
Submitted:
10 May 2024
Posted:
10 May 2024
You are already at the latest version
Abstract
Traumatic vascular injuries consist in direct or indirect damage to arteries and/or veins and accounts for 3% of all traumatic injuries. Typical consequences are hemorrhage and ischemia.
Extremities vascular injuries can occur isolated or in association in major trauma with other organ injuries. They account for 1-2% of patients admitted to Emergency Department, for approximately 50% of all arterial injuries. Lower extremities are more frequently injured than the upper ones in adult population.
The outcome of vascular injuries is strictly correlated to the environment and the time background. Treatment can be challenging notably in polytrauma because of the dilemma of which injury should be prioritized and treatment delay can cause disability or even death especially for limb vascular injury.
Our purposes are to discuss the role of Computed Tomography Angiography (CTA) in the diagnosis of vascular trauma and its optimized protocol to achieve the definitive diagnosis, and to assess the radiological signs of vascular injuries and the possible pitfalls.
Keywords:
peripheral arterial injuries
; CTA
; CT Angiography
; vascular trauma
; blunt trauma
; penetrating trauma
; dissection
; transection
; pseudoaneurysm
Introduction
Vascular trauma accounts for 3% of all traumatic injuries[1,2,3]. Extremities vascular injuries can occur isolated or in association in major trauma with other organ injuries and they account for 1-2% of patients admitted to emergency room (ER) and account for approximately 50% of all arterial injuries [4,5,6], with a prevalence of lower extremities injuries over the upper extremities in adult population [7]. Traumatic vascular injury is characterized by damage to arteries and/or veins. Typical consequences are hemorrhage and ischemia, and the outcome of vascular injuries is strictly correlated to the environment and the time background [8]. Treatment delay can cause disability or even death especially for limb vascular injury, physiological and preclinical studies reveal that muscle damage is present at 3 hours of ischemia time and is near complete, and irreversible, at 6 hours [9,10]. Vascular peripheral injury is highly morbid and limb salvage is a rule rather than an exception [11,12], it can occur in isolation or as a part of polytrauma and the treatment can be challenging because of the dilemma of which injury should be prioritized [11,12].
Types of Peripheral Vascular Injuries
One of the most important things to understand is that vascular injury is not synonymous with active bleeding. Vascular injury manifestations include hemorrhage and ischemia. Vessel injuries can manifest as vasospasm, contusion, intimal flaps, intimal disruption or hematoma, external compression, laceration, transection, focal wall defect with pseudoaneurysm, arteriovenous fistula [13,14]. Vessel disruption is the most common injury and can be complete or incomplete. It may also present as an expanding or pulsatile hematoma. Complete disruption presents with active hemorrhage decreasing in time due to spasm and thrombosis. In incomplete disruption, blood flow can be maintained, ischemia may not occur, and pseudoaneurysm can develop [15]. Intimal injuries lead to thrombosis or intimal flap formation that may cause distal ischemia. Dissection caused by intimal injuries may also have a delayed presentation.
In penetrating traumas, arteriovenous fistulas may frequently occur, in relation to the narrow course between arteries and veins, furthermore these lesions may have a delayed presentation. Arterial spasm determines reversible limb ischemia, but all other vascular lesions should be first excluded[15,16].
Mechanism of Peripheral Vascular Injuries
Limb ischemia is the primary cause of concern in distal extremity injuries with peripheral arterial trauma; whereas proximal transections of the axillo-subclavian or ilio-femoral axis represent a life-threatening risk of exsanguination due to a greater caliber of the vessels and greater difficulty in compression in these locations [5].
Vascular injury can occur in blunt, penetrating, blast, and iatrogenic trauma.
In civilian settings, blunt trauma has always been the leading cause of injury but penetrating trauma is becoming more frequent because of the increase of urban violence [17,18,19,20]. Gunshot injuries depend on projectile velocity, mass, and characteristics [21,22], and they determine severe tissue damage. Penetrating stab wounds have low energy character and constitute 70-90% of cases [23] and usually result in lacerations or transection without contusion [24]. Vessel transection can be complete or incomplete, in complete transection artery often retract and spams with sequentially thrombosis, instead massive bleeding can occur in incomplete transection. In penetrating trauma, according to the extent of the wound, various clinical manifestations may occur, from a puncture wound with minimal bleeding and minute signs of peripheral ischemia to a large laceration of the skin with life-threatening hemorrhage [25].
Blunt vascular trauma is the effect of the shearing or compressive forces that lead to contusion, tearing, and dissection of the blood vessel, and it is often the result of major soft tissue loss and concomitant fractures [14,26].
Blast trauma is the consequence of explosive detonation, and vessel injury may be damaged by a duplex mechanism. The blast wave determines shrapnel secondary fragment that damage vessels directly as it happens in penetrating trauma, on the other hand the blast wind determines body displacement and injury are related to blunt mechanism [15,16]. Iatrogenic vascular injuries are defined as injuries sustained to an artery during an operation and percutaneous interventions, and they are becoming more frequent with the development of mini-invasive and endovascular techniques [27,28]. The most common complication of vascular access in the endovascular approach is hematoma and pseudoaneurysm in the access site [29]. The rate of these incidents varies between 0.5 and 1.0% and recently was decreased using various vascular sealing systems. When arterial vessels are iatrogenically damaged, massive bleeding is rare.Arteriovenous fistula, intimal lesion, thrombosis, rupture, acute limb ischemia, and pseudoaneurysm may also occur. The common femoral artery is the most common site of this trauma, and damage may occur at the vessel access point, at the site of intervention, or anywhere in between [15].
Vascular injury during orthopedic surgery is not a frequent complication, with an incidence of 0.05–0.1% [30,31]. During the hip or knee replacement, the mechanism of injury is usually indirect, as in blunt trauma, from torsion and elongation forces that result in intimal tear and vessel thrombosis. During the open repositions, the mechanism is usually direct, as in penetrating trauma caused by a stabilization material and fixation that results in arterial damage.
The common injury sites are in the upper limbs the armpit, the medial part of the arm, and the ulnar fossa due to a superficial position of the vascular structures; in the lower limb, the groin, the medial thigh area, and the popliteal fossa [25]. Most peripheral vascular injuries involve the superficial femoral artery or brachial artery [32]. Vascular trauma can be or cannot be associated with bone fractures, and the absence of bone fractures cannot exclude the presence of vascular damage. Common fractures associated with loss of distal perfusion are those with bone displacement, segmentation, comminution, or floating joint [5]. The most common location is the femur with an associated wedge-shaped or butterfly fragment at a level close to Hunter’s canal, fracture dislocations of the knee, fracture dislocations of the ankle. Severe soft tissue and bony injury distal to the trifurcation of the leg arteries are frequently associated with injury to all three calf vessels with often non-viable muscle in multiple compartments and segmental bone loss with a high risk of amputation.
Primary Survey
Specific procedures of bleeding control should be carried out during the pre-hospital settings. Open extremity fractures occur in an environment of high energy transfer [33] and are rarely associated with major hemorrhage. Control of catastrophic hemorrhage is the first stage of the primary survey, together with airway management and cervical spine stabilization (CABCDE: Circulation (exsanguinating hemorrhage), Airway, Breathing, Circulation, Disability, Exposure) [34]. Hemorrhage control may be achieved by applying direct wound compression and compression dressing to the source of major bleeding, and contemporaneity maintaining tissue perfusion. Tourniquet has been used in military settings, although in civilian settings, the use of limb constrictive devices before the onset of hemorrhagic shock provides temporary control of hemorrhage and precious time to transfer the patient safely to the hospital [15]. A tourniquet is usually applied on the arm or thigh, less often in distal areas (forearm, below the knee), usually 8 cm above the suspected vascular lesion [25,33]. The time of tourniquet application must be noted or written to avoid unnecessarily prolonged ischemia. Blind clamping of an actively bleeding vessel is potentially detrimental to vascular tissue and accompanying nerves and should be avoided. Hemostatic dressings and substances are used, and they usually take 3–5 min to initiate coagulation between the dressing and injury site [35,36].
Whether accompanied by major hemorrhage or not, a devascularised limb associated with an open fracture [37], is a clinical emergency requiring prompt recognition and treatment.
In this setting, the Gustilo-Anderson classification, a grading system of open fractures, is used to predict limb-threatening septic complications that require secondary amputation on the basis of the degree of soft-tissue injury in mangled extremity injuries. These injuries (type IIIB and IIIC) involve at least three of the four major systems: integument, soft tissue, bone, nerves and vessels [38] (Figure 1). Type IIIC fractures are characterized by extensive bone loss, periosteal stripping with devitalized fragments, massive contamination, poor soft-tissue coverage and arterial injuries that require reperfusion[5]. Approximately 40% of Gustavo type III fractures are associated with significant arterial injuries[5,37,39,40].
Blood loss and hemodynamic instability are higher in proximal artery injuries, and upper and lower arterial limb injuries may present differently because of morphological differences in vessel size and muscle compartments [7].
Recognition is based on hard clinical signs, including lack of palpable pulses, continued bleeding, or an expanding hematoma [41]. Fractures or joint dislocations should be reduced as this may restore distal circulation. The assessment of pulses should not rely on the use of Doppler ultrasound and the ankle-brachial pressure index (ABPI) [42].
Diagnosis of Peripheral Vascular Injuries
Clinical Manifestations
Hemorrhage and tissue ischemia are the main clinical manifestations of vascular trauma. Symptoms of lower limb vascular injuries can be described as hard or soft signs. Hard signs include arterial bleeding, loss of pulse, expanding hematoma, bruit or thrill, and signs of ischemia, and indicate the need for immediate surgical intervention [5]. The classic 6P syndromes defined as paresthesia, pulselessness, paralysis, pain, pallor, and poikilothermia can diagnose damage to lower limbs arteries.
Soft signs include a history of prehospital blood loss, diminished pulse, moderate hematoma, proximity to a large vessel or bony injury, and ipsilateral neurologic deficit, and indicate the need for further diagnostic imaging [11,12,43]. It is important to underline that negative clinical exams do not rule out vascular trauma, especially in the calf, where low blood compensation can masquerade the vessel injury[11,12,44].
Auxiliary Examination
The ankle-brachial-index (ABI) is the ratio of ankle blood pressure to brachial blood pressure and can identify limb ischemia. A normal ABI index (>0.90) has a high sensitivity to rule out vascular injury in the lower limb; instead, an ABI <0.90 necessitates further investigation [45,46]. ABI represents an important diagnostic tool in the evaluation of lower limb injuries (10, 11, 44), but preexisting peripheral vascular disease makes it less reliable, necessitating additional imaging [11,12].
Many traumatic vascular lesions can be occult on clinical examination, such as non-flow-limiting pseudoaneurysm of inline arteries and transections of nonline arteries such as the profunda femoris [47].
Ultrasound
Ultrasound (US) is widely used in the setting of trauma, and peripheral vascular examination may detect features of vascular injuries such as luminal narrowing, intramural hematoma, flaps, posttraumatic stenosis, the” yin-yang” sign characteristic of pseudoaneurysm and acute occlusion [11,12,48,49]. The use of Color Doppler increase ultrasound accuracy and has a sensitivity up to 94% [11,12,50]. US has several limits in the diagnosis of peripheral vascular injuries with a certain false negative rate. Ultrasound is operator-dependent and requires experienced staff, and more importantly cannot access some areas due to bony structures, open wounds, large hematomas, bulky dressing, or splints [11,12,51]. Moreover, high BMI and subcutaneous emphysema negatively impact ultrasound examination [11,12,52].In penetrating trauma, ultrasound is not sensible enough to rule out vascular injuries [52,53,54]. Generally, Doppler US and the ankle-brachial pressure index (ABPI) are associated with a substantial false negative rate and inter-observer variability[15,33,42] so they are not routinely used to rule out vascular injuries, instead positive US may obviate CTA [52,55].
MDCTA or CTA
Digital Subtraction Angiography (DSA) is considered the gold standard in peripheral vascular injuries, allowing diagnosis and treatment, however, the technological progress of Multidetector Computed Tomography (MDCT) scanners makes MDCT with CT Angiography (CTA) the imaging of choice in evaluating patients with suspected peripheral artery injuries, replacing DSA as first diagnostic step allowing an accurate definition of peripheral vascular injuries and other associated trauma lesions [11,12]. Moreover, because vascular limb traumas can occur in isolation or as a part of polytrauma, total body CTA may be performed in a single time, allowing the detection of vascular limbs and other cranial-neck-thoracic-abdominal-pelvic and musculoskeletal injuries. Currently, 85% of patients with multi-system trauma undergo admission whole-body trauma CT [10,56]; with simultaneous considerations of extremities and intracavitary injuries[32,41,57].
CT angiography is not indicated routinely in polytraumatized patients, but in the case of risk factors (open fractures, distal tibia fractures, multiple fractures in one extremity, or isolated fractures of the proximal third of the fibula) with at least 1 between hard and soft signs (hard signs: absent distal pulses, pulsatile bleeding, cold/pale limb, expanding hematoma, palpable thrill, audible bruit; soft signs: decreased pulses compared to the contralateral side, any peripheral nerve deficit(s), small local hemorrhage(s), a wound near an artery, non-pulsatile hematoma) [5,30,38,55,56,58] however, in patients with suspected vascular injuries, a negative CTA was also used as rationale for immediate discharge [59].
CTA Protocol
A specific protocol for a patient suspected limb trauma should be chosen both on the parameters of the scanner and about whether the CTA is acquired alone or as part of a whole-body examination [5].
The patient is supine positioned feet first. Scanning width and position of the limbs depend on the context: in polytrauma patients, the volume is extended to the lower limbs, with legs at the isocenter to the gantry and feet slightly externally rotated; containment bands are always preferred if injuries allow them and especially in uncooperative patients. The upper limbs involved are imaged in adduction along the flanks, favoring the traumatized side in centering the patient; depending on the size of the patient, one or both upper limbs can be included in this way.
In the case of isolated limb trauma, the position of the lower limbs is identical, while the positioning of the upper limbs depends on the type of trauma. If possible, the injured upper limb is placed over the head with the palm raised and extended fingers, if not the arm is scanned in a prone position with the upper limb adducted along the flanks. In some severe injured upper limb trauma, the patient may be not able to mobilize the arm and it can be scanned adducted to the body[57,60].
All devices that can generate artifacts, such as rings and chains, should be removed before scanning if possible. Pillows and tape can be used to immobilize the upper extremity and fingers as much as possible.
About the contrast agent, the higher the iodine concentration, the better the quality of the study because the higher the density of the vessels.
Vascular venous access is obtained with an angiocath caliber of 18- or 20-gauge adequate for the flow (at least 3 ml/sec), followed by a 40-mL saline flush at the same rate.
The positioning of the intravenous cannula should be chosen concerning the body area to be studied; for evaluating the lower limbs, the venous access should be positioned in the antecubital fossa and on the opposite site of the injured arm to prevent that the dense venous contrast obscures the arterial side. However, in the case of a study of both upper limbs, in the absence of a central venous access, a pedideal venous access could be chosen, which however would not allow the use of high flows[61].
The amount of contrast agent depends on the patient weight, iodine delivery rate (IDR) and on the length of the scanning duration. The examination starts with a biplane scout topogram to prescribe the scanning range and FOV.
CT scans are acquired in the caudal-cranial direction from the inferior aspect of the aortic arch to the tips of the fingers and in the cranio-caudal direction when the upper limbs are placed above the head [60].
It is suggested to acquire an unenhanced scan to focus spontaneous hyper densities such as bone fragments and for comparison with the post-contrast acquisitions, to better understand contrast agent distribution. If dual energy CT machine is available, the use of virtual unenhanced scan can be considered as well as iodine maps that may help in the detection of vascular alterations[62]. Then a multiphasic CT study is suggested with arterial, portal phase with delayed phase acquisition in selected cases[63].
Arterial scanning delay is determined by automated bolus tracking with the region of interest on the aortic arch for the upper limb examinations or in the whole-body CT examination, and on the abdominal aorta in case of lower limb examinations. Automated bolus tracking is recommended to obtain optimal acquisition timing, particularly in patients with decrease cardiac output.
The venous scan is acquired about 60-70 seconds after the contrast agent injection and is essential to detect venous injuries and bleeding and to differentiate contained vascular injuries from actively bleeding lesions[64].
Late phase, acquired 180 seconds after the contrast agent injection, offers a further help in detecting late bleeding and solve doubts [64].
CTA Imaging Findings
CTA features of arterial traumas reflect the depth of mural involvement, and they are characterized by different CT findings (Figure 2) [5,65,66]:
- Arterial Transections represents the complete rupture of the vessel, and determines the loss of distal opacification, a massive hematoma and active bleeding [5] (Figure 3). Active arterial bleeding is visualized as contrast extravasation in the arterial phase, which enlarges in venous and delayed phases [67]. In partial transection, the arterial tear involves the three layers of the vessel wall, without affecting the entire vessel’s circumference, distal opacification is appreciable although reduced luminal caliber and opacification can be detected [5,55].
- Pseudoaneurysm is caused by focal arterial wall tear involving intimal and medial layers, and represents a collection of blood contained only by the adventitia layer or surrounding tissue [5,56,59]. It appears as an outpouching sac with a round and smooth margin in continuity with the arterial adjacent lumen (Figure 4). Pseudoaneurysm bleeding appears as irregular, lobulated perilesional contrast blush [65,68]. Pre-exiting calcification or pseudoaneurysm should be differentiate form active bleeding; delayed phase acquisition can be useful because in active bleeding the contrast extravasation dissipates along tissue planes instead pseudoaneurysm and calcification remain stable [60,67].
- Dissection is caused by an intimal tear, resulting into an intimal flap, which can float in the vessel lumen or cause occlusion [5]; at CT it appears as a semilunar luminal deformation or eccentric stenosis or complete occlusion. Findings in dissection can be subtle but if evident at CT, the intimal flap can be classically seen as a linear flap within the vessel lumen [5,65,69,70] (Figure 5).
- Luminal narrowing: the vessel wall appears lobulated with eccentric narrowing, it can be the result of extrinsic compression, non-occlusive thrombus, or dissection (Figure 3).
- Vasospasm: it is represented by a concentric, focal and segmental luminal narrowing with smooth margin, caused by the contraction of the arterial wall, as a response to an injury [5].It can be difficult to differentiate from an intimal tear and occlusion in distal small arteries [71,72]. The differential diagnosis between vasospam and dissection often requires DSA for the proper management (Figure 6).
Figure 3.
CTA, coronal planes, MIP (A), and 3D reconstructions (B). Arterial transections of proximal and medium tracts of right superficial femoral artery. In this patient, it could be noted both the complete loss of opacification of the proximal tract (white arrows) and the lower opacification of the downstream revascularized tract (yellow arrows) of the right superficial femoral artery, with reduced luminal caliber (narrowing).
Figure 3.
CTA, coronal planes, MIP (A), and 3D reconstructions (B). Arterial transections of proximal and medium tracts of right superficial femoral artery. In this patient, it could be noted both the complete loss of opacification of the proximal tract (white arrows) and the lower opacification of the downstream revascularized tract (yellow arrows) of the right superficial femoral artery, with reduced luminal caliber (narrowing).

Figure 4.
CTA, axial planes. Right common femoral artery pseudoaneurysm can be noted (arrow). It appears as an outpouching sac with a round margin in continuity with the arterial adjacent lumen. In this case, imminent signs of rupture of the pseudoaneurysm can be seen, as irregular and lobulated margins and the adjacent hematoma.
Figure 4.
CTA, axial planes. Right common femoral artery pseudoaneurysm can be noted (arrow). It appears as an outpouching sac with a round margin in continuity with the arterial adjacent lumen. In this case, imminent signs of rupture of the pseudoaneurysm can be seen, as irregular and lobulated margins and the adjacent hematoma.
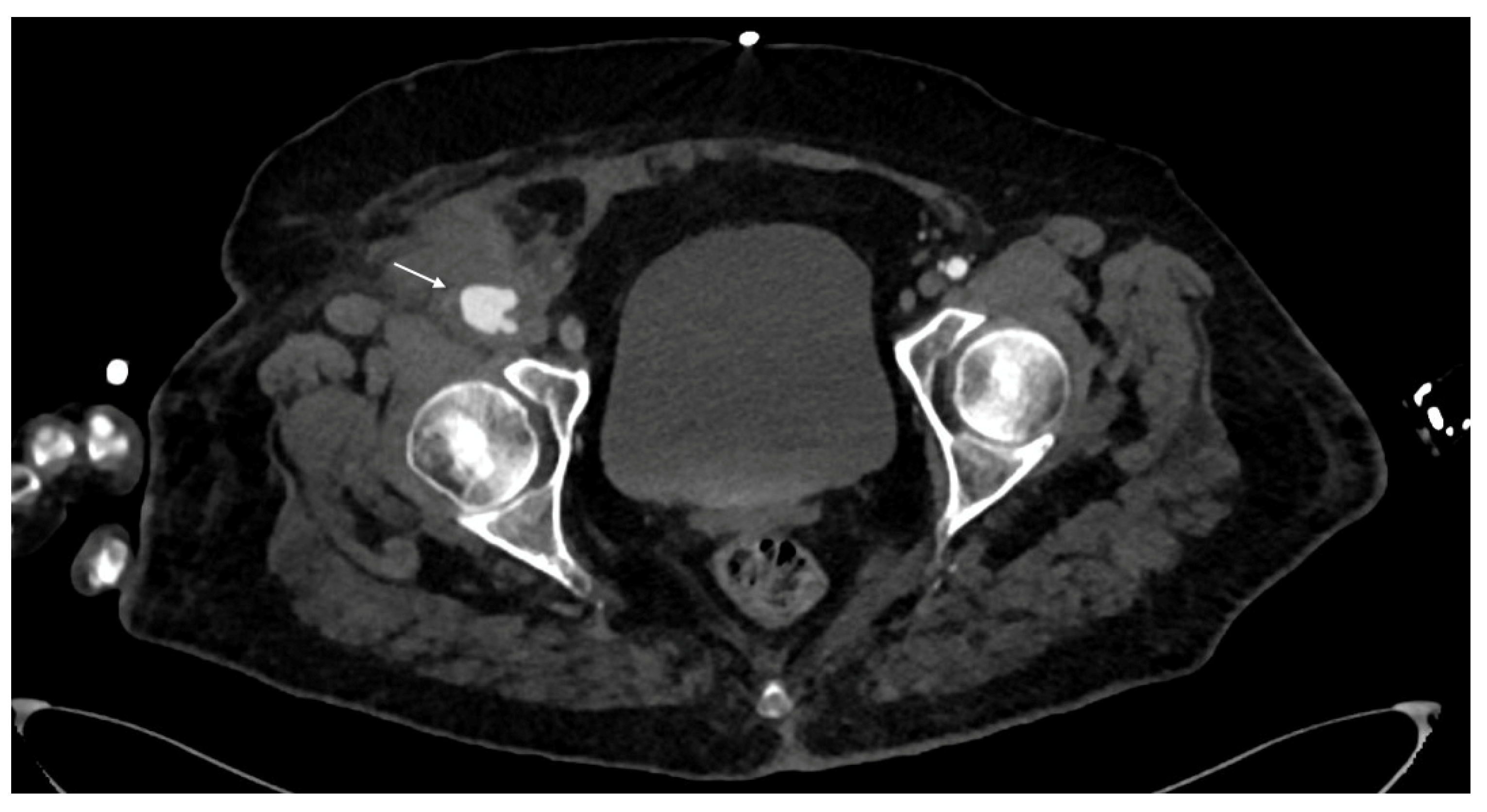
Figure 5.
CTA, axial planes. Right deep femoral artery dissection can be seen (arrow), resulting in a linear flap within the vessel lumen.
Figure 5.
CTA, axial planes. Right deep femoral artery dissection can be seen (arrow), resulting in a linear flap within the vessel lumen.
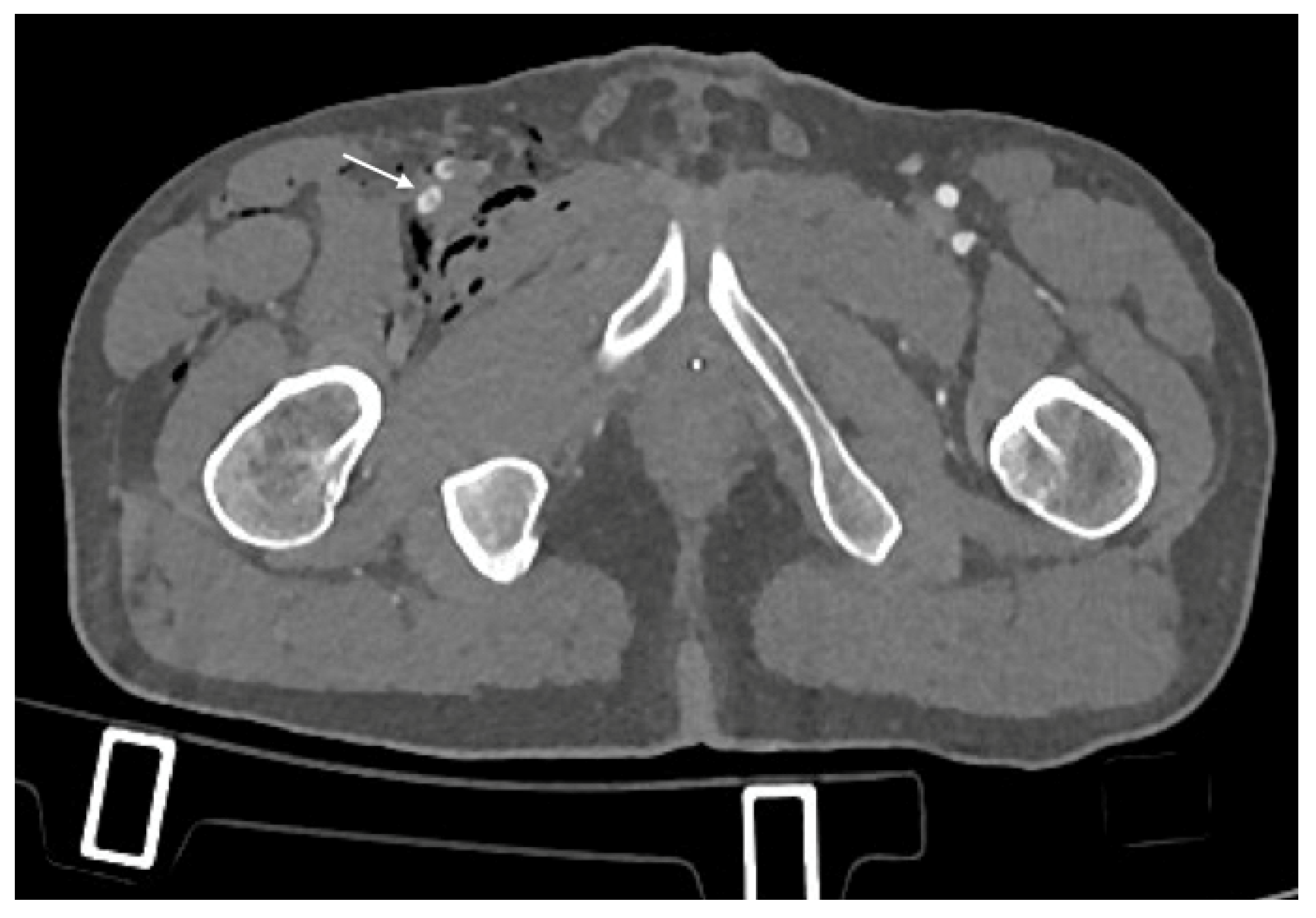
Figure 6.
CTA, axial planes. Left popliteal arteriovenous fistula: a direct connection between the artery and the vein with early venous enhancement in the arterial phase and communicating channel with the artery can be detected (arrow).
Figure 6.
CTA, axial planes. Left popliteal arteriovenous fistula: a direct connection between the artery and the vein with early venous enhancement in the arterial phase and communicating channel with the artery can be detected (arrow).
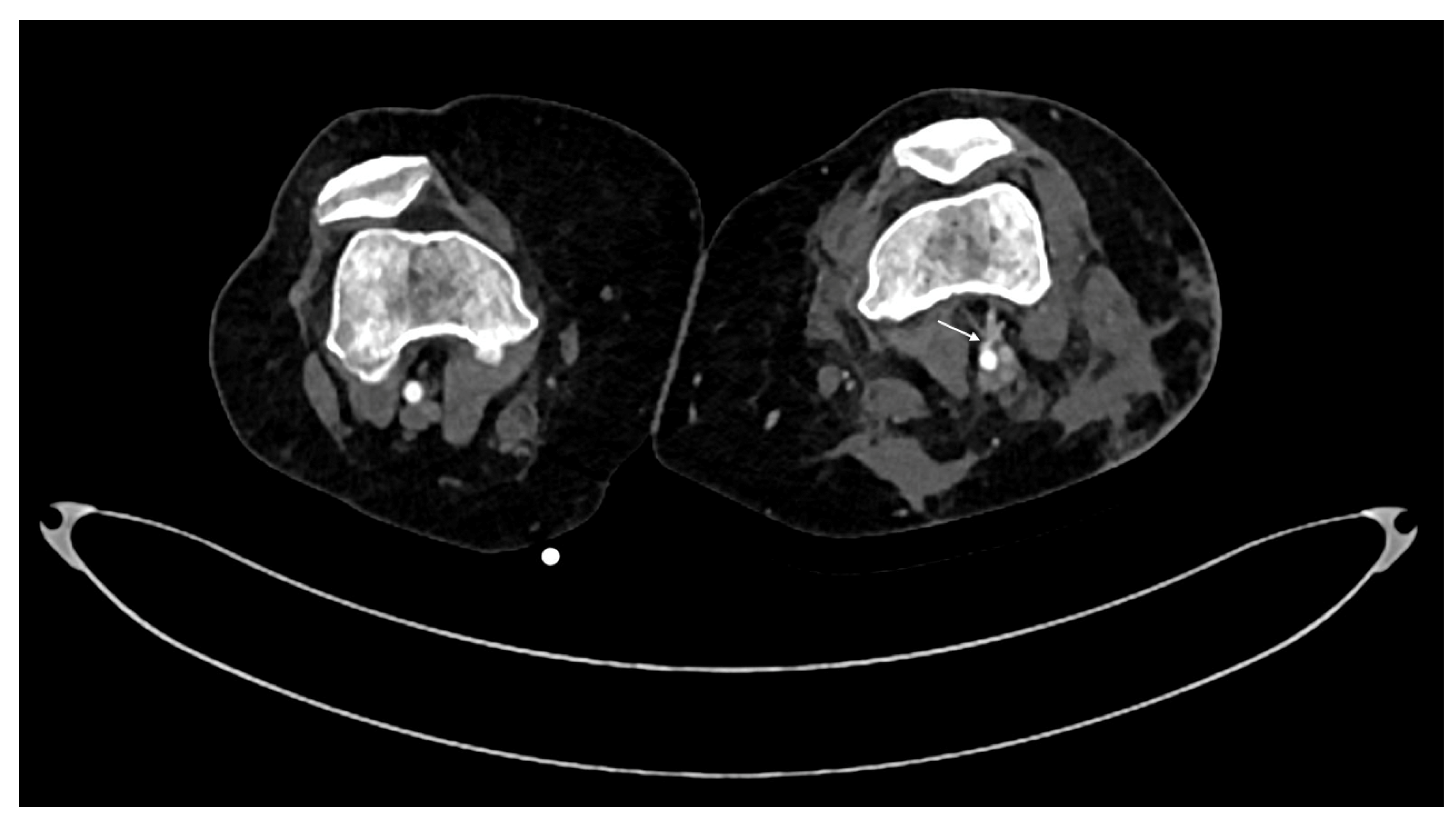
Figure 7.
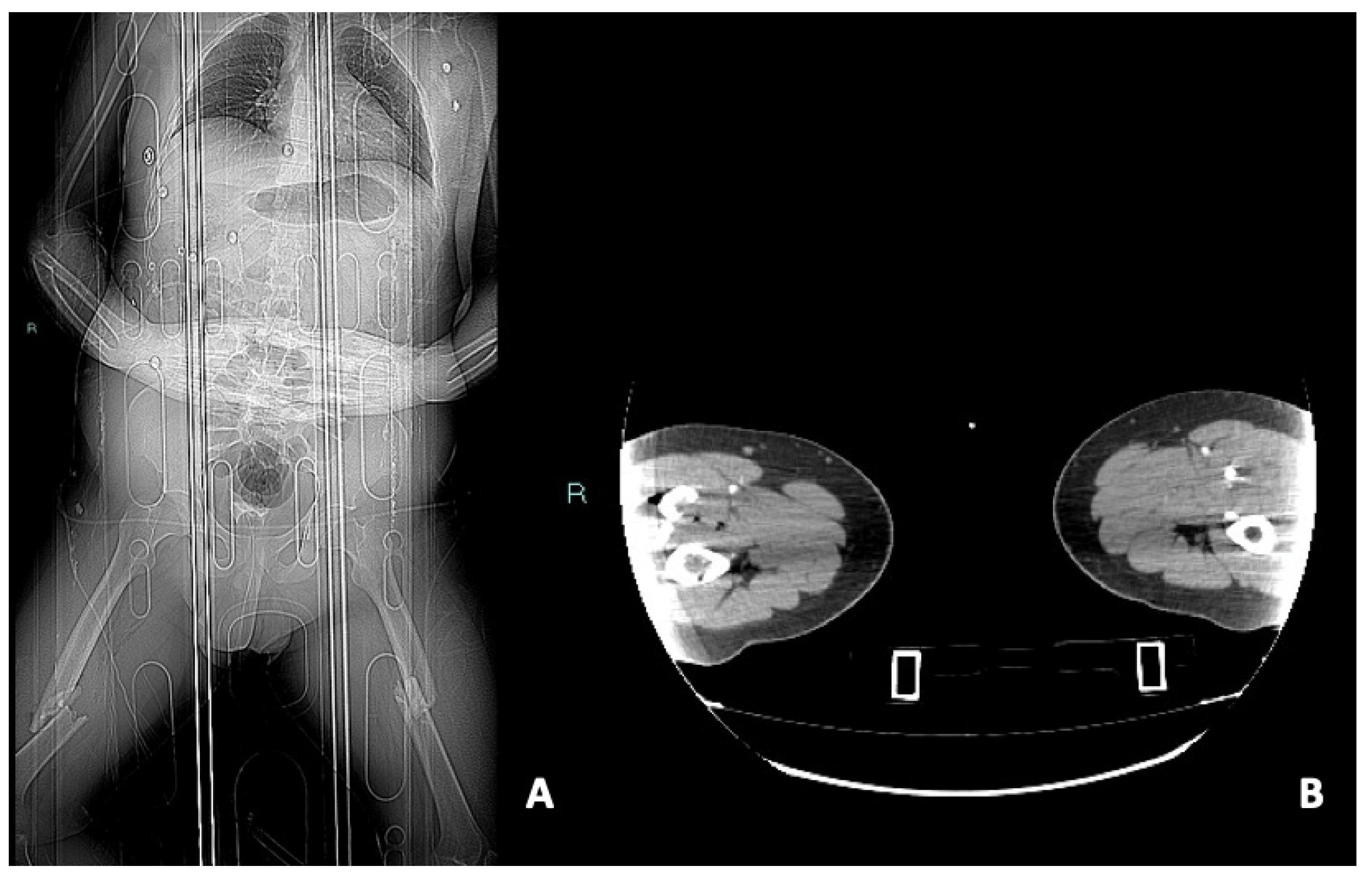
CTA scout (A) and arterial phase, axial planes (B). In this case, the correct positioning with a wide field of view was not possible, causing nondiagnostic examination. When these conditions happen, a second limb acquisition is essential and could be performed by decentralizing the patient on the CT table and focusing the exam on the limb of interest.
Figure 7.
CTA scout (A) and arterial phase, axial planes (B). In this case, the correct positioning with a wide field of view was not possible, causing nondiagnostic examination. When these conditions happen, a second limb acquisition is essential and could be performed by decentralizing the patient on the CT table and focusing the exam on the limb of interest.
MDCT Protocol and Reporting
MDCT exam acquisition in peripheral vascular trauma can be challenging. In isolated limb trauma, CTA of lower or upper limbs can be acquired with specific protocol, taking into account that optimal acquisition of upper limbs in traumatic patients can be difficult and not optimal because of the limitation to raise both arms owing to injury. Bolus tracking, fixed delays, and test injection are recommended, and test injection is recommended. A fixed delay of 20-30 sec in healthy patients has been proposed in order to image both upper and lower limbs [60,66]adequately. In polytraumatized patients, an adequate examination of the upper and lower limbs can be challenging, and 8% of extremity trauma CTA have been reporting nondiagnostic [66] due to early scan timing for body trauma assessment. With a second contrast arterial bolus and with the advent of dual source, the midcalf and forearm can be reimaged with the same bolus and minimal venous opacification interference [65,73]. It’s preferable to use a wide-field-of view that includes both limbs, which helps the radiologist to assess vascular trauma by comparing the two sides and to determine technique equivocal findings due to distal nonenhancement for early scan timing[72]. Other factors that may negatively influence CTA diagnostic accuracy are artifacts related to beam hardening from hardware, ballistic fragments, and debris [73]. Mechanism of trauma should be taken into account, especially in penetrating gunshot injuries, to adopt higher peak kilovoltage and tube current, narrow collimation and iterative protocol in order to reduce artifacts[5].
CTA reporting should include description of arterial damage with its location and length, degree of stenosis (>50% luminal caliber) and level of restitution [68]. The precise determination of the length between the transition point of a normal artery and an abnormal artery can be difficult to assess, especially in the case of a long non opacified segment. The accuracy in determining the extension of vascular lesion can be underestimated due to adjacent soft tissue [5,74]. In penetrating trauma wound tracks or ballistic fragments within 5 mm of a neurovascular bundle must be considered suggestive of vascular injury [75].
Madhuripan et al. [67] proposed a systematic approach to CTA, that can be useful in clinical practice. The exam should be first evaluated to assess the quality of vessel opacification. MIP (maximum intensity projection) are useful for a first and fast primary assessment of exam quality and major findings. MPR and 3D images provide a global view of findings and, if possible, the comparison of both limbs could be helpful in pointing out the lesion that should be conformed on axial images. Each vessel should be examined on axial images carefully for caliber, wall alteration, opacification, and extravasation. Meticulous assessment of major vessels run-off is relevant and major branches need to be followed along their course. Particularly attention should be given to perforators in both upper and lower limbs especially in penetrating trauma. Smaller branches opacification of arches of hands and feet is variable and vascular damage should be rule out in case of distal ischemia and no proximal vascular damage. Postprocessing workstation can be used with vascular optional tools to aid the diagnosis. Assessment of nonvascular structures should be carried out in standard and bone windows (fractures, hematomas, soft tissue, lacerations, foreign bodies). Incidental findings should be reported [67].
CTA Pitfalls
Correct positioning with a wide field of view is essential but not always possible, causing nondiagnostic examination[76] (Figure 7). A second limb acquisition could be performed by decentralizing the patient on the CT table and focusing the exam on the limb of interest
Distal poor opacification may occur if adequate flow if not obtained or for delays due to cardiac output, in the latter situation bolus tracking may be helpful [66].Non optimal opacification especially of distal arteries may be avoided with a second contrast bolus or with a second acquisition immediately after the first arterial phase. In penetrating trauma or in case of severe compressing hematomas, a delayed phase may be acquired to determine late extravasation[76].
Motion artifacts should be avoided immobilizing the patients [66]. Streak artifacts from metallic fragments could determine CT diagnostic inaccuracy (Figure 8), the iterative filter should be applied in order to reduce these artifacts and distal vessels should be carefully examined [66]. In comminuted fracture, radiologists must pay attention to individuating active bleeding among bony fragments, comparing the unenhanced and arterial phases. Satisfaction errors should be avoided because 12% of patients presents concomitant multiple vascular injuries [7,38,60,66,67,70,76,77,78,79].
Peripheral Vascular Injury Grading
Characteristically peripheral vascular injuries (PVI) are graded based on location and not on the type of lesion, according to the AAST Organ Injury Scale grading of PVI (Table 1), and can be distinguished into occlusive or nonocclusive, depending on vascular patency [7]. Nonocclusive injuries are intimal irregularity/tear (Grade I, <25% narrowing), dissection/intramural, hematoma (Grade II, ≥25% narrowing), or partial transection with pseudoaneurysm formation (Grade III). Occlusive injuries include thrombotic occlusion (Grade IV, vessel wall is preserved) or complete transection (Grade V) [7]. The more common arteries involved are radial and ulnar arteries in the upper limb and the popliteal and superficial femoral arteries in the lower limbs [6,7]. Depending on the percentage of vessel circumference involved, lesion should be upgraded if more than 50% of vessel circumference in involved, and oppositely downgraded if less than 25% of vessel circumference is involve.
CTA Timing in Peripheral Vascular Injury Assessment
An ABI of >0.9 at clinical examination generally excludes the need for additional imaging. On the other hand, patients with hard signs of PVI should be directed to the operating room and in multiple penetrating and blunt vascular trauma a hybrid operating room allows also to perform angiography for diagnostic and therapeutical purposes without delay in treatment [11,12].
Hemodynamically unstable patients with soft signs of PVI should be directed to the operating room for resuscitation and appropriate evaluation/intervention [7]. The other category of patients that requires immediate exploration without the need for imaging are patients with peripheral vascular injury and signs of ischemia[81,82].
In hemodynamically stable patients with concerns of PVI, additional evaluation (ABI and ultrasound evaluation), but the presence of peripheral pulses alone cannot reliably exclude vascular injuries, and the presence of clinical signs requires further investigation [77]. Since 2012, the Eastern Association for the Surgery of Trauma (EAST) guidelines [7,79] considers CTA the first-line modality for investigating blunt and penetrating PVIs [78] with clinical suspect of PVI. DSA in these patients should be reserved for interventional purposes or if CTA is nondiagnostic or inconclusive due to artifacts from retained metallic objects [7,69].
Complication of Peripheral Vascular Injuries
Davenport et al. (13) reported poor prognostic factors of vascular injury repair. First, the delay in treatment (>6 hours) determines irreversible muscle damage[9,83]. Other negative prognostic factors that should be considered are pre-existing chronic lower limb ischemia, initial clinical presentation with limb ischemia, injury to lower extremities, and an absent Doppler Ultrasound signal at hospital admission. Factors that also negatively influence the outcome are a blunt traumatic mechanism and other associated injuries requiring immediate treatment. Pseudoaneurysms are more common in penetrating and iatrogenic trauma, and they are determined by a partial vessel disruption with bleeding in a contained intramural hematoma. Arteriovenous fistulas are more frequent in penetrating trauma, and they can develop later as pulsatile and palpable thrill. Compartment syndrome develops when the pressure within the muscular compartment rises above 30 mmHg, and it is caused by a reperfusion injury after ischemia and is more common in young males with muscle mass [84]. Predisposing factors to compartment syndrome are crush injury, prolonged hypotension, arterial occlusion or a combined arterial and venous injury, and vein ligation. It more commonly occurs as result of tibial shaft fractures or distal radius fractures [84], and CT imaging is not advocated for the diagnosis of compartment syndrome, although at CT muscle enlargement with focal or geographic areas of hypoattenuation may indicate rhabdomyolysis, and intramuscular collection with peripheral rim enhancement may indicated signs of myonecrosis [85]. Early fasciotomies need to be considered and high suspicious should be carried out in these patients. Unluckily amputation can represent the first line treatment in case of severe soft tissue damage, irreversible ischemia, and neurological damage. Amputation may also be determined by delay in diagnosis of popliteal artery and crural vessel damages or if there have been delays in resuscitation.
Conclusions
CTA of peripheral vascular trauma requires knowledge of vessels anatomy and deep understanding of trauma mechanism in order to properly identify lesions.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study.
Informed Consent Statement
Patient consent was waived.
Data Availability Statement
Date are available on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Feliciano DV RT: Evaluation and treatment of vascular injuries. In: Skeletal Trauma Basic Science, Management and Reconstruction. edn. Philadelphia: Elsevier Saunders; 2015: 423-435.
- Mattox, K.L.; Feliciano, D.V.; Burch, J.; Beall, A.C., Jr.; Jordan, G.L., Jr.; De Bakey, M.E. Five thousand seven hundred sixty cardiovascular injuries in 4459 patients. Epidemiologic evolution 1958 to 1987. Ann Surg 1989, 209, 698–705, discussion 706-697. [Google Scholar] [CrossRef] [PubMed]
- Michaels, A.J.; Gerndt, S.J.; Taheri, P.A.; Wang, S.C.; Wahl, W.L.; Simeone, D.M.; Williams, D.M.; Greenfield, L.J.; Rodriguez, J.L. Blunt force injury of the abdominal aorta. J Trauma 1996, 41, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Branco, B.C.; Musonza, T.; Long, M.A.; Chung, J.; Todd, S.R.; Wall, M.J., Jr.; Mills, J.L., Sr.; Gilani, R. Survival trends after inferior vena cava and aortic injuries in the United States. J Vasc Surg 2018, 68, 1880–1888. [Google Scholar] [CrossRef] [PubMed]
- Dreizin, D.; Smith, E.B.; Champ, K.; Morrison, J.J. Roles of Trauma CT and CTA in Salvaging the Threatened or Mangled Extremity. Radiographics 2022, 42, E50–E67. [Google Scholar] [CrossRef] [PubMed]
- Franz, R.W.; Shah, K.J.; Halaharvi, D.; Franz, E.T.; Hartman, J.F.; Wright, M.L. A 5-year review of management of lower extremity arterial injuries at an urban level I trauma center. J Vasc Surg 2011, 53, 1604–1610. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, L.; Coimbra, R.; Goes, A.M.O., Jr.; Reva, V.; Santorelli, J.; Moore, E.E.; Galante, J.; Abu-Zidan, F.; Peitzman, A.B.; Ordonez, C.; et al. American Association for the Surgery of Trauma-World Society of Emergency Surgery guidelines on diagnosis and management of peripheral vascular injuries. J Trauma Acute Care Surg 2020, 89, 1183–1196. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.L.; Li, J.Y.; Jiang, P.; Jia, W.; Tian, X.; Cheng, Z.Y.; Zhang, Y.X. Literature review of peripheral vascular trauma: Is the era of intervention coming? Chin J Traumatol 2020, 23, 5–9. [Google Scholar] [CrossRef]
- Blaisdell, F.W. The pathophysiology of skeletal muscle ischemia and the reperfusion syndrome: a review. Cardiovasc Surg 2002, 10, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Schueller, G.; Scaglione, M.; Linsenmaier, U.; Schueller-Weidekamm, C.; Andreoli, C.; De Vargas Macciucca, M.; Gualdi, G. The key role of the radiologist in the management of polytrauma patients: indications for MDCT imaging in emergency radiology. Radiol Med 2015, 120, 641–654. [Google Scholar] [CrossRef]
- Ntola, V.C.; Hardcastle, T.C. Diagnostic Approaches to Vascular Injury in Polytrauma-A Literature Review. Diagnostics (Basel), 2023; 13. [Google Scholar]
- Ntola, V.C.; Hardcastle, T.C.; Nkwanyana, N.M. Management of vascular injuries on ICU patients: KZN experience. Injury 2024, 111418. [Google Scholar] [CrossRef]
- Evans, C.; Chaplin, T.; Zelt, D. Management of Major Vascular Injuries: Neck, Extremities, and Other Things that Bleed. Emerg Med Clin North Am 2018, 36, 181–202. [Google Scholar] [CrossRef]
- Iacobellis, F.; Scaglione, M.; Brillantino, A.; Scuderi, M.G.; Giurazza, F.; Grassi, R.; Noschese, G.; Niola, R.; Al Zuhir, N.Y.S.; Romano, L. The additional value of the arterial phase in the CT assessment of liver vascular injuries after high-energy blunt trauma. Emerg Radiol 2019, 26, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Davenport, R.T.N.; Walsh, M. Vascula Trauma. Surgery (Oxford) 2009, 27, 331–336. [Google Scholar] [CrossRef]
- Perkins, Z.B.; De’Ath, H.D.; Aylwin, C.; Brohi, K.; Walsh, M.; Tai, N.R. Epidemiology and outcome of vascular trauma at a British Major Trauma Centre. Eur J Vasc Endovasc Surg 2012, 44, 203–209. [Google Scholar] [CrossRef]
- Frykberg, E.R. Popliteal vascular injuries. Surg Clin North Am 2002, 82, 67–89. [Google Scholar] [CrossRef] [PubMed]
- Rozycki, G.S.; Tremblay, L.N.; Feliciano, D.V.; McClelland, W.B. Blunt vascular trauma in the extremity: diagnosis, management, and outcome. J Trauma 2003, 55, 814–824. [Google Scholar] [CrossRef]
- Feliciano, D.V.; Moore, E.E.; West, M.A.; Moore, F.A.; Davis, J.W.; Cocanour, C.S.; Scalea, T.M.; McIntyre, R.C., Jr. Western Trauma Association critical decisions in trauma: evaluation and management of peripheral vascular injury, part, I.I. J Trauma Acute Care Surg 2013, 75, 391–397. [Google Scholar] [CrossRef]
- Sciarretta, J.D.; Macedo, F.I.; Otero, C.A.; Figueroa, J.N.; Pizano, L.R.; Namias, N. Management of traumatic popliteal vascular injuries in a level I trauma center: A 6-year experience. Int J Surg 2015, 18, 136–141. [Google Scholar] [CrossRef]
- Slama, R.; Villaume, F. Penetrating Vascular Injury: Diagnosis and Management Updates. Emerg Med Clin North Am 2017, 35, 789–801. [Google Scholar] [CrossRef]
- Pinto, A.; Russo, A.; Reginelli, A.; Iacobellis, F.; Di Serafino, M.; Giovine, S.; Romano, L. Gunshot Wounds: Ballistics and Imaging Findings. Semin Ultrasound CT MR 2019, 40, 25–35. [Google Scholar] [CrossRef]
- Kumar, M.K.; Badole, C.; Patond, K. Salvage versus amputation: Utility of mangled extremity severity score in severely injured lower limbs. Indian J Orthop 2007, 41, 183–187. [Google Scholar] [PubMed]
- Meyer, J.P.; Lim, L.T.; Schuler, J.J.; Castronuovo, J.J.; Buchbinder, D.; Woelfel, G.F.; Flanigan, P. Peripheral vascular trauma from close-range shotgun injuries. Arch Surg 1985, 120, 1126–1131. [Google Scholar] [CrossRef]
- Szaniewski, K.B.T.; Sikora, T. Vascular Trauma. In: Emergency Medicine and Trauma. edn. Edited by IntechOpen: 1-18.
- Usman, R.; Jamil, M.; Anwer, M.F. Evaluation, Surgical Management and Outcome of Traumatic Extremity Vascular Injuries: A 5-year Level-1 Trauma Centres Experience. Ann Vasc Dis 2018, 11, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Rich, N.M.; Hobson, R.W., 2nd; Fedde, C.W. Vascular trauma secondary to diagnostic and therapeutic procedures. Am J Surg 1974, 128, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Giswold, M.E.; Landry, G.J.; Taylor, L.M.; Moneta, G.L. Iatrogenic arterial injury is an increasingly important cause of arterial trauma. Am J Surg 2004, 187, 590–592, discussion 592-593. [Google Scholar] [CrossRef] [PubMed]
- Eleshra, A.; Kim, D.; Park, H.S.; Lee, T. Access site pseudoaneurysms after endovascular intervention for peripheral arterial diseases. Ann Surg Treat Res 2019, 96, 305–312. [Google Scholar] [CrossRef]
- Lopera, J.E.; Restrepo, C.S.; Gonzales, A.; Trimmer, C.K.; Arko, F. Aortoiliac vascular injuries after misplacement of fixation screws. J Trauma 2010, 69, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Pulido, L.; Slenker, N.; Macgibeny, M.; Purtill, J.J.; Rothman, R.H. Vascular injuries after total joint arthroplasty. J Arthroplasty 2008, 23, 1115–1121. [Google Scholar] [CrossRef]
- Scalea, J.R.; Crawford, R.; Scurci, S.; Danquah, J.; Sarkar, R.; Kufera, J.; O’Connor, J.; Scalea, T.M. Below-the-knee arterial injury: the type of vessel may be more important than the number of vessels injured. J Trauma Acute Care Surg 2014, 77, 920–925. [Google Scholar] [CrossRef]
- Eccles S HB, Khan U,, McFadyen I N, J, S N: Vascular Injuries. In., edn. Edited by Fractures SftMoO: Oxford Medicine Online; 2020: 93-102.
- Ritondale, J.; Piehl, M.; Caputo, S.; Broome, J.; McLafferty, B.; Anderson, A.; Belding, C.; Tatum, D.; Taghavi, S.; McGrew, P.; et al. The Impact of a Prehospital “x-ABC” Resuscitation Sequence in Patients with Severe Hemorrhage. J Am Coll Surg 2024.
- Prichayudh, S.; Rassamee, P.; Sriussadaporn, S.; Pak-Art, R.; Sriussadaporn, S.; Kritayakirana, K.; Samorn, P.; Narueponjirakul, N.; Uthaipaisanwong, A. Abdominal vascular injuries: Blunt vs. penetrating. Injury 2019, 50, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Davidovic, L.B.; Cinara, I.S.; Ille, T.; Kostic, D.M.; Dragas, M.V.; Markovic, D.M. Civil and war peripheral arterial trauma: review of risk factors associated with limb loss. Vascular 2005, 13, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Gustilo, R.B.; Mendoza, R.M.; Williams, D.N. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma 1984, 24, 742–746. [Google Scholar] [CrossRef]
- Durham, R.M.; Mistry, B.M.; Mazuski, J.E.; Shapiro, M.; Jacobs, D. Outcome and utility of scoring systems in the management of the mangled extremity. Am J Surg 1996, 172, 569–573, discussion 573-564. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.S.; Goldner, R.D.; Urbaniak, J.R.; Nunley, J.A.; Hardaker, W.T., Jr. Management of severe musculoskeletal injuries of the upper extremity. J Orthop Trauma 1990, 4, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Gustilo, R.B.; Anderson, J.T. JSBS classics. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones. Retrospective and prospective analyses. J Bone Joint Surg Am 2002, 84, 682. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Fractures (complex): assessment and management. London: National Institute for Health and Care Excellence (UK). 2016.
- Ewing, T.E.H.G.; Perron, A.D.; Strout, T.D. Inter-rater reliability and false positive result rates of ankle brachial index measurements performed by emergency providers. Ann Emerg Med 2010, 56, S132–133. [Google Scholar] [CrossRef]
- Nguyen, T.; Kalish, J.; Woodson, J. Management of civilian and military vascular trauma: lessons learned. Semin Vasc Surg 2010, 23, 235–242. [Google Scholar] [CrossRef]
- Dennis, J.W.; Frykberg, E.R.; Veldenz, H.C.; Huffman, S.; Menawat, S.S. Validation of nonoperative management of occult vascular injuries and accuracy of physical examination alone in penetrating extremity trauma: 5- to 10-year follow-up. J Trauma 1998, 44, 243–252, discussion 242-243. [Google Scholar] [CrossRef]
- Adragao, T.; Pires, A.; Branco, P.; Castro, R.; Oliveira, A.; Nogueira, C.; Bordalo, J.; Curto, J.D.; Prata, M.M. Ankle--brachial index, vascular calcifications and mortality in dialysis patients. Nephrol Dial Transplant 2012, 27, 318–325, discussion 572-563. [Google Scholar] [CrossRef]
- Johansen, K.; Daines, M.; Howey, T.; Helfet, D.; Hansen, S.T., Jr. Objective criteria accurately predict amputation following lower extremity trauma. J Trauma 1990, 30, 568–572, discussion 572-563. [Google Scholar] [CrossRef] [PubMed]
- Halvorson, J.J.; Anz, A.; Langfitt, M.; Deonanan, J.K.; Scott, A.; Teasdall, R.D.; Carroll, E.A. Vascular injury associated with extremity trauma: initial diagnosis and management. J Am Acad Orthop Surg 2011, 19, 495–504. [Google Scholar] [CrossRef]
- Latteri, S.; Malaguarnera, G.; Mannino, M.; Pesce, A.; Curro, G.; Tamburrini, S.; Scuderi, M. Ultrasound as point of care in management of polytrauma and its complication. J Ultrasound 2017, 20, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Tamburrini, S.; Consoli, L.; Garrone, M.; Sfuncia, G.; Lugara, M.; Coppola, M.G.; Piccirillo, M.; Toto, R.; Stella, S.M.; Sofia, S.; et al. The “Black Pattern”, a Simplified Ultrasound Approach to Non-Traumatic Abdominal Emergencies. Tomography 2022, 8, 798–814. [Google Scholar] [CrossRef] [PubMed]
- Stacy, M.R.; Dearth, C.L. Multimodality Imaging Approaches for Evaluating Traumatic Extremity Injuries: Implications for Military Medicine. Adv Wound Care (New Rochelle) 2017, 6, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Tisherman, S.A. Management of Major Vascular Injury: Open. Otolaryngol Clin North Am 2016, 49, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Montorfano, M.A.; Pla, F.; Vera, L.; Cardillo, O.; Nigra, S.G.; Montorfano, L.M. Point-of-care ultrasound and Doppler ultrasound evaluation of vascular injuries in penetrating and blunt trauma. Crit Ultrasound J 2017, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Patterson, B.O.; Holt, P.J.; Cleanthis, M.; Tai, N.; Carrell, T.; Loosemore, T.M.; London Vascular Injuries Working, G. Imaging vascular trauma. Br J Surg 2012, 99, 494–505. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, E.; Dennis, J.W.; Vu, J.H.; Frykberg, E.R. Redefining the role of arterial imaging in the management of penetrating zone 3 neck injuries. Vascular 2005, 13, 158–163. [Google Scholar] [CrossRef] [PubMed]
- deSouza, I.S.; Benabbas, R.; McKee, S.; Zangbar, B.; Jain, A.; Paladino, L.; Boudourakis, L.; Sinert, R. Accuracy of Physical Examination, Ankle-Brachial Index, and Ultrasonography in the Diagnosis of Arterial Injury in Patients With Penetrating Extremity Trauma: A Systematic Review and Meta-analysis. Acad Emerg Med 2017, 24, 994–1017. [Google Scholar] [CrossRef]
- Costantini, T.W.; Coimbra, R.; Holcomb, J.B.; Podbielski, J.M.; Catalano, R.; Blackburn, A.; Scalea, T.M.; Stein, D.M.; Williams, L.; Conflitti, J.; et al. Current management of hemorrhage from severe pelvic fractures: Results of an American Association for the Surgery of Trauma multi-institutional trial. J Trauma Acute Care Surg 2016, 80, 717–723, discussion 723-715. [Google Scholar] [CrossRef] [PubMed]
- Dreizin, D.; Munera, F. Blunt polytrauma: evaluation with 64-section whole-body CT angiography. Radiographics 2012, 32, 609–631. [Google Scholar] [CrossRef] [PubMed]
- Monazzam, S.; Goodell, P.B.; Salcedo, E.S.; Nelson, S.H.; Wolinsky, P.R. When are CT angiograms indicated for patients with lower extremity fractures? A review of 275 extremities. J Trauma Acute Care Surg 2017, 82, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.P.; Rambau, G.; Tennent, D.J.; Osborn, P.M. The Role of CT Angiography in Evaluating Lower Extremity Trauma: 157 Patient Case Series at a Military Treatment Facility. Mil Med 2019, 184, e490–e493. [Google Scholar] [CrossRef] [PubMed]
- Bozlar, U.; Ogur, T.; Norton, P.T.; Khaja, M.S.; All, J.; Hagspiel, K.D. CT angiography of the upper extremity arterial system: Part 1-Anatomy, technique, and use in trauma patients. AJR Am J Roentgenol 2013, 201, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Walkoff, L.; Nagpal, P.; Khandelwal, A. Imaging primer for CT angiography in peripheral vascular trauma. Emerg Radiol 2021, 28, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Abu-Omar, A.; Murray, N.; Ali, I.T.; Khosa, F.; Barrett, S.; Sheikh, A.; Nicolaou, S.; Tamburrini, S.; Iacobellis, F.; Sica, G.; et al. Utility of Dual-Energy Computed Tomography in Clinical Conundra. Diagnostics (Basel), 2024; 14. [Google Scholar]
- Wirth, S.; Hebebrand, J.; Basilico, R.; Berger, F.H.; Blanco, A.; Calli, C.; Dumba, M.; Linsenmaier, U.; Muck, F.; Nieboer, K.H.; et al. European Society of Emergency Radiology: guideline on radiological polytrauma imaging and service (short version). Insights Imaging 2020, 11, 135. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, F.; Ierardi, A.M.; Mazzei, M.A.; Magenta Biasina, A.; Carrafiello, G.; Nicola, R.; Scaglione, M. Dual-phase CT for the assessment of acute vascular injuries in high-energy blunt trauma: the imaging findings and management implications. Br J Radiol 2016, 89, 20150952. [Google Scholar] [CrossRef] [PubMed]
- Gakhal, M.S.; Sartip, K.A. CT angiography signs of lower extremity vascular trauma. AJR Am J Roentgenol 2009, 193, W49–W57. [Google Scholar] [CrossRef]
- Miller-Thomas, M.M.; West, O.C.; Cohen, A.M. Diagnosing traumatic arterial injury in the extremities with CT angiography: pearls and pitfalls. Radiographics 2005, 25 (Suppl. 1), S133–142. [Google Scholar] [CrossRef]
- Madhuripan, N.; Mehta, P.; Smolinski, S.E.; Njuguna, N. Computed Tomography Angiography of the Extremities in Emergencies. Semin Ultrasound CT MR 2017, 38, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.; Efron, D.T.; Fishman, E.K. Multidetector CT and three-dimensional CT angiography of upper extremity arterial injury. Emerg Radiol 2015, 22, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Jens, S.; Kerstens, M.K.; Legemate, D.A.; Reekers, J.A.; Bipat, S.; Koelemay, M.J. Diagnostic performance of computed tomography angiography in peripheral arterial injury due to trauma: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg 2013, 46, 329–337. [Google Scholar] [CrossRef]
- Nagpal, K.; Ahmed, K.; Cuschieri, R. Diagnosis and management of acute traumatic arteriovenous fistula. Int J Angiol 2008, 17, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Rieger, M.; Mallouhi, A.; Tauscher, T.; Lutz, M.; Jaschke, W.R. Traumatic arterial injuries of the extremities: initial evaluation with MDCT angiography. AJR Am J Roentgenol 2006, 186, 656–664. [Google Scholar] [CrossRef]
- Uyeda, J.W.; Anderson, S.W.; Sakai, O.; Soto, J.A. CT angiography in trauma. Radiol Clin North Am 2010, 48, 423–438. [Google Scholar] [CrossRef] [PubMed]
- Colip, C.G.; Gorantla, V.; LeBedis, C.A.; Soto, J.A.; Anderson, S.W. Extremity CTA for penetrating trauma: 10-year experience using a 64-detector row CT scanner. Emerg Radiol 2017, 24, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Yaremchuk, M.J.; Brumback, R.J.; Manson, P.N.; Burgess, A.R.; Poka, A.; Weiland, A.J. Acute and definitive management of traumatic osteocutaneous defects of the lower extremity. Plast Reconstr Surg 1987, 80, 1–14. [Google Scholar] [CrossRef]
- Pieroni, S.; Foster, B.R.; Anderson, S.W.; Kertesz, J.L.; Rhea, J.T.; Soto, J.A. Use of 64-row multidetector CT angiography in blunt and penetrating trauma of the upper and lower extremities. Radiographics 2009, 29, 863–876. [Google Scholar] [CrossRef]
- Scaglione, M.; Iaselli, F.; Sica, G.; Feragalli, B.; Nicola, R. Errors in imaging of traumatic injuries. Abdom Imaging 2015, 40, 2091–2098. [Google Scholar] [CrossRef]
- Joseph, T.I.; Ratnakanthan, P.J.; Paul, E.; Clements, W. Utility of computed tomography angiography in traumatic lower limb injury: Review of clinical impact in level 1 trauma centre. Injury 2021, 52, 3064–3067. [Google Scholar] [CrossRef] [PubMed]
- le Roux, A.; Du Plessis, A.M.; Pitcher, R. Yield of CT angiography in penetrating lower extremity trauma. Emerg Radiol 2021, 28, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Fox, N.; Rajani, R.R.; Bokhari, F.; Chiu, W.C.; Kerwin, A.; Seamon, M.J.; Skarupa, D.; Frykberg, E. Eastern Association for the Surgery of, T. Evaluation and management of penetrating lower extremity arterial trauma: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg.
- Moore, E.E.; Malangoni, M.A.; Cogbill, T.H.; Peterson, N.E.; Champion, H.R.; Jurkovich, G.J.; Shackford, S.R. Organ injury scaling VII: cervical vascular, peripheral vascular, adrenal, penis, testis, and scrotum. J Trauma 1996, 41, 523–524. [Google Scholar] [CrossRef] [PubMed]
- Velmahos, G.C.; Toutouzas, K.G.; Vassiliu, P.; Sarkisyan, G.; Chan, L.S.; Hanks, S.H.; Berne, T.V.; Demetriades, D. A prospective study on the safety and efficacy of angiographic embolization for pelvic and visceral injuries. J Trauma 2002, 53, 303–308, discussion 308. [Google Scholar] [CrossRef]
- Goes, A.M.O.; Parreira, J.G.; Kleinsorge, G.H.D.; Dalio, M.B.; Alves, P.H.F.; Gomes, F.; de Araujo, W.J.B.; Joviliano, E.E.; de Oliveira, J.C.P. Brazilian guidelines on diagnosis and management of traumatic vascular injuries. J Vasc Bras 2023, 22, e20230042. [Google Scholar] [CrossRef]
- Percival, T.J.; Rasmussen, T.E. Reperfusion strategies in the management of extremity vascular injury with ischaemia. Br J Surg 2012, 99 (Suppl. 1), 66–74. [Google Scholar] [CrossRef]
- McQueen, M.M.; Gaston, P.; Court-Brown, C.M. Acute compartment syndrome. Who is at risk? J Bone Joint Surg Br 2000, 82, 200–203. [Google Scholar] [CrossRef]
- Lu, C.H.; Tsang, Y.M.; Yu, C.W.; Wu, M.Z.; Hsu, C.Y.; Shih, T.T. Rhabdomyolysis: magnetic resonance imaging and computed tomography findings. J Comput Assist Tomogr 2007, 31, 368–374. [Google Scholar] [CrossRef]
Figure 1.
CTA, axial planes (A-B). According to Gustilo-Anderson classification, these two different patients were classified as grade IIIB (A) and IIIC (B) respectively, involving at least three of the four major systems: integument, soft tissue, bone, nerves and vessels. In both these patients the left lower limb fractures are characterized by extensive bone loss, periosteal stripping with devitalized fragments, massive contamination and poor soft-tissue coverage. In A, the left peroneal artery contusion can be noted (arrow), while in B the left arteries cannot be recognized, indicating arterial injuries that require reperfusion.
Figure 1.
CTA, axial planes (A-B). According to Gustilo-Anderson classification, these two different patients were classified as grade IIIB (A) and IIIC (B) respectively, involving at least three of the four major systems: integument, soft tissue, bone, nerves and vessels. In both these patients the left lower limb fractures are characterized by extensive bone loss, periosteal stripping with devitalized fragments, massive contamination and poor soft-tissue coverage. In A, the left peroneal artery contusion can be noted (arrow), while in B the left arteries cannot be recognized, indicating arterial injuries that require reperfusion.
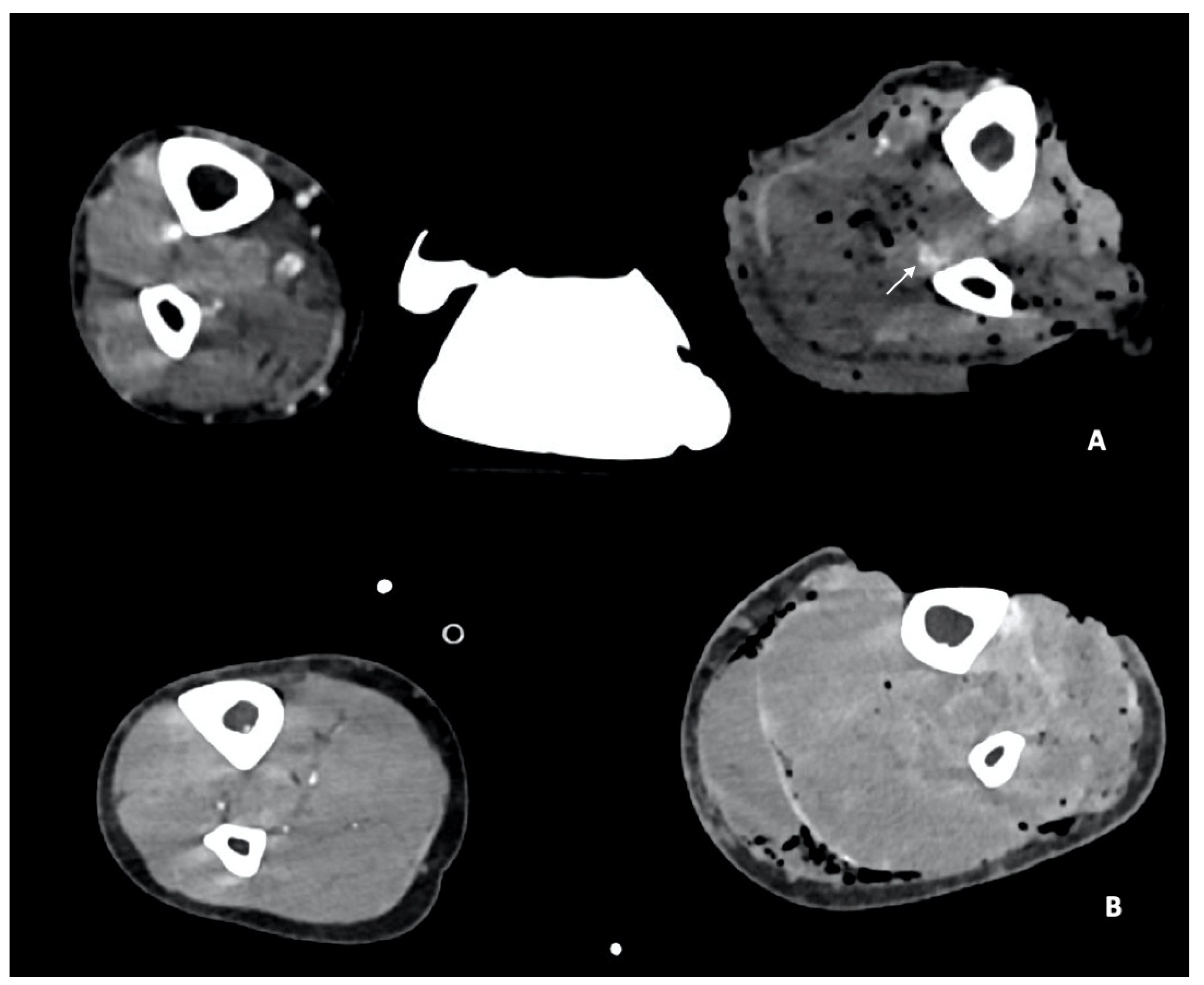
Figure 2.
The drawing shows the main findings of arterial trauma, represented by arterial transection (A), pseudoaneurysm (B), dissection (C), luminal narrowing (D) and arteriovenous fistula (E).
Figure 2.
The drawing shows the main findings of arterial trauma, represented by arterial transection (A), pseudoaneurysm (B), dissection (C), luminal narrowing (D) and arteriovenous fistula (E).
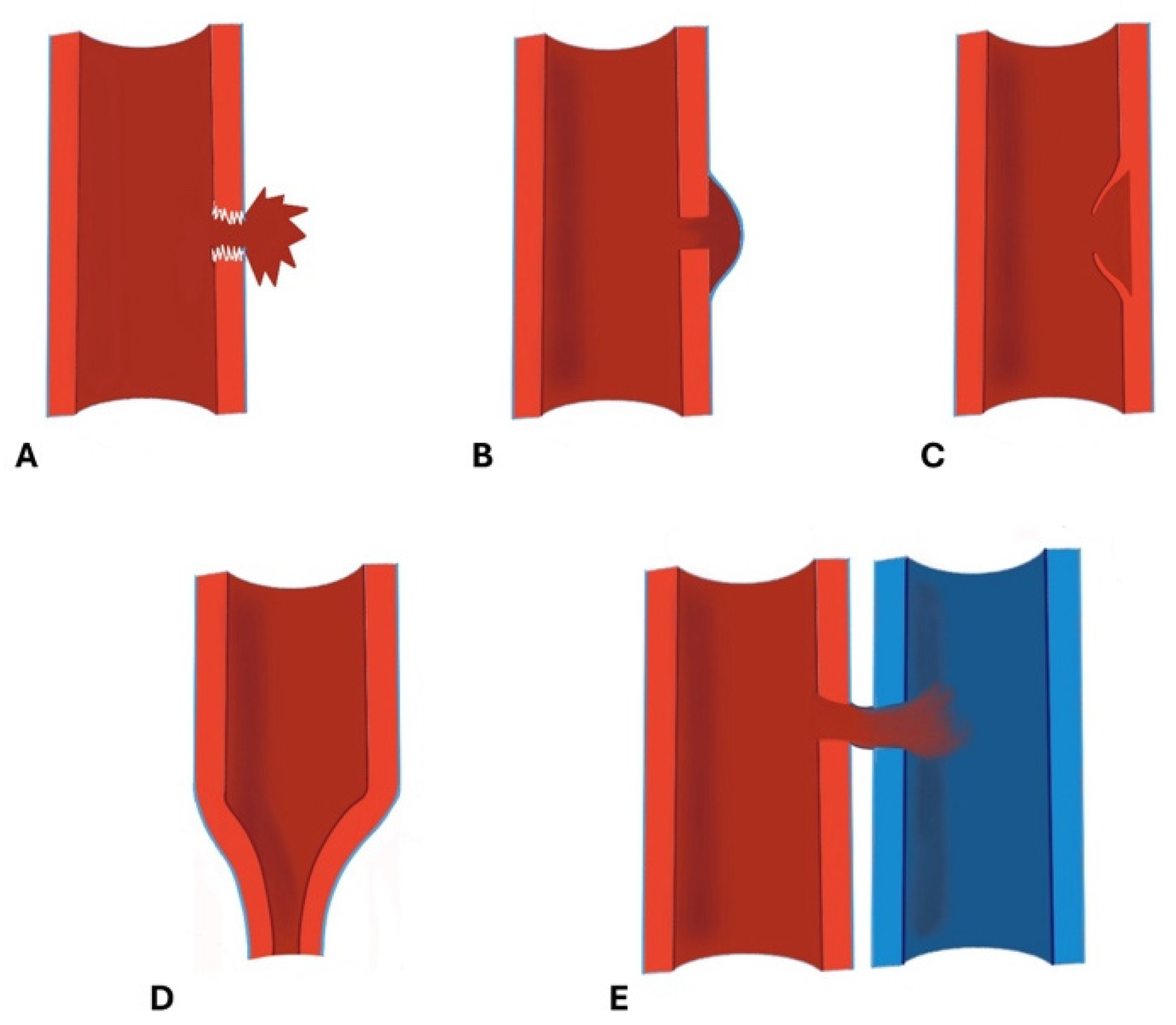
Figure 8.
CTA, arterial phase, axial planes. In this patient, artifacts from metal arthroplasty of the left lower limb made the examination nondiagnostic. An iterative filter must be applied in order to reduce these artifacts.
Figure 8.
CTA, arterial phase, axial planes. In this patient, artifacts from metal arthroplasty of the left lower limb made the examination nondiagnostic. An iterative filter must be applied in order to reduce these artifacts.
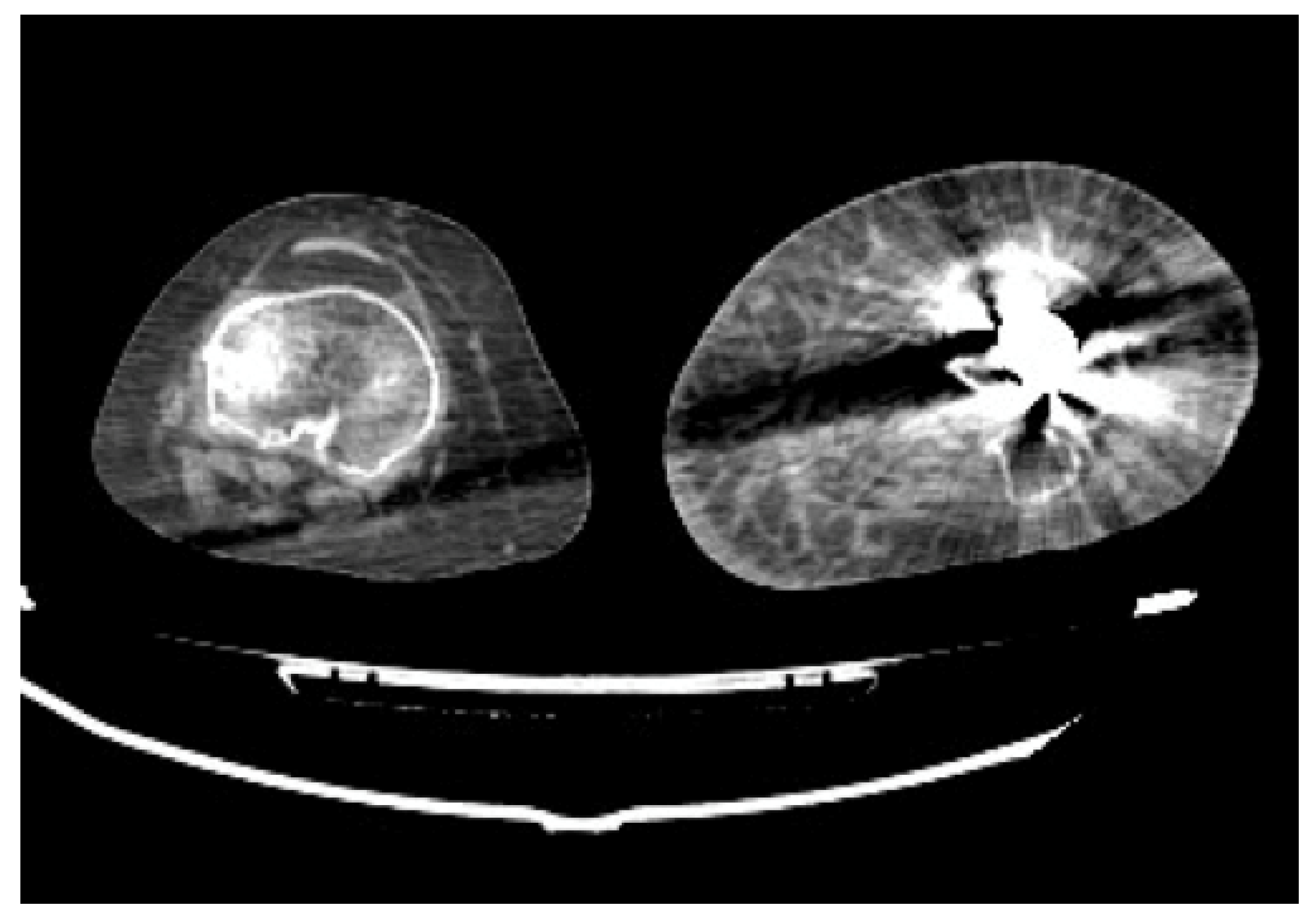

Table 1.
AAST Organ Injury Scale Grading of peripheral vascular injury [80].
Table 1.
AAST Organ Injury Scale Grading of peripheral vascular injury [80].
| Grade | Injury |
|---|---|
| I | Digital artery/vein, Palmar artery/vein, deep palmar artery/vein, dorsalis pedis artery, plantar artery/vein, non-named arterial/venous branches. |
| II | Basilic/cephalic vein, saphenous vein, radial artery, ulnar artery. |
| III | Axillary vein, superficial/deep femoral vein, popliteal vein, brachial artery, anterior tibial artery, posterior tibial artery, peroneal artery, tibioperoneal trunk. |
| IV | Superficial/deep femoral artery, popliteal artery. |
| V | Axillary artery, common femoral artery. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



