
Submitted:
26 April 2024
Posted:
28 April 2024
You are already at the latest version
Abstract
Background: Self-harm (SH) refers to self-injury or intentional self-poisoning with varying degrees of suicidal intent and is a major public health issue for children and adolescents (C&A) worldwide. Given significant gaps exist in our understanding of the associated psychopathology in C&A, this paper outlines the protocol for a prospective clinical study examining risk factors of SH and additional candidate parameters (not routinely assessed) during an acute SH episode. Methods: The EXPAAND (EXploring Psychiatric and Attentional risk-factors in Adolescents Needing intervention for Deliberate self-harm) is a randomised control trial to assess additional novel candidate risk factors for SH in C&A and to evaluate the effectiveness of SH-targeted brief psychological intervention (Therapeutic Assessment (TA)), within a real-world acute clinical setting, as we include neurodiversity and gender diversity in this study. EXPAAND is conducted in 4 phases: (i) recruitment & randomisation; (ii) extended assessment; (iii) randomised intervention; and (iv) follow-up observational period to ascertain clinical outcomes for comparison. Expected Results: We envisage that by diagnosing and treating attentional disorders when detected will mitigate potential confounding effects of these conditions. We also expect that SH-focused TA will be effective in reducing subsequent SH and in improving engagement in follow-up and subsequent treatments.
Keywords:
self-harm
; children and adolescents
; neurodiversity
; ADHD
; gender diversity
; psychotherapy
Introduction
There has been a significant increase in the of number children and adolescents (C&A) presenting with self-harm (SH) to hospital emergency departments (ED), highlighting the urgency of this problem, its personal and societal costs, as well as the high service burden to acute medical and mental health services [1,2,3]. Our EXPAAND (Exploring Psychiatric And Attentional risk-factors in Adolescents Needing intervention for Deliberate self-harm) project aims to improve understanding of SH, its risk drivers, and more effective treatments for this population, which is at a significantly higher risk of death by suicide [17].
One in five individuals who die by suicide have visited the ED within 4 weeks of their death [4]. ED provides a catch-all service for C&A and families in distress and a critical entry point for youth suicide prevention [5]. Among adolescents, there is a global trend of increased ED visits for mental health crisis, including SH, particularly among females [6,7,8]. Within the past decade, Western Australian EDs have experienced an unprecedent 214% increase in SH presentations of 13 to 17-year-olds, and a corresponding 403% increase in the under 13-year-olds [9]. In Australia nationwide, SH presentations to EDs have tracked similar upward trends, with the greatest increase in attendance by the younger females [2]. A recent Australian study reported an increase in ED presentations with suicidal risk by individuals aged 10–24 years between 2015 and February 2020 (pre-COVID) with an 8.4% per annum increase, further increasing to 19.2% from March 2020 into 2021 (during COVID pandemic) [10]. Similar increases were observed internationally during pandemic with a shift towards more ED presentations from SH and with higher suicide risk (versus ED presentations relating to depressive and anxiety symptoms), resulting in more inpatient mental health admissions [8,11,12,13,14].
Graded exposure to SH desensitizes young people to potentially life-threatening suicidal behaviors with an associated dose-response relationship, yielding a ten-fold increased risk of suicidal behaviour in young people, independent of depressive symptoms [15]. Wilkinson and colleagues provided support to Joiner’s interpersonal-psychological theory of suicide [16], underscoring the ‘acquired capability’ of suicide that habituates the innate fear of death and closes the gap between thought and action. A more recent prospective study by Hawton and colleagues provides further support for Joiner’s theory. They reported a higher 12-month incidence of suicide in individuals aged 10-18 years with repeated SH that amounted to 30 times higher than the expected rate in the general population [17]. As such, chronicity (i.e., recurrence) of SH can be considered a proxy index of severity in SH.
The rate of re-presentation at EDs is a well-established measure of escalating SH, but only small number of studies focused specifically on younger population. A large study from the Irish national self-harm registry reported 19.2% of individuals aged 10–29 years returning to ED within 12 months; and of these, adolescent females of 15–19 years old were at a higher risk of re-attempts than young adults [18]. Consistent with previous literature, the repetition of SH and the number of self-harm episodes were positively correlated, while increasing age, cutting as the method of self-harm, and history of psychiatric treatment were all found to be the independent risk factors (RFs) for repetition [18]. An Australian study (n=952) yielded slightly higher representation rate of 23% within 12 months, but for those with three or more prior presentations, the rates of re-presentation were even higher with 62% at 12 months [19]. Longitudinally, the Multicentre Study of Self-harm in England (N = 3920) found that repetition of SH occurred in 27.3% of individuals aged 10-18 years between 2000 and 2007 [20] and identified that self-cutting as a method of SH in C&A conveys greater risk of repetition and of suicide than self-poisoning [20]. Also in UK, Geulayov and colleagues provided a rare insight into the longitudinal pattern of SH presentation for very young patients [21]; and reported 13.5% recurrence rate over a 12-month period for children with SH, with repetition being more common for girls than boys. More specifically, repetition after the index episode occurred in 8.5% of 11-year-olds and in 17.9% of the 12-year-olds. Overall, recurring SH remains a very high-RF of overall poor outcomes, especially among individuals with high-volume repeat self-harm attendances and with previous SH predicting future SH [22].
Well-established drivers of SH include: borderline personality traits (especially those reflective of intrapersonal functions - emotion-regulation, avoidance of aversive affect and self-punishment) [23]; post-traumatic stress disorder, specifically among females [24]; mood disorders, particularly melancholic depressive or bipolar disorder [25]; anxiety disorders, especially in combination with mood disorders; substance use, an independent RF for SH [26]; and disordered eating symptoms, with impulsivity found to be a significant unique predictor of SH, a shared RF for bulimic symptoms [27]. More recent literature reports dissociative symptoms [30], Sluggish Cognitive Tempo (SCT; now known as Cognitive Disengagement Syndrome) [31], and alexithymia problems [28,29], which are transdiagnostic symptoms, are associated with SH. Dissociation compromises judgement and mediates the relationship between SH and experience of trauma [30]. Alexithymia, a trait characterised by difficulties identifying and expressing one’s own emotions [32], is a strong predictor of SH in an adult population, over and above depression. Alexithymia is thought to hinder emotion regulation processes [33] thereby increasing risk of SH. EXPAAND aims to capture this broader range of RFs to evaluate their clinical relevance and potential utility.
Recent literature reports significant associations between ADHD and SH [34]. Septier and colleagues' systematic review and meta-analysis found a significant association between ADHD and suicidal ideations, suicidal plans, suicidal attempts, and completed suicide (pooled Odds Ratio=6.69; 95% CI, 3.24-17.393) [35]. Apart from ADHD being an important driver of SH, independent from other covariates, further studies indicate that treatments of ADHD reduce the subsequent risks of SH [36,37]. Liu and colleagues reported that ADHD medication lowered the odds of suicide attempts by 0.76 (95% CI, 0.58-1.00; P = .049) at population-level analysis, whilst the individual level of analysis showed a 0.69 reduction [36]. Lieslethto and colleagues utilised the national Swedish register database to examine 22,601 individuals with BPD and the link between different interventions and subsequent SH and completed suicide in individuals with BPD [38]; and found that ADHD medication treatment reduced the risk of attempted or completed suicide (HR, 0.83; 95% CI, 0.73-0.95 P = .001), with lisdexamphetamine and methylphenidate showing significant reductions. Overall, the combined findings suggest that ADHD medication intervention can potentially reduce the risk of suicidal attempts for those with ADHD [36]; and for those with comorbid BPD [38]. By inference, any study examining the predictors of SH and potential psychological intervention approaches must evaluate the presence of ADHD and mitigate its influence in its study design. The EXPAAND study therefore provides a novel innovation, in accounting for the confounding effects of ADHD as a key focus and methodological consideration (see Method and Analysis section below).
Despite an increasing body of research on SH, rates of C&A SH continue to increase [39,40,41], suggesting significant gaps in our understanding of psychopathological and pivotal drivers; and addressing these is an urgent priority for suicide prevention. As an innovation, EXPAAND aims to address these gaps, by capturing a broader range of contributing phenomena and thereby providing novel insights to inform more efficacious treatment - within real-life clinical settings, inclusive of gender diversity and neurodiversity.
Another key focus of EXPAAND is to evaluate the effectiveness of a brief psychological intervention for SH - Therapeutic Assessment (TA) [42]. TA has been developed to target SH, especially in adolescents and differs from traditional Therapeutic Assessment approach, which was first developed by Finn [43,44,45]. TA utilises information taken for SH-related psychosocial and risk assessments to inform patients and develop new strategies to reduce SH recurrence. It is a brief intervention that can be completed within 60-90 minutes and utilises elements of cognitive-behavioural and analytic therapy approaches by co-constructing a cycle diagram, which discovers and identifies SH triggers, maladaptive coping strategies and the psychological, physiological, and interpersonal drivers that maintain SH cycles. The therapist and young person co-construct an understanding of the young person’s difficulties, this new perspective enhances motivation for change and develops individualised strategies, including proactive utilisation of identified protective factors in the young person’s family and social systems, as alternatives for SH. The young person is then invited to select problems to target, within a motivational framework, followed by exploring alternative solutions to these problems, called ‘Exits’. The intervention is consolidated in the form of a Therapeutic Letter, which serves as a record and guide for the client when they next experience crisis.
TA has been manualised [42] and has been included in the 2015 Cochrane Review of effective interventions for self-harm in C&A [46], as it demonstrated improved engagement in treatments [47] and at 2-year follow-up [48].
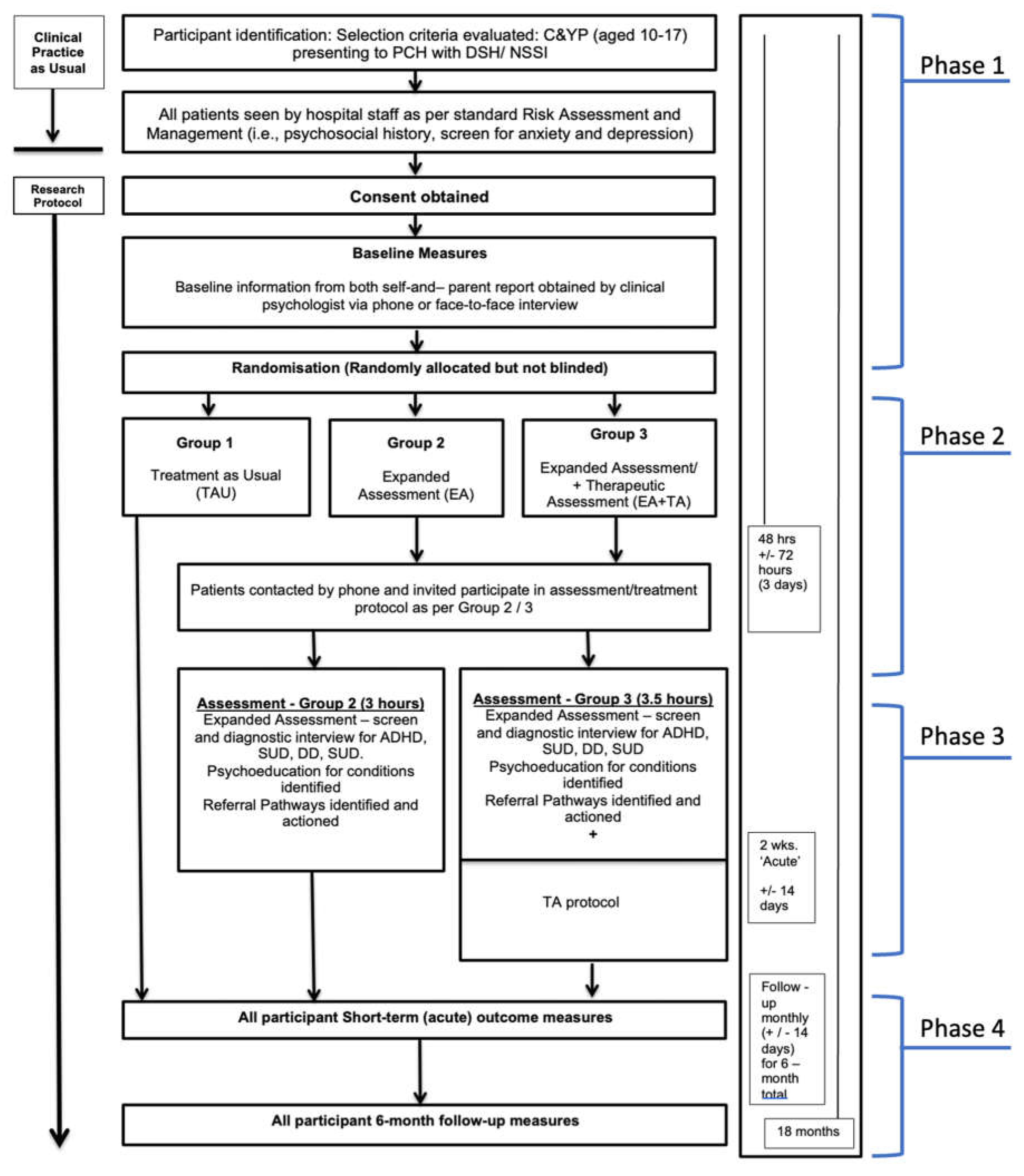
Figure 1.
Summary of 4 phases of EXPAAND.
Experimental Design
Aims and Hypotheses
EXPAAND has two key aims, underpinned by two main hypotheses. First aim, is to capture a broad range of RF in its routine assessment via range of psychometric measures, and examine the rates/relevance of these constructs in C&A who present with SH crisis in ED. Second, is to evaluate TA, as an effective brief psychological intervention, in the context of providing extended assessment and treatment of ADHD and SCT when detected. These objectives will be accomplished across 4 phases of this study.
Phase 1 includes recruitment, screening, and randomisation of C&A patients presenting to ED. Phase 2 explores SH pathways of drivers by Extended Assessment (EA), involving an intensive diagnostic and profiling assessment. This is followed by Phase 3, an Intervention Comparison, to explore the effect of TA as a brief intervention. As ADHD is a significant driver of SH independent of other covariates, we consider that it will likely be important to treat ADHD to mitigate its impacts on confounding the effects of TA. Phase 3 therefore includes three arms: (i) Arm 1 is treatment as usual (TAU), (ii) Arm 2 includes EA plus ADHD treatment if indicated (i.e. EA(+ADHDmed)1), and (iii) Arm 3 includes Arm 2 interventions augmented by TA (EA(+ADHDmed)+TA). The recruitment, consent, blinding, and randomisation processes, as well as data collection, management statistical analyses, monitoring processes are described in detail in the Method section. In Phase 4, we are following-up participants for 6-months, capturing re-presentation rates to ED, with further self-harm episodes as the main outcome parameter.
Our first hypothesis is that there exists a range of diagnostic and transdiagnostic mechanisms driving SH in C&A, and some of these are not routinely assessed in C&A within the acute SH episodes. In addition to conventional well-established RF (such as borderline traits, substance use, trauma, and PTSD), we expect that ADHD [37], SCT [31], Dissociative Disorder [30] and Alexithymia [28,29], are also key drivers. We aim to capture these phenomena via validated psychometric tools and evaluate quantitatively their associations with SH in C&A. Moreover, we will evaluate whether there is a dose-response relationship between these RF and the chronicity of SH (i.e., recurrent SH episodes). These aims will be accomplished by Phase 1 and 2 of EXPAAND.
Secondly, we hypothesize that TA [42] adapted for SH, will be effective in reducing subsequent SH. This is because SH-focused TA specifically help C&A to identify cues and reasons for SH and consider exit points in the cycle of SH [47]. We aim to evaluate the effectiveness of TA via a nested RCT within EXPAAND, executed in Phase 3 and 4. As ADHD and SCT are known significant drivers of SH independent of other covariates, we consider it important to diagnose and treat these attentional problems to avoid these confounding and diluting the effects of TA. For these reasons, Phase 3 also includes screening for ADHD and SCT, and diagnosing and treating these when detected. We expect that patients in Arm 2, and especially Arm 3, will experience reduced clinical symptoms (episodes of SH), improved engagement with treatment, and reduced health service usage, as compared to Arm 1 TAU.
Materials and Methods
Trial Design and Conceptual Framework
This manuscript is prepared in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines (see Supplementary Material for the SPIRIT 33 item checklist [49];EXPAAND consists of a nested interventional trial, with a three-arm (parallel group) randomised controlled trial, within a larger study.
Study Setting
This study is conducted in the ED of Perth Children’s Hospital (PCH), a tertiary paediatric hospital with 298-bed capacity. It is the only state-wide specialist children’s hospital located in Perth (with a population of 2.7 million), Western Australia. PCH includes specialised metropolitan C&A mental health services.
Eligibility Criteria
To be eligible for study participation, patients must be between 10-17 years of age, present to the PCH ED after an episode of SH during the study recruitment period, and assent to comply with study procedures. Their parents/caregivers must also consent to their participation.
Patients are excluded from the study if they meet the criteria for psychosis (ICD-10: F20-29), or have intellectual disability (profound, severe, moderate, or mild). Other exclusion criteria include pregnancy, lack of consent, or lack of concordance for consent between parent and patient.
Sample Size
The sample size is based on a power calculation to detect a statistically significant difference between the intervention and control group of a small-to-medium effect size (Cohen's f of 0.175) after 6 months. Based on an audit of clinical records in 2019, we calculated that we would be able to recruit at least 300 participants over a 12-month period. The project time frame is a 12-month recruitment and assessment phase, followed by 6-months follow-up phase, for a total timeframe of 18-months. For each participant individually, study participation will involve a total 6-month timeframe from assessment to follow-up.
Phase 1: Participant Recruitment and Study procedures
C&A and their parents/caregivers are given the option to participate in EXPAAND when they access routine care as usual at the PCH ED. This is communicated via the Mental Health Clinical Nurse Specialist, or the Clinical Psychologist, or Project Co-Ordinator (ZP). ‘Treatment as usual’ in PCH ED is not impacted or altered by this research project.
All patients are given initial screening with psychometric questionnaires, as detailed in the Table 1. All recruited participants are screened, and then randomised into three intervention groups: (i) Arm 1 is treatment as usual (TAU), (ii) Arm 2 includes EA plus ADHD treatment if indicated (i.e. EA(+ADHDmed)), and (iii) Arm 3 includes Arm 2 interventions augmented by TA.
Detailed Procedure
Randomization process: Randomisation is stratified by (i) gender and (ii) history of repeated SH. Treatment allocation is carried out by computer-generated minimisation, incorporating weighted randomisation using a local implementation of the MimimPy algorithm [53] assigned to one of the 3 arms described above. The weighted randomisation gives an 80% probability of each participant being allocated the treatment that minimised existing imbalances across strata defined by gender (coded as ‘male’, ‘female’, or ‘other’) and index presentation type (First-time/Recurrent). The software is accessible on a secure local server and treatment allocation is ascertained by the Principal Investigator upon completion of the consent process and recruitment. Beside gender, SH participants are classified into two groups: (i) those of first-time presentation of SH to ED, and (ii) those with ‘repeated SH’ (defined as ‘second or more presentation of SH to ED’). During follow-up assessments after 6 months, the outcome assessor remains blinded regarding a participant's condition.
Phase 2: Expanded assessment
Part 1: Ascertaining drivers and risk factors of SH – An extensive battery of psychiatric assessment measures and semi-structured diagnostic interviews was ascertained from participants randomized to Arm 2 and 3, as detailed in Table 2. SH and chronicity of SH is evaluated for associations with these measures.
These measures are selected based on a review and critical appraisal of contemporary literature, which identified several measurable and potentially treatable traits and disorders of psychopathology associated with SH. These parameters capture potential novel candidate RFs for SH in C&A and will be explored in real life clinical settings, inclusive of gender diversity and neurodiversity. Naturally, an increased understanding of these conditions and diagnoses - specifically the processes and mechanisms that underlie them with regards to difficulties with emotional regulation and impulsivity in the context SH - will represent a significant enrichment of current understanding of escalating SH in C&A. This process will inform development of more effective treatments. More specifically, apart from examining conventional RFs for SH, EXPAAND will also evaluate the links of SH and severity with the symptoms of ADHD [37], SCT [31], dissociation [30] and alexithymia [28,29]. Phase 2 data will provide opportunities to explore these.
Part 2 Assessing and diagnosing ADHD and SCT. To mitigate the extent of ADHD confounding the treatment effect of TA, we screen and assess ADHD and SCT using research-standard semi-structured interviews (i.e., K-SADS-PL [63] and BSCTS-CA [64]). When confirmed, participants are offered the opportunities for further clinical evaluation and treatment by our paediatrician at PCH (C.D) when participants enter Phase 3 described below.
Phase 3 Nested RCT of three groups:
(i) Arm 1 - TAU, (ii) Arm 2 - Expanded Assessment (EA(+ADHDmed) and (iii) Amr 3 - Expanded Assessment augmented by Therapeutic Assessment intervention (EA(+ADHDmed)+TA)
Management of TAU Group:
Treatment-as-usual (TAU) group
The TAU group is managed according to the standard protocol, stipulated in the ‘Clinical Care as Usual Protocol’ at PCH ED for C&A. This protocol specifies the process by which a young person is triaged by an ED Nurse who provides an initial assessment; and if required, the young person is then treated by an ED doctor (i.e., a junior doctor, supervised by a Consultant Paediatric Emergency Physician). If a patient is referred for mental health assessment by a Clinical Nurse Specialist or Mental Health Nurse, they receive psycho-social assessment, including screening for a standard battery of co-morbid mental health conditions, such as depression and anxiety, and SH risk assessment (including risk and protective factors) to inform a Risk Management Plan.
The standard Care Plan (i.e., discharge plan) may lead to: (i) admission to the mental health ward for further risk containment; or (ii) discharge into the community, where standard procedure includes a follow-up with a sub-acute appointment within one-week at a community mental health clinic or a mental health clinician in the private sector. At all times, participants in the study are encouraged to engage in their existing treatments.
Management of Arm 2 and Arm 3 Groups:
The participants, who are randomly allocated to Arm 2 (EA(+ADHDmed) or Arm 3 (EA(+ADHDmed)+TA), are given additional resources embedded within the study protocol, above and beyond the standard care.
Arm 3 participants are given TA [24], which includes following major components that are summarised in Table 3.
Phase 4: Procedures to obtain outcome measures for three group comparisons (i.e., TAU vs ‘EA(+ADHDmed)’ vs ‘EA(+ADHDmed)+TA’)
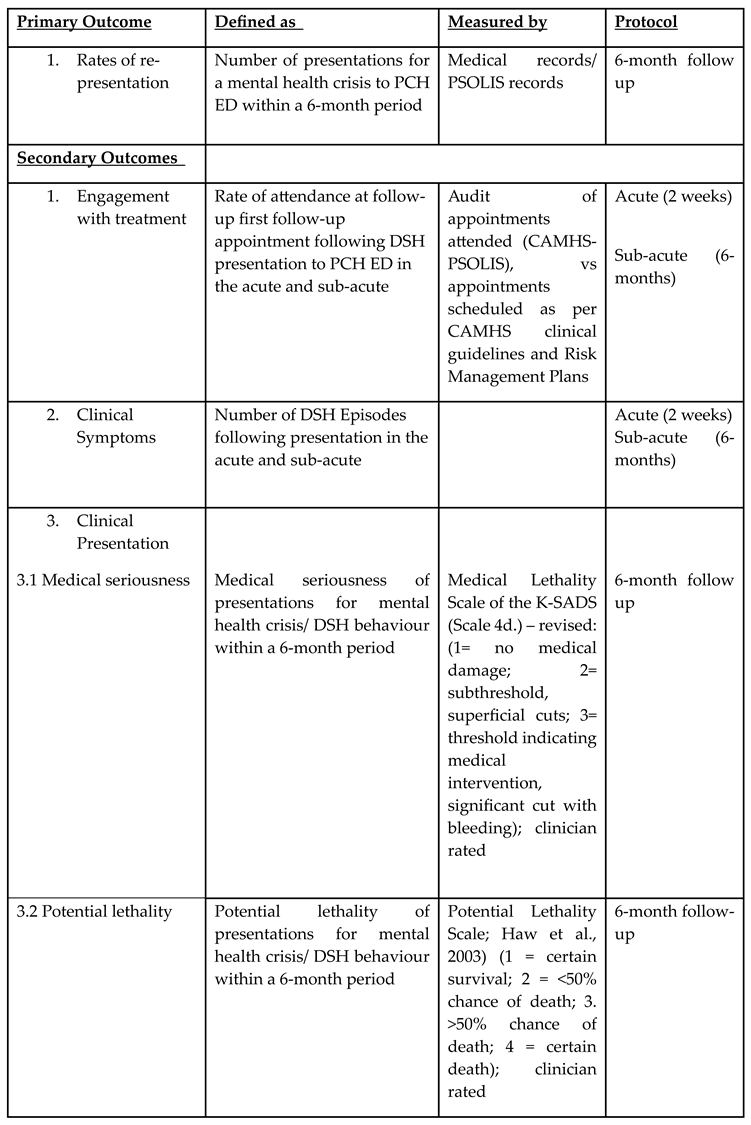
In Phase 4, we utilise standardised outcome measures to evaluate the effects of Phase 3 RCT interventions. This final phase involves a naturalistic observation component, whereby service utilization (i.e., re-presentation to ED with further SH episode) by participants is captured and mapped over a 6-month period. Participants’ clinical characteristics are also recorded as part of their clinical trajectory and linked with the morbidity index of SH behavior (i.e., ‘first-time presentation’ vs ‘recurrent SH presentation’ as designated in Phase 1 during the first index episode).
Details of outcome measures for this project are summarised in Table 4.
Data Analysis
The study outcomes are examined by multivariate analyses, including logistic regression, difference-in-difference regression, and Poisson regression. Continuous variables are analysed by ANOVAs with respect to group comparisons. This study includes descriptive and hypothesis-testing statistical analyses of multi-source psycho-social, psychometric, and diagnostic data.
Addressing and Mitigating Information Bias
The decisions on primary and co-morbid clinical syndromes are reviewed by a panel of at least three clinicians (Consultant Psychiatrist, Consultant Paediatrician, and Clinical Psychologist). Clinical review meetings are held on a fortnightly basis. Clinical decisions are made on the basis that a majority rule (63%) is reached.
Ethics and Dissemination
Ethical approval from the ethics committee of the Government of WA Health Ethics has been obtained (RGS0000003060). We will publish the results in peer-reviewed journals, and present at conferences, continuing professional development events, and consumer and carer events. Findings will be shared with professional and consumer organisations, to promote translation into health care practices.
We will provide participants communications about this study in peer-reviewed journals, and conference presentations. We will present our findings to clinicians in general medical practitioners, general practice clinicians and psychiatrists.
Expected Results
The prevalence of ADHD in clinical populations has been reported to vary. In adult clinical populations, prevalence ranges from 7% to 39% [50] and 13% to 47% [51]. In youth populations, one study in adolescents admitted to ED with suicidal attempts reported 65% prevalence of ADHD, which was more common than major depression in this group (43.5 %); other characteristics of this sample included predominance of females, very few having confirmed ADHD diagnosis and majority exhibiting symptoms associated with the inattentive subtype of ADHD [52]. Given the magnitude of variability in the literature, we cannot predict the precise prevalence of ADHD/SCT in the EXPAAND sample, or the extent to which ADHD/SCT can confound and dilute the effects of TA. For these reasons, we include in EXPAAND a research-standard routine diagnostic assessment for ADHD/SCT for all patients in the two intervention arms, and subsequent pharmacotherapy for those who are diagnosed positive for ADHD/SCT and consent to receive treatments. However, EXPAAND is not powered to test the sole effect of diagnosing and treating ADHD, due to the unpredictability of ADHD/SCT prevalence in clinical samples. Nevertheless, post-hoc analysis of such an effect may become available if the ADHD prevalence is high in EXPAAND, thereby yielding enough participants with ADHD within Arms 2 and 3 for meaningful comparisons. In terms of expected results, we envisage that by diagnosing and treating ADHD and SCT when detected we will mitigate potential confounding effects of these conditions, which will result in reduced episodes of SH, improved engagement with treatment, and reduced health service usage.
We also expect that SH-focused TA will be effective in reducing subsequent SH and in improving engagement in follow-up and subsequent treatments. This is because TA demonstrated clinical effectiveness for SH in C&A [46,47] and at 2-year follow-up [48]. TA is a manualised brief intervention in reducing suicidality, and its effectiveness has not been evaluated in its application for participants recruited from ED during acute suicidal crisis. It is a short intervention, and EXPAAND can potentially evaluate its cost-effectiveness within an acute SH episode, given SH individuals often do not attend subsequent community follow-up appointments after the crisis episode.
Conclusions
The EXPAAND project represents an innovative approach to studying SH in C&A within an acute clinical setting. To evaluate a wider broader spectrum of risk factors and drivers of SH, EXPAAND assesses a broad range of psychiatric and attention-spectrum phenomena, many of which are ‘blind spots’ in conventional acute care. EXPAAND also includes a nested RCT to test the effectiveness of TA in this high-risk population of young people. EXPAAND is also novel and innovative in its methodological design by mitigating the potential effects of ADHD and SCT confounding and diluting the intervention effects of TA by evaluating, diagnosing, and treating these conditions. Overall, EXPAAND, to our knowledge, is a highly innovative study on SA in C&A embedded in real life clinical settings, and is inclusive of both gender diversity and neurodiversity.
Acknowledgements
This project has been developed via collaboration between research team members as well as other medical professionals, the CAHS Research Support team, including consultation with a Biostatistician. The project received the major beneficiary grant from Chanel 7 Telethon Trust and PCH Foundation.
| 1 | *(ADHD med) is bracketed, as it is not given to all participants in Arm 2 and 3, but given only to those with pre-existing ADHD diagnosis, or those who are diagnosed with ADHD de novo during EXPAAND Phase 2 and consent to taking ADHD medications. |
References
- Hawton K: Saunders KE, O’Connor RC. Self-harm and suicide in adolescents. The Lancet. 2012 Jun 1;379(9834):2373–82. [CrossRef]
- Torok M, Burnett AC, McGillivray L, et al. Self-harm in 5-to-24 year olds: Retrospective Examination of Hospital Presentations to emergency departments in New South Wales, Australia, 2012 to 2020. PLOS ONE. 2023 Aug 10;18(8). [CrossRef]
- Neufeld SAS. The burden of young people’s mental health conditions in Europe: No cause for complacency. The Lancet Regional Health - Europe. 2022 May;16:100364. [CrossRef]
- Quinlivan L, Cooper J, Meehan D, et al. Predictive accuracy of risk scales following self-harm: multicentre, prospective cohort study. Br J Psychiatry. 2017;210(6):429-436. [CrossRef]
- National Mental Health Commission. Monitoring mental health and suicide prevention reform: National Report 2019. Sydney: NMHC; 2019.
- Krass P, Dalton E, Doupnik SK, Esposito J. US Pediatric Emergency Department visits for mental health conditions during the COVID-19 pandemic. JAMA Network Open. 2021 Apr 30;4(4). [CrossRef]
- Holland KM, Jones C, Vivolo-Kantor AM, et al. Trends in US Emergency Department Visits for Mental Health, Overdose, and Violence Outcomes Before and During the COVID-19 Pandemic. JAMA Psychiatry. 2021;78(4):372-379. [CrossRef]
- Yard E, Radhakrishnan L, Ballesteros MF, et al. Emergency Department Visits for Suspected Suicide Attempts Among Persons Aged 12-25 Years Before and During the COVID-19 Pandemic - United States, January 2019-May 2021. MMWR Morb Mortal Wkly Rep. 2021;70(24):888-894. Published 2021 Jun 18. [CrossRef]
- Ombudsmun WA. Volume 1: Ombudsman’s Foreword and Executive Summary. Western Australia; 2020.
- Sara G, Wu J, Uesi J, et al. Growth in emergency department self-harm or suicidal ideation presentations in young people: Comparing trends before and since the COVID-19 first wave in New South Wales, Australia. Aust N Z J Psychiatry. 2023;57(1):58-68. [CrossRef]
- Shankar LG, Habich M, Rosenman M, et al. Mental Health Emergency Department Visits by Children Before and During the COVID-19 Pandemic. Acad Pediatr. 2022;22(7):1127-1132. [CrossRef]
- Racine N, McArthur BA, Cooke JE, et al.Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-analysis. JAMA Pediatr. 2021;175(11):1142-1150. [CrossRef]
- Ougrin D, Wong BH, Vaezinejad M, et al. Pandemic-related emergency psychiatric presentations for self-harm of children and adolescents in 10 countries (PREP-kids): a retrospective international cohort study. Eur Child Adolesc Psychiatry. 2022;31(7):1-13. [CrossRef]
- Woo HG, Park S, Yon H, et al. National Trends in Sadness, Suicidality, and COVID-19 Pandemic-Related Risk Factors Among South Korean Adolescents From 2005 to 2021. JAMA Netw Open. 2023;6(5):e2314838. Published 2023 May 1. [CrossRef]
- Joiner TE Jr, Brown JS, Wingate LR. The psychology and neurobiology of suicidal behavior. Annu Rev Psychol. 2005;56:287-314. [CrossRef]
- Wilkinson P, Goodyer I. Non-suicidal self-injury. Eur Child Adolesc Psychiatry. 2011;20(2):103-108. [CrossRef]
- Hawton K, Bale L, Brand F, et al. Mortality in children and adolescents following presentation to hospital after non-fatal self-harm in the Multicentre Study of Self-harm: a prospective observational cohort study. Lancet Child Adolesc Health. 2020;4(2):111-120. [CrossRef]
- Bennardi M, McMahon E, Corcoran P, et al. Risk of repeated self-harm and associated factors in children, adolescents and young adults. BMC Psychiatry. 2016;16(1):421. Published 2016 Nov 24. [CrossRef]
- Summers P, O'Loughlin R, O'Donnell S, et al. Repeated presentation of children and adolescents to the emergency department following self-harm: A retrospective audit of hospital data. Emerg Med Australas. 2020;32(2):320-326. [CrossRef]
- Hawton K, Bergen H, Kapur N, et al. Repetition of self-harm and suicide following self-harm in children and adolescents: findings from the Multicentre Study of Self-harm in England. J Child Psychol Psychiatry. 2012;53(12):1212-1219. [CrossRef]
- Geulayov G, Casey D, Bale L, et al. Self-harm in children 12 years and younger: characteristics and outcomes based on the Multicentre Study of Self-harm in England. Soc Psychiatry Psychiatr Epidemiol. 2022;57(1):139-148. [CrossRef]
- Plener PL, Schumacher TS, Munz LM, Groschwitz RC. The longitudinal course of non-suicidal self-injury and deliberate self-harm: a systematic review of the literature. Borderline Personal Disord Emot Dysregul. 2015;2:2. Published 2015 Jan 30. [CrossRef]
- Taylor PJ, Jomar K, Dhingra K, et al. A meta-analysis of the prevalence of different functions of non-suicidal self-injury [published correction appears in J Affect Disord. 2019 Dec 1;259:440]. J Affect Disord. 2018;227:759-769. [CrossRef]
- Eskander N, Vadukapuram R, Zahid S, et al. Post-traumatic Stress Disorder and Suicidal Behaviors in American Adolescents: Analysis of 159,500 Psychiatric Hospitalizations. Cureus. 2020;12(5):e8017. Published 2020 May 7. [CrossRef]
- Parker, G. & Ricciardi, T. (2019). The Risk of Suicide and Self-Harm in Adolescents Is Influenced by the “Type” of Mood Disorder. The Journal of Nervous and Mental Disease, 207 (1), 1-5. [CrossRef]
- Gili M, Castellví P, Vives M, et al. Mental disorders as risk factors for suicidal behavior in young people: A meta-analysis and systematic review of longitudinal studies. J Affect Disord. 2019;245:152-162. [CrossRef]
- Krug I, Arroyo MD, Giles S, et al. A new integrative model for the co-occurrence of non-suicidal self-injury behaviours and eating disorder symptoms. J Eat Disord. 2021;9(1):153. Published 2021 Nov 22. [CrossRef]
- Preece DA, Mehta A, Becerra R, et al. Why is alexithymia a risk factor for affective disorder symptoms? The role of emotion regulation. J Affect Disord. 2022;296:337-341. [CrossRef]
- Norman H, Oskis A, Marzano L, Coulson M. The relationship between self-harm and alexithymia: A systematic review and meta-analysis. Scand J Psychol. 2020;61(6):855-876. [CrossRef]
- Hoyos C, Mancini V, Furlong Y, et al. The role of dissociation and abuse among adolescents who self-harm. Aust N Z J Psychiatry. 2019;53(10):989-999. [CrossRef]
- Becker SP, Leopold DR, Burns GL, et al. The Internal, External, and Diagnostic Validity of Sluggish Cognitive Tempo: A Meta-Analysis and Critical Review. J Am Acad Child Adolesc Psychiatry. 2016;55(3):163-178. [CrossRef]
- Preece, D. A., & Gross, J. J. (2023). Conceptualizing alexithymia. Personality and Individual Differences, 215, [112375]. [CrossRef]
- Preece DA, Mehta A, Petrova K, et al. Alexithymia and emotion regulation. J Affect Disord. 2023;324:232-238. [CrossRef]
- Allely CS. The association of ADHD symptoms to self-harm behaviours: a systematic PRISMA review. BMC Psychiatry. 2014;14:133. Published 2014 May 7. [CrossRef]
- Septier M, Stordeur C, Zhang J, et al. Association between suicidal spectrum behaviors and Attention-Deficit/Hyperactivity Disorder: A systematic review and meta-analysis. Neurosci Biobehav Rev. 2019;103:109-118. [CrossRef]
- Liu WJ, Mao HJ, Hu LL, et al. Attention-deficit/hyperactivity disorder medication and risk of suicide attempt: A meta-analysis of observational studies. Pharmacoepidemiology and drug safety. 2020 Nov;29(11):1364-72.
- Chen W, Taylor E. Resilience and self-control impairment. Handbook of resilience in children: Springer; 2023. p. 175-211.
- Lieslehto J, Tiihonen J, Lähteenvuo M, et al. Comparative Effectiveness of Pharmacotherapies for the Risk of Attempted or Completed Suicide Among Persons With Borderline Personality Disorder. JAMA Netw Open. 2023;6(6):e2317130. Published 2023 Jun 1. [CrossRef]
- Gillies D, Christou MA, Dixon AC, et al. Prevalence and Characteristics of Self-Harm in Adolescents: Meta-Analyses of Community-Based Studies 1990-2015. J Am Acad Child Adolesc Psychiatry. 2018;57(10):733-741. [CrossRef]
- Borschmann R, Kinner SA. Responding to the rising prevalence of self-harm. Lancet Psychiatry. 2019;6(7):548-549. [CrossRef]
- Zetterqvist M, Jonsson LS, Landberg Å, Svedin CG. A potential increase in adolescent nonsuicidal self-injury during covid-19: A comparison of data from three different time points during 2011 - 2021. Psychiatry Res. 2021;305:114208. [CrossRef]
- Ougrin D, Zundel T, Ng AV. Self-harm in young people: A therapeutic assessment manual: CRC Press; 2009.
- Finn SE, Tonsager ME. How therapeutic assessment became humanistic. The Humanistic Psychologist. 2002;30(1-2):10-22. [CrossRef]
- Finn SE, Fischer CT, Handler L. Collaborative/therapeutic assessment: Basic concepts, history, and research. Collaborative/therapeutic assessment: A casebook and guide. Hoboken, NJ, US: John Wiley & Sons Inc; 2012. p. 1-24.
- Finn B. Exploring interactions between motivation and cognition to better shape self-regulated learning. Journal of Applied research in Memory and Cognition. 2020;9(4):461-7. [CrossRef]
- Hawton K, Witt KG, Taylor Salisbury TL, et al. Interventions for self-harm in children and adolescents. Cochrane Database Syst Rev. 2015;2015(12):CD012013. Published 2015 Dec 21. [CrossRef]
- Ougrin D, Zundel T, Ng A, et al. Trial of Therapeutic Assessment in London: randomised controlled trial of Therapeutic Assessment versus standard psychosocial assessment in adolescents presenting with self-harm. Arch Dis Child. 2011;96(2):148-153. [CrossRef]
- Ougrin D, Boege I, Stahl D, et al. Randomised controlled trial of therapeutic assessment versus usual assessment in adolescents with self-harm: 2-year follow-up. Arch Dis Child. 2013;98(10):772-776. [CrossRef]
- Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 Statement: defining standard protocol items for clinical trials. Rev Panam Salud Publica. 2015;38(6):506-514.
- Gerhand S, Saville CWN. ADHD prevalence in the psychiatric population. Int J Psychiatry Clin Pract. 2022;26(2):165-177. [CrossRef]
- Adamis D, Flynn C, Wrigley M, et al. ADHD in Adults: A Systematic Review and Meta-Analysis of Prevalence Studies in Outpatient Psychiatric Clinics. J Atten Disord. 2022;26(12):1523-1534. [CrossRef]
- Manor I, Gutnik I, Ben-Dor DH, et al. Possible association between attention deficit hyperactivity disorder and attempted suicide in adolescents - a pilot study. Eur Psychiatry. 2010;25(3):146-150. [CrossRef]
- Saghaei M, Saghaei S. Implementation of an open-source customizable minimization program for allocation of patients to parallel groups in clinical trials. J Biomed Sci Eng. 2011;4(11):734-9. [CrossRef]
- Swanson J, Deutsch C, Cantwell D, et al. Genes and attention-deficit hyperactivity disorder. Clinical Neuroscience Research. 2001;1(3):207-16. [CrossRef]
- Becker SP, Luebbe AM, Joyce AM. Child Concentration Inventory. Psychological Assessment. 2015. [CrossRef]
- Knight JR, Sherritt L, Harris SK, et al. Validity of brief alcohol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcohol Clin Exp Res. 2003;27(1):67-73. [CrossRef]
- Knight JR, Sherritt L, Shrier LA, et al. Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Arch Pediatr Adolesc Med. 2002;156(6):607-614. [CrossRef]
- Armstrong JG, Putnam FW, Carlson EB, et al. Development and validation of a measure of adolescent dissociation: the Adolescent Dissociative Experiences Scale. J Nerv Ment Dis. 1997;185(8):491-497. [CrossRef]
- Preece D, Becerra R, Robinson K, et al. The psychometric assessment of alexithymia: Development and validation of the Perth Alexithymia Questionnaire. Personality and Individual Differences. 2018;132:32-44. [CrossRef]
- Zapolski TC, Stairs AM, Settles RF, et al. The measurement of dispositions to rash action in children. Assessment. 2010;17(1):116-125. [CrossRef]
- Whiteside, S.P. and Lynam, D.R. (2001) The Five Factor Model and Impulsivity: Using a Structural Model of Personality to Understand Impulsivity. Personality and Individual Differences, 30, 669-689. [CrossRef]
- Gullone E, Taffe J. The Emotion Regulation Questionnaire for Children and Adolescents (ERQ-CA): a psychometric evaluation. Psychol Assess. 2012;24(2):409-417. [CrossRef]
- Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980-988. [CrossRef]
- Barkley RA. Barkley sluggish cognitive tempo scale--children and adolescents (BSCTS-CA): Guilford Publications; 2018.
- Ross CA, Duffy CMM, Ellason JW, et al. Prevalence, Reliability and Validity of Dissociative Disorders in an Inpatient Setting, Journal of Trauma & Dissociation, 3:1, 7-17. [CrossRef]

Table 1.
List of baseline measures.
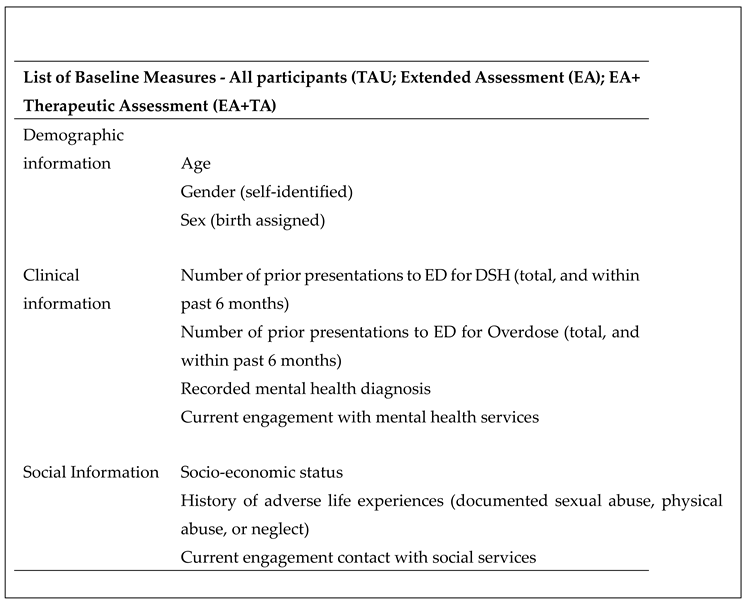 |
Table 2.
List of measures for active treatment groups.
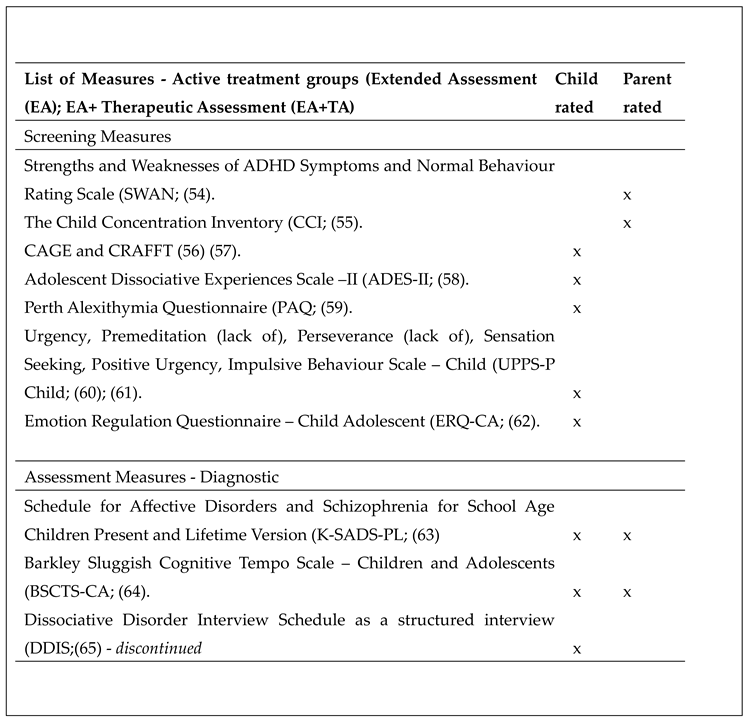 |
Table 2.
List of measures for active treatment groups.
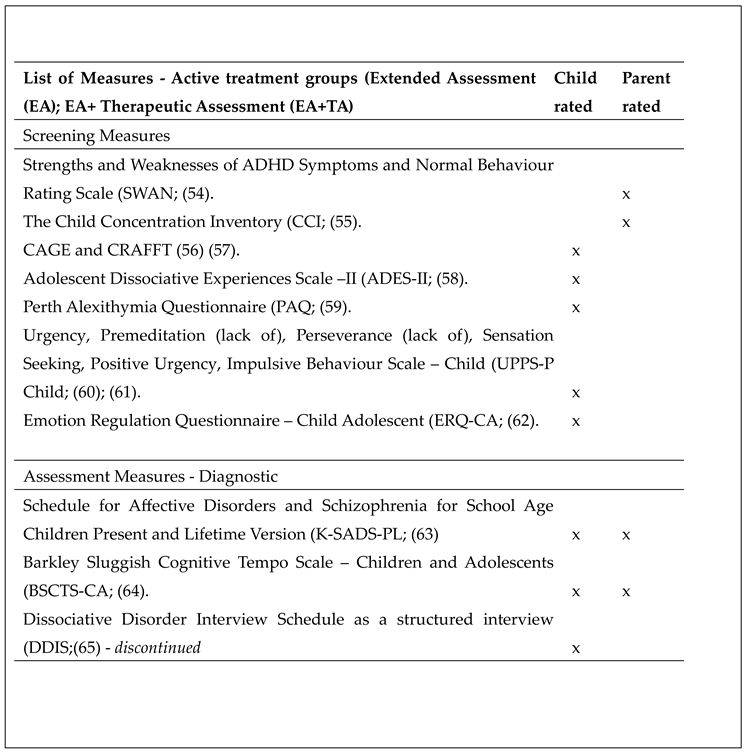 |
Table 3.
THERAPEUTIC ASSESSMENT STEPS.
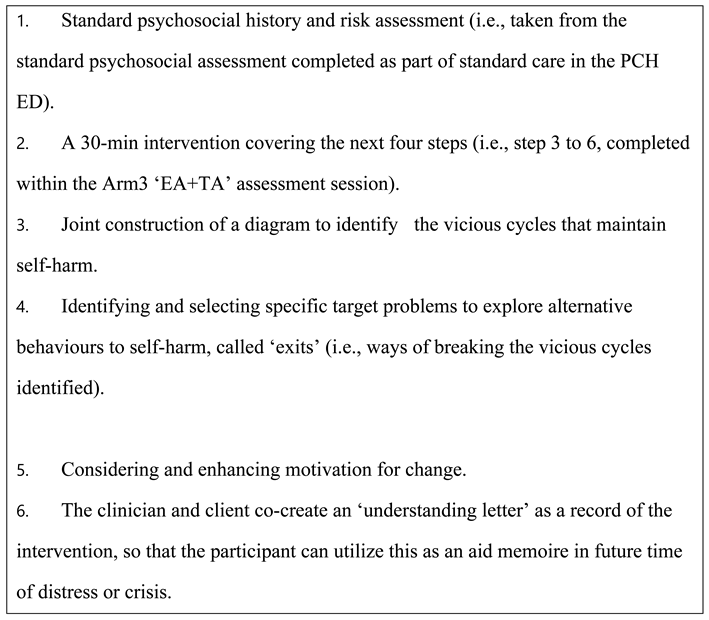 |
Table 4.
OUTCOME MEASURES.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



