
Submitted:
30 April 2024
Posted:
01 May 2024
You are already at the latest version
Abstract
Colonoscopy, essential for diagnosing and treating colorectal cancer, relies on effective bowel preparation to inspect the colonic mucosa fully. Traditional education methods include printed instructions and verbal explanations, but these may not ensure clear patient understanding. Poor bowel preparation can obscure mucosal visibility, delaying cancer diagnosis and treatment. Using the outpatient’s Android mobile device, the mobile health care model is provided as a nursing guide to assist in bowel preparation for colonoscopy. This single-blinded, randomized trial en-rolled patients for colonoscopy at a Northern Taiwan gastroenterology center. Eligible patients were physically and mentally healthy and could communicate in Chinese. The study tested the ColonClean app during bowel preparation. After the procedure, endoscopists rated the prepara-tion quality using the Aronchick Scale. Data analysis with SPSS software (version 25.0) evaluated if the app significantly improved bowel preparation compared to those who did not use it. Forty patients were recruited for both the control (conventional method) and experimental (conven-tional method plus ColonClean app) groups. In the experimental group, endoscopists assessed bowel preparation quality; all achieved at least "Fair," with 75% receiving "Excellent" or "Good" ratings. The ColonClean App enhanced bowel preparation quality more effectively than tradi-tional nursing guidance.
Keywords:
Mobile Health Care Model
; Mobile Health Application
; Bowel Preparation
; Nursing Guidance
1. Introduction
Colorectal cancer ranks third in incidence and second in mortality rates globally [1]. Early-stage colorectal cancer often presents no symptoms, leading to warning signs being overlooked [2,3]. The World Health Organization indicates that 30%–50% of all cancer cases are preventable, highlighting the importance of preventive measures [4,5].
Colonoscopy offers advantages in both diagnosis and treatment, allowing for direct sampling and excision of lesions, thus preventing adenomatous polyps from progressing to cancer. It is an accurate and well-tolerated examination method [6-8]. Bowel preparation before colonoscopy involves dietary restrictions and using bowel-cleansing agents to remove fecal matter from the colon, providing optimal conditions for mucosal visualization during the procedure [9,10]. This step is crucial for the overall integrity of colonoscopy [7,11]. An incomplete colonoscopy prevents adequate visualization of the colonic mucosa, hampers the detection of lesions, and delays cancer diagnosis and treatment [12].
Bowel preparation quality is assessed during colonoscopy using the Aronchick Bowel Preparation Scale, which evaluates the percentage of colonic mucosa covered by feces [13]. A thorough bowel preparation provides the physician with a clear view of the entire colonic mucosa during the examination, enabling the identification of polyps or other abnormalities. This enhanced visibility contributed to a 5% increase in adenoma detection rates [14]. Conversely, inadequate bowel preparation may lead to missed pathological findings, prolonged procedure times, failed detection of cancerous lesions, and increased risk of adverse events during the examination [15-17].
Traditional methods of bowel preparation education before colonoscopy involve providing printed care instruction sheets accompanied by verbal explanations. However, conveying bowel preparation instructions solely through text and oral communication may not ensure patients’ clear understanding. Complex and lengthy instructions can lead to poor adherence, with up to 25%–30% of patients achieving inadequate bowel preparation [14]. Poor bowel preparation is associated with a high rate of missed polyps, particularly sessile polyps on the colonic mucosa. Therefore, improving bowel preparation quality is crucial [7,11,18].
The World Health Organization defines mobile health as using wireless communication devices to support public health and clinical practice, recognizing it as a safe and cost-effective care method [19,20]. Smartphone apps have become increasingly popular in healthcare, offering solutions to many traditional healthcare challenges. With the advent of the digital and mobile era, mobile health apps have emerged as an important trend in the healthcare industry, offering various lifestyle and health management tools such as smoking cessation support and exercise tracking.
Effective nursing guidance can provide planned nursing behaviors, aiding patients in understanding and addressing health issues. Besides conventional methods using printed care instruction sheets, various approaches such as educational booklets, videos, images, telephone calls, and text message reminders have been used to improve bowel preparation efficacy. However, integrating smartphone apps with verbal and printed nursing guidance education can further enhance bowel preparation efficacy by 10% [21,22]. Regardless of the method used, the goal is to improve the quality of bowel preparation.
Following the COVID-19 pandemic and the need to reduce virus transmission by maintaining physical distance, mobile health apps have become even more critical [23,24]. During current public health emergencies, using personal communication tools to provide remote medical services has become essential [25,26]. Using mobile devices in conjunction with mobile apps to assist traditional printed nursing guidance, supplemented with verbal instructions for bowel preparation, can enhance the level of bowel preparation. Using mobile apps to reinforce patient education on bowel preparation can improve the overall quality of bowel preparation [17,27].
In this study, a mobile health app called ColonClean was designed using mobile devices and information and communication technology. It was developed on the Android operating system as a nursing guidance tool for bowel preparation. This approach provides a safe and cost-effective method of guidance. Bowel preparation requirements are complex and challenging to understand and remember. Effective use of reminders, food diagrams, step-by-step illustrations of bowel-cleansing medication, and audiovisual aids can enhance patient understanding of bowel preparation. Reference images of fecal characteristics also help patients to understand whether their bowel movements meet the requirements for colonoscopy, increasing patient compliance.
Integrating mobile app design with traditional verbal and printed nursing guidance methods strengthens a mobile health care model, enhancing health service information. It is hoped that in the future, whether for outpatient cases, hospitalized patients, or individuals requiring bowel preparation, this approach can reinforce education on bowel preparation and increase preparation levels, which will facilitate comprehensive colonoscopy, leading to the successful completion of the procedure and ultimately reducing healthcare costs.
2. Materials and Methods
2.1. Study Procedures
An approval from the Institutional Review Board of the Taipei Veterans General Hospital has been obtained prior to commencement of the study (approval number: 2021-10-007AC). It was conducted from October 27, 2021, to December 31, 2022.
2.2. Study Design
This study was conducted in the outpatient clinics of the Gastroenterology and Endoscopy Center in Northern Taiwan. It adopted a quantitative research approach, using a single-blind, randomized, quasi-experimental design with a posttest-only, equivalent-group design.
2.3. Population
Individuals recommended by their physicians to undergo colonoscopy had to meet the following criteria:
- Aged ≥20 years.
- Able to communicate in Taiwanese or Mandarin.
- No visual or hearing impairments.
- Own an Android-based mobile device.
- No severe mental or cognitive impairments and able to comply with the study requirements.
Individuals were enrolled in this study after its purpose and content had been explained to them, and they had provided consent by signing the informed consent form.
Based on the reference research design [28], a sample size of 64 individuals was estimated for this study using the G*Power for Windows software (version 3.1.9.7), considering a statistical power (1−β) of 0.8 and α value of 0.05, and considering the importance of bowel preparation, a moderate effect size of 0.3. Considering a dropout rate of 20% to account for potential sample loss and invalid data, it was decided that this study should include 80 participants, with 40 allocated to each of the experimental and control groups.
Two sheets of paper with 0 and 1 written on them were prepared to allocate participants to the respective groups. Participants drew one of these sheets to determine their group assignment. Those who drew the sheet with the number 0 were assigned to the control group, while those who drew the sheet with the number 1 were assigned to the experimental group. After the cases were included in the study, both groups completed the basic data questionnaire within 3 days after the colonoscopy.
2.4. Research Tool (Mobile Health app)
The ColonClean app was created on the Android operating system and developed by a team consisting of a clinical nurse, a user interface designer, and an information engineer. The app design was based on an assessment of current needs and supported via a literature review.
Regarding the precautions for bowel preparation before colonoscopy, the paper-based nursing guidance leaflet includes the purpose of colonoscopy, precautions for using bowel preparation drugs, dietary preparation, and precautions after colonoscopy. The control group used conventional paper-based nursing instruction leaflets combined with oral instructions. In addition to the printed care instructions and verbal instructions, the experimental group also used the ColonClean app as an intervention. Participants in the experimental group downloaded the ColonClean app to their smartphones or mobile devices through the provided QR code. The app has a dedicated icon on its home screen for easy access. After receiving instructions from the researchers on how to use the app, the participants in the experimental group entered their personal information, their exam date, and the details of the bowel preparation medication they would use.
Patients in both groups received one-on-one instruction during the nursing guidance process. These instructions were provided in a dedicated waiting area at the outpatient clinic before their appointment and continued until the participant fully understood the information provided. The ColonClean app was designed for the Android operating system. Its content was identical to the printed nursing instructions [29], but it enhanced user understanding by replacing text descriptions with cartoon images and step-by-step visuals. For example, dietary choices, instructions for bowel preparation medication use, and other relevant information are presented using cartoon images and visual flowcharts to facilitate better understanding. The app includes a feature for recording water intake after taking bowel preparation medication to promote the effectiveness of bowel preparation by helping users ensure they consume sufficient water.
The app also guides interpreting the last bowel movement, including suggestions based on images of different types of bowel movements and a visualization of the level of bowel preparation for colonoscopy. All aspects of bowel preparation are also presented in a dedicated video section, allowing users to understand the process through audiovisual means (Figure 1).
Participants in the control group had to be mindful of the starting time for bowel preparation. In contrast, the ColonClean app provided reminders and notifications to participants in the experimental group starting three days before their examination. These reminders suggest initiating dietary restrictions, such as avoiding high-fiber fruits and vegetables. Two days before the examination, the app reminds users to switch to a low-residue diet (e.g., congee, white noodles). On the day before the examination, the app notifies users to follow a clear liquid diet (e.g., oil-free broth and sports drinks) and provides instructions on how to use bowel preparation medications.
During the bowel preparation period, users can use the app to access information on dietary choices, recommendations for water intake, the importance of bowel preparation, and reference images for interpreting the last bowel movement. The app also provides audiovisual content to help users understand how to use bowel preparation medications. On the day of the examination, participants in the experimental group could take a photo of their last bowel movement and compare it with the built-in images in the ColonClean app to assess whether their bowel preparation quality meets the requirements of excellent, good, fair, or poor. If participants encounter any issues during the bowel preparation process, they can refer to the app’s built-in “Notes and Precautions” section for assistance.
2.5. Endoscopists’ Qualifications
To ensure consistency in assessing the bowel preparation quality in this study, both endoscopists performing colonoscopies possessed qualifications as specialist physicians in gastrointestinal endoscopy and were attending physicians. They had at least one year of service at the Gastroenterology and Endoscopy Center and performed over 500 colonoscopies yearly. In the single-blind study design, the endoscopists were unaware of the group assignments of the study participants. The endoscopists evaluated the effectiveness of bowel preparation in the study subjects using the Aronchick Bowel Preparation Scale.
2.6. Statistical Analysis
The data were analyzed using SPSS software (version 25.0). The number and percentages of participants in each category of the Aronchick Bowel Preparation Scale were compared between the experimental and control groups using a Chi-square test to determine whether bowel preparation quality, as judged by endoscopists, differed significantly between them.
3. Results
3.1. Participants’ Characteristics
This study included 80 participants who were randomly assigned to either the experimental (n = 40) or control (n = 40) group. All 80 participants completed colonoscopy without any mid-process cancellations or exclusions due to missing data. The two groups differed significantly only in body mass index (BMI; p = 0.020). The participants’ demographic characteristics were as follows: 51.2% were male, 30% were aged 51–60 years, their mean BMI was 23.79 ± 3.97, their highest educational attainment was a college/university degree (45%), most were married (76.25%), 21.25% reported constipation, 35% had a history of abdominal surgery, 15% had a history of diabetes, 17.5% had a family history of colorectal cancer, and 60% had previous experience with colonoscopy (Table 1).
3.2. Bowel Preparation Quality
This study compared the frequency and percentage of bowel preparation quality determined by endoscopists using the Aronchick Bowel Preparation Scale between groups using a Chi-square test (Table 2). It investigated whether bowel preparation quality, as judged by endoscopists, differed significantly between the experimental and control groups (Figure 2).
The endoscopists assessed the bowel preparation quality according to the Aronchick Bowel Preparation Scale during the colonoscopy procedure, classifying it as “Excellent,” “Good,” “Fair,” or “Poor,” and documenting it in the colonoscopy report after the examination. In the experimental group, 10 participants (25%) were rated as Fair, 26 (65%) as Good, and 4 (10%) as Excellent. In the control group, 7 participants (17.5%) were rated as Poor, 13 (32.5%) as Fair, 19 (47.5%) as Good, and 1 (2.5%) as Excellent. The chi-square test indicated a significant difference between groups (p = 0.016).
Analysis of the two groups revealed a predominance of yellow watery stool characteristics reported during the last bowel movement, consistent with Shin et al. (2019) [30], which suggests suitability for colonoscopy examination based on stool attributes.
This study’s results demonstrate that bowel preparation quality was significantly superior in the experimental group compared to the control group. This finding has significant implications for clinical nursing guidance and practice, suggesting that a mobile healthcare model can effectively assist individuals in achieving better bowel preparation before endoscopic examinations. This improvement can potentially enhance the efficiency and accuracy of examinations, reduce procedural complexity, increase patient satisfaction, and possibly lower the risk of complications and adverse events associated with the procedure.
This research used the ColonClean app to educate users on bowel preparation effectiveness, as assessed by endoscopists using the Aronchick Bowel Preparation Scale. While the “Poor” category was not observed, the proportions of “Excellent” and “Good” ratings did not meet the domestic colonoscopy quality target of over 90% [31].
The quality of bowel preparation and attainment of complete cecal intubation are indispensable components of a comprehensive and successful colonoscopy procedure. Complete cecal intubation is a vital metric in evaluating colonoscopy screening quality, involving the insertion of the colonoscope near the ileocecal valve to thoroughly examine the cecum, including the intermediate area between the appendiceal orifice and the ileocecal valve. As approximately 15% of all polyps and cancerous tumors are located in the cecum, a cecal intubation rate of ≥90% is recommended to facilitate the detection of hidden lesions, enabling effective further diagnosis and treatment [32-34].
The cecal intubation rate was 100% among participants in both the experimental and control groups, with no interruptions or cancellations of colonoscopy procedures. The participants found the bowel preparation process to be strenuous. To facilitate the successful completion of colonoscopy examinations, the study hospitals used a Flushing Pump OFP-2 during the procedures. Physicians often used this equipment to cleanse the colon when the quality of bowel preparation allowed for the flushing and suctioning of fecal matter and debris. This approach yielded outcomes consistent with scholarly findings, demonstrating complete cecal intubation rates. Participants undergoing colonoscopy examinations endured the challenges associated with bowel preparation. The study hospitals aimed to mitigate the rate of incomplete colonoscopy examinations and reduce the likelihood of repeat procedures by leveraging professional-grade equipment [35].
4. Discussion
The effectiveness of different nursing instruction methods on bowel preparation is crucial. For outpatient cases, understanding the importance of bowel preparation before colonoscopy and the procedure itself is pivotal for a successful examination [36]. Difficulty understanding the requirements for bowel preparation or misconceptions about its significance during the first colonoscopy can lead to inadequate preparation, affecting the effectiveness of the examination and potentially masking underlying conditions [37,38]. When the proportion of inadequate bowel preparation exceeds 10%–15%, it is necessary to reassess the preparation plan and implement improvement measures. Updated methods of bowel preparation guidance can further educate patients on adhering to pre-preparation instructions, enhancing the likelihood of achieving optimal intestinal cleansing [39,40,41]. However, relying solely on paper-based nursing instruction sheets and verbal communication is insufficient. In addition to conventional methods, it is recommended that healthcare professionals use various educational strategies to achieve a more comprehensive level of bowel preparation [41].
Enhanced education by healthcare professionals significantly improves compliance with bowel preparation. For colonoscopy, educational pamphlets may serve as relevant, cost-effective, and valuable materials. Healthcare professionals explain the bowel preparation process clearly to patients during outpatient visits and provide pamphlets with clear, color-coded illustrations as reinforcement tools for verbal communication [42]. The pamphlets emphasize dietary restrictions, the importance of adequate hydration, and the potential side effects of bowel preparation medications. A previous study found that an enhanced patient education program significantly increased the level of bowel preparation for colonoscopy, with a significantly higher proportion of excellent preparation in the intervention group than in the control group (98.7% vs. 52.3%, p < 0.001).
Another study [43] recruited 657 research participants aged 18–85 years with a history of failed bowel preparation from 11 hospitals in Spain who were randomly assigned to either the control group, which received paper-based nursing instruction sheets and verbal explanations, or the intervention group, which received additional reinforcement through telephone education by nurses within 48 hours before their colonoscopy. The primary goals of the enhanced nursing instruction were to ensure compliance with dietary restrictions and intake of bowel preparation medications, emphasize the importance of proper bowel preparation, and address any concerns or doubts during the preparation process. Its results showed no significant difference in the level of bowel preparation between the two groups (77.3% vs. 72%, p = 0.12). However, there was a trend towards more adequate bowel preparation, with an improvement of approximately 11.5%. There was also a trend towards improved colonoscopy completion rates among participants who received nurse-led telephone education. These findings suggest that telephone reinforcement education by nurses may be an effective tool for improving bowel preparation.
In another study, nurses provided patients with a colonoscopy information booklet for bowel preparation education, covering dietary arrangements, methods of using bowel preparation medications, and the colonoscopy procedure [44]. In addition to verbal instructions, patients received two video SMS messages on their smartphones. Its results indicated that educational video SMS messages delivered via smartphones led to better bowel preparation, serving as a tool to enhance the safety and effectiveness of colonoscopy. However, this educational method may be more beneficial for individuals aged under 40 years who are likely more frequent and proficient smartphone users than older adults.
Another approach involves using paper-based nursing instruction sheets with vivid illustrations and simple, understandable text supplemented by verbal explanations. Information related to the paper-based content was also sent through the WeChat mobile social media application, providing online real-time assistance for bowel preparation guidance. The results showed a 90.1% completion rate of bowel preparation. When comparing the reinforcement measures provided through WeChat and SMS, WeChat was found to be superior to SMS in achieving optimal levels of bowel preparation [45,46].
Mobile health apps represent a novel educational tool that can facilitate better and more comprehensive bowel preparation before colonoscopy. In outpatient settings, patients receive push notifications starting four days before the colonoscopy, providing visual aids of low-residue and clear liquid diets, reminders on when to start consuming appropriate diet types, and notifications regarding the use of bowel preparation medications. These apps feature visual aids and reminders, resulting in 92.3% of users achieving optimal levels of bowel preparation, with 60.6% reaching excellent levels [17,47].
In this study, the ColonClean app began sending reminders to start bowel preparation three days before the colonoscopy, along with recommendations on dietary restrictions. During the preparation period, users can access text and image-based guidance on dietary choices, recommended fluid intake, the importance of intestinal cleansing, and reference materials on the characteristics of the last bowel movement. Video references are also available to help understand how to use bowel cleansing medications. On the day of the examination, users take a photo of their last bowel movement and compare it with the images built into the ColonClean app to assess whether the quality of their bowel preparation meets the criteria of excellent, good, fair, or poor. As a supportive tool for bowel preparation guidance, the ColonClean app effectively increased the proportion of excellent and good preparation levels to 75%. It is believed that compared to methods such as phone calls or SMS, the ColonClean app can also reduce the workload of healthcare personnel, making it more suitable for the current COVID-19 pandemic situation in our country. Regardless of the method used, it should align with the culture and requirements at the time, aiming to achieve optimal benefits at a minimal cost.
This study has several study limitations. First, this study was only conducted at one medical center in Northern Taiwan. While the ColonClean app was used as a tool for bowel preparation nursing guidance, variations in the choice and use of bowel cleansing medications among different medical institutions and differences in physicians’ medication preferences may exist. It is recommended that future studies be conducted at various medical institutions to confirm whether nursing guidance programs for bowel preparation before colonoscopy, assisted by mobile healthcare models, yield superior effectiveness. Second, the ColonClean app developed in this study was designed explicitly for the Android operating system on mobile devices. It does not support other operating systems. It is suggested that future research develop mobile healthcare apps compatible with all major operating systems to serve as comprehensive nursing guidance tools for bowel preparation.
This study has several study suggestions. First, while the ColonClean app provides users with cartoon images, videos, and other means to understand bowel preparation, it is suggested that real-time interactive features be added to address any issues encountered during the preparation process. Their inclusion would effectively stabilize users’ emotions during preparation and reduce concerns about incomplete bowel preparation. Second, in response to the advent of artificial intelligence (AI), it is recommended to integrate AI recognition functionality into the ColonClean app to understand the nature of the last bowel movement [48]. Using AI, the app could automatically identify and determine the attributes of the last bowel movement, which would provide analysis and effective recommendations for individuals with poor bowel preparation quality, thereby enhancing the overall quality of bowel preparation [49,50]. Third, for future optimization of the ColonClean app, it is suggested that it be promoted or listed on various app store platforms to make it accessible to a wider audience. By offering compatibility with different operating systems and devices, the app could be made available to individuals needing bowel preparation, thereby benefiting a larger population.
5. Conclusions
Early-stage colorectal cancer is often asymptomatic and can easily go unnoticed. Colonoscopy can identify colorectal diseases, precancerous lesions, or malignant tumors to allow for further diagnosis and treatment, thereby enabling early detection and intervention to reduce the incidence and mortality of colorectal cancer. During the colonoscopy, endoscopists can directly sample lesions and remove adenomatous polyps, preventing their progression to colorectal cancer. Adequate bowel preparation before the colonoscopy is crucial for the integrity of the examination. Fecal matter is removed from the colon through a dual strategy of dietary restrictions and bowel cleansing medications, providing a clear view of the colonic mucosa for the endoscopist’s assessment.
Traditionally, bowel preparation guidance has relied on paper-based instructions supplemented by verbal explanations. However, using the ColonClean app for pre-colonoscopy bowel preparation guidance has enhanced users’ understanding of dietary concepts, such as clear liquid, low-residue, and high-fiber diets, through visual aids. Push notifications remind users of dietary, medication, and appointment timing, enhancing the accuracy and compliance of bowel preparation. The app effectively assists individuals in completing bowel preparation tasks by adopting a user-centered approach.
The mobile healthcare model established through the ColonClean app enables users to perceive the convenience and assistance of using their mobile devices combined with the mobile health app. The COVID-19 pandemic has altered individuals’ lifestyles, necessitating the maintenance of physical distancing from others to reduce virus transmission, once again highlighting the importance of mobile health apps. In the future, the diverse development trends of smart healthcare aspire to use mobile health apps as unique tools for bowel preparation, aiming to achieve optimal bowel preparation quality and effectively reduce the incidence and mortality of colorectal cancer.
One approach to enhancing health service information in mobile healthcare models is to use mobile apps as a method of nursing guidance to assist patients. It is hoped that in the future, whether for outpatient cases, hospitalized patients, or those requiring bowel preparation, this approach can strengthen the effectiveness of bowel preparation education, enabling smooth completion of colonoscopies, avoiding interruptions, effectively reducing the workload on nursing staff, and decreasing medical costs.
Author Contributions
Conceptualization, Hui-Yu Chen; Data curation, Hui-Yu Chen; Formal analysis, Hui-Yu Chen; Methodology, Hui-Yu Chen; Supervision, Ming-Hsiang Tu; Validation, Hui-Yu Chen; Writing – original draft, Hui-Yu Chen; Writing – review & editing, Ming-Hsiang Tu and Miao-Yen Chen. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
An approval from the Institutional Review Board of the Taipei Veterans General Hospital has been obtained prior to commencement of the study (approval number: 2021-10-007AC).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to the ethics protocol of this study.
Acknowledgments
Acknowledgment and sincere thanks to the Outpatient cases from a gastroenterology and endoscopy center who participated in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: a Cancer Journal for Clinicians. 2021;71(3):209-249. [CrossRef]
- Plackett, R., Kaushal, A., Kassianos, A. P., Cross, A., Lewins, D., Sheringham, J., ... & von Wagner, C. (2020). Use of social media to promote cancer screening and early diagnosis: Scoping Review. Journal of medical Internet research, 22(11), e21582. [CrossRef]
- Vos, S. C., Sutton, J., Gibson, C. B., & Butts, C. T. (2019). Celebrity cancer on Twitter: mapping a novel opportunity for cancer prevention. Cancer Control, 26(1), 1073274819825826. [CrossRef]
- Shams-White, M. M., Brockton, N. T., Mitrou, P., Romaguera, D., Brown, S., Bender, A., ... & Reedy, J. (2019). Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) cancer prevention recommendations: a standardized scoring system. Nutrients, 11(7), 1572. [CrossRef]
- Shams-White, M. M., Romaguera, D., Mitrou, P., Reedy, J., Bender, A., & Brockton, N. T. (2020). Further Guidance in Implementing the Standardized 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Score. Cancer Epidemiology and Prevention Biomarkers, 29(5), 889-894. [CrossRef]
- Ciuti, G., Skonieczna-Żydecka, K., Marlicz, W., Iacovacci, V., Liu, H., Stoyanov, D., ... & Koulaouzidis, A. (2020). Frontiers of robotic colonoscopy: a comprehensive review of robotic colonoscopes and technologies. Journal of Clinical Medicine, 9(6), 1648. [CrossRef]
- Patel N, Kashyap S, Mori A. Bowel Preparation. 2020 Aug 22. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing;2021 Jan–. PMID: 30570989.
- Sharara, A. I., & Daher, H. B. (2019). Bowel cleansing strategies after suboptimal bowel preparation. Clinical Gastroenterology and Hepatology, 17(7), 1239-1241. [CrossRef]
- Nam, S. J., Park, S. C., Lee, S. J., Lee, S. H., Kim, J. H., Bang, C. S., & Seo, H. I. (2022). Randomized trial of oral sulfate solution versus polyethylene glycol–ascorbic acid for bowel cleansing in elderly people. Journal of Gastroenterology and Hepatology, 37(2), 319-326. [CrossRef]
- Zad, M., Do, C. N., Heffernan, A., Johnston, L., & Al-Ansari, M. (2020, Apr). Factors affecting bowel preparation adequacy and procedural time. JGH Open, 4(2), 206-214. [CrossRef]
- Hung, S. Y., Chen, H. C., & Chen, W. T. (2020, Mar 27). A Randomized Trial Comparing the Bowel Cleansing Efficacy of Sodium Picosulfate/Magnesium Citrate and Polyethylene Glycol/Bisacodyl (The Bowklean Study). Sci Rep, 10(1), 5604. [CrossRef]
- Chen, C., Shi, M., Liao, Z., Chen, W., Wu, Y., & Tian, X. (2022). Oral sulfate solution benefits polyp and adenoma detection during colonoscopy: Meta-analysis of randomized controlled trials. Digestive Endoscopy. [CrossRef]
- Donovan, K., Manem, N., Miller, D., Yodice, M., Kabbach, G., Feustel, P., & Tadros, M. (2021). The Impact of Patient Education Level on Split-Dose Colonoscopy Bowel Preparation for CRC Prevention. Journal of Cancer Education, 1-6. [CrossRef]
- Ye, Z., Chen, J., Xuan, Z., Gao, M., & Yang, H. (2020). Educational video improves bowel preparation in patients undergoing colonoscopy: a systematic review and meta-analysis. Annals of palliative medicine, 9(3), 671-680. [CrossRef]
- Hernández, G., Gimeno-García, A. Z., & Quintero, E. (2019). Strategies to improve inadequate bowel preparation for colonoscopy. Frontiers in medicine, 6, 245. [CrossRef]
- Niedermaier, T., Amitay, E. L., Gies, A., Weigl, K., Hoffmeister, M., & Brenner, H. (2020). Impact of Inadequate Bowel Cleansing on Colonoscopic Findings in Routine Screening Practice. Clinical and Translational Gastroenterology, 11(4), e00169. [CrossRef]
- Walter, B., Frank, R., Ludwig, L., Dikopoulos, N., Mayr, M., Neu, B., ... & Meining, A. (2021). Smartphone application to reinforce education increases high-quality preparation for colorectal cancer screening colonoscopies in a randomized trial. Clinical Gastroenterology and Hepatology, 19(2), 331-338. [CrossRef]
- Gandhi, K., Tofani, C., Sokach, C., Patel, D., Kastenberg, D., & Daskalakis, C. (2018). Patient characteristics associated with quality of colonoscopy preparation: a systematic review and meta-analysis. Clinical Gastroenterology and Hepatology, 16(3), 357-369.
- El Benny, M., Kabakian-Khasholian, T., El-Jardali, F., & Bardus, M. (2021). Application of the eHealth literacy model in digital health interventions: scoping review. Journal of medical Internet research, 23(6), e23473. [CrossRef]
- Smith, B., & Magnani, J. W. (2019). New technologies, new disparities: The intersection of electronic health and digital health literacy. International journal of cardiology, 292, 280-282. [CrossRef]
- Sewitch, M. J., Fallone, C. A., Ghali, P., & Lee, G. E. (2019). What Patients Want in a Smartphone App That Supports Colonoscopy Preparation: Qualitative Study to Inform a User-Centered Smartphone App. JMIR mHealth and uHealth, 7(7), e12242. [CrossRef]
- El Bizri, M., El Sheikh, M., Lee, G. E., & Sewitch, M. J. (2021). Mobile health technologies supporting colonoscopy preparation: A systematic review and meta-analysis of randomized controlled trials. PloS one, 16(3), e0248679. [CrossRef]
- Greenhalgh, T., Koh, G. C. H., & Car, J. (2020). Covid-19: a remote assessment in primary care. Bmj, 368. [CrossRef]
- Thulesius, H. (2020). Increased importance of digital medicine and eHealth during the Covid-19 pandemic. Scandinavian Journal of Primary Health Care, 38(2). [CrossRef]
- Ming, L. C., Untong, N., Aliudin, N. A., Osili, N., Kifli, N., Tan, C. S., ... & Goh, H. P. (2020). Mobile health apps on COVID-19 launched in the early days of the pandemic: content analysis and review. JMIR mHealth and uHealth, 8(9), e19796. [CrossRef]
- Alanzi, T.(2021). A review of mobile applications available in the app and google play stores used during the COVID-19 outbreak. Journal of Multidisciplinary Healthcare, 14, 45. [CrossRef]
- Guo, B., Zuo, X., Li, Z., Liu, J., Xu, N., Li, X., & Zhu, A. (2020). Improving the quality of bowel preparation through an app for inpatients undergoing colonoscopy: A randomized controlled trial. Journal of Advanced Nursing, 76(4), 1037-1045. [CrossRef]
- Wen, M. C., Kau, K., Huang, S. S., Huang, W. H., Tsai, L. Y., Tsai, T. Y., & Tsay, S. L. (2020). Smartphone education improves embarrassment, bowel preparation, and satisfaction with care in patients receiving colonoscopy: A randomized controlled trail. Medicine, 99(46).
- Walter, B., Schmid, R., & von Delius, S. (2017). A smartphone app for improvement of colonoscopy preparation (ColoprAPP): Development and feasibility study. JMIR mHealth and uHealth, 5(9), e138. [CrossRef]
- Shin SY, Ga KS, Kim IY, et al. Predictive factors for inadequate bowel preparation using low-volume polyethylene glycol (PEG) plus ascorbic acid for an outpatient colonoscopy. Scientific Reports. 2019;9(1). [CrossRef]
- Hassan C, East J, Radaelli F, et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2019. Endoscopy. 2019;51(08):775-794. [CrossRef]
- Lund, M., Trads, M., Njor, S. H., Erichsen, R., & Andersen, B. (2019). Quality indicators for screening colonoscopy and colonoscopist performance and the subsequent risk of interval colorectal cancer: a systematic review. JBI database of systematic reviews and implementation reports, 17(11), 2265-2300. [CrossRef]
- Muslim, O. T., & Al-Obaidi, H. O. (2021). Cecal and ilial intubation rates in colonoscopy: Comparative study. Journal of Population Therapeutics and Clinical Pharmacology= Journal de la Therapeutique des Populations et de la Pharmacologie Clinique, 28(2), e1-e6.
- Siau, K., Hodson, J., Ravindran, S., Rutter, M. D., Iacucci, M., & Dunckley, P. (2019). Variability in cecal intubation rate by calculation method: a call for standardization of key performance indicators in endoscopy. Gastrointestinal Endoscopy, 89(5), 1026-1036. [CrossRef]
- Liu, C., Gao, H., Yuan, X., Zhang, Z., Xie, J., Yu, C., & Xu, L. (2022). Minimal water exchange by the air-water valve versus left water exchange in unsedated colonoscopy: a randomized controlled trial. Endoscopy, (AAM). [CrossRef]
- Soeder, M., Turshudzhyan, A., Rosenberg, L., & Tadros, M. (2022). High-Quality Colonoscopy: A Review of Quality Indicators and Best Practices. Gastroenterology Insights, 13(2), 162-172. [CrossRef]
- Shamim, S., Andresen, Y. L. M., Vind Thaysen, H., Hovdenak Jakobsen, I., Nielsen, J., Kjaergaard Danielsen, A., & Konradsen, H. (2021). Experiences of patients undergoing bowel preparation and colonoscopy: a qualitative longitudinal study. Journal of multidisciplinary healthcare, 349-358. [CrossRef]
- Tontini, G. E., Prada, A., Sferrazza, S., Ciprandi, G., & Vecchi, M. (2021). The unmet needs for identifying the ideal bowel preparation. JGH open, 5(10), 1135-1141. [CrossRef]
- Butterly, L. F., Nadel, M. R., Anderson, J. C., Robinson, C. M., Weiss, J. E., Lieberman, D., & Shapiro, J. A. (2020). Impact of colonoscopy bowel preparation quality on follow-up interval recommendations for average-risk patients with normal screening colonoscopies: data from the New Hampshire Colonoscopy Registry. Journal of clinical gastroenterology.
- Thorlacius, H., Wurm, G., Nemeth, A., & Toth, E. (2017). Koloskopier måste kvalitetssäkras.
- Arslanca, G., & Aygün, M. (2022). Effect of nurse-performed enhanced patient education on colonoscopy bowel preparation quality. Revista Latino-Americana de Enfermagem, 30.
- Janahiraman, S., Tay, C. Y., Lee, J. M., Lim, W. L., Khiew, C. H., Ishak, I., ... & Chew, C. K. (2020). Effect of an intensive patient educational programme on the quality of bowel preparation for colonoscopy: a single-blind randomised controlled trial. BMJ open gastroenterology, 7(1), e000376. [CrossRef]
- Alvarez-Gonzalez, M. A., Sánchez, M. Á. P., Cabredo, B. B., García-Rodríguez, A., Larramona, S. F., Nogales, O., ... & Gimeno-García, A. Z. (2020). Educational nurse-led telephone intervention shortly before colonoscopy as a salvage strategy after previous bowel preparation failure: a multicenter randomized trial. Endoscopy, 52(11), 1026-1035. [CrossRef]
- Park, J., & Kim, T. O. (2019). How can we achieve good compliance for bowel preparation?. Clinical endoscopy, 52(1), 3-4. [CrossRef]
- Kang, X., Zhao, L., Leung, F., Luo, H., Wang, L., Wu, J., ... & Guo, X. (2016). Delivery of instructions via mobile social media app increases quality of bowel preparation. Clinical Gastroenterology and Hepatology, 14(3), 429-435. [CrossRef]
- Wang, S. L., Wang, Q., Yao, J., Zhao, S. B., Wang, L. S., Li, Z. S., & Bai, Y. (2019). Effect of WeChat and short message service on bowel preparation: an endoscopist-blinded, randomized controlled trial. European Journal of Gastroenterology & Hepatology, 31(2), 170-177. [CrossRef]
- Desai, M., Nutalapati, V., Bansal, A., Buckles, D., Bonino, J., Olyaee, M., & Rastogi, A. (2019). Use of smartphone applications to improve quality of bowel preparation for colonoscopy: a systematic review and meta-analysis. Endoscopy international open, 7(02), E216-E224. [CrossRef]
- Gimeno-García AZ, Federica Benítez-Zafra, Nicolás-Pérez D, Hernández-Guerra M. Colon Bowel Preparation in the Era of Artificial Intelligence: Is There Potential for Enhancing Colon Bowel Cleansing? Medicina-lithuania. 2023;59(10):1834-1834.
- Barakat-Johnson, M., Jones, A., Burger, M., Leong, T., Frotjold, A., Randall, S., ... & Coyer, F. (2022). Reshaping wound care: Evaluation of an artificial intelligence app to improve wound assessment and management amid the COVID-19 pandemic. International Wound Journal, 19(6), 1561-1577. [CrossRef]
- Zhu, Y., Zhang, D. F., Wu, H. L., Fu, P. Y., Feng, L., Zhuang, K., ... & Zhou, P. H. (2023). Improving bowel preparation for colonoscopy with a smartphone application driven by artificial intelligence. NPJ Digital Medicine, 6(1), 41. [CrossRef]
Figure 1.
The content of the ColonClean app.
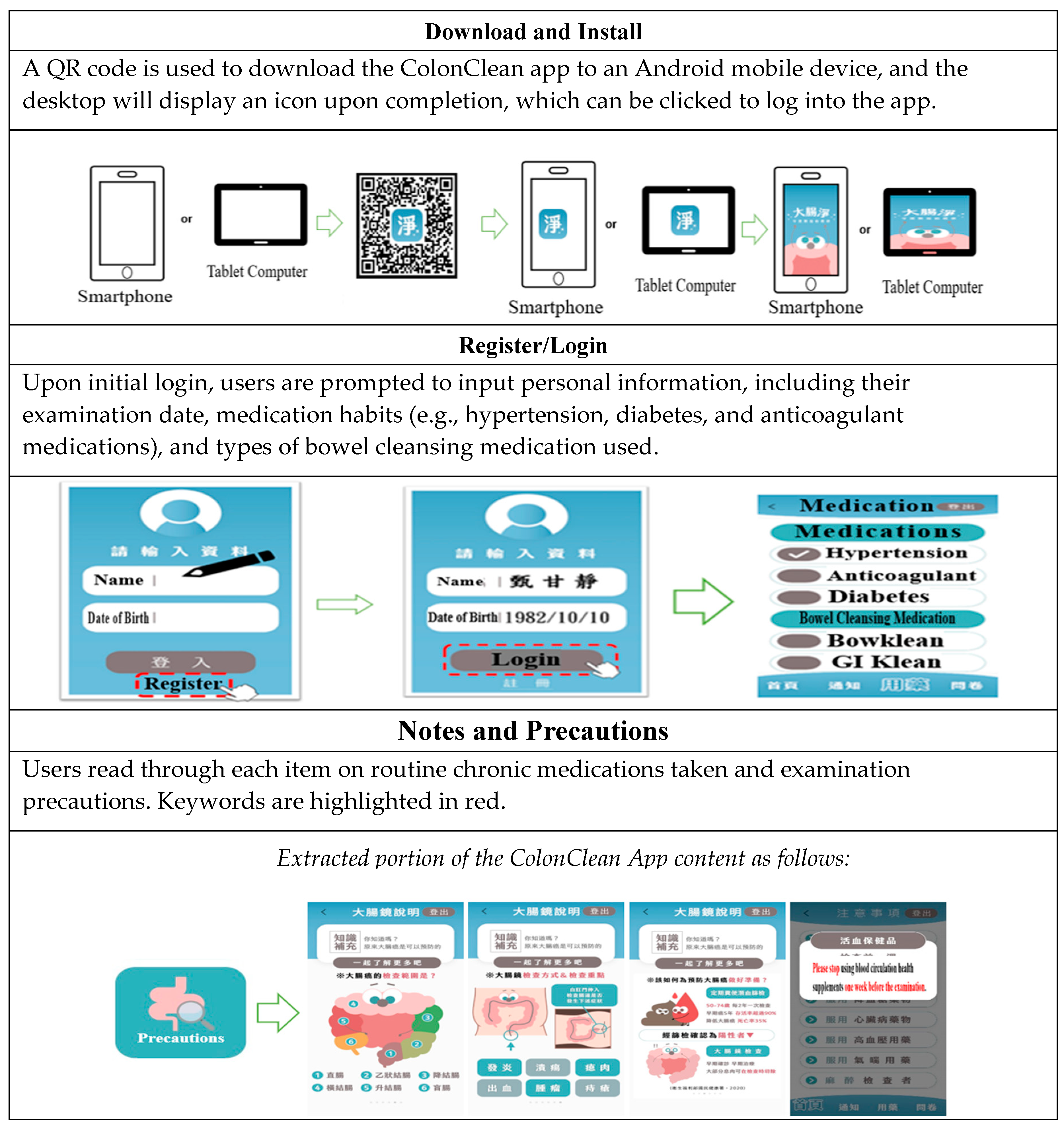
Figure 2.
Endoscopists’ assessment of bowel preparation quality.
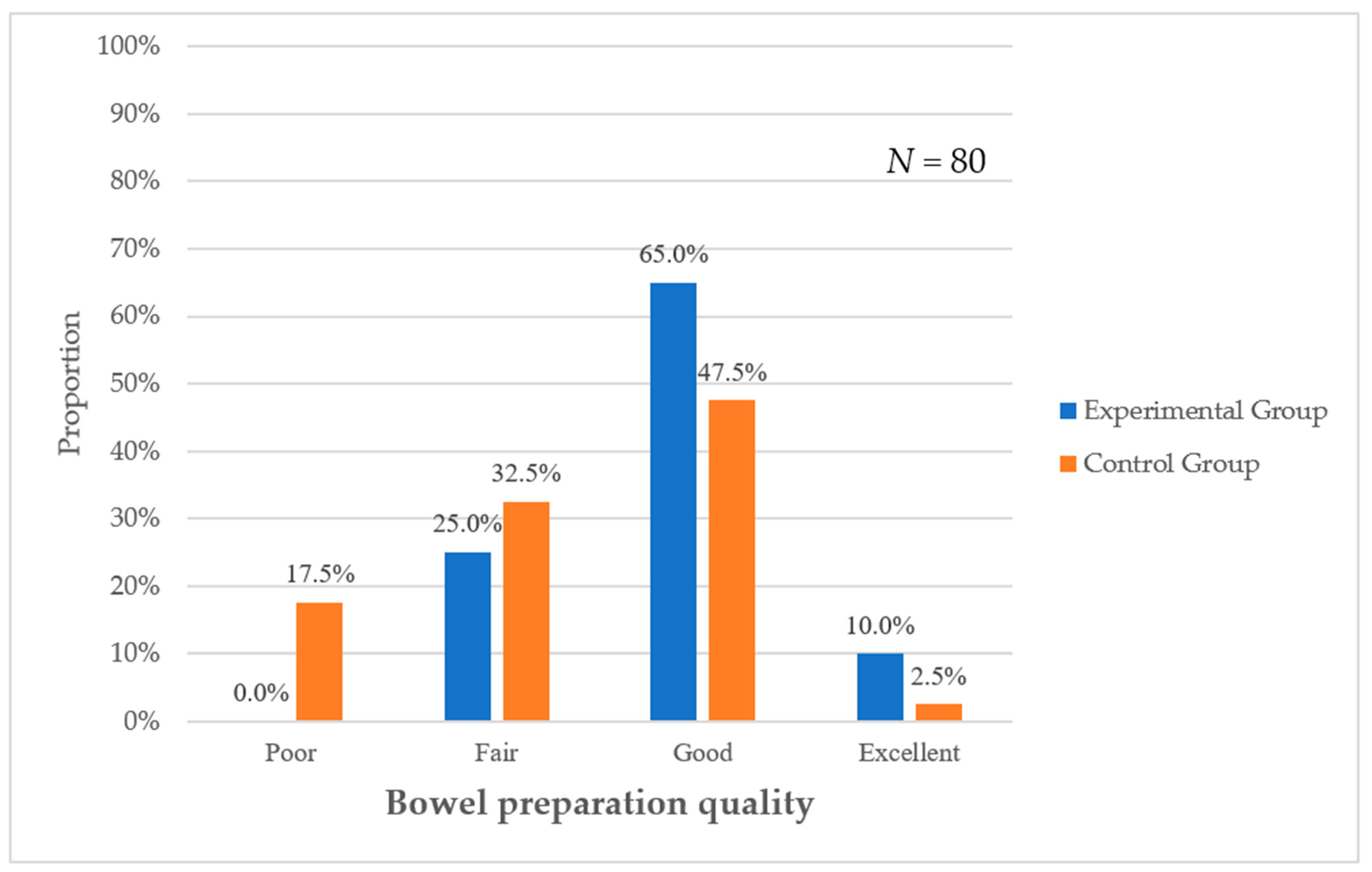

Table 1.
Participants’ basic characteristics (N = 80).
| Variable | All samples (N = 80) |
Group | pa | ||||
| Experimental (n = 40) |
Control (n = 40) |
||||||
| Male, n (%) | 41 (51.2) | 17 (42.5) | 24 (60) | 0.12 | |||
| Age (years), n (%) | 0.58 | ||||||
| 20–30 | 2 (2.5) | 2 (5.0) | 0 (0.0) | ||||
| 31–40 | 11 (13.8) | 5 (12.5) | 6 (15.0) | ||||
| 41–50 | 17 (21.3) | 6 (15.0) | 11 (27.5) | ||||
| 51–60 | 24 (30.0) | 15 (37.5) | 9 (22.5) | ||||
| 61–70 | 10 (12.5) | 7 (17.5) | 3 (7.5) | ||||
| 71–80 | 16 (20.0) | 5 (12.5) | 11 (27.5) | ||||
| BMI, mean ± SD | 23.79 ± 3.97 | 22.58 ± 3.22 | 25.0 ± 4.72 | 0.02* | |||
| Education level, n (%) | 0.16 | ||||||
| Elementary school | 6 (7.5) | 3 (7.5) | 3 (7.5) | ||||
| Junior high school | 8 (10.0) | 2 (5.0) | 6 (15.0) | ||||
| High school/ vocational |
17 (21.3) | 6 (15.0) | 11 (27.5) | ||||
| College/university | 36 (45.0) | 22 (55.0) | 14 (35.0) | ||||
| Research institute or above | 13 (16.3) | 7 (17.5) | 6 (15.0) | ||||
| Married, n (%) | 61 (76.25) | 31 (77.5) | 30 (75.0) | 0.23 | |||
| Constipated, n (%) | 17 (21.25) | 10 (25) | 7 (17.5) | 0.27 | |||
| Abdominal surgery, n (%) | 28 (35.0) | 13 (32.5) | 15 (37.5) | 0.64 | |||
| Diabetes, n (%) | 12 (15.0) | 5 (12.5) | 7 (17.5) | 0.54 | |||
| Family history of colorectal cancer, n (%) |
14 (17.5) | 7 (17.5) | 7 (17.5) | 1.00 | |||
| Colonoscopy experience, n (%) |
48 (60.0) | 26 (65.0) | 22 (55.0) | 0.51 | |||
a Comparison between the experimental and control groups. Note: *, p < 0.05.
Table 2.
Frequency and percentage of endoscopists’ assessment of bowel preparation quality by group.
Table 2.
Frequency and percentage of endoscopists’ assessment of bowel preparation quality by group.
| Group | P | |||||
| Experimental | Control | |||||
| n | % | n | % | 0.016* | ||
| Endoscopist’s judgment of bowel preparation quality | Poor | 0 | 0.0 | 7 | 17.5 | |
| Fair | 10 | 25.0 | 13 | 32.5 | ||
| Good | 26 | 65.0 | 19 | 47.5 | ||
| Excellent | 4 | 10.0 | 1 | 2.5 | ||
| Total | 40 | 100.0 | 40 | 100.0 | ||
Note: *, p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



