
Submitted:
05 May 2024
Posted:
06 May 2024
You are already at the latest version
Abstract
The article presents the case of a 27-year-old female patient with idiopathic congenital complete heart block who was referred by her primary care physician for cardiological evaluation. The conduction disturbance was recognized at the age of 6 years and was asymptomatic. The disqualification from pacemaker implantation included detailed history of a patient’s symptoms, echocardiographic assessment of the heart, exercise testing and ECG Holter monitoring. The aid of salbutamol administered orally was also useful.
Keywords:
congenital heart block
; cardiac pacemaker
; atropine
; salbutamol
1. Introduction
Complete heart block (CHB), also known as third-degree atrioventricular block (AV III block), is a disturbance with abnormal propagation of the electrical impulses due to structural or functional abnormalities of the cardiac conduction system at the level of AV junction or below it. CHB might occur in a structurally normal heart as an isolated disorder or might accompany various congenital heart defects [1]. CHB is classified as congenital AV block if is diagnosed in utero, at birth or within the first month of life. Childhood AV block diagnosis is made when CHB is identified between the first month and eighteen years of life [2]. In general, the incidence of third-degree congenital AV heart block is 1 in 15,000–22,000 live births [1,3,4]. CHB as a complication of an autoimmune process is characterized by high neonatal mortality rate whereas the overall mortality without cardiac pacing reaches 8-16% in infants and is half this rate in children and adults [5,6].
Apart from a diversified etiology, CHB is associated with different clinical presentations. Thus, patients may be asymptomatic or present with reduced exercise capacity, syncopal attacks, and symptoms of heart failure related to bradycardia [2]. Nevertheless, imaging studies can reveal alterations of atrial and ventricular myocardium associated with proinflammatory state with signs myocarditis and endocardial fibroelastosis. This would lead to atrial and ventricular dilatation, hyperechogenicity especially of the atrial walls due to fibrosis and reduced ventricular contractility with clinical complications of chronic heart failure with pericardial effusion, ascites or fetal hydrops [7,8]. Moreover, all these pathological phenomena can promote diverse heart arrhythmias. Although sudden cardiac death is rare, bradycardia itself may predispose to dangerous ventricular arrhythmias such as polymorphic ventricular tachycardia called torasade-de-pointes [9].
If the heart block is transient, usually no further therapy is required. Whenever congenital CHB is permanent, cardiac pacing should be considered even in children, if there are no contraindications [10]. On the other hand, the question arises, does literally everyone with congenital CHB requires permanent cardiac stimulation?
A doctor consulting or caring for a patient with congenital AV block always has concerns about whether to refer the patient for pacemaker implantation or not, or not yet ("pace or not-to-pace")? Thus, which essential tools, apart from resting electrocardiogram (ECG), need to be used to assess a patient for indications for pacemaker implantation?
- Detailed medical history needs to be collected in order to answer the question if there are there any symptoms (syncope, exercise intolerance, palpitations, symptoms of heart failure).
- Physical examination ought to check the signs of bradycardia and heart failure.
- Echocardiography should be performed to assess the presence of valvular heart disease and to assess the size and function of the heart. In some patients, long-term AV block may cause left ventricular dyssynchrony.
- Exercise ECG should be performed and chronotropic capacity and exercise tolerance should be assessed.
- ECG monitoring using the Holter method to assess the average, minimum and maximum rhythm rate, assess whether there is ventricular arrhythmia and inhibitions and interruptions in the leading rhythm and QT interval duration [11].
2. Case Presentation
We present the case of a 27-year-old female patient with congenital CHB who was referred by her primary care physician for cardiological evaluation. The complete AV block was recognized when she was 6 years old. Neither structural abnormalities of the heart were found, nor autoimmune diseases could be confirmed in the diagnostics performed at the time of diagnosis and in the subsequent follow-up. The idiopathic CHB was recognized. Ever since the patient has been asymptomatic and denied all the above-mentioned symptoms what was the main reason why her parents did not consent to the girl having a pacemaker implanted, neither the patient did herself. Additionally, there was no history of other chronic conditions requiring pharmacological treatment and no family history of heart diseases and conduction problems.
The ECG recording is shown in Figure 1, Figure 2 and Figure 3. We have two separate rhythms - sinus rhythm of atria (sinus P waves visible) approximately 70 beats per minute (bpm), and AV link rhythm 45 bpm (cycle’s length of 1330 ms). The QT interval is 440 ms, corrected QT interval - QTc is 380 ms.
Transthoracic echocardiography showed normal function (left ventricular ejection fraction - EF of 65%) and normal sizes of the heart chambers and atrioventricular valves’ function. The treadmill exercise test performed according to the Bruce’s protocol showed good chronotropic efficiency with an acceleration of the heart rate from 45 bpm to approximately 80 bpm. The patient had a very good exercise tolerance of 12.4 metabolic equivalents (METs), without any disturbing clinical symptoms. Holter ECG monitoring showed a mean heart rate with junctional rhythm of 54 bpm (minimal heart rate 41 bpm, maximal heart rate 78 bpm). The mean atrial sinus rhythm was 74 bpm. No supraventricular or ventricular arrhythmias were recorded. There were no pauses above 3 seconds.
Therefore, after the initial diagnosis, there are no reasons to recommend the patient for pacemaker implantation. So far, the patient has been using salbutamol 4 mg once daily and tropane alkaloids (atropine 0.25 mg atropine sulfate) once daily orally. We have modified the treatment. Only salbutamol 4 mg once daily per os was left once daily.
3. Discussion
In children and adolescents CHB associated with an autoimmune disease, predominantly systemic lupus erythematosus or Sjoegren's syndrome, is the most common form. The congenital CHB associated with neonatal lupus is considered a form of passively acquired autoimmune disease in which maternal autoantibodies to the intracellular ribonucleoproteins Ro (SS-A) and La (SS-B). They cross the placenta and through fetal circulation bind to L-type calcium channels of cardiomyocytes which induces perturbation of calcium metabolism, leads to apoptosis of cells, local inflammation and fibrosis of cardiac conduction system [12]. Women with serum titers of anti-Ro antibody carry a 3% risk of having a child with neonatal lupus syndrome. Recurrence rates are about 18% [13]. Interestingly, only 2–5% of pregnancies with elevated circulating maternal anti-Ro/SSA or anti-La/SSB antibodies levels result in fetuses with CHB [3].
Secondary CHBs are one of the main complications of a congenital heart disease surgery [14]. The most common structural abnormalities involve transposition of the great vessels and defects of the AV septum [15]. Noteworthy, in many patients the cause of third-degree congenital AV block is unknown. These idiopathic forms of CHB might be associated with genetic abnormalities without apparent associations with autoimmune diseases and observed in a structurally normal heart [2]. CHB might have the background of complex pathophysiological processes related to certain genetic variants of genes and gene networks coding ion channels, including SCN5A, SCN1B, SCN10A, TRPM4, KCINK17, CAVB, KCNJ2, HCN4, LMNA, ANKB, NKX2-5 and TBX5, and cardiac connexin proteins leading to isolated AV block or to progressive cardiac conduction disease with various intraventricular conduction disturbances [1,16,17]. Moreover, inherited progressive cardiac conduction disease (PCCD) with interventricular and AV conduction disturbances with subsequent CHB has been identified to be associated with mutations of genes encoding for proteins crucial for cardiac chamber formation, endocardial cushion remodeling and conduction system development [18]. CHB in children and young adults can occur as a consequence of a broad array of causes such as infectious process with myocarditis, infiltrative processes, metabolic abnormalities, hypothyroidism, pathological neurocardiogenic mechanisms or even coronary artery disease. It can be also met in Lyme carditis and Chagas disease and inflammatory conditions of Kawasaki disease and acute rheumatic carditis [19,20]. CHB is among rare but typical complications of surgical and catheterization-induced trauma and interventional procedures with perimembranous ventricular septum defect and catheter ablations of AV nodal reentrant tachycardia and septal accessory pathways, especially of parahisian localization [2,21].
After determining the cause of the AV block, every symptomatic and non-reversible CHB requires permanent pacemaker implantation [10,11]. Certainly, in the absence of contraindications to the procedure including severe coagulation abnormalities, excessive risk of bleeding due to vascular access, local infection at implantation site or ongoing bacteremia. There is also an issue of patient’s consent or the consent of parents of an underage patient. At times, the aesthetic reasons are responsible for the lack of consent to implantation, especially in women [22]. Additionally, another reason for refusal may be fear of complications. The most common complications of pacemaker implantation procedure cover lead-related reinterventions (including dislodgement, malposition, subclavian crush syndrome, etc.), implantable electronic devices (CIED)-related infections (superficial infection, pocket infections, systemic infections), pneumothorax, hemothorax, brachial plexus injury, cardiac perforation, coronary sinus dissection/perforation, need for revision due to pain/discomfort, diaphragmatic stimulation requiring reintervention, hematoma, tricuspid regurgitation, pacemaker syndrome, generator/lead problem, deep venous thrombosis (acute or chronic) and death [11]. In a real-life study on >81,000 adult cardiac implantable electronic devices’ recipients major complications occurred in 8.2% of patients within 90 days of hospital discharge [23]. The scale of the problem in the pediatric population is significantly greater [24].
Classic right ventricular stimulation with right ventricular apex position of the lead tip is easily accessible and provides a stable position. Unfortunately, it has been shown to be complicated by ventricular desynchronization, myocardial dystrophic changes and cardiac dilatation and is recognized as an important cause of dilated cardiomyopathy (pacing-induced cardiomyopathy) [8,25]. Techniques of cardiac pacing have been evolving throughout the years to allow safer and more efficient performance of the heart even in patients with heart defects and after corrective surgeries. Some of these complications could be significantly reduced by implementation of cardiac resynchronization therapy (CRT) with an extra lead placed in coronary sinus tributary responsible for stimulation of lateral and posterior walls of the left ventricle at the same time of interventricular septum activation evoked by right ventricular lead [26,27]. In the very recent years, we have also witnessed the flourishing of the methods based on conduction system pacing (CSP) encompassing direct His bundle and its branches stimulation. CRT and CSP, together referred as cardiac physiologic pacing (CPP), are widely propagated in order to avoid or mitigate heart failure development related do permanent pacing [28].
Cardiac pacing in pediatric patients encounters its distinctive problems related to anatomy and somatic growth. Although the smallest infants, with weight below 15-20 kg, are served best with epicardial systems, epicardial leads are susceptible to fracture and exit block development and require a major operation. To the contrary, endocardial systems are associated with increased venous thrombosis in infants, which may result in loss of venous access. Moreover, extraction of transvenous leads in children is more difficult and bears higher risk of periprocedural complications. Nevertheless, the longevity of endocardial system, especially with spare lead loops, exceeds the endurance of epicardial ones [29,30]. As the transvenously implanted leads are considered the Achilles’ heel of pacemakers, and after years they need to be replaced with new ones, great hopes are associated with leadless systems. Advances in battery technology and miniaturization of electronics now offer the opportunity to implant the whole pacemaker system into the right ventricle in selected groups of patients, e.g. without venous access. The latest models are even equipped with AV synchronization function based on a sensor detecting mechanical movements of atria [31]. It seems that also new methods introduced in the treatment of bradycardia such as cardioneuroablation may find application in some patients with AV blocks [32].
What are the indications for permanent pacing in adult patients with congenital AV block? According to the current European Society of Cardiology 2021 guidelines on cardiac pacing, the indication for permanent cardiac pacing in class I recommendations is the presence of one of the following risk factors of aforementioned CHB complications:
- occurrence of the symptoms mentioned earlier
- left ventricular systolic dysfunction
- pauses > 3 times the basic rhythm (e.g. in our case the average cycle is 1330 ms, so the pause > 3.990 ms (> ~ 4 seconds)
- escape rhythm with wide QRS complexes
- prolonged QTc interval; it should be remembered that Bazett's correction rule overestimates QTc for rhythms above 100 bpm and underestimates QTc for rhythms below 50 bpm.
- occurrence of complex ventricular arrhythmias
The presented female patient with applied pharmacology had none of the risk factors, thus pacemaker implantation could be avoided. Nevertheless, the constant observation and repeated evaluations of these risk factors on regular basis is necessary.
The role of pharmacological treatment of CHB is limited. Tracing the natural history of CHB development in collagen tissue diseases, its onset commonly occurs between 18 and 24 weeks of gestational age [35,36]. It is frequently preceded by ventricular ectopy, junctional and ventricular tachycardia, changes of ST-T and QT interval prolongation. The fetus then adopts to bradycardia usually of 50-70 bpm. Nevertheless, on some occasions heart rate drops below 50 bpm and displays low variability. In these cases a beta-adrenergic agonist terbutaline might be used to increase heart rate. Additionally, the use of dexamethasone in CHB in some centers was linked to reduced long-term cardiomyopathy. Intravenous immunoglobulin has been shown to prevent mortality in fetuses with hydrops. It also reduced endocardial fibroelastosis and subsequent ventricular dysfunction. Moreover, dexamethasone or betamethasone and hydroxychloroquine hampered progression in partial AV block to CHB in systemic lupus erythematosus [36,37]. In some centers prenatal treatment, apart from intravenous immunoglobulins, includes also plasmapheresis and their combinations with steroids [38,39]. In these regimens the side effects of the drugs need to be considered. The side effects only of fluorinated steroids include miscarriage, oligohydramnios, delayed development and growth retardation, adrenal insufficiency. The therapy complications in mothers involving diabetes, hypertension and weight gain might be significant [1].
After birth, bradycardia usually of <70 bpm can initially be controlled by drugs such as isoprenaline, atropine, epinephrine, dopamine alone or in combinations with temporary cardiac pacing to prevent sudden death and before permanent pacing introduction [2,40,41].
As for pharmacological treatment of adult patient with CHB, which is rather an alternative approach, data are scarce and stem from case-by-case basis. The drugs used there decrease vagal nerve activity – like atropine and its derivative or stimulate sympathetic nervous system like salbutamol [42]. There are also reports on methylxanthines - theophylline and aminophylline (a theophylline derivative) with positive effects in CHB [43].
4. Conclusions
Congenital complete heart block is a condition that potentially requires pacemaker implantation. As treatment with permanent cardiac pacing might be associated with periprocedural complications and numerous inconveniences in life, the disqualification from pacemaker includes detailed history, echocardiographic assessment of the heart, exercise testing and ECG Holter monitoring. The aid of chronotropic positive drugs might be useful.
Author Contributions
Conceptualization, P.K., B.P.; Methodology, P.K., B.P.; Software, P.K., J.W.; Validation, P.K., B.P.; Formal Analysis, P.K., B.P. and J.W.; Investigation, P.K., B.P.; Resources, B.P., J.W.; Data curation, P.K., B.P.; Writing—original draft preparation, P.K., J.W.; Writing—review and editing, P.K., J.W.; Visualization, P.K., B.P. and J.W.; Supervision, B.P., J.W.; Project administration, P.K., B.P. and J.W.; Funding acquisition, P.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from the patient involved in the study.
Data Availability Statement
The study did not report any data.
Acknowledgments
The authors would like to thank the patient for her participation in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Melim, C.; Pimenta, J.; Areias, J.C. Congenital atrioventricular heart block: From diagnosis to treatment. Rev. Port. Cardiol. 2022, 41, 231–240. [Google Scholar] [CrossRef]
- Baruteau, A.E.; Pass, R.H.; Thambo, J.B.; Behaghel, A.; Le Pennec, S.; Perdreau, E.; Combes, N.; Liberman, L.; McLeod, C.J. Congenital and childhood atrioventricular blocks: Pathophysiology and contemporary management. Eur. J. Pediatr. 2016, 175, 1235–1248. [Google Scholar] [CrossRef] [PubMed]
- Brito-Zeron, P.; Izmirly, P.M.; Ramos-Casals, M.; Buyon, J.P.; Khamashta, M.A. The clinical spectrum of autoimmune congenital heart block. Nat. Rev. Rheumatol. 2015, 11, 301–312. [Google Scholar] [CrossRef]
- Ho, A.; Gordon, P.; Rosenthal, E.; Simpson, J.; Miller, O.; Sharland, G. Isolated complete heart block in the fetus. Am. J. Cardiol. 2015, 116, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Jaeggi, E.T.; Hamilton, R.M.; Silverman, E.D.; Zamora, S.A.; Hornberger, L.K. Outcome of children with fetal, neonatal or childhood diagnosis of isolated congenital atrioventricular block. A single institution's experience of 30 years. J. Am. Coll. Cardiol. 2002, 39, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Michaëlsson, M.; Jonzon, A.; Riesenfeld, T. Isolated congenital complete atrioventricular block in adult life. A prospective study. Circulation 1995, 92, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Clark, T.J.; Tan, J.H.; Delaney, S.; Jolley, J.A. Ultrasound findings in fetal congenital heart block associated with maternal anti-Ro/SSA and anti-La/SSB antibodies. Ultrasound Q. 2015, 31, 34–36. [Google Scholar] [CrossRef] [PubMed]
- Moak, J.P.; Barron, K.S.; Hougen, T.J.; Wiles, H.B.; Balaji, S.; Sreeram, N.; Cohen, M.H.; Nordenberg, A.; Van Hare, G.F.; Friedman, R.A.; et al. Congenital heart block: Development of late-onset cardiomyopathy, a previously underappreciated sequela. J. Am. Coll. Cardiol. 2001, 37, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Nikolic, G.; Arnold, J.; Coles, D.M. Torsade de pointes and asystole in a child with complete heart block and prolonged QT interval. Aust. Paediatr. J. 1983, 19, 187–191. [Google Scholar] [CrossRef]
- Shah, M.J.; Silka, M.J.; Avari Silva, J.N.; Balaji, S.; Beach, C.M.; Benjamin, M.N.; Berul, C.I.; Cannon, B.; Cecchin, F.; Cohen, M.I.; Dalal, A.S.; et al. 2021 PACES expert consensus statement on the indications and management of cardiovascular implantable electronic devices in pediatric patients. Cardiol. Young 2021, 31, 1738–1769. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef] [PubMed]
- Ambrosi, A.; Wahren-Herlenius, M. Congenital heart block: Evidence for a pathogenic role of maternal autoantibodies. Arthritis Res. Ther. 2012, 14, 208. [Google Scholar] [CrossRef] [PubMed]
- Buyon, J.P.; Heibert, R.; Copel, J.; Craft, J.; Friedman, D.; Katholi, M.; Lee, L.A.; Provost, T.T.; Reichlin, M.; Rider, L.; et al. Autoimmune-associated congenital heart block: Mortality, morbidity, and recurrence rates obtained from a national neonatal lupus registry. J. Am. Coll. Cardiol. 1998, 31, 1658–1666. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.S.; Rausa, J.; Villarreal, E.; Farias, J.S.; Flores, S. Postoperative atrioventricular block in pediatric patients: Impact of congenital cardiac malformations and medications. Pediatr. Cardiol. 2024, 45, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Brugada, J.; Blom, N.; Sarquella-Brugada, G.; Blomstrom-Lundqvist, C.; Deanfield, J.; Janousek, J.; Abrams, D.; Bauersfeld, U.; Brugada, R.; Drago, F.; et al. Pharmacological and non-pharmacological therapy for arrhythmias in the pediatric population: EHRA and AEPC-Arrhythmia Working Group joint consensus statement. Europace 2013, 15, 1337–1382. [Google Scholar] [CrossRef] [PubMed]
- Kanter, R.J.; Pfeiffer, R.; Hu, D.; Barajas-Martinez, H.; Carboni, M.P.; Antzelevitch, C. Brugada-like syndrome in infancy presenting with rapid ventricular tachycardia and intraventricular conduction delay. Circulation 2012, 125, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Makita, N.; Seki, A.; Sumitomo, N.; Chkourko, H.; Fukuhara, S.; Watanabe, H.; Shimizu, W.; Bezzina, C.R.; Hasdemir, C.; Mugishima, H. A connexin40 mutation associated with a malignant variant of progressive familial heart block type I. Circ. Arrhythm. Electrophysiol. 2012, 5, 163–172. [Google Scholar] [CrossRef] [PubMed]
- McCulley, D.J.; Black, B.L. Transcription factor pathways and congenital heart disease. Curr. Top. Dev. Biol. 2012, 100, 253–277. [Google Scholar] [CrossRef]
- Forrester, J.D.; Mead, P. Third-degree heart block associated with lyme carditis: Review of published cases. Clin. Infect. Dis. 2014, 59, 996–1000. [Google Scholar] [CrossRef]
- Barra, S.N.; Providência, R.; Paiva, L.; Nascimento, J.; Marques, A.L. A review on advanced atrioventricular block in young or middle-aged adults. Pacing Clin. Electrophysiol. 2012, 35, 1395–1405. [Google Scholar] [CrossRef]
- Yildirim, I.; Karagöz, T.; Ertuğrul, I.; Karagöz, A.H.; Özer, S. Efficacy and safety of cryoablation of parahissian accessory pathways in children: A single institution study. Pacing Clin. Electrophysiol. 2013, 36, 1495–1502. [Google Scholar] [CrossRef] [PubMed]
- Salinas, C.A.; Ezzeddine, F.M.; Mulpuru, S.K.; Asirvatham, S.J.; Sharaf, B.A. Cardiac implantable electronic devices in female patients: Esthetic, breast implant, and anatomic considerations. J. Cardiovasc. Electrophysiol. 2024, 35, 747–761, Online ahead of print. [Google Scholar] [CrossRef]
- Ranasinghe, I.; Labrosciano, C.; Horton, D.; Ganesan, A.; Curtis, J.P.; Krumholz, H.M.; McGavigan, A.; Hossain, S.; Air, T.; Hariharaputhiran, S. Institutional variation in quality of cardiovascular implantable electronic device implantation: A cohort study. Ann. Intern. Med. 2019, 171, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Winkler, F.; Von Felten, S.; Gass, M.; Berger, F.; Weber, R.; Dave, H.; Balmer, C. Lead and generator dysfunction in children and adolescents with epicardial pacemaker and implantable cardioverter defibrillator systems: The challenge of early recognition. Pacing Clin. Electrophysiol. 2024, 47, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Thambo, J.B.; Bordachar, P.; Garrigue, S.; Lafitte, S.; Sanders, P.; Reuter, S.; Girardot, R.; Crepin, D.; Reant, P.; Roudaut, R.; et al. Detrimental ventricular remodeling in patients with congenital complete heart block and chronic right ventricular apical pacing. Circulation 2004, 110, 3766–3772. [Google Scholar] [CrossRef] [PubMed]
- Wiliński, J.; Czarnecka, D.; Kloch-Badełek, M. Cardiac resynchronization therapy in the treatment of chronic heart failure. Przew. Lek. 2008, 4, 48–53. [Google Scholar]
- Wiliński, J.; Czarnecka, D.; Wojciechowska, W.; Kloch-Badełek, M.; Jastrzębski, M.; Bacior, B.; Sondej, T.; Kusak, P.; Przybyła, A.; Kawecka-Jaszcz, K. Clinical and classic echocardiographic features of patients with, and without, left ventricle reverse remodeling following the introduction of cardiac resynchronization therapy. Cardiol. J. 2011, 18, 157–164. [Google Scholar] [PubMed]
- Chung, M.K.; Patton, K.K.; Lau, C.P.; Dal Forno, A.R.J.; Al-Khatib, S.M.; Arora, V.; Birgersdotter-Green, U.M.; Cha, Y.M.; Chung, E.H.; Cronin, E.M. ; 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm 2023, 20, e17–e91. [Google Scholar] [CrossRef]
- Takeuchi, D.; Tomizawa, Y. Pacing device therapy in infants and children: A review. J. Artif. Organs. 2013, 16, 23–33. [Google Scholar] [CrossRef]
- Wilhelm, B.J.; Thöne, M.; El-Scheich, T.; Livert, D.; Angelico, R.; Osswald, B. Complications and risk assessment of 25 years in pediatric pacing. Ann. Thorac. Surg. 2015, 100, 147–153. [Google Scholar] [CrossRef]
- Vouliotis, A.I.; Roberts, P.R.; Dilaveris, P.; Gatzoulis, K.; Yue, A.; Tsioufis, K. Leadless pacemakers: Current achievements and future perspectives. Eur. Cardiol. 2023, 18, e49. [Google Scholar] [CrossRef]
- Pachon-M, J.C.; Ortencio, F.A.; Pachon-M, E.I.; Lobo, T.; Santillana-P, T.G.; Pachon, C.T. , Cunha-P, M.Z.; Pachon-M, J.C.M.; Zerpa-A, J.C.; Amarante, R.C. Treatment of symptomatic functional atrioventricular block by cardioneuroablation as an alternative to pacemaker implantation. JACC Case Rep. 2022, 4, 990–995. [Google Scholar] [CrossRef] [PubMed]
- Kukla, P.; Jastrzębski, M.; Fijorek, K.; Stec, S.; Bryniarski, L.; Czarnecka, D.; Baranchuk, A. Electrocardiographic parameters indicating worse evolution in patients with acquired long QT syndrome and torsades de pointes. Ann. Noninvasive Electrocardiol. 2016, 21, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, R.; Wojciechowski, D.; Kozłowski, D.; Kukla, P.; Kurpesa, M.; Lelakowski, J.; Maciejewska, M.; Średniawa, B.; Wranicz, J.K. Electrocardiographic criteria for diagnosis of the heart chamber enlargement, necrosis and repolarization abnormalities including acute coronary syndromes. Experts' group statement of the Working Group on Noninvasive Electrocardiology and Telemedicine of the Polish Cardiac Society. Kardiol Pol. 2016, 74, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Cuneo, B.F.; Strasburger, J.F.; Huhta, J.C.; Gotteiner, N.L.; Wakai, R.T. Electrophysiological characteristics of fetal atrioventricular block. J. Am. Coll. Cardiol. 2008, 51, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Strasburger, J.F.; Eckstein, G.; Butler, M.; Noffke, P.; Wacker-Gussmann, A. Fetal arrhythmia diagnosis and pharmacologic management. J. Clin. Pharmacol. 2022, 62, S53–S66. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Silverman, E.; Golding, F.; Guerra, V.; Hiraki, L.; Thakur, V.; Jaeggi, E. Effects of transplacental dexamethasone therapy on fetal immune-mediated complete heart block. Fetal Diagn. Ther. 2021, 48, 183–188. [Google Scholar] [CrossRef]
- Friedman, D.M.; Llanos, C.; Izmirly, P.M.; Brock, B.; Byron, J.; Copel, J.; Cummiskey, K.; Dooley, M.A.; Foley, J.; Graves, C.; et al. Evaluation of fetuses in a study of intravenous immunoglobulin as preventive therapy for congenital heart block: Results of a multicenter, prospective, open-label clinical trial. Arthritis Rheum. 2010, 62, 1138–1146. [Google Scholar] [CrossRef] [PubMed]
- Ruffatti, A.; Cerutti, A.; Favaro, M.; Del Ross, T.; Calligaro, A.; Hoxha, A.; Marson, P.; Leoni, L.; Milanesi, O. Plasmapheresis, intravenous immunoglobulins and bethametasone - a combined protocol to treat autoimmune congenital heart block: A prospective cohort study. Clin. Exp. Rheumatol. 2016, 34, 706–713. [Google Scholar]
- De Caluwé, E.; Van De Bruaene, A.; Willems, R.; Troost, E.; Gewillig, M.; Rega, F.; Budts, W. Long-term follow-up of children with heart block born from mothers with systemic lupus erythematosus: A retrospective study from the database pediatric and congenital heart disease in University Hospitals Leuven. Pacing Clin. Electrophysiol. 2016, 39, 935–943. [Google Scholar] [CrossRef]
- Kusumoto, F.H.; Schoenfeld, M.H.; Barrett, C.; Edgerton, J.R.; Ellenbogen, K.A.; Gold, M.R.; Goldschlager, N.F.; Hamilton, R.M.; Joglar, J.A.; Kim, R.J.; et al. 2018 ACC/AHA/HRS Guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2019, 140, e382–e482. [Google Scholar] [CrossRef] [PubMed]
- Practical Medicine, Drug Index, Krakow, Poland. Available online: https://indeks.mp.pl (accessed on 25 April 2024).
- Hondo, H.; Kowase, S.; Shunichi, A.; Osada, J.; Aoki, H.; Yumoto, H. Theophylline to treat prolonged paroxysmal complete atrioventricular block without conduction disorder or structural heart disease after COVID-19 infection: A case report. Heart Rhythm Case Rep. 2022, 8, 229–232. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Resting electrocardiograms at standard paper speed of 25 mm/s and normal calibration of 1 mV = 10 mm. Limb leads I-III, sinus rhythm cycle 840 ms (71 bpm), junctional rhythm cycle 1330 ms (45 bpm).
Figure 1.
Resting electrocardiograms at standard paper speed of 25 mm/s and normal calibration of 1 mV = 10 mm. Limb leads I-III, sinus rhythm cycle 840 ms (71 bpm), junctional rhythm cycle 1330 ms (45 bpm).
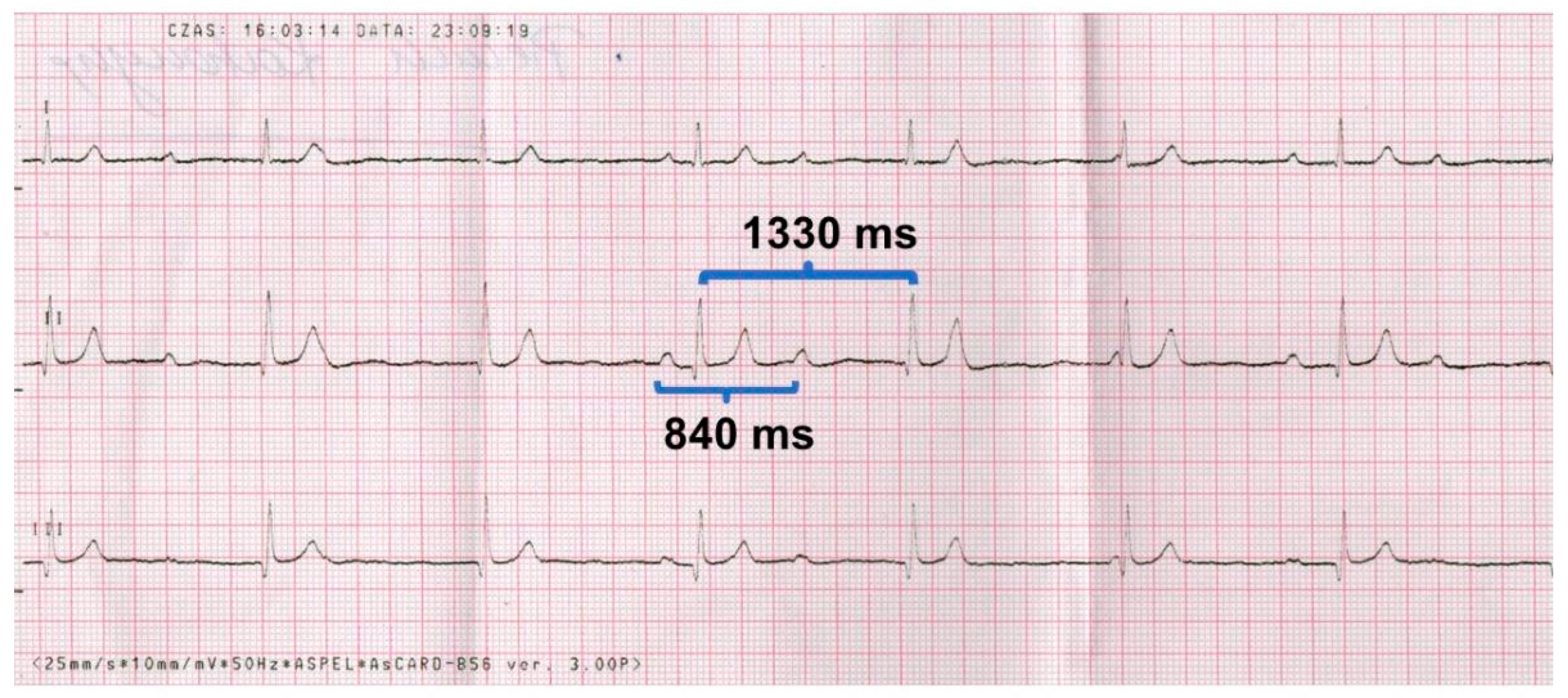
Figure 2.
ECG before exercise test. Sinus rhythm 68/min and AV link rhythm 52/min.
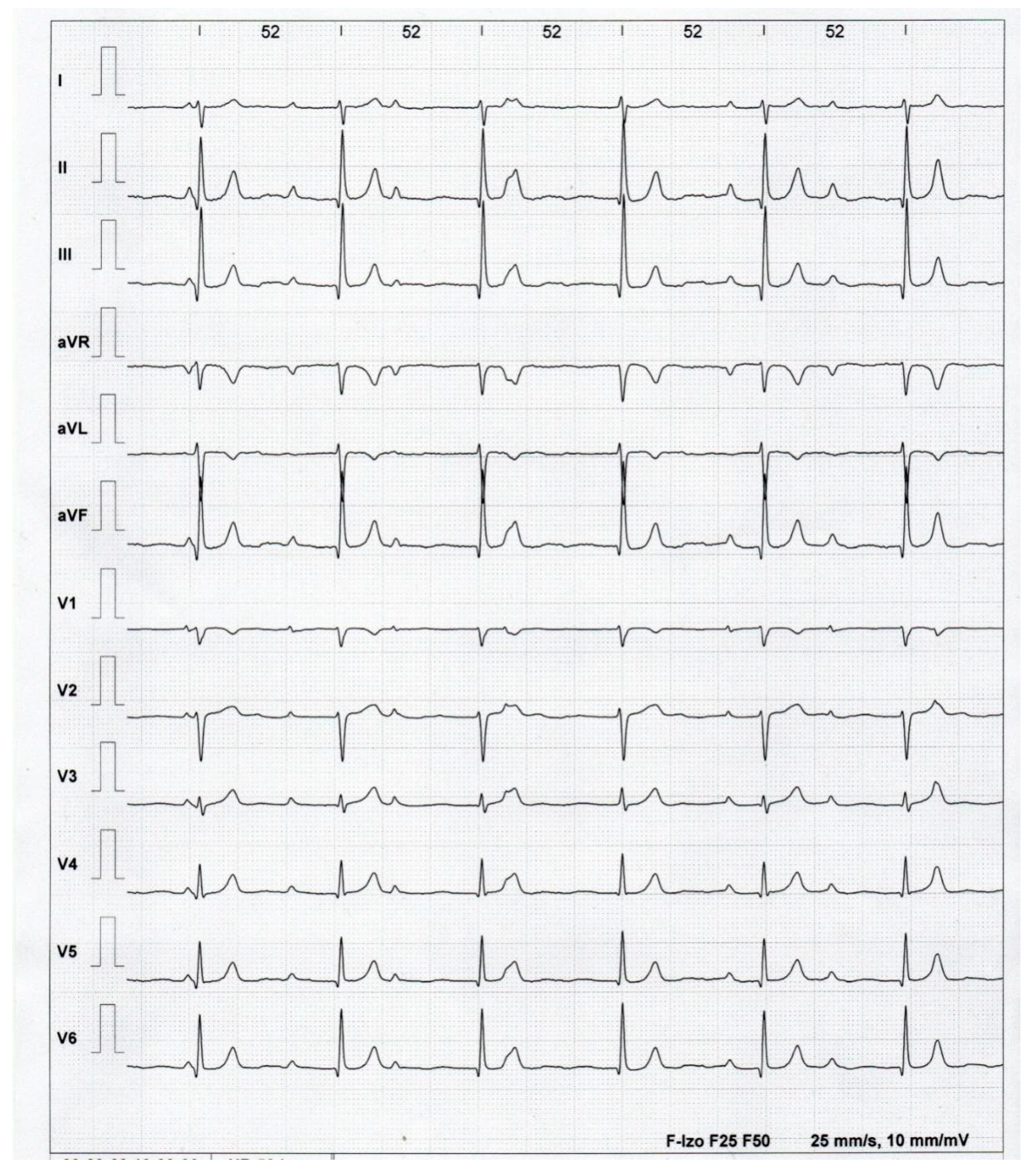
Figure 3.
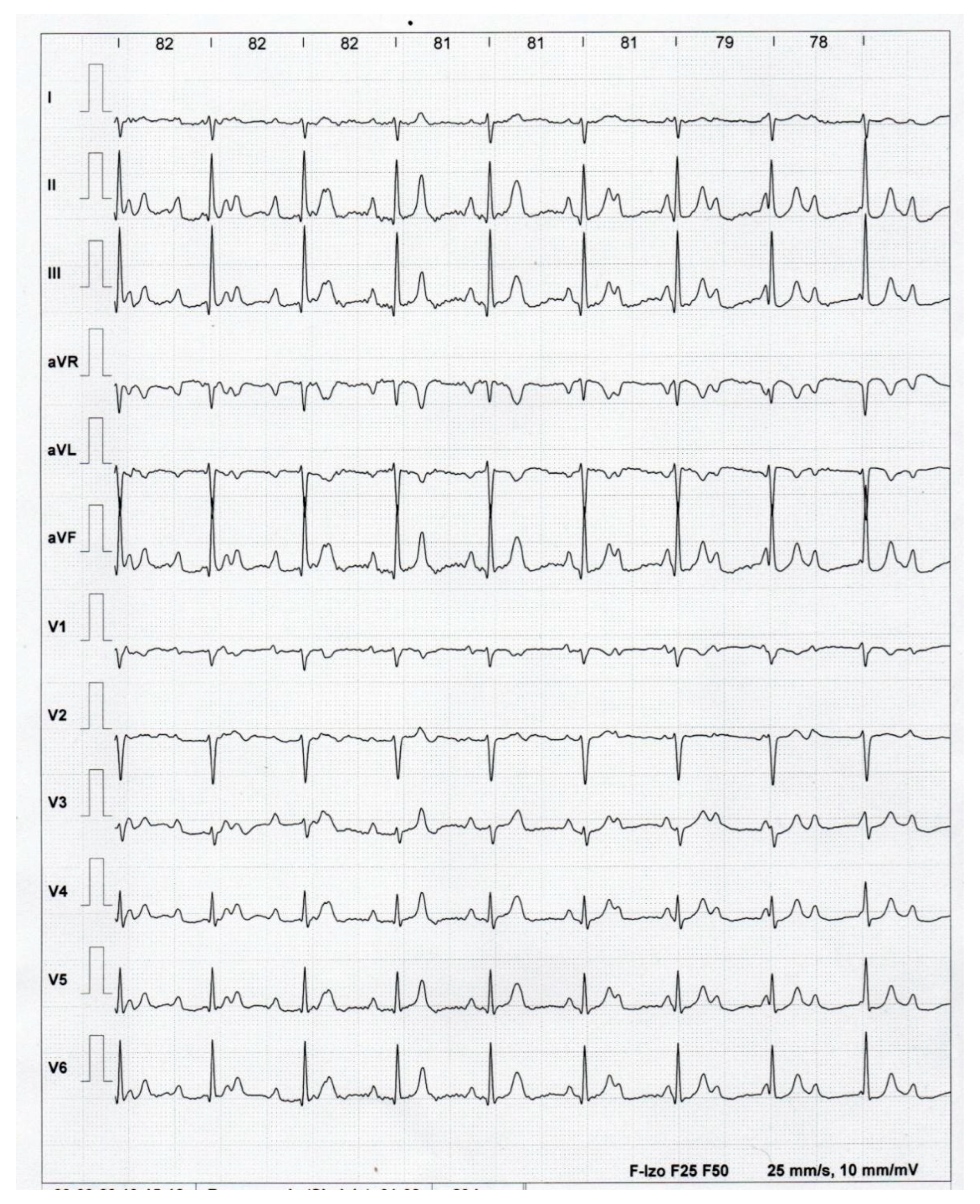
ECG at the top of the exercise test. The sinus rhythm accelerated to 136/min (cycle 440 ms), and the junctional rhythm accelerated to 82 bpm.
Figure 3.
ECG at the top of the exercise test. The sinus rhythm accelerated to 136/min (cycle 440 ms), and the junctional rhythm accelerated to 82 bpm.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



