
Submitted:
30 April 2024
Posted:
02 May 2024
You are already at the latest version
Abstract
Lyme disease is a highly prevalent tick-borne infection caused by Borrelia burgdorferi spirochetes in North America and Eurasia. Diagnosis of the early disease remains difficult with the currently approved serological tests in the absence of noticeable tick bite or erythema migrans due to presentation of non-specific symptoms and the absence of antibodies early in infection. Furthermore, it is difficult to distinguish persistence of disease and reinfection in the endemic regions. If not treated early, infection spreads throughout the body and affects most organs with disease manifestations including arthritis, musculoskeletal pain, neuroborreliosis and acrodermatitis chronicum atrophicans. Although most patients recover after antibiotic treatment, ~10-12% of show recurrence of symptoms known as post-treatment Lyme disease syndrome (PTLDS). Various causes of PTLDS are not well-defined; however, the spirochete persisters, antigenic debris, dysregulation of immunological response in individuals or a combination of these factors are proposed to result in continuation of Lyme disease manifestations. Based on these considerations, this review highlights currently employed treatment approaches with antimicrobials and vaccines being tried for prevention of B. burgdorferi infection. We also summarize combinatorial approaches that could be employed to alleviate symptoms to improve the quality of life of the individuals suffering from long Lyme disease.
Keywords:
Lyme disease
; Borrelia burgdorferi
; Treatment
; antimicrobials
; Post-treatment Lyme disease syndrome
; PTLDS
INTRODUCTION
Lyme disease is the most common vector borne disease, especially in the United States and Europe. It is caused by a spirochete group, Borrelia burgdorferi sensu lato, and approximately half a million cases per year are reported just in the United States [1]. The incidence of Lyme disease is on the rise due to a combination of factors like increased habitat range of the main vectors, Ixodes scapularis tick in the USA and I. pacificus in Europe, intersection of human domiciles with tick or animal host and extended seasonal activity caused by climate change, amongst others [2]. The average cost for addressing this disease to the US economy is estimated to be $3 billion in direct cost with even greater losses owing to the lost work hours [3].
Broad spectrum antibiotics such as amoxicillin, ceftriaxone, cefuroxime axetil and doxycycline are often used prophylactically for treatment of early to late Lyme disease at present, but this sometimes results in considerable adverse effects in patients due to the disruption of host microbiome and the selection for resistance in off-target bacteria [4,5]. Moreover, there remains concern among some scientists and researchers that some of these antibiotics do not fully eliminate B. burgdorferi infections [6,7,8,9]. The most concerning fact is that ~10-12% of the infected individuals treated with antibiotics show recrudescence of symptoms referred to as post-treatment Lyme disease syndrome (PTLDS), thus revealing the unmet need for the development of therapeutic agents against potential persistent forms of B. burgdorferi and to diminish the persistent subjective symptoms. In addition, prominent surface antigen(s) as vaccine are currently in the clinical trials to prevent B. burgdorferi infection. For instance the vaccine candidate VLA15 has shown great promise in the second clinical trial phase [10,11] . We review here the current treatment approaches used and potential perspectives for developing combination of existing or novel antimicrobials with alternative treatment approaches to alleviate suffering of patients with long Lyme disease.
I. Treatment Recommendation for Lyme disease
Lyme disease presents a significant health concern globally, particularly in the endemic regions of Europe and North America where infected ticks are prevalent. As the leading tick-borne illness and the fastest-growing vector-borne disease in the United States, Lyme disease poses a substantial burden on public health systems and individuals in the endemic regions. It has been noted that all the 50 states of USA have B. burgdorferi-carrying ticks [12], which are maintained in nature by mice, deer, rabbits, squirrels as well as affect pet dogs and cats. Despite increased awareness and efforts to control tick populations, the incidence of Lyme disease continues to increase, necessitating effective treatment strategies to mitigate its impact on humans and pets. Failure to promptly administer treatment usually results in disseminated infection to various organs and the onset of severe and persistent complications [13,14]. Various studies have indicated that a prolonged duration between symptom initiation and therapeutic intervention, i.e., time-to-treatment correlates with long-term unfavorable outcomes in Lyme disease patients [15,16,17,18].
- A. Prevention, diagnosis and treatment for acute Lyme disease
Following exposure to an infected tick, Lyme disease symptoms appear within a few days to weeks. There are some symptoms which are associated with this stage, although all individuals may not experience the early signs [19]. The primary symptom of acute Lyme disease is frequently a unique rash known as erythema migrans. This rash commonly emerges at the position of tick bite and gradually expands over time, often resembling a bull's-eye; however, every infected person does not develop erythema migrans lesion. Other symptoms commonly associated with acute Lyme disease include non-specific flu-like symptoms, including chills, fever, fatigue, muscle and joint discomfort, headache, and swollen lymph nodes. Some individuals may also face neurological symptoms like meningitis, facial paralysis, or nerve pain radiating from the spine. Rarely, acute Lyme disease can lead to heart-related symptoms such as palpitations, chest pain, or heart block [20]. Acute Lyme disease is usually diagnosed depending upon clinical symptoms and a history of probable tick exposure. United States Food and Drug Administration (FDA) has approved a two serological test regime that consist of immunoassays (EIA) using two enzyme, that can be run in sequence or simultaneously [21] or Western blot test after EIA to identify antibodies against B. burgdorferi [22,23,24].
- 1. Post-exposure prophylaxis following tick bite and erythema migrans detection
The risk of contracting B. burgdorferi and other tick-borne pathogens can be reduced in most effective way by taking steps to prevent tick exposure [25]. This can be accomplished by conducting daily tick checks, wearing protective clothing, using tick repellents, and quickly removing any ticks observed on the body [26]. The routine use of serologic testing or antimicrobial prophylaxis after a tick bite is not worthwhile for preventing Lyme disease. However, under specific conditions, it might be appropriate to consider administering a single dose of doxycycline, particularly when the local infection rate with B. burgdorferi is higher than 20% and the tick has remained attached to skin for more than 36 hours. In such cases, treatment should be initiated within 72 hours of tick removal. Prophylaxis after I. pacificus bite is generally unnecessary unless higher infection rates are documented [27]. Detection by the healthcare providers proficient in identifying ticks, especially engorged ones, can be helpful. Individuals who have removed ticks should be monitored for up to 30 days for signs of tickborne diseases and are recommended to seek medical attention [28,29,30].
Rebman and coworkers studied the time to treatment effective in early Lyme disease [31]. They divided the patients into two groups. The 1st group included the participants who displayed erythema migrans and the 2nd group of patients who initially experienced flu like symptoms. Multivariate analyses revealed a significant reduction (22%) in treatment initiation time for erythema migrans participants than those participants who had reported to experience various subjective symptoms initially. This study suggests that preliminary presentation of symptoms significantly affects time-to-treatment in early Lyme disease [31]. Overall, timely diagnosis and appropriate treatment plays a main role in preventing the progression to advanced stages of the Lyme disease [32]. Patients who receive timely and suitable antibiotic therapy in the early phases generally experience fast and complete recovery. The treatment regimens outlined in Table 1 are designed specifically for managing the acute Lyme disease; however, modifications to these protocols might be needed depending on factors like medical history, age, underlying health conditions, susceptibility to various allergies or pregnancy [30,33].
Adults with erythema migrans of early Lyme disease are usually treated with a 14-day regimen of either amoxicillin (500 mg three times daily), doxycycline (100 mg twice daily), or cefuroxime axetil (500 mg twice daily). The treatment duration may range from 14 to 21 days for amoxicillin or cefuroxime axetil and 10 to 21 days for doxycycline. These antibiotics have shown significant effectiveness in managing erythema migrans and its related symptoms in numerous studies [30,34,35]. Doxycycline is effective but not advised for children under 8 years of age, in pregnant women and during lactation. For these individuals the recommended antibiotics include cefuroxime axetil or amoxicillin.
The efficacy of doxycycline as treatment was reported in a study involving 607 participants, with 93% of them receiving doxycycline in courses lasting 11, 11-15, or 16 days. Less than 1% of patients experienced treatment failure, and over half of the cases were due to reinfection [36]. Doxycycline als has rare but possible side effects, including esophageal perforation, photosensitivity and pseudotumor cerebri [46]. A study comparing the effectiveness of doxycycline and cefuroxime in treating adult patients with erythema migrans found that 45 out of 51 patients receiving doxycycline and 51 out of 55 individuals taking cefuroxime exhibited satisfactory outcomes [47]. Another study compared the efficacy of doxycycline and cefuroxime in treating children with erythema migrans and documented that 92% of the children treated with cefuroxime experienced complete symptom resolution, compared to 67% of those treated with doxycycline [43].
There is ongoing debate and discussions over the years about the ideal length of antibiotic treatment for Lyme disease [36,48,49,50]. Shorter courses of antibiotics are often preferred due to lower costs, decrease in the risk of side effects that also minimizes the chance of developing resistance. For example, research on doxycycline's effectiveness in treatment indicated that a 7-day course of antibiotics might be sufficient. This finding is important for consideration by clinicians who may be reluctant to prescribe shorter antibiotic courses and have concerns that it may not fully clear the infection [51]. It is important to note that the International Lyme and Associated Diseases Society proposes a 21-day regimen of doxycycline for patients exhibiting erythema migrans [52].
Macrolide antibiotics are not typically recommended as the first choice for treating Lyme disease due to their reduced efficacy compared to primary antimicrobials mentioned above [53]. They can still be considered for treatment of patients who are intolerant or are unable to take first-line antibiotics; however, these patients need to be carefully monitored to assess the success of treatment and resolution of clinical symptoms [54,55,56]. First generation cephalosporins, such as cephalexin, lack efficacy in treating Lyme disease [57]. In cases where distinguishing erythema migrans from bacterial cellulitis poses a challenge, treatment with cefuroxime axetil or amoxicillin-clavulanic acid is considered suitable. Early Lyme disease patients who don’t have neurological involvement or advanced atrioventricular heart block are not advised to receive ceftriaxone [58] because ceftriaxone poses a greater risk of adverse effects compared to other orally administered antimicrobials [30].
- 2. Treatment of other complications in early stages of Lyme disease
The effect of B. burgdorferi on the nervous system was reported in approximately 40% of patients examined [59]. Neurological involvement often extends across multiple regions of the nervous system. Symptoms may include headaches, sensitivity to light, abnormal sensations (dysesthesias), stiffness in the neck, and irritability. Progression of the disease during its early stages commonly presents with neurological manifestations such as meningitis, cranial neuritis, and radiculoneuritis, either independently or in conjunction [59]. In Europe, meningoradiculoneuritis also known as Garin-Bujadoux-Bannwarth syndrome, is a frequent appearance of acute Lyme borreliosis in adults, typically occurring after erythema migrans signs [60,61,62]. In children, the condition often manifests as isolated meningitis without radicular symptoms [60,63,64,65,66]. Central nervous system involvement is not common and occur in around 4% of Lyme neuroborreliosis cases [60,61].
The investigation of early Lyme neuroborreliosis was documented in eight randomized controlled trials (RCTs) and eight prospective cohort studies that examined the efficiency of antibiotic treatment duration [67]. For RCTs, antibiotics were generally prescribed for 14 to 21 days, with one trial extending the duration to 100 days [67]. In contrast, prospective cohort studies employed treatment durations ranging from 10 to 30 days, though these durations were not consistently specified across various studies. A direct comparison between different lengths of treatment was not documented in any of these studies. The primary endpoint that focused on neurological residual symptoms after treatment showed significant variability ranging from 10% to 66% in RCTs and from 7% to 44% in prospective cohort studies [68]. The inconsistencies in these results were due to non-standardized survey methods, diverse assessment timeframes, and different patient self-assessment approaches. Interestingly, a controlled study involving 152 patients with Lyme disease provided indirect evidence that extending treatment beyond three weeks offered no additional benefits [67]. About 90% of the patients experienced excellent or very good outcomes after one year, regardless of the duration of their treatment [67]. The study highlighted the lack of scientific support for extending antibiotics prescription beyond the recommended 14-day treatment for early Lyme neuroborreliosis [69].
Selection of the antibiotic and understanding its associated effects is very important for an effective treatment strategy. Clinical trials have evaluated the efficacy of doxycycline as well as β-lactam antibiotics, including ceftriaxone, penicillin G, and cefotaxime for Lyme neuroborreliosis treatment. These antibiotics are known for their ability to effectively penetrate the cerebrospinal fluid (CSF). A meta-analysis of data showed that oral doxycycline and intravenous (IV) β-lactam antibiotics had comparable efficacy in improving neurological symptoms at both 4-12 months and even after 12 months of infection [68]. These results are supporting an earlier meta-analysis done by American researchers [70]. A subsequent study of RCT investigated secondary endpoints, such as fatigue and quality of life, and found no significant differences between patients treated with doxycycline or β-lactam antibiotics after a 30-month period [71,72]. Additionally, two RCTs found no disparity between these antibiotic regimens regarding cerebrospinal fluid pleocytosis [68,72,73]. Likewise, there was no significant difference between the two treatments in in terms of reported side effects like nausea, redness of the skin, diarrhea, constipation, dizziness and thrombophlebitis [67,74]. Severe side effects such as cholecystitis, stomatitis, duodenal ulcers, and allergic reactions were significantly rare in these studies.
Two RCTs compared cefotaxime and penicillin for treating neurological Lyme disease and reported that cefotaxime caused a significant reduction in residual neurological symptoms between 4 to 12 months, while penicillin resulted in fewer side effects [75,76]. The most common reported side effects were Herxheimer-like reactions and mild diarrhea. However, due to the limited reporting of major side effects including allergic reactions, shock and colitis, and the significant risk of bias in both studies, absolute recommendation for a single treatment approach could not be made [68]. In fact, there is no reliable or analyzable data on the effectiveness of antibiotic combination therapy with chloroquine, carbapenems, or metronidazole for treating the condition [68].
Lyme carditis symptoms usually appear within a few days to up to a month (averaging 21 days) after the onset of the infection. This condition is most commonly observed in the summer to fall months [77,78,79]. Recent studies suggest that Lyme carditis incidence may be lower than previously estimated 4-10% of the untreated patients [79,80]. The highest incidence of Lyme carditis was observed in childhood and middle age, with young adult and middle-aged men being most affected. Although the reason for predominance among male population remains unclear, more severe exposure or higher susceptibility could be contributing factors [80]. Cardiac involvement in Lyme disease can manifest in various forms, most commonly as atrioventricular nodal block which can rapidly progress to complete heart block [77,81,82]. Other manifestations include atrial and ventricular arrhythmias, sinus node and distal conduction system involvement [83,84,85,86]. The infection of B. burgdorferi can also exhibit as pericarditis and acute myocarditis, which may lead to ventricular dysfunction [87]. Most individuals recover with supportive treatment and antibiotic therapy, there have been cases where the infection had fatal consequence [79]. It is still unclear whether an infection with B. burgdorferi can cause chronic cardiomyopathy [88,89,90].
There is a lack of high-quality trials for specifically evaluation of antibiotic treatment options for Lyme carditis, including choices of medication, methods of administration, and treatment duration. Current recommendations are based on varied studies with small patient groups for Lyme carditis, as well as on observational data [67,91,92]. A randomized controlled trial assessed the efficacy of oral doxycycline versus IV ceftriaxone in acute B. burgdorferi infection patients, where 6.5% of participants had carditis [91]. Authors of this study reported a comparable efficacy of these antibiotic treatments, although IV ceftriaxone was associated with a notably higher incidence of gastrointestinal side effects, while doxycycline was linked to a greater occurrence of dermatological adverse events. Thus, carditis can be treated like the other manifestations of Lyme disease.
Patients diagnosed with myopericarditis or atrioventricular heart block in early stages of disease are usually cured with a 14-day course of oral or IV antibiotics. Hospitalization is advised for symptomatic patients showing with chest pain, dyspnea or syncope [77]. Continuous monitoring is advised, particularly for patients with second or third level atrioventricular block, or those with prolonged PR intervals exceeding 30 milliseconds, as the severity of blockage may rapidly worsen [77]. Hospitalized patients were initially treated with IV antibiotics such as ceftriaxone. Those who require a temporary pacemaker should consult a cardiologist for specialized management [93,94]. Once the advanced heart block resolves, it was recommended that pacemaker usage may cease, and patients can transition to oral antibiotics for completion of therapy and outpatient management [94].
- 3. Progression of Lyme disease symptoms post-antibiotic therapy
According to many studies neurological symptoms were improved within weeks to months after receiving antibiotic treatment course of 10–14 days. For instance, a prospective study involving 77 Bannwarth's syndrome participants revealed that 88% of individuals experienced positive outcomes 12 months post-treatment [95]. Consistently, previous cohort studies showed encouraging results, with 90.6% symptom-free patients in three months after antibiotic therapy, and 95.2% showed very good outcomes after a 33 months median follow-up [60,96]. Another cohort study, which assessed predominantly early Lyme neuroborreliosis, found that 88% of patients' daily activities remained unaffected after a five-year observation period [97]. A systematic review of 687 patients with confirmed Lyme neuroborreliosis revealed the following post-antibiotic treatment neurological symptoms: cranial nerve paresis (3.6%), sensory disorders (5.24%), extremity paresis (2.33%), pain (2.77%), and unsteady dizziness/gait/ataxia (2.62%) [98].
In the early stages of Lyme disease, adults with acute neurological symptoms such as meningitis or radiculopathy are advised to undergo treatment with IV ceftriaxone. The recommended dosage was 2g administered once daily for a period of 14 days (range: 10–28 days) [73]. Penicillin G or cefotaxime could also be used as acceptable alternatives for parenteral therapy [75]. For patient’s intolerant to β-lactam antibiotics, oral doxycycline given for 10–28 days at 200–400mg/day divided in 2 doses was considered sufficient. Children under 8 years old can be treated with ceftriaxone intravenously, or with cefotaxime or penicillin G at appropriate doses. Oral doxycycline has also shown success in this age group. Though antibiotic therapy may not accelerate seventh cranial nerve palsy resolution, it's essential to prevent further complications [30].
- B. Late-stage Lyme disease
Late Lyme disease refers to the advanced disseminated phase that occurs when the infection is left untreated or inadequately treated during the early stages. This stage typically manifests weeks, months, or even years after the initial tick bite. Late Lyme disease presents a range of symptoms that may affect various body systems, including the joints, nervous system, and heart. Managing late-stage Lyme disease poses challenges due to diverse and sometimes debilitating symptoms, highlighting the importance of early detection and prompt treatment to prevent progression to this stage. We have summarized various treatment approaches for acute to late Lyme disease currently used in Figure 1.
- 1. Lyme arthritis and neuroborreliosis
It was believed initially that arthritis occurred in 60% of untreated cases of erythema migrans [99]; however, surveillance data over several years has shown that arthritis is presented in ~30% of cases per year. It is important to know that arthritis experiencing Lyme disease patients may actually be lower in percentage, as sometimes joint pain is mistakenly identified as arthritis (joint inflammation). Early RCTs have shown that IV antibiotics are more efficient in Lyme arthritis (LA) treatment in comparison to placebo [100,101], and two other studies reported that IV cephalosporins were better than IV penicillin in resolving arthritis symptoms [76,102]. A randomized controlled trial showed that about 90% of both children and adults patients saw their arthritis resolve within 1–3 months when oral doxycycline (100 mg twice daily) or amoxicillin plus probenecid (500 mg every 6 hours) was given [103,104]; however, difference between the treatment groups in the incidence of Lyme neuroborreliosis was not statistically significant. The doxycycline dosage regimen in this trial differed from the standard regimen for Lyme neuroborreliosis, which is in general orally given 200 mg/day. Although the results were not significant, a tendency of gastrointestinal unpleasant events and allergic reactions was higher in amoxicillin group. There are not any studies directly comparing the effectiveness of cefuroxime axetil with other oral antibiotics or placebo in treating LA. Therefore, the effectiveness of cefuroxime axetil is inferred from studies that have investigated its success in treating Lyme disease in early stages and preventing late-stage manifestations.
Oral antibiotics offer several advantages over IV antibiotics, including ease of administration, fewer serious complications, and lower cost. Given their equivalent effectiveness, this approach using amoxicillin, doxycycline, or cefuroxime axetil antibiotic treatment of LA for 28 days is suggested to be effective. In late-stage Lyme disease, adults showing neurological involvement of either the peripheral or central nervous system require careful management. Although rare, some patients who received oral antibiotics for treatment later exhibited clinical signs of neurological disease [103,104] likely due to the dosing regimen and choice of antibiotic. Patients who develop neuroborreliosis despite receiving oral treatment may require IV therapy with ceftriaxone for a period of 2 to 4 weeks, or alternatives such as cefotaxime or penicillin G, and should undergo a neurological evaluation, which may include a lumbar puncture [30]. For patients who have confirmed arthritis and neurological disease, parenteral therapy using ceftriaxone, cefotaxime, or penicillin G was recommended [30]. If joint swelling continued after an initial course of oral therapy, another round of oral antibiotics or IV ceftriaxone could be undertaken. Symptomatic treatment with non-steroidal anti-inflammatory drugs or corticosteroid injections can be considered if arthritis persists despite antimicrobial therapy [30].
- 2. Acrodermatitis chronica atrophicans (ACA)
ACA is a dermatologic appearance of late-stage Lyme disease usually associated with B. afzelii [105] and usually manifests as a chronic, progressive skin disorder marked by skin atrophy, discoloration, and fibrosis, primarily affecting the extremities such as the hands and feet. ACA is more commonly observed in endemic regions of Lyme disease in Europe, particularly in central and eastern countries. The condition is often associated with a long-standing infection, as it tends to develop months to years after initial exposure to Lyme spirochetes. Display of ACA could indicate the chronic nature of Lyme disease and the need for appropriate management and follow-up [30]. ACA is usually curable with a 21 day régime of commonly used antibiotics for erythema migrans including doxycycline, amoxicillin, and cefuroxime axetil; however, a controlled study to compare the effectiveness of oral versus parenteral antibiotic therapy in treating ACA is needed to establish precise treatment regimen [30]. Erythema migrans typically requires treatment for two weeks and acrodermatitis for a minimum of four weeks [106].
- 3. Treatment of pregnant women
There has been an ongoing discussion regarding the potential transmission of Borrelia spp. from mother to fetus since the 1980s. Prior to the recognition of Lyme disease, Lampert et al. [107] reported cases in 1975 of infantile illnesses that showed clinical syndromes similar to Lyme disease. One of these cases described an infant who initially displayed an erythema marginatum rash as a newborn, which later developed into symptoms such as a painful and swollen right knee over a span of several months [107].
The Infectious Diseases Society of America issued guidelines depending upon evidence for Lyme disease treatment [108]. The best antimicrobial therapy is still not fully established for pregnant women experiencing Lyme disease. Current recommendations for treatment of pregnant women are the same as non-pregnant individuals, based on their disease appearance; however, certain commonly used drugs, such as doxycycline, are not suitable for pregnant women. Although more research is necessary to evaluate the safety of doxycycline during pregnancy and breastfeeding [109,110,111]. Amoxicillin and third generation cephalosporins are the preferred treatment options during pregnancy, as they are considered safe. The first-generation cephalosporins should be avoided because they have been found ineffective in both laboratory and clinical settings [58].
Timely treatment is essential for gestational borreliosis. Early localized infections are usually managed with a 14–21 day course of oral amoxicillin, taken at a dosage of 500 mg three times a day [108,112]. For patients who are allergic to amoxicillin, cefuroxime axetil at a dosage of 500 mg twice daily could be used as replacement. When neurological complications occur, IV ceftriaxone (2 gm daily) or cefotaxime (2 gm three times daily) is recommended for 14 to 28 days. The oral regimen mentioned above can only be adequate in cases where only facial nerve palsy is observed with no signs of neuroborreliosis. Arthritis requires extended treatment with oral regimen lasting 30–60 days or IV agents, depending on the severity of the condition. For first-degree atrioventricular block, oral treatment is often sufficient while more severe cardiac appearances require IV therapy and probably cardiac monitoring. The women who are unable to tolerate amoxicillin or cefuroxime axetil may consider using macrolide antibiotics as supported by findings from large serological evaluations [113,114]. The existing evidence does not support routine treatment of women who test positive for B. burgdorferi antibodies at the time of conception.
A review encompassing data from studies involving mothers who received antimicrobial treatment during pregnancy [115], and those who received no treatment [113,116] found a significantly lower risk of adverse events when mothers received treatment during pregnancy, with IV antimicrobial therapy yielding the lowest adverse outcomes. Conversely, the use of oral antimicrobials was associated with three times greater unfavorable outcomes, while the risk was six times higher in the untreated mothers. Additional studies without specified treatment protocols further supported a trend towards reduced (0.5-1.3%) adverse outcomes with antimicrobial treatment among large cohorts [117,118], while adverse outcomes among untreated mothers was found to be 30 times greater.
Although the rate of adverse outcomes was reduced by using antimicrobials, the best strategy to prevent Lyme disease during pregnancy is to avoid exposure to ticks and prompt removal can reduce the risk of transmission [28,119,120]. The use of tick repellents like DEET is effective tick bite prevention measure and has no known risk to the developing fetus [121,122]. Some practitioners prescribe amoxicillin for pregnant women, especially with prolonged tick attachment (>48 hours) in highly endemic regions. Careful monitoring for symptoms of tick-borne illness is required if prophylactic antibiotics aren't given after tick exposure.
II. Contribution of host and bacterial factors in Lyme disease
- A. Human genetic factors affecting Lyme disease
A recent human genome wide study explored phenotypic and genetic risk factors to identify the most prominent genetic variations association with susceptibility to Lyme disease [123]. The SCGB1D2 is usually present majorly in the skin, sweat, and other secretions. Interestingly, two known variants and an unknown common missense mutation located in the gene encoding secretoglobin family 1D member 2 (SCGB1D2) proteins were noticed to enhance Lyme disease susceptibility. The in vivo inhibition of B. burgdorferi growth was observed after recombinant SCGB1D2 treatment in murine infection model. Thus, results of this study suggested that SCGB1D2 protein could be a host defense factor that protects against Lyme disease.
The immune response dysregulation that tilts the balance towards the production of proinflammatory cytokines plays critical role in persistence of symptoms or PTLDS [124,125,126,127,128]. For instance, in a SNP microarray analysis of 48 LA patients, arthritis resolved in 22 patients following antibiotic treatment (responsive) while 26 patients exhibited persistent arthritis after antibiotic therapy for 2-3 months (refractory). Between these groups, about 1200 SNPs varied in frequency (B allele frequency >0.3). The analysis of principal component of 28 SNPs showed total separation between patients with refractory vs responsive course, implicating human genetic variation in influencing Lyme disease severity. Furthermore, top 10 SNPs that varied in frequency amongst the patients in refractory and responsive LA groups were correlated with the levels of crucial inflammatory mediators (IFNγ and IL-17) and anti-inflammatory cytokine IL-10 in their serum. To evaluate the influence of SNPs on immune or clinical phenotype, the frequency of the SNPs in patients was correlated with the duration of arthritis. Together these results reflected association of certain human genotype mutations with persistent arthritis and Lyme disease. Although, the mechanisms that influence mutation and the exact outcome of these SNPs were not determined.
Innate immune responses are equally stimulated by Toll-like receptors (TLRs). On the cells surface, TLR1 forms heterodimer with TLR2 to recognize lipoproteins and triacyl-peptides. Studies have shown that TLR1 polymorphism enhanced lipopeptide response, important during B. burgdorferi infection and results in increased Th1 inflammatory response [129,130].
- B. Essential components of metabolic pathways in B. burgdorferi
Genomic studies identify essential genes, enzymes, and metabolic pathways necessary for survival in B. burgdorferi that are absent, or are significantly different in the host, can be promising targets for drug development. For instance, computational in silico genome scale modelling of B. burgdorferi’s metabolism (iBB151) was constructed and the map was used to envisage important enzymatic reactions and genes whose inhibition affected bacterial growth [131]. The model described 208 enzymatic reactions of which 77 were predicted to be essential for growth targeting mevalonate pathway, alanine racemase, cell-wall synthesis, aminoacyl-tRNA ligases, adenosylhomocysteine nucleosidase and glutamate racemase pathways. The predicted essential reactions from iBB151 (B. burgdorferi constructed model) were compared with E. coli (iML1515) and Staphylococcus aureus (iYS854) reaction models to identify enzymes whose inactivation is specifically lethal to B. burgdorferi. Based upon these reactions, 28 possible narrow spectrum drug targets of five major pathways (Folates, Glycolysis, Nucleotides Lipids and Mevalonate pathway) specifically in B. burgdorferi were predicted. Small enzyme inhibitor molecules were repurposed and used to validate the predicted hits as drug targets. Among these, four were experimentally assessed for inhibition of growth in each of the three bacterial species, B. burgdorferi, E. coli and S. aureus. Theophylline and premetrexed were found to be uniquely critical for targeting pyridoxal kinase and serine hydroxymethyl transferase enzymes, respectively in B. burgdorferi and demonstrated B. burgdorferi growth inhibition in vitro.
Inhibition of metal acquisition and homeostasis by preventing metal uptake and utilization is a novel target for antimicrobial development. Manganese for instance, is a crucial co-factor for several protein and enzyme functions including superoxide dismutase machinery that protects B. burgdorferi from intracellular superoxide. Through a combination of in silico protein structure prediction and molecular docking, a single known Mn transporter, metal transporter A (BmtA) in Borrelia was targeted. Subsequent screening of FDA approved libraries for potential compounds that could bind to the BmtA predicted structure with great affinity led to the identification of desloratadine and Yhohimbine which inhibited Borrelicidal activity in vitro. Treatment of the spirochaete with desloratadine led to significant loss of intracellular Mn specifically and severe destruction of the bacterial cell wall [132].
In most pathogenic organisms, reactive oxygen species (ROS) generated by host immune system affect iron-sulphur clusters, DNA and polyunsaturated lipids and cysteinyl residues, causing growth inhibition and cell death. B. burgdorferi lacks intracellular iron and the DNA is unlikely the target for cell destruction by ROS via Fenton reaction. By challenging B. burgdorferi B31A3 cultures with oxidants (H202 or t-butyl hydroperoxide) Boylan and colleagues observed in vitro growth inhibition of spirochaete due to lipid peroxidation. The authors further confirmed membrane lipids and not DNA as the target of ROS in B. burgdorferi [133,134].
3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGR) is a crucial regulatory and rate limiting enzyme that is associated with the mevalonic pathway. B. burgdorferi genome encodes a functional 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGR EC 1.1.1.88) which contributes to a vital component necessary for peptidoglycan and cell wall biogenesis [135]. Commercially available statins, such as simvastatin and lovastatin affected in vitro growth of B. burgdorferi MSK5 strain by inhibiting HMGR [136] and reduced the burden of spirochetes in mouse models. Moreover, treating infected mice with lovastatin notably upregulates several cytokines associated with the TH2 immune response, including IL-4, IL-5, IL-9, IL-10, and IL-13 [135,137] and likely decreased bacterial burden in treated mice by either direct interference with spirochetal growth, modulation of the immune response, limitation of cholesterol availability to the spirochetes, or a combination of these mechanisms.
Methylthioadenosine (MTA)/S-adenosylhomocysteine (SAH) nucleosidase that hydolyses three substrates including 5-deoxyadenosine (5’dADO) is found in many bacterial species but is absent in humans. It cleaves to the glycosidic linkage of the nucleoside generating the thiol-sugars adenine, 5-methylribose or S-ribosyl homocysteine. MTA/SAH nucleosidases are also known to prevent synthesis of polyamine and methyltransferase activities of many organisms [138,139]. B. burgdorferi is the only bacterial species that possesses three homologues of MTA/SAH nucleosidase, (Bgp, Pfs and MtnN), of which two are exported and have been explored as drug target for B. burgdorferi [32,140,141]. Several substrate analogs and inhibitors show promise in blocking these enzymes activities in vitro and Formycin A and 5’-p-Nitrophenylthioadenosine (pNO2PhTA) showed low MIC values. Structure-based modelling was used to envisage the interaction of MTA analogues with B. burgdorferi nucleosidases and to forecast modifications that may give rise to selective anti-borrelial agents.
- C. B. burgdorferi persisters and Lyme arthritis
The formation of persister cells of B. burgdorferi with increased tolerance to conventional antibiotics has been reported [142]. In a time-dependent killing assay, a biphasic killing pattern showed the presence of persisters. Initially, majority of the cell population is speedily killed followed by a lower death rate of the subpopulation of persistent/tolerant cells [143,144]. As with other investigated microbes, the fraction of B. burgdorferi persisters equally remains largely unchanged even with increased antibiotic levels while some drugs, such as Daptomycin and Mitomycin C (though slightly toxic) were reported to eliminate both exponential culture and persister B. burgdorferi cells [142,145].
LA patients do not respond positively to the first course of antibiotics treatment of 28 days [146], with presence of B. burgdorferi DNA in synovial fluid, requiring additional 1-2 months treatment. In patients with antibiotic-resistant Lyme arthritis, synovial fluid was negative for B. burgdorferi DNA by PCR, but patients responded to tumor necrosis factor (TNF) inhibitors or anti-inflammatory agents. Recent reports implicate chemically atypical peptidoglycan (PGBb) fragments of B. burgdorferi shed into surrounding milieu during growth as a major contributor to inflammatory responses in LA, hence, potentiating other Lyme disease manifestations [147]. LA patients mount immunoglobulin G response against PGBb which is notably increased in the synovial fluid than serum. This unusual peptidoglycan sugar arrangement in B. burgdorferi (noted by the presence of N-acetylhexosamine (HexNAc) linked to N-acetylglucosamine in muropeptides) has been equally reported to be resistant to lysozyme degradation and could be key to the extension of B. burgdorferi half-life in the synovial fluid of LA patients [148]. In view of these, the antimicrobials specifically targeting this peptidoglycan could potentially be effective in LA treatment.
- D. Causes and treatment of PTLDS
Although antibiotics effectively treat most Lyme disease cases, around 10–20% of patients report lingering symptoms, including depression, cognitive impairment, joint and muscle aches and fatigue [149]. These constant symptoms persist for over six months following the conclusion of treatment for Lyme disease [150]. These persistent symptoms, collectively known as PTLDS, present ongoing challenges in terms of understanding their root causes, identifying optimal treatment strategies, and comprehending their epidemiology. Notably, this condition lacks recognition from major health authorities like the Centers for Disease Control and Prevention (CDC), Infectious Diseases Society of America (IDSA) or the American Academy of Neurology. Typically, alternative practitioners make this diagnosis, which has gained significant attention from the media and patient advocacy groups [151] while proof to support the notion that PTLDS results from persistent B. burgdorferi infection is lacking [152]. According to several studies, patients diagnosed with PTLDS often face difficulties in their daily lives, including work, social interactions, and family relationships [153] and their overall quality of life resemble with individuals afflicted by other chronic conditions [154]. Despite the significant impact of PTLDS, its causes, predisposing factors, and effective diagnostic and treatment strategies remain unknown making it challenging for patients, as well as for the healthcare providers in its management and has led to considerable confusion and debate within the medical community. To address this issue and provide a foundation for future research on PTLDS, the proposed definition say that a person will only be identified as having PTLDS if there is previous confirmation and evidence of Lyme disease infection with valid test method. This diagnosis should be conducted by reputable laboratories using validated methods and interpretation criteria. Relying on unvalidated test methods including blood microscopy and urine antigen should be avoided. Despite ongoing debate, current evidence does not support the idea of prolonged B. burgdorferi infection causing persistent symptoms after completing advised Lyme disease treatment. Although a history of Lyme disease results in re-administration of antibiotics in some cases (Figure 1), prolonged antibiotic treatment is not recommended for patients experiencing ongoing subjective symptoms beyond six months after receiving standard treatment for Lyme disease [155].
- 1. Causes identified for PTLDS
The exact causes of PTLDS remain unclear and likely involve multiple factors. One theory suggests that regardless of antibiotic therapy, persistent live B. burgdorferi or its antigens may contribute to ongoing symptoms [147]. There is not any clear evidence supporting this theory [147,156,157]. It has been suggested that exposure to antimicrobials may promote the adaptation of Borrelia, leading to persister forms that are less susceptible to antibiotic therapy in vitro [142,158,159,160]. While some studies have identified B. burgdorferi in tissues of experimentally infected animals even after treatment, evidence of persistent infection in humans remains inconclusive [6,161,162,163]. Moreover, xenodiagnostic studies in animals have shown inconsistent results, with no recovery of cultivable organisms [6]. In humans, there is no concluding evidence of persister organism forms [164]. Furthermore, in the context of other infectious diseases, achieving complete eradication of the infection is seldom employed as a criterion to determine if the infection cured or treatment should be ended [165]. Existing evidence suggests that antibiotic treatments which are routinely recommended to treat Lyme disease are effective, with no reported antimicrobial resistance in B. burgdorferi strains [166].
The symptoms of Lyme disease are mainly triggered by innate and adaptive immune responses of the host, as B. burgdorferi does not produce exotoxins. Therefore, these symptoms are likely associated with the activation of immune responses following release of inflammatory cytokines [2]. There is a possibility that the immune system remains activated in response to the presence of bacteria or their remnants even after the infection has been cleared, resulting in ongoing inflammation and persistent symptoms. Post-antibiotic treatment LA, a well-researched aspect of Lyme disease following treatment, is believed to result from autoimmunity and chronic inflammation [167]. In contrast to this persistent LA, the relationship between PTLDS and immune dysregulation remains unclear. Several studies have investigated whether ongoing immune responses might contribute to prolonged symptoms following a Lyme disease diagnosis [168,169]. Elevated levels of immune modulators such as CCL19 and IL-23 have been observed initially in early stages of Lyme disease and were more common in patients with PTLDS [168,169]. Despite the initial presence of antibody responses, they declined over time, and culture results consistently returned negative, indicating no active infection [169]. Some patients with PTLDS have shown mild elevations in C-reactive protein, an indicator of inflammation [170]. Additionally, some individuals have shown elevated levels of serum antibodies reactive to neural antigens [171]. None of these studies offer definitive proof that a previous B. burgdorferi infection is responsible for the symptoms of PTLDS. The importance of these elevated immune or inflammatory markers in a clinical context is still unclear. Moreover, if PTLDS is caused by an autoimmune response, the improvement will only be possible with the use of immune-modulating therapies [172].
Another possible cause of PTLDS could be increased sensitivity to pain, The symptoms observed might be caused by central sensitization and the increased activity of nerve pathways reacting to sensory input after an infection. This pattern of symptoms is seen in other infections too [173]. Furthermore, many PTLDS symptoms resemble those of chronic fatigue syndrome and fibromyalgia, conditions also linked to central sensitization. In these cases, changes in neurotransmitters or neuromodulators can lead to increased sensitivity to pain (hyperalgesia) and pain from non-painful stimuli (allodynia). As these conditions share similar symptoms, treatments used for chronic fatigue syndrome or fibromyalgia might benefit PTLDS patients who meet the criteria for these overlapping conditions [174].
Individuals with pre-existing health conditions or genetic biases may be more susceptible towards developing PTLDS or experiencing severe and prolonged symptoms. A cohort study assessed trends in clinical and quality-of-life (QOL) measures among patients with Lyme disease. Patients with late-stage Lyme disease had the lowest baseline QOL scores, which were later improved with follow-up. The presence of underlying health conditions was significantly associated to lower QOL scores and long-term symptoms [175]. Although antibiotics can effectively treat Lyme disease but depending upon host responses post-treatment complications may arise, emphasizing the need for further investigation [167].
Psychological factors may play a role in developing PTLDS. A study was conducted which assessed Life Events Checklist (LEC) and revealed that a higher exposure to previous traumatic life events was independently linked to an elevated risk of meeting PTLDS criteria. This implies that individuals with a history of trauma may be more prone to developing persistent symptoms following Lyme disease treatment. Although participants with prior Lyme disease exhibited higher scores on the depression subscale of the Beck Depression Inventory-II (BDI-II), the cohort group did not significantly predict moderate/severe depression symptoms, suggesting that depression may not be the primary driver of increased symptom reporting in PTLDS [176].
- 2. Approaches to improve quality of life after Lyme disease
It remains challenging to improve the quality of life of individuals who continue to experience subjective symptoms even after completion of treatment. A population-based study revealed that one-third of Lyme disease patients faced delays in treatment, which was linked to the development of PTLDS. Minimum delay in seeking medical care and initiating treatment could overcome this problem [177]. A study investigated the likelihood of PTLDS in participants with the history of Lyme disease as compared to another group of participants who do not have Lyme disease. Pain, fatigue, depression, and quality of life were assessed among these groups using surveys. The study showed that out of all the participants with the history of Lyme disease 13.7% met the criteria for PTLDS showing 5.28 times higher likelihood of developing symptoms in comparison to just 4.1% of those who does not have history of Lyme disease[176].
Currently there are not any specific treatments available for PTLDS recommended by The Infectious Diseases Society of America (IDSA), The American Academy of Neurology (AAN) and the Ad Hoc International Lyme Disease Group. Although there are many studies on extended use of antibiotic treatments for PTLDS, the specific antibiotics, duration, symptoms, and outcomes can vary across studies. Many studies identify cognitive deficits as a common symptom of PTLDS, frequently reported by patients themselves and probably due to the great impact on a person's daily activities. Nevertheless, it's important to consider patients' perceptions of their illness, as both subjective and objective cognitive deficits can profoundly impact a patient's life and daily functioning.
A study in the northeastern United States focused on individuals who continued to experience symptoms after completing treatment for Lyme disease. Participants were divided into two groups depending upon antibody positive test or erythema migrans lesion history. Both groups were split further into experimental and placebo groups, receiving either ceftriaxone and doxycycline or placebo. Initially, participants showed no significant differences in cognitive function, pain, role functioning, memory, or attention. After treatment, all groups improved equally, suggesting no additional benefit from antibiotics. Researchers suggested that improvements could be attributed to reduced pain and better mood. This implies that self-reported symptoms may not always match objective testing and may not respond to antibiotic treatment [178]. There are many other placebo-controlled studies in patients with Lyme disease who exhibited symptoms of PTLDS that showed that a long term antibiotic use was ineffective [172,178,179,180] and poses risks of severe side effects, including complications from IV catheters [30,70,152,179,181,182,183,184]. In fact, reports of severe or fatal bacterial infections resulting from long-term antibiotic therapy require serious consideration [185].
Current research on potential treatments for PTLDS and recommendations of CDC indicated that patients treated with either oral or IV antibiotics faced higher risks of developing infections and electrolyte imbalances compared to those who did not receive antibiotic treatment [186]. Studies on the repeated use of antibiotics showed an increased risk of infection without symptom improvement [185]. A 2017 case study highlighted that ceftriaxone caused hemolytic anemia and acute kidney injury in a patient with PTLDS [187]. These findings suggest antibiotics may not offer significant relief and that PTLDS may not stem from a latent B. burgdorferi infection [188]. As there is no definitive treatment standard beyond supportive care, there is a need for new therapies to effectively address PTLDS. Although the exact cause of PTLDS remains unclear, some studies suggest that antimicrobial resistance emergence in B. burgdorferi may contribute to its development [189,190].
III. Vaccines to prevent B. burgdorferi infection and Lyme disease
Research into vaccines for Lyme disease prevention has seen renewed interest in current years. LYMErix was the only licensed vaccine in the United States from 1998–2002 and effectively reduced Lyme disease infections in vaccinated adults by 80%. However, the vaccine was discontinued due to concern about vaccine triggering an autoimmune response and thus, low adoption rates. A six-component vaccine targets the outer surface protein A (OspA) to induce an antibody response against all stains of Borrelia causing Lyme disease [191]. OspA is a lipoprotein on the outer membrane of B. burgdorferi that can be targeted by antibodies to kill the organism in the tick’s midgut before transmission. A multivalent OspA-based vaccine (VLA15), that targets various clinically relevant Borrelia species and OspA serotypes found in US and Europe is composed of three proteins with each harboring the C-terminal fragment of OspA serotypes linked in pairs to form three fusion proteins. Triple immunization of mice with the vaccine protected them from infection when challenged with in vitro grown spirochetes as well as the infected ticks [11,192,193].
Similarly using same approach as VLA15, a prototype vaccine that makes use of Helicobacter pylori ferritin nanoparticles that are fused with seven OspA serotypes from B. garinii, B. bavariensis, B. afzelii and B. burgdorferi, exhibited long-lasting high-titer antibody response in both rhesus macaque and mouse infection models [191]. Other vaccine approaches include an OspA-encoding lipid nanoparticle-encapsulated nucleoside-modified mRNA (mRNA-LNP) vaccine assessed for protective efficacy and immunogenicity in comparison to alum-adjuvanted OspA protein subunit vaccine [194]. In addition, a subunit vaccine containing a combination of OspA and 14 immunogenic linear epitopes (“chimeritope”) from different OspC isotypes [195] has also been evaluated as promising candidate. In another study experimental study, the outer surface protein, Cspz, associated with complement evasion had also been explored as a vaccine candidate [196]. Currently, Valneva SE and Pfizer Inc report positive Phase 2 clinical trial data with the phase three trials about to start. VLA15 testing after two (0 and 6 months) or three (0, 2 and 6 months) administrations of primary series doses in 5-11, 12-17 and 18-65 year age groups showed higher success in the adult participants (18-65) who received three doses compared to those who received two doses [10,197]. Multiple tick-borne disease can also be prevented by developing ant-tick vaccines. For instance, mice that were administered with antiserum to the tick protein, Salp15, then subsequently challenged with B. burgdorferi were protected from colonization [198]. Moreover, tick protein could elicit “tick immunity” or a situation whereby the host is resistant to tick bites.
IV. Future prospective
Although copious amount of evidence suggests the presence of drug-tolerant persisters, antigenic debris, impaired immunological response or a combination of these as culprits, the exact root cause behind the prolongation of the post treatment symptoms still remains unclear [199,220]. Some antibiotics act synergistically and could serve as a future therapeutic intervention in alleviating Lyme disease symptoms. These include trimethoprim and sulfonamide, aminoglycosides and β-lactams [200]. Also, fluoroquinolones and aminoglycosides have been shown to kill or non-growing cells [201,202].
Acupuncture has been used for centuries in Asian medicine to alleviate pain and inflammation. From a clinical perspective, ST36 (sciatic nerve) stimulation is the most common treatment in acupuncture for inflammatory and infectious disorders by acting through stimulation of Vagus nerve [203]. Recent studies show that electroacupuncture can alleviate LA symptoms in mice although it didn't impact spirochete burden [204]. Further reports highlight acupuncture's effectiveness in alleviating Lyme disease symptoms like migraines and musculoskeletal pain. In a case of a 44-year-old female who underwent acupuncture alongside antibiotic treatment, in significant symptom resolution was observed over 10 months suggesting that it could also reduce Lyme disease symptoms [205,206]. A novel therapeutic approach to treat PTLDS involved engineering Chimeric Antigen Receptor (CAR) T-cells to target and eliminate B. burgdorferi. The efficacy of these CAR T-cells needs to be tested in vitro and in vivo using reliable animal models before being administered to patients. This innovative proposal seeks to establish a treatment protocol for PTLDS, offering relief and hope to patients suffering from this chronic and debilitating condition [207].
To summarize, treatment of Lyme disease could also be tailored to patients’ immune response system, genetic make-up, and other host-factors to minimize relapses or degeneration to chronic conditions which could improve outcomes. There is need for technological remote monitoring of individuals in rural communities where Lyme disease is endemic. In addition, public awareness in the form of education, surveillance and early intervention could go a long way to reduce burden of infection in the rural communities. Finally, a combinatorial approach involving antibiotic and alternative treatment approaches like acupuncture or the use of anti-inflammatory agents in the cases of severe symptoms could be explored to alleviate suffering and patients’ post-treatment and improving their quality of life.
A tick bite resulting in the development of erythema migrans is often a clear indication of Lyme disease in the endemic regions. In some cases, erythema migrans may be treated prophylactically without a confirmed diagnosis of Lyme disease; however, after confirmed diagnosis, antibiotic treatment is usually initiated. Despite antibiotic therapy, some patients may continue to exhibit Lyme disease symptoms, which could be attributed to either reinfection or incomplete clearance of spirochetes. In such cases, additional antibiotic treatment is often administered, and the commonly used antibiotics are doxycycline (100 mg, twice per day orally), amoxicillin (500 mg, three times per day orally) and cefuroxime (500 mg, twice per day orally). While many patients experience symptom resolution after completion of antibiotic treatment regimen, ~10–20% report persistent symptoms, including fatigue, cognitive impairment, joint and muscle aches, and depression or PTLDS. In the absence of a documented tick bite history or erythema migrans but the presence of non-specific symptoms, treatment is delayed and could result in the development of late stage disseminated Lyme disease presenting a range of symptoms affecting the joints, nervous system, and ACA. Treatment of late-stage Lyme disease may result in symptom resolution or progression to PTLDS. Although no standard treatment is recommended for PTLDS at present, a combinatorial therapeutic intervention including antibiotics with anti-inflammatory agents or with alternative treatments like acupuncture could be explored in the future to manage PTLDS.
References
- Schwartz, I.; Margos, G.; Casjens, S.R.; Qiu, W.-G.; Eggers, C.H. Multipartite genome of Lyme disease Borrelia: structure, variation and prophages. Current issues in molecular biology 2021, 42, 409–454. [Google Scholar] [PubMed]
- Steere, A.C.; Strle, F.; Wormser, G.P.; Hu, L.T.; Branda, J.A.; Hovius, J.W.; Li, X.; Mead, P.S. Lyme borreliosis. Nature reviews Disease primers 2016, 2, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Adrion, E.R.; Aucott, J.; Lemke, K.W.; Weiner, J.P. Health care costs, utilization and patterns of care following Lyme disease. PloS one 2015, 10, e0116767. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.R.; Collins, J.J.; Relman, D.A. Antibiotics and the gut microbiota. The Journal of clinical investigation 2014, 124, 4212–4218. [Google Scholar] [CrossRef] [PubMed]
- Willing, B.P.; Russell, S.L.; Finlay, B.B. Shifting the balance: antibiotic effects on host–microbiota mutualism. Nature Reviews Microbiology 2011, 9, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Embers, M.E.; Barthold, S.W.; Borda, J.T.; Bowers, L.; Doyle, L.; Hodzic, E.; Jacobs, M.B.; Hasenkampf, N.R.; Martin, D.S.; Narasimhan, S. Persistence of Borrelia burgdorferi in rhesus macaques following antibiotic treatment of disseminated infection. PloS one 2012, 7, e29914. [Google Scholar] [CrossRef]
- Feng, J.; Shi, W.; Zhang, S.; Zhang, Y. Identification of new compounds with high activity against stationary phase Borrelia burgdorferi from the NCI compound collection. Emerging Microbes & Infections 2015, 4, 1–15. [Google Scholar]
- Hodzic, E.; Imai, D.; Feng, S.; Barthold, S.W. Resurgence of persisting non-cultivable Borrelia burgdorferi following antibiotic treatment in mice. PloS one 2014, 9, e86907. [Google Scholar] [CrossRef] [PubMed]
- Radolf, J.D.; Caimano, M.J.; Stevenson, B.; Hu, L.T. Of ticks, mice and men: understanding the dual-host lifestyle of Lyme disease spirochaetes. Nature reviews microbiology 2012, 10, 87–99. [Google Scholar] [CrossRef]
- Hajdusek, O.; Perner, J. VLA15, a new global Lyme disease vaccine undergoes clinical trials. The Lancet Infectious Diseases 2023, 23, 1105–1106. [Google Scholar] [CrossRef]
- Comstedt, P.; Schüler, W.; Meinke, A.; Lundberg, U. The novel Lyme borreliosis vaccine VLA15 shows broad protection against Borrelia species expressing six different OspA serotypes. PloS one 2017, 12, e0184357. [Google Scholar] [CrossRef] [PubMed]
- Lee-Lewandrowski, E.; Chen, Z.; Branda, J.; Baron, J.; Kaufman, H.W. Laboratory Blood-Based Testing for Lyme Disease at a National Reference Laboratory: A 7-Year Experience (2010-2016). American Journal of Clinical Pathology 2019, 152, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Mead, P.S. Epidemiology of Lyme disease. Infectious Disease Clinics 2015, 29, 187–210. [Google Scholar] [CrossRef] [PubMed]
- Wormser, G.; Dattwyler, R.; Shapiro, E.; Halperin, J.; Steere, A.; Klempner, M.; Krause, P.; Bakken, J.; Strle, F.; Stanek, G. Erratum: The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: Clinical practice guidelines by the Infectious Diseases Society of America (Clinical Infectious Diseases (2006) 43,(1089-1134)). Clinical Infectious Diseases 2007, 45. [Google Scholar]
- Knudtzen, F.C.; Andersen, N.S.; Jensen, T.G.; Skarphédinsson, S. Characteristics and clinical outcome of Lyme neuroborreliosis in a high endemic area, 1995–2014: a retrospective cohort study in Denmark. Clinical Infectious Diseases 2017, 65, 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- Ljøstad, U.; Mygland, Å. Remaining complaints 1 year after treatment for acute Lyme neuroborreliosis; frequency, pattern and risk factors. European Journal of Neurology 2010, 17, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Shadick, N.A.; Phillips, C.B.; Sangha, O.; Logigian, E.L.; Kaplan, R.F.; Wright, E.A.; Fossel, A.H.; Fossel, K.; Berardi, V.; Lew, R.A. Musculoskeletal and neurologic outcomes in patients with previously treated Lyme disease. Annals of Internal Medicine 1999, 131, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Eikeland, R.; Mygland, Å.; Herlofson, K.; Ljøstad, U. Risk factors for a non-favorable outcome after treated E uropean neuroborreliosis. Acta Neurologica Scandinavica 2013, 127, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Rahn, D.W.; Malawista, S.E. Lyme disease: recommendations for diagnosis and treatment. Annals of internal medicine 1991, 114, 472–481. [Google Scholar] [CrossRef]
- Control, C.f.D.; Prevention. Lyme disease data and surveillance. Centers for Disease Control and Prevention, Atlanta, GA: https://www. cdc. gov/lyme/datasurveillance/index. html.[Google Scholar] 2019.
- Mead, P.; Petersen, J.; Hinckley, A. Updated CDC recommendation for serologic diagnosis of Lyme disease. Morbidity and Mortality Weekly Report 2019, 68, 703–703. [Google Scholar] [CrossRef]
- Wormser, G.P.; Schriefer, M.; Aguero-Rosenfeld, M.E.; Levin, A.; Steere, A.C.; Nadelman, R.B.; Nowakowski, J.; Marques, A.; Johnson, B.J.; Dumler, J.S. Single-tier testing with the C6 peptide ELISA kit compared with two-tier testing for Lyme disease. Diagnostic microbiology and infectious disease 2013, 75, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Dressler, F.; Whalen, J.A.; Reinhardt, B.N.; Steere, A.C. Western blotting in the serodiagnosis of Lyme disease. Journal of Infectious Diseases 1993, 167, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Depietropaolo, D.L.; Powers, J.H.; Gill, J.M.; Foy, A.J. Diagnosis of Lyme disease. American family physician 2005, 72, 297–304. [Google Scholar] [PubMed]
- Diseases, C.o.I. Prevention of Lyme disease. Pediatrics 2000, 105, 142–147. [Google Scholar] [CrossRef]
- Eisen, L. Control of ixodid ticks and prevention of tick-borne diseases in the United States: The prospect of a new Lyme disease vaccine and the continuing problem with tick exposure on residential properties. Ticks and tick-borne diseases 2021, 12, 101649. [Google Scholar] [CrossRef] [PubMed]
- Nadelman, R.B.; Nowakowski, J.; Fish, D.; Falco, R.C.; Freeman, K.; McKenna, D.; Welch, P.; Marcus, R.; Agüero-Rosenfeld, M.E.; Dennis, D.T. Prophylaxis with single-dose doxycycline for the prevention of Lyme disease after an Ixodes scapularis tick bite. New England Journal of Medicine 2001, 345, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Costello, C.M.; Steere, A.C.; Pinkerton, R.E.; Feder, H.M. A prospective study of tick bites in an endemic area for Lyme disease. The Journal of infectious diseases 1989, 159, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Salzman, M.; Rubin, L.; Sood, S. Prevention of Lyme disease after tick bites. The New England journal of medicine 1993, 328, 137–139. [Google Scholar] [PubMed]
- Wormser, G.P.; Dattwyler, R.J.; Shapiro, E.D.; Halperin, J.J.; Steere, A.C.; Klempner, M.S.; Krause, P.J.; Bakken, J.S.; Strle, F.; Stanek, G. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clinical Infectious Diseases 2006, 43, 1089–1134. [Google Scholar] [CrossRef]
- Rebman, A.W.; Yang, T.; Yoon, I.; Powell, D.; Geller, S.A.; Aucott, J.N. Initial Presentation and Time to Treatment in Early Lyme Disease. The American journal of tropical medicine and hygiene 2023, tpmd220437–tpmd220437. [Google Scholar] [CrossRef]
- Cornell, K.A.; Knippel, R.J.; Cortright, G.R.; Fonken, M.; Guerrero, C.; Hall, A.R.; Mitchell, K.A.; Thurston, J.H.; Erstad, P.; Tao, A. Characterization of 5′-methylthioadenosine/S-adenosylhomocysteine nucleosidases from Borrelia burgdorferi: Antibiotic targets for Lyme disease. Biochimica et Biophysica Acta (BBA)-General Subjects 2020, 1864, 129455. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.P.; Schoen, R.T.; Rahn, D.W.; Sikand, V.K.; Nowakowski, J.; Parenti, D.L.; Holman, M.S.; Persing, D.H.; Steere, A.C. Clinical characteristics and treatment outcome of early Lyme disease in patients with microbiologically confirmed erythema migrans. Annals of internal medicine 2002, 136, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Luger, S.W.; Paparone, P.; Wormser, G.P.; Nadelman, R.B.; Grunwaldt, E.; Gomez, G.; Wisniewski, M.; Collins, J.J. Comparison of cefuroxime axetil and doxycycline in treatment of patients with early Lyme disease associated with erythema migrans. Antimicrobial agents and chemotherapy 1995, 39, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Eliassen, K.; Reiso, H.; Berild, D.; Lindbæk, M. Comparison of phenoxymethylpenicillin, amoxicillin, and doxycycline for erythema migrans in general practice. A randomized controlled trial with a 1-year follow-up. Clinical Microbiology and Infection 2018, 24, 1290–1296. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, T.J.; Tata, S.; Berth, W.; Mathiason, M.A.; Agger, W.A. Antibiotic treatment duration and long-term outcomes of patients with early Lyme disease from a Lyme disease–hyperendemic area. Clinical infectious diseases 2010, 50, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Nowakowski, J.; Nadelman, R.B.; Forseter, G.; McKenna, D.; Wormser, G.P. Doxycycline versus tetracycline therapy for Lyme disease associated with erythema migrans. Journal of the American Academy of Dermatology 1995, 32, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Stupica, D.; Lusa, L.; Ružić-Sabljić, E.; Cerar, T.; Strle, F. Treatment of erythema migrans with doxycycline for 10 days versus 15 days. Clinical infectious diseases 2012, 55, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Wormser, G.P.; Brady, K.C.; Cho, M.S.; Scavarda, C.A.; McKenna, D. Efficacy of a 14-day course of amoxicillin for patients with erythema migrans. Diagnostic microbiology and infectious disease 2019, 94, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Torbahn, G.; Hofmann, H.; Rücker, G.; Bischoff, K.; Freitag, M.H.; Dersch, R.; Fingerle, V.; Motschall, E.; Meerpohl, J.J.; Schmucker, C. Efficacy and safety of antibiotic therapy in early cutaneous Lyme borreliosis: a network meta-analysis. JAMA dermatology 2018, 154, 1292–1303. [Google Scholar] [CrossRef]
- Chason, M.E.; Monaghan, M.; Wang, J.; Cheng, Y.; DeBiasi, R.L. Symptom resolution in pediatric patients with Lyme disease. Journal of the Pediatric Infectious Diseases Society 2019, 8, 170–173. [Google Scholar] [CrossRef]
- Meissner, H.C.; Steere, A.C. Management of pediatric Lyme disease: updates from 2020 Lyme guidelines. Pediatrics 2022, 149, e2021054980. [Google Scholar] [CrossRef] [PubMed]
- Eppes, S.C.; Childs, J.A. Comparative study of cefuroxime axetil versus amoxicillin in children with early Lyme disease. Pediatrics 2002, 109, 1173–1177. [Google Scholar] [CrossRef] [PubMed]
- Arnez, M.; Radsel-Medvescek, A.; Pleterski-Rigler, D.; Ruzic-Sabljic, E.; Strle, F. Comparison of cefuroxime axetil and phenoxymethyl penicillin for the treatment of children with solitary erythema migrans. Wiener Klinische Wochenschrift 1999, 111, 916–922. [Google Scholar] [PubMed]
- Cerar, D.; Cerar, T.; Ružić-Sabljić, E.; Wormser, G.P.; Strle, F. Subjective symptoms after treatment of early Lyme disease. The American journal of medicine 2010, 123, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Angelette, A.L.; Rando, L.L.; Wadhwa, R.D.; Barras, A.A.; Delacroix, B.M.; Talbot, N.C.; Ahmadzadeh, S.; Shekoohi, S.; Cornett, E.M.; Kaye, A.M. Tetracycline-, doxycycline-, minocycline-induced pseudotumor cerebri and esophageal perforation. Advances in Therapy 2023, 40, 1366–1378. [Google Scholar] [CrossRef] [PubMed]
- Nadelman, R.B.; Luger, S.W.; Frank, E.; Wisniewski, M.; Collins, J.J.; Wormser, G.P. Comparison of cefuroxime axetil and doxycycline in the treatment of early Lyme disease. Annals of internal medicine 1992, 117, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Auwaerter, P.G.; Kobayashi, T.; Wormser, G.P. Guidelines for Lyme disease are updated. The American journal of medicine 2021, 134, 1314–1316. [Google Scholar] [CrossRef] [PubMed]
- Stricker, R.B.; Johnson, L. Long-term outcomes in patients with early lyme disease: more false hope? Clinical Infectious Diseases 2010, 50, 1683–1684. [Google Scholar] [CrossRef]
- Wormser, G.P.; Ramanathan, R.; Nowakowski, J.; McKenna, D.; Holmgren, D.; Visintainer, P.; Dornbush, R.; Singh, B.; Nadelman, R.B. Duration of antibiotic therapy for early Lyme disease: a randomized, double-blind, placebo-controlled trial. Annals of internal medicine 2003, 138, 697–704. [Google Scholar] [CrossRef]
- Eldin, C.; Hansmann, Y. Erythema migrans: Lyme disease does not need prolonged therapy. The Lancet Infectious Diseases 2023, 23, 271–272. [Google Scholar] [CrossRef]
- Cameron, D.J.; Johnson, L.B.; Maloney, E.L. Evidence assessments and guideline recommendations in Lyme disease: the clinical management of known tick bites, erythema migrans rashes and persistent disease. Expert review of anti-infective therapy 2014, 12, 1103–1135. [Google Scholar] [CrossRef] [PubMed]
- Hercogová, J. Lyme borreliosis. In European Handbook of Dermatological Treatments; Springer, 2023; pp. 599–604. [Google Scholar]
- Hunfeld, K.-P.; Wichelhaus, T.A.; Rödel, R.; Acker, G.; Brade, V.; Kraiczy, P. Comparison of in vitro activities of ketolides, macrolides, and an azalide against the spirochete Borrelia burgdorferi. Antimicrobial agents and chemotherapy 2004, 48, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Labro, M. Anti-inflammatory activity of macrolides: a new therapeutic potential? The Journal of antimicrobial chemotherapy 1998, 41, 37–46. [Google Scholar] [CrossRef]
- Boston, I. Macrolide therapy of chronic Lyme disease. Signature 2003, 9111, P1136–I1142. [Google Scholar]
- Nowakowski, J.; McKenna, D.; Nadelman, R.B.; Cooper, D.; Bittker, S.; Holmgren, D.; Pavia, C.; Johnson, R.C.; Wormser, G.P. Failure of treatment with cephalexin for Lyme disease. Archives of Family Medicine 2000, 9, 563. [Google Scholar] [CrossRef] [PubMed]
- Agger, W.; Callister, S.; Jobe, D. In vitro susceptibilities of Borrelia burgdorferi to five oral cephalosporins and ceftriaxone. Antimicrobial agents and chemotherapy 1992, 36, 1788–1790. [Google Scholar] [CrossRef] [PubMed]
- Fallon, B.A.; Nields, J.A. Lyme disease: a neuropsychiatric illness. American Journal of Psychiatry 1994, 151, 1571–1583. [Google Scholar] [PubMed]
- HANSEN, K.; LEBECH, A.-M. The clinical and epidemiological profile of lyme neuroborreliosis in Denmark 1985–1990: a prospective study of 187 patients with Borrelia burgdorferi specific intrathecal antibody productionm. Brain 1992, 115, 399–423. [Google Scholar] [CrossRef] [PubMed]
- Oschmann, P.; Dorndorf, W.; Hornig, C.; Schäfer, C.; Wellensiek, H.; Pflughaupt, K. Stages and syndromes of neuroborreliosis. Journal of neurology 1998, 245, 262–272. [Google Scholar] [CrossRef]
- Kaiser, R. Variable CSF findings in early and late Lyme neuroborreliosis: a follow-up study in 47 patients. Journal of neurology 1994, 242, 26–36. [Google Scholar] [CrossRef]
- Berglund, J.; Eitrem, R.; Ornstein, K.; Lindberg, A.; Ringnér, Å.; Elmrud, H.; Carlsson, M.; Runehagen, A.; Svanborg, C.; Norrby, R. An epidemiologic study of Lyme disease in southern Sweden. New England Journal of Medicine 1995, 333, 1319–1324. [Google Scholar] [CrossRef] [PubMed]
- Koedel, U.; Fingerle, V.; Pfister, H.-W. Lyme neuroborreliosis—epidemiology, diagnosis and management. Nature Reviews Neurology 2015, 11, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Christen, H.-J. Lyme neuroborreliosis in children. Annals of medicine 1996, 28, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Pfister, H.-W.; Wilske, B. Lyme borreliosis: basic science and clinical aspects. The Lancet 1994, 343, 1013–1016. [Google Scholar] [CrossRef] [PubMed]
- Oksi, J.; Nikoskelainen, J.; Hiekkanen, H.; Lauhio, A.; Peltomaa, M.; Pitkäranta, A.; Nyman, D.; Granlund, H.; Carlsson, S.-A.; Seppälä, I. Duration of antibiotic treatment in disseminated Lyme borreliosis: a double-blind, randomized, placebo-controlled, multicenter clinical study. European Journal of Clinical Microbiology & Infectious Diseases 2007, 26, 571–581. [Google Scholar]
- Dersch, R.; Freitag, M.; Schmidt, S.; Sommer, H.; Rauer, S.; Meerpohl, J. Efficacy and safety of pharmacological treatments for acute L yme neuroborreliosis–a systematic review. European journal of neurology 2015, 22, 1249–1259. [Google Scholar] [CrossRef] [PubMed]
- Mygland, Å.; Ljøstad, U.; Fingerle, V.; Rupprecht, T.; Schmutzhard, E.; Steiner, I. EFNS guidelines on the diagnosis and management of European Lyme neuroborreliosis. European journal of neurology 2010, 17, 8–e4. [Google Scholar] [CrossRef]
- Halperin, J.; Shapiro, E.; Logigian, E.; Belman, A.; Dotevall, L.; Wormser, G.; Krupp, L.; Gronseth, G.; Bever Jr, C. Practice parameter: treatment of nervous system Lyme disease (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2007, 69, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Eikeland, R.; Mygland, Å.; Herlofson, K.; Ljøstad, U. European neuroborreliosis: quality of life 30 months after treatment. Acta Neurologica Scandinavica 2011, 124, 349–354. [Google Scholar] [CrossRef]
- Ljøstad, U.; Skogvoll, E.; Eikeland, R.; Midgard, R.; Skarpaas, T.; Berg, Å.; Mygland, Å. Oral doxycycline versus intravenous ceftriaxone for European Lyme neuroborreliosis: a multicentre, non-inferiority, double-blind, randomised trial. The Lancet Neurology 2008, 7, 690–695. [Google Scholar] [CrossRef]
- Karlsson, M.; Hammers-Berggren, S.; Lindquist, L.; Stiernstedt, G.; Svenungsson, B. Comparison of intravenous penicillin G and oral doxycycline for treatment of Lyme neuroborreliosis. Neurology 1994, 44, 1203–1203. [Google Scholar] [CrossRef] [PubMed]
- Pfister, H.-W.; Preac-Mursic, V.; Wilske, B.; Schielke, E.; Sörgel, F.; Einhaupl, K.M. Randomized comparison of ceftriaxone and cefotaxime in Lyme neuroborreliosis. Journal of Infectious Diseases 1991, 163, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Pfister, H.-W.; Preac-Mursic, V.; Wilske, B.; Einhäupl, K.M. Cefotaxime vs penicillin G for acute neurologic manifestations in Lyme borreliosis: a prospective randomized study. Archives of neurology 1989, 46, 1190–1194. [Google Scholar] [CrossRef] [PubMed]
- Hassler, D.; Zöller, L.; Haude, M.; Hufnagel, H.; Heinrich, F.; Sonntag, H. Cefotaxime versus penicillin in the late stage of Lyme disease--prospective, randomized therapeutic study. Infection 1990, 18, 16–20. [Google Scholar] [CrossRef] [PubMed]
- STEERE, A.C.; BATSFORD, W.P.; WEINBERG, M.; ALEXANDER, J.; BERGER, H.J.; WOLFSON, S.; MALAWISTA, S.E. Lyme carditis: cardiac abnormalities of Lyme disease. Annals of internal medicine 1980, 93, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Krause, P.J.; Bockenstedt, L.K. Lyme disease and the heart. Circulation 2013, 127, e451–e454. [Google Scholar] [CrossRef] [PubMed]
- Forrester, J.D.; Meiman, J.; Mullins, J.; Nelson, R.; Ertel, S.-H.; Cartter, M.; Brown, C.M.; Lijewski, V.; Schiffman, E.; Neitzel, D. Notes from the field: update on Lyme carditis, groups at high risk, and frequency of associated sudden cardiac death--United States. MMWR Morb Mortal Wkly Rep 2014, 63, 982–983. [Google Scholar]
- Kwit, N.A.; Nelson, C.A.; Max, R.; Mead, P.S. Risk factors for clinician-diagnosed Lyme arthritis, facial palsy, carditis, and meningitis in patients from high-incidence states. In Proceedings of the Open Forum Infectious Diseases, 2018; p. ofx254. [Google Scholar]
- RUBIN, D.A.; SORBERA, C.; NIKITIN, P.; MCALLISTER, A.; WORMSER, G.P.; NADELMAN, R.B. Prospective evaluation of heart block complicating early Lyme disease. Pacing and Clinical Electrophysiology 1992, 15, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Welsh, E.J.; Cohn, K.A.; Nigrovic, L.E.; Thompson, A.D.; Hines, E.M.; Lyons, T.W.; Glatz, A.C.; Shah, S.S. Electrocardiograph abnormalities in children with Lyme meningitis. Journal of the Pediatric Infectious Diseases Society 2012, 1, 293–298. [Google Scholar] [CrossRef]
- Oktay, A.A.; Dibs, S.R.; Friedman, H. Sinus pause in association with Lyme carditis. Texas Heart Institute Journal 2015, 42, 248–250. [Google Scholar] [CrossRef]
- Rey, M.-J.; Zimmermann, M.; Adamec, R.; Fleisch, M.; Viquerat, C.; De Freudenreich, J. Intra-hisian 2: 1 atrioventricular block secondary to Lyme disease. European heart journal 1991, 12, 1048–1051. [Google Scholar] [CrossRef] [PubMed]
- Van der Linde, M.; Crijns, H.; De Koning, J.; Hoogkamp-Korstanje, J.; De Graaf, J.; Piers, D.A.; Van der Galien, A.; Lie, K. Range of atrioventricular conduction disturbances in Lyme borreliosis: a report of four cases and review of other published reports. Heart 1990, 63, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, Y.J.; Brennan, J.J.; Rosenfeld, L.E. Lyme myocarditis presenting as fascicular tachycardia with underlying complete heart block. Journal of cardiovascular electrophysiology 1997, 8, 323–324. [Google Scholar] [CrossRef] [PubMed]
- Petr Kuchynka, M.; Tomas Palecek, M.; Stepan Havranek, M.; Vitkova, I.; Nemecek, E.; Trckova, R.; Krsek, D.; Podzimkova, J.; Fikrle, M.; Danek, B.A. Recent-onset dilated cardiomyopathy associated with Borrelia burgdorferi infection. Herz 2015, 40, 892. [Google Scholar] [CrossRef]
- N’guyen, Y.; Lesaffre, F.; Metz, D.; de Martino, S.; Jaulhac, B.; Andréoletti, L. No serological evidence for Borrelia burgdorferi sensu lato infection in patients with dilated cardiomyopathy in Northern France. Infectious Diseases 2016, 48, 763–764. [Google Scholar] [CrossRef] [PubMed]
- Gasser, R.; Dusleag, J.; Reisinger, E. Reversal by ceftriaxone of dilated cardiomyopathy Borrelia burgdorferi infection. 1992.
- Kubánek, M.; Šramko, M.; Berenová, D.; Hulínská, D.; Hrbáčková, H.; Malušková, J.; Lodererová, A.; Málek, I.; Kautzner, J. Detection of Borrelia burgdorferi sensu lato in endomyocardial biopsy specimens in individuals with recent-onset dilated cardiomyopathy. European journal of heart failure 2012, 14, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Dattwyler, R.J.; Luft, B.J.; Kunkel, M.J.; Finkel, M.F.; Wormser, G.P.; Rush, T.J.; Grunwaldt, E.; Agger, W.A.; Franklin, M.; Oswald, D. Ceftriaxone compared with doxycycline for the treatment of acute disseminated Lyme disease. New England Journal of Medicine 1997, 337, 289–295. [Google Scholar] [CrossRef]
- Pritt, B.S.; Respicio-Kingry, L.B.; Sloan, L.M.; Schriefer, M.E.; Replogle, A.J.; Bjork, J.; Liu, G.; Kingry, L.C.; Mead, P.S.; Neitzel, D.F. Borrelia mayonii sp. nov., a member of the Borrelia burgdorferi sensu lato complex, detected in patients and ticks in the upper midwestern United States. International journal of systematic and evolutionary microbiology 2016, 66, 4878–4880. [Google Scholar] [CrossRef] [PubMed]
- Sigal, L.H. Early disseminated Lyme disease: cardiac manifestations. The American journal of medicine 1995, 98, 25S–29S. [Google Scholar] [CrossRef]
- Pinto, D.S. Cardiac manifestations of Lyme disease. Medical Clinics 2002, 86, 285–296. [Google Scholar] [CrossRef]
- Ogrinc, K.; Lusa, L.; Lotrič-Furlan, S.; Bogovič, P.; Stupica, D.; Cerar, T.; Ružić-Sabljić, E.; Strle, F. Course and outcome of early European Lyme neuroborreliosis (Bannwarth syndrome): clinical and laboratory findings. Reviews of Infectious Diseases 2016, 63, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, R. Verlauf der akuten und chronischen Neuroborreliose nach Behandlung mit Ceftriaxon. Der Nervenarzt 2004, 6, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Berglund, J.; Stjernberg, L.; Ornstein, K.; Tykesson-Joelsson, K.; Walter, H. 5-y Follow-up study of patients with neuroborreliosis. Scandinavian journal of infectious diseases 2002, 34, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Dersch, R.; Sommer, H.; Rauer, S.; Meerpohl, J. Prevalence and spectrum of residual symptoms in Lyme neuroborreliosis after pharmacological treatment: a systematic review. Journal of neurology 2016, 263, 17–24. [Google Scholar] [CrossRef] [PubMed]
- STEERE, A.C.; SCHOEN, R.T.; TAYLOR, E. The clinical evolution of Lyme arthritis. Annals of internal medicine 1987, 107, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Caperton, E.M.; Heim-Duthoy, K.L.; Matzke, G.R.; Peterson, P.K.; Johnson, R.C. Ceftriaxone therapy of chronic inflammatory arthritis. Archives of Internal Medicine 1990, 150, 1677–1682. [Google Scholar] [CrossRef]
- Steere, A.C.; Green, J.; Schoen, R.T.; Taylor, E.; Hutchinson, G.J.; Rahn, D.W.; Malawista, S.E. Successful parenteral penicillin therapy of established Lyme arthritis. New England Journal of Medicine 1985, 312, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Dattwyler, R.; Volkman, D.; Halperin, J.; Luft, B. Treatment of late Lyme borreliosis—randomised comparison of ceftriaxone and penicillin. The Lancet 1988, 331, 1191–1194. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C. Treatment of Lyme arthritis. 2019, 46, 871–873.
- Steere, A.C.; Levin, R.E.; Molloy, P.J.; Kalish, R.A.; Abraham Iii, J.H.; Liu, N.Y.; Schmid, C.H. Treatment of Lyme arthritis. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology 1994, 37, 878–888. [Google Scholar]
- Stanek, G.; Wormser, G.P.; Gray, J.; Strle, F. Lyme borreliosis. The Lancet 2012, 379, 461–473. [Google Scholar] [CrossRef]
- Muellegger, R.R.; Glatz, M. Skin manifestations of lyme borreliosis: diagnosis and management. American journal of clinical dermatology 2008, 9, 355–368. [Google Scholar] [CrossRef]
- Lampert, F.; Belohradsky, B.; Förster, C.; Eife, R.; Kollmann, D.; Stochdorph, O.; Gokel, J.; Meister, P.; Lampert, P. Infantile chronic relapsing inflammation of the brain, skin, and joints. The Lancet 1975, 305, 1250–1251. [Google Scholar] [CrossRef] [PubMed]
- Wormser, G.P.; Nadelman, R.B.; Dattwyler, R.J.; Dennis, D.T.; Shapiro, E.D.; Steere, A.C.; Rush, T.J.; Rahn, D.W.; Coyle, P.K.; Persing, D.H. Practice guidelines for the treatment of Lyme disease. Clinical infectious diseases 2000, 31, S1–S14. [Google Scholar] [CrossRef] [PubMed]
- Muanda, F.T.; Sheehy, O.; Bérard, A. Use of antibiotics during pregnancy and risk of spontaneous abortion. Cmaj 2017, 189, E625–E633. [Google Scholar] [CrossRef] [PubMed]
- Muanda, F.T.; Sheehy, O.; Bérard, A. Use of antibiotics during pregnancy and the risk of major congenital malformations: a population based cohort study. British journal of clinical pharmacology 2017, 83, 2557–2571. [Google Scholar] [CrossRef] [PubMed]
- Wormser, G.P.; Wormser, R.P.; Strle, F.; Myers, R.; Cunha, B.A. How safe is doxycycline for young children or for pregnant or breastfeeding women? Diagnostic microbiology and infectious disease 2019, 93, 238–242. [Google Scholar] [CrossRef]
- Silver, H.M. Lyme disease during pregnancy. Infectious Disease Clinics 1997, 11, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, L.E.; Steere, A.C.; Benach, J.L.; Slade, J.D.; Broome, C.V. Lyme disease during pregnancy. Jama 1986, 255, 3394–3396. [Google Scholar] [CrossRef] [PubMed]
- Strobino, B.A.; Williams, C.L.; Abid, S.; Ghalson, R.; Spierling, P. Lyme disease and pregnancy outcome: A prospective s of two thousand prenatal patients. American journal of obstetrics and gynecology 1993, 169, 367–374. [Google Scholar] [CrossRef]
- Cook, M.J.; Moynan, D.; Avramovic, G.; Lambert, J.S. An In-Depth Review of the Benefits of Antibiotic Use in the Treatment of Borreliosis in Pregnancy. Applied Microbiology 2023, 3, 312–321. [Google Scholar] [CrossRef]
- Lakos, A.; Solymosi, N. Maternal Lyme borreliosis and pregnancy outcome. International Journal of Infectious Diseases 2010, 14, e494–e498. [Google Scholar] [CrossRef]
- Williams, C.; Strobino, B.; Weinstein, A.; Spierling, P.; Medici, F. Maternal Lyme disease and congenital malformations: a cord blood serosurvey in endemic and control areas. Paediatric and Perinatal Epidemiology 1995, 9, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Strobino, B.; Abid, S.; Gewitz, M. Maternal Lyme disease and congenital heart disease: a case-control study in an endemic area. American journal of obstetrics and gynecology 1999, 180, 711–716. [Google Scholar] [CrossRef]
- Shapiro, E.D.; Gerber, M.A.; Holabird, N.B.; Berg, A.T.; Feder Jr, H.M.; Bell, G.L.; Rys, P.N.; Persing, D.H. A controlled trial of antimicrobial prophylaxis for Lyme disease after deer-tick bites. New England Journal of Medicine 1992, 327, 1769–1773. [Google Scholar] [CrossRef]
- Agre, F.; Schwartz, R. The value of early treatment of deer tick bites for the prevention of Lyme disease. American journal of diseases of children 1993, 147, 945–947. [Google Scholar] [CrossRef]
- McGready, R.; Hamilton, K.a.; Simpson, J.a.; Cho, T.; Luxemburger, C.; Edwards, R.; Looareesuwan, S.; White, N.; Nosten, F.; Lindsay, S. Safety of the insect repellent N, N-diethyl-M-toluamide (DEET) in pregnancy. American Journal of Tropical Medicine and Hygiene 2001, 65. [Google Scholar] [CrossRef] [PubMed]
- Koren, G.; Matsui, D.; Bailey, B. DEET-based insect repellents: safety implications for children and pregnant and lactating women. Cmaj 2003, 169, 209–212. [Google Scholar]
- Strausz, S.; Abner, E.; Blacker, G.; Galloway, S.; Hansen, P.; Feng, Q.; Lee, B.T.; Jones, S.E.; Haapaniemi, H.; Raak, S. SCGB1D2 inhibits growth of Borrelia burgdorferi and affects susceptibility to Lyme disease. Nature Communications 2024, 15, 2041. [Google Scholar] [CrossRef]
- Shen, S.; Shin, J.J.; Strle, K.; McHugh, G.; Li, X.; Glickstein, L.J.; Drouin, E.E.; Steere, A.C. Treg cell numbers and function in patients with antibiotic-refractory or antibiotic-responsive Lyme arthritis. Arthritis Rheum 2010, 62, 2127–2137. [Google Scholar] [CrossRef] [PubMed]
- Strle, K.; Sulka, K.B.; Pianta, A.; Crowley, J.T.; Arvikar, S.L.; Anselmo, A.; Sadreyev, R.; Steere, A.C. T-Helper 17 Cell Cytokine Responses in Lyme Disease Correlate With Borrelia burgdorferi Antibodies During Early Infection and With Autoantibodies Late in the Illness in Patients With Antibiotic-Refractory Lyme Arthritis. Clin Infect Dis 2017, 64, 930–938. [Google Scholar] [CrossRef]
- Vudattu, N.K.; Strle, K.; Steere, A.C.; Drouin, E.E. Dysregulation of CD4+CD25(high) T cells in the synovial fluid of patients with antibiotic-refractory Lyme arthritis. Arthritis Rheum 2013, 65, 1643–1653. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.H.; Shapiro, E.D.; Soffer, G.K. A Review of Post-treatment Lyme Disease Syndrome and Chronic Lyme Disease for the Practicing Immunologist. Clin Rev Allergy Immunol 2021. [Google Scholar] [CrossRef] [PubMed]
- Cerar, T.; Ogrinc, K.; Lotric-Furlan, S.; Kobal, J.; Levicnik-Stezinar, S.; Strle, F.; Ruzic-Sabljic, E. Diagnostic value of cytokines and chemokines in lyme neuroborreliosis. Clin Vaccine Immunol 2013, 20, 1578–1584. [Google Scholar] [CrossRef] [PubMed]
- Strle, K.; Shin, J.J.; Glickstein, L.J.; Steere, A.C. Association of a Toll-like receptor 1 polymorphism with heightened Th1 inflammatory responses and antibiotic-refractory Lyme arthritis. Arthritis Rheum 2012, 64, 1497–1507. [Google Scholar] [CrossRef] [PubMed]
- Hawn, T.R.; Misch, E.A.; Dunstan, S.J.; Thwaites, G.E.; Lan, N.T.; Quy, H.T.; Chau, T.T.; Rodrigues, S.; Nachman, A.; Janer, M.; et al. A common human TLR1 polymorphism regulates the innate immune response to lipopeptides. Eur J Immunol 2007, 37, 2280–2289. [Google Scholar] [CrossRef] [PubMed]
- Gwynne, P.J.; Stocks, K.-L.K.; Karozichian, E.S.; Pandit, A.; Hu, L.T. Metabolic modeling predicts unique drug targets in Borrelia burgdorferi. Msystems 2023, 8, e00835–e00823. [Google Scholar] [CrossRef] [PubMed]
- Wagh, D.; Pothineni, V.R.; Inayathullah, M.; Liu, S.; Kim, K.-M.; Rajadas, J. Borreliacidal activity of Borrelia metal transporter A (BmtA) binding small molecules by manganese transport inhibition. Drug design, development and therapy 2015, 805-816.
- Boylan, J.A.; Gherardini, F.C. Determining the cellular targets of reactive oxygen species in Borrelia burgdorferi. Bacterial Pathogenesis: Methods and Protocols 2008, 213-221.
- Boylan, J.A.; Lawrence, K.A.; Downey, J.S.; Gherardini, F.C. Borrelia burgdorferi membranes are the primary targets of reactive oxygen species. Molecular microbiology 2008, 68, 786–799. [Google Scholar] [CrossRef] [PubMed]
- Van Laar, T.A.; Lin, Y.-H.; Miller, C.L.; Karna, S.R.; Chambers, J.P.; Seshu, J. Effect of levels of acetate on the mevalonate pathway of Borrelia burgdorferi. PloS one 2012, 7, e38171. [Google Scholar] [CrossRef] [PubMed]
- Stupica, D.; Bajrović, F.F.; Blagus, R.; Cerar Kišek, T.; Collinet-Adler, S.; Ružić-Sabljić, E.; Velušček, M. Association between statin use and clinical course, microbiologic characteristics, and long-term outcome of early Lyme borreliosis. A post hoc analysis of prospective clinical trials of adult patients with erythema migrans. Plos one 2021, 16, e0261194. [Google Scholar] [CrossRef]
- Van Laar, T.A.; Hole, C.; Karna, S.R.; Miller, C.L.; Reddick, R.; Wormley, F.L.; Seshu, J. Statins reduce spirochetal burden and modulate immune responses in the C3H/HeN mouse model of Lyme disease. Microbes and infection 2016, 18, 430–435. [Google Scholar] [CrossRef]
- Parveen, N.; Cornell, K.A.; Bono, J.L.; Chamberland, C.; Rosa, P.; Leong, J.M. Bgp, a secreted glycosaminoglycan-binding protein of Borrelia burgdorferi strain N40, displays nucleosidase activity and is not essential for infection of immunodeficient mice. Infection and immunity 2006, 74, 3016–3020. [Google Scholar] [CrossRef] [PubMed]
- Parveen, N.; Cornell, K.A. Methylthioadenosine/S-adenosylhomocysteine nucleosidase, a critical enzyme for bacterial metabolism. Molecular microbiology 2011, 79, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Cornell, K.A.; Primus, S.; Martinez, J.A.; Parveen, N. Assessment of methylthioadenosine/S-adenosylhomocysteine nucleosidases of Borrelia burgdorferi as targets for novel antimicrobials using a novel high-throughput method. Journal of antimicrobial chemotherapy 2009, 63, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Chakraborti, M.; Schlachter, S.; Primus, S.; Wagner, J.; Sweet, B.; Carr, Z.; Cornell, K.A.; Parveen, N. Evaluation of nucleoside analogs as antimicrobials targeting unique enzymes in borrelia burgdorferi. Pathogens 2020, 9, 678. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.; Brown, A.V.; Matluck, N.E.; Hu, L.T.; Lewis, K. Borrelia burgdorferi, the causative agent of Lyme disease, forms drug-tolerant persister cells. Antimicrobial agents and chemotherapy 2015, 59, 4616–4624. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K. Persister cells, dormancy and infectious disease. Nature Reviews Microbiology 2007, 5, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Maisonneuve, E.; Gerdes, K. Molecular mechanisms underlying bacterial persisters. Cell 2014, 157, 539–548. [Google Scholar] [CrossRef]
- Feng, J.; Wang, T.; Shi, W.; Zhang, S.; Sullivan, D.; Auwaerter, P.G.; Zhang, Y. Identification of novel activity against Borrelia burgdorferi persisters using an FDA approved drug library. Emerging microbes & infections 2014, 3, 1–8. [Google Scholar]
- Marques, A. Chronic Lyme disease: a review. Infectious disease clinics of North America 2008, 22, 341–360. [Google Scholar] [CrossRef]
- Jutras, B.L.; Lochhead, R.B.; Kloos, Z.A.; Biboy, J.; Strle, K.; Booth, C.J.; Govers, S.K.; Gray, J.; Schumann, P.; Vollmer, W. Borrelia burgdorferi peptidoglycan is a persistent antigen in patients with Lyme arthritis. Proceedings of the National Academy of Sciences 2019, 116, 13498–13507. [Google Scholar] [CrossRef]
- DeHart, T.G.; Kushelman, M.R.; Hildreth, S.B.; Helm, R.F.; Jutras, B.L. The unusual cell wall of the Lyme disease spirochaete Borrelia burgdorferi is shaped by a tick sugar. Nature Microbiology 2021, 6, 1583–1592. [Google Scholar] [CrossRef]
- Melia, M.T.; Auwaerter, P.G. Time for a different approach to Lyme disease and long-term symptoms. N Engl J Med 2016, 374, 1277–1278. [Google Scholar] [CrossRef]
- Kullberg, B.J.; Vrijmoeth, H.D.; van de Schoor, F.; Hovius, J.W. Lyme borreliosis: diagnosis and management. Bmj 2020, 369. [Google Scholar] [CrossRef] [PubMed]
- ED, S. Clinical practice: Lyme disease. N Engl J Med 2014, 371, 683–684. [Google Scholar] [CrossRef]
- Feder Jr, H.M.; Johnson, B.J.; O'Connell, S.; Shapiro, E.D.; Steere, A.C.; Wormser, G.P.; Group, A.H.I.L.D. A critical appraisal of “chronic Lyme disease”. New England Journal of Medicine 2007, 357, 1422–1430. [Google Scholar] [CrossRef] [PubMed]
- Zubcevik, N.; Mao, C.; Wang, Q.M.; Bose, E.L.; Octavien, R.N.; Crandell, D.; Wood, L.J. Symptom clusters and functional impairment in individuals treated for Lyme borreliosis. Frontiers in Medicine 2020, 7, 464. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.M.; Frost, A. Illness perceptions, coping, and health-related quality of life among individuals experiencing chronic Lyme disease. Chronic Illness 2022, 18, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Klempner, M.S.; Baker, P.J.; Shapiro, E.D.; Marques, A.; Dattwyler, R.J.; Halperin, J.J.; Wormser, G.P. Treatment trials for post-Lyme disease symptoms revisited. The American journal of medicine 2013, 126, 665–669. [Google Scholar] [CrossRef]
- Chaconas, G.; Castellanos, M.; Verhey, T.B. Changing of the guard: How the Lyme disease spirochete subverts the host immune response. Journal of Biological Chemistry 2020, 295, 301–313. [Google Scholar] [CrossRef]
- Tracy, K.E.; Baumgarth, N. Borrelia burgdorferi manipulates innate and adaptive immunity to establish persistence in rodent reservoir hosts. Frontiers in immunology 2017, 8, 241161. [Google Scholar] [CrossRef]
- Feng, J.; Li, T.; Yee, R.; Yuan, Y.; Bai, C.; Cai, M.; Shi, W.; Embers, M.; Brayton, C.; Saeki, H. Stationary phase persister/biofilm microcolony of Borrelia burgdorferi causes more severe disease in a mouse model of Lyme arthritis: implications for understanding persistence, Post-treatment Lyme Disease Syndrome (PTLDS), and treatment failure. Discovery medicine 2019, 27, 125–138. [Google Scholar]
- Caskey, J.R.; Embers, M.E. Persister development by Borrelia burgdorferi populations in vitro. Antimicrobial agents and chemotherapy 2015, 59, 6288–6295. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Shi, W.; Zhang, S.; Zhang, Y. Persister mechanisms in Borrelia burgdorferi: implications for improved intervention. Emerging microbes & infections 2015, 4, 1–3. [Google Scholar]
- Cabello, F.C.; Godfrey, H.P.; Bugrysheva, J.V.; Newman, S.A. Sleeper cells: the stringent response and persistence in the Borreliella (Borrelia) burgdorferi enzootic cycle. Environmental microbiology 2017, 19, 3846–3862. [Google Scholar] [CrossRef]
- Hodzic, E.; Imai, D.M.; Escobar, E. Generality of post-antimicrobial treatment persistence of Borrelia burgdorferi strains N40 and B31 in genetically susceptible and resistant mouse strains. Infection and immunity 2019, 87. [Google Scholar] [CrossRef]
- Straubinger, R.K.; Summers, B.A.; Chang, Y.-F.; Appel, M. Persistence of Borrelia burgdorferi in experimentally infected dogs after antibiotic treatment. Journal of clinical microbiology 1997, 35, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Nadelman, R.B.; Nowakowski, J.; Forseter, G.; Bittker, S.; Cooper, D.; Goldberg, N.; McKenna, D.; Wormser, G.P. Failure to isolate Borrelia burgdorferi after antimicrobial therapy in culture-documented Lyme borreliosis associated with erythema migrans: report of a prospective study. The American journal of medicine 1993, 94, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.J.; Wormser, G.P. The clinical relevance of studies on Borrelia burgdorferi persisters. The American Journal of Medicine 2017, 130, 1009–1010. [Google Scholar] [CrossRef]
- Hunfeld, K.-P.; Kraiczy, P.; Kekoukh, E.; Schäfer, V.; Brade, V. Standardised in vitro susceptibility testing of Borrelia burgdorferi against well-known and newly developed antimicrobial agents—possible implications for new therapeutic approaches to Lyme disease. International journal of medical microbiology 2002, 291, 125–137. [Google Scholar] [CrossRef]
- Steere, A.C. Posttreatment Lyme disease syndromes: distinct pathogenesis caused by maladaptive host responses. The Journal of clinical investigation 2020, 130, 2148–2151. [Google Scholar] [CrossRef]
- Aucott, J.N.; Soloski, M.J.; Rebman, A.W.; Crowder, L.A.; Lahey, L.J.; Wagner, C.A.; Robinson, W.H.; Bechtold, K.T. CCL19 as a chemokine risk factor for posttreatment Lyme disease syndrome: a prospective clinical cohort study. Clinical and Vaccine Immunology 2016, 23, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Strle, K.; Stupica, D.; Drouin, E.E.; Steere, A.C.; Strle, F. Elevated levels of IL-23 in a subset of patients with post–Lyme disease symptoms following erythema migrans. Clinical infectious diseases 2014, 58, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Uhde, M.; Ajamian, M.; Li, X.; Wormser, G.P.; Marques, A.; Alaedini, A. Expression of C-reactive protein and serum amyloid A in early to late manifestations of Lyme disease. Clinical infectious diseases 2016, 63, 1399–1404. [Google Scholar] [CrossRef] [PubMed]
- Jacek, E.; Fallon, B.A.; Chandra, A.; Crow, M.K.; Wormser, G.P.; Alaedini, A. Increased IFNα activity and differential antibody response in patients with a history of Lyme disease and persistent cognitive deficits. Journal of neuroimmunology 2013, 255, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Klempner, M.S.; Hu, L.T.; Evans, J.; Schmid, C.H.; Johnson, G.M.; Trevino, R.P.; Norton, D.; Levy, L.; Wall, D.; McCall, J. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. New England Journal of Medicine 2001, 345, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D.; Reeves, W.C.; Lloyd, A. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: prospective cohort study. Bmj 2006, 333, 575. [Google Scholar] [CrossRef] [PubMed]
- Batheja, S.; Nields, J.A.; Landa, A.; Fallon, B.A. Post-treatment lyme syndrome and central sensitization. The Journal of neuropsychiatry and clinical neurosciences 2013, 25, 176–186. [Google Scholar] [CrossRef]
- Wills, A.B.; Spaulding, A.B.; Adjemian, J.; Prevots, D.R.; Turk, S.-P.; Williams, C.; Marques, A. Long-term follow-up of patients with Lyme disease: longitudinal analysis of clinical and quality-of-life measures. Clinical Infectious Diseases 2016, 62, 1546–1551. [Google Scholar] [CrossRef]
- Aucott, J.N.; Yang, T.; Yoon, I.; Powell, D.; Geller, S.A.; Rebman, A.W. Risk of post-treatment Lyme disease in patients with ideally-treated early Lyme disease: A prospective cohort study. International Journal of Infectious Diseases 2022, 116, 230–237. [Google Scholar] [CrossRef]
- Hirsch, A.G.; Poulsen, M.N.; Nordberg, C.; Moon, K.A.; Rebman, A.W.; Aucott, J.N.; Heaney, C.D.; Schwartz, B.S. Risk factors and outcomes of treatment delays in Lyme disease: a population-based retrospective cohort study. Frontiers in Medicine 2020, 7, 560018. [Google Scholar] [CrossRef]
- Kaplan, R.; Trevino, R.; Johnson, G.; Levy, L.; Dornbush, R.; Hu, L.; Evans, J.; Weinstein, A.; Schmid, C.; Klempner, M. Cognitive function in post-treatment Lyme disease Do additional antibiotics help? Neurology 2003, 60, 1916–1922. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; Hyman, L.G.; Grimson, R.; Coyle, P.; Melville, P.; Ahnn, S.; Dattwyler, R.; Chandler, B. Study and treatment of post Lyme disease (STOP-LD) A randomized double masked clinical trial. Neurology 2003, 60, 1923–1930. [Google Scholar] [CrossRef] [PubMed]
- Fallon, B.A.; Keilp, J.G.; Corbera, K.M.; Petkova, E.; Britton, C.B.; Dwyer, E.; Slavov, I.; Cheng, J.; Dobkin, J.; Nelson, D. A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy. Neurology 2008, 70, 992–1003. [Google Scholar] [CrossRef]
- Patel, R.; Grogg, K.L.; Edwards, W.D.; Wright, A.J.; Schwenk, N.M. Death from inappropriate therapy for Lyme disease. Clinical infectious diseases 2000, 31, 1107–1109. [Google Scholar] [CrossRef] [PubMed]
- Berende, A.; ter Hofstede, H.J.; Vos, F.J.; van Middendorp, H.; Vogelaar, M.L.; Tromp, M.; van den Hoogen, F.H.; Donders, A.R.T.; Evers, A.W.; Kullberg, B.J. Randomized trial of longer-term therapy for symptoms attributed to Lyme disease. New England Journal of Medicine 2016, 374, 1209–1220. [Google Scholar] [CrossRef] [PubMed]
- Goodlet, K.J.; Fairman, K.A. Adverse events associated with antibiotics and intravenous therapies for post–Lyme disease syndrome in a commercially insured sample. Clinical Infectious Diseases 2018, 67, 1568–1574. [Google Scholar] [CrossRef] [PubMed]
- Lantos, P.M.; Rumbaugh, J.; Bockenstedt, L.K.; Falck-Ytter, Y.T.; Aguero-Rosenfeld, M.E.; Auwaerter, P.G.; Baldwin, K.; Bannuru, R.R.; Belani, K.K.; Bowie, W.R. Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 guidelines for the prevention, diagnosis and treatment of Lyme disease. Clinical Infectious Diseases 2021, 72, e1–e48. [Google Scholar] [CrossRef]
- Marzec, N.S. Serious bacterial infections acquired during treatment of patients given a diagnosis of chronic Lyme disease—United States. MMWR. Morbidity and mortality weekly report 2017, 66. [Google Scholar] [CrossRef] [PubMed]
- Stiehm, E.R. Adverse effects of human immunoglobulin therapy. Transfusion medicine reviews 2013, 27, 171–178. [Google Scholar] [CrossRef]
- De Wilde, M.; Speeckaert, M.; Callens, R.; Van Biesen, W. Ceftriaxone-induced immune hemolytic anemia as a life-threatening complication of antibiotic treatment of ‘chronic Lyme disease’. Acta clinica Belgica 2017, 72, 133–137. [Google Scholar] [CrossRef]
- Maksimyan, S.; Syed, M.S.; Soti, V. Post-treatment Lyme disease syndrome: need for diagnosis and treatment. Cureus 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Bockenstedt, L.K.; Radolf, J.D. Editorial commentary: xenodiagnosis for posttreatment Lyme disease syndrome: resolving the conundrum or adding to it? 2014, 58, 946–948.
- Hodzic, E.; Feng, S.; Holden, K.; Freet, K.J.; Barthold, S.W. Persistence of Borrelia burgdorferi following antibiotic treatment in mice. Antimicrobial agents and chemotherapy 2008, 52, 1728–1736. [Google Scholar] [CrossRef] [PubMed]
- Kamp, H.D.; Swanson, K.A.; Wei, R.R.; Dhal, P.K.; Dharanipragada, R.; Kern, A.; Sharma, B.; Sima, R.; Hajdusek, O.; Hu, L.T. Design of a broadly reactive Lyme disease vaccine. npj Vaccines 2020, 5, 33. [Google Scholar] [CrossRef] [PubMed]
- Comstedt, P.; Hanner, M.; Schüler, W.; Meinke, A.; Lundberg, U. Design and development of a novel vaccine for protection against Lyme borreliosis. PloS one 2014, 9, e113294. [Google Scholar]
- Comstedt, P.; Hanner, M.; Schüler, W.; Meinke, A.; Schlegl, R.; Lundberg, U. Characterization and optimization of a novel vaccine for protection against Lyme borreliosis. Vaccine 2015, 33, 5982–5988. [Google Scholar] [CrossRef] [PubMed]
- Pine, M.; Arora, G.; Hart, T.M.; Bettini, E.; Gaudette, B.T.; Muramatsu, H.; Tombácz, I.; Kambayashi, T.; Tam, Y.K.; Brisson, D. Development of an mRNA-lipid nanoparticle vaccine against Lyme disease. Molecular Therapy 2023, 31, 2702–2714. [Google Scholar] [CrossRef] [PubMed]
- Marconi, R.T.; Garcia-Tapia, D.; Hoevers, J.; Honsberger, N.; King, V.L.; Ritter, D.; Schwahn, D.J.; Swearingin, L.; Weber, A.; Winkler, M.T.C. VANGUARD® crLyme: A next generation Lyme disease vaccine that prevents B. burgdorferi infection in dogs. Vaccine: X 2020, 6, 100079. [Google Scholar] [CrossRef] [PubMed]
- Marcinkiewicz, A.L.; Lieknina, I.; Kotelovica, S.; Yang, X.; Kraiczy, P.; Pal, U.; Lin, Y.-P.; Tars, K. Eliminating factor H-binding activity of Borrelia burgdorferi CspZ combined with virus-like particle conjugation enhances its efficacy as a Lyme disease vaccine. Frontiers in immunology 2018, 9, 325322. [Google Scholar] [CrossRef]
- Phase 2 Study Of VLA15, A Vaccine Candidate Against Lyme Borreliosis, In A Healthy Pediatric And Adult Study Population. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04801420 (accessed on.
- Dai, J.; Wang, P.; Adusumilli, S.; Booth, C.J.; Narasimhan, S.; Anguita, J.; Fikrig, E. Antibodies against a tick protein, Salp15, protect mice from the Lyme disease agent. Cell host & microbe 2009, 6, 482–492. [Google Scholar]
- Bobe, J.R.; Jutras, B.L.; Horn, E.J.; Embers, M.E.; Bailey, A.; Moritz, R.L.; Zhang, Y.; Soloski, M.J.; Ostfeld, R.S.; Marconi, R.T. Recent progress in Lyme disease and remaining challenges. Frontiers in medicine 2021, 8, 666554. [Google Scholar] [CrossRef]
- Levin, S.; Harris, A.A. Principles of combination therapy. Bulletin of the New York Academy of Medicine 1975, 51, 1020. [Google Scholar] [PubMed]
- Keren, I.; Kaldalu, N.; Spoering, A.; Wang, Y.; Lewis, K. Persister cells and tolerance to antimicrobials. FEMS microbiology letters 2004, 230, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Spoering, A.L.; Lewis, K. Biofilms and planktonic cells of Pseudomonas aeruginosa have similar resistance to killing by antimicrobials. Journal of bacteriology 2001, 183, 6746–6751. [Google Scholar] [CrossRef] [PubMed]
- Ulloa, L.; Quiroz-Gonzalez, S.; Torres-Rosas, R. Nerve stimulation: immunomodulation and control of inflammation. Trends in molecular medicine 2017, 23, 1103–1120. [Google Scholar] [CrossRef] [PubMed]
- Akoolo, L.; Djokic, V.; Rocha, S.C.; Ulloa, L.; Parveen, N. Sciatic–Vagal Nerve Stimulation by Electroacupuncture Alleviates Inflammatory Arthritis in Lyme Disease-Susceptible C3H Mice. Frontiers in immunology 2022, 13, 930287. [Google Scholar] [CrossRef]
- Adams, A.; Hipple, A.; Thompson, S.H. Acupuncture and Chinese Herbs Relieve Long-Term Symptoms of Lyme Disease: A Case Report. Convergent Points: An East-West Case Report Journal 2023, 2. [Google Scholar]
- Bartecchi, C.E. Efficacy of acupuncture vs placebo. In Proceedings of the Mayo Clinic Proceedings; 2006; p. 1263. [Google Scholar]
- Conn, M.; Avery, S.; Bhatia, A.; Alnamos, A.A. Gene Therapy for Post-Treatment Lyme Disease Syndrome.
Figure 1.
Lyme disease treatment at different stages of infection and PTLDS.
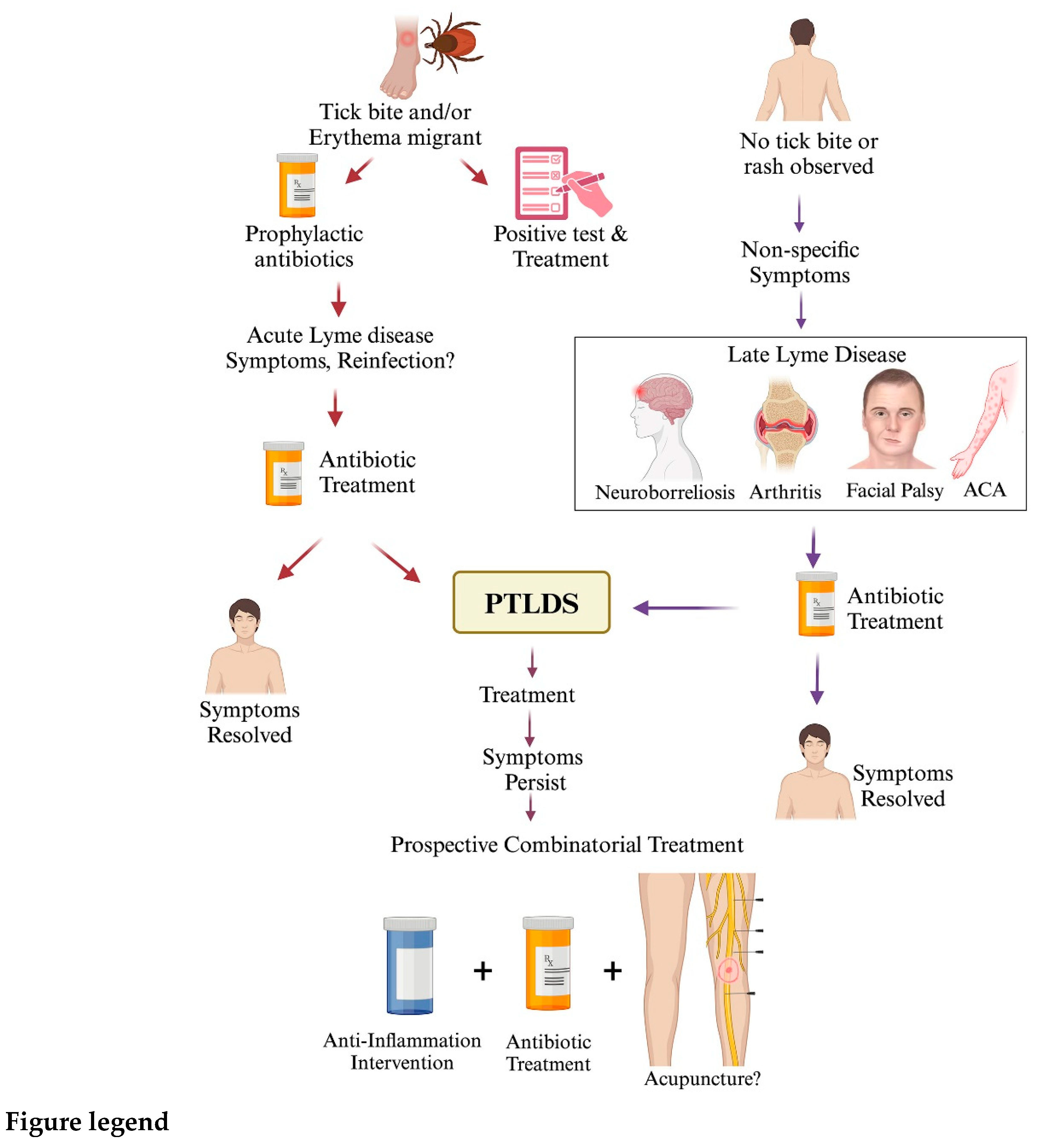

Table 1.
Recommended antimicrobial regimens for treating patients with Lyme disease.
| Drug | Dosage for adults | Dosage for Children | Duration(Days) | References |
| Doxycycline | 100 mg, twice per day orally | 4.4 mg/kg per day orally, divided into 2 doses | 10–14 | [30,33,35,36,37,38,39,40,41,42] |
| Amoxicillin | 500 mg, three times per day orally | 50 mg/kg per day orally, divided into 3 doses | 14 | [30,33,34,36,40,41,43] |
| Cefuroxime | 500 mg, twice per day orally | 30 mg/kg per day orally, divided into 2 doses | 14 | [30,34,40,43,44,45] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



