
Submitted:
29 April 2024
Posted:
30 April 2024
You are already at the latest version
Abstract
Pressure Ulcers (PU) are a debilitating and often painful condition. They are localized lesions on the skin and/or underlying tissues and are common in the elderly, immobile people, diabetics and vascular disease or malnutrition, as well as in those requiring intensive or palliative care. Prevention and treatment of PU involve strategies to optimize hydration, circulation and nutrition. Nutrition plays a key role in pressure ulcer care because wounds require macronutrients and micronutrients to heal. Reports relating to the effectiveness of "Complementary Enzyme Therapy" also in the vulnological field led us to this study, the aim of which was to test the activity of a biodynamic nutritional supplement (Citozym®), characterized by a marked antioxidant activity, administered topically and/or systemically, in patients suffering from PU. The treatment showed a marked reduction in bedsores and in many cases their complete healing. Furthermore, it was possible to observe a lower incidence of side effects compared to conventional therapies. The results obtained, confirmed by various tests, and recognized by the scientific community, allow us to conclude that treatment with Citozym® could represent a new and effective strategy for the treatment of PU.
Keywords:
Pressure Ulcers
; biodynamic therapy
; nutritional supplement
Introduction
Despite increasing attention over the past 20 years, the prevalence of PU has remained essentially unchanged, while costs associated with treatment continue to increase [1]. Doctors and healthcare professionals can play a significant role in preventing PU by becoming aware of at-risk populations and implementing appropriate preventative strategies. Furthermore, doctors and healthcare Professionals should be able to recognize early changes that occur before skin injury and correctly identify and classify PU to avoid delays in providing appropriate care. In individuals with normal mobility, and mental state, prolonged pressure elicits a feedback response that requires a change in body position; however, when the feedback response is absent or impaired, sustained pressure ultimately leads to tissue ischemia, lesions and necrosis [2]. The pathophysiology, risk factors, epidemiology, social and economic burdens, and clinical presentation of PU are current topics in research projects [3]. Wound healing is a multicellular physiological process of programmed and reproducible cooperation of the cells involved. It is one of the most complex biological processes that occur during human life. Wounds are the result of tissue breakdown with loss of normal anatomical structure and consecutive loss of normal tissue function [4]. The wound healing process generates tissue remaking and reconstitution, as well as restoration of the tensile strength of damaged tissue. This begins within seconds of injury with homeostasis, followed by phases of inflammation, proliferation and tissue remodeling, to restore tissue integrity and the barrier function of the skin [5]. From a metabolic point of view, all these phases require an energy and protein substrate, sufficient to ensure good wound healing. Ulcers with a poor healing prognosis include leg ulcers, such as venous, arterial, or mixed ulcers, PU, and neuropathic foot/leg ulcers [6]. PU, which affects a large number of individuals representative of the world’s population, represents a serious and growing threat with a negative economic impact. This pathology also leads to personal problems, both social and psychological. Inflicted wounds are difficult to heal and lead to repeated recurrences. At-risk patients require a thorough evaluation that includes a detailed medical history, skin examination, and evaluation of the patient’s support systems. Risk assessment tools have been developed to identify those at greatest risk and reduce the incidence of PU, with the idea that those at risk may benefit from more rigorous interventions [7]. There is a lack of agreement on predictive risk factors which has led to the proliferation of various tools that include different variables of interest. Nutritional intake plays a key role in the repair of damaged tissues [8]. Recently the patient’s diet has also been addressed as an adjuvant in the treatment of these dermatological pathologies [9]. In particular, it has been suggested that an adequate intake of macronutrients and micronutrients may play an important role in the healing process of ulcers. The proposed double-blind study presents data relating to the prospective, randomized and, controlled evaluation of the effects of a biodynamic nutritional supplement, particularly useful in this group of difficult-to-heal lesions, also for its ability to counteract enzymatic imbalances and for its documented antiseptic activities. Altered enzymatic machinery is a substantial biochemical feature of epidermal cell metabolism that changes the metabolic profile from oxidative phosphorylation to amplified glycolysis as well as increased lactate production under hypoxic conditions. Overexpression of several enzymes in PU has been indicated as a cause of delayed wound healing [10]. Therefore, being able to reprogram the function of these enzymes could represent an attractive avenue for the treatment of bedsores. Citozym® is a product that belongs to a new generation of nutritional supplements, defined as “Biodynamic”, which can provide functional foods obtained from specific enzymatic conversions and therefore “nourish” the cells directly and quickly [11]. This experimental investigation aimed to use this nutritional supplement to verify its capacity as an authentic therapeutic target for the therapy of PU. The positive results obtained suggest that further investigations into biodynamic enzymology should focus on exploring the molecular mechanisms of various pathologies.
2. Materials and Methods
2.1. Patients
All participants selected from the hospital outpatient Department of the Investigative Dermatology Institute, (IDI) Russia (Dr. A. Shevchenko), received verbal and written information about the study and informed consent was obtained by everyone before the start of the experiment. Initially, 90 patients were included in the sample and selected, but 10 were withdrawn from the group due to personal characteristics and pathologies unrelated to the intervention. The study was conducted as a prospective; randomized, controlled, double-blind investigation to observe clinical parameters and patient experiences during therapy aimed at healing PU, comparing conventional treatment (see attachment), with Citozym® therapy. The researcher responsible for patient selection reviewed all patients and made the final decision on whether the patient met the inclusion criteria or not. Exclusion criteria from the study included: patients with severe general diseases, patients who required local anesthesia for treatment, and patients who smoked. For the randomization procedure, an urn containing 80 numbers corresponding to the enrolled patients was prepared. The four sets of numbers were divided as follows: “1-20 control”, “21 to 41 topical treatments”, “42 to 62 systemic treatments” and “63 to 83 combined topical+ systemic treatments”.
2.2. Fundamental Characteristics of the Sample Examined
To eliminate data influenced by events unrelated to the experimental protocol, the study required 3 months of preliminary observation. The implementation of the project and the observation of the results took 10 months (analysis and selection of patients; 4 months—staging of ulcers -1 month, experimentation—2 months; data analysis and healing potential -2 months, preparation of the project final report -1 month). All included subjects received a copy of the “Free and Informed Consent Form” and signed it after having been guided and informed on the procedures to be adopted during the study. All patients provided permission for this study, including the use of images (for recording metric data). All these supporting documents have been validated by an official ethics committee (UTVI Protocol 352-2022). The experimentation is part of the research project “Activation of a collaboration and scientific research program between the Department of Biology (M.S.M.F.N.) and Citozeatec s.r.l. (Food Supplements and Cellular Pathologies) RM 070622”.The selected patients underwent an initial evaluation and monitored several times a week for 3 consecutive months. The observations, photographs and measurements were carried out in the first two months of treatment. The third month allowed us to verify the permanence of the healing to avoid relapses of the pathology. The wounds of all patients were documented by measurements and photographs, according to a sequence of wound bed preparation and dressings. The sample was composed of 80 men, more than half were 70 years old or older (57.5%—n =46). Nearly a third (33.7%—n = 27) had a diagnosis of diabetes mellitus and more than half (63%—n= 50) had hypertension. 10% (n = 8) were alcoholics and 5% (n = 4) were smokers. Initial ulcer characteristics, lesion duration, lesion area, Pressure Ulcer Scale for Healing score (PUSH Tool 3) [12], and quality of life (QL) [13] varied considerably. The lesions ranged from small to large and lasted for months showing various healing conditions. The primary objective was to calculate the percent rate of wound contraction using the re-epithelialization index (RI) over a two-month period. Secondary objectives were healing rate assessed by the wound closure (millimeters per week of growth at wound edges), nutritional and laboratory parameters and anthropometric measurements (data not shown). Body weight and height were measured using a portable electronic scale. Since obesity contributes to immobility and subsequent pressure on skin surfaces, knowledge of the relationship between obesity and development of pressure ulcers in intensive care patients will provide better understanding of which patients are at high risk for pressure ulcers and allow more efficient prevention [14]. Nutritional intake was assessed before and after Citozym® treatments. Body mass index (BMI) was calculated by dividing weight by height squared, expressed in kg/m2. All these parametric assessments were classified according to the guidelines suggested by the CONSORT-Outcomes 2022 [15]. These types of evaluations made it possible to study a homogeneous group of volunteers.
2.3. Metric Measurements and Photographic Monitoring
The principal medical researchers measured and photographed all wounds weekly, always with the same photographic equipment (Huawei P30 Leica Guad Camera). A sterile ruler, a 125 MEB-6/150 vernier caliper (eezee.com.sg-Singapore 139951), and image processing software for surface area and perimeter calculations were used to collect and record wound measurement data. Many patients did not consent to the disclosure of images taken of wounds being treated. Photographic images taken of patients were considered private data and treated as such. The classification of the observed ulcers was carried out in accordance with international standards which include: Stage I: Intact skin with localized, non-blanchable erythema over a bony prominence. The area may be painful, hard or soft, and warmer or colder than the surrounding tissue. Darkly pigmented skin may not show visible whitening; however the color of the Stage I ulcer will appear different from the color of the surrounding skin and indicates that the patient is at risk of further tissue damage if the pressure is not relieved. Stage II: Partial thickness wound presenting as a shallow, open ulcer with a red/pink wound bed. It may also present as an intact or open/ruptured blister filled with serum or sero-sanguineous fluid. Fragments of scaly skin may be present which do not hide the depth of tissue loss. Stage III: full thickness wound. Subcutaneous tissue may be visible but bones, tendons and muscles are not exposed. Scaling or eschar may be present, but this does not mask the depth of tissue loss. Stage IV: Full-thickness wound with exposed bone, tendon, or muscle. Scaling or slough may be present in some parts of the wound bed, but this does not hide the depth of tissue loss.
2.4. Percent Rate of Wound Contraction and Calculation of Linear Growth (Re-Epithelialization)
In addition to the metric data, it was also possible to calculate the percentage rate of contraction and the linear growth of the wound edges. The percentage rate of wound contraction can be used to monitor an ulcer over time. Weekly comparisons of wound area reduction rates can be converted into wound healing trajectory curves, particularly in the first 2-4 weeks of treatment. Wounds that show a rate of area reduction of 10-15% per week predict healing; those showing 30–50% area reduction in the first 2–4 weeks have high healing potential.
2.5. Citozym® Treatment Protocol
The administration of the nutritional supplement Citozym® (Citozeatec Italia-FDA registration 12932524008 Pin no. bfJ3h263) was carried out according to a scheme considered useful for testing both the direct action of the product on the wound (topical effect) and the action exerted by oral administration (systemic), or simultaneously (topical plus systemic) (see attached therapeutic protocol).The possibility of being able to test the general improvement of the patient, following the treatment adopted, is obtained through investigation methods accepted by the scientific community [15]. Before treating a skin lesion it is important to observe and evaluate it. For this assessment to be as objective and reproducible as possible, it is advisable to use internationally recognized classification tools. The staging of a lesion is important in order to use a common language that allows the different operators to be able to understand the lesion and together decide on therapeutic strategies by optimizing resources. There are different anatomical classifications, the most used are the EPUAP, 1997 (European Pressure Ulcer Advisory Panel, Guidelines on the treatment of PU) and the NPUAP (National Pressure Ulcer Advisory Panel) [16,17]. The anatomical classification allows the depth of the wound to be identified, describing its progressive worsening. In these terms it takes on an important prognostic meaning: the first two phases lead to an intact return while in the subsequent ones, since the musculoskeletal system is involved, sequelae are expected which require a greater use of resources. The individual variables considered were: Evaluation of wound surface reduction after treatment; re-epithelialization, the PUSH score and Quality of Life (QV). ok
2.6. Re-Epithelialization
Keratinocytes, the main cellular component of the epidermis, are not only important for maintaining the barrier but also for its restoration in case of injury through a process known as epithelialization [18]. Epithelialization is defined as a process of covering the denuded epithelial surface [19]. The cellular and molecular processes involved in the initiation, maintenance, and completion of epithelialization are essential for successful wound closure. Many research efforts have focused on understanding these processes in both acute and chronic wounds. Calorie and protein requirements in a healing wound are higher than average for non-wounded tissue. A poor diet causes a nutrient deficit, protein degradation and, slowed tissue recovery. To close the defect in the epidermis, keratinocytes at the wound edge must first loosen their adhesion to each other and to the basal lamina and must develop the flexibility necessary to support migration onto the newly deposited matrix. This process is modulated sequentially starting from the disassembly of cell-cell and cell-substrate contacts maintained through desmosomes and hemidesmosomes, respectively. Epithelialization plays a crucial role in wound healing, as it is impossible to achieve wound closure if it fails. This phase of wound repair involves the initiation, proliferation, migration, and differentiation of keratinocytes at injury sites, along with the repair and reorganization of compromised dermal structures. The size, severity, and location of a wound will determine how quickly complete healing can be achieved. Generally, larger wounds take longer to heal than smaller wounds.
2.7. The Push Tool Test 3
This is a dynamic monitoring system in which the pressure ulcer is observed and evaluated, classifies the lesion taking into account the surface, exudates and the type of tissue involved [12]. Record the sub-scores for each of these characteristics; then the sub-scores are added to obtain the total score. Therefore, the total score measured over a period of time indicates whether the lesion has improved or not. The scale collects quantitative and qualitative characteristics useful for describing the lesion in the most objective way possible and being able to compare the results of treatment over time. The length-by-width data is obtained from the estimate of the surface area in cm2. Evaluation of exudates is performed after dressing and before applying any topical agent to the wound. The estimate of exudates (drainage) is classified as absent, light, moderate, or strong. Tissue type refers to the types of tissue present in the wound bed; necrotic with a score 4, squamous with a score 3, if the wound is clean with granulation tissue with a score 2, epithelial tissue with a score 1, while with a score 0 if the lesion is closed.
2.8. Quality of Life (QL)
The World Health Organization Quality of Life (WHOQOL) defines “Quality of Life” as an individual’s perception of their position in life in the context of the culture and value systems in which they live and concerning their goals, expectations, standards and concerns [20]. In research, QL measurements can help determine whether new clinical treatments are effective enough in improving a patient’s life. This form of measurement is sometimes called “patient-reported outcome. Researchers need to establish the effects that a new treatment has on a subject. There is currently a broad consensus on some fundamental aspects that any tool aimed at quantifying it must necessarily consider: physical functioning and well-being; psychological functioning and well-being (mainly emotional and cognitive aspects); social functioning and well-being; physical symptoms (both those relating to the specific pathology and those resulting from any treatments for that pathology). Various parameters allow the evaluation of QL in patients treated with therapies that have the aim of improving the state of health and potentially improving the patient’s QL. The QL parameters assessed are pain and discomfort, energy and effort, daily life, sleep and rest, mobility and working capacity. The values for each parameter are: 0 = very bad; 1 = tolerable; 2 = moderate; 3 = good and 4 = excellent.
2.9. Statistical Analysis
The data obtained in this study were described as means, standard deviations (SD), and standard errors or frequencies and percentages. The comparison between therapies and groups took into account the analysis of variance (ANOVA) model with two sources of variation. The comparison of two evaluation moments with respect to the quantitative variables was carried out with the Student’s t-test for paired samples. Regarding wound-related variables, considering the possibility of patients with more than one ulcer, each patient was considered as a cluster. For the comparisons of interest, the estimation model for relationships with quantitative variables and the estimation model for relationships with clusters were used for dichotomous variables. P values <0.05 indicated statistical significance. Data were analyzed with Stata/SEv.14.1 statistical software (Stata Corp LP, USA).
3. Results and Discussion
3.1. Re-Epithelialization
The decrease in the area of PU indicates the formation of epithelium covering the underlying connective tissue. Re-epithelialization describes the reemergence of a wound with new epithelium. The cellular and molecular processes involved in the initiation, maintenance, and completion of epithelialization are essential for successful wound closure. It is therefore a precious prognostic sign for the reduction of the ulcer [21]. The controlled treatment of PU was carried out according to the last update of the WHS guidelines [22]. In the panel of Figure 1, it is evident that ulcers treated for 60 days with the topical or the systemic procedure compared to controls showed about 75% reduction in wound area. The combined topical and systemic treatment reduced the wound area by 95%. The control treatment reduced the ulcer area by 25% in 60 days. The results presented in Figure 1, relating to the combined, topical and systemic treatments, highlight the regenerative action of Citozym® with regard to the formation of new epithelium, which is expressed by promoting wound closure by stimulating the growth of new tissues. The data also seem to be confirmed by direct observation of the wound on the patient (Figure 2) where wound closure is highlighted more completely in the combined treatment, compared to the topical treatment alone.
In diabetic patients, hyperglycemia impairs neutrophil function and reduces host defenses [23]. The result leads to a tendency to bacterial infections that slow down and reduce wound healing. Patients with one or more of these risk factors accelerate the development of wounds that may be slow to heal and predispose to secondary infections. Without treatment, this type of wound can become infected. This can lead to extreme outcomes such as sepsis. The arrest of the tissue repair process of a lesion, linked to an increase in bacterial load, determines the appearance of first and local signs of inflammation which can be considered as the beginning of an evolving infection. The application of Citozym® according to the protocol reported in the “Methods Section” has made it possible, in many cases, to control and reduce the increase in germs, allowing the tissue repair process to resume in a almost sterile environment.
Figure 3 and Figure 4 show respectively the reduction of a diabetic ulcer treated with the Citozym® protocol (topical + systemic), kept perfectly sterile and in the closing phase and the complete closure of a forearm ulcer completely covered by ‘epidermis.
Figure 5 highlights the 75% reduction of an ulcer in the lower leg treated with combined therapy for approximately 60 days. The almost complete re-epithelialization of the wound. is evident.
Figure 6 shows the 85% reduction in pressure ulcer area in the foot treated with the combined therapy for approximately 60 days.
3.2. PUSH Score
Before treating a skin lesion it is important to observe and evaluate it. For this assessment to be as objective and reproducible as possible, it is advisable to use internationally recognized classification tools. When staging a lesion it is important to use a common language that allows the different operators to understand the lesion and decide on therapeutic strategies together, optimizing resources. The anatomical classification allows the depth of the wound to be identified, describing its progressive worsening. In these terms it takes on an important prognostic meaning: the first two phases lead to an intact return while in the subsequent ones, since the musculoskeletal system is involved, sequelae are expected which require a greater use of resources. In addition to assessing the depth of the lesion, staging allows a prognostic measure in terms of time/healing. A stage III-IV lesion will be repaired in a very long time and with a much higher commitment of human and economic resources compared to a stage I-II lesion on which a timely and precise intervention can lead to resolution in a few days. The Push Tool 3 is a dynamic monitoring system in which wound pressure is observed and measured. Classifies the lesion taking into account the surface, exudates and, the type of tissue involved. The length-by-width data is obtained from the estimate of the surface area in cm2. Evaluation of exudates is performed after dressing and before applying any topical agent to the wound. Record a sub-score for each of these characteristics; then the sub-scores are added to obtain the total score. Therefore, the total score measured over a period of time indicates whether the lesion has improved or not. Figure 7 highlights the results obtained with the systemic, topical and combined topical plus systemic treatment respectively. It appears clear that the closure of the wound following the re-epithelialization of the affected area occurred within the times foreseen by the trial, more rapidly in the combined treatment.
From Figure 7 it can be observed that the Total score of the PUSH test in control patients is reduced by 6.52% in 60 days, while in the systemic treatment in the same period, it is reduced by 36.6%. Topical treatment reduced the total PUSH score by 26.83%. The combined treatment was more effective, bringing the total PUSH score to values of 15%.
3.3. Quality of Life (QL)
QL is an important endpoint in medical and healthcare research, and QL research involves a variety of patient groups and different research projects. Various parameters allow the evaluation of QL in patients treated with therapies that have the aim of improving the state of health and potentially improving the patient’s QL. The QL parameters evaluated are pain and discomfort, energy and effort, daily life, sleep and rest, mobility and work capacity. QL is an important concept in the field of health and medicine. QL is a complex concept that is interpreted and defined differently within and across disciplines, including the fields of health and medicine. Pressure ulcers have a significant effect on patients’ QL. For the present study, a questionnaire was proposed to all participants. The majority of subjects enrolled for the treatment reported psychosocial disorders, such as depression (60.5%), negative perception of body image (67.8%), difficulties in relationships with peers (81.9%), physical and mental tiredness (75.7%), weakness during leisure activities (65.2%) and reduced physical activity (69.5%). A further questionnaire highlighted the presence of physical effects resulting from recurrent infections of the ulcers or injuries to the lower limbs, which required hospitalization. Exuding ulcers was particularly problematic in its management because patients had to use additional materials, a process that is time-consuming and requires significant financial costs. Therefore, the physical, psychological, economic and social consequences experienced by these patients significantly reduced their QL.
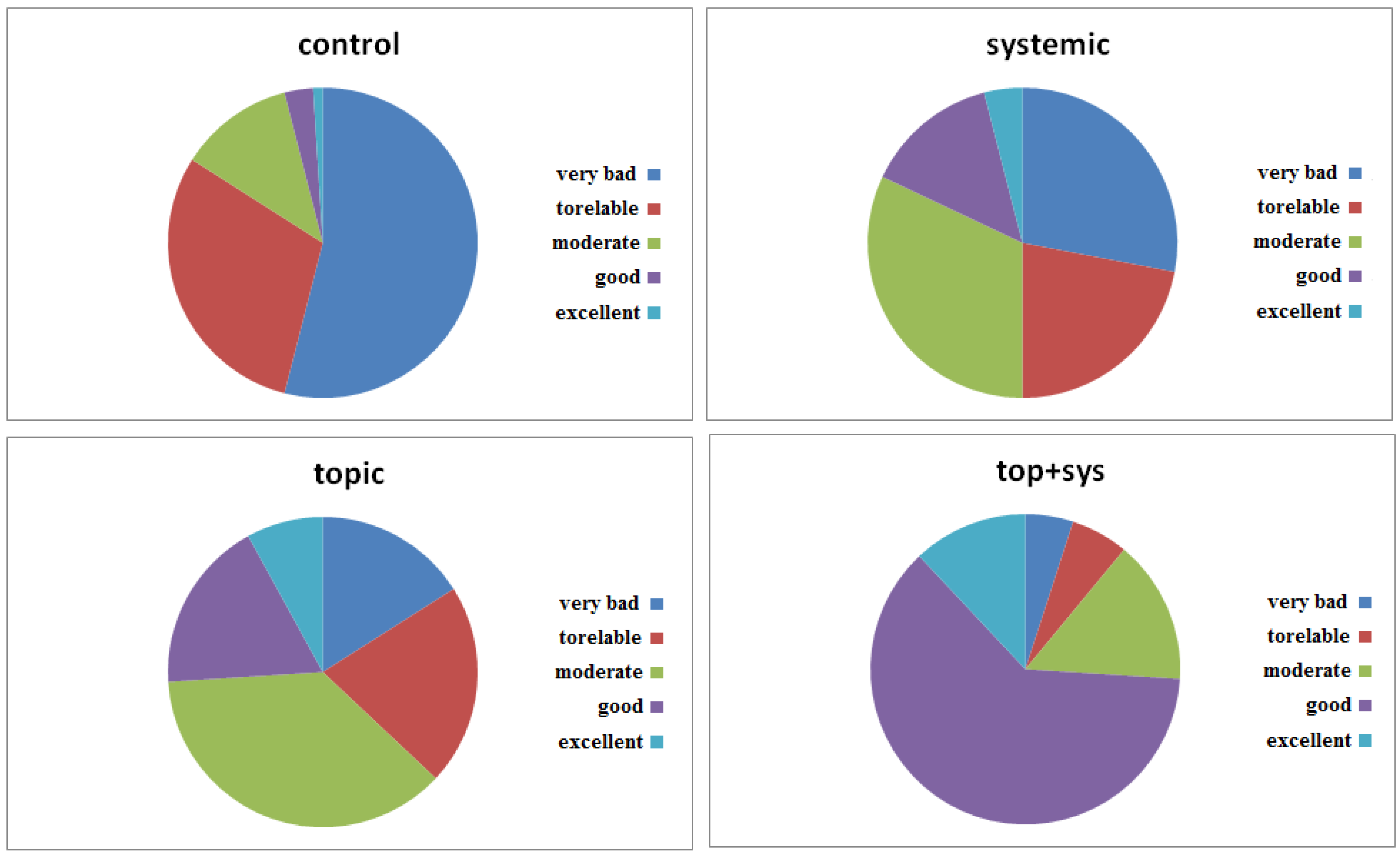
From Figure 8, representing the QL trend in patients treated with the experimental protocol mentioned, it can be seen that the PU treatment, to which the patients were subjected not only showed improvement and healing of the wound but also an increase in the QL of the patient. The test proposed to patients included several questions, aimed at highlighting five fundamental points of the QL scale. In particular, the evaluation of the patient’s general condition, both physical and mental, was required. As can be seen from Figure 8, the percentages of positive outcomes were very high. In particular, in patients treated with combined therapy (topical+systemic), the “Good” level of satisfaction was 62%, followed by “excellent” at 12% and “moderate” at 15%. The “tolerable” and “very bad” percentages reach 6% and 5% respectively. In conclusion, it is possible to deduce that the proposed treatment is widely appreciated by a large number of patients. These data when compared with the results of conventional therapy highlight the effectiveness of the application of the biodynamic supplement Citozym in the therapy of pressure ulcers. The conventional treatment highlighted a low level of QL with “very bad” percentages of 54% and “torelable” percentages of 30%. Furthermore, from Figure 8 it is also possible to deduce that the systemic treatment alone was less effective than the topical treatment.
Conclusions
This study demonstrated that within 60 days it is entirely possible to stimulate the healing process of pressure ulcer wounds, which are difficult to heal, using a biodynamic food supplement (Citozym®) applied topically and systemically. All of these elements in combination have been found directly linked to the wound healing process, even in diabetic patients. Regarding the clinical and laboratory parameters evaluated during the study, no significant differences were found in blood pressure, glycemia, renal function (creatinine), albumin and pre-albumin levels (data not shown). To our knowledge, this is the first published study highlighting the utility of this specific blend of enzyme-based bioactive nutrients in wound healing. Furthermore, our sample size was quite large and the inclusion or exclusion criteria did not significantly affect the generalizability of the data. The strength of our study is that specific micronutrients from Citozym® were administered in the context of adequate nutritional care and patients received similar nutritional support to promote new tissue formation. Likewise, the rate of patients who were generally unresponsive to wound care was similar among the 4 treatment groups and was less than 2%. Regarding the generalizability of the data, less stringent exclusion criteria were allowed due to the age of patients with a certain degree of comorbidity, although some restrictions were unavoidable. Our findings apply to long-term care residents and patients receiving home care services and, given the aging population, could have a large effect on public health. Other settings, such as intensive care units, were not considered. In our study, adherence to therapy was high, because it was integrated with daily care, distributed throughout the day and, not left to the patient’s initiative and ability to undertake. In conclusion, in malnourished patients with PU receiving nutritional support and guideline-based wound care management, the use of an active biodynamic and enzymatic dietary supplement provides additional wound-healing benefits. The issue of cost-effectiveness should be addressed to support its use. Nutritional intervention should be considered an integral part of pressure ulcer care. The authors thank all healthcare workers and providers for their assistance in recruitment, clinical support, and data collection.
Author Contributions
Conceptualization; Ferorelli P., Beninati S. and Borromeo I. Methodology: Ferorelli P. and Beninati S. Resources; Shevchenko A., Antonelli F. Writing-original draft; Ferorelli P. and Beninati S. –Review & editing; Ferorelli P., Radaelli M., Mischiati C. and Feriotto G.
Funding
This research was funded by A.R.S.S. grant number AF324CY-2021.
Institutional Review Board Statement
Research project “Scientific Research program between the Dept. of Biology and Citozeatec s.r.l.” food Supplement and cellular Pathologies RM 070622.
Informed Consent Statement
All participants/patients provided informed consent for the publication of their anonymized case details.
Conflicts of Interest
None.
References
- Klugarová J, Pokorná A, Hussain S, Vrbová T, Slezáková S, Búřilová P, Saibertová S, Dolanová D, Klugar M. Economic evaluations of interventions for the prevention and treatment of PU: an umbrella review protocol. JBI Evid Synth. 2022, 20(2):633-639.
- Hill JE, Edney S, Hamer O, Williams A, Harris C. Interventions for the treatment and prevention of PU.Br J Community Nurs. 2022 ;27(Sup6):S28-S36.
- Lyu Y, Huang YL, Li ZY, Lin F. Interventions and strategies to prevent medical device-related pressure injury in adult patients: A systematic review. J Clin Nurs. 2023;32(19-20):6863-6878.
- Mervis JS, Phillips TJ. Pressure Ulcers: Pathophysiology, epidemiology, risk factors, and presentation. J Am Acad Dermatol. 2019;81(4):881-890.
- Headlam J, Illsley A. Pressure Ulcers: an overview.Br J Hosp Med (London). 2020:2;81(12):1-9.
- Rajkumar J, Chandan N, Lio P, Shi V. The Skin Barrier and Moisturization: Function, Disruption, and Mechanisms of Repair. Pharmacol Physiol. 2023;36(4):174-185.
- Jaul E. Assessment and management of PU in the elderly: current strategies. Drugs Aging. 2010;27(4):311-325.
- Palmieri B, Vadalà M, Laurino C. Nutrition in wound healing: investigation of the molecular mechanisms, a narrative review. J Wound Care. 2019 ;28(10):683-693.
- Brunner S, Mayer H, Qin H, Breidert M, Dietrich M, Müller Staub M Interventions to optimise nutrition in older people in hospitals and long-term care: Umbrella review. Scand J Caring Sci. 2022;36(3):579-598.
- Kremer M, Burkemper N. Aging Skin and Wound Healing. Clin Geriatr Med. 2024;40(1):1-10.
- Ferorelli P., Antonelli F., Shevchenko A., Mischiati C., Doepp M., Lenzi S., Borromeo I. Feriotto G., Beninati S. Reduction in fatigue symptoms following the administration of nutritional supplements in patients with multiple sclerosis. Med Sci (Basel). 2021;9(3):52-58.
- Gardner SE, Hillis SL, Frantz RA.J A prospective study of the PUSH tool in diabetic foot ulcers. Wound Ostomy Continence Nurs. 2011;38(4):385-393.
- Haraldstad K, Wahl A, Andenæs R, Andersen JR, Andersen MH, Beisland E, et al.; A systematic review of quality of life research in medicine and health sciences. LIVSFORSK network. Qual Life Res. 2019;28(10):2641-2650.
- Hyun S., X. Li, Vermillion B., Newton C., Fall M., Kaewprag P., Moffatt-Bruce S., MD, and Lenz E.R. Body Mass Index and Pressure Ulcers: Improved Predictability of Pressure Ulcers in Intensive Care Patients. Am J Crit Care. 2014,23(6): 494–501.
- Butcher N.J, Monsour A., Mew E.J., et al. Guidelines for Reporting Outcomes in Trial Protocols: The CONSORT-Outcomes 2022 Extension. jama. 2022;328(22):2252-2264.
- Butcher NJ, Monsour A, Mew EJ, Chan AW, Moher D, Mayo-Wilson E, Terwee CB, et al.. Statement of the European Pressure Ulcer Advisory Panel--pressure ulcer classification: differentiation between PU and moisture lesions. JAMA. 2022;328(23):2345-2356.
- Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised National Pressure Ulcer Advisory Panel Pressure Injury Staging System: J Wound Ostomy Continence Nurs. 2016 Nov/Dec;43(6):585-597.
- Bártolo I, Reis RL, Marques AP, Cerqueira MT. Keratinocyte Growth Factor-Based Strategies for Wound Re-Epithelialization.Tissue Eng Part B Rev. 2022 Jun;28(3):665-676.
- Pastar I., Stojadinovic O., Yin, N.C. et al. Epithelialization in Wound Healing: A Comprehensive Review. 2014, 3(7):445-464.
- Felce D, Perry J. Quality of life:its definition and measurement. Res. Dev. Disa. 1995,16(1):51-57.
- Rodrigues M, Kosaric N, Bonham CA, Gurtner GC. Wound Healing: A Cellular Perspective. Physiol Rev. 2019;99(1):665-706.
- Gould L.J., Jenny Alderden J., Rummana Aslam R. et al. WHS guidelines for the treatment of pressure ulcers-2023 update. Wound Repair Regen. 2024. 32(1):6-33.
- Marhoffer W, Stein M, Mäser E, Federlin K. Reduced phagocytic capacity of circulating granulocytes in diabetes mellitus. Immun Infekt. 1992;20(1):10-2.
Figure 1.
Variation in wound contraction during the planned treatments. The reduction in wound area (cm2) indicates the speed of re-epithelialization of the wound. The measurement was conducted during the two months of treatment (see Methods section).
Figure 1.
Variation in wound contraction during the planned treatments. The reduction in wound area (cm2) indicates the speed of re-epithelialization of the wound. The measurement was conducted during the two months of treatment (see Methods section).
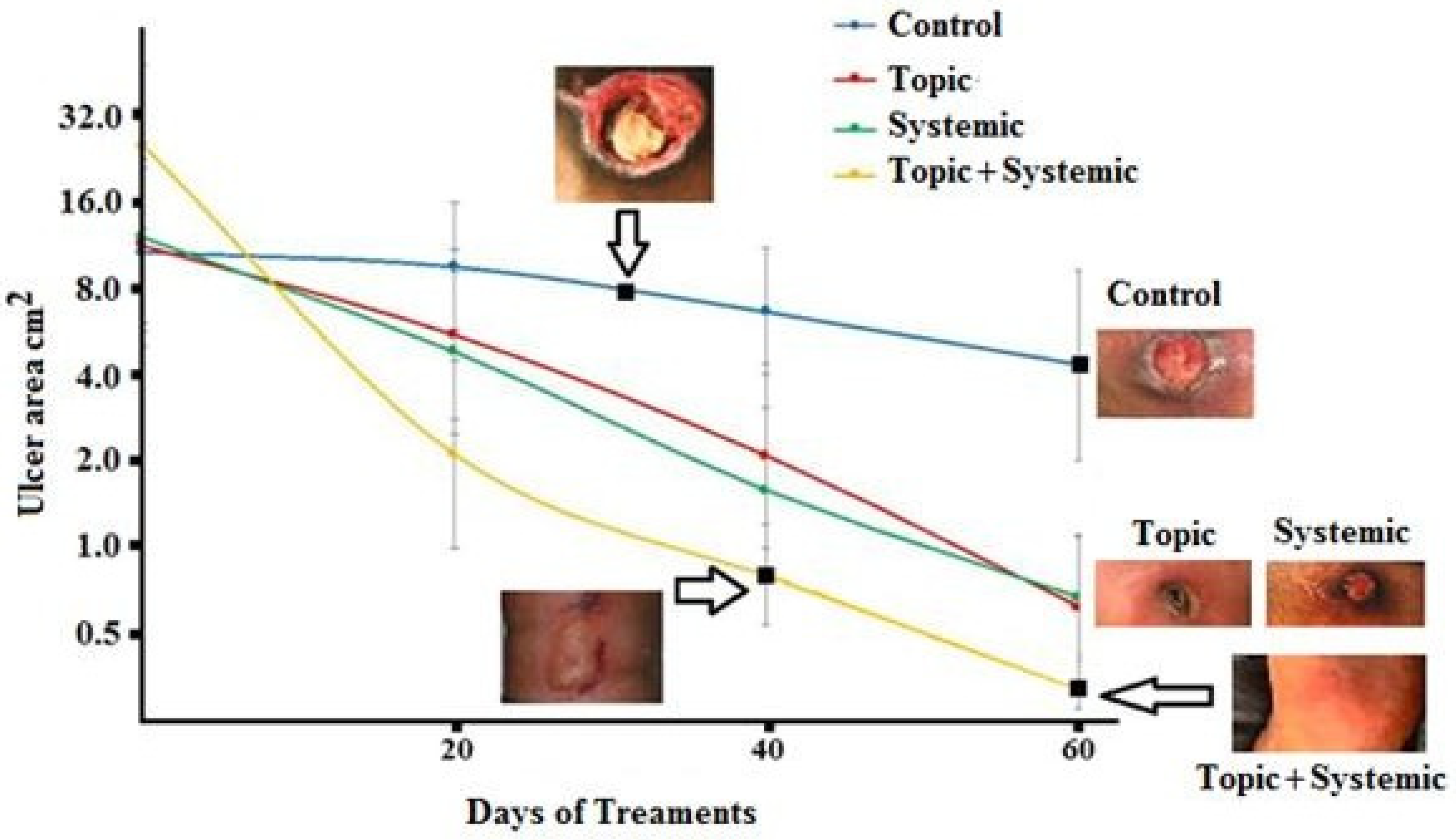
Figure 2.
Representative photographic images of the reduction of PU in a 77 years old patient treated with Citozym® using the topical/systemic combination (1,2,3,4) and in a 67 years old patient treated with topical therapy alone (5, 6,7, 8). Note the incomplete reduction of the wound in the exclusively topical treatment (photo 8) and the complete closure in the combined topical + systemic treatment (photo 4).
Figure 2.
Representative photographic images of the reduction of PU in a 77 years old patient treated with Citozym® using the topical/systemic combination (1,2,3,4) and in a 67 years old patient treated with topical therapy alone (5, 6,7, 8). Note the incomplete reduction of the wound in the exclusively topical treatment (photo 8) and the complete closure in the combined topical + systemic treatment (photo 4).
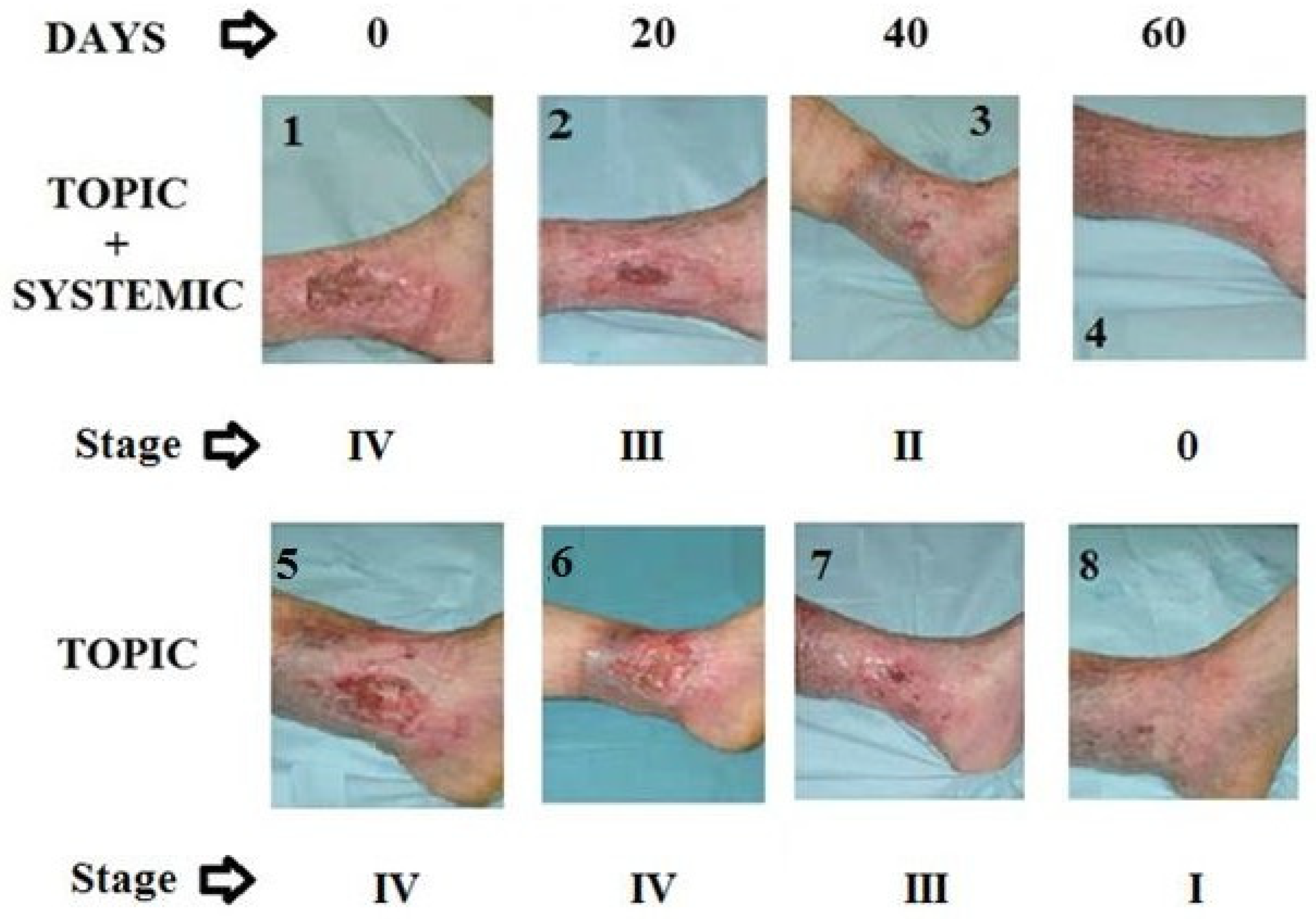
Figure 3.
Reduction of the ulcer area treated with combined therapy for 60 days. Representative photographic images of pressure ulcer reduction in a 57-years-old diabetic patient treated with Citozym® using the topical/systemic combination. Note the more complete partial but sterile closure in the combined topical + systemic treatment).
Figure 3.
Reduction of the ulcer area treated with combined therapy for 60 days. Representative photographic images of pressure ulcer reduction in a 57-years-old diabetic patient treated with Citozym® using the topical/systemic combination. Note the more complete partial but sterile closure in the combined topical + systemic treatment).

Figure 4.
Reduction of the ulcer area treated with combined therapy for 60 days. Representative photographic images of a forearm pressure ulcer reduction in a 45-years-old patient treated with Citozym® using the topical/systemic combination. Note complete re-epithelialization and closure by the combined treatments.
Figure 4.
Reduction of the ulcer area treated with combined therapy for 60 days. Representative photographic images of a forearm pressure ulcer reduction in a 45-years-old patient treated with Citozym® using the topical/systemic combination. Note complete re-epithelialization and closure by the combined treatments.

Figure 5.
Reduction in pressure ulcer area treated with combined therapy for approximately 60 days. Representative photographic images of the reduction of PU in a 77 year old diabetic patient treated with Citozym®, using the topical/systemic combination. The wound was reduced by approximately 75%.
Figure 5.
Reduction in pressure ulcer area treated with combined therapy for approximately 60 days. Representative photographic images of the reduction of PU in a 77 year old diabetic patient treated with Citozym®, using the topical/systemic combination. The wound was reduced by approximately 75%.
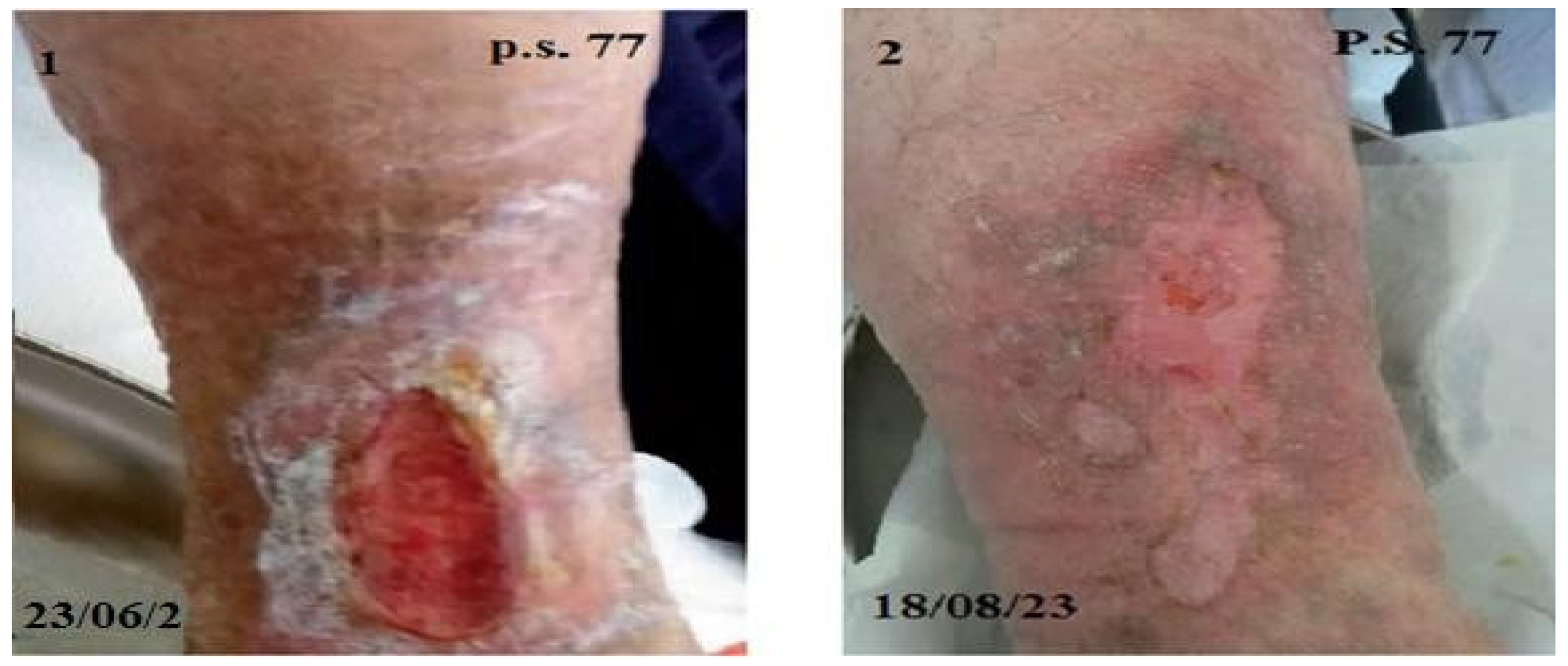
Figure 6.
Reduction in the area of PU in the foot treated with combined therapy for approximately 60 days. Representative photographic images of pressure ulcer reduction in a 78-year-old patient treated with Citozym®, using the topical/systemic combination. The wound was reduced by approximately 85%.
Figure 6.
Reduction in the area of PU in the foot treated with combined therapy for approximately 60 days. Representative photographic images of pressure ulcer reduction in a 78-year-old patient treated with Citozym®, using the topical/systemic combination. The wound was reduced by approximately 85%.

Figure 7.
PUSH test tool derived from the collection of parameters indicated on patients examined and treated as described in methods. The length-by-width data is obtained from the estimate of the surface area in cm2. Evaluation of exudates is performed after dressing and before applying any topical agent to the wound.
Figure 7.
PUSH test tool derived from the collection of parameters indicated on patients examined and treated as described in methods. The length-by-width data is obtained from the estimate of the surface area in cm2. Evaluation of exudates is performed after dressing and before applying any topical agent to the wound.
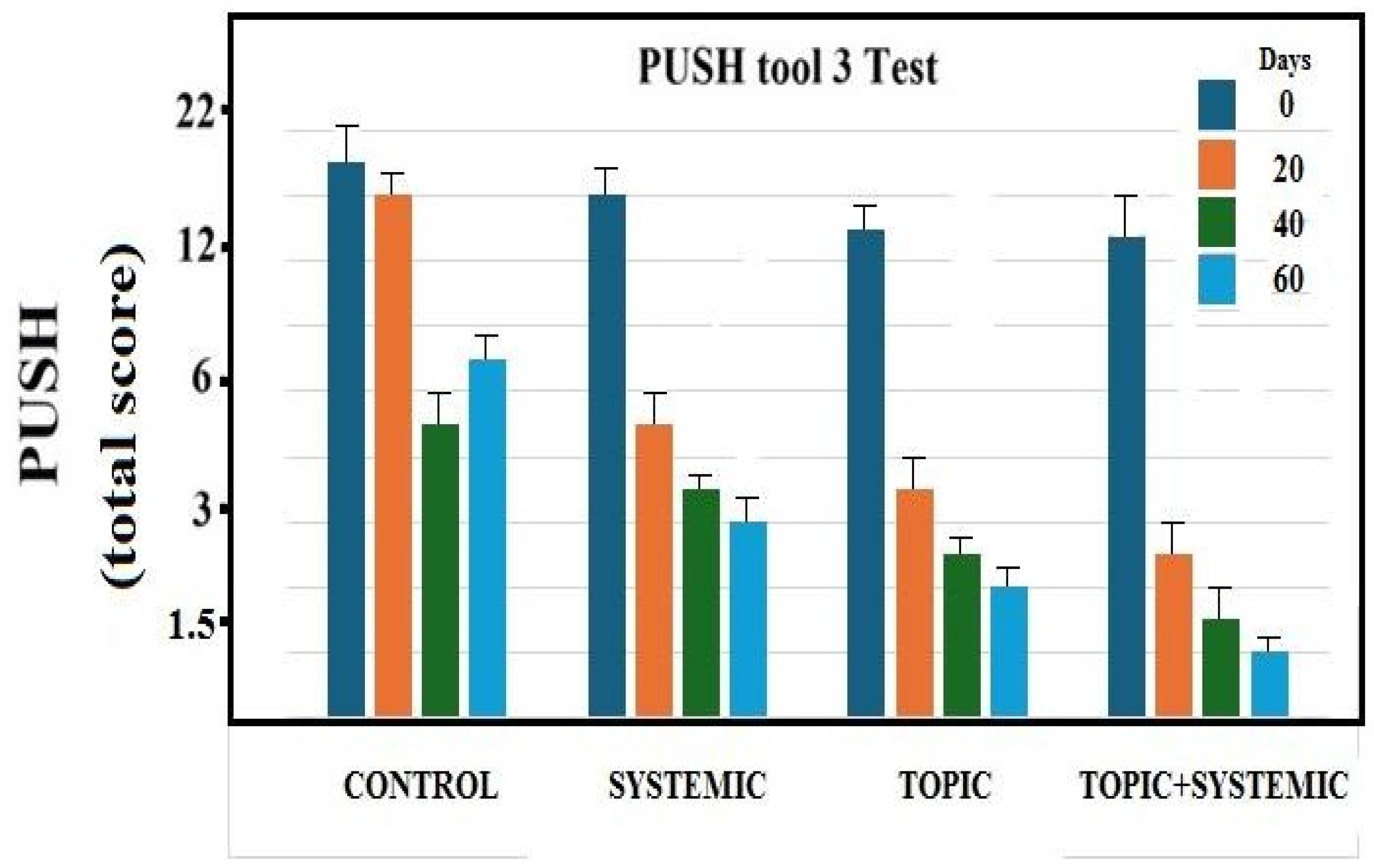
Figure 8.
QL tests obtained by collecting the experience of patients subjected to the therapies indicated in the Methods section. Each parameter in the graph corresponds to the percentage of survey responses after therapy. The answers, although subjective and linked to the patient’s sensitivity, can represent the intrinsic value of the well-being achieved by the patient following the therapy.
Figure 8.
QL tests obtained by collecting the experience of patients subjected to the therapies indicated in the Methods section. Each parameter in the graph corresponds to the percentage of survey responses after therapy. The answers, although subjective and linked to the patient’s sensitivity, can represent the intrinsic value of the well-being achieved by the patient following the therapy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



