
Submitted:
07 May 2024
Posted:
07 May 2024
You are already at the latest version
Abstract
3D-printed models with high anatomic fidelity are an increasingly viable tool in simulation-based medical education. One advantage of 3D models is they provide enhanced tactile and spatial understanding of complex anatomy to develop technical skills used in minimally invasive procedures. We propose that 3D anatomical models can improve the development of Interventional Radiology vascular access skills – first described in the 1950s as the Seldinger Technique – for pre-clerkship medical students. Early adoption of 3D-printed technology in pre-clinical medical education can lead to improved student engagement and satisfaction when learning procedural techniques. This study involved creating a 3D model of the upper extremity vasculature from an anonymized CT angiogram, using it as a medical education tool for 31 pre-clinical medical students practicing the Seldinger Technique on a prefabricated venipuncture arm, and assessing student satisfaction with this form of learning. Overall, attendees responded positively to the incorporation of the 3D model in medical education to improve their anatomic understanding and application to the Seldinger Technique. These results indicate that the use of 3D models in simulation-based medical education can provide benefits to acquiring technical skills and the potential to decrease training costs without harming a patient.
Keywords:
3D printing
; simulation-based medical education
; interventional radiology
; vasculature
; minimally invasive procedures
; undergraduate medical education
; medical education
1. Introduction
The increased access to 3D printers, decreased material costs, and prevalence of open-source computer-assisted design programs such as 3D-Slicer have marked an explosion of 3D model applications in the medical field [1]. High fidelity anatomic models are increasingly being used in pre-surgical planning, patient education, and simulation-based medical education [2].
In medical education, studies have suggested prior didactic education followed by handling of a tangible model enhances understanding of the complex relationships between adjacent anatomic structures [2]. Unique 3D models of a patient’s cardiovascular system have been utilized to improve surgeons’ technical skills, assist with planning difficult procedures (e.g., selecting appropriate instruments for complex cases) and handling intraoperative troubleshooting [3,4,5]. Further benefits include improvements in intraoperative time, clinical outcomes, and reduction in post operative complications through preprocedural planning of difficult cases [6].
One of the first studies evaluating the efficacy of incorporating a 3D model as a patient education tool involved a population of patients recently diagnosed with renal cancer. 3D models of the kidney and associated tumor were printed for each patient using their prior imaging studies. They were used during preprocedural consultation and shown to enhance patient understanding of renal anatomy and physiology and the planned surgical procedure after a post-consultation survey [7].
In medical education, 3D models can enhance learning by emphasizing visual, spatial, and tactile information. Unlike formalin preserved cadavers, 3D-printed models are reusable, less expensive, and less toxic [2,3,8]. Moreover, they have been used in the development of technical skills in simulation-based medical education particularly in the field of Interventional Radiology for training vascular access techniques [9].
This brief report describes and discusses a small-scale pilot study at a single institution of an educational seminar for preclerkship medical students that involved the development of a 3D model of the upper extremity vasculature to be used as a tool in learning the Seldinger Technique. The design and implementation of the seminar followed a 2019 technical report by Goudie et. al, and extends that work by including a hands-on application of the learned material in the educational seminar on a venipuncture arm [9].
The goals for this simulation-based educational seminar were to improve learner comprehension of upper vasculature anatomy and the Seldinger Technique; stimulate learner desire for the inclusion of 3D-printed models in future simulation-based educational events; and to test the feasibility of hosting a small-scale, hands-on educational seminar that utilized custom 3D-printed anatomical models for preclerkship medical students.
2. Materials and Methods
2.1. 3D Model Development
3D-Slicer is free, open-source software used for computer aided design with Digital Imaging and Communications in Medicine (D.I.C.O.M.) data (https://www.slicer.org). This software provides a suite of tools for post-processing CT imaging studies and several anonymized imaging studies that can be used to design a model. One such provided study, a CT angiogram of the chest was used to create a 3D model of the right upper extremity vasculature. In an angiogram, contrast can be injected into the upper extremity venous system and the imaging is performed as it enters vascular space. Consequently, the radio opaque contrast provided the visualization required to delineate surrounding anatomic structures as a function of its Hounsfield units. The region of interest included the basilic and cephalic veins, sites commonly targeted for obtaining peripheral access using the Seldinger technique. The vascular bed was manually segmented to isolate it from the surrounding anatomy, hollowed, and perforating vessels removed (see Figure 1). Finally, the post processed design was converted to stereolithography format (.STL) and printed using a MakerBot printing platform using polylactic acid (P.L.A.) filament (see Figure 2).
The final model is 16cm in length, 5cm in width and rigid, owing to the P.L.A. filament consistency. Unfortunately, the canalization of the upper extremity vascular bed did not translate to the printing process because the model had to be resized to fit the printing platform. However, the model functioned as a visual and tactile educational tool prior to performing the Seldinger Technique on the prefabricated venipuncture arms.
2.2. Accompanying Educational Material
A 3D model of a vascular bed was used as an educational tool prior simulating the Seldinger Technique on VEVOR Intravenous Phlebotomy Practice arms using a Terumo Pinnacle® Precision Access System micropuncture kit (see Figure 3). This approach was hypothesized to provide a better understanding of the region of interest prior to performing the procedure. Tactile and visual components of 3D-printed models aid procedural training by reinforcing a mental representation of the target vasculature prior to performing the procedure. In contrast to laparoscopic and open surgery, common interventional radiology procedures are performed using tactile feedback and fluoroscopy thus limiting the resolution of the area of interest. The benefit of the addition of the venipuncture arm is a more realistic simulation of cannulating a vessel using a micropuncture kit. These venipuncture arms have internal rubber tubing simulating a vascular system originating at elbow and extending distally to the wrist. Further, red colored dye can be pressurized within the internal tubing to provide visual and tactile feedback to the user regarding successful access of the tubing with the introducer needle (see Figure 4).
The Terumo Pinnacle® Precision Access System, a stand-alone, sterile micropuncture kit, was used for intravenous access. It contains a 21-gauge beveled introducer needle, 0.035 cm nitinol guidewire, dilator, and two-way catheter used for establishing peripheral access.
2.3. Session Participants and Post-Session Survey
Institutional Review Board of Quinnipiac University for studies involving humans’ protocol #10623 was obtained on October 17, 2023. Interest in the event was generated through the creation of an electronic flyer which was advertised through the office of student affairs. Attendance was offered at one of two back-to-back, identical seminar sessions. Pre-clerkship medical students were recruited through an online sign-up sheet. A total of 31 first- and second-year medical students, from the Frank H. Netter MD School of Medicine at Quinnipiac University, attended the event which entailed a presentation and hands-on demonstration of and practice time with the Seldinger Technique.
3. Results
3.1. Seminars
Two identical, one-hour seminars were held back-to-back at the Frank H. Netter MD School of Medicine at Quinnipiac University, CT on November 30th, 2023. There were nineteen and twelve attendees at the first and second seminar, respectively. The primary author (D. H.) created the educational material and trained two facilitators to perform the Seldinger technique and aid throughout the seminar.
The PowerPoint presentation provided an overview of 3D-printing in medical education, the printing process including model creation, an introduction to the Seldinger technique and an overview of the contents within the micropuncture kit. The 3D-printed upper extremity venous model was passed around to students in groups of 4-6 per table (see Figure 6). Targeted didactic explanation was provided through the presentation focused on the common cannulation sites such as the basilic and cephalic veins to reinforce understanding of the anatomy. The contents of the micropuncture kits were reviewed including guidewire material, needle gauge-sizes, and usage in cannulation procedures. A live demonstration of the Seldinger Technique was performed with dedicated time for questions. Students from each group took turns performing the Seldinger Technique on a VEVOR Intravenous Phlebotomy Practice arm (see Figure 7).
3.2. Attendee Satisfaction
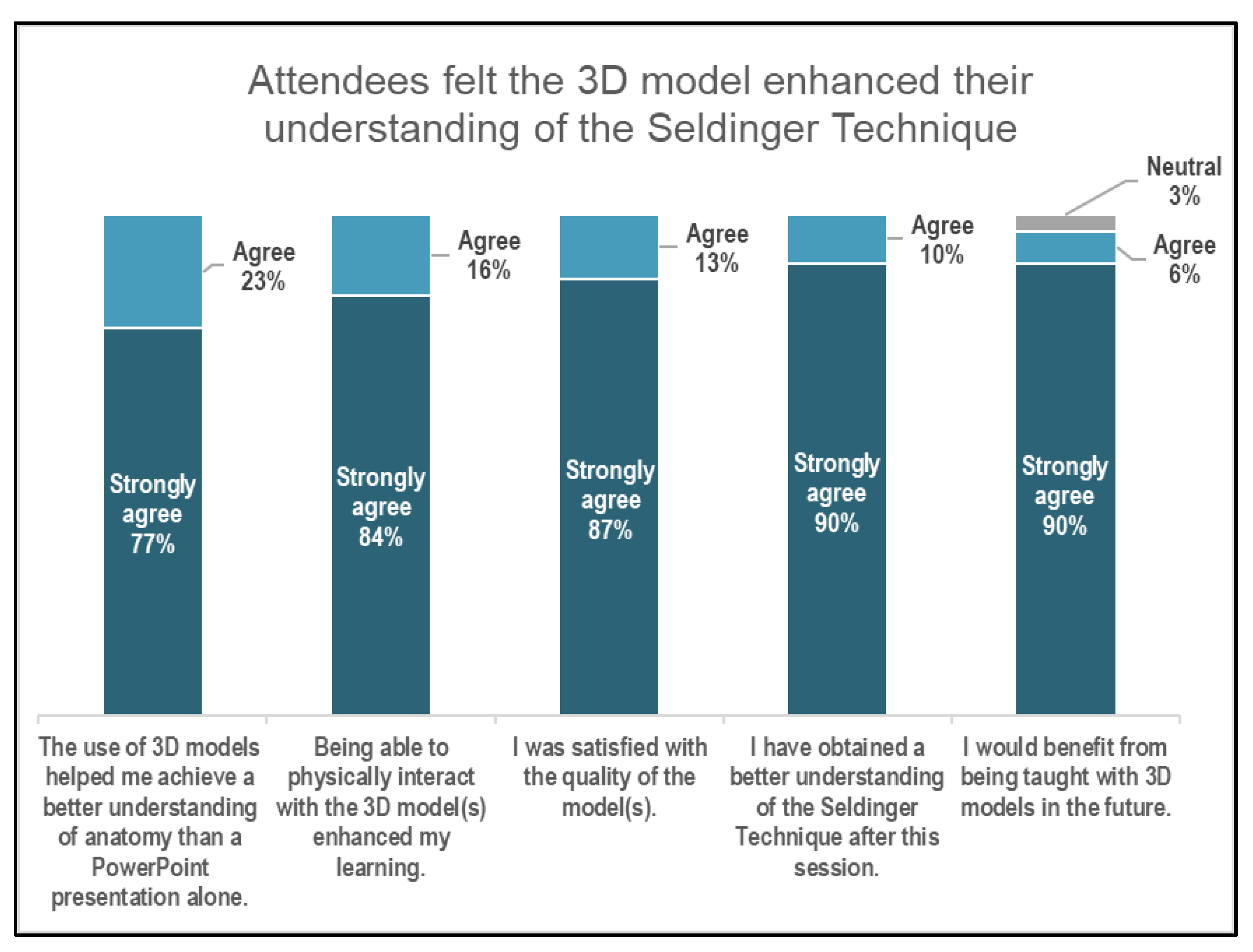
Most respondents felt positively about the incorporation of a 3D model as an educational tool (see Figure 8).
Of the attendees: 77% strongly agreed and 23% agreed that “The Use of 3D models helped me achieve a better understanding of anatomy than a PowerPoint presentation alone.”; 84% strongly agreed and 16% agreed that “Being able to physically interact with the 3D model(s) enhanced my learning.”; 87% strongly agreed and 13% agreed that “I was satisfied with the quality of the model(s).”; 90% strongly agreed and 10% agreed that “I have obtained a better understanding of the Seldinger Technique after this session.”; and 90% strongly agreed and 6% agreed that “I would benefit from being taught with 3D models in the future.” Only one attendee choose “Neutral” as their response to the statement, “I would benefit from being taught with 3D models in the future.”
Ad hoc informal comments from attendees noted that areas of enhanced learning included the physical interaction of the model and noting the anatomy prior to performing a hands-on technique on the venipuncture arm. Of note, the respondents were less likely to strongly agree that addition of a 3D model alone without a PowerPoint presentation covering relevant anatomy was more conducive to understanding.
4. Discussion
In the evolving landscape of medical education, the integration of 3D-printed anatomical models offers a pragmatic approach to enhancing traditional learning methodologies. This brief report explores the impact of high-fidelity 3D models, specifically within the realm of pre-clerkship medical education, focusing on Interventional Radiology's Seldinger Technique for vascular access. Leveraging advancements in 3D printing technology, we designed a pilot educational seminar that utilized a custom 3D-printed model of the upper extremity vasculature. This model served as a tactile and spatial learning tool for 31 pre-clinical medical students at the Frank H. Netter MD School of Medicine, Quinnipiac University. The seminar aimed to improve anatomical comprehension, stimulate interest in the inclusion of 3D models in future educational settings, and assess the feasibility of such integrative teaching approaches. The positive feedback from participants highlights the potential of 3D models to significantly enhance understanding of complex anatomical structures and technical procedural skills, suggesting a promising direction for the future of medical education.
Our work extends the work of Goudie et al (2019) by including a hands-on application of the learned material in the educational seminar [9]. We followed the framework of Garcia et al for the creation of a 3D anatomic model in their 2019 technical report: (1) selecting the anatomical area of interest, (2) the creation of the 3D geometry, (3) the optimization of the file for the printing and the appropriate selection of (4) the 3D printer and (5) materials [8]. All of which we were able to reproduce.
4.1. Lessons Learned
In our educational seminar, the anatomic area of interest was the upper extremity vasculature; chosen to improve understanding of a common cannulation technique called the Seldinger Technique.
Notably, the model had to be resized to fit the MakerBot 3D printer platform thus losing finer details such as vessel patency. It was printed via filament extrusion using a rigid polymer and could not be punctured with cannulation equipment. Future iterations of the model could focus on printing using resin-based materials which are a class of softer, more pliable material that more accurately reflects tissue texture. Potential areas of improvement include revising the model to be scaled to anatomic size and ensuring patency of the vessels to facilitate insertion of cannulation tools. Further, labeling of the model with coloring indicating the different vessel branches may improve understanding of the anatomy.
3D-Slicer is a powerful suite of post processing tools for the generation of custom 3D models. It continues to be well-supported by developers with a robust set of how-to instructions and guides. Online resources include several step-by-step instructions for loading and segmentation of D.I.C.O.M. imaging studies. It took approximately 3-4 weeks of reading and iterative manual segmentation to understand how to generate a 3D model with anatomic fidelity.
Thirty-one first- and second-year medical students attended an educational seminar using a 3D model of the upper extremity vascular along with a proprietary latex phlebotomy arm to reinforce understanding of the Seldinger Technique. This format of learning was well received by attendees. Students positively commented on the tactile feedback with cannulation using the introducer needle, guidewire, and insertion of the catheter. Moreover, the presence of tubing pressurized with red colored dye simulated blood and provided learners confidence they had successfully gained access to the vascular space. As the cost of 3D printing decreases, it is feasible that more complex training models can be created to simulate cannulation and insertion of central lines via the internal jugular vein or femoral vein.
4.2. Sustainability
Factors influencing scalability and reproducibility include the size of the room, material costs, and training of facilitators. In this instance, the seminar was held in a multipurpose educational room with four monitors to show the presentation. One challenge was the proximity to outlets and other electrical devices that could potentially become saturated with the simulated blood. In terms of cost, five venipuncture arms ordered online cost approximately $300 USD, micropuncture kits can be found for $200 USD in a package of ten. Many universities are investing in 3D printers which are becoming cheaper and P.L.A. filament is relatively cheap at $30/kg USD.
4.3. Strengths & Limitations
The strengths of our study include highlighting the robust utility of 3D-printed models in enhancing anatomical understanding and procedural skills in a simulated medical education setting. One significant strength is the direct enhancement of spatial and tactile learning, allowing students to grasp complex vascular structures and techniques such as the Seldinger Technique effectively. Furthermore, the use of these models has shown to stimulate learner engagement and satisfaction, potentially revolutionizing traditional learning paradigms in medical education. The positive feedback from students underscores the potential of such technology to supplement, if not partially replace, more traditional teaching tools, such as cadavers, which are more costly and less versatile.
However, the study is not without limitations. The main limitation arises from its small scale and the specificity of the sample, which consisted solely of pre-clerkship medical students from a single institution, potentially limiting the generalizability of our findings. Additionally, while the integration of the 3D model with didactic teaching was overall well-received, the feedback indicated that the 3D model alone might not be sufficient for complete understanding without the supportive didactic component. This suggests a need for a balanced educational approach that combines multiple teaching modalities. Further research with larger, more diverse cohorts, treatment-control study design, and longitudinal follow-up could provide deeper insights into the long-term benefits and learning retention from using 3D models in medical education.
5. Conclusions
3D printing of models with high anatomic fidelity will continue to have a growing impact on medical education. Unique features inherent to models include improved durability, lower cost and toxicity compared to formalin-based cadavers. Additional areas of impact include preprocedural surgical planning, patient education, and prosthetic development. With the prevalence of open-source computer assisted designing software such as 3D Slicer, users now have the tools to create unique models for a variety of medical education applications. This project demonstrates an application with the use of a 3D-printed model along with a venipuncture arm for students to interact with when learning technical skills in simulation-based medical education. Positive feedback from students indicated that this approach can be an effective teaching method.
Author Contributions
Conceptualization, D.H.; methodology, D.H. & D.M.; software, D.H.; formal analysis, D.H.; investigation, D.H.; resources, D.H.; data curation, D.H.; writing—original draft preparation, D.H.; writing—review and editing, D.H. & D.M.; visualization, D.H.; supervision, D.M.; project administration, D.H. & D.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Quinnipiac University for studies involving humans’ protocol #10623 on 10/17/2023.
Informed Consent Statement
Participant consent was waived because (a) information obtained was recorded by the investigator in such a manner that the identity of the human subjects cannot readily be ascertained, directly or through identifiers linked to the subjects and (b) any disclosure of the human subjects ' responses outside the research would not reasonably place the subjects at risk of criminal or civil liability or be damaging to the participants ' financial standing, employability, educational advancement, or reputation.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy concerns.
Acknowledgments
Westley Shay (Q.U. Radiology Assistant program) provided the expired micropuncture kits used during the educational seminar. Tania Grgurich (Q.U. Radiology Assistant program) provided insight into the 3D printing process of anatomic models. Brian Shoemaker (post-doctoral chemical engineering student) printed out the 3D-model of the upper extremity vasculature using the Makerbot 3D printer. Marissa Hashizume and Andrew Liu assisted during the educational seminar.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Fedorov, A. , et al., 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn Reson Imaging, 2012. 30(9): p. 1323-41. [CrossRef]
- Otton, J.M. , et al., 3D printing from cardiovascular CT: a practical guide and review. Cardiovasc Diagn Ther, 2017. 7(5): p. 507-526. [CrossRef]
- Ballard, D.H. , et al., Clinical Applications of 3D Printing: Primer for Radiologists. Acad Radiol, 2018. 25(1): p. 52-65. [CrossRef]
- Itagaki, M.W. , Using 3D printed models for planning and guidance during endovascular intervention: a technical advance. Diagn Interv Radiol, 2015. 21(4): p. 338-41. [CrossRef]
- Yuan, D. , et al., Precise treatment of aortic aneurysm by three-dimensional printing and simulation before endovascular intervention. Sci Rep, 2017. 7(1): p. 795. [CrossRef]
- Trace, A.P. , et al., Radiology's Emerging Role in 3-D Printing Applications in Health Care. J Am Coll Radiol, 2016. 13(7): p. 856-862 e4. [CrossRef]
- Bernhard, J.C. , et al., Personalized 3D printed model of kidney and tumor anatomy: a useful tool for patient education. World J Urol, 2016. 34(3): p. 337-45. [CrossRef]
- Garcia, J. , et al., 3D printing materials and their use in medical education: a review of current technology and trends for the future. BMJ Simul Technol Enhanc Learn, 2018. 4(1): p. 27-40. [CrossRef]
- Goudie, C. , et al., The Use of 3D Printed Vasculature for Simulation-based Medical Education Within Interventional Radiology. Cureus, 2019. 11(4): p. e4381. [CrossRef]
Figure 1.
Graphical User Interface of 3D Slicer 5.4.0 depicting the manually segmented right upper extremity vasculature in green.
Figure 1.
Graphical User Interface of 3D Slicer 5.4.0 depicting the manually segmented right upper extremity vasculature in green.
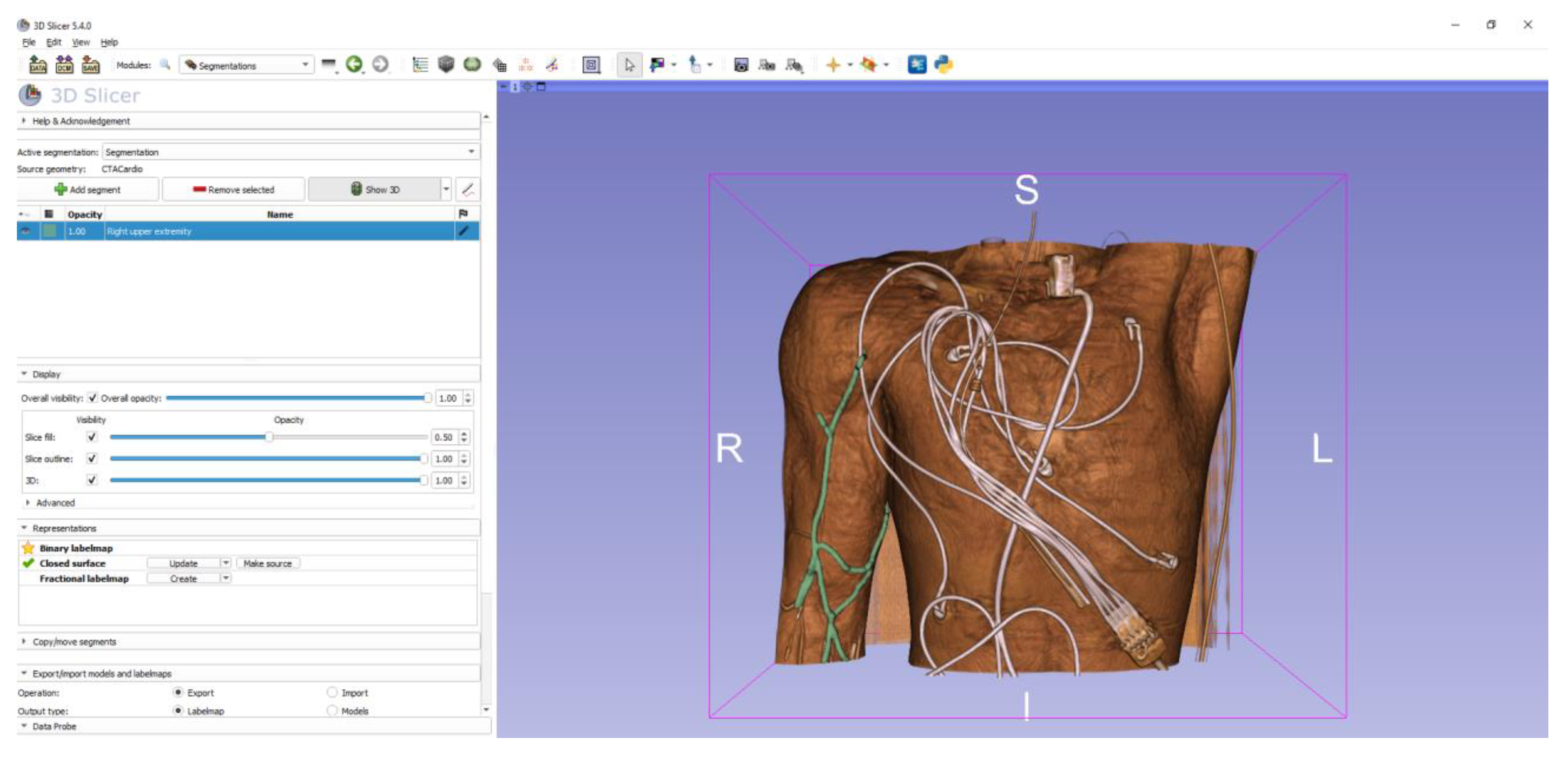
Figure 2.
(a) The left image is a manually segmented, post processed right upper extremity vasculature model isolated from a CT Angiogram in .STL file format. (b) The right image is the final product printed on a MakerBot filament extruding printer using P.L.A., a rigid polymer as the material, and measures 16cm x 5cm. Photo credit: David Hyndman.
Figure 2.
(a) The left image is a manually segmented, post processed right upper extremity vasculature model isolated from a CT Angiogram in .STL file format. (b) The right image is the final product printed on a MakerBot filament extruding printer using P.L.A., a rigid polymer as the material, and measures 16cm x 5cm. Photo credit: David Hyndman.
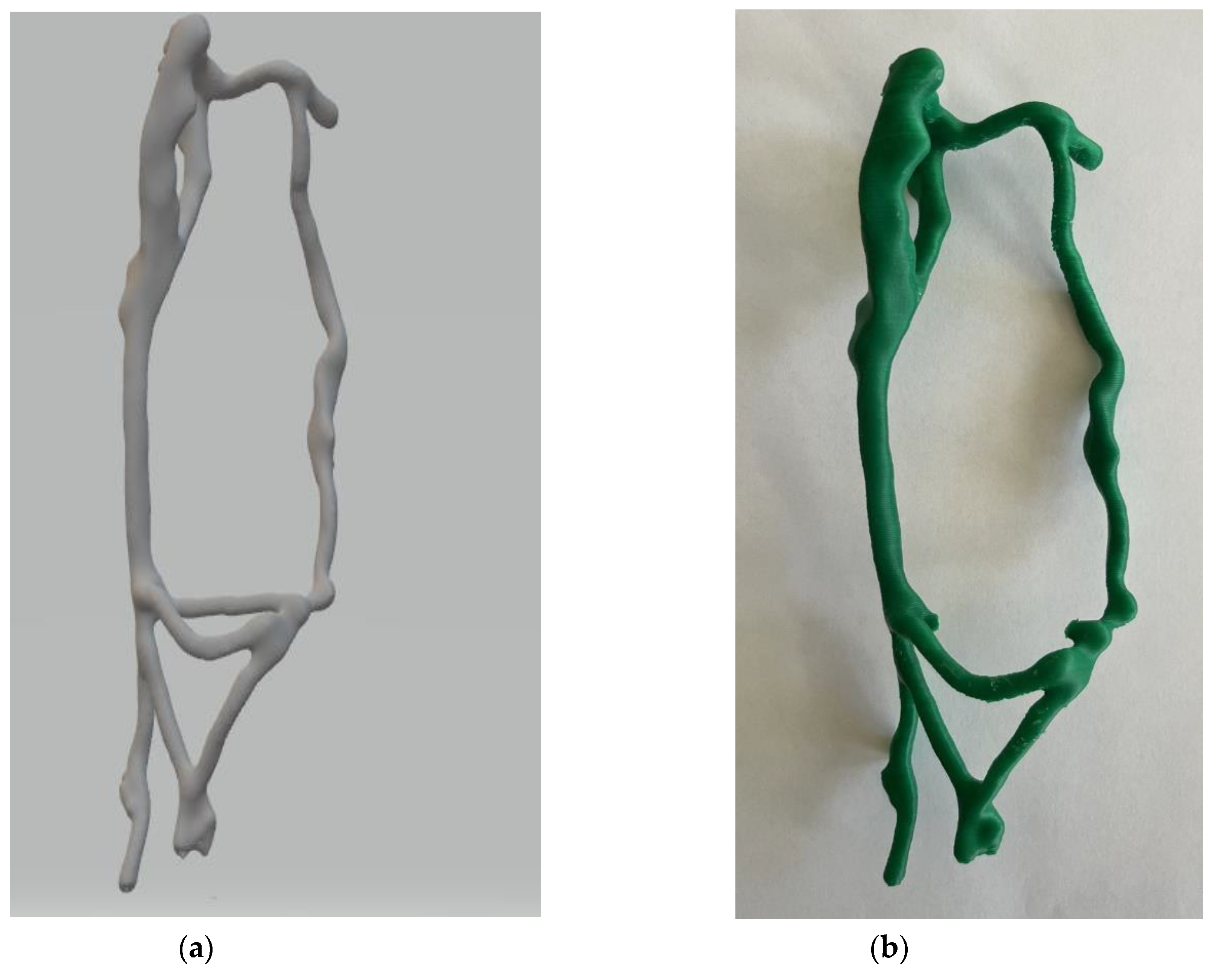
Figure 3.
VEVOR Intravenous Phlebotomy Practice arm and Terumo Pinnacle® Precision Access System. Each group of medical students performed the Seldinger Technique on the practice arm using a micropuncture kit. Photo credit: David Hyndman.
Figure 3.
VEVOR Intravenous Phlebotomy Practice arm and Terumo Pinnacle® Precision Access System. Each group of medical students performed the Seldinger Technique on the practice arm using a micropuncture kit. Photo credit: David Hyndman.
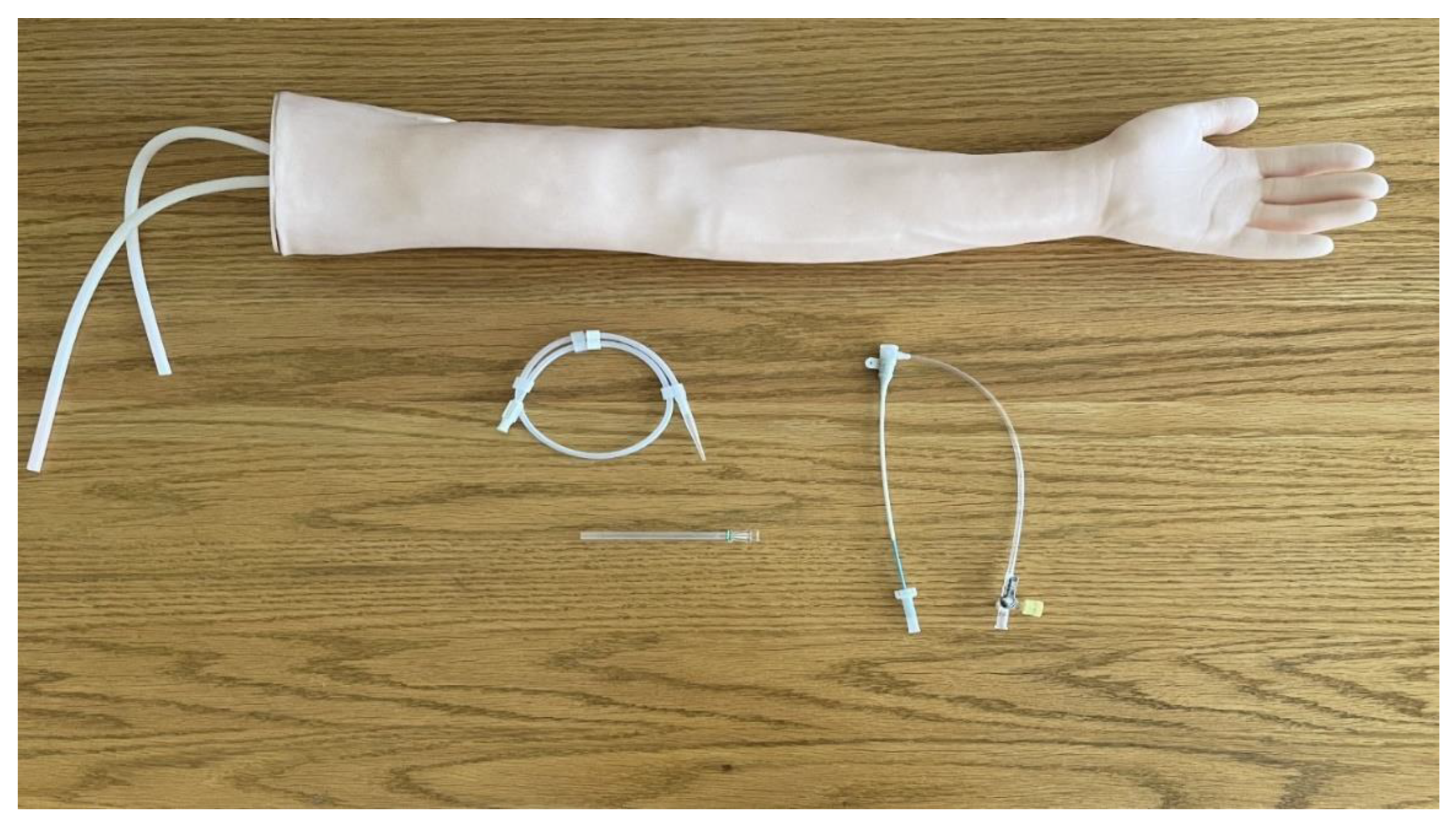
Figure 4.
Four tables were set up with the VEVOR Intravenous Phlebotomy Practice arm, pressurized red dye simulating blood, and a Terumo Pinnacle® Precision Access System. Attendees of the seminar were broken into groups of 4-6 per table and event facilitators provided real time guidance during the hands-on portion of the event. Photo credit: David Hyndman.
Figure 4.
Four tables were set up with the VEVOR Intravenous Phlebotomy Practice arm, pressurized red dye simulating blood, and a Terumo Pinnacle® Precision Access System. Attendees of the seminar were broken into groups of 4-6 per table and event facilitators provided real time guidance during the hands-on portion of the event. Photo credit: David Hyndman.
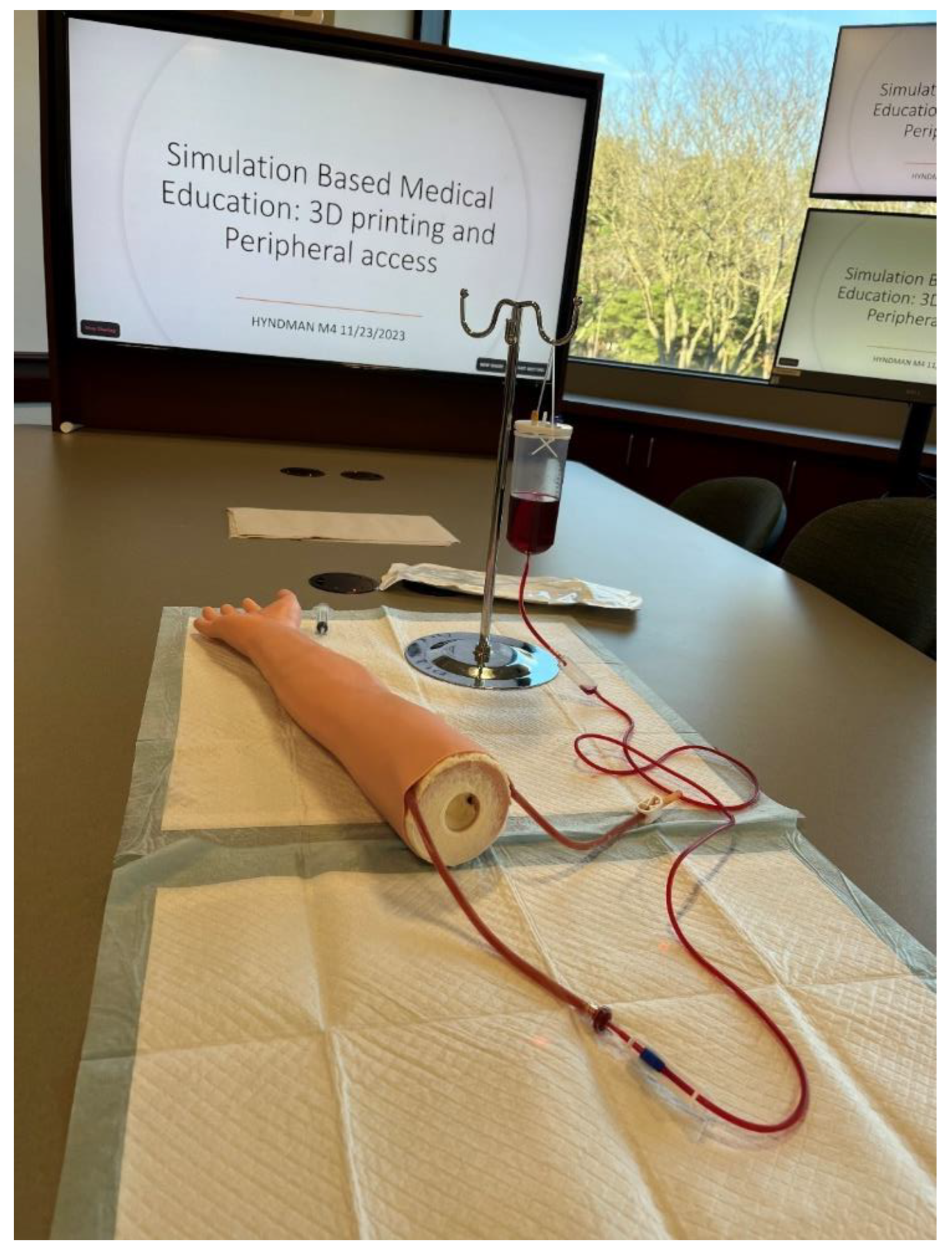
Figure 5.
Survey instrument adapted from Gouldie et al technical report [9].
Figure 5.
Survey instrument adapted from Gouldie et al technical report [9].
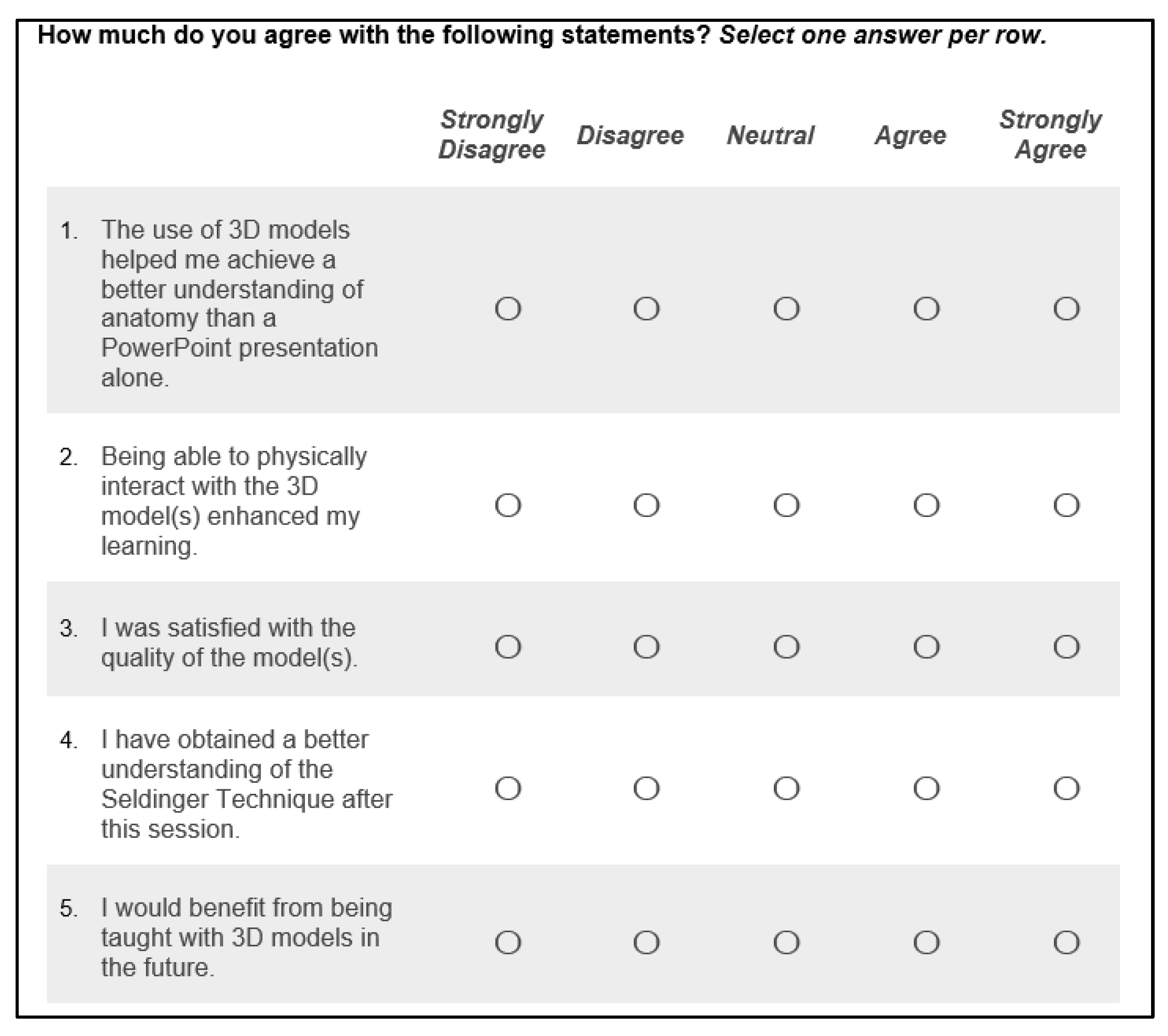
Figure 6.
The 3D model of the upper extremity vasculature is passed around attendees during the PowerPoint presentation. Photo credit: David Hyndman.
Figure 6.
The 3D model of the upper extremity vasculature is passed around attendees during the PowerPoint presentation. Photo credit: David Hyndman.
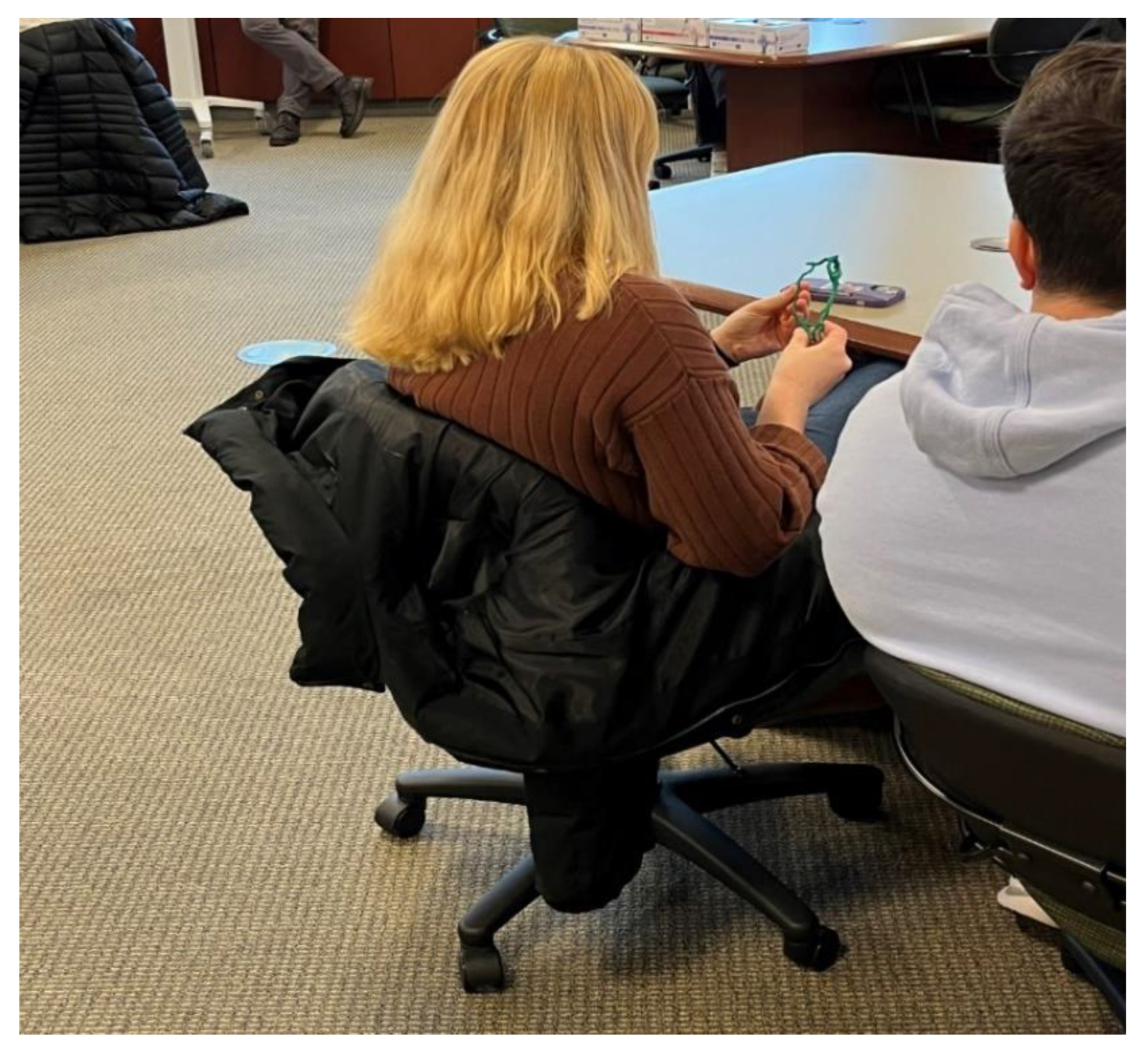
Figure 7.
A student performing the Seldinger technique on a VEVOR venipuncture arm using a Terumo micropuncture kit during the educational seminar. Photo credit: David Hyndman.
Figure 7.
A student performing the Seldinger technique on a VEVOR venipuncture arm using a Terumo micropuncture kit during the educational seminar. Photo credit: David Hyndman.
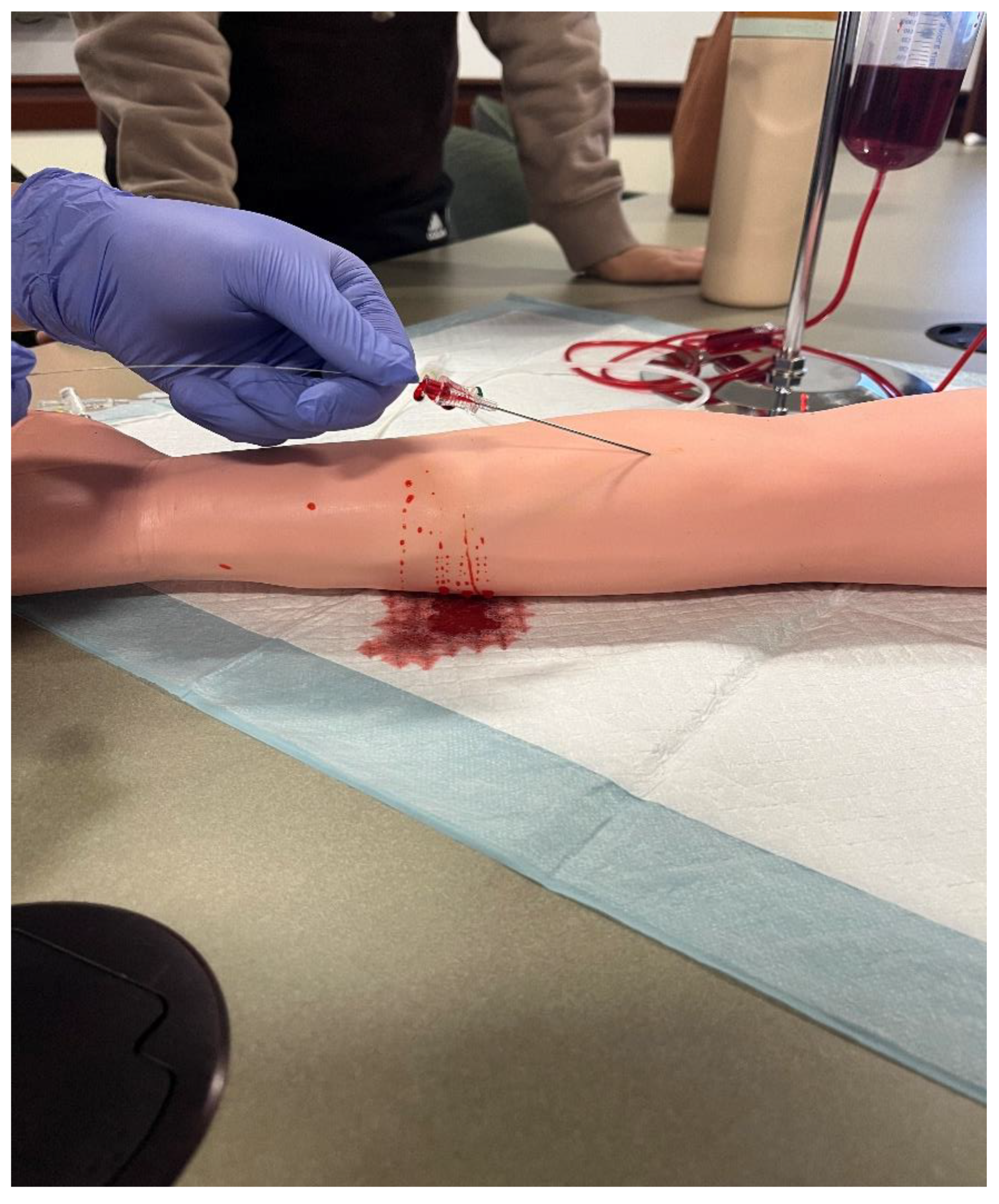
Figure 8.
Post-event results from survey adopted from Goudie et al. n = 31. Likert 5-point response scales range from Strongly Disagree to Strongly Agree.
Figure 8.
Post-event results from survey adopted from Goudie et al. n = 31. Likert 5-point response scales range from Strongly Disagree to Strongly Agree.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



