of whole-lymph node processing and quantitative analysis by PCR to detect this biomarker | |
| Pathologic evaluation of sentinel lymph nodes in oral squamous cell carcinoma | 2010 | Trivedi N, Ravindran H, Sundram S et al. | Head and Neck | 10.1002/hed.21345 | 80 patients with primary HNSCC | HNSCC | Frozen section, imprint-cytology, hematoxylin-eosin staining, serial step sectioning (SSS) with hematoxylin-eosin, and immunohistochemistry (IHC) | SSS upstaged the disease in a further 7 patients (9%). Frozen section detected macrometastasis in 7 of 8 cases but failed to detect smaller metastases | |
| Overexpression of cornulin in histologically normal adjacent tissue predicts occult nodal metastases in head and neck | 2010 | Weinberger P, Merkley M, Jackson L et al. | Cancer Research | 10.1158/1538-7445.AM10-3286 | A cohort of 7 cN0 HNSCC patients who subsequently underwent planned neck dissection as part of their treatment was selected | HNSCC | Snap frozen tissue was enriched for tumor and adjacent normal tissue by laser capture microdissection. Total protein was extracted and separated by saturation-labeling 2D difference in-gel electrophoresis (2D-DIGE). | There were 31 proteins underexpressed in occult metastases patients, with the top candidate being 11.9 fold lower in the occult metastasis group. There were 29 proteins overexpressed, with the top candidate being 6.6 fold higher in the occult metastasis group. This protein was identified as Cornulin, a novel HNSCC biomarker. | P < 0.001 |
| Usefulness of 18F-FDG PET/CT examination in the diagnosis of head and neck cancer - Preliminary results | 2010 | Kuźmińska M, Osuch-Wójcikiewicz E, Fronczewska-Wieniawska K et al. | Otolaryngologia Polska | 10.1016/S0030-6657(11)70704-1 | 41 patients diagnosed with head and neck cancer | HNSCC | 45 PET/CT examinations were performed in 41 patients | Based on PET/CT imaging the recurrent disease was diagnosed in 9 patients, cervical lymph node metastases - in 12 patients, distant metastases - in 6 patients, possible primary tumour localization - in 3 patients. In 7 cases additional foci of increased FDG uptake were revealed outside the head and neck. | |
| Relationships between metastasis-associated protein (MTA) 1 and lymphatic metastasis in tonsil cancer. | 2011 | Park J, Jung C, Sun D et al. | European archives of oto-rhino-laryngology | 10.1007/s00405-010-1478-6 | 43 clinical N0 patients with tonsillar cancer | Tonsillar cancer | Immunohistochemical analysis of 43 tonsillar neoplasm tissues was performed using antibodies raised to MTA1. | There was a significant correlation between the expression of MTA1 and lymph node metastasis | P = 0.034 |
| Podoplanin expression correlates with sentinel lymph node metastasis in early squamous cell carcinomas of the oral cavity and oropharynx. | 2011 | Huber G, Fritzsche F, Züllig L et al. | International journal of cancer | 10.1002/ijc.25795 | 120 patients with HNSCC of the oral cavity and oropharynx undergoing a SLN biopsy were enrolled | Oral cavity and oropharynx squamous cell carcinoma | Cancer cell-expressed podoplanin was determined by immunohistochemistry using tissue microarrays | SLN examination revealed occult metastasis in 45 patients (37.5%). Twenty-nine of 120 (24.2%) primary HNSCC showed podoplanin expression. Podoplanin expression correlated significantly with SLN metastasis and remained a significant predictor for lymph node status even after controlling for tumor stage | p = 0.029 |
| Muscle invasion in oral tongue squamous cell carcinoma as a predictor of nodal status and local recurrence: just as effective as depth of invasion? | 2011 | Chandler K, Vance C, Budnick S et al. | Head and neck pathology | 10.1007/s12105-011-0296-5 | 61 cases of oral tongue squamous cell carcinoma stage T1 | Oral tongue squamous cell carcinoma | Tissue samples were examined histologically to assess muscle invasion and DOI | Cases with muscle invasion had a 23.3% PPV of occult lymph node metastasis. Cases with DOI of greater than 3 mm had a 29.7% PPV of occult lymph node metastasis. | |
| Human papillomavirus type 16 oropharyngeal cancers in lymph nodes as a marker of metastases | 2011 | Mirghani H, Moreau F, Lefèvre M et al. | Archives of otolaryngology–head & neck surgery | 10.1001/archoto.2011.141 | 11 patients with HPV-16(+) OSCC and 3 control patients with HPV-16(-) OSCC. | Oral squamous cell carcinoma | Viral load quantification using reverse transcriptase-polymerase chain reaction was retrospectively performed in primary tumors and in cervical lymph nodes, originating from levels IIa, IIb, and III. A total of 45 lymph node levels were analyzed. | The viral load value was significantly higher in metastatic lymph nodes than in tumor-free lymph nodes | P < 0.001 |
| Down regulation of e-cadherin (ECAD) - a predictor for occult metastatic disease in sentinel node biopsy of early squamous cell carcinomas of the oral cavity and oropharynx | 2011 | Huber G, Züllig L, Soltermann A et al. | BMC Cancer | 10.1186/1471-2407-11-217 | 120 patients | Oral cavity SCC (n = 110) (91.7%; mostly tongue);Oropharyngeal SCC (n=10) (8.3%). | E-Cadherin expression in tumour tissue with microarray technique | Differentiation grade and down regulation of E-Cadherin expression significantly correlate with positive lymph node status in univariate and multivariate analysis. | Differentiation grade (p = 0.018);Down regulation of E-Cadherin expression (p = 0.005) |
| Detection of occult lymph node metastasis in oral tongue squamous cell carcinoma | 2011 | Suresh A, Jeevan M, Trivedi N et al. | Oral Oncology | 10.1016/j.oraloncology.2011.06.290 | 44 patients (126 nodes) with oral tongue cancer | Oral tongue SCC | 126 samples of lymph nodes analyzed by quantitative PCR (QPCR). The detection efficacies were compared to pathological evaluation by frozen sections, serial step sectioning (SSS) with H&E as well as cytokeratin immunohistochemistry (IHC); | An evaluation using two markers (CK14 and DSG3) further increased the efficacy, while a combined evaluation identified all the patients with occult metastasis. | Sensitivity: 0.88; specificity: 0.85;Combined evaluation sensitivity: 1. |
| Can a metastatic gene expression profile outperform tumor size as a predictor of occult lymph node metastasis in oral cancer patients? | 2011 | Méndez E, Lohavanichbutr P, Fan W et al. | Clinical cancer research | 10.1158/1078-0432.CCR-10-0175 | 187 recruited subjects with primary OSCC or dysplasia | Oral squamous cell carcinoma | Affymetrix U133 2.0 plus arrays was used to compare the tumor genome-wide gene expression of 73 node-positive OSCC with 40 node-negative (≥18 months) OSCC | Regression identified a four-gene model (MYO5A, RFN145, FBXO32 and CTONG2002744) as the most predictive of nodal metastasis. | p = 0.011 |
| Nuclear BMI-1 expression in laryngeal carcinoma correlates with lymph node pathological status | 2012 | Allegra E, Puzzo L, Zuccalà V et al. | World Journal of Surgical Oncology | 10.1186/1477-7819-10-206 | 64 previously untreated patients who underwent surgical excision of laryngeal squamous cell carcinoma with neck dissection were included in this study. | Laryngeal SCC | The expression of B cell-specific Moloney murine leukemia virus integration site 1 (BMI-1) was examined immunohistochemically on formalin-fixed paraffin-embedded primary tissue specimens. | High cBMI-1 expression correlated significantly withdistant metastasis | p < 0.05 |
| LINE-1 and alu methylation patterns in lymph node metastases of head and neck cancers | 2012 | Kitkumthorn N, Keelawat S, Rattanatanyong P et al. | Asian Pacific Journal of Cancer Prevention | 10.7314/APJCP.2012.13.9.4469 | 61 lymph nodes from patients with HNSCC | HNSCC | 61 lymph nodes were divided into 3 groups: 1) non-metastatic head and neck cancer (NM);2) histologically negative for tumor cells of cases with metastatic head and neck cancer (LN);3) histologically positive for tumor cells (LP). | LINE-1 methylation of both LN and LP was altered.The LINE-1 methylation changes in LN have the same pattern as that in LP. This epigenomic change may be due to the presence of occult metastatic tumor in LN cases. | Lower LINE-1 methylation levels (p<0.001);Higher percentage of mCuC (p<0.01);Lower percentage of uCmC (p<0.001);Higher percentage of uCuC (p<0.001) |
| Loss of NKX3-1 as a potential marker for an increased risk of occult lymph node metastasis and poor prognosis in oral squamous cell carcinoma. | 2012 | Miyaguchi K, Uzawa N, Mogushi K et al. | International journal of oncology | 10.3892/ijo.2012.1373 | 60 OSCC patients | Oral squamous cell carcinoma | Genomic DNAs from 60 OSCC patients using Affymetrix mapping arrays | Quantitative RT-PCR and immunohistochemistry (IHC) analyses also showed significantly lower expression of NKX3-1 in the cases with occult LNM | |
| Identification of novel molecular markers for detecting lymph node metastasis of oral squamous cell carcinoma | 2012 | Oka R, Nakashiro K, Goda H et al. | Cancer Research | 10.1158/1538-7445.AM2012-720 | 7 patients with OSCC | Oral squamous cell carcinoma | The gene expression profiles in 7 metastatic lymph nodes from patients with OSCC, 1 benign lymph node, and 5 salivary gland tissues from non-cancerous patients by microarray analysis. The overexpression of 36 genes in all metastatic lymph nodes but not in benign lymph node and salivary glands was examinated in newly 15 metastatic lymph nodes and 9 benign lymph nodes by real-time quantitative RT-PCR method | Among the 36 genes, the expression of annexin A8-like 2 (ANXA8L2) and desmoglein 3 (DSG3) was commonly detected in metastatic lymph nodes at much higher level but not in benign lymph nodes at all. | |
| Expression of chemokine receptor CCR7 in oral squamous cell carcinoma with and without cervical metastasis | 2012 | Lourenc¸o S, Silami M, Camisasca D et al. | European Journal of Cancer | 10.1016/S0959-8049(12)71708-2 | 41 patients with OSCC | Oral squamous cell carcinoma | Paraffin embedded samples from both the tumor and cervical lymph nodes. Semi-seriated H&Estained sections and immunohistochemical reaction using anti-cytokeratin AE1/AE3 antibody were performed in metastasis-free cervical lymph nodes. | There was a significant association between pathological stage and cervical metastasis. A trend for an association with CCR7 expression in tumors was noted in relation to cervical metastasis and tumor thickness | pathological stage and cervical metastasis p = 0.00;CCR7 expression and cervical metastasis (p = 0.058) and tumor thickness (p = 0.051) |
| DSG3 as a biomarker for the ultrasensitive detection of occult lymph node metastasis in oral cancer using nanostructured immunoarrays | 2013 | Patel V, Martin D, Malhotra R et al. | Oral Oncology | 10.1016/j.oraloncology.2012.08.001 | 317 HNSCC cases | HNSCC | Multiple general cancer- and HNSCC-tissue microarrays (TMAs), in negative and positive HNSCC metastatic cervical lymph nodes, and in a variety of HNSCC and control cell lines | DSG3 is highly expressed in all HNSCC lesions and their metastatic cervical lymph nodes, but absent in non-invaded lymph nodes. | |
| Proteomic markers in early buccal mucosa squamous cell cancers | 2013 | Nair S, Malgundkar S, Patil A et al. | European Journal of Cancer | 10.1016/S0959-8049(13)70161-8 | 90 patients with early stage (T1/T2) buccal mucosa cancers | Oral squamous cell carcinoma | Tissue microarrays was prepared and the sectons stained with antibodies for 19 markers | Higher expression of SFN and TCTP are associated with lower risk of nodal metastasis | p = 0.003 |
| Oropharyngeal cancers: significance of HPV16 detection in neck lymph nodes. | 2013 | Mirghani H, Ferchiou M, Moreau F et al. | Journal of clinical virology | 10.1016/j.jcv.2013.02.009 | 11 patients with HPV16-positive OPSCC and 3 patients with HPV16-negative OPSCC | Oropharyngeal squamous cell carcinoma | HP16-viral load (VL) was quantified by real-time-polymerase-chain reaction in primary tumours and neck LNs | All metastatic LNs from HPV16-positive OPSCC had a high VL and the viral DNA was located within tumoural cells | |
| E-cadherin and β-catenin expression in well-differentiated and moderately-differentiated oral squamous cell carcinoma: Relations with clinical variables | 2013 | Rosado P, Lequerica-Fernández P, Fernández S et al. | British Journal of Oral and Maxillofacial Surgery | 10.1016/j.bjoms.2012.03.018 | 69 patients who had been operated on for oral SCC. | Oral squamous cell carcinoma | Tissue samples of oral squamous cell carcinomas were examined immunohistochemically | E-cadherin was significantly associated with histological grade and alcohol consumption, and β-catenin was significantly associated with nodal stage, TNM stage, and E-cadherin expression. | E-cadherin with histological grade (p = 0.002)alcohol consumption (p = 0.05); β-catenin with nodal stage (p = 0.02), TNM stage (p = 0.009), and E-cadherin expression (p = 0.01). |
| Discovery of DNA methylation markers that predict nodal metastases in oral squamous cell carcinoma | 2013 | Clausen M, Melchers L, De Bruin L et al. | Oral Oncology | 10.1016/j.oraloncology.2013.03.011 | 6 oral squamous cell carcinomas (OSCC) with nodal metastas es (N+) and 6 OSCC without nodal metastases (N0) | Oral squamous cell carcinoma | Global methylation levels on DNA extracted from 6 oral squamous cell carcinomas (OSCC) with nodal metastas es (N+) and 6 OSCC without nodal metastases (N0) by MethylCap -Seq. | The most promising methylation markers will be further validated on a N-status validation cohort containing 463 cases for which complete clinicopathological and follow-up data are available | |
| Activin A immunoexpression is useful to predict occult lymph node metastasis and overall survival in oral tongue squamous cell carcinoma | 2013 | Coletta R, Rodrigues P, Kelner N et al. | Virchows Archiv | 10.1007/s00428-013-1444- | 110 patients with primary TSCC | Oral tongue squamous cell carcinoma | Clinicopathological features and immunohistochemical detection of carcinoma-associated fibroblasts and activin A | Activin A high expression was significantly associated with presence of occult lymph node metastasis | p=0.006 |
| Staging of cervical lymph nodes in oral squamous cell carcinoma: Adding ultrasound in clinically lymph node negative patients may improve diagnostic work-up | 2014 | Norling R, Buron B, Therkildsen M et al. | PLoS ONE | 10.1371/journal.pone.0090360 | 51 patients with OSCC classified as cN0 by CT/MRI | Oral squamous cell carcinoma | US prior to sentinel node biopsy or selective neck dissection | Short axial diameter was the best size criterion for detection of metastases. The number of patients with occult metastases decreased from 16 out of 51 (31%) to 9 out of 51 (18%). | |
| Prognostic significance of cyclin D1 and E-cadherin expression in laryngeal squamous cell carcinoma | 2014 | Ahmed R, Shawky A, Hamed R | Pathology and Oncology Research | 10.1007/s12253-014-9741-6 | 75 patients with laryngeal squamous cell carcinoma | Laryngeal squamous cell carcinoma | Tumor tissue sampleswere examined for cyclin D1 and E-cadherin expression by immunohistochemistry. | Cyclin D1 was found to be a significant independent prognostic factor of lymph node metastasis | p = 0.001 |
| Significance of myofibroblast appearance in squamous cell carcinoma of the oral cavity on the occurrence of occult regional metastases, distant metastases, and survival. | 2015 | Luksic I, Suton P, Manojlovic S et al. | International journal of oral and maxillofacial surgery | 10.1016/j.ijom.2015.05.009 | 52 patients with cT1-T3N0 OSCC | Oral squamous cell carcinoma | The frequency of myofibroblasts within the tumour stroma was assessed immunohistochemically and compared with other clinical and histopathological factors in surgical resection specimens | An increased presence of myofibroblasts in the tumour stroma was significantly correlated with T stage, the presence of occult neck metastasis, regional recurrence, and distant metastasis | Myofibroblasts with T stage P=0.019, occult neck metastasis P<0.001, regional recurrence P=0.037, and distant metastasis P=0.008 |
| Does SPECT/CT offer incremental benefit over planar lympho-scintigraphy in sentinel node biopsies in oral cavity squamous cell carcinomas? | 2015 | Chandra P, Dhake S, Agrawal A et al. | Indian Journal of Nuclear Medicine | 44 patients with clinically node negative oral cavity SCC | Oral squamous cell carcinoma | 99mTc-labelled Human Serum Albumin Nanocolloid was injected at 2-4 sites on the edge of the tumour 3-6 hours before surgery. Static lymphoscintigraphy in two planes followed by SPECT/CT (low mA) was done. | PL revealed 77 hotspots with a mean of 1.75 per patient and SPECT revealed 92 hotspots with a mean of 2.5 per patient. Additional hotpots were identified in 8 patients on SPECT/CT, including 3 patients, where PL didn’t detect any nodes. | ||
| Clinical relevance of copy number profiling in oral and oropharyngeal squamous cell carcinoma | 2015 | van Kempen P, Noorlag R, Braunius W et al. | Cancer Medicine | 10.1002/cam4.499 | 191 oropharyngeal squamous cell carcinomas (OPSCC) and 164 oral cavity squamous cell carcinomas (OSCC) | Oral and oropharyngeal squamous cell carcinoma | Copy number status in 36 common oncogenes and tumor suppressor genes correlated with human papillomavirus (HPV) status in OPSCC, with occult lymph node status in OSCC and with patient survival. | In clinically lymph node-negative OSCC (Stage I-II), gain of the 11q13 region was significantly correlated with occult lymph node metastases | Negative predictive value of 81% |
| Activin A regulates cell interactions in the microenvironment of oral squamous cell carcinomas | 2015 | Coletta R, Bufalino A, Sobral L et al. | Cancer Research | 10.1158/1538-7445 | 115 OSCC patients | Oral squamous cell carcinoma | Immunohistochemical analysis of 115 OSCC samples | Increased activin A expression is significantly correlated with presence of regional metastasis | p=0.034 |
| Activin A immunoexpression as predictor of occult lymph node metastasis and overall survival in oral tongue squamous cell carcinoma. | 2015 | Kelner N, Rodrigues P, Bufalino A et al. | Head & neck | 10.1002/hed.23627 | 110 patients with primary oral tongue SCC | Oral tongue squamous cell carcinoma | Immunohistochemical detection of carcinoma-associated fibroblasts (CAFs) and activin A on tissue samples | Only high immunohistochemical expression of activin A was significantly associated with presence of occult lymph node metastasis | p =0 .006 |
| Accuracy of microRNAs as markers for the detection of neck lymph node metastases in patients with head and neck squamous cell carcinoma. | 2015 | de Carvalho A, Scapulatempo-Neto C, Maia D et al. | BMC medicine | 10.1186/s12916-015-0350-3 | 161 patients with HNSCC | HNSCC | The most differentially expressed microRNAs were validated by qRT-PCR in two independent cohorts: i) 48 FFPE lymph node samples, and ii) 113 FNA lymph node biopsies. | Seven microRNAs highly expressed in metastatic lymph nodes from the discovery set were validated in FFPE lymph node samples. MiR-203 and miR-205 identified all metastatic samples | |
| Prediction of occult lymph node metastasis in squamous cell carcinoma of the oral cavity and the oropharynx using peritumoral Prospero homeobox protein 1 lymphatic nuclear quantification. | 2016 | Mermod M, Bongiovanni M, Petrova T et al. | Head & neck | 10.1002/hed.24452 | Oral cavity and the oropharynx squamous cell carcinoma | Staining of the specific lymphatic endothelial cells nuclear marker, PROX1, as an indicator of lymphatic vessel density was determined by counting the number of positive cells in squamous cell carcinomas (SCCs) of the oral cavity and the oropharynx with clinically negative necks | Peritumoral PROX1 lymphatic nuclear count significantly correlated with the detection of OLNM in multivariate analysis | p < 0.005 | |
| Determining the potential of desmoglein 3 as a sensitive and specific immunohistochemical marker for the detection of micrometastasis in patients with primary oral squamous cell carcinoma. | 2016 | Nagvekar S, Spadigam A, Dhupar A | Contemporary oncology | 10.5114/wo.2016.64596 | 10 patients who underwent neck dissection for primary OSCC | Oral squamous cell carcinoma | Forty-seven lymph node specimens were immunostained with DSG3 | DSG3 positivity was noted in the six positive lymph nodes. However, when using DSG3 as an immunohistochemical marker, no additional micrometastatic deposits were evident in the histologically negative nodes | |
| Detection of cervical lymph node micrometastasis and isolated tumor cells in oral squamous cell carcinoma using immunohistochemistry and serial sectioning. | 2016 | Dhawan I, Sandhu S, Bhandari R et al. | Journal of oral and maxillofacial pathology | 10.4103/0973-029X.190946 | 10 patients treated with radical neck dissection for primary OSCC. | Oral squamous cell carcinoma | 133 LNs were subjected to SS at 100 μm intervals. The sections were stained with routine H&E staining, pan-CK and analyzed for MM and ITC | The application of combination of SS and IHC using pan-CK (AE1/AE3) revealed the presence of MM and ITC in 2.25% of the LNs diagnosed as negative on routine H&E examination | |
| Clinical significance of three-dimensional measurement of tumour thickness on magnetic resonance imaging in patients with oral tongue squamous cell carcinoma. | 2016 | Kwon M, Moon H, Nam S et al. | European radiology | 10.1007/s00330-015-3884-z | 53 OTSCC patients | Oral tongue squamous cell carcinoma | Tumour thickness measured on axial, coronal, and sagittal views was compared to that in pathologic specimens. | TT in all three planes was significantly correlated with lymph node (LN) metastasis. Occult LN metastasis was found in 15 of 39 (38.5%) patients | |
| Worst Pattern Of Invasion and occult cervical metastases for oral squamous carcinoma | 2017 | Velosa C, Shi Q, Stevens T et al. | Head and Neck | 10.1002/hed.24754 | 323 patients with T1T2cNo oral cavity squamous carcinoma | Oral squamous cell carcinoma | The resection specimens were examined for worst pattern of invasion, perineural invasion, and lymphocytic host responses | High-risk classification is significantly associated with decreased time to local recurrence and regional metastasis. For patients undergoing END, 31 (20%) had occult-positive lymph nodes. WPOI-5 is significantly predictive of occult cervical metastases | Local recurrence (p = .0128) and regional metastasis (p = .052). WPOI-5 (p 0< .0001). |
| Predictive Significance of Tumor Depth and Budding for Late Lymph Node Metastases in Patients with Clinical N0 Early Oral Tongue Carcinoma | 2017 | Hori Y, Kubota A, Yokose T et al. | Head and neck pathology | 10.1007/s12105-017-0814-1 | 48 patients with early oral tongue squamous cell carcinoma | Oral tongue squamous cell carcinoma | Associations between the histopathological factors and late lymph metastasis were analyzed | High-grade tumor budding is an independent predictive factor for neck recurrenc | p < 0.01 |
| Positron emission tomography-CT prediction of occult nodal metastasis in recurrent laryngeal cancer. | 2017 | Rosko A, Birkeland A, Shuman A et al. | Head & neck | 10.1002/hed.24719 | 46 clinically and radiographically N0 patients with recurrent laryngeal cancer | Laryngeal SCC | PET-CT examination before salvage laryngectomy with neck dissection | Two patients (16.7%) had true-positive PET-CT results, whereas 10 patients (83.3%) had false-negative scans, 1 patient (2.9%) had a false-positive result and 33 patients (97.1%) had a true-negative PET-CT. | |
| Molecular marker based intra-operative diagnostic assay for detection of lymph node metastasis in hnscc | 2017 | James B, Kontharaman S, Kumar M et al. | Head and Neck | 24 patients with HNSCC | HNSCC | positive (17) and negative (7) lymph nodes metastases | Sandwich ELISA indicated the best combination of antibodies and the Lateral Flow test (LFT) assays developed with combination for DSG-3, showed a sensitivity of 72.5% and specificity of 55.6% in detecting positive lymph node samples (11 positive & 9 negative lymph nodes) | ||
| MFAP5 and TNNC1: Potential markers for predicting occult cervical lymphatic metastasis and prognosis in early stage tongue cancer | 2017 | Yang X, Wu K, Li S et al. | Oncotarget | 10.18632/oncotarget.12446 | 12 patients underwent surgical resection for TSCC and selective neck dissection | Oral tongue SCC | Microarray in TSCC fresh tumor and normal tissue specimens with CLNM (n = 6) compared to those without CLNM (n = 6). | Over-expression of MFAP5 and TNNC1 were correlated with CLNM, metastasis relapse-free survival and overall survival | p < 0.001 |
| Immunohistochemical detection of lymph node-DTCs in patients with node-negative HNSCC | 2017 | Sproll C, Freund A, Hassel A et al. | International Journal of Cancer | 10.1002/ijc.30617 | 50 pN0-HNSCC patients | HNSCC | A total of 1.137 exactly mapped LNs. Three immunohistochemistry (IHC) assays using antibodies directed against CK5/14 and CD44v6 | 7 micrometastases (MM) in five patients and 31 disseminated tumor cells (DTCs) in 12 patients. | |
| Feasibility of panitumumab-IRDye800 for metastatic lymph node identification in patients with head-and-neck squamous cell carcinoma | 2017 | Van Den Berg N | Molecular Imaging and Biology | 10.1007/s11307-01-017-1138-y | 10 patients with HNSCC | HNSCC | Excised LN samples evaluated on high-sensitivity fluorescence systems and histopathotologically evaluated (including hematoxylin and eosin (H&E) and EGFR staining) and unstained paraffin-embedded sections) | Fluorescence imaging of panitumumab-IRdye800 predicted the LN status correctly in all cases with 164 true negative nodes, 8 true positive nodes, 0 false-positive nodes and 0 false-negative nodes | |
| Cytokeratin 19 expression in early oral squamous cell carcinoma and their metastasis: Inadequate biomarker for one-step nucleic acid amplification implementation in sentinel lymph node biopsy procedure | 2017 | Noorlag R, van Es R, de Bree R et al. | Head and Neck | 10.1002/hed.24847 | 207 patients with OSCC | Oral squamous cell carcinoma | Immunohistochemical CK19 expression was done in 65 cases of paired nodal metastases. | CK19 was expressed in 65% of all OSCC and even less in early OSCC (56%), with poor correlation between primary tumor and (occult) nodal metastasis. | |
| Clinical application of bio-markers for detection of nodal metastasis in head and neck squamous cell carcinoma | 2017 | Kothandaraman S, James B, Raghavan N et al. | Head and Neck | HNSCC | A retrospective (from tissue repository) and prospective (lymph node sample collection) validation of markers ). The validation of these markers will be done by IHC | Using antibodies to desmoglein-3 (DSG-3), with 17 positive and negative lymph node samples, a sensitivity of 72.5% and specificity of 55.6% was achieved for the detection of nodal metastasis using a Lateral Flow Test assay system | |||
| Amplification and protein overexpression of cyclin D1: Predictor of occult nodal metastasis in early oral cancer | 2017 | Noorlag R, Boeve K, Witjes M et al. | Head and Neck | 10.1002/hed.24584 | 158 patients with early tongue and floor of mouth (FOM) squamous cell carcinomas | Oral squamous cell carcinoma | Both CCND1 amplification and cyclin D1, FADD, and cortactin protein expression were correlated with occult nodal metastases from tissue samples | CCND1 amplification and cyclin D1 expression correlated with occult nodal metastases. | |
| Tumor budding is a predict marker of occult node metastasis and prognosis in patients with cT2N0 TSCC | 2018 | Yamana K, Sakata J, Yoshida R et al. | Cancer Science | A total 100 patients with clinical T2N0 TSCC. | Tongue squamous cell carcinoma | Tissue samples | OCLNM was significantly associated with endophytic growth pattern, depth of invasion (> 3.3mm) and tumor budding (> 4) in univariate analysis. Multivariate analysis revealed that the tumor budding (> 4) was independently associated with the OCLNM. | ||
| Tumor budding as a novel predictor of occult metastasis in cT2N0 tongue squamous cell carcinoma | 2018 | Sakata J, Yamana K, Yoshida R et al. | Human Pathology | 10.1016/j.humpath.2017.12.021 | 97 patients with cT2N0 TSCC who underwent surgical resection of their primary lesion | Tongue squamous cell carcinoma | Tumor budding using immunohistochemical staining for cytokeratin AE1/AE3 and hematoxylin and eosin staining (HE). | Tumor budding score ≥4 is a significant independent predictive factor for the occurrence of occult neck metastasis, which in turn is a significant independent prognostic factor. | |
| Prognostic implication of NOTCH1 in early stage oral squamous cell cancer with occult metastases. | 2018 | Wang S, Fan H, Xu J et al. | Clinical oral investigations | 10.1007/s00784-017-2197-9 | 144 patients with early stage (cT1T2N0) OSCC | Oral squamous cell carcinoma | Tissue samples analyzed for the impact of the immunohistochemical expression of CD133, NANOG, and NOTCH1 | CD133, NANOG, and NOTCH1 were significantly associated with lymph node metastasis | CD133: p = 0.035; NANOG: p = 0.024, NOTCH1: p = 0.043 |
| Pre-treatment Neutrophil-to-Lymphocyte Ratio as a predictor for occult cervical metastasis in early stage (T1-T2 cN0) squamous cell carcinoma of the oral tongue. | 2018 | Abbate V, Dell’Aversana Orabona G, Salzano G et al. | Surgical oncology | 10.1016/j.suronc.2018.06.002 | 110 patients suffering from early stage OTSCC | Oral tongue squamous cell carcinoma | Tissue samples analyzed for Neutrophil-to lymphocyte ratio (NLR) in predicting occult cervical metastasis in stage I and II OTSCC | A statistically significant relationship between high levels of pre-treatment NLR and probability rate for neck occult metastases has been found | p = 0.000496 |
| MYO5A inhibition by miR-145 acts as a predictive marker of occult neck lymph node metastasis in human laryngeal squamous cell carcinoma | 2018 | Zhao X, Zhang W, Ji W | OncoTargets and Therapy | 10.2147/OTT.S164597 | 132 patients with LSCC | Laryngeal squamous cell carcinoma | MYO5A and miR-145 expression was analyzed in tissue samples | Downregulation of miR-145 in LSCC, which was negatively correlated with MYO5A suppression of LSCC progression and metastasis. MiR-145 directly regulated MYO5A expression in vitro and suppressed LSCC proliferation and invasion while promoting apoptosis by inhibiting MYO5A. | |
| Tumor Infiltrating Lymphocytes in Occult Primary HPV+ Oropharyngeal Squamous Cell Carcinoma (OPSCC): Comparison of the Primary Tumor and Regional Lymph Node Metastases | 2019 | Lukens J, Pustylnikov S, Montone K et al. | International Journal of Radiation Oncology Biology Physics | 10.1016/j.ijrobp.2019.06.1539 | 14 patients presenting with initially occult primary HPV+ OPSCC managed with trans-oral robotic surgery (TORS) and neck dissection, with a final TNM stage of pT1 N2b | Oropharyngeal squamous cell carcinoma | Immunohistochemistry (IHC) was performed on paired specimens from the primary site and involved nodes for CD3, CD8, FOXP3, PD-L1, and CTLA-4 | Occult primary tumors had a higher percentage of CD3+ and CD8+ TILs compared to tumor in lymph nodes. There was a higher concentration of FOXP3+ TILs in primary tumors compared to nodal tumor and a trend towards a higher percentage of CTLA-4+ cells | CD3+ (p = 0.006), CD8+ T cells (p = 0.01). FOXP3+ TILs (p = 0.01), CTLA-4+ cells (p = 0.09) |
| Selected molecular markers as indicators of clinical profile, tumor characteristics and treatment outcome in squamous cell carcinoma of the larynx | 2019 | Iype E, Balakrishnan L | Journal of Clinical Oncology | 10.1200/jco.2019.37.15_suppl.e17522 | 72 cases of laryngeal squamous cell carcinoma | Laryngeal squamous cell carcinoma | Samples from patients who underwent laryngectomy were taken and analyzed prospectively. Immunoreactivity in tissue sections was evaluated as negative when no positive cells were observed within the tumor, weak (1+) , moderate (2+) , and strong or intense (3+) | Proliferation markers EGFR, Cyclin D1 and Ki 67, individually and collectively were predictive of extracapsular spread and perineural spread of tumour. The significant expression of Cox-2 was highly predictive of Node positivity. Markers of aggressiveness were identified as p53, Bcl-2 Cox-2. Markers of invasiveness were EGFR, Cyclin D1 and Ki 67. Markers predicting survival were p53, BCl-2, Cyclin D1 and Ki 67. | |
| Prediction of Occult Lymph Node Metastasis in Head and Neck Cancer with CD31 Vessel | 2019 | Mermod M, Bongiovanni M, Petrova T et al. | Otolaryngology - Head and Neck Surgery (United States) | 10.1177/0194599818791779 | 56 cases of squamous cell carcinoma | Oral cavity SCC (n = 50);Oropharyngeal SCC (n = 6) | Intra- and peritumoral microvascular density values | Peritumoral CD31 microvascular density was significantly associated with occult LNM in multivariate analysis | P< 0.01 |
| Immunohistochemical quantification of partial-EMT in oral cavity squamous cell carcinoma primary tumors is associated with nodal metastasis | 2019 | Parikh A, Puram S, Faquin W et al. | Oral Oncology | 10.1016/j.oraloncology.2019.104458 | 99 OCSCC patients (47 with low volume T2 disease, 52 with high volume T4 disease, and ∼50% in each group with nodal metastasis) | Oral cavity SCC | Tissue microarrays (TMA) were created using 2 mm cores from patients | There were associations of p-EMT scores with higher grade, PNI, and node positivity, including occult node positivity | p-EMT scores with higher grade (p = 0.04), PNI (p = 0.003), and node positivity (p = 0.02), including occult node positivity (p = 0.005) |
| Gene Expression Subtype Predicts Nodal Metastasis and Survival in Human Papillomavirus-Negative Head and Neck Cancer. | 2019 | Zevallos J, Mazul A, Walter V et al. | The Laryngoscope | 10.1002/lary.27340 | 309 OCSCC cases and 125 LSCC | Oral cavity squamous cell carcinoma and laryngeal squamous cell carcinoma | Clinically node-negative OCSCC cases in order to test the predictive value of gene expression subtypes in detecting occult nodal metastasis | In a subset analysis of clinically T1-2N0M0 OCSCC, we demonstrate that the mesenchymal subtype was predictive of occult nodal metastasis | (RR=3.38, 95% CI 1.08–10.69) |
| Significance of SUV Max for Predicting Occult Lymph Node Metastasis and Prognosis in Early-Stage Tongue Squamous Cell Carcinoma. | 2020 | Xu C, Li H, Seng D et al. | Journal of oncology | 10.1155/2020/6241637 | 120 cT1-2N0 tongue SCC patients | Tongue squamous cell carcinoma | The association between SUV max and occult lymph node metastasis was analyzed | In 60 patients with an SUV max >9.7, 13 patients had occult metastasis, and the difference was significant | p=0.041 |
| Pre-operative cellular dissociation grading in biopsies is highly predictive of post-operative tumour stage and patient outcome in head and neck squamous cell carcinoma. | 2020 | Jesinghaus M, Steiger K, Stögbauer F et al. | British journal of cancer | 10.1038/s41416-019-0719-8 | 160 patients with HNSCC | HNSCC | CDG in n = 160 pre-therapeutic biopsies from patients who received standardised treatment following German guidelines | Pre-operative CDG was highly predictive of post-operative tumour stage, including the prediction of occult lymph node metastasis. | p < 0.001 |
| EVI1 as a marker for lymph node metastasis in HNSCC | 2020 | Idel C, Ribbat-Idel J, Kuppler P et al. | International Journal of Molecular Sciences | 10.3390/ijms21030854 | Anonymized retrospective cohort of 389 patients suffering from HNSCC | Oral HNSCC n = 97;Oropharyngeal HNSCC n = 133;Hypopharyngeal HNSCC n = 48;Laryngeal HNSCC n= 111; | Tissue samples of Primary Tumors, Lymph nodes Metastasis, Distant Metastasis, and Local Recurrences | EVI1 expression in PTs that had at least one cervical lymph node metastasis (LM) was significantly higher than in those PTs that had not formed LMs yet.At the time of the first diagnosis, EVI1 expression in PT tissue could discriminate between nodal positive and nodal negative patients. | p < 0.05. |
| One-step nucleic acid amplification for detecting lymph node metastasis of head and neck squamous cell carcinoma | 2020 | Peigné L, Godey F, Le Gallo M et al. | Oral Oncology | 10.1016/j.oraloncology.2019.104553 | 26 cN0 HNSCC patients | HNSCC | 157 LN were prospectively analyzed. Each node was cut into 4 equal pieces alternatively sent to pathological analysis and OSNA technique. IHC CK19 was performed on the primary tumor biopsy and RT-qPCR of CK19, PVA and EPCAM on the LN lysate of discordant cases. | SNA detected 21 metastases. There were 139 concordant LN (88.5%). | After elimination of allocation bias, false negative rate was 1.3%, sensitivity and specificity were 90% and 95.6%, PPV and NPV were 75% and 98.5%. |
| Circulating Hybrid Cells as a Marker of Nodal Metastases in Oral Cavity Squamous Cell Carcinoma | 2020 | Anderson Y, Wong M, Clayburgh D | International Journal of Radiation Oncology Biology Physics | 10.1016/j.ijrobp.2019.11.347 | 20 cN0 OCSCCa patients undergoing resection of the primary tumor and neck dissection for staging. | Oral squamous cell carcinoma | Peripheral blood samples were obtained and it was performed immunohistochemistry on the samples to identify cells co-expressing both cytokeratin (tumor cell marker) and CD45 (macrophage marker), indicating a circulating hybrid cell | There was a statistically significant difference between CHC levels of cN0 patients who remained pN0, and those that converted to pN1+. The level of CHCs in the peripheral blood correlated with the presence of both overt and pathologically identified occult cervical nodal metastases | p = 0.005; 0.002; 0.0001 |
| Pretreatment Blood Markers in the Prediction of Occult Neck Metastasis: A 10-Year Retrospective Study. | 2021 | Ventura E, Barros J, Salgado I et al. | Cureus | 10.7759/cureus.16641 | 102 patients with early-stage OSCC of the tongue | Oral squamous cell carcinoma of the tongue | Role of pretreatment inflammatory blood markers in predicting occult neck metastasis. We also evaluated neutrophil-lymphocyte ratio (NLR) association with the depth of invasion (DOI) of the primary tumor | Significant association of NLR and monocyte-lymphocyte ratio with neck status on univariate analysis. Multivariate analysis showed that only NLR was an independent risk factor for occult metastasis among inflammatory blood markers. | p=0.001; 0.011; 0.02 |
| Pre-treatment neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as predictors of occult cervical metastasis in clinically negative neck supraglottic and glottic cancer | 2021 | Salzano G, Perri F, Maglitto F et al. | Journal of Personalized Medicine | 10.3390/jpm11121252 | 387 patients with LSCC | Laryngeal squamous cell carcinoma | Data of patients affected by LSCC, who had been surgically treated by means of laryngectomy and END between January 2006 and January 2021, were retrospectively reviewed, using information retrieved from a database dedicated to such procedures in a single tertiary care referral institute. | A total of 27.7% of patients were found positive for neck node metastasis (the pN+ group), while 78/108 (72.3%) patients were found to be negative for the presence of neck metastasis (the pN0 group). High values of NLR, but not PLR, significantly correlated with the probability of OM, and an NLR value of 2.26 corresponds to a probability of OM of 20%. | |
| The occult nodal metastasis rate of early tongue cancer (T1–T2): A protocol for a systematic review and meta-analysis | 2021 | Choi K, Park S, Kim J et al. | Medicine | 10.1097/MD.0000000000024327 | 19 enrolled studies with a total of 1567 cases included. | All studies enrolled T1 and T2 oral tongue cancer patients (with clinically negative for lymph node metastasis) | Tissue samples | The occult nodal metastasis rate was not significantly affected by neither T2 ratio among T1–T2 nor reported year of the studies. | P = 0.426 and 0.921 |
| Metastatic and sentinel lymph node mapping using intravenously delivered Panitumumab- | 2021 | Krishnan G, van den Berg N, Nishio N et al. | Theranostics | 10.7150/THNO.59196 | 27 patients with oral squamous cell carcinoma (OSCC), 18 of whom were clinically node negative (cN0). | Oral squamous cell carcinoma | Patients were infused intravenously with 50mg of Panitumumab-IRDye800CW prior to surgical resection of their primary tumour with neck dissection and/or SLNB. Lymphadenectomy specimens underwent fluorescence molecular imaging to evaluate tracer distribution to LNs. | The median MFI of metastatic LNs was significantly higher than the median MFI of benign LNs | 0.06 versus 0.02, p < 0.05 |
| Detecting head and neck lymph node metastases with white light reflectance spectroscopy; a pilot study. | 2021 | Bugter O, Aaboubout Y, Algoe M et al. | Oral oncology | 10.1016/j.oraloncology.2021.105627 | 9 patients with a total of nineteen LNs were included. | HNSCC | Intraoperative SFR spectroscopy measurements of LNs with and without malignancies. | Three parameters, blood volume fraction (BVF), microvascular saturation (StO(2)), and Rayleigh amplitude, were significantly lower in positive LNs. They were combined into one optical parameter ‘delta’, using discriminant analysis. Delta was significantly decreased in positive LNs. | p = 0,0006 |
| Deregulation of extracellular matrix modeling with molecular prognostic markers revealed by transcriptome sequencing and validations in Oral Tongue squamous cell carcinoma. | 2021 | Thangaraj S, Shyamsundar V, Krishnamurthy A et al. | Scientific reports | 10.1038/s41598-020-78624-4 | 100 patients with Oral Tongue Squamous Cell Carcinoma (OTSCC), | Oral Tongue Squamous Cell Carcinoma | Transcriptome analysis of OTSCC patients identified the key genes and deregulated pathways. A panel of 26 marker genes was shortlisted and validated using real-time PCR | Up-regulation of Tenacin C (TNC) and Podoplanin (PDPN) was significantly correlated with occult node positivity. | |
| Circulating hybrid cells predict presence of occult nodal metastases in oral cavity carcinoma | 2021 | Henn T, Anderson A, Hollett Y et al. | Head and Neck | 10.1002/hed.26692 | 22 patients with cN0 OCSCC | Oral squamous cell carcinoma | Peripheral blood samples for CHCs with co-expression of cytokeratin (tumor) and CD45 (leukocyte) using immunofluorescence microscopy, then correlated levels with pathologic lymph node status. | CHC levels exceeded CTCs and correlated with the presence of both clinically overt and occult nodal metastases | p = 0.002; 0.006 |
| Tumor–stroma ratio can predict lymph-node metastasis in cT1/2N0 oral tongue squamous cell carcinoma independent of tumor budding grade | 2022 | Sakai T, Saito Y, Tateishi Y et al. | International Journal of Clinical Oncology | 10.1007/s10147-022-02249-y | 70 patients with cT1/2N0 OTSCC | Oral Tongue squamous cell carcinoma | BG and TSR were evaluated using hematoxylin–eosin staining and cytokeratin AE1/AE3 immunostaining. | NLM correlated with the pathological depth of invasion (pDOI), TBG and TSR in univariate analysis and pDOI and TSR in multivariate analysis. | p < 0.001, p = 0.008, p < 0.001 , p = 0.01, p = 0.02 |
| The prognostic role of the pre-treatment neutrophil to lymphocyte ratio (NLR) and tumor depth of invasion (DOI) in early-stage squamous cell carcinomas of the oral tongue. | 2022 | Salzano G, Dell’Aversana Orabona G, Abbate V et al. | Oral and maxillofacial surgery | 10.1007/s10006-021-00969-5 | 110 patients affected by early-stage (cT1-T2 cN0) OTSCC | Oral Tongue squamous cell carcinoma | Tissue samples analyzed for pre-treatment neutrophil to lymphocyte ratio (NLR) and tumor depth of invasion (DOI) | A DOI greater than 5.4 mm and a NLR greater than 2.93 are associated with an increased risk of presenting occult cervical metastases | |
| Semaphorin-3F/Neuropilin-2 Transcriptional Expression as a Predictive Biomarker of Occult Lymph Node Metastases in HNSCC | 2022 | Meler-Claramonte C, Avilés-Jurado F, Vilaseca I et al. | Cancers | 10.3390/cancers14092259 | 53 patients with cN0 squamous cell carcinoma | HNSCC | Tissue samples analyzed for he transcriptional expression of SEMA3F and NRP2 | Patients with occult lymph node metastases (cN0/pN+) had significantly lower SEMA3F expression values than patients without lymph node involvement (cN0/pN0). Considering the expression of the SEMA3F-NRP2 genes, patients were classified into two groups according to the risk of occult nodal metastasis: Group 1 (n = 34), high SEMA3F/low NRP2 expression, with a low risk of occult nodal involvement (14.7% cN0/pN+); Group 2 (n = 19), low SEMA3F or high SEMA3F/high NRP2 expression, with a high risk of occult nodal involvement (78.9% cN0/pN+). | |
| Dissecting Tissue Compartment-Specific Protein Signatures in Primary and Metastatic Oropharyngeal Squamous Cell Carcinomas. | 2022 | Sadeghirad H, Monkman J, Mehdi A et al. | Frontiers in immunology | 10.3389/fimmu.2022.895513 | 43 patients with primary tumors and 11 with nodal metastases | Oropharyngeal squamous cell carcinoma | Targeted spatial proteomic approaches to primary and lymph node metastasis from an oropharyngeal SCC | Overall survival (OS) analysis indicated CD25 in tumor regions of primary tumors to be associated with reduced survival, while progesterone receptor (PR) was associated with an improved OS | p = 0.003, p = 0.015 |
| Circulating tumor cells as a predictor for poor prognostic factors and overall survival in treatment naïve oral squamous cell carcinoma patients | 2022 | Qayyumi B, Bharde A, Aland G et al. | Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology | 10.1016/j.oooo.2022.02.018 | 152 patients with treatment naïve oral squamous cell carcinoma. Sensitivity analysis was performed by including 40 healthy controls. | Oral SCC | CTCs were isolated using OncoDiscover technique from presurgically obtained peripheral blood | CTCs above 20.5 were suggestive of nodal metastasis with a linear trend for detecting occult metastasis | P < 0.0001P =0.061 |
| Tumour budding-based grading as independent prognostic biomarker in HPV-positive and HPV-negative head and neck cancer | 2023 | Stögbauer F, Beck S, Ourailidis I et al. | British Journal of Cancer | 10.1038/s41416-023-02240-y | 331 HPV-positive and HPV-negative cases from TCGA. | HNSCC | TB and MCNS were analysed digitally in 1 and 10 high-power fields (HPF) | Analysing MCNS did not add prognostic significance to quantifying TB. CDG was a significant prognostic marker in HPV-negative and HPV-positive tumours and prognostically superior to the WHO and BG systems. High CDG was associated with clinically occult lymph-node metastases | |
| Expression of Connexins 37, 40 and 45, Pannexin 1 and Vimentin in Laryngeal Squamous Cell Carcinomas | 2023 | Mizdrak I, Mizdrak M, Racetin A et al. | Genes | 10.3390/genes14020446 | 34 patients who underwent (hemi-)laryngectomy and regional lymphadenectomy due to LSCC | Laryngeal squamous cell carcinoma | Samples of tumor tissue and adjacent normal mucosa embedded in paraffin blocks were stained using the immunofluorescence method and were semi-quantitatively analyzed. | The expression of Cx37, Cx40, and Panx1 differed between cancer and adjacent normal mucosa and between histological grades, being the highest in well-differentiated (G1) cancer and low/absent in poorly differentiated (G3) cancer | p < 0.05 |
| Diagnostic performance of FDG PET/MRI for cervical lymph node metastasis in patients with clinically N0 head and neck cancer | 2023 | Cebeci S, Aydos U, Yeniceri A et al. | European Review for Medical and Pharmacological Sciences | 10.26355/eurrev_202305_32459 | 44 patients who underwent neck dissection with the diagnosis of HNSCC | HNSCC | Clinical examinations, including ultrasonography, were performed to identify cervical metastases in HNSCC patients with preoperative cN0. A nuclear medicine specialist visually evaluated the MRI, PET, and PET/MRI results | PET/MRI was more successful in distinguishing pathological N0 and N+ patients | 83.3% sensitivity, 92.1% specificity, 97.2% NPV, 62.5% PPV and 90.9% accuracy |
| The modified Polsby-Popper score is a novel quantitative histomorphology biomarker with potential to predict lymph node positivity and cancer-specific survival in tongue squamous cell carcinoma | 2024 | Csury T, Csury A, Balk M et al. | Oncology Research and Treatment | 10.1159/000535363 | Patients with pT1-pT4a squamous cell carcinomas of the mobile tongue (TSCC) | Tongue squamous cell carcinoma | A total of 100 formalin-fixed paraffin-embedded (FFPE) primary tumor specimens | pT category, tumor grade, pNX nodal status and the presence of manifest metastatic cervical lymph nodes at the time of diagnosis were all found to be significant predictors of OS. | pT category (p = 0.044), tumor grade (p = 0.036), pNX nodal status (p = 0.004), and the presence of manifest metastatic cervical lymph nodes at the time of diagnosis (p = 0.002) |
| Predictors of Occult Metastasis and Prognostic Factors in Patients with cN0 Oral Cancer Who Underwent Elective Neck Dissection. | 2024 | Yamagata K, Fukuzawa S, Noguchi A et al. | Diseases (Basel, Switzerland) | 10.3390/diseases12020039 | 86 patients with OSCC | Oral squamous cell carcinoma | Nodal nodes samples for occult metastasis and risk factors for poor prognosis after SOHND. | OS was significantly associated with pN | p = 0.015 |
| Blood Markers Predicting Clinically Occult Lymph Node Metastasis in Head and Neck Squamous Cell Carcinoma. | 2024 | Gaudioso P, Borsetto D, Polesel J et al. | ORL; journal for oto-rhino-laryngology and its related specialties | 10.1159/000534079 | 472 patients diagnosed with cN0 HNSCC who underwent up-front surgery. | HNSCC | Baseline neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), systemic inflammatory marker (SIM), and systemic immune-inflammation index (SII) were calculated from available blood parameters. | Oro-hypopharyngeal and oral cancers, locally advanced stage were associated with an increased risk of pathological lymph node involvement. NLR, LMR, PLR, SIM, and SII were significantly associated at multivariable analysis. NLR >2.12 was the most reliable at predicting occult lymph node metastasis | OR = 5.22; 95% CI: 2.14-12.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



