
Submitted:
29 April 2024
Posted:
29 April 2024
You are already at the latest version
Abstract
Gabapentin (GBP) was originally developed as a potential agonist for Gamma-Amino-Butyric-Acid (GABA) receptors, aiming to inhibit the activation of pain-signaling neurons. Contrary to initial expectations, it does not bind to GABA receptors. Instead, it exhibits several distinct pharmacological activities, including: (1) binding to the alpha-2-delta protein subunit of voltage-gated calcium channels in the central nervous system, thereby blocking the excitatory influx of calcium; (2) reducing the expression and phosphorylation of CaMKII via modulation of ERK1/2 phosphorylation; (3) inhibiting glutamate release and interfering with the activation of NMDA receptors; (4) enhancing GABA synthesis; (5) increasing cell-surface expression of δGABA_A receptors, contributing to its antinociceptive, anticonvulsant, and anxiolytic-like effects. Additionally, GBP displays (6) inhibition of NF-kB activation and subsequent production of inflammatory cytokines, and (7) stimulation of the purinergic adenosine A1 receptor, which supports its anti-inflammatory and wound-healing properties. Initially approved for treating seizures and postherpetic neuralgia, GBP is now broadly used for various conditions, including psychiatric disorders, acute and chronic neuropathic pain, and sleep disturbances. Recently, as an eye drop formulation, it has also been explored as a therapeutic option for ocular surface discomfort in conditions such as dry eye, neurotrophic keratitis, corneal ulcers, and neuropathic ocular pain. This review aims to summarize the evidence supporting the molecular effects of GBP, with a special emphasis on its applications in ocular surface diseases.
Keywords:
gabapentin
; GABA
; dry eye
; neuropathic pain
; eye drops
1. Introduction
Gamma-aminobutyric acid (GABA) and glutamate (GLU) play crucial roles in the control of neuropathic pain through their actions within the central nervous system (CNS). These neurotransmitters separately activate two distinct classes of receptors: ionotropic and metabotropic. Ionotropic receptors work as ligand-gated ion channels, inducing rapid synaptic transmission, while metabotropic receptors belong to the G-protein coupled receptor (GPCR) family, contributing to the neuro-modulatory effects mediated by glutamate and GABA. Remarkably, within the pain neuraxis, these receptors can be found at various points along the pathway in the nervous system that processes pain signals, thus regulating how pain signals are transmitted and perceived by the brain [1].
GABA is an amino acid that works as the primary inhibitory neurotransmitter for the CNS. It functions to reduce neuronal excitability by inhibiting nerve transmission. In the context of neuropathic pain, GABAergic inhibitory interneurons modulate the transmission of pain signals within the spinal cord and brain. GABAergic signaling inhibits the activation of pain-signaling neurons, dampening their transmission. GABA exerts its inhibitory effect through two types of specific receptors, GABA_A (ionotropic) and GABA_B (metabotropic), which show different pharmacological, structural, and molecular differences. GABA receptors are the most common in the nervous system. Upon ligand binding they change their shape slightly to allow negatively charged chloride ions to pass through their channel into the neuron, thus reducing its excitability. Therefore, GABA is classified as an inhibitory neurotransmitter. Dysfunction in GABAergic neurotransmission, such as a decrease in GABAergic inhibitory activity, can lead to hyperexcitability of pain-signaling pathways, contributing to the development and maintenance of neuropathic pain [2].
Glutamate (GLU) is the primary excitatory neurotransmitter in the CNS. Glutamatergic signaling plays a key role in the transmission and amplification of pain signals. In neuropathic pain conditions, excessive release of glutamate and increased activation of glutamate receptors contribute to neuronal hyperexcitability and central sensitization, leading to the amplification and prolongation of pain signals. Glutamate receptors, particularly N-methyl-D-aspartate (NMDA) receptors, are implicated in the development and maintenance of neuropathic pain by mediating synaptic plasticity and the induction of central sensitization [3].
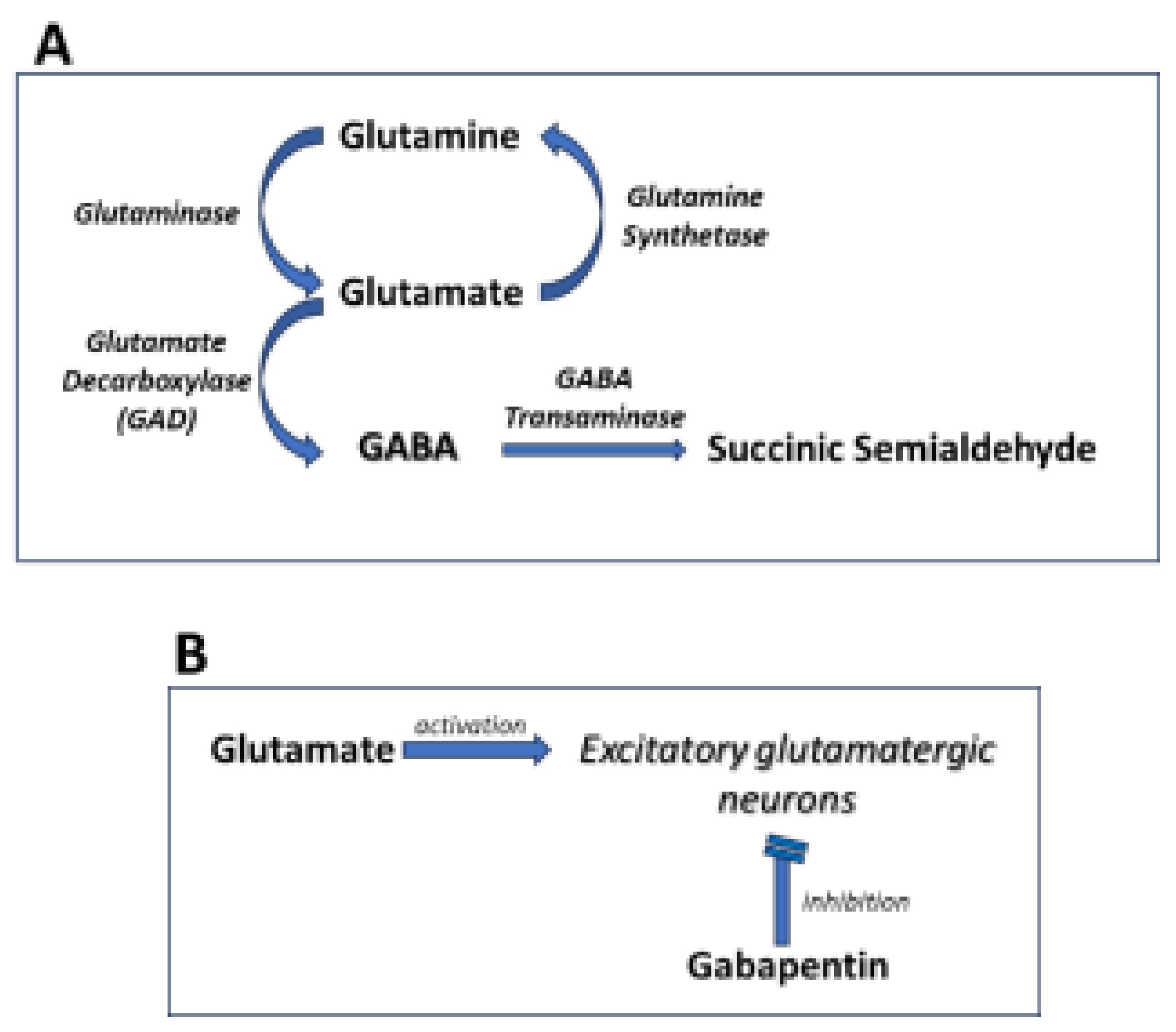
Figure 1.
Mechanisms of Gabapentin Antalgic Action: GABA Synthesis and Glutamatergic Inhibition A. The pathways leading to GABA synthesis and degradation. B. The analgesic effect of gabapentin depends on the inhibition of excitatory glutamatergic neurons, occurring through mechanisms that do not involve GABA receptors.
Figure 1.
Mechanisms of Gabapentin Antalgic Action: GABA Synthesis and Glutamatergic Inhibition A. The pathways leading to GABA synthesis and degradation. B. The analgesic effect of gabapentin depends on the inhibition of excitatory glutamatergic neurons, occurring through mechanisms that do not involve GABA receptors.
Considering the involvement of GABA and glutamate in neuropathic pain, pharmacological interventions aimed at enhancing GABAergic inhibition or modulating glutamatergic excitatory signaling are of significant interest for its management. Medications like gabapentin (GBP), which interact with voltage-gated calcium channels and indirectly influence GABA and glutamate neurotransmitter systems, are commonly employed for their efficacy in alleviating neuropathic pain.
2. Pharmacology of GBP Action
GBP is a non-anesthetic drug with analgesic and anticonvulsant properties. It has demonstrated efficacy in the treatment of partial epileptic seizures and neuropathic pain [4,5]. GBP was made by the addition of a cyclohexyl group to GABA, which allowed this form of GABA to cross the blood-brain barrier.
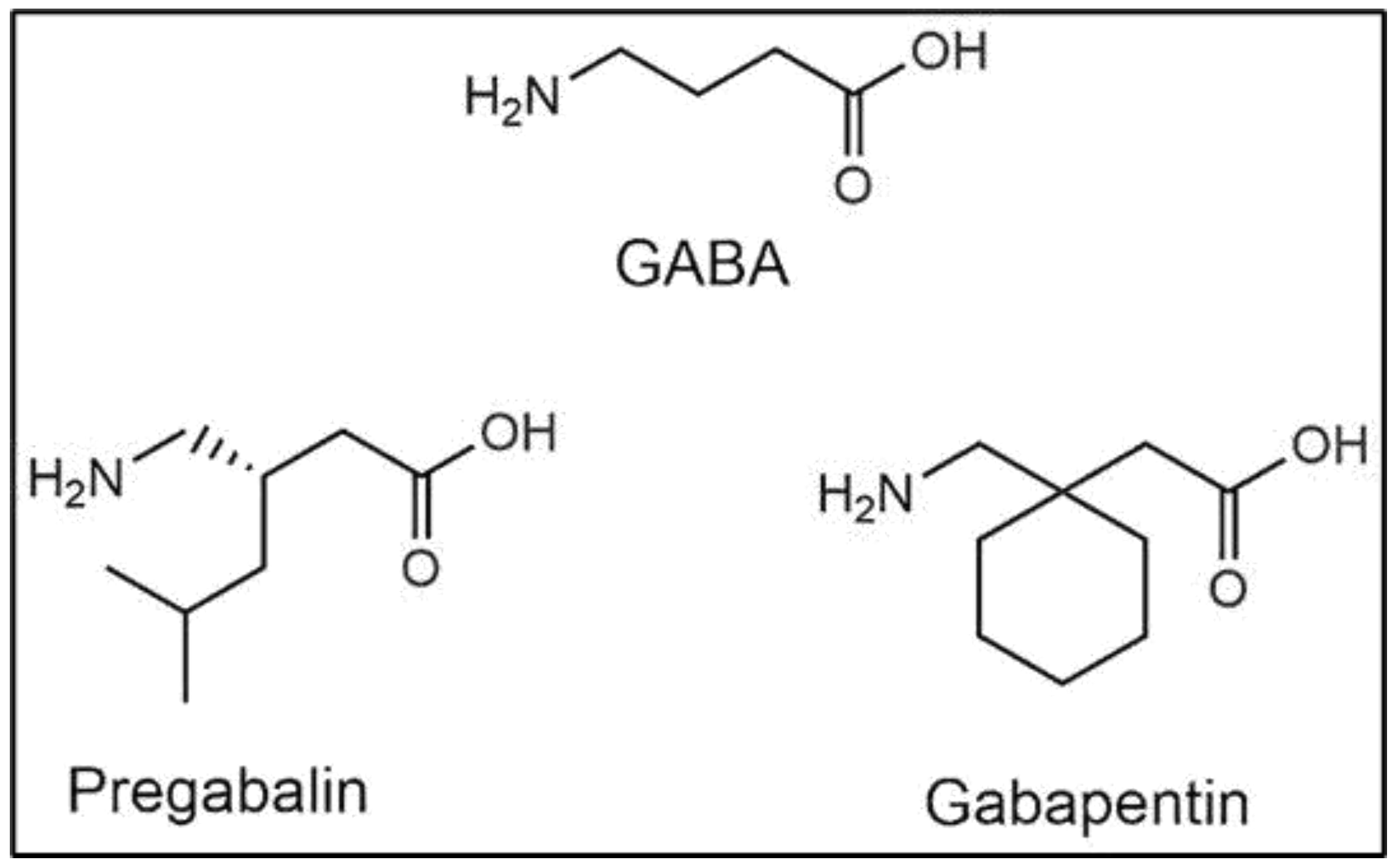
Figure 2.
Gabapentinoids in Pharmacology: Structurally related to gamma-aminobutyric acid (GABA), Gabapentin does not appear to interact with GABA receptors or influence its synaptic reuptake [6]. Pregabalin is an alternative pharmaceutical form of gabapentin, showing very similar properties [7]. Gabapentin and pregabalin are collectively indicated as gabapentinoids.
Figure 2.
Gabapentinoids in Pharmacology: Structurally related to gamma-aminobutyric acid (GABA), Gabapentin does not appear to interact with GABA receptors or influence its synaptic reuptake [6]. Pregabalin is an alternative pharmaceutical form of gabapentin, showing very similar properties [7]. Gabapentin and pregabalin are collectively indicated as gabapentinoids.
GBP was originally developed to mimic the neurotransmitter GABA to potentially act as an agonist at GABA receptors, so as to inhibit the activation of pain-signaling neurons. However, it does not significantly bind to GABA_A or GABA_B receptors and does not directly influence GABA uptake or degradation [8]. The mechanisms through which GBP exerts its effects are somewhat different from the initial hypothesis and include the following.
2.1. Effects on Voltage-Gated Calcium Channels
At the neuronal level, GBP inhibits the activity of voltage-dependent L-type calcium channels by binding to the α2-δ1 and α2-δ2 subunits. It also acts as an inhibitor on voltage-dependent N-type calcium channels. In this way, it reduces the influx of calcium ions into presynaptic terminals and decreases the release of excitatory neurotransmitters, such as glutamate. This action contributes to its anticonvulsant and analgesic effects [6,9]. These studies describe the effects of GBP on calcium channel currents and trafficking, shedding light on its mechanism of action. The binding of GBP to the α2-δ1 and α2-δ2 subunits of voltage-gated calcium channels has little acute effect on calcium currents. At the same time, chronic exposure to GBP inhibits calcium currents in heterologous expression systems and dorsal root ganglion neurons. This inhibition occurs when GBP is included for 17-20 h before recording, but not if included for 3-6 h. This suggests that GBP’s inhibition of calcium currents requires chronic exposure. GBP primarily acts at an intracellular location, requiring uptake into cells. This effect is mediated by α2-δ subunits of calcium channels, as mutations preventing GBP binding abolish its inhibitory effect [9]. GBP disrupts the trafficking of α2-δ2 and calcium channel subunits, reducing their cell-surface expression. This disruption occurs chronically and is not observed with acute GBP exposure. These findings suggest that GBP may displace an endogenous ligand that positively modulates α2-δ subunit function, leading to impaired trafficking of calcium channels [6]. GBP’s effects on calcium channel currents and trafficking contribute to its mechanism of action, potentially explaining its therapeutic effects in conditions such as epilepsy and neuropathic pain.
2.2. Effects on CaMKII
Experimental evidence has suggested that Ca2+/calmodulin-dependent protein kinase II (CaMKII) may contribute to GBP’s analgesic effects in a rat model of chronic constriction injury (CCI). GBP or saline were given to rats undergoing CCI, and mechanical allodynia and thermal hyperalgesia were assessed. GBP significantly reduced pain sensitivity in treated rats, with maximal effects observed on postoperative day 8. Additionally, GBP decreased the expression and phosphorylation of CaMKII in the spinal cord of CCI rats. These findings suggest that GBP’s analgesic effects in treated rats may be mediated, at least in part, by modulation of CaMKII expression and phosphorylation in the spinal cord [10].
2.3. Effects on Glutamate Receptors
GBP may reduce excitatory neurotransmission by decreasing GLU release, thereby interfering with the activation of NMDA (N-methyl-D-aspartate) receptors. This mechanism likely contributes to its anticonvulsant properties and potentially also its analgesic properties. A study in a rat neuropathic pain model demonstrated that systemic or intrathecal GBP administration effectively reduced mechanical and cold hypersensitivity, with intrathecal administration showing superior efficacy. GBP also attenuated the formalin-induced release of GLU and aspartate in the spinal cord dorsal horn, suggesting its ability to alleviate neuropathic pain symptoms by inhibiting glutamate release in this region [11]. In a different model system, GBP effects were evaluated on neurotransmitter-gated ion channels and GIRK (G protein-coupled inwardly rectifying potassium) channels in the spinal cord, hypothesizing it as a possible site of action. Xenopus laevis oocytes genetically manipulated to express human receptors/channels revealed no effect of GBP on GABA(A) receptors, glycine receptors, or GIRK channels, even at high concentrations. However, GBP concentration-dependently inhibited NMDA receptors, with significant inhibition at 10 microM. Notably, at 30 microM, GBP competitively inhibited NMDA receptors without altering their response curve, suggesting a non-competitive inhibition. Glycine attenuated this effect in a concentration-dependent manner. These findings indicated that GBP’s antinociceptive property may be attributed to its inhibition of NMDA receptors, rather than GABA(A) receptors, glycine receptors, or GIRK channels [12]. Additionally, pre-treatment with GBP protected rat hippocampal CA1 neurons against NMDA-induced excitotoxicity by inhibiting NMDA receptor-activated ion currents, thus attenuating glutamate-induced neuronal injury [13], finally confirming the inhibitory effects of GBP on the GLU/NMDA-receptor system. Even more interesting is the recent finding that the α2-δ1 subunit of voltage-gated ion channels, a known binding site for gabapentinoids used to manage neuropathic pain and epilepsy, plays a significant role in neuropathic pain hypersensitivity through its association with NMDA receptors. Specifically, overexpression of Cacna2d1, the gene encoding α2-δ1, increased both presynaptic and postsynaptic NMDA receptor activity in spinal dorsal horn neurons, leading to pain hypersensitivity. Conversely, knockdown or removal of Cacna2d1 normalized the increased NMDA receptor activity induced by nerve injury. Further investigation revealed that α2-δ1 forms a complex with NMDA receptors in both rodent and human spinal cords, predominantly through its C terminus, promoting the surface trafficking and synaptic targeting of NMDA receptors. GBP or a peptide interfering with the C terminus of α2-δ1 normalized NMDA receptor synaptic targeting and activity increased by nerve injury. These findings highlight α2-δ1 as a critical NMDA receptor-interacting protein that enhances its synaptic delivery in neuropathic pain. Moreover, Gabapentinoids alleviate neuropathic pain by inhibiting the forward trafficking of α2-δ1-NMDA receptor complexes [14].
2.4. Effects on GABA Synthesis
Although GBP does not act directly on GABA receptors, it appears to enhance the GABA synthetic pathway. In fact, in laboratory settings, GBP enhances the function of glutamic acid decarboxylase (GAD), responsible for synthesizing GABA, and inhibits GABA-transaminase, responsible for its degradation, however only at high concentrations. Studies using nuclear magnetic resonance (NMR) spectroscopy on human and rat brains suggested that GBP enhances the production of GABA [15]. Therefore, by increasing the synthesis of GABA, GBP may indirectly enhance inhibitory neurotransmission, although this effect does not appear to be the primary mechanism of action. However, further studies did not confirm these findings, rather reporting that GBP boosted the presence of δGABA_A receptors and heightened a steady inhibitory current in neurons. This rise in expression probably plays a role in the calming effects of GABA, as evidenced by GBP-induced reductions in coordination and anxiety in normal mice, but not in mice lacking the δ subunit. Interestingly, both normal and δ subunit-lacking mice experienced pain relief from GBP, indicating the presence of other different mechanisms of action, independent of GABA receptors. Notably, levels of GABA_A receptor activators and neurosteroids in the brain remained unchanged in response to GBP [16]. Accordingly, a most recent study reported that gabapentin and pregabalin did not acutely increase cellular GABA levels in the healthy rat forebrain. Instead, they modestly decrease cellular glutamate levels [17]. These findings further support the hypothesis that while gabapentin and pregabalin may modulate glutamate levels, their primary mechanism of action may not involve direct modulation of GABA levels in the healthy rat brain.
2.5. Antinflammatory Effects
GBP also exerts an antinflammatory action, as demonstrated in different model systems. In vitro, using human neuroblastoma cells (SH-SY5Y) and rat glioma cells (C6) [18] demonstrated that GBP can counteract the activation of the NF-kB factor induced by Substance P (SP), involved in the induction of inflammatory episodes. In vivo, in a rat model of neuropathic pain, GBP increased the levels of IL-10, an anti-inflammatory cytokine capable of inhibiting interferon-gamma (INFγ), and the expression of pro-inflammatory cytokines like TNF-α, IL-1, IL-6, IL-8, and IL-12 [19]. The anti-inflammatory activity of GBP has also been demonstrated in a murine model of carrageenan-induced peritonitis. GBP treatment reduced the production of inflammation mediators and pro-inflammatory cytokines, neutrophil infiltration, and oxidative stress [20]. Most recently, the anti-inflammatory effects of GBP on ventricular remodeling post-myocardial infarction (MI) were investigated in a rat model of MI, and by in vitro experiments with the THP-1 macrophage cell line. In vivo, GBP administration following MI led to reduced expression of the pro-inflammatory marker inducible nitric oxide synthase (iNOS) and decreased levels of inflammatory cytokines such as TNF-α and IL1β. Additionally, GBP promoted the expression of markers associated with anti-inflammatory M2 macrophages and increased levels of anti-inflammatory factors such as chitinase-like 3, IL-10, and TGFβ. Furthermore, GBP treatment improved cardiac function, reduced infarct size, and decreased cardiac fibrosis. In vitro experiments demonstrated that GBP reduced the expression of pro-inflammatory factors in LPS-stimulated macrophages. This effect was partially mediated by PPAR-γ activation and involved downregulation of α2δ1 calcium channel expression in macrophage membranes, leading to decreased intracellular calcium levels. Overall, GBP mitigated cardiac remodeling post-MI by suppressing inflammation through PPAR-γ activation and calcium regulation [21].
2.6. Effects on Adenosine A1 Receptors
GBP has also been reported to interact with other molecular targets, such as the stimulation of the adenosine A1 receptor subtype, involved in modulating neurotransmitter release, neuronal excitability, and inflammation. Adenosine A1 receptors were supposed to play a role in the anticonvulsive effects of certain drugs, including GBP, in a mouse model of seizures induced by the mitochondrial toxin 3-nitropropionic acid (3-NPA) [22]. This study investigated the impact of adenosine receptor antagonists on the anticonvulsive effects of various drugs, including diazepam, phenobarbital, valproate, and GBP. The results showed that antagonists of adenosine A1 receptors, such as aminophylline and 8-cyclopentyl-1,3-dipropylxanthine (DPCPX), diminished the protective effects of these drugs against 3-NPA-induced seizures. This suggests that the activation of adenosine A1 receptors may contribute to the anticonvulsive potential of these medications in this particular model. Moreover, the study found that the non-penetrating adenosine A1/A2 receptor antagonist, 8-(p-sulfophenyl)theophylline (8pSPT), was ineffective, indicating that the central action of adenosine A1 receptors is crucial for the observed effects. Furthermore, the antagonists aminophylline and DPCPX reversed the protective effects of adenosine A1 receptor agonists, suggesting that adenosine A1 receptor stimulation is involved in the anticonvulsant actions of these agonists. Overall, these results imply that the activation of central adenosine A1 receptors may contribute to the anticonvulsive effects of diazepam, phenobarbital, valproate, and GBP in the context of 3-NPA-induced seizures [22]. Another study used a rat model system of mechanical allodynia induced by nerve ligation injury. In this case, GBP and an adenosine A1 receptor agonist, R-PIA, were administered intrathecally to investigate their individual and combined effects on the neuropathic pain symptoms. The obtained results indicated that both GBP and R-PIA produced dose-dependent reductions in mechanical allodynia when administered individually. Moreover, when GBP and R-PIA were coadministered, they synergistically enhanced the antiallodynic effect. This synergistic interaction suggests that GBP potentiates the efficacy of R-PIA in alleviating mechanical allodynia. Additionally, intrathecal administration of an adenosine A1 receptor antagonist reversed the maximal antiallodynic effect observed in the combination group, indicating that activation by GBP and R-PIA of adenosine A1 receptors at the spinal level is necessary for their synergistic interaction on mechanical allodynia [23]. A further study used animal models of complex regional pain syndrome type-I and partial sciatic nerve ligation (PSNL), in which the efficacy of GBP in alleviating neuropathic pain-like behavior was investigated. Neuropathic pain was induced by unilateral prolonged hind paw ischemia and reperfusion (I/R) or PSNL procedures, resulting in stimulus-evoked mechanical hyperalgesia. GBP administration over 3 weeks led to a dose-dependent inhibition of mechanical hyperalgesia in the animals, thus suggesting that GBP effectively alleviated neuropathic pain-like behavior in these animal models. Furthermore, the study explored the contribution of adenosine receptor subtypes to the anti-hyperalgesic effect of GBP. Administration of caffeine, a non-selective adenosine A1 and A2 receptor antagonist, or 1,3-dipropyl-8-cyclopentylxanthine (DPCPX), a selective adenosine A1 subtype receptor antagonist, alongside GBP blocked its anti-hyperalgesic effect. This indicates that the mechanism underlying GBP’s efficacy may involve the activation of adenosine A1 subtype receptors [24]. Overall, these findings suggest that GBP effectively reduces neuropathic pain-like behavior in animal models, and this effect may be mediated, at least in part, by the activation of adenosine A1 subtype receptors.
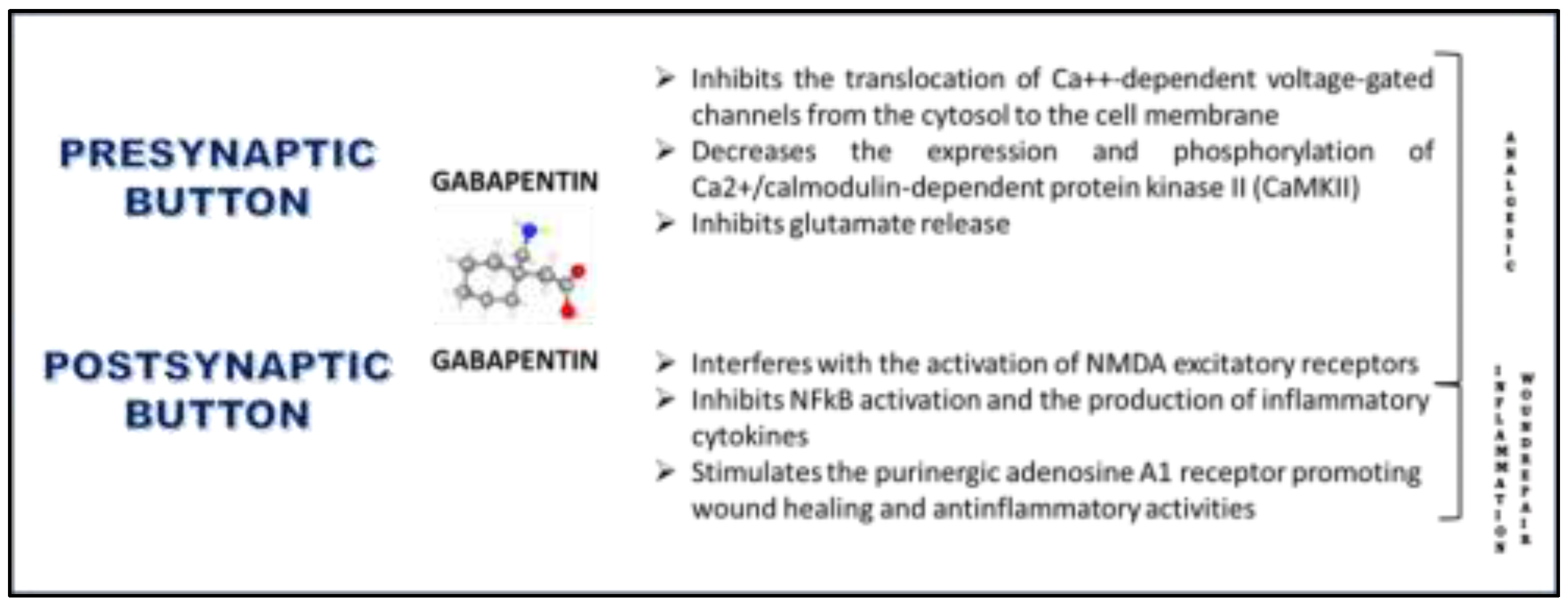
Figure 3.
The interactions of gabapentin occur at both pre- and post-synaptic terminals of neurons and involve various mechanisms leading to analgesic, anti-inflammatory, and wound-healing effects.
Figure 3.
The interactions of gabapentin occur at both pre- and post-synaptic terminals of neurons and involve various mechanisms leading to analgesic, anti-inflammatory, and wound-healing effects.
In conclusion, gabapentinoids, including GBP, have emerged as valuable adjuncts in perioperative pain management, aiming to minimize nociceptive input and mitigate the risk of central sensitization [25]. Despite their classification as calcium channel blockers, the precise mechanisms underlying their analgesic effects remain incompletely understood. While their efficacy in neuropathic pain is well-established, their role in postoperative pain management is less defined. Research into the mechanisms of action and effects of gabapentinoids, particularly in experimental animal models and human studies, provides insights into their analgesic properties. Gabapentinoids exert their analgesic effects through multifaceted mechanisms that collectively modulate pain perception. At the spinal level, gabapentinoids inhibit calcium-mediated neurotransmitter release by targeting α2δ-1 subunits, thereby reducing the transmission of pain signals in the dorsal horn. Additionally, they depress dorsal horn sensitivity by interfering with the forward trafficking and recycling of α2δ-1 subunits from dorsal root ganglion neurons. This modulation of dorsal horn sensitivity contributes to the attenuation of pain signaling. Furthermore, gabapentinoids stimulate the uptake of glutamate by excitatory amino acid transporters, potentially dampening excitatory signals in pain pathways. They also inhibit descending serotonergic facilitation, thereby preventing the amplification of pain signals and reducing the risk of central sensitization. Conversely, gabapentinoids promote descending inhibition, augmenting the body’s endogenous pain-suppression mechanisms. Beyond their actions at the spinal level, gabapentinoids exert anti-inflammatory effects, which can mitigate inflammation-induced pain. Moreover, they may influence the affective component of pain, contributing to overall pain relief. While animal studies consistently demonstrate the effectiveness of gabapentinoids in inflammatory and postoperative pain models, clinical evidence in human models is variable. This suggests the need for further research to elucidate the clinical utility of gabapentinoids in postoperative pain management and optimize their therapeutic use. In summary, the analgesic effects of gabapentinoids in perioperative pain management stem from their multifaceted actions on pain pathways, encompassing modulation of neurotransmitter release, dorsal horn sensitivity, descending pain modulation, anti-inflammatory actions, and affective pain processing. Understanding these mechanisms is crucial for optimizing their clinical use and improving pain management outcomes in surgical patients.
2.7. Effects on Wound-Healing
Finally, GBP also facilitated wound healing as shown in two different experimental contexts, both involving rat models, which highlighted varied outcomes depending on the formulation and application of GBP. In the first study, the effects of GBP and pregabalin on wound healing in non-diabetic rat models were evaluated [26]. Here, both GBP and pregabalin appeared to delay wound healing initially compared to a control group treated with saline, with increased inflammation noted up to day 13. However, between days 13 and 21, GBP exhibited better healing outcomes than pregabalin. In a second study [27], GBP was conjugated with melittin (a peptide found in bee venom) and formulated into nanoparticles to treat diabetic wounds in rats. This nanoconjugate showed enhanced wound healing properties, evidenced by expedited wound contraction, significant antioxidant activities (preventing malondialdehyde accumulation and promoting activity of superoxide dismutase and glutathione peroxidase), and superior anti-inflammatory effects (inhibiting the expression of pro-inflammatory cytokines like IL-6 and TNF-α). Additionally, it supported the proliferation phase of healing by increasing the expression of growth factors such as TGF-β, VEGF-A, and PDGFR-β, and it boosted the synthesis of hydroxyproline and collagen (Col 1A1). This suggests that GBP, when used in a specific nanoconjugate formulation, can significantly enhance various phases of the wound healing process in diabetic models, including inflammation modulation, oxidative stress reduction, and tissue regeneration. From these studies, it can be inferred that GBP has a complex role in wound healing that may vary significantly based on the model of injury (e.g., diabetic vs. non-diabetic wounds), the stage of wound healing, and the specific formulation and combination with other compounds. GBP’s efficacy seems to improve when it is part of a targeted delivery system, such as in the form of a nanoconjugate, which can enhance its bioavailability and therapeutic impact on wound healing processes.
3. Current Therapeutic Applications of Systemic GBP
3.1. Psychiatric Disorders
GBP is primarily known for its use in treating neurological conditions such as epilepsy and neuropathic pain. Its role in the treatment of psychiatric disorders is less established and generally considered off-label [28]. Nonetheless, some evidence suggests that GBP may have potential therapeutic benefits in certain psychiatric conditions. While it appears to have some benefits for anxiety disorders, GBP has shown limited benefit in bipolar disorder and has been used in alcohol craving, withdrawal symptoms, and as an adjunctive therapy for opioid dependence [29]. A recent review indicates that GBP demonstrates efficacy in treating alcohol withdrawal and alcohol use disorder. It is supported as a third-line treatment option for social anxiety disorder and severe panic disorder, backed by sufficient evidence. However, the evidence does not support its use in conditions such as bipolar disorder, major depressive disorder (MDD), posttraumatic stress disorder (PTSD), obsessive-compulsive disorder (OCD), stimulant use disorder, or opioid withdrawal [30].
3.2. Anxiety Disorders
Some studies have explored the use of GBP in the treatment of anxiety disorders, including generalized anxiety disorder (GAD), social anxiety disorder (SAD), and panic disorder. GBP has been investigated as an adjunctive treatment to traditional anxiolytics or as a monotherapy. While findings are mixed, some studies suggest that GBP may have anxiolytic effects and could be beneficial in reducing anxiety symptoms [31,32]. This action of GBP appears to work through its binding to the α2δ-1 subunit of voltage-gated calcium channels. This subunit is also involved in binding with thrombospondin, a glycoprotein that facilitates cell-matrix interactions and can modulate synaptic formation and the function of neural circuits. These interactions influence processes such as nociception (pain perception) and potentially other neurological functions [33]. However, research has shown that individuals with a previous history of substance use disorders are at an increased risk of abusing Gabapentinoids, a class of drugs that includes GBP and pregabalin. When these medications are misused alongside illegal drugs, the harmful effects associated with drug abuse can become more severe. Evidence of rising misuse of Gabapentinoids has been confirmed by drug screening practices and analyses performed during autopsies, which have noted higher levels of these substances. Due to the growing concerns about their potential for abuse, many countries have taken regulatory measures by categorizing Gabapentinoids as controlled substances. This classification aims to curb abuse by imposing stricter regulations on prescription, distribution, and consumption [34].
3.3. Substance Use Disorders
Emerging evidence, albeit conflicting, suggests that GBP may offer benefits in the treatment of substance use disorders, notably alcohol use disorder and opioid withdrawal. GBP has been proposed to alleviate cravings and withdrawal symptoms, potentially enhancing treatment outcomes for individuals struggling with substance use disorders [35,36].
3.4. Bipolar Disorder
GBP’s potential utility in bipolar disorder primarily concerns its mood-stabilizing and anxiolytic effects. It has been explored as a treatment option for managing various symptoms of bipolar disorder, including anxiety, agitation, and mood swings. Some studies suggest that GBP can be beneficial for patients who experience rapid cycling or mixed states in bipolar disorder. The evidence from controlled clinical trials regarding GBP’s efficacy in bipolar disorder remains inconclusive. Several small studies and clinical reports have suggested that it may help manage symptoms of bipolar disorder, particularly in patients who are resistant to other treatments. However, larger and more rigorous studies have generally not confirmed these findings. As a result, GBP is not typically considered a first-line treatment or a standard therapy for bipolar disorder by current clinical guidelines [37,38]. GBP’s mechanism involves binding to the α2δ subunit of voltage-gated calcium channels, which might modulate neurotransmitter release and neuronal excitability—factors that could potentially affect mood regulation. Despite this, the exact mechanism by which GBP might exert mood-stabilizing effects remains unclear. In clinical practice, GBP is sometimes used off-label when other mood stabilizers are ineffective, not tolerated, or contraindicated [39]. Its relatively benign side effect profile compared to other mood stabilizers can also make it a preferred option for certain patients. While GBP has some potential in managing certain aspects of bipolar disorder, especially in complex, treatment-resistant cases or as an adjunct treatment, it should not be used as a primary treatment for bipolar disorder without careful consideration and monitoring by a healthcare provider. Further research is needed to better define its role and efficacy in bipolar disorder management.
3.5. Insomnia
GBP has been explored as a potential treatment for pathologic insomnia, particularly in individuals with comorbid psychiatric conditions such as anxiety, restless leg syndrome (RLS), or bipolar disorder. Some studies have found that GBP may improve sleep quality and reduce insomnia symptoms, possibly by modulating neurotransmitter systems involved in sleep regulation [38,40,41]. Contrasting evidence stemmed from other reports [42].
Overall, while GBP’s role in the treatment of psychiatric disorders is not as well-established as its use in neurological conditions, there is some evidence suggesting potential benefits in certain conditions. However, more research is needed to clarify its efficacy, safety, and optimal dosing strategies in psychiatric settings. Additionally, GBP should be used cautiously and under close supervision, as it can have side effects and may interact with other medications used to treat psychiatric disorders.
3.6. Pain Management
GBP was originally developed as an analgesic, and indeed GBP’s efficacy for neuropathic pain and postherpetic neuralgia is well-established, with its use as monotherapy or adjunctive therapy supported by case reports and reviews [43]. GBP treatments have also shown efficacy in diabetic peripheral neuropathy [44]; postherpetic neuralgia (PHN) [45], trigeminal neuralgia [46]; neuropathic pain further to paclitaxel chemotherapy [47], and cancer-related pain in pregnant patients [48]. Pain control in pediatric patients has also been described [49,50].
4. Experimental Evidence of Ophthalmic Use of GBP
4.1. Inflammation and Neuropathic Ocular Pain
The impact of GBP on the inflammatory response was evaluated in rabbit corneal cells (SIRC) stimulated with lipopolysaccharide (LPS). The study investigated the expression of various inflammatory markers, including TNF-α, IL-1β, cPLA2, COX-2, and PGE2, in corneal cells treated with or without GBP following LPS stimulation. GBP treatment notably decreased the production of cytokines, activation of cPLA2, expression of COX-2, and levels of PGE2 in SIRC corneal cells [51]. A seminal study by [52] investigated the response to GBP treatment in patients affected by dry eye accompanied by features of neuropathic ocular pain (NOP). Their findings suggested that GBP treatment may be effective, particularly in patients with systemic comorbidities and less pain response evoked by mechanical and chemical stimuli, indicating its potential for refractory cases not fully responsive to conventional topical treatments. A similar study, published one year later [53] evaluated the efficacy of GBP treatment in dry eye disease and neuropathic ocular pain, demonstrating its effectiveness in improving ocular surface discomfort when combined with artificial tear and cyclosporine drops treatments. Oral GBP demonstrated analgesic efficacy also in clinical studies on postoperative pain of patients subjected to photorefractive keratectomy [54,55,56]. The role of GBP in pain control was also explored through its use in managing postoperative pain following corneal collagen crosslinking (CXL) procedures for keratoconus. Patients were either treated with GBP or ketorolac post-surgery, and their pain levels were assessed using a numeric pain scale. The findings indicate that GBP, administered in 300 mg capsules every 8 h for the first three days after surgery, was as effective as ketorolac in controlling pain. There were no significant differences in pain scores between the two groups at any assessment point, nor were there notable differences in eye symptoms or systemic side effects related to the medications. This suggests that GBP is a viable option for pain management after corneal collagen crosslinking procedures, comparable to ketorolac in efficacy [57]. Moreover, a case report indicated GBP as an efficient analgesic intervention to control pain in a painful, blind glaucomatous eye [58]. Additionally, a case report by [59] highlighted the successful resolution of chronic neuropathic ocular pain with GBP, emphasizing its utility in addressing ocular discomfort even in the absence of significant ophthalmic findings. Aside from pain control, a GBP derivative has shown interesting neuroprotective activities. GBP-lactam (GBP-L), a derivative of GBP, exhibited significant neuroprotective effects on retinal ganglion cells (RGCs) across several experimental models of ischemia and neurodegeneration. The primary mechanism underlying these protective effects involves the modulation of mitochondrial ATP-sensitive potassium (K_ATP) channels, which play a crucial role in cellular survival during metabolic stress [60]. GBP-L’s ability to diminish glutamate release under ischemic-like conditions has been particularly notable. Glutamate, a neurotransmitter that becomes a potent neurotoxin under stress conditions, can induce significant neuronal damage and death via excitotoxic pathways. By reducing the ischemia-induced glutamate release, GBP-L minimizes these excitotoxic insults to neurons, thereby enhancing their survival. In vivo studies further underscore the efficacy of GBP-L in enhancing the survival of retinal ganglion cells following acute retinal ischemia. Importantly, GBP-L’s protective effects are evident not only when administered before the onset of ischemia but also when given during the reperfusion phase. This suggests its potential application in clinical settings, such as in the treatment of optic neuropathies and glaucoma, where mitigating ischemic damage is crucial [61]. Interestingly, GBP, the parent compound of GBP-L, does not exhibit similar neuroprotective properties in these models, indicating a distinct pharmacokinetic and pharmacodynamic profile for GBP-L. The uncharged nature of GBP-L possibly allows it to penetrate cellular membranes more effectively than GBP, facilitating its access to intracellular sites of action, particularly within mitochondria. The neuroprotective mechanism of GBP-L has been further elucidated through pharmacological experiments using glibenclamide, a blocker of K_ATP channels. The reversal of GBP-L’s neuroprotective effects by glibenclamide highlights the role of these channels in mediating its actions. Moreover, selective mitochondrial K_ATP channel blockers such as 5-hydroxydecanoate have also been shown to negate the survival-promoting effects of GBP-L, confirming the specificity of its action on mitochondrial components of the K_ATP channels [62]. In conclusion, the research on GBP-L presents it as a potent neuroprotective agent with specific actions on mitochondrial K_ATP channels, offering a promising therapeutic approach for conditions characterized by ischemic and excitotoxic neuronal damage. This distinct mechanism and enhanced efficacy compared to its precursor, GBP, positions GBP-L as a potential novel treatment for neurodegenerative diseases affecting the retina and other neuronal tissues.
These studies collectively underscore the promising role of GBP as a potential therapeutic intervention for managing ocular surface discomfort, particularly in cases with neuropathic components that may be refractory to conventional treatments.
4.2. Topical Formulation and Treatment with GBP Eye Drops
Considering the properties of GBP mentioned earlier, topical administration as eye drops could preserve its therapeutic benefits for the eye while minimizing systemic side effects associated with systemic delivery. An ophthalmic formulation of 0.5% GBP was prepared in an isotonic buffered solution (pH 7.0; 298 mOsm). Endotoxin-induced uveitis (EIU) was induced in rabbits by injecting LPS into the eye, and clinical signs of ocular inflammation were evaluated in tears, aqueous, cornea, conjunctiva, and iris-ciliary body at 7 and 24 h post-injection with or without topical application of 0.5% GBP. GBP significantly reduced both clinical symptoms and inflammation biomarkers compared to the LPS group at both time points [51]. These findings suggest that an ophthalmic formulation containing GBP could be beneficial in treating inflammatory conditions associated with ocular pain like uveitis, and further clinical research is warranted to validate this potential application. Moreover, its main mechanism of action makes GBP an analgesic with no anesthetic effects. GBP primarily acts by modulating the activity of voltage-gated calcium channels in the central nervous system. By inhibiting calcium influx, GBP reduces the release of excitatory neurotransmitters such as glutamate and substance P, which are involved in pain signaling pathways. This modulation of neurotransmitter release results in a reduction of pain transmission, making GBP an effective analgesic agent. This is relevant for topical applications on the eye because an anesthetic would be expected to decrease lacrimation, with negative effects on eye lubrication and corneal pain. In a recent study on rabbit eyes, it was indeed shown that topical application of GBP as eye drops (formulated at 2% in PBS) exhibited analgesic properties without inducing anesthesia, in comparison to a typical anesthetic drug such as oxybuprocaine [63]. Interestingly, GBP not only failed to reduce tear production but unexpectedly increased it. This increase seems to be mediated by the upregulation of acetylcholine and norepinephrine, along with the induction of aquaporin 5 (AQP5) expression in the lacrimal gland. Furthermore, in vitro experiments on the primary human corneal epithelial cell line HCE-F [64] suggested that GBP directly stimulates AQP5 expression in corneal cells. This implies that corneal cells may contribute to the enhanced tear production stimulated by GBP, working alongside the lacrimal glands to restore the tear film and reduce friction on the ocular surface, a known trigger for ocular pain. These results were further corroborated by a recent publication, in which a ceria-based nanocarrier system encapsulating GBP, was designed to effectively alleviate dry eye symptoms [65]. The nanocarrier was engineered by coating nanoceria with thiolated gelatin, which is subsequently cross-linked with glutaraldehyde, enhancing biocompatibility along with providing antioxidant, anti-inflammatory, antiangiogenic, antiapoptotic, and neuroprotective properties. The inclusion of abundant thiol groups on the gelatin was made to improve cellular uptake and mucin-binding of the nanocarrier, thus increasing ocular retention and therapeutic efficacy. The moderate cross-linking employed allowed for a controlled, slow release of GBP, facilitating stimulation of the lacrimal glands and restoration of the tear film. In a rabbit model of dry eye, topical application of this GBP-loaded nanocarrier formulation led to significant improvement in symptoms, including corneal epithelial repair, preservation of corneal nerve density, and enhanced tear production, outperforming the free drug. These findings highlight the potential and safety of this novel nanoformulation for advancing DE pharmacotherapy.
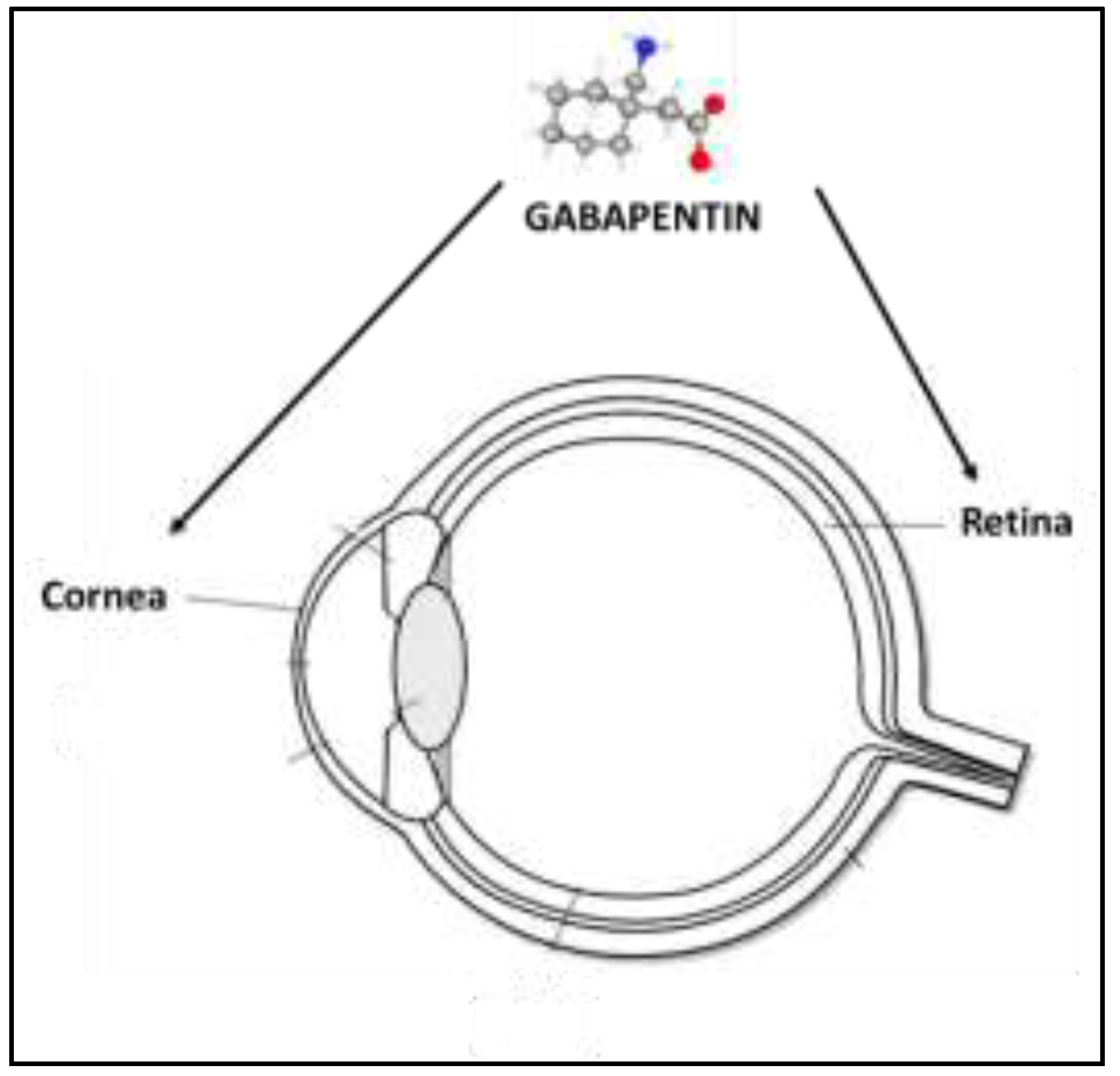
Figure 4.
Ophthalmic application of gabapentin. Gabapentin has demonstrated efficacy in managing ocular pain associated with dry eye and/or corneal ulcers. Additionally, its secretagogue activity aids in preserving ocular surface hydration. Its neuroprotective properties may contribute to the survival of retinal ganglion cells in conditions such as glaucoma or retinal dystrophies.
Figure 4.
Ophthalmic application of gabapentin. Gabapentin has demonstrated efficacy in managing ocular pain associated with dry eye and/or corneal ulcers. Additionally, its secretagogue activity aids in preserving ocular surface hydration. Its neuroprotective properties may contribute to the survival of retinal ganglion cells in conditions such as glaucoma or retinal dystrophies.
Finally, taking advantage of the multifaceted properties of GBP, including its documented role in promoting wound repair [26,27], preliminary evidence suggested that the application of sterile GBP solutions directly into the eyes of patients with corneal ulcers could enhance corneal lesion healing, without notable adverse effects. Indeed, anecdotal data from a patent application (WO 2017129577 A1) highlighted the beneficial effects of topical GBP eye drops (0.5% GBP with 0.15% hyaluronic acid) on corneal ulcer healing across a range of patients, including three children aged 2, 3, and 4 years, and two adults aged 77 and 85 years, encompassing both sexes.
In conclusion, GBP possesses analgesic, anti-inflammatory, and secretagogue properties, making it a potentially valuable treatment for several conditions affecting the ocular surface, particularly in cases of neuropathic pain and dry eye disease.
References
- Goudet C, Magnaghi V, Landry M, Nagy F, Gereau RW 4th, Pin JP. Metabotropic receptors for glutamate and GABA in pain. Brain Res Rev. 2009 Apr;60(1):43-56. [CrossRef]
- Vargas RA. The GABAergic System: An Overview of Physiology, Physiopathology and Therapeutics. Int J Clin Pharmacol Pharmacother. 2018; 3: 142. [CrossRef]
- Osikowicz M, Mika J, Przewlocka B. The glutamatergic system as a target for neuropathic pain relief. Exp Physiol. 2013 Feb;98(2):372-84. [CrossRef]
- Honarmand A, Safavi M, Zare M. Gabapentin: An update of its pharmacological properties and therapeutic use in epilepsy. J Res Med Sci. 2011 Aug;16(8):1062-9. PMCID: PMC3263084. [PubMed]
- Edelsberg JS, Lord C, Oster G. Systematic review and meta-analysis of efficacy, safety, and tolerability data from randomized controlled trials of drugs used to treat postherpetic neuralgia. Ann Pharmacother. 2011 Dec;45(12):1483-90. Epub 2011 Nov 15. [CrossRef] [PubMed]
- Hendrich J, Van Minh AT, Heblich F, Nieto-Rostro M, Watschinger K, Striessnig J, Wratten J, Davies A, Dolphin AC. Pharmacological disruption of calcium channel trafficking by the alpha2delta ligand gabapentin. Proc Natl Acad Sci U S A. 2008 Mar 4;105(9):3628-33. Epub 2008 Feb 25. PMCID: PMC2265195. [CrossRef] [PubMed]
- Tzellos TG, Papazisis G, Amaniti E, Kouvelas D. Efficacy of pregabalin and gabapentin for neuropathic pain in spinal-cord injury: an evidence-based evaluation of the literature. Eur J Clin Pharmacol. 2008 Sep;64(9):851-8. Epub 2008 Jul 8. [CrossRef] [PubMed]
- Taylor CP. Mechanisms of action of gabapentin. Rev Neurol (Paris). 1997;153 Suppl 1:S39-45. [PubMed]
- Heblich F, Tran Van Minh A, Hendrich J, Watschinger K, Dolphin AC. Time course and specificity of the pharmacological disruption of the trafficking of voltage-gated calcium channels by gabapentin. Channels (Austin). 2008 Jan-Feb;2(1):4-9. Epub 2008 Apr 4. [CrossRef] [PubMed]
- Ma LL, Liu W, Huang YG, Yang N, Zuo PP. Analgesic effect of gabapentin in a rat model for chronic constrictive injury. Chin Med J (Engl). 2011 Dec;124(24):4304-9. [PubMed]
- Coderre TJ, Kumar N, Lefebvre CD, Yu JS. Evidence that gabapentin reduces neuropathic pain by inhibiting the spinal release of glutamate. J Neurochem. 2005 Aug;94(4):1131-9. [CrossRef] [PubMed]
- Hara K, Sata T. Inhibitory effect of gabapentin on N-methyl-D-aspartate receptors expressed in Xenopus oocytes. Acta Anaesthesiol Scand. 2007 Jan;51(1):122-8. Epub 2006 Oct 31. [CrossRef] [PubMed]
- Kim YS, Chang HK, Lee JW, Sung YH, Kim SE, Shin MS, Yi JW, Park JH, Kim H, Kim CJ. Protective effect of gabapentin on N-methyl-D-aspartate-induced excitotoxicity in rat hippocampal CA1 neurons. J Pharmacol Sci. 2009 Jan;109(1):144-7. [CrossRef] [PubMed]
- Chen J, Li L, Chen SR, Chen H, Xie JD, Sirrieh RE, MacLean DM, Zhang Y, Zhou MH, Jayaraman V, Pan HL. The α2δ-1-NMDA Receptor Complex Is Critically Involved in Neuropathic Pain Development and Gabapentin Therapeutic Actions. Cell Rep. 2018 Feb 27;22(9):2307-2321. Erratum in: Cell Rep. 2022 Jan 25;38(4):110308. [CrossRef]
- Taylor CP, Gee NS, Su TZ, Kocsis JD, Welty DF, Brown JP, Dooley DJ, Boden P, Singh L. A summary of mechanistic hypotheses of gabapentin pharmacology. Epilepsy Res. 1998 Feb;29(3):233-49. [CrossRef] [PubMed]
- Yu J, Wang DS, Bonin RP, Penna A, Alavian-Ghavanini A, Zurek AA, Rauw G, Baker GB, Orser BA. Gabapentin increases expression of δ subunit-containing GABAA receptors. EBioMedicine. 2019 Apr;42:203-213. Epub 2019 Mar 14. PMCID: PMC6491385. [CrossRef] [PubMed]
- Errante LD, Petroff OA. Acute effects of gabapentin and pregabalin on rat forebrain cellular GABA, glutamate, and glutamine concentrations. Seizure. 2003 Jul;12(5):300-6. [CrossRef] [PubMed]
- Park S, Ahn ES, Han DW, Lee JH, Min KT, Kim H, Hong YW. Pregabalin and gabapentin inhibit substance P-induced NF-kappaB activation in neuroblastoma and glioma cells. J Cell Biochem. 2008 Oct 1;105(2):414-23. [CrossRef] [PubMed]
- Lee BS, Jun IG, Kim SH, Park JY. Intrathecal gabapentin increases interleukin-10 expression and inhibits pro-inflammatory cytokine in a rat model of neuropathic pain. J Korean Med Sci. 2013 Feb;28(2):308-14. Epub 2013 Jan 29. PMCID: PMC3565145. [CrossRef] [PubMed]
- Dias JM, de Brito TV, de Aguiar Magalhães D, da Silva Santos PW, Batista JA, do Nascimento Dias EG, de Barros Fernandes H, Damasceno SR, Silva RO, Aragão KS, Souza MH, Medeiros JV, Barbosa AL. Gabapentin, a synthetic analog of gamma-aminobutyric acid, reverses systemic acute inflammation and oxidative stress in mice. Inflammation. 2014 Oct;37(5):1826-36. [CrossRef] [PubMed]
- Li Z, Wang S, Qin Y, Yang B, Wang C, Lu T, Xu J, Zhu L, Yuan C, Han W. Gabapentin attenuates cardiac remodeling after myocardial infarction by inhibiting M1 macrophage polarization through the peroxisome proliferator-activated receptor-γ pathway. Eur J Pharmacol. 2024 Mar 15;967:176398. Epub 2024 Feb 11. [CrossRef] [PubMed]
- Zuchora B, Wielosz M, Urbańska EM. Adenosine A1 receptors and the anticonvulsant potential of drugs effective in the model of 3-nitropropionic acid-induced seizures in mice. Eur Neuropsychopharmacol. 2005 Jan;15(1):85-93. [CrossRef] [PubMed]
- Park JY, Jun IG. The interaction of gabapentin and N6-(2-phenylisopropyl)-adenosine R-(-)isomer (R-PIA) on mechanical allodynia in rats with a spinal nerve ligation. J Korean Med Sci. 2008 Aug;23(4):678-84. PMCID: PMC2526387. [CrossRef] [PubMed]
- Martins DF, Prado MR, Daruge-Neto E, Batisti AP, Emer AA, Mazzardo-Martins L, Santos AR, Piovezan AP. Caffeine prevents antihyperalgesic effect of gabapentin in an animal model of CRPS-I: evidence for the involvement of spinal adenosine A1 receptor. J Peripher Nerv Syst. 2015 Dec;20(4):403-9. [CrossRef] [PubMed]
- Chincholkar M. Analgesic mechanisms of gabapentinoids and effects in experimental pain models: a narrative review. Br J Anaesth. 2018 Jun;120(6):1315-1334. Epub 2018 Apr 12. [CrossRef] [PubMed]
- Sarıtaş TB, Korkmaz M, Sevimli A, Sarıtaş ZK. Comparison of the effects of gabapentin and pregabalin on wound healing in rats. Int Wound J. 2016 Oct;13(5):748-53. Epub 2014 Oct 28. PMCID: PMC7949902. [CrossRef] [PubMed]
- Asfour HZ, Alhakamy NA, Ahmed OAA, Fahmy UA, Md S, El-Moselhy MA, Rizg WY, Alghaith AF, Eid BG, Abdel-Naim AB. Enhanced healing efficacy of an optimized gabapentin-melittin nanoconjugate gel-loaded formulation in excised wounds of diabetic rats. Drug Deliv. 2022 Dec;29(1):1892-1902. PMCID: PMC9246110. [CrossRef] [PubMed]
- Costales B, Goodin AJ. Outpatient Off-Label Gabapentin Use for Psychiatric Indications Among U.S. Adults, 2011-2016. Psychiatr Serv. 2021 Nov 1;72(11):1246-1253. Epub 2021 May 21. [CrossRef] [PubMed]
- Berlin RK, Butler PM, Perloff MD. Gabapentin Therapy in Psychiatric Disorders: A Systematic Review. Prim Care Companion CNS Disord. 2015 Oct 22;17(5):10.4088/PCC.15r01821. PMCID: PMC4732322. [CrossRef] [PubMed]
- Martin JC, Gainer D. Psychiatric Uses of Gabapentin. Innov Clin Neurosci. 2022 Jul-Sep;19(7-9):55-60. PMCID: PMC9507147. [PubMed]
- Garakani A, Murrough JW, Freire RC, Thom RP, Larkin K, Buono FD, Iosifescu DV. Pharmacotherapy of Anxiety Disorders: Current and Emerging Treatment Options. Front Psychiatry. 2020 Dec 23;11:595584. PMCID: PMC7786299. [CrossRef] [PubMed]
- Gaba A, Shah K, Olson C, Munjal S. Treatment of Acute Intermittent Porphyria-Associated Anxiety Disorder With Gabapentin: Case Report and Review of Literature. J Clin Psychopharmacol. 2024 Jan-Feb 01;44(1):58-60. [CrossRef] [PubMed]
- Felsted JA, Meng A, Ameroso D, Rios M. Sex-specific Effects of α2δ-1 in the Ventromedial Hypothalamus of Female Mice Controlling Glucose and Lipid Balance. Endocrinology. 2020 Jul 1;161(7):bqaa068. PMCID: PMC7286619. [CrossRef] [PubMed]
- İspir GZ, Danışman M, Katar KS. A Hidden Pandemic? Abuse of Gabapentinoids: A Brief Review of Recent Studies. Curr Drug Res Rev. 2023 Nov 28. Epub ahead of print. [CrossRef] [PubMed]
- Modesto-Lowe V, Barron GC, Aronow B, Chaplin M. Gabapentin for alcohol use disorder: A good option, or cause for concern? Cleve Clin J Med. 2019 Dec;86(12):815-823. [CrossRef] [PubMed]
- Buttram ME, Kurtz SP, Ellis MS, Cicero TJ. Gabapentin prescribed during substance abuse treatment: The perspective of treatment providers. J Subst Abuse Treat. 2019 Oct;105:1-4. Epub 2019 Jul 21. PMCID: PMC6709710. [CrossRef] [PubMed]
- Ng QX, Han MX, Teoh SE, Yaow CYL, Lim YL, Chee KT. A Systematic Review of the Clinical Use of Gabapentin and Pregabalin in Bipolar Disorder. Pharmaceuticals (Basel). 2021 Aug 24;14(9):834. PMCID: PMC8469561. [CrossRef] [PubMed]
- Hong JSW, Atkinson LZ, Al-Juffali N, Awad A, Geddes JR, Tunbridge EM, Harrison PJ, Cipriani A. Gabapentin and pregabalin in bipolar disorder, anxiety states, and insomnia: Systematic review, meta-analysis, and rationale. Mol Psychiatry. 2022 Mar;27(3):1339-1349. Epub 2021 Nov 24. PMCID: PMC9095464. [CrossRef] [PubMed]
- Goodman CW, Brett AS. A Clinical Overview of Off-label Use of Gabapentinoid Drugs. JAMA Intern Med. 2019 May 1;179(5):695-701. [CrossRef] [PubMed]
- Pellitteri G, Versace S, Merlino G, Nilo A, Gigli GL, Valente M. A comprehensive update on the ADMET considerations for α2δ calcium channel ligand medications for treating restless legs syndrome. Expert Opin Drug Metab Toxicol. 2024 Mar;20(3):133-142. Epub 2024 Mar 15. [CrossRef] [PubMed]
- Shen Y, Li W, Ma M, Jiang W. Efficacy and Safety of Gabapentin in Improving Sleep Quality of Patients with Sensory Nervous System Diseases: A Meta-Analysis. Altern Ther Health Med. 2023 Jul;29(5):380-385. [PubMed]
- Saul H, Gursul D, Cassidy S, Harrison P. Little evidence supports gabapentinoid use in bipolar disorder or insomnia. BMJ. 2022 Nov 18;379:o2576. [CrossRef] [PubMed]
- Ruan QZ, Robinson CL, Simopoulos TT, Burns JC, Madabhushi SV, Gill JS. Comparative Descriptive Analysis of Physician Versus Patient-Directed Gabapentin Usage In Chronic Pain - A Preliminary Report. Pain Physician. 2023 Oct;26(6):E687-E693. [PubMed]
- Bragg S, Marrison ST, Haley S. Diabetic Peripheral Neuropathy: Prevention and Treatment. Am Fam Physician. 2024 Mar;109(3):226-232. [PubMed]
- Albrecht PJ, Liu Y, Houk G, Ruggiero B, Banov D, Dockum M, Day AJ, Rice FL, Bassani G. Cutaneous targets for topical pain medications in patients with neuropathic pain: individual differential expression of biomarkers supports the need for personalized medicine. Pain Rep. 2024 Feb 16;9(2):e1119. PMCID: PMC10876238. [CrossRef] [PubMed]
- De Stefano G, Di Pietro G, Truini A, Cruccu G, Di Stefano G. Considerations When Using Gabapentinoids to Treat Trigeminal Neuralgia: A Review. Neuropsychiatr Dis Treat. 2023 Sep 19;19:2007-2012. PMCID: PMC10517700. [CrossRef] [PubMed]
- Patel P, Rajput HS, Chavda K, Mistry S, Bhagat S, Hadia R, Saiyed M, Khadela A. Assessing the effectiveness of gabapentin in paclitaxel-induced arthralgia, myalgia, and neuropathic pain: An observational, cohort study. J Oncol Pharm Pract. 2024 Jan 5:10781552231225148. Epub ahead of print. [CrossRef] [PubMed]
- Zerfas I, McGinn R, Smith MA. Pharmacologic Management of Cancer-Related Pain in Pregnant Patients. Drugs. 2023 Aug;83(12):1067-1076. Epub 2023 Jun 22. [CrossRef] [PubMed]
- Drake R, Prael G, Phyo Y, Chang S, Hunt J, Herbert A, Mott C, Hynson J, Phillips M, Cossich M, Mherekumombe M, Kim MS, Chong PH, Abitz M, Bernada M, Avery M, Doogue M, Rowett D, Currow D. Gabapentin for Pain in Pediatric Palliative Care. J Pain Symptom Manage. 2024 Mar;67(3):212-222.e1. Epub 2023 Nov 29. [CrossRef] [PubMed]
- Fleser L, Tibbetts E, Hanson A, Chu EC, Gura K, Tom C, Williams K, Levy P. Evaluating Gabapentin Dosing, Efficacy and Safety in Infants. J Pediatr Pharmacol Ther. 2024 Apr;29(2):159-168. Epub 2024 Apr 8. PMCID: PMC11001217. [CrossRef] [PubMed]
- Anfuso CD, Olivieri M, Fidilio A, Lupo G, Rusciano D, Pezzino S, Gagliano C, Drago F, Bucolo C. Gabapentin Attenuates Ocular Inflammation: In vitro and In vivo Studies. Front Pharmacol. 2017 Apr 4;8:173. PMCID: PMC5378778. [CrossRef] [PubMed]
- Yoon HJ, Kim J, Yoon KC. Treatment Response to Gabapentin in Neuropathic Ocular Pain Associated with Dry Eye. J Clin Med. 2020 Nov 22;9(11):3765. PMCID: PMC7700262. [CrossRef] [PubMed]
- Ongun N, Ongun GT. Is gabapentin effective in dry eye disease and neuropathic ocular pain? Acta Neurol Belg. 2021 Apr;121(2):397-401. Epub 2019 May 27. [CrossRef] [PubMed]
- Nissman SA, Tractenberg RE, Babbar-Goel A, Pasternak JF. Oral gabapentin for the treatment of postoperative pain after photorefractive keratectomy. Am J Ophthalmol. 2008 Apr;145(4):623-629. Epub 2008 Jan 28. [CrossRef] [PubMed]
- Lichtinger A, Purcell TL, Schanzlin DJ, Chayet AS. Gabapentin for postoperative pain after photorefractive keratectomy: a prospective, randomized, double-blind, placebo-controlled trial. J Refract Surg. 2011 Aug;27(8):613-7. Epub 2011 Feb 28. [CrossRef] [PubMed]
- Pakravan M, Roshani M, Yazdani S, Faramazi A, Yaseri M. Pregabalin and gabapentin for post-photorefractive keratectomy pain: a randomized controlled trial. Eur J Ophthalmol. 2012;22 Suppl 7:S106-13. [CrossRef] [PubMed]
- Serna-Ojeda JC, Santana-Cruz O, Quiroz-Casian N, González-Mendoza E, Mercado-Orozco JL, Navas A, Lichtinger A, Graue-Hernandez EO. Pain Management in Corneal Collagen Crosslinking for Keratoconus: A Comparative Case Series. J Ocul Pharmacol Ther. 2019 Jul/Aug;35(6):325-330. Epub 2019 Jun 19. [CrossRef] [PubMed]
- Kavalieratos CS, Dimou T. Gabapentin therapy for painful, blind glaucomatous eye: case report. Pain Med. 2008 Apr;9(3):377-8. [CrossRef] [PubMed]
- Michael R, Jeffers JV, Messenger W, Aref AA. Gabapentin for presumed neuropathic ocular pain. Am J Ophthalmol Case Rep. 2020 Jul 22;19:100836. PMCID: PMC7390772. [CrossRef] [PubMed]
- Jehle T, Lagrèze WA, Blauth E, Knörle R, Schnierle P, Lücking CH, Feuerstein TJ. Gabapentin-lactam (8-aza-spiro [5,4]decan-9-on; GBP-L) inhibits oxygen glucose deprivation-induced [3H]glutmate release and is a neuroprotective agent in amodel of acute retinal ischemia. Naunyn Schmiedebergs Arch Pharmacol. 2000 Jul;362(1):74-81. [CrossRef] [PubMed]
- Lagrèze WA, Müller-Velten R, Feuerstein TJ. The neuroprotective properties of gabapentin-lactam. Graefes Arch Clin Exp Ophthalmol. 2001 Nov;239(11):845-9. [CrossRef] [PubMed]
- Pielen A, Kirsch M, Hofmann HD, Feuerstein TJ, Lagrèze WA. Retinal ganglion cell survival is enhanced by gabapentin-lactam in vitro: evidence for involvement of mitochondrial KATP channels. Graefes Arch Clin Exp Ophthalmol. 2004 Mar;242(3):240-4. Epub 2004 Feb 10. [CrossRef] [PubMed]
- Cammalleri M, Amato R, Olivieri M, Pezzino S, Bagnoli P, Dal Monte M, Rusciano D. Effects of Topical Gabapentin on Ocular Pain and Tear Secretion. Front Pharmacol. 2021 Jun 7;12:671238. PMCID: PMC8216672. [CrossRef] [PubMed]
- Cristaldi M, Olivieri M, Spampinato G, Anfuso CD, Scalia M, Lupo G, Rusciano D. Isolation and Characterization of a New Human Corneal Epithelial Cell Line: HCE-F. Cornea. 2020 Nov;39(11):1419-1425. [CrossRef] [PubMed]
- Yang CJ, Anand A, Huang CC, Lai JY. Unveiling the Power of Gabapentin-Loaded Nanoceria with Multiple Therapeutic Capabilities for the Treatment of Dry Eye Disease. ACS Nano. 2023 Dec 26;17(24):25118-25135Epub 2023 Dec 5. [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



