Submitted:
02 May 2024
Posted:
07 May 2024
You are already at the latest version
Abstract
Background/Objectives: This study aims to investigate the influence of root canal morphology and various treatment variables on the outcomes of root canal treatments (RCT) in mandibular second molars, assessed through cone-beam computed tomography (CBCT) imaging. Methods: A total of 150 CBCT images were examined, comprising 100 cases of persistent endodontic infections and 50 from previously treated root canals with normal apices in mandibular second molars. CBCT was utilized to evaluate root canal configuration, the radiographic quality of coronal restorations and treated canal systems, and the presence of periapical lesions. Statistical analyses were performed to explore correlations between these factors. Results: The presence of a C-shaped root canal configuration did not demonstrate a significant correlation with periapical lesions (p=0.05). Factors influencing endodontic treatment outcomes included the presence of missing canals (p=0.018), underfilling or overfilling (p=0.045), and inadequate coronal restoration (p=0.006). The presence of a missing canal was identified as the variable most significantly associated with periapical lesions (OR=3.103). Leaky canals were more commonly observed in C-shaped root canals (p<0.001). Conclusions: Regardless of the root canal morphology of mandibular second molars, successful RCT depends on thorough disinfection to eliminate any untreated canals, precise three-dimensional filling of the canals at the correct working length, and a securely sealed coronal restoration to prevent leakage.
Keywords:
non-surgical endodontics
; periapical diseases
; cone-beam computed tomography
; treatment outcomes
1. Introduction
Root Canal Treatment (RCT) hinges on achieving complete sterilization and sealing of the canal interior [1]. To achieve this, it's essential to ensure proper shaping, irrigation, and three-dimensional filling of the canals. The success of each RCT step is significantly impacted by the anatomical features of the canal, with complexities like isthmi and fins known to decrease success rates [2,3]. Beyond anatomy, intra- and post-operative factors related to treatment quality are crucial determinants of RCT success [4]. The presence of missing canals, the state of canal obturation, and the quality of coronal restoration have been widely recognized as crucial factors influencing the success or failure of RCT [5,6].
The mandibular second molar is notorious for its anatomical complexity and variability in root canal morphology [7]. Among these variations, the C-shaped canal, where the buccal aspect of the canal systems is fused, is known to have a relatively high occurrence rate [8]. Treating C-shaped canals is difficult due to their complicated anatomical features [9]. The presence of isthmi in C-shaped canals can serve as reservoirs for bacteria and debris, which may not be effectively reached or cleaned using traditional shaping and cleaning techniques [10]. Additionally, sealing the root canal in three dimensions is challenging, making the mandibular second molar one of the most difficult teeth for RCT. Persistent endodontic infection leads to the failure of RCT [11].
Numerous studies have aimed to uncover factors contributing to the failure of RCT by investigating the anatomical features, pre-operative pulpal status, and treatment variables of teeth displaying persistent endodontic infection [12]. These investigations aid in comprehending the complexity of RCT and considering various factors to enhance clinical outcomes. Prior research on C-shaped root canal studies predominantly focused on anatomical features through the analysis of extracted teeth [8,13,14,15]. However, to explore the correlation between post-RCT clinical symptoms and anatomical structure, cone-beam computed tomography (CBCT) emerges as a valuable tool [6]. CBCT allows for evaluating root canal configurations and treatment quality without the need for tooth extraction [16]. The insights gained from CBCT offer clues to pinpoint the underlying causes of patient discomfort.
The aim of this study is to assess the influence of root canal morphology and treatment quality on the outcomes of RCT in mandibular second molars, through a retrospective analysis conducted using CBCT imaging. Additionally, this study examines any potential relationship between C-shaped canals and the quality of RCT.
2. Materials and Methods
2.1. Case Selection
The study was approved by the Institutional Review Board (IRB no. B-2308-849-103) of the Seoul National University Bundang Hospital. The case group for this study comprised 100 patients who visited Department of Conservative Dentistry from July of 2020 to June of 2023 with complaints of consultation for endodontic retreatment in mandibular second molar that showed periapical radiolucency and persistent discomfort. They were diagnosed as either symptomatic apical periodontitis or periapical abscess and have been taken CBCT for further evaluation with their consent.
The control group consisted of 50 patients who visited Department of Oral and Maxillofacial Surgery in a same period. These individuals had undergone CBCT for the extraction of the mandibular third molar and had an adjacent second molar that had previously undergone RCT with currently normal periapical status, presenting no clinical symptoms.
- -
- Inclusion criteria: Endodontically treated mandibular molar with its root growth completed, has to be fully included in CBCT’s imaging range, while its clear and complete images available.
- -
- Exclusion criteria: Presence of periodontitis at least in a moderate stage. Diagnosis of conditions other than pulpal or periapical lesions (such as fibro-osseous lesions, benign neoplasms, oral cancer, etc.). Difficulty in radiographic interpretation due to metal artifacts associated with the tooth.
2.2. CBCT Analysis
CBCT image was taken with Kodak 9500 3D system (Carestream Health, Rochester, NY, USA) at a tube voltage of 80kV, a tube current of 15mA, and an exposure time of 10.8 seconds. The resulting image consisted of axial cross-sectional slices with a thickness of 0.2mm, parallel to the occlusal plane.
Every image of axial, sagittal, and coronal sliced samples of each scan was analyzed by 2 examiners using On Demand3D app (Cybermed, Seoul, Korea). Multiple host and treatment variables were recorded from the patients’ records. According to the study design, the following analysis was conducted (Figure 1).
2.2.1. An Anatomical Factor: Root Canal Morphology Classification
C-shaped canal generally means that a transverse section of root canal is in a shape of letter “C” [8]. Root canal shows various types of shape as it repeats dividing into few branches and getting back through anastomosis, following long axis of root. Usually, C-shaped canal is not completely connected from canal orifice to apical foramen. Therefore in this study, C-shaped canal was defined if a tooth shows forementioned C-shape at least once in entire root canal section when it was observed in axial view of CBCT [9]. The subtypes of C-shaped canals were further classified into C1 to C5 based on the shape observed in the axial view of the middle 1/3 of the root, following the classification proposed by Fan [7] (Figure 2).
2.2.2. Treatment Factors: Intra- and Post-Operative Factors
The following treatment factors were chosen as criteria for assessing the quality of RCT (Table 1). Obturation density, missed canal, obturation level, and iatrogenic problems are intra-operative factors, while coronal restoration is a post-operative factor.
Figure 1.
Study design. The impact of root canal features and the treatment variables on the outcome of root canal treatment was individually investigated. Additionally, the correlation between C-shape presence and the treatment quality was explored.
Figure 1.
Study design. The impact of root canal features and the treatment variables on the outcome of root canal treatment was individually investigated. Additionally, the correlation between C-shape presence and the treatment quality was explored.
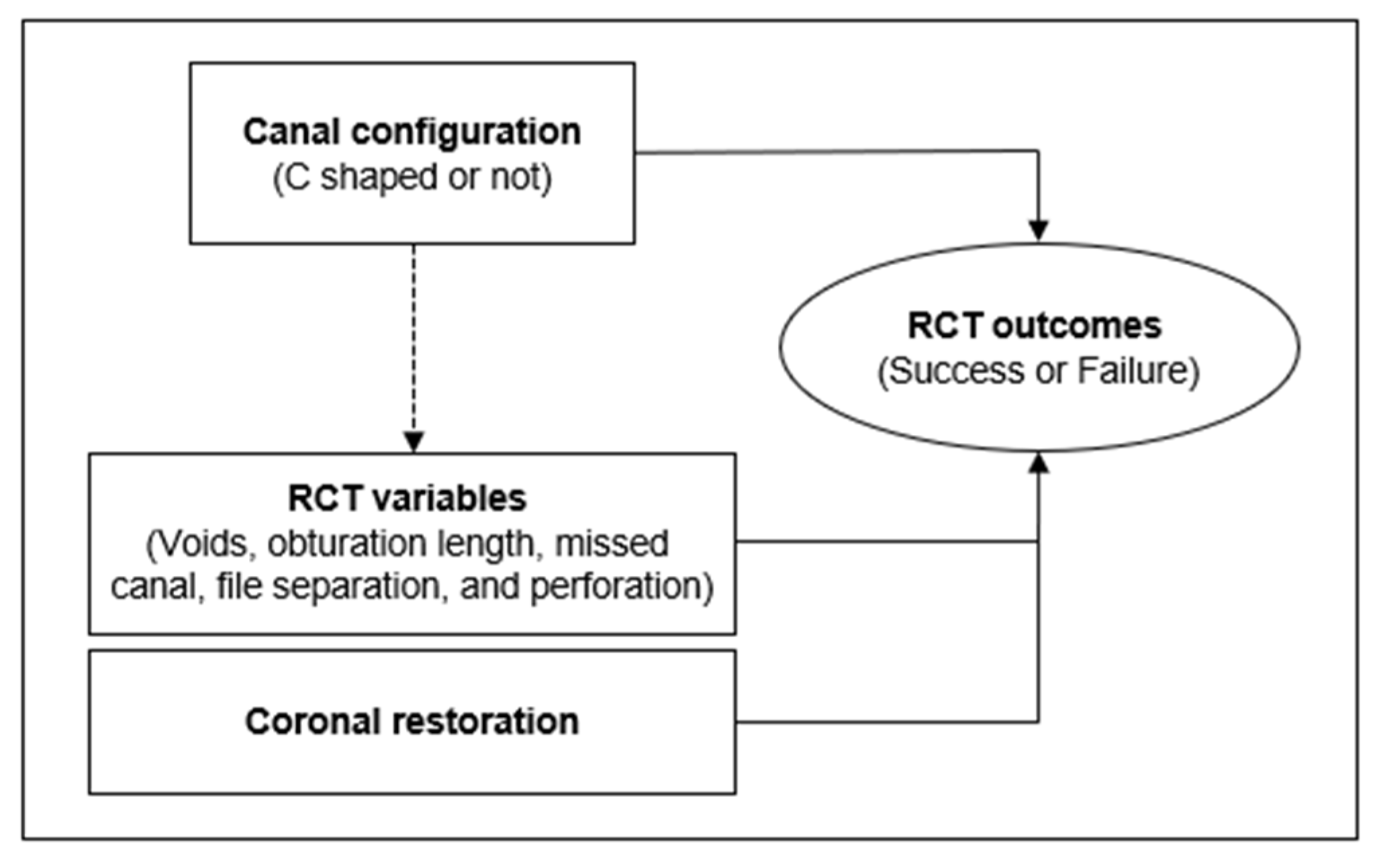
Figure 2.
Classification of C-shaped canal. (a) C1, Uninterrupted ‘C’ with no separation or division. (b) C2, Canal shape resembled a semicolon. (c) C3, Two or three separate canals. (d) C4, Only one round or oval canal. (e) C5, No canal lumen (usually seen near the apex only).
Figure 2.
Classification of C-shaped canal. (a) C1, Uninterrupted ‘C’ with no separation or division. (b) C2, Canal shape resembled a semicolon. (c) C3, Two or three separate canals. (d) C4, Only one round or oval canal. (e) C5, No canal lumen (usually seen near the apex only).
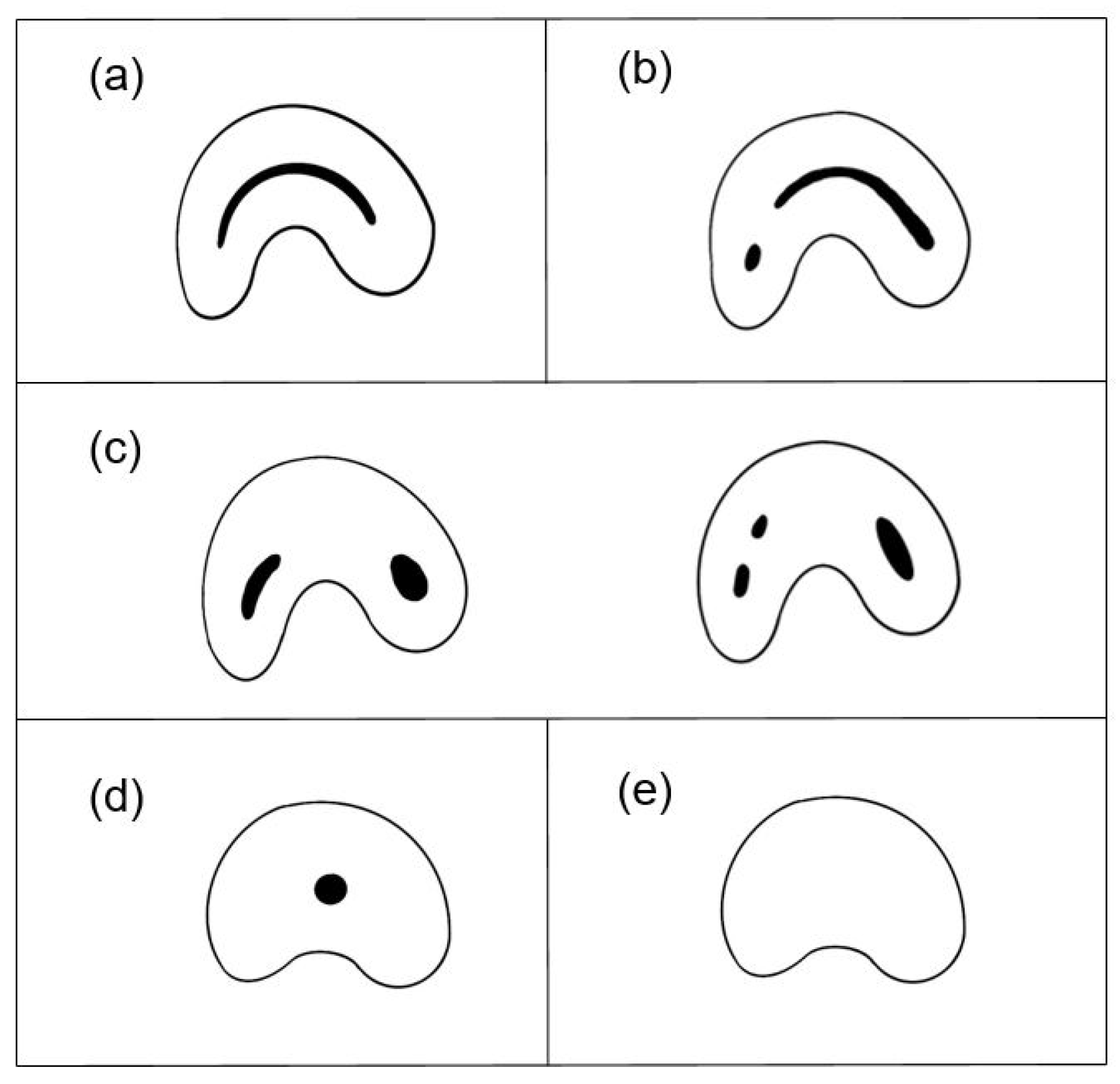
Figure 3.
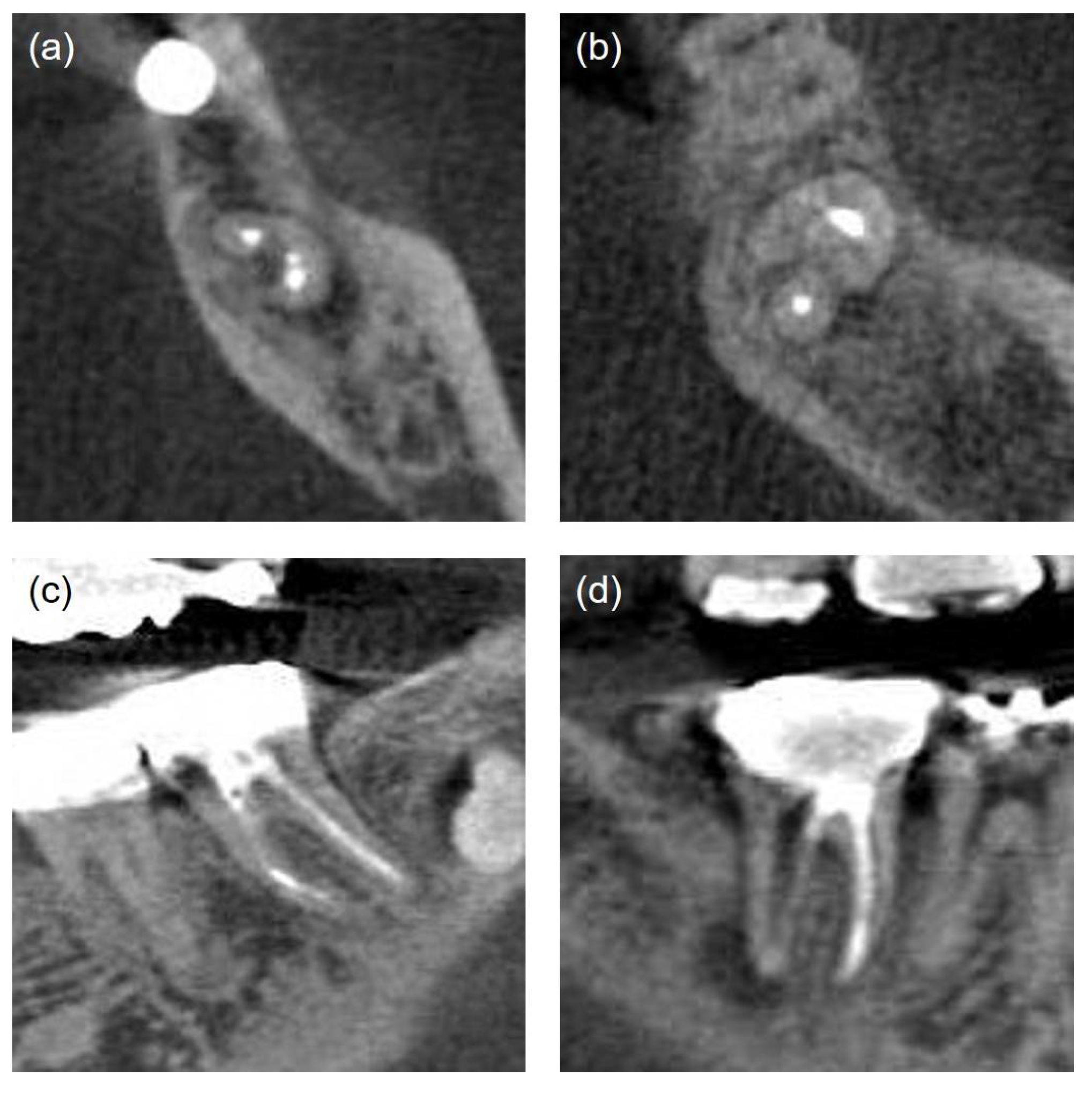
The quality of root canal treatment was evaluated by analyzing CBCT cross-sectional images. (a) The untreated isthmus area of the C-shaped canal in the mandibular right second molar, axial view. (b) The missed mesio-lingual canal in the mandibular right second molar, axial view. (c) Instrument fracture in the mesial root canal of the mandibular left second molar, coronal view. (d) Perforation in the furcation area of the mandibular right second molar, coronal view.
Figure 3.
The quality of root canal treatment was evaluated by analyzing CBCT cross-sectional images. (a) The untreated isthmus area of the C-shaped canal in the mandibular right second molar, axial view. (b) The missed mesio-lingual canal in the mandibular right second molar, axial view. (c) Instrument fracture in the mesial root canal of the mandibular left second molar, coronal view. (d) Perforation in the furcation area of the mandibular right second molar, coronal view.
2.3. Statistical Analysis
Chi-square tests were applied to examine the relationship between the outcome of RCT and the canal shape of the mandibular second molar. Additionally, multiple logistic regression analysis was conducted to assess how anatomical and various treatment factors influenced the failure of root canal treatment. A significance level (p-value) of 0.05 was chosen for all analyses. Statistical analyses were performed using SPSS ver28.0 (SPSS Inc., Illinois, USA).
3. Results
3.1. An Anatomical Factor: The Root Canal Morphology
To assess the anatomical complexity of the root canal, we evaluated whether it exhibited a C-shaped configuration or not, and examined the impact of this configuration on the success rate of root canal treatment. As seen in Table 2, the results from the examination using CBCT revealed that out of the total 150 teeth, 77 (51.3%) had a C-shaped canal configuration. The success rate for C-type canals was 26%, compared to 41.1% for non-C-type canals. The C-shaped canal configuration does not significantly influence the success rate of root canal treatment (p=0.05). Among the subtypes of C-shaped canals, C1 (uninterrupted ‘C’ with no separation or division) was the most prevalent, accounting for 55% of the total, followed by C2 (canal shape resembled a semicolon), which constituted 26% (Figure 4).
3.2. Intra- and Post-Operative Treatment Factors: Missing Canals, Obturation Length, Leaky Canals, Iatrogenic Problems, and Coronal Restoration
We investigated the influence of missing canals, obturation length, leaky canals, iatrogenic events, and coronal leakage on the failure of root canal treatment (Table 3). In cases of missing or untreated canals, failure rate was 82.6%, whereas it was 59.6% when all canals were treated. Analysis on obturation length correlation with success rate showed lower success rate of 14.3% with inappropriate length, compared to 41.1% with appropriate length. Presence of voids in the root canal on CBCT imaging, resulting in leaky canals, led to a failure rate of 77.5%, compared to 54.3% with adequately filled canal. Iatrogenic problems like file separation or perforation were detected in 9 teeth. Coronal restoration status was analyzed in 146 teeth, excluding those with previously removed restorations. Failure rate of RCT was higher at 78.9% when coronal restoration was inappropriate, compared to 53.3% with well-done restoration. As seen in Table 4, according to logistic regression analysis, missing canal, improper obturation length, and coronal leakage were significant variables influencing the success or failure of root canal treatment. If a missing canal exists, the likelihood of endodontic failure is 3.103 times higher, improper obturation length increases the failure rate by 2.909 times, and the presence of coronal leakage raises it by 3.057 times. According to these findings, the presence of a missing canal emerges as the most significant factor influencing the failure of RCT.
3.3. The Correlation between an Anatomical Factor and Treatment Factors
To investigate the influence of anatomical canal morphology on the quality of en-dodontic treatment, the treatment factors according to canal configurations were compared. The incidence of inhomogenous obturation density was significantly higher in C-type canals compared to non-C-type canals (P<0.001). There was no significant difference in the prevalence of missing canals, inadequate obturation length, or iatrogenic problems between C-type and non-C-type canals (Table 5).
4. Discussion
When identifying the causes of RCT failure, it is essential to consider both anatomical factors and treatment factors together. The root canal complexity increases the difficulty of RCT and makes proper canal cleaning and filling more challenging. As a result, remaining bacteria and their biofilms can lead to the failure of RCT and subsequently progress to apical periodontitis or apical abscess [18,19]. The mandibular second molar is known to have the most complicated canal system of all teeth [20]. Therefore, this study aimed to investigate the impact of anatomical and treatment factors on RCT outcomes of the mandibular second molars.
Whether the root canal is a "C shape" or not is not a significant factor influencing the success or failure of RCT. According to another study comparing healing outcomes of C-shaped mandibular second molars, the success rate for teeth with a "C shape" was 70.9%, while the success rate for teeth without a "C shape" was 66.6%, with no significant difference observed [21]. There are studies suggesting a lower success rate of RCT in mandibular molars [22]. However, there are also studies indicating no significant difference in success rates among teeth. Another study concluded that the success rate of treatment was not adversely affected by tooth type or anatomical complexity [4]. It is true that the complexity of root canal morphology can impact the complete disinfection of the root canal. However, the C shape form is a part of root canal complexity. In addition to the C shape, other factors determining complexity include lateral canals, apical ramifications, isthmuses, curvatures, and so on. It is believed that these factors collectively influence the shaping and obturation of the root canal [23,24,25,26].
Other than root canal anatomy, when looking at the effect of treatment quality on outcomes of RCT, obturation level and the presence of missing canal, and coronal leakage act as significant factors. Working length and obturation level are known to significantly affect the result of RCT. It is reported that if canal fillings are 2mm short from root apex then the success rate of RCT drops down to 68~77%, and if it is over-filled through the apex then the RCT shows about 75% of success rate [1,27]. This study also shows significant decrease in success rate of RCT as root canal gets over-filled or under-filled. In addition, the presence of missing canals emerged as a significant factor contributing to the failure of RCT in this study as well. Here, in cases where a canal is missed, the failure rate of RCT was 82.6%. This aligns with the findings of previous studies examining the impact of missed canals on periapical lesions [6]. From aetiologic point of view, it seems reasonable that infected and untreated root canal could possibly be a trigger of apical lesion. Many case studies claim that missed canal has a close relationship with apical lesion, with odds ratios ranging from about 4.4 to 6.25 [6,16,28].
On the other hand, obturation density and iatrogenic problems were not identified as significant factors influencing the outcome of RCT in this study. There are conflicting findings about the effect of intracanal instrument fracture on the prognosis of RCT [29,30] . In this regard, McGuigan[31] claims that remaining of fractured instrument depends on presence of apical disease before RCT. However, since there is no available information on the apical status before RCT in this study, it becomes challenging to analyze the relationship between instrument fracture and the success or failure of RCT. In addition, the low incidence of iatrogenic problems (such as file separation and perforation) in this study poses a challenge when attempting to accurately assess their low correlation with the success rate of root canal treatment. In terms of obturation density, the quality of the coronal restoration played a more significant role in determining endodontic success than the quality of the root filling [32,33]. These results are consistent with our study findings, which suggest that coronal leakage significantly influences the failure of root canal treatment.
When examining differences in treatment factors based on canal configuration, it appears that a C-shaped morphology may significantly affect the attainment of inhomogeneous obturation density. C-shaped canals are characterized by canals interconnected by fins and isthmuses, making it challenging to achieve three-dimensional sealing of the root canal system with conventional endodontic materials. Therefore, in cases of C-shaped canals, it is necessary to consider various techniques for achieving three-dimensional canal filling after adequate debridement and irrigation have been completed [34].
In this study, 51.3% of the subjects exhibited C-shaped canal in the mandibular second molar. Previous studies have reported that the occurrence of C-shaped canal has a wide range of distribution of 3 to 39.2% worldwide and is significantly more common in Asian populations. In South Korea, especially, C-shaped canal occurrence rate in mandibular second molar is reported to be around 30 to 40% [35]. The higher prevalence of C-shaped root canals, compared to other studies, is presumed to be attributed to the patient groups composed of individuals referred from local dental clinics due to root canal treatment failure. Among subtypes of C shaped canal, C1, which refers to uninterrupted C-shaped root canal, was the most common, aligning with findings from previous research [36,37]. Each canal subtypes made no significant difference in occurrence of persistent endodontic infection.
This study analyzed CBCT images of root canal-treated teeth. After the introduction of computed tomography (CT) into endodontics by Tachibana and Matsumoto in 1990, CBCT, capable of capturing images with low radiation, has been used to assess the anatomical form and pathological elements of root canals [38]. CBCT enables three-dimensional cross-sectional evaluation without the need for tooth extraction [39]. Furthermore, according to a study comparing the accuracy of various radiographic methods, CBCT demonstrated the highest accuracy in determining root canal configuration. In terms of accuracy, it is comparable to the modified canal staining and clearing technique performed on extracted teeth [40]. Consequently, in endodontic practice, it serves as a valuable diagnostic aid for formulating treatment plans or assessing treatment outcomes, especially when significant anatomical deviations in root canal anatomy are suspected in 2D images [41]. However, it's not feasible to perform CBCT for every endodontic treatment. In cases where patients continue to complain of discomfort after RCT or when anomalies or pathological issues within the root canal are suspected based on 2D radiographs, CBCT imaging should be considered.
Studies report that the success rate of primary root canal treatment ranges from 92% to 96% when there is no presence of apical periodontitis before the procedure. However, if apical periodontitis is present, the success rate drops to 62% to 83% [42]. Hence, it is hard to separate the success or failure of RCT from the apical status before the treatment. However, this study focuses on teeth for which the RCT has already been completed. There is a limitation as the preoperative condition of the pulp and apex of the targeted teeth was not included.
In conclusion, based on the evaluation of the impact of root canal morphology and treatment quality on persistent endodontic infection using CBCT imaging, successful RCT for mandibular second molars necessitates thorough disinfection to address any untreated canals, precise three-dimensional canal obturation at the correct working length, and a securely sealed coronal restoration to prevent leakage, irrespective of the root canal morphology.
Author Contributions
Conceptualization, D.P. and J.Y.; Methodology, D.P.; Data curation, D.P.; Investigation, D.P.; Formal analysis, D.P. and J.Y.; Writing—original draft preparation, D.P.; writing—review and editing, W.S. and J.Y.; visualization, W.S.; supervision, J.Y.; project administration, J.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Seoul National University Bundang Hospital (IRB no. B-2308-849-103). Approval date: 08/17/2023.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting reported results are not provided due to ethical restrictions, but can be provided upon request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Chugal, N.M.; Clive, J.M.; Spangberg, L.S. Endodontic infection: some biologic and treatment factors associated with outcome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003, 96, 81-90. [CrossRef]
- Vertucci, F.J. Root canal morphology and its relationship to endodontic procedures. Endodontic Topics 2005, 10, 3-29. [CrossRef]
- Lloyd, A.; Uhles, J.P.; Clement, D.J.; Garcia-Godoy, F. Elimination of intracanal tissue and debris through a novel laser-activated system assessed using high-resolution micro-computed tomography: a pilot study. J Endod 2014, 40, 584-587. [CrossRef]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: systematic review of the literature -- Part 2. Influence of clinical factors. Int Endod J 2008, 41, 6-31. [CrossRef]
- Tronstad, L.; Asbjornsen, K.; Doving, L.; Pedersen, I.; Eriksen, H.M. Influence of coronal restorations on the periapical health of endodontically treated teeth. Endod Dent Traumatol 2000, 16, 218-221. [CrossRef]
- Baruwa, A.O.; Martins, J.N.R.; Meirinhos, J.; Pereira, B.; Gouveia, J.; Quaresma, S.A.; Monroe, A.; Ginjeira, A. The Influence of Missed Canals on the Prevalence of Periapical Lesions in Endodontically Treated Teeth: A Cross-sectional Study. J Endod 2020, 46, 34-39 e31. [CrossRef]
- Fan, B.; Cheung, G.S.; Fan, M.; Gutmann, J.L.; Bian, Z. C-shaped canal system in mandibular second molars: Part I--Anatomical features. J Endod 2004, 30, 899-903. [CrossRef]
- Melton, D.C.; Krell, K.V.; Fuller, M.W. Anatomical and histological features of C-shaped canals in mandibular second molars. J Endod 1991, 17, 384-388. [CrossRef]
- Kato, A.; Ziegler, A.; Higuchi, N.; Nakata, K.; Nakamura, H.; Ohno, N. Aetiology, incidence and morphology of the C-shaped root canal system and its impact on clinical endodontics. Int Endod J 2014, 47, 1012-1033. [CrossRef]
- Grocholewicz, K.; Lipski, M.; Weyna, E. Endodontic and prosthetic treatment of teeth with C-shaped root canals. Ann Acad Med Stetin 2009, 55, 55-59.
- Nair, P.N. On the causes of persistent apical periodontitis: a review. Int Endod J 2006, 39, 249-281. [CrossRef]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: systematic review of the literature - part 1. Effects of study characteristics on probability of success. Int Endod J 2007, 40, 921-939. [CrossRef]
- Kotoku, K. [Morphological studies on the roots of Japanese mandibular second molars]. Shikwa Gakuho 1985, 85, 43-64.
- Carlsen, O. Root complex and root canal system: a correlation analysis using one-rooted mandibular second molars. Scand J Dent Res 1990, 98, 273-285. [CrossRef]
- Fan, W.; Fan, B.; Gutmann, J.L.; Cheung, G.S. Identification of C-shaped canal in mandibular second molars. Part I: radiographic and anatomical features revealed by intraradicular contrast medium. J Endod 2007, 33, 806-810. [CrossRef]
- Karabucak, B.; Bunes, A.; Chehoud, C.; Kohli, M.R.; Setzer, F. Prevalence of Apical Periodontitis in Endodontically Treated Premolars and Molars with Untreated Canal: A Cone-beam Computed Tomography Study. J Endod 2016, 42, 538-541. [CrossRef]
- Song, M.; Park, M.; Lee, C.Y.; Kim, E. Periapical status related to the quality of coronal restorations and root fillings in a Korean population. J Endod 2014, 40, 182-186. [CrossRef]
- Siqueira Junior, J.F.; Rocas, I.D.N.; Marceliano-Alves, M.F.; Perez, A.R.; Ricucci, D. Unprepared root canal surface areas: causes, clinical implications, and therapeutic strategies. Braz Oral Res 2018, 32, e65. [CrossRef]
- Jara, C.M.; Hartmann, R.C.; Bottcher, D.E.; Souza, T.S.; Gomes, M.S.; Figueiredo, J.A.P. Influence of apical enlargement on the repair of apical periodontitis in rats. Int Endod J 2018, 51, 1261-1270. [CrossRef]
- Maggiore, C.; Gallottini, L.; Resi, J.P. Mandibular first and second molar. The variability of roots and root canal system. Minerva Stomatol 1998, 47, 409-416.
- Ahn, H.R.; Moon, Y.M.; Hong, S.O.; Seo, M.S. Healing outcomes of root canal treatment for C-shaped mandibular second molars: a retrospective analysis. Restor Dent Endod 2016, 41, 262-270. [CrossRef]
- Barbakow, F.H.; Cleaton-Jones, P.; Friedman, D. An evaluation of 566 cases of root canal therapy in general dental practice. 2. Postoperative observations. J Endod 1980, 6, 485-489. [CrossRef]
- Siqueira, J.F., Jr.; Rocas, I.N.; Lopes, H.P. Patterns of microbial colonization in primary root canal infections. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002, 93, 174-178. [CrossRef]
- Ricucci, D.; Siqueira, J.F., Jr. Biofilms and apical periodontitis: study of prevalence and association with clinical and histopathologic findings. J Endod 2010, 36, 1277-1288. [CrossRef]
- Ricucci, D.; Siqueira, J.F., Jr.; Bate, A.L.; Pitt Ford, T.R. Histologic investigation of root canal-treated teeth with apical periodontitis: a retrospective study from twenty-four patients. J Endod 2009, 35, 493-502. [CrossRef]
- Versiani, M.A.; Martins, J.; Ordinola-Zapata, R. Anatomical complexities affecting root canal preparation: a narrative review. Aust Dent J 2023, 68 Suppl 1, S5-S23. [CrossRef]
- Lin, L.M.; Skribner, J.E.; Gaengler, P. Factors associated with endodontic treatment failures. J Endod 1992, 18, 625-627. [CrossRef]
- Costa, F.; Pacheco-Yanes, J.; Siqueira, J.F., Jr.; Oliveira, A.C.S.; Gazzaneo, I.; Amorim, C.A.; Santos, P.H.B.; Alves, F.R.F. Association between missed canals and apical periodontitis. Int Endod J 2019, 52, 400-406. [CrossRef]
- Spili, P.; Parashos, P.; Messer, H.H. The impact of instrument fracture on outcome of endodontic treatment. J Endod 2005, 31, 845-850. [CrossRef]
- Crump, M.C.; Natkin, E. Relationship of broken root canal instruments to endodontic case prognosis: a clinical investigation. J Am Dent Assoc 1970, 80, 1341-1347. [CrossRef]
- McGuigan, M.B.; Louca, C.; Duncan, H.F. The impact of fractured endodontic instruments on treatment outcome. Br Dent J 2013, 214, 285-289. [CrossRef]
- Ray, H.A.; Trope, M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J 1995, 28, 12-18. [CrossRef]
- Jang, Y.E.; Kim, Y.; Kim, S.Y.; Kim, B.S. Predicting early endodontic treatment failure following primary root canal treatment. BMC Oral Health 2024, 24, 327. [CrossRef]
- Walid, N. The use of two pluggers for the obturation of an uncommon C-shaped canal. J Endod 2000, 26, 422-424. [CrossRef]
- Jin, G.C.; Lee, S.J.; Roh, B.D. Anatomical study of C-shaped canals in mandibular second molars by analysis of computed tomography. J Endod 2006, 32, 10-13. [CrossRef]
- Jafarzadeh, H.; Wu, Y.N. The C-shaped root canal configuration: a review. J Endod 2007, 33, 517-523. [CrossRef]
- Fernandes, M.; de Ataide, I.; Wagle, R. C-shaped root canal configuration: A review of literature. J Conserv Dent 2014, 17, 312-319. [CrossRef]
- Patel, S.; Durack, C.; Abella, F.; Shemesh, H.; Roig, M.; Lemberg, K. Cone beam computed tomography in Endodontics - a review. Int Endod J 2015, 48, 3-15. [CrossRef]
- Kim, Y.; Lee, S.J.; Woo, J. Morphology of maxillary first and second molars analyzed by cone-beam computed tomography in a korean population: variations in the number of roots and canals and the incidence of fusion. J Endod 2012, 38, 1063-1068. [CrossRef]
- Neelakantan, P.; Subbarao, C.; Subbarao, C.V. Comparative evaluation of modified canal staining and clearing technique, cone-beam computed tomography, peripheral quantitative computed tomography, spiral computed tomography, and plain and contrast medium-enhanced digital radiography in studying root canal morphology. J Endod 2010, 36, 1547-1551. [CrossRef]
- Chan, F.; Brown, L.F.; Parashos, P. CBCT in contemporary endodontics. Aust Dent J 2023, 68 Suppl 1, S39-S55. [CrossRef]
- de Chevigny, C.; Dao, T.T.; Basrani, B.R.; Marquis, V.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment outcome in endodontics: the Toronto study--phase 4: initial treatment. J Endod 2008, 34, 258-263. [CrossRef]
Figure 4.
The subtype distribution of C-shaped canal.
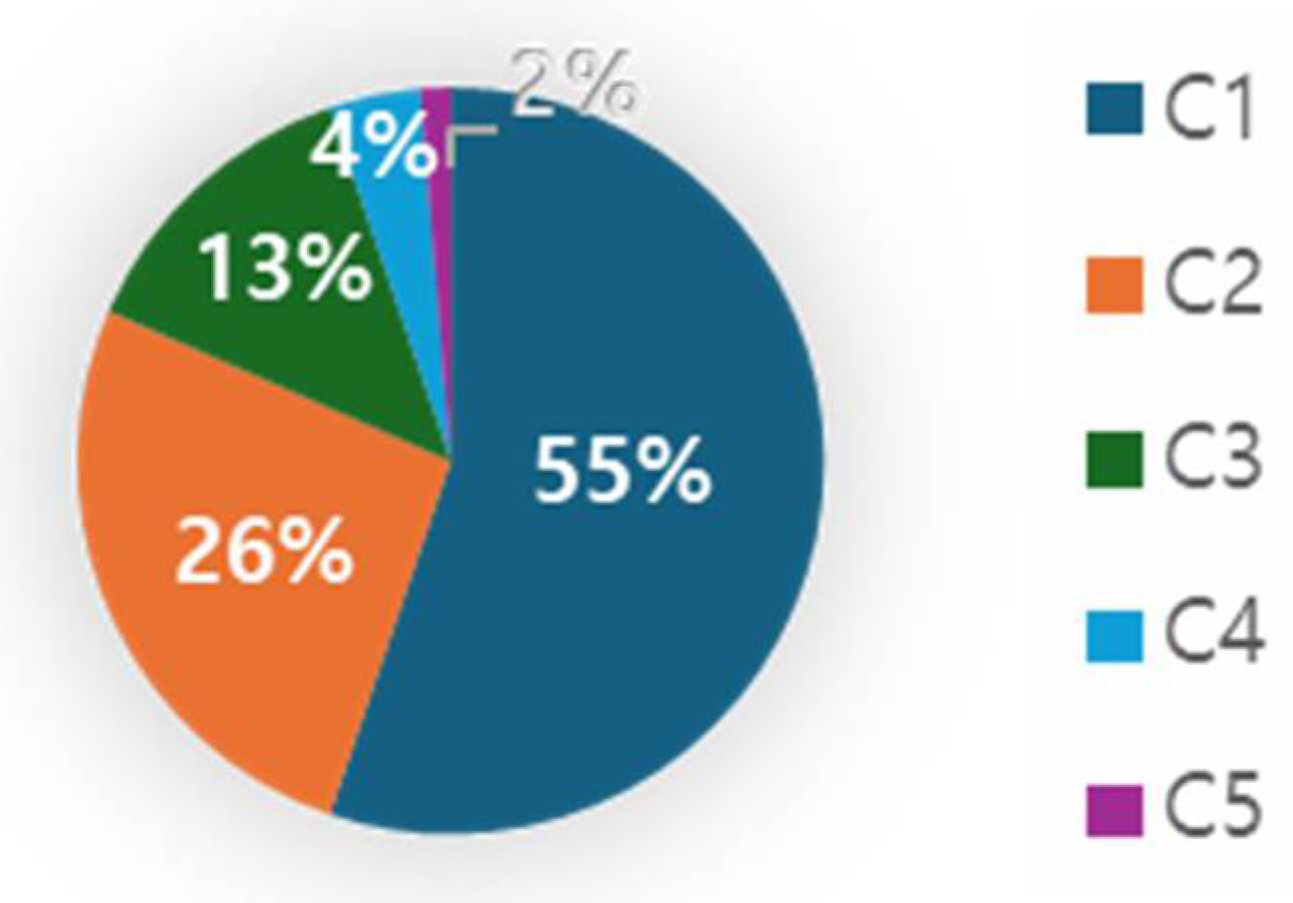

Table 1.
Treatment variable examined through CBCT imaging.
| factors | description | |
| Obturation density [1] | Good | Homogeneous radiopaque material and no visible space. No more than 2 small voids (<1mm) |
| Poor | Non-uniform radiodensity, with the canal space visible laterally and apically. Isthmus area that had not been treated (Figure 3-a) | |
| Missed canal [17] |
Unfilled canals appearing from cemento-enamel junction to apex including canals splitting from a main canal at coronal, mid, or apical third (Figure 3-b) | |
| Obturation level [1] | Obturation level of a filling material was measured in millimeters relative to the radiographic apex | |
| Normal | Fillings within 2mm short of the radiographic apex | |
| improper | Fillings more than 2mm short of the radiographic apex / Excess root filling, Sealer extrusion | |
| Iatrogenic problem | File separation, Perforation (present/absent) (Figure 3-c, d). | |
| Coronal restoration [17] | Adequate | Any permanent restoration that appeared intact radiographically and had no comment on the clinical examination record |
| Inadequate | Any permanent restoration with detectable radiographic sings of overhangs, open margins, or recurrent caries or comments such as “ill-fitting margin” or “secondary dental caries” on the clinical examination record. | |
Table 2.
Endodontic treatment outcome relative to anatomical factor.
| C-shape N=77 (100%) |
Non C-shape N=73 (100%) |
Total N=150 |
|
|---|---|---|---|
| Success | 20 (26%) | 30 (41.1%) | 50 |
| Failure | 57 (74%) | 43 (58.9%) | 100 |
| χ2(p) | 3.856 (p=0.05) | ||
∗ Significant P value at 0.05 level.
Table 3.
Endodontic treatment outcome according to treatment factors.
| Treatment factors | N | Endodontic outcome | |
| Success (N=50) |
Failure (N=100) |
||
| Missing canal | |||
| Present | 46 | 8 (17.4%) | 38 (82.6%) |
| Absent | 104 | 42 (40.4%) | 62 (59.6%) |
| Obturation length | |||
| Adequate | 107 | 44 (41.1%) | 63 (58.9%) |
| Inadequate | 42 | 6 (14.3%) | 36 (85.7%) |
| Obturation density | |||
| Poor | 80 | 18 (22.5%) | 62 (77.5%) |
| Good | 70 | 32 (45.7%) | 38 (54.3%) |
| Iatrogenic problem | |||
| Present | 9 | 3 (33.3%) | 6 (66.7%) |
| Absent | 141 | 47 (33.3%) | 94 (66.7%) |
| Coronal restoration | |||
| Adequate | 75 | 35 (46.7%) | 40 (53.3%) |
| Inadequate | 71 | 15 (21.1%) | 56 (78.9%) |
Table 4.
Endodontic treatment outcome according to anatomical and treatment factors. Logistic regression analysis.
Table 4.
Endodontic treatment outcome according to anatomical and treatment factors. Logistic regression analysis.
| Endodontic Failure | |||||
| B | S.E. | Wald | p | Exp (B) | |
| C-configuration | 0.115 | 0.504 | 0.053 | 0.819 | 1.122 |
| Missing canal | 1.132 | 0.478 | 5.606 | 0.018* | 3.103 |
| Obturation length | 1.068 | 0.533 | 4.019 | 0.045* | 2.909 |
| Obturation density | 0.572 | 0.508 | 1.267 | 0.260 | 1.772 |
| Iatrogenic events | -0.110 | 0.819 | 0.018 | 0.893 | 0.896 |
| Coronal leakage | 1.117 | 0.405 | 7.619 | 0.006* | 3.057 |
B, coefficient for the constant; S.E., standard error; Exp (B), the exponentiation of the B constant, which is an odds ratio. *Indicates significant differences (p < 0.05).
Table 5.
Treatment quality according to canal configuration.
| C-shape | Non C-shape | X2 | p value | |
| Missing canal (N=46) | 25 (54.3%) | 21 (45.7%) | 0.241 | 0.623 |
| Inadequate obturation length (N=42) |
26 (61.9%) | 16 (38.1%) | 2.450 | 0.118 |
| Poor obturation density (N=80) |
65 (81.3%) | 15 (18.7%) | 61.416 | <0.001* |
| Iatrogenic problem (N=9) |
3 (33.3%) | 6 (66.7%) | 0.318 † |
∗ Significant p value at 0.05 level. †Fisher’s exact test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



