
Submitted:
13 May 2024
Posted:
14 May 2024
You are already at the latest version
Abstract
Chronic exposure to the nephrotoxic metal pollutant, cadmium (Cd), has been associated with hypertension, but the mechanism by which it raises blood pressure is not understood. We hypothesize that exposure to Cd reduces the glomerular filtration rate (GFR), which in turn, causes a rise in blood pressure. Data were collected from 447 Thai subjects with a mean age of 51.1 years, of which 48.8% had hypertension, 15.4% had diabetes and 6.9% had an estimated GFR (eGFR) below 60 mL/min/1.73 m2 (low eGFR). The mean blood and urinary Cd concentrations were 2.75 and 4.23 µg/L, respectively. The prevalence odds ratio (POR) for hypertension rose twofold in those with blood Cd levels of 0.61-1.69 µg/L or urinary Cd excretion levels ≥ 0.98 µg/g creatinine. In the hypertensive group, the eGFR was inversely associated with age (β =−0.517), the Cd excretion rate (β = −0.177), and diabetes (β = −0.175). Mean eGFR in the normotensive group was 7.5 mL/min/1.73 m2 higher than the hypertensive with a similar Cd body burden. Mean systolic blood pressure (SBP) in those with low or medium eGFR plus heavy Cd body burden was 9.5 mmHg higher than those with the same Cd body burden and a normal eGFR. By mediation analysis, a 22.7% increase in SBP and a 5% increase in diastolic blood pressure (DBP) were attributable to the effect of Cd on GFR. Thus, a rise of blood pressure appears to be a consequence of GFR loss due to Cd-induced kidney damage. This finding is consistent with a well-known role of the kidney in long-term blood pressure regulation.
Keywords:
blood pressure
; cadmium
; glomerular filtration rate
; hypertension
; kidneys
; mediation analysis
1. Introduction
Hypertension, indicated by systolic blood pressure (SBP) ≥ 140 mmHg or diastolic blood pressure (DBP) ≥ 90 mmHg, is a common risk factor for cardiovascular disease (CVD) and can be both a cause and a consequence of chronic kidney disease (CKD) [1,2]. Similarly, because of its ubiquitous environmental presence, exposure to the nephrotoxic metal pollutant cadmium (Cd) is also a significant risk factor for CVD [3] and CKD [4].
In a dose-response meta-analysis, Verzelloni et al. (2024) found that the risks of heart failure, coronary heart disease, and stroke were all increased with Cd exposure in a dose-dependent manner. The risk of having CVD rose 2.58-fold and 2.79-fold at blood Cd level of 1 μg/L and urinary Cd excretion rate of 0.5 μg/g creatinine, respectively. Furthermore, a 1.76-fold increase in death from CVD among U.S. citizens with hypertension was associated with elevated Cd exposure, indicated by blood Cd levels ≥ 0.80 μg/L [5]. At the same Cd exposure level, the risk of death from CVD rose 2.12-fold among non-smokers who have hypertension [5]. A 49% increase in all-cause mortality among the diabetics was associated with urinary Cd levels > 0.60 μg/L [6]. A 75% increase in deaths from any cause among those with CKD was associated with urinary Cd levels ≥ 0.60 μg/g creatinine [7].
Effects of environmental exposure to Cd on blood pressure has been well documented in studies of the general populations in the U.S. [8,9,10], Canada [11], China [12,13,14], Korea [15,16], and Japan [17]. A cross-sectional study of U.S. population found there was an increased risk of hypertension due to Cd in non-smoking women [8], while a prospective cohort study of American Indians has implicated Cd exposure as a causative factor in blood pressure increment and hypertension [10].
For non-occupationally exposed populations, diet is the main source of Cd exposure other than passive and active smoking [18,19,20,21]. The intestinal absorption rate of Cd can be as high as 45% [22,23] as Cd can be absorbed through several metal transporters for metal nutrients, iron, zinc, copper and calcium (Fe, Zn, Cu and Ca) [24,25]. Furthermore, Cd complexed with metallothionein (MT) and phytochelatin (PC), can be absorbed through transcytosis as well as receptor-mediated endocytosis [26,27,28]. Notably, however, there are no physiologic mechanisms for Cd elimination. Continued exposure will consequently lead to its accumulation in tissues and organs throughout the body, notably kidneys.
The kidneys play an indispensable role in long-term blood pressure regulation [2], and the principal site of Cd toxicity due to a preferential accumulation of Cd in the proximal tubular epithelium [29,30]. As these cells die, Cd complexed with MT (CdMT) is released into tubular lumen and excreted in urine [31]. Because most or all excreted Cd originates from injured or dying kidney tubular epithelial cells, the excretion of Cd itself indicates the severity of the kidney injury due to Cd accumulation at the present time [31]. A correlation between kidney accumulation and urinary Cd concentration forms the basis for urinary Cd as an indicator of long-term exposure to Cd or its body burden [32].
A few studies have explored the mechanism by which Cd accumulation in the kidney raised blood pressure. The present study aimed to test the hypothesis that an increase in blood pressure is the result of a declining GFR due to kidney damage from toxic Cd accumulation. Thus, we quantified changes in eGFR, systolic and diastolic blood pressures (SBP and DBP) according to Cd exposure levels, indicated by excretion of Cd (ECd) and blood Cd concentrations ([Cd]b) in those diagnosed with and without hypertension. A declining eGFR, is a common sequela of ischemic acute tubular necrosis, acute and chronic tubulointerstitial fibrosis, all of which create impediments to filtration [33,34].
2. Results
2.1. Demorphraphic and Biologic Characteristics of Participants
A total of 447 persons (333 women and 114 men) with a mean age of 51.1 years, were recruited to this study (Table 1).
Overall mean [Cd]u and [Cd]b values were 4.23 and 2.75 µg/L, respectively. Participants were grouped by the tertile of the Cd excretion rate [(ECd/Ccr) ×100]. Corresponding mean (ECd/Ccr) ×100 values in the low, middle and high tertile groups were 0.38, 2.28 and 6.89 µg/L filtrate, equivalent to ECd/Ecr of 0.48, 3.07 and 8.48 µg/g creatinine. Mean blood Cd concentration [Cd]b values in the low, middle and high tertiles of Cd burden were 0.72, 2.37 and 5.14 µg/L, respectively.
[Cd]u and [Cd]b correlated strongly with each other in both women and men with respective Pearson’s correlation coefficients of 0.688 and 0.615. After controlling for age, [Cd]u and [Cd]b correlations remained with partial r values of 0.584 and 0.658 in women and men, respectively.
The percentages (%) of smoking in the top (42.7%) and middle (34.9%) ECd/Ccr tertile groups were higher than the low (16.2%) tertile group. The % hypertension were similar across ECd/Ccr tertiles, but diabetes was more prevalent in the low tertile (39.2%) compared with the middle (3.4%) and high (4.0%) tertile groups. In parallel, low eGFR was more prevalent in the low tertile (10.3%) than in the middle (1.3%) and top (8.7%) tertiles.
Mean age (56.6 years), mean BMI (25.5 kg/m2), mean SBP (134 mmHg) and mean DBP (83 mmHg) in the low tertile group were all statistically higher than the middle and top ECd/Ccr tertile groups. The mean eGFR of 84 mL/min/1.73m2 in the low tertile was 7-12 mL/min/1.73 m2 below the mean eGFR values in the middle and top tertiles.
2.2. Hypertension Prevalence in Relation to Cd Burden
In logistic regression analysis, six independent variables incorporated in a regression model were age, BMI, gender, smoking, diabetes, and Cd burden which was described as, mild, moderate, and heavy (Table 2).
The prevalence odds ratio (POR) for hypertension was associated with two variables, namely BMI (POR 1.082, 95% CI:1.027-1.140) and a medium Cd burden (POR 2.114, 95% CI: 1.049-4.260). An increase in POR for hypertension was statistically insignificantly in the heavy Cd burden group (p = 0.092).
Table 3 provides results from an analogous logistic regression analysis, where [Cd]b was used as a Cd exposure indicator.
POR for hypertension was again associated with the increment of BMI and Cd exposure levels. POR for hypertension rose to 1.083 (95% CI: 1.029-1.140) per every 1 kg/m2 increase in BMI. Compared with [Cd]b < 0.60 µg/L, the POR for hypertension were increased to 2.113 (95% CI: 1.191-3.749) and 1.833 (95% CI: 1.000-3.360) in those with [Cd]b of 0.61-1.69, and 1.70-3.38 µg/L, respectively. An increment of the POR for hypertension in those with the top [Cd]b quartile ([Cd]b > 6.92 µg/L) was not statistically significant (p = 0.082).
2.3. Cd-Induced eGFR Reduction
Scatterplots that related eGFR to the excretion rate of Cd are presented in Figure 1.
A significant inverse dose-response relationship was observed between eGFR and ECd/Ccr in women (β = −0.167) and men (β −0.322) with medium plus heavy Cd burdens (Figure 1b), but not in those with a mild Cd burden (Figure 1a).
Similarly, lower eGFR values were associated with higher ECd/Ccr values in those with normotension (β = −0.034) and hypertension (β = −0.070) with the medium plus heavy Cd burdens (Figure 1d). In comparison, eGFR and ECd/Ccr were not corelated with each other in the groups with a mild Cd burden, regardless of blood pressure status (Figure 1c).
In an additional covariance analysis, it was apparent that Cd may have decreased eGFR, when (ECd/Ccr)×100 rose above 1 µg/L filtrate (Figure 2).
In the group with a mild Cd burden, covariate-adjusted mean eGFR values did not differ in any pairs of subgroups based on gender, smoking status, and diabetes (Figure 2a). A covariate-adjusted mean eGFR in the hypertensive with medium plus heavy Cd burdens, was 7.5 mL/min/1.73m2 lower (p = 0.038), compared with the normotensive who had the same overall Cd burden (Figure 2b). Furthermore, a covariate-adjusted mean eGFR in those with heavy Cd burden was 10.7 mL/min/1.73m2 lower, compared with the medium Cd burden group (p = 0.003) (Figure 2b).
In a multiple regression of eGFR, age, BMI, log2[(ECd/Ccr) ×105], gender, hypertension, smoking, and diabetes contributed, respectively to 27.9%, 24.8%, 31.8% and 24.2% the variation in eGFR in women, men, the normotensive and hypertensive groups (Table 4).
In women, lower eGFR values were associated with older age (β =−0.528) higher ECd/Ccr (β = −0.121), and diabetes (β = −0.133). In men, lower eGFR values were associated with older age (β =−0.505) and hypertension (β =−0.203). In the normotensive group, eGFR was inversely associated with age (β =−0.559) while showing a positive association with smoking. In the hypertensive group, eGFR was inversely associated with age (β =−0.517), ECd/Ccr (β = −0.177), and diabetes (β = −0.175).
2.4. Inverse Relationships between Blood Pressure and eGFR
Scatterplots relating blood pressure measurements to eGFR can be found in Figure 3.
A significant inverse dose-response relationship was observed between SBP and eGFR in women (β = −0.227) and men (β −0.320) of the medium plus heavy Cd burden group (Figure 3b), but not a mild Cd burden group (Figure 3a). In comparison, DBP did correlate with eGFR in women or men in any Cd burden groups (Figure 3c,d).
In a covariance analysis, an increased mean SBP appeared to be related to Cd burden, eGFR, and diabetes (Figure 4).
Mean SBP in the group medium plus heavy Cd burdens with low eGFR was 9.5 mmHg higher than the group with the sane Cd burdens, but had normal eGFR (Figure 3b). At the mild Cd burden level, mean SBP in those with low and normal eGFR did not differ, but the mean SBP in diabetics was 7.4 mmHg higher than those without diabetes (Figure 3a). At the medium plus high Cd burden, mean SBP in those with diabetes was increased further to 18.4 mmHg higher than those without diabetes (Figure 3b).
Mean DBP values among subgroups did not appear to be affected by Cd burden or eGFR groups, but the covariate adjusted mean DBP in diabetics with medium plus high Cd burden was 9.5 mmHg higher, compared with those without diabetes.
2.5. Regression Analysis of Blood Pressure Increment
In a multiple linear regression analysis, age, BMI, log2[(ECd/Ccr)×105], eGFR, gender, hypertension, smoking, and diabetes were independent variables (Table 5)
Age, BMI, log2[(ECd/Ccr)×105], eGFR, gender, hypertension, smoking, and diabetes together contributed, respectively to 19.9%, 15.7%, and 15.0% of the variation in SBP in all subjects, the mild Cd burden, and medium plus heavy Cd burden groups. The fractional DBP variation explained by these independent variables in the mild Cd burden, and medium plus heavy Cd burden groups were 4.6%, 0% and 5.8%, respectively.
In an inclusive analysis, higher SBP values were associated with older age (β = 0.243), higher BMI (β = 0.113), lower eGFR (β = −0.106) and diabetes (β = 0.216). In the mild Cd burden group, SBP showed positive associations with BMI (β = 0.395) and diabetes (β = 0.202). In the medium plus high Cd burden group, SBP showed a significant association with diabetes (β = 0.265), while showing an inverse association with eGFR (β = −0.176).
In an equivalent inclusive analysis, higher DBP values were associated only with higher BMI values (β = 0.123). In the medium plus high Cd burden group only, higher DBP values were associated with higher BMI (β = 0.123), lower eGFR (β = −0.130), and diabetes (β = 0.193).
2.6. Mediation Analysis
We employed mediation analysis to explore if Cd increases blood pressure through its effect on GFR. In this analysis, eGFR was a single mediator, while ECd/Ccr was an independent variable, and SBP or DBP was as dependent variable (Figure 5).
As “a” and “c” values indicated, Cd had a direct effect on eGFR and SBP, but not DBP. In comparison, “b” values in models 1 and 2 indicated there were significant inverse relationships between eGFR with SBP and DBP. The products of regression coefficients “a*b” indicated that respective 22.7% and 5% of the effects of Cd on SBP and DBP were mediated by a fall of eGFR.
3. Discussion
Among 447 study subjects, nearly half (48.8%) had hypertension, while 15.4% and 6.9% had diabetes and low eGFR, respectively. The prevalence of low eGFR in our study was in line with a 6.3% found in a study from Taiwan [37]. However, the % of hypertension and diabetes in the present study were higher than those recorded in studies from U.S. where % hypertension and diabetes were 39% and 10.3%-13%, respectively [38,39]. Mean Cd excretion rate was 0.003 µg/L filtrate, corresponding to 4.03 µg/g creatinine. The mean blood and urinary Cd concentrations were 2.75 and 4.23 µg/L, respectively.
Previously, an effect of smoking on the risk of CVD has been found to be partially mediated by Cd [40,41]. Therefore, it was crucial to adjust for the potential confounding effects of smoking and diabetes on blood pressure increases. Enough numbers of smokers, hypertensive, and diabetic cases were the strength of our study because they enabled adjustment for confounding risk factors. The limitations of the present study include a one-time assessment of Cd exposure and its effects.
An increased risk of hypertension was associated with both urinary and blood Cd levels (Table 2 and Table 3). POR for hypertension rose two-fold in the medium burden group and those with the blood Cd quartiles 2 and 3. However, the increases in POR for hypertension in those with heavy burden of Cd (POR 1.66) and those with the top blood Cd quartile (POR 1.80) were not statistically significant. Thus, Cd effects on blood pressure appeared to be particularly strong in low-dose exposure conditions.
In a Chinese case-control study, a 1.33-fold increase in the risk of hypertension was associated with urinary Cd levels > 1.07 μg/L [13]. In the present study, a two-fold rise in POR for hypertension was observed in the medium burden group with urinary Cd levels > 0.57 µg/L (Table 2). A 2.6-fold increase in risk of hypertension was seen in white and Mexican-American women who had blood Cd levels ≥ 0.4 µg/L [8]. In the present study, an increase in POR for hypertension was found in those who had blood Cd of 0.61−3.38 µg/L (Table 3).
In a study from Korea, increases in prevalence of pre-hypertension and hypertension were associated with doubling blood Cd from 0.62 to 1.33 µg/L in men, and from 0.73 to 1.57 µg/L in women [15]. In a study of residents in a Cd-polluted area of China, increased risk of hypertension was associated with blood Cd of 1–1.7 µg/L [12].
In a Canadian study, SBP and DBP were positively associated with blood Cd, but the risk of hypertension fell 52% in women who were current smokers [11]. A similar observation was made in a U.S. population study, where associations between blood pressure measurements and blood Cd were particularly strong in non-smokers, moderate in former smokers, and weak or negligible in current smokers [8].
The urinary and blood Cd levels found to be associated with a significant increase in risk of hypertension varied among populations. This may be due to different susceptibility to hypertension or some protective factors. For instance, white and Mexican-American women were found to be more susceptible to an effect of Cd on blood pressure than black women; an increased risk of hypertension was seen in Caucasian (OR 1.54) and Mexican-American women (OR 2.38) who had blood Cd as little as 0.4 µg/L, but not in black women or white, black, or Mexican-American men [9].
Similarly, a female preponderance effect of Cd on blood pressure was also evident from data in Table 4, where an inverse association of eGFR and Cd burden was found only in women (β = −0.121). In men, eGFR did not show a significant association with Cd exposure (β = −0.077), but hypertension (β =−0.203). In a Taiwanese study, an association of urinary Cd and a marker of tubular damage, N-acetyl-β-D-glucosaminidase (NAG), was observed in women only [42].
Independent effects of Cd and hypertension on eGFR were found only those with medium and heavy Cd burdens (Figure 2). The hypertensive with medium plus heavy Cd burdens had mean eGFR 7.5 mL/min/1.73 m2 lower, compared with the normotensive who had the same overall Cd burden (p = 0.038) (Figure 2b). Similarly, those with a medium Cd burden had mean eGFR 10.7 mL/min/1.73m2 lower than those with heavy Cd burden (p = 0.003).
Independent effects of Cd and diabetes on SBP and DBP were revealed in a covariance analysis (Figure 3). The mean SBP in diabetics with low Cd burden was 7.4 mmHg higher than those without diabetes with the same low Cd burden (Figure 3a). In comparison, mean SBP in diabetics who had medium plus heavy Cd burdens was 18.4 mmHg higher than those without diabetes (Figure 3b). Unlike SBP, a significant rise in DBP was found only in the diabetic group with medium plus heavy Cd burdens (Figure 4d).
To the best of our knowledge, the present study has provided, for the first time, evidence linking Cd-induced eGFR reduction to a rise in blood pressure, especially SBP (Figure 3). SBP was inversely associated with eGFR in women (β = −0.227) and men (β = −0.320) who had medium plus heavy Cd burdens. Like SBP, DBP showed an inverse association with eGFR, but such association was weak and statistically insignificant (Figure 3a,b vs. Figure 3c,d). A covariance analysis confirmed an inverse relationship between SBP and eGFR (Figure 4). Subjects with medium plus heavy Cd burdens and low eGFR had mean SBP 9.5 mmHg higher than those with a normal eGFR and the same overall Cd burden (Figure 3b). The mediation analysis confirmed that GFR reduction was a partial mediator of Cd effect on blood pressure increases (Figure 5).
In summary, we have shown that increases in blood pressure may be a consequence of a decrease in GFR induced by Cd. The indispensable role of kidney in long-term blood pressure regulation is well established [1]; as its function is declining (indicated by low eGFR), less water and sodium would be eliminated by the kidney, which may increase blood pressure. Rats with Cd-induced hypertension showed increased sodium retention and reduced sodium excretion [43,44,45]. Thus, increased tubular avidity for filtered sodium appeared to be a possible mechanism by which lifelong, low-dose Cd intake causes hypertension.
4. Materials and Methods
4.1. Participants
Participants were recruited from Nakhon Si Thammarat Province in the south and Mae Sot District in the northwest of Thailand [46,47]. All subjects were provided with details of study objectives, study procedures, benefits, and potential risks, and they all provided written informed consent. The Office of the Human Research Ethics Committee of Walailak University approved the study protocol for the Nakhon Si Thammarat group [46]. The study protocol for the Mae Sot group was approved by the Institutional Ethical Committees of Chiang Mai University and the Mae Sot Hospital [47].
Levels of various contaminants, including arsenic, chromium, lead and Cd in samples of soils and food crops in Nakhon Si Thammarat were within permissible ranges [48], and no association was found between water arsenic concentration and the risk of diabetes [48,49]. In comparison, the Cd concentration of the paddy soil samples from the Mae Sot district exceeded the standard of 0.15 mg/kg, and the rice samples collected from household storage contained four times the amount of the permissible Cd level of 0.1 mg/kg [50]. In a health survey of residents (n = 5273) of Mae Sot District, urinary CD excretion levels correlated with hypertension and diabetes [51].
4.2. Blood Pressure and Cadmium Exposure Ascertainment
The diagnosis of hypertension was based on questionnaires, a physician’s diagnosis or use of antihypertensive medication, and ascertained by a single measurement of systolic and diastolic blood pressures (SBP and DBP). Cd exposure was based on urinary Cd excretion (ECd) and blood Cd concentration ([Cd]b). Simultaneous urine and whole blood sampling were undertaken after overnight fast. Aliquots of blood and urine samples were stored at −80 °C for later analysis.
Atomic absorption spectrophotometry was used to determine urinary and blood levels of [Cd]u and [Cd]b using multielement standards (Merck KGaA, Darmstadt, Germany) for instrument calibration. For quality control and assurance purposes, blood and urine samples from subjects, blood control samples (ClinChek, Munich, Germany) and the reference urine metal controls (Lyphocheck, Bio-Rad, Hercules, CA, USA) were simultaneously analyzed.
The limit of detection (LOD) for Cd in blood or urine was 0.3 µg/L for [Cd]b and 0.1 µg/L for [Cd]u. The Cd concentration assigned to a sample that contained Cd below its LOD was assigned a value of the LOD divided by the square root of 2 [52].
4.3. Normalization of Cadmium Excretion Rate
ECd was normalized to creatinine clearance (Ccr) as ECd/Ccr = [Cd]u[cr]p/[cr]u, where [Cd]u = urine concentration of Cd (mass/volume); [cr]p = plasma creatinine concentration (mg/dL) and [cr]u = urine creatinine concentration (mg/dL). ECd/Ccr was expressed as an amount of Cd excreted per volume of the glomerular filtrate. Ccr-normalization corrects for urine dilution and functioning nephrons.
ECd was normalized to Ecr as [Cd]u/[cr]u, where [Cd]u = urine concentration of Cd (mass/volume) and [cr]u = urine creatinine concentration (mg/dL). ECd/Ecr was expressed in μg/g creatinine. Ecr-normalization corrects for urine dilution, but it is influenced by muscle mass. The effect of Cd exposure on GFR was obscure, when ECd was normalized to Ecr [53].
4.4. Estimated Glomerular Filtration Rate (eGFR)
We used the GFR estimating equations, established by the chronic kidney disease epidemiology collaboration (CKD-EPI) to compute the estimated GFR (eGFR) [35]. The CKD-EPI equations have been validated with inulin clearance [54].
Male eGFR = 141 × [cr]p/0.9Y × 0.993age, where Y = −0.411 if [cr]p ≤ 0.9 mg/dL and Y = −1.209 if [cr]p > 0.9 mg/dL.
Female eGFR = 144 × [cr]p/0.7Y × 0.993age, where Y = −0.329 if [cr]p ≤ 0.7 mg/dL and Y = −1.209 if [cr]p > 0.7 mg/dL.
4.5. Statistical Analysis
Data were analyzed with IBM SPSS Statistics 21 (IBM Inc., New York, NY, USA). The Kruskal-Wallis test was used to assess differences in means across tertiles of Cd burden, and the Pearson chi-squared test was used to assess differences in percentages. Distribution of continuous variables was assessed by the one-sample Kolmogorov–Smirnov test. A logarithmic transformation was applied to variables that showed rightward skewing. A simple mediation model with a single mediator was used in the mediation analysis [55,56].
Prevalence Odds Ratio (POR) for hypertension, which was defined SBP ≥ 140 mmHg or DBP ≥ 90 mmHg [1] was determined by logistic regression. Multiple linear regression was used to identify variables affecting eGFR, SBP, and DBP. Mean eGFR, mean SBP and mean DBP were adjusted for covariates and interactions using univariate analysis with Bonferroni correction. For all tests, p-values ≤ 0.05 were considered as statistical significance.
5. Conclusions
By mediation analysis, a 22.7% increase in SBP and a 5% increase in DBP were attributable to Cd-induced loss of GFR. Thus, Cd raised SBP more markedly than DBP. A two-fold increased risk of hypertension was associated with urinary Cd excretion of 0.98 µg/g creatinine and a blood Cd level of 0.61 µg/L. As these are levels that are reported widely in studies of non-occupationally exposed populations from across the world, it is imperative that authorities closely monitor the environmental levels of Cd, especially in staple foods.
Author Contributions
Conceptualization, S.S.; D.A.V. and A.B.Đ.; methodology, S.Y.; T.K. and P.P.; formal analysis, S.S. and A.B.Đ; investigation, S.S; S.Y.; T.K. and P.P.; resources, D.A.V.; S.Y. and A.B.Đ.; data curation, S.S. and S.Y.; writing—original draft preparation, S.S.; writing—review and editing, S.S.; D.A.V. and A.B.Đ.; project administration, S.S. and S.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This is not applicable for the present study, which used archived data.
Informed Consent Statement
Written informed consent has been obtained from study subjects.
Data Availability Statement
All data are contained within this article.
Acknowledgments
This work was supported with resources from the Centre for Kidney Disease Research, Translational Research Institute, the Department of Kidney and Transplant Services, Princess Alexandra Hospital, the Department of Toxicology, Faculty of Pharmacy, University of Belgrade, Serbia.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bloch, M.J.; Basile, J.N. Review of recent literature in hypertension: Updated clinical practice guidelines for chronic kidney disease now include albuminuria in the classification system. J. Clin. Hypertens. 2013, 15, 865–867. [Google Scholar] [CrossRef] [PubMed]
- Crowley, S.D.; Coffman, T.M. The inextricable role of the kidney in hypertension. J. Clin. Investig. 2014, 124, 2341–2347. [Google Scholar]
- Verzelloni, P.; Urbano, T.; Wise, L.A.; Vinceti, M.; Filippini, T. Cadmium exposure and cardiovascular disease risk: A systematic review and dose-response meta-analysis. Environ. Pollut. 2024, 345, 123462. [Google Scholar] [CrossRef] [PubMed]
- Doccioli, C.; Sera, F.; Francavilla, A.; Cupisti, A.; Biggeri, A. Association of cadmium environmental exposure with chronic kidney disease: A systematic review and meta-analysis. Sci. Total Environ. 2024, 906, 167165. [Google Scholar] [CrossRef]
- Chen, S.; Shen, R.; Shen, J.; Lyu, L.; Wei, T. Association of blood cadmium with all-cause and cause-specific mortality in patients with hypertension. Front. Public Health 2023, 11, 1106732. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, D.; Shi, F.; Wang, F.; Liu, X.; Wen, H.; Mubarik, S.; Yu, C. Association of serum 25(OH)D, cadmium, CRP with all-cause, cause-specific mortality: A prospective cohort study. Front. Nutr. 2022, 9, 803985. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, X.; Ma, Z.; Dang, Y.; Yang, Y.; Cao, S.; Ouyang, C.; Shi, X.; Pan, J.; Hu, X. Associations of urinary and blood cadmium concentrations with all-cause mortality in US adults with chronic kidney disease: A prospective cohort study. Environ. Sci. Pollut. Res. Int. 2023, 30, 61659–61671. [Google Scholar] [CrossRef] [PubMed]
- Tellez-Plaza, M.; Navas-Acien, A.; Crainiceanu, C.M.; Guallar, E. Cadmium exposure and hypertension in the 1999-2004 National Health and Nutrition Examination Survey (NHANES). Environ. Health Perspect. 2008, 116, 51–56. [Google Scholar] [CrossRef]
- Scinicariello, F.; Abadin, H.G.; Murray, H.E. Association of low-level blood lead and blood pressure in NHANES 1999-2006. Environ. Res. 2011, 111, 1249–1257. [Google Scholar] [CrossRef]
- Oliver-Williams, C.; Howard, A.G.; Navas-Acien, A.; Howard, B.V.; Tellez-Plaza, M.; Franceschini, N. Cadmium body burden, hypertension, and changes in blood pressure over time: Results from a prospective cohort study in American Indians. J. Am. Soc. Hypertens. 2018, 12, 426–437.e9. [Google Scholar] [CrossRef]
- Garner, R.E.; Levallois, P. Associations between cadmium levels in blood and urine, blood pressure and hypertension among Canadian adults. Environ. Res. 2017, 155, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, Z.; Zhu, G.; Liang, Y.; Jin, T. Benchmark dose estimation of cadmium reference level for hypertension in a Chinese population. Environ. Toxicol. Pharmacol. 2015, 39, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Liu, D.; Jiang, S.; Zhang, K.; Zhou, H.; Lu, Q. Polymorphisms in gene MMP-2 modify the association of cadmium exposure with hypertension risk. Environ. Int. 2019, 124, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.; Wu, H.B.; Niu, Q.S.; Jia, P.P.; Qin, Q.R.; Wang, X.D.; He, J.L.; Yang, W.J.; Huang, F. Exposure to multiple metals and the risk of hypertension in adults: A prospective cohort study in a local area on the Yangtze River, China. Environ. Int. 2021, 153, 106538. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.K.; Kim, Y. Association of blood cadmium with hypertension in the Korean general population: Analysis of the 2008–2010 Korean National Health and Nutrition Examination Survey data. Am. J. Ind. Med. 2012, 55, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.A.; Park, E.; Kim, S.; Kim, B. Influence of serum ferritin combined with blood cadmium concentrations on blood pressure and hypertension: From the Korean National Health and Nutrition Examination Survey. Chemosphere 2022, 288, 132469. [Google Scholar] [CrossRef] [PubMed]
- Kaneda, M.; Wai, K.M.; Kanda, A.; Ando, M.; Murashita, K.; Nakaji, S.; Ihara, K. Low level of serum cadmium in relation to blood pressures among Japanese general population. Biol. Trace Element Res. 2021, 200, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Kataoka, Y.; Hayashi, K.; Matsuda, R.; Uneyama, C. Dietary exposure of the Japanese general population to elements: Total diet study 2013–2018. Food Saf. 2022, 10, 83–101. [Google Scholar] [CrossRef]
- Almerud, P.; Zamaratskaia, G.; Lindroos, A.K.; Bjermo, H.; Andersson, E.M.; Lundh, T.; Ankarberg, E.H.; Lignell, S. Cadmium, total mercury, and lead in blood and associations with diet, sociodemographic factors, and smoking in Swedish adolescents. Environ. Res. 2021, 197, 110991. [Google Scholar] [CrossRef]
- Kim, J.; Song, H.; Lee, J.; Kim, Y.J.; Chung, H.S.; Yu, J.M.; Jang, G.; Park, R.; Chung, W.; Oh, C.M.; Moon, S. Smoking and passive smoking increases mortality through mediation effect of cadmium exposure in the United States. Sci. Rep. 2023, 13, 3878. [Google Scholar] [CrossRef]
- Hill, D.T.; Jandev, V.; Petroni, M.; Atallah-Yunes, N.; Bendinskas, K.; Brann, L.S.; Heffernan, K.; Larsen, D.A.; MacKenzie, J.A.; Palmer, C.D.; et al. Airborne levels of cadmium are correlated with urinary cadmium concentrations among young children living in the New York state city of Syracuse, USA. Environ. Res. 2023, 223, 115450. [Google Scholar] [CrossRef]
- Kikuchi, Y.; Nomiyama, T.; Kumagai, N.; Dekio, F.; Uemura, T.; Takebayashi, T.; Nishiwaki, Y.; Matsumoto, Y.; Sano, Y.; Hosoda, K.; et al. Uptake of cadmium in meals from the digestive tract of young non-smoking Japanese female volunteers. J. Occup. Health 2003, 45, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, H.; Oguma, E.; Sasaki, S.; Miyamoto, K.; Ikeda, Y.; Machida, M.; Kayama, F. Comprehensive study of the effects of age, iron deficiency, diabetes mellitus, and cadmium burden on dietary cadmium absorption in cadmium-exposed female Japanese farmers. Toxicol. Appl. Pharmacol. 2004, 196, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Phelps, K.R. Chapter 14: Cadmium Exposure and Toxicity. In Metal Toxicology Handbook; Bagchi, D., Bagchi, M., Eds.; CRC Press: Boca Raton, FL, USA, 2021; pp. 219–274. [Google Scholar]
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Phelps, K.R. Estimation of health risks associated with dietary cadmium exposure. Arch. Toxicol. 2023, 97, 329–358. [Google Scholar] [CrossRef]
- Fujita, Y.; el Belbasi, H.I.; Min, K.S.; Onosaka, S.; Okada, Y.; Matsumoto, Y.; Mutoh, N.; Tanaka, K. Fate of cadmium bound to phytochelatin in rats. Res. Commun. Chem. Pathol. Pharmacol. 1993, 82, 357–365. [Google Scholar] [PubMed]
- Langelueddecke, C.; Roussa, E.; Fenton, R.A.; Thévenod, F. Expression and function of the lipocalin-2 (24p3/NGAL) receptor in rodent and human intestinal epithelia. PLoS ONE 2013, 8, e71586. [Google Scholar] [CrossRef] [PubMed]
- Langelueddecke, C.; Lee, W.K.; Thévenod, F. Differential transcytosis and toxicity of the hNGAL receptor ligands cadmium-metallothionein and cadmium-phytochelatin in colon-like Caco-2 cells: Implications for in vivo cadmium toxicity. Toxicol. Lett. 2014, 226, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Baker, J.R.; Reilly, P.E.; Moore, M.R.; Williams, D.J. Cadmium levels in the lung, liver, kidney cortex, and urine samples from Australians without occupational exposure to metals. Arch. Environ. Health 2002, 57, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Barregard, L.; Sallsten, G.; Lundh, T.; Mölne, J. Low-level exposure to lead, cadmium and mercury, and histopathological findings in kidney biopsies. Environ. Res. 2022, 211, 113119. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Ruangyuttikarn, W.; Nishijo, M.; Gobe, G.C.; Phelps, K.R. The source and pathophysiologic significance of excreted cadmium. Toxics 2019, 7, 55. [Google Scholar] [CrossRef]
- Akerstrom, M.; Barregard, L.; Lundh, T.; Sallsten, G. The relationship between cadmium in kidney and cadmium in urine and blood in an environmentally exposed population. Toxicol. Appl. Pharmacol. 2013, 268, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Gobe, G.C.; Vesey, D.A.; Phelps, K.R. Cadmium and lead exposure, nephrotoxicity, and mortality. Toxics 2020, 8, 86. [Google Scholar] [CrossRef]
- Lang, S.M.; Schiffl, H. Smoking status, cadmium, and chronic kidney disease. Renal Replacement Therapy 2024, 10, 17. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Scmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Phelps, K.R.; Gosmanova, E.O. A generic method for analysis of plasma concentrations. Clin. Nephrol. 2020, 94, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.J.; Hung, C.H.; Wang, C.W.; Tu, H.P.; Li, C.H.; Tsai, C.C.; Lin, W.Y.; Chen, S.C.; Kuo, C.H. Associations among heavy metals and proteinuria and chronic kidney disease. Diagnostics (Basel) 2021, 11, 282. [Google Scholar] [CrossRef] [PubMed]
- Shi, P.; Yan, H.; Fan, X.; Xi, S. A benchmark dose analysis for urinary cadmium and type 2 diabetes mellitus. Environ. Pollut. 2021, 273, 116519. [Google Scholar] [CrossRef]
- Lee, J.; Oh, S.; Kang, H.; Kim, S.; Lee, G.; Li, L.; Kim, C.T.; An, J.N.; Oh, Y.K.; Lim, C.S.; et al. Environment-Wide Association Study of CKD. Clin. J. Am. Soc. Nephrol. 2020, 15, 766–775. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Fagerberg, B.; Sallsten, G.; Borné, Y.; Hedblad, B.; Engström, G.; Barregard, L.; Andersson, E.M. Smoking-induced risk of future cardiovascular disease is partly mediated by cadmium in tobacco: Malmö Diet and Cancer Cohort Study. Environ. Health 2019, 18, 56. [Google Scholar] [CrossRef]
- Hecht, E.M.; Landy, D.C.; Ahn, S.; Hlaing, W.M.; Hennekens, C.H. Hypothesis: cadmium explains, in part, why smoking increases the risk of cardiovascular disease. J. Cardiovasc. Pharmacol. Ther. 2013, 18, 550–554. [Google Scholar] [CrossRef]
- Liao, K.W.; Chien, L.C.; Chen, Y.C.; Kao, H.C. Sex-specific differences in early renal impairment associated with arsenic, lead, and cadmium exposure among young adults in Taiwan. Environ. Sci. Pollut. Res. Int. 2022, 29, 52655–52664. [Google Scholar] [CrossRef] [PubMed]
- Perry, H.M.; Erlanger, M.; Perry, E.F. Increase in the systolic pressure of rats chronically fed cadmium. Environ. Health Perspect. 1979, 28, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Perry, H.M., Jr.; Erlanger, M.W. Sodium retention in rats with cadmium-induced hypertension. Sci. Total Environ. 1981, 22, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Peña, A.; Iturri, S.J. Cadmium as hypertensive agent. Effect on ion excretion in rats. Comp. Biochem. Physiol. C Comp. Pharmacol. Toxicol. 1993, 106, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Yimthiang, S.; Pouyfung, P.; Khamphaya, T.; Kuraeiad, S.; Wongrith, P.; Vesey, D.A.; Gobe, G.C.; Satarug, S. Effects of environmental exposure to cadmium and lead on the risks of diabetes and kidney dysfunction. Int. J. Environ. Res. Public Health 2022, 19, 2259. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Swaddiwudhipong, W.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Modeling cadmium exposures in low- and high-exposure areas in Thailand. Environ. Health Perspect. 2013, 121, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Zarcinas, B.A.; Pongsakul, P.; McLaughlin, M.J.; Cozens, G. Heavy metals in soils and crops in Southeast Asia. 2. Thailand. Environ. Geochem. Health 2004, 26, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Sripaoraya, K.; Siriwong, W.; Pavittranon, S.; Chapman, R.S. Environmental arsenic exposure and risk of diabetes type 2 in Ron Phibun subdistrict, Nakhon Si Thammarat Province, Thailand: unmatched and matched case-control studies. Risk Manag Healthc Policy 2017, 10, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Suwatvitayakorn, P.; Ko, M.S.; Kim, K.W.; Chanpiwat, P. Human health risk assessment of cadmium exposure through rice consumption in cadmium-contaminated areas of the Mae Tao sub-district, Tak, Thailand. Environ. Geochem. Health 2020, 42, 2331–2344. [Google Scholar] [CrossRef]
- Swaddiwudhipong, W.; Mahasakpan, P.; Limpatanachote, P.; Krintratun, S. Correlations of urinary cadmium with hypertension and diabetes in persons living in cadmium-contaminated villages in northwestern Thailand: A population study. Environ. Res. 2010, 110, 612–616. [Google Scholar] [CrossRef]
- Hornung, R.W.; Reed, L.D. Estimation of average concentration in the presence of nondetectable values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Nishijo, M.; Ruangyuttikarn, W.; Gobe, G.C.; Phelps, K.R. The effect of cadmium on GFR is clarified by normalization of excretion rates to creatinine clearance. Int. J. Mol. Sci. 2021, 22, 1762. [Google Scholar] [CrossRef] [PubMed]
- White, C.A.; Allen, C.M.; Akbari, A.; Collier, C.P.; Holland, D.C.; Day, A.G.; Knoll, G.A. Comparison of the new and traditional CKD-EPI GFR estimation equations with urinary inulin clearance: A study of equation performance. Clin. Chim. Acta 2019, 488, 189–195. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, D.P.; Warsi, G.; Dwyer, J.H. A simulation study of mediated effect measures. Multiv. Behav. Res. 1995, 30, 41–62. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Meth. Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef]
Figure 1.
An inverse dose-response relationship of eGFR and cadmium excretion rate. Scatterplots relate eGFR to log[(ECd/Ccr) ×105] in participants grouped by gender (a,b), blood pressure status (c,d), and cadmium burden; (ECd/Ccr)×100 < 1 and ≥ 1 µg/L filtrate. Coefficients of determination (R2) and standardized β-coefficients for all scatterplots, numbers of participants in subgroups, and p-values are provided.
Figure 1.
An inverse dose-response relationship of eGFR and cadmium excretion rate. Scatterplots relate eGFR to log[(ECd/Ccr) ×105] in participants grouped by gender (a,b), blood pressure status (c,d), and cadmium burden; (ECd/Ccr)×100 < 1 and ≥ 1 µg/L filtrate. Coefficients of determination (R2) and standardized β-coefficients for all scatterplots, numbers of participants in subgroups, and p-values are provided.
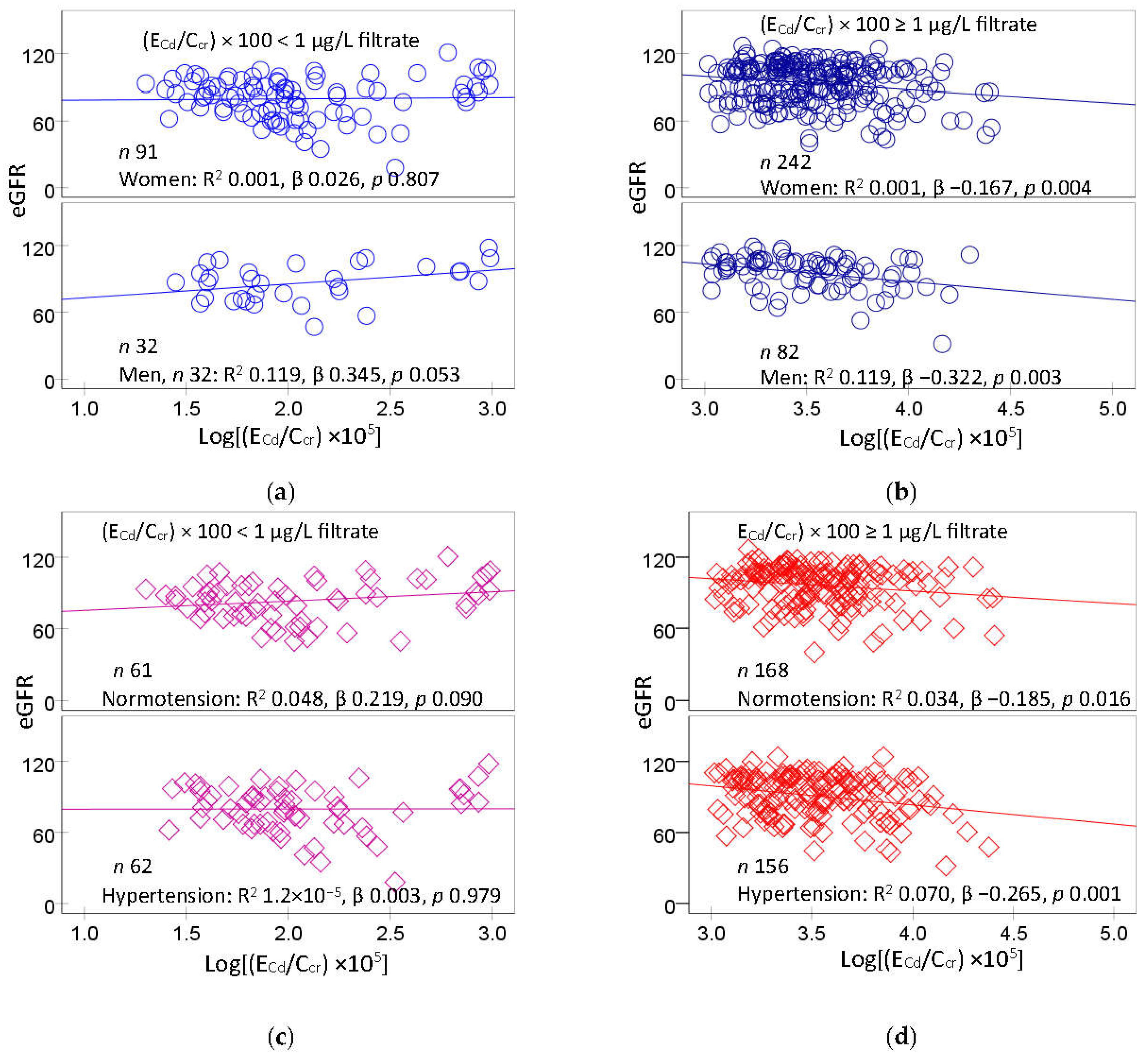
Figure 2.
Effects of cadmium burden and other variables on eGFR. Bar graphs depict mean eGFR in participants with (ECd/Ccr) × 100 < 1 and ≥ 1 µg/L filtrate (a,b) stratified by gender, smoking status, diabetes, and blood pressure status. Mean eGFR values were obtained via univariate covariance analysis with adjustment for covariates; age, BMI, gender, smoking, hypertension, diabetes and interactions.
Figure 2.
Effects of cadmium burden and other variables on eGFR. Bar graphs depict mean eGFR in participants with (ECd/Ccr) × 100 < 1 and ≥ 1 µg/L filtrate (a,b) stratified by gender, smoking status, diabetes, and blood pressure status. Mean eGFR values were obtained via univariate covariance analysis with adjustment for covariates; age, BMI, gender, smoking, hypertension, diabetes and interactions.
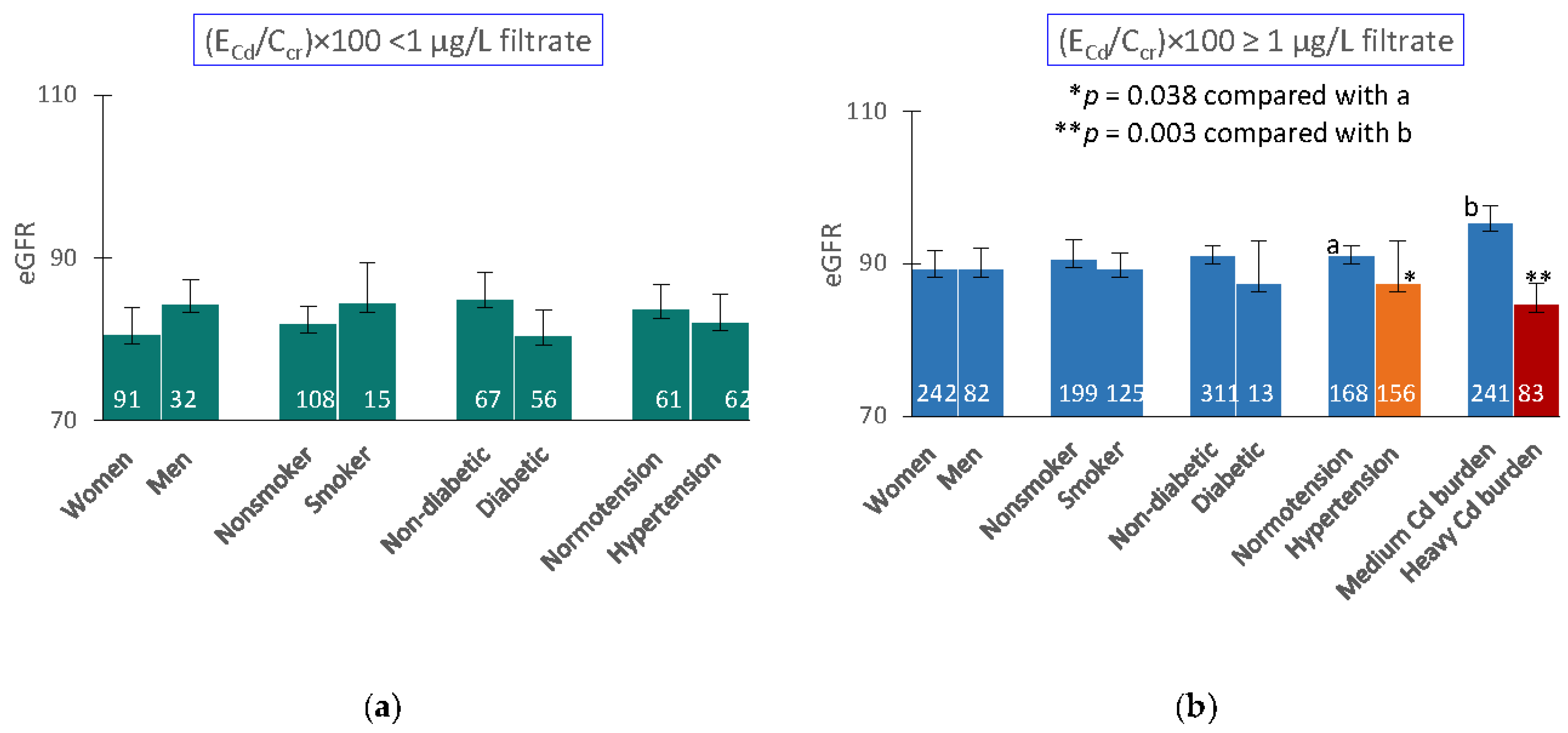
Figure 3.
eGFR as a predictor of blood pressure increases. Scatterplots relate SBP (a,b) and DBP (c,d) to eGFR in women and men with (ECd/Ccr)×100 of < 1 and ≥ 1 µg/L filtrate. Coefficients of determination (R2) and standardized β-coefficients for all scatterplots, numbers of participants in subgroups, and p-values are provided.
Figure 3.
eGFR as a predictor of blood pressure increases. Scatterplots relate SBP (a,b) and DBP (c,d) to eGFR in women and men with (ECd/Ccr)×100 of < 1 and ≥ 1 µg/L filtrate. Coefficients of determination (R2) and standardized β-coefficients for all scatterplots, numbers of participants in subgroups, and p-values are provided.
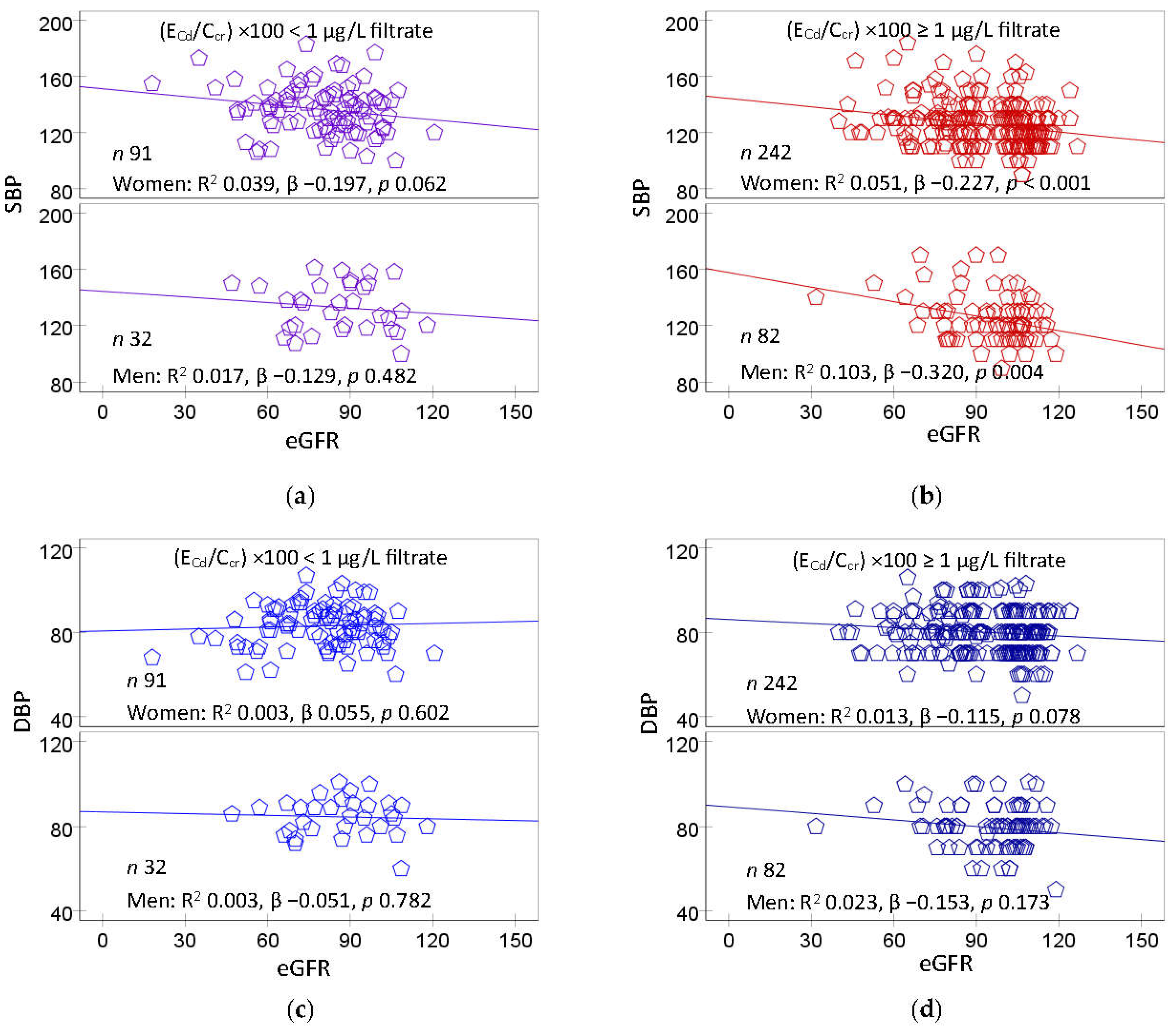
Figure 4.
Effects of cadmium burden and other variables on blood pressure. Bar graphs represent mean SBP (a,b) and DBP (c,d) in participants with (ECd/Ccr) × 100 < 1 and ≥ 1 µg/L filtrate. Mean SBP and mean DBP values were obtained via univariate covariance analysis with adjustment for covariates; age, BMI, gender, smoking, diabetes, eGFR levels, and interactions.
Figure 4.
Effects of cadmium burden and other variables on blood pressure. Bar graphs represent mean SBP (a,b) and DBP (c,d) in participants with (ECd/Ccr) × 100 < 1 and ≥ 1 µg/L filtrate. Mean SBP and mean DBP values were obtained via univariate covariance analysis with adjustment for covariates; age, BMI, gender, smoking, diabetes, eGFR levels, and interactions.
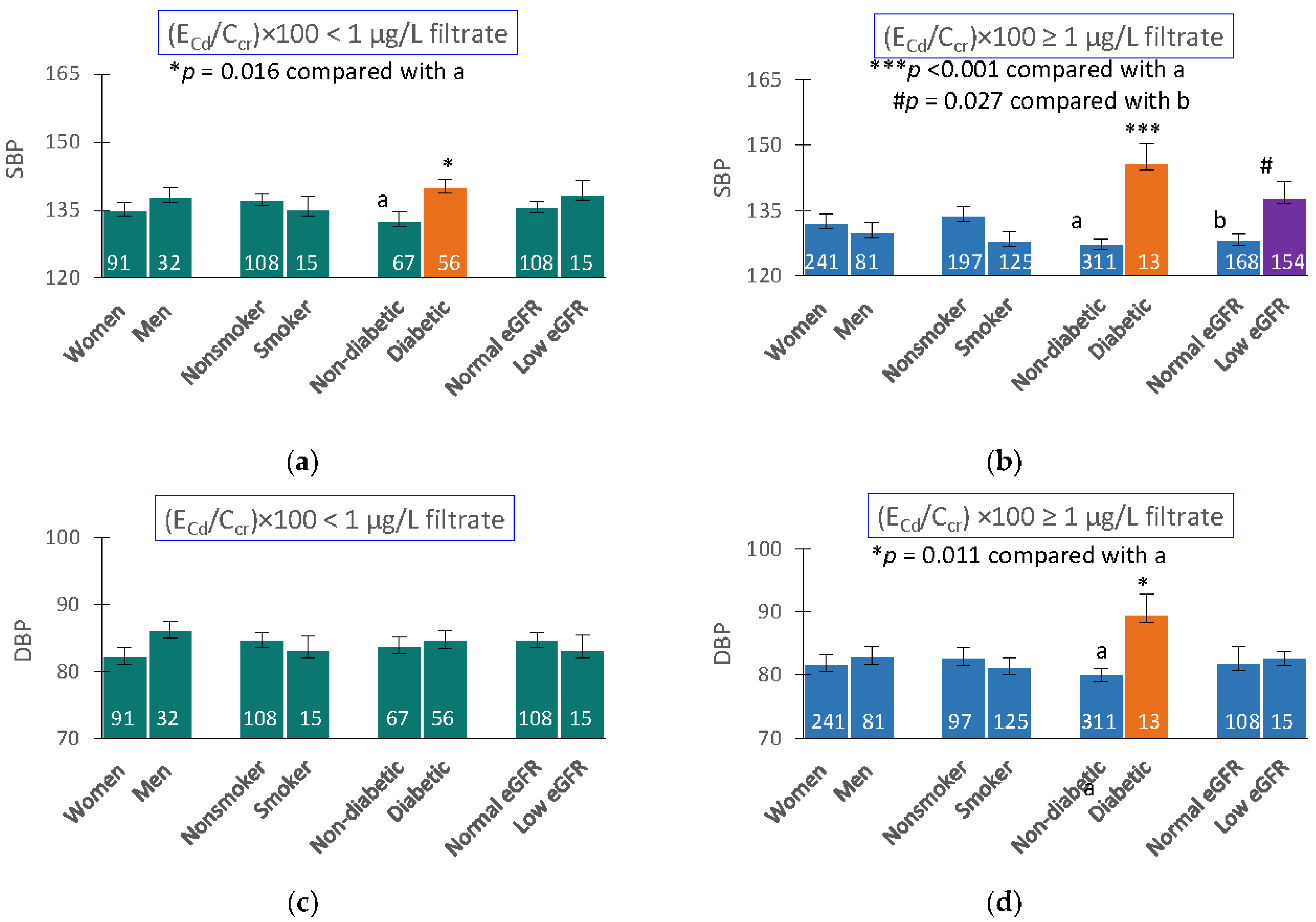
Figure 5.
Mediation analysis of the effect of cadmium on blood pressure. (a) A model depicts eGFR as a mediator of the effect of Cd on blood pressure increases. (b) Unstandardized β coefficients describing relationships of a Cd with eGFR (a) blood pressure (c) and eGFR with blood pressure (b). .
Figure 5.
Mediation analysis of the effect of cadmium on blood pressure. (a) A model depicts eGFR as a mediator of the effect of Cd on blood pressure increases. (b) Unstandardized β coefficients describing relationships of a Cd with eGFR (a) blood pressure (c) and eGFR with blood pressure (b). .
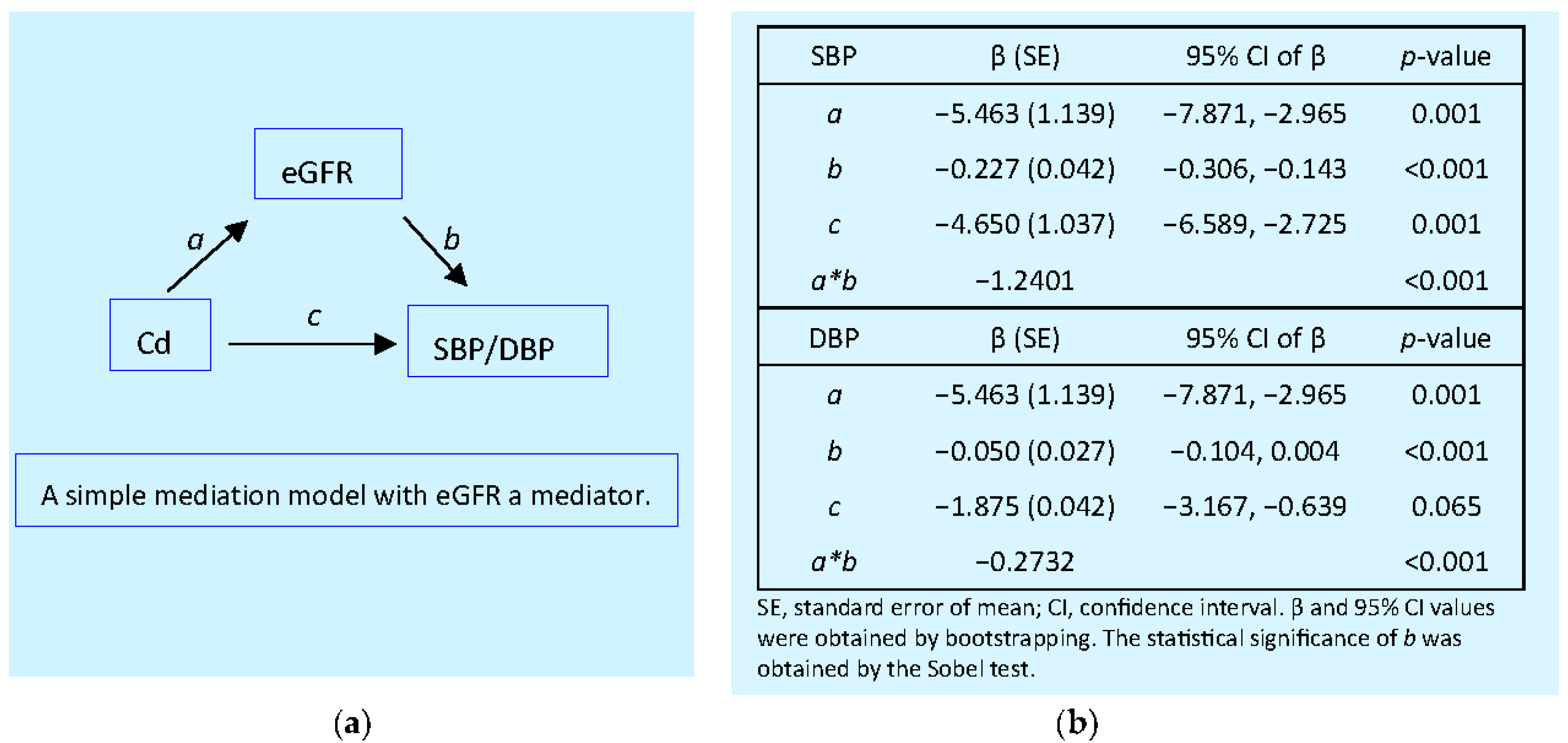

Table 1.
Descriptive characteristics of study subjects according to cadmium burden tertiles.
| Parameters | All, n = 447 | Cd Burden Tertiles | p | ||
|---|---|---|---|---|---|
| Low, n =148 | Middle, n =149 | High, n = 150 | |||
| Age, years | 51.1 ± 8.6 | 56.6 ± 9.7 | 48.1 ± 6.9 | 48.7 ± 6.1 | <0.001 |
| BMI, kg/m2 | 24.8 ± 4.0 | 25.5 ± 4.5 | 24.8 ± 3.8 | 24.0 ± 3.4 | 0.006 |
| eGFR a, mL/min/1.73m2 | 90 ± 18 | 84 ± 18 | 96 ± 17 | 91 ± 18 | <0.001 |
| % eGFR ≤ 60 mL/min/1.73m2 | 6.9 | 10.3 | 1.3 | 8.7 | 0.005 |
| % Hypertension | 48.8 | 51.4 | 46.3 | 48.7 | 0.685 |
| % Smoking | 31.1 | 16.2 | 34.9 | 42.7 | <0.001 |
| % Diabetes | 15.4 | 39.2 | 3.4 | 4.0 | <0.001 |
| Systolic blood pressure, mmHg | 128 ± 17 | 134 ± 17 | 126 ± 16 | 126 ± 16 | <0.001 |
| Diastolic blood pressure, mmHg | 81 ± 10 | 83 ± 10 | 80 ± 10 | 80 ± 11 | 0.019 |
| [cr]p, mg/dL | 0.82 ± 0.22 | 0.86 ± 0.25 | 0.77 ± 0.17 | 0.83 ± 0.23 | 0.001 |
| [cr]u, mg/dL | 114 ± 74 | 113 ± 72 | 131 ± 72 | 99 ± 75 | <0.001 |
| [Cd]b, µg/L | 2.75 ± 3.19 | 0.72 ± 0.83 | 2.37 ± 2.06 | 5.14 ± 3.95 | <0.001 |
| [Cd]u, µg/L | 4.23 ± 5.68 | 0.71 ± 1.20 | 3.91 ± 2.50 | 8.03 ± 7.86 | <0.001 |
| Normalized to Ecr (ECd/Ecr) b | |||||
| ECd/Ecr, µg/g creatinine | 4.03 ± 4.42 | 0.48 ± 0.62 | 3.07 ± 0.93 | 8.48 ± 4.87 | <0.001 |
| Normalized to Ccr, (ECd/Ccr) c | |||||
| (ECd/Ccr) ×100, µg/L filtrate | 3.20 ± 3.73 | 0.38 ± 0.46 | 2.28 ± 0.56 | 6.89 ± 4.31 | <0.001 |
n, number of subjects; BMI, body mass index; eGFR, estimated glomerular filtration rate; cr, creatinine; alb, albumin; Cd, cadmium; ACR, albumin-to-creatinine ratio. a eGFR was determined using the CKD-EPI equations [35]. b ECd/Ecr = [Cd]u/[cr]u. c ECd/Ccr = [Cd]u[cr]p/[cr]u [36]. SBP and DBP data were from 445 subjects. All other data were from 447 subjects. Arithmetic mean ± standard deviation (SD) values are provided for all continuous variables. p ≤ 0.05 identifies statistical significance.
Table 2.
Prevalence odds ratios for hypertension in relation to cadmium burden and other independent variables.
Table 2.
Prevalence odds ratios for hypertension in relation to cadmium burden and other independent variables.
| Independent Variables/Factors |
Hypertension | ||||
|---|---|---|---|---|---|
| β Coefficients | POR | 95% CI | p | ||
| (SE) | Lower | Upper | |||
| Age, years | 0.023 (0.014) | 1.024 | 0.997 | 1.051 | 0.085 |
| BMI, kg/m2 | 0.079 (0.027) | 1.082 | 1.027 | 1.140 | 0.003 |
| Gender | −0.070 (0.260) | 0.932 | 0.560 | 1.551 | 0.788 |
| Smoking | −0.444 (0.250) | 0.642 | 0.393 | 1.048 | 0.076 |
| Diabetes | 0.575 (0.329) | 1.777 | 0.932 | 3.388 | 0.081 |
| Cd burden a | |||||
| Mild | Referent | ||||
| Moderate | 0.748 | 2.114 | 1.049 | 4.260 | 0.036 |
| Heavy | 0.504 | 1.655 | 0.921 | 2.973 | 0.092 |
POR, prevalence odds ratio; CI, confidence interval; β, regression coefficient; SE, standard error of mean; BMI, body mass index; eGFR, estimated glomerular filtration rate. aMild, moderate and heavy Cd burdens were defined, respectively as (ECd/Ccr) ×100 < 1, 1−4.99 and ≥ 5 µg/L filtrate. Arithmetic means (SD) of (ECd/Ccr) ×100 in the low, medium and high Cd burden groups were 0.20 (0.26), 2.69 (1.08) and 9.11 (4.72) µg/L filtrate, respectively. Corresponding numbers of subjects in these Cd burden groups were 123, 241, and 83. For all tests, p-values ≤ 0.05 indicate a statistically significant effect of individual independent variables to the POR for hypertension.
Table 3.
Prevalence odds ratios for hypertension in relation to blood cadmium quartiles.
| Independent Variables/Factors |
Hypertension | ||||
|---|---|---|---|---|---|
| β Coefficients | POR | 95% CI | p | ||
| (SE) | Lower | Upper | |||
| Age, years | 0.018 (0.012) | 1.018 | 0.994 | 1.042 | 0.148 |
| BMI, kg/m2 | 0.080 (0.026) | 1.083 | 1.029 | 1.140 | 0.002 |
| Gender | −0.050 (0.254) | 0.951 | 0.578 | 1.565 | 0.844 |
| Smoking | −0.433 (0.255) | 0.649 | 0.394 | 1.069 | 0.089 |
| Diabetes | 0.422 (0.294) | 1.526 | 0.858 | 2.713 | 0.150 |
| Quartile of [Cd]b, µg/L | |||||
| Q1: < 0.60 | Referent | ||||
| Q2: 0.61−1.69 | 0.748 (0.293) | 2.113 | 1.191 | 3.749 | 0.011 |
| Q3: 1.70−3.38 | 0.606 (0.309) | 1.833 | 1.000 | 3.360 | 0.050 |
| Q4: >3.38 | 0.587 (0.337) | 1.798 | 0.928 | 3.482 | 0.082 |
POR, prevalence odds ratio; CI, confidence interval; β, regression coefficient; SE, standard error of mean; BMI, body mass index; eGFR, estimated glomerular filtration rate. Arithmetic means (SD) of [Cd]b quartiles 1, 2, 3 and 4 were 0.21 (0.22), 1.11 (0.30), 2.44 (0.52) and 6.72 (3.72) µg/L, respectively. Corresponding numbers of subjects in [Cd]b quartiles 1, 2, 3 and 4 quartile groups were 126, 117, 119 and 120. For all tests, p-values ≤ 0.05 indicate a statistically significant effect of individual independent variables to the POR for hypertension.
Table 4.
Comparing inverse associations of eGFR with cadmium excretion rate in subjects grouped by gender and blood pressure status.
Table 4.
Comparing inverse associations of eGFR with cadmium excretion rate in subjects grouped by gender and blood pressure status.
| Independent variables/ Factors |
eGFR, mL/min/1.73m2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Women, n = 333 |
Men, n = 114 |
Normotension, n = 229 |
Hypertension, n = 218 |
|||||
| β | p | β | p | β | p | β | p | |
| Age, years | −0.528 | <0.001 | −0.505 | <0.001 | −0.559 | <0.001 | −0.517 | <0.001 |
| BMI, kg/m2 | −0.050 | 0.308 | −0.136 | 0.122 | −0.037 | 0.532 | −0.077 | 0.216 |
| Log2[(ECd/Ccr)×105], µg/L filtrate | −0.121 | 0.051 | −0.077 | 0.463 | −0.056 | 0.440 | −0.177 | 0.023 |
| Gender | − | − | − | − | −0.017 | 0.787 | −0.012 | 0.870 |
| Hypertension | −0.045 | 0.344 | −0.203 | 0.018 | − | − | − | − |
| Smoking | 0.031 | 0.533 | 0.043 | 0.624 | 0.152 | 0.020 | −0.098 | 0.178 |
| Diabetes | −0.133 | 0.016 | −0.018 | 0.854 | −0.049 | 0.445 | −0.175 | 0.012 |
| Adjusted R2 | 0.279 | <0.001 | 0.248 | <0.001 | 0.318 | <0.001 | 0.242 | <0.001 |
n, number of subjects; eGFR, estimated glomerular filtration rate; β, standardized regression coefficient; BMI, body mass index; adjusted R2, coefficient of determination. β indicates strength of association of eGFR with seven independent variables (first column). Adjusted R2 indicates the proportion of eGFR variation explained by all independent variables. p-values ≤ 0.05 indicate statistically significant associations of independent variables and eGFR.
Table 5.
Multiple linear regression analysis to evaluate association of systolic and diastolic blood pressures with cadmium, eGFR and other variables.
Table 5.
Multiple linear regression analysis to evaluate association of systolic and diastolic blood pressures with cadmium, eGFR and other variables.
| Independent Variables/Factors |
SBP or DBP | |||||
|---|---|---|---|---|---|---|
| All, n = 447 | Mild Cd Burden a n = 123 |
Medium + Heavy n = 324 |
||||
| β | p | β | p | β | p | |
| Model 1: SBP | ||||||
| Age, years | 0.243 | <0.001 | 0.395 | <0.001 | 0.091 | 0.143 |
| BMI, kg/m2 | 0.113 | 0.013 | 0.081 | 0.361 | 0.097 | 0.084 |
| Log2[(ECd/Ccr)× 105], µg/L filtrate | 0.027 | 0.624 | 0.080 | 0.372 | −0.051 | 0.352 |
| eGFR, mL/min/1.73m2 | −0.106 | 0.036 | 0.011 | 0.907 | −0.176 | 0.004 |
| Gender | −0.044 | 0.378 | −0.096 | 0.360 | −0.024 | 0.688 |
| Smoking | −0.075 | 0.145 | −0.176 | 0.093 | −0.031 | 0.600 |
| Diabetes | 0.216 | <0.001 | 0.202 | 0.020 | 0.265 | <0.001 |
| Adjusted R2 | 0.199 | <0.001 | 0.157 | <0.001 | 0.150 | <0.001 |
| Model 2: DBP | ||||||
| Age, years | −0.028 | 0.650 | 0.036 | 0.739 | −0.081 | 0.213 |
| BMI, kg/m2 | 0.123 | 0.013 | 0.069 | 0.475 | 0.123 | 0.037 |
| Log2[(ECd/Ccr)× 105], µg/L filtrate | −0.069 | 0.255 | −0.059 | 0.546 | −0.025 | 0.660 |
| eGFR, mL/min/1.73m2 | −0.085 | 0.123 | 0.057 | 0.582 | −0.130 | 0.041 |
| Gender | −0.055 | 0.314 | −0.207 | 0.074 | −0.003 | 0.968 |
| Smoking | −0.050 | 0.373 | −0.209 | 0.068 | 0.008 | 0.897 |
| Diabetes | 0.102 | 0.064 | 0.027 | 0.775 | 0.193 | 0.001 |
| Adjusted R2 | 0.046 | <0.001 | −0.005 | 0.498 | 0.058 | 0.001 |
a Mild, medium plus heavy Cd burdens were defined as (ECd/Ccr) ×100 < 1 and ≥ 1 µg/L, respectively. eGFR, estimated glomerular filtration rate; β, standardized regression coefficient; adjusted R2, coefficient of determination. β indicates strength of association of eGFR with seven independent variables (first column). Adjusted R2 indicates the fraction of SBP and DBP variability that all independent variables explained. p-values ≤ 0.05 indicate a statistically significant associations of independent variables and blood pressure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



