
Submitted:
30 April 2024
Posted:
01 May 2024
You are already at the latest version
Abstract
Background: Tachycardia-induced cardiomyopathy (TIC) is caused by prolonged tachycardia leading to left ventricular dilatation and systolic dysfunction with heart failure. Although TIC is more common in adult, it is rare in early infant. Methods: Clinical testing was performed as part of medical evaluation and management. Next gene se-quencing (NGS) was performed for a patient with TIC. Literature review about TIC was con-ducted. Results: The case was a 5-month-old infant referred the hospital due to symptoms with heart failure at least lasting two months. Heart rate was 200 beats per minute, left ventricular ejection fraction fell below 14%, and electrocardiograms showed atrial flutter, suggesting TIC. After cardiover-sion, there was no recurrence of atrial flutter, and cardiac function was improved at 98 days after tachycardia arrest. There were no pathogenic variants identified according to NGS. Literature review identified 8 early infantile cases with TIC reported. However, there were no previous re-ports such as our case with longer duration of TIC. Conclusions: Improvement of cardiac function depends on the duration of TIC. TIC should be considered in all patients with a dilated cardiomyopathy of uncertain origin and who have tachycardias such as atrial flutter.
Keywords:
tachycardia-induced cardiomyopathy
; atrial flutter
; heart failure
1. Introduction
Tachycardia-induced cardiomyopathy (TIC) is a myocardial disorder that is caused by prolonged tachycardia, leading to left ventricular (LV) dilatation and systolic dysfunction with clinical symptoms and palpitation of heart failure (HF). The most common arrhythmias of TIC were ectopic atrial tachycardia (AT) (59%), permanent junctional reciprocating tachycardia (23%), and ventricular tachycardia (7%) [1]. There is a bias in the occurrence of TIC for each arrhythmia, ranging from 10% in patients with AT to 50% in patients with atrial fibrillation[2,3,4]. In adults, atrial fibrillation is the most important cause of TIC, as is AT and permanent junction reciprocal tachycardia in children[1,5].
TIC is totally or partially reversible after normalization of the heart rate (HR)[6,7,8]. In infants, the ventricular rate during tachycardia is much faster than normal and the initial symptoms cannot be verbalized, so cardiac failure symptoms often do not appear until several days after the onset of tachycardia [9]. In addition, compared with elderly TIC patients, newborns and infants with TIC tend to present with objective symptoms, such as dyspnea or poor body weight gain, not subjective symptoms, resulting in the prolongation of TIC.
However, TIC due to atrial flutter (AFL) is very rare, and there have been no cases of infants who are LGE negative but require considerable time to recover to normal cardiac function. Here, we report the case of an infant with TIC due to AFL, negative for LGE, who took a long time to recover to normal cardiac function and had no genetic background suggestive of cardiomyopathy. In addition, a literature review was conducted to determine the severity and prognosis of TIC in infants.
2. Materials and Methods
Written and informed consent was obtained. Clinical testing was performed as part of medical evaluation and management at Toyama University Hospital. This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the Research Ethics Committee of University of Toyama in Japan (IRB # I2017003). Written informed consent was obtained from his parents and his brother to participate, according to institutional guidelines.
Variant Screening
After obtaining informed consent from the parents of the patients, DNA was isolated from whole blood samples. Next-generation sequencing (NGS) of 203 cardiac disease-related genes associated with cardiomyopathy and channelopathies was performed using the Ion PGM System (Life Technologies, Carlsbad, CA, USA) [10]. Only variants present in genes other than the top 1% of genes with high variability and meeting acceptable quality scores (Phred-scaled genotype quality score, ≥20; read depth, ≥15; and Allele Fraction, ≥35) were included. Following quality control procedures, a total of 303,993 variants were obtained from the dataset. These variants were utilized for downstream analysis. Sanger sequencing was used to validate the results of NGS for all pathogenic variant candidates that passed these selection criteria. For this purpose, the nucleotide sequences of the amplified fragments were directly sequenced bidirectionally using the Big Dye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems, Foster City, CA), and sequence analysis was conducted using the ABI 3130xl automated sequencer (Applied Biosystems).
Data analysis and variant classification
We conducted primary, secondary, and tertiary analysis, including optimization of signal processing, base calling, sequence alignment, and variant analysis, using Torrent Suite and Ion Reporter Software 5.0 (Life Technologies). The allele frequencies of all detected variants were determined using the gnomAD (v2.1.1) database, which includes data from 1,208 Japanese individuals, and the Japanese Multi Omics Reference Panel (jMorp) ToMMo 54KJPN. Variants with a minor allele frequency of 0.005 or higher in the gnomAD and HGVD populations were excluded. Variant evaluation was manually performed based on detailed information obtained from ClinVar (https://www.ncbi.nlm.nih.gov/clinvar/) and the Human Gene Mutation Database (HGMD, http://www.hgmd.cf.ac.uk/ac/index.php). Variants were classified according to the American College of Medical Genetics and Genomics (ACMG) guidelines. To assess the pathogenicity of the remaining variants, we utilized five different in silico prediction algorithms: SIFT, Align GVGD, MutationTaster2, PolyPhen-2, and CADD. Variants predicted to be deleterious or pathogenic by at least four of the five in silico algorithms were considered to have a high likelihood of pathogenicity.
Literature review
We searched PubMed (from inception until March 31, 2024) for publications about tachycardia-induced cardiomyopathy and infant with search phrase (“tachycardia-induced cardiomyopathy” and “early infant” [Title/Abstract]). Our search strategy included gene names in the title or abstract. We also checked the bibliographies of all relevant studies and reviews identified. Clinical phenotypic data and genotypes were extracted.
3. Results
The patient was a 5-month-old boy. He was born at 39 weeks and 3 days by normal vaginal delivery with a birthweight of 3.144 g and an Apgar score of 8 points (1 min) and 9 points (5 min) after an uncomplicated pregnancy. He had no previous or family history of any type of illness. He had been losing weight for 2 months prior to admission (Figure 1). One month before hospital admission, he developed a wet cough, which did not improve with any medicine, and wheezing was also observed. Five days before hospital admission, the patient had poor feeding, and the local clinic noted tachycardia with a rate of 190 beats per minute (bpm). Steroids were prescribed for wheezing, but these symptoms were not improved. On the day of hospital admission, a chest X-ray showed an enlarged cardiothoracic ratio, and an echocardiography showed reduced left ventricular contraction. The patient was urgently transferred to our hospital.
His status He was drowsy, and had a pale face, his extremities were cold. On hospital admission, his vitals were as follows: pulse 200 beats per minute, blood pressure 50 mmHg at systole and 24 mmHg at diastole, percutaneous oxygen saturation (SpO2) 98 % at (room air), respiratory rate 40 breaths per minute, body temperature 36.3 degrees Celsius. A mild systolic murmur (Levine grade 1/6) was audible at the left sternal border. There were coarse crackles in the bilateral lung. A slightly hard liver was palpated 2 cm below the costal ribs. There was no edema in the extremities, but peripheral coldness was present, and capillary refilling time was more than 2 seconds. There is no family history of cardiomyopathy.
Laboratory test appeared high concentration level of NT-proBNP (8320 pg/mL) and troponin I (69.7 pg/mL). Other laboratory data and bloody gas data were shown as follows; Blood tests: WBC 12260 /μL (Neut% 73.0%), Hb 9.8 g/dL, PLT 453,000 /μL, AST 35 U/L, ALT 15 U/L, LD 311 U/L, CK 29 U/L, Nt-proBNP 8320 pg/mL, troponin I 69.7 pg/mL, CRP 0.17 mg/dL, TSH 2.26 mIU/L, freeT3 2.2 pg/mL, freeT4 1.4 ng/dL; H-FABP negative. Blood gas (venous blood, after intubation): pH 7.500, pCO2 31.2 mmHg, HCO3- 24.1 mmol/L, BE 1.6 mmol/L, Lac 1.0 mmol/L.
Cardiothoracic ratio was 0.63, and lung congestion was observed on chest X-ray (Figure 2a). On echocardiography, left ventricular wall motion was diffusely decreased (Figure 2b). The left ventricular ejection fraction (LVEF) was 13.7%, and The left ventricular end-diastolic diameter (LVDD) was 39.7 mm (+7.0 SD). On electrocardiogram (ECG), HR was 200 beats per minute, and sawtooth wave was observed (Figure 2c).
The patient was determined to be in shock and immediately admitted to the intensive care unit. He was intubated, ventilated, and started on dopamine (5 µg/kg/min), dobutamine (5 µg/kg/min), adrenaline (0.04 µg/kg/min), and olprinone (0.3 µg/kg/min) for acute heart failure treatment. However, the HR increased to more than 200 beats per minute, and hypotension persisted. There were Sawtooth waves were visible in twelve-lead ECG. We ruled out hereditary cardiomyopathy or secondary cardiomyopathy as the cause of acute heart failure. Structural heart abnormalities were not detected. Mental and motor developmental were normal. Metabolic or neuromuscular disease was denied. We suspected the TIC due to AFL as the most likely cause. Therefore, synchronized electrical cardioversion was performed (1 J/kg), and normal sinus rhythm was achieved (Figure 2d). Treatment for heart failure was continued with dopamine, dobutamine, adrenaline, and olprinone. The LVEF remained around 20 %, and the LVDD was 40.0 mm (+7.2 SD). Dopamine was discontinued on the 5th day, and the adrenaline was discontinued on the 11th day after admission. In the meantime, angiotensin-converting-enzyme inhibitors and carvedilol were added. He was We extubated on the 12th day. Tolvaptan was introduced for congestion on the 16th day. Dobutamine was terminated on the 21st day, and olprinone was on the 29th day, respectively. The serum level of Nt-proBNP was decreased at day 40 (8320 pg/mL at day 1 to 129 pg/mL at day 40), and AFL was not recurred. He was discharged from the hospital on the 41st day, and the LVEF was 40 % and the LVDD was 33.5 mm (+4.4 SD).
At 98 days after admission, the LVEF was improved at 59 %, and the LVDD was 30 mm (2.6 SD), respectively; at 161 days, the LVEF was 62 %, and the LVDD was 31 mm (2.4 SD). Cardiac catheterization at 10 months after admission (at the age of 15 months) showed LVEF of 75%, cardiac index (CI) 3.8 L/min/m2, and left ventricular end-diastolic pressure 6 mmHg.
A cardiac magnetic resonance image was performed one year after admission, and delayed contrast late gadolinium enhancement (LGE) was negative. In addition, genetic testing by NGS with cardiovascular diseases-panel performed to differentiate primary cardiomyopathy, not showing any known underling predisposition.
Now, he is 3 years old and stay healthy with normal mental and mortar development.
Literature Review
Our literature review identified 8 early infantile cases with TIC reported: 3 cases with permanent junctional reciprocating tachycardia and supraventricular tachycardia, and 2 cases with AFL. All cases had prominent tachycardia and reduced LV function; however, their outcomes were fairly good. Onset of TIC was not clear except for one case.
4. Discussion
The duration of prolonged tachycardia is vital for the recovery of cardiac function in patients with TIC. In our case, TIC may have manifested at least 2 months before admission because of body weight loss without any other reasons. The patient has the TIC due to AFL with a structurally normal heart and was only recognized when he was in shock. Normal sinus rhythm was achieved by once synchronized electrical cardioversion and there was no AFL recurrence. It took 98 days from treatments to recover for normal cardiac function.
In children with TIC, as in this case, the patient’s inability to recognize palpitations or verbalize symptoms often delays medical attention, and heart failure often develops. Considering that the patient had been losing weight for 2 months prior to this case, and that he was in heart failure at that point, the arrhythmia was likely recognized prior to that time.
AFL is an uncommon arrhythmia in newborns and infants. Due to the low incidence of AFL in this age, previous reports have been limited regarding the most efficacious therapy and expected prognosis. Texter et al. reported that infants with AFL who presented over three months were statistically more likely to develop congestive heart failure [18]. They also reported that 34% of patients had AFL complicated by congestive HF, recurrence, another arrhythmia, or AFL refractory to conversion to sinus rhythm [18]. Therefore, early recognition of the relationship of causative arrhythmia to TIC is necessary in providing treatment that improves symptoms and LV functional status [1].
The mechanism of cardiomyopathy development due to sustained tachycardia is unknown, but several theories have been proposed. Possible mechanisms for cardiac dysfunction with TIC include decreased blood flow to the myocardium [19], depletion of adenosine triphosphate (ATP) [20], and decreased beta-adrenergic receptors [20]. Sustained tachycardia causes abnormal cellular remodeling and decreases the number of microtubules within myocardial cells, which may contribute to myocardial contractile dysfunction [21]. Chronic tachycardia may also cause depletion of high-energy phosphate, which may lead to decreased intracellular sarcolemmal sodium/potassium ATPase activity and altered enzyme distribution affecting calcium handling [22]. Thus, infants and young children may function more rapidly because of reduced intracellular calcium stores. Pathophysiologically, the pathogenesis of TIC is based on remodeling processes such as neurohormonal overactivation, release of natriuretic peptides, secretion of inflammatory cytokines, ventricular and atrial dilation without hypertrophy against a background of extracellular matrix changes, reduced systolic and diastolic function, increased filling pressures [23,24]. There are also abnormalities in excitation-contraction coupling, intracellular mitochondrial apparatus, calcium processing, and energy production due to oxidative stress [25,26].
The evaluation of a patient with newly developed HF requires a high index of suspicion for underlying tachyarrhythmias. Systolic ventricular dysfunction is often the first manifestation of TIC seen on the echocardiogram, followed by prolonged dysfunction and then LV dilation [27]. The differential diagnosis of infants who present with acute HF and have normal hearts is often difficult because of multiple possible etiologies. They may be infectious, familial, metabolic, mitochondrial, toxic, inflammatory, or neuromuscular, but most cases are idiopathic. Genetic and metabolic etiologies such as storage disorders, mitochondrial disorders, and carnitine deficiency should also be considered in infants with newly developed cardiomyopathy. The diagnostic challenge in TIC is differentiating TIC from nonischemic dilated cardiomyopathy (DCM) [24]. DCM is defined as “myocardial disease characterized by LV or biventricular diastolic and systolic dysfunction despite the absence of pressure or volume overload or coronary artery disease sufficient to explain the dysfunction[28].” Despite the fact that it can be caused by a variety of etiologies and thus can have a variety of pathologic manifestations, DCM is the second most frequent HF phenotype after ischemic heart disease and is an indication for cardiac transplantation [29]. Patients with TIC have higher HR and lower LVEF at diagnosis, with more recovery of LVEF after HR normalization [30]. In contrast, patients with DCM tend to have a wider QRS complex, more frequent LGE, and more rehospitalizations during follow-up [31]. From a histopathologic and immunologic standpoint, TIC has a stronger myocardial expression of major histocompatibility complex class II molecules than nonischemic/nonvalvular DCM, CD68+ macrophage infiltration is particularly strong, a generally lower presence of T cells and macrophages, larger cardiomyocyte size, lower degree of myocardial fibrosis, and a more altered distribution of mitochondrial patterns [32]. In our case, genetic testing was performed to elucidate the background of HF whether TIC or DCM, and there was no obvious genetic background shown. TIC should be considered in the diagnosis of patients with a DCM of uncertain origin and who have tachycardias or AFL.
The duration of prolonged tachycardia is vital in the recovery of cardiac function with TIC. Because TIC is a reversible cause of cardiac dysfunction in children, early diagnosis and effective management are critical [33]. In animal models, cardiac output, atrial pressure, calcium uptake, and creatinine kinase function have been reported to normalize 2-4 weeks after cessation of tachycardia, but some changes, such as LV fibrosis or dilation, persist for several weeks despite removal of tachycardia and may cause delayed normalization of EF [34,35]. In our case, although it is difficult to determine when arrhythmias began, TIC may be started at least before two months before admission because of body weight loss without any other reasons. In a report of 50 cases of AFL under one year of age, 36 cases (72%) developed AFL within 48 hours of birth and 44 (88%) within two weeks of delivery [18]. For a group of children with cardiac dysfunction (LVEF < less than 50%) and left ventricular dilatation (LVDD z-score > 2.0) due to TIC, the median time to recovery from treatment takes 51 days for the normal LVEF and 71 days for the normal LVDD [1]. Previous studies have reported that recovery of left ventricular systolic function takes weeks to months and reverse remodeling months to years[1]. In adults, once HR is normalized by medical therapy, electrical cardioversion, or radiofrequency ablation, clinical and functional recovery of the heart is reported to be rapid, usually not exceeding 6 months [23,36,37]. In children, the median time to EF normalization was 1.5 months [38]. In other pediatric reports, the median time to recovery was 51 days for LVEF and 71 days for LVEDD; two patients (4%) underwent heart transplantation and one (1%) died [1]. Predictors of LV systolic function recovery by multivariate analysis were younger age, percentage of tachycardia standardized, use of mechanical circulatory support, and increased LVEF; for normalization of LV size, only lower baseline LVEDD was a predictor [1]. In our case, recovery of the normal LVEF took 98 days, and recovery of the normal LVDD took 163 days. Considering that most cases of pediatric AFL tend to develop during the neonatal period and cardiac function gradually improved in our case than that in previous cases, it is likely that our patient also had a long-standing AFL that might persist from the neonatal period. This is supported by the fact that our patient had severe cardiac dysfunction after a normal rhythm was achieved by cardioversion.
Patients with recovered TIC maintain a large LV volume and some degree of negative remodeling [23,39]. This may be related to persistence of interstitial fibrosis despite recovery of myocardial function [40]. LGE on cardiac MRI has proved to help assess myocardial fibrosis in several cardiomyopathies [41]. In patients with TIC, LGE may have a role in differentiating TIC from primary cardiomyopathy and in predicting improvement in left ventricular function. The prevalence of LGE in the TIC group is 16%, and interestingly, LGE is confined to the midmyocardium [30]. The presence of LGE in patients with TIC has a prognostic impact and can be used as a predictor of increased cardiac events [42]. The presence of LGE was an independent predictor of a lack of recovery of the LVEF in TIC patients (p=0.004) [30]. The presence of LGE was associated with lack of LVEF normalization at 6 months [43]. LGE was more frequent in the TIC group than in the DCM group. In multivariate analysis, the presence of LGE was an independent predictor of lack of LVEF recovery [30]. In our case, the HF recovery was longer than other reports, but we were confident that the HF would improve soon because the LGE was negative.
Sixty-nine percent of TCMP patients underwent defibrillation or ablation [31]. Treatment strategy, such as antiarrhythmic drug therapy or catheter ablation, had no significant effect on cardiomyopathy recovery. This suggests that the negative inotropic effects of antiarrhythmic drugs do not preclude myocardial recovery, as has been previously proposed [44]. In addition, in a previous report of 24 cases, five patients with recurrent tachycardia showed a rapid decrease in EF in adult patients [45], suggesting that prevention of recurrent arrhythmia is important in TIC in adult patient. In contrast, recurrence is rare in pediatric patients, after once AFL is cessation [18], meaning that prophylactic administration of antiarrhythmic drugs is not unnecessary. In our case, preventative medication was not administered, AFL has not been occurred for more than three years.
5. Conclusions
Improvement of cardiac function depends on the duration of TIC. Early recognition and intervention of TIC is necessary to provide infantile patients with better outcome, given the potential for recovery with appropriate treatment. TIC should be considered for a new diagnosis of LV dysfunction or HF when persistent tachycardia is present.
Author Contributions
TS and KH designed the study and drafted the manuscript. Data were extracted by TS, KT, ST, MO, HN, KI, and SO and independently verified by KH. The quality of the included studies was assessed by YT, YH, NN, and KH. All authors read, critically appraised, provided feedback, and approved the final manuscript.
Funding
Keiichi Hirono is supported by grants from The Ministry of Education, Culture, Sports, Science, and Technology in Japan (Grant-in-Aid for Scientific Research No. 22K07932).
Institutional Review Board Statement
This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the Research Ethics Committee of University of Toyama in Japan. Written informed consent was obtained from his parents and his brother to participate, according to institutional guidelines.
Informed Consent Statement
Written informed consent was obtained from his parents and his brother to publish for their personal or clinical details along with any identifying images, according to institutional guidelines.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Acknowledgments
The authors wish to acknowledge to Hitoshi Moriuchi, Haruna Hirai and Eriko Masuda for their expert technical assistance.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Moore, J.P.; Patel, P.A.; Shannon, K.M.; Albers, E.L.; Salerno, J.C.; Stein, M.A.; Stephenson, E.A.; Mohan, S.; Shah, M.J.; Asakai, H.; et al. Predictors of myocardial recovery in pediatric tachycardia-induced cardiomyopathy. Hear. Rhythm. 2014, 11, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Medi, C.; Kalman, J.M.; Haqqani, H.; Vohra, J.K.; Morton, J.B.; Sparks, P.B.; Kistler, P.M. Tachycardia-Mediated Cardiomyopathy Secondary to Focal Atrial Tachycardia: Long-Term Outcome After Catheter Ablation. Circ. 2009, 53, 1791–1797. [Google Scholar] [CrossRef] [PubMed]
- Ju, W.; Yang, B.; Li, M.; Zhang, F.; Chen, H.; Gu, K.; Yu, J.; Cao, K.; Chen, M. Tachycardiomyopathy Complicated by Focal Atrial Tachycardia: Incidence, Risk Factors, and Long-Term Outcome. J. Cardiovasc. Electrophysiol. 2014, 25, 953–957. [Google Scholar] [CrossRef] [PubMed]
- Ling, L.-H.; Kistler, P.M.; Kalman, J.M.; Schilling, R.J.; Hunter, R.J. Comorbidity of atrial fibrillation and heart failure. Nat. Rev. Cardiol. 2016, 13, 131–147. [Google Scholar] [CrossRef] [PubMed]
- Gopinathannair, R.; Etheridge, S.P.; Marchlinski, F.E.; Spinale, F.G.; Lakkireddy, D.; Olshansky, B. Arrhythmia-Induced Cardiomyopathies: Mechanisms, Recognition, and Management. J Am Coll Cardiol. 2015;66:1714-28.
- Walsh, R.; Thomson, K.L.; Ware, J.S.; Funke, B.H.; Woodley, J.; McGuire, K.J.; Mazzarotto, F.; Blair, E.; Seller, A.; Taylor, J.C.; et al. Reassessment of Mendelian gene pathogenicity using 7,855 cardiomyopathy cases and 60,706 reference samples. Genet. Med. 2017, 19, 192–203. [Google Scholar] [CrossRef]
- Gallagher, J.J. Tachycardia and cardiomyopathy: The chicken-egg dilemma revisited. Circ. 1985, 6, 1172–1173. [Google Scholar] [CrossRef]
- Raymond-Paquin, A.; Nattel, S.; Wakili, R.; Tadros, R. Mechanisms and Clinical Significance of Arrhythmia-Induced Cardiomyopathy. Can. J. Cardiol. 2018, 34, 1449–1460. [Google Scholar] [CrossRef]
- Mares, J.C.; Bar-Cohen, Y. Tachycardia-Induced Cardiomyopathy in a 1-Month-Old Infant. Case Rep. Pediatr. 2012, 2012, 1–4. [Google Scholar] [CrossRef]
- Isojima, T.; Kato, N.; Ito, Y.; Kanzaki, S.; Murata, M. Growth standard charts for Japanese children with mean and standard deviation (SD) values based on the year 2000 national survey. Clin. Pediatr. Endocrinol. 2016, 25, 71–76. [Google Scholar] [CrossRef]
- Van Hare, G.F.; Witherell, C.L.; Lesh, M.D. Follow-up of radiofrequency catheter ablation in children: results in 100 consecutive patients. J Am Coll Cardiol. 1994;23:1651-9.
- Sanchez, C.; Benito, F.; Moreno, F. Reversibility of tachycardia-induced cardiomyopathy after radiofrequency ablation of incessant supraventricular tachycardia in infants. Heart 1995, 74, 332–333. [Google Scholar] [CrossRef]
- Schulze, O.; Kammeraad, J.; Ramanna, H.; Sreeram, N. Catheter ablation for tachyarrhythmia-induced cardiomyopathy in infants. Int. J. Cardiol. 2000, 74, 99–100. [Google Scholar] [CrossRef] [PubMed]
- Felt, J.; Arora, R.; Sethuraman, U. Respiratory Distress in an Infant: An Uncommon Cause for a Common Complaint. J. Emerg. Med. 2016, 50, e57–e60. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, M.; Ruttan, T.K.; Kienstra, A.J.; Wilkinson, M. Making the Quick Diagnosis: A Case of Neonatal Shock. J. Emerg. Med. 2017, 52, e139–e144. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, M.; Tramma, D.; Thomaidis, K.; Papadopoulou-Legbelou, K. Tachycardia induced cardiomyopathy in an infant with atrial flutter: A challenging but reversible cause of heart failure. Pediatr. Neonatol. 2019, 60, 477–478. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, K.; Ferns, S.J. Epicardial Ablation of Persistent Junctional Reciprocating Tachycardia in an Infant With Tachycardia-Induced Cardiomyopathy. JACC: Case Rep. 2021, 3, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Texter, K.M.; Kertesz, N.J.; Friedman, R.A.; Fenrich, A.L. Atrial Flutter in Infants. Circ. 2006, 48, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Spinale, F.G.; Tanaka, R.; A Crawford, F.; Zile, M.R. Changes in myocardial blood flow during development of and recovery from tachycardia-induced cardiomyopathy. Circulation 1992, 85, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Moe, G.W.; Montgomery, C.; Howard, R.J.; A Grima, E.; Armstrong, P.W. Left ventricular myocardial blood flow, metabolism, and effects of treatment with enalapril: further insights into the mechanisms of canine experimental pacing-induced heart failure. . 1993, 121, 294–301. [Google Scholar]
- Horenstein, M.; Saarel, E.; Dick, M.; Karpawich, P. Reversible Symptomatic Dilated Cardiomyopathy in Older Children and Young Adolescents Due to Primary Non-Sinus Supraventricular Tachyarrhythmias. Pediatr. Cardiol. 2003, 24, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Fenelon, G.; Wijns, W.; Andries, E.; Brugada, P. Tachycardiomyopathy: Mechanisms and Clinical Implications. Pacing Clin. Electrophysiol. 1996, 19, 95–106. [Google Scholar] [CrossRef]
- Huizar, J.F.; Ellenbogen, K.A.; Tan, A.Y.; Kaszala, K. Arrhythmia-Induced Cardiomyopathy: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019;73:2328-44.
- Bozkurt, B.; Colvin, M.; Cook, J.; Cooper, L.T.; Deswal, A.; Fonarow, G.C.; Francis, G.S.; Lenihan, D.; Lewis, E.F.; McNamara, D.M.; et al. Current Diagnostic and Treatment Strategies for Specific Dilated Cardiomyopathies: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e579–e646. [Google Scholar] [CrossRef] [PubMed]
- Spinale, F.G.; de Gasparo, M.; Whitebread, S.; Hebbar, L.; Clair, M.J.; Melton, D.M.; et al. Modulation of the renin-angiotensin pathway through enzyme inhibition specific receptor blockade in pacing-induced heart failure:, I. Effects on left ventricular performance and neurohormonal systems. Circulation. 1997;96:2385-96.
- A Riegger, G.; Elsner, D.; Kromer, E.P.; Daffner, C.; Forssmann, W.G.; Muders, F.; Pascher, E.W.; Kochsiek, K. Atrial natriuretic peptide in congestive heart failure in the dog: plasma levels, cyclic guanosine monophosphate, ultrastructure of atrial myoendocrine cells, and hemodynamic, hormonal, and renal effects. Circulation 1988, 77, 398–406. [Google Scholar] [CrossRef] [PubMed]
- De Giovanni, J.V.; Dindar, A.; Griffith, M.J.; A Edgar, R.; Silove, E.D.; Stumper, O.; Wright, J.C. Recovery pattern of left ventricular dysfunction following radiofrequency ablation of incessant supraventricular tachycardia in infants and children. Heart 1998, 79, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Seferović, P.M.; Polovina, M.; Bauersachs, J.; Arad, M.; Ben Gal, T.; Lund, L.H.; Felix, S.B.; Arbustini, E.; Caforio, A.L.P.; Farmakis, D.; et al. Heart failure in cardiomyopathies: a position paper from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 553–576. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.E.; Law, Y.M.; Asante-Korang, A.; Austin, E.D.; Dipchand, A.I.; Everitt, M.D.; Hsu, D.T.; Lin, K.Y.; Price, J.F.; Wilkinson, J.D.; et al. Cardiomyopathy in Children: Classification and Diagnosis: A Scientific Statement From the American Heart Association. Circulation 2019, 140, E9–E68. [Google Scholar] [CrossRef] [PubMed]
- Vera, A.; Cecconi, A.; Martínez-Vives, P.; Olivera, M.J.; Hernández, S.; López-Melgar, B.; Rojas-González, A.; Díez-Villanueva, P.; Salamanca, J.; Tejelo, J.; et al. Electrocardiogram and CMR to differentiate tachycardia-induced cardiomyopathy from dilated cardiomyopathy in patients admitted for heart failure. Hear. Vessel. 2022, 37, 1850–1858. [Google Scholar] [CrossRef] [PubMed]
- Spahic, A.; Chen, T.-H.; Geller, J.C.; Saenger, J.; Ohlow, M. Life in the fast lane: clinical and immunohistological characteristics of tachycardia-induced cardiomyopathy—a retrospective study in 684 patients. Herzschrittmachertherapie + Elektrophysiologie 2020, 31, 292–300. [Google Scholar] [CrossRef]
- Mueller, K.A.; Heinzmann, D.; Klingel, K.; Fallier-Becker, P.; Kandolf, R.; Kilias, A.; Walker-Allgaier, B.; Borst, O.; Kumbrink, J.; Kirchner, T.; et al. Histopathological and Immunological Characteristics of Tachycardia-Induced Cardiomyopathy. Circ. 2017, 69, 2160–2172. [Google Scholar] [CrossRef]
- Moore, J.P.; Wang, S.; Albers, E.L.; Salerno, J.C.; Stephenson, E.A.; Shah, M.J.; Pflaumer, A.; Czosek, R.J.; Garnreiter, J.M.; Collins, K.; et al. A Clinical Risk Score to Improve the Diagnosis of Tachycardia-Induced Cardiomyopathy in Childhood. Am. J. Cardiol. 2016, 118, 1074–1080. [Google Scholar] [CrossRef]
- Shinbane, J.S.; A Wood, M.; Jensen, D.; A Ellenbogen, K.; Fitzpatrick, A.P.; Scheinman, M.M. Tachycardia-Induced Cardiomyopathy: A Review of Animal Models and Clinical Studies. Circ. 1997, 29, 709–715. [Google Scholar] [CrossRef]
- O'Brien, P.J.; Moe, G.W.; Nowack, L.M.; Grima, E.A.; Armstrong, P.W. Sarcoplasmic reticulum Ca-release channel and ATP-synthesis activities are early myocardial markers of heart failure produced by rapid ventricular pacing in dogs. Can. J. Physiol. Pharmacol. 1994, 72, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Cruz FE, Cheriex EC, Smeets JL, Atie J, Peres AK, Penn OC, et al. Reversibility of tachycardia-induced cardiomyopathy after cure of incessant supraventricular tachycardia. J Am Coll Cardiol. 1990;16:739-44.
- Lip, G.Y.; Heinzel, F.R.; Gaita, F.; Juanatey, J.R.G.; Le Heuzey, J.Y.; Potpara, T.; Svendsen, J.H.; Vos, M.A.; Anker, S.D.; Coats, A.J.; et al. European Heart Rhythm Association/Heart Failure Association joint consensus document on arrhythmias in heart failure, endorsed by the Heart Rhythm Society and the Asia Pacific Heart Rhythm Society. Eur. 2016, 18, 12–36. [Google Scholar] [CrossRef] [PubMed]
- Dohain, A.M.; Lotfy, W.; Abdelmohsen, G.; Sobhy, R.; Abdelaziz, O.; Elsaadany, M.; Abdelsalam, M.H.; Ibrahim, H. Functional recovery of cardiomyopathy induced by atrial tachycardia in children: Insight from cardiac strain imaging. Pacing Clin. Electrophysiol. 2021, 44, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Ling, L.-H.; Kalman, J.M.; Ellims, A.H.; Iles, L.M.; Medi, C.; Sherratt, C.; Kaye, D.M.; Hare, J.L.; Kistler, P.M.; Taylor, A.J. Diffuse Ventricular Fibrosis Is a Late Outcome of Tachycardia-Mediated Cardiomyopathy After Successful Ablation. Circ. Arrhythmia Electrophysiol. 2013, 6, 697–704. [Google Scholar] [CrossRef]
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kühl, U.; Maisch, B.; McKenna, W.J.; et al. Classification of the cardiomyopathies: a position statement from the european society of cardiology working group on myocardial and pericardial diseases. Eur. Hear. J. 2007, 29, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Mewton, N.; Liu, C.Y.; Croisille, P.; Bluemke, D.; Lima, J.A. Assessment of Myocardial Fibrosis With Cardiovascular Magnetic Resonance. Circ. 2011, 57, 891–903. [Google Scholar] [CrossRef]
- West, A.M.; Kramer, C.M. Cardiovascular Magnetic Resonance Imaging of Myocardial Infarction, Viability, and Cardiomyopathies. Curr. Probl. Cardiol. 2010, 35, 176–220. [Google Scholar] [CrossRef]
- Hasdemir, C.; Yuksel, A.; Camli, D.; Kartal, Y.; Simsek, E.; Musayev, O.; Isayev, E.; Aydin, M.; Can, L.H. Late Gadolinium Enhancement CMR in Patients with Tachycardia-Induced Cardiomyopathy Caused by Idiopathic Ventricular Arrhythmias. Pacing Clin. Electrophysiol. 2012, 35, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Lashus, A.G.; Case, C.L.; Gillette, P.C. Catheter Ablation Treatment of Supraventricular Tachycardia–Induced Cardiomyopathy. Arch. Pediatr. Adolesc. Med. 1997, 151, 264–6. [Google Scholar] [CrossRef]
- Nerheim, P.; Birger-Botkin, S.; Piracha, L.; Olshansky, B.; B, S.; B, G.; T, N.; F, G.; J, V.; S, C.; et al. Heart Failure and Sudden Death in Patients With Tachycardia-Induced Cardiomyopathy and Recurrent Tachycardia. Circulation 2004, 110, 247–252. [Google Scholar] [CrossRef]
Figure 1.
Cross-sectional growth chart showing growth retardation of the patients during TIC. Red line shows the growth of body heigh. Blue line shows the growth of body weight. This chart is adopted from The Japanese Society for Pediatric Endocrinology [10].
Figure 1.
Cross-sectional growth chart showing growth retardation of the patients during TIC. Red line shows the growth of body heigh. Blue line shows the growth of body weight. This chart is adopted from The Japanese Society for Pediatric Endocrinology [10].
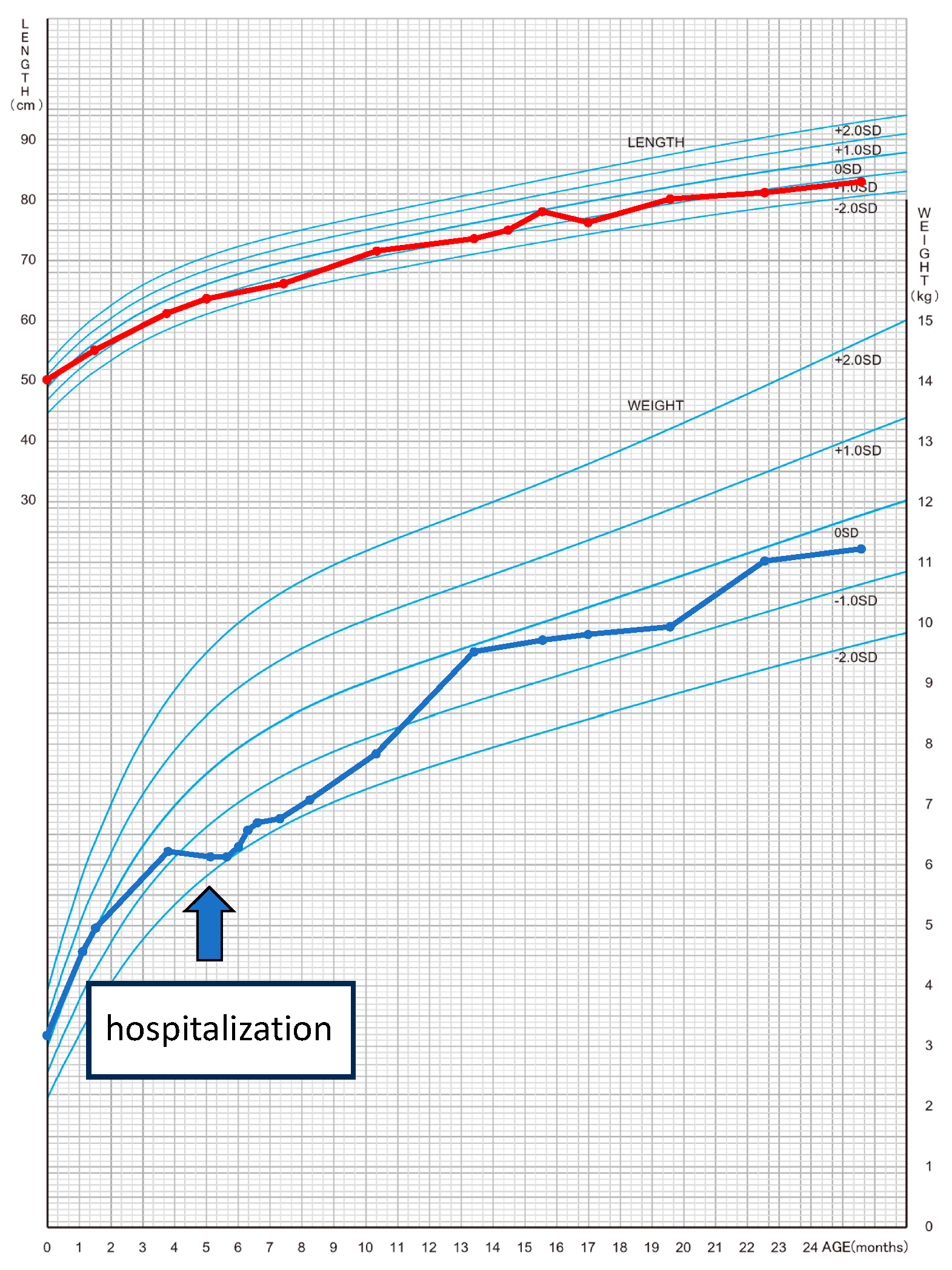
Figure 2.
(a) Chest X-ray A/P view showing cardiomegaly with a cardiothoracic ratio of 0.62 and lung congestion. (b) Echocardiography showed that left ventricular dilation and wall motion diffusely decreased. LVEF, 13.7%; LVDd, 39.7 mm(+7.0SD); mild mitral regurgitation. (c) Typical AF with 2:1 conduction. The arrows indicate the flutter waves. (d) Sinus rhythm after synchronized electrical cardioversion.
Figure 2.
(a) Chest X-ray A/P view showing cardiomegaly with a cardiothoracic ratio of 0.62 and lung congestion. (b) Echocardiography showed that left ventricular dilation and wall motion diffusely decreased. LVEF, 13.7%; LVDd, 39.7 mm(+7.0SD); mild mitral regurgitation. (c) Typical AF with 2:1 conduction. The arrows indicate the flutter waves. (d) Sinus rhythm after synchronized electrical cardioversion.
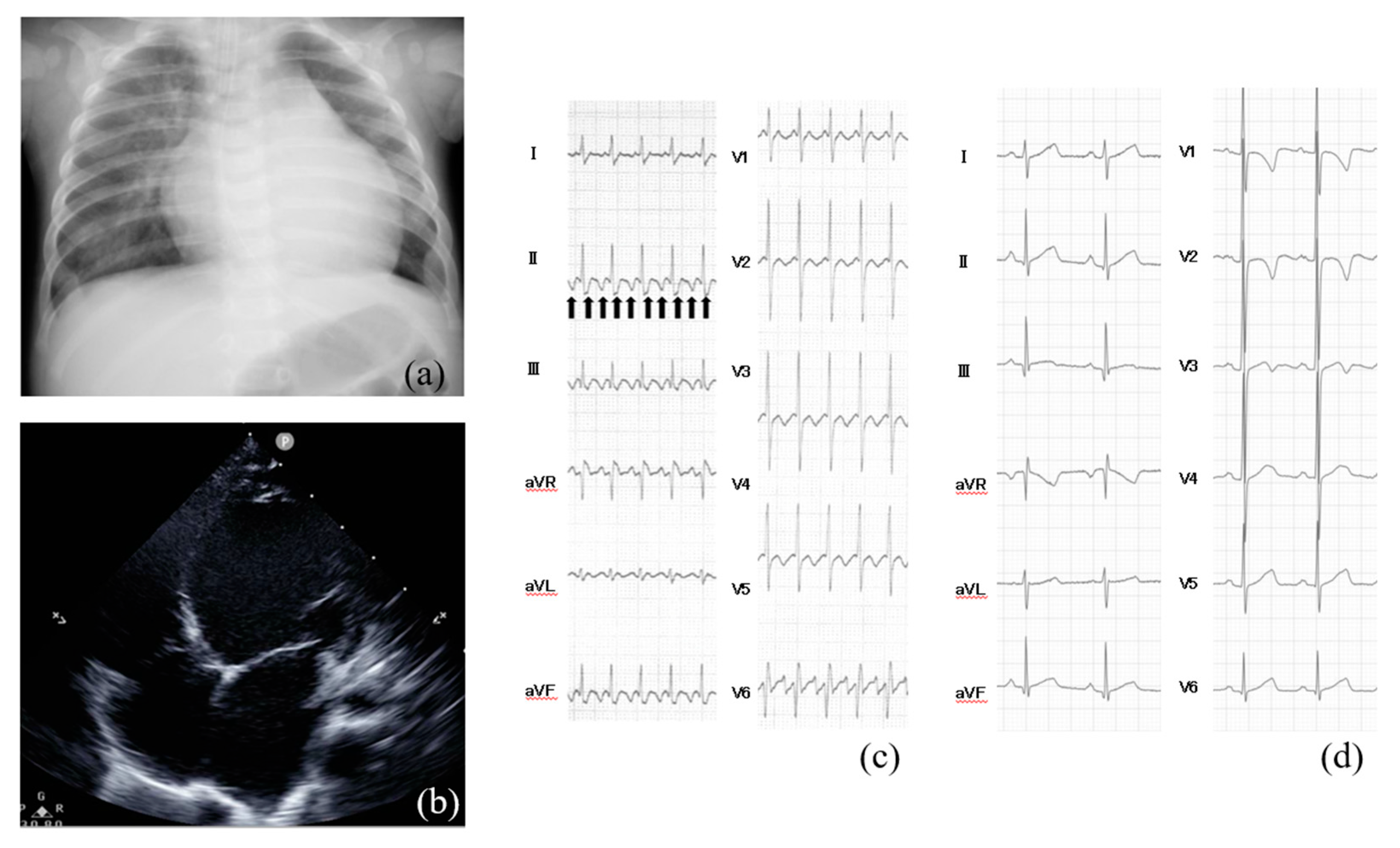

Table 1.
Literature review summary with tachycardia-induced cardiomyopathy in early infant.
| Author | Age of TIC | Cause of tachycardia | Heart rate (beats/min) | Duration from the onset | LV function on echocardiogram | Medication | Non-pharmacological therapy | LV function on echocardiogram after treatment | Prognosis |
|---|---|---|---|---|---|---|---|---|---|
| Van Hare GF, et al.[11] | 5-week-old | PJRT | N/A | N/A | LVFS 5% | flecainide and sotalol | catheter ablation | improved | alive |
| Sanchez C, et al.[12] | 3-month-old | PJRT | 230 | 20 days | LVFS 20% | digoxin and amiodarone | catheter ablation | improved | alive |
| Schulze OC, et al.[13] | 3-week-old | PJRT | 230 | N/A | LVFS 15% | no | catheter ablation | improved | alive |
| Mares JC, et al.[9] | 1-month-old | SVT | 260 | N/A | LVFS 13% | flecainide | no | improved | alive |
| Jon Felt, et al.[14] | 7-week-old | AFL | 195 | N/A | LVFS 17% | amiodarone | electrical cardioversion | improved | alive |
| Gardiner M, et al.[15] | 24-day-old | SVT | 270 | N/A | LVEF 35% | adenosine | no | improved | alive |
| Papadopoulou M, et al.[16] | 1-month-old | AFL | 216 | N/A | LVFS 19-21%, LVEF 42-45% | no | electrical cardioversion | improved | alive |
| McKenzie K, et al.[17] | 3-month-old | SVT | N/A | 1 month | LVEF 22% | digoxin, beta-blocker and amiodarone | catheter ablation | improved | alive |
PJRT: permanent junctional reciprocating tachycardia, SVT: supraventricular tachycardia, AFL: atrial flutter, LVFS: left ventricular fractional shortening, LVEF: left ventricular ejection fraction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



