
Submitted:
04 May 2024
Posted:
06 May 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Throughout the Covid19 period, families were forced to stay indoors, adapting to online school-ing, remote work, and virtual social engagements, inevitably altering the dynamics within households. There is a notable increase in mental health challenges in terms of anxiety and de-pression in children and adolescents. This study intends to explore the psychosocial effects of the Covid-19 pandemic in Italian families adopting self- and proxy-report questionnaires on anxiety, anger, and health-related quality of life. The results showed that approximately 20% obtained a clinical anxiety score and only 10% obtained a clinical anger score. There was found a difference in the perception of the quality of life reported by the child and that perceived by the parent. The stepwise regression model showed that total anxiety scores were predicted by sex, quality of life scores from the parents' self-report version and total anger score. Another stepwise regression model identified physiological and social anxiety as the best predictors that impact the quality of life. Parental well-being actively influences the well-being of children, so it is fundamental to implement preventive programmes and promote child well-being providing parents the most adequate support possible.
Keywords:
Covid19
; Quality of life
; Psychological symptoms
; Children
; Adolescents
; Parents
; Predictive models
1. Introduction
The onset of the COVID-19 pandemic has brought about an era of unparalleled global upheaval, significantly affecting people of various demographic backgrounds. Throughout this period, families found themselves forced to stay indoors, adapting to online schooling, remote work, and virtual social activities, inevitably altering the dynamics within households [1,2]. Parents were forced to simultaneously manage their professional responsibilities, childcare activities, and housework, leading to increased stress, fatigue, and consequently negatively affecting their productivity [1,3,4,5].
Furthermore, the period of social isolation introduced various stressors and concerns that significantly affected the well-being and mental health of children and adolescents. Abrupt disruptions in daily routines, including sudden interruptions in school attendance and limited contact with peers and relatives, together with hidden or manifest concerns of parents, contributed to increased uncertainty [6]. As is known, psychological development is characterised by transformations and challenges as individuals strive for autonomy from their parents, construct their identity [7,8] and, particularly during adolescence, undergo social development and a greater need for social interactions [9].
In this regard, the findings of cross-sectional and longitudinal investigations, as well as systematic reviews and meta-analyses on the psychological impact of the COVID-19 lockdown and the subsequent periods, highlight a marked decline in health-related quality of life (HRQoL) among children and adolescents [7,10,11].
Therefore, it can be stated that the Covid-19 pandemic has worsened the quality of life and well-being of many people, in particular those who lived in a situation of physical, psychological, or social hardship even before the outbreak of the health emergency [12]. Families with school-age children were most affected because they have to give them support and take care of their development in stressful difficult conditions [5].
Regarding the HRQoL assessment, it is important to note that the literature shows that there is a widely acknowledged gap between children's self-reported information and that provided by their parents regarding the children's health and well-being [13,14]. This incongruence is extensively documented in the pediatric and adult literature, and proxy assessors often underestimate the quality of life related to child health compared to self-reports [14,15,16]. This divergence can be attributed to various factors related to the child, the parent, and the specific domains of quality of life related to health being considered [13]. In particular, in child populations, proxy HRQoL assessments can be influenced by external variables, such as a parent's own HRQoL [17]. While parental input is valuable when children cannot provide independent responses, it is crucial to recognise that children's self-reports offer a more accurate reflection of their health status. Ideally, individuals themselves should serve as primary informants about their HRQoL, symptoms, sensations, and health conditions[13,18].
At the same time, in this post-Covid era, there has also been a notable increase in mental health challenges in terms of anxiety and depression in children and adolescents [10,11,19]. De Bles et al [20] suggest a possible association between anxiety and depressive disorders and possible links of the last two also with trait anger, even if it depends on the definition of the construct of anger [21].
Regarding psychopathology, several studies indicate an increase of 83% in the number of accesses to child neuropsychiatry services during the pandemic period [22], and anxiety has become the most prevalent mental disorder among the youth population in Europe [23]. Both fatigue and parental stress are identified as risk factors for the development of negative mental health outcomes in both parents and children [24]. Spinelli et al. [5] found that parental perception, particularly their struggles in managing the various stressors imposed by quarantine, was significantly linked to parental stress and psychological problems in children. Furthermore, another investigation [25] highlights the significant impact of parental involvement (PI) and parental stress on children's academic adjustment and overall quality of life (QoL).
1.1. Aims
The final objective of the study is to understand the associations between the impact of Covid-19, symptoms, and the quality of life of children or adolescents and their parents.
Specifically, the following study intends to:
1. Conduct a screening of anxiety, anger symptoms, and quality of life (QoL) in Italian children and adolescents and their parents using self- and proxy-report tools based on data available in the literature.
2. Investigate the disparities between children's self-reported perception of quality of life and the perception reported by their parents (proxy-report), with a specific focus on evaluating the role of fatigue in children's quality of life.
3. Understand the associations between various symptoms, sociodemographic variables, and parental well-being by proposing predictive models on anxiety and quality of life.
2. Materials and Methods
2.1. Participants
The first sample consists of 131 subjects aged between 6 and 16 years, the average age is 12.44 years (SD = 2.743; range = 6-16 years). The sample is characterised by 60 men (45.8% of the total) and 71 women (54.2% of the total). The descriptive statistics regarding the class attended indicate that 35 subjects attend primary school (26.7% of the total), 50 subjects attend lower secondary school (38.2% of the total) and 46 subjects attend upper secondary school (35.1 % of the total).
The second sample consists of 131 subjects aged 30 to 66 years, the average age of the sample is 46.46 years (SD = 6.025; range = 30-66 years), only one subject did not specify his age. The descriptive statistics and frequencies regarding the data collected from the sociodemographic questionnaire administered to subjects and their parents are summarised in Table 1.
2.2. Procedure
After obtaining the consent of the Psychology Ethics Committee (protocol code 4039, University of Padua), both parents of the children signed the written informed consent. On this occasion, the objectives of the study were specified, the information necessary for the purposes of the research, the methods of data collection and the duration necessary for their collection. After completing the informed consent, the families received two links to access the questionnaires anonymously and protected on the LimeSurvey platform, one reserved exclusively for the child and one for a parent. It was specified that, for each child, only one parent completed the questionnaires assigned to them. The data necessary for this study were collected between April and June 2022 by psychology students at the University of Padua referring to different regions of the country.
2.3. Instruments
2.3.1. Sociodemographic Questionnaire
Parents filled out a sociodemographic questionnaire with questions about themselves: sex, their highest year of schooling, their education, their perceived economic situation, their type of home situation, their romantic relationship, and their type of employment.
2.3.2. Revised Children’s Manifest Anxiety Scale – Second Edition [26]
It is a brief self-report inventory measuring the level and nature of anxiety in 6- to 19-year-olds. The test is now composed of 49 items that cover the following scales: Physiological Anxiety, Worry, Social Anxiety, Defensiveness, and Inconsistent Responding Index. Scoring is carried out exclusively through the Giunti Psychometrics online testing platform, Giunti Testing, regardless of the method of administration. Scoring occurs automatically and calculates the subject's score, while also producing a graphic profile. The scores in the content scales are standardised and known as normalised T-points, the T-points have a mean of 50 and a standard deviation of 10, the term "normalised" indicates that each value of a T-point corresponds to the same percentile rank for each scale.
2.3.3. ChIA [27]
It is a self-administered questionnaire that identifies the type of situations that provoke anger in children and adolescents and the intensity of their responses to these situations. Short, quick, and economical, the ChIA is one of the few tools available that provide the child and adolescent's perspective on their anger. Consisting of 39 statements, it provides a total score, an incongruent response index (IRI), and scores relating to four subscales: Frustration, Physical aggression, Relationships with peers, Relationship with authorities. The statements are written in a very simple way, so that they can be understood by young children or those with learning problems, but so that they are not considered childish by older children and therefore rejected. The various answer options correspond to the drawing of four pictograms with expressions ranging from happiness to extreme anger. Whoever fills out the questionnaire simply has to mark the answer that indicates how angry they would be in the situation described. Scoring is carried out exclusively through the online testing platform of Giunti Psychometric, Giunti Testing, regardless of the method of administration choice. It happens automatically, and, in addition to calculating the score, the programme also produces a graphical report. ChIA scores are transformed into normalised T scores that have a mean of 50 and a standard deviation of 10. The term 'normalised' means that the value of each T score on each scale corresponds to the same percentile as the value of the score on each other stairs. Higher scores reflect higher levels of anger, similarly lower scores reflect lower levels of anger.
2.3.4. PedsQoL 3.0 Multidimensional Fatigue Scale [28]
It is an 18-item questionnaire that includes three dimensions. The questionnaire aims to investigate total fatigue, i.e. general fatigue, sleep-related fatigue, and cognitive fatigue in individuals from 2 years of age. It aims to identify how fatigue affects HRQOL of individuals. It is characterised by the self-report version available from 5 years of age and the proxy-report version for parents available from 2 years of age of the child. It is a simple and quick to administer tool. It can be administered individually or in groups through paper and pencil or in the form of a semi-structured interview. The responses to the items are on a five-level Likert scale (where 0 corresponds to Never and 4 corresponds to Almost always) which indicates the frequency with which a subject perceives or identifies with the sensations and situations described by the items.
The scoring procedure takes place manually, as indicated in the manual, the first step to follow consists of transforming the scores. The items are classified with an inverse score and linearly transformed within a scale of values from 0 to 100. The values of the responses to the items will be transformed as follows: 0=100; 1=75; 2=50; 3=25; 4=0. The score of each dimension (general fatigue, sleep-related fatigue, and cognitive fatigue) is obtained by calculating the average value of the scores transformed into the 6 items from which it is composed. Calculating the total score is obtained by averaging the transformed scores of the 18 items in the questionnaire. The scoring manual suggests that higher values are correlated with a better quality of life related to health and fewer problems or symptoms; on the contrary, lower scores are correlated with greater fatigue and worse quality of life.
2.4. Plan of Statistical Analyses
Descriptive analyses will identify the clinical or normal distribution of anxiety and anger levels in children and adolescents after their specific cut-off point. Correlational analyses and then stepwise regression models will explain the main factors that impact the quality of life related to children and adolescents after the Covid period.
3. Results
3.1. Perceptions of Anxiety, Anger, and Quality of Life of Children and Adolescents Compared to Norms
RCMAS-2 test scores were divided into the scales described and identified in the Reynolds & Richmond manual [26]. The results showed that approximately 70% of the sample obtained an average total anxiety score, while approximately 20% obtained an above average anxiety score (Figure 1a).
With reference to the first objective of this research, approximately 80% of the sample obtained an average test score in ChIA. Only 10% obtained a score above the clinically significant average; this suggests that the distribution of anger levels in the present sample is normal on average and not clinically significant (Figure 1b).
The PedsQLTM 3.0 Multidimensional Fatigue Scale test scores are converted according to the manual instructions and were recoded and divided into four categories that qualitatively describe the score in relation to the quality of life of the subjects (Table 2).
Most of the children and adolescents reported moderate total quality of life (62.72%) while 10.7% scored low quality of life and 22.1% high.
Parents also self-reported QoL scores, showing a worse picture with 19.1% with low perception (Table 3).
3.2. Comparison of Quality of Life Scores between Parents and Children
A paired-sample T test was performed to compare the mean scores of the various areas of quality of life reported by children and adolescents and the same scores reported by parents. Differences are significant (p<.005) for the sleep area (t = -4.61, df = 130), the cognitive area (t = -2.91, df = 130) and the total quality of life one (t = -3.09, df = 130). Consequently, the second objective of the present study, which was to examine the presence of a difference in the perception of the quality of life reported by the child and that perceived by the parent, was confirmed. The results of the analysis are reported in Figure 2.
3.3. What Are the Factors That Influence Anxiety Symptoms in Children and Adolescents?
First, a series of bivariate Pearson correlations were carried out between the sociodemographic variables of the children, the parents' quality of life, the anger scores, and the anxiety symptoms. Starting from these correlations, hierarchical linear regression models were proposed using the stepwise method.
The first linear regression sets the total Anxiety scores on the RCMAS-2 test as the dependent variable, while the independent variables are sex, quality of life scores from the parents' self-report version, and total Anger scores on the ChIA test. The third model turns out to be significant (p<.005) and explains most of the variance (15%), the variables mentioned above turn out to be significant predictors of the dependent variable (Table 4).
3.3. What Are the Factors That Influence the Perceived Quality of Life of Children and Adolescents?
The second proposed hierarchical linear regression sets as a dependent variable the scores of the total quality of life of the self-report version reported by the children/young people and as independent variables the scores of physiological anxiety and social anxiety, anxiety subscales of the RCMAS-2 test. The second model turns out to be significant (p<.005) and explains most of the variance (33%), the variables mentioned above turn out to be significant predictors of the dependent variable (Table 5).
4. Discussion
The first objective of the present study was to perform a screening of disorders related to anxiety, anger, and the level of quality of life of Italian children and adolescents. The results suggest that more than half of the subjects fall within age-specific average scores. For the Total Anxiety scale and for the Physiological Anxiety and Worry subscales, more than 20% of the sample achieved clinically relevant scores above the average for their age group. For the social anxiety subscale, only 18.3% of the sample obtained a clinically significant score above the average for the age group. These results suggest that anxiety is a common disorder in the child population and confirm the results of the meta-analysis by Racine et al. [11], which stated that one in five children experienced clinical symptoms of anxiety. By comparing data before the pandemic, the results of Racine's study suggest that mental health difficulties double in young people [11].
Only 15% of the sample achieved high levels of anger that were clinically significant for the Anger toward Authority subscale. These results can be explained by the fact that the sample is mostly made up of adolescents, and in this age group, it is typical to feel anger and frustration towards adult figures who exercise authority over them. An additional explanation could be supported by the excessive frustration caused by the restrictions that children and adolescents have been forced to implement during the Covid-19 pandemic, which manifests itself through hostility towards authority figures [29]. Another information that emerged from the test results is that a very low percentage of subjects, approximately 3% of the sample, obtained clinically significant high levels for the physical aggression subscale, and approximately 17% of the sample obtained extremely low levels of anger, which are equally clinically significant. These last results contradict the results of the study by Reid and colleagues [29] which analysed psychological distress and the implementation of antisocial behaviours before and after the outbreak of the Covid-19 pandemic in young people in the American population, finding an increase in frustration in the subjects and, consequently, an increase in aggressive behaviours. In this sample, the levels of physical aggression are below the normal threshold for the age group, the anger is probably internalised and channelled towards the self and not towards the other. Their anger levels are normal; however, the data regarding the subjects' levels of physical aggression appear to be below threshold for a good percentage of the sample. Probably the aggression of the subjects in this sample is not channelled outward, but directed towards the self, this determines an internalisation of anger symptoms which could contribute to the worsening of the subject's anxious internalising symptoms and, therefore, worsen his psychological well-being.
The results showed that the children have fairly high levels of quality of life, around 80% of the sample obtained medium-high values in all areas. Subjects are more affected by sleep-related and cognitive fatigue, as approximately 20% of the sample has lower levels of quality of life in both areas. There is a decline in their overall HRQoL throughout the course of the COVID-19 pandemic that does not necessarily subside when the the lockdowns ended [10]. Regarding the results of the parents' group, on average 70% of the sample obtained medium-high levels of quality of life in all areas. General and cognitive fatigue compromised the quality of life levels of the sample the most, as 35% and 25% of the subjects achieved low quality of life levels in these areas, respectively. These data confirm the results of other studies [12,24] that identified a decrease in health-related quality of life and an increase in anxiety and stress levels after the Covid-19 pandemic.
The second objective of the study was to investigate the presence of a difference in the perception of quality of life between the child or adolescent and the parent within the self-report and proxy-report versions in the evaluation of fatigue. The results show that there is a difference between children and parents in perception of quality of life in all areas, in particular for the evaluation of total quality of life. The data suggest that parents tend to overestimate their children's well-being. These results confirm the data present in the literature on the presence of significant differences between the self-report and proxy-report versions in the evaluation of one's internal states and one's health status [13].
To satisfy the third objective of the following study and therefore to understand whether there were factors that could influence anxiety symptoms in children. The gender of the woman, the quality of life perceived by parents, and the levels of total anger of children have a significant impact on their anxiety symptoms. These results are in agreement with the data present in the reference literature. Female sex as a predictor of the subject's anxiety levels confirms the data present in the literature that states that in mental illnesses in childhood and adolescence, female sex has been associated with greater anxiety and depressive symptoms [11]. The results that emerged in the present study regarding the fact that the quality of life of parents and specifically fatigue predict the mental health levels of their children, specifically their anxiety symptomatology.
Parent management of stress at an individual and dyadic level significantly affects their children's emotional and behavioural problems [5]. Furthermore, emotional support provided by parents constitutes a fundamental protective factor against the manifestation of psychopathological symptoms in their children [6]. The last factor examined explains how children or adolescents' anger levels predict their anxiety levels. This result supports the data provided in the literature on the topic. Studies conducted in the adult population with anxiety disorders have highlighted higher rates and intensity of anger compared to control groups, and anger is also individually associated with the severity of anxiety disorder [30]. Generally, higher rates of anger are more common in people with depression or anxiety disorders [31].
Another important result to discuss is that related to the predictive factors related to the total quality of life of children, which is significantly influenced by their levels of physiological anxiety and social anxiety. These results are in line with the data presented in the literature on the impairment of quality of life in individuals with anxiety disorders. The impact is robust as it appears to be independent of the severity of symptoms, demographic variables, somatic health, and diagnostic comorbidity [31]. The decrease in quality of life in the social domain of patients with anxiety disorders could potentially contribute to the aetiology of individuals' psychiatric comorbid conditions, exacerbated individuals' health and conditions. In addition, a low quality of life can represent a risk factor for relapse after successful treatment for anxiety disorder [31].
With regard to the results in relation to the last objective of the present study, the resulting clinical implications are different. First of all, it emerges that the individual's quality of life is strongly influenced by the subject's social anxiety and worries; in addition, it is seen how the individual's total anxiety is influenced and predicted by the parent's quality of life, therefore on the well-being of the parent and the level of anger of the subject himself. Starting from these considerations, it must be kept in mind that in situations of prevention and promotion of health and well-being, it is essential to also implement anger management and control programmes in order to guarantee better well-being and prevent the evolution of anxious symptoms. To ensure and promote mental health in children and adolescents, it is useful to carry out anger management and control interventions to limit the emergence of anxious symptoms as much as possible and consequently worsen the subject's quality of life.
One of the strengths of the following study concerns the fact that the number of samples is quite high and the subjects come from different Italian regions, the samples are homogeneous and that of children is characterised by a fairly wide age range. Various standardised tests were used, with good psychometric properties that analyse associated constructs; in this way, it was possible to understand the relationship between the various variables and the constructs in greater depth. A further strong point consists of the fact that information was also collected from parents, it was thus possible to understand the relationship between their well being and how this influences that of their children.
Possible limitations of the following study concern the fact that there is a lack of data relating to the mental health of subjects prior to the outbreak of the Covid-19 pandemic, it was not possible to carry out a comparison and understand how this influenced the mental health of the subjects of the reference samples. Furthermore, the sample of parents is heterogeneous and predominantly characterised by mothers. A final limitation is characterised by the fact that there is a possibility that the responses to the items of the various tests and questionnaires administered to the subjects have been altered due to the phenomenon of social desirability or due to concerns regarding the possibility of showing a negative or too problematic image of oneself.
Possible future developments of the following study may include data on a specific clinical population to understand how the Covid-19 pandemic has affected the well-being and mental health of different groups of subjects. Another possible future direction is a more in-depth analysis of the relationship between the variables and a collection of more information regarding the health status of the parents to understand how their different psychological problems influence those of their children.
5. Conclusions
To conclude the following essay, it can be stated that it is essential to pay attention to the mental health of the child population and their parents. Parental well-being actively influences the well-being of children; consequently, when implementing preventive programmes and promoting child well-being, it is essential to also take into consideration the presence and role of parents in order to provide them with the most adequate support possible. It is also important to note that this study showed that the construct of anger is strongly correlated with anxiety and the latter is strongly correlated with quality of life. It is appropriate, when organising programmes for prevention and promotion of well-being, to reflect on how these constructs are related to each other and how important it is to organise a complete intervention also orientated towards the management of externalising symptoms such as anger to prevent the emergence of internalising symptoms of an anxious nature.
Author Contributions
Conceptualization, M.T.; methodology, R.M.I.; formal analysis, R.M.I.; investigation, R.M.I..; resources, M.T.; data curation, M.T.; writing—original draft preparation, R.M.I. and M.T.; writing—review and editing, R.M.I; supervision, M.T.; project administration, M.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Psychology Ethics Committee of the University of Padua (protocol code: 4039; date of approval: 3.2.2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
The raw data supporting the conclusions of this article will be available from the authors on request.
Acknowledgments
We acknowledge all children / adolescents and their parents who participated in this research.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Balenzano, C.; Moro, G.; Girardi, S. Families in the pandemic between challenges and opportunities: An empirical study of parents with preschool and school-age children. Italian Sociological Review 2020, 10(3S), 777–800. [Google Scholar]
- Petts, R.J.; Carlson, D.L.; Pepin, J.R. A gendered pandemic: Childcare, homeschooling, and parents' employment during COVID-19. Gender, Work and Organization 2020, 28(S2), 515–534. [Google Scholar] [CrossRef]
- Johnson, M.S.; Skjerdingstad, N.; Ebrahimi, O.V.; Hoffart, A.; Johnson, S.U. (2022). Parenting in a pandemic: Parental stress, anxiety and depression among parents during the government-initiated physical distancing measures following the first wave of COVID-19. Stress and Health 2022, 38(4), 637–652. [Google Scholar] [CrossRef]
- Yamamura, E.; Tsustsui, Y. The impact of closing schools on working from home during the COVID-19 pandemic: Evidence using panel data from Japan. Reviews of Household Economics 2021, 19, 41–60. [Google Scholar] [CrossRef]
- Spinelli, M.; Lionetti, F.; Pastore, M.; Fasolo, M. Parents' stress and children's psychological problems in families facing the COVID-19 outbreak in Italy. Frontiers in psychology 2020, 11, 1713. [Google Scholar] [CrossRef]
- Cerniglia, L.; Cimino, S.; Ammaniti, M. L’impatto del periodo di isolamento legato al Covid-19 nello sviluppo psicologico infantile. Psicologia clinica dello sviluppo 2020, 24(2), 187–190. [Google Scholar]
- Ravens-Sieberer, U., Erhart, M., Devine, J., Gilbert, M., Reiss, F., Barkmann, C.,... & Kaman, A. Child and adolescent mental health during the COVID-19 pandemic: results of the three-wave longitudinal COPSY study. Journal of Adolescent Health 2022, 71(5), 570–578.
- Arnett, J.J. The Oxford handbook of emerging adulthood, 3rd ed.; Oxford University: NY, USA, 2015. [Google Scholar]
- Orben, A.; Tomova, L.; Blakemore, S.J. The effects of social deprivation on adolescent development and mental health. Lancet Child Adol Health 2020, 4(8), 634–640. [Google Scholar] [CrossRef]
- Orban, E.; Li, L.Y.; Gilbert, M.; Napp, A.K.; Kaman, A.; Topf, S.; Boecker, M.; Devine, J.; Reiß, F.; Wendel, F.; Jung-Sievers, C.; Ernst, V.S.; Franze, M.; Möhler, E.; Breitinger, E.; Bender, S.; Ravens-Sieberer, U. Mental health and quality of life in children and adolescents during the COVID-19 pandemic: a systematic review of longitudinal studies. Frontiers in Public Health 2024, 11, 1275917. [Google Scholar] [CrossRef]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a meta-analysis. JAMA pediatrics 2021, 175(11), 1142–1150. [Google Scholar] [CrossRef]
- Ferreira, L.N.; Pereira, L.N.; da Fé Brás, M.; Ilchuk, K. Quality of life under the COVID-19 quarantine. Quality of Life Research 2021, 30, 1389–1405. [Google Scholar] [CrossRef]
- Eiser, C.; Varni, J.W. Health-related quality of life and symptom reporting: similarities and differences between children and their parents. European journal of pediatrics 2013, 172, 1299–1304. [Google Scholar] [CrossRef]
- Khanna, D.; Khadka, J.; Mpundu-Kaambwa, C.; Lay, K.; Russo, R.; Ratcliffe, J. Are we agreed? Self-versus proxy-reporting of paediatric health-related quality of life (HRQoL) using generic preference-based measures: a systematic review and meta-analysis. Pharmacoeconomics 2022, 40(11), 1043–1067. [Google Scholar] [CrossRef]
- Matza, L.S.; Patrick, D.L.; Riley, A.W.; Alexander, J.J.; Rajmil, L.; Pleil, A.M.; Bullinger, M. Pediatric patient-reported outcome instruments for research to support medical product labeling: report of the ISPOR PRO good research practices for the assessment of children and adolescents task force. Value Health 2013, 16(4), 461–479. [Google Scholar] [CrossRef]
- Roddenberry, A.; Renk, K. Quality of life in pediatric cancer patients: the relationships among parents’ characteristics, children’s characteristics, and informant concordance. J Child Fam Stud 2008, 17(3), 402–26. [Google Scholar] [CrossRef]
- Otero, S.; Eiser, C.; Wright, N.; Butler, G. Implications of parent and child quality of life assessments for decisions about growth hormone treatment in eligible children. Child Care Health Dev 2013, 39(6), 782–8. [Google Scholar] [CrossRef]
- Brazier, J.; Ratcliffe, J.; Saloman, J.; Tsuchiya, A. Measuring and valuing health benefits for economic evaluation, 2nd ed.; University Press: Oxford, UK, 2016. [Google Scholar]
- Ravens-Sieberer, U.; Erhart, M.; Devine, J.; Gilbert, M.; Reiss, F.; Barkmann, C.; Siegel, N.A.; Simon, A.M.; Hurrelmann, K.; Schlack, R.; Hölling, H.; Wieler, L.H.; Kaman, A. Child and adolescent mental health during the COVID-19 pandemic: results of the three-wave longitudinal COPSY study. Journal of Adolescent Health 2022, 7(5), 570–578. [Google Scholar] [CrossRef]
- De Bles, N.J.; Ottenheim, N.R.; van Hemert, A.M.; Pütz, L.E.; van der Does, A.W.; Penninx, B.W.; Giltay, E.J. Trait anger and anger attacks in relation to depressive and anxiety disorders. Journal of affective disorders 2019, 259, 259–265. [Google Scholar] [CrossRef]
- Cox, D.E.; Harrison, D.W. Models of anger: contributions from psychophysiology, neuropsychology and the cognitive behavioral perspective. Brain Structure and Function 2008, 212, 371–385. [Google Scholar] [CrossRef]
- Bozzola, E.; Ferrara, P.; Spina, G.; Villani, A.; Roversi, M.; Raponi, M.; Corsello, G.; Staiano, A. The pandemic within the pandemic: the surge of neuropsychological disorders in Italian children during the COVID-19 era. Italian Journal of Pediatrics 2022, 48(1), 1–8. [Google Scholar] [CrossRef]
- Ludwig-Walz, H.; Dannheim, I.; Pfadenhauer, L.M.; Fegert, J.M.; Bujard, M. Anxiety among children and adolescents during the COVID-19 pandemic in Europe: a systematic review protocol. Systematic Reviews 2023, 12(1), 1–9. [Google Scholar] [CrossRef]
- Marchetti, D.; Fontanesi, L.; Mazza, C.; Di Giandomenico, S.; Roma, P.; Verrocchio, M.C. Parenting-related exhaustion during the Italian COVID-19 lockdown. Journal of pediatric psychology 2020, 45, 1114–1123. [Google Scholar] [CrossRef]
- Mocho, H.; Martins, C.; dos Santos, R.; Nunes, C. Parental Involvement and Stress in Children’s Quality of Life: A Longitudinal Study with Portuguese Parents during the COVID-19 Pandemic Period. Children 2024, 11(4), 440. [Google Scholar] [CrossRef]
- Reynolds, C.R.; Richmond, B.O. Revised children’s manifest anxiety scale: Second edition (RCMAS-2); WPS Online Evaluation system: Los Angeles, CA, 2008. Italian adaption by Scozzari, S., Sella, F., Di Pietro, M.; Giunti Psychometrics: Firenze, Italy, 2012. [Google Scholar]
- Nelson, W.; M Finch, A.J. Children’s Inventory of Anger (ChIA); Western Psychological Services: Los Angeles, USA, 2000; Italian adaptation by Ardizzone, I., Ferrara, M.; Giunti Psychometrics: Firenze, Italy, 2013. [Google Scholar]
- Varni, J.W.; Limbers, C.A.; Bryant, W.P.; Wilson, D.P. The PedsQL multidimensional fatigue scale in pediatric obesity: feasibility, reliability and validity. Int J Pediatr Obes. 2010, 5(1), 34–42. [Google Scholar] [CrossRef]
- Reid, J.A.; Chenneville, T.; Gardy, S.M.; Baglivio, M.T. An exploratory study of COVID-19’s impact on psychological distress and antisocial behavior among justice-involved youth. Crime & Delinquency 2022, 68(8), 1271–1291. [Google Scholar]
- Walsh, L.M.; Benjamin Wolk, C.; Becker-Haimes, E.M.; Jensen-Doss, A.; Beidas, R.S. The relationship between anger and anxiety symptoms in youth with anxiety disorders. Journal of child and adolescent counseling 2018, 4(2), 117–133. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Cisler, J.M.; Tolin, D.F. Quality of life in the anxiety disorders: a meta-analytic review. Clinical psychology review 2007, 27(5), 572–581. [Google Scholar] [CrossRef]
Figure 1.
Distribution of children and adolescents' scores on the anxiety scales of the RCMAS-2 test (a) and on the ChIA scores (b).
Figure 1.
Distribution of children and adolescents' scores on the anxiety scales of the RCMAS-2 test (a) and on the ChIA scores (b).
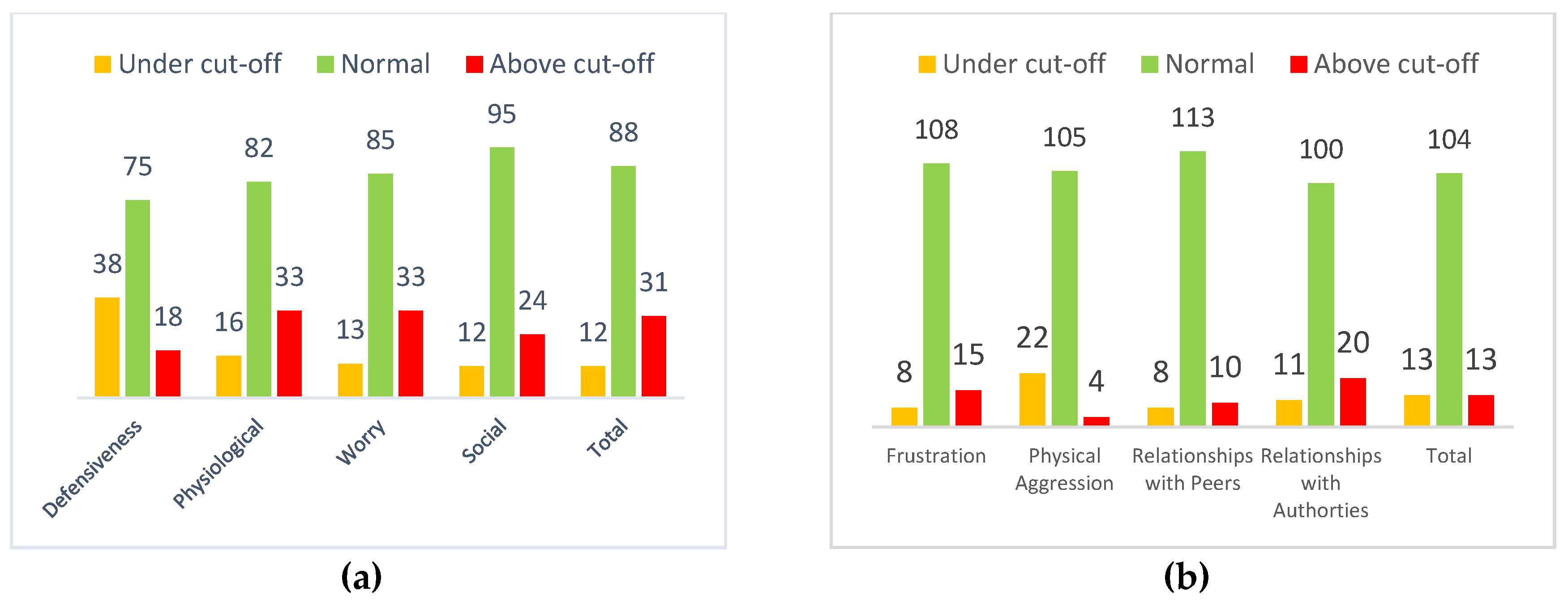
Figure 2.
Comparison of self-report and proxy means of Quality of Life scores.
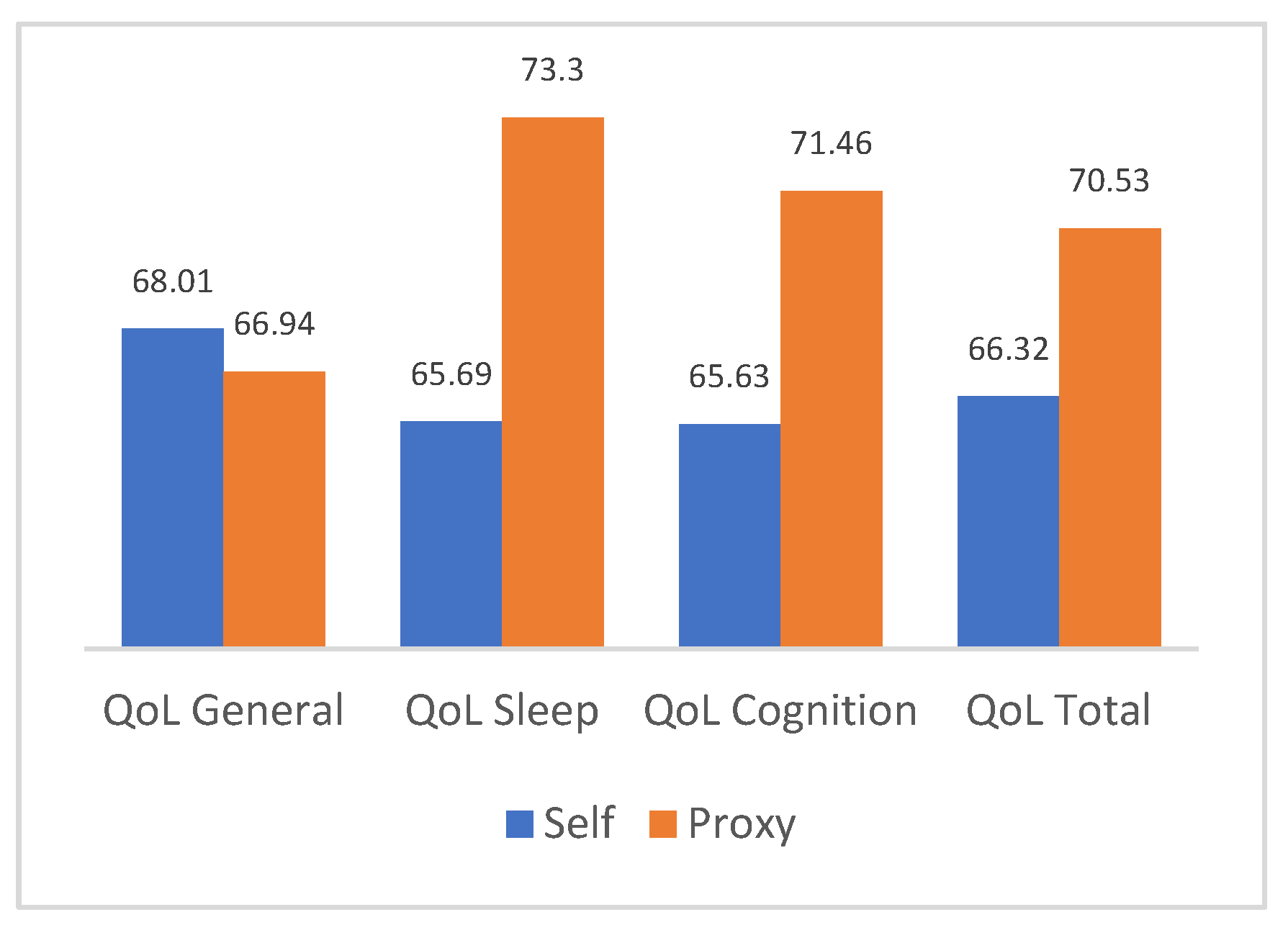

Table 1.
Sociodemographic characteristics of samples.
| Statistics | Frequencies | ||||||
|---|---|---|---|---|---|---|---|
| Min | Max | M | SD | ||||
| Children’s age | 6 | 16 | 12.44 | 2.74 | |||
| Children’s gender | Male Female |
60 71 |
45.8% 54.2% |
||||
| Children’s School level | Primary school Secondary school, 1st Secondary school 2nd |
35 50 46 |
26.7% 38.2% 35.1% |
||||
| Parental Age | 30 | 66 | 46.46 | 6.02 | |||
| Parent’s gender | Male Female |
26 105 |
19.8% 80.2% |
||||
| Parental Schooling Years | 5 | 20 | 13.82 | 3.42 | |||
| Parental Civil status |
Single parent Twice parents |
10 121 |
7.6% 92.4% |
||||
| Parental Perceived economic condition |
Low Medium High |
23 72 36 |
16.6% 55.0% 27.5% |
||||
Table 2.
Distribution of Quality of Life scores along with children and adolescents’ self-reports.
| QoL General | QoL Sleep | QoV cognition | Total QoL total | |||||
|---|---|---|---|---|---|---|---|---|
| Freq. | Perc. | Freq. | Perc. | Freq. | Perc. | Freq. | Perc. | |
| Very low QOL | 1 | 0.8% | 6 | 4.6% | 6 | 4.6% | 0 | 0% |
| Low Quality of Life | 21 | 16% | 19 | 14.5% | 21 | 16% | 14 | 10.7% |
| Moderate QoL | 72 | 55% | 75 | 57.3% | 65 | 49.6% | 88 | 67.2% |
| Good QoL | 37 | 28.2% | 31 | 23.7% | 39 | 29.8% | 29 | 22.1% |
| Total | 131 | 100% | 131 | 100% | 131 | 100% | 131 | 100% |
Table 3.
Distribution of Quality of Life scores along parental self-reports.
| QoL General | QoL Sleep | QoL cognition QoL total | ||||||
|---|---|---|---|---|---|---|---|---|
| Freq. | Perc. | Freq. | Perc. | Freq. Perc. Freq- | Perc. | |||
| Very low QOL | 8 | 6.1% | 0 | 0% | 4 | 3.1% | 1 | 0.8% |
| Low QoL |
36 | 27.5% | 16 | 12.2% | 30 | 22.9% | 25 | 19.1% |
| Moderate QoL | 66 | 50.4% | 67 | 51.1% | 50 | 38.2% | 76 | 58% |
| Good QoL | 21 | 16% | 48 | 36.6% | 47 | 35.9% | 29 | 22.1% |
| Total | 131 | 100% | 131 | 100% | 131 | 100% | 131 100% | |
Table 4.
Stepwise regression model with anxiety in children and adolescents as dependent variable.
| Model | Anovaa | Coefficientsa | |||||||
|---|---|---|---|---|---|---|---|---|---|
| R-square | Df | F | p. | Beta | T | P | |||
| Model | .15 | 3 | 7.6 | .0001b | |||||
| Sex | .22 | 2.68 | .008* | ||||||
| Parents of PEDS TOT self-report | -.197 | -2.40 | .018* | ||||||
| Total Anger | .24 | 2.93 | .004* | ||||||
aDependent variable: Total anxiety b Predictors: Sex, PEDS TOT self-report parents, Total Anger. * p<.005.
Table 5.
Stepwise regression model with self-report quality of life for children and adolescents as dependent variable.
Table 5.
Stepwise regression model with self-report quality of life for children and adolescents as dependent variable.
| Model | Anovaa | Coefficientsa | |||||
|---|---|---|---|---|---|---|---|
| R-square | Df | F | p. | Beta | T | P | |
| Model | .33 | 2 | 31.67 | .0001b | |||
| Physiological anxiety | -.34 | -4.12 | .0001* | ||||
| Social Anxiety | -.32 | -3.90 | .0001* | ||||
aDependent variable: PEDS TOT self-report children/adolescents b Predictors: Physical anxiety, Social anxiety * p<.005.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



