
Submitted:
08 May 2024
Posted:
09 May 2024
You are already at the latest version
Abstract
Background: Gender differences characterize the prevalence and attitudes toward weight management. Despite limited evidence suggesting greater weight loss in women with anti-obesity pharmacotherapy, gender-specific analysis remains underexplored. This retrospective study aimed to evaluate the gender-specific response to liraglutide 3.0 mg treatment in people with obesity without type 2 diabetes (T2D). Methods: Data were collected from 47 patients (31 women, 16 men), with age > 18 years, BMI ≥ 30 kg/m^2, absence of T2D, and with exclusion of prior anti-obesity treatment, comorbidities, or bariatric surgery. Only patients who maintained the liraglutide 3.0 mg dose for at least 6 months were included. Results: Both sexes showed significant reductions in weight and BMI at 3 and 6 months. Men achieved greater weight loss (WL), BMI reduction, % WL, WL >5% and >10% than women, and they also showed more significant improvements in metabolic parameters (total and LDL cholesterol, Fibrosis-4 Index FIB-4). No significant gender differences were observed in glucose metabolism or renal function. Conclusion: This study showed a greater therapeutic effect of liraglutide 3.0 mg in men. Given men's higher risk of cardiovascular disease (CVD), and underrepresentation in clinical weight loss programs, these findings may increase male engagement and improve their CVD risk.
Keywords:
Obesity
; gender
; GLP1-RAs
; Liraglutide
; weight loss
1. Introduction
Over the past two decades, the increase in morbidity and mortality associated with excess body weight has made obesity a major health problem with implications for both public health and healthcare expenditure [1,2].
Results from studies analyzing changes in obesity rates from 1980 to 2019 have shown a significant increase in prevalence in both men (from 3.2% to 12.2%) and women (from 6% to 15.7%). In particular, in recent years, young men aged 20-44 years appear to have a higher prevalence of overweight/obesity than young women, but this trend seems to be reverse after the age of 45, probably due to menopausal changes in women [3]. In Italy, excess body weight was found to be higher in men than in women (53.6% vs. 35.7%), with an increasing trend with age [4].
In general, women are more likely to be diagnosed with obesity, and to seek and receive all types of obesity treatment, including lifestyle modification, pharmacotherapy, and bariatric surgery. This propensity for intervention among women raises concerns about gender disparities in obesity treatment [5].
Several studies have shown that weight loss significantly reduces the risk of obesity related complications [1]. In addition, the availability of new anti-obesity drugs has renewed interest in pharmacological therapy of obesity, which has been recognized as an innovative strategy for its management [6]. However, the clinical approach to obesity often does not take into account gender differences, which can influence the management of obesity and improve the treatment of obesity [5].
Orlistat, naltrexone/bupropion, and liraglutide, are approved anti-obesity drugs in Italy. Among the Glucagon-like peptide-1 receptor agonists (GLP1-RAs), liraglutide has been shown to promote weight loss in patients with T2D [7], leading to its approval for chronic weight control at a daily dose of 3.0 mg in people with overweight and without T2D [8]. Despite previous clinical trials demonstrating the superior efficacy of liraglutide 3.0 mg in promoting weight loss in women compared with men [9], there has been limited real-world research on the gender-specific clinical response to this drug.
Since pharmacodynamic and pharmacokinetic analyses suggest that gender may significantly influence the effect of these drugs [7], we decided to plan this retrospective study to evaluate a potential gender difference in response to liraglutide 3.0 mg treatment in a cohort of people with obesity and without T2D.
2. Materials and Methods
2.1. Study Population
We conducted a single-center retrospective study of patients with obesity and without T2D treated with liraglutide 3.0 mg who attended the Obesity Unit of the Santa Maria Goretti Hospital in Latina, Italy from October 2022 to October 2023, according to the following criteria:
- inclusion criteria: age > 18 years, presence of obesity (body mass index BMI ≥ 30 kg/m^2), absence of T2D according to ADA criteria [10], and other metabolic comorbidities and treatments;
- exclusion criteria: previous anti-obesity treatment (GLP1-RAs or others) and/or bariatric surgery, pregnancy.
Liraglutide treatment was titrated from 0.6 mg to 3.0 mg weekly. Only patients who reached the maximum dose of liraglutide (3.0 mg) during the five-week titration period, and maintained this dose for at least 6 months of follow-up, were included in the study.
2.2. Data Collection and Definition
Demographic and anthropometric parameters such as age, weight and BMI, and clinical data including glucose metabolism, lipid profile, liver and renal function were collected retrospectively from the electronic reporting system of our obesity unit.
Body weight (BW), height and BMI (calculated as weight (kg) divided by the square of height (m)) were used to express anthropometric parameters. Measurement of fasting blood glucose and glycated hemoglobin (FBG and HbA1c) allowed evaluation of glucose metabolism. The lipid profile was assessed by total cholesterol, LDL cholesterol, HDL cholesterol and triglycerides (TG). To examine liver function, transaminases (AST and ALT) were measured and the Fibrosis-4 Index score (FIB-4) was calculated using the formula: (age [years] × aspartate transaminase AST [U/L])/(platelets [109/L] × (alanine transaminase ALT [U/L])1/2) [11]. Renal function was assessed by serum creatinine.
The anthropometric data were collected at baseline T0 and after 3 months T1 (2-4 months, average 3 months) and 6 months T2 (5-7 months, average 6 months) of treatment. The metabolic parameters were collected at baseline (T0) and after 6 months of treatment (T2).
At each visit, medical staff recorded the patient's weight and defined weight loss as the difference between the follow-up weight and the baseline weight. BMI change was also calculated as the difference between the follow-up BMI and the baseline BMI. If there were multiple visits within 2-4 months, the lowest weight was used, and if there were multiple visits within 5-7 months of the last visit, the weight closest to 6 months was used.
The percentage weight loss (%WL), and the percentage of patients who lost at least 5% or 10% of their initial weight at 3 and 6 months, respectively, were recorded.
The prescription of anti-obesity pharmacotherapy is not reimbursed by the Italian healthcare system, and the high cost represents one of the main barriers to treatment, as not all patients are able to afford it. In some real-world studies, patient payment for obesity medications has been identified as a cause of higher discontinuation rates [12]. In this study, during data collection, the patient's visit date, prescribed dose, and number of liraglutide prescriptions were reviewed to determine whether the medication had been discontinued. This approach has the potential to provide adequate data for indirect assessment of patient adherence.
2.3. Statistical Analysis
Means (± standard deviation) were used to represent baseline variables. Percentages were used for categorical variables. The paired t-test was used to compare changes in continuous variables that were normally distributed over the follow-up period within the two groups (women and men). The independent t-test was used to compare changes in continuous variables that were normally distributed over the follow-up period between the two groups (women and men). Non-normally distributed continuous variables were described using the Mann-Whitney U test, whereas Pearson's chi-squared test (or Fisher's exact test) was used to compare categorical variables. A p < 0.05 (5%) was considered significant in all statistical analyses performed with IBM SPSS Statistics software for Windows, version 21.0.
3. Results
Initially, we reviewed the medical records of 72 patients with obesity who started treatment with liraglutide. Of these, 47 patients who reached the maximum dose of liraglutide (3.0 mg) during the five-week titration period and maintained this dose for at least 6 months of follow-up were included in the study.
Data were collected from 31 (65.9%) women and 16 (34.0%) men with a mean age of 50.8 (± 11.8) years, body weight of 110.2 (± 14.1) kg, and BMI of 39.3 (± 5.4) kg/m^2.
The baseline analysis (T0) showed no significant differences in BMI (37.5 ± 5.6 kg/m^2 vs. 40.1 ± 5.2 kg/m^2, p=0.12) and weight (115.4 ± 18.1 kg/m^2 vs. 108.3 ± 12.2 kg/m^2, p=0.10) between men and women (Table 1).
In the male group, the results showed a significant reduction in BW and BMI at 3 months (-10.7 ± 6.1 kg; -3.6 ± 2.4 kg/m^2, p<0.0001) and at 6 months (-17.9 ± 6.7 kg; -6.0 ± 2.7 kg/m^2, p<0.0001). Analysis of metabolic parameters showed a significant reduction in LDL cholesterol (-19.0 ± 16.5, p<0.0001) mg/dl and FIB-4 (-0.25 ± 0.23, p=0.05). No significant differences were observed in the change of HbA1c (-0.23 ± 0.9%, p=0.57), FBG (-8.1 ± 16.4 mg/dl, p=0.23), total cholesterol (-14.0 ± 32.6 mg/dl, p=0.23), HDL cholesterol (-2.0 ± 14.5 mg/dl, p=0.70), TG (-9.1 ± 59.9, p=0.68), creatinine (-0.02 ± 0.14 mg/dl, p=0.67), AST (-3.5 ± 5.6 U/L, p=0.12) and ALT (-5.0 ± 15.1 U/L, p=0.38). In the female group, the results showed a significant reduction in body weight and BMI at 3 months (-7.1 ± 3.1 kg; -2.6 ± 1.1 kg/m^2, p<0.0001) and at 6 months (-11.9 ± 5.3; -4.4 ± 1.9 kg/m^2, p<0.0001). Analysis of metabolic parameters showed a significant reduction in FBG (-5.4 ± 9.4 mg/dl, p=0.03). No significant differences were found in HbA1c (-0.16 ± 0.6%, p=0.31), total cholesterol (9.5 ± 22.1 mg/dl, p=0.11), LDL cholesterol (6.8 ± 21.2 mg/dl, p=0.20), HDL cholesterol (1.1 ± 7.1 mg/dl, p=0.59), TG (2.8 ± 51.9, p=0.83), creatinine (-0.02 ± 0.06 mg/dl, p=0.28), AST (-2.1 ± 4.8 U/L, p=0.10), ALT (-3.4 ± 7.7 U/L, p=0.10) and FIB-4 (-0.003 ± 0.12, p=0.92).
When comparing the two groups (men vs. women), men showed more significant reductions in weight (-10.7 ± 6.1 kg vs. -7.1 ± 3.1 kg, p<0.0001) at 3 months, and at 6 months (-17.9 ± 6.7 kg vs. -11.9 ± 5.3 kg, p<0.0001) of follow-up than women (Table 2; Figure 1).
Similar results were found for BMI, with men showing higher reduction (-3.6 ± 2.4 kg/m^2 vs. -2.6 ± 1.1 kg/m^2, p=0.08) at 3 months, and at 6 months (-6.0 ± 2.7 kg/m^2 vs. -4.4 ± 1.9 kg/m^2, p=0.07) of follow-up than women (Table 2; Figure 2).
At 3 months, WL > 5% was achieved in 93.7% (N=15/16) of men vs. 58.0% (N=18/31) of women (p<0.0001), and %WL was higher in men than in women (-9.2 ± 5.1% vs. -6.5 ± 2.9%, p<0.0001) (Table 2; Figure 3); at 6 months, WL > 10% was observed in 87.5% (N=14/16) of men vs. 29.0% (N=9/31) of women (p<0.0001), and %WL was higher in men than women (-15.2 ± 5.4 % vs. -10.5 ± 4.4 %, p<0.0001) (Table 2; Figure 3).
No significant differences in metabolic parameters were observed between the two groups, except for a significantly greater reduction in total cholesterol (-14.0 ± 32.6 mg/dl vs. 9.5 ± 22.1 mg/dl, p<0.0001) and LDL cholesterol (-19.0 ± 16.5 mg/dl vs. 6.8 ± 21.2 mg/dl, p<0.0001) (Table 3), and FIB-4 (-0.25 ± 0.23 vs. -0.003 ± 0.12, p<0.0001) in the male group than in the female group (Table 3).
4. Discussion
Obesity is a multifactorial condition characterized by excessive fat accumulation [1] resulting from complex interactions among physiological, social, cultural, and environmental factors [13]. In 2016, the World Health Organization estimated the global prevalence of obesity at 11% for men and 15% for women, while the World Obesity Federation predicts that by 2030, the prevalence of obesity will be higher in men (one in seven) than in women (one in five) [14].
Epidemiological differences in the prevalence of obesity by gender vary between countries and populations [15]. For example, data from the Italian National Institute of Statistics (ISTAT) in 2021 showed a higher prevalence of overweight in men compared to women (53.6% vs. 35.7%) [4].
Recognizing the role of gender in health management, funding agencies such as the Canadian Institutes of Health Research, the European Commission, and the U.S. National Institutes of Health have begun to require the inclusion of gender considerations in study design, and outcome analyses [6]. However, gender-specific evaluations of anti-obesity drugs remain limited.
Specifically, among the approved anti-obesity drugs, few studies have examined the gender-specific efficacy of orlistat, with conflicting results [16,17]. Similarly, for naltrexone/bupropion, a higher pharmacokinetic response (e.g., volume of distribution normalized for body weight, maximum plasma concentration) was observed in women than in men, but this was not confirmed by further studies [18,19,20].
For liraglutide, few studies have shown gender differences in its effects on weight loss [21], as well as in its pharmacokinetics and pharmacodynamics [6]. Furthermore, although studies have shown that the drug is associated with a 5-10% weight loss rate [22], which is considered clinically relevant for improving obesity-related complications and quality of life [23], it is not clear whether there are gender differences. In addition, limited research has been conducted on the gender response to the beneficial effects of GLP1-RAs on metabolic parameters such as glucose metabolism, lipid profiles, renal and hepatic function. This may explain why, to date, there are no published studies suggesting the need for gender-specific dosage recommendations for these drugs [6].
To this end, our study aims to evaluate the gender-specific responses to liraglutide 3.0 mg, the only GLP1-RAs approved in Italy for the treatment of obesity in people without T2D.
Our results show a higher prevalence in women (65.9%) than in men (34.0%), which is consistent with electronic medical records from different health care systems and clinical trials of anti-obesity drugs, which have shown that participants with obesity are more likely to be women than men [5; 6]. Similarly, Italian data from the international ACTION IO (Awareness, Care, and Treatment In Obesity MaNagement - an International Observation) study, which assessed the perceptions and barriers to obesity management among people with obesity and healthcare professionals, showed that men perceived weight management as less critical. One reason for this finding appears to be that men believe they can self-control their weight [24]. This observation may explain why a literature review of randomized clinical trials on this topic found difficulties in recruiting men, with an average sex ratio of 27% in men and 73% in women, posing challenges in recruiting participants of the male sex [25].
The main findings of our study are as follows:
- Both sexes showed significant reductions in WL and BMI after 3 and 6 months of liraglutide treatment, with significantly greater reductions in both weight (Figure 1), and BMI (Figure 2) in men. In addition, the percentage of patients achieving WL > 5% at 3 months and WL > 10% at 6 months was significantly higher in men.
As reported in the literature, liraglutide 3.0 mg has demonstrated greater inter-individual variability in weight loss response, but predictive models for individual treatment efficacy have not yet been developed [8]. Studies in the literature suggest that women tend to achieve greater weight loss with all GLP1-RA classes. This was confirmed by a retrospective study showing greater weight loss in women than in men after exenatide treatment (-7.0 kg vs. -3.3 kg) [26], and similar results were observed for BMI, with women showing greater reductions in BMI than men [21,27]. These results are not consistent with our findings, but it must be emphasized that these studies included patients with obesity and concomitant T2D status, different types of GLP1-RAs, and a mean age of patients < 50 years in the latter study.
For liraglutide 3.0 mg, a retrospective analysis of clinical trials showed that women achieved greater weight loss than men, suggesting that men may be less sensitive to liraglutide [7]. However, this analysis included populations with high variability in age, weight, BMI, and drug dose.
Taken together, the gender-specific effect of liraglutide on weight loss observed in the literature suggests that approximately 50% of the observed gender differences may be due to the greater exposure of women to liraglutide [28], probably related to their lower body surface area associated with their lower baseline body weight [29]. In contrast, another study found that women with higher baseline BMI were associated with greater weight loss [21], but these groups were not homogeneous, as these women were slightly heavier than men at on a baseline.
Pharmacokinetic analysis has shown that female sex is an independent predictor of increased exposure to liraglutide, which may contribute to improved weight loss outcomes [21]. However, the uniformity of baseline body weight and BMI characteristics between genders in our study may provide another explanation for these conclusions regarding differential drug exposure. In addition to pharmacokinetic analysis, differences in behavior and attitudes toward medications may also explain how gender influences response to anti-obesity therapies [28].
We hypothesize that possible mechanisms behind the higher response of men than women suggested by our study may be linked to age-related factors. In fact, the mean age of both sexes was about 50 years, which can be considered as the perimenopausal period in women, and hormonal changes may affect the results of treatment. In fact, menopause is associated with weight gain and changes in body composition due to increased adipose tissue, especially visceral fat, and decreased lean mass [30].
- 2.
- The analysis of metabolic parameters showed a significant reduction in total and LDL cholesterol, and FIB-4 in men. However, there was no significant gender difference in glucose metabolism and renal function.
Previous literature has highlighted gender differences in HbA1c responses to GLP1-RAs, with females showing superiority in the 18-64 age group, and males showing superiority in the 65+ age group [21,31]. These differences are difficult to interpret because this study included patients treated with other hypoglycemic agents. In addition, a higher percentage of women than men started with a higher baseline HbA1c (>7%), which was associated with a higher likelihood of achieving glycemic control during follow-up.
Regarding the lipid profile, we observed a greater significant reduction in total cholesterol and LDL cholesterol in men than in women. It is important to evaluate whether the effects of GLP1-RAs on these variables recognized as CVD risk factors show patterns of sexual dimorphism. Although several studies have examined the effect of GLP1-RAs on CVD risk, few have stratified this analysis by sex. Only one study with exenatide showed no reduction in LDL cholesterol in women, suggesting the possible existence of a sex-specific effect of the drug on the lipid profile [21,32]. We hypothesize that these differences could be explained either by direct effects of liraglutide in men or by menopause-related metabolic changes in women, including central adiposity and lipid profile changes [33].
Although the potential reno-protective effects of liraglutide have been documented, gender-specific effects remain underexplored [34]. In our study, minimal changes in serum creatinine were observed with no significant gender differences.
Finally, liraglutide has demonstrated efficacy in improving liver function and reducing the severity of nonalcoholic fatty liver disease (NAFLD), but without gender-based analysis [35,36]. Our results highlighted a reduction in liver enzymes and FIB-4 in both groups, but significantly slightly higher in men.
4.1. Study Limitations and Strenghts
Although our study provides valuable information on gender-specific responses to liraglutide therapy, several limitations must be acknowledged. These include the small sample size, which is predominantly female as in the literature, and the retrospective study design. In addition, the study did not take into account confounding factors such as dietary habits and physical activity levels.
Despite these limitations, the strength of our study lies in its comprehensive real-world evaluation of participants who reached maximum treatment doses after regular titration, thereby improving internal validity. In addition, the focus of our study on a homogeneous cohort of participants goes beyond previous literature and provides further insight into the gender-specific response to liraglutide therapy.
5. Conclusions
In conclusion, although the World Health Organization (WHO) declared obesity a global epidemic in 1997 [37], gender-specific considerations are often overlooked in the clinical management of this disease. Our study suggests a gender difference in the response to liraglutide 3.0 mg therapy, with a greater therapeutic effect in men.
Possible explanations for our findings include sex-specific pharmacodynamics or hormonal influences, which warrant further investigation through large-scale randomized clinical trials to better understand the underlying mechanisms of gender-specific responses.
Given the increased risk of cardiovascular disease (CVD) in men, their reluctance to acknowledge their obesity status [38], and the large impact that improvements in weight, lipid profiles, and liver disease have on CVD risk, our findings may encourage clinicians to increase the involvement of the male population in screening and weight management programs. This proactive approach may be particularly beneficial for men, not only because of their higher cardiovascular risk compared to women, but also because they tend to be underrepresented in weight management interventions.
Author Contributions
Conceptualization, Danila Capoccia; Data curation, Gloria Guarisco, Marianna Chinucci and Chiara Gaita; Methodology, Ilaria Milani, Gloria Guarisco, Marianna Chinucci and Chiara Gaita; Supervision, Frida Leonetti and Danila Capoccia; Validation, Frida Leonetti; Writing – original draft, Ilaria Milani; Writing – review & editing, Frida Leonetti and Danila Capoccia. All authors proofread the manuscript and agreed with the submission and publication.
Funding
This research received no funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the retrospective nature of the study.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wang J-Y, Wang Q-W, Yang X-Y, et al. (2023) GLP−1 receptor agonists for the treatment of obesity: Role as a promising approach. Front. Endocrinol14:1085799. [CrossRef]
- Malik, V.S., Willet, W.C. & Hu, F.B. (2020), Nearly a decade on — trends, risk factors and policy implications in global obesity. Nat Rev Endocrinol 16, 615–616. [CrossRef]
- Boutari, Chrysoula et al. (2022) A 2022 update on the epidemiology of obesity and a call to action: as its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism: clinical and experimental, Vol 133. [CrossRef]
- Italian Central Statistics Institute (Istituto Nazionale di Statistica). BES 2021: Equitable and sustainable well-beeing in Italy, Available at: https://www.istat.it/it/files/2021/10/BES-Report-2020.pdf.
- 5. Cooper, A.J., Gupta, S.R., Moustafa, A.F. et al. (2021) Sex/Gender Differences in Obesity Prevalence, Comorbidities, and Treatment. Curr Obes Rep 10, 458–466 https://doi.org/10.1007/s13679-021-00453-x.
- Muscogiuri, G., Verde, L., Vetrani, C., Barrea, L., Savastano, S., & Colao, A. (2024). Obesity: a gender-view. Journal of endocrinological investigation, 47(2), 299–306. [CrossRef]
- Cataldi, M., Muscogiuri, G., Savastano, S., et al. (2019). Gender-related issues in the pharmacology of new anti-obesity drugs. Obesity reviews: an official journal of the International Association for the Study of Obesity, 20(3), 375–384. Gender-related issues in the pharmacology of new anti-obesity drugs. [CrossRef]
- Jensterle, M., Rizzo, M., Haluzík, M. et al. (2022) Efficacy of GLP-1 RA Approved for Weight Management in Patients With or Without Diabetes: A Narrative Review. Adv Ther 39, 2452–2467. 39. [CrossRef]
- Santini, S., Vionnet, N., Pasquier, J., et al. (2023). Marked weight loss on liraglutide 3.0 mg: Real-life experience of a Swiss cohort with obesity. Obesity (Silver Spring, Md.), 31(1), 74–82. [CrossRef]
- ElSayed, N. A., Aleppo, G., Aroda, V. R, et al. (2023). 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes-2023. Diabetes care, 46(Suppl 1), S19–S40. [CrossRef]
- European Association for Study of Liver, & Asociacion Latinoamericana para el Estudio del Higado (2015). EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. Journal of hepatology, 63(1), 237–264. [CrossRef]
- Tempia Valenta, S., Stecchi, M., Perazza, F. et al. (2023) Liraglutide 3.0 mg and mental health: can psychiatric symptoms be associated to adherence to therapy? Insights from a clinical audit. Eat Weight Disord 28, 99. [CrossRef]
- Kapoor, N., Arora, S., & Kalra, S. (2021). Gender Disparities in People Living with Obesity - An Unchartered Territory. Journal of mid-life health, 12(2), 103–107. [CrossRef]
- World Obesity Federation. World Obesity Atlas 2022. London: World Obesity Federation; (2002) 4:1–289. Available at: https://www.worldobesity.org/resources/resource-library/world-obesity-atlas-2022.
- Jaacks, L. M., Vandevijvere, S., Pan, A., et al. (2019). The obesity transition: stages of the global epidemic. The lancet. Diabetes & endocrinology, 7(3), 231–240. [CrossRef]
- Tchoukhine, E., Takala, P., Hakko, H., et al. (2011). Orlistat in clozapine- or olanzapine-treated patients with overweight or obesity: a 16-week open-label extension phase and both phases of a randomized controlled trial. The Journal of clinical psychiatry, 72(3), 326–330. [CrossRef]
- Robertson, C., Avenell, A., Boachie, C., et al. (2016). Should weight loss and maintenance programmes be designed differently for men? A systematic review of long-term randomised controlled trials presenting data for men and women: The ROMEO project. Obesity research & clinical practice, 10(1), 70–84. [CrossRef]
- Stewart, J.J., Berkel, H.J., Parish, R.C. et al. (2001), Single-Dose Pharmacokinetics of Bupropion in Adolescents: Effects of Smoking Status and Gender. The Journal of Clinical Pharmacology, 41: 770-778. [CrossRef]
- Findlay, J.W.A., Van Wyck Fleet, J., Smith, P.G. et al. (1981) Pharmacokinetics of bupropion, a novel antidepressant agent, following oral administration to healthy subjects. Eur J Clin Pharmacol 21, 127–135. [CrossRef]
- Laib, A. K., Brünen, S., Pfeifer, P., Vincent, P., & Hiemke, C. (2014). Serum concentrations of hydroxybupropion for dose optimization of depressed patients treated with bupropion. Therapeutic drug monitoring, 36(4), 473–479. [CrossRef]
- Rentzeperi, E., Pegiou, S., Koufakis, T., Grammatiki, M., & Kotsa, K. (2022). Sex Differences in Response to Treatment with Glucagon-like Peptide 1 Receptor Agonists: Opportunities for a Tailored Approach to Diabetes and Obesity Care. Journal of personalized medicine, 12(3), 454. [CrossRef]
- Nuffer, W. A., & Trujillo, J. M. (2015). Liraglutide: A New Option for the Treatment of Obesity. Pharmacotherapy, 35(10), 926–934. [CrossRef]
- Wharton, S., Liu, A., Pakseresht, A., Nørtoft, E., et al. (2019). Real-World Clinical Effectiveness of Liraglutide 3.0 mg for Weight Management in Canada. Obesity (Silver Spring, Md.), 27(6), 917–924. [CrossRef]
- Sbraccia, P., Busetto, L., Santini, F. et al. (2021) Misperceptions and barriers to obesity management: Italian data from the ACTION-IO study. Eat Weight Disord 26, 817–828 (2021). [CrossRef]
- Pagoto, S. L., Schneider, K. L., Oleski, J. L., Luciani, J. M., Bodenlos, J. S., & Whited, M. C. (2012). Male inclusion in randomized controlled trials of lifestyle weight loss interventions. Obesity (Silver Spring, Md.), 20(6), 1234–1239. [CrossRef]
- Buysschaert, M., Preumont, V., Oriot, P. R., et al. (2010). One-year metabolic outcomes in patients with type 2 diabetes treated with exenatide in routine practice. Diabetes & metabolism, 36(5), 381–388. [CrossRef]
- Quan, H., Zhang, H., Wei, W., & Fang, T. (2016). Gender-related different effects of a combined therapy of Exenatide and Metformin on overweight or obesity patients with type 2 diabetes mellitus. Journal of diabetes and its complications, 30(4), 686–692. [CrossRef]
- Mirabelli, M.; Chiefari, E.; Caroleo, P.; et al (2020) Long-Term Effectiveness of Liraglutide for Weight Management and Glycemic Control in Type 2 Diabetes. Int. J. Environ. Res. Public Health, 17, 207. [CrossRef]
- Overgaard, R.V., Petri, K.C., Jacobsen, L.V. et al. Liraglutide 3.0 mg for Weight Management: A Population Pharmacokinetic Analysis. Clin Pharmacokinet 55, 1413–1422 (2016). [CrossRef]
- Kodoth, V., Scaccia, S., & Aggarwal, B. (2022). Adverse Changes in Body Composition During the Menopausal Transition and Relation to Cardiovascular Risk: A Contemporary Review. Women's health reports (New Rochelle, N.Y.), 3(1), 573–581. [CrossRef]
- Durden, E., Lenhart, G., Lopez-Gonzalez, L., Hammer, M., & Langer, J. (2016). Predictors of glycemic control and diabetes-related costs among type 2 diabetes patients initiating therapy with liraglutide in the United States. Journal of medical economics, 19(4), 403–413. [CrossRef]
- Pencek, R., Blickensderfer, A., Li, Y., Brunell, S. C., & Anderson, P. W. (2012). Exenatide twice daily: analysis of effectiveness and safety data stratified by age, sex, race, duration of diabetes, and body mass index. Postgraduate medicine, 124(4), 21–32. [CrossRef]
- Ryczkowska, K., Adach, W., Janikowski, K., Banach, M., & Bielecka-Dabrowa, A. (2022). Menopause and women's cardiovascular health: is it really an obvious relationship?. Archives of medical science : AMS, 19(2), 458–466. [CrossRef]
- Li, K., Sun, J., Huang, N., Ma, Y., Han, F., Liu, Y., Hou, N., & Sun, X. (2020). Liraglutide improves obesity-induced renal injury by alleviating uncoupling of the glomerular VEGF-NO axis in obese mice. Clinical and experimental pharmacology & physiology, 47(12), 1978–1984. [CrossRef]
- Lv, X., Dong, Y., Hu, L., Lu, F., Zhou, C., & Qin, S. (2020). Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) for the management of nonalcoholic fatty liver disease (NAFLD): A systematic review. Endocrinology, diabetes & metabolism, 3(3), e00163. [CrossRef]
- Yen, FS., Hou, MC., Wei, J.CC. et al. (2024) Effects of glucagon-like peptide-1 receptor agonists on liver-related and cardiovascular mortality in patients with type 2 diabetes. BMC Med 22, 8 (2024). [CrossRef]
- James W. P. (2008). WHO recognition of the global obesity epidemic. International journal of obesity (2005), 32 Suppl 7, S120–S126. [CrossRef]
- Crimmins, E. M., Shim, H., Zhang, Y. S., & Kim, J. K. (2019). Differences between Men and Women in Mortality and the Health Dimensions of the Morbidity Process. Clinical chemistry, 65(1), 135–145. [CrossRef]
Figure 1.
Weight loss after 3 months and 6 months of Liraglutide 3.0 mg treatment.
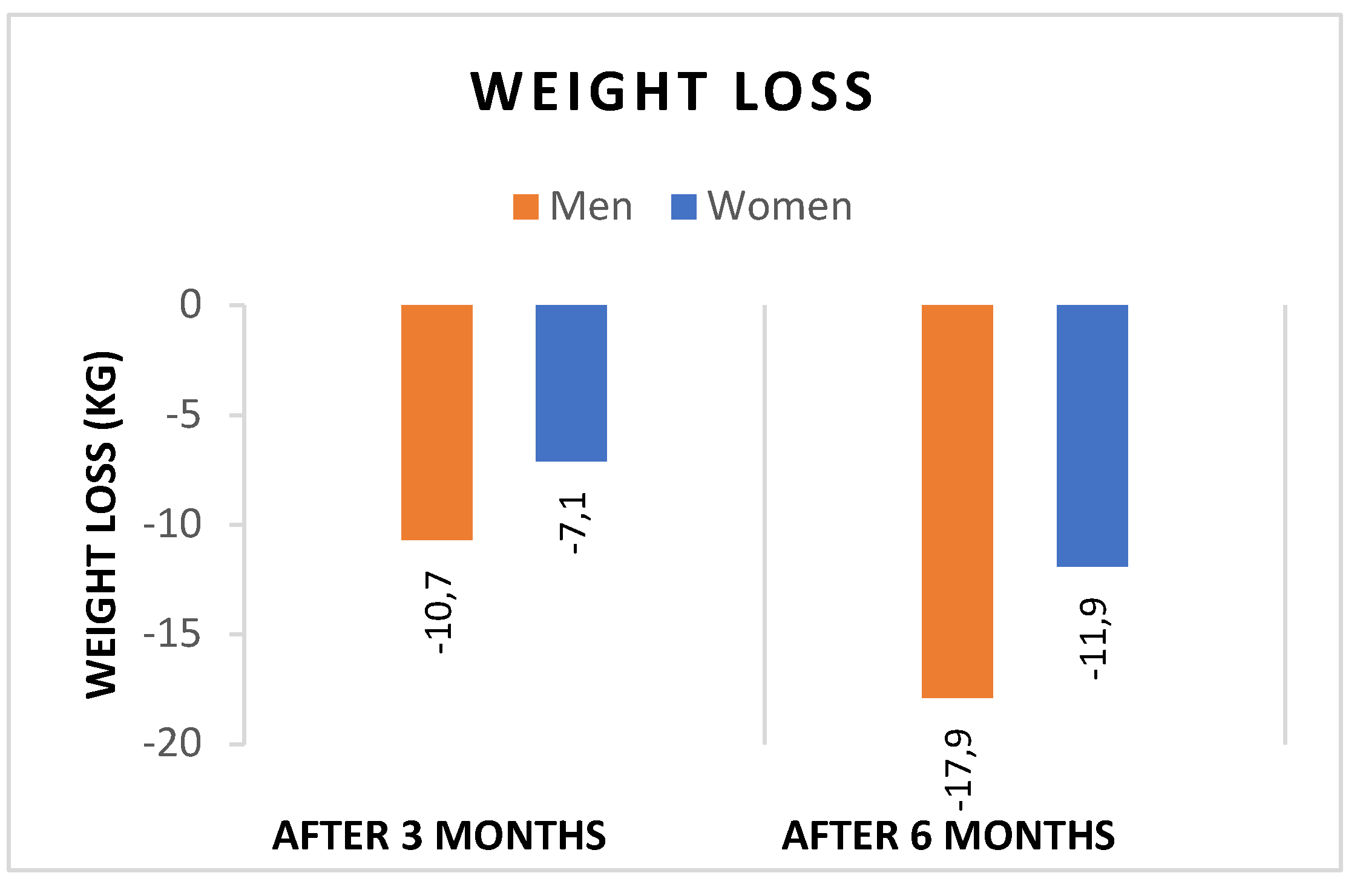
Figure 2.
BMI change after 3 months and 6 months of Liraglutide 3.0 mg treatment.
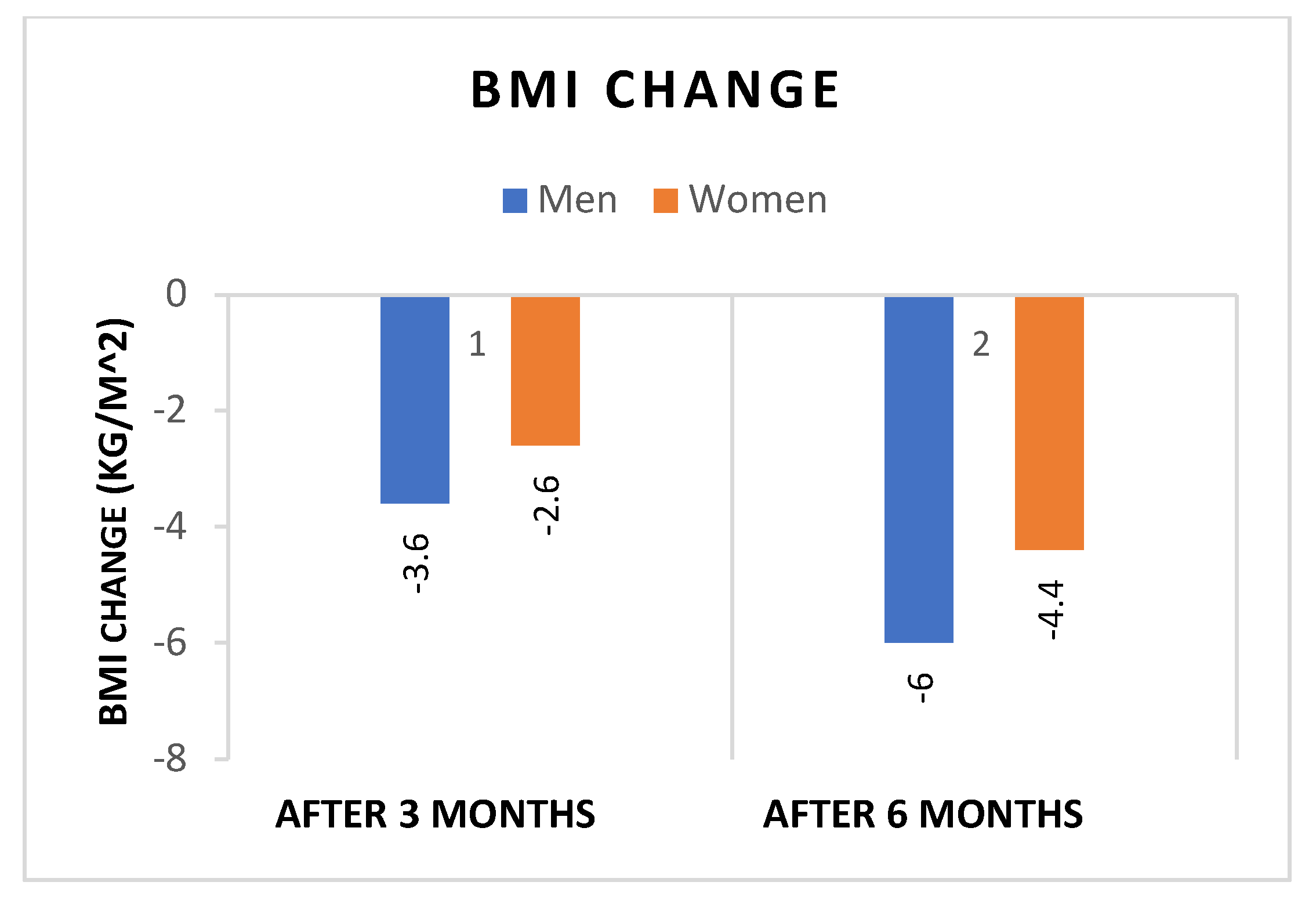
Figure 3.
Percentage of weight loss after 3 months and after 6 months of Liraglutide 3.0 mg treatment.
Figure 3.
Percentage of weight loss after 3 months and after 6 months of Liraglutide 3.0 mg treatment.
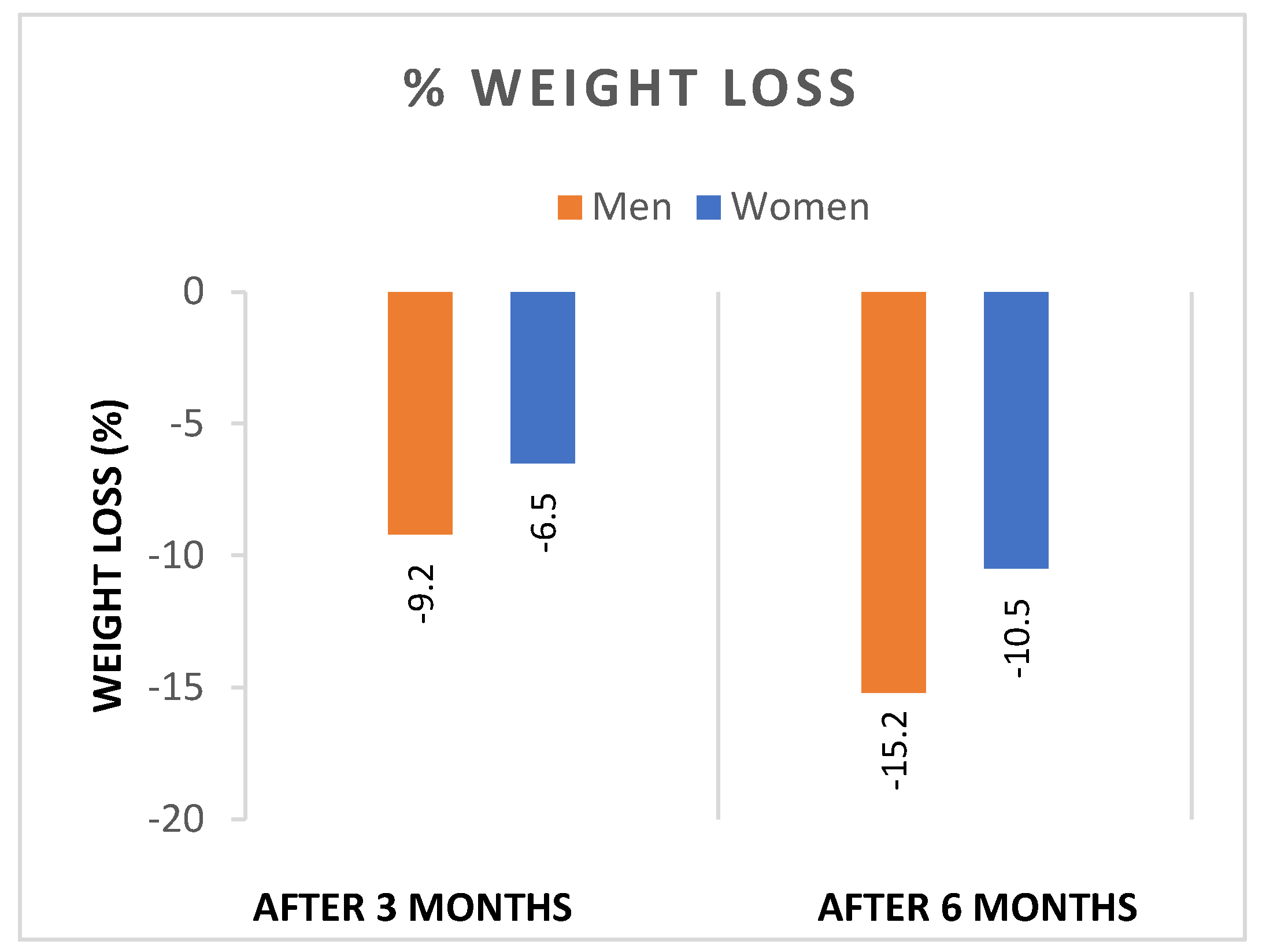

Table 1.
Baseline (T0) clinical characteristics of the study population (n = 47) treated with Liraglutide 3.0 mg.
Table 1.
Baseline (T0) clinical characteristics of the study population (n = 47) treated with Liraglutide 3.0 mg.
| Men | Women | p-value | |
|---|---|---|---|
| Gender (%) | 16/47 (34.0%) | 31/47 (65.9%) | |
| Age (years) | 52 ± 14.3 | 50 ± 11.5 | p=0.46 |
| Weight (kg) | 115.4 ± 18.1 | 108.3 ± 12.2 | p=0.12. |
| BMI (kg/m2) | 37.5 ± 5.6 | 40.1 ± 5.2 | p=0.10 |
| FBG (mg/dl) | 99.8 ± 20.9 | 92.3 ± 13.6 | p=0.16 |
| HbA1c (%) | 5.7 ± 0.54 | 5.54 ± 0.3 | p=0.16 |
| Total cholesterol (mg/dl) | 180.2±42.7 | 180.9 ± 26.6 | p=0.95 |
| LDL (mg/dl) | 106.0 ± 33.6 | 103.3± 25.3 | p=0.79 |
| HDL (mg/dl) | 50.2 ± 6.3 | 51.3 ± 9.8 | p=0.72 |
| TG (mg/dl) | 141.6 ± 73.5 | 115.6 ± 68.0 | p=0.31 |
| Creatinine /mg/dl) | 1.0 ± 0.2 | 0.7 ± 0.1 | <0.0001 |
| AST (U/L) | 23.45 ± 9.4 | 18.2 ± 4.2 | <0.0001 |
| ALT (U/L) | 33.2 ± 19.4 | 20.5 ± 6.7 | <0.0001 |
| FIB-4 | 1.1 ± 0.3 | 0.7 ± 0.3 | <0.0001 |
Data are mean ± standard deviation (SD) or n (%). BMI= Body Mass Index; HbA1c: glycated hemoglobin; LDL= Low Density Lipoprotein; HDL: High Density Lipoprotein; FBG= blood glucose; TG= triglycerides; FIB-4= Fibrosis-4 index; AST= Aspartate Transaminase; ALT= Alanine Transaminase.
Table 2.
Changes in weight, BMI, %WL and %WL >5-10% after 3 months (T1) and 6 months (T2) of Liraglutide treatment.
Table 2.
Changes in weight, BMI, %WL and %WL >5-10% after 3 months (T1) and 6 months (T2) of Liraglutide treatment.
| Men | Women | p-value | |
|---|---|---|---|
| Weight (kg) | |||
| T1-T0 | -10.7 ± 6.1 | -7.1 ± 3.1 | <0.0001 |
| T2-T1 | -17.9 ± 6.7 | -11.9 ± 5.3 | <0.0001 |
| BMI (kg/m2) | |||
| T1-T0 | -3.6 ± 2.4 | -2.6 ± 1.1 | p=0.08 |
| T2-T0 | -6.0 ± 2.7 | -4.4 ± 1.9 | p=0.07 |
| %WL | |||
| T1-T0 | -9.2 ± 5.1 | -6.5 ± 2.9 | <0.0001 |
| T2-T1 | -15.2 ± 5.4 | -10.5 ± 4.4 | <0.0001 |
| WL > 5 % | N=15/16, 93.7% | N=18/31, 58.0% | <0.0001 |
| WL > 10 % | N=14/16, 87.5% | N=9/31, 29.0% | <0.0001 |
Data are mean ± standard deviation (SD) or n (%). WL=weight loss; %WL= Percentage weight loss; BMI= Body Mass Index;.
Table 3.
Changes in metabolic parameters after 3 months (T1) and 6 months (T2) of Liraglutide treatment.
Table 3.
Changes in metabolic parameters after 3 months (T1) and 6 months (T2) of Liraglutide treatment.
| Men | Women | p-value | |
|---|---|---|---|
| FBG (mg/dl) T2-T0 | -8.1 ± 16.4 | -5.4 ± 9.4 | p=0.61 |
| HbA1c (%) T2-T0 | -0.23 ± 0.9 | -0.16 ± 0.6 | p=0.83 |
| Total cholesterol (mg/dl) T2-T0 | -14.0± 32.6 | 9.5 ± 22.1 | <0.0001 |
| LDL (mg/dl) T2-T0 | -19.0 ± 16.5 | 6.8 ± 21.2 | <0.0001 |
| HDL (mg/dl) T2-T0 | -2.0 ± 14.5 | 1.1 ± 7.1 | p=0.14 |
| TG (mg/dl) T2-T0 | -9.1 ± 59.9 | 2.8 ± 51.9 | p=0.56 |
| Creatinine (mg/dl) T2-T0 | -0.02 ± 0.14 | -0.02 ± 0.06 | p=0.99 |
| AST (U/L) T2-T0 | -3.5 ± 5.6 | -2.1 ± 4.8 | p=0.54 |
| ALT (U/L) T2-T0 | -5.0 ± 15.1 | -3.4 ± 7.7 | p=0.74 |
| FIB-4 T2-T0 | -0.25 ± 0.23 | -0.003 ± 0.12 | <0.0001 |
Data are mean ± standard deviation (SD) or n (%). HbA1c: glycated hemoglobin; LDL= Low Density Lipoprotein; HDL: High Density Lipoprotein; FBG= blood glucose; TG= triglycerides; FIB-4= Fibrosis-4 index; AST= Aspartate Transaminase; ALT= Alanine Transaminase.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



