
Submitted:
08 May 2024
Posted:
08 May 2024
You are already at the latest version
Abstract
This research aimed to study and compare prevalence of work-related musculoskeletal (MSK) problem and perceived discomfort among port crane operators consisting of quay and rubber tyred gantry (RTG) cranes working in the Laem Chabang Deep-sea Port, Thailand. Direct interviews for a cross-sectional analysis was selected for this unique job with a small amount of sample size. A standardized modified version of the Nordic Musculoskeletal Questionnaire (NMQ) was lunched for 26 male participants, consisting of 11 quay and 15 RTG, where a priori power analysis using G*Power suggested the minimum as 24 for the hypothesis test. Socio-demographic characteristics showed no significant difference among them. The NMQ revealed lower back as the highest prevalent body part (76.9%) followed by neck, shoulders and upper back at the same percentage (23.1%) for all port crane group, with up to 96.2% reporting MSK problem over the past 12 months. And Borg scale rating, assessing the perceived discomfort, revealed lower back with the highest score (2.38) followed by upper back (0.65), shoulders (0.54) and neck (0.5). Remarkably, the comparation between the quey and RTG crane operators on the MSK prevalence (χ2 test) and perceived discomfort levels (Kruskal-Wallis test), regarding different 9 body parts, revealed a significant difference between the two on upper back with quay crane having more problem than the RTG at p < 0.05. while the rest of them were mainly in the same direction. MSK contributors such as: working awkward posture, mental stress, height, trolley distance and vibration are considerably the main causes of this. However, the larger in scale of exposure to those for the quey crane compared to the RTG might have led to the distinguishing MSK problem found in this study which require thoroughly deliberation for the particular solutions.
Keywords:
port crane operators
; quay crane
; rubber tyred gantry crane
; work-related musculoskeletal problem
; perceived discomfort
1. Introduction
Maritime shipping industry plays an important function in an international trade. Reportedly around 80% of the overall volume had been achieved by this sector [1]. For Thailand, up to 90% of imports and exports were made via ports cargo shipments [2]. And over the past decade, a statistic from 2008 to 2018 reveals that an average of 8,890,500.000 Twenty foot Equivalent Unit (TEU) passed through Thailand’s container ports per year, with 11,185,200.000 TEU as the highest record in the year 2018 [3].
Containerization allows goods transportations across sea and land efficiently. Container port terminals perform an essential role in sea-land trading chains. For the import of goods processes, the containers from the vessels will be lifted and placed to the trailer trucks by large sized terminal cranes so called quay cranes, working just next to the container ship at the port terminal. These containers will be transshipped to the stack area. In this process, all the containers allocation are achieved by relatively smaller sized cranes named Rubber Tyred Gantry container cranes or shorten as the RTG. Their job is to handle the inbound or outbound containers temporarily stored in the shipyards, normally in the form of stacked containers [4,5].
In general, the container cranes’ control station are placed in the cabin suspended above the terminal ground at around 30-40 m. height [6]. In order to complete the task, the container crane operators have to perform the task in static and non-neutral sitting postures. It is done through leaning forward to gain the view below via looking straight through the cabin’s glass floor. Beside that, they also have to work for a long session at about 4-6 hours each [7,8].
Work-related musculoskeletal disorders (WMSDs) remark the health problem that involves musculoskeletal system including: muscles, nerves, blood vessels, ligaments and tendons [9]. It becomes the most common work-related health problem in many regions in which in Asia-Pacific, about 12 – 45% of its general population was found being in this trouble [10].
Container crane operators are among those at risk of the WMSDs. So far, it had proved hardly to find studies that compare both Quay and RTG cranes together. This research aimed to study the prevalence of MSK problem and discomfort level among the container crane operators including the quay and RTG crane, working in Thailand’s special economic zone.
2. Materials and Methods
2.1. Study Design
Research’s study design was achieved by a cross-sectional analysis conducted on 2 different types of container crane operators including quay and RTG. Laem Chabang international deep-sea port was selected for this study. This is due to its size which ranks as the nation biggest seaport. Moreover, it had a world class reputation as the 21st world’s biggest maritime port with the capacity of 8.07 million TEUs handled in the year 2018 [11,12].
2.2. Participants
Crane operators were recruited voluntarily form the studied deep seaport, where 9 unites of quay cranes and 27 units of RTG were deployed across 4 piers at the moment of the study [13]. The inclusion criteria consisted of just male gender with at least 1 year experience in this job, having no historic medical record for the musculoskeletal disorder and willingly agreed to join the research project via signing the informed consent. Only twenty-six met the criteria and participated in the study. This number was still adequate for the hypothesis test since a priori power analysis using G*Power version 3.1.9.7 [14], in order to achieve 80% power for detecting effect size = 0.6 and at a significance criterion of α = .05, suggested that the minimum sample size was 24.
2.3. Questionnaires and Data Collection
Data collection was done using a standardized modified version of Nordic Musculoskeletal Questionnaire (NMQ) [15], which was translated into Thai language by authors. The NMQ was utilized in the investigation as the tool acquiring for the prevalence of self-reported musculoskeletal (MSK) problem over 9 body parts. Alongside, a perceived discomfort survey was also launched with Borg CR10 scale [16,17]. All information obtained was achieved via direct interviews, conducting by research team’s experts with fully extensive explanations provided when required.
2.4. Data and Statistical Analysis
The IBM SPSS version 20.0 (IBM Corp., USA) was utilized in a statistical analysis. Descriptive statistics were used to figure for the sociodemographic and anthropometric features. The Chi-square test implementing Fisher’s exact test was used to validate the similarity in statistics among both groups for all studied parameters. Meanwhile, the Kruskal-Wallis test was employed to verify statistical difference among the two for the perceived discomfort levels across all 9 body parts. All statistics significances were set at p = 0.05.
3. Results
3.1. Socio-Demographic Characteristics
All port cranes operators group (a combination between quay and RTG cranes) in this study had an average age at 42.865 years old (Quay = 43.864; RTG = 42.133) with the minimum age at 28.3 years old (Quay = 28.3; RTG = 36.0) and the maximum age at 58.3 years old (Quay = 58.3; RTG = 54.0). Calculating via Body Mass Index (BMI), pre-obese stage was found the highest prevalence for all of the studied groups: all port (35), quay (15) and the RTG crane (19). The result from Chi square test showed that quay and RTG crane had no difference in statistics across all socio-demographic characteristics. Details about the demographic information can be presented in Table 1.
3.2. Self-Reported Anthropometric MSK Problem Prevalence
For all port cranes operators group, lower back was the body part showing the most prevalence of MSK problem at 76.92 percent. Neck, shoulder and upper back followed far behind at the same percentage as 23.08. If considering separately, quay crane had the lower back as the most prevalence at 34.62 percent and the upper back for the second at 19.23 percent. The RTG also had the lower back as the most prevalence at 42.31 percent and shoulder as the second at 15.38 percent. The least affected body part belonged to elbows, this was for all groups with 3.85, 0 and 3.85 percent for all port cranes, quay and the RTG respectively. Information about these can be showed in Figure 1.
3.3. Prevalence of Self-Reported MSK Problem during the Last 12-Months and Past 7 Days
The results showed that none of them reported the existence of MSK problem during the last 7 days. Almost the entire number of the container cranes operators reported the existence of MSK problem during the last 12 months, with as much as 96% for the all port cranes operators group, 100% for quay and 93% for the RTG. By means of this, only 4% for all port cranes operators group reported none MSK problem during the last 12-months and 7% for the RTG, as showed graphically in Figure 2.
3.4. Perceived Discomfort (Borg CR10 Scale)
Perceived discomfort levels were represented by a 10-point Borg scale with score ranging from 0 (not at all) to 10 (maximal exertion). The results showed that lower back was remarkably the most affected body part for all port cranes group with the scale of 2.38, as well as for the quay and RTG cranes with the scales of 2.55 and 2.27 respectively. The second most prevalent for all port cranes group was upper back at 0.65 followed by the shoulders and neck at 0.54 and 0.5 respectively. Considering separately on the quay crane, upper back showed the second most problematic at 1.45, followed by neck at 0.36. For the RTG, the second most was in turn a shoulder at 0.73, followed by the neck at 0.6, as shown all the details in Figure 3.
3.5. MSK Prevalence and Perceived Discomfort Levels among Quay and RTG Crane Operators Regarding Different Body Parts
Among both groups, out of nine body parts, the results showed a significant difference in statistics on upper back for the MSK prevalence and perceived discomfort levels. The noticeable point is that it occurred in the way that quay crane operators developed higher MSK problem than in the RTG crane at p-value = 0.032 and 0.015 for the MSK prevalence and perceived discomfort scores respectively. All the detailed information is shown in Table 2.
4. Discussion
Quay and RTG crane operators are considerably one of the key links to the success of containerization in maritime transportation. This research once again revealed that lower back was the most prevalent MSK problem with as much as 76.92% for all port cranes operators group, which acted as a representative of all port cranes combined. And apparently, it was followed by a group of the second most prevalent MSK problem with the same amount of 23.08% on the body parts, consisting of: neck, shoulders and upper back.
Working posture could be one of the key contributors for this problem, since quay and RTG crane operators are required to work in prolonged static non-neutral sitting postures. In order to maneuver the containers being loaded/unloaded down below, they have to lean their trunk forward unneutrally, to gain the most perfect working visibility, over a relatively long period of time. This awkward operating postures pose a potential risk in working since the ergonomics assessment tool, Rapid Upper Limb Assessment (RULA), previously assessing by Mohd Azlan, et al. (2019), revealed the score up to 5-6; which means further investigation and change of work procedure are needed [18].
To achieve this task, trunk muscles, particularly lower back, have to be largely and constantly employed over an operating period. In reality, the lower back would not work alone, it must be closely cooperated with others posture-related muscles, which seemingly link to a set of the second most problematic body parts found in this study. This is to maintain the stabilization of the spine and by working in this condition for about 4 hours per shift for each session, it could dangerously overstress all the employed trunk muscles for both types of the crane [7].
Beside this, vibration which mostly occurs in the cabin during the operation also has a great latency to increasing the scale of the MSK problem to the level that even worse [19,20,21,22]. As known that there are two classifications of the vibration exposure, the whole body vibration (WBV) and the hand-arm vibration (HAV), in this case WBV seemed to be the main cause of this issue since all the vibration was transmitted to the entire body via either seat or feet [23]. A study from Muhammad Azmi, et al. (2017) revealed that the measured daily exposure value A(8) of WBV occurring in these types of crane was about 0.24 m/s2 to 0.42 m/s2, which slightly lower than a limit value of 0.5 m/s2, declared by the ISO 2631-1 and EN2002/44/EC. Even though the value still lower than the standard, it occurred with the maximum range of about 84% of its threshold and being exposed to it over a long period of time, plus with the high postural stress due to an extremely awkward posture in which this could potentially increase the risk of LBP very easily [24,25,26]. This is in line with other found studies reporting that crane operators who exposed to WBV for a period longer than 5 years were more at risk to hospitalization or even permanent work disabilities due to the back disorders, and in particular for the lumbar disc herniation, than a control group [27,28].
If considering by types of the crane, the result from the quay crane is also consistent with studies from Mohd Azlan et al. (2019) and Z.A. Kadir et al. (2015) who conducted the research, surveying MSK problem using NMQ among the quay crane operators in Malaysia’s seaport, and they found that lower back showed the most problematic body part [18,29]. The similar results were also derived from Maryam Nourollahi-Darabad et al. (2018), they achieved the research assessing the prevalence of musculoskeletal symptoms using Nordic questionnaire among Rubber Tired Gantry (RTG) crane operators in Iran. Although not exactly the same type of the crane being discussed, the RTG crane largely requires similar working characteristics of the quay crane. They also reported the lower back was the most prevalent MSK problem with 85.8% followed by neck (75.8%), knee (68.3%) and shoulders (63.3%) respectively [30].
In the same direction of the results from the self-reported MSK problem, it is not surprising for the perceived discomfort scales obtained from an all port crane operators group that, lower back showed the highest score at 2.38 which means they perceived discomfort intensity between weak (2) and moderate (3) [31]. The lower back was again followed far behind by a bunch of the second most problematic body parts consisting of: upper back (0.65), shoulders (0.54) and neck (0.5) respectively, by which the score of 0.5 means extremely weak or just noticeable and 1 means very weak [31].
Considering the second most problematic group of the muscles, quay crane operators experienced more trouble than the RTG ones, evidencing through the statistics (at p-value = 0.05) for both Chi-square test (for the MSK problem prevalence) and the Kruskal-Wallis test (for the perceived discomfort). The feasible causes that could contribute to this might be from many reasonable factors. Both types of the crane operators have to adopt very similar working postures. They had to maintain an awkward static loading posture with the trunk flexing as much as 30 – 40 degrees forwards and 60 – 70 degrees forwards for the neck, as demonstrated in picture 4(a) for quey crane and 4(b) for the RTG crane [32].
Working with this extreme non-neutral siting posture seems to be very much problematic enough, beside this, their arms and hands still had to be used in controlling the container movement with extreme precision all the time. Operating in this condition, from the height of about 30 – 40 meter from the working surface and with no room for error allowed, requires a constant muscular work load [33]. With all these circumstances combined, spine’s bones, discs, muscles, ligaments, and other soft tissues are placed under the relatively high tension. As a result, it consequently generates high pressure on both physical and mental stresses which eventually leads to the fatigue that could develop into pain and MSDs respectively in long run [34].
For a RTG cranes, they generally have the height and trolley length of about 12 - 21 and 15 – 30 m. respectively, as demonstrated in the Figure 4(b). If compared with the quay crane, the RTG cranes are clearly smaller in size. The quay crane’s working station or cabin is higher and also having a longer travelling distance, with as much as about 45 – 55 m long the RTG crane [35]. All of these facts combined, thereby, it could lead to a greater vibration generated as well as a longer exposure time, due to the longer in distance of travelling, that could contribute to the more MSK problems found on the quey crane compared to the RTG one.
Low frequency vibrations transmitted to the cabin are generated by quay crane while travelling backward and forward passing boom junctions with significant accelerate and decelerate movement [32]. Interactively, the greater effects on physical and mental stresses in the quay crane compared to the RTG could have led to the notable results finding in this study. Consequently, it suggests that quey crane operators statistically developed more problem on the upper back than in the RTG ones, while the rest of them seemed to advance in the same direction.
The upper back in general word is medically referred to the thoracic spine which positions in the middle between cervical spine (neck) and lumbar spine (lower back). The upper back functions as if a tree trunk that acts like a main structure connecting other skeletons and muscles together. Furthermore, it also plays a key role in maintaining our upper body upright [36]. When compared with its neighboring muscles: cervical spine (neck) and lumbar spine (lower back), the upper back is relatively more immobile; and as a result, pain over upper back was less reported than the lower back and neck respectively. But when it does occur, a long-term poor awkward posture which definitely is an extensive contributor in this work, particularly in the quey crane, or an injury over the thoracic spine’s sturdiness could be the major possible causes [37].
The obvious appearance of MSK symptoms over 12-months (96.2%) rather than a 7 days period in this study is affirmatively in line with many studies conducting in the crane operators (with the rate more than 70%) and with lower back as the most prevalent [29,38]. This could imply and link to the long-term chronic problem which could have led to the development of the MSDs in long run [39]. This is in accordance with what found by Mohd Azlan (2017), he concluded that quay crane operators who exposed to those working conditions for more than 5 years were 7 time more likely experiencing symptoms leading to stop workings due to the LBP [40].
There were no statistically significant associations found between independence factors (age, BMI and work experience) and both of the studied contributions (occurrence of MSK problem and the perceived discomfort) across all 9 body parts. This could have suggested that the operation tasks of port crane could have had potential contributions to whoever working in this job, particularly for employees working over a long period of time. Supported by so many evidences, lower back was clearly the most troubled body part, along with the second most affected ones: upper back, shoulders and neck reported in this study. This finding could help affirm once again for the ongoing MSK problematic situation and serve as an essential information in problem solving to suit with particular type of deep-sea port crane in the future.
5. Conclusions
Port crane operators either quay or RTG crane in Thailand and around the world are facing a high risk of WMSDs. Despite their differences in age, BMI and work experience, this study likely revealed that port crane workers whoever having been working longer than 12 months would potentially develop MSK problems: mostly on lower back, followed by a group of the upper back, shoulders and neck. Exposure to the larger scale of ergonomics hazards in quay crane compared to the RTG seemed to be the main contributors that mark a significant difference among the two on the upper back. Engineering measures, educations/trainings and managements must be adopted against the prolonged static non-neutral sitting postures and the existing cabin vibration. Furthermore, job characteristics related health assessment in the recruitment or new job promotion must be strictly implemented and included into the management policy.
6. Limitations
Regarding the amount of quey and RTG canes operating in the sea-port are relatively small, locally and globally. The available participants in this study were also proportionally limited and when combined with the companies’ strict working schedules and safety rules enforcing in work, this had led to the restricted number of the subjects.
Author Contributions
Conceptualization, Teerayut Sa-ngiamsak; Data curation, Teerayut Sa-ngiamsak; Formal analysis, Teerayut Sa-ngiamsak; Funding acquisition, Teerayut Sa-ngiamsak; Investigation, Teerayut Sa-ngiamsak; Methodology, Teerayut Sa-ngiamsak; Project administration, Anamai Thetkathuek; Resources, Teerayut Sa-ngiamsak; Software, Teerayut Sa-ngiamsak; Supervision, Teerayut Sa-ngiamsak; Validation, Teerayut Sa-ngiamsak; Visualization, Teerayut Sa-ngiamsak; Writing – original draft, Teerayut Sa-ngiamsak; Writing – review & editing, Teerayut Sa-ngiamsak.
Funding
This research was funded by the Faculty of Public Health, Burapha University, Thailand, grant number 009/2560.
Institutional Review Board Statement
This study was approved by the Institutional Review Board (IRB) committee of the Burapha University, Thailand Burapha University Ethics Committee for Human Research (IRB No. Sci 025/2560).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data described in this study are accessible directly from the corresponding author upon request. Due to the confidentiality concerns, the data are not publicly available.
Acknowledgments
The research team would like to thanks to all crane operators from all participating companies, together with their management teams for the excellent cooperation in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- UNCTAD. Review of Maritime Transport (Series). Available online: https://unctad.org/en/Pages/Publications/Review-of-Maritime-Transport-(Series).aspx (accessed on 24 Aug).
- Thailand Convention & Exhibition Bureau. Maritime industry of Thailand. Available online: https://intelligence.businesseventsthailand.com/en/industry/maritime-industry (accessed on 25 Aug).
- CEIC. Thailand Container Port Throughput. Available online: https://www.ceicdata.com/en/indicator/thailand/container-port-throughput (accessed on.
- Chang, D.; Fang, T.; Fan, Y. Dynamic rolling strategy for multi-vessel quay crane scheduling. Advanced Engineering Informatics 2017, 34, 60–69. [Google Scholar] [CrossRef]
- Galle, V.; Barnhart, C.; Jaillet, P. Yard Crane Scheduling for container storage, retrieval, and relocation. European Journal of Operational Research 2018, 271, 288–316. [Google Scholar] [CrossRef]
- Eko Mardiyanto; Denny Ardyanto; Notobroto, H. B. Container Crane Operator Ergonomics Analysis PT. X Port Of Tanjung Perak, Surabaya. Civil and Environmental Research 2015, 17, 4. [Google Scholar]
- Leban, B.; Fancello, G.; Fadda, P.; Pau, M. Changes in trunk sway of quay crane operators during work shift: A possible marker for fatigue? Applied Ergonomics 2017, 65, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Fadda, P.; Meloni, M.; Fancello, G.; Pau, M.; Medda, A.; Pinna, C.; Del Rio, A.; Lecca, L.I.; Setzu, D.; Leban, B. Multidisciplinary Study of Biological Parameters and Fatigue Evolution in Quay Crane Operators. Procedia Manufacturing 2015, 3, 3301–3308. [Google Scholar] [CrossRef]
- OSHA. Ergonomics. Available online: https://www.osha.gov/SLTC/ergonomics/ (accessed on.
- Haq SA, R.J. , Darmawan J, Chopra A.. WHO-ILAR-COPCORD in the Asia-Pacific: the past, present and future. Int J Rheum Dis. 2008;11(1):4–10. 2008, 11, 4–10. [Google Scholar]
- World Shipping Council. Top 50 world container ports. Available online: http://www.worldshipping.org/about-the-industry/global-trade/top-50-world-container-ports (accessed on 14 May).
- Hutchisonports. Laem Chabang Port. Available online: https://hutchisonports.co.th/laem-chabang-port/ (accessed on 31 Aug.).
- Laem Chabang International Terminal Co., L. Facility & Equipment. Available online: https://www.lcit.com/facilityEquipment.asp (accessed on.
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sorensen, F.; Andersson, G.; Jorgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon 1987, 18, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Shariat, A.; Cleland, J.A.; Danaee, M.; Alizadeh, R.; Sangelaji, B.; Kargarfard, M.; Ansari, N.N.; Sepehr, F.H.; Tamrin, S.B.M. Borg CR-10 scale as a new approach to monitoring office exercise training. Work (Reading, Mass.) 2018, 60, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Griep, M.I.; Borg, E.; Collys, K.; Massart, D.L. Category ratio scale as an alternative to magnitude matching for age-related taste and odour perception. Food Quality and Preference 1998, 9, 67–72. [Google Scholar] [CrossRef]
- Mohd Azlan Fahmi Muhammad Azmi; Azanizawati Ma’aram; Aini Zuhra Abdul Kadir; Ngadiman, N. H.A. Risk Factors of Low Back Pain Amongst Port Crane Operator in Malaysia International Journal of Innovative Technology and Exploring Engineering (IJITEE) 2019, 8, 1434–1439.
- National Institute for Occupational Safety and Health (NIOSH). Musculoskeletal Disorders and Workplace Factors. Available online: https://www.cdc.gov/niosh/docs/97-141/pdfs/97-141.pdf. (accessed on 19 Aug.).
- Bovenzi, M. , Pinto, I., Stacchini, N. Low back pain in port machinery operators. Journal of Sound and vibration 2002, 253, 3–20. [Google Scholar] [CrossRef]
- Pigini, L.; , Colombini, D., Brieda, S., Fanti, M. Ergonomic solutions in designing workstations for operators of cranes on harbours. Available online: http://www.epmresearch.org/userfiles/files/2006%20IEA%2010-14%20LUGLIO%20MAASTRICHTPIGINI-BRIEDA.pdf. (accessed on 19 Aug).
- Huysmans, M.A.; de Looze, M.P.; Hoozemans, M.J.M.; van der Beek, A.J.; van Dieën, J.H. The effect of joystick handle size and gain at two levels of required precision on performance and physical load on crane operators. Ergonomics 2006, 49, 1021–1035. [Google Scholar] [CrossRef]
- OSHA Safety Manual. OCCUPATIONAL VIBRATION EXPOSURE. Available online: https://www.safetymanualosha.com/occupational-vibration-exposure/ (accessed on December).
- MOHD AZLAN; AZMI, F. B.M. ERGONOMICS OF QUAY CRANE WORKSTATION Faculty of Mechanical Universiti Teknologi Malaysia 2017.
- Marjanen, Y. Validation and improvement of the ISO 2631-1 (1997) standard method for evaluating discomfort from whole-body vibration in a multi-axis environment. 2010.
- Standardization, I.O.f. Guide for the evaluation of human exposure to whole body vibration - Part 1. General requirements.
- Bongers, P.M.; Boshuizen, H.C.; Hulshof, C.T.J.; Koemeester, A.P. Back disorders in crane operators exposed to whole-body vibration. International Archives of Occupational and Environmental Health 1988, 60, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Wahlström, J.; Burström, L.; Johnson, P.W.; Nilsson, T.; Järvholm, B. Exposure to whole-body vibration and hospitalization due to lumbar disc herniation. Int Arch Occup Environ Health 2018, 91, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Z. A. Kadir; R. Mohammad; Othman, N.;. Low Back Pain Problem amongst Port Crane Operator. Journal of Advanced Research in Applied Sciences and Engineering Technology 2015, 1, 13–26. [Google Scholar]
- Nourollahi-Darabad, M.; Mazloumi, A.; Saraji, G.N.; Afshari, D.; Foroushani, A.R. Full shift assessment of back and head postures in overhead crane operators with and without symptoms. Journal of Occupational Health 2018, 60, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Hareendran, A.; Leidy, N.K.; Monz, B.U.; Winnette, R.; Becker, K.; Mahler, D.A. Proposing a standardized method for evaluating patient report of the intensity of dyspnea during exercise testing in COPD. International journal of chronic obstructive pulmonary disease 2012, 7, 345–355. [Google Scholar] [CrossRef] [PubMed]
- PEMA, P.E.M.A. Crane Operator Health & Safety; Port Equipment Manufacturers Association (PEMA): Brussels, Belgium, 2018; p. 8. [Google Scholar]
- Liebherr Container Cranes. Technical Description Ship to Shore Gantry Cranes. Available online: https://www.liebherr.com/shared/media/maritime-cranes/downloads-and-brochures/brochures/lcc/liebherr-sts-cranes-technical-description.pdf (accessed on Aug, 5).
- Precision pain care & rehabilitation. Causes of Upper Back Pain. Available online: https://www.precisionpaincarerehab.com/blog/causes-of-upper-back-pain-21297.html (accessed on Aug, 3).
- Liebherr Container Cranes. Technical Description Rubber Tyre Gantry Crane. Available online: https://www.liebherr.com/shared/media/maritime-cranes/downloads-and-brochures/brochures/lcc/liebherr-rtg-cranes-technical-description.pdf (accessed on Aug, 5).
- Stewart G., Eidelson; Cristol, H. Upper Back Pain Causes, Risk Factors, Diagnosis and Treatment Written by Stewart G. Eidelson, MD and Hope Cristol; Reviewed by Reginald Q. Knight, MD, MHA. Available online: https://www.spineuniverse.com/conditions/upper-back-pain (accessed on.
- J. Talbot Sellers, D. All About Upper Back Pain. Available online: https://www.spine-health.com/conditions/upper-back-pain/all-about-upper-back-pain (accessed on Aug, 3).
- Nourollahi-Darabad, M.; Mazloumi, A.; Saraji, G.N.; Afshari, D.; Foroushani, A.R. Full shift assessment of back and head postures in overhead crane operators with and without symptoms. J Occup Health 2018, 60, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Sa-ngiamsak, T. Exploring study protocols examining muscle fatigue among transportation and transshipment operators: a systematic review. International Journal of Occupational and Environmental Safety, 2019; 3, 11. [Google Scholar] [CrossRef]
- MOHD AZLAN FAHMI B MUHAMMAD AZMI. ERGONOMICS OF QUAY CRANE WORKSTATION. Universiti Teknologi Malaysia, Malaysia, 2017.
Figure 1.
Prevalence of self-reported anthropometric MSK problem by body parts.
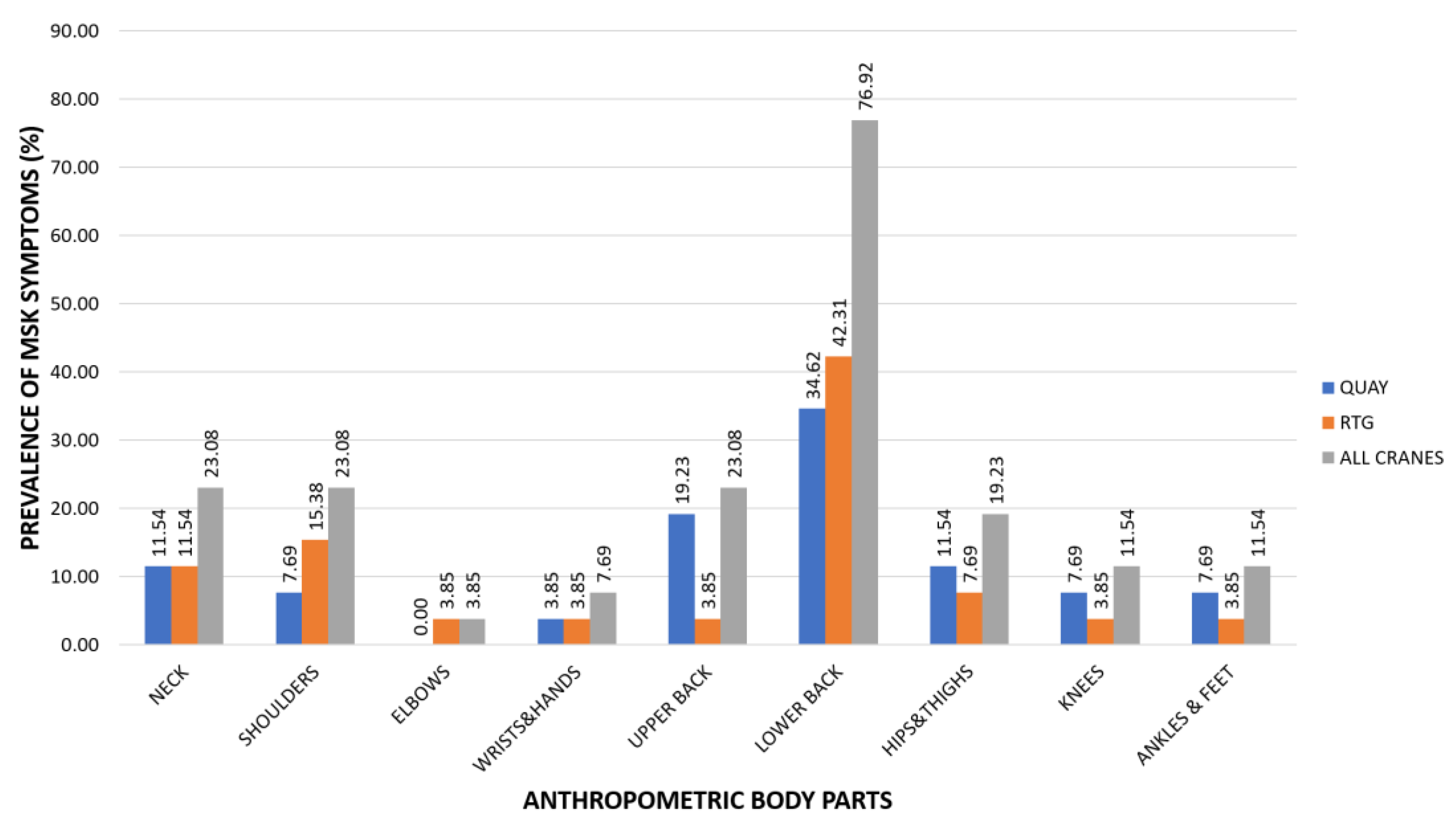
Figure 2.
Prevalence of self-reported MSK problem during the last 12-months and past 7 days.
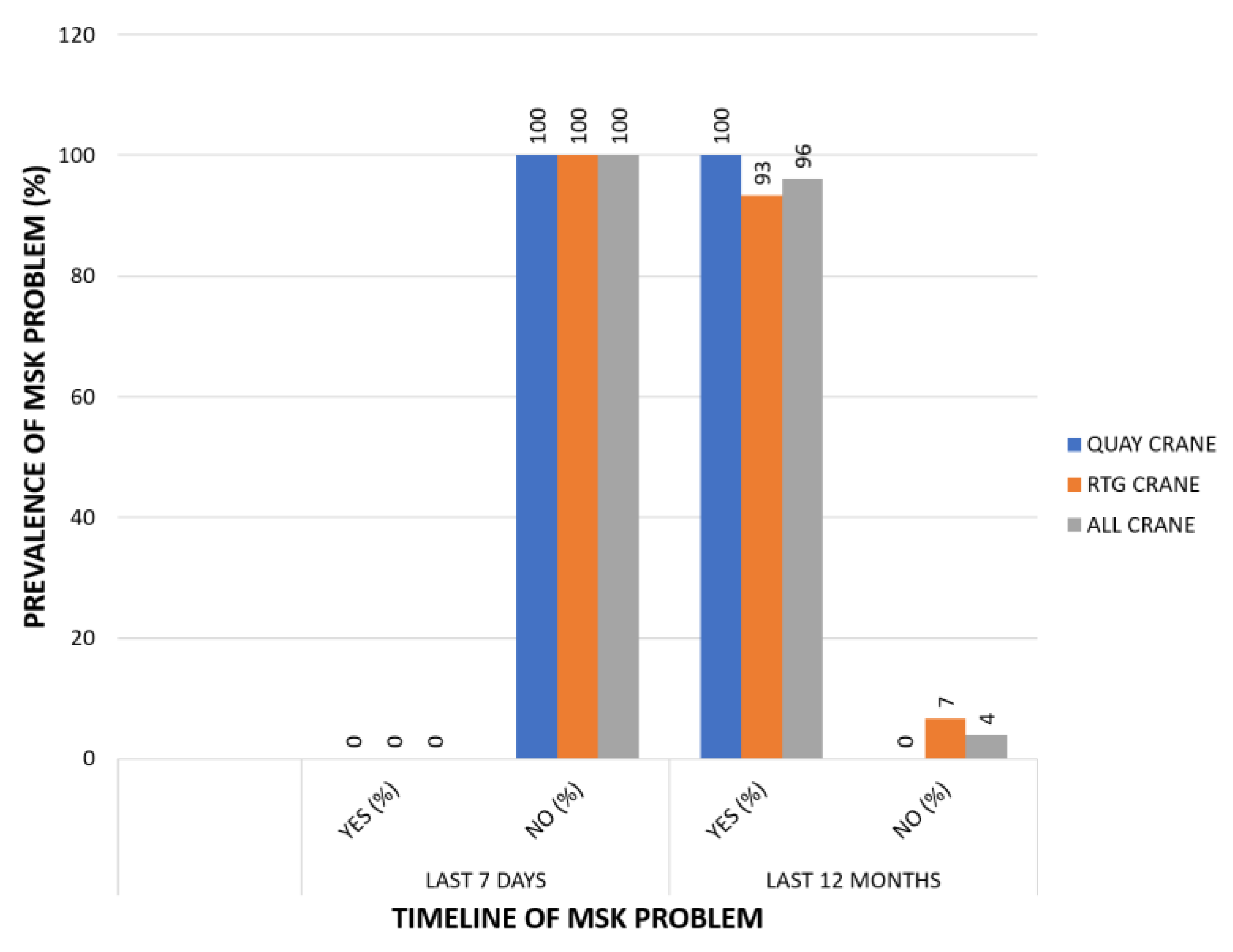
Figure 3.
Perceived discomfort scores (Borg CR10 scale) by body parts.
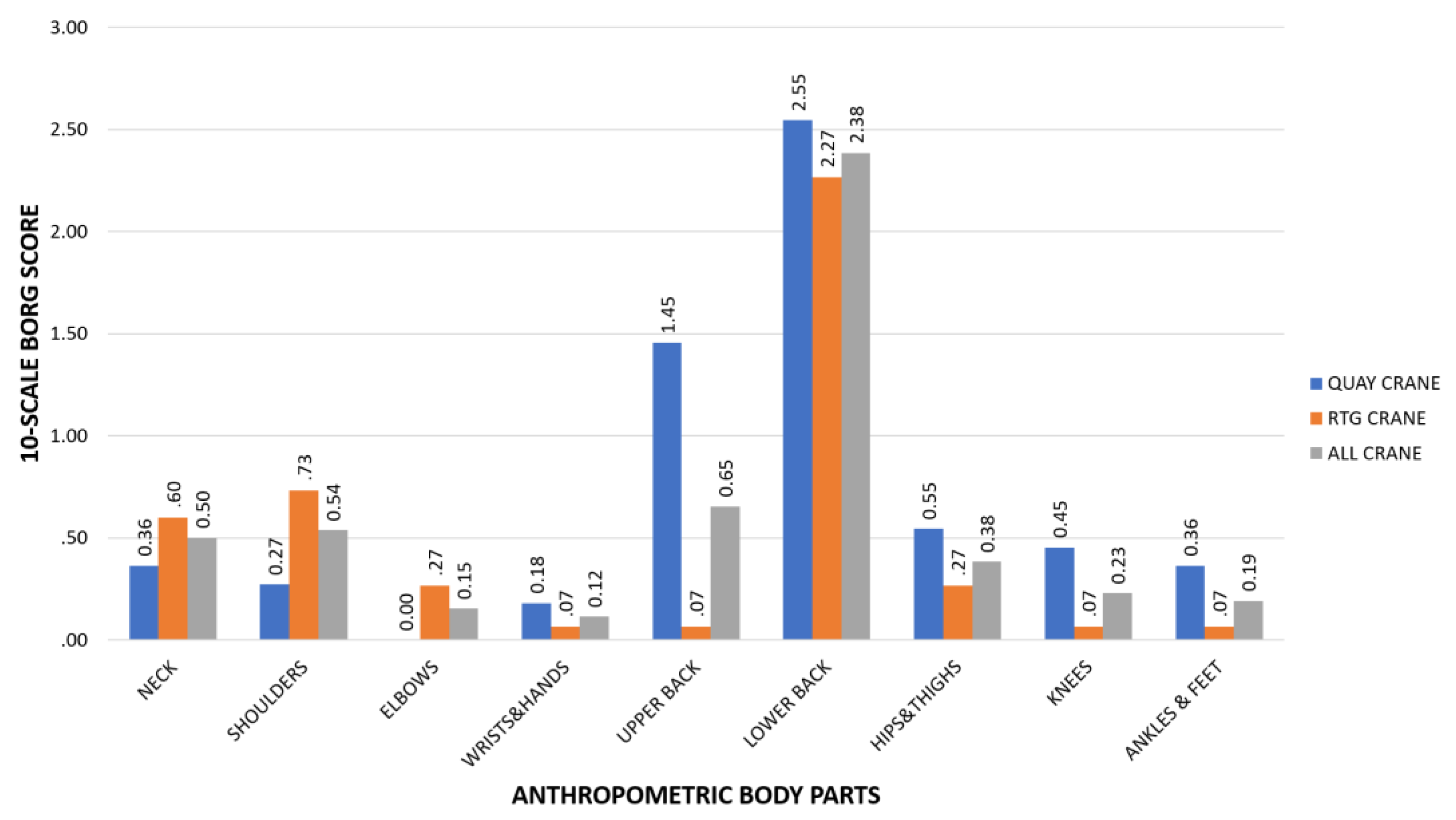
Figure 4.
Deep-sea port container cranes and their sitting postures (a) Quey crane (b) RTG crane.



Table 1.
Socio-demographic characteristics of port cranes operators.
| Variable | Quay | RTG | All Port Cranes* | |||||
|---|---|---|---|---|---|---|---|---|
| Main category | Sub category | (n) | (%) | (n) | (%) | (n) | (%) | |
| Age (years) | 20-30 | 1 | 4 | 0 | 0 | 1 | 4 | |
| 31-40 | 3 | 12 | 8 | 31 | 11 | 42 | ||
| 41-50 | 4 | 15 | 5 | 19 | 9 | 35 | ||
| 51-60 | 3 | 12 | 2 | 8 | 5 | 19 | ||
| Total | 11 | 42 | 15 | 58 | 26 | 100 | ||
| Statistics | χ2 | 3 | n/a | |||||
| p | 0.464 | |||||||
| BMI | Underweight (BMI < 18.5) | 0 | 0 | 1 | 4 | 1 | 4 | |
| Healthy Normal (18.6 - 22.9) | 1 | 4 | 4 | 15 | 5 | 19 | ||
| Overweight (23.0 - 24.9) | 4 | 15 | 2 | 8 | 6 | 23 | ||
| Pre-Obese (25.0 - 29.9) | 4 | 15 | 5 | 19 | 9 | 35 | ||
| Obese (BMI ≥ 30.0) | 2 | 8 | 3 | 12 | 5 | 19 | ||
| Total | 11 | 42 | 15 | 58 | 26 | 100 | ||
| Statistics | χ2 | 3.147 | n/a | |||||
| p | 0.641 | |||||||
| Education | Lower than Senior High School/Vocational Certificate | 5 | 19 | 3 | 12 | 8 | 31 | |
| Senior High School/Vocational Certificate | 5 | 19 | 7 | 27 | 12 | 46 | ||
| Diploma/High Vocational Certificate | 1 | 4 | 4 | 15 | 5 | 19 | ||
| Bachelor Degrees or Higher | 0 | 0 | 1 | 4 | 1 | 4 | ||
| Total | 11 | 42 | 15 | 58 | 26 | 100 | ||
| Statistics | χ2 | 2.903 | n/a | |||||
| p | 0.407 | |||||||
| Work Experience(years) | < 1 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 1-5 | 3 | 12 | 3 | 12 | 6 | 23 | ||
| 6-10 | 4 | 15 | 5 | 19 | 9 | 35 | ||
| 11-15 | 1 | 4 | 4 | 15 | 5 | 19 | ||
| 16-20 | 2 | 8 | 2 | 8 | 4 | 15 | ||
| 21-25 | 1 | 4 | 1 | 4 | 2 | 8 | ||
| Total | 11 | 42 | 15 | 58 | 26 | 100 | ||
| Statistics | χ2 | 1.737 | n/a | |||||
| p | 0.918 | |||||||
* Combination between quay and RTG crane.
Table 2.
MSK prevalence and perceived discomfort levels among quay and RTG crane operators regarding different body parts.
Table 2.
MSK prevalence and perceived discomfort levels among quay and RTG crane operators regarding different body parts.
| Factors | MSK Prevalence | Perceived discomfort scores | |||||
| Statistics | Quay | RTG | Statistics | Quay | RTG | ||
| Body Parts | Neck | Yes (%) | 11.54 | 11.54 | Mean | 0.36 | 0.60 |
| No (%) | 30.77 | 46.15 | SD | 0.67 | 1.45 | ||
| χ2 | 0.189 | χ2 | 0.061 | ||||
| p | 0.509 | p | 0.805 | ||||
| Shoulders | Yes (%) | 7.69 | 15.38 | Mean | 0.27 | 0.73 | |
| No (%) | 34.62 | 42.31 | SD | 0.65 | 2.09 | ||
| χ2 | 0.257 | χ2 | 0.036 | ||||
| p | 0.491 | p | 0.850 | ||||
| Elbows | Yes (%) | 0.00 | 3.85 | Mean | 0.00 | 0.27 | |
| No (%) | 42.31 | 53.85 | SD | 0.00 | 0.80 | ||
| χ2 | 0.763 | χ2 | 1.525 | ||||
| p | 0.577 | p | 0.217 | ||||
| Wrists & Hands | Yes (%) | 3.85 | 3.85 | Mean | 0.18 | 0.07 | |
| No (%) | 38.46 | 53.85 | SD | 0.60 | 0.26 | ||
| χ2 | 0.053 | χ2 | 0.079 | ||||
| p | 0.677 | p | 0.779 | ||||
| Upper back | Yes (%) | 19.23 | 3.85 | Mean | 1.45 | 0.07 | |
| No (%) | 23.08 | 53.85 | SD | 1.81 | 0.26 | ||
| χ2 | 5.379 | χ2 | 5.894 | ||||
| p | 0.032* | p | 0.015* | ||||
| Lower Back | Yes (%) | 34.62 | 42.31 | Mean | 2.55 | 2.27 | |
| No (%) | 7.69 | 15.38 | SD | 2.11 | 2.22 | ||
| χ2 | 0.257 | χ2 | 0.143 | ||||
| p | 0.491 | p | 0.706 | ||||
| Hips & Thighs | Yes (%) | 11.54 | 7.69 | Mean | 0.55 | 0.27 | |
| No (%) | 30.77 | 50.00 | SD | 1.04 | 0.80 | ||
| χ2 | 0.794 | χ2 | 0.753 | ||||
| p | 0.346 | p | 0.385 | ||||
| Knees | Yes (%) | 7.69 | 3.85 | Mean | 0.45 | 0.07 | |
| No (%) | 34.62 | 53.85 | SD | 1.04 | 0.26 | ||
| χ2 | 0.824 | χ2 | 0.964 | ||||
| p | 0.381 | p | 0.326 | ||||
| Ankles & Feet | Yes (%) | 7.69 | 3.85 | Mean | 0.36 | 0.07 | |
| No (%) | 34.62 | 53.85 | SD | 0.92 | 0.26 | ||
| χ2 | 0.824 | χ2 | 0.875 | ||||
| p | 0.381 | p | 0.349 | ||||
* Significance in statistics analysis at p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



