
Submitted:
16 May 2024
Posted:
16 May 2024
You are already at the latest version
Abstract
Lung cancer remains one of the leading causes of cancer-related mortality worldwide. There is evidence of a complex interplay between lung cancer and interstitial lung disease (ILD), affecting disease progression, management strategies, and patient outcomes. Both conditions develop as the result of common risk factors such as smoking, environmental exposures, and genetic predispositions. The presence of ILD poses diagnostic and therapeutic challenges in lung cancer management, including difficulties in interpreting radiological findings, increased susceptibility to treatment-related toxicities, such as acute exacerbation of ILD after surgery and pneumonitis after radiation therapy and immunotherapy. Moreover, due to the lack of large, phase III randomized controlled trials in patients with lung cancer and ILDs, the evidence-based therapeutic options remain limited. The role of antifibrotic treatment in the prevention of lung-cancer-related treatment toxicities remains to be elucidated. Emerging diagnostic modalities and biomarkers, and optimizing personalized treatment strategies are essential to improve outcomes in this patient population.
Keywords:
interstitial lung disease
; lung cancer
; IPF
1. Introduction
Lung cancer and interstitial lung diseases (ILD) share distinct biological pathways, even though the precise genetic and cellular mechanisms remain incompletely understood. ILDs can progress to pulmonary fibrosis, which is characterized by the progressive scarring and thickening of lung tissue, which can lead to impaired lung function [1]. Numerous signaling pathways and microenvironments have been identified as disruptors of tissue architecture, contributing to dysfunction in both conditions and leading to loss of lung function, impaired gas exchange, and respiratory symptoms such as dyspnea. Despite these commonalities, lung tumorigenesis and fibrosis are characterized by highly heterogeneous behaviors, emphasizing the need for personalized therapeutic approaches tailored to individual patients.
As an example, one of the most progressive forms of ILD, idiopathic pulmonary fibrosis (IPF), is influenced by genetic predisposition, aging, and environmental factors. Current evidence indicates that in genetically predisposed individuals, especially those over 60 years of age, environmental exposures lead to alterations in lung epithelium, initiating aberrant cellular activation and localized expansion of fibroblasts, ultimately resulting in fibrotic remodeling, loss of lung architecture, and functional deterioration, with the escalating mechanical stiffness perpetuating the fibrotic response through cell-autonomous and matrix-dependent processes [2].
On the other hand, lung cancer is a characterized by the uncontrolled growth of malignant cells in the lungs through activation of the variety of signaling pathways [3,4]. Although these two conditions are distinct, there is evidence suggesting shared pathomechanisms, aggravating factors and signaling pathways between them. Indeed, the coexistence of pulmonary fibrosis and lung cancer is not uncommon [5,6]. Existence of IPF itself causes to a 7% to 20% increased risk of lung cancer development [7]. Also, there is a significantly higher prevalence of lung cancer in the ‘combined IPF and emphysema’ (CPFE) cohort as compared with fibrosis only [8].
Moreover, lung transplant patients with IPF exhibit higher rates of lung cancer, suggesting shared molecular connections between the two diseases [9]. Such shared molecular pathways of established lung cancer and pulmonary fibrosis are the epithelial-mesenchymal transition (EMT), mesenchymal activation and SFTPA mutation [10].
Also, lung cancer manifests in the peripheral regions of the lungs, where especially fibrotic changes typical of Usual Interstitial Pneumonia (UIP) are prevalent, and adenocarcinoma and squamous cell carcinoma are the predominant types observed in individuals with IPF [11]. In more detail, pulmonary fibrosis and lung cancer share common risk factors, such as smoking, occupational/environmental exposures (e.g., asbestos, silica), and genetic predisposition. These shared risk factors may contribute to the development of both conditions in the same individual, significantly impacting disease survival [8].
The global burden of lung cancer and ILDs is increasing [6,12,13].Due to the increased risk of lung cancer in individuals with pulmonary fibrosis, there is growing interest in instituting screening and surveillance programs for this population. The presence of pulmonary fibrosis in individuals with lung cancer has clinical implications, influencing both treatment decisions and prognosis [14]. The compromised lung function associated with pulmonary fibrosis may limit certain treatment options, and the overall prognosis for individuals with both conditions may be poorer compared to those with lung cancer alone. Early detection of lung cancer is anticipated to facilitate more effective treatment and lead to improved outcomes. This emphasizes the importance of understanding the interplay between pulmonary fibrosis and lung cancer for better management and outcomes in affected individuals [6,15].
As research continues to unravel the intricate molecular and cellular landscapes of both conditions, the prospect of identifying converging points in the pathogenic processes holds promise for innovative and more effective therapeutic interventions. Integrating insights from the research of cancer and fibrosis not only enhances our understanding of these diseases but also offers a potential roadmap for the development of targeted therapies that address the unique challenges posed by the heterogeneity observed in lung tumorigenesis and fibrogenesis. Recognizing the commonalities in the underlying pathways between cancer and pulmonary fibrosis opens avenues for the development of novel therapeutic strategies and personalized approaches and may prove essential in optimizing treatment outcomes of individuals with lung cancer and fibrosis.
2. Pathophysiology
Specific pathologic mechanisms and factors have been proposed to contribute to the association between pulmonary fibrosis and lung cancer. Shared genetic and molecular pathways, as indicated by genetic alterations in specific genes and signaling pathways, may contribute to the development of both pulmonary fibrosis and lung cancer [2,6,16]. This shared susceptibility involves such genetic factors as aberrations in key genes like TGF-β and p53, with evidence suggesting that specific genetic factors related to lung development, tissue repair, and cell cycle regulation, such as mutations in relevant genes, may play roles in the development of both conditions [17].
Specific gene mutations, including those involving the oncogene p53, fragile histidine triads, microsatellite instability, and loss of heterozygosity, are observed in many of IPF cases, particularly in the characteristic peripheral honeycombed lung regions [18]. Mutations associated with cancer, such as those affecting telomere shortening and telomerase expression, are also found in familial IPF, suggesting shared genetic factors [19]. Jan kinase and SFTP mutations were found in families with PF and lung cancer.
Chronic inflammation is a common feature in both pulmonary fibrosis and tumor development and is associated with the fibrotic process in some ILDs [6,20]. The inflammatory microenvironment may create conditions that promote the initiation and progression of cancer cells in the lungs [21]. Furthermore, the fibrotic changes in pulmonary fibrosis involve excessive deposition of collagen and other extracellular matrix components, leading to tissue remodeling and scarring [22]. This altered lung architecture and the increased stiffness may create a microenvironment that is promoting the growth of cancer cells [23,24] and may involve modifications in the extracellular matrix and cytokine profiles [10,25].
Tyrosine kinases, integral to multiple signaling pathways regulating cell growth, differentiation, adhesion, and motility, as well as cell death, are normally controlled by transmembrane receptors and ligands. However, aberrant kinase activities have been linked to the development, progression, and metastasis of various cancers and some types of ILD as well [26]. It is in line with this note that nintedanib, a triple kinase inhibitor, is effective in both lung fibrosis as well as lung cancer, and is authorised for both conditions [26]. Further, hypomethylation of oncogenes and methylation of tumor suppressor genes, established pathogenic mechanisms in many tumors, are also observed in patients with IPF, with recent studies revealing reciprocal changes in global methylation patterns between IPF and lung cancers, and hypermethylation of the CD90/Thy-1 promoter region in IPF contributing to the loss of the glycoprotein Thy-1, associated with invasive cancer behaviors and the transition from fibroblasts to myofibroblasts [27].
Fibrosis is intricately linked to the persistent action of transforming growth factor (TGF)-β, a regulator of various intracellular mediators and pathways associated with cell growth, organ development, the immune system, metastasis, and cancer progression. The "TGF-β paradox" is observed, according to which TGF-β promotes cellular growth in cancer cells but has the opposite effect in benign cells [28]. This is attributed to the activation of the extracellular signal-regulated kinase (ERK) pathway in malignant cells and its inactivation in non-cancer cells.
TGF-β, PDGF, VEGF, and FGF are implicated in both lung cancer and lung fibrosis, with VEGF potentially promoting cell survival and proliferation through ERK1/2 and PI3K activation and VEGF mRNA being elevated levels in IPF patient endothelial progenitor cells [29]. The downregulation of TGF-β receptors is a pivotal event leading to changes in cellular behavior, with low receptor levels promoting metastasis, cancer progression, and playing a crucial role in early carcinogenesis [30]. Lung cancer in individuals with pulmonary fibrosis tends to be more aggressive, with TGF-β playing a crucial role by being produced by both pulmonary fibrosis-associated fibroblasts and cancer-derived epithelial cells, promoting myofibroblast recruitment at cancer margins, safeguarding them from apoptosis, and facilitating their invasion through basement membranes and the process of EMT [31].
Furthermore, the elevated expression of Programmed Cell Death-Ligand 1 (PD-L1) is observed in both IPF and lung cancer, where PD-L1, a cell surface protein, interacts with the PD1 receptor on T-cells, leading to immune response suppression and contributing to the pathogenesis of these diseases [32].
Additionally, the MET signaling pathway (a receptor tyrosine kinase whose ligand is hepatocyte growth factor), a crucial regulator of cell growth and proliferation activated in response to hypoxia, plays a significant role in both IPF and lung cancer [33]. Activation of the MET pathway promotes increased cell proliferation, tumor growth, and the expression of genes related to cell proliferation; the upregulation of the MET signaling pathway occurs in fibroblasts and myofibroblasts, contributing to the excessive collagen deposition and tissue fibrosis characteristic of the disease [34].
Pulmonary fibrosis is linked to cellular senescence, a state characterized by the secretion of pro-inflammatory factors that promote inflammation and tissue remodeling, potentially contributing to the development of cancer through the senescence-associated secretory phenotype (SASP) and the creation of a microenvironment supportive of cancer growth [35].
In both cancer and pulmonary fibrosis (particularly IPF), molecules including laminin, heat shock protein 27, and fascin, expressed by bronchiolar basal cells, are associated with cell migration and invasion, contributing to the invasive front of tumors and expressed in epithelial cells around fibroblast foci [36]. Additionally, matrix metalloproteases and integrins, known for their role in cell invasion, are strongly linked to the development of stem cell-like properties in cancer cells and, in the context of IPF, promote the initiation, maintenance, and resolution of tissue fibrosis, with clinical trials investigating inhibitors such as the humanized antibody STX-100 and specific antibodies against αvβ6 [37].
EMT is a process where epithelial cells undergo changes to become more mesenchymal, and this is implicated in both fibrosis and cancer. The transition of cells from an epithelial to a mesenchymal phenotype can promote tissue remodeling and contribute to cancer progression. EMT is implicated in fibrosis and cancer metastasis. In the lung, EMT may contribute to tissue remodeling and create a microenvironment supporting cancer growth [38].
Circulating and cell-free DNA, as well as abnormal expression levels of mRNA, are considered diagnostic and prognostic biomarkers for both cancer and IPF, with aberrant expression of certain short non-protein-coding RNAs in IPF influencing genes associated with fibrosis, ECM regulation, EMT induction, and apoptosis, potentially contributing to functional deterioration in pulmonary fibrosis patients [39,40].
Intercellular channels formed by connexins (Cxs) play a crucial role in metabolic and electrical coupling of cells, with Cx43 being the most abundant on fibroblast membranes, contributing to tissue repair and wound healing; however, reduced expression of Cx43 in primary lung fibroblasts from patients with IPF with limited intercellular communication and reflects common defects in contact inhibition and uncontrolled proliferation seen in both IPF and cancer cells [41].
3. Epidemiology of Lung Cancer in ILD
ILDs, particularly IPF, are established risk factors for lung cancer. An estimated 17.5-fold greater prevalence of NSCLC among IPF patients compared to the general population has been reported in a large Korean database, even after adjustment for age, smoking history and sex [42]. Patients with connective tissue disease (CTD)-related ILD exhibit a 1.7 to 2 times higher likelihood of developing lung cancer than ILD patients without CTD, with a relative risk increase ranging from 3.5 to 7.3 for any ILD subtype [43]. Notably, lung cancer incidence is higher in connective tissue disease-associated ILD (CTD-ILD) patients under 60 years compared to non-CTD-ILD (excluding IPF) patients [43]. Systemic sclerosis and ILD are associated with lung cancer risk. Data from a US Registry suggest that in individuals with ILD and conditions like rheumatoid arthritis, polymyositis/dermatomyositis, or systemic sclerosis, the risk was significantly increased, reaching up to 4.95 times higher as compared to the general population[44]. In a recently published study of 51,899 patients with newly-diagnosed rheumatoid arthritis, the hazard ratio of developing lung cancer in 4.5 years of follow-up was 1.39. This correlated to male gender and smoking but -surprisingly- not to the presence of ILD [45]. However, the presence of ILD is a significant risk factor for mortality in patients with rheumatoid arthritis who are also diagnosed with lung cancer: The estimated mortality of lung cancer in patients with chronic ILD with a UIP pattern was five times higher than the general population in a study of 2702 patients with rheumatoid arthritis [46]. Even the finding of ILAs in CT-screening has been associated with an increased risk of 33% of lung cancer [47]. Other studies have suggested HR of lung cancer diagnosis in patients with ILAs as high of 2.77 [48].
In a retrospective analysis of a large Medicare database of approximately 55,000 patients with NSCLC, the prevalence of IPF was 1.6% [49]. Studies from various regions consistently report elevated lung cancer prevalence in IPF patients compared to the general population, with rates ranging from 2.7% to 48%, with a median prevalence of 11.6% in European cohorts of patients with IPF and 15.3% in Asian cohorts [50]. In Korea the prevalence of lung cancer in IPF was reported to be 6.4% [51]. A recently published, European large multicenter study of 3178 patients with IPF reported development of lung cancer in 10.2% of the patients [52].
The cumulative incidence of lung cancer rises significantly over time in IPF patients, with rates of 1.1% at 1 year, 8.7% at 3 years, 15.9% at 5 years, and 31.1% at 10 years [53]. A longitudinal cohort study from Korea showcased a cumulative NSCLC incidence of 3.3%, 15.4%, and 54.7% at 1, 5, and 10 years post-IPF diagnosis, respectively[54]. In a large European study, the incidence of lung cancer in IPF was 14.1 and 26.6% among patients who were alive by the end of 3-year and 10-year follow-up, respectively [52]. The incidence of lung cancer in IPF cases is considerably higher compared to the general population, with reported rates ranging from 3.34 to nearly 5 [44,55]. In a study of NSCLC in patients with ILD, lung cancer was manifested approximately 2.4 years following ILD diagnosis [56].
Risk factors for lung cancer in ILDs include male gender, age, decreased lung function with a decline in FVC> 10% per year, low DLCO and smoking[53,57]. Combined pulmonary fibrosis and emphysema have a nine times increased risk of developing lung cancer, compared to subjects without underlying disease [58,59].
The most common histological type in patients with IPF is squamous carcinoma, followed by adenocarcinoma, contrary to the general population, in which adenocarcinoma is the most common histological type [51,60]. Mucinous adenocarcinoma has also been reported with increased frequency in patients with IPF [61]. Patients with IPF have a higher frequency of lung cancer occurrence in the lower lobes compared to other ILD patients and to the general population, who have a propensity for the upper lobes [52,60]. Patients with lung cancer and UIP histology predominantly exhibited subpleural lung cancer in the lower lobes (75.5%), consistent with the typical distribution pattern of UIP [52,62]. Squamous cell carcinoma was the most common cancer type (62.8%) in this group [52]. In contrast, in the non-UIP ILD group, lung cancer primarily occurred in the upper lobes (68.1%), with adenocarcinoma being the predominant cancer type (55.2%) [62].
The prognosis for NSCLC patients with concurrent IPF is poorer than for those with either condition alone, persisting even when adjusting for baseline lung function, with 5-year survival of 14.5% for lung cancer patients with IPF compared to 30.1% to those without [63]. This difference includes stages I-III of NSCLC, while in stage IV NSCLC and SCLC the survival difference is similarly low in IPF vs. non-IPF categories [63,64,65]. Survival outcomes vary based on ILD subtype, with lung cancer survival being poorer in patients with IPF compared to those with nonspecific interstitial pneumonia (NSIP) or cryptogenic organizing pneumonia (COP)[66,67,68].
4. Diagnostic Approach to the Patients with ILD and Suspected Lung Cancer
In individuals with ILD, diagnosis of lung cancer can be difficult, since clinical symptoms and functional changes can be attributed to the ILD, until lung cancer is suspected. Moreover, suspicious, subtle changes in chest CT- may be recognized later and on retrospective, due to the already existing fibrotic alterations of the lung (Figure 1) [52,53]. Careful comparison of CTs, in order to recognize new solitary nodules, is important. Since ILDs and particularly IPF is a risk factor for lung cancer development, annual HRCTs for follow-up of the IPF and eventual development of pulmonary nodules may be reasonable in these patients [69]. New pulmonary nodules should be further evaluated according to the high-risk group Fleischner criteria [69,70]. It is important to consider that the tumor size may be underestimated by 10% in patients with ILDs [71]. Additionally, evaluation of mediastinal lymph nodes with CT can be difficult in patients with ILD, since reactive mediastinal lymph node enlargement is common in these patients, therefore reducing the specificity of this method for detecting lung cancer [72,73].
For nodules with a size above 8 mm, most experts would agree that PET-CT can help to identify the malignant character of a nodule and provide information for possible, extra thoracic lung cancer involvement, accessible to biopsy [74,75,76]. Tissue sampling of suspicious mediastinal lymph nodes can be made using endobronchial ultrasound-guided transbronchial needle biopsy (EBUS-TBNB) and of peripheral lesions with radial EBUS [77]. The latter can be challenging due to the presence of fibrotic changes in the surrounding lung [77,78]. CT-guided transthoracic needle biopsy is an alternative, technically more difficult in patients with ILD, when the nodule is located in the lower lobes, due to motion artifacts and non-diagnostic results, due to sampling of fibrotic areas [79].
The approach described above might be more appropriate for patients with mild to medium lung functional impairment [80]. The approach to patients with end-stage fibrotic ILD, severely debilitated due to respiratory failure might be more conservative, since therapeutic options in these patients for lung cancer may be limited. A ‘liquid biopsy’, aiming to disclose driver mutations and to identify individual treatment in debilitated patients may also be taken into consideration. In all cases, shared decision making should be done with the patients [80].
Limitations of the diagnostic modalities in patients with ILDs, suspected of having lung cancer are presented in Table 1.
5. Treatment of NSCLC in Patients with ILDs
5.1. Surgical Therapy
Surgical resections in patients with ILD remain challenging, due to the fact that patients with ILD who are considered for surgical treatment of their malignancy often have an impaired lung function, advanced age and many comorbidities. Moreover, a surgical procedure is a risk factor for postoperative AE-ILD, which increases the perioperative mortality [81]. As a result, ILD per se is a risk factor for increased morbidity and mortality after lung resection for lung cancer [82]. A retrospective cohort analysis of 128,723 patients who underwent lung surgery for NSCLC, among them 1873 with ILD, showed a postoperative mortality of 5.1% in patients with ILD vs. 1.2% in patients without ILD, ARDS 1.9% in ILD vs. 0.5% without ILD and of composite morbidity and mortality of 13.2% in ILD vs. 7.4% without ILD [82]. ILD remained a predictor of mortality, even after adjustment for lung function, comorbidities and extent of resection [82].
Kumar et al. [83] reported an incidence of post-operative AE-ILD of 21%, with a mortality of 80% . The extent of surgical resection was also associated with mortality [83]. In a study of Park et al., the reported incidence of acute complications (ARDS and ALI) was 28% in 100 patients, with an overall operative mortality of 14%. Pre-existing comorbidities and reduced DLCO were associated with increased risk of AE-ILD in univariate analysis [84]. In a large, retrospective study from Japan, Sato et al. [85] analyzed data of 1763 patients with ILD who underwent pulmonary resections for lung cancer. The study showed an incidence of AE of 9,3% (164 patients) with a mortality rate of 43,9%. AE-ILD was the main cause of 30-day mortality, accounting for 72% of deaths. Risk factors for AE-ILD were male sex and history of previous AE-ILD. A UIP pattern in HRCT and an FVC value of <80% predicted were also identified as risk factors for AE-ILD [85]. Preoperative steroid use was associated with a 2,86 times increased ratio of AE-ILD. KL-6 serum levels above 1000 U/ml correlated to increased risk of AE-ILD (OR 2,14) [85]. Patients with CPFE have been reported to have an increased mortality comparable to the patients with emphysema alone. The incidence of AE-ILD was lower as in patients with IPF alone [86].
Min Seo Ki et al [87] demonstrated in a propensity score matching study of 104 patients that long term prognosis is affected negatively in ILD (5-year survival rate 66% vs 78.8%, P= .007), although there was no difference between groups in postoperative mortality [87]. Moreover, mortality was significantly higher in patients with a stage III ILD-GAP score [87]. A correlation of GAP score with mortality was also reported from Ueno et al. [88]. In the same study the degree of fibrosis in HRCT, increased BMI and a higher CRP were independently associated with mortality [88].
Regarding the range of the resection, most studies report an increased risk of complications, including AE-ILD with more extensive surgery [85]. Compared to a wedge resection, performance of lobectomy or segmentectomy had an OR of 3,83 and performance of a pneumonectomy or bilobectomy had an OR of 5,7 of AE-ILD [85]. Huang et al also showed that patients that underwent lobectomy or bilobectomy had a higher range of complications compared to the patients that underwent sublobar resections [81]. In this study the AE rate was 15,4% with a mortality of 9,0%. In the multivariate analysis however, age, comorbidities and blood loss but not the extent of surgery were the risk factors for 90-day complications [81]. Tsutani et al. [89], in a study of 107 patients with stage I NSCLC, showed no difference in overall survival between patients that underwent lobectomy and sublobar resections. The risk of a higher locoregional recovery by very limited resections can, however, not be ignored: regarding sublobar resections, Motono et al. showed that in patient with ILD and stage IA NSCLC, wedge resection is a poor prognostic factor and that a segmentectomy seems a better option [90]. Phase III randomized controlled trials are running to confirm the clinical effectiveness of sublobar resection such as wedge resection or segmentectomy for early NSCLC with IPF as compared to lobectomy, with primary endpoint being the overall survival [91]: a planned total of 430 patients will be enrolled from 50 institutions over 5 years [91]. In a recent meta-analysis of 2202 patients with UIP pattern, the overall incidence of AE of UIP postoperatively was 14.6% and sublobar resection was significantly associated with reduced risk of postoperative AE (OR 0.521)[92].
Apart from the extent of the surgical resection, the location of the resected lobe is another important factor regarding the post-operative course of patients with ILDs: Fukui et al [93] studied the difference between upper and lower lobectomy and concluded that there is no statistical difference in mortality and morbidity. This remained after adjusting for the concomitant presence of emphysema. However, upper lobectomy had a larger impact on postoperative respiratory function [93].
Repeated surgery in lung cancer patients with interstitial lung disease is rare and extremely challenging. Sato et al. showed in a small sample study (of 13 patients) that repeated surgery was associated with a high percentage of AE-IPF, but it could be beneficial in carefully selected patients [94].
An important aspect is the prevention of peri-operative AE-ILD. Pirfenidone is an antifibrotic agent, licensed for the treatment of patients with IPF. Iwata et al showed in a phase II trial that the use of perioperative pirfenidone was safe and had promising results for the prevention of AE-ILD [95]. In a retrospective study of 100 patients with IPF, who were surgically treated for lung cancer, patients treated with pirfenidone had fewer AE-IPF compared to the patients without antifibrotic treatment [96]. A prospective phase III study examining the effect of pirfenidone in preventing AE-IPF and survival is running [97].
5.2. Radiation Therapy
Radiation of the lesions in the lung is an integral part of the therapy in lung cancer. In general, it is indicated for patients with early-stage NSCLC, who are not surgical candidates, due to poor lung function or comorbidities, in cases of R1 surgical resection, as well in locally advanced NSCLC in combination with chemotherapy [98,99]. In SCLC, lung radiation therapy is indicated in limited disease [100]. Moreover, lung radiation therapy is indicated in urgent situations, such as superior vena cava syndrome [99]. Stereotactic body radiation therapy (SBRT) is the treatment of choice for non-surgical candidates with early-stage disease, due to the reduced risk of induced side-effects [99,101]. Radiation therapy, particularly when applied for locally advanced disease affects greater lung fields and requires higher radiation doses. A well-known side-effect of radiation therapy is radiation pneumonitis [102]. For this reason, patients with ILDs have been excluded from clinical trials of radiation therapy in patients with lung cancer [102].
Retrospective data suggest that the frequency of radiation pneumonitis in patients with ILDs is significantly higher than patients without ILD: A study involving 537 Stage I lung cancer patients treated with SBRT, including 39 patients with ILD-related imaging features, revealed that ILD patients had significantly higher rates of grade ≥2 (20.5% vs. 5.8%) and grade ≥3 (10.3% vs. 1.0%) radiation pneumonitis compared to non-ILD patients [103]. Moreover, ILD patients exhibited more extensive radiation pneumonitis beyond the radiotherapy treatment fields. A retrospective analysis of patients with Stage I lung cancer, including 6% with pre-existing ILD, found a significantly higher rate of severe radiation pneumonitis in ILD patients compared to the overall group [104]. Specifically, 32% of ILD patients experienced grade ≥3 radiation pneumonitis and 21% had grade 5 radiation pneumonitis [104]. In an analysis of 66 patients involving metastatic or primary tumors treated with SBRT, the presence of subclinical ILD was identified as the sole factor significantly linked to the occurrence of grade 2 to 5 radiation pneumonitis [105].
Preliminary data suggest that proton beam therapy (PBT) may be more advantageous compared to SBRT; particularly for patients with ILDs [106]. However, PBT is not widely available and large data series regarding its use in ILDs and lung cancer are missing.
The effect of radiation therapy in ILD was also studied in a retrospective study of 87 patients with subclinical ILD and NSCLC, treated with conventionally fractionated radiotherapy [107]. Most of the patients had Stage III NSCLC and received sequential chemoradiotherapy. Grade ≥2 radiation pneumonitis occurred in 51.7% of patients, while more severe radiation pneumonitis was associated with concurrent chemoradiotherapy. The mean lung dose, the ILD involvement and prior gemcitabine use were linked to increased risk of severe pneumonitis [107]. ILD involvement of >10% of lung field predicted acute development of radiation pneumonitis [108]. Increased SUV of the fibrotic lung in PET-CT has also been associated with increased frequency of radiation pneumonitis [109].
According to a systematic review trying to summarize the above aspects, the overall median incidence of grade ≥3 radiation pneumonitis in patients with ILDs undergoing radiation therapy for lung cancer was 19.7% (range 8-46%). Patients treated with particle beam therapy or stereotactic ablative radiotherapy had a lower incidence (median 12.5%) than those treated with conventional radical radiotherapy (31.8%). Grade 5 radiation pneumonitis occurred with a median rate of 11.9% (range: 0–60%). Severe radiation pneumonitis was independently predicted by the existence of ILD. When idiopathic pulmonary fibrosis (IPF) or the usual interstitial pneumonia (UIP) pattern were present, severe radiation pneumonitis was more common than when these conditions weren't [102].
Radiotherapy is not commonly utilized in patients with IPF due to its possible detrimental effects. According to a recently published retrospective, multicenter European study, only a small percentage of 12.5% of patients diagnosed with both IPF and lung cancer underwent radiotherapy [52]. However, physicians involved in the clinical care of patients with IPF and lung cancer would consider radiotherapy, particularly SBRT in carefully selected patients [80].
5.3. Percutaneous Ablation
Percutaneous image-guided ablation is a technique for the treatment of small tumors in early NSCLC, with results like sublobar resection and SBRT [110]. It can be applied as radiofrequency, microwave or cryoablation [110,111]. Due to the local effect, this approach might be of value in patients with ILDs [112], although data are scarce: mortality rates of 7.1% to 8.7% due to AE-ILD have been reported with a lung toxicity of 25% [113,114]. Complications, such as pneumothorax, bronchopleural fistula and pneumonia have been reported [112,115].
5.4. Systemic Therapy for Lung Cancer in Patients with ILDs
5.4.1. Chemotherapy
Chemotherapy plays a cardinal role in the treatment of patients with locally advanced and metastatic lung cancer [99,100]. Regarding NSCLC, histology and molecular markers are decisive for the appropriate treatment regimen selection. Before the introduction of immune checkpoint inhibitors (ICI), patients typically underwent first-line chemotherapy, often involving a platinum-based doublet regimen [116,117]. This regimen commonly included either carboplatin or cisplatin along with taxanes, etoposid or pemetrexed. Patients with ILDs have been mostly excluded from phase III controlled randomized trials examining the effect of systemic therapy in lung cancer. This was due to the possible risk of AE-ILD and drug-induced pneumonitis in patients with ILDs. However, case series, registries, phase II trials and a phase III trial (J-Sonic trial) have given insight to the effect of chemotherapy in patients with ILDs, and particularly IPF [71,118]. Patients with IPF and SCLC have a significantly higher incidence of AE-IPF compared to patients with IPF and NSCLC after first-line treatment (31% vs. 63%) [119]. A recent meta-analysis has shown that AE was significantly more common in IPF than in non-IPF ILD after chemotherapy [120]. Increased FDG avidity in the contralateral lung on FDG PET/CT has been reported to be correlated with the risk of chemotherapy-related AE and may assist in identifying high-risk patients [121]. Certain medications increase the risk of pneumotoxicity and AE-ILD. A meta-analysis of 684 patients with ILD who underwent first-line chemotherapy for NSCLC, showed a response rate of 43%. AE-ILD was approximately 8% in the context of chemotherapy, with lower rates (5%) observed in regimens containing nab-paclitaxel compared to other regimens (12%) [122]. For patients receiving docetaxel or gemcitabine, reported ILD exacerbation rates were 28% and 43%, respectively, while vinorelbine was not associated with AE-ILD in a small retrospective study [119]. Pemetrexed has shown increased toxicity in patients with IPF compared to those with other ILDs and significantly higher compared to patients without underlying ILD [123,124].
The above-mentioned data illustrate the effectiveness of first-line platinum doublet chemotherapy in patients with interstitial lung disease (ILD) [122]. Although the incidence of ILD exacerbation was generally less than 10% in most studies, some patients did experience fatal AE-ILD [122].
Targeted therapies, such as EGFR-tyrosine kinase inhibitors or anaplastic lymphoma kinase inhibitors (ALK) have been associated with pneumotoxicity [125]. Some studies suggest that targeted therapies might be associated with increased risk of pneumotoxicity in patients with pre-existing ILD [126]. However, no large studies evaluating these treatments in patients with underlying ILD exist.
Nintedanib is a tyrosine-kinase inhibitor which exhibits its antiangiogenic properties through targeting vascular endothelial growth factor receptor (VEGF), fibroblast growth factor (FGF)receptor and platelet-derived growth factor (PDGF) receptor. In combination with docetaxel, it is used as a second line therapy in patients diagnosed with adenocarcinoma, after failure of first line chemotherapy [127]. Nintedanib has also been approved for the treatment of IPF as it was shown that it slows down the progression of disease and reduces the risk of acute exacerbation at a dose of 150mg bid [128].
There were observations in patients with NSCLC and IPF who received nintedanib for the treatment of progression of IPF, while chemotherapy for cancer had failed, that a reduction of the size of cancerous lesions was achieved as well, while lung function was preserved. The doses used for treatment were 100 to150 bid [129,130,131,132]. In an attempt to examine the optimal treatment for patients with lung cancer and IPF, a randomized phase 3 trial (J-SONIC) compared the efficacy and safety of nintedanib plus chemotherapy to chemotherapy alone [118].In this study, the primary end-point, which was exacerbation-free survival, was not met as there was no significant difference between the two groups. The combination of nintedanib with chemotherapy was well tolerated and prevented FVC decline at 12 weeks. Overall Response Rate (ORR) was significantly improved for nintedanib plus chemo vs chemotherapy in patients with nonsquamous histology [118]. Overall survival was improved only in patients with nonsquamous histology and patients with GAP (gender-age-physiology) stage I [118].
5.4.2. Immunotherapy
Management of lung cancer in patients with ILD is notably difficult. While standard of care in patients with advanced or metastatic NSCLC is a combination of a platinum- based doublet with immunotherapy [98], patients with ILDs are faced with skepticism in the fear of adverse events. Immunotherapy refers to immune checkpoint inhibitors (ICIs) and includes PD-1 inhibitors (such as nivolumab and pembrolizumab) and PD-L1 inhibitors such as atezolizumab and durvalumab). Adverse events can occur at any time in any organ [141] but particularly ICI-related pneumonitis which in the context of IPF could be devastating due to their altered lung function, is the reason why patients with IPF are excluded from the majority of the studies. However, in patients without ILDs and NSCLs, immune-related adverse effects correlate to better outcome [142]. Patients with ILD and lung cancer have similar levels of PD-L1 compared to the ones without ILD and increased tissue levels of PD-L1 are associated with better outcomes [143]. Other studies however report that PD-1 expression was increased, while PD-L1 expression was decreased, in mediastinal lymph nodes of patients with IPF compared to lung cancer and in IPF lungs compared to control lungs [73]. Mediastinal lymph nodes of bleomycin-treated mice showed increased size and higher PD-1, PD-L1 mRNA levels compared to controls, while pembrolizumab attenuated bleomycin-induced fibrosis [73].
Monotherapy with ICIs for patients with NSCLC without ILD has an incidence of pneumonitis between 3%-6% which rises up to 10% when ICIs are combined [144]. The incidence of pneumonitis in IPF is estimated between 7.3% and 42.9% with the data coming from retrospective studies including patients with NSCLC and IPF or ILA [145]. As it was shown in a retrospective study with 123 patients with NSCLC treated with nivolumab and pembrolizumab, when fibrosis score, defined visually in CT-scan according to the classification of Kazerooni et al. [146], increased from zero to >/ 1, the incidence of pneumonitis increased from 5.8% to 35.1% [147]. Increased fibrosis score and ground glass opacities are reported as risk factors for the development of ICI-related pneumonitis in some studies [147,148,149]. A multicenter retrospective study from Japan which included 200 patients with chronic interstitial pneumonia who were treated with ICIs, showed pneumonitis grades 3–5 in 15.5% and death in 4.5% of the patients. Pneumonitis manifested radiologically preferentially as organising pneumonia (OP) (47.5%) while diffuse alveolar damage (DAD) pattern was observed in 31.1% of the patients; DAD patients had a significantly worse prognosis than those with a non-DAD pattern. Immune-related adverse events occurred in approximately 50% of patients. Patients with adverse effects had a better prognosis than those without (median PFS 200 days versus 77 days, p<0.001; median OS 597 days versus 390 days p=0.0074). The objective response rate and disease control rate were 41.3% and 68.5%, respectively [150]. A meta-analysis of 179 patients in 10 studies with pre-existing ILD treated with ICIs for NSCLC showed that the overall response rate in patients with preexisting ILD was significantly higher than that in patients without ILD (OR, 1.99; 95% CI, 1.31-3.00) and the disease-control rate and progression-free survival in patients with preexisting ILD were not inferior to those without ILD. The meta-analysis found a significantly higher incidence rate of any grade and grade 3 or higher CIP in patients with NSCLC and preexisting ILD than in those patients without ILD (OR, 3.23; OR, 2.91) [151].
Case reports and a pilot study where nivolumab was administered as second-line therapy to patients with lung cancer and concomitant IPF after first line chemotherapy failed, suggested that nivolumab might be safely used in these patients. No signs of pneumonitis were observed during 12 weeks of treatment and efficacy showed partial response or stable disease [152,153] . A multicenter open-label single-arm phase II trial followed in order to evaluate the efficacy and safety of nivolumab in patients with mild IPF and NSCLC: grade 2 pneumonitis was seen in 11% of the patients. The 6 months PFS rates was 56%, response rate was 39% and disease control rate was 72% [154]. These results are corroborated by another retrospective study with 461 patients (412 without ILD and 49 with ILD) who were treated with nivolumab or pembrolizumab, which showed that despite the increased frequency of pneumonitis, the response rate (RR), the disease control rate (DCR), the progression free survival (PFS) and the overall survival (OS) were non-inferior in the ILD-NSCLC group than the patients with NSCLC without pre-existing ILD [155].
Most of the published case reports and original studies included Asian populations: in these patients, increased risk of AE-ILD and chemotherapy-associated toxicity, including EGFR and TKI treatment has been reported [156]. Therefore, additional studies in populations of other ethnic origins are useful for comparison and extrapolation of the previous reported results. In a retrospective French study of 10,452 patients with advanced NSCLC who were treated with nivolumab, the effect of immunotherapy was examined in 148 patients (1.4%) with ILD. The overall survival time and the time- to- treatment duration was similar between patients with and without ILDs [157]. Survival was similar in patients with idiopathic ILD, autoimmune/ granulomatous ILD and ILDs of other known cause, although the results should be interpreted with caution due to the small numbers in the different groups [157].
Although hesitancy to use immunotherapy in this group of patients is explained by the minimal, mostly retrospective research into the field, ICIs can be used in this population after assessing risks and benefits, so that therapy is tailored to the individual patient.
Treatment options for patients with NSCLC and ILDs are summarized in Table 2.
6. Treatment Options for SCLC Patients with ILD
SCLC is less common as NSCLC in patients with ILDs, accounting for approximately 20% of lung cancers [158]. Most reports suggest that the presence of ILD, and particularly of IPF, is associated with reduced overall survival [159,160,161,162]. Individuals diagnosed with SCLC and ILD exhibit similar responses to standard treatment to the general population, provided they tolerate chemotherapy [159,160,163]. Pneumonitis was more often seen in patients with ILD and was associated with worse survival [160,164].
A phase II study of 33 recruited patients with unresectable SCLC and IPF, examining the safety and efficacy of carboplatin, etoposide and nintedanib was recently Published: the incidence of AE-IPF after chemotherapy was 3% with an ORR of 68.8%, PFS of 4.2 months and overall survival of 13.4 months, suggesting a role for nintedanib in preventing AE-IPF due to chemotherapy [165].
7. Palliative Care
Patients with fibrotic ILDs, and particularly IPF, have a dismal prognosis. The combination of fibrotic ILDs with lung cancer is a difficult situation for the patient, as well as for the treating physician. Impaired lung function, the risk of AE and pneumonitis, and comorbidities make many patients unfit or too frail for the usual therapeutic choices in the general population. The results of the DIAMORFOSIS study underline this problem [80]. Palliative treatment refers not only to pre-mortal interventions. Palliative treatment can greatly help alleviate patient´s symptoms in an early stage, particularly dyspnea, cough and pain. Therefore, open discussion with the patients and their families is of paramount importance for improving their quality of life.
8. Conclusions
The relationship between lung cancer and ILD underscores the complexity of treatment decisions and potential complications. Retrospective studies have revealed varying rates of pneumonitis, including AE-ILD, in patients with ILD undergoing different therapeutic approaches for lung cancer. Factors such as the extent of ILD involvement, surgical resection, radiation dose, and specific chemotherapy agents have been identified as significant contributors to the mortality risk due to complications in these patients. These findings emphasize the need for careful consideration of treatment modalities and personalized approaches for individuals with both lung cancer and ILD. Future research and prospective studies are essential to refine treatment guidelines and enhance our understanding of the optimal management strategies for this complex patient population.
Author Contributions
Conceptualization, P.S. and F.D.; writing—original draft preparation, all authors.; writing—review and editing, P.S., A.G, F.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wijsenbeek, M.; Suzuki, A.; Maher, T.M. Interstitial lung diseases. The Lancet 2022, 400, 769–786. [Google Scholar] [CrossRef] [PubMed]
- Pardo, A.; Selman, M. The Interplay of the Genetic Architecture, Aging, and Environmental Factors in the Pathogenesis of Idiopathic Pulmonary Fibrosis. American Journal of Respiratory Cell and Molecular Biology 2021, 64, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Fang, Z.; Meng, Q.; Xu, J.; Wang, W.; Zhang, B.; Liu, J.; Liang, C.; Hua, J.; Zhao, Y.; Yu, X.; et al. Signaling pathways in cancer-associated fibroblasts: recent advances and future perspectives. Cancer Communications 2023, 43, 3–41. [Google Scholar] [CrossRef] [PubMed]
- Karampitsakos, T.; Tzilas, V.; Tringidou, R.; Steiropoulos, P.; Aidinis, V.; Papiris, S.A.; Bouros, D.; Tzouvelekis, A. Lung cancer in patients with idiopathic pulmonary fibrosis. Pulmonary Pharmacology & Therapeutics 2017, 45, 1–10. [Google Scholar] [CrossRef]
- Daniels, C.E.; Jett, J.R. Does interstitial lung disease predispose to lung cancer? Current Opinion in Pulmonary Medicine 2005, 11, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Archontogeorgis, K.; Steiropoulos, P.; Tzouvelekis, A.; Nena, E.; Bouros, D. Lung cancer and interstitial lung diseases: a systematic review. Pulm Med 2012, 2012, 315918. [Google Scholar] [CrossRef] [PubMed]
- Ballester, B.; Milara, J.; Cortijo, J. Idiopathic Pulmonary Fibrosis and Lung Cancer: Mechanisms and Molecular Targets. International Journal of Molecular Sciences 2019, 20, 593. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, K.M.; Tomassetti, S.; Tsitoura, E.; Vancheri, C. Idiopathic pulmonary fibrosis and lung cancer. Current Opinion in Pulmonary Medicine 2015, 21, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, L.E.L.; Drent, M.; van Haren, E.H.J.; Verschakelen, J.A.; Verleden, G.M. Lung cancer in idiopathic pulmonary fibrosis patients diagnosed during or after lung transplantation. Respiratory Medicine Case Reports 2012, 5, 37–39. [Google Scholar] [CrossRef]
- Tzouvelekis, A.; Gomatou, G.; Bouros, E.; Trigidou, R.; Tzilas, V.; Bouros, D. Common Pathogenic Mechanisms Between Idiopathic Pulmonary Fibrosis and Lung Cancer. Chest 2019, 156, 383–391. [Google Scholar] [CrossRef]
- Li, J.; Yang, M.; Li, P.; Su, Z.; Gao, P.; Zhang, J. Idiopathic pulmonary fibrosis will increase the risk of lung cancer. Chin Med J (Engl) 2014, 127, 3142–3149. [Google Scholar]
- Global Burden of Disease Cancer, C.; Kocarnik, J.M.; Compton, K.; Dean, F.E.; Fu, W.; Gaw, B.L.; Harvey, J.D.; Henrikson, H.J.; Lu, D.; Pennini, A.; et al. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol 2022, 8, 420–444. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, G.B.D.C.R.D. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the Global Burden of Disease Study 2019. EClinicalMedicine 2023, 59, 101936. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.-F.; Flaherty, K.R.; Lasky, J.A.; et al. An Official ATS/ERS/JRS/ALAT Statement: Idiopathic Pulmonary Fibrosis: Evidence-based Guidelines for Diagnosis and Management. American Journal of Respiratory and Critical Care Medicine 2011, 183, 788–824. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Wu, W.; Chen, N.; Song, H.; Lu, T.; Yang, Z.; Wang, Z.; Zhou, J.; Liu, L. Clinical characteristics and outcomes of lung cancer patients with combined pulmonary fibrosis and emphysema: a systematic review and meta-analysis of 13 studies. Journal of Thoracic Disease 2017, 9, 5322–5334. [Google Scholar] [CrossRef]
- Todd, N.W.; Luzina, I.G.; Atamas, S.P. Molecular and cellular mechanisms of pulmonary fibrosis. Fibrogenesis & Tissue Repair 2012, 5. [Google Scholar] [CrossRef] [PubMed]
- Armanios, M.Y.; Chen, J.J.L.; Cogan, J.D.; Alder, J.K.; Ingersoll, R.G.; Markin, C.; Lawson, W.E.; Xie, M.; Vulto, I.; Phillips, J.A.; et al. Telomerase Mutations in Families with Idiopathic Pulmonary Fibrosis. New England Journal of Medicine 2007, 356, 1317–1326. [Google Scholar] [CrossRef]
- Demopoulos, K.; Arvanitis, D.A.; Vassilakis, D.A.; Siafakas, N.M.; Spandidos, D.A. MYCL1, FHIT, SPARC, p16 INK4 and TP53 genes associated to lung cancer in idiopathic pulmonary fibrosis. Journal of Cellular and Molecular Medicine 2002, 6, 215–222. [Google Scholar] [CrossRef]
- Liu, T.; Chung, M.J.; Ullenbruch, M.; Yu, H.; Jin, H.; Hu, B.; Choi, Y.Y.; Ishikawa, F.; Phan, S.H. Telomerase activity is required for bleomycin-induced pulmonary fibrosis in mice. Journal of Clinical Investigation 2007. [Google Scholar] [CrossRef]
- Selman, M.; Pardo, A. Role of epithelial cells in idiopathic pulmonary fibrosis: from innocent targets to serial killers. Proc Am Thorac Soc 2006, 3, 364–372. [Google Scholar] [CrossRef]
- O'Callaghan, D.S.; O'Donnell, D.; O'Connell, F.; O'Byrne, K.J. The Role of Inflammation in the Pathogenesis of Non-small Cell Lung Cancer. Journal of Thoracic Oncology 2010, 5, 2024–2036. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.G.; Simpson, J.K.; Saini, G.; Bentley, J.H.; Russell, A.-M.; Braybrooke, R.; Molyneaux, P.L.; McKeever, T.M.; Wells, A.U.; Flynn, A.; et al. Longitudinal change in collagen degradation biomarkers in idiopathic pulmonary fibrosis: an analysis from the prospective, multicentre PROFILE study. The Lancet Respiratory Medicine 2015, 3, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, I.E.; Eickelberg, O. The Impact of TGF-β on Lung Fibrosis. Proceedings of the American Thoracic Society 2012, 9, 111–116. [Google Scholar] [CrossRef]
- Selman, M.s.; Thannickal, V.J.; Pardo, A.; Zisman, D.A.; Martinez, F.J.; Lynch, J.P. Idiopathic Pulmonary Fibrosis. Drugs 2004, 64, 405–430. [Google Scholar] [CrossRef] [PubMed]
- Oikonomidi, I.; Burbridge, E.; Cavadas, M.; Sullivan, G.; Collis, B.; Naegele, H.; Clancy, D.; Brezinova, J.; Hu, T.; Bileck, A.; et al. iTAP, a novel iRhom interactor, controls TNF secretion by policing the stability of iRhom/TACE. eLife 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Grimminger, F.; Schermuly, R.T.; Ghofrani, H.A. Targeting non-malignant disorders with tyrosine kinase inhibitors. Nature Reviews Drug Discovery 2010, 9, 956–970. [Google Scholar] [CrossRef] [PubMed]
- Rabinovich, E.I.; Kapetanaki, M.G.; Steinfeld, I.; Gibson, K.F.; Pandit, K.V.; Yu, G.; Yakhini, Z.; Kaminski, N. Global Methylation Patterns in Idiopathic Pulmonary Fibrosis. PLoS ONE 2012, 7, e33770. [Google Scholar] [CrossRef]
- Zhang, Q.; Yu, N.; Lee, C. Mysteries of TGF-b Paradox in Benign and Malignant Cells. Frontiers in Oncology 2014, 4. [Google Scholar] [CrossRef]
- Malli, F.; Koutsokera, A.; Paraskeva, E.; Zakynthinos, E.; Papagianni, M.; Makris, D.; Tsilioni, I.; Molyvdas, P.A.; Gourgoulianis, K.I.; Daniil, Z. Endothelial Progenitor Cells in the Pathogenesis of Idiopathic Pulmonary Fibrosis: An Evolving Concept. PLoS ONE 2013, 8, e53658. [Google Scholar] [CrossRef]
- Abu Qubo, A.; Numan, J.; Snijder, J.; Padilla, M.; Austin, J.H.M.; Capaccione, K.M.; Pernia, M.; Bustamante, J.; O'Connor, T.; Salvatore, M.M. Idiopathic pulmonary fibrosis and lung cancer: future directions and challenges. Breathe 2022, 18, 220147. [Google Scholar] [CrossRef]
- Kinoshita, T.; Goto, T. Molecular Mechanisms of Pulmonary Fibrogenesis and Its Progression to Lung Cancer: A Review. International Journal of Molecular Sciences 2019, 20, 1461. [Google Scholar] [CrossRef] [PubMed]
- Patsoukis, N.; Wang, Q.; Strauss, L.; Boussiotis, V.A. Revisiting the PD-1 pathway. Science Advances 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Organ, S.L.; Tsao, M.-S. An overview of the c-MET signaling pathway. Therapeutic Advances in Medical Oncology 2011, 3, S7–S19. [Google Scholar] [CrossRef] [PubMed]
- Stella, G.M.; Gentile, A.; Balderacchi, A.; Meloni, F.; Milan, M.; Benvenuti, S. Ockham’s razor for the MET-driven invasive growth linking idiopathic pulmonary fibrosis and cancer. Journal of Translational Medicine 2016, 14. [Google Scholar] [CrossRef] [PubMed]
- Kuwano, K.; Araya, J.; Hara, H.; Minagawa, S.; Takasaka, N.; Ito, S.; Kobayashi, K.; Nakayama, K. Cellular senescence and autophagy in the pathogenesis of chronic obstructive pulmonary disease (COPD) and idiopathic pulmonary fibrosis (IPF). Respiratory Investigation 2016, 54, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research, N. Comprehensive molecular profiling of lung adenocarcinoma. Nature 2014, 511, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Kidera, Y.; van Tsubaki, M.; Yamazoe, Y.; Shoji, K.; Nakamura, H.; Ogaki, M.; Satou, T.; Itoh, T.; Isozaki, M.; Kaneko, J.; et al. Reduction of lung metastasis, cell invasion, and adhesion in mouse melanoma by statin-induced blockade of the Rho/Rho-associated coiled-coil-containing protein kinase pathway. Journal of Experimental & Clinical Cancer Research 2010, 29. [Google Scholar] [CrossRef]
- Kim, K.K.; Kugler, M.C.; Wolters, P.J.; Robillard, L.; Galvez, M.G.; Brumwell, A.N.; Sheppard, D.; Chapman, H.A. Alveolar epithelial cell mesenchymal transition develops in vivo during pulmonary fibrosis and is regulated by the extracellular matrix. Proceedings of the National Academy of Sciences 2006, 103, 13180–13185. [Google Scholar] [CrossRef]
- Lovat, F.; Valeri, N.; Croce, C.M. MicroRNAs in the Pathogenesis of Cancer. Seminars in Oncology 2011, 38, 724–733. [Google Scholar] [CrossRef]
- Schwarzenbach, H.; Hoon, D.S.B.; Pantel, K. Cell-free nucleic acids as biomarkers in cancer patients. Nature Reviews Cancer 2011, 11, 426–437. [Google Scholar] [CrossRef]
- Trovato-Salinaro, A.; Trovato-Salinaro, E.; Failla, M.; Mastruzzo, C.; Tomaselli, V.; Gili, E.; Crimi, N.; Condorelli, F.D.; Vancheri, C. Altered intercellular communication in lung fibroblast cultures from patients with idiopathic pulmonary fibrosis. Respiratory Research 2006, 7. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.I.; Park, J.S.; Lee, M.Y.; Park, B.; Kim, H.J.; Park, S.H.; Choi, W.I.; Lee, C.W. Prevalence of lung cancer in patients with interstitial lung disease is higher than in those with chronic obstructive pulmonary disease. Medicine (Baltimore) 2018, 97, e0071. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.I.; Lee, D.Y.; Choi, H.G.; Lee, C.W. Lung Cancer development and mortality in interstitial lung disease with and without connective tissue diseases: a five-year Nationwide population-based study. Respir Res 2019, 20, 117. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Nouraie, M.; Chen, X.; Zou, R.H.; Sellares, J.; Veraldi, K.L.; Chiarchiaro, J.; Lindell, K.; Wilson, D.O.; Kaminski, N.; et al. Characteristics of lung cancer among patients with idiopathic pulmonary fibrosis and interstitial lung disease - analysis of institutional and population data. Respir Res 2018, 19, 195. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.H.; Cho, J.H.; Eun, Y.; Han, K.; Jung, J.; Cho, I.Y.; Yoo, J.E.; Lee, H.; Kim, H.; Park, S.Y.; et al. Rheumatoid Arthritis and Risk of Lung Cancer: A Nationwide Cohort Study. J Thorac Oncol 2024, 19, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Kakutani, T.; Hashimoto, A.; Tominaga, A.; Kodama, K.; Nogi, S.; Tsuno, H.; Ogihara, H.; Nunokawa, T.; Komiya, A.; Furukawa, H.; et al. Related factors, increased mortality and causes of death in patients with rheumatoid arthritis-associated interstitial lung disease. Mod Rheumatol 2020, 30, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Whittaker Brown, S.A.; Padilla, M.; Mhango, G.; Powell, C.; Salvatore, M.; Henschke, C.; Yankelevitz, D.; Sigel, K.; de-Torres, J.P.; Wisnivesky, J. Interstitial Lung Abnormalities and Lung Cancer Risk in the National Lung Screening Trial. Chest 2019, 156, 1195–1203. [Google Scholar] [CrossRef]
- Axelsson, G.T.; Putman, R.K.; Aspelund, T.; Gudmundsson, E.F.; Hida, T.; Araki, T.; Nishino, M.; Hatabu, H.; Gudnason, V.; Hunninghake, G.M.; et al. The associations of interstitial lung abnormalities with cancer diagnoses and mortality. Eur Respir J 2020, 56. [Google Scholar] [CrossRef]
- Whittaker Brown, S.A.; Padilla, M.; Mhango, G.; Taioli, E.; Powell, C.; Wisnivesky, J. Outcomes of Older Patients with Pulmonary Fibrosis and Non-Small Cell Lung Cancer. Ann Am Thorac Soc 2019, 16, 1034–1040. [Google Scholar] [CrossRef]
- Brown, S.W.; Dobelle, M.; Padilla, M.; Agovino, M.; Wisnivesky, J.P.; Hashim, D.; Boffetta, P. Idiopathic Pulmonary Fibrosis and Lung Cancer. A Systematic Review and Meta-analysis. Ann Am Thorac Soc 2019, 16, 1041–1051. [Google Scholar] [CrossRef]
- Song, M.J.; Kim, S.Y.; Park, M.S.; Kang, M.J.; Lee, S.H.; Park, S.C. A nationwide population-based study of incidence and mortality of lung cancer in idiopathic pulmonary fibrosis. Sci Rep 2021, 11, 2596. [Google Scholar] [CrossRef] [PubMed]
- Karampitsakos, T.; Spagnolo, P.; Mogulkoc, N.; Wuyts, W.A.; Tomassetti, S.; Bendstrup, E.; Molina-Molina, M.; Manali, E.D.; Unat, O.S.; Bonella, F.; et al. Lung cancer in patients with idiopathic pulmonary fibrosis: A retrospective multicentre study in Europe. Respirology 2023, 28, 56–65. [Google Scholar] [CrossRef]
- Yoo, H.; Jeong, B.H.; Chung, M.J.; Lee, K.S.; Kwon, O.J.; Chung, M.P. Risk factors and clinical characteristics of lung cancer in idiopathic pulmonary fibrosis: a retrospective cohort study. BMC Pulm Med 2019, 19, 149. [Google Scholar] [CrossRef]
- Ozawa, Y.; Suda, T.; Naito, T.; Enomoto, N.; Hashimoto, D.; Fujisawa, T.; Nakamura, Y.; Inui, N.; Nakamura, H.; Chida, K. Cumulative incidence of and predictive factors for lung cancer in IPF. Respirology 2009, 14, 723–728. [Google Scholar] [CrossRef]
- Le Jeune, I.; Gribbin, J.; West, J.; Smith, C.; Cullinan, P.; Hubbard, R. The incidence of cancer in patients with idiopathic pulmonary fibrosis and sarcoidosis in the UK. Respir Med 2007, 101, 2534–2540. [Google Scholar] [CrossRef]
- Barczi, E.; Nagy, T.; Starobinski, L.; Kolonics-Farkas, A.; Eszes, N.; Bohacs, A.; Tarnoki, A.D.; Tarnoki, D.L.; Muller, V. Impact of interstitial lung disease and simultaneous lung cancer on therapeutic possibilities and survival. Thorac Cancer 2020, 11, 1911–1917. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Saeki, K.; Waseda, Y.; Murata, A.; Takato, H.; Ichikawa, Y.; Yasui, M.; Kimura, H.; Hamaguchi, Y.; Matsushita, T.; et al. Lung cancer in connective tissue disease-associated interstitial lung disease: clinical features and impact on outcomes. J Thorac Dis 2018, 10, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Jiang, Y. Meta-analysis: clinical features and treatments of lung cancer in combined pulmonary fibrosis and emphysema. Sarcoidosis Vasc Diffuse Lung Dis 2023, 40, e2023045. [Google Scholar] [CrossRef]
- Koo, H.J.; Do, K.H.; Lee, J.B.; Alblushi, S.; Lee, S.M. Lung Cancer in Combined Pulmonary Fibrosis and Emphysema: A Systematic Review and Meta-Analysis. PLoS One 2016, 11, e0161437. [Google Scholar] [CrossRef]
- Tomassetti, S.; Gurioli, C.; Ryu, J.H.; Decker, P.A.; Ravaglia, C.; Tantalocco, P.; Buccioli, M.; Piciucchi, S.; Sverzellati, N.; Dubini, A.; et al. The impact of lung cancer on survival of idiopathic pulmonary fibrosis. Chest 2015, 147, 157–164. [Google Scholar] [CrossRef]
- Masai, K.; Tsuta, K.; Motoi, N.; Shiraishi, K.; Furuta, K.; Suzuki, S.; Asakura, K.; Nakagawa, K.; Sakurai, H.; Watanabe, S.I.; et al. Clinicopathological, Immunohistochemical, and Genetic Features of Primary Lung Adenocarcinoma Occurring in the Setting of Usual Interstitial Pneumonia Pattern. J Thorac Oncol 2016, 11, 2141–2149. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Kawabata, Y.; Koyama, N.; Ikeya, T.; Hoshi, E.; Takayanagi, N.; Koyama, S. A clinicopathological study of surgically resected lung cancer in patients with usual interstitial pneumonia. Respir Med 2017, 129, 158–163. [Google Scholar] [CrossRef]
- Kim, H.C.; Lee, S.; Song, J.W. Impact of idiopathic pulmonary fibrosis on clinical outcomes of lung cancer patients. Sci Rep 2021, 11, 8312. [Google Scholar] [CrossRef] [PubMed]
- Mauclet, C.; Dupont, M.V.; Roelandt, K.; Regnier, M.; Delos, M.; Pirard, L.; Vander Borght, T.; Dahlqvist, C.; Froidure, A.; Rondelet, B.; et al. Treatment and Prognosis of Patients with Lung Cancer and Combined Interstitial Lung Disease. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Alomaish, H.; Ung, Y.; Wang, S.; Tyrrell, P.N.; Zahra, S.A.; Oikonomou, A. Survival analysis in lung cancer patients with interstitial lung disease. PLoS One 2021, 16, e0255375. [Google Scholar] [CrossRef] [PubMed]
- Azuma, Y.; Sakamoto, S.; Homma, S.; Sano, A.; Sakai, T.; Koezuka, S.; Otsuka, H.; Tochigi, N.; Kishi, K.; Iyoda, A. Impact of accurate diagnosis of interstitial lung diseases on postoperative outcomes in lung cancer. Gen Thorac Cardiovasc Surg 2023, 71, 129–137. [Google Scholar] [CrossRef]
- Maeda, H.; Kanzaki, M.; Sakamoto, K.; Isaka, T.; Oyama, K.; Murasugi, M.; Onuki, T. Effect of collagen vascular disease-associated interstitial lung disease on the outcomes of lung cancer surgery. Surg Today 2017, 47, 1072–1079. [Google Scholar] [CrossRef]
- Kreuter, M.; Ehlers-Tenenbaum, S.; Schaaf, M.; Oltmanns, U.; Palmowski, K.; Hoffmann, H.; Schnabel, P.A.; Heussel, C.P.; Puderbach, M.; Herth, F.J.; et al. Treatment and outcome of lung cancer in idiopathic interstitial pneumonias. Sarcoidosis Vasc Diffuse Lung Dis 2015, 31, 266–274. [Google Scholar] [PubMed]
- Tzouvelekis, A.; Spagnolo, P.; Bonella, F.; Vancheri, C.; Tzilas, V.; Crestani, B.; Kreuter, M.; Bouros, D. Patients with IPF and lung cancer: diagnosis and management. Lancet Respir Med 2018, 6, 86–88. [Google Scholar] [CrossRef]
- Bueno, J.; Landeras, L.; Chung, J.H. Updated Fleischner Society Guidelines for Managing Incidental Pulmonary Nodules: Common Questions and Challenging Scenarios. Radiographics 2018, 38, 1337–1350. [Google Scholar] [CrossRef]
- Naccache, J.M.; Gibiot, Q.; Monnet, I.; Antoine, M.; Wislez, M.; Chouaid, C.; Cadranel, J. Lung cancer and interstitial lung disease: a literature review. J Thorac Dis 2018, 10, 3829–3844. [Google Scholar] [CrossRef] [PubMed]
- Sgalla, G.; Larici, A.R.; Golfi, N.; Calvello, M.; Farchione, A.; Del Ciello, A.; Varone, F.; Iovene, B.; Manfredi, R.; Richeldi, L. Mediastinal lymph node enlargement in idiopathic pulmonary fibrosis: relationships with disease progression and pulmonary function trends. BMC Pulm Med 2020, 20, 249. [Google Scholar] [CrossRef] [PubMed]
- Karampitsakos, T.; Galaris, A.; Chrysikos, S.; Papaioannou, O.; Vamvakaris, I.; Barbayianni, I.; Kanellopoulou, P.; Grammenoudi, S.; Anagnostopoulos, N.; Stratakos, G.; et al. Expression of PD-1/PD-L1 axis in mediastinal lymph nodes and lung tissue of human and experimental lung fibrosis indicates a potential therapeutic target for idiopathic pulmonary fibrosis. Respir Res 2023, 24, 279. [Google Scholar] [CrossRef] [PubMed]
- Jeon, T.Y.; Lee, K.S.; Yi, C.A.; Chung, M.P.; Kwon, O.J.; Kim, B.T.; Shim, Y.M. Incremental value of PET/CT Over CT for mediastinal nodal staging of non-small cell lung cancer: Comparison between patients with and without idiopathic pulmonary fibrosis. AJR Am J Roentgenol 2010, 195, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Sung, C.; Lee, H.S.; Yoon, H.Y.; Kim, S.J.; Oh, J.S.; Song, J.W.; Kim, M.Y.; Ryu, J.S. Is (18)F-FDG PET/CT useful for the differential diagnosis of solitary pulmonary nodules in patients with idiopathic pulmonary fibrosis? Ann Nucl Med 2018, 32, 492–498. [Google Scholar] [CrossRef]
- Nomura, K.; Fukui, M.; Hattori, A.; Matsunaga, T.; Takamochi, K.; Suzuki, K. Diagnostic Value of Nodal Staging of Lung Cancer With Usual Interstitial Pneumonia Using PET. Ann Thorac Surg 2022, 114, 2073–2079. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, C.; Seol, H.Y.; Chung, H.S.; Mok, J.; Lee, G.; Jo, E.J.; Kim, M.H.; Lee, K.; Kim, K.U.; et al. Safety and Diagnostic Yield of Radial Probe Endobronchial Ultrasound-Guided Biopsy for Peripheral Lung Lesions in Patients with Idiopathic Pulmonary Fibrosis: A Multicenter Cross-Sectional Study. Respiration 2022, 101, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Nogawa, H.; Matsumoto, Y.; Tanaka, M.; Tsuchida, T. Diagnostic usefulness of bronchoscopy for peripheral pulmonary lesions in patients with idiopathic pulmonary fibrosis. J Thorac Dis 2021, 13, 6304–6313. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.J.; Yun, G.; Yoon, S.H.; Song, H.; Kim, J.; Kim, J.; Park, J.S.; Lee, K.W.; Lee, K.H. Accuracy and complications of percutaneous transthoracic needle lung biopsy for the diagnosis of malignancy in patients with idiopathic pulmonary fibrosis. Eur Radiol 2021, 31, 9000–9011. [Google Scholar] [CrossRef] [PubMed]
- Tzouvelekis, A.; Antoniou, K.; Kreuter, M.; Evison, M.; Blum, T.G.; Poletti, V.; Grigoriu, B.; Vancheri, C.; Spagnolo, P.; Karampitsakos, T.; et al. The DIAMORFOSIS (DIAgnosis and Management Of lung canceR and FibrOSIS) survey: international survey and call for consensus. ERJ Open Res 2021, 7. [Google Scholar] [CrossRef]
- Huang, C.; Sun, Y.G.; Ma, C.; Jiao, P.; Wu, Q.J.; Tian, W.X.; Yu, H.B.; Tong, H.F. Surgical outcomes and perioperative risk factors of patients with interstitial lung disease after pulmonary resection. J Cardiothorac Surg 2024, 19, 72. [Google Scholar] [CrossRef] [PubMed]
- Axtell, A.L.; David, E.A.; Block, M.I.; Parsons, N.; Habib, R.; Muniappan, A. Association Between Interstitial Lung Disease and Outcomes After Lung Cancer Resection. Ann Thorac Surg 2023, 116, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Goldstraw, P.; Yamada, K.; Nicholson, A.G.; Wells, A.U.; Hansell, D.M.; Dubois, R.M.; Ladas, G. Pulmonary fibrosis and lung cancer: risk and benefit analysis of pulmonary resection. J Thorac Cardiovasc Surg 2003, 125, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Kim, H.K.; Kim, K.; Kim, J.; Shim, Y.M.; Choi, Y.S. Prediction of acute pulmonary complications after resection of lung cancer in patients with preexisting interstitial lung disease. Thorac Cardiovasc Surg 2011, 59, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Teramukai, S.; Kondo, H.; Watanabe, A.; Ebina, M.; Kishi, K.; Fujii, Y.; Mitsudomi, T.; Yoshimura, M.; Maniwa, T.; et al. Impact and predictors of acute exacerbation of interstitial lung diseases after pulmonary resection for lung cancer. J Thorac Cardiovasc Surg 2014, 147, 1604–1611. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, H.; Sugino, K.; Hata, Y.; Makino, T.; Koezuka, S.; Isobe, K.; Tochigi, N.; Shibuya, K.; Homma, S.; Iyoda, A. Clinical features and outcomes of patients with lung cancer as well as combined pulmonary fibrosis and emphysema. Mol Clin Oncol 2016, 5, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Ki, M.S.; Kim, S.Y.; Kim, E.Y.; Jung, J.Y.; Kang, Y.A.; Park, M.S.; Kim, Y.S.; Park, S.Y.; Lee, S.H. Clinical Outcomes and Prognosis of Patients With Interstitial Lung Disease Undergoing Lung Cancer Surgery: A Propensity Score Matching Study. Clin Lung Cancer 2023, 24, e27–e38. [Google Scholar] [CrossRef] [PubMed]
- Ueno, F.; Kitaguchi, Y.; Shiina, T.; Asaka, S.; Yasuo, M.; Wada, Y.; Kinjo, T.; Yoshizawa, A.; Hanaoka, M. The Interstitial Lung Disease-Gender-Age-Physiology Index Can Predict the Prognosis in Surgically Resected Patients with Interstitial Lung Disease and Concomitant Lung Cancer. Respiration 2020, 99, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Tsutani, Y.; Mimura, T.; Kai, Y.; Ito, M.; Misumi, K.; Miyata, Y.; Okada, M. Outcomes after lobar versus sublobar resection for clinical stage I non-small cell lung cancer in patients with interstitial lung disease. J Thorac Cardiovasc Surg 2017, 154, 1089–1096. [Google Scholar] [CrossRef]
- Motono, N.; Ishikawa, M.; Iwai, S.; Iijima, Y.; Uramoto, H. Interstitial lung disease and wedge resection are poor prognostic factors for non-small cell lung cancer. J Thorac Dis 2022, 14, 1052–1060. [Google Scholar] [CrossRef]
- Tanaka, K.; Tsutani, Y.; Wakabayashi, M.; Mizutani, T.; Aokage, K.; Miyata, Y.; Kuroda, H.; Saji, H.; Watanabe, S.I.; Okada, M.; et al. Sublobar resection versus lobectomy for patients with resectable stage I non-small cell lung cancer with idiopathic pulmonary fibrosis: a phase III study evaluating survival (JCOG1708, SURPRISE). Jpn J Clin Oncol 2020, 50, 1076–1079. [Google Scholar] [CrossRef]
- Patel, A.J.; Walters, G.I.; Watkins, S.; Rogers, V.; Fallouh, H.; Kalkat, M.; Naidu, B.; Bishay, E.S. Lung cancer resection in patients with underlying usual interstitial pneumonia: a meta-analysis. BMJ Open Respir Res 2023, 10. [Google Scholar] [CrossRef]
- Fukui, M.; Takamochi, K.; Suzuki, K.; Hotta, A.; Ando, K.; Matsunaga, T.; Oh, S.; Suzuki, K. Lobe-specific outcomes of surgery for lung cancer patients with idiopathic interstitial pneumonias. Gen Thorac Cardiovasc Surg 2020, 68, 812–819. [Google Scholar] [CrossRef]
- Sato, S.; Shimizu, Y.; Goto, T.; Kitahara, A.; Koike, T.; Ishikawa, H.; Watanabe, T.; Tsuchida, M. Survival after repeated surgery for lung cancer with idiopathic pulmonary fibrosis: a retrospective study. BMC Pulm Med 2018, 18, 134. [Google Scholar] [CrossRef] [PubMed]
- Iwata, T.; Yoshino, I.; Yoshida, S.; Ikeda, N.; Tsuboi, M.; Asato, Y.; Katakami, N.; Sakamoto, K.; Yamashita, Y.; Okami, J.; et al. A phase II trial evaluating the efficacy and safety of perioperative pirfenidone for prevention of acute exacerbation of idiopathic pulmonary fibrosis in lung cancer patients undergoing pulmonary resection: West Japan Oncology Group 6711 L (PEOPLE Study). Respir Res 2016, 17, 90. [Google Scholar] [CrossRef]
- Kanayama, M.; Mori, M.; Matsumiya, H.; Taira, A.; Shinohara, S.; Kuwata, T.; Imanishi, N.; Yoneda, K.; Kuroda, K.; Tanaka, F. Perioperative pirfenidone treatment for lung cancer patients with idiopathic pulmonary fibrosis. Surg Today 2020, 50, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Sakairi, Y.; Yoshino, I.; Iwata, T.; Yoshida, S.; Kuwano, K.; Azuma, A.; Sakai, S.; Kobayashi, K. A randomized controlled phase III trial protocol: perioperative pirfenidone therapy in patients with non-small cell lung cancer combined with idiopathic pulmonary fibrosis to confirm the preventative effect against postoperative acute exacerbation: the PIII-PEOPLE study (NEJ034). J Thorac Dis 2023, 15, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D'Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2022, 20, 497–530. [Google Scholar] [CrossRef]
- Remon, J.; Soria, J.C.; Peters, S.; clinicalguidelines@esmo. org, E.G.C.E.a. Early and locally advanced non-small-cell lung cancer: an update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy. Ann Oncol 2021, 32, 1637–1642. [Google Scholar] [CrossRef]
- Dingemans, A.C.; Fruh, M.; Ardizzoni, A.; Besse, B.; Faivre-Finn, C.; Hendriks, L.E.; Lantuejoul, S.; Peters, S.; Reguart, N.; Rudin, C.M.; et al. Small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up(☆). Ann Oncol 2021, 32, 839–853. [Google Scholar] [CrossRef]
- Stanic, S.; Paulus, R.; Timmerman, R.D.; Michalski, J.M.; Barriger, R.B.; Bezjak, A.; Videtic, G.M.; Bradley, J. No clinically significant changes in pulmonary function following stereotactic body radiation therapy for early- stage peripheral non-small cell lung cancer: an analysis of RTOG 0236. Int J Radiat Oncol Biol Phys 2014, 88, 1092–1099. [Google Scholar] [CrossRef]
- Saha, A.; Dickinson, P.; Shrimali, R.K.; Salem, A.; Agarwal, S. Is Thoracic Radiotherapy an Absolute Contraindication for Treatment of Lung Cancer Patients With Interstitial Lung Disease? A Systematic Review. Clin Oncol (R Coll Radiol) 2022, 34, e493–e504. [Google Scholar] [CrossRef] [PubMed]
- Glick, D.; Lyen, S.; Kandel, S.; Shapera, S.; Le, L.W.; Lindsay, P.; Wong, O.; Bezjak, A.; Brade, A.; Cho, B.C.J.; et al. Impact of Pretreatment Interstitial Lung Disease on Radiation Pneumonitis and Survival in Patients Treated With Lung Stereotactic Body Radiation Therapy (SBRT). Clin Lung Cancer 2018, 19, e219–e226. [Google Scholar] [CrossRef] [PubMed]
- Bahig, H.; Filion, E.; Vu, T.; Chalaoui, J.; Lambert, L.; Roberge, D.; Gagnon, M.; Fortin, B.; Beliveau-Nadeau, D.; Mathieu, D.; et al. Severe radiation pneumonitis after lung stereotactic ablative radiation therapy in patients with interstitial lung disease. Pract Radiat Oncol 2016, 6, 367–374. [Google Scholar] [CrossRef]
- Okubo, M.; Itonaga, T.; Saito, T.; Shiraishi, S.; Mikami, R.; Nakayama, H.; Sakurada, A.; Sugahara, S.; Koizumi, K.; Tokuuye, K. Predicting risk factors for radiation pneumonitis after stereotactic body radiation therapy for primary or metastatic lung tumours. Br J Radiol 2017, 90, 20160508. [Google Scholar] [CrossRef]
- Kim, H.; Pyo, H.; Noh, J.M.; Lee, W.; Park, B.; Park, H.Y.; Yoo, H. Preliminary result of definitive radiotherapy in patients with non-small cell lung cancer who have underlying idiopathic pulmonary fibrosis: comparison between X-ray and proton therapy. Radiat Oncol 2019, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Liu, H.; Wu, H.; Liang, S.; Xu, Y. Risk factors for radiation pneumonitis in lung cancer patients with subclinical interstitial lung disease after thoracic radiation therapy. Radiat Oncol 2021, 16, 70. [Google Scholar] [CrossRef]
- Ozawa, Y.; Abe, T.; Omae, M.; Matsui, T.; Kato, M.; Hasegawa, H.; Enomoto, Y.; Ishihara, T.; Inui, N.; Yamada, K.; et al. Impact of Preexisting Interstitial Lung Disease on Acute, Extensive Radiation Pneumonitis: Retrospective Analysis of Patients with Lung Cancer. PLoS One 2015, 10, e0140437. [Google Scholar] [CrossRef]
- Castillo, R.; Pham, N.; Ansari, S.; Meshkov, D.; Castillo, S.; Li, M.; Olanrewaju, A.; Hobbs, B.; Castillo, E.; Guerrero, T. Pre-radiotherapy FDG PET predicts radiation pneumonitis in lung cancer. Radiat Oncol 2014, 9, 74. [Google Scholar] [CrossRef]
- Li, Y.; Yang, F.; Huang, Y.Y.; Wang, T. Sublobar resection versus ablation for stage I non-small-cell lung cancer: a meta-analysis. J Cardiothorac Surg 2022, 17, 17. [Google Scholar] [CrossRef]
- Dupuy, D.E.; Fernando, H.C.; Hillman, S.; Ng, T.; Tan, A.D.; Sharma, A.; Rilling, W.S.; Hong, K.; Putnam, J.B. Radiofrequency ablation of stage IA non-small cell lung cancer in medically inoperable patients: Results from the American College of Surgeons Oncology Group Z4033 (Alliance) trial. Cancer 2015, 121, 3491–3498. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Bie, Z.; Li, Y.; Guo, R.; Li, X. Safety and efficacy of CT-guided percutaneous microwave ablation for stage I non-small cell lung cancer in patients with comorbid idiopathic pulmonary fibrosis. Eur Radiol 2023. [Google Scholar] [CrossRef] [PubMed]
- Kashima, M.; Yamakado, K.; Takaki, H.; Kodama, H.; Yamada, T.; Uraki, J.; Nakatsuka, A. Complications after 1000 lung radiofrequency ablation sessions in 420 patients: a single center's experiences. AJR Am J Roentgenol 2011, 197, W576–580. [Google Scholar] [CrossRef]
- Chen, H.; Senan, S.; Nossent, E.J.; Boldt, R.G.; Warner, A.; Palma, D.A.; Louie, A.V. Treatment-Related Toxicity in Patients With Early-Stage Non-Small Cell Lung Cancer and Coexisting Interstitial Lung Disease: A Systematic Review. Int J Radiat Oncol Biol Phys 2017, 98, 622–631. [Google Scholar] [CrossRef]
- Li, B.; Bie, Z.; Li, Y.; Guo, R.; Wang, C.; Li, X. Synchronous percutaneous core-needle biopsy and microwave ablation for stage I non-small cell lung cancer in patients with Idiopathic pulmonary fibrosis: initial experience. Int J Hyperthermia 2023, 40, 2270793. [Google Scholar] [CrossRef]
- Singh, N.; Jaiyesimi, I.A.; Ismaila, N.; Leighl, N.B.; Mamdani, H.; Phillips, T.; Owen, D.H. Therapy for Stage IV Non-Small-Cell Lung Cancer Without Driver Alterations: ASCO Living Guideline, Version 2023.1. J Clin Oncol 2023, 41, e51–e62. [Google Scholar] [CrossRef]
- Singh, N.; Jaiyesimi, I.A.; Ismaila, N.; Leighl, N.B.; Mamdani, H.; Phillips, T.; Owen, D.H. Therapy for Stage IV Non-Small-Cell Lung Cancer With Driver Alterations: ASCO Living Guideline, Version 2023.1. J Clin Oncol 2023, 41, e42–e50. [Google Scholar] [CrossRef] [PubMed]
- Otsubo, K.; Kishimoto, J.; Ando, M.; Kenmotsu, H.; Minegishi, Y.; Horinouchi, H.; Kato, T.; Ichihara, E.; Kondo, M.; Atagi, S.; et al. Nintedanib plus chemotherapy for nonsmall cell lung cancer with idiopathic pulmonary fibrosis: a randomised phase 3 trial. Eur Respir J 2022, 60. [Google Scholar] [CrossRef]
- Kenmotsu, H.; Naito, T.; Kimura, M.; Ono, A.; Shukuya, T.; Nakamura, Y.; Tsuya, A.; Kaira, K.; Murakami, H.; Takahashi, T.; et al. The risk of cytotoxic chemotherapy-related exacerbation of interstitial lung disease with lung cancer. J Thorac Oncol 2011, 6, 1242–1246. [Google Scholar] [CrossRef]
- Wang, Z.; Bai, J.; Liu, Y.; Li, P.; Jiao, G. Risk factors for acute exacerbation of interstitial lung disease during chemotherapy for lung cancer: a systematic review and meta-analysis. Front Oncol 2023, 13, 1250688. [Google Scholar] [CrossRef]
- Akaike, K.; Saruwatari, K.; Matsushima, R.; Fujino, K.; Morinaga, J.; Oda, S.; Takahashi, H.; Shiraishi, S.; Okabayashi, H.; Hamada, S.; et al. Clinical impact of SUV(max) of interstitial lesions in lung cancer patients with interstitial lung disease who underwent pulmonary resection. J Thorac Dis 2022, 14, 3801–3810. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Miao, L.; Hu, Y.; Zhou, Y. The Efficacy and Safety of First-Line Chemotherapy in Patients With Non-small Cell Lung Cancer and Interstitial Lung Disease: A Systematic Review and Meta-Analysis. Front Oncol 2020, 10, 1636. [Google Scholar] [CrossRef] [PubMed]
- Fujita, T.; Kuroki, T.; Hayama, N.; Shiraishi, Y.; Amano, H.; Nakamura, M.; Hirano, S.; Tabeta, H.; Nakamura, S. Pemetrexed Plus Platinum for Patients With Advanced Non-small Cell Lung Cancer and Interstitial Lung Disease. In Vivo 2019, 33, 2059–2064. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Shukuya, T.; Takahashi, F.; Mori, K.; Suina, K.; Asao, T.; Kanemaru, R.; Honma, Y.; Muraki, K.; Sugano, K.; et al. Pemetrexed for advanced non-small cell lung cancer patients with interstitial lung disease. BMC Cancer 2014, 14, 508. [Google Scholar] [CrossRef] [PubMed]
- Suh, C.H.; Kim, K.W.; Pyo, J.; Hatabu, H.; Nishino, M. The incidence of ALK inhibitor-related pneumonitis in advanced non-small-cell lung cancer patients: A systematic review and meta-analysis. Lung Cancer 2019, 132, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Johkoh, T.; Sakai, F.; Kusumoto, M.; Arakawa, H.; Harada, R.; Ueda, M.; Kudoh, S.; Fukuoka, M. Association between baseline pulmonary status and interstitial lung disease in patients with non-small-cell lung cancer treated with erlotinib--a cohort study. Clin Lung Cancer 2014, 15, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, S. Nintedanib: A Review of Its Use as Second-Line Treatment in Adults with Advanced Non-Small Cell Lung Cancer of Adenocarcinoma Histology. Target Oncol 2015, 10, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Richeldi, L.; du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med 2014, 370, 2071–2082. [Google Scholar] [CrossRef] [PubMed]
- Dabholkar, S.; Gao, B.; Chuong, B. Nintedanib-A case of treating concurrent idiopathic pulmonary fibrosis and non-small cell lung cancer. Respirol Case Rep 2022, 10, e0902. [Google Scholar] [CrossRef]
- Shiratori, T.; Tanaka, H.; Tabe, C.; Tsuchiya, J.; Ishioka, Y.; Itoga, M.; Taima, K.; Takanashi, S.; Tasaka, S. Effect of nintedanib on non-small cell lung cancer in a patient with idiopathic pulmonary fibrosis: A case report and literature review. Thorac Cancer 2020, 11, 1720–1723. [Google Scholar] [CrossRef]
- Fukunaga, K.; Yokoe, S.; Kawashima, S.; Uchida, Y.; Nakagawa, H.; Nakano, Y. Nintedanib prevented fibrosis progression and lung cancer growth in idiopathic pulmonary fibrosis. Respirol Case Rep 2018, 6, e00363. [Google Scholar] [CrossRef] [PubMed]
- Kai, Y.; Matsuda, M.; Fukuoka, A.; Hontsu, S.; Yamauchi, M.; Yoshikawa, M.; Muro, S. Remarkable response of non-small cell lung cancer to nintedanib treatment in a patient with idiopathic pulmonary fibrosis. Thorac Cancer 2021, 12, 1457–1460. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.; Markart, P.; Drakopanagiotakis, F.; Mamazhakypov, A.; Schaefer, L.; Didiasova, M.; Wygrecka, M. Pirfenidone inhibits motility of NSCLC cells by interfering with the urokinase system. Cell Signal 2020, 65, 109432. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Wang, Y.; Luo, D.; Cheng, Z.; Zeng, Q.; Wang, G.; Chen, M.; Zhang, S.; Luo, P. Pirfenidone inhibits TGF-beta1-induced metabolic reprogramming during epithelial-mesenchymal transition in non-small cell lung cancer. J Cell Mol Med 2024, 28, e18059. [Google Scholar] [CrossRef] [PubMed]
- Branco, H.; Oliveira, J.; Antunes, C.; Santos, L.L.; Vasconcelos, M.H.; Xavier, C.P.R. Pirfenidone Sensitizes NCI-H460 Non-Small Cell Lung Cancer Cells to Paclitaxel and to a Combination of Paclitaxel with Carboplatin. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Kurimoto, R.; Ebata, T.; Iwasawa, S.; Ishiwata, T.; Tada, Y.; Tatsumi, K.; Takiguchi, Y. Pirfenidone may revert the epithelial-to-mesenchymal transition in human lung adenocarcinoma. Oncol Lett 2017, 14, 944–950. [Google Scholar] [CrossRef]
- Mediavilla-Varela, M.; Boateng, K.; Noyes, D.; Antonia, S.J. The anti-fibrotic agent pirfenidone synergizes with cisplatin in killing tumor cells and cancer-associated fibroblasts. BMC Cancer 2016, 16, 176. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Yano, Y.; Kuge, T.; Okabe, F.; Ishijima, M.; Uenami, T.; Kanazu, M.; Akazawa, Y.; Yamaguchi, T.; Mori, M. Safety and effectiveness of pirfenidone combined with carboplatin-based chemotherapy in patients with idiopathic pulmonary fibrosis and non-small cell lung cancer: A retrospective cohort study. Thorac Cancer 2020, 11, 3317–3325. [Google Scholar] [CrossRef] [PubMed]
- Hamada, S.; Ichiyasu, H.; Ikeda, T.; Inaba, M.; Kashiwabara, K.; Sadamatsu, T.; Sato, N.; Akaike, K.; Okabayashi, H.; Saruwatari, K.; et al. Protective effect of bevacizumab on chemotherapy-related acute exacerbation of interstitial lung disease in patients with advanced non-squamous non-small cell lung cancer. BMC Pulm Med 2019, 19, 72. [Google Scholar] [CrossRef]
- Wang, Y.; Gong, X.; Hu, Y.; Yi, Q.; Zhang, Q.; Miao, L.; Zhou, Y. Anti-Angiogenic Drugs Inhibit Interstitial Lung Disease Progression in Patients With Advanced Non-Small Cell Lung Cancer. Front Oncol 2022, 12, 873709. [Google Scholar] [CrossRef]
- Esfahani, K.; Meti, N.; Miller, W.H., Jr.; Hudson, M. Adverse events associated with immune checkpoint inhibitor treatment for cancer. CMAJ 2019, 191, E40–E46. [Google Scholar] [CrossRef] [PubMed]
- Haratani, K.; Hayashi, H.; Chiba, Y.; Kudo, K.; Yonesaka, K.; Kato, R.; Kaneda, H.; Hasegawa, Y.; Tanaka, K.; Takeda, M.; et al. Association of Immune-Related Adverse Events With Nivolumab Efficacy in Non-Small-Cell Lung Cancer. JAMA Oncol 2018, 4, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Shibaki, R.; Murakami, S.; Matsumoto, Y.; Goto, Y.; Kanda, S.; Horinouchi, H.; Fujiwara, Y.; Yamamoto, N.; Motoi, N.; Kusumoto, M.; et al. Tumor expression and usefulness as a biomarker of programmed death ligand 1 in advanced non-small cell lung cancer patients with preexisting interstitial lung disease. Med Oncol 2019, 36, 49. [Google Scholar] [CrossRef] [PubMed]
- Duitman, J.; van den Ende, T.; Spek, C.A. Immune Checkpoints as Promising Targets for the Treatment of Idiopathic Pulmonary Fibrosis? J Clin Med 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Frank, A.J.; Dagogo-Jack, I.; Dobre, I.A.; Tait, S.; Schumacher, L.; Fintelmann, F.J.; Fingerman, L.M.; Keane, F.K.; Montesi, S.B. Management of Lung Cancer in the Patient with Interstitial Lung Disease. Oncologist 2023, 28, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Kazerooni, E.A.; Martinez, F.J.; Flint, A.; Jamadar, D.A.; Gross, B.H.; Spizarny, D.L.; Cascade, P.N.; Whyte, R.I.; Lynch, J.P., 3rd; Toews, G. Thin-section CT obtained at 10-mm increments versus limited three-level thin-section CT for idiopathic pulmonary fibrosis: correlation with pathologic scoring. AJR Am J Roentgenol 1997, 169, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Shimizu, J.; Hasegawa, T.; Horio, Y.; Inaba, Y.; Yatabe, Y.; Hida, T. Pre-existing pulmonary fibrosis is a risk factor for anti-PD-1-related pneumonitis in patients with non-small cell lung cancer: A retrospective analysis. Lung Cancer 2018, 125, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, Y.; Masuda, T.; Yamaguchi, K.; Sakamoto, S.; Horimasu, Y.; Nakashima, T.; Miyamoto, S.; Tsutani, Y.; Iwamoto, H.; Fujitaka, K.; et al. Pre-existing interstitial lung abnormalities are risk factors for immune checkpoint inhibitor-induced interstitial lung disease in non-small cell lung cancer. Respir Investig 2019, 57, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, N.; Honda, T.; Sema, M.; Kawahara, T.; Jin, Y.; Natsume, I.; Chiaki, T.; Yamashita, T.; Tsukada, Y.; Taki, R.; et al. The utility of ground-glass attenuation score for anticancer treatment-related acute exacerbation of interstitial lung disease among lung cancer patients with interstitial lung disease. Int J Clin Oncol 2020, 25, 282–291. [Google Scholar] [CrossRef]
- Isobe, K.; Nakamura, Y.; Sakamoto, S.; Tomii, K.; Takimoto, T.; Miyazaki, Y.; Matsumoto, M.; Sugino, K.; Ichikado, K.; Moriguchi, S.; et al. Immune checkpoint inhibitors in patients with lung cancer having chronic interstitial pneumonia. ERJ Open Res 2024, 10. [Google Scholar] [CrossRef]
- Zhang, M.; Fan, Y.; Nie, L.; Wang, G.; Sun, K.; Cheng, Y. Clinical Outcomes of Immune Checkpoint Inhibitor Therapy in Patients With Advanced Non-small Cell Lung Cancer and Preexisting Interstitial Lung Diseases: A Systematic Review and Meta-analysis. Chest 2022, 161, 1675–1686. [Google Scholar] [CrossRef] [PubMed]
- Khunger, M.; Velcheti, V. A Case of a Patient with Idiopathic Pulmonary Fibrosis with Lung Squamous Cell Carcinoma Treated with Nivolumab. J Thorac Oncol 2017, 12, e96–e97. [Google Scholar] [CrossRef] [PubMed]
- Ide, M.; Tanaka, K.; Sunami, S.; Asoh, T.; Maeyama, T.; Tsuruta, N.; Nakanishi, Y.; Okamoto, I. Durable response to nivolumab in a lung adenocarcinoma patient with idiopathic pulmonary fibrosis. Thorac Cancer 2018, 9, 1519–1521. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, D.; Yomota, M.; Sekine, A.; Morita, M.; Morimoto, T.; Hosomi, Y.; Ogura, T.; Tomioka, H.; Tomii, K. Nivolumab for advanced non-small cell lung cancer patients with mild idiopathic interstitial pneumonia: A multicenter, open-label single-arm phase II trial. Lung Cancer 2019, 134, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Tasaka, Y.; Honda, T.; Nishiyama, N.; Tsutsui, T.; Saito, H.; Watabe, H.; Shimaya, K.; Mochizuki, A.; Tsuyuki, S.; Kawahara, T.; et al. Non-inferior clinical outcomes of immune checkpoint inhibitors in non-small cell lung cancer patients with interstitial lung disease. Lung Cancer 2021, 155, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Kudoh, S.; Kato, H.; Nishiwaki, Y.; Fukuoka, M.; Nakata, K.; Ichinose, Y.; Tsuboi, M.; Yokota, S.; Nakagawa, K.; Suga, M.; et al. Interstitial lung disease in Japanese patients with lung cancer: a cohort and nested case-control study. Am J Respir Crit Care Med 2008, 177, 1348–1357. [Google Scholar] [CrossRef] [PubMed]
- Assie, J.B.; Chouaid, C.; Nunes, H.; Reynaud, D.; Gaudin, A.F.; Grumberg, V.; Jolivel, R.; Jouaneton, B.; Cotte, F.E.; Duchemann, B. Outcome following nivolumab treatment in patients with advanced non-small cell lung cancer and comorbid interstitial lung disease in a real-world setting. Ther Adv Med Oncol 2023, 15, 17588359231152847. [Google Scholar] [CrossRef] [PubMed]
- JafariNezhad, A.; YektaKooshali, M.H. Lung cancer in idiopathic pulmonary fibrosis: A systematic review and meta-analysis. PLoS One 2018, 13, e0202360. [Google Scholar] [CrossRef]
- Kashiwabara, K.; Semba, H.; Fujii, S.; Tsumura, S.; Aoki, R. Difference in benefit of chemotherapy between small cell lung cancer patients with interstitial pneumonia and patients with non-small cell lung cancer. Anticancer Res 2015, 35, 1065–1071. [Google Scholar]
- Togashi, Y.; Masago, K.; Handa, T.; Tanizawa, K.; Okuda, C.; Sakamori, Y.; Nagai, H.; Kim, Y.H.; Mishima, M. Prognostic significance of preexisting interstitial lung disease in Japanese patients with small-cell lung cancer. Clin Lung Cancer 2012, 13, 304–311. [Google Scholar] [CrossRef]
- Kanaji, N.; Shimizu, J.; Sakai, K.; Ueda, Y.; Miyawaki, H.; Watanabe, N.; Uemura, T.; Hida, T.; Inoue, T.; Watanabe, N.; et al. Clinical features of patients with small cell lung cancer and idiopathic pulmonary fibrosis treated with chemotherapy or chemoradiotherapy. Ther Adv Respir Dis 2020, 14, 1753466620963866. [Google Scholar] [CrossRef] [PubMed]
- Koyama, N.; Iwai, Y.; Nagai, Y.; Aoshiba, K.; Nakamura, H. Idiopathic pulmonary fibrosis in small cell lung cancer as a predictive factor for poor clinical outcome and risk of its exacerbation. PLoS One 2019, 14, e0221718. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Yoh, K.; Goto, K.; Niho, S.; Umemura, S.; Ohmatsu, H.; Ohe, Y. Safety and efficacy of platinum agents plus etoposide for patients with small cell lung cancer with interstitial lung disease. Anticancer Res 2013, 33, 1175–1179. [Google Scholar] [PubMed]
- Nakao, S.; Yamaguchi, K.; Sakamoto, S.; Horimasu, Y.; Masuda, T.; Miyamoto, S.; Nakashima, T.; Iwamoto, H.; Fujitaka, K.; Hamada, H.; et al. Chemotherapy-associated Acute Exacerbation of Interstitial Lung Disease Shortens Survival Especially in Small Cell Lung Cancer. Anticancer Res 2019, 39, 5725–5731. [Google Scholar] [CrossRef]
- Ikeda, S.; Ogura, T.; Kato, T.; Kenmotsu, H.; Agemi, Y.; Tokito, T.; Ito, K.; Isomoto, K.; Takiguchi, Y.; Yoneshima, Y.; et al. Nintedanib plus Chemotherapy for Small Cell Lung Cancer with Comorbid Idiopathic Pulmonary Fibrosis. Ann Am Thorac Soc 2024. [Google Scholar] [CrossRef]
Figure 1.
Lung cancer in a patient with combined pulmonary fibrosis and emphysema. The tumor is located in the right lower lobe (arrows).
Figure 1.
Lung cancer in a patient with combined pulmonary fibrosis and emphysema. The tumor is located in the right lower lobe (arrows).
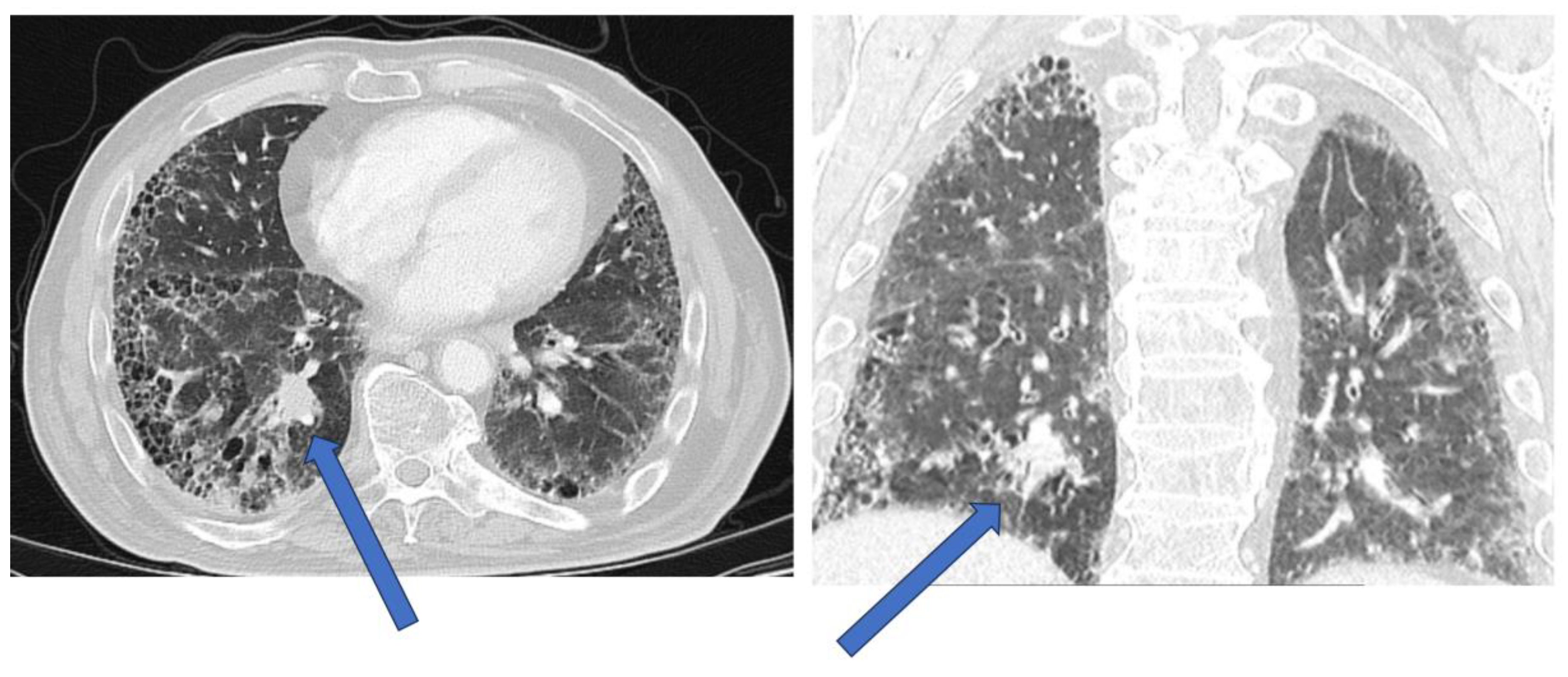

Table 1.
Challenges of different modalities for the diagnosis of lung cancer in patients with ILDs.
| Modality | Diagnostic challenges |
|---|---|
| Pulmonary function tests (PFTs) | In CPFE, preserved lung volumes in patients may overestimate patients´ functional operability. DLCO is the most sensitive parameter |
| HRCT | Tumors may be directly adjacent to fibrotic lesions, with underestimation of tumor size. Reduced sensitivity and specificity in evaluating mediastinal lymph nodes (reactive mediastinal lymph node enlargement may be seen in ILDs without lung cancer) |
| PET-scan | FDG-positive mediastinal lymph nodes may be reactive and not due to lung cancer infiltration |
| CT-guided biopsy | Motion artifacts and biopsy of fibrotic lesions adjacent to the tumor may give inconclusive results. Pneumothorax may be more difficult to treat. |
| Bronchoscopy with biopsy | Small risk of acute exacerbation of ILD (AE-ILD). Tumor identification with radial EBUS or navigational bronchoscopy in fibrotic milieu may be more challenging, compared to patients without ILDs |
| Surgical biopsy | Increased risk of AE-ILD |
Table 2.
Proposed treatment for patients with NSCLC and ILDs. Decisions to be taken in oncology board, considering patient´s wishes, comorbidities, NSCLC stadium and ILD stadium. Oncologic outcomes and preservation of lung function to be considered. Close monitoring for AE-ILD and pneumonitis required.
Table 2.
Proposed treatment for patients with NSCLC and ILDs. Decisions to be taken in oncology board, considering patient´s wishes, comorbidities, NSCLC stadium and ILD stadium. Oncologic outcomes and preservation of lung function to be considered. Close monitoring for AE-ILD and pneumonitis required.
| Stage of NSCLC | Treatment Options for NSCLC with ILD |
|---|---|
| Stage I | - Surgical resection (Lobectomy or segmentectomy): for patients with stable and well-controlled ILD, with mild to moderately-impaired lung function- Stereotactic body radiation therapy (SBRT): alternative to surgery for patients who are not surgical candidates due to their ILD, due to poor lung function or comorbidities. Option in a minority of very carefully selected patients due to the possible detrimental risk of pneumonitis. - Percutaneous image-guided ablation to be considered in patients with poor lung function and small tumors |
| Stage II | - Surgical resection: for patients with stable and well-controlled ILD, with mild to medium-impaired lung function- SBRT: For patients who are not suitable for surgery due to ILD, SBRT may be considered. Option in a minority of very carefully selected patients due to the possible detrimental risk of pneumonitis. |
| Stage III | -Radiochemotherapy: standard of treatment for locally advanced NSCLC. Decision to proceed in patients with ILD to be taken in oncology board, considering the potential risk of AE-ILD. Sequential, instead of concomitant therapy may be associated with reduced risk of pulmonary toxicity. Radiation therapy is an option in a minority of very carefully selected patients due to the possible detrimental risk of pneumonitis.- Immunotherapy: may be considered in patients with stable ILD and mild to moderately-impaired lung function, as part of the treatment regimen. |
| Stage IV | - Systemic therapy: chemotherapy, targeted therapy, immunotherapy, or a combination of the above depending on the patient's performance status, ILD status and comorbidities.- Palliative care: in advanced stages of NSCLC or end-stage ILD |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



