Submitted:
08 May 2024
Posted:
09 May 2024
You are already at the latest version
Abstract
In the most cases, invasive ductal carcinoma (IDC) of the breast is identifiable when they present with classic infiltrative growth pattern. However, subset of IDC can occur in a very sneaky way, significantly mimicking the appearance of ductal carcinoma in situ (DCIS). In this condition, it’s much easier to miss the invasive component without pulling ancillary staining when morphologic findings are extremely compatible with DCIS, especially the diagnosis of DCIS was made on the previous biopsy. Here, we reported a 55 year-old female who was noted to have microcalcification at the 11:00 o’clock of the right posterior breast on routine mammographic examination in 09/2023. Biopsy of the calcification area in 10/2023 reported high grade DCIS (ER+ PR-). Histologic examination of subsequent mastectomy specimen showed two separate DCIS-looking areas (Figure 1A-D and Figure 2). Immunohistochemical (IHC) staining showed that myoepithelial markers, smooth muscle myosin heavy chain (SMMHC), p63, CK5/6 and S100, were retained at the periphery of all the expanded acini in one area (Figure 1E-H). Unexpectedly and surprisingly, myoepithelial markers were completely lost at the periphery of part of the DCIS-looking acini in another area (Figure 3A-H), immunohistochemically compatible with the diagnosis of invasive ductal carcinoma admixed with DCIS. Knowing that invasive ductal carcinoma of the breast can present as DCIS-looking morphology, especially given the condition that the diagnosis of DCIS was rendered on the previous biopsy, will enhance awareness of pathologists to recognize DCIS-looking invasive ductal carcinoma. In turn, this will prevent misdiagnosis and under-treatment of patients with invasive ductal carcinoma of the breast.
Keywords:
ductal carcinoma in situ
; invasive ductal carcinoma
; breast cancer
1. Introduction
Breast carcinoma is the most commonly seen female malignancy in all age groups with significant increased risk of increase age [1]. Invasive ductal carcinoma (IDC) is the most common histologic subtype of breast cancer (BCs), occupying approximately 90% of all BCs [2]. Ductal carcinoma in situ (DCIS) is regarded as a direct precursor to IDC, and characterized by a malignant proliferation of ductal epithelial cells within the ductal-lobular system without stromal invasion [3]. DCIS contributes to approximately 20% of newly diagnosed breast cancer cases, in which approximately 25–60% of untreated DCIS cases have been reported to progress to IDC after a median follow-up of 9–24 years [4,5].
IDC shows significant overlapping with DCIS, including epidemiological risk factors such as age and family history, genetic factor such as BRCA1/BRCA2, and molecular status such as ER, PR and HER2 [6]. IDC can be divided into multiple subtypes, including tubular, mucinous, papillary, cribriform, pleomorphic and solid [6], which shares a great portion of histomorphological overlapping with DCIS, including papillary, micropapillary, cribriform and comedo-necrosis [7]. Among these, solid pattern of IDC is one of the most common subtypes that is underestimated and misdiagnosed as DCIS. The aim of this case is to shed light on the big pitfall in diagnosing IDC in a background of extensive DCIS.
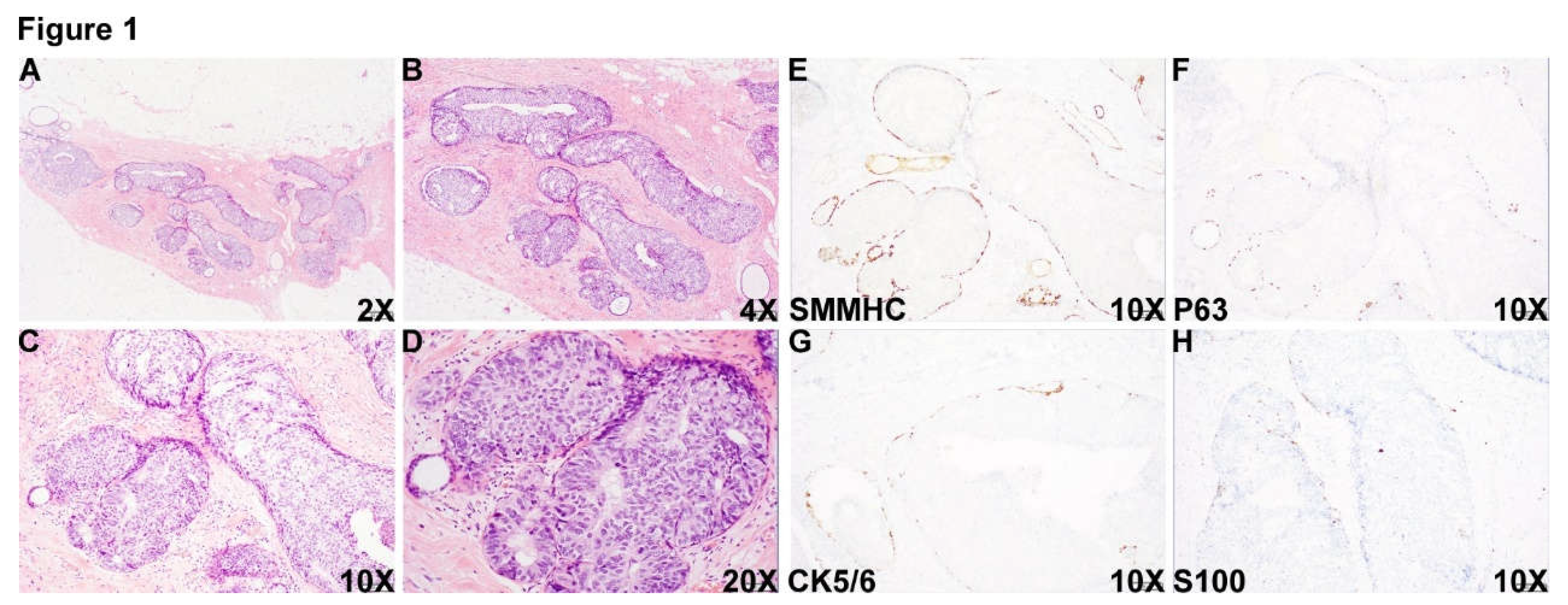
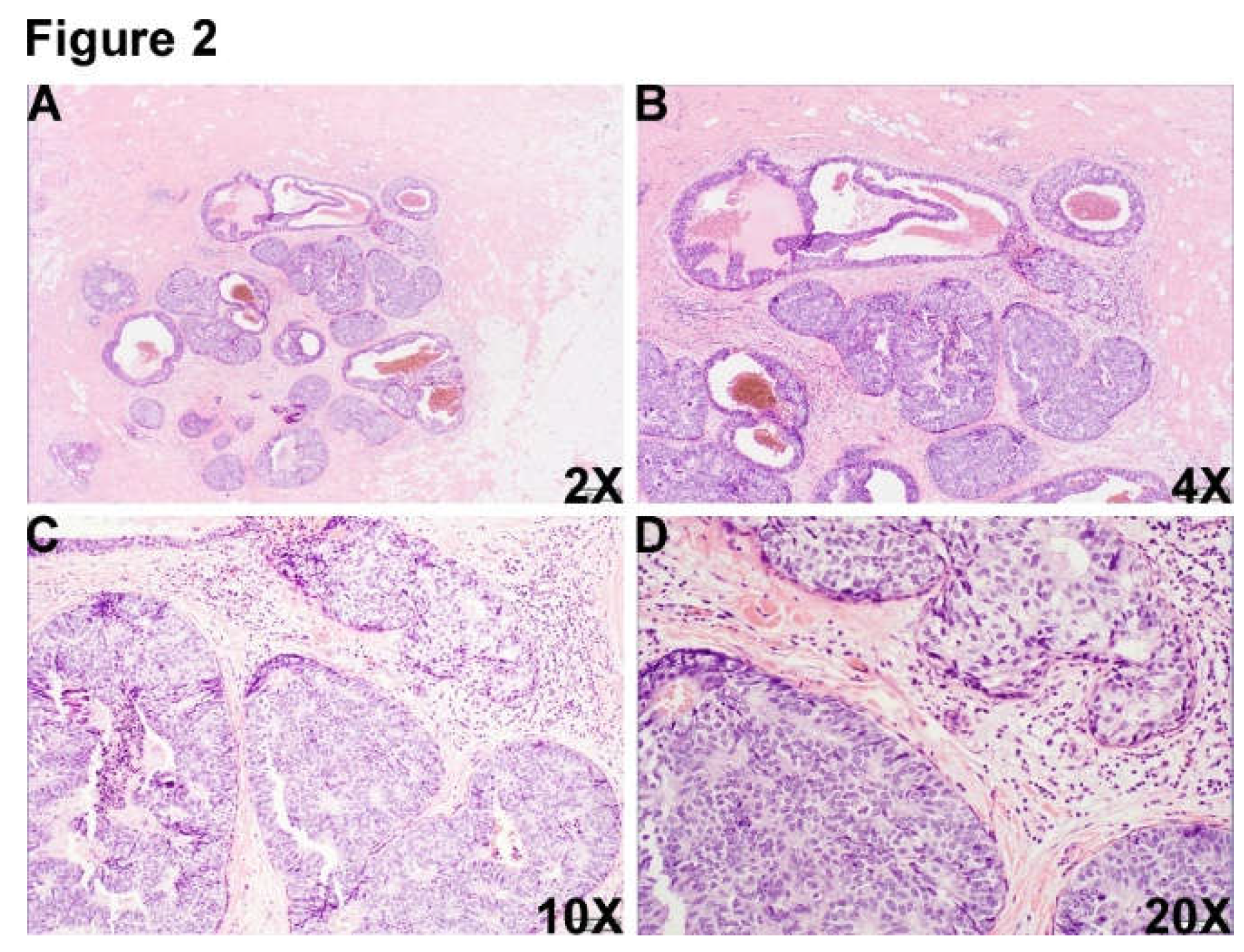
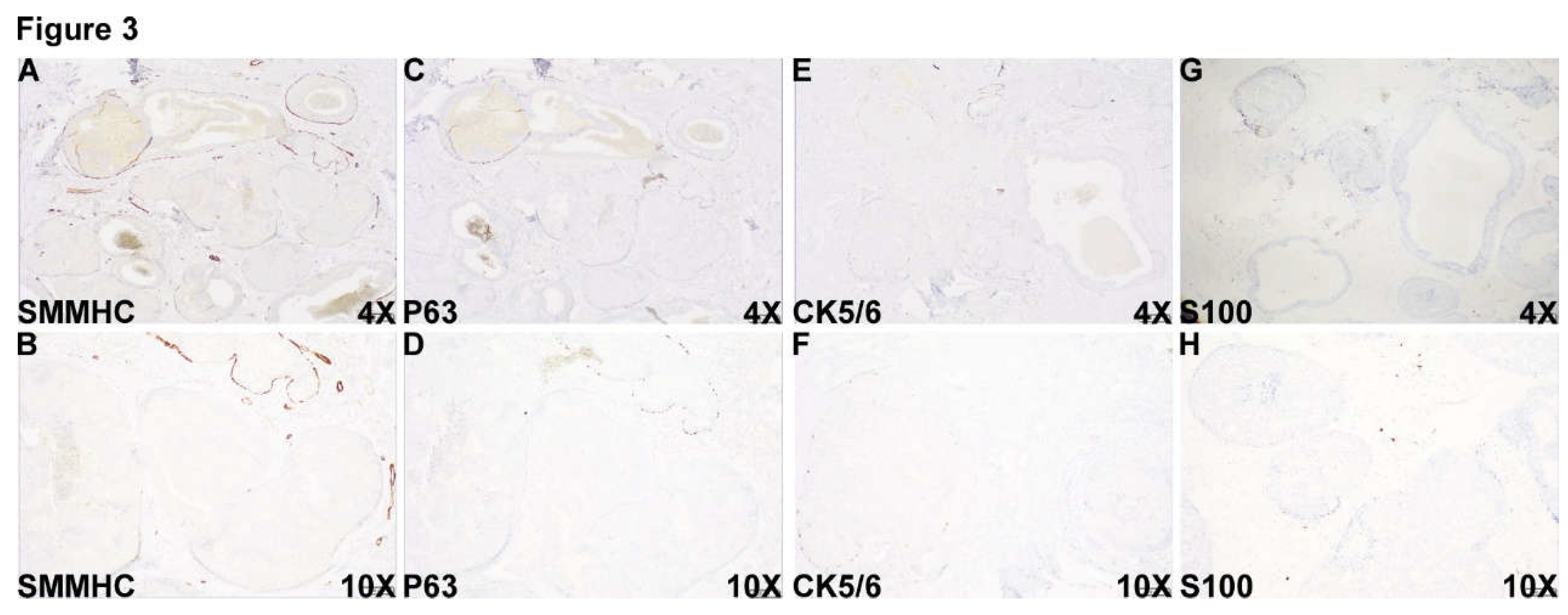
Figure 1.
DCIS area. A 55 year-old female who was noted to have microcalcification at the 11:00 o’clock of the right posterior breast on routine mammographic examination in outside hospital and biopsy of the calcification area showed reported high grade DCIS, ER+ PR- (Pathologic slides were not available to review). The patient was transferred to our institution for mastectomy resection. Histologic examination of the specimen showed an area with multiple densely packed well-border expanded acini composed of monotonous epithelioid cells (Figure 1A-D, 2X (A), 4X (B), 10X (C) and 20X (D)). Immunohistochemical (IHC) staining showed that myoepithelial markers, smooth muscle myosin heavy chain (SMMHC) (Figure 1E), p63 (Figure 1F), CK5/6 (Figure 1G) and S100 (Figure 1H), were retained at the periphery of all the expanded acini, supporting the diagnosis of DCIS in this area.
Figure 1.
DCIS area. A 55 year-old female who was noted to have microcalcification at the 11:00 o’clock of the right posterior breast on routine mammographic examination in outside hospital and biopsy of the calcification area showed reported high grade DCIS, ER+ PR- (Pathologic slides were not available to review). The patient was transferred to our institution for mastectomy resection. Histologic examination of the specimen showed an area with multiple densely packed well-border expanded acini composed of monotonous epithelioid cells (Figure 1A-D, 2X (A), 4X (B), 10X (C) and 20X (D)). Immunohistochemical (IHC) staining showed that myoepithelial markers, smooth muscle myosin heavy chain (SMMHC) (Figure 1E), p63 (Figure 1F), CK5/6 (Figure 1G) and S100 (Figure 1H), were retained at the periphery of all the expanded acini, supporting the diagnosis of DCIS in this area.
Figure 2.
There was another morphologically similar area adjacent to DCIS area, which was composed of multiple well-border expanded acini composed of monotonous epithelioid cells and dilated cystic change (Figure 2A-D, 2X (A), 4X (B), 10X (C) and 20X (D).).
Figure 2.
There was another morphologically similar area adjacent to DCIS area, which was composed of multiple well-border expanded acini composed of monotonous epithelioid cells and dilated cystic change (Figure 2A-D, 2X (A), 4X (B), 10X (C) and 20X (D).).
Figure 3.
Unexpectedly and surprisingly, myoepithelial markers, including SMMHC (Figure 3A and B), p63(Figure 3C and D), CK5/6 (Figure 3E and F) and S100 (Figure 3G and H) were completely lost at the periphery of part of the DCIS-looking acini in this area, immunohistochemically compatible with the diagnosis of invasive ductal carcinoma admixed with DCIS.
Figure 3.
Unexpectedly and surprisingly, myoepithelial markers, including SMMHC (Figure 3A and B), p63(Figure 3C and D), CK5/6 (Figure 3E and F) and S100 (Figure 3G and H) were completely lost at the periphery of part of the DCIS-looking acini in this area, immunohistochemically compatible with the diagnosis of invasive ductal carcinoma admixed with DCIS.
In this case, the diagnosis of DCIS is easily made without the awareness of DCIS-looking IDC morphology. This case will definitely increase recognition and awareness of pathologists to always consider the possibility of IDC in expansile DCIS-looking area.
References
- Giaquinto AN, Sung H, Miller KD, Kramer JL, Newman LA, Minihan A, Jemal A, Siegel RL: Breast Cancer Statistics, 2022. CA Cancer J Clin 2022, 72(6):524-541.
- Li CI, Anderson BO, Daling JR, Moe RE: Trends in incidence rates of invasive lobular and ductal breast carcinoma. JAMA 2003, 289(11):1421-1424.
- Badve SS, Gokmen-Polar Y: Ductal carcinoma in situ of breast: update 2019. Pathology 2019, 51(6):563-569.
- Sanders ME, Schuyler PA, Dupont WD, Page DL: The natural history of low-grade ductal carcinoma in situ of the breast in women treated by biopsy only revealed over 30 years of long-term follow-up. Cancer 2005, 103(12):2481-2484. [CrossRef]
- Collins LC, Tamimi RM, Baer HJ, Connolly JL, Colditz GA, Schnitt SJ: Outcome of patients with ductal carcinoma in situ untreated after diagnostic biopsy: results from the Nurses' Health Study. Cancer 2005, 103(9):1778-1784. [CrossRef]
- Harvey JA: Unusual breast cancers: useful clues to expanding the differential diagnosis. Radiology 2007, 242(3):683-694. [CrossRef]
- Shaaban AM, Hilton B, Clements K, Provenzano E, Cheung S, Wallis MG, Sawyer E, Thomas JS, Hanby AM, Pinder SE et al: Pathological features of 11,337 patients with primary ductal carcinoma in situ (DCIS) and subsequent events: results from the UK Sloane Project. Br J Cancer 2021, 124(5):1009-1017. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



