
Submitted:
01 May 2024
Posted:
02 May 2024
You are already at the latest version
Abstract
Buruli ulcer is a chronic ulcerative disease of skin and subcutaneous tissues caused by infection with Mycobacterium ulcerans. Although Australian possums are known to be susceptible to Buruli ulcer, many aspects of the disease in possums, including welfare impacts, remain largely unreported. Severe clinical Buruli ulcer was identified in four common ringtail possums (Pseudocheirus peregrinus) from Melbourne, Victoria. All four possums were euthanised due to welfare concerns and poor prognosis, based on the presence of deep ulcerative lesions to paws, some of which exposed carpal or tarsal bones. These lesions were considered likely to cause partial or complete loss of limb function, which would severely affect the welfare and survival of these wild arboreal animals. Histologically, there was severe ulcerative necrotising pyogranulomatous dermatitis, panniculitis, and myositis, with intralesional acid-fast bacteria. M. ulcerans was detected by real-time PCR in all swabs and biological tissues collected from all four cases. Buruli ulcer may be an important and under-recognised cause of poor possum welfare in endemic areas. In addition to severe cutaneous lesions, infection extends to underlying bones and joints, and the systemic distribution of M. ulcerans throughout all major tissues and internal organs, as observed in these four cases, may further impact the health and fitness of infected possums. Further research is needed to investigate the epidemiology, pathogenesis and impacts of Buruli ulcer in possums, and to inform the design of interventions that may protect the health and welfare of possums and other affected animal species.
Keywords:
Animal welfare
; Buruli ulcer
; Mycobacterium ulcerans
; possums
; wild animals
Introduction
Buruli, or Bairnsdale, ulcer (BU) is a chronic, necrotising and debilitating disease of skin and subcutaneous tissues caused by Mycobacterium ulcerans (MU). BU is predominantly described and reported as a human disease, but cases are occasionally reported in Australian domestic and wild animals [1,2,3]. Most human cases are reported in sub-Saharan Africa, however the incidence of BU appears to be declining in this region[4]. Australia is the only high-income country reporting significant endemic human BU[4]. The most significant disease focus is in Victoria, where cases have been increasing in number, severity and geographical distribution over the past decade[5,6], with suburban cases now frequently reported in the state’s two largest cities, Melbourne and Geelong.
BU appears to be both vector-borne and zoonotic in Victoria, with increasing evidence implicating certain species of mosquito and possum as MU vectors and reservoirs, respectively[7,8,9]. Common ringtail (CRT, Pseudocheirus peregrinus) and common brushtail (Trichosurus vulpecula) possums, both of which are endemic and abundant throughout Victoria, can excrete significant amounts of viable MU into the environment via their faeces[7]. Possums are also susceptible to clinical disease: a 2014 paper described clinical BU in 27 possums, most of which had cutaneous ulcers on the face (exposing bone in one case), limbs and/or tail[10]. Pathology and/or the presence of MU was confirmed by PCR in some internal tissues including lung and liver[10], however the welfare impacts of BU on the affected possums were not evaluated or discussed.
We conducted surveillance of free-living possums across Victoria as part of the NHMRC-funded ‘Beating Buruli in Victoria’ project led by the University of Melbourne’s Doherty Institute and the Melbourne Veterinary School (UniMelb AEC 22910; DELWP permits 10009447 and 10010257). Possums that died or were euthanised for any reason at two veterinary clinics in Werribee and North Melbourne, Victoria, between May 2021 and December 2022 were collected and stored at -20°C. Necropsies were conducted on thawed possums at the Melbourne Veterinary School. Findings were recorded on customised necropsy sheets (see Supplementary document 1) that include a silhouette for mapping any cutaneous lesions indicative of BU, and categorisation of clinical BU as mild, moderate or severe, based on the World Health Organization’s BU disease classification for assessment of human cases[11]. Sample collection included plain microbiological swabs of each possum’s oral cavity, cloaca, pouch (where applicable) and any skin lesions, and a duplicate set of tissue and organ sections (full list in Supplementary document 1) and any dissected ulcerative skin lesions collected into formalin for histopathology, and into cryovials stored at -80° for PCR, culture and genomic analysis where indicated.
This case series describes the clinical and laboratory findings from four cases of severe BU in CRTs that were euthanised due to the welfare impacts of the disease.
Case Reports
Case 1
History
An adult male CRT that regularly visited a residential property in Essendon, Victoria, was observed in April 2021 to have cutaneous ulcerations. Several CRTs frequented this property, including a female CRT with severe cutaneous lesions captured at this address in 2019, which was euthanised and later diagnosed with BU[12]. The male possum was captured and taken to a veterinary clinic, where it was euthanised due to the severity of its ulcerative lesions and a high clinical suspicion of BU given the location’s history.
Post-Mortem Examination
The body condition score was assessed as 2 out of 5. Two deep ulcerative cutaneous lesions were observed on the right hind paw and scrotum, which would likely have been aligned and in contact when the possum was sitting crouched (Figure 1). The first digit of the right hind paw was ulcerated down to the bone at the proximal aspect of the first metacarpal, with the entire distal portion of the bone exposed. The ulcer on the ventral scrotum measured approximately 3 cm x 2 cm, extended to the level of the testicular fascia, and was granulated and proliferative in appearance, with undermined edges. Multifocally, nodules of approximately 1 mm diameter, presumptively interpreted as microgranulomas, were observed throughout the lungs.
Laboratory Investigations
MU was detected by PCR testing on all swabs (skin, oral cavity and cloaca), and on all tissues collected during necropsy (ulcers, ear, nose, front footpad, hind footpad, submandibular lymph node, lung, liver, spleen, kidney, adrenal gland, body cavity fluid, gut contents, stomach, small intestine, caecum, large intestine, faeces). MU was cultured from a sample of the testicular ulcer, and genome sequencing confirmed that the genotype matched the MU isolate obtained from the female CRT confirmed with BU from the same location in 2019.
Histological examination of the skin lesions revealed the presence of severe ulcerative necrotising pyogranulomatous dermatitis, cellulitis and myositis, with abundant intralesional Gram positive and acid-fast bacilli as observed with Ziehl-Neelsen (ZN) staining. Severe autolysis and freeze-thaw artifact prevented meaningful histological interpretation of the organ sections, including the lungs.
Case 2
History
An adult male CRT with multiple skin lesions was captured in Bentleigh, Victoria in December 2021, and taken to a veterinary clinic. The severity of its cutaneous ulcerations necessitated euthanasia.
Post-Mortem Examination
Eight ulcerative lesions were identified (Figure 2):
- Single dry erythematous ulcers approximately 1 cm2 in diameter with white margins on the palmar surfaces of each fore paw; two lateral carpal bones of the left paw were exposed;
- Two shallow dry, scabbed lesions approximately 1-1.5 cm2 on the plantar surfaces of each hind paw;
- One shallow erythematous ulcer encircled by white margins surrounding the central cloaca; and
- One approximately 3 mm2 blackened oedematous ulcer with necrotic focus encompassing the distal tail tip.
The body condition score was assessed as 2/5. No other abnormalities were detected at necropsy.
Laboratory Investigations
MU was detected by PCR in all swabs (ulcers, oral cavity, cloaca) and all tissue samples collected during necropsy (ulcers, ear, nose, front footpad, hind footpad, submandibular lymph node, heart, lung, liver, spleen, kidney, adrenal gland, body cavity fluid, gut contents, stomach, small intestine, caecum, large intestine, faeces).
Histopathology of the skin lesions confirmed the presence of severe ulcerative necrotising pyogranulomatous dermatitis and panniculitis, with intralesional acid-fast bacilli observed in ZN-stained sections, in four grossly observed ulcers (tail, left hind, and right hind limb ulcers). The tail and one right forelimb ulcer were the deepest, expanding to the underlying bone. Histologically, the left forelimb lesion was one of pyogranulomatous dermatitis, with the overlying epidermis showing epidermal hyperplasia and other changes consistent with ongoing cutaneous healing. All lesions were ZN negative. The liver showed minimal multifocal lymphoplasmacytic aggregation, interpreted as incidental. The pancreas showed possible mild acinar atrophy, consistent with poor nutritional condition. The heart, brain, meninges, kidneys, and stomach showed no noteworthy changes. The presence of freeze-thaw artifact and autolysis effects in the intestines and other examined organs prevented meaningful evaluation.
Case 3
History
A moribund adult female CRT was found on the ground in Essendon, Victoria in October 2022. It was taken to a veterinary clinic, where it was euthanised due to severe swelling and necrosis of three of its paws.
Post-Mortem Examination
Body condition was assessed as poor (1.5/5). Severe ulcerative lesions were observed on three paws (see Figure 3), and on the tail:
- The right forepaw was markedly oedematous, and bore an approximately 2.5 cm x 1 cm almost circumferential proliferative ulcerative lesion covering most of its palmar aspect and extending partially to the dorsal aspect of digit 1.
- The dorsal surface of the left hind paw was similarly swollen and bore an approximately 2 cm x 1.5 cm ulcer between digits 1 and 2, with deeply undermined caudal wound edges. The ulcer was covered by a plug of necrotic material and extended deep into the underlying muscle and tendon.
- The craniodorsal aspect of digit 4 of the right hind paw was similarly swollen, ulcerated to the level of the underlying subcutis, and contained thick purulent exudate; the nail was absent.
- Two shallow dry circular ulcers were present on the hairless ventral surface of the tail, approximately halfway down the white furred section, and approximately 1.5 cm apart. The proximal ulcer was approximately 3 mm2 and the distal ulcer was approximately 6 mm2.
Laboratory Investigations
All swabs (ulcers, oral cavity, cloaca, pouch) and all tissues collected during necropsy (ulcers, ear, nose, front footpad, hind footpad, submandibular lymph node, heart, lung, liver, spleen, kidney, adrenal gland, body cavity fluid, gut contents, stomach, small intestine, caecum, large intestine, faeces) were PCR positive for MU.
Histologically, the cutaneous ulcers from the paws showed exceedingly severe changes, consisting of ulcerative necrotising pyogranulomatous dermatitis and cellulitis with myriad bacteria both on the surface and deep within the dermis and underlying tissues, that were gram positive (surface) and ZN positive (dermis, subcutis). The right hindlimb ulcer was covered by thick serocellular crust. The right forelimb ulcer appeared to show more extensive necrosis.
There was marked pulmonary oedema, with thrombosis of several medium calibre vessels and several mild lymphohistiocytic aggregates, however granulomas were not definitively detected. Diffuse moderate periportal, random and intra-sinusoidal aggregation of neutrophils and lymphocytes and fewer histiocytes were observed in liver sections (moderate neutrophilic, lymphohistiocytic hepatitis). No bacteria were observed on histochemical staining of lung, liver or kidney sections. The brain, heart, kidneys, spleen, and stomach showed no noteworthy changes.
Case 4
History
A trapping event was conducted in December 2022 on the Essendon property where Case 1 and the previous BU-positive female CRT from 2019 were identified. This was undertaken in response to reports from the resident of additional possums with lesions.
A young adult male CRT was trapped and examined under general anaesthesia (isoflurane in oxygen administered via face mask). Body condition score was assessed as 2/5, and the coat appeared dull. The left hind paw was grossly swollen to approximately twice the normal size, with a suppurative linear opening on the dorsal aspect. Examination and palpation of the paw indicated structural deformities and likely function loss. Three partially contracted ulcerative lesions were also observed on the tail. The possum was euthanised on welfare grounds due to the severity of the hind paw lesions.
Post-Mortem Examination
- There was an approximately 4 mm x 2 mm linear epidermal ulcer exuding suppurative material on the dorsal aspect of the markedly oedematous left dorsal hind paw, dissection through which revealed a tunnelling wound that extended through the subcutaneous tissues to a central cavity involving striated muscle, ligaments and tendons (see Figure 4).
- Three discrete, scabbed, dry, 3-5 mm2 ulcerative lesions were present on the ventral surface of the tail: two on the proximal portion, and the third in the proximal portion of the distal white section.
No noteworthy macroscopic changes were detected in the remaining body systems.
Laboratory Investigations
PCR testing confirmed the presence of MU DNA in all swabs (ulcers, oral cavity, cloaca) and all tissues (ulcers, ear, nose, front footpad, hind footpad, submandibular lymph node, heart, lung, liver, spleen, kidney, adrenal gland, body cavity fluid, gut contents, stomach, small intestine, caecum, large intestine, faeces, bone marrow) collected during necropsy.
Histologic examination of the lesions revealed widespread dermal and subcutaneous necrosis, and discrete deep ulcers extending to the underlying subcutaneous connective tissue and striated muscle. The ulcer beds were filled with debris, fibrin, oedema fluid and degenerate leukocytes. There was mild epidermal hyperplasia of the tail ulcer margins, and lymphoid aggregates multifocally in the subcutis. ZN staining revealed moderate to large numbers of acid-fast bacteria in all lesions, concentrated in areas of tissue necrosis. Multifocal, mild to moderate portal hepatitis was observed, however the presence of freeze-thaw artifact and autolysis effects prevented further detection and interpretation of other changes that may have been present in this and other tissues.
Discussion
This report describes four cases of severe BU in CRTs from Melbourne’s inner suburbs, where BU is considered endemic. These possums, euthanised due to welfare implications of the disease, all exhibited severe deep ulceration of one or more paws with swelling, necrosis and destruction of skin and underlying tissue, and exposed carpal/tarsal bones in two cases. Histological examination of the cutaneous ulcerations revealed severe ulcerative necrotising pyogranulomatous dermatitis and cellulitis, with intralesional Gram-positive and acid-fast bacteria observed both superficially and deep within the lesions.
Systemic infections were also confirmed in all four possums, with MU detected by PCR in all tissue and internal organ samples collected during necropsy. Faeces collected from all four possums were also PCR positive for MU, implicating these possums as potential sources of environmental contamination for zoonotic transmission to humans. Mild to moderate hepatitis was observed in Cases 3 and 4, and pulmonary changes were observed in Cases 1 and 3. No other significant histopathological changes were noted in the other examined organs, and no acid-fast bacteria were observed in stained organ or tissue sections. This could indicate that the presence of MU in organs (confirmed by PCR) was not associated with pathological changes, or may reflect inadvertent sampling bias or the effects of freeze-thaw artifacts and autolysis that were present to varying degrees in all four possums. In future, conducting necropsies on fresh rather than frozen possums, and/or performing in-situ PCR or immunohistochemistry with an MU antibody on tissue blocks may better detect MU presence or absence within organs of PCR-positive possums.
Severe, chronic BU as described in these four cases would likely have affected all Five Domains[13] of the possums’ welfare. Assessment of the size, severity and locations of the ulcerative cutaneous lesions indicated likely functional impairment of affected limbs, thereby impeding the possums’ normal behaviours, and restricting their ability to navigate their environments and obtain food and water. Despite the lack of histopathological changes detected in these cases as discussed above, the systemic distribution of MU bacteria throughout all the major internal organs, as reported here, may be associated with impaired function of cardiovascular, respiratory, digestive, reproductive and/or immune systems, which would further reduce animal mobility, fitness and welfare. The below average body condition scores of these four possums and the possible pancreatic atrophy observed in Case 2 indicate reduced ability to obtain sufficient nutrition, and could reflect systemic impacts of severe BU. Extensive ulcerative lesions, particularly of the oedematous type as observed in cases 3 and 4, may also cause chronic pain[14], which could further affect the mental domain of severely affected animals. These findings suggest that BU may be an important cause of impaired possum health and welfare.
Interestingly, the presence of epidermal hyperplasia and multifocal lymphoid aggregates observed in the subcutis of Case 2′s left forelimb lesion and at least one of Case 4’s tail ulcers indicate that some level of lesion healing is possible in CRTs. This is a novel finding in this species; to date, spontaneous resolution of BU lesions has only been reported in one common and one mountain brushtail possum[10], however the long-term outcomes of the lesions are unknown as both individuals were lost to follow up. Complete resolution of untreated BU lesions can occur in people, however the mechanism by which the host’s immune system is able to overcome the immunosuppressive effects of the mycolactone toxin produced by MU is unclear[15]. The frequency, extent and mechanisms by which spontaneous lesion healing occurs in possums are yet to be determined.
The distribution of BU lesions may give an insight into the methods by which possums become infected with MU. The predominance of BU lesions occurring on the distal limbs and tails of these four possums aligns with previously published findings by Fyfe, et al. [7] and O’Brien, et al. [10], who also reported lesions on possums’ noses, lips and ears. These relatively less furred regions may be more susceptible to bites from MU-harbouring mosquitoes. Paws and tails used for climbing may more frequently incur micro-traumas that are susceptible to bacterial invasion; similarly, faces and ears may receive more injuries during fights with other possums. Direct BU transmission from a possum was recently described in a Victorian man who developed BU on his finger several months after being bitten by a CRT[16]. While ingestion of MU via contaminated food or water might explain the transient MU faecal positivity observed in some clinically unaffected possums[7,10], it is less likely to cause severe cutaneous ulcerations as observed in these four cases.
BU is not currently a notifiable animal disease in Victoria, and a low awareness of the disease among veterinarians means BU cases in animals are likely to be substantially under-recognised, particularly in free-ranging wildlife that are not regularly presented to veterinary clinics. State government-funded wildlife rescue organisation Wildlife Victoria reported 75 cases of ulcerative conditions in rescued possums between 2013-2022, with an upward trend observed since 2018 (excluding 2020/2021, potentially due to decreased reporting during the COVID-19 pandemic)[17]. BU was included as a differential diagnosis for cutaneous ulcerations in possums in the recently updated Victorian Wildlife Disease Rehabilitation Guidelines[18], however, more targeted educational outreach to veterinarians, wildlife carers and pet owners about BU in animals is needed.
At present, possums with severe cutaneous lesions presenting to veterinary clinics in BU-endemic areas in Victoria are typically euthanised without attempting diagnosis. Loss of limbs or limb function, untreatable infectious disease, and chronic ill health are all recognised conditions that may preclude successful rehabilitation and release of wild animals, and are all indicators for euthanasia[19]. While human cases of BU are successfully treated with long courses of antibiotics, frequent dressing changes and/or surgery[11,15,20], these interventions are neither established nor likely to be suitable for free-living wildlife including possums. Furthermore, such interventions are likely in themselves to have additional welfare impacts from stress associated with human handling, proximity and captivity[18,19].
Other zoonotic mycobacteria species are maintained in abundant small, free-ranging mammalian wildlife species in urban environments. Natural infections of red squirrels with lepromatous leprosy, caused by infection with M. leprae and M. lepromatosis, were recently confirmed in the UK[21]. A small longitudinal field-based study conducted over two years described clinical leprosy in wild British squirrels as a chronic, progressive ulcerative disease; lesions appeared to undergo repeated ulceration-healing cycles, but usually progressed from mild-moderate lesions to severe lesions within six months[21]. Bovine tuberculosis, caused by the related M. bovis that can cause serious disease in cattle and people, is maintained in many free ranging wildlife species across the globe, including brushtail possums (Trichosurus vulpecula) in New Zealand, and European badgers (Meles meles) in the UK[22]. While there is a wealth of international literature pertaining to the epidemiology, surveillance, diagnosis and control of bovine tuberculosis in various wild animal species, discussions are largely focused on the role of wildlife in maintenance of the pathogen in the transmission cycle, and the impacts of M. bovis on the health and welfare of infected wild animals and populations are largely lacking.
Humane management strategies for prevention of MU infection and/or reduced severity of clinical BU in possums are needed. Aside from ethical considerations, culling wildlife to control infectious diseases has shown equivocal results and may counterintuitively increase both transmission and geographical distribution of pathogens[23,24]. Oral bait vaccination may be a feasible strategy for control of BU in possums. The M. tuberculosis bacille Calmette-Guérin (BCG) vaccine has been successfully used in New Zealand for the control of bovine tuberculosis (M. bovis) in brushtail possums[25,26], and early results indicate that BCG vaccination protects against BU in mice[27]. A recent article[28] proposes a series of laboratory and field-based studies to trial BCG vaccination against MU infection in possums, and to optimise palatability, delivery and efficacy of oral bait vaccine formulations targeted to ringtail and brushtail possums. Successful BU disease control in possums could have manifold benefits including reducing individual morbidity and mortality, decreasing disease transmission and protecting collective health and welfare of possum populations. Given the strong evidence implicating possums as zoonotic reservoirs of MU in Victoria [9], successful control of BU in possums may also benefit public health.
This case series provides an important first step for integrating animal welfare into BU research, however, more research, development and educational outreach are needed. Longitudinal studies, involving repeated sampling of individual possums and assessment of a range of behavioural, immunological and other factors would enable a deeper understanding of the disease progression and welfare impacts of BU over time. Other key aspects of BU in possums yet to be addressed include identification of the source(s) of MU infection; determination of incubation periods and fatality rates in naturally infected animals; identifying risk or protective factors for MU infection and clinical disease; and exploring disease transmission dynamics both within and between possum populations, and the mechanisms and extent to which zoonotic and/or vector-borne transmission to humans occurs.
Conclusions
This case series highlights the significant threat that BU poses to the health and welfare of Australian possums, due to effects of severe chronic ulcerations of skin and underlying tissues, and systemic disease. These findings underscore the need for research investigating the broader impacts of BU on possums and other wildlife, and for informed interventions that can safeguard individual wellbeing and collective protection against this important zoonotic disease in endemic areas of Australia.
Acknowledgments
Funding for this study was provided by the Australian National Health and Medical Research Council (NHMRC) grant GNT1196396. We would like to thank Dr Tristan Rich, Samantha Lovett and the staff of Lort Smith Animal Hospital, the veterinary staff of the former U-Vet Werribee Animal Hospital (The University of Melbourne), and Jessica Haining and other Anatomic Pathology lab staff at the Melbourne Veterinary School who were involved in the collection, transport and storage of possum cadavers for our study. We would like to acknowledge the tireless advocacy of Natalie J. Russell on behalf of the Essendon possums, and are grateful to Dr Sarah Frith, Katherine Whittaker, Dr Liz Dobson, Dr Richard Ploeg, and Dr Smitha Georgy for their assistance with various aspects of these cases.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
BU, Buruli/Bairnsdale ulcer; BCG, bacille Calmette-Guérin (vaccine against M. tuberculosis); CRT, common ringtail possum (Pseudocheirus peregrinus); MU, Mycobacterium ulcerans; ZN, Ziehl-Neelsen
References
- Mitchell PJ, Jerrett IV, Slee KJ. Skin ulcers caused by Mycobacterium ulcerans in koalas near Bairnsdale, Australia. Pathology 1984;16:256-260. https://pubmed.ncbi.nlm.nih.gov/6514393/.
- 2. Van Zyl A, Daniel J, Wayne J et al. Mycobacterium ulcerans infections in two horses in south-eastern Australia. Aust Vet J 2010;88:101-106. [CrossRef]
- 3. O’Brien CR, McMillan E, Harris O et al. Localised Mycobacterium ulcerans infection in four dogs. Aust Vet J 2011;89:506-510. [CrossRef]
- WHO. WHO Meeting on Buruli ulcer and other skin NTDs- Final report. 25-27 March 2019. World Health Organization (WHO), Geneva, Switzerland, 2019:212. https://apps.who.int/iris/rest/bitstreams/1257101/retrieve.
- DH. Victoria, local public health areas and local government areas surveillance summary report. https://www.health.vic.gov.au/infectious-diseases/local-government-areas-surveillance-report. 2023. Retrieved 12/1/2023.
- Tai AYC, Athan E, Friedman ND et al. Increased Severity and Spread of Mycobacterium ulcerans, Southeastern Australia. Emerg Infect Dis 2018;24:58-64. [CrossRef]
- Fyfe JAM, Lavender CJ, Handasyde KA et al. A major role for mammals in the ecology of Mycobacterium ulcerans. PLOS Negl Trop Dis 2010;4:e791. [CrossRef]
- Johnson PDR, Azuolas J, Lavender CJ et al. Mycobacterium ulcerans in mosquitoes captured during outbreak of Buruli ulcer, southeastern Australia. Emerg Infect Dis 2007;13:1653-1660. [CrossRef]
- Mee PT, Buultjens AH, Oliver J et al. A transmission chain linking Mycobacterium ulcerans with Aedes notoscriptus mosquitoes, possums and human Buruli ulcer cases in southeastern Australia. bioRxiv, 2023:39. [CrossRef]
- O’Brien CR, Handasyde KA, Hibble J et al. Clinical, microbiological and pathological findings of Mycobacterium ulcerans infection in three Australian possum species. PLOS Negl Trop Dis 2014;8:e2666. [CrossRef]
- WHO. Treatment of Mycobacterium ulcerans disease (Buruli ulcer)- Guidance for health workers. World Health Organization (WHO), Geneva, Switzerland, 2012:76. https://www.who.int/publications/i/item/9789241503402.
- Ban S, Cox-Whitton K, Grillo T. Mycobacterium ulcerans in a ringtail possum in a new location. Animal Health Surveillance Quarterly 2020;25 (3):13-17. http://www.sciquest.org.nz/elibrary/edition/8052.
- Mellor DJ, Beausoleil NJ, Littlewood KE et al. The 2020 Five Domains Model: including human–animal interactions in assessments of animal welfare. Animals 2020;10:1870. [CrossRef]
- O’Brien DP, Friedman ND, McDonald A et al. Clinical features and risk factors of oedematous Mycobacterium ulcerans lesions in an Australian population: beware cellulitis in an endemic area. PLOS Negl Trop Dis 2014;8:e2612. [CrossRef]
- Yotsu RR, Richardson M, Ishii N. Drugs for treating Buruli ulcer (Mycobacterium ulcerans disease). Cochrane Database Syst Rev 2018. [CrossRef]
- Xu RW, Stinear TP, Johnson PDR, O’Brien DP. Possum bites man: case of Buruli ulcer following possum bite. Med J Aust 2022;216:452-453. https://onlinelibrary.wiley.com/doi/full/10.5694/mja2.51505.
- Wildlife Victoria. Ulcerative lesions in Victorian possums, 2013-2022 [unpublished data]. 2023. www.wildlifevictoria.org.au/.
- DEECA. Victorian Wildlife Rehabilitation Guidelines. https://www.wildlife.vic.gov.au/victorian-wildlife-rehabilitation-guidelines/victorian-wildlife-rehabilitation-guidelines. 2023. Retrieved 10/9/2023.
- Agriculture Victoria. Code of Practice for the Welfare of Wildlife During Rehabilitation. Agriculture Victoria, Canberra, Australia, 2020. https://agriculture.vic.gov.au/livestock-and-animals/animal-welfare-victoria/pocta-act-1986/victorian-codes-of-practice-for-animal-welfare/code-of-practice-for-the-welfare-of-wildlife-during-rehabilitation.
- O’Brien DP, Jenkin G, Buntine J et al. Treatment and prevention of Mycobacterium ulcerans infection (Buruli ulcer) in Australia: guideline update. Med J Aust 2014;200:267-270. [CrossRef]
- Schilling AK, van Hooij A, Lurz PWW et al. Clinical progression of leprosy in Eurasian red squirrels (Sciurus vulgaris) in a naturally infected wild population. J Zoo WIldl Med 2021;52:1159-1166. https://pubmed.ncbi.nlm.nih.gov/34998285/.
- Fitzgerald SD, Kaneene JB. Wildlife reservoirs of bovine tuberculosis worldwide: hosts, pathology, surveillance, and control. Vet Pathol 2013;50:488-499. [CrossRef]
- Miguel E, Grosbois V, Caron A et al. A systemic approach to assess the potential and risks of wildlife culling for infectious disease control. Commun Biol 2020;3. [CrossRef]
- Mysterud A, Rauset GR, Van Moorter B et al. The last moves: The effect of hunting and culling on the risk of disease spread from a population of reindeer. J Appl Ecol 2020;57:2509-2518. [CrossRef]
- Corner LAL, Norton S, Buddle BM, Morris RS. The efficacy of bacille Calmette-Guérin vaccine in wild brushtail possums (Trichosurus vulpecula). Res Vet Sci 2002;73:145-152. [CrossRef]
- Tompkins DM, Ramsey DSL, Cross ML et al. Oral vaccination reduces the incidence of tuberculosis in free-living brushtail possums. Proc Royal Soc B 2009;276:2987-2995. [CrossRef]
- Muhi S, Stinear TP. Systematic review of M. bovis BCG and other candidate vaccines for Buruli ulcer prophylaxis. Vaccine 2021;39:7238-7252. https://www.sciencedirect.com/science/article/pii/S0264410X21007003.
- O’Brien DP, Blasdell K, Muhi S et al. Is BCG vaccination of possums the solution to the Buruli ulcer epidemic in south-eastern Australia? Med J Aust 2023. [CrossRef]
Figure 1.
Severe cutaneous and systemic M. ulcerans infection in a male common ringtail possum from Essendon, Victoria (Case 1). Left: Extensive, deep ulcers are visible on the right hind paw, exposing the distal portion of the metacarpal bone of digit 1, and the scrotum. These lesions would likely have been aligned and in contact when the animal was sitting crouched. (Photo credit: Jean Lee) Right: Lesions presumptively interpreted as multifocal pulmonary microgranulomas were observed grossly.
Figure 1.
Severe cutaneous and systemic M. ulcerans infection in a male common ringtail possum from Essendon, Victoria (Case 1). Left: Extensive, deep ulcers are visible on the right hind paw, exposing the distal portion of the metacarpal bone of digit 1, and the scrotum. These lesions would likely have been aligned and in contact when the animal was sitting crouched. (Photo credit: Jean Lee) Right: Lesions presumptively interpreted as multifocal pulmonary microgranulomas were observed grossly.

Figure 2.
Severe ulcerative BU lesions in a common ringtail possum from Richmond, Victoria (Case 2). Left: Palmar surface of left forepaw, with lateral carpal bones exposed. Right: View of hindquarters showing desiccated ulcers on both hind paws, the cloaca, and the distal tip of the tail.
Figure 2.
Severe ulcerative BU lesions in a common ringtail possum from Richmond, Victoria (Case 2). Left: Palmar surface of left forepaw, with lateral carpal bones exposed. Right: View of hindquarters showing desiccated ulcers on both hind paws, the cloaca, and the distal tip of the tail.

Figure 3.
Three of the ulcerative BU lesions observed in a female common ringtail possum from Essendon (Case 3). Left: Dorsal surface of left hind paw with deeply undermined wound edges, and tendons and bone visible under the central necrotic plug. Centre: Craniodorsal aspect of right hind paw, showing the exudative ulcerated surface of digit 4 and missing nail. Right: Palmar view of the extensive proliferative ulcerative lesion partially encircling the right fore paw.
Figure 3.
Three of the ulcerative BU lesions observed in a female common ringtail possum from Essendon (Case 3). Left: Dorsal surface of left hind paw with deeply undermined wound edges, and tendons and bone visible under the central necrotic plug. Centre: Craniodorsal aspect of right hind paw, showing the exudative ulcerated surface of digit 4 and missing nail. Right: Palmar view of the extensive proliferative ulcerative lesion partially encircling the right fore paw.

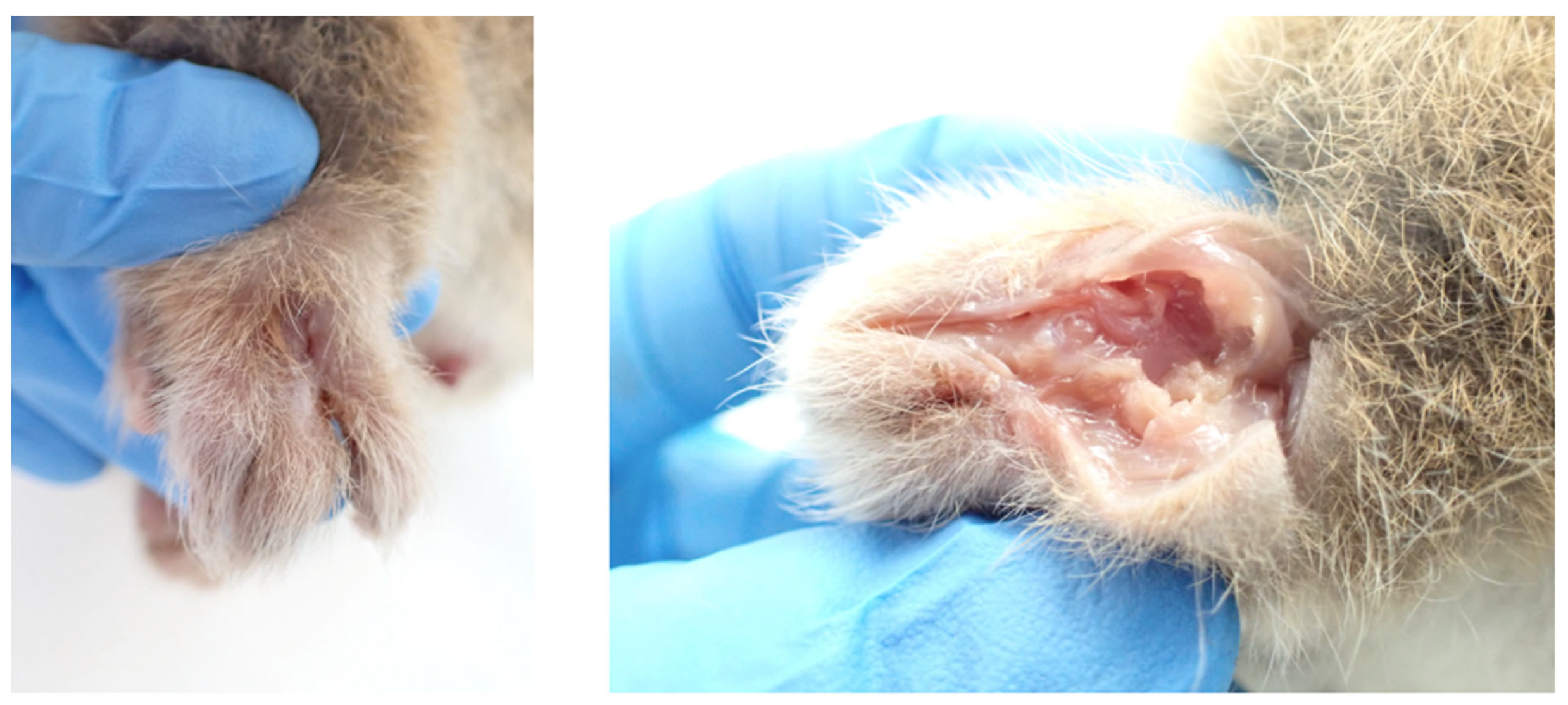
Figure 4.
Oedematous lesion with tunneling wound on the right hind paw of a male common ringtail possum from Essendon (Case 4). Left: Oedematous dorsal surface of left hind paw with linear sinus. Right: Dorsal view of left hind paw after incision through the sinus revealed a central cavity exposing striated muscle, ligaments and tendons.
Figure 4.
Oedematous lesion with tunneling wound on the right hind paw of a male common ringtail possum from Essendon (Case 4). Left: Oedematous dorsal surface of left hind paw with linear sinus. Right: Dorsal view of left hind paw after incision through the sinus revealed a central cavity exposing striated muscle, ligaments and tendons.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



