
Submitted:
05 May 2024
Posted:
06 May 2024
You are already at the latest version
Abstract
: Shear-wave elastography (SWE) has become popular in clinical practice for many diseases.However, there are not adequate research for spleen-related diseases.This study aimed to investigate the potential of quantitative values obtained through SWE in evaluating spleen pathologies in the pediatric population and to demonstrate its perfomance to differentiate splenomegaly-related diseases.Research group retrospectively included children with pathological diagnoses related to spleen from November 2016 to April 2021 and they were categorized three groups as portal hypertension (PH), benign lymphoid hyperplasia (BLH), malignant infiltration (MI).Spleen sizes and parenchymal stiffness were also calculated for each group.Subsequently, mean spleen stiffness in each compared with normal values within the same age group.In total 2781 children (1379 children for study group, 1402 children for control group) were enrolled to the study.The highest stiffness were observed in the PH group, which is statistically higher than others (p<0.05). Although the mean spleen stiffness in the group with BLH was higher than the control and MI group, the difference was not statistically significant (p=0.08).The mean stiffness in the group with MI was significantly lower than both the control group (p=0.005) and PH (p=0.01).In conclusion, using SWE in the differential diagnosis of etiologies causing splenomegaly, could make important contribution.
Keywords:
childhood
; spleen
; stiffness
; ultrasound
; Shear Wave Elastography (SWE)
1. Introduction
During the initial stages of ultrasound elastography, tissues were manually compressed, and the response of tissues to this force was measured to evaluate tissue stiffness, which limited the examination of only superficial tissues[1]. After modern advancements, however, more objective and quantitative measurements could become possible through modern elastography devices. This has led to their utilization as a part of routine clinical practice, especially for differentiating between malignant and benign lesions in parenchymal tissues such as prostate, thyroid and breast [2,3,4,5,6,7,8].
Shear Wave Elastography (SWE), is one of the current method in ultrasound elastography, which is increasingly preferred in diagnosis, providing both quantitative and qualitative values about the elasticity of the related tissue. This method utilizes ultrasound waves to determine the elasticity of tissues and assist detecting differences among tissues [9]. Transient elastography (TE) is another SWE technique which is mostly used in the liver and spleen. Unlike other SWE methods in which the stimulus is an acoustic push pulse, shear waves are generated by mechanical stimulus in TE. Each methods have their advantages and disadvantages, but there are still insufficient studies that have established quality standards for SWE compared to the numerous studies conducted for TE but both methods have been promising diagnostic methods [10,11,12,13,14,15,16].
The spleen, the largest organ of the immune system, has also become a subject of increasing interest in elastography studies. As a result of that, SWE can be beneficial in differential diagnosis about the diseases which affect spleen. While numerous studies in the literature have examined the relationship between spleen stiffness and the severity of liver fibrosis in patients with portal hypertension, studies focusing on elastography examinations in patients with spleen enlargement due to causes other than portal hypertension are limited in number and have small sample sizes [17,18,19,20,21,22,23,24].
Ultrasound elastography has shown significant advancements in recent years. Quantitative methods, such as transient elastography, acoustic radiation force impulse, and shear wave elastography, have superseded qualitative methods[25,26]. Due to the spleen's surface location, sonoelastography can provide precise measurements of its hardness with high reliability[27]. Currently, numerous researchers are studying the alterations in spleen elasticity among individuals afflicted with hepatitis B virus or hepatitis C virus, as well as those with liver fibrosis, portal hypertension, esophageal varices, or myelofibrosis[16,18,28,29]. This paper examines the function and present condition of accessible qualitative ultrasound elastography techniques, encompassing recent developments in the assessment of spleen stiffness and its clinical usefulness. Research findings indicate that there is a direct relationship between the stiffness of the spleen and the presence of liver fibrosis. This information is valuable in assessing the extent of fibrosis according to the METAVIR scoring system[30]. Patients with hepatitis B virus or hepatitis C virus see an increase in spleen stiffness, even if the elasticity of the liver remains unchanged. Moreover, it is valuable in the diagnosis of portal hypertension or the prediction of the presence of esophageal varices[18]. Furthermore, spleen sonoelastography can assist in the identification of suitable candidates for liver transplantation and in determining the optimal approach for portal vein reconstruction in patients with biliary atresia following Kasai portoenterostomy[31]. Spleen stiffness in myelofibrosis is directly related to bone marrow fibrosis and can be utilised as a measure to evaluate the effectiveness of treatment [32]. Spleen sonoelastography is additionally valuable for monitoring the functionality of transjugular intrahepatic portosystemic shunts [33].
The aim of this study was to demonstrate the potential of quantitative data obtained through SWE in the evaluation of spleen pathologies in the pediatric population. As a secondary goal, the study aimed to demonstrate the diagnostic efficacy of SWE in distinguishing diseases that lead to splenomegaly, including benign causes such as lymphoid hyperplasia, malignant infiltrative diseases, and portal hypertension.
2. Material and Methods
2.1. Patients
The study was conducted after obtaining approval from the ethics committee of our tertiary health care hospital (No. 80576354-050-99/169, 05.2019). It included a retrospective analysis of pediatric patients who were referred to the radiology deparment for abdominal ultrasonography (US) over a period of 5 years, from November 2016 to April 2021, did not meet the exclusion criteria and had pathological diagnoses related to spleen. Patients were divied into three groups (benign lymphoid hyperplasia, malignant infiltrative diseases and portal hypertension) according to their pathologies. Patients with a history of acute splenic injury, splenic laceration, splenic surgery, previous treatment with non-selective beta-blockers, shunt placement, band ligation, liver transplantation, overt hepatic encephalopathy, intrahepatic or extrahepatic malignancies other than lymphoid maligninant infiltration; portal vein thrombosis or cavernous transformation; presence of other chronic liver disease, including autoimmune hepatitis, any other viral hepatitis and alcoholic were excluded from the study (Table 1). Both written and verbal information were presented to the parents of the participants prior to the examination, and their consent was obtained in writing.
2.2. Methods
Measurements were performed by a single radiologist using a 2D-SWE (two-dimensional shear wave elastography measurements) feature-equipped US device (Siemens Acuson S3000 Ultrasound System HELX Evolution 12791052 Erlangen / Germany) with a 1-5 MHz convex probe. The spleen was imaged from a total of 10 different points, including the upper pole, lower pole, and midportion, using a 10 mm2 rectangular region of interest (ROI) after the patients were placed in the supine position and took a deep inspiration (Figure 1, Figure 2 and Figure 3). Multiple measurements have been conducted at various levels to obtain a value that reflects the entire splenic parenchyma. The average of these measurements was recorded as the splenic stiffness (kPa). The measured splenic dimensions and SWE-derived parenchymal stiffness were categorized according to the participants' diagnoses. Subsequently, the mean splenic stiffness in each group was calculated and compared with the normal values within the same age group.
2.3. Statistical Analysis
The data were analyzed using the Statistical Package for Social Sciences (SPSS) for Windows 20 (SPSS Inc., Chicago, IL). Normal distribution of the data was assessed using the Kolmogorov-Smirnov test and Shapiro-Wilk test. Normally distributed numerical variables were presented as mean ± standard deviation, while non-normally distributed variables were presented as minimum-maximum values. Categorical variables were presented as numbers and percentages. The comparison of mean age and gender differences between patients and the control group was conducted using independent sample t-test and chi-square test, respectively. The stiffness of normal spleens and pathological spleens was compared using the independent Student’s t-test. The degrees of stiffness in spleen enlargements secondary to different diseases were compared among themselves using the independent Student’s t-test. P-value < 0.05 was considered statistically significant.
3. Results
The study group included 1379 patients, of whom 892 (64.6%) were male, 487 (35.3%) were females, with a mean age of 10 years±2 months. Distribution of the patients into different pathology subgroups can be found in Table 2. The control group consisted of 1402 individuals, of whom 779 (55.5%) were male, 623 (44.4%) were female, with a mean age 8 years±8 months. The mean age of the whole population is 9.27±5 months. There is no difference between the mean ages of the study and control groups (p>0.05). The pediatric population is defined in the literature as the age group ranging from 0 to 18 years. Our study population falls within the age range of 3 to 17 years, aligning closely with this definition and there was no significant difference in the mean age between the groups.
The mean splenic craniocaudal dimension in the patient group was 14.17±3.39 cm, meanwhile it was 7.89±1.53 cm in control group; the mean splenic craniocaudal dimension was significantly higher in the patient group (p=0.002). The mean splenic stiffness of the study group was 14.26±1.33 kPa, which is significantly higher than that of control group (13.56±3.58 kPa, p=0.03). No significant correlation was defined between splenic craniocaudal size and stiffness in the both control and study groups (p>0.05).
In patients with splenomegaly, the highest quantitative values for splenic stiffness were observed in the portal hypertension group (16.63±8.36 kPa), with significantly higher stiffness than both the control group (13.56±2.56 kPa, p=0.004) and the group with malignant infiltration (10.58±4.77 kPa, p=0.01). The mean splenic stiffness in the benign lymphoid hyperplasia group was higher than that in the control group, but the difference was not statistically significant (p=0.63). Although the mean splenic stiffness in the benign lymphoid hyperplasia group (14.11±4.14 kPa) was higher than that in the malignant infiltration group (10.58±4.77 kPa), the difference was not statistically significant (p=0.08). The mean splenic stiffness in the malignant infiltration group was significantly lower than that in both the control group (p=0.005) and the group with splenic enlargement due to portal hypertension (p=0.01).
In our study, patients with portal hypertension experienced the greatest increase in spleen stiffness. In the study group, the highest quantitative values for splenic stiffness were observed in the portal hypertension group, which was significantly higher than malignant infiltration, benign lymphoid infiltration subgroups, and the control group, as well (p=0,01). The mean splenic stiffness in the benign lymphoid hyperplasia group was similar with the control group (p=0,09) and significantly higher than the malign infiltration subgroup (p=0,003). Spleen stiffness was found to be significantly lowest in malignant infiltrative diseases compared to the control group and the other study subgroups (p=0.01) (Table 3).
4. Discussion
In our study, the mean splenic craniocaudal length in the patient population was calculated as 14.17±3.39 cm, and it was observed to be statistically higher than that of the control group (p<0.05). When the patients in the study group were subgrouped based on etiology, the highest splenic stiffness value was reached in the portal hypertension group with 16.63±8.36 kPa. Although the stiffness degree in the benign lymphoid hyperplasia group was higher than that in the control group and malignant infiltration group with an average of 14.11±4.14 kPa, it was not statistically significant (p>0.05). Conversely, in the malignant infiltration group, the mean splenic stiffness was found to be significantly lower compared to other subgroups and the control group, with 10.58±4.77 kPa (p<0.05). To the best of our knowledge, Our study stands as the most extensive study in the literature, focusing on and comparing splenic stiffness in the pediatric population and the impact of various etiological factors on splenic stiffness.
Spleen is generally evaluated using ultrasonography as the primary imaging technique. Nevertheless, considering the constraints of CT and MRI, ultrasound can serve as a valuable adjunctive instrument. Ultrasound is not only uncomplicated and cost-effective, but it may also be conducted directly at the patient's bedside. Furthermore, prior research has demonstrated that ultrasound is a valuable instrument for assessing tonsils, and the volume measures acquired using ultrasound align with real values consistently. Ultrasound imaging technologies inherently exhibit the presence of signal-dependent noise. Ultrasound images inherently contain speckle noise. The intrinsic presence of it is observed during the picture acquisition phase. The presence of this noise might impede the identification of structures and can diminish the clarity of the image. Despeckling is a crucial preprocessing technique in ultrasonic imaging that enhances the precision of diagnostic and treatment planning. Despeckling strategies are employed to diminish or eradicate this noise while maintaining the fundamental information. Extensive research has been conducted in this domain to eliminate speckle noise while maintaining the integrity of medical information in the image. The ultrasound machines utilised in the present investigation are equipped with this technology, enabling the acquisition of high-resolution ultrasound (US) and shear wave elastography (SWE) pictures, facilitating successful sonographic imaging and analysis. Shear wave elastography is a novel technique employed to assess the rigidity of different tissues and organs, including the liver, breast, and thyroid. In recent years, there has been a growing utilisation of SWE to noninvasively detect both normal and cancerous cervical lymph nodes, typically by assessing the stiffness of the lymph nodes. Contrary to other imaging methods, the research affirms that SWE is a noninvasive, cost-effective, convenient, and reliable technology. It can be used in real-time to assess tissue stiffness [34].
The pediatric population is a group with unique characteristics, and therefore, normative values should be derived from studies conducted within this specific population. To the best of our knowledge, there is a lack of studies in the English literature regarding spleen stiffness values in pediatric populations. Consequently, the obtained values are presented by comparing them with previous studies conducted in adult populations. We believe that the results obtained from this study will make significant contributions to the clinical differentiation of diseases affecting splenic stiffness in the future. In the literature, it has been demonstrated in a study that in the assessment of another soft tissue in the pediatric population using SWE, there is no correlation between age, height, weight, and body mass index (BMI) with SWE values. Similarly, in our study, similar data were obtained [35].
In recent years, numerous studies have been conducted using ultrasound elastography methods to investigate the relationship between liver fibrosis severity and spleen stiffness, especially in patients with portal hypertension. However, studies focusing on elastography examination in patients with spleen enlargement due to causes other than portal hypertension have been limited in number and patient population. In this study, we aimed to investigate whether measuring spleen stiffness in a patient with spleen enlargement would contribute to the diagnosis [36,37]. We believe that our study will serve as a guide for future, more comprehensive research in the assessment of splenic stiffness using non-invasive methods such as SWE in the differentiation of diseases affecting the spleen.
In a recent study investigating the splenic stiffness in healthy children within the literature, have demonstrated that there is no significant difference among age groups and genders. Furthermore, the study demonstrated that the splenic stiffness values in healthy children ranged between 5.6 and 6.5 kPa [23]. Although our study did not have significant differences in the distribution among groups, a direct comparison between groups based on age and gender was not conducted.
Intrahepatic vascular resistance increases due to the development of fibrosis in the liver, leading to portal hypertension. Hypertension results in the development of collateral vessels and arterial vasodilatation, which increases blood flow to the spleen. An increase in spleen hardness is expected due to these mechanisms. However, splenomegaly in portal hypertension is not only due to congestion, but tissue hyperplasia and fibrosis also play an important role in this process. Studies in the literature show an increase in spleen hardness in portal hypertension [38,39,40]. Although the main aim of our study was not to investigate the relationship between liver fibrosis severity and spleen hardness, a significant increase in spleen hardness in portal hypertension was observed, consistent with other studies.
In another study by Bavu et al., the degree of liver fibrosis was evaluated using supersonic shear imaging specifically in patients with hepatitis C [41]. In our study, similar to the elastographic values ranging from 7.73 kPa to 41.27 kPa with SWE in patients with portal hypertension-related splenomegaly, liver elastographic values also showed a wide range of values between 4.50 kPa and 33.96 kPa. In the comparison of ROC curves, it was observed that as the fibrosis level increased with supersonic shear imaging, the elastographic values increased for moderate and advanced fibrosis levels. The ROC curve value for grade 2 fibrosis stage (2 F) was 0.846; the ROC curve value for grade 3 F was 0.857; and the ROC curve value for grade 4 F was 0.940. In this comparative study conducted using ROC curves for each fibrosis degree, it was observed that supersonic shear imaging, an elastographic method, became significantly more effective as the fibrosis stage increased, and it was shown to be a non-invasive, fast, simple, and reliable method for evaluating liver fibrosis.
Hirooka et al., found that spleen stiffness could be a significant independent factor in the staging of fibrosis and cirrhosis as a non-invasive diagnostic assessment in cases confirmed by simultaneous liver biopsy in chronic liver patients. It was shown that elastographic values had significant diagnostic predictability in predicting gastroesophageal varices in patients with advanced liver failure with necroinflammation on biopsy and hepatic venous pressure gradient above 12 mm-Hg (p=0.007). It was determined that measuring spleen stiffness with elastography alone or in combination with other non-invasive diagnostic tests could facilitate the non-invasive diagnosis of severe liver disease and could be applied reliably and repeatedly in the diagnosis of esophageal varices [42]. In comparison with our study group with portal hypertension-related splenomegaly, an increase in elastographic values was observed between the patient and control groups based on the kPa parameter. In this study, patients with advanced liver fibrosis with esophageal varices were evaluated, and non-invasive tests that would help to classify cirrhotic patients into different risk categories were investigated. It was found that elastographic measurements correlated with HVPG, except for patients with vascular anomalies and portohepatic shunts, and that spleen stiffness was a predictive assessment method for predicting OV and the prognosis of chronic liver disease.
All studies conducted on patients with portal hypertension due to chronic liver disease show that SWE is the most effective elastographic examination compared to other modalities and reduces the need for repeated endoscopy and measurement of hepatic portal venous gas in portal hypertension patients [8,38,39,43]. Furthermore, studies indicate that SWE could serve as an alternative to invasive methods for evaluating fibrosis in patients with portal hypertension and chronic liver disease. For these reasons, all patients included in our study were evaluated with SWE.
Transient elastography (TE) is an alternative technique utilized predominantly in the assessment of liver stiffness, measuring the speed of shear waves generated by vibrations. In the study that evaluated specific subgroups of causes of liver fibrosis, TE's diagnostic accuracy for cirrhosis diagnosis was evaluated independently of underlying liver disease with a meta-analysis [14]. In our portal hypertension group, we observed an increase in elastographic values compared to the control group, which is consistent with the findings of this study. Additionally, as correlated with other studies in the literature, the fibrosis stage increases proportionally with elastographic values. Furthermore, studies have shown that SWE could serve as an effective alternative to invasive methods for evaluating fibrosis in patients with portal hypertension and chronic liver disease [41,44].
The study by Fraquelli et al. investigated the use of transient elastography (TE) to facilitate the non-invasive diagnosis of advanced liver disease and predict the development of esophageal varices, either alone or in conjunction with hepatic elasticity. The research concluded that this method is a reliable assessment and should be evaluated in multicenter studies correlated with other research. The findings suggest that TE could be a valuable tool in the non-invasive assessment of liver disease and its complications, such as esophageal varices [45].
The study by Shaarma et al. aimed to investigate the effectiveness of TE elastography in assessing esophageal varices (EV) in patients with cirrhosis, given the variable sensitivity and specificity of non-invasive tests in predicting EV. The research compared the spleen stiffness measured by elastography with liver stiffness and other non-invasive tests, and evaluated EV in comparison with hepatic venous pressure gradient and upper gastrointestinal endoscopy. The findings demonstrated that spleen elastography provided more significant results than liver elastography, suggesting that splenic elasticity measured by elastography is an effective assessment in diagnosing esophageal varices, distinguishing large varices from small ones, and increasing the predictability of esophageal variceal bleeding [18,29].
In benign lymphoid hyperplasia of the spleen, an increase in the number and size of white pulp elements is observed due to the increased lymphocytes, while the architecture of the spleen structures (red and white pulp) is preserved. In malignant infiltrative processes, this architecture is disrupted. Consistent with studies in the literature, our study demonstrated that spleen stiffness in benign lymphoid hyperplasia was lower than the group of portal hypertension and higher than the control group [20,24]. However, spleen elastography has not been evaluated in the literature for diseases with specific diagnoses in this group. There is a need for high case number studies to evaluate cases with specific diagnoses of splenomegaly due to lymphoid hyperplasia.
In our study, we observed that patients with splenomegaly due to malignant infiltration had the lowest stiffness values. Although there are not enough studies with a large number of cases in the literature on this subject, the decrease in spleen stiffness values may be due to the limited number of patients or necrosis developing in the spleen parenchyma. Meng et al. demonstrated that necrotic areas were observed in the spleen in 70% of 17 patients with splenic lymphoma [46]. Additionally, the coexistence of different diseases in the malignant infiltrative group reduces the reliability of our findings. More studies with a larger number of patients are needed to address this issue further.
Our study has several limitations. Firstly, the evaluation was performed by a single radiologist during our study, there is the lack of inter-observer agreement assessment as a major limitation but we believe that it was mitigated with the high number of patients in our study. Furthermore, the retrospective nature of our study may introduce bias in patient selection. To mitigate this, we aimed to include as many eligible patients as possible who met the inclusion criteria. Patient’s follow-up data did not obtained. Therefore, we could not evaluate the possible correlation between the splenic stifness value and outcome of the diseases. The lack of numerical homogeneity among the groups in the study has been another limitation. Finally, as our study is of a retrospective nature, some cases lack significant laboratory and anamnesis data, which may limit the statistical significance of the results. Therefore, potential correlations between the mentioned parameters and stiffness values could not be assessed.
5. Conclusion
In conclusion, our study using the Shear Wave Elastography method to examine spleen stiffness in pediatric patients has provided valuable insights and has positioned SWE as a hopeful additional tool for comprehensive evaluations of pediatric spleen-related diseases. Our findings highlight potential connections between the causes of diseases and changes in spleen stiffness. Therefore, we believe that SWE could be a promising and non-invasive tool for assessing spleen in pediatric patients, yet further studies with supporting results are still needed.
Funding
Nil.
Competing Interest
The authors declare that they have no competing interests
Availability of data and material
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Acknowledgments
Not Applicable.
Consent for Publication
Written consent to publish this information was obtained from study participant or their parents. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards
Data availability
Data available on request due to privacy/ethical restrictions
Authors' contribution
T.C. and H.B.B. conceived and planned the experiments. T.C. O.T. S.A. K.M. M.K. and H.B.B. contributed to sample preparation. T.C. S.A. K.M. and M.K. contributed to the interpretation of the results. O.T. took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript.
References
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef] [PubMed]
- Cantisani, V.; De Silvestri, A.; Scotti, V.; Fresilli, D.; Tarsitano, M.G.; Polti, G.; Guiban, O.; Polito, E.; Pacini, P.; Durante, C.J.F.i.o. US-elastography with different techniques for thyroid nodule characterization: systematic review and meta-analysis. 2022, 12, 845549.
- Cantisani, V.; David, E.; Barr, R.G.; Radzina, M.; de Soccio, V.; Elia, D.; De Felice, C.; Pediconi, F.; Gigli, S.; Occhiato, R.J.U.i.d.M.-E.J.o.U. US-elastography for breast lesion characterization: prospective comparison of US BIRADS, strain elastography and shear wave elastography. 2021, 42, 533–540.
- Ginat, D.T.; Destounis, S.V.; Barr, R.G.; Castaneda, B.; Strang, J.G.; Rubens, D.J.J.R. US elastography of breast and prostate lesions. 2009, 29, 2007–2016.
- Ryu, J.; Jeong, W.K.J.U. Current status of musculoskeletal application of shear wave elastography. 2017, 36, 185.
- Correas, J.-M.; Tissier, A.-M.; Khairoune, A.; Khoury, G.; Eiss, D.; Hélénon, O.J.D.; imaging, i. Ultrasound elastography of the prostate: state of the art. 2013, 94, 551–560.
- Pedersen, M.R.; Sloth Osther, P.J.; Nissen, H.D.; Vedsted, P.; Møller, H.; Rafaelsen, S.R. Elastography and diffusion-weighted MRI in patients with testicular microlithiasis, normal testicular tissue, and testicular cancer: an observational study. Acta radiologica (Stockholm, Sweden : 1987) 2019, 60, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.l.; Ding, H.; Fu, T.t.; Peng, S.y.; Chen, S.y.; Luo, J.j.; Wang, W.p.J.H.R. Portal hypertension in hepatitis B-related cirrhosis: diagnostic accuracy of liver and spleen stiffness by 2-D shear-wave elastography. 2019, 49, 540–549.
- Pawluś, A.; Inglot, M.; Chabowski, M.; Szymańska, K.; Inglot, M.; Patyk, M.; Słonina, J.; Caseiro-Alves, F.; Janczak, D.; Zaleska-Dorobisz, U.J.T.B.J.o.R. Shear wave elastography (SWE) of the spleen in patients with hepatitis B and C but without significant liver fibrosis. 2016, 89, 20160423.
- Chang, J.M.; Moon, W.K.; Cho, N.; Yi, A.; Koo, H.R.; Han, W.; Noh, D.-Y.; Moon, H.-G.; Kim, S.J.J.B.c.r. ; treatment. Clinical application of shear wave elastography (SWE) in the diagnosis of benign and malignant breast diseases. 2011, 129, 89–97. [Google Scholar]
- Hu, X.; Liu, Y.; Qian, L.J.M. Diagnostic potential of real-time elastography (RTE) and shear wave elastography (SWE) to differentiate benign and malignant thyroid nodules: A systematic review and meta-analysis. 2017, 96. 96.
- Ferraioli, G.; Tinelli, C.; Dal Bello, B.; Zicchetti, M.; Filice, G.; Filice, C.; Hepatology, L.F.S.G.J. Accuracy of real-time shear wave elastography for assessing liver fibrosis in chronic hepatitis C: a pilot study. 2012, 56, 2125–2133.
- Mancini, M.; Salomone Megna, A.; Ragucci, M.; De Luca, M.; Marino Marsilia, G.; Nardone, G.; Coccoli, P.; Prinster, A.; Mannelli, L.; Vergara, E.J.P.o. Reproducibility of shear wave elastography (SWE) in patients with chronic liver disease. 2017, 12, e0185391.
- Friedrich-Rust, M.; Ong, M.F.; Martens, S.; Sarrazin, C.; Bojunga, J.; Zeuzem, S.; Herrmann, E. Performance of transient elastography for the staging of liver fibrosis: a meta-analysis. Gastroenterology 2008, 134, 960–974. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.G.; Wilson, S.R.; Rubens, D.; Garcia-Tsao, G.; Ferraioli, G.J.R. Update to the society of radiologists in ultrasound liver elastography consensus statement. 2020, 296, 263–274.
- Sandrin, L.; Fourquet, B.; Hasquenoph, J.-M.; Yon, S.; Fournier, C.; Mal, F.; Christidis, C.; Ziol, M.; Poulet, B.; Kazemi, F.J.U.i.m.; et al. Transient elastography: a new noninvasive method for assessment of hepatic fibrosis. 2003, 29, 1705–1713.
- Giuffrè, M.; Macor, D.; Masutti, F.; Abazia, C.; Tinè, F.; Patti, R.; Buonocore, M.R.; Colombo, A.; Visintin, A.; Campigotto, M.; et al. Evaluation of spleen stiffness in healthy volunteers using point shear wave elastography. Annals of Hepatology 2019, 18, 736–741. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Kirnake, V.; Tyagi, P.; Bansal, N.; Singla, V.; Kumar, A.; Arora, A.J.O.j.o.t.A.C.o.G. ; ACG. Spleen stiffness in patients with cirrhosis in predicting esophageal varices. 2013, 108, 1101–1107. [Google Scholar]
- Rewisha, E.; Elsabaawy, M.; Alsebaey, A.; Elmazaly, M.; Tharwa, E.J.o. Evaluation of the Role of Liver and Splenic Transient Elastography in Chronic Hepatitis C Related Fibrosis. J Liver Disease Transplant 5: 3. 2016, 5, 35–06. [Google Scholar] [CrossRef]
- Batur, A.; Alagoz, S.; Durmaz, F.; Baran, A.I.; Ekinci, O.J.U.Q. Measurement of spleen stiffness by shear-wave elastography for prediction of splenomegaly etiology. 2019, 35, 153–156.
- GIBIINO, G.; Garcovich, M.; Ainora, M.; Zocco, M.J.E.R.f.M.; Sciences, P. Spleen ultrasound elastography: state of the art and future directions-a systematic review. 2019, 23. 23.
- Webb, M.; Zimran, A.; Dinur, T.; Shibolet, O.; Levit, S.; Steinberg, D.M.; Salomon, O. Are transient and shear wave elastography useful tools in Gaucher disease? Blood cells, molecules & diseases 2018, 68, 143–147. [Google Scholar] [CrossRef]
- Bhatia, A.; Bhatia, H.; Saxena, A.K.; Lal, S.B.; Sodhi, K.S. Shear wave elastography of the spleen using elastography point quantification: stiffness values in healthy children. Abdominal Radiology 2022, 47, 2128–2134. [Google Scholar] [CrossRef] [PubMed]
- Yalçın, K.; Demir, B.Ç.J.A.R. Spleen stiffness measurement by shear wave elastography using acoustic radiation force impulse in predicting the etiology of splenomegaly. 2021, 46, 609–615.
- Barr, R.G.; Wilson, S.R.; Rubens, D.; Garcia-Tsao, G.; Ferraioli, G. Update to the Society of Radiologists in Ultrasound Liver Elastography Consensus Statement. 2020, 296, 263–274. [CrossRef]
- Cui, X.W.; Li, K.N.; Yi, A.J.; Wang, B.; Wei, Q.; Wu, G.G.; Dietrich, C.F. Ultrasound elastography. Endoscopic ultrasound 2022, 11, 252–274. [Google Scholar] [CrossRef] [PubMed]
- Mazur, R.; Celmer, M.; Silicki, J.; Hołownia, D.; Pozowski, P.; Międzybrodzki, K. Clinical applications of spleen ultrasound elastography - a review. Journal of ultrasonography 2018, 18, 37–41. [Google Scholar] [CrossRef]
- Wu, M.; Wu, L.; Jin, J.; Wang, J.; Li, S.; Zeng, J.; Guo, H.; Zheng, J.; Chen, S.; Zheng, R.J.R. Liver stiffness measured with two-dimensional shear-wave elastography is predictive of liver-related events in patients with chronic liver disease due to hepatis B viral infection. 2020, 295, 353–360.
- Kim, H.Y.; Jin, E.H.; Kim, W.; Lee, J.Y.; Woo, H.; Oh, S.; Seo, J.-Y.; Oh, H.S.; Chung, K.H.; Jung, Y.J.J.M. The role of spleen stiffness in determining the severity and bleeding risk of esophageal varices in cirrhotic patients. 2015, 94. 94.
- Rozario, R.; Ramakrishna, B.J.J.o.h. Histopathological study of chronic hepatitis B and C: a comparison of two scoring systems. 2003, 38, 223–229.
- Uchida, H.; Sakamoto, S.; Kobayashi, M.; Shigeta, T.; Matsunami, M.; Sasaki, K.; Kanazawa, H.; Fukuda, A.; Kanamori, Y.; Miyasaka, M.J.J.o.p.s. The degree of spleen stiffness measured on acoustic radiation force impulse elastography predicts the severity of portal hypertension in patients with biliary atresia after portoenterostomy. 2015, 50, 559–564.
- Benedetti, E.; Tavarozzi, R.; Morganti, R.; Bruno, B.; Bramanti, E.; Baratè, C.; Balducci, S.; Iovino, L.; Ricci, F.; Ricchiuto, V.; et al. Organ Stiffness in the Work-Up of Myelofibrosis and Philadelphia-Negative Chronic Myeloproliferative Neoplasms. Journal of clinical medicine 2020, 9. [Google Scholar] [CrossRef]
- Mazur, R.; Celmer, M.; Silicki, J.; Hołownia, D.; Pozowski, P.; Międzybrodzki, K.J.J.o.u. Clinical applications of spleen ultrasound elastography–a review. 2018, 18, 37–41.
- Ece, B.; Aydin, S.J.C. Can Shear Wave Elastography Help Differentiate Acute Tonsillitis from Normal Tonsils in Pediatric Patients: A Prospective Preliminary Study. 2023, 10, 704.
- Aydin, S.; Senbil, D.C.; Karavas, E.; Kadirhan, O.; Kantarci, M. Shear-wave Elastography of Palatine Tonsils: A Normative Study in Children. Journal of medical ultrasound 2023, 31, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Garra, B.S.J.A.i. Elastography: history, principles, and technique comparison. 2015, 40, 680–697.
- Ormachea, J.; Parker, K.J.P.i.M. ; Biology. Elastography imaging: the 30 year perspective. 2020, 65, 24TR06. [Google Scholar]
- Jansen, C.; Bogs, C.; Verlinden, W.; Thiele, M.; Möller, P.; Görtzen, J.; Lehmann, J.; Vanwolleghem, T.; Vonghia, L.; Praktiknjo, M.J.L.I. Shear-wave elastography of the liver and spleen identifies clinically significant portal hypertension: a prospective multicentre study. 2017, 37, 396–405.
- Elkrief, L.; Rautou, P.-E.; Ronot, M.; Lambert, S.; Dioguardi Burgio, M.; Francoz, C.; Plessier, A.; Durand, F.; Valla, D.; Lebrec, D.J.R. Prospective comparison of spleen and liver stiffness by using shear-wave and transient elastography for detection of portal hypertension in cirrhosis. 2015, 275, 589–598.
- Nedredal, G.I.; Yin, M.; McKenzie, T.; Lillegard, J.; Luebke-Wheeler, J.; Talwalkar, J.; Ehman, R.; Nyberg, S.L. Portal hypertension correlates with splenic stiffness as measured with MR elastography. Journal of magnetic resonance imaging : JMRI 2011, 34, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Bavu, E.; Gennisson, J.L.; Couade, M.; Bercoff, J.; Mallet, V.; Fink, M.; Badel, A.; Vallet-Pichard, A.; Nalpas, B.; Tanter, M.; et al. Noninvasive in vivo liver fibrosis evaluation using supersonic shear imaging: a clinical study on 113 hepatitis C virus patients. Ultrasound in medicine & biology 2011, 37, 1361–1373. [Google Scholar] [CrossRef]
- Hirooka, M.; Ochi, H.; Koizumi, Y.; Kisaka, Y.; Abe, M.; Ikeda, Y.; Matsuura, B.; Hiasa, Y.; Onji, M.J.R. Splenic elasticity measured with real-time tissue elastography is a marker of portal hypertension. 2011, 261, 960–968.
- Jeon, S.K.; Lee, J.M.; Joo, I.; Yoon, J.H.; Lee, D.H.; Han, J.K.J.A.r. Two-dimensional shear wave elastography with propagation maps for the assessment of liver fibrosis and clinically significant portal hypertension in patients with chronic liver disease: a prospective study. 2020, 27, 798–806.
- Shan, Q.Y.; Liu, B.X.; Tian, W.S.; Wang, W.; Zhou, L.Y.; Wang, Y.; Xie, X.Y. Elastography of shear wave speed imaging for the evaluation of liver fibrosis: A meta-analysis. Hepatology research : the official journal of the Japan Society of Hepatology 2016, 46, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- Fraquelli, M.; Conti, C.B.; Giunta, M.; Gridavilla, D.; Tosetti, G.; Baccarin, A.; Casazza, G.; D’Ambrosio, R.; Nicolini, A.; Primignani, M.J.G. Assessing spleen stiffness by point shear-wave elastography: Is it feasible and reproducible in patients with chronic liver disease? Is it useful to predict portal hypertension? 2019, 1, 205–213. [Google Scholar]
- Li, M.; Zhang, L.; Wu, N.; Huang, W.; Lv, N.J.P.O. Imaging findings of primary splenic lymphoma: a review of 17 cases in which diagnosis was made at splenectomy. 2013, 8, e80264.
Figure 1.
Splenic Stiffness Evaluation in 14-year-old Boy with Benign Lymphoid Hyperplasia (Splenic craniocaudal lenght: 14 cm, Stiffness on SWE: 13.36 kPa).
Figure 1.
Splenic Stiffness Evaluation in 14-year-old Boy with Benign Lymphoid Hyperplasia (Splenic craniocaudal lenght: 14 cm, Stiffness on SWE: 13.36 kPa).
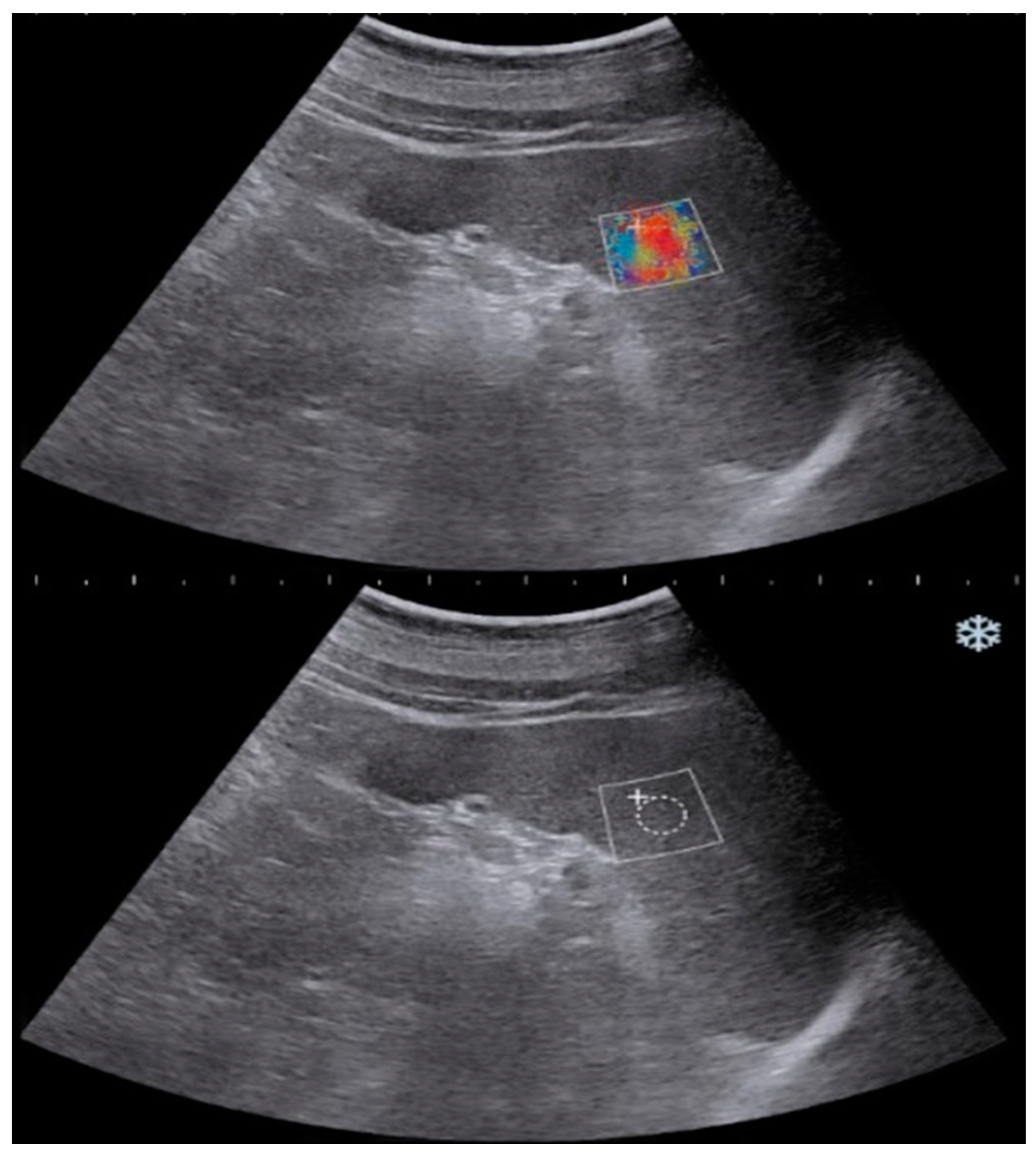
Figure 2.
SWE Imaging and Assessment in 16-year-old Boy with Sickle Cell Anemia (Splenic craniocaudal lenght 14.3 cm, Stiffness on SWE: 14.05 kPa).
Figure 2.
SWE Imaging and Assessment in 16-year-old Boy with Sickle Cell Anemia (Splenic craniocaudal lenght 14.3 cm, Stiffness on SWE: 14.05 kPa).
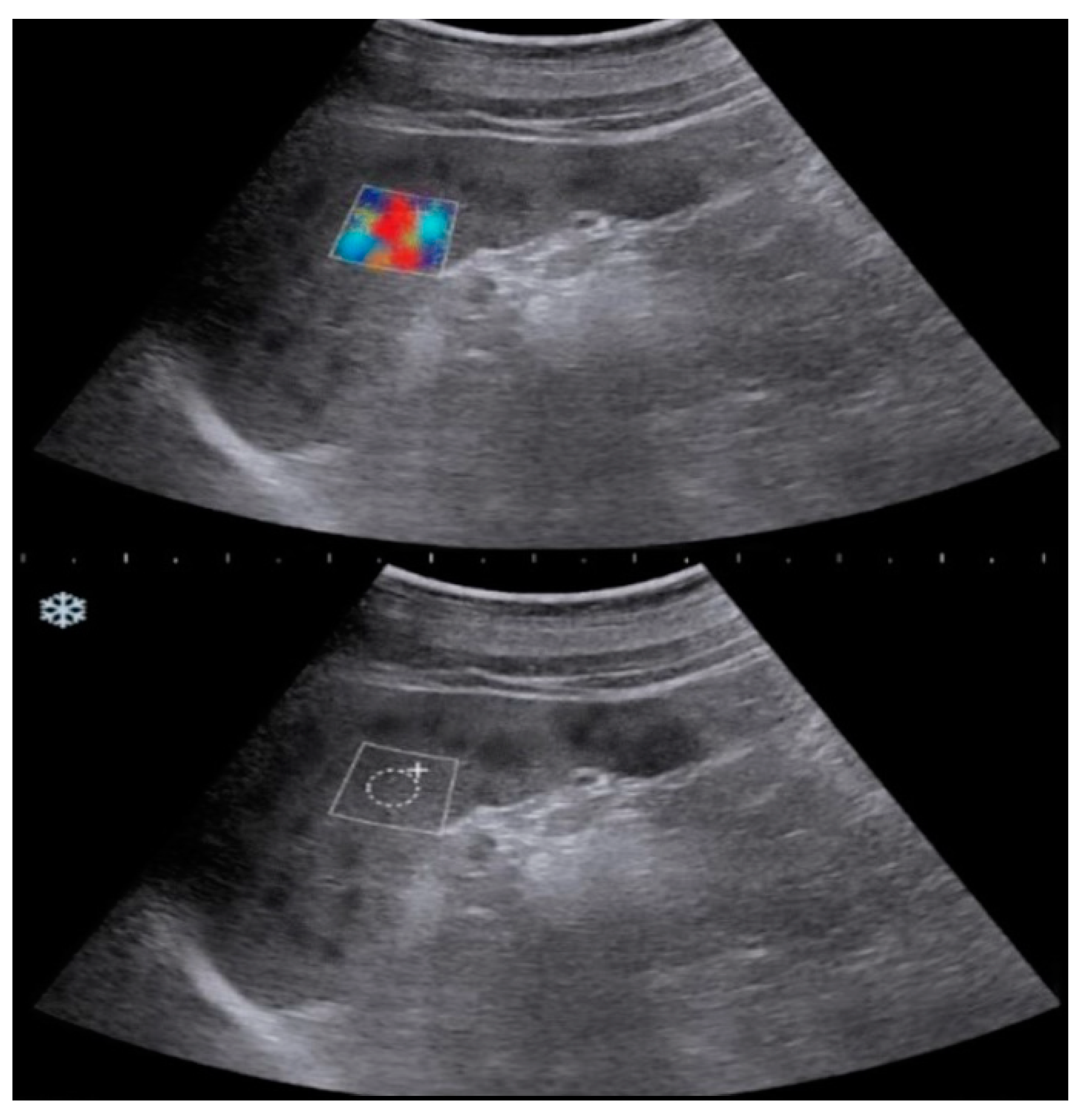
Figure 3.
Splenic Stiffness Evaluation in 12-year-old Girl with Benign Lymphoid Hyperplasia (Splenic craniocaudal lenght: 16.2 cm, Stiffness on SWE: 13.27 kPa).
Figure 3.
Splenic Stiffness Evaluation in 12-year-old Girl with Benign Lymphoid Hyperplasia (Splenic craniocaudal lenght: 16.2 cm, Stiffness on SWE: 13.27 kPa).
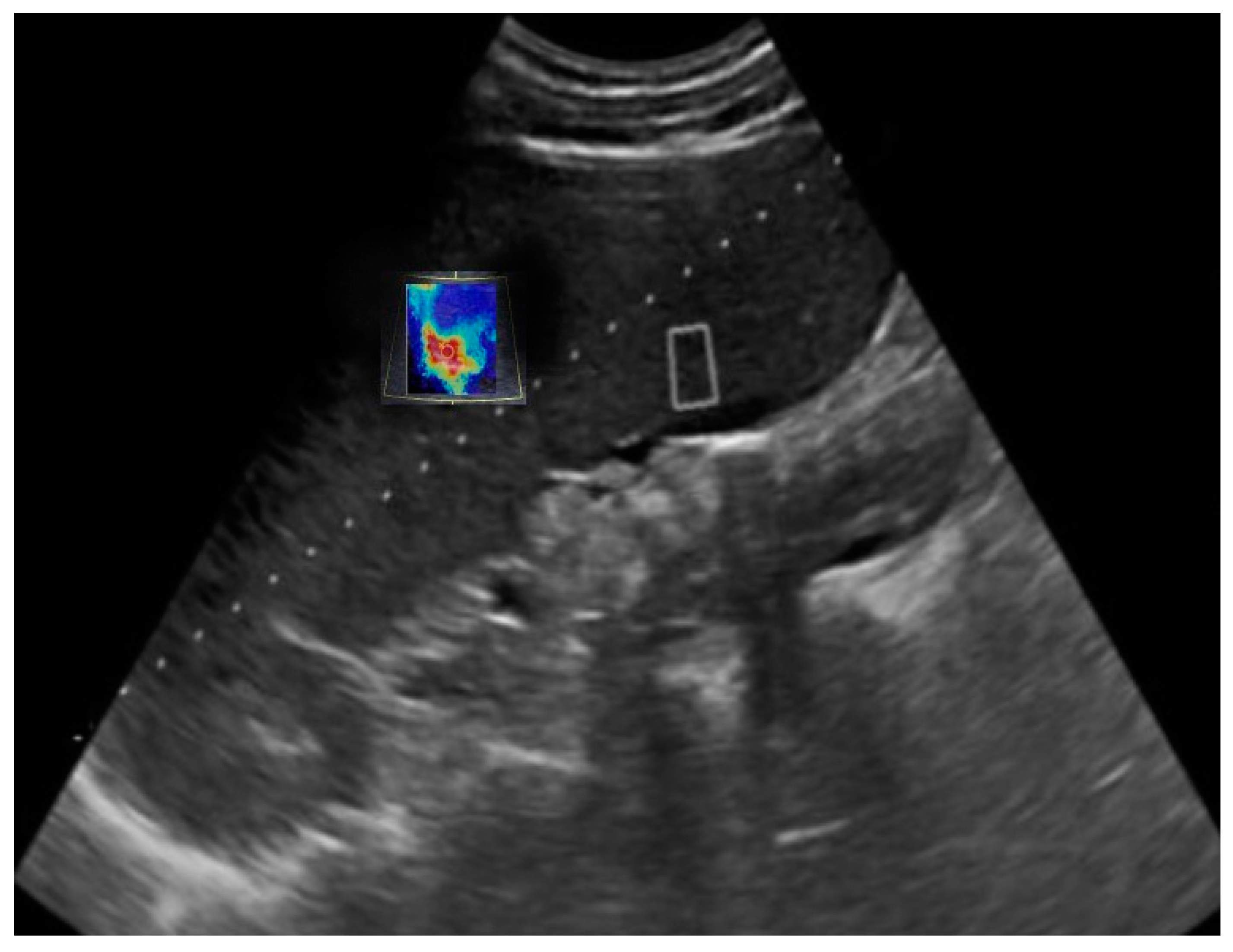

Table 1.
Exclusion Criteria and Number of Excluded Patient From the Study.
| Exclusion Criteria | n(Excluded Patients) |
|---|---|
| History of Acute Splenic İnjury | 12 |
| Splenic Surgery | 8 |
| Previous Treatment with Non-Selective Beta-Blockers | 5 |
| Shunt Placement | 4 |
| Band Ligation | 1 |
| Liver Transplantation | 3 |
| Overt Hepatic Encephalopathy | 3 |
| İntrahepatic or Extrahepatic Malignancies Other Than Lymphoid Maligninant İnfiltration | 9 |
| Portal Vein Thrombosis or Cavernous Transformation | 7 |
| Presence of Other Chronic Liver Disease | 6 |
Table 2.
Distribution of the patients in the study group.
| Male n(%) | Female n(%) | Total n(%) | |
|---|---|---|---|
| Study Group | 892 (64.6) | 487(35.3) | 1379 (100) |
|
126 (9.1) | 67 (4.8) | 193 (13.9) |
|
213 (15.4) | 144 (10.4) | 357 (25.8) |
|
553 (40.1) | 276 (20) | 829 (60.1) |
| Control Group | 779 (55.5) | 623 (44.4) | 1402 (100) |
Table 3.
Mean stiffness values according to groups.
| Groups | Mean splenic stiffness value |
|---|---|
| Control group | 13.56±3.58 kPa |
| Malignant Infiltration | 10.58±1.18 kPa |
| Portal Hypertansion | 16.63±7.73 kPa |
| Benign Lymphoid Hyperplasia | 14.11±3.91 kPa |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



