
Submitted:
15 May 2024
Posted:
16 May 2024
You are already at the latest version
Abstract
Cytomegalovirus (CMV) is the leading infectious cause of brain defects and neurological dysfunctions, including sensorineural hearing loss (SNHL). A targeted screening in neonates failing the hearing screen is currently recommended in Italy according to national guidelines. However, SNHL may not be present at birth; also, congenital CMV (cCMV) may manifest with subtle signs other than SNHL. Therefore, inclusion of additional criteria for cCMV screening appears clinically valuable. Starting January 2021, we have implemented an expanded targeted cCMV screening at our center, with testing in case of maternal CMV infection during pregnancy, inadequate antenatal care, maternal HIV infection or immunosuppression, birthweight and/or head circumference.
Keywords:
Cytomegalovirus
; screening
; targeted
; newborn
; congenital
; infection
1. Introduction.
Congenital cytomegalovirus (cCMV), with a prevalence of approximately 0.2-2.2% [1], is the leading infectious cause of brain defects and neurological dysfunctions in newborns and children [2,3].
Approximately 10-15% of cCMV infected infants show symptoms at birth, such as microcephaly, intracranial calcifications, sensorineural hearing loss (SNHL), petechiae, and retinitis [4].
In contrast, 85-90% of congenitally infected newborns have no such clear evidence of disease at birth, thus making diagnosis challenging in the absence of a newborn screening program. Clinical presentation can be non-specific and subtle, including low birthweight (BW), head circumference (HC) <10th centile, jaundice, hepatosplenomegaly, and mild thrombocytopenia [5,6]. Importantly, 10-15% of the congenitally infected, asymptomatic neonates will develop late-onset symptoms of cCMV infection, among which SNHL is the most common [7,8]. In the absence of a screening, these babies do not receive a diagnosis and, therefore, an appropriate follow-up, and almost none of them is identified until speech and language delays are obvious [5].
Although several studies have suggested the potential benefits of a universal newborn screening for cCMV to detect all infants at risk of sequelae, there is still an ongoing debate about the feasibility of such a program [9,10,11,12,13,14,15,16].
Italian guidelines do not currently recommend universal newborn cCMV screening [17]. However, considering that SNHL is the most common cCMV-related sign in otherwise apparently healthy neonates and cCMV is the most common non-genetic cause of childhood SNHL [18], these guidelines highlights the importance of performing cCMV screening in all neonates failing the hearing screen, which is indeed universally recommended in Italy [17,19,20]. Unfortunately, this targeted cCMV screening program fails to identify those infected neonates without SNHL at birth [21,22,23].
In this context, it is important to identify other potential subtle clinical manifestations of cCMV, such as low BW, that could appropriately indicate the need for newborn screening, thus facilitating a timely diagnosis [6,24].
Findings from the implementation and routine clinical use of such expanded targeted programs in centers located in North America, Japan, and Israel have been recently reported, highlighting their feasibility and improved detection rates of cCMV-infected neonates compared to cCMV testing under a hearing-targeted only approach [14,25,26,27,28,29]. In contrast, no data are available regarding expanded targeted cCMV newborn screening programs in Italy.
Here we present the results of the first three years of use of such a screening program at our academic maternity center, located in Northern Italy, and detail the main indications prompting cCMV screening as well as incidence of symptomatic and asymptomatic cCMV at birth in our cohort.
2. Materials and Methods
2.1. Study Population
This is a prospective cohort study including all neonates born at our university maternity center and screened for cCMV infection within 21 days after birth, between January 2021 and December 2023.
Since 2018, a hearing-targeted cCMV screening program has been active at our Institution, with testing performed in neonates failing the hearing screen. Starting January 1st, 2021, this screening program has been expanded, with cCMV testing performed on live-born neonates if one of the following condition was present: suspected or confirmed maternal CMV infection during pregnancy, antenatal diagnosis of fetal growth restriction (FGR) according to Delphi criteria [30], antenatal ultrasound suspicion of fetal infection (e.g., hyperechoic bowel, liver anomalies, ventriculomegaly, etc.), antenatal amniocentesis positive for CMV DNA, maternal HIV infection with detectable viral load and/or suppressed CD4+ count, maternal immunosuppressive therapy, prematurity <37 weeks’ gestation, BW and/or HC <10th centile according to InterGrowth-21 (IG-21) charts [31], failed neonatal hearing screening, thrombocytopenia (platelet count <150 platelets/microL) or other neonatological indications (e.g., hepatomegaly, hepatitis). In January 2023, an additional criterion for testing was added: inadequate antenatal care (i.e., first antenatal visit after 14 weeks’ gestation or less than 3 antenatal assessment throughout gestation).
In order to assess all newborns with indications for cCMV infection screening according to our expanded protocol, we simultaneously implemented a standardized medical record system which monitors requests for CMV PCR testing, including the reasons for testing. Also, whenever a condition requiring cCMV testing is typed into the system, an alert is generated to prompt the assisting physician into ordering it.
For all newborns tested, we have collected the mother’s medical data, course of pregnancy, gestational age at delivery and delivery’s mode, in addition to newborn’s day of birth, BW and BW centile, HC centile, APGAR score at the 1st and 5th minute of life, cord blood pH value, and results of blood tests, physical examination, and instrumental and hearing tests carried out in early days of life. Whenever available, maternal serological status for CMV was also collected. Of note, the 2011 Italian guideline on low-risk pregnancy recommended against universal serological screening for CMV in pregnancy [32], thus resulting in an unknown maternal serological status in some of our newborns. At our center, maternal CMV IgG, IgM, and IgG avidity are measured by a chemiluminescence method on LIAISON® (DiaSorin), following the manufacturer’s recommendations.
Both an antenatal and postnatal outpatient clinic for perinatal infections is available at our Institution for women with suspected or confirmed CMV infection in pregnancy or fetal CMV infection and their newborns, respectively. For those pregnant women undergoing serological screening and being diagnosed with primary CMV infection during the peri-conceptional period or in pregnancy within 24 weeks’ gestation, valacyclovir (VCV) was administered (8 g/day) according to the Italian Drug Agency (AIFA) statement [33].
2.2. Sample Collection and CMV DNA Detection
In our study, screening was performed by CMV DNA identification on saliva samples [16]. In case of positivity, a urine sample was assessed for confirmatory purposes [15]. In some cases, particularly those born during the initial months after protocol implementation, testing was performed only on urine samples.
Saliva samples were collected using a cotton swab (COPAN®) positioned in the cheek to collect pooled saliva (UTM-RT transport medium, COPAN®). Collection would occur at least two hours after the last breastfeeding to limit false positive results. The samples were stored at 4°C until they were transported to hospital laboratory within 6 hours. Urine samples were collected using an adhesive perineal bag for newborns (Urine specimen collection bag, MedEvolution®).
CMV testing was performed firstly with a full off board extraction by magnetic beads technology using InGenius instruments. Then, through isothermal nucleic acid amplification by ELITechGroup CMV ELITe MGB® kit, consisting in a real-time polymerase chain reaction (rt-PCR) method automatically conducted on the AB 7500 fast dx thermocycler. The results were elaborated by the software and expressed in a quantitative way (limit of detection: <650 copies/mL).
Patients were classified as cCMV-infected if they had a positive PCR result on urine. In these cases, viral load was also quantified on whole blood.
2.3. Management of cCMV-Infected Newborns
Once the positivity is found, patients undergo a standard workup, including complete blood count, hepatic and kidney serum profiles, hearing testing (otoacoustic emission - OAE, automatic auditory brainstem response – aABR, and ABR threshold exam), ophthalmologic visit with fundus oculi examination, head and abdomen ultrasound, neuropsychiatric visit, brain magnetic resonance imaging (MRI) [34].
For all positive infants, the follow-up protocol includes ongoing clinical assessments, with evaluations by neuropsychiatrists and hearing assessments until the age of 6 years.
According to the 2017 Expert Consensus Statement by the European Society of Pediatric Infectious Disease (ESPID) on management of cCMV-infected newborns [35], symptomatic infants are treated within 30 days of life with Valgancyclovir (ValGCV) 16 mg/kg/dose every 12 hours orally, substituted with intravenous Gancyclovir (GCV) 6 mg/kg/dose in cases of food intolerance. Antiviral treatment in neonates with isolated sensorineural hearing loss (SNHL) is discussed on an individual basis. ValGCV is continued for a duration ranging from 6 weeks to 6 months.
2.4. Statistical Analysis
Descriptive statistics were employed to describe the study population, with absolute and relative frequencies for categorical variables, and mean ± standard deviation or median and interquartile range for normally and not-normally distributed continuous variables, respectively. Distribution of continuous variables was assessed visually.
Overlapping indications for testing were considered separately for the calculation of prevalence by testing indication.
The prevalence rate of cCMV infection was calculated as the number of cCMV neonates per 100 live births with a 95% confidence interval (CI), assuming the Poisson approximation to the binomial distribution. Analyses have been performed for the overall prevalence of cCMV infection, to determine the detection rate of our expanded screening program, and for symptomatic and asymptomatic cCMV at birth.
SPSS (version 28) and Prism GraphPad (version 10) were employed for the analyses.
2.5. Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Brianza Ethics Committee (protocol code 3156, date of approval 30 January 2020). Informed consent on the use of anonymized data was obtained from the parents or legal guardians of all subjects involved in the study.
3. Results
During the study period, a total of 7,651 infants were live born, 940 (12.3%) of whom were tested for cCMV infection. One hundred and fourteen (12.1%) neonates were from multiple gestations, and in 36 of them, both twins had indication for cCMV testing.

Table 1.
General characteristics of the mothers and their newborns.
| Maternal characteristics (n=904) | |
| Chronic diseases | 169 (18.7) |
| Pregnancy-related pathological conditions | 482 (53.4) |
| Multiple pregnancy | 78 (8.6) |
| Maternal CMV infection in pregnancy | 42 (4.6) |
| Vaginal birth | 660 (70) |
|
Neonatal characteristics (n=940) | |
| Male gender | 468 (49.8) |
| Term gestation (>37 wks) | 699 (74.4) |
| Birthweight (grams) | 2495.2±600.7 |
Birthweight centile
|
17.2±22.8 633 (67.3) 12 (1.3) |
Head circumference centile
|
31.2±26.6 270 (28.7) 32 (3.4) |
The results are expressed as N (%) and mean ± SD. Chronic diseases include dysthyroidisms, pregestational diabetes, multiple sclerosis, maternal cardiopathy, chronic hypertension, epilepsy, and psychiatric disorders. Pregnancy-related pathological conditions include hypertensive disorders of pregnancy, gestational diabetes, dysthyroidisms, fetal growth restriction, fetal congenital malformation, placental anomalies, preterm premature rupture of membranes.
Most of the tested babies (n=699, 74.4%) were born at term after 37 weeks’ gestation, at a mean gestational age of 382/7 weeks (range 226/7-421/7 weeks).
The most common indication for cCMV testing was BW <10th centile (n= 633, 67.3%), followed by HC <10th centile (n=270, 28.7%), and preterm birth (n=241, 25.6%) (Figure 1). Maternal CMV infection indicated cCMV screening in 42 (4.5%) neonates, whereas 22 newborns were tested because of a failed hearing screen (2.3%). No cases had maternal HIV with detectable viral load and/or suppressed CD4+ count as indication for cCMV testing. All neonates were tested for cCMV within 21 days of life.
Figure 1. Graphic representation of indications’ distribution for CMV testing. On X axis there are indications for CMV testing in order of frequency. They are described as follows: birthweight <10th centile (BW <10th), head circumference <10th centile (HC <10th), preterm birth <37 weeks’ gestation (PTB), thrombocytopenia (Low PLT), other neonatological indications (Other; it includes abnormal transcranial ultrasound findings and discrepancy between abdominal and head circumference), suspected or confirmed maternal CMV infection (Mum CMV), failed hearing screen (Failed hear.), maternal immunosuppression (Immunosup.), inadequate antenatal care (Inad ANC), and maternal HIV infection with detectable viral load and/or suppressed CD4+ count (Mum HIV+).
Of the 940 tested newborn, 66.6% (n=626) had 1 criteria, 25.9% (n=243) 2 criteria, and 7.6% (n=71) 3 or more criteria for testing.
There were no cases with indication for cCMV infection screening who were not tested.
Saliva PCR was performed as first screening test in almost all newborns (n=917, 97.6%); in 23 (2.4%) cases, a saliva sample was not collected, and screening test was performed on urine. No cases of false positive results with saliva PCR were registered.
Eleven newborns were diagnosed as congenitally infected, for a prevalence of 1.17% (95%CI 0.48-1.86) on tested neonates and of 0.14% (95%CI 0.06-0.23) on live born infants. (Table 2).
The highest prevalence of cCMV was among infants tested because of maternal CMV infection (8/42, 19%), followed by thrombocytopenia (4/67, 6%), preterm birth (3/241, 1.2%), HC <10th centile (3/270, 1.1%), and BW <10th centile (6/633, 0.95%). None of the eleven cCMV infected newborns had a failed hearing test at birth, but two (cases n. 4 and 10) showed an abnormal result of the ABR threshold exam at two months and 3 weeks of age, respectively, which prompted ValGCV therapy initiation; normal findings were recognized at follow-up.
In four cases (n. 4, 5, 9 and 11), the solely indication for neonatal testing was maternal CMV infection, thus leading to a prevalence of asymptomatic cCMV infection at birth of 0.42% (95%CI 0.84-0.01). In the remaining seven cases, cCMV infection followed the ESPID criteria for being symptomatic at birth (prevalence 0.74%, 95%CI 0.20-1.29). Of note, case n. 3 had a deficient growth as only indication for testing.
Maternal CMV infection, alongside antenatal ultrasound signs suggestive of fetal infection and an amniocentesis positive for CMV DNA, was an additional criterion for cCMV testing in cases n. 1 and 8; case n.1 also presented several other indications for testing at neonatal assessment after birth (Table 2).
Urine and whole blood were assessed in all eleven cCMV neonates: urine was CMV DNA-positive in all of them with a mean viral load of 55,879,733.09 copies/mL, whereas whole blood test was positive in ten out of eleven cCMV-infected neonates, with a mean viral load of 2,278,113.90 copies/mL. Eight (72.7%) of the congenitally infected patients had saliva tested, with a mean CMV viral load of 20,276,203.25 copies/mL.
An adverse clinical outcome was observed in two of the congenitally infected babies (n. 1 and 2), whereas the remaining neonates showed either a mildly abnormal (cases n. 3 and 6) or a regular follow-up.
The clinical case of neonate n. 1 has been previously published [36]. Briefly, there was a diagnosis of fetal ascites and hyperechoic bowel at 204/7 weeks, and the analysis of amniotic fluid revealed CMV DNA. The woman was started on VCV 8g/day according to the AIFA statement [33]. Fetal brain anomalies, confirmed by MRI, developed at 27 weeks, alongside with polyhydramnios at 33 weeks. At 341/7 weeks an emergency cesarean section was performed for non-reassuring fetal heart rate with the birth of a female neonate weighing 1,550 gr. Immediately after birth, she required intubation for severe dyspnea. Intravenous GCV was started leading to negative CMV DNA in blood on the eighth day of life. Clinical conditions progressively deteriorated with severe respiratory and right heart failure refractory to maximizing ventilator support. After parental counseling, comfort care was started with exitus occurring on the 11th day of life.
Neonate n. 2 had a diagnosis of FGR at 272/7 weeks. Maternal CMV serology was performed for the first time at 273/7 weeks’ gestation, showing positive IgG (122 U/mL; CLIA, positive >22) and negative IgM (11.1 U/mL; CLIA, negative <12) with high IgG avidity (0.357; CLIA, high >0.250). The woman declined amniocentesis. An emergency cesarean section was performed at 336/7 weeks for worsening fetal conditions. The female neonate weighed 1,050 gr, with a HC of 28 cm. Apgar score was 6 and 8 at 1st and 5th minute, respectively. CMV DNA assessed on the first day of life was positive on blood and urine (Table 2). Blood exams revealed thrombocytopenia (53.000/uL), and cerebral MRI diagnosed ventriculomegaly and polymicrogyria. ValGCV was started on the 10th day of life and was continued for 6 months. At the latest follow-up at 31 months of age, the infant shows cognitive delay and motor impairment, but no SNHL, with a physical growth around the 10th centile.
In case n. 3 there was a diagnosis of late-onset FGR at 361/7 weeks, which led to the birth of a male neonate weighing 2,300 gr at 371/7 weeks, with a regular HC. Apgar score was 9 and 10 at 1st and 5th minute of life. Positive CMV DNA testing was identified on the third day of life on urine (Table 2). All additional tests performed during the hospitalization were unremarkable. At the two-year follow up, the neonate showed a mild speech delay, which was confirmed at the subsequent visits.
Case n.6 had a diagnosis of FGR at 276/7 weeks, which was confirmed at subsequent ultrasounds with an estimated fetal weight <3rd centile. Maternal serology and virology for CMV were assessed for the first time at 354/7 weeks with evidence of positive IgG and IgM and CMV DNA on urine sample (1,350.0 copies/mL). Amniocentesis, performed at 365/7 weeks, revealed presence of CMV DNA in the amniotic fluid (206,000,000 copies/mL) and the woman was started on VCV 8 gr/day, according to AIFA statement. Labor was induced at 381/7 weeks for FGR, and a female neonate was born, with a weight of 1,900 gr. CMV DNA was positive on saliva and urine collected at birth (Table 2). Blood tests showed mild thrombocytopenia. Additional testing as unremarkable. A mild cognitive impairment and four-limbs hypotonia were identified at the one-year follow-up.
4. Discussion
Here we report the results of the first three years of clinical use of an expanded targeted screening program for cCMV, implemented at our academic maternity center in Northern Italy, relying on PCR method on saliva and urine samples within 21 days after birth.
Our findings are in line with previous studies investigating the clinical use of an expanded targeted cCMV screening program and identifying improved detection rates compared to a hearing-targeted screening program [14,26,27,28].
None of the eleven congenitally infected neonates identified in this three year-long cohort received cCMV testing because of failed hearing screen. Although being beneficial and feasible, hearing-targeted newborn screening programs have already shown limitations regarding their yield of cCMV-infected neonates [6,14,23,37]. The median age of SNHL onset in children with asymptomatic cCMV infection at birth is 44 months, with only 25% of asymptomatic children showing SNHL within the first month of life. In addition, CMV-associated SNHL is uniquely characterized by fluctuating hearing levels, thus making the diagnosis of SNHL in the absence of a cCMV-dedicated follow-up even more challenging [5,7,8].
Importantly, our incidence rate of 1.17% is close to the 1.08% figure recently reported by Chiereghin and colleagues in a research study assessing the feasibility and clinical validity of a universal newborn cCMV screening program at their center located in Northern Italy [15]. Similar detection rates between expanded and universal cCMV screening programs have also been reported by studies conducted in the United State and Israel [14,27], further supporting the clinical relevance of an expanded targeted screening.
Four out of the eleven cCMV newborns identified in our cohort were completely asymptomatic at birth with maternal infection as the solely indication for cCMV testing and one showed only deficient growth with low BW.
In a context where universal maternal serological screening for CMV is not recommended and newborn cCMV screening is performed only for failed hearing screening, these five diagnoses of cCMV infection would have been missed, thus preventing adequate neonatal assessment and follow-up evaluations. Of note, the newborn tested only because of low BW (case n. 3) displayed an abnormal follow-up with mild speech delay requiring rehabilitative intervention; also, newborn n. 4 showed a delayed onset (2 months of age) of bilateral SNHL, which resolved after antiviral treatment (regular follow-up at 25 months).
During the study period, the available Italian guideline on uncomplicated pregnancies (2011) recommended against a universal CMV serological screening in pregnancy [32]. Notwithstanding this, Italian obstetricians have been used to prescribe such screening, particularly in women with risk factors for CMV infection acquisition, such as young children <3 years of age [38].
A suspected or confirmed maternal infection was only the sixth indication for frequency for cCMV testing in our cohort (n=42, 4.5%) but showed the highest prevalence of cCMV by identifying eight (8/42, 19%) cCMV infected neonates, four of whom were asymptomatic. Of note, the Italian guideline has been recently updated (December 2023) and currently recommends a universal CMV screening in the first and second trimester of pregnancy in women with negative serostatus [39]. Knowledge of maternal CMV serology could further strengthen the clinical validity of our expanded targeted screening program [40].
However, considering that CMV seroprevalence in women of childbearing age in Italy is approximately 65% [41] and that cCMV can occur not only after primary but also non-primary maternal infection [42], as observed in our cases n. 1, 5, and 8, inclusion of additional criteria in the expanded screening, such as BW <10th centile, is extremely relevant. Importantly, BW <10th centile was the main indication for cCMV testing in our cohort, with a rate of 67.3% (n= 633), similar to that reported by Suarez and colleagues (68.2%) [14].
Of note, Italy is currently the only country recommending universal maternal CMV screening in pregnancy, with Canadian guidelines supporting universal screening only in those provinces with availability of IgG avidity testing [39,43,44].
There were no cases with indication for cCMV infection screening who were not tested, and all exams were performed within 21 days of life, the temporal cut-off for differentiating congenital from postnatal infections [45]. These results suggest that the standardized medical record system we had implemented to prompt the physician into testing for cCMV once one of the conditions listed as screening criterion was typed into the system was effective and avoided missed or delayed diagnoses.
Diagnosis of cCMV is based on the identification of CMV DNA by PCR on a urine sample collected within 21 days of life. Although this test presents high sensitivity (>97%) and specificity (99.9%) [25], its execution in a neonate can be challenging and time-consuming. Therefore, alternative biological substrates for identifying CMV DNA have been assessed in the last decade and large-scale studies investigating saliva samples have reported similar accuracy to urine samples alongside improved ease of execution [46,47], with negligible false positive rates (0.03%-0.14%) due to breastfeeding [48].
Almost 96% of the neonates in our cohort underwent screening by rt-PCR on saliva samples, with no cases of false positivity, further highlighting the feasibility and reliability of this screening method in the context of an expanded screening program.
Our study was conducted in an academic maternity center with a dedicated antenatal and postnatal clinic for perinatal infections, thus possibly limiting generalizability of our findings. Also, our Institution serves as a referral center for high-risk pregnancies identified in four nearby first level-care hospitals; therefore, our results may not be reflective of other centers given the potential referral bias. Although with a retrospective design, our research findings are strengthened by the use of a standardized medical record system to identify all newborns with indications for cCMV testing, thus avoiding limitations related to patients’ chart review.
5. Conclusions
In conclusion, our data show that the implementation of an expanded targeted newborn screening program for cCMV is feasible and of clinical value, by improving the detection rate of congenital infection compared to a targeted screening based only on failed hearing test. Importantly, the observed rate of cCMV identification approximates that obtained in a similar geographical context by a universal screening program. This allows early identification of newborns who could benefit from an antiviral treatment and/or dedicated follow-up.
The recent implementation of a universal CMV serological screening program in pregnancy according to the 2023 updated Italian guideline on uncomplicated pregnancies would further strengthen the clinical relevance of such expanded CMV screening program including maternal CMV infection as testing criterion.
Further research on the feasibility and cost-effectiveness of an expanded targeted newborn screening program across different maternity and nursery settings is pivotal to inform clinical practice.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Brianza Ethics Committee (protocol code 3156, date of approval 30 January 2020).
Informed Consent Statement
Informed consent on the use of anonymized data was obtained from the parents or legal guardians of all subjects involved in the study.
Data Availability Statement
Data are available upon reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cannon MJ, Schmid DS, Hyde TB: Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev Med Virol 2010;20(4): 202-213. [CrossRef]
- Kenneson A, Cannon MJ: Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Rev Med Virol 2007;17(4): 253-276.
- Gandhi MK, Khanna R: Human cytomegalovirus: clinical aspects, immune regulation, and emerging treatments. Lancet Infect Dis 2004;4(12): 725-738. [CrossRef]
- Dollard SC, Grosse SD, Ross DS: New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection. Rev Med Virol 2007;17(5): 355-363.
- Grosse SD, Leung J, Lanzieri TM: Identification of congenital CMV cases in administrative databases and implications for monitoring prevalence, healthcare utilization, and costs. Curr Med Res Opin 2021;37(5): 769-779.
- Sorichetti B, Goshen O, Pauwels J, Kozak FK, Tilley P, Krajden M, et al.: Symptomatic Congenital Cytomegalovirus Infection Is Underdiagnosed in British Columbia. J Pediatr 2016;169: 316-317.
- Grosse SD, Ross DS, Dollard SC: Congenital cytomegalovirus (CMV) infection as a cause of permanent bilateral hearing loss: a quantitative assessment. J Clin Virol 2008;41(2): 57-62.
- Lanzieri TM, Chung W, Flores M, Blum P, Caviness AC, Bialek SR, et al.: Hearing Loss in Children With Asymptomatic Congenital Cytomegalovirus Infection. Pediatrics 2017;139(3).
- Fowler KB, Dahle AJ, Boppana SB, Pass RF: Newborn hearing screening: will children with hearing loss caused by congenital cytomegalovirus infection be missed? J Pediatr 1999;135(1): 60-64.
- Fowler KB, Boppana SB: Congenital cytomegalovirus (CMV) infection and hearing deficit. J Clin Virol 2006;35(2): 226-231.
- Ross S, Long SS, Kimberlin DW: Closer to Universal Newborn Screening for Congenital Cytomegalovirus Infection but Far Away from Antiviral Therapy in All Infected Infants. J Pediatr 2018;199: 7-9.
- Gantt S, Dionne F, Kozak FK, Goshen O, Goldfarb DM, Park AH, et al.: Cost-effectiveness of Universal and Targeted Newborn Screening for Congenital Cytomegalovirus Infection. JAMA Pediatr 2016;170(12): 1173-1180.
- Letamendia-Richard E, Périllaud-Dubois C, de La Guillonnière L, Thouard I, Cordier AG, Roque-Afonso AM, et al.: Universal newborn screening for congenital cytomegalovirus infection: feasibility and relevance in a French type-III maternity cohort. Bjog 2022;129(2): 291-299.
- Suarez D, Nielson C, McVicar SB, Sidesinger M, Ostrander B, O’Brien E, et al.: Analysis of an Expanded Targeted Early Cytomegalovirus Testing Program. Otolaryngol Head Neck Surg 2023;169(3): 679-686. [CrossRef]
- Chiereghin A, Pavia C, Turello G, Borgatti EC, Baiesi Pillastrini F, Gabrielli L, et al.: Universal Newborn Screening for Congenital Cytomegalovirus Infection - From Infant to Maternal Infection: A Prospective Multicenter Study. Front Pediatr 2022;10: 909646.
- Gantt S: Newborn cytomegalovirus screening: is this the new standard? Curr Opin Otolaryngol Head Neck Surg 2023;31(6): 382-387. Curr Opin Otolaryngol Head Neck Surg.
- Morando C, Conti G, Bubbico L, Aversa S, Araimo G, Frezza S, et al.: ORGANIZZAZIONE, ESECUZIONE E GESTIONE DELLO SCREENING NEONATALE DELLA SORDITÀ CONGENITA: GUIDA PRATICA. 2020.
- Nance WE, Lim BG, Dodson KM: Importance of congenital cytomegalovirus infections as a cause for pre-lingual hearing loss. J Clin Virol 2006;35(2): 221-225. [CrossRef]
- Berrettini S, Ghirri P, Lazzerini F, Lenzi G, Forli F: Newborn hearing screening protocol in tuscany region. Ital J Pediatr 2017;43(1): 82.
- Ciccia M, Monari C, Vitagliano G, Zarro N, Sandri F: Usefulness of a flow chart for targeted screening of congenital cytomegalovirus-related hearing loss. J Neonatal Perinatal Med 2018;11(3): 339-343.
- Fowler KB, McCollister FP, Sabo DL, Shoup AG, Owen KE, Woodruff JL, et al.: A Targeted Approach for Congenital Cytomegalovirus Screening Within Newborn Hearing Screening. Pediatrics 2017;139(2).
- Minami SB, Yamanobe Y, Nakano A, Sakamoto H, Masuda S, Takiguchi T, et al.: A High Risk of Missing Congenital Cytomegalovirus-Associated Hearing Loss through Newborn Hearing Screening in Japan. J Clin Med 2021;10(21).
- Vancor E, Shapiro ED, Loyal J: Results of a Targeted Screening Program for Congenital Cytomegalovirus Infection in Infants Who Fail Newborn Hearing Screening. J Pediatric Infect Dis Soc 2019;8(1): 55-59.
- van der Weiden S, de Jong EP, Te Pas AB, Middeldorp JM, Vossen AC, Rijken M, et al.: Is routine TORCH screening and urine CMV culture warranted in small for gestational age neonates? Early Hum Dev 2011;87(2): 103-107.
- Zhang Y, Egashira T, Egashira M, Ogiwara S, Tomino H, Shichijo A, et al.: Expanded targeted screening for congenital cytomegalovirus infection. Congenit Anom (Kyoto) 2023;63(3): 79-82.
- Akiva MH, Hyde De Souza H, Lamarre V, Boucoiran I, Gantt S, Renaud C, et al.: Identifying Clinical Criteria for an Expanded Targeted Approach to Screening for Congenital Cytomegalovirus Infection-A Retrospective Study. Int J Neonatal Screen 2023;9(3).
- Masarweh K, Felszer-Fisch C, Shinwell E, Hasanein J, Peniakov M, Weiner SA, et al.: The Yield of Targeted Examination for the Detection of Symptomatic Congenital Cytomegalovirus Infection. Isr Med Assoc J 2021;23(5): 318-322.
- Levit Y, Dym L, Yochpaz S, Manor Y, Adler A, Halutz O, et al.: Assessment of Risk Indicators for Targeted Cytomegalovirus Screening in Neonates. Neonatology 2020;117(6): 750-755.
- McCrary H, Shi K, Newberry I: Outcomes from an expanded targeted early cytomegalovirus testing program. . J Pediatr Infect Dis 2020;15(4): 189-194.
- Gordijn SJ, Beune IM, Thilaganathan B, Papageorghiou A, Baschat AA, Baker PN, et al.: Consensus definition of fetal growth restriction: a Delphi procedure. Ultrasound Obstet Gynecol 2016;48(3): 333-339.
- Villar J, Cheikh Ismail L, Victora CG, Ohuma EO, Bertino E, Altman DG, et al.: International standards for newborn weight, length, and head circumference by gestational age and sex: the Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014;384(9946): 857-868.
- Istituto Superiore di Sanita’: La gravidanza fisiologica. Antenatal care for uncomplicated pregnancy. Sistema Nazionale Linee Guida (SNLG). 2011.
- Agenzia Italiana del Farmaco (AIFA). Inserimento del medicinale «Valaciclovir» (originatore o biosimilare) nell’elenco dei medicinali erogabili a totale carico del Servizio Sanitario Nazionale, per la prevenzione dell’infezione fetale e il trattamento della malattia fetale da citomegalovirus. In: (AIFA) AIdF, ed. Determina n 142618/2020, 20A07138) Gazzetta Ufficiale - Serie Generale n.322 del 30 dicembre 2020. 2020.
- AMCLI, SIGO, SIMaST, SIMIT, SIN, SIP: Percorsi diagnostico-assistenziali in Ostetricia-Ginecologia e Neonatologia. Citomegalovirus. 2012.
- Luck SE, Wieringa JW, Blázquez-Gamero D, Henneke P, Schuster K, Butler K, et al.: Congenital Cytomegalovirus: A European Expert Consensus Statement on Diagnosis and Management. Pediatr Infect Dis J 2017;36(12): 1205-1213.
- Fernicola F, Carli A, Arienti F, Viola Vasarri M, Lanteri L, Scandella G, et al.: Fatal severe persistent pulmonary hypertension with lung microvasculature parietal hyperplasia in a neonate with congenital cytomegalovirus infection treated in-utero with valacyclovir: A case report. Eur J Obstet Gynecol Reprod Biol 2024;294: 245-246.
- Diener ML, Zick CD, McVicar SB, Boettger J, Park AH: Outcomes From a Hearing-Targeted Cytomegalovirus Screening Program. Pediatrics 2017;139(2).
- Adler SP, Marshall B: Cytomegalovirus infections. Pediatr Rev 2007;28(3): 92-100.
- Istituto Superiore di Sanità: La gravidanza fisiologica, parte I. Antenatal care for uncomplicated pregnancy, part I. Sistema Nazionale Linee Guida (SNLG). 2023.
- Lazzarotto T, Gabrielli L, Lanari M, Guerra B, Bellucci T, Sassi M, et al.: Congenital cytomegalovirus infection: recent advances in the diagnosis of maternal infection. Hum Immunol 2004;65(5): 410-415.
- Dalmartello M, Parazzini F, Pedron M, Pertile R, Collini L, La Vecchia C, et al.: Coverage and outcomes of antenatal tests for infections: a population based survey in the Province of Trento, Italy. J Matern Fetal Neonatal Med 2019;32(12): 2049-2055.
- Maltezou PG, Kourlaba G, Kourkouni Ε, Luck S, Blázquez-Gamero D, Ville Y, et al.: Maternal type of CMV infection and sequelae in infants with congenital CMV: Systematic review and meta-analysis. J Clin Virol 2020;129: 104518.
- Boucoiran I, Yudin M, Poliquin V, Caddy S, Gantt S, Castillo E: Guideline No. 420: Cytomegalovirus Infection in Pregnancy. J Obstet Gynaecol Can 2021;43(7): 893-908.
- Khalil A HP, Jones CE, et al., on behalf of the Royal College of Obstetricians and Gynaecologists: Scientific Impact Paper No. 56: Congenital Cytomegalovirus Infection: Update on Screening, Diagnosis and Treatment (2nd edition). Peer review draft. 2023.
- Kimberlin D, Barnett E, Lynfield R, Sawyer M: Cytomegalovirus Infection. In Red Book: 2021–2024 Report of the Committee on Infectious Diseases. American Academy of Pediatrics: Itasca, IL, USA. 2021.
- Gantt S, Bitnun A, Renaud C, Kakkar F, Vaudry W: Diagnosis and management of infants with congenital cytomegalovirus infection. Paediatr Child Health 2017;22(2): 72-74.
- Boppana SB, Ross SA, Shimamura M, Palmer AL, Ahmed A, Michaels MG, et al.: Saliva polymerase-chain-reaction assay for cytomegalovirus screening in newborns. N Engl J Med 2011;364(22): 2111-2118.
- Ross SA, Michaels MG, Ahmed A, Palmer AL, Sánchez PJ, Bernstein DI, et al.: Contribution of Breastfeeding to False-Positive Saliva Polymerase Chain Reaction for Newborn Congenital Cytomegalovirus Screening. J Infect Dis 2018;217(10): 1612-1615.
Figure 1.
Indications for cCMV testing.
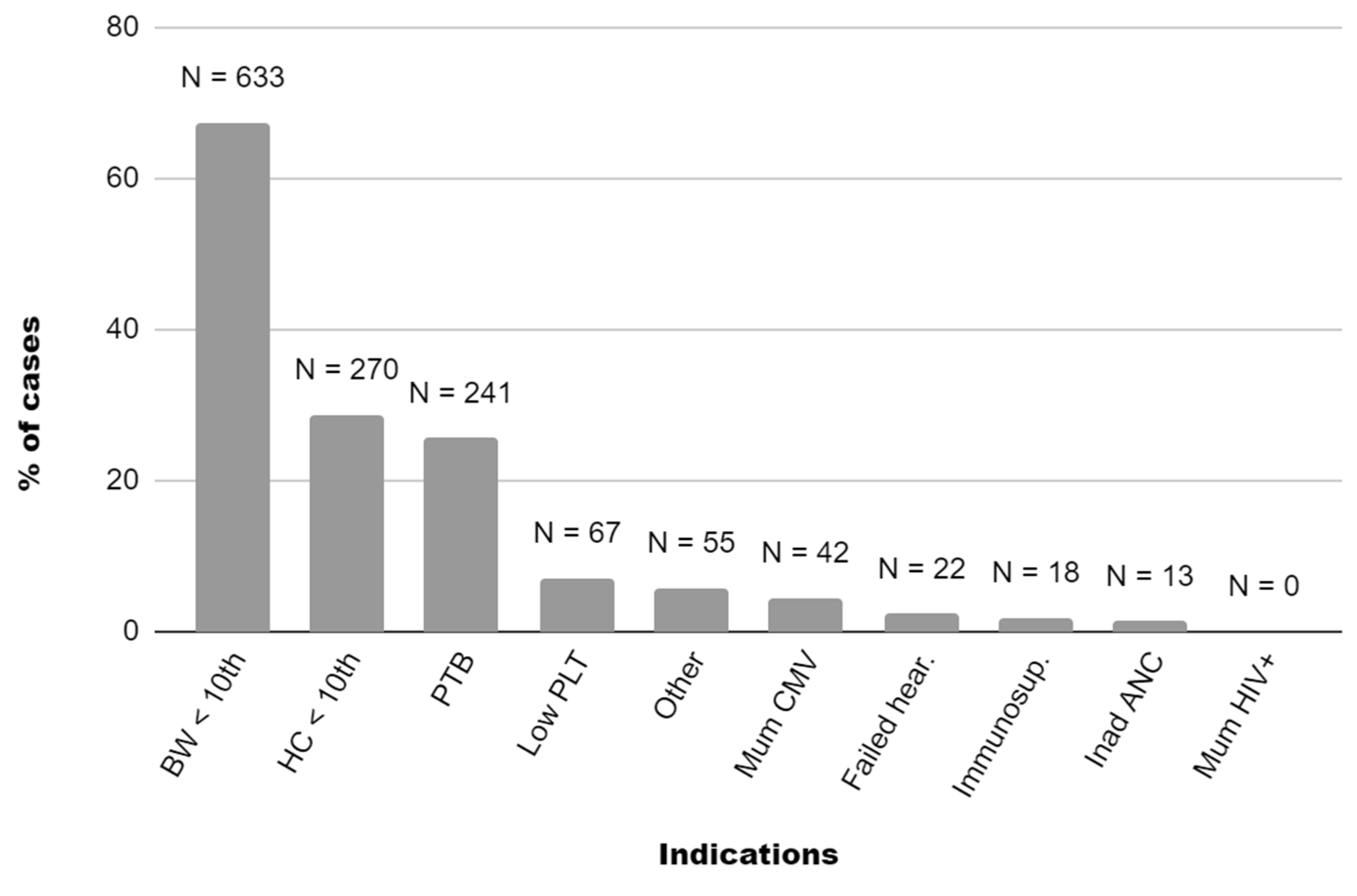
Table 2.
cCMV infected newborns.
| Patients | n. 1 | n. 2 | n. 3 | n. 4 | n. 5 | n. 6 | n. 7 | n. 8 | n. 9 | n. 10 | n. 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Maternal CMV status at beginning of pregnancy |
Seropositive | Unknown | Unknown | Seronegative | Seropositive | Unknown | Unknown | Sero positive |
Sero negative |
Sero negative |
Sero negative |
| Indication for CMV testing | Mat. CMV NPI (peri-conception/1st trim.) FGR (amnio+) BW<10 PTB Low PLT Petechiae |
FGR BW&HC<10 PTB Low PLT Petechiae Hepatitis |
FGR BW<10 |
Mat. CMV PI (24-28 weeks) |
Mat. CMV NPI (peri-conception/1st trim.) |
Mat. CMV PI (unknown timing) FGR (amnio+) BW&HC<10 Low PLT |
FGR BW<10 Low PLT Petechiae |
Mat. CMV NPI (peri-conception/1st trim.) Fetal ascites (amnio+) PTB Ascites |
Mat. CMV PI (1st trim.) |
Mat. CMV PI (26-30 weeks) BW&HC <10 |
Mat. CMV PI (1st trim.) |
| VCV in pregnancy | Yes | No | No | No | No | Yes | No | Yes | Yes | No | Yes |
| Gender | Female | Female | Male | Male | Female | Female | Male | Male | Female | Male | Male |
| Delivery mode | CS | CS | CS | VB | VB | VB | CS | CS | VB | VB | VB |
| GA (weeks) |
33 5/7 | 33 6/7 | 37 1/7 | 37 5/7 | 40 3/7 | 38 1/7 | 37 5/7 | 36 1/7 | 39 3/7 | 41 4/7 | 39 6/7 |
| BW centile | 4 | 0 | 4 | 45 | 12 | 0 | 2 | 92 | 61 | 4 | 67 |
| HC centile | 35 | 1 | 25 | 70 | 33 | 0 | 70 | 97 | 79 | 0 | 74 |
| NBHS result | Pass | Pass | Pass | Pass | Pass | Pass | Pass | Pass | Pass | Pass | Pass |
| CMV-positive specimens | Saliva, urine | Urine | Urine | Saliva, urine | Saliva, urine | Saliva, urine | Saliva, urine | Saliva, urine | Saliva, urine | Urine | Saliva, urine |
| Saliva VL (copies/mL) |
19,498 | - | - | 50,000,000 | 44,296,505 | 20,575,137 | 2,699,368 | 13,619,118 | 18,000,000 | - | 13,000,000 |
| Urine VL (copies/mL) | 386,791 | 177,000,000 | 22,581,862 | 3,947,803 | 5,100,000 | 212,000,000 | 5,650,371 | 88,000,000 | 4,700,260 | 309,977 | 95,000,000 |
| Whole blood VL (copies/mL) | 477 | 155,808 | 22,581,862 | 2,289 | Neg. | 4,161 | 13,899 | 975 | 4,128 | 390 | 17,150 |
| Additional CNS findings (TCUS & MRI) |
Left periventricular cystic lesion, ventriculo megaly |
Ventriculo megaly, polymicro gyria |
None | None | None | None | None | None | None | None | None |
| GCV ValGCV |
Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | No |
| Follow-up (length in months) |
Deceased on 11th day of life | Cognitive delay and motor impairment (31 mo) |
Mild speech delay (36 mo) |
Abnormal bilateral ABR threshold at 2 months, then regular (25 mo) |
Regular (26 mo) |
Mild cognitive delay and motor impairment (15 mo) |
Regular (6 mo) |
Regular (9 mo) |
Regular (9 mo) |
Abnormal left ear ABR threshold at 3 weeks, then regular (7 mo) |
Regular (6 mo) |
Mat., maternal; CMV, cytomegalovirus; NPI, non-primary infection; PI, primary infection; FGR, fetal growth restriction; amnio+, amniocentesis positive for CMV DNA; BW, birthweight; HC, head circumference; PTB, preterm birth; low PLT, platelet (thrombocytopenia); VCV, valacyclovir; CS, cesarean section; VB, vaginal birth; GA, gestational age; NBHS, newborn hearing screening; VL, viral load; CNS, central nervous system; TCUS, transcranial ultrasound; MRI, magnetic resonance imaging; GCV, gancyclovir; valGCV, valgancyclovir; mo, months.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



