
Submitted:
10 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
Despite significant prevention efforts, the numbers of physically inactive individuals, chronic illnesses, exhaustion syndromes and sick leaves are increasing. A still unresolved problem with exercise promotion is the low participation of sedentary persons. This collective term covers heterogeneous subgroups. Their engagement with movement campaigns and resistance to change are influenced by numerous factors. Our aim was to analyse survey data on health, performance, lifestyle habits and the approachability to physical activity campaigns obtained from the Germany-wide ActIv survey. From 2,888 study participants aged 50-60 years, 668 persons were categorised into the subgroups "never-athletes", "sports-dropouts", "always-athletes" and "sports-beginners". Large and significant group differences were found for BMI, assessment of quality of life, health and fitness, risk factors and health problems. 42.5% of "never-athletes" and 32.5% of "sports-dropouts" did not state any barriers to sport. There are substantial disparities between the non-athlete groups in terms of their motivation to exercise. In contrast, there are comparatively minor differences in motivation between "sports-dropouts" and "sports-beginners", whose health and fitness are the primary motivators for sport. Our analyses suggest that (i) negative health and performance trends cannot be compensated by appeals for voluntary participation in exercise programmes and (ii) powerful incentive systems are required.
Keywords:
Lifestyle
; physical inactivity
; health risk factors
; barriers to sport
; motives for sport
; exercise promotion
; incentive systems
1. Introduction
The enormous technological progress since the 1950s has led to huge changes in the living environments of modern societies, profoundly altering the lifestyles of nearly all demographic groups [1,2,3,4,5,6]. On the one hand, increasing prosperity has resulted in the availability of cheap and abundant food [7,8,9,10]. On the other hand, advancements in technology at work, in transportation, at home, and during leisure time have led to a massive reduction in physical activity [1,3,11,12,13,14].
Using data from the "U.S. National Health and Nutrition Examination Survey", Church et al. [3] calculated the changes in energy expenditure and obesity prevalence of US employees from 1960 to 2008. In the 1960s, approximately 50% of the working population performed activities meeting the WHO recommendations for daily energy expenditure [15]. By 2008, this figure has decreased to only 20%. Over this period, the average body weight of US employees increased from 76.9 kg to 91.8 kg. The globally visible consequences of hypercaloric diets and permanent sitting are known to be responsible factors for the significant increases in overweight, obesity, fatty liver, diabetes mellitus, circulatory disorders and other diseases [8,14,16,17,18,19,20].
Since 2008 the issue has become even more pressing, marked by a notable surge in mechanisation, automation and digitalisation within the realm of work [21,22,23,24]. The spread of working from home and the future use of artificial intelligence may further increase the extent of physical inactivity among the majority of employees [5,6,25,26]. Changes in the household, in the leisure sector and in transportation are also exacerbating the problem [1,11,12,14]. Intensive and excessive consumption of digital media during leisure time is now prevalent across all generations worldwide [25,26,27,28,29]. This trend also applies to prolonged sitting in cars and on public transport [11,14]. In Germany, for example, 40 per cent of commuters also use their cars for distances of less than five kilometres [30].
The somatic consequences of a lack of exercise have been the focus of numerous studies in the past [7,17,20,31,32,33,34,35,36]. However, the significant effects on mental well-being are also becoming increasingly apparent [26,37,38,39]. The global prevalences of burnout, mental disorders and depressive symptoms are on the rise [27,28,39,40].
For decades, educational and preventive campaigns have targeted the motivation of individuals to adopt a more physically active lifestyle and enabling them to establish sufficient exercise and healthy dietary habits into their daily routines [6,8,14,15,20,41,42]. However, it is widely acknowledged that their effectiveness is insufficient and that lasting lifestyle changes are rarely achieved despite countless health campaigns. Despite better knowledge, numerous sources of information and offers (medical consultations, state health education, health insurance campaigns, etc.), the opportunities for active leisure activities are seldom utilised and unhealthy diets are usually continued [6,31,43,44].
One reason for this frequent failure may be the lack of important key data on target group-orientated and sustainable health promotion. Analysing the literature and campaigns that have been carried out provide a surprising result: although there are numerous studies, surveys and health reports, there are only a few target group-specific key data on strategic and application-oriented health and performance promotion [31,35,45,46,47] (Rütten et al 2005). The 2019 German Diabetes Surveillance Report, for example, lists detailed key figures on diabetes incidence, diabetes costs and the effectiveness of treatment programmes and differentiates these by age, gender and regional distribution using location and dispersion measures [48]. However, there is no important distinction between physically active individuals and those who do not exercise.
Regular exercise is one of the most effective and cost-effective measures for the prevention and treatment of many chronic diseases [6,23,49,50,51,52]. If physical activity is to be effectively promoted for the prevention and treatment of diseases, precise knowledge about barriers to exercise, attractors and motives for exercising, everyday habits and health attitudes etc. is essential. One way of obtaining such data that has rarely been utilised to date is to conduct targeted surveys of persons with different levels of physical activity. Few studies show that the distinction between sporty and inactive groups of individuals is not sufficient [34,45,46,47,50,53].
In this study, therefore, a further differentiation was made between two non-athlete groups ("never-athletes" and " sports-dropouts ") and two athlete groups ("sports-beginners" and "always-athletes"). Through comparing these sub-groups, our objective was to identify prevention-relevant differences and important information for health campaigns were to be determined. Key questions we sought to address included: What motivates physically inactive individuals to engage in sports? What are the most common barriers to exercise? What factors prompt newcomers to sport to initiate or resume participation? For this purpose we analysed over 10,000 data records from the Germany-wide ActIv (Activate Individuals) survey, which gathers detailed health and performance-related data from the population. However, in order to mitigate age effects, only data from individuals aged 50-60 were compared.
The two groups of never-athletes and always-athletes served as anchor values. Only individuals who stated that they had not done any sport for at least 20 years or their entire lives ("never-athletes") or, in the case of "always-athletes", that they had been active in sport for at least 20 years were included. The other two sport status groups consisted of persons who had not done sport for 5 years ("sports-dropouts") or who had been active in sport for 5 years ("sports-beginners ").
Our study focussed on sedentary adults, with comparisons made to groups engaged in sports activities. The objectives were twofold: (i) to identify group differences in the assessment of health, fitness, and lifestyle habits, as well as motives and barriers to exercise, and (ii) increase the data available for the design of target group-specific exercise and health campaigns.
2. Materials and Methods
2.1. Data Collection
In the ActIv project (www.dshs-koeln.de/forschungsgruppe-leistungsepidemiologie/forschung/activ-projekt/ ), health-maintaining and disease-causing factors are analysed in the context of life situations, everyday habits and attitudes. Database are modularised online surveys, survey links are available on portals tailored to specific educational, occupational, and interest-based categories (e.g., technicians, teachers, taxi drivers, long-distance lorry drivers, nutrition, health, exercise, and sports forums, universities). In addition, the data collections are performed in regional survey facilities (e.g. in health centres, doctors' surgeries, rehabilitation facilities, public and commercial facilities (clubs, fitness studios, medical supply stores, hairdressers). Immediately after the survey, participants receive feedback regarding their individual health resources and risk factors, aimed at enhancing awareness of the importance of personal lifestyle choices. The ActIv project has obtained ethical approval from the ethics committee of the German Sport University Cologne and has implemented a comprehensive data protection protocol.
2.2. Survey Content
The survey content encompasses socio-demographic and anthropometric data (educational status, year of birth, gender, height, weight) and inquiries of health, fitness and quality of life, health complaints, medical history and medication consumption, everyday activities and sports, sports biography, and motives and barriers to sports. Likert scales with 5-point response options were used to measure personal assessments. The body mass index (BMI) was determined from the reported data on body weight and height.
Only completed and quality-checked questionnaires were analysed. The questionnaire items encompass nominal, categorical and scaled responses. The entries were automatically plausibility-checked.
2.3. Survey Sample
From data obtained from 10,041 ActIv participants, 2,888 data sets of individuals aged 50-60 years were selected based on their sporting status and its duration. Participants were divided into the following categories: “never-athletes”, “sports-dropouts”, “sports beginners”, and “always-athletes”, based on their responses to the following two questions: (1) How do you categorise yourself in terms of sport? (Possible answers: non-athlete/recreational or healthy athlete/active competitive athlete); (2) Are you currently active in sport? (Answer options: Yes/ No, I am currently taking a break (for health, professional, or private reasons)/ No).
Non-athletes were queried about the duration they had been out of sport and had the option of indicating the number of years or selecting the response option "I have never participated in any sport". Athletes were asked the same question regarding the length of time they had been involved in sport.
As described in the introduction, the following inclusion and exclusion criteria were applied: Only data from individuals who had refrained from participating in sports for a minimum of 20 years or their entire lives ("never-athletes"), or those who had consistently engaged in sports activities ("always-athletes"), were considered. The groups of "sports-dropouts" and "sports-beginners" only included persons who had not done any sport or taken part in sport for at least one year and no more than five years. This was intended to prevent distortions resulting from information provided by individuals who had only been active in sport for a few months, for example, or who had to take a break from sport for several months due to injury or illness. The sport status groups were homogeneous in terms of gender and education.
2.4. Statistics
The data was analysed using IBM© SPSS© Statistics 24.0. The descriptive statistics included the calculation of position and dispersion measures (arithmetic mean, standard deviation). The comparison of dichotomous or ordinal-scaled parameters was carried out using cross-tabulations and chi-square tests. The comparison of variables from two independent samples was carried out using the T-test. Two-factor analysis of variance and Scheffé post-hoc test were used to compare interval-scaled characteristics. The prerequisites were checked before calculating the mean comparisons. A probability of error of p<0.05 was accepted as significant for all tests. The sport status groups were homogeneous in terms of gender and education.
3. Results
From 2,888 study participants aged 50-60 years, 668 persons (296 men, 372 women) could be assigned to the 4 sport status groups (“never-athletes”, “sports-dropouts”, “sports-beginners”, “always-athletes”). Table 1 lists the group mean values for age, height, weight, BMI and group sizes (numbers of men (above) and women (below)). The mean differences in body weight and BMI mean values are significant (p<0,05). Figure 1 shows the group differences (<0,05) in the BMI classes of the male and female study participants: Among the "never-athletes", only 12.9% of men and 10.0% of women are of normal weight, compared to 22.6% of men and 35.4% of women among the "sports dropouts".
3.1. Assessment of Own Quality of Life, Health and Fitness
There are also significant differences between the sport status groups in the assessment of quality of life, personal health and fitness. While 83.1% ("always-athletes") and 62.5% ("sports-beginners") of the active sports groups rated their quality of life as high, 55.8% of "sports-dropouts" and 40.4% of "never-athletes" did so (p<0.05).
Figure 3 shows the group differences for the statement "Overall, I feel healthy." (p<0,05). This statement is not true for 46.9% of "never-athletes" and 33.4% of “sports-dropouts”. Among the "sports-beginners" and "always-athletes", 14.0% and 7.3% respectively disagree with this statement.
The group differences (p<0.05) are even clearer in the assessment of performance ("Overall, I feel able to perform."), which can be seen in Figure 4. 54.3% of the "never-athletes" and 41.8% of the "sports-dropouts" disagree with this statement. In the active sports groups, the figures are 18.6% ("sport-beginners") and 7.9% ("always-athletes").
3.2. Unfavourable Lifestyle Habits and Health Problems
Participants were asked about unfavourable lifestyle habits using a selection list ("Which lifestyle habits are so unfavourable to you that they could affect your health?"). Multiple answers were permitted for the 10 options listed. Table 2 shows the frequencies of the individual unfavourable lifestyle habits. It is easy to see that the two inactive groups cite unfavourable lifestyle habits more frequently (p<0.05). Lack of exercise is most frequently seen as a potential cause of health impairments among the "never athletes" (69.3%) and the "sports dropouts" (53.3%).
Three or more negative lifestyle habits are reported by 40% of "never-athletes", 31.1% of “sports-dropouts”, 18.6% of "sport-beginners” and 10.4% of "always-athletes". No unfavourable lifestyle habits were reported by 13.1% of "never-athletes", 16.2% of "sports-dropouts", 30.2% of "sports-beginners" and 37,3% of "always-athletes".
Health problems are reported significantly more frequently in the two non-athlete groups. 56.1% of "never-athletes", 55.1% of "sport-dropouts", 39.6% of "sports-beginners" and 29.6% of "always-athletes" report that they have had health problems in the last 12 months. Table 3 shows the frequency of health complaints in the last 12 months. Back pain, muscle pain and joint pain occur most frequently in all sports status groups. 37.5% of "never-athletes", 38.3% of "sport-dropouts", 19.5% of "sports-beginners" and 12.1% of "always-athletes" had at least three health problems in the last 12 months.
3.3. Motivation to Do Sport
As expected, there are clear differences between the four sport status groups in terms of both motivation and barriers to do sport.
Figure 5 shows the study participants' assessment of the statement "I am motivated to do sport". 87.9% of "always-athletes", 66.7% of "sports-beginners", 49.2% of "sports-dropouts" and 16.5% of "never-athletes" stated that they are motivated to do sport (p<0.05). In the non-athlete groups, it is striking that over 50% of "never-athletes" disagree with the statement, while only around 15% of "sports-dropouts" do (p<0.05).
The individual motives for doing sport are listed in Table 4. In response to the question "What motivates you or would motivate you to do sport?", the two sports groups stated sports motivators significantly more often than the non-athletes (p<0.05). With regard to physical activity promotion campaigns, the strongest motivators are particularly important for "never-athletes", "sports-dropouts" and "sports-beginners": in addition to health, body weight and stress reduction, physical performance is also a relevant attractor. It is interesting to note that only 30.1% of "never-athletes", but 66.0% of "sports-dropouts" cite "enjoyment of sport" as a motive.
The group of "sport-beginners" was asked the additional question "Why did you start doing sport?". The five most common reasons for taking up sport are physical reasons (70.3%), physical fitness (60.2%), weight reduction/weight control (55.5%), stress reduction/balancing (53.9%) and enjoyment of sport (32.8%).
3.4. Barriers to sport
Participants were also asked about barriers to sport using a 5-point Likert scale ("What prevents you from doing (more) sport?"). As depicted in Table 5, individuals who are inactive in sport cite more frequent and more numerous obstacles (p<0.05). Health reasons, lack of motivation and lack of time were the three most frequently cited obstacles for "never-athletes" and "sports dropouts". However, an important result regarding the barriers is not shown in Table 5: 42.5% of the "never-athletes" and 32.5% of the "sports dropouts" did not specify any sports barrier.
In the case of "sports-beginners" and "always-athletes", lack of time is the most frequently cited barrier to sport at over 60%.
4. Discussion
Negative everyday habits such as lack of exercise and a hypercaloric diet not only lead to widespread chronic diseases and escalating medical expenses but also inflict considerable financial damage in the workplace [54,55,56,57,58,59]. Well before the onset of obesity and chronic illnesses (e.g. diabetes, fatty liver, circulatory diseases), employees often experience reduced resilience, declining productivity and a significant drop in performance [33,44,57,60,61,62].
Despite countless prevention campaigns, the number of days of incapacity for work, fatigue syndromes and chronic illnesses is increasing [52,63,64,65,66]. It is obvious that their effectiveness is not sufficient and that they need to be better targeted at "sedentary persons". The fact that in Germany, for example, the majority of the population is chronically ill and ¾ of adults do not achieve the recommended amount of health-effective exercise [67,68,69], leads to the conclusion that there are numerous and heterogeneous prevention target groups in the population. Attractors and motives for exercise, barriers, responsiveness/accessibility to exercise campaigns and willingness to change can differ significantly among individuals of the same age, gender, education, occupation and place of residence and are also influenced by other factors (e.g. personal environment, life situation, sports biography, health, well-being and attitudes) [45,53,64,70]. More detailed knowledge about sedentary individuals is necessary in order to understand why they do not take part in exercise programmes, for example, and how they can be encouraged to incorporate physical and sporting activities into their everyday lives in the long term [46,70,71,72,73,74].
Surveys have been repeatedly used to obtain starting points and key data for effective physical activity promotion. The prerequisites and limitations of surveys should of course be known: our ActIv online surveys also have methodological pitfalls that should not be underestimated. In addition to incorrect entries, there are fundamental questions regarding distortions due to subjective assessments, missing objective measurement results (such as for body weight, height and BMI) and the extent to which the results of our cross-sectional surveys are representative. A further methodological limitation is that cross-sectional studies cannot necessarily prove causal relationships. Despite these limitations, focussing on the primary criterion "sports status" with the formation of the 4 main groups (never-athletes, sports-dropouts, sports-beginners and always-athletes) provides important key data: The data from the "sport dropouts" and "sport beginners" are particularly interesting, as it is possible to find out, for example, why "sport-beginners" have (re)started doing sport or what the most common barriers are for "sport-dropouts".
As can be deduced from the list of the numerous factors influencing physical activity behaviour (see above), it is likely that differentiation into sport status groups is not sufficient either. It is obvious that non-athletes have individual inclinations, motives and limitations: Consider, for example, a permanently sedentary 35-year-old IT programmer (with a preference for soft drinks and fast food), a smoking single parent 43-year-old office administrator, a 54-year-old taxi driver with type II diabetes or a 62-year-old obese pensioner with gonarthrosis. In order to reduce the influence of the age factor and the age-associated bias, only individuals aged 50-60 were included in our analyses.
As expected, there were statistically significant differences between the sport status groups in body weight, BMI (Tab. 1) and in the proportion of overweight and obese individuals (Fig. 1). However, the group differences (p<0.05) in the assessment of their own quality of life, health and fitness were unexpectedly clear (Fig. 2-4). It is worrying for the healthcare system and the economy that only 1/5 of "never-athletes" and ¼ of "sports dropouts" feel healthy. Almost 40% of non-athletes had at least three health problems in the last 12 months. The self-assessments of fitness are just as worrying: only one in six "never-athletes" and one in four "non-athletes" believe they are fit. In view of ageing workforces and the lack of healthy and high-performing employees, these figures emphasise the need for effective health and exercise campaigns [6,14,31,44,51,58,59,62,72,75,76].
In this context, our analyses point to three findings relevant to prevention. Firstly, it should be noted that both non-athlete groups are obviously aware of unfavourable lifestyle habits (Table 2): Exercise behaviour was cited as the most common negative everyday habit that can affect health. Conversely, this means that many physically inactive individuals are not lacking in knowledge. Rather, the central problem for sendentary persons appears to be insufficient motivation [5,21,25,34,44,45,47,55,73,74,77,78,79,80].
This leads to the second prevention-relevant finding of our study, the large differences in motivation among the non-athlete groups (Fig 5). The "sports-dropouts" are much more motivated to exercise than the "never-athletes" (49.20% vs. 16.50%). In contrast, only 15.2% of "sports-dropouts" disagree with the statement "I am motivated to do sports". The negative attitude of this group is therefore close to that of the "sport-beginners" (11.6%), while the majority of "never-athletes" (52.5%) state that they are not motivated to exercise.
In their cluster analyses, Vanden Auweele et al. [47] already showed large differences in the approachability of non-athletes and the mostly lacking accessibility for exercise campaigns. The authors believe that only a small proportion of the 35-65 year old physically inactive study participants will voluntarily establish an active lifestyle. Leyk et al [46] also found varying degrees of motivation among non-athletic groups of 20-29 year old men. The survey results of Smeets et al. [74] speak in favour of the great importance of motivation. The study shows that primarily motivated - but not unmotivated - individuals were willing to read information and feedback on their physical activities.
It is likely that the motivation to exercise decreases with increasing duration of physical inactivity. The comparison of "never-athletes", "sports-dropouts" and "sports-beginners" (Table 5) suggests that the differences in motivation between the two non-athlete groups are greater than between "sports-dropouts" and "sports-beginners". The simple question "Since when have you not done any sport?" could therefore be a predictor for the accessibility of non-athletes to exercise programmes and relevant in counselling sessions. Incidentally, the biggest differences between "never-athletes" and " sports-dropouts" are in the motive "physical fitness" (delta 35.9%) and the motive "enjoyment of sport" (delta 26.2%). The question "What motivates you or would motivate you to do sport?" could also be a predictor for the accessibility of sedentary persons.
The third prevention-relevant finding of our study results from the information on the existing barriers. Approximately one third of the "sports dropouts" and over 40% of the "never-athletes" do not state any barriers. Lack of time is one of the three most common barriers (Table 5). These findings match the results of a 1-year model study [44]: The aim here was to estimate how many employees in a department could be motivated to participate in a broad-based health and fitness campaign under nearly ideal conditions. A total of 1,010 employees were provided access to numerous sports programmes, monthly expert lectures and individual health consultations during working hours. However, fewer than 50% of the workforce took part in the kick-off events. By the end of the study, the number of participants had dwindled to less than 20%. The study shows that non-athletes are hardly motivated to do sport despite the excellent framework conditions. A notable 37.3% of non-athletes stated no obstacles or only one obstacle (over 50%). Lack of time was the most frequently cited barrier to sports participation, exceeding over 50%
As to be expected among 50-60 year old "sports-beginners", health is the most common reason for (re)starting sport at 70.3%. It is worth noting that physical fitness is the second most common attractor at 60%. The newcomers to sport exercise almost three times a week and, at 187 minutes per week, were above the recommended WHO minimum duration of 150 minutes [6,14,15]. Older non-athletes can therefore definitely establish an active lifestyle. Finally, in this context, attention is drawn to another encouraging study for ageing and inactive societies [19]: Nationwide surveys of long-distance runners and analyses of over 900,000 half/marathon participants aged 20-80 reveal that over 25% of persons aged 50-69 years had only initiated sports participation within the last five years. This high proportion of "newcomers to sport" shows that older former "non-athletes" can even successfully complete a marathon within a few years through regular training. Similar to health, weight reduction/control, and stress reduction/balancing, physical performance evidently emerges as one of the most prevalent motives for engaging in sports.
5. Conclusions
There are major differences in the population in terms of motivation and willingness to participate in fitness and health promotion measures. A small proportion of individuals who are inactive in sports succeed in doing so, either independently motivated or with the help of good prevention campaigns.
Our genome is geared towards exercise. The drastic reduction in physical activity at work, in transport, at home and in our leisure time has led to the emergence of lifestyle environments that cause illness - despite the prosperity of modern societies. The bottom line is that digital media and artificial intelligence will further increase sedentary behaviour. Low-movement embossing in childhood and adolescence could turn even more persons into non-athletes and never-exercisers in the future.
It is obvious that the negative health and performance trends cannot be compensated for by appeals for voluntary participation in exercise programmes alone. In addition to structural measures to promote physical activity in all areas of society, education and prevention programmes, powerful incentive systems are required to motivate sedentary persons at an individual level to "rethink" and to teach the necessary personal skills to establish a healthy and performance-enhancing active lifestyle.
Author Contributions
Conceptualization, D.L. and T.R.; methodology, D.L., N.H., T.R. and H.L.; formal analysis, N.H. , R.L.; and H.L.; investigation, R.L. and H.L.; resources, D.L., S.K., and R.L.; data curation, N.H. and R.L.; writing—original draft preparation, D.L. and H.L.; writing—review and editing, D.L., N.H., E.V., S.K. , R.L. and H.L.; visualization, N.H. and E.V.; supervision, D.L. and S.K.; project administration, D.L., T.R., S.K., R.L. and E.V..
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the German Sport University Cologne (Nr. 079/ 2020, 20.08.2020)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The ActIv surveys are conducted using the Unipark programme developed by Tivian (https://www.unipark.com/ ). The data is stored on Tivian's protected data servers and is not publicly accessible. Nevertheless, we are happy to answer questions about our data and analyses from colleagues, which can be sent to our email address Leistungsepidemiologie@dshs-koeln.de.
Acknowledgments
We are very grateful to Mr. Michael Trunzler (Research Group Epidemiology of Performance, German Sport University Cologne) and Mr. Fabian Brunet (Faculty of Computer Science, University Koblenz, Germany) for their excellent IT support in the large-scale project ActIv and their valuable technical-scientific contributions to this study.
Conflicts of Interest
Herbert Löllgen serves as a consultant in the field of cardiology for ESA. The other authors have no conflicts of interest to declare.
References
- Akindutire, I.O.; Olanipekun, J.A. Sedentary Life-Style as Inhibition to Good Quality of Life and Longevity. Journal of Education and Practice 2017, 8, 39–43. [Google Scholar]
- Brownson, R.C.; Boehmer, T.K.; Luke, D.A. Declining rates of physical activity in the United States: what are the contributors? Annu. Rev. Public Health 2005, 26, 421–443. [Google Scholar] [CrossRef]
- Church, T.S.; Thomas, D.M.; Tudor-Locke, C.; Katzmarzyk, P.T.; Earnest, C.P.; Rodarte, R.Q.; Martin, C.K.; Blair, S.N.; Bouchard, C. Trends over 5 decades in U.S. occupation-related physical activity and their associations with obesity. PLoS One 2011, 6, e19657. [Google Scholar] [CrossRef] [PubMed]
- Cordain, L.; Gotshall, R.W.; Eaton, S.B. Physical activity, energy expenditure and fitness: an evolutionary perspective. Int. J. Sports Med. 1998, 19, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Pawlik, L. Todesursache: Bewegungsmangel: Die ignorierte Pandemie des digitalen Lebens, der Arbeit und der Bildung. Padiatr. Padol. 2021, 56, 8–14. [Google Scholar] [CrossRef]
- 6. World Health Organization. Global status report on physical activity 2022; 9789.
- Leyk, D.; Rüther, T.; Wunderlich, M.; Heiß, A.; Küchmeister, G.; Piekarski, C.; Löllgen, H. Sporting activity, prevalence of overweight, and risk factors: cross-sectional study of more than 12 500 participants aged 16 to 25 years. Dtsch. Arztebl. Int. 2008, 105, 793–800. [Google Scholar] [CrossRef]
- World Health Organization. Global strategy on diet, physical activity, and health; World Health Organization: Geneva, Switzerland, 2004; ISBN 9241592222. [Google Scholar]
- Headey, D.D.; Alderman, H.H. The Relative Caloric Prices of Healthy and Unhealthy Foods Differ Systematically across Income Levels and Continents. J. Nutr. 2019, 149, 2020–2033. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Moubarac, J.-C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-processed products are becoming dominant in the global food system. Obes. Rev. 2013, 14 Suppl 2, 21–28. [Google Scholar] [CrossRef]
- Mackay, A.; Mackay, D.F.; Celis-Morales, C.A.; Lyall, D.M.; Gray, S.R.; Sattar, N.; Gill, J.M.R.; Pell, J.P.; Anderson, J.J. The association between driving time and unhealthy lifestyles: a cross-sectional, general population study of 386 493 UK Biobank participants. J. Public Health (Oxf) 2019, 41, 527–534. [Google Scholar] [CrossRef]
- Park, J.H.; Moon, J.H.; Kim, H.J.; Kong, M.H.; Oh, Y.H. Sedentary Lifestyle: Overview of Updated Evidence of Potential Health Risks. Korean J Fam Med 2020, 41, 365–373. [Google Scholar] [CrossRef]
- Statista Research Department. Gesundheit - Gehstrecke an einem typischen Wochentag 1910-2010 | Statista. Available online: https://de.statista.com/statistik/daten/studie/441323/umfrage/durchschnittliche-taegliche-gehstrecke-an-einem-typischen-wochentag/ (accessed on 25 April 2024).
- World Health Organization. WHO guidelines on physical activity and sedentary behaviour; World Health Organization: Geneva, 2020; ISBN 978-92-4-001512-8. [Google Scholar]
- World Health Organization. Global recommendations on physical activity for health; World Health Organization: Geneva, Switzerland, 2010; ISBN 978. [Google Scholar]
- Brittain, E.L.; Han, L.; Annis, J.; Master, H.; Hughes, A.; Roden, D.M.; Harris, P.A.; Ruderfer, D.M. Physical Activity and Incident Obesity Across the Spectrum of Genetic Risk for Obesity. JAMA Netw Open 2024, 7, e243821. [Google Scholar] [CrossRef] [PubMed]
- Church, T.; Martin, C.K. The Obesity Epidemic: A Consequence of Reduced Energy Expenditure and the Uncoupling of Energy Intake? Obesity (Silver Spring) 2018, 26, 14–16. [Google Scholar] [CrossRef]
- Dwyer, M.J.; Pasini, M.; Dominicis, S. de; Righi, E. Physical activity: Benefits and challenges during the COVID-19 pandemic. Scand. J. Med. Sci. Sports 2020, 30, 1291–1294. [Google Scholar] [CrossRef] [PubMed]
- Leyk, D.; Rüther, T.; Wunderlich, M.; Sievert, A.; Essfeld, D.; Witzki, A.; Erley, O.; Küchmeister, G.; Piekarski, C.; Löllgen, H. Physical performance in middle age and old age: good news for our sedentary and aging society. Dtsch. Arztebl. Int. 2010, 107, 809–816. [Google Scholar] [CrossRef]
- World Health Organization. European Charter on counteracting obesity. Diet and physical activity for health Istanbul 2006.
- Dempsey, P.C.; Biddle, S.J.H.; Buman, M.P.; Chastin, S.; Ekelund, U.; Friedenreich, C.M.; Katzmarzyk, P.T.; Leitzmann, M.F.; Stamatakis, E.; van der Ploeg, H.P.; et al. New global guidelines on sedentary behaviour and health for adults: broadening the behavioural targets. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 151. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, A.N.; Lachman, M.E. Behavior Change with Fitness Technology in Sedentary Adults: A Review of the Evidence for Increasing Physical Activity. Front. Public Health 2016, 4, 289. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Healy, G.N.; Winkler, E.; Clark, B.K.; Gardiner, P.A.; Owen, N.; Dunstan, D.W. Prolonged sedentary time and physical activity in workplace and non-work contexts: a cross-sectional study of office, customer service and call centre employees. Int J Behav Nutr Phys Act 2012, 9, 128. [Google Scholar] [CrossRef]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- Precht, L.-M.; Mertens, F.; Brickau, D.S.; Kramm, R.J.; Margraf, J.; Stirnberg, J.; Brailovskaia, J. Engaging in physical activity instead of (over)using the smartphone: An experimental investigation of lifestyle interventions to prevent problematic smartphone use and to promote mental health. Z. Gesundh. Wiss. 2023, 1–19. [Google Scholar] [CrossRef]
- Derks, D.; Bakker, A.B. Smartphone Use, Work-Home Interference, and Burnout: A Diary Study on the Role of Recovery. Applied Psychology 2014, 63, 411–440. [Google Scholar] [CrossRef]
- Duncan, M.J.; Kuzik, N.; Silva, D.A.S.; Bélanger, R.E.; Carson, V.; Chaput, J.-P.; Faulkner, G.; Ferro, M.A.; Turcotte-Tremblay, A.-M.; Leatherdale, S.T.; et al. “Goldilocks days” for adolescent mental health: Movement behaviour combinations for well-being, anxiety and depression by gender. Mental Health and Physical Activity 2024, 26, 100572. [Google Scholar] [CrossRef]
- Watts, E.L.; Matthews, C.E.; Freeman, J.R.; Gorzelitz, J.S.; Hong, H.G.; Liao, L.M.; McClain, K.M.; Saint-Maurice, P.F.; Shiroma, E.J.; Moore, S.C. Association of Leisure Time Physical Activity Types and Risks of All-Cause, Cardiovascular, and Cancer Mortality Among Older Adults. JAMA Netw. Open 2022, 5, e2228510. [Google Scholar] [CrossRef] [PubMed]
- Datenreport 2021: Ein Sozialbericht für die Bundesrepublik Deutschland; Bundeszentrale für Politische Bildung; Deutschland; Wissenschaftszentrum Berlin für Sozialforschung; Deutsches Institut für Wirtschaftsforschung; Bundeszentrale für politische Bildung: Bonn, 2021; ISBN 9783838972091.
- Huffman, M.K.; Reed, J.B.; Carpenter, T.; Amireault, S. Maintenance motives for physical activity among older adults: a protocol for a systematic review and meta-analysis. BMJ Open 2020, 10, e032605. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; Hill, O.T.; Bulathsinhala, L.; McKinnon, C.J.; Montain, S.J.; Young, A.J.; Smith, T.J. Trends in overweight and obesity in soldiers entering the US Army, 1989-2012. Obesity 2015, 23, 662–670. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Stamatakis, E.; Kelly, P.; Strain, T.; Murtagh, E.M.; Ding, D.; Murphy, M.H. Self-rated walking pace and all-cause, cardiovascular disease and cancer mortality: individual participant pooled analysis of 50 225 walkers from 11 population British cohorts. Br J Sports Med 2018, 52, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.C.E.; Tittlbach, S.; Bös, K.; Woll, A. Different Types of Physical Activity and Fitness and Health in Adults: An 18-Year Longitudinal Study. Biomed Res. Int. 2017, 2017, 1785217. [Google Scholar] [CrossRef]
- Vaara, J.P.; Santtila, M.; Vasankari, T.; Fogelholm, M.; Mäntysaari, M.; Pihlainen, K.; Vaara, E.; Kyröläinen, H. Cardiorespiratory and muscular fitness in young adult Finnish men between 2003 and 2015. Scand. J. Med. Sci. Sports 2020, 30, 716–724. [Google Scholar] [CrossRef]
- Junghanns, G.; Kersten, N. Informationsüberflutung am Arbeitsplatz. Zbl Arbeitsmed 2019, 69, 119–132. [Google Scholar] [CrossRef]
- Stothart, C.; Mitchum, A.; Yehnert, C. The attentional cost of receiving a cell phone notification. J. Exp. Psychol. Hum. Percept. Perform. 2015, 41, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Vahedi, Z.; Saiphoo, A. The association between smartphone use, stress, and anxiety: A meta-analytic review. Stress Health 2018, 34, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Friedl, K.E.; Breivik, T.J.; Carter, R.; Leyk, D.; Opstad, P.K.; Taverniers, J.; Trousselard, M. Soldier Health Habits and the Metabolically Optimized Brain. Mil. Med. 2016, 181, e1499–e1507. [Google Scholar] [CrossRef] [PubMed]
- 41. 23. International Society for Physical Activity and Health, Global Advocacy for Physical Activity. The Toronto Charter for Physical Activity: A Global Call for Action. J. Phys. Act. Health, 3. [CrossRef]
- Oja, P.; Kelly, P.; Pedisic, Z.; Titze, S.; Bauman, A.; Foster, C.; Hamer, M.; Hillsdon, M.; Stamatakis, E. Associations of specific types of sports and exercise with all-cause and cardiovascular-disease mortality: a cohort study of 80 306 British adults. Br. J. Sports Med. 2017, 51, 812–817. [Google Scholar] [CrossRef]
- Leyk, D.; Rüther, T.; Witzki, A.; Sievert, A.; Moedl, A.; Blettner, M.; Hackfort, D.; Löllgen, H. Physical fitness, weight, smoking, and exercise patterns in young adults. Dtsch. Arztebl. Int. 2012, 109, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Leyk, D.; Rohde, U.; Hartmann, N.D.; Preuß, P.A.; Sievert, A.; Witzki, A. Results of a workplace health campaign: what can be achieved? Dtsch. Arztebl. Int. 2014, 111, 320–327. [Google Scholar] [CrossRef]
- Rütten, A.; Abu-Omar, K.; Meierjürgen, R.; Lutz, A.; Adlwarth, W. Was bewegt die Nicht-Beweger? Praev Gesundheitsf 2009, 4, 245–250. [Google Scholar] [CrossRef]
- Leyk, D.; Witzki, A.; Sievert, A.; Rohde, U.; Moedl, A.; Rüther, T.; Löllgen, H.; Hackfort, D. Importance of sports during youth and exercise barriers in 20- to 29-year-old male nonathletes differently motivated for regular physical activities. J. Strength Cond. Res. 2012, 26 Suppl 2, S15–22. [Google Scholar] [CrossRef]
- Vanden Auweele, Y.; Rzewnicki, R.; van Mele, V. Reasons for not exercising and exercise intentions: a study of middle-aged sedentary adults. J. Sports Sci. 1997, 15, 151–165. [Google Scholar] [CrossRef]
- Diabetes in Deutschland: Bericht der Nationalen Diabetes-Surveillance 2019; Scheidt-Nave, C. , Ed.; Robert Koch-Institut: Berlin, 2019; ISBN 978-3-89606-302-1. [Google Scholar]
- Leyk, D. The preventive and therapeutic roles of regular physical activity. Dtsch. Arztebl. Int. 2009, 106, 713–714. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Rezende, L.F.M.; Joh, H.-K.; Keum, N.; Ferrari, G.; Rey-Lopez, J.P.; Rimm, E.B.; Tabung, F.K.; Giovannucci, E.L. Long-Term Leisure-Time Physical Activity Intensity and All-Cause and Cause-Specific Mortality: A Prospective Cohort of US Adults. Circulation 2022, 146, 523–534. [Google Scholar] [CrossRef]
- Vina, J.; Sanchis-Gomar, F.; Martinez-Bello, V.; Gomez-Cabrera, M.C. Exercise acts as a drug; the pharmacological benefits of exercise. Br. J. Pharmacol. 2012, 167, 1–12. [Google Scholar] [CrossRef]
- Löllgen, H.; Zupet, P.; Bachl, N.; Debruyne, A. Physical Activity, Exercise Prescription for Health and Home-Based Rehabilitation. Sustainability 2020, 12, 10230. [Google Scholar] [CrossRef]
- Rütten, A.; Abu-Omar, K.; Adlwarth, W.; Meierjürgen, R. Bewegungsarme Lebensstile. Zur Klassifizierung unterschiedlicher Zielgruppen für eine gesundheitsförderliche körperliche Aktivierung. Gesundheitswesen (Bundesverband der Arzte des Offentlichen Gesundheitsdienstes (Germany)) 2007, 69, 393–400. [Google Scholar] [CrossRef]
- Kanerva, N.; Pietiläinen, O.; Lallukka, T.; Rahkonen, O.; Lahti, J. Unhealthy lifestyle and sleep problems as risk factors for increased direct employers' cost of short-term sickness absence. Scand. J. Work Environ. Health 2018, 44, 192–201. [Google Scholar] [CrossRef]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M. The economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Heath, G.; Schmidt, M.; Lee, I.-M. Physical activity epidemiology, Third edition; Human Kinetics: Champaign, IL USA, 2022; ISBN 9781492593010. [Google Scholar]
- Pescatello, L.S.; Hennessy, E.A.; Katzmarzyk, P.T.; Kraus, W.E.; Fish, A.F.; Craft, L.L.; Johnson, B.T. Best Practices for Meta-Reviews in Physical Activity and Health Research: Insights From the Physical Activity Guidelines for Americans Advisory Committee Scientific Report. J. Phys. Act. Health 2021, 18, 1437–1445. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Leyk, D.; Helmhout, P. Impact of Lifestyle and Health Status on Military Fitness. Final Report of NATO Task Group HFM-178. North Atlantic Treaty Organisation – Research and Technology Organisation (www.rto.nato.int). Neuilly-Sur-Seine Cedex France 2012.
- Ambrosetti, M.; Abreu, A.; Corrà, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.E.; Schmid, J.-P.; Vigorito, C.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 460–495. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Ekblom-Bak, E.; Ekblom, Ö.; Andersson, G.; Wallin, P.; Söderling, J.; Hemmingsson, E.; Ekblom, B. Decline in cardiorespiratory fitness in the Swedish working force between 1995 and 2017. Scand. J. Med. Sci. Sports 2019, 29, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Thornton, J.S.; Frémont, P.; Khan, K.; Poirier, P.; Fowles, J.; Wells, G.D.; Frankovich, R.J. Physical activity prescription: a critical opportunity to address a modifiable risk factor for the prevention and management of chronic disease: a position statement by the Canadian Academy of Sport and Exercise Medicine. Br J Sports Med 2016, 50, 1109–1114. [Google Scholar] [CrossRef] [PubMed]
- Kokkinos, P.; Faselis, C.; Samuel, I.B.H.; Lavie, C.J.; Zhang, J.; Vargas, J.D.; Pittaras, A.; Doumas, M.; Karasik, P.; Moore, H.; et al. Changes in Cardiorespiratory Fitness and Survival in Patients With or Without Cardiovascular Disease. Journal of the American College of Cardiology 2023, 81, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.N.; Rezende, L.F.M.; Ferrari, G.; Del Pozo Cruz, B.; Lee, I.-M.; Stamatakis, E. Do the associations of daily steps with mortality and incident cardiovascular disease differ by sedentary time levels? A device-based cohort study. Br J Sports Med 2024, 58, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Ekelund, U.; Ding, D.; Hamer, M.; Bauman, A.E.; Lee, I.-M. Is the time right for quantitative public health guidelines on sitting? A narrative review of sedentary behaviour research paradigms and findings. Br J Sports Med 2019, 53, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Deutscher Ärzteverlag GmbH, Redaktion Deutsches Ärzteblatt. Mehr als die Hälfte der deutschen Bevölkerung ist chronisch krank. Available online: https://www.aerzteblatt.de/nachrichten/116897/Mehr-als-die-Haelfte-der-deutschen-Bevoelkerung-ist-chronisch-krank (accessed on 25 April 2024).
- Deutscher Ärzteverlag GmbH, Redaktion Deutsches Ärzteblatt. Zahl der Krankheitstage deutlich gestiegen. Available online: https://www.aerzteblatt.de/nachrichten/106881/Zahl-der-Krankheitstage-deutlich-gestiegen (accessed on 25 April 2024).
- 69. Robert Koch-Institut. Gesundheit in Deutschland aktuell - GEDA 2019/2020.
- Abel, T.; Hofmann, K.; Ackermann, S.; Bucher, S.; Sakarya, S. Health literacy among young adults: a short survey tool for public health and health promotion research. Health Promotion International 2015, 30, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Herraiz-Adillo, Á.; Ahlqvist, V.H.; Higueras-Fresnillo, S.; Hedman, K.; Hagström, E.; Fortuin-de Smidt, M.; Daka, B.; Lenander, C.; Berglind, D.; Östgren, C.J.; et al. Physical fitness in male adolescents and atherosclerosis in middle age: a population-based cohort study. Br J Sports Med 2024, 58, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting Physical Activity and Exercise: JACC Health Promotion Series. Journal of the American College of Cardiology 2018, 72, 1622–1639. [Google Scholar] [CrossRef]
- Sallis, J.F.; Hovell, M.F. Determinants of exercise behavior. Exerc. Sport Sci. Rev. 1990, 18, 307–330. [Google Scholar] [CrossRef]
- Smeets, T.; Brug, J.; Vries, H. de. Effects of tailoring health messages on physical activity. Health Educ. Res. 2008, 23, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Leijon, M.E.; Kallings, L.; Faskunger, J.; Lörum, G.; Björjession, M.; Stähle, A. Swedish National Institute of Public Health and Professionals Associatins for Physical Activity: Physical Actitivty in the Prevention of Treatment and Desease Stockholm, 2010.
- Löllgen, H.; Bachl, N.; Pitsiladis, Y.; Pigozzi, F.; Casasco, M. Die magische Kraft der körperlichen Aktivität: das Zehn-Säulen-Modell. Kardiologie 2024, 18, 74–84. [Google Scholar] [CrossRef]
- Baumgartner, N.; Leyk, D.; Reilly, T.J. Chapter 4 - Incentivization. North Atlantic Treaty Organization (NATO) (ed): STO-TR-HFM-269: Combat integration: Implications for physical employment standards. Neuilly-Sur-Seine Cedex 2019; 4-1 - 4-24.
- Sørensen, J.B.; Skovgaard, T.; Puggaard, L. Exercise on prescription in general practice: a systematic review. Scand. J. Prim. Health Care 2006, 24, 69–74. [Google Scholar] [CrossRef]
- Leyk, D.; Hartmann, N.; Nestler, K.; Rüther, T.; Sievert, A.; Rohde, U.; Witzki, A. Physical activity, health perception, barriers to exercise in adult non-athletes and athletes- influence of sport during youth. In Book of abstracts: 24th Annual Congress of the European College of Sport Science, 3-6 July 2019, Prague - Czech Republic; Bunc, V., Tsolakidis, E.K., Eds.; European College of Sport Science: Twenty-fourth Annual Congress of the European College of Sport Science, Köln, 2019; ISBN 9783981841428. [Google Scholar]
- Leyk, D. The problem of “individual operational readiness”: facts and options. WMM 2021, 122–126. [Google Scholar]
Figure 1.
BMI classes of persons aged 50-60 (296 men, 372 women) with different sport status (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”).
Figure 1.
BMI classes of persons aged 50-60 (296 men, 372 women) with different sport status (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”).
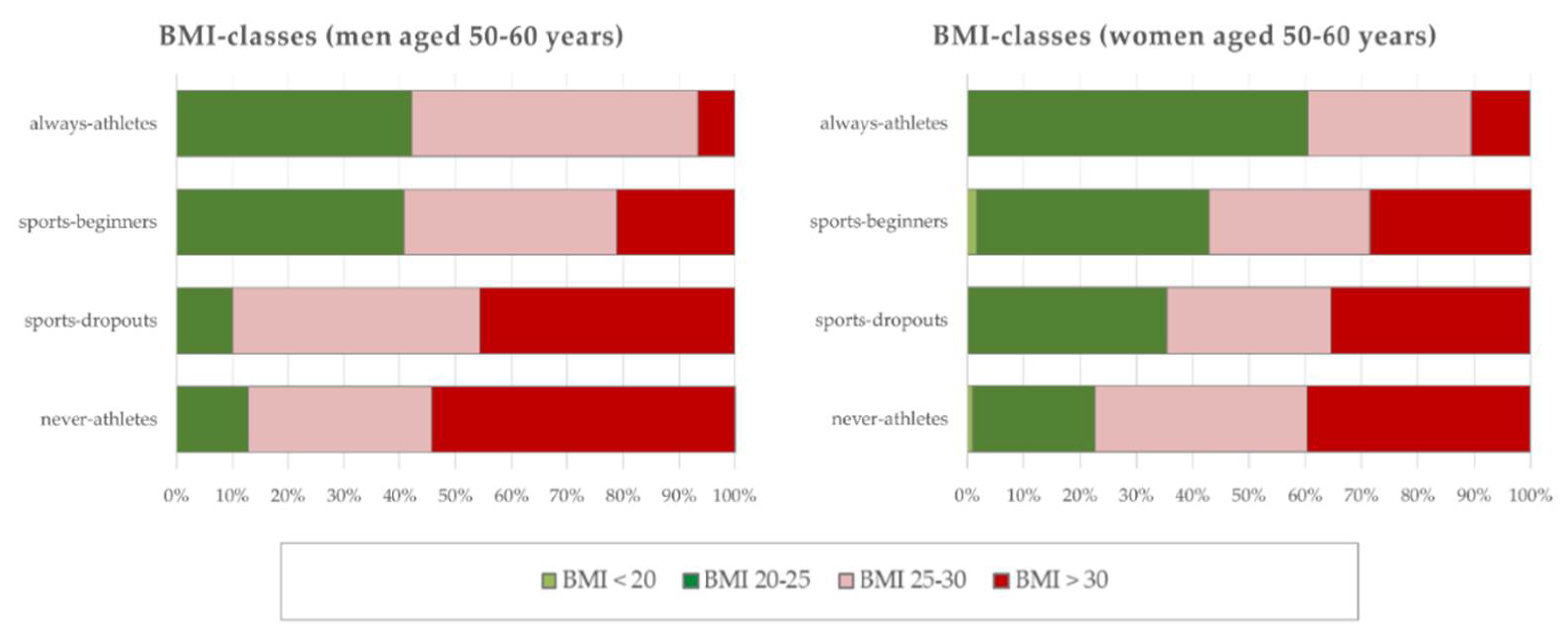
Figure 2.
Assessment of quality of life (using a 5-point Likert scale) - responses from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the question "How would you rate your overall quality of life?".
Figure 2.
Assessment of quality of life (using a 5-point Likert scale) - responses from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the question "How would you rate your overall quality of life?".
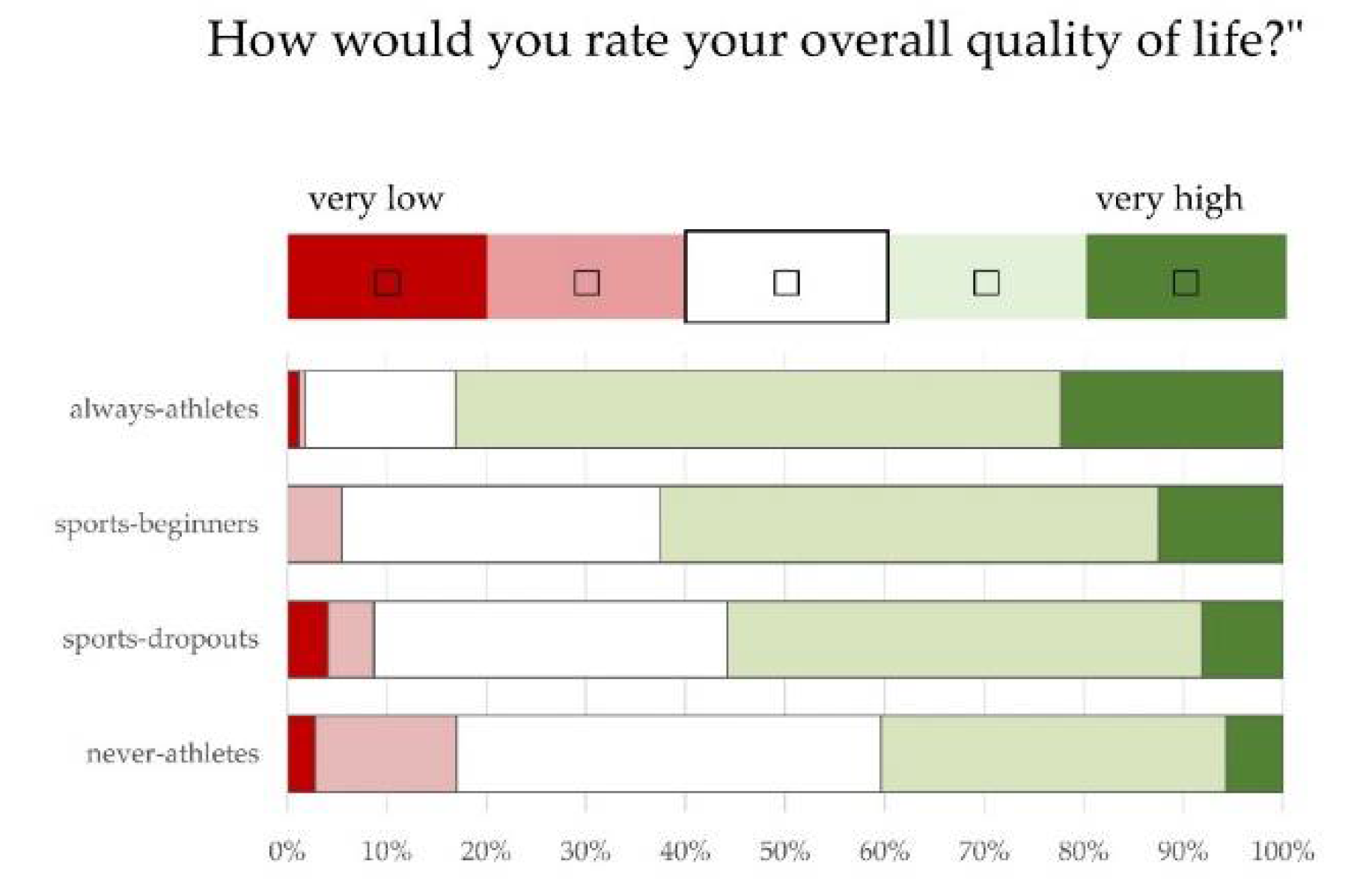
Figure 3.
Assessment of health (using a 5-point Likert scale) - information from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) on the statement "Overall, I feel healthy".
Figure 3.
Assessment of health (using a 5-point Likert scale) - information from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) on the statement "Overall, I feel healthy".
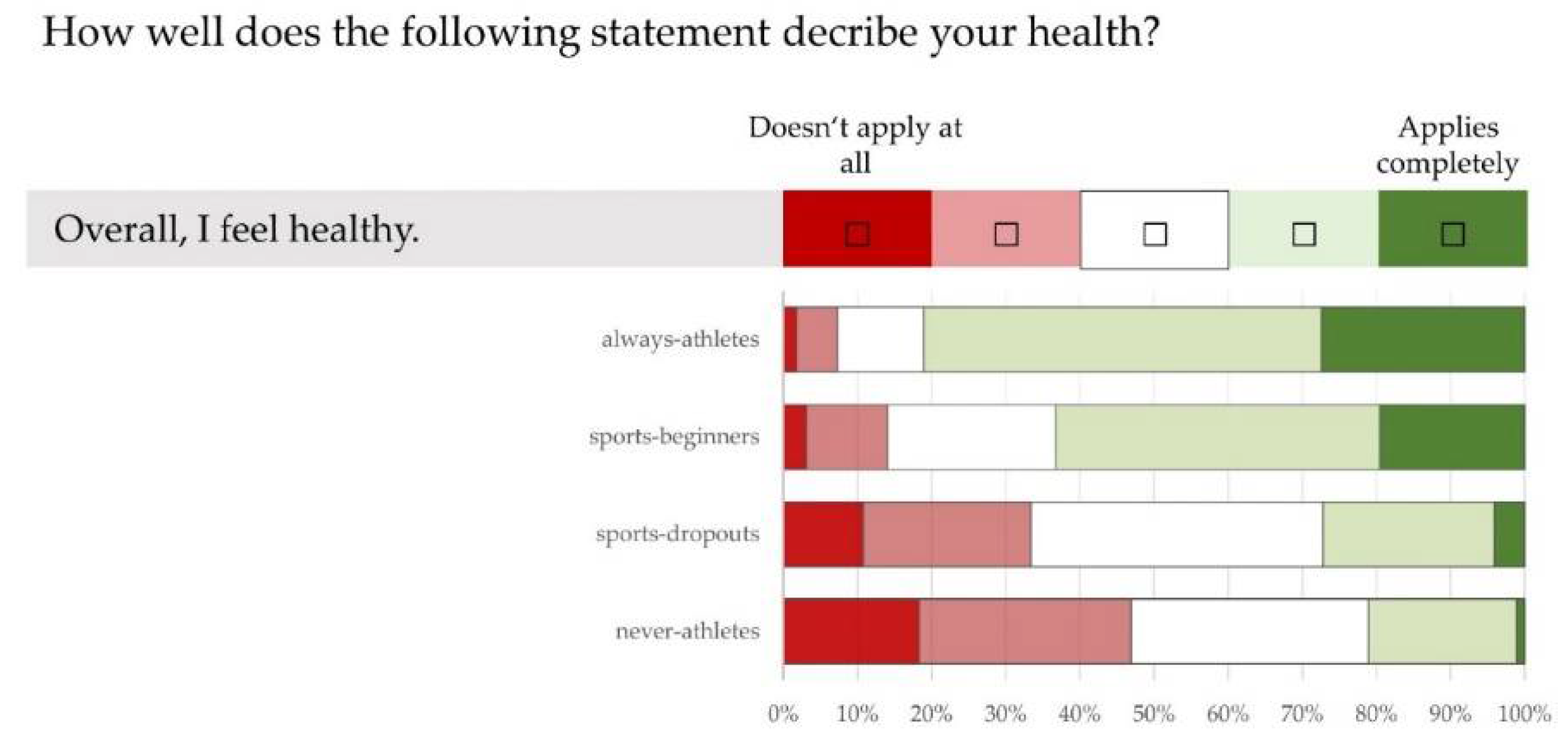
Figure 4.
Assessment of own performance (using a 5-point Likert scale) - information from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) on the statement "Overall, I feel able to perform".
Figure 4.
Assessment of own performance (using a 5-point Likert scale) - information from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) on the statement "Overall, I feel able to perform".
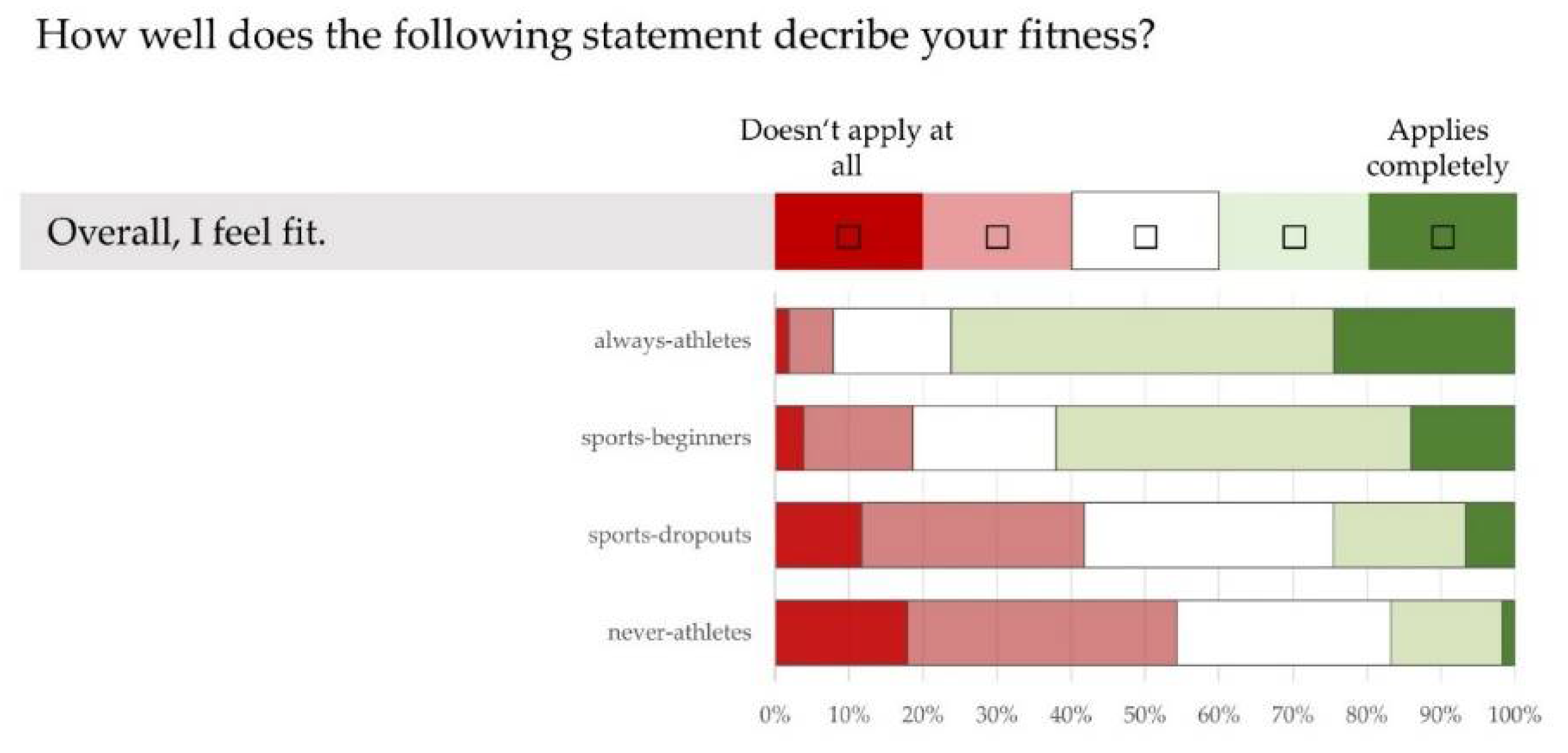
Figure 5.
Assessment of motivation to do sport (using a 5-point Likert scale) - responses from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the statement "I am motivated to do sport".
Figure 5.
Assessment of motivation to do sport (using a 5-point Likert scale) - responses from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the statement "I am motivated to do sport".
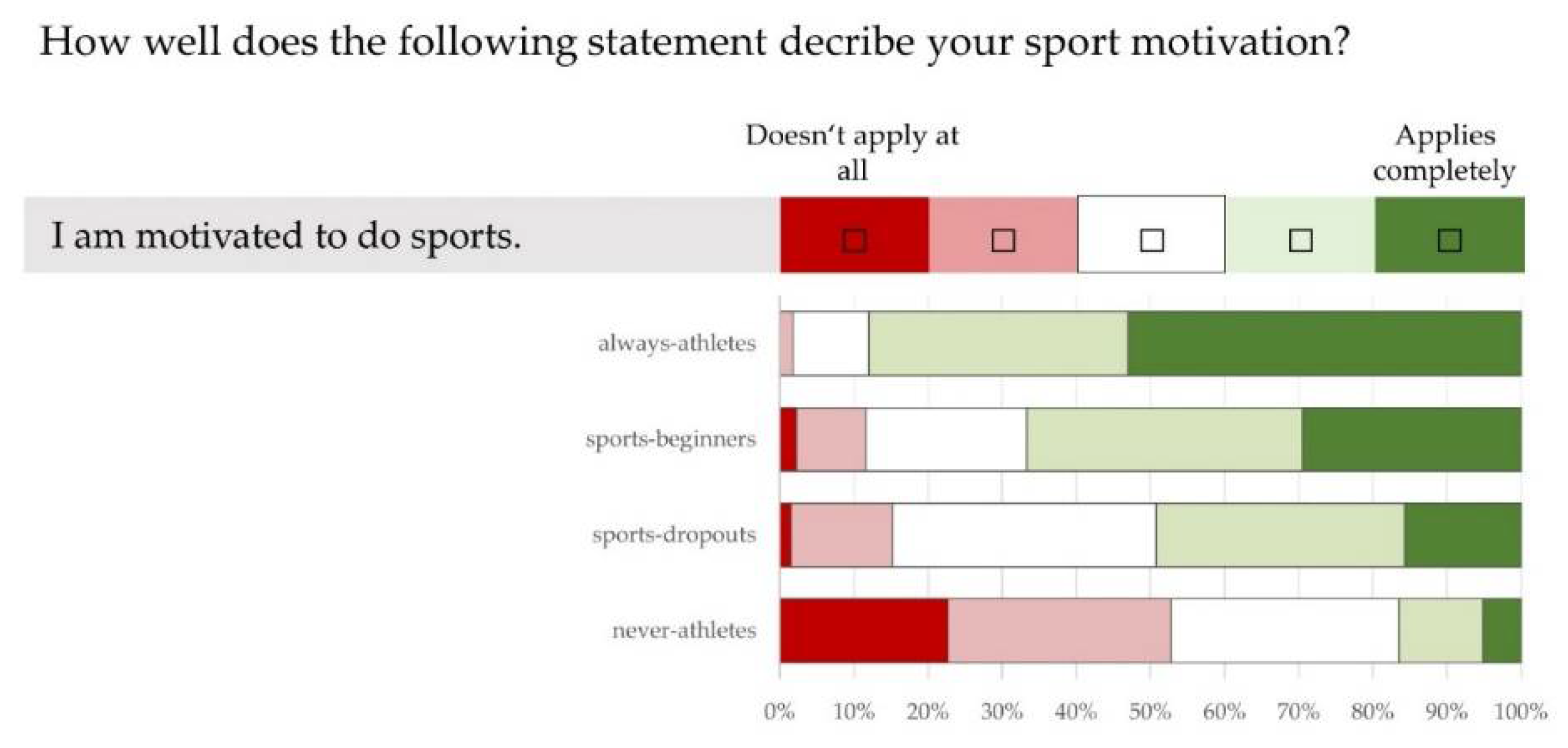

Table 1.
Mean Age, body height, body weight and body mass index (BMI) of 50-60 year old men (above; n= 296) and women (below; n=372) with different sport status (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”). Means + Standard deviation.
Table 1.
Mean Age, body height, body weight and body mass index (BMI) of 50-60 year old men (above; n= 296) and women (below; n=372) with different sport status (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”). Means + Standard deviation.
| Men | never-athletes | sports-dropouts | sports-beginners | always-athletes |
|---|---|---|---|---|
| Number of men | 70 | 70 | 66 | 90 |
| Age (years) | 56.2+2.4 | 55.8+2.6 | 54.3+2.8 | 55.2+2.8 |
| Body height (cm) | 180.2+7.3 | 181.2+6.9 | 180.7+6.0 | 179.3+6.5 |
| Body weight (kg) | 101.3+18.6 | 97.7+15.6 | 86.4+12.7 | 82.9+10.2 |
| BMI | 31.16+5.2 | 29.74+4.4 | 26.46+3.7 | 25.67+2.8 |
| Women | never-athletes | sports-dropouts | sports-beginners | always-athletes |
| Number of women | 106 | 127 | 63 | 76 |
| Age (years) | 55.4+2.7 | 55.6+2.5 | 55.1+2.7 | 55.0+2.6 |
| Body height (cm) | 168.3+7.3 | 167.2+5.8 | 167.4+5.1 | 168.4+6.8 |
| Body weight (kg) | 85.7+20.7 | 79.0+16.9 | 78.0+20.2 | 70.61+13.4 |
| BMI | 30.5+7.7 | 28.3+5.7 | 27.8+6.6 | 24.9+4.2 |
Table 2.
Frequency of unfavourable lifestyle habits - responses from 50-60 year olds (n= 668) with different sporting status (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the question "Which lifestyle habits are so unfavourable that they could affect your health?
Table 2.
Frequency of unfavourable lifestyle habits - responses from 50-60 year olds (n= 668) with different sporting status (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the question "Which lifestyle habits are so unfavourable that they could affect your health?
| never-athletes | sports-dropouts | sports-beginners | always-athletes | |
|---|---|---|---|---|
| Exercise behaviour | 69.3% | 53.3% | 22.5% | 11.4% |
| Diet/eating behaviour | 39.2% | 29.4% | 25.6% | 12.7% |
| Consumption of stimulants (coffee, sweets, etc.) | 37.5% | 46.2% | 34.1% | 36.1% |
| Sleeping habits | 23.9% | 28.4% | 24.8% | 18.1% |
| Smoking behaviour | 22.7% | 9.1% | 11.6% | 4.2% |
| Consumption of medication | 9.7% | 8.6% | 3.1% | 4.8% |
| Alcohol consumption | 5.7% | 7.1% | 12.4% | 16.9% |
| Social media / TV consumption / gaming habits | 4.0% | 7.1% | 5.4% | 4.8% |
| Drug use | 0.0% | 0.0% | 1.6% | 1.2% |
Table 3.
Frequency of health problems in the last 12 months - responses from individuals aged 50-60 (n= 668) with different sporting statuses (“always-athletes”, “sports-beginners”, “sports-dropouts”, “never-athletes”) to the question "Have you experienced the following health problems in the last 12 months?".
Table 3.
Frequency of health problems in the last 12 months - responses from individuals aged 50-60 (n= 668) with different sporting statuses (“always-athletes”, “sports-beginners”, “sports-dropouts”, “never-athletes”) to the question "Have you experienced the following health problems in the last 12 months?".
| never-athletes | sports-dropouts | sports-beginners | always-athletes | |
|---|---|---|---|---|
| Back pain | 76.10% | 68.00% | 51.20% | 42.20% |
| Muscle or joint pain | 73.90% | 74.60% | 57.40% | 49.40% |
| Dizziness | 31.30% | 33.50% | 21.70% | 17.50% |
| Breathing problems | 20.50% | 19.80% | 9.30% | 4.20% |
| Chest pain | 9.70% | 9.60% | 4.70% | 4.20% |
| Fall due to health problems | 6.80% | 7.60% | 6.20% | 1.20% |
| Loss of consciousness | 1.70% | 1.50% | 0.00% | 2.40% |
Table 4.
Most common motives for doing sport - responses from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the question "What motivates you or would motivate you to do sport?”.
Table 4.
Most common motives for doing sport - responses from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the question "What motivates you or would motivate you to do sport?”.
| never-athletes | sports-dropouts | sports-beginners | always-athletes | |
|---|---|---|---|---|
| Health reasons | 69.3% | 84.8% | 88.4% | 87.3% |
| Weight reduction/weight control | 61.4% | 66.0% | 69.8% | 68.1% |
| Physical performance | 49.4% | 75.6% | 79.1% | 91.0% |
| Stress reduction / balance | 41.5% | 65.0% | 62.0% | 81.9% |
| Enjoyment of sport | 30.1% | 66.0% | 54.3% | 86.1% |
| Motivation to achieve something | 26.1% | 45.2% | 47.3% | 64.5% |
| Community experience | 23.3% | 41.1% | 20.9% | 41.6% |
| Sporty, good looks | 22.7% | 32.0% | 25.6% | 51.8% |
| Personal environment (acquaintances, friends, family) | 18.8% | 31.0% | 24.8% | 44.0% |
| Other reasons | 3.4% | 2.0% | 3.1% | 1.8% |
Table 5.
Most common barriers to doing sport - responses from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the question "What prevents you from doing (more) sport?".
Table 5.
Most common barriers to doing sport - responses from 50-60 year olds (n= 668) with different sporting statuses (“always-athletes”, “sport-beginners”, “sports-dropouts”, “never-athletes”) to the question "What prevents you from doing (more) sport?".
| never-athletes | sports-dropouts | sports-beginners | always-athletes | |
|---|---|---|---|---|
| Health reasons | 70.9% | 73.1% | 36.5% | 34.5% |
| Lack of motivation | 53.4% | 31.3% | 25.0% | 16.4% |
| Lack of time | 45.6% | 40.3% | 63.5% | 61.8% |
| No fun in sports | 35.9% | 9.7% | 19.2% | 5.5% |
| Lack of sports partners (acquaintances, friends, family) | 35.9% | 21.6% | 11.5% | 12.7% |
| Sport is too strenuous | 31.1% | 10.4% | 17.3% | 7.3% |
| No suitable sports programme | 30.1% | 24.6% | 11.5% | 5.5% |
| Other reasons | 2.8% | 7.6% | 2.3% | 1.2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



