
Submitted:
07 May 2024
Posted:
08 May 2024
You are already at the latest version
Abstract
This study assessed the performance of low-dose CT lung scans across various acquisition parameters and examined the impact of iterative reconstruction (IR) algorithms on image quality for lung cancer screening. The performance of multi-slice CT scanners was assessed by using a Catphan 600 phantom, specifically within the CTP404 test module that contains materials like Teflon, Delrin, Acrylic, Polystyrene, LDPE, PMP, Air, and water. Three protocols were selected and categorized into standard, low dose, and ultra-low dose. The standard protocol featured a tube voltage of 100 kVp for single-detector CT, a pitch of 0.75, detector collimation of 0.60 mm, and a gantry rotation time of 0.33 seconds, with 5 mm slice thickness. Images were reconstructed using standard kernels like B80f and 170f, combined with either FBP or various IR algorithms. Findings indicated that the noise power spectrum (NPS) peak value (HU2mm2) increased with higher IR levels, with FBP showing the highest peak. Additionally, NPS spatial frequency diminished as IR levels rose. Optimizing contrast and spatial resolution for both background and regions of interest involved adjusting the target transfer function (TTF) and contrast-to-noise ratio (CNR), crucial for protocol optimization. Proper adjustment of IR levels is vital, as higher levels can alter image texture and affect NPS spatial frequency. The results of this study showed that the use of IR algorithms in low-dose CT lung scans significantly improved image quality, particularly in terms of noise reduction and spatial resolution. However, the choice of acquisition parameters also played a crucial
Keywords:
Computed Tomography
; lung cancer screening
; Iterative Reconstruction
; Task-Based Assessment
; Ultra-low dose
; Noise Power Spectrum.
1. Introduction
Lung cancer is the world's deadliest cancer. It was reported that 11.4 percent of the estimated 2.3 million new cancer cases in 2020 were cancer cases, and it remained the leading cause of cancer death, accounting for 18 percent of the estimated 1.8 million cancer deaths [1]. Most lung cancers are not detected at an early stage. The patient will be tested for lung cancer using detection techniques such as sputum cytology, chest radiography, or computed tomography (CT). However, CT has a higher precision in cancer interpretation than the other two methods. Sputum cytology and chest radiography have low sensitivity in detecting early tumors, resulting in an increase in lung cancer mortality [2,3].
Because of its increased accuracy in diagnosing cancer, computed tomography (CT) is a promising screening tool [4,5]. Unfortunately, it exposes a large number of people to radiation, raising concerns about potential risks such as patient mortality [6,7,8]. Low-dose radiation CT has been shown to identify microscopic lung nodules more effectively. Low dose CT is a technique that creates a series of detailed images of internal organs using a computer linked to X-ray equipment that emits a very low dose of radiation. The images were captured from various angles and then used to create three-dimensional views of tissues and organs.
With parameter changes to reduce dosage exposure, there are observable trade-offs between dose exposure and image quality [9,10,11]. The X-ray tube current and voltage rotation time, helical pitch, section thickness, scan duration, and dose adjustment technique all influence radiation dose; by improving image quality, the reconstruction algorithm and image filters allow CT parameters to be adjusted to reduce radiation exposure [12,13]. Previous research has shown that applying the iterative reconstruction algorithm to phantom images maintains high image quality and object detectability for human radiological evaluation of CT exams, with noise reduction of up to 60 and dose reduction of up to 85 percent to the patient [14,15,16].
A low contrast detectability LCD is used to objectively measure the image quality of a CT scanner. The ability of a CT scanner to distinguish between objects with identical x-ray attenuation coefficients is referred to as LCD. It refers to imaging technology's ability to differentiate between objects with similar properties in the context of other clinical imaging techniques. This procedure is the most effective method for improving image quality and evaluating the possibility of reducing radiation exposure.
Research conducted by Sumitani et al. (2008) regarding sputum cytology and chest radiography was unable to demonstrate that screening could reduce lung cancer mortality [17]. CT scans were found to be more accurate in detecting lung cancer, however, the standard radiation dose used to produce a high-quality image would expose patients to an excessive amount of radiation, which must be avoided. Hanif et al. suggested that low-dose CT imaging protocols may result in a loss of image quality due to noise and artefacts throughout the image space [18,19]. Noise in CT is caused by the difference in attenuation coefficients between voxels, which reduces the signal-to-noise ratio of the CT images [20,21].
The use of small voxels can improve the visibility of fine details while reducing blurriness. To balance the effects of radiation dosage and image quality, iterative reconstruction (IR) algorithms have been developed to achieve the desired medicinal benefits while minimizing radiation exposure [22,23]. IR is a computational approach which alters the weighting of image data through a cyclical process to decrease noise while maintaining resolution and image quality [24]. Research has shown that IR techniques can be effective in decreasing image noise, yet the spatial resolution may be affected in terms of contrast resolution [25]. Therefore, the purpose of this research is to evaluate task-based assessment of low dose CT lung examination and to examine the influence of the iterative construction algorithm on image quality of low dose CT lung cancer screening.
2. Materials and Methods
2.1. Phantom Study
The performance of different acquisitions in terms of image quality was evaluated in this study using Catphan®-600 (see Figure 1). The CTP404 test module of the Catphan-600 included samples of Teflon, Delrin, Acrylic, Polystyrene, low-density polyethylene (LDPE), polymethyl pentene (PMP), air, and a small water vial [26]. The pixel size can be computed by counting the pixels in the x and y axes that divide the test cylinders. Additionally, the module contains fixed acrylic spheres to assess the scanner's capacity to capture spherical sub volumes, with diameters of 2, 4, 6, 8, and 10 mm. The phantom was positioned on the table's gantry end, with the box hinges facing away from the gantry. It is recommended that the box be placed on the surface of the table instead of a table pad to ensure consistency. To open the box, the lid is rotated 180° and extra weight is required to balance out the phantom's weight. The patient straps can be used to provide additional stability.
2.2. CT Image Acquistion
In this study, we conducted a scan of a phantom using the parameters listed in Table 1. The tube voltage for standard dose computed tomography (SDCT) was set at 100 kVp, the pitch was 0.75, the detector collimation was 0.60 mm, and the gantry rotation time was 0.33 seconds. The slices were 5 mm thick, and the reconstruction was done with a standard kernel such as B80f and 170f, combined with either filtered back projection or different levels of iterative algorithms. The parameters for the low dose CT (LD CT) and SD CT scans were the same as for the ultra-low dose CT (ULD CT) scans, except for the tube voltage, which was 100 kVp for the LD CT and SD CT scans and 80 kVp for the ULD CT scans.
2.3. CT Image Quality Assessment
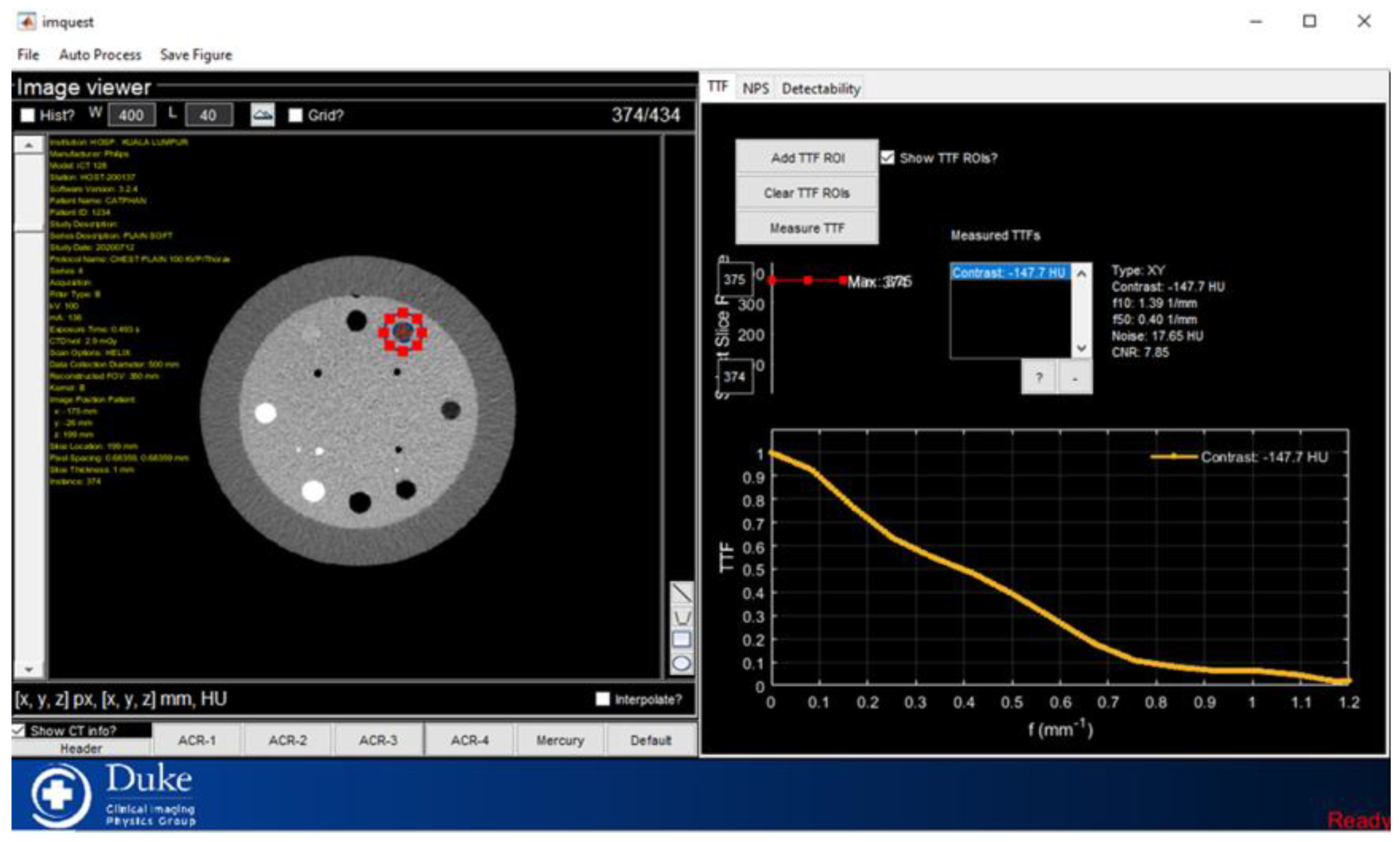
Physical image quality can be determined through physical measurements such as sharpness, noise, and contrast. In this study, we utilized ImQuest, a CT image analysis tool designed for task-based image quality assessment. The software was reported by the American Association of Physicists in Medicine (AAPM) in Publication No. 233 (2019). ImQuest uses TG 233 approaches to measure resolution in terms of TTF, noise in terms of NPS, and CNR [27,28]. Since some image quality assessments are impossible to measure mathematically, an image computing technique is used to quantify the results. For instance, NPS requires a Fourier noise autocorrelation transformation, while TTF is determined by the magnitude of the discrete Fourier transform of the LSF.
The term TTF is used to characterize image spatial resolution that evaluates comparable spatial resolution to improve image quality. TTF in the CTP404 of the phantom insert rod was analyzed using a circular ROI. NPS was then used to assess the image's noise texture. NPS was thus calculated with a square box of 80mm × 80mm in the center. A CNR estimate is also included in the LCD relational data. The rod insert measurements were obtained using the CTP404 module.
Figure 2.
Placement of the ROI at rod insert for the TTF calculation.
2.4. Statistical Analysis
The statistical analysis was carried out using SPSS V25.0 (SPSS, version 25.0 for Windows, Chicago, Illinois, USA) and Real Statistics software (RealStat.xlsx) that is integrated with Microsoft Excel 2013. The sample characteristics and data were expressed as absolute frequencies or means and standard deviations, as appropriate. The values in this study were presented in tables. Normality assessment of the data was conducted through the Shapiro-Wilk test, indicating a normal distribution. This led to the utilization of a one-way analysis of variance (ANOVA) to compare the mean values of TTF, NPS, and CNR across the three different FBP reconstruction algorithms (S1, S3, and S5). Post-hoc analysis was then performed using the Bonferroni correction method, with statistical significance set at a p-value < 0.05.
3. Results
3.1. Standard Dose
NPS, TTF, and CNR values are evaluated using four different IR algorithms as well as two additional TTF inserts, acrylic and LDPE inserts. As shown in Table 3.1, all four different IR algorithm settings are tested with three groups of radiation dose such as standard dose, low dose, and ultra-low dose with different acquisition parameters. TTF's spatial frequency is calculated by multiplying the spatial frequency by 0.5, which is 50% of the TTF value. Measurements were made three times to ensure that the results were accurate.
The standard dose parameter adjustment reduces the pitch to 0.75 compared to the low dose pitch of 0.9. While both have the same overall scan parameters, only the pitch value can differ. Pitch is one of the variables that can be changed to optimize image quality in terms of LCD performance by reducing image noise and maintaining a low radiation dose to the patient. Table 1 shows the NPS, TTF50%, and CNR values for both inserts. Each image slice is measured, and the standard deviation represents the variation in the data dispersion of all repeated measurements. Peak NPS values are shown to decrease as the IR algorithm level increases.
S5 had a lower NPS peak than FBP, S1, and S3. However, S1 has the highest NPS spatial frequency values among the other IR algorithms, while S5 has the lowest. Following that, as the IR level increases, the TTF spatial frequency of the acrylic insert decreases significantly. The TTF spatial frequency of the LDPE insert, on the other hand, shows an ambiguous pattern in that it decreases as IR increases but suddenly rises as IR increases at S5. As the IR increases, the CNR values for acrylic inserts increase significantly. The CNR value for FBP is negative, indicating that there is less signal than noise, whereas the CNR values for other IR are positive, indicating that there is more activation signal than noise.
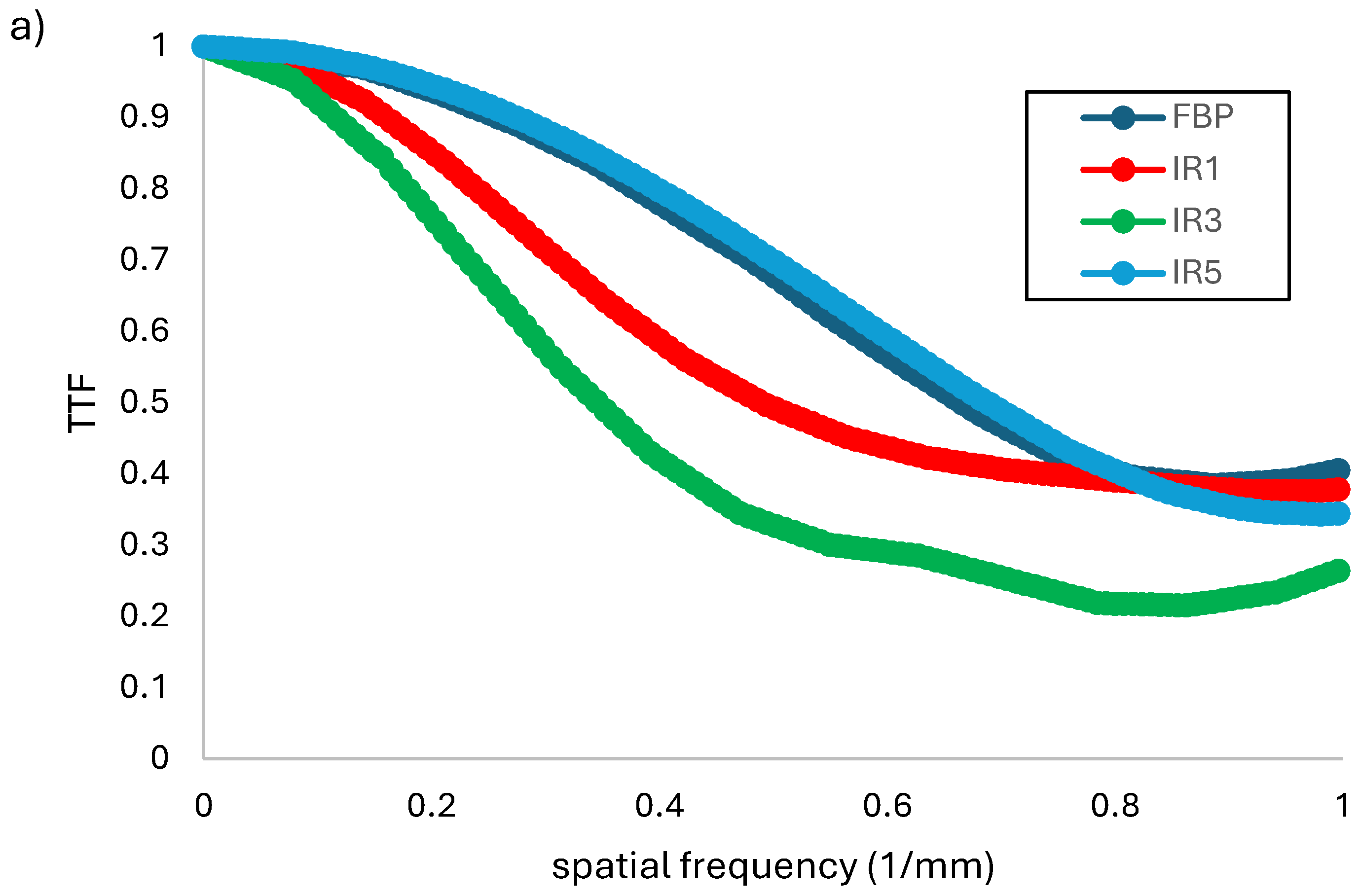
Figure 1(a) shows the relationship between TTF and spatial frequency (1/mm) at various levels of IR algorithms with acrylic insert. TTF values tend to fall as IR rises. According to table 4.1, the spatial frequency of TTF at 50% decreases as IR increases due to differences in spatial resolution. It demonstrates that as IR increased, which is essentially constant, so did the TTF's efficiency. This enhancement improves the TTF and, as a result, the spatial resolution, resulting in a frequency deviation on the ESF curves. The TTF spatial frequency of LDPE inserts is lower than that of acrylic, as shown in Figure 1(b). It could be the result of a different background contrast. When the highest IR levels are used, the TTF results show the highest value of f50 when using the LDPE insert. However, unlike acrylic, LDPE produces inconsistent results for different IR levels. At 0.89 mm-1, the FBP has a higher TTF spatial value than IR1 and IR3. Racine et al. (2021) discovered that a higher TTF value indicates better spatial resolution [29].
Figure 1.
Relationship of TTF and spatial frequency (1/mm) obtained at different levels of IR algorithms of standard dose group for (a) acrylic rod insert and (b) LDPE.
Figure 1.
Relationship of TTF and spatial frequency (1/mm) obtained at different levels of IR algorithms of standard dose group for (a) acrylic rod insert and (b) LDPE.
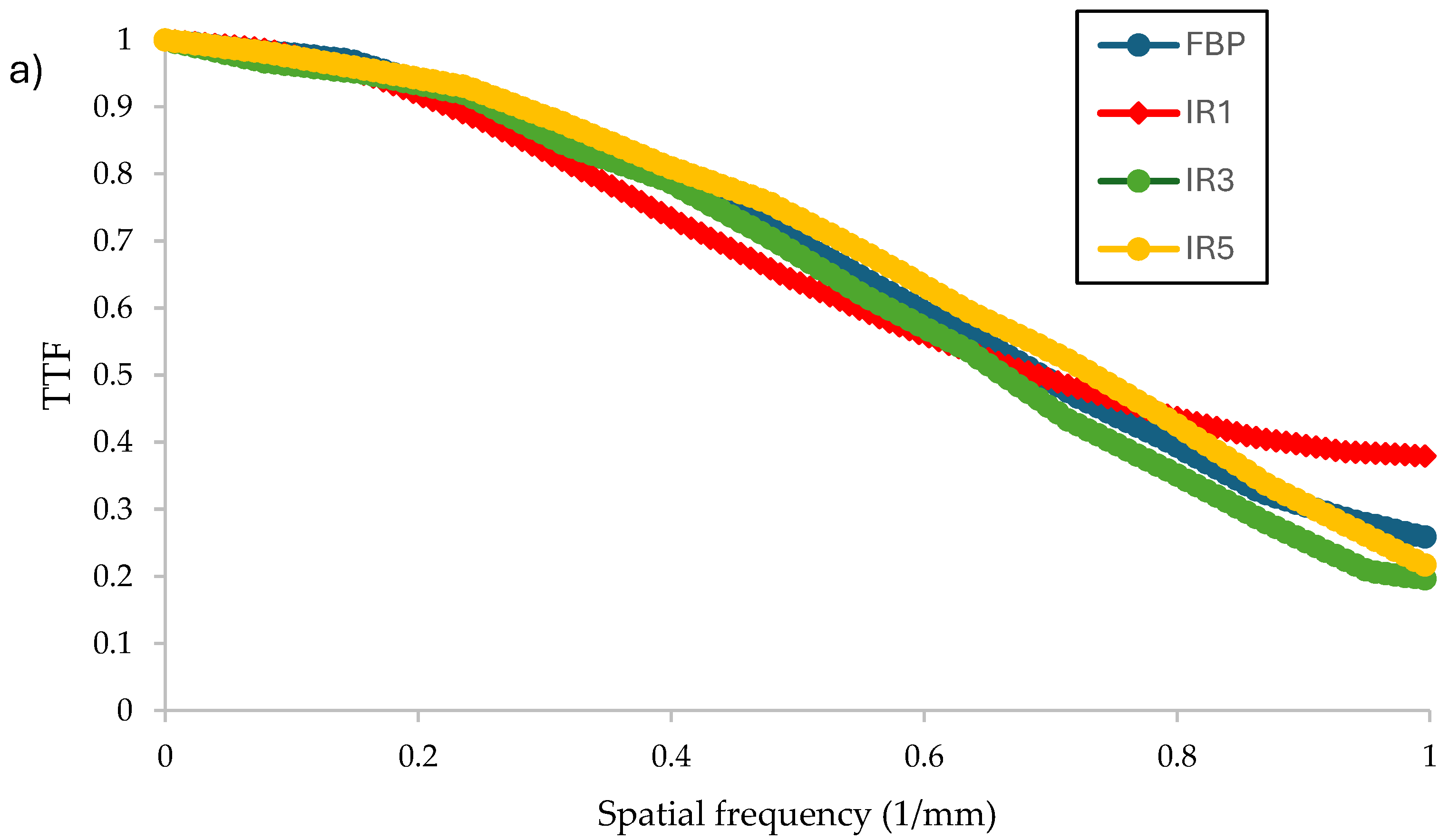
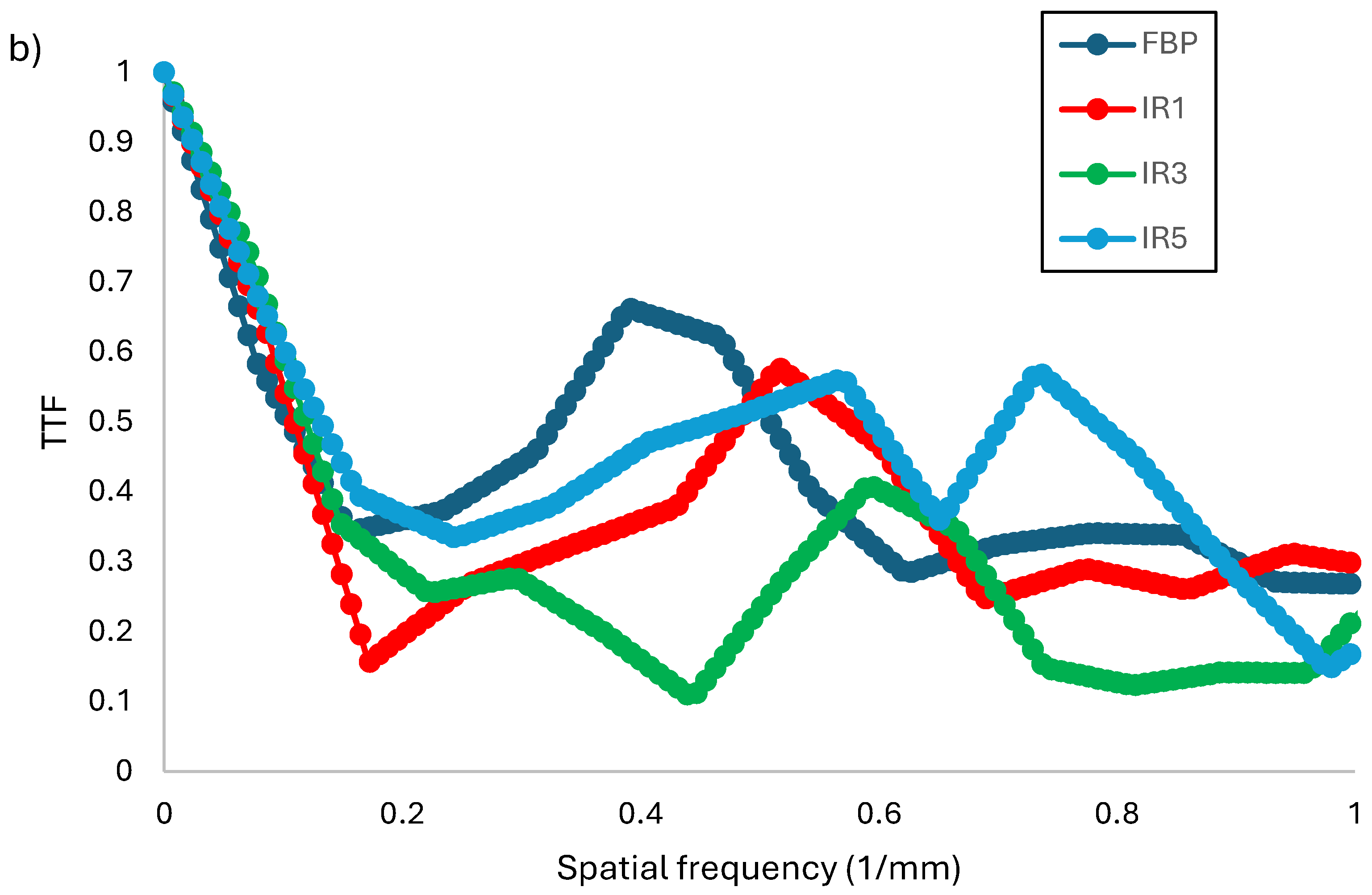
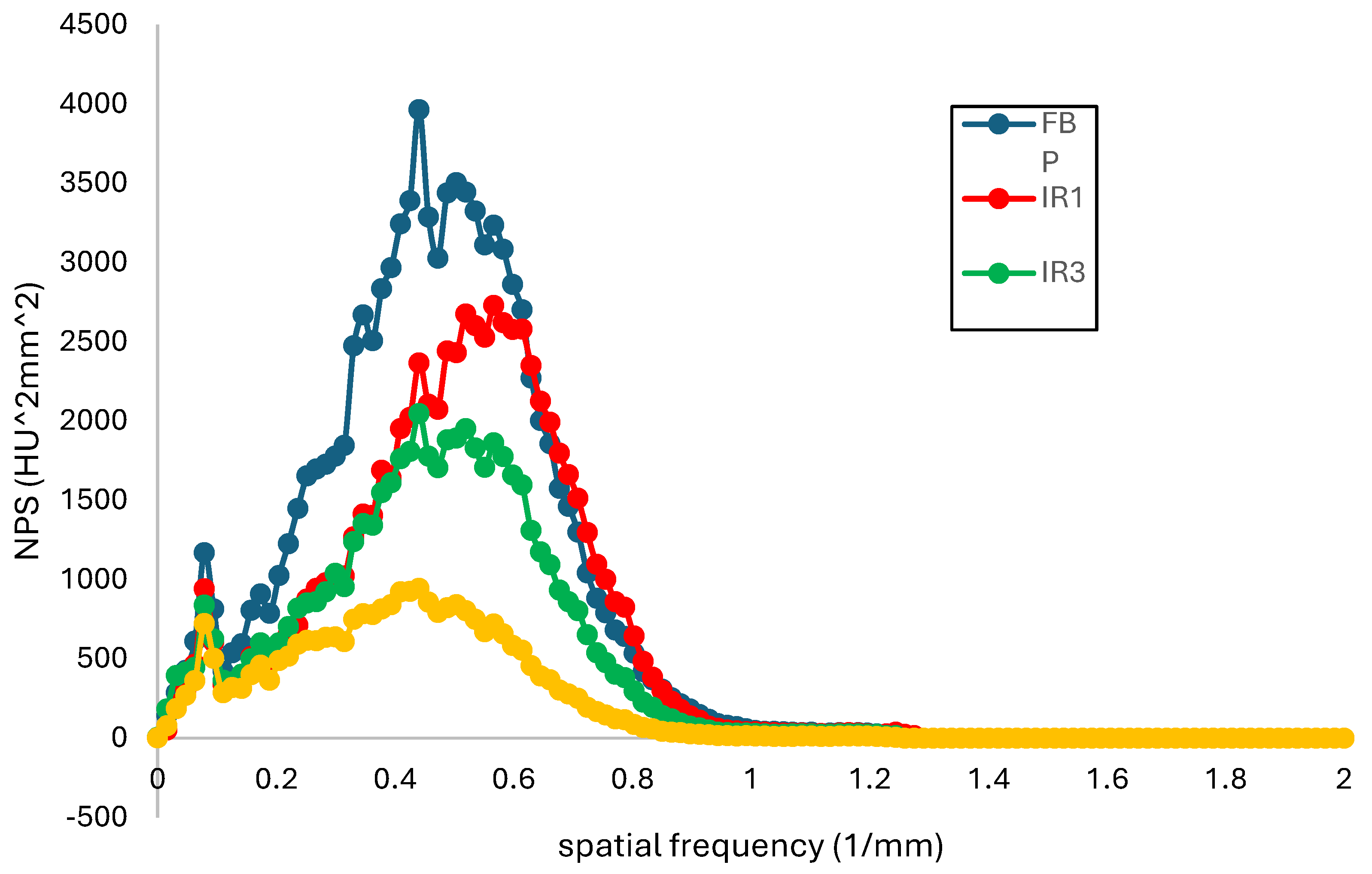
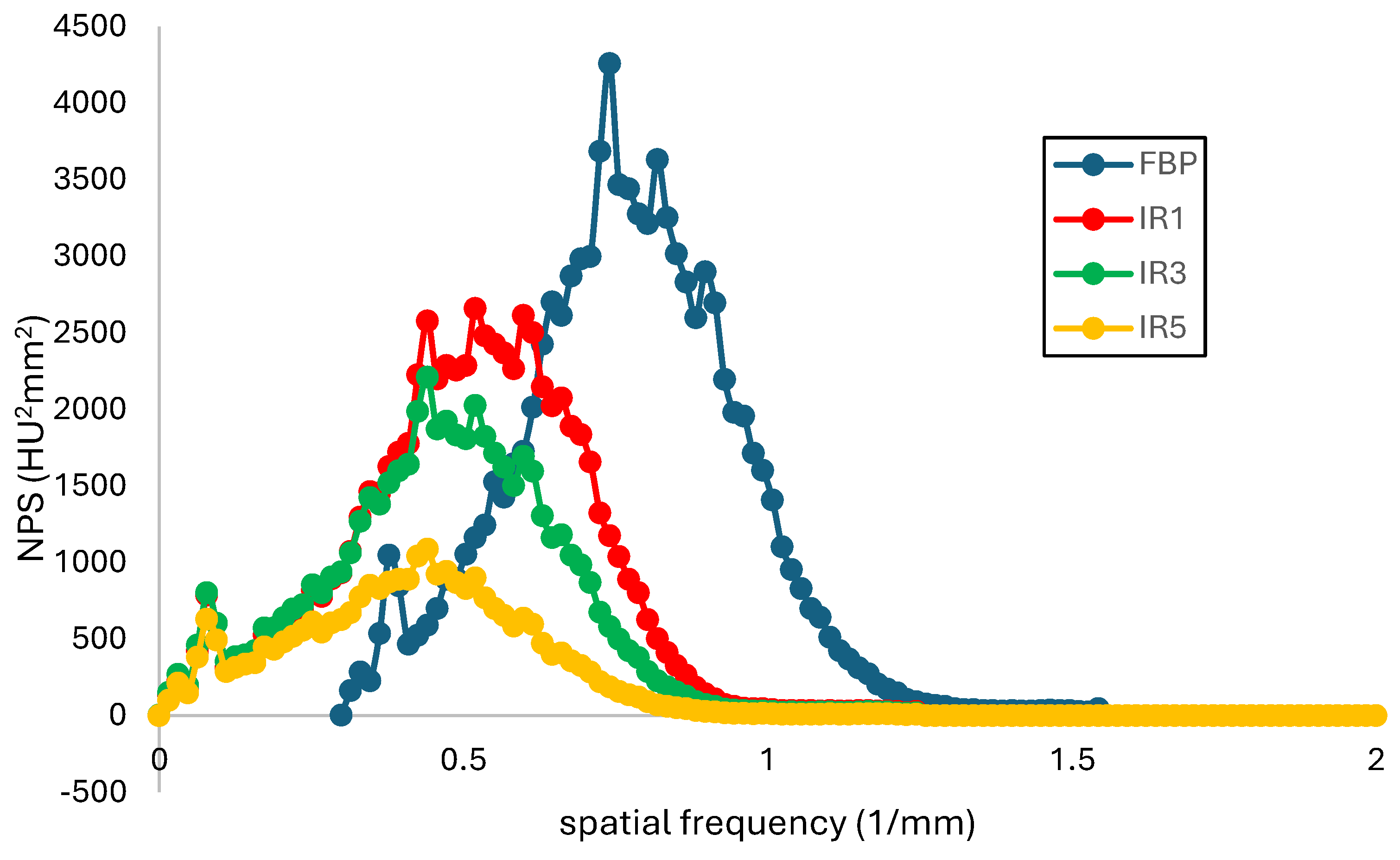
Figure 2 depicts the relationship between NPS and spatial frequency at various levels of IR algorithms. NPS spatial frequency data is the frequency at which the NPS maximum is reached. As the level of the IR algorithms increased, the NPS peak frequency was found to adjust to a lower frequency. Furthermore, as the peak NPS or amplitude of the NPS increases, so does the overall magnitude of the noise. NPS amplitude was used to assess magnitude changes and to examine noise texture. The NPS peak value decreases as the level of IR algorithms increases, as shown in Table 2. Furthermore, Figure 2 shows that as the IR level increases, the NPS spatial frequency decreases. A higher NPS spatial frequency indicates a finer image, while a lower NPS spatial frequency indicates grainy noise. However, the value of IR level 1 differs from previous studies in that it has a higher spatial frequency than the other IR algorithms. In contrast, the comparison of NPS between the FBP and the various levels of SAFIRE revealed a shift in the peak of the curve towards lower frequencies as SAFIRE levels increased. The comparison of NPS between the FBP and the various levels of SAFIRE, on the other hand, revealed a shift in the peak of the curve towards lower frequencies as SAFIRE levels increased, as stated in the report by Macri et al. (2015) and used to validate the noise reduction [30]. Additionally, an increase in SAFIRE levels resulted in an increase in image smoothing.
Figure 2.
Relationship of NPS (HU2mm2) with spatial frequency (1/mm) obtained at different levels of IR algorithms for group standard dose.
Figure 2.
Relationship of NPS (HU2mm2) with spatial frequency (1/mm) obtained at different levels of IR algorithms for group standard dose.
3.2. Low Dose
The low dose group used an acquisition parameter of 100 kVp and a pitch of 0.9, whereas the standard uses a pitch of 0.75. The amount of pitch used distinguishes the low dose from the standard dose. Lower pitch allows for the creation of narrower image slices. As image slices become thinner, partial volume averaging becomes easier to solve; the LCD is then optimized.
Table 3 compares the values NPS, TTF, and CNR for different IR algorithm levels in the low dose group for both acrylic and ldpe inserts. As the IR increases, so does the NPS peak value (HU2 mm2). FBP has the highest peak value for NPS. Following that, as the IR level increased, the NPS spatial frequency decreased. It shows that as the IR level increases, image sharpness decreases. Aside from that, the TTF spatial frequency value for each insert differs from one another. The TTF for acrylic inserts varies as IR levels rise. When using the S3, the maximum TTF value is 1.36 0.30 mm-1. As the IR increases, so does the pattern for LDPE inserts. The greatest value when using S5 is 1.84 0.21 mm-1. When S5 is used, the value of CNR decreases while it increases for acrylic inserts. S3 has the highest CNR value when compared to FBP, S1, and S5. FBP and S1 have negative CNR values, indicating that there is less signal than noise in those two variables. As CNR increases, it should become easier to interpret because the image and background are more contrasted, making it easier to distinguish one from the other. In terms of LDPE inserts, it emphasizes how all findings are negative, indicating that noise outweighs signal. It is more difficult to distinguish between the area of interest and the background. Meanwhile, when S3 is used, it has the highest CNR value, which is equivalent to acrylic inserts.
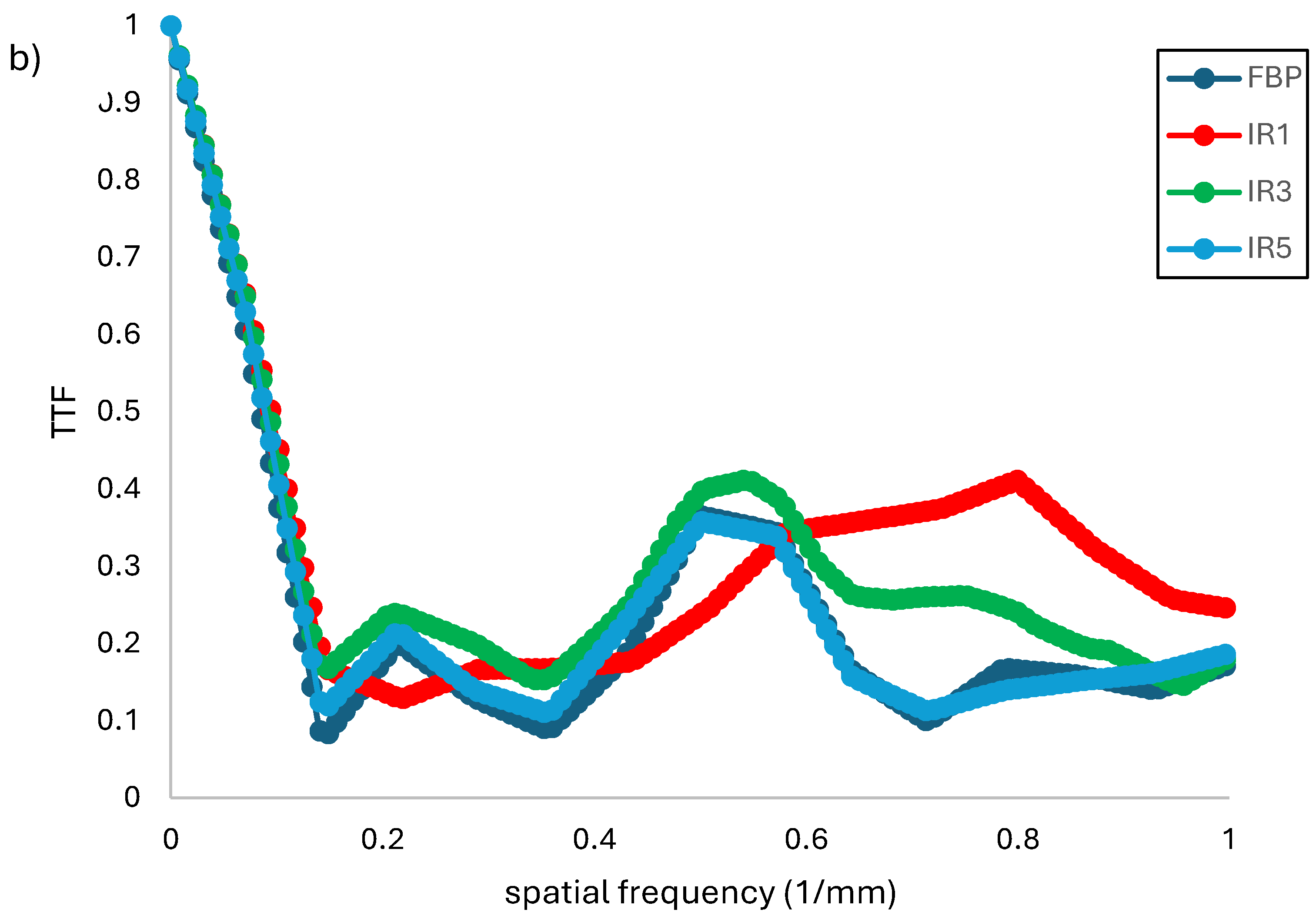
Figure 3(a) depicts the relationship between TTF, and spatial frequency obtained at various levels of IR algorithms for the low dose group using acrylic rod insert. As the IR increases, the TTF values decrease. TTF was lower with S3 at 50% with an acrylic insert than with S5 and FBP, which had a similar declining trend. In Figure 4.5, however, S3 TTF at 50% was greater than FBP when the ldpe insert was used. Despite the fact that LDPE insert pattern TTF degrades more slowly than acrylic insert. As previously stated, it could be due to the different background contrast. According to Greffier et al. (2019), one distinction between IR and FBP is that IR's spatial resolution is dependent on contrast and dose [27,31,32]. When S3 for different rod inserts produced contrasting results while using the same parameter but a different contrast for the region of interest, this dependence became more apparent.
Figure 3.
Relationship of TTF and spatial frequency (1/mm) obtained at different levels of IR algorithms for low dose group of (a) acrylic rod insert and (b) LDPE.
Figure 3.
Relationship of TTF and spatial frequency (1/mm) obtained at different levels of IR algorithms for low dose group of (a) acrylic rod insert and (b) LDPE.
As shown in Figure 4, the peak of the NPS decreases as the IR level increases. Additionally, the spatial frequency of the NPS shifts to a lower frequency when the IR levels change. This contrasts with Figure 2, which shows a constant decrease in spatial frequency. In Figure 3, the highest IR applied has the lowest spatial frequency, resulting in a less sharp image, but it also has the lowest NPS peak value, indicating a lower noise magnitude. Furthermore, when different reconstructions are compared, the spatial frequency of the NPS changes as the IR increases, moving towards lower frequencies. This suggests that the image quality in terms of noise texture is lower than it should be.
Figure 4.
Relationship of NPS (HU2mm2) with spatial frequency (1/mm) obtained at different levels of IR algorithms for low dose group.
Figure 4.
Relationship of NPS (HU2mm2) with spatial frequency (1/mm) obtained at different levels of IR algorithms for low dose group.
3.3. Ultra Low Dose
The ULD CT set has the same scan parameters as the SD CT set, except for the tube voltage. The lower kilovoltage of the ULD CT set increases the photoelectric interaction and attenuation level, resulting in an improved CNR value and LCD performance. However, if the other exposure parameters are not adjusted or the kilovoltage is too low, the noise level will rise. Table 4 shows the NPS, TTF, and CNR values for various IR algorithm levels for ULD. As the IR increases, the peak NPS value decreases, with S5 having the lowest peak NPS value compared to FBP. The spatial frequency of the NPS also changes, increasing from FBP to S1, but decreasing from S3 to S5. The image in S1 has the highest spatial frequency, giving it a smoother texture than the other images. Conversely, S5 has the lowest frequency, making the image texture blurrier. The TTF spatial frequency decreases by 50% as the IR level increases in both acrylic and LDPE inserts, with FBP having the highest TTF spatial frequency value.
IR 4's ability to detect lesions proved to be the best in our opinion. The following study was then conducted, and to avoid ruling out the possibility of IR strength 5 being superior, IR 5 was included in addition to IR strengths 3 and 4. Furthermore, the CNR value for the acrylic insert is always negative and decreases as the IR increases. According to Macri (2016), CNR for LDCT and ULDCT was significantly reduced, whereas IR successfully increased these values [30]. The LDPE insert is relevant because it depicts the rising CNR value as IR increases.
The amount of contrast in the rod inserts affects both the TTF values and the IR algorithm modification. Figure 5(a) and Figure 5(b) demonstrate the contrast between the two insert rods for acrylic and LDPE, respectively, which is reflected in the difference in TTF spatial frequency. The two inserts follow a similar pattern, with S5 having the lowest TTF value and FBP having the highest. Rotzinger et al. (2018) found that, excluding low-contrast objects, ASiR-V had spatial resolution comparable to or slightly better than FBP [33]. When the ASiR-V level was increased, low contrast objects resulted in a significant loss of spatial resolution when compared to FBP. This is consistent with Paruccini et al. (2017)'s previous work, which used TTFs to adjust low-contrast spatial resolution with iDose and IMR [34]. Surprisingly, they also discovered that as iDose and IMR levels increased, so did quantitative image blur. The spatial frequency of TTF at 50% did not vary with dose level but decreased as the ASIR percentage increased.
In comparison to Figure 2 and Figure 4, Figure 6 shows a less dramatic trend in NPS peak values. This is because lower energy photons are absorbed as they pass through dense areas, resulting in a higher average beam energy. As a result, an NPS peak of 80 kVp is more likely than a tube voltage of 100 kVp. Additionally, the spatial frequency of the NPS is not balanced, with S1 having a higher frequency than S3 and S5.
5. Conclusion
This study aims to evaluate the effects of low dose CT acquisition parameters and iterative reconstruction on image quality. Retrospective patients are used to assess the diagnostic performance, as they are less likely to show additional image quality measurements than using a phantom. The TTF and CNR are the most important performance measures for protocol optimization, as they focus on improving the contrast and spatial resolution for the background and region of interest. It is essential to adjust the acquisition parameters correctly, as a lower tube voltage can reduce the CNR values. The IR algorithm also affects image quality by decreasing the magnitude of NPS noise, which can have a negative impact on the detectability of the region of interest. The findings of this study will be beneficial for further procedure improvements.
Author Contributions
Conceptualization, MKAK; Formal analysis, EH; Investigation, DSAM; Project administration, MKAK and NAM; Resources, HHH; Supervision, MKAK and MMAK; Validation, MJI and NAM; Visualization, MKAK; Writing – original draft, DSAM and EH; Writing – review & editing, MKAK.
Institutional Review Board Statement
Not relevant.
Informed Consent Statement
Not applicable.
Data Availability Statement
All relevant data are included in the study.
Acknowledgments
This research was funded by Universiti Putra Malaysia under Geran Berimpak Putra (GP/GBP-FS 9704400).
Conflicts of Interest
The authors disclose that they have no conflict of interests.
References
- Siang, K.C.; Kok, C.; John, M.; Cth, F. A Review of Lung Cancer Research in Malaysia. Med. J. Malaysia 2016, 71, 70–78. [Google Scholar]
- Diederich, S.; Wormanns, D. Impact of low-dose CT on lung cancer screening. Lung Cancer 2004, 45. [Google Scholar] [CrossRef]
- Melamed, M.R. Lung cancer screening results in the National Cancer Institute New York Study. Cancer 2000, 89, 2356–2362. [Google Scholar] [CrossRef]
- Harun, H.H.; Abdul Karim, M.K.; Muhammad, N.A.; Awang Kechik, M.M.; Chew, M.T.; Talib, Z.A. Task-based assessment on various optimization protocols of computed tomography Pulmonary Angiography examination. Radiat. Phys. Chem. 2021, 188, 109692. [Google Scholar] [CrossRef]
- Kalender, W. X-ray computed tomography. Phys. Med. Biol. 2006. [Google Scholar] [CrossRef]
- Brenner, D.J. Minimising medically unwarranted computed tomography scans. Ann. ICRP 2012, 41, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Kalender, W. a; Buchenau, S.; Deak, P.; Kellermeier, M.; Langner, O.; van Straten, M.; Vollmar, S.; Wilharm, S. Technical approaches to the optimisation of CT. Phys. Medica 2008, 24, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Huda, W. Computing patient specific effective doses and radiation risks in CT. Phys. Medica 2012, 28, 333. [Google Scholar] [CrossRef]
- Papadakis, A.E.; Damilakis, J. Automatic Tube Current Modulation and Tube Voltage Selection in Pediatric Computed Tomography: A Phantom Study on Radiation Dose and Image Quality. Invest. Radiol. 2019, 54, 265–272. [Google Scholar] [CrossRef]
- Chang, Y.L.; Lee, C.M.; Hsiao, W.T.; Hsu, F.Y.; Kuo, M.J.; Chiu, J.H. Dose evaluation of multi-slice CT for different parameters in chest examinations using TLD method. Radiat. Meas. 2010, 45, 701–703. [Google Scholar] [CrossRef]
- Huda, W.; Sterzik, A.; Tipnis, S.; Schoepf, U.J. Organ doses to adult patients for chest CT. Med. Phys. 2010, 37, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, N.A.; Kayun, Z.; Abu Hassan, H.; Wong, J.H.D.; Ng, K.H.; Karim, M.K.A. Evaluation of Organ Dose and Image Quality Metrics of Pediatric CT Chest-Abdomen-Pelvis (CAP) Examination: An Anthropomorphic Phantom Study. Appl. Sci. 2021, 11, 2047. [Google Scholar] [CrossRef]
- Solomon, J.; Ba, A.; Bochud, F.; Samei, E. Comparison of low-contrast detectability between two CT reconstruction algorithms using voxel-based 3D printed textured phantoms. Med. Phys. 2016, 43, 6497–6506. [Google Scholar] [CrossRef]
- Adibah Yusof, N.A.; Abdul Karim, M.K.; Asikin, N.M.; Paiman, S.; Awang Kechik, M.M.; Abdul Rahman, M.A.; Noor, N.M. CT reconstruction algorithm and low contrast detectability of phantom study: a systematic review and meta-analysis. Curr. Med. Imaging Former. Curr. Med. Imaging Rev. 2022, 18, 1–9. [Google Scholar] [CrossRef]
- Lee, T.Y.; Chhem, R.K. Impact of new technologies on dose reduction in CT. Eur. J. Radiol. 2010, 76, 28–35. [Google Scholar] [CrossRef]
- Desai, G.S.; Thabet, A.; Elias, A.Y.A.; Sahani, D. V Comparative assessment of three image reconstruction techniques for image quality and radiation dose in patients undergoing abdominopelvic multidetector CT examinations. Br. J. Radiol. 2013, 86, 20120161–20120161. [Google Scholar] [CrossRef]
- Sumitani, M.; Takifuji, N.; Nanjyo, S.; Imahashi, Y.; Kiyota, H.; Takeda, K.; Yamamoto, R.; Tada, H. Clinical relevance of sputum cytology and chest X-ray in patients with suspected lung tumors. Intern. Med. 2008, 47, 1199–1205. [Google Scholar] [CrossRef]
- Harun, H.H.; Abdul Karim, M.K.; Abbas, Z.; Abdul Rahman, M.A.; Sabarudin, A.; Ng, K.H. Association of Radiation Doses and Cancer Risks from CT Pulmonary Angiography Examinations in Relation to Body Diameter. Diagnostics 2020, 10, 681. [Google Scholar] [CrossRef]
- Kawashima, H.; Ichikawa, K.; Matsubara, K.; Nagata, H.; Takata, T.; Kobayashi, S. Quality evaluation of image-based iterative reconstruction for CT: Comparison with hybrid iterative reconstruction. J. Appl. Clin. Med. Phys. 2019, 20, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Nyman, U.; Bjorkdahl, P.; Olsson, M.L.; Gunnarsson, M.; Goldman, B. Low-dose radiation with 80-kVp computed tomography to diagnose pulmonary embolism: A feasibility study. Acta radiol. 2012, 53, 1004–1013. [Google Scholar] [CrossRef]
- Liu, W.; Zhu, Y.; Tang, L.; Zhu, X.; Xu, Y.; Yang, G. Effect of various environments and computed tomography scanning parameters on renal volume measurements in vitro: A phantom study. Exp. Ther. Med. 2016, 12, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Davidson, R.; Alsleem, H.; Floor, M.; van der Burght, R. A new image quality measure in CT: Feasibility of a contrast-detail measurement method. Radiography 2016, 22, 274–281. [Google Scholar]
- Yu, L.; Fletcher, J.G.; Shiung, M.; Thomas, K.B.; Matsumoto, J.M.; Zingula, S.N.; McCollough, C.H. Radiation dose reduction in pediatric body CT using iterative reconstruction and a novel image-based denoising method. Am. J. Roentgenol. 2015, 205, 1026–1037. [Google Scholar] [CrossRef] [PubMed]
- Sookpeng, S.; Martin, C.J.; Gentle, D.J. Investigation of the influence of image reconstruction filter and scan parameters on operation of automatic tube current modulation systems for different CT scanners. Radiat. Prot. Dosimetry 2015, 163, 521–530. [Google Scholar] [PubMed]
- Kayun, Z.; Karim, M.K.A.A.; Muhammad, N.A.; Aljewaw, O.B.; Chew, M.T.; Harun, H.H.; Tsuey, C.M.; Harun, H.H. Implication of applying iterative reconstruction on Low Contrast Detectability in CT brain examination. Radiat. Phys. Chem. 2021, 188, 109676. [Google Scholar] [CrossRef]
- Gulliksrud, K.; Stokke, C.; Trægde Martinsen, A.C. How to measure CT image quality: Variations in CT-numbers, uniformity and low contrast resolution for a CT quality assurance phantom. Phys. Medica 2014, 30, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Greffier, J.; Frandon, J.; Larbi, A.; Beregi, J.P.; Pereira, F. CT iterative reconstruction algorithms: a task-based image quality assessment. Eur. Radiol. 2020, 30, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Group, A.T. Performance Evaluation of Computed Tomography Systems; 2019; ISBN 9781936366699. [Google Scholar]
- Racine, D.; Viry, A.; Becce, F.; Schmidt, S.; Ba, A.; Bochud, F.O.; Edyvean, S.; Schegerer, A.; Verdun, F.R. Objective comparison of high-contrast spatial resolution and low-contrast detectability for various clinical protocols on multiple CT scanners. Med. Phys. 2017, 44, e153–e163. [Google Scholar] [CrossRef]
- Macri, F.; Greffier, J.; Pereira, F.R.; Mandoul, C.; Khasanova, E.; Gualdi, G.; Beregi, J.P. Ultra-low-dose chest CT with iterative reconstruction does not alter anatomical image quality. Diagn. Interv. Imaging 2016, 97, 1131–1140. [Google Scholar] [CrossRef]
- Greffier, J.; Pereira, F.; Hamard, A.; Addala, T.; Beregi, J.P.; Frandon, J. Effect of tin filter-based spectral shaping CT on image quality and radiation dose for routine use on ultralow-dose CT protocols: A phantom study. Diagn. Interv. Imaging 2020, 101, 373–381. [Google Scholar]
- Richard, S.; Husarik, D.B.; Yadava, G.; Murphy, S.N.; Samei, E. Towards task-based assessment of CT performance: System and object MTF across different reconstruction algorithms. Med. Phys. 2012, 39, 4115–4122. [Google Scholar] [CrossRef] [PubMed]
- Rotzinger, D.C.; Racine, D.; Beigelman-Aubry, C.; Alfudhili, K.M.; Keller, N.; Monnin, P.; Verdun, F.R.; Becce, F. Task-Based Model Observer Assessment of A Partial Model-Based Iterative Reconstruction Algorithm in Thoracic Oncologic Multidetector CT. Sci. Rep. 2018, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Paruccini, N.; Villa, R.; Pasquali, C.; Spadavecchia, C.; Baglivi, A.; Crespi, A. Evaluation of a commercial Model Based Iterative reconstruction algorithm in computed tomography. Phys. Medica 2017, 41, 58–70. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
CATPHAN®-600 was positioned based on the standard CT lung.
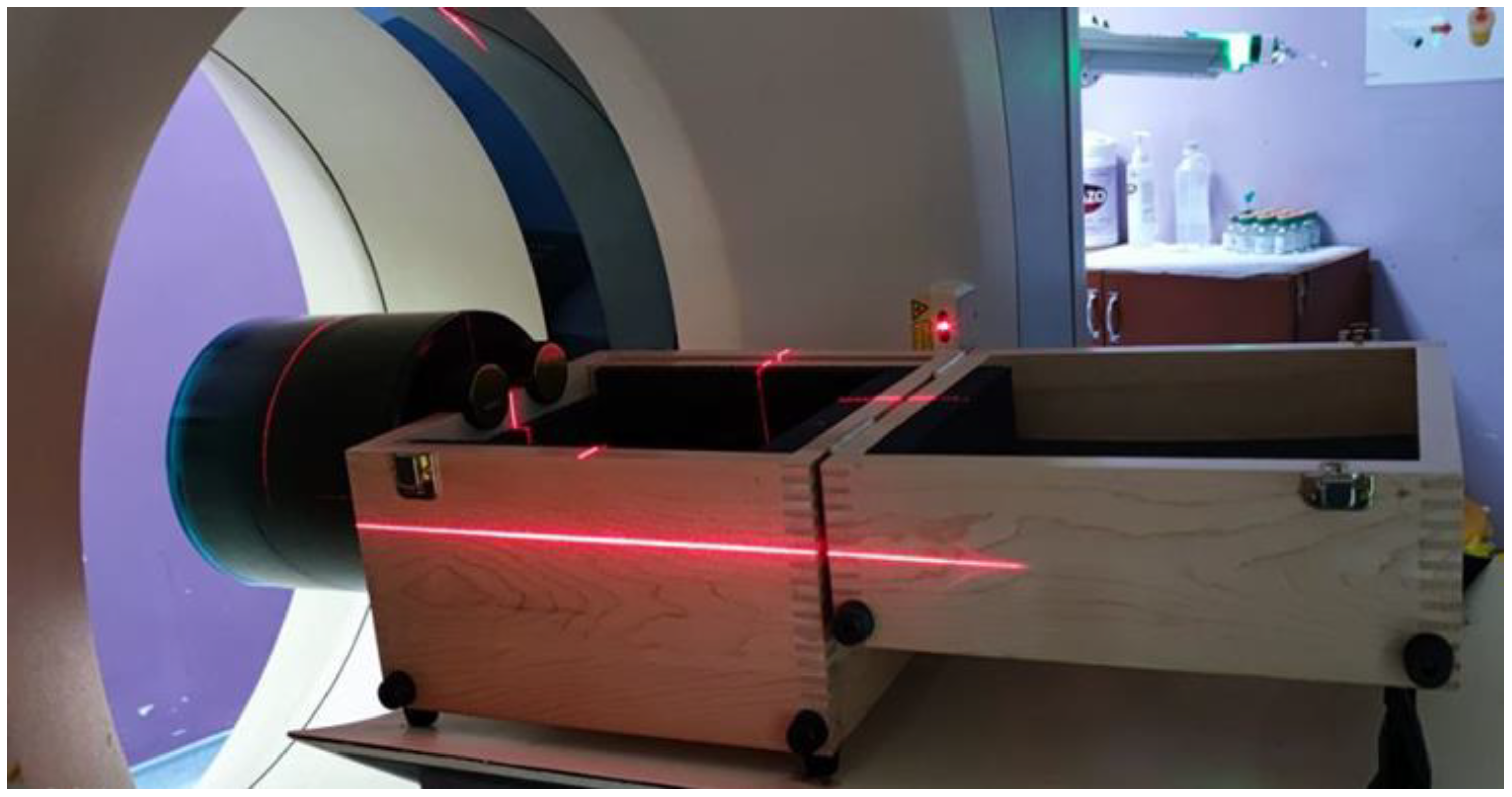
Figure 5.
Relationship of TTF and spatial frequency (1/mm) obtained at different levels of IR algorithms for group ultra-low dose of (a) acrylic rod insert and (b)LDPE.
Figure 5.
Relationship of TTF and spatial frequency (1/mm) obtained at different levels of IR algorithms for group ultra-low dose of (a) acrylic rod insert and (b)LDPE.
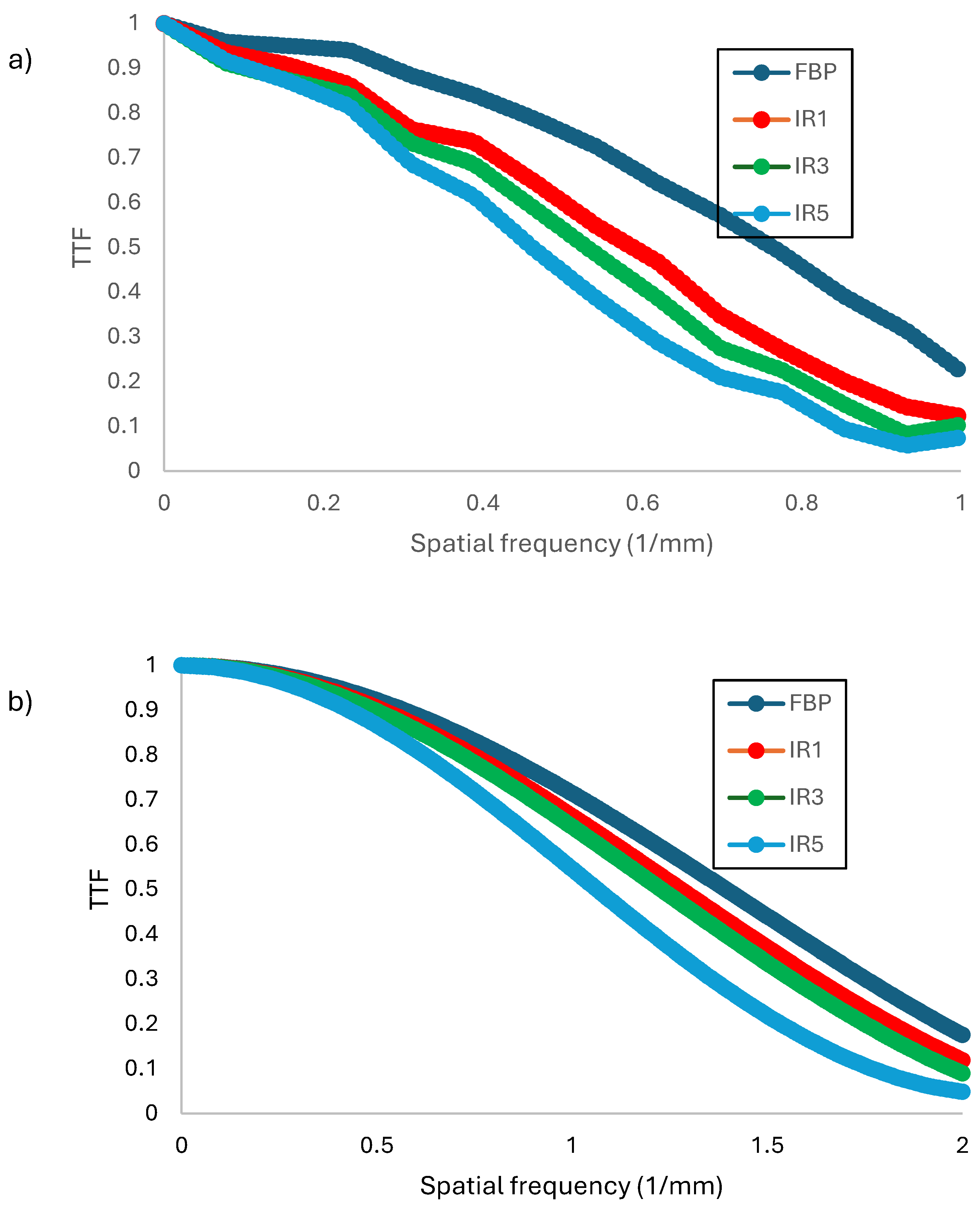
Figure 4.
9 Relationship of NPS (HU2mm2) with spatial frequency (1/mm) obtained at different levels of IR algorithms for ultra-low dose group.
Figure 4.
9 Relationship of NPS (HU2mm2) with spatial frequency (1/mm) obtained at different levels of IR algorithms for ultra-low dose group.
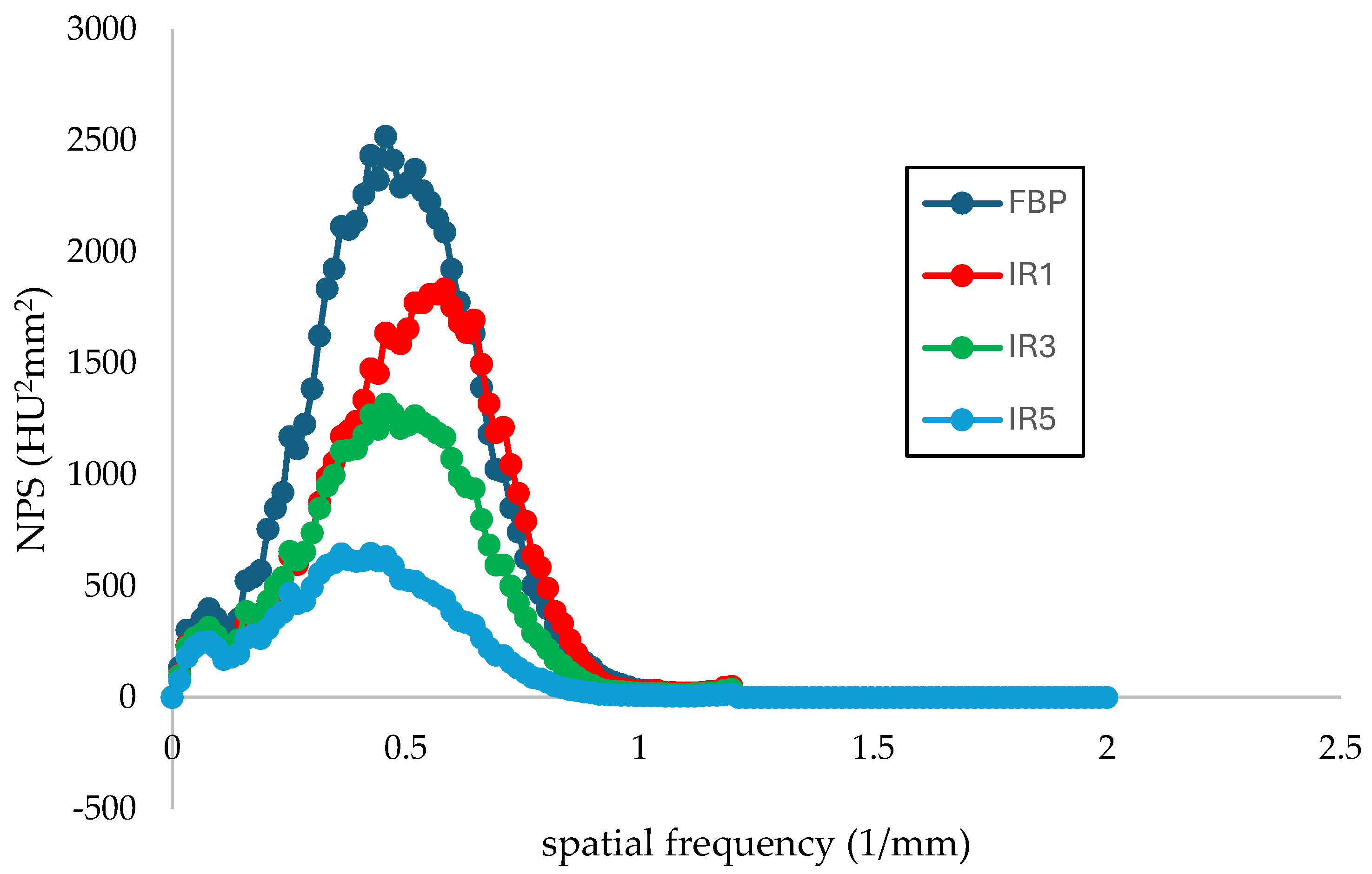

Table 1.
Data acquisition settings for phantom scanning.
| PARAMETER | Standard | Low dose | Ultra-low dose | |||||||||
| SDCT FBP | SDCT IR low | SDCT IR med | SDCT IR high | LDCT FBP | LDCT IR low | LDCT IR med | LDCT IR high | ULDCT FBP | ULDCT IR low | ULDCT IR med | ULDCT IR high | |
| kV | 100 | 100 | 80 | |||||||||
| mA | xyz-modulation | xyz-modulation | xyz-modulation | |||||||||
| Gantry rotation (s) | 0.33 | 0.33 | 0.33 | |||||||||
| Detector collimation (mm) | 0.6 | 0.6 | 0.6 | |||||||||
| Pitch | 0.75 | 0.9 | 0.9 | |||||||||
| Slice Thickness (mm) | 5 | 5 | 5 | |||||||||
| Kernel | B80f | I70f | I70f | I70f | B80f | I70f | I70f | I70f | B80f | I70f | I70f | I70f |
| Image Reconstructor | FBP | S1 | S3 | S5 | FBP | S1 | S3 | S5 | FBP | S1 | S3 | S5 |
Table 2.
A comparison of the value NPS, TTF, CNR for different IR algorithm levels for standard dose group.
Table 2.
A comparison of the value NPS, TTF, CNR for different IR algorithm levels for standard dose group.
| Variable | Rods Insert | IR algorithm levels | |||
| FBP | S1 | S3 | S5 | ||
| NPS peak value (HU2 mm2) |
n. a | 3965.32 ± 1128.10 | 2620.17± 837.44 | 2047.20± 621.09 |
925.64± 300.16 |
| NPS spatial frequency | n. a | 0.44 ± 0.58 | 0.58 ± 0.58 | 0.44 ± 0.58 | 0.43 ± 0.58 |
| TTF50% spatial frequency (1/mm) | acrylic | 1.29 ± 0.26 | 1.05 ± 0.55 | 0.86 ± 0.34 | 0.73 ± 0.10 |
| LDPE | 0.89 ± 0.63 | 0.77 ± 0.59 | 0.88 ± 0.51 | 0.90 ± 0.63 | |
| CNR | acrylic | -1.38 ± 1.80 | 0.17 ± 2.43 | 1.73 ± 0.76 | 4.19 ± 2.31 |
| LDPE | 0.36 ± 0.12 | -0.07 ± 0.60 | -0.44 ± 0.23 | -0.01 ± 0.29 | |
Table 3.
A comparison of the value NPS, TTF, CNR for different IR algorithm levels for low dose group.
Table 3.
A comparison of the value NPS, TTF, CNR for different IR algorithm levels for low dose group.
| Variable | Rods Insert | IR algorithm levels | |||
| FBP | S1 | S3 | S5 | ||
| NPS peak value (HU2 mm2) | n. a | 4257.87 ± 1128.23 | 2660.96 ± 824.32 | 2210.70 ± 626.64 | 1086.75 ± 313.25 |
| NPS spatial frequency | n. a | 0.74 ± 0.58 | 0.52 ± 0.58 | 0.44 ± 0.58 | 0.44 ± 0.58 |
| TTF spatial frequency | Acrylic | 1.31 ± 0.31 | 0.91 ± 0.40 | 1.36 ± 0.30 | 1.27 ± 0.92 |
| LDPE | 0.09 | 1.84 ± 0.21 | 1.32 ± 1.07 | 0.09 | |
| CNR | Acrylic | -2.60 ± 2.50 | -0.63 ± 2.93 | 2.15 ± 3.51 | 0.46 ± 5.84 |
| LDPE | -0.93 | -0.85 ± 0.05 | -0.59 ± 0.15 | -1.04 | |
Table 4.
A comparison of the value NPS, TTF, CNR for different IR algorithm levels for ultra-low dose group.
Table 4.
A comparison of the value NPS, TTF, CNR for different IR algorithm levels for ultra-low dose group.
| Variable | Rods Insert | IR algorithm levels | |||
| FBP | S1 | S3 | S5 | ||
| NPS peak value (HU) | n. a | 2519.34 ± 797.27 | 1834.36 ± 592.07 | 1316.63 ± 427.47 | 618.56 ±209.76 |
| NPS spatial frequency (1/mm) | n. a | 0.46 ± 0.58 | 0.58 ±0.58 | 0.46 ±0.58 | 0.38 ± 0.58 |
| TTF spatial frequency (f50) (1/mm) | acrylic | 1.63 ± 0.02 | 0.99 ±0.70 | 0.54 ±0.07 | 0.46 ± 0.04 |
| LDPE | 1.39 ± 0.05 | 1.28 | 1.23 | 1.06 | |
| CNR | acrylic | -1.23 ± 0.65 | -1.31 ± 0.14 | -1.77 ± 0.39 | -2.50 ± 0.48 |
| LDPE | 2.04 ± 0.06 | 2.02 | 2.61 | 4.06 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



