
Submitted:
29 April 2024
Posted:
29 April 2024
You are already at the latest version
Abstract
Varicella (chickenpox) is one of the most common infectious diseases in preschool children and can be prevented by immunization. While immunization program promotes higher vaccine coverage, there are still challenges with implementing vaccination programs particularly in low-income countries. Economic barriers can increase inequality in vaccination, which highlights the importance of distributing cost-effective varicella vaccines. Varicella vaccines have been developed with two main Varicella-Zoster Virus (VZV) strains globally: MAV/06 and Oka strains. Most of the vaccines are based on the Oka strain, while MAV/06 strain vaccines were exclusively developed by GC Biopharma. Although more than 30 million doses of MAV/06 vaccines as cost-effective vaccines have been distributed internationally, there is no comprehensive review on safety, immunogenicity, and effectiveness of MAV/06 vaccines in the literature. This paper aims to summarize and present more than 30 years of accumulated evidence from research on safety, immunogenicity, and effectiveness of MAV/06 vaccines. We expect that MAV/06 vaccines as cost-effective varicella vaccines make a significant contribution to improving global public health and health equality in children.
Keywords:
varicella
; MAV/06 strain
; cost-effective vaccine
; safety
; immunogenicity
; vaccine coverage
1. Introduction
Varicella-Zoster virus (VZV) is a type of herpesvirus with high infectivity, typically causing chickenpox in childhood and generally shingles in adulthood [1,2,3,4,5,6]. VZV belongs to the Herpesviridae family and is a double-stranded DNA virus, with only one serotype but divided into five major genotypes (clade 1 to 5). Clades 1 and 3 are usually found in Europe and America, clade 2 in Asia, clade 4, 5 in Africa [4,5,7,8,9].
The virus spreads through direct contact between individuals or inhalation of aerosol droplets from respiratory secretions of chickenpox patients, entering host cells via the upper respiratory tract or conjunctiva. After primary infection with VZV, the virus remains dormant in sensory ganglia and can later trigger shingles [4,5,6,10].
Infection with varicella leads to fever and typically manifests as vesicular rash on the trunk or head, with an incubation period of 14-16 days and a duration of around 6 days post-onset [5,10]. Healthy children generally develop around 250 to 500 skin vesicles. While severity and complications of chickenpox can increase among immunocompromised individuals, even healthy children or adults can experience rare but severe complications, including death [5,6].
VZV is globally distributed, and in countries without national immunization programs (NIP), most individuals become infected by adolescence, with the highest incidence observed in preschool or early elementary school children. Chickenpox also exhibits a strong seasonal pattern in temperate and some tropical climates, with the highest incidence occurring between winter and spring. Outbreaks can occur periodically in schools or daycare centers [4,5,6,11,12,13]. Globally, chickenpox affects over 140 million individuals annually, resulting in serious complications requiring hospitalization in over 4 million cases and causing over 4,000 deaths [5,6,14]. Prior to vaccination in the United States, approximately 4 million cases of chickenpox occurred annually, leading to over 10,000 hospitalizations and over 100 deaths each year [6,14]. Chickenpox significantly contributes to the burden of disease from secondary infections (e.g., group A streptococcal infections) among children [15]. Most hospitalizations due to chickenpox occur in children, resulting in significant absenteeism from school and work for parents caring for sick children. Therefore, some countries have implemented vaccination programs during childhood to control or eliminate chickenpox [5].
The United States was the first country to introduce the one-dose varicella vaccine into its NIP program in 1995. Since then, several countries have been introducing the varicella vaccine as a universal vaccination program, with its effectiveness being demonstrated through various studies. In the United States, a two-dose program was introduced in 2006. During twenty-five years after the introduction of the varicella NIP in the United States, the incidence of chickenpox has decreased by over 97% in all age groups, and particularly in individuals under 20 years of age [5,16,17,18]. In most countries where the varicella vaccine has been introduced into national vaccination programs, incidence and hospitalization rates have decreased by over 80%, indicating that vaccination is an effective method for preventing chickenpox. Therefore, the introduction of a varicella NIP has been recommended from a public health and economic perspective [5,14,19,20].
However, there are still many countries that have not introduced the varicella vaccine as a NIP [17,19,20,21,22,23,24,25,26,27,28]. In particular, most low-income countries in Africa lack a varicella NIP [17,19,29]. And within low- and middle-income countries, generally, vaccination coverage is lower in the children with low socioeconomic background (household wealth and mother’s education level) [30]. Cost-effective varicella vaccines are an essential prerequisite for increasing vaccine coverage and reducing vaccination inequality particularly among the children in low- and middle-income countries.
The objective of this study is to provide a comprehensive review of the characteristics, safety, immunogenicity, and effectiveness of the MAV/06 varicella vaccine developed by GC Biopharma Corp., and qualified by the World Health Organization (WHO) for routine childhood immunization in many countries.
2. Varicella Vaccines
The currently licensed vaccines for preventing chickenpox are the live attenuated vaccines, which include the Oka strain and the MAV/06 strain. Both strains belong to Clade 2 and are genetically very similar [31,32,33,34].
The majority of varicella vaccines used worldwide are derived from the wild-type pOka virus, which has been attenuated to create the vOka strain, known as the Oka-derived varicella vaccine. Vaccines derived from this attenuated virus are produced by Biken, MSD, GSK, and other manufacturers in China, among others [5,17,35,36].
3. MAV/06 Varicella Vaccines
3.1. Development History
3.1.1. Isolation of MAV Strain
3.1.2. Attenuation of MAV/06 Strain
To attenuate the obtained varicella viruses, several passages were carried out in normal human embryonic lung diploid cells (LuMa, normal human embryonic Lung diploid MogAm) and normal guinea pig lung diploid cells (GEL) through multiple cultivation steps (Table 3). To confirm the degree of attenuation, temperature sensitivity tests and cell susceptibility tests, which were previously used in the attenuation of the Oka virus strain [40] were employed. Among the varicella viruses tested, the sixth virus (designated MAV/06 virus) exhibited the highest cell susceptibility and the lowest temperature sensitivity. Therefore, it was selected as the attenuated varicella virus strain for GC Biopharma Corp.'s varicella vaccine [37].
Subsequent sequencing studies of varicella vaccines revealed 42 known single nucleotide polymorphisms (SNPs) occurring during the attenuation process from wild type to attenuated varicella viruses [31,33,41,42]. To confirm whether the MAV/06 vaccine was well attenuated, sequencing comparison studies were conducted with Oka-derived varicella vaccines. The results showed that levels of nucleotide sequence variations at the 42 SNP positions were similar between the MAV/06 vaccine and to vOka-derived varicella vaccines such as VARILRIX and VARIVAX. Based on these findings, it was confirmed that the MAV/06 vaccine was well attenuated [31,43].
3.1.3. Genomic characteristics of MAV/06 Strain
- Genotyping
To date, there are multiple VZV strains whose whole genome sequence has been identified, and their nature can be divided into the pathogenic wild-type (Dumas and pOka, Table 4), which induces disease in humans, and the vaccine-type, which induces defensive immunity. The Oka strain (vOka, VARILRIX, and VARIVAX) and the MAV/06 strain (BARYCELA inj. and Varicella Vaccine-GCC inj. (Suduvax), Table 4).
As a result, the whole genome sequence length of the MAV/06 strain was 124,758 bp, and the structure of VZV consisting of TRL, UL, IRL, IRS, US, and TRS was identified. This confirms that the MAV/06 virus does not exhibit significant differences compared to other representative wild-type viruses and vOka-derived viruses [34] (Table 4).

Table 4.
Genome structure of VZV strain [34].
Table 4.
Genome structure of VZV strain [34].
| Strain | Accession Number | Full Length (bp) | Length (bp) | |||||
|---|---|---|---|---|---|---|---|---|
| TRL1 | UL2 | IRL3 | IRS4 | US5 | TRS6 | |||
| Dumas | NC001348 | 124,884 | 88 | 104,836 | 88 | 7,320 | 5,232 | 7,320 |
| pOka* | AB097933 | 125,125 | 88 | 104,798 | 88 | 7,463 | 5,225 | 7,463 |
| vOka* | AB097932 | 125,078 | 88 | 104,822 | 88 | 7,427 | 5,232 | 7,421 |
| VARILRIX | DQ008354 | 124,821 | 88 | 104,761 | 88 | 7,326 | 5,231 | 7,327 |
| VARIVAX | DQ008355 | 124,815 | 88 | 104,758 | 88 | 7,324 | 5,232 | 7,325 |
| MAV/06* | JF306641 | 124,758 | 88 | 104,798 | 88 | 7,276 | 5,232 | 7,276 |
1TRL (Terminal long repeat); 2UL (Unique long region); 3IRL (Internal long repeat); 4IRS (Internal short repeat); 5US (Unique short region); 6TRS (Terminal short repeat); *pOka (parental Oka), *vOka (vaccine Oka), *MAV/06 (BARYCELA inj. & Varicella Vaccine-GCC inj.).
- Clade analysis
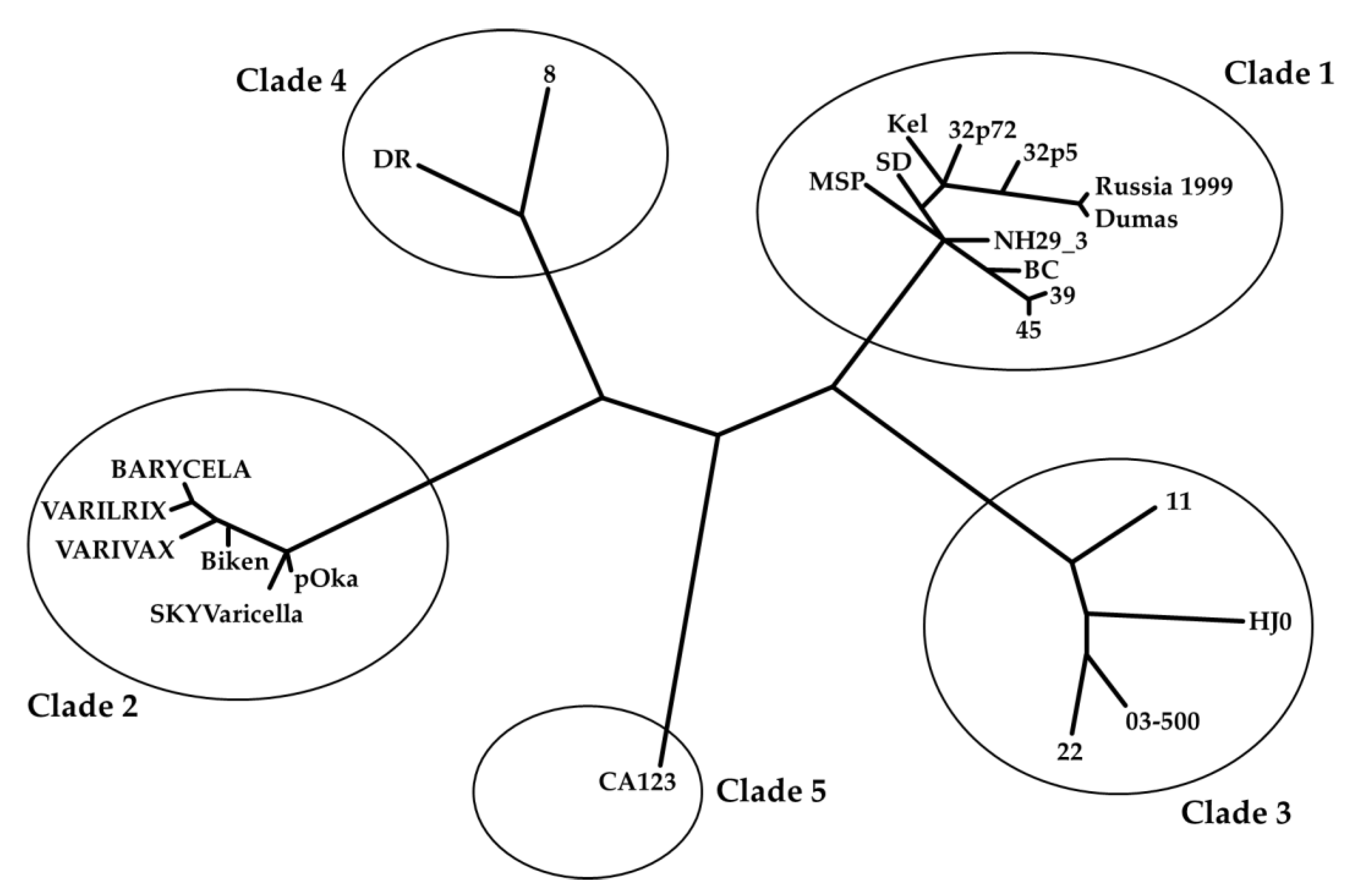
The MAV/06 vaccine underwent whole-genome sequencing in three studies, allowing for the confirmation of its genetic characteristics. The results of the whole-genome sequencing revealed that the MAV/06 vaccine belongs genetically to the same clade (Clade 2) as the well-known Oka-derived vaccines (VARIVAX, VARILRIX and Biken) [31,34,43] (Figure 1).
3.2. Product Information
There are two varicella vaccines that are derived from the MAV/06 strain: BARYCELA inj. and Varicella Vaccine-GCC inj. (Suduvax).
Varicella Vaccine-GCC inj. was developed by GC Biopharma Corp. using MAV/06 strain and LuMA cell line, which became the world’s second licensed varicella vaccine in 1993 [34,43,44].
The second generations MAV/06 varicella vaccine, BARYCELA inj., was developed by GC Biopharma Corp. using MAV/06 strain and MRC-5 cell line and licensed in 2020 [45,46]. BARYCELA inj. features an enhanced manufacturing process and greater stability compared to Varicella Vaccine-GCC inj. Antibiotic additives are generally used to prevent contamination of cells during a manufacturing process of vaccines. There are possibilities that these antibiotics may cause adverse drug reactions such as anaphylaxis in some people after administration. BARYCELA inj. is the world’s first and only antibiotic-free varicella vaccine that eliminates the risk of adverse reactions and assures improved safety [47,48,49,50,51].
For each vial of Varicella Vaccine-GCC inj., not less than 1,400 PFU of live attenuated VZVs are supplied in lyophilized powder. In addition to the active ingredient, each vial contains the following ingredients: sucrose (as a stabilizer), glycine (as a stabilizer), sodium L-glutamate hydrate (as a stabilizer), gelatin (as a stabilizer), L-cysteine (as a stabilizer), edetate disodium (as a stabilizer), Na₂HPO₄.12H₂O (as a buffer) and NaH₂PO₄.2H₂O (as a buffer). For each annexed vial of diluent, a volume of 0.7mL sterile water for injection is included in a kit. Varicella Vaccine-GCC inj. becomes a transparent colorless or yellowish solution when reconstituted with the diluent supplied and is stored at 2-8℃ with a shelf life of 2 years.
For each vial of BARYCELA inj., not less than 3,800 PFU of live attenuated VZVs are supplied in lyophilized powder. In addition to the active ingredient, each vial contains the following ingredients: Sucrose (as a stabilizer), Glycine (as a stabilizer), Sodium L-glutamate hydrate (as a stabilizer), Gelatin (as a stabilizer), L-cysteine (as a stabilizer), Disodium edetate hydrate (as a stabilizer), Urea (as a stabilizer); Dibasic sodium phosphate hydrate (as a buffer), Potassium dihydrogen phosphate (as a buffer). For each enclosed vial of diluent, a volume of 0.7 mL sterile water for injection is included in a kit. BARYCELA inj. becomes a transparent colorless or pale-yellow solution when reconstituted with the diluent supplied and is stored at 2-8℃ with a shelf life of 2 years.
3.3. Registration and Distribution
3.3.1. Registration
- Varicella Vaccine-GCC inj. (Suduvax) [44]
Varicella Vaccine-GCC inj. was first approved in 1993 in South Korea and later approved in other Asian and South American countries (Table 5).
BARYCELA inj. was first approved in 2020 and launched in 2021 in South Korea. It was included in the list of prequalified varicella vaccines by the World Health Organization (WHO) in 2023 (Table 5). In the same year, this vaccine was approved in Pakistan. As of 2024, regulatory approval processes are underway in about 10 countries, including Turkiye, Saudi Arabia, Vietnam in Asia, and countries in South America such as Brazil and Argentina.
| Vaccine | Country | Approved date | Trade Name |
|---|---|---|---|
| Varicella Vaccine-GCC inj. | S.Korea | June, 1993 | Suduvax inj. |
| Peru | March, 2000 | Varicella vaccine KGCC | |
| Dominica | December, 2000 | VACUNA DE VARICELA GCC, 1,400 PFU/0.7mL | |
| Indonesia | September, 2001 | Varicella vaccine KGCC | |
| Philippines | June, 2005 | V-z vax | |
| Egypt | August, 2006 | Varicella vaccine GCC | |
| Thailand | March, 2007 | Varicella vaccine-GCC inj. | |
| Vietnam | October, 2008 | Varicella vaccine-GCC inj. | |
| Colombia | September, 2011 | Vacuna contra la varicella GCC inyeccion | |
| Guatemala | April, 2019 | Vacuna contra la Varicela | |
| BARYCELA inj. | S.Korea | March, 2020 | BARYCELA inj. |
| WHO | February, 2023 | BARYCELA inj. | |
| Pakistan | June, 2023 | BARYCELA inj. |
3.3.2. Distribution
- Varicella Vaccine-GCC inj. (Suduvax)[44]
Varicella Vaccine-GCC inj. has been shipped and exported to 26 countries, totaling over 29 million doses (Total 26 countries; Aruba, Anguilla, Antigua and Barbuda, Barbados, Bahamas, Bermuda, Brazil, British Virgin Islands, Cayman Islands, Chile, Colombia, Costa Rica, Ecuador, Grenada, Guatemala, Nepal, Panama, Paraguay, Philippines, S.Korea, Saint Lucia, Saudi Arabia, Thailand, Trinidad and Tobago, Turkiye, Vietnam).
- BARYCELA inj.[55]
BARYCELA inj. has been shipped and exported to 6 countries, totaling over 520,000 doses (Total 6 countries; Aruba, Antigua and Barbuda, Guatemala, S.Korea, Saint Lucia, Trinidad and Tobago).
- Over the past 30 years, MAV/06 varicella vaccines have been distributed to over 20 countries worldwide, totaling approximately 30 million doses. Through the Pan American Health Organization (PAHO) bidding, the vaccines have been stably supplied to countries in Central and South America. Throughout this process, MAV/06 varicella vaccines have been confirmed as the most cost-effective option, offering the most rational pricing in terms of cost [56,57,58] (Table 6). On average, the price of the MAV/06 vaccine supplied to the PAHO was 20% lower than that of the Oka vaccines during 2021-2023 according to the PAHO.
3.4. Safety, Immunogenicity and Effectiveness
3.4.1. Safety
The evidence of the safety of MAV/06 vaccines has been accumulated and demonstrated through several clinical trials and 30 years of real-world use. The secured safety data is as follows:
- Evidence from clinical trials
The safety of the MAV/06 vaccine has been confirmed through various clinical trials. When summarizing the safety results obtained from these trials, the following points emerge:
MAV/06 vaccine has demonstrated satisfactory safety profiles across different age groups, including infants, children, adolescents, and adults.
Safety assessments conducted in both healthy individuals and those with compromised immune function (such as immunocompromised infants) have shown satisfactory outcomes.
No significant differences in safety profiles were observed between MAV/06 vaccine and comparator vaccine (such as VARIVAX) in randomized controlled trials.
The vaccine exhibited satisfactory safety outcomes at different dosage levels, ranging from 300 PFU to 25,000 PFU.
Safety assessments conducted in various countries, including S.Korea, Thailand, the Philippines, and Vietnam, have consistently confirmed the safety of MAV/06 vaccine across diverse populations.
Overall, the comprehensive safety data obtained from multiple clinical trials support the conclusion that the MAV/06 vaccine is safe for use in the prevention of varicella infection (Table 7).
- 1.
- Safety and immunogenicity of live attenuated varicella vaccine (MAV/06 strain) in adults and children (1994) [59]
In Korea, safety was confirmed by administering MAV/06 vaccines ranging from 300 PFU to 2,000 PFU to a total of 62 healthy adults and children (30 adults, 32 infants). Safety issues were not observed, and no serious adverse events were reported. Additionally, no significant adverse effects were identified.
- 2.
- Immunogenicity and safety of live attenuated vaccine (MAV/06 strain) on healthy children and immunocompromised children (1995) [60]
In Korea, safety was confirmed by administering the MAV/06 vaccine to a total of 177 healthy infants, children, and adolescents (aged 12 months to 19 years), as well as 22 immunocompromised infants (who had undergone medical treatment for conditions such as 6 leukemia, 10 solid tumors, and 6 nephrotic syndromes). No unusual adverse events were observed.
- 3.
- Immunogenicity and safety of a new live attenuated varicella vaccine (MAV/06 strain) among healthy Filipino children of ages 9 months to 17 years (2001) [61]
In the Philippines, the MAV/06 vaccine was administered to a total of 375 healthy infants and children (aged 9 months to 17 years). Safety was assessed by dividing the participants into age-specific groups, and the vaccine was well tolerated with no serious or unusual adverse events were reported.
- 4.
In Korea, a total of 39 healthy adults were recruited, with the WHO pre-qualified vaccine VARIVAX serving as the control vaccine. The BARYCELA inj. vaccine was administered at different doses (2,000 PFU, 8,000 PFU, 25,000 PFU) to assess safety. No significant safety issue was observed in the overall trends and no serious adverse event was reported (ClinicalTrials.gov ID; NCT02367638).
- 5.
In Thailand, a total of 299 healthy infants and children (aged 12 months to 12 years) were recruited. The WHO pre-qualified vaccine VARIVAX served as the control vaccine. The BARYCELA inj. vaccine was administered at different doses (2,000 PFU, 8,000 PFU, 25,000 PFU) to assess safety. Vaccination with all groups was safe and well-tolerated in subjects aged 12 months to 12 years (ClinicalTrials.gov ID; NCT03375502).
- 6.
In both Korea and Thailand, a total of 515 healthy infants and children (aged 12 months to 12 years) were recruited. The WHO pre-qualified vaccine VARIVAX served as the control vaccine. The subjects were randomly assigned in a 1:1 ratio, with 258 subjects receiving BARYCELA and 257 subjects receiving VARIVAX. Safety was assessed, and it was confirmed that there were no significant differences compared to the control group (ClinicalTrials.gov ID; NCT03375502).
- 7.
In Vietnam, a total of 250 healthy infants and children were vaccinated with BARYCELA vaccine. Safety was assessed by dividing the participants into age-specific groups, and safety findings continue to support good safety profile in healthy children aged 12 months to 12 years. Satisfactory safety was confirmed in all groups (ClinicalTrials.gov ID; NCT05664152).
- Evidence from post-marketing real world uses
Once a medicine receives regulatory approval and is marketed, periodic benefit-risk evaluation reports (PBRER), previously known as Periodic Safety Update Reports (PSUR), are prepared according to the ICH E2C (R2) guideline [69].
As of March 2024, four reports have been compiled for Varicella Vaccine-GCC inj., while six reports have been prepared for BARYCELA inj. These reports include information on the quantities of vaccines supplied during a specific period and adverse reaction cases reported in the field during that period.
Varicella Vaccine-GCC inj. was distributed a total of 29,224,770 doses from 2005 to June 2022. Among these, there were 120 reports about adverse drug reactions. BARYCELA inj. has been distributed 528,360 doses since 2020 and 3 voluntary adverse reaction reports have been accumulated [44,46,55,70,71,72,73,74,75,76] (Table 8).
Table 8.
Summary of PBRER(PSUR) for Varicella Vaccine-GCC inj. and BARYCELA inj. [44,46,55,70,71,72,73,74,75,76].
| Vaccine | Report version | Reporting Period | Distribution (vials) | Overall reported ADRs1 cases | Conclusion |
|---|---|---|---|---|---|
| Varicella Vaccine-GCC inj. | PSUR v1.0 | January 2005-June 2013 | 6,512,915 | 3 | There were no new safety issues associated with Varicella Vaccine-GCC inj. during this PSUR reporting period |
| PSUR v2.1 | June 2013- June 2016 | 5,070,608 | 30 | There were no new safety issues associated with Varicella Vaccine-GCC inj. during this PSUR reporting period | |
| PBRER v3.0 | June 2016-June 2019 | 11,475,897 | 77 | No new relevant safety findings which would necessitate an analysis and a change in the current reference safety information | |
| PBRER v4.0 | June 2019-June 2022 | 6,165,350 | 10 | No new relevant safety findings which would necessitate an analysis and a change in the current reference safety information | |
| Total | 29,224,770 | 120 | - | ||
| BARYCELA inj. | PBRER v1.0 | March 2020-September 2020 | - * | - | No new relevant safety findings which would necessitate an analysis and a change in the current reference safety information |
| PBRER v2.0 | September 2020 -March 2021 | - * | - | No new relevant safety findings which would necessitate an analysis and a change in the current reference safety information | |
| PBRER v3.0 | March 2021-September 2021 | - * | - | No new relevant safety findings which would necessitate an analysis and a change in the current reference safety information | |
| PBRER v4.0 | September 2021 -March 2022 | 52,070 | - | No new relevant safety findings which would necessitate an analysis and a change in the current reference safety information | |
| PBRER v5.0 | March 2022-March 2023 | 182,980 | 1 | No new relevant safety findings which would necessitate an analysis and a change in the current reference safety information | |
| PBRER v6.0 | March 2023-March 2024 | 293,310 | 2 | No new relevant safety findings which would necessitate an analysis and a change in the current reference safety information | |
| Total | 528,360 | 3 | - | ||
1ADRs: Adverse Drug Reactions, *No launch.
Although direct comparison may be limited due to differences in pharmacovigilance reporting systems among manufacturers and countries, as well as variations in reporting practices across nations, it can be observed that MAV/06 vaccine demonstrates a lower incidence of adverse reactions compared to other varicella vaccines. This suggests favorable safety outcomes post-market approval (Table 9) [77,78,79].
- Strain Interchangeability
Some countries have incorporated a two-dose regimen of varicella vaccine into their NIP, and the WHO also recommends a two-dose vaccination to further reduce the incidence of varicella cases and to decrease outbreaks in the community [6].
In line with this, a study was conducted to assess the safety of cross-vaccination with MAV/06 and vOka-derived vaccines when administered in a two-dose regimen [80].
The study involved a total of 406 Korean infants, who received the first and second doses of vaccination with MAV/06-vOka, vOka-MAV/06, MAV/06-MAV/06 and vOka-vOka, respectively. The study confirmed that there were no safety concerns associated with this cross-strain vaccination regimen.
- Antibiotic-Free
Antibiotics (e.g., Kanamycin, Neomycin, and Erythromycin) are generally used to prevent contamination of cells during a manufacturing process of vaccines. There are possibilities that these antibiotics may cause adverse drug reactions such as anaphylaxis in some people after administration [81]. However, BARYCELA inj. is a varicella vaccine that does not contain antibiotics, thus eliminating the risk of adverse reactions associated with antibiotics [47,49,50,51].
3.4.2. Immunogenicity
The gold standard test for measuring VZV antibodies is the Fluorescent Antibody to Membrane Antigen (FAMA) assay, developed in the 1970s. Additionally, the glycoprotein enzyme-linked immunosorbent assay (gpELISA) is commonly used. Generally, an FAMA antibody titer of 1:4 or higher is considered seropositive, indicating protection against varicella [5,82,83].
The immunogenicity of MAV/06 vaccines have been investigated tested through several clinical trials and studies.
- Results of clinical trials
Through various clinical trials, high post-vaccination antibody titers and very high seroconversion rates (SCRs) have been confirmed.
In South Korea, the SCR of MAV/06 vaccines (BARYCELA inj. and Varicella Vaccine-GCC inj.) were close to 100% in healthy infants and children aged 12 months to 19 years, and immunocompromised children.
In the Philippines, healthy infants and children aged 9 months to 17 years, the SCR of Varicella Vaccine-GCC inj. was close to 100% at both 6 weeks and 5 years after vaccination.
In Thailand, the SCR of BARYCELA inj. was close to 100% in healthy infants and children aged 12 months to 12 years.
In Vietnam, healthy infants and children, high antibody titers of 69.9 and 126.5 were observed after vaccination with BARYCELA inj. (Table 10).
- Safety and immunogenicity of live attenuated varicella vaccine (MAV/06 strain) in children (1994) [59]
In South Korea, a total of 32 healthy children with negative FAMA antibodies before vaccination were vaccinated with MAV/06 vaccine doses ranging from 300 PFU to 1,000 PFU to confirm immunogenicity. The results showed that regardless of the vaccine dose, children had a 100% SCR and high antibody levels 4 weeks after vaccination.
- 2.
- Immunogenicity and safety of live attenuated vaccine (MAV/06 strain) on healthy children and immunocompromised children (1995) [60]
In South Korea, a total of 161 healthy children and adolescents (aged 12 months to 19 years) and 18 immunocompromised children (who had undergone medical treatment for conditions such as 6 leukemia, 10 solid tumors, and 6 nephrotic syndromes) were vaccinated with MAV/06 vaccine to confirm immunogenicity. After 4 weeks, both healthy children and immunocompromised children showed a 100% SCR.
- 3.
- Immunogenicity and safety of a new live attenuated varicella vaccine (MAV/06 strain) among healthy Filipino children of ages 9 months to 17 years (2001) [61]
In the Philippines, a total of 299 healthy infants and children (aged 9 months to 17 years) were vaccinated with MAV/06 vaccine, and immunogenicity was assessed by age group. The average SCR was confirmed to be 99.7% six weeks after vaccination.
- 4.
In 2001, a clinical study was conducted in the Philippines to assess the immunogenicity and safety of the vaccine [61]. Five years later, long-term immunogenicity and protective efficacy were evaluated. Among the 299 healthy children enrolled in the study, 163 were followed up, and 162 of them were confirmed to be seropositive (99.4%).
- 5.
In a study conducted in Korea, a total of 39 healthy adults were vaccinated with BARYCELA inj. at different doses (2,000 PFU, 8,000 PFU, 25,000 PFU) with WHO pre-qualified vaccine VARIVAX as the control vaccine. After 6 weeks, the FAMA GMT results for each dose were found to be 78.8, 90.5, and 68.6, respectively (ClinicalTrials.gov ID; NCT02367638).
- 6.
In a study conducted in Thailand, a total of 193 healthy infants and children (12 months to 12 years) were vaccinated with BARYCELA inj. at different doses (2,000 PFU, 8,000 PFU, 25,000 PFU) with WHO pre-qualified vaccine VARIVAX as the control vaccine. After 6 weeks, the results showed a 100% SCR for each dose, with geometric mean titer (GMT) results of 85.5, 109.9, and 65.6, respectively (ClinicalTrials.gov ID; NCT03375502).
- 7.
In both Korea and Thailand, a total of 478 healthy infants and children (aged 12 months to 12 years) were enrolled in a randomized, 1:1 controlled trial, with WHO pre-qualified vaccine VARIVAX as the control vaccine and BARYCELA as the test vaccine (239 subjects in each group). After 6 weeks, the test group showed non-inferiority compared to the control group in terms of immunogenicity. The SCR results were 97.9% and 99.2% for the test and control groups, respectively. The GMT results were 74.2 and 112.7, respectively (ClinicalTrials.gov ID; NCT03375502).
- 8.
In Vietnam, a total of 246 healthy infants and children were vaccinated with the BARYCELA vaccine. They were divided into age-specific groups to assess immunogenicity. After 6 weeks, the GMT results for each age group were 69.9 and 126.5, respectively (ClinicalTrials.gov ID; NCT05664152).
- Results of seroprevalence study
In 2016, a study conducted in South Korea examined the seropositivity rate among total 715 children who received the varicella vaccines distributed in Korea. In the study, the seropositivity of the MAV/06 vaccine using the FAMA test was 74%, while the seropositivity of a vOka derived vaccine (Vari-L) was 63% [85]. This result is similar to the findings from previous studies conducted in the United States in 2006 (76%) [5,86] and in Korea in 2010 (83.6%) [82] (Table 11).
Furthermore, in a Korean study [85], there was a tendency that antibody levels (assessed with gpELISA tests) decreased as age of children increased from 1 to 4 years. However, there was no significant difference in the tendency between the MAV/06 vaccine group and the Oka vaccine group, indicating a long-term persistence of antibodies of the MAV/06 vaccines would be similar to that of the Oka vaccine [85].
- Cell-Mediated Immunity (CMI)
CMI is known to play a crucial role in regulating VZV and providing protection against additional VZV infections. Therefore, it was investigated whether CMI is induced after MAV/06 vaccination using a non-clinical animal model, and the results confirmed the induction of CMI through a Th1 cell-mediated response [87].
- Cross-reactive humoral immunity
VZV exhibits genetic variation regionally, but currently licensed varicella vaccines are all developed based on clade 2 strains [4,7,88]. Studies have investigated whether antibodies generated from Oka varicella vaccines elicit immune responses against different genotypes of varicella viruses [89]. Similarly, research has been conducted to assess cross-reactivity of antibodies generated after MAV/06 vaccination with varicella viruses of different clades, using both animal and human sera [87,90]. The findings indicate that antibodies generated after MAV/06 vaccination show effective immune responses against varicella viruses of different clades (clade 1, 3, and 5), including wild-type clade 2 viruses, demonstrating high and similar FAMA antibody titers across different clades [90].
3.4.3. Effectiveness
After conducting clinical trial on immunogenicity and safety of MAV/06 vaccine in the Philippines in 2001, a follow-up effectiveness study was conducted for 5 years. Out of 299 healthy children enrolled in the previous clinical trial, 163 were able to be observed up to 5 years after the clinical trial. None of them contracted chickenpox during the follow-up period, indicating 100% protection over the follow-up period [74,84].
In addition, two separate groups of Korean researchers investigated changes in the varicella epidemiology in Korean populations before and after the introduction of a one-dose universal varicella vaccination program in 2005. They reported that varicella incidence significantly decreased by 60-67%, and the peak age of varicella occurrence also shifted towards older ages [91,92,93]. Furthermore, according to a recent study [94], the incidence rate of complicated varicella cases among Korean children significantly (96%) decreased from 137 per 100,000 persons in 2010 to 6 per 100,000 persons in 2021. Considering that MAV/06 vaccine was predominantly distributed in Korea during this period, all of the above results indirectly support the effectiveness of the MAV/06 vaccine in Korean populations.
In a retrospective birth cohort study in 2011 in Korea where the vaccine coverage was higher than 95%, the incidence rate of break-through varicella cases in the cohort that received a single dose of MAV/06 vaccine was 27.1 per 1,000 person-years during a follow-up period of six years [95,96]. This rate was similar to the results of other studies conducted in the United States using the vOka-derived vaccine, which reported a range of 21.7-28.3 cases per 1,000 person-years [97,98,99,100].
GC Biopharma Corp. is currently conducting an effectiveness study with a follow-up period of six years in 1,000 Korean children who received the BARYCELA vaccine [55]. We expect that the on-going study will provide another good evidence of the effectiveness of the MAV/06 vaccines.
4. Conclusions
MAV/06 varicella vaccines, which are developed by GC Biopharma Corp., have been distributed worldwide with more than 30 million doses over the past 30 years, ensuring stable vaccine supply to numerous countries. Through various clinical trials and post-marketing experiences, their safety, including strain-interchangeability, has been confirmed. Especially, the recently developed BARYCELA inj. is antibiotic-free, addressing safety concerns associated with antibiotics. Outstanding humoral (utilizing the FAMA assay and cross-reactivity test) and cell-mediated immunogenicity of the MAV/06 vaccines has been demonstrated through diverse clinical trials and research. Moreover, several studies have supported the effectiveness of MAV/06 vaccines, although on-going and future studies will add more evidence. Overall, we think that safety, immunogenicity, and effectiveness of MAV/06 varicella vaccines are at least comparable to vOka vaccines, while MAV/06 vaccines have been more cost-effective for low-and middle-income countries than vOka vaccines.
Varicella vaccine administration is the most effective method for preventing chickenpox. We expect that MAV/06 vaccines as cost-effective varicella vaccines make a significant contribution to improving global public health and health equality in children.
Author Contributions
Conceptualization, Shin, Y.; Ryu, H.; Kim, G.; Yang, S.; and Choi, B. K.; writing—original draft preparation, Shin, Y.; Ryu, H.; writing—review and editing, Kim, G.; Yang, S.; Lee, J.; and Choi, B. K.; visualization, Shin, Y.; Ryu, H.; supervision, Choi, B. K.; project administration, Lee, J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
We thank Mina Lee from Sunchon National University for support with analysis of the data including figures and tables.
Conflicts of Interest
All authors are employees of GC Biopharma Corp. Involvement of GC Biopharma Corp. employee did not compromise the scientific integrity of this work.
References
- Depledge, D.P.; Sadaoka, T.; Ouwendijk, W.J.D. Molecular Aspects of Varicella-Zoster Virus Latency. Viruses 2018, 10. [CrossRef]
- Gershon, A.A.; Silverstein, S.J. Varicella-Zoster Virus. In Clinical Virology: Third Edition; 2022.
- Zerboni, L.; Sen, N.; Oliver, S.L.; Arvin, A.M. Molecular Mechanisms of Varicella Zoster Virus Pathogenesis. Nat Rev Microbiol 2014, 12. [CrossRef]
- Gershon, A.A.; Breuer, J.; Cohen, J.I.; Cohrs, R.J.; Gershon, M.D.; Gilden, D.; Grose, C.; Hambleton, S.; Kennedy, P.G.E.; Oxman, M.N.; et al. Varicella Zoster Virus Infection. Nat Rev Dis Primers 2015, 1. [CrossRef]
- Plotkin, S.; Orenstein, W.; Offit, P.; Kathryn, M.E. Plotkin’s Vaccines ; 7th Edition.; 2018; pp. 1145-1180.
- Varicella and Herpes Zoster Vaccines: WHO Position Paper, June 2014 - Recommendations. Vaccine 2016, 34.
- Barrett-Muir, W.; Scott, F.T.; Aaby, P.; John, J.; Matondo, P.; Chaudhry, Q.L.; Siqueira, M.; Poulsen, A.; Yaminishi, K.; Breuer, J. Genetic Variation of Varicella-Zoster Virus: Evidence for Geographical Separation of Strains. In Proceedings of the Journal of Medical Virology; 2003; Vol. 70. [CrossRef]
- Breuer, J.; Grose, C.; Norberg, P.; Tipples, G.; Schmid, D.S. A Proposal for a Common Nomenclature for Viral Clades That Form the Species Varicella-Zoster Virus: Summary of VZV Nomenclature Meeting 2008, Barts and the London School of Medicine and Dentistry, 24-25 July 2008. Journal of General Virology 2010, 91. [CrossRef]
- Garcés-Ayala, F.; Rodríguez-Castillo, A.; Ortiz-Alcántara, J.M.; Gonzalez-Durán, E.; Segura-Candelas, J.M.; Pérez-Agüeros, S.I.; Escobar-Escamilla, N.; Méndez-Tenorio, A.; Diaz-Quiñonez, J.A.; Ramirez-González, J.E. Full-Genome Sequence of a Novel Varicella-Zoster Virus Clade Isolated in Mexico. Genome Announc 2015, 3. [CrossRef]
- Chen, J.J.; Zhu, Z.; Gershon, A.A.; Gershon, M.D. Mannose 6-Phosphate Receptor Dependence of Varicella Zoster Virus Infection in Vitro and in the Epidermis during Varicella and Zoster. Cell 2004, 119. [CrossRef]
- Sengupta, N.; Breuer, J. A Global Perspective of the Epidemiology and Burden of Varicella-Zoster Virus. Curr Pediatr Rev 2010, 5. [CrossRef]
- Finger, R.; Hughes, J.P.; Meade, B.J.; Pelletier, A.R.; Palmer, C.T. Age-Specific Incidence of Chickenpox. Public Health Reports 1994, 109.
- Lolekha, S.; Tanthiphabha, W.; Sornchai, P.; Kosuwan, P.; Sutra, S.; Warachit, B.; Chup-Upprakarn, S.; Hutagalung, Y.; Weil, J.; Bock, H.L. Effect of Climatic Factors and Population Density on Varicella Zoster Virus Epidemiology within a Tropical Country. American Journal of Tropical Medicine and Hygiene 2001, 64. [CrossRef]
- Marin, M.; Leung, J.; Gershon, A.A. Transmission of Vaccine-Strain Varicella-Zoster Virus: A Systematic Review. Pediatrics 2019, 144. [CrossRef]
- Ramilo, O. Bacterial Complications of Primary Varicella in Children. Clinical Infectious Diseases 1996, 23. [CrossRef]
- Marin, M.; Seward, J.F.; Gershon, A.A. 25 Years of Varicella Vaccination in the United States. Journal of Infectious Diseases 2022, 226, S375–S379. [CrossRef]
- Lee, Y.H.; Choe, Y.J.; Lee, J.; Kim, E.; Lee, J.Y.; Hong, K.; Yoon, Y.; Kim, Y.K. Global Varicella Vaccination Programs. Clin Exp Pediatr 2022, 65, 555–562. [CrossRef]
- Marin, M.; Lopez, A.S.; Melgar, M.; Dooling, K.; Curns, A.T.; Leung, J. Decline in Severe Varicella Disease during the United States Varicella Vaccination Program: Hospitalizations and Deaths, 1990–2019. Journal of Infectious Diseases 2022, 226. [CrossRef]
- Varela, F.H.; Pinto, L.A.; Scotta, M.C. Global Impact of Varicella Vaccination Programs. Hum Vaccin Immunother 2019, 15, 645–657. [CrossRef]
- Marijam, A.; Safonova, E.; Scherbakov, M.; Shpeer, E.; Van Oorschot, D.; Rudakova, A.; Tatochenko, V.; Briko, N. Cost Effectiveness and Budget Impact of Universal Varicella Vaccination in Russia. Hum Vaccin Immunother 2022, 18. [CrossRef]
- Bonanni, P.; Breuer, J.; Gershon, A.; Gershon, M.; Hryniewicz, W.; Papaevangelou, V.; Rentier, B.; Rümke, H.; Sadzot-Delvaux, C.; Senterre, J.; et al. Varicella Vaccination in Europe - Taking the Practical Approach. BMC Med 2009, 7. [CrossRef]
- Chacon-Cruz, E.; Meroc, E.; Costa-Clemens, S.A.; Clemens, R.; Verstraeten, T. Economic Evaluation of Universal Varicella Vaccination in Mexico. Pediatric Infectious Disease Journal 2022, 41. [CrossRef]
- Feng, H.; Zhang, H.; Ma, C.; Zhang, H.; Yin, D.; Fang, H. National and Provincial Burden of Varicella Disease and Cost-Effectiveness of Childhood Varicella Vaccination in China from 2019 to 2049: A Modelling Analysis. Lancet Reg Health West Pac 2023, 32. [CrossRef]
- Chui, K.S.; Wu, H.L.; You, J.H.S. Cost-Effectiveness Analysis of Varicella Vaccine as Post-Exposure Prophylaxis in Hong Kong. Scand J Infect Dis 2014, 46. [CrossRef]
- Azzari, C.; Baldo, V.; Giuffrida, S.; Gani, R.; O’brien, E.; Alimenti, C.; Daniels, V.J.; Wolfson, L.J. The Cost-Effectiveness of Universal Varicella Vaccination in Italy: A Model-Based Assessment of Vaccination Strategies. ClinicoEconomics and Outcomes Research 2020, 12. [CrossRef]
- Wolff, E.; Widgren, K.; Tomba, G.S.; Roth, A.; Lep, T.; Andersson, S. Cost-Effectiveness of Varicella and Herpes Zoster Vaccination in Sweden: An Economic Evaluation Using a Dynamic Transmission Model. PLoS One 2021, 16. [CrossRef]
- Scuffham, P.; Devlin, N.; Eberhart-Phillips, J.; Wilson-Salt, R. The Cost-Effectiveness of Introducing a Varicella Vaccine to the New Zealand Immunisation Schedule. Soc Sci Med 1999, 49. [CrossRef]
- Pawaskar, M.; Burgess, C.; Pillsbury, M.; Wisløff, T.; Flem, E. Clinical and Economic Impact of Universal Varicella Vaccination in Norway: A Modeling Study. PLoS One 2021, 16. [CrossRef]
- Hussey, H.; Abdullahi, L.; Collins, J.; Muloiwa, R.; Hussey, G.; Kagina, B. Varicella Zoster Virus-Associated Morbidity and Mortality in Africa - A Systematic Review. BMC Infect Dis 2017, 17. [CrossRef]
- Ali, H.A.; Hartner, A.M.; Echeverria-Londono, S.; Roth, J.; Li, X.; Abbas, K.; Portnoy, A.; Vynnycky, E.; Woodruff, K.; Ferguson, N.M.; et al. Vaccine Equity in Low and Middle Income Countries: A Systematic Review and Meta-Analysis. Int J Equity Health 2022, 21. [CrossRef]
- Moon, J.Y.; Seo, J.; Lee, J.; Park, D. Assessment of Attenuation of Varicella-Zoster Virus Vaccines Based on Genomic Comparison. J Med Virol 2023, 95. [CrossRef]
- Argaw, T.; Cohen, J.I.; Klutch, M.; Lekstrom, K.; Yoshikawa, T.; Asano, Y.; Krause, P.R. Nucleotide Sequences That Distinguish Oka Vaccine from Parental Oka and Other Varicella-Zoster Virus Isolates. Journal of Infectious Diseases 2000, 181. [CrossRef]
- Gomi, Y.; Sunamachi, H.; Mori, Y.; Nagaike, K.; Takahashi, M.; Yamanishi, K. Comparison of the Complete DNA Sequences of the Oka Varicella Vaccine and Its Parental Virus. J Virol 2002, 76. [CrossRef]
- Kim, J.; Jung, G.; Kim, Y.; Ji, G.; Kim, H.; Wang, W.; Park, H.; Park, S.; Kim, G.; Kwon, S.; et al. Sequencing and Characterization of Varicella-Zoster Virus Vaccine Strain SuduVax. Virol J 2011, 8. [CrossRef]
- Depledge, D.P.; Yamanishi, K.; Gomi, Y.; Gershon, A.A.; Breuer, J. Deep Sequencing of Distinct Preparations of the Live Attenuated Varicella-Zoster Virus Vaccine Reveals a Conserved Core of Attenuating Single-Nucleotide Polymorphisms. J Virol 2016, 90. [CrossRef]
- Hao, B.; Chen, Z.; Zeng, G.; Huang, L.; Luan, C.; Xie, Z.; Chen, J.; Bao, M.; Tian, X.; Xu, B.; et al. Efficacy, Safety and Immunogenicity of Live Attenuated Varicella Vaccine in Healthy Children in China: Double-Blind, Randomized, Placebo-Controlled Clinical Trial. Clinical Microbiology and Infection 2019, 25. [CrossRef]
- Hwang KK; Chun BH; Park HS; Park SY; Kim KY; Moon HM Marker Test for Attenuation of Varicella-Zoster Viruses Isolated in Korea. J of Kor Soc of Virology 1992, 22, 105–109.
- Park SY; Hwang KK; Choi MK; Ryu YW; Paik SB; Kim KH Propagation of Varicella-Zoster Virus Isolated in Korea. J kor Soc Virol 1991, 21, 1–9.
- WHO Prequalified Vaccines. Available online: URL (https://extranet.who.int/prequal/vaccines/prequalified-vaccines).
- Hayakawa, Y.; Torigoe, S.; Shiraki, K.; Yamanishi, K.; Takahashi, M. Biologic and Biophysical Markers of a Live Varicella Vaccine Strain (Oka): Identification of Clinical Isolates from Vaccine Recipients. Journal of Infectious Diseases 1984, 149. [CrossRef]
- Schmid, D.S. Varicella-Zoster Virus Vaccine: Molecular Genetics. Curr Top Microbiol Immunol 2010, 342. [CrossRef]
- Loparev, V.N.; Rubtcova, E.; Seward, J.F.; Levin, M.J.; Schmid, D.S. DNA Sequence Variability in Isolates Recovered from Patients with Postvaccination Rash or Herpes Zoster Caused by Oka Varicella Vaccine. Journal of Infectious Diseases 2007, 195. [CrossRef]
- Jeon, J.S.; Won, Y.H.; Kim, I.K.; Ahn, J.H.; Shin, O.S.; Kim, J.H.; Lee, C.H. Analysis of Single Nucleotide Polymorphism among Varicella-Zoster Virus and Identification of Vaccine-Specific Sites. Virology 2016, 496. [CrossRef]
- Ko EB.; Park HI.; Park HM.; Shin SK. Periodic Benefit Risk Evaluation Report for: Varicella Vaccine-GCC Inj._ver4.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2022.
- Information approved by the Ministry of Food and Drug Safety of the Republic of Korea for BARYCELA. Available online: URL (https://nedrug.mfds.go.kr/searchDrug).
- Park JW.; Lee JS.; Park HM.; Shin SK. Periodic Benefit Risk Evaluation Report for: BARYCELA Inj._ver5.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2023.
- BARYCELA package insert. Available online: URL (https://extranet.who.int/prequal/sites/default/files/vwa_ vaccine/pq_381_varicella__GC_PI-2023.pdf).
- Information approved by the Ministry of Food and Drug Safety of the Republic of Korea for SKYvaricella. Available online: URL (https://nedrug.mfds.go.kr/searchDrug).
- VARIVAX package insert. Available online: URL (https://www.fda.gov/media/76008/download?Attachment).
- VARILRIX product monograph. Available online: URL (https://ca.gsk.com/Media/6263/Varilrix.Pdf).
- SKYvaricella package insert. Available online: URL (https://extranet.who.int/prequal/sites/default/files/vwa_ vaccine/pq_347_varicella_1dose_SK_PI-2019.pdf).
- Information approved by the Ministry of Food and Drug Safety of the Republic of Korea for Varicella Vaccine-GCC. Available online: URL (https://nedrug.mfds.go.kr/searchDrug).
- Varicella Vaccine-GCC package insert. Available online: URL (https://www.globalgreencross.com/eng/index.do).
- Drug Regulatory Authority of Pakistan. (T.F. Complex, Mauve Area, G-9/4 Islamabad, Pakistan). Minutes of 329th Meeting of Registration Board Held on 6th to 8th June, 2023_Pakistan;. Unpublished work, 2023.
- Park HI.; Kim JA.; Park HM.; Shin SK. Periodic Benefit Risk Evaluation Report for: BARYCELA Inj._ver6.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2024.
- Expanded Program of Immunization Vaccine Prices for year 2023. Available online: URL (https://www.paho.org /en/documents/paho-revolving-fund-vaccine-prices-2023).
- Expanded Program of Immunization Vaccine Prices for year 2022. Available online: URL (https://www.paho.org /en/documents/paho-revolving-fund-vaccine-prices-2022).
- Expanded Program of Immunization Vaccine Prices for year 2021. Available online: URL (https://www.paho.org /en/documents/paho-revolving-fund-vaccine-prices-2021).
- Sohn, Y.M.; Park, C.Y.; Hwang, K.K.; Woo, G.J.; Park, S.Y. Safety and Immunogenicity of Live Attenuated Varicella Virus Vaccine (MAV/06 Strain). Kor Pediatr Soc 1994, 37, 1405–1413.
- Immunogenicity and Safety of Live Attenuated Vaccine(MAV/06srtain) on Healthy Children and Immunocompromised Children. Available online: URL (https://www.e-cep.org/journal/ view.php?number=1995380604).
- Gonzales, MA.L.M.; Gonzaga, E.M. Final Report_Immunogenicity and Safety of a New Live Attenuated Varicella Vaccine (MAV/06 Strain) among Healthy Filipino Children of Ages 9 Months to 17 Years; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2001.
- Lim DS.; Clinical Study Report_MG1111_P1 _ver1.0; 2015; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2015.
- Dose-escalation Phase 1 to Evaluate the Safety and Efficacy of MG1111 in Healthy Adults. Available online: URL (https://clinicaltrials.gov/study/NCT02367638?cond=mg1111&rank=2).
- A Study of MG1111 in Healthy Children. Available online: URL (https://clinicaltrials.gov/study/ NCT03375502?cond=mg1111&rank=1).
- Kang JH.; Clinical Study Report_MG1111_P2,3_Stage1,2; 2018; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2018.
- Choi, U.Y.; Kim, K.H.; Lee, J.; Eun, B.W.; Kim, D.H.; Ma, S.H.; Kim, C.S.; Lapphra, K.; Tangsathapornpong, A.; Kosalaraksa, P.; et al. Immunogenicity and Safety Profiles of a New MAV/06 Strain Varicella Vaccine in Healthy Children: A Multinational, Multicenter, Randomized, Double-Blinded, Active-Controlled Phase III Study. Vaccine 2021, 39. [CrossRef]
- An Open-label, Bridging Study of BARYCELA Inj. in Healthy Vietnamese Children Aged Between 12 Months to 12 Years. Available online: URL (https://clinicaltrials.gov/study/NCT05664152?cond=mg1111&rank=3).
- Le Minh Giang.; Clinical Study Report_Bridging Study for Marketing Authorization in Vietnam_ver2.0; 2024; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2024.
- ICH guideline E2C (R2) on periodic benefit-risk evaluation report (PBRER). Available online: URL (https://www. https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/international-conference-harmonisation-technical-requirements-registration-pharmaceuticals-human-use-guideline-e2c-r2-periodic-benefit-risk-evaluation-report-step-5_en.pdf).
- Yoo DJ.; Kim JA.; Ko EB.; Park HM.; Kim C. Periodic Benefit Risk Evaluation Report for: BARYCELA Inj._ver1.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2020.
- Ko EB.; Lee MJ.; Park HM.; Kim C. Periodic Benefit Risk Evaluation Report for: BARYCELA Inj._ver2.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2021.
- Jeong JE.; Lee JS.; Park HM.; Shin SK. Periodic Benefit Risk Evaluation Report for: BARYCELA Inj._ver3.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2021.
- Jeong JE.; Kim JA.; Park HM.; Shin SK. Periodic Benefit Risk Evaluation Report for: BARYCELA Inj._ver4.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2022.
- Beth S.; Lee SY.; Kim SH.; Lee CH. Periodic Safety Update Report for: Varicella Vaccine-GCC Inj._ver1.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2014.
- Lee JS.; Park HM. Periodic Safety Update Report for: Varicella Vaccine-GCC Inj._ver2.1; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2018.
- Yoo DJ.; Kim YA.; Park HM.; Kim C. Periodic Benefit Risk Evaluation Report for: Varicella Vaccine-GCC Inj._ver3.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2019.
- Yoshikawa, T.; Ando, Y.; Nakagawa, T.; Gomi, Y. Safety Profile of the Varicella Vaccine (Oka Vaccine Strain) Based on Reported Cases from 2005 to 2015 in Japan. Vaccine 2016, 34. [CrossRef]
- Galea, S.A.; Sweet, A.; Beninger, P.; Steinberg, S.P.; LaRussa, P.S.; Gershon, A.A.; Sharrar, R.G. The Safety Profile of Varicella Vaccine: A 10-Year Review. In Proceedings of the Journal of Infectious Diseases; 2008; Vol. 197.
- Sharrar, R.G.; LaRussa, P.; Galea, S.A.; Steinberg, S.P.; Sweet, A.R.; Keatley, R.M.; Wells, M.E.; Stephenson, W.P.; Gershon, A.A. The Postmarketing Safety Profile of Varicella Vaccine. Vaccine 2000, 19. [CrossRef]
- Kang, H.M.; Kim, G.; Choe, Y.J. Safety of Interchanging the Live Attenuated MAV/06 Strain and OKA Strain Varicella Vaccines in Children. Vaccines (Basel) 2023, 11. [CrossRef]
- Mahler, V.; Junker, A.C. Anaphylaxis to Additives in Vaccines. Allergo J Int 2022, 31.
- Kim, S.H.; Lee, H.J.; Park, S.E.; Oh, S.H.; Lee, S.Y.; Choi, E.H. Seroprevalence Rate after One Dose of Varicella Vaccine in Infants. Journal of Infection 2010, 61. [CrossRef]
- Gershon, A.A. The Immunological Basis for Immunization Series : Module 10: Varicella-Zoster Virus; Immunization, Vaccines and Biologicals, WHO: 20 Avenue Appia, 1211 Geneva 27, Switzerland, 2008; ISBN 9789241596770.
- Gonzaga, E.M. Final Report_A 5-Year Follow-up Immunogenicity Study For a Live Attenuated Varicella Vaccine (MAV/06 Strain) Among Healthy Filipino Children Immunized at Ages 9 Months to 17 Years from May 2000 to April 2001_ver1.0; GC Biopharma, Yongin-si, Gyeonggi-do, Republic of Korea. Unpublished Report, 2006.
- Choi, U.Y.; Huh, D.H.; Kim, J.H.; Kang, J.H. Seropositivity of Varicella Zoster Virus in Vaccinated Korean Children and MAV Vaccine Group. Hum Vaccin Immunother 2016, 12. [CrossRef]
- Michalik, D.E.; Steinberg, S.P.; LaRussa, P.S.; Edwards, K.M.; Wright, P.F.; Arvin, A.M.; Gans, H.A.; Gershon, A.A. Primary Vaccine Failure after 1 Dose of Varicella Vaccine in Healthy Children. Journal of Infectious Diseases 2008, 197. [CrossRef]
- Shin, D.; Shin, Y.; Kim, E.; Nam, H.; Nan, H.; Lee, J. Immunological Characteristics of MAV/06 Strain of Varicella-Zoster Virus Vaccine in an Animal Model. BMC Immunol 2022, 23. [CrossRef]
- Quinlivan, M.; Hawrami, K.; Barrett-Muir, W.; Aaby, P.; Arvin, A.; Chow, V.T.; John, T.J.; Matondo, P.; Peiris, M.; Poulsen, A.; et al. The Molecular Epidemiology of Varicella-Zoster Virus: Evidence for Geographic Segregation. Journal of Infectious Diseases 2002, 186. [CrossRef]
- Sauerbrei, A.; Stefanski, J.; Gruhn, B.; Wutzler, P. Immune Response of Varicella Vaccinees to Different Varicella-Zoster Virus Genotypes. Vaccine 2011, 29. [CrossRef]
- Hwang, J.Y.; Kim, Y.; Lee, K.M.; Shin, O.S.; Gim, J.A.; Shin, Y.; Park, H. Cross-Reactive Humoral Immunity of Clade 2 Oka and MAV/06 Strain-Based Varicella Vaccines against Different Clades of Varicella–Zoster Virus. Hum Vaccin Immunother 2023, 19. [CrossRef]
- Choi, J.K.; Park, S.H.; Park, S.; Choi, S.M.; Kim, S.H.; Lee, D.G.; Yoo, J.H.; Choi, J.H.; Kang, J.H. Trends in Varicella and Herpes Zoster Epidemiology before and after the Implementation of Universal One-Dose Varicella Vaccination over One Decade in South Korea, 2003–2015. Hum Vaccin Immunother 2019, 15. [CrossRef]
- Jung, J.; Ko, Y.J.; Kim, Y.E.; Huh, K.; Park, B.J.; Yoon, S.J. Epidemiological Impact of the Korean National Immunization Program on Varicella Incidence. J Korean Med Sci 2019, 34. [CrossRef]
- Choi, B.K.; Shin, J.H.; Lee, J.E.; Koh, S.B. Letter to the Editor: Effectiveness of the Varicella Vaccine in Korea: Unresolved Issues. J Korean Med Sci 2021, 36. [CrossRef]
- Cho, H.; Sun, E.; Jeon, S.; Ann, S.; Choi, B. Trends in the Incidence of Varicella Cases with Complications among Korean Children during 2010-2020 after the Universal One-Dose Varicella Vaccination Program. In Proceedings of the 38th International Conference for Pharmacoepidemiology, GC Bioharma, Copenhagen, Denmark, 2022; 1016.
- Choi EH. Effectivenss of Varicella Immunization in Korea; 2017; J Korean Med Sci 2021, published.
- Hong, K.; Sohn, S.; Choe, Y.J.; Rhie, K.; Lee, J.K.; Han, M.S.; Chun, B.C.; Choi, E.H. Waning Effectiveness of One-Dose Universal Varicella Vaccination in South Korea, 2011–2018: A Propensity Score Matched National Population Cohort. J Korean Med Sci 2021, 36. [CrossRef]
- Zhu, S.; Zeng, F.; Xia, L.; He, H.; Zhang, J. Incidence Rate of Breakthrough Varicella Observed in Healthy Children after 1 or 2 Doses of Varicella Vaccine: Results from a Meta-Analysis. Am J Infect Control 2018, 46. [CrossRef]
- Clements, D.A.; Moreira, S.P.; Coplan, P.M.; Bland, C.L.; Walter, E.B. Postlicensure Study of Varicella Vaccine Effectiveness in a Day-Care Setting. Pediatric Infectious Disease Journal 1999, 18. [CrossRef]
- Black, S.; Ray, P.; Shinefield, H.; Saddier, P.; Nikas, A. Lack of Association between Age at Varicella Vaccination and Risk of Breakthrough Varicella, within the Northern California Kaiser Permanente Medical Care Program. In Proceedings of the Journal of Infectious Diseases; 2008; Vol. 197.
- Choi, B.K.; Cho, H.; Shin, Y.; Lee, E.K. Letter to the Editor: Effectiveness of the Varicella Vaccine Among Korean Children: Suggestions for Future Research. J Korean Med Sci 2022, 37. [CrossRef]
Figure 1.
Phylogenetic tree showing five major varicella-zoster virus (VZV) clades include Oka & MAV/06 [5,31,34].
| Strain | Trade Name | Manufacturer | Country | WHO prequalification |
|---|---|---|---|---|
| Oka/Biken | OKAVAX | Biken | Japan | - |
| Oka/Merck | VARIVAX | MSD | USA | Yes |
| Oka/RIT | VARILRIX | GSK | Belgium | - |
| Oka | VARI-L | Changchun Keygen Biological Products | China | - |
| Oka | Varicella Vaccine, Live | Sinovac | China | Yes |
| Oka/SK | SKYVaricella | SK Bioscience | S.Korea | Yes |
| MAV/06 | Varicella Vaccine-GCC inj. (Suduvax) | GC Biopharma Corp. | S.Korea | - |
| MAV/06 | BARYCELA | GC Biopharma Corp. | S.Korea | Yes |
Table 2.
Isolation of Varicella-Zoster Virus from vesicle fluid of varicella patients [38].
Table 2.
Isolation of Varicella-Zoster Virus from vesicle fluid of varicella patients [38].
| Isolate | Clinical Symptom | Ages(months)/Sex |
|---|---|---|
| MAV 1/1 | Varicella | 22/Male |
| MAV/2 | Varicella | 16/Male |
| MAV/3 | Varicella | 20/Male |
| MAV/4 | Varicella | 45/Female |
| MAV/5 | Varicella | 28/Female |
| MAV/6 | Varicella | 33/Male |
| MAV/7 | Varicella | 23/Male |
1 MAV (MogAm Virus).
Table 3.
Number of passage levels in the MAV/06 strain for attenuation [37].
Table 3.
Number of passage levels in the MAV/06 strain for attenuation [37].
| Cell | Passage Number | Remark |
|---|---|---|
| HEL1 | 11 | LuMa2 cell |
| GEL3 | 13 | - |
| HEL | 8 | LuMa cell |
| HEL | 4 | MRC-54 cell |
| HEL | 24 | LuMa cell |
1 HEL (Human Embryonic Lung diploid cell), 2LuMa (normal human embryonic Lung diploid MogAm), 3 GEL (Guinea-pig Embryonic Lung diploid cell), 4 MRC-5 (Medical Research Council cell strain 5).
Table 6.
Varicella vaccine prices disclosed on PAHO (US$ per dose) [56–58.]
| Strain | 2021 | 2022 | 2023 | Average |
|---|---|---|---|---|
| Oka | 16.93 | 16.19 | 16.93 | 16.68 |
| MAV/06 | 13.80 | 12.50 | 13.80 | 13.37 |
Table 7.
Safety information of MAV/06 vaccines confirmed through clinical trials.
| Clinical trial (year) | Cohort | Number of subjects by cohort | Country |
|---|---|---|---|
| 1994* [59] | 300 PFU1 500 PFU 1,000 PFU 1,500 PFU 2,000 PFU |
6 children 7 children 19 adults, 13 children 6 children 11 adults |
S.Korea |
| 1995* [60] | Healthy children Immunocompromised children |
177 children 22 children (6 leukemia, 10 solid tumors, 6 nephrotic syndromes) |
S.Korea |
| 2001* [61] | 9-12 months 1-12 years 13-17 years |
102 children 172 children 101 children |
Philippines |
| 2015** [62,63] | 2,000 PFU 8,000 PFU 25,000 PFU |
10 adults 10 adults 10 adults |
S.Korea |
| 2017** [64,65] | 2,000 PFU 8,000 PFU 25,000 PFU |
75 children 75 children 76 children |
Thailand |
| 2018** [64,65,66] | MG11112 | 258 children | S.Korea/Thailand |
| 2024** [67,68] | 12-24 months 2-12 years |
124 children 126 children |
Vietnam |
1PFU: Plaque Forming Unit, 2MG1111: project code of BARYCELA, * Varicella Vaccine-GCC inj., **BARYCELA inj.
Table 9.
Comparison of the incidence of reported adverse events between MAV/06 and Oka vaccines during post-approval use periods [44,46,55,70,71,72,73,74,75,76,77,78,79].
| Strain | Oka | MAV/06 | |||
|---|---|---|---|---|---|
| Vaccine | VARIVAX1 | VARIVAX2 | OKAVAX3 | Varicella Vaccine-GCC inj. | BARYCELA inj. |
| Total number of vials distributed | 16,100,000 | 55,700,000 | 9,467,000 | 29,224,770 | 528,360 |
| Number of reported adverse events | 7,963 | 16,683 | 351 | 120 | 3 |
| Estimated incidence rates (/100,000 doses) | 49.46 | 29.95 | 3.71 | 0.41 | 0.57 |
Table 10.
Immunogenicity of MAV/06 vaccines in clinical trials.
| Clinical trial (year) | Cohort | SCR1 No, of subjects achieved/ No. of total subjects (%) | FAMA GMT2 (95% CI) |
|---|---|---|---|
| 1994* [59] | 300 PFU3 500 PFU 1,000 PFU 1,500 PFU |
6/6(100) 7/7(100) 13/13(100) 6/6(100) |
72.0 116.2 83.3 160.9 |
| 1995* [60] | Healthy children Immunocompromised children |
161/161(100) 18/18(100) |
173.7 111.4 |
| 2001* [61] | 9-12 months 1-12 years 13-17 years |
100/100(100) 99/100(99) 99/99(100) |
741.7 227.6 500.9 |
| 2006* [74,84] | 9-12 months 1-12 years 13-17 years |
49/49(100) 62/62(100) 51/52(98.1) |
20.6 (15.3, 25.8) 26.4 (19.2, 33.7) 27.0 (18.7, 35.3) |
| 2015** [62,63] | 2,000 PFU 8,000 PFU 25,000 PFU |
- - - |
78.8 (44.3, 140.0) 90.5 (53.0, 154.6) 68.6 (41.9, 112.3) |
| 2017** [64,65] | 2,000 PFU 8,000 PFU 25,000 PFU |
43/43(100) 41/41(100) 57/57(100) |
85.5 (63.7, 114.9) 109.9 (88.6, 136,5) 65.6 (51.4, 83.6) |
| 2018** [64,65,66] | BARYCELA VARIVAX |
234/239(97.9) 237/239(99.2) |
74.2 (65.0, 84.8) 112.7 (99.1, 128.1) |
| 2024** [67,68] | 12-24 months 2-12 years |
- - |
69.9 (63.7, 76.7)*** 126.5 (95.0, 168.5)*** |
1SCR: Sero Conversion Rate (≥1:4), 2GMT: Geometric Mean Titer, 3PFU: Plaque Forming Unit, * Varicella Vaccine-GCC inj., **BARYCELA inj., ***gpELISA GMT.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



