
Submitted:
11 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
The mortality rate of women during the gestation period or after delivery is very high worldwide. ToRCH pathogens [Toxoplasma gondii (T.gondii), Rubella Virus (RV), Cytomegalovirus (CMV), and Herpes Simplex Virus (HSV)] are transmitted vertically and are associated with mortality and complications both in the mother and the fetus or children. Therefore, this study is designed to investigate the ToRCH pathogen-induced histopathological changes in placental tissues and associated post-obstetric complications in Pakistani women. Women (N = 68) included in this study were divided into Group A (women with current abortion and bad obstetric history-BOH) and Group B (women with normal delivery and BOH). The venous blood collected was analyzed for ToRCH antibodies through ELISA. A small piece of placenta tissue taken after delivery or abortion was subjected to nucleic acid (NA) detection through PCR using ToRCH pathogen-specific primers. The placental tissue was analyzed for histopathological changes under a microscope. The data obtained were analyzed using percentages and the Chi square test. Overall ToRCH antibody positivity was 64.70% (44/68). Of these, IgM (Immunoglobulin M) was found in 17.65% (12/68), IgG (Immunoglobulin G) in 45.59% (31/68), and one case (1.47%) was seropositive for both IgM and IgG. The NA was detected in 66.18% (45/68) of the placental tissues of the study population. The higher prevalence of antibodies for T.gondii and RV (23.53% each) and NA for RV, CMV, and HSV (17.99% each) was observed in the study population. The ToRCH infection (antibodies and NA) with BOH complications was statistically found to be non-significant (p> 0.05). Overall discrepancies in ToRCH antibodies and NA positivity were found in 86.76% (59/68) of cases, especially for RV (26.47%). Chorionic villitis (CV) in placental tissues was observed in 20.59% (14/68), i.e., 13.23% of Group A and 7.35% of Group B. Of the total, four women with T.gondii, six with RV, and three each with CMV and HSV infection were found with CV. The most common BOH complications observed were recurrent spontaneous abortions (RSAs) (47.05%, 32/68), stillbirth (22.05%, 15/68), congenital abnormalities (14.70%, 10/68), etc. It was observed that RSAs were associated with CV (10.29%) in the study population. The BOH complication and CV were found to be statistically non-significant (p> 0.05). It is concluded that ToRCH pathogens are prevalent in the study population, and CV was the only histopathological change found and associated with BOH complications.
Keywords:
ToRCH pathogen
; antibodies
; nucleic acid (NA)
; placenta
; chorionic villitis (CV)
; bad obstetric history (BOH)
1. Introduction
The mortality rate of pregnant women during the gestation period or after delivery is about 0.287 million per year worldwide [1]. The vast majority of maternal deaths (95%) and perinatal deaths (exceeding 7.6 million) occurred in underprivileged areas worldwide [1,2], which can lead to frustration among families and cause a burden on the health economy. The BOH is one of the leading causes of death in pregnant women [3]. Various complications of BOH, like RSAs, account for 15 to 20% of all pregnancies [4], and the stillbirth rate is 3-5/1000 of total births [5]. The other complications include intrauterine growth retardation (IUGR), early neonatal expiry, and/or congenital abnormalities (CA) [6]. Infectious agents like ToRCH pathogens are among the etiological factors of BOH [3]. These pathogens are transmissible inside the uterus at different trimesters of pregnancy, depending on the age of gestation at the time of infection, the severity of the maternal disease, the virulence of the organism, and impairment in the placental tissues [7,8]. Since the placenta is the connecting link between the mother and the fetus, therefore, placental pathophysiological changes may have negative impacts on the mother's and the fetus's or baby's health [9,10,11].
Pakistan is one of the top-ranked counties for BOH complications, and the maternal mortality rate is 186 deaths per 100,000 live births [12]. Various studies showed that ToRCH pathogens are highly prevalent across the globe, and the rate is relatively high among Asian women at childbearing age [13]. Similarly, a wide distribution of these pathogens is reported in Pakistan [14,15,16,17,18,19,20,21]. Therefore, this study is designed to analyze ToRCH pathogen-induced histopathological changes in placental tissues and associated post-obstetric complications in women from Pakistan.
2. Materials and Methods
2.1. Study Area/Design
The study was conducted in Peshawar, the capital city of the Khyber Pakhtunkhwa province of Pakistan. The study was carried out from May 2022 to April 2023. Women (N = 68) with a previous history of BOH and ages 18–47 were enrolled in this study. The study subjects were divided into two groups: Group A (n = 43), comprised of women with current abortions at the time of sample collection, and Group B (n = 25), which contains women with normal delivery.
2.2. Inclusion Criteria
Women within the reproductive age range, any ethnic group, with regular and normal menstrual cycles, normal body weight, and no serious diagnosed disease were included in the study population. Furthermore, women with a history of two or more adverse pregnancy outcomes were the main inclusion criteria.
2.3. Samples and Data Collection
Venous blood (3 mL) was collected in sterile tubes, and serum was separated and stored at -20 °C at the Laboratory of Virology and Immunology, Department of Zoology, University of Peshawar. Placental tissues were collected after delivery or abortion by expert medical personnel at Lady Reading Hospital, Peshawar, and preserved in 300 mL of Tris-EDTA buffer (Tris-HCl 10 mM; EDTA 1 mM). Data, including demographic and clinical results, was collected through a pre-designed questionnaire. A proper written consent was obtained from study participants at the time of sample and data collection.
2.4. Ethical Approval
The present study was approved by the Ethical Committee, University of Peshawar, under Applicant # 313/EC/F.LIFE/UOP-2020, dated November 3, 2020.
2.5. Enzyme Linked Immune Sorbent Assay (ELISA)
Antibodies (IgM and IgG) of ToRCH pathogens were detected in serum through IgM and IgG ELISA kits (DRG International USA) for each pathogen, according to the instructions of the manufacturer.
2.6. Nucleic acid (NA) Extraction
DNA for T.gondii, CMV, and HSV, and RNA for RV, were extracted from placenta tissues using the TRIzol TM Reagent Kit (Thermo Fisher Scientific, USA) following the manufacturer’s protocol.
2.6.1. Nucleic Acid Amplification
The DNA of T.gondii, CMV, and HSV was amplified using the protocols of Sadek et al. [22], Munro et al. [23], and Coyle et al. [24], respectively, while RNA of RV was reverse transcribed to cDNA using RevertAid RTase (Thermo Fisher Scientific, USA) and amplified according to the protocol of Bosma et al. [25]. The amplifications were carried out using the Dream Taq Green PCR Master Mix (Thermo Fisher Scientific, USA) according to the manufacturer’s instructions.
2.6.2. Gel Electrophoresis
PCR-amplified products were electrophoresed on a 2% agarose gel visualized under UV light and compared with the 50-bp DNA ladder.
2.7. Histopathological Examination of Placenta Tissues
The placental tissues were fixed with 10% formalin, dehydrated in ethanol (70% and 100%), and then embedded in paraffin wax using routine tissue processing. A four-μm-thick section was cut from each block prepared, deparaffinized, rehydrated, and stained with hematoxylin and eosin. The prepared slide was then observed under a microscope for histopathological changes. The microscopic examinations were reported by a consultant histopathologist at the Northwest General Hospital and Research Center in Peshawar, Pakistan.
2.8. Data Analysis
The data were analyzed in percentages, and a χ2 test was applied where a p-value <0.05 was considered statistically significant.
3. Results
3.1. Demographics of Study Population
The demographic factors of the study population are shown in Table 1. The participants of the study were divided into three age groups (G-I, G-II, and G-III). Most of the women in Group A and B were of age group G-II. At the time of abortion, 41.86% of women were in the 1st trimester, 44.18% in the 2nd trimester, and 13.95% in the 3rd trimester of pregnancy.
The overall seropositivity of ToRCH pathogens was 64.70% (44/68). Of these, IgM was 17.64% (12/68) [16.17% (11/68) in Group A and 1.47% (1/68) in Group B], while IgG was 45.58% (31/68) [32.25% (10/31) in Group A and 67.74% (21/31) in Group B]. One case (1.47%) in Group A was reported positive for both IgM and IgG. Overall, the NA of ToRCH pathogens in placental tissues was detected in 66.18% (45/68) [38.23% (26/68) in Group A and 27.94% (19/68) in Group B] (Table 1 and Table 2).
Overall, the highest frequency of antibodies was observed for T.gondii and RV (23.53%, 16/68), but few were positive for NA of T.gondii (9/16) and RV (12/16). The prevalence of CMV (10.29%, 7/68) and HSV (5.88%, 4/68) antibodies was lower than NA. The prevalence of NA was high for RV, CMV, and HSV (each 17.64%, 12/68) (Table 2). The ToRCH pathogen and associated obstetric complications were found to be statistically non-significant (p > 0.05).
The most common BOH complications observed were RSAs (47.05%, 32/68) and stillbirth (22.05%, 15/68), while others like IUGR, neonatal deaths and CA were less common (Table 1).
3.2. Discrepancies of ToRCH Antibodies and NA Positivity
Some discrepancies were observed in ToRCH antibodies and NA positivity and are shown in Table 3. ToRCH antibodies and NA positivity varied in different women, and the discrepancies were 86.76% (59/68). On the basis of the presence or absence of IgM, IgG, and NA, the study population was divided into six categories, according to discrepant results i.e. Cat-I (IgM, IgG positive, and NA negative), Cat-II (IgM and NA positive, IgG negative), Cat-III (only IgM positive), Cat-IV (only IgG positive), Cat-V (IgG and NA positive), Cat-VI (only NA positive).
The discrepancies were more frequent in Cat-V (in the case of T.gondii and RV) and Cat-VI (in the case of HSV and CMV) (Table 3).
3.3. ToRCH Pathogens and Histopathological Changes
Placental tissue changes examined were compared with ToRCH antibodies and NA positivity and are shown in Table 4. The histopathological changes were compared with normal placental tissue (Figure 1). The only change observed was CV (14/68, 20.59%), as shown in Figure 2 (a and b). Of the total, CV was more prevalent (9/68, 13.23%) in Group A than in Group B (5/68, 7.35%). RV (37.5%) and CMV (25%) infections seem more responsible for CV, as compared to T. gondii (18.75%) and HSV (16.66%).
3.4. Association CV Positivity with BOH Complications
In Group A, a high frequency of CV (7/32, 21.87%) was observed in women with RSAs, the prevalent obstetric complication. Similarly, stillbirth was the second most common complication found (8/43, 18.60%), but fewer CV cases were observed (1/8, 12.5%). While fewer women (4/43, 9.30%) were affected by neonatal deaths as their BOH, CV was observed more (2/4, 50%). Other complications like IUGR (2/43, 4.65%) and congenital abnormalities-CA (6/43, 13.95%) were also found to be less common, but CV was examined in (1/2, 50%) IUGR and (1/6, 16.7%) CA-positive women.
In Group B, the high BOH complication observed was RSAs and was more prevalent (9/25, 36%) than still birth (7/25, 28%), and 3/9 and 1/7 cases of these women were affected by CV, respectively. The least observed complications were neonatal deaths (5/25, 20%) and CA (4/25, 16%), in which CV (1/5 cases) was observed only in neonatal deaths that affected women, while no one case with a CA positive was found to be affected by CV. IUGR was not found in Group B. Statistically, the p-value > 0.05 was not significant in the association of BOH complications with CV.
4. Discussion
It is well documented that pregnancy is associated with increased susceptibility and severity toward infectious diseases due to several hormonal and immunological alterations that occur during the course of pregnancy [26,27,28,29]. ToRCH pathogens are one of the causes responsible for the mortality of pregnant women, especially during the gestation period or after delivery, worldwide. The majority of these deaths, as well as the perinatal ones, are due to pathogen-associated complications and altered placental histology. The seropositivity of ToRCH infection was high in the study population of the present study (Table 2). The prevalence of ToRCH pathogens is prevalent in Pakistan, as reported from different regions [14,15,16,17,18,19,20,21].
The high frequency of T.gondii and RV antibodies (Table 2) was frequent in women with histological changes in the study population. The high frequency of IgM was noted in RV and IgG in T.gondii-infected women. Similar situations were also reported by others [30,31]. The high prevalence of RV may be due to the fact that it can transmit easily and spread through the respiratory tract [30]. The chronic infection with RV leads to hypoplastic organomegaly in the fetus, which leads to BOH [32]. T.gondii is normally transmitted through food, and its chances of spreading in underdeveloped communities are greater [30]. The high seroprevalence of T.gondii IgG in the current study population may be due to the exposure of the study population to different modes of pathogen transmission, like poor personal hygienic practices, more animal contact, giving more time for agriculture work where soil is contaminated with the infected cat faces, poor sanitary conditions, and a lack of awareness because of the poor education system [33]. Moreover, CMV and HSV are less frequent in the study population due to their prevalence in the area. The frequency of these viruses is linked with the spread, study subjects, and area in other studies [34,35,36]. The ToRCH pathogens and associated obstetric complications were found to be statistically non-significant (p> 0.05).
The ToRCH pathogens were detected in placental tissues and were compared with antibody results. The occurrence of active (NA detection) RV, CMV, and HSV was high (Table 2), which leads to BOH. Other studies from different parts of the world also showed the high prevalence of these pathogens in pregnant women that caused BOH, like RSAs, neonatal deaths, etc. [11,13,35,36,37]. Sometimes false seropositivity due to the probability of some other microbial infections leads to the diagnosis of the actual pathogen [18], and PCR remains the ultimate diagnostic tool. The NA in placental tissue portrays the actual position of the ToRCH pathogen and its consequences for BOH outcomes. The viral pathogens (RV, CMV, and HSV) were each positive in 17.64% in study population (Table 2). The presence of viral NA infection in the majority of pregnant women despite antibody development indicates the possibility of reinfection or immunosuppressive condition in most of the cases [33]. One of the women was observed with T.gondii IgM and IgG at the same time (Table 3), which might indicate the presence of two different strains of the pathogens circulating in the study area. It is reported that reinfection with a variant strain can cause infections even in the presence of detectable IgG levels [38].
Some of the women who were observed with IgM (Cat-III) or IgG (Cat-IV) only showed acute or chronic infection. The IgG positivity may be due to the previous exposure of the patient to these pathogens [34,39]. The IgM and NA presence (Cat-II) were also found, which indicates the high load of pathogens present in placental tissues. In most of the women, IgG and NA were both positive (Cat-V) and showed a persistent infection with the ToRCH pathogens. It is noteworthy that few of the women were positive for NA only (Cat-VI) in the case of T.gondii and RV, while there was a high prevalence of CMV and HSV. Both the CMV and HSV cause latent infection [40,41], and it is quite possible that they evade the immune system and IgM and IgG may not be detected [42,43].
ToRCH pathogens represent the majority of placental infections associated with chronic inflammation [44], as they can enter the intra-amniotic space and overcome the defense mechanisms of the placenta that protect against vertical microbial transmission [42]. In the present study, the placental tissue examination revealed that CV was the main histopathological condition observed in the study population. The CV was frequent in women with T.gondii and RV infection (Table 4). RV infects the epithelium of CV and the endothelium of the blood vessels of the placenta [45].
Among women experiencing BOH complications, a considerable number (20.59%) of the study population were identified with CV (Table 5). This suggests an association between CV and BOH complications [46]. It has been previously reported that infection with the ToRCH complex leads to spontaneous abortions [18,47,48]. ToRCH infection during the gestation period causes disturbances in the early development of the placenta with the involvement of the vascular component and the villous profile, with a negative impact on the pregnancy resulting in miscarriage [49]. Although the p-value > 0.05 in relation to BOH complications with CV was not significant, The ToRCH pathogen can induce histopathological conditions like products of conception, inflammatory infiltrates, chronic endometritis, etc. [50] and pregnancy loss [51].
It is concluded that ToRCH pathogens are prevalent in the study area. CV is the most frequent histopathological condition found in the study population, associated with BOH complications. The results support the need for ToRCH pathogen screening among reproductive-age women in general and particularly during early pregnancy, which will help to treat women in the area timely and will thus help reduce the risk of morbidity and mortality.
Author Contributions
Conceptualization, M.N. and S.K.; methodology, M.N.; investigation, N.S. and S.N.; resources, S.K., D.S.A.; writing—original draft preparation, M.N.; review and editing, M.A., F.R., S.A. and T.A.S.; visualization, N.S.; supervision, S.K.; funding acquisition, D.S.A. and K.A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Princess Nourah bint Abdul Rahman University Saudi Arabia Researchers Supporting Project No. PNURSP2024R465.
Institutional Review Board Statement
The study was approved by the Ethical Committee, University of Peshawar, under Applicant # 313/EC/F.LIFE/UOP-2020, dated November 3, 2020.
Data Availability Statement
All the data are included within the article.
Acknowledgments
The authors extend their appreciation to the Deanship of Scientific Research at Princess Nourah bint Abdul Rahman University Saudi Arabia.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- WHO, 2023; https://www.who.int/news-room/fact-sheets/detail/maternal-mortality. Accessed on date November 2, 2023.
- Qadir M, Amir S, Jadoon S, Marwat M. Frequency and causes of perinatal mortality in a tertiary care hospital in Peshawar, Pakistan. GJMS. 2018, 16, 15–19. [Google Scholar] [CrossRef]
- Nath J, Malhotra S, Rani N. A study on bad obstetrics history-with special emphasis on etiological high-risk factors. Neonat Pediatr Med. 2021, 7, 1–3. [Google Scholar]
- Ghazaey S, Keify F, Mirzaei F, Maleki M, Tootian S, Ahadian M, Abbaszadegan MR. Chromosomal analysis of couples with repeated spontaneous abortions in northeastern iran. Int. J. fertile. Steril. 2015, 9, 47. [Google Scholar] [CrossRef] [PubMed]
- Ahmed J, Alam A, Khokhar S, Khowaja S, Kumar R, Greenow C-R. Exploring women’s experience of health care use during pregnancy and child birth to understand factors contributing to perinatal deaths in Pakistan: A qualitative study. PloS One. 2020, 15, e0232823. [Google Scholar]
- Qi Y, Zhu S, Li C, Wu H, Yue H, Zhang Y, Zhu B, Ma J, Feng Z, Kong H, Cai X. Sero epidemiology of ToRCH antibodies in the reproductive-aged women in China. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2020, 254, 114–118. [Google Scholar]
- Manjunathachar HV, Singh KN, Chouksey V, Kumar R, Sharma RK, Barde PV. Prevalence of ToRCH infections and its associated poor outcome in high-risk pregnant women of central India: time to think for prevention strategies. Indian journal of medical microbiology. 2020, 38, 379–384. [Google Scholar] [CrossRef]
- Boyer SG, Boyer KM. Update on ToRCH infections in the newborn infant. Newborn Infant Nurs. Rev. 2004, 4, 70–80. [Google Scholar] [CrossRef]
- Kumar S, Sudarshan V. Placental histopathology in high-risk pregnancy. Journal of Obstetrics and Gynecology. 2018, 39-45.
- Ghidini A, Salafia CM. Histologic placental lesions in women with recurrent preterm delivery. Acta obstetricia et gynecologica Scandinavica. 2005, 84, 547–550. [Google Scholar] [CrossRef] [PubMed]
- Boyd TK, Redline RW. Chronic histiocytic intervillositis: a placental lesion associated with recurrent reproductive loss. Hum Pathol. 2000, 31, 1389–1396. [Google Scholar] [CrossRef]
- Shaeen SK, Tharwani ZH, Bilal W, Islam Z, Essar MY. Maternal mortality in Pakistan: challenges, efforts, and recommendations. Annals of Medicine and Surgery. 2022, 81, 104380. [Google Scholar]
- Liu Y, Wu Y, Wang F, Wang S, Zhao W, Chen L, Tu S, Qian Y, Liao Y, Huang Y, Zhang R. The Association between Previous ToRCH Infections and Pregnancy and Neonatal Outcomes in IVF/ICSI-ET: A Retrospective Cohort Study. Front. Endocrinol. 2020, 11, 466. [Google Scholar] [CrossRef] [PubMed]
- Karamat S, Khan FA, Saeed S, Jafri A, Langhani SK, Saleem A. Occurrence of Seropositivity of Toxoplasma gondii, Cytomegalovirus, and Rubella Infections in Pregnant Women. Pak. J. Med. Health Sci. 2022, 16, 25–25. [Google Scholar]
- Mahmood F, Zafar M, Noreen S, Gul S, Ullah I. Khattak S. Evaluation of Herpes, Cytomegalovirus, Rubella, and Toxoplasma Gondii Infections in Swabi, KPK, Pakistan. Pak. J. Med. Health Sci. 2022, 16, 967–967. [Google Scholar]
- Saddam GA, Rehman A, Shahzad A. Prevalence of Cytomegalovirus, Rubella and Toxoplasma gondii among Internally Displaced Women of District North Waziristan, Pakistan with Home Obstetric History. J Biomed Res Environ Sci. 2021, 2, 1231–1237. [Google Scholar] [CrossRef]
- Zeb MA, Jamal SF, Mir A, Khan AA, Ullah A. Frequency of Torch Infections during Pregnancy in Peshawar, Pakistan. Adv. Appl. Sci. Res. 2018, 9, 22–26. [Google Scholar]
- Jamil S, Ahmed B, Ali S, Bashir S, Mahmood N, Idress M. Assessment of ELISA and real time PCR in diagnosis of Cytomegalovirus and Herpes Simplex Virus in Pregnant Women of Peshawar, Pakistan. Int. J. Biosci. 2017, 11, 35–42. [Google Scholar] [CrossRef]
- Mujtaba G, Khurshid A, Sharif S, Alam MM, Aamir U-B, Shaukat S, Angez M, Rana MS, Umair M, Shah AA, Zaidi SSZ. Distribution of cytomegalovirus genotypes among neonates born to infected mothers in Islamabad, Pakistan. PLoS One. 2016, 11, e0156049. [Google Scholar]
- Shah AA, Muhammad H, Farooqi N, Gul N, Khan AA, Nabi G, Khan SN. Association of ToRCH Agents with Spontaneous Abortion in Patients with Bad Obstetric History. WJZ. 2015, 10, 291–294. [Google Scholar]
- Ali S, Khan FA, Mian AA, Afzal MS. Seroprevalence of cytomegalovirus, herpes simplex virus and rubella virus among pregnant women in KPK province of Pakistan. JIDC. 2014, 8, 389–390. [Google Scholar] [CrossRef]
- Sadek OA, Abdel-Hameed ZM, Kuraa HM. Molecular detection of Toxoplasma gondii DNA in raw goat and sheep milk with discussion of its public health importance in Assiut Governorate. Assiut Vet. Med. J. 2015, 61, 166–177. [Google Scholar] [CrossRef]
- Munro SC, Hall B, Whybin LR, Leader L, Robertson P, Maine GT, Rawlinson WD. Diagnosis of and screening for cytomegalovirus infection in pregnant women. J. Clin. Microbial. 2005, 43, 4713–4718. [Google Scholar] [CrossRef] [PubMed]
- Coyle PV, Desai A, Wyatt D, McCaughey C, O’Neill HJ. A comparison of virus isolation, indirect immunofluorescence and nested multiplex polymerase chain reaction for the diagnosis of primary and recurrent herpes simplex type 1 and type 2 infections. J. Virol. Methods. 1999, 83, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Bosma TJ, Corbett KM, O'Shea S, Banatvala JE, Best JM. PCR for detection of rubella virus RNA in clinical samples. J. Clin. Microbial. 1995, 33, 1075–1079. [Google Scholar] [CrossRef] [PubMed]
- Abdoli A, Pirestani M. Are pregnant women with chronic helminth infections more susceptible to congenital infections? Front Immunol. 2014, 5, 53. [Google Scholar]
- Kourtis AP, Read JS, Jamieson DJ. Pregnancy and infection. N Engl J Med. 2014, 370, 2211–2218. [Google Scholar] [CrossRef] [PubMed]
- Krishnan L, Nguyen T, McComb S. From mice to women: the conundrum of immunity to infection during pregnancy. J Reprod Immunol. 2013, 97, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Sappenfield E, Jamieson DJ, Kourtis AP. Pregnancy and susceptibility to infectious diseases. Infect Dis Obstet Gynecol doi. 2013, 2013, 752852. [Google Scholar]
- Obaid HM, Juma S-A. ToRCH screening test in pregnant women of Kirkuk city. MJS. 2016, 27, 17–25. [Google Scholar]
- Sadik MS, Fatima H, Jamil K, Patil C. Study of ToRCH profile in patients with bad obstetric history. Biol Med. 2012, 4, 95. [Google Scholar]
- Kishore J, Misra R, Paisal A, Pradeep Y. Adverse reproductive outcome induced by Parvovirus B19 and ToRCH infections in women with high-risk pregnancy. JIDC. 2011, 5, 868–873. [Google Scholar] [CrossRef]
- Vora KS, Gupta P, Saiyed S, Prajapati B, Natesan S. Prevalence of ToRCH Infections during Pregnancy: A Prospective Cohort Study in Tribal Region of Gujarat, India. ASWH. 2020, 2, 16–22. [Google Scholar]
- Kakayi ST, Haji HO, Al-Daoody AAK. Incidence of Miscarriage in Pregnant Women due to ToRCH Co-Infection in Erbil City/Iraq. JUBPAS. 2021, 29, 1–15. [Google Scholar]
- AL-Saeed AT, Abdulmalek IY, Ismail HG. ToRCH Infections in Mothers with BOH as a Cause of Neonatal Miscarriages and Fetal Malformation in Duhok Province, Kurdistan Region/Iraq. Sci J Univ Zakho. 2015, 3, 183–193.
- Jasim M, Majeed HA, Ali AI. Performance of Serological Diagnosis of ToRCH Agents in Aborted versus non aborted Women of West province in Iraq Tikrit Med J. 2011, 17. [Google Scholar]
- Jahromi AS, Kazemi A, Manshoori G, Madani A, Moosavy S, Seddigh B. Seroprevalence of rubella virus in women with spontaneous abortion. Am. J. Infec. Dis. 2011, 7, 16–19. [Google Scholar] [CrossRef]
- 38. Nirmal K, Saha R, Ramachandran VG. Khan AM. ToRCH infection in antenatal women: A 5-year hospital-based study. EJMS.. 2017; 54-57.
- Ali MS, Qowaider SR, Almal NYB. and Kahald FA. Seroprevalence of Antibodies to Cytomegalovirus, Rubella Virus and T. gondii among aborted women in El-Beida City. Saudi J Biomed Res. 2020, 5, 357–362. [Google Scholar] [CrossRef]
- Manandhar T, Hò G-T, Pump WC, Blasczyk R and Bade-Doeding C. Battle between Host Immune Cellular Responses and HCMV Immune Evasion. Int. J. Mol. Sci. 2019; 20: 3626.
- Goodrum, F. Human Cytomegalovirus Latency: Approaching the Gordian Knot. Annu Rev Virol. 2016, 3, 333–357. [Google Scholar] [CrossRef]
- Deftereou TE, Trypidi A, Alexiadi CA, Theotokis P, Manthou ME, Meditskou S, Simopoulou M, Lambropoulou M, Maria L. Congenital herpes simplex virus: A histopathological view of the placenta. Cureus. 2022, 14, e29101. [Google Scholar]
- Jackson SE, Mason GM, Wills MR. Human cytomegalovirus immunity and immune evasion. Virus Research. 2011, 157, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Al-Adnani M, Marnerides A. Chronic inflammatory conditions of the placenta. Diagnostic Histopathology. 2023, 29, 554–562. [Google Scholar] [CrossRef]
- Chudnovets A, Liu J, Narasimhan H, Liu Y, Burd I. Role of inflammation in virus pathogenesis during pregnancy. J Virol. 2020, 95, 10–128. [Google Scholar]
- Pretorius V, Wright CA, Hall DR, Schubert PT. Chronic villitis of unknown aetiology: Association with adverse pregnancy outcomes in a high-risk population in South Africa. In Obstetrics and Gynaecology Forum. 2019, 29, 7–12. [Google Scholar]
- Haseeb A, Khattak AA, Hayat A, ur Rehman M, Bano SA, Ahmed B, Khan I, Rehman A, Ullah R. and Barki S. Seroprevalence of ToRCH in Aborted versus non-aborted Women. J Infect. 2011, 63, 200–206.
- Turbadkar D, Mathur M. and Pele M. Seroprevelance of ToRCH infection in bad obstetric history. Indian J Med Microbiol. 2003, 21, 108–110. [Google Scholar]
- Irina T, Valeriu D. The role of ToRCH infection in early miscarriage. morphological study. German international journal of science. 2023, 1, 58–62. [Google Scholar]
- Mahmoud AM, Hagag HM, Ismail KA, Alharthi AM, Altalhi AA, Jaafer NF, Alharthi HH, Elwethenani AA, Khan KH, Al-ajmani SH, et al. Prevalence of Infectious Agents Causing Abortion in Pregnant Women Using Serological Tests and Histopathological Analysis. Appl Microbiol. 2023, 3, 698–708. [Google Scholar] [CrossRef]
- Dimitriadis E, Menkhorst E, Saito S, Kutteh WH, Brosens JJ. Recurrent pregnancy loss. Nat. Rev. Dis. Prim. 2020, 6, 98. [Google Scholar] [CrossRef]
Figure 1.
Normal villi showing cytotrophoblast, synscitiotrophoblasts, extraembryonic mesoderm and fetal vessels (10x).
Figure 1.
Normal villi showing cytotrophoblast, synscitiotrophoblasts, extraembryonic mesoderm and fetal vessels (10x).
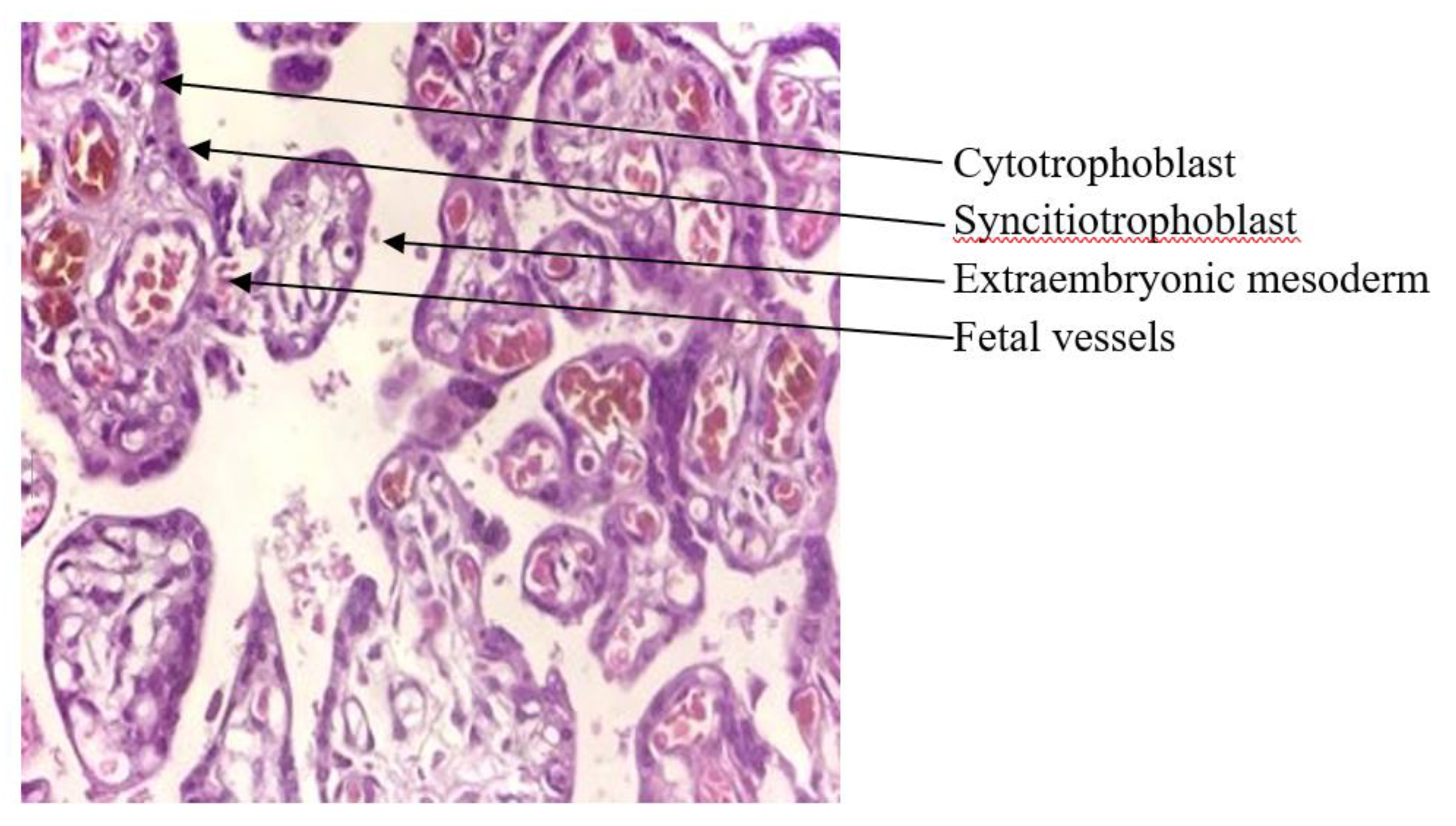
Figure 2.
Acute villitis and intervillitis. (a) Neutrophilic infiltrates in the villi (acute villitis, arrows). (b) Intervillositis with micro abscesses (arrows).
Figure 2.
Acute villitis and intervillitis. (a) Neutrophilic infiltrates in the villi (acute villitis, arrows). (b) Intervillositis with micro abscesses (arrows).
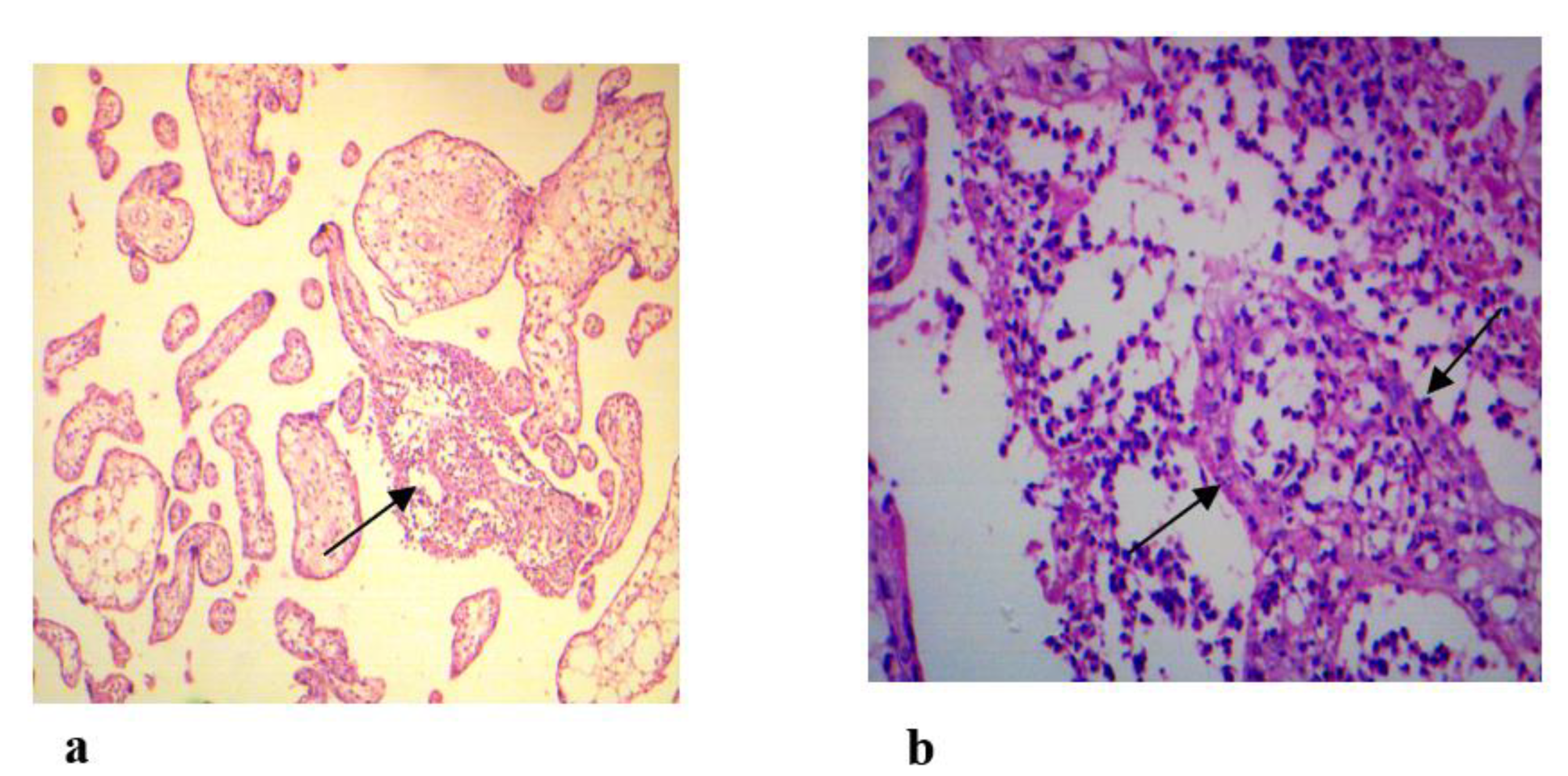

Table 1.
Demographics of the Study Population (N = 68).
| Variables | Group A n (%) |
Group B n (%) |
|
|---|---|---|---|
|
Age Groups (Years) |
G-I = 18-27 | 13 (19.11) | 9 (13.23) |
| G-II = 28-37 | 24 (35.29) | 10 (14.70) | |
| G-III = 38-47 | 6 (8.82) | 6 (8.82) | |
| Trimesters | 1st | 18 (41.86) | - |
| 2nd | 19 (44.18) | - | |
| 3rd | 6 (13.95) | - | |
|
Antibodies (Positivity) |
IgM | 11 (16.17) | 1 (1.47) |
| IgG | 10 (14.70) | 21 (30.88) | |
| IgM and IgG | 1 (1.47) | - | |
| NA | Positive | 26 (38.23) | 19 (27.94) |
| BOH Complications | RSAs | 23 (33.82) | 9 (13.23) |
| Stillbirth | 8 (11.76) | 7 (10.29) | |
| IUGR | 2 (2.94) | - | |
| Neonatal death | 4 (5.88) | 5 (7.35) | |
| CA | 6 (8.82) | 4 (5.88) | |
Table 2.
Frequency of ToRCH Antibodies and NA Positivity.
| Groups (n) |
T.gondii | RV | CMV | HSV | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| IgM n (%) |
IgG n (%) |
NA n (%) |
IgM n (%) |
IgG n (%) |
NA n (%) |
IgM n (%) |
IgG n (%) |
NA n (%) |
IgG n (%) |
NA n (%) |
|
|
Group A (43) |
2 (4.65) | 4 (9.30) | 6 (13.95) | 6 (13.95) | 3 (6.97) | 8 (18.6) | 3 (6.97) | 1 (2.32) | 6 (13.95) | 2 (4.65) | 6 (13.95) |
|
Group B (25) |
- | 10 (40) | 3 (12) | 1 (4) | 6 (24) | 4 (16) | - | 3 (12) | 6 (24) | 2 (8) | 6 (24) |
| Total (68) | 2 (2.94) | 14 (20.6) | 9 (13.23) | 7 (10.29) | 9 (13.23) | 12 (17.64) | 3 (4.41) | 4 (5.88) | 12 (17.64) | 4 (5.88) | 12 (17.64) |
|
p-value |
0.062 | 0.088 | 0.113 | 1.000 | |||||||
Note: One case in Group A was positive for both T.gondii IgM and IgG.
Table 3.
Discrepancies of ToRCH in Different Categories.
| Category |
T. gondii n (%) |
RV n (%) |
CMV n (%) |
HSV n (%) |
Total n (%) |
|---|---|---|---|---|---|
| Cat-I | 1 (1.47) | - | - | - | 1 (1.47) |
| Cat-II | 2 (2.94) | 4 (5.88) | 3 (4.41) | - | 9 (13.23) |
| Cat-III | - | 3 (4.41) | - | - | 3 (4.41) |
| Cat-IV | 7 (10.29) | 3 (4.41) | - | - | 10 (14.70) |
| Cat-V | 6 (8.82) | 6 (8.82) | 4 (5.88) | 4 (5.88) | 20 (29.41) |
| Cat-VI | 1 (1.47) | 2 (2.94) | 5 (7.35) | 8 (11.76) | 16 (23.52) |
| Total | 17 (25) | 18 (26.47) | 12 (17.64) | 12 (17.64) | 59 86.76) |
Table 4.
Histopathological Changes in Placental Tissues of ToRCH Positive Women.
| Groups (n) |
T.gondii | RV | CMV | HSV | ||||
|---|---|---|---|---|---|---|---|---|
| Ab/CV | NA/CV | Ab/CV | NA/CV | Ab/CV | NA/CV | Ab/CV | NA/CV | |
|
Group A (43) |
6/3 | 6/2 | 9/3 | 8/4 | 4/2 | 6/2 | 2/1 | 6/1 |
|
Group B (25) |
10/1 | 3/1 | 7/2 | 4/2 | 3/0 | 6/1 | 2/2 | 6/1 |
| Total = 68 | 16/4 | 9/3 | 16/5 | 12/6 | 7 /2 | 12/3 | 4/3 | 12/2 |
Note: Ab = Antibodies.
Table 5.
Correlation of CV with BOH complications.
| BOH complications (n) |
Group A n (%) |
Group B n (%) |
Total n (%) |
|---|---|---|---|
| RSAs (32) | 4 (12.5) | 3 (9.37) | 7 (21.87) |
| Stillbirths (15) | 1 (6.66) | 1 (6.66) | 2 (13.33) |
| IUGR (2) | 1 (50) | - | 1 (50) |
| Neonatal deaths (9) | 2 (22.2) | 1 (11.1) | 3 (33.3) |
| CA (10) | 1 (10) | - | 1 (10) |
| p-value | 0.826 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



