
Submitted:
17 May 2024
Posted:
20 May 2024
You are already at the latest version
Abstract
: Schizophrenia and schizoaffective disorder are generally treated with second-generation antipsychotic drugs. These drugs are mostly D2 and 5-HT2A antagonists. They improve positive schizophrenia symptoms sufficiently well; however, they ameliorate negative schizophrenia symptoms and cognitive functions to a small extent. We review novel antipsychotic drugs exerting a partial agonism at dopaminergic and serotonergic receptors such as cariprazine, brexipiprazole and lumateperone. Besides, the mechanisms of actions of non-anti-dopaminergic antipsychotic drugs are pointed out. Updated neural networks are used to explain the mechanism of action of M4 and M1 receptor agonists, for example xanomeline combined with trospium or emraclidine, and trace-amine-associated receptor 1 agonists (TAAR1), for example ulataront. Phase 3 clinical trials of new third generation antipsychotic drugs are presented. Novel antipsychotic drugs with a partial agonism at D2 and D3 receptors improve positive and negative schizophrenia symptoms as well as cognitive symptoms better than second generation antipsychotic drugs. Besides, they are well tolerated. M4 and M1 receptor agonists, i.e. xanomeline combined with trospium or emraclidine, and TAAR1 agonists, i.e. ulataront, have promising results in clinical trials; they well improve negative schizophrenia symptoms and cognitive functions. Phase 3 clinical trials offer promising results for anti-dopaminergic and non-anti-dopaminergic novel antipsychotic drugs. These new non-anti-dopaminergic antipsychotic drugs better emend negative schizophrenia symptoms, and they better improve cognitive functions than second-generation antipsychotic drugs. Promising new antipsychotic drugs are cariprazine, brexipiprazole, lumateperone, ulataront, and xanomeline combined with trospium. Although phase 3 clinical studies are not yet completed, they showed a therapeutic effect superior to those achieved by second-generation antipsychotic drugs. They are tolerated very well, and they better treat negative schizophrenia symptoms and improve cognitive functions.
Keywords:
antipsychotic drug
; M4 and M1 receptor agonist
; negative schizophrenia symptoms
; neural network
; schizophrenia
; trace-amine-associated receptor 1 agonist
; ulataront
; xanomeline
1. Introduction
Schizophrenia and schizoaffective disorder are chronic disabling diseases with positive, negative, affective, and cognitive symptoms. Generally, these mental diseases are treated with antipsychotic drugs. Schizophrenic disorders have a genetic etiology in 80% of cases. The disposable antipsychotic drugs have different therapeutic effects on positive and negative schizophrenic symptoms, and they can cause movement disturbances, that is extrapyramidal symptoms (EPS). The often-prescribed antipsychotic drugs have an antagonism at D2 and 5-HT2A receptors [1,2]. Some new antipsychotic drugs have been developed, among them the third-generation antipsychotic drugs which exert a partial agonism at dopaminergic and serotonergic receptors. Antipsychotic drugs without exerting an antagonism or a partial agonism at dopaminergic receptors are available as well. Xanomeline, combined with trospium, an anticholinergic drug, and trace-amine associated receptor 1 (TAAR1) agonists, have been developed and are being examined in clinical studies [3]. M4 and M1 receptor agonists, i.e., xanomeline combined with trospium, exert an antipsychotic effect, because an agonism at M4 and M1 muscarinic cholinergic receptors promotes the blockade of D2 dopaminergic receptors. In this review, the neural networks involved in the prefrontal cortex in schizophrenia are updated. Clinical studies should still be carried out to know whether these new antipsychotic drugs are therapeutically comparable or superior to often used antipsychotic drugs [1]. In the first clinical studies performed, cariprazine, brexipiprazole, lumateperone, xanomeline, and ulataront well treated negative schizophrenia symptoms and improved cognitive functions [4,5]. The aim of this review is to update the therapeutic advantages of third-generation antipsychotic drugs in comparison to second-generation antipsychotic drugs and to point out the results of first phase 3 clinical studies.
2. Clinical Antipsychotic Effect of Second-Generation Antipsychotic Drugs
Second-generation antipsychotic drugs such as risperidone, olanzapine, quetiapine, and clozapine are used in the treatment of schizophrenia and schizoaffective disorder in a wide range. Most of these drugs are D2 and 5-HT2A receptor antagonists and only clozapine has a D3 and D4 and 5-HT2A antagonistic effect and a 5-HT1A agonistic effect. Clozapine can be administered in treatment-resistant psychotic disorders. All second-generations antipsychotic drugs can cause movement disturbances, i.e., EPS. Only clozapine does not have these side effects, because it does not block the D2 receptor [6,7]. These drugs have a good antipsychotic effect, they improve above all positive antipsychotic schizophrenia symptoms, and also negative schizophrenia symptoms, but to a lesser degree. Olanzapine better improves mutism, depression, social withdrawal than other second-generation antipsychotic drugs [7]. Olanzapine, quetiapine and clozapine have a prolactin-sparing effect; risperidone in contrast raises prolactin levels, because it has a high affinity for the D2 receptor [4,5,6].
3. Mechanisms of Action of Recently Developed Antipsychotic Drugs
Some third-generation antipsychotic drugs have been developed. Cariprazine, brexipiprazole and lumateperone have a partial agonistic effect at dopaminergic and serotonergic receptors. This partial agonism at D2 and 5-HT2A receptors might better improve negative schizophrenia symptoms, because these symptoms are associated to hypoactive dopaminergic and serotonergic neurons in the prefrontal cortex [5,8,9,10,11,12]. Three new third-generation antipsychotic drugs do not block dopaminergic receptors, namely TAAR1 agonists, M4 and M1 receptor agonists. The antipsychotic effects of these new drugs appear in Table 1 [13,14].
4. Why Is the Development of Novel Antipsychotic Drugs Necessary, What Are the Missing Clinical Effects in the Efficacy of Second-Generation Antipsychotic Drugs?
Although second-generation antipsychotic drugs are widely used in the treatment of schizophrenia patients, they have lacking therapeutic effects and cause many negative adverse effects. First of all, they do not treat sufficiently negative schizophrenia symptoms such as mutism, social withdrawal and depression. Besides, it could not be shown that these drugs improve cognitive functions. They can cause movement disturbances, and libido is reduced [8]. However, antipsychotic drugs like cariprazine, brexipiprazole, and lumateperone better ameliorate cognitive functions. Besides, they do not reduce libido, and they do not influence movement. Promising new drugs like ulataront and xanomeline combined with trospium have a good therapeutic effect in improving cognitive functions [15].

Table 1.
Mechanism of action and therapeutic effects in phase 3 clinical trials of novel antipsychotic drugs.
Table 1.
Mechanism of action and therapeutic effects in phase 3 clinical trials of novel antipsychotic drugs.
| _ | Cariprazine | Brexipiprazole | Luma- teperone |
SEP 363856 | Xanome-line combined with trospium |
|---|---|---|---|---|---|
| Food and Drug Administration (FDA) approval | Approved for treatment of schizophrenia and acute mania in bipolar disorder in 2015 | Approved for treatment of schizophrenia and as an adjunctive therapy for major depression and for agitated patients with Alzheimer’s disease in 2015 | Approved for treatment of adult patients with schizo-phrenia in 2019 | Ulataront (SEP 363856) has got a break-through therapy designation for treatment of schizophrenia by FDA | The approval of xanomeline, combined with trospium for treatment of schizophrenia is expected in September, 2024 |
| Mecha-nisms of action | A partial agonism at D2/D3 receptors with a higher affinity for D3 receptors and an agonism at 5-HT1A receptors | A partial agonism at D2/D3 receptors and has a 5-HT1A agonism | A partial agonism at D2/5-HT2A receptors; blocks serotonin reuptake, and interferes with glutamate neurotrans-mission | An agonistic effect at TAAR1/5-HT1A receptors. It stabilizes mono-aminergic neurotransmission, i.e., dopaminergic and serotonergic neurons | An agonistic effect at M1/M4 receptors. M1/M4 muscarinic cholinergic neurons stimulation leads to the blockade of D2 dopa-minergic neurons in the prefrontal cortex |
| Thera-peutic effects | Ameliorates positive and negative schizophrenia symptoms and depressive symptoms | Improves positive and negative schizophrenia symptoms and depressive symptoms | emends well positive and negative schizo-phrenia symptoms and ameliorates social capabilities | emends well positive and negative schizophrenia symptoms and improves cognitive functions | improves well positive and negative schizo-phrenia symptoms and cognitive functions |
| Thera-peutic effects on positive schizo-phrenia symptoms | Improves | Improves | Ameliorates | Good therapeutic effect | improves well |
| Thera-peutic effects on negative schizo-phrenia symptoms | Good therapeutic effect | Good therapeutic effect | Ame-liorates | Improves | Improves |
| Thera-peutic effects on affective symptoms | Good anti-depressive and antimanic effects | Good therapeutic effect on depressive and manic symptoms | Good therapeutic effect on depressive and manic symptoms | Good therapeutic effect on depressive and manic symptoms | Good therapeutic effect on depressive and manic symptoms |
| Thera-peutic effects on cognitive symptoms | Improves | Improves | Improves social capabilities | Improves | Improves |
| Adverse effects | Movement disturbances are reduced; however, akathisia appears in 11% of patients. Metabolic and cardiac adverse effects are reduced | The frequency of movement disturbances, and cardiac and metabolic adverse effects are reduced | Movement disturbances and metabolic and cardiac adverse effects are largely reduced | It caused very few adverse effects, for example movement disturbances or cardiac and metabolic adverse effects | Movement distur-bances and metabolic and cardia adverse effects are seen scarcely and rarely |
| References | [3,9,10,14,16,17,18,19] | [19,20,21,22] | [22,23,24,25] | [26,27] | [28,29,30,31,32,33,34,35,36] |
4.1. Cariprazine
Cariprazine is a new third-generation antipsychotic drug which was approved by FDA in 2015 for the treatment of schizophrenia and affective disorders. It can be applied for the treatment of acute mania in bipolar disorder [37]. Cariprazine has a partial agonism at D2 and D3 receptors with a 10-fold higher affinity for the D3 receptor. Besides, it has an agonism at 5-HT1A receptors. Its antidopaminergic effects is stronger than with aripiprazole and brexipiprazole [38]. It exerts antipsychotic, antimanic and antidepressive effects. In clinical trials, it showed comparable antipsychotic effects like risperidone. In these trials, cariprazine improved psychotic symptoms, namely positive as well as negative schizophrenia symptoms and cognitive functions. Cariprazine is an activating antipsychotic drug, therefore it can cause sleep disturtances [39]. However, cariprazine can cause akathisia in 11 % of the patients treated. Moreover, cariprazine exerts antimanic and antidepressive actions (see Table 2) Cariprazine can emend psychotic, depressive and manic symptoms, the treatment with this drug better improves quality of life than a pharmacotherapy with risperidone. It can be used in treatment-resistant forms as an alternative of clozapine [2,8,13,15,17,18,37,38,39].
4.2. Brexipiprazole
Brexipiprazole is a third-generation antipsychotic drug which was approved for the treatment of schizophrenia and major depression bipolar disorder in 2015. It can be used as an augmentation therapy in the treatment of major depression [37].This drug has a partial agonism at D2 and D3 receptors and an agonism at 5-HT1A receptors and an antagonism at 5-HT2A receptors. [20,38]. The occurrence of adverse effects is reduced, i.e., movement disturbances and metabolic and cardiac side effects. Brexipiprazole causes adverse effects like akathisia, headache, somnolence, tremor, weight gain. Brexipiprazole is neither sedating nor activating, it seldom causes sleep disturbances [39]. 86 clinical trials were undertaken to study the antipsychotic effects of brexipiprazole; it improved negative schizophrenia symptoms, as well as affective and cognitive symptoms (see Table 2) [20,21,37,38,39,40].
4.3. Lumateperone
Lumateperone is a new antipsychotic drug which was approved for the treatment of adult patients suffering from schizophrenia in 2019 [23]. It exerts a partial agonism at D2 and 5-HT2A receptors, blocks serotonin reuptake and interferes with the glutamatergic neurotransmission [24,25]. Lumateperone reduces dopamine release, therefore dopamine activity is more reduced than with other antipsychotic drugs [40]. It has an antidepressive effects by the blockade of the serotonin release and by the antagonism of 5-HT2A receptors. The occurrence of movement disturbances, i.e., EPS and metabolic and cardiac side effects have been largely reduced. 20 clinical trials were performed with 1,900 participants, and it was shown that lumateperone improved negative schizophrenia symptoms and social capabilities (see Table 2) The short-term effects of these newer antipsychotic drugs show less adverse effects and a good therapeutic effects on negative schizophrenia symptoms, however long-term studies are very rare. [23,24,25,26,39,40].
4.4. TAAR1 Agonists
Trace-amine-associated receptor 1 agonists (TAAR1 agonists) play a key role in the monoamine neurotransmission; through a 5-HT1A agonistic effect and an agonism at trace-amine-associated 1 receptors (TAAR 1), they also might have a therapeutic effect in schizophrenia, anxiety, and addiction. Ulataront (SEP 363856), a TAAR1 agonist, has being examined in clinical trials in phase 3 for the treatment of schizophrenia [27]. In these trials, it improved positive and negative schizophrenia symptoms. Ulataront activates TAAR1 and 5-HT1A receptors. In clinical trials, it also improved positive and negative schizophrenia symptoms in an exacerbation of this disorder. It did not cause movement disturbances nor raised prolactin levels [27]. In the first clinical trial (NCT 02969382) performed with ulataront (SEP 363856), this TAAR1 agonist improved not only positive, but also negative schizophrenia symptoms and cognitive symptoms. This new drug caused very few adverse effects, for example EPS and metabolic and cardiac side effects. An exacerbation of acute schizophrenia can be observed as an adverse effect in the treatment with SEP 363856 [28]. TAAR1 agonists stabilize the monoamine neurotransmission also through a 5-HT1A agonistic effect [28]. By stimulating TAAR 1 and 5-HT1A receptors, monoamine neurons, i.e., dopaminergic and serotonergic neurons are stabilized, namely that a normoactive neurotransmission is enabled (see Table 2) [14].
4.5. Xanomeline Combined with Trospium
M4 and M1 receptor agonists are promising antipsychotic drugs that might be used in the treatment of schizophrenia. Xanomeline, an M4 and M1 receptor agonist, combined with trospium, an anticholinergic drug, can be approved by FDA for the treatment of schizophrenia patients. The decision about this approval will be taken on September 26, 2024. Dose-dependent cholinergic side effects such as nausea, vomiting, diarrhea, sweating and hypersalivation can be reduced by the administration of the anticholinergic drug trospium [13]. In a phase I trial, a group of healthy volunteers receiving xanomeline alone was compared with a group treated with xanomeline, combined with trospium. The results was that the cholinergic adverse effects were reduced by 49 %, and the antipsychotic effects were not changed [40,41]. The long-term effect of stimulating M1 and M4 receptors indicates a weakening of the receptor occupancy and activation [42,43]. The effect of xanomeline on the sleep architecture was examined in animal experiements. It was found that a direct stimulation of muscarinic cholinergic neurons produces increases in wake and arousal an decreases in the non-rapid eye movement [44].Three clinical studies in comparison with placebo have been performed. Xanomeline, combined with trospium ameliorated positive and negative schizophrenia symptoms, improved cognitive deficits, and it was well tolerated [28,29,30]. Xanomeline, combined with trospium, improved cognitive and negative schizophrenia symptoms in phase 2 and 3 clinical trials, because in schizophrenia a reduced cholinergic signaling occurs in the hippocampus, dorsolateral prefrontal cortex, and basal ganglia (see Table 2) [31,32,33,34,35]. According to the neural networks involved schizophrenia, a direct interaction between D2 dopaminergic and M1 and M4 muscarinic cholinergic neurons exists in the hippocampus and prefrontal cortex (see Figure 1). M1 and M4 muscarinic cholinergic neurons activate medium spiny neurons in the prefrontal cortex, namely GABAergic and somatostatinergic neurons, which strongly presynaptically inhibit D2 dopaminergic neurons via GABAA and somatostatin 1 receptors. D2 dopaminergic neurons activate GABAergic neurons, and the latter neurons inhibit glutamatergic neurons, which transmit an activating potential via NMDA receptors to muscarinic cholinergic neurons [36].
A positive allosteric modulator of the M4 receptor is emraclidine, which has been tested in a phase 2 clinical trial in comparison to placebo. In this trial, emraclidine ameliorated positive, negative and cognitive schizophrenia symptoms [37].
Neural pathways involved in schizophrenia in the prefrontal cortex. Classical neurotransmitters and neuropeptides: Ach: acetylcholine; DA: dopamine; GABA: gamma-aminobutyric acid; Glu: glutamate; SST: somatostatin. Specific receptors: D2: dopaminergic receptor; GABAA: GABAergic receptor; M1: muscarinic cholinergic receptor; NMDA: ionotropic glutamatergic receptor; SST1: somatostatin receptor. A minus mark signifies a presynaptic inhibitory potential, and a plus mark signifies a postsynaptic excitatory potential. A minus and plus mark signifies a partial agonism at the specific receptor. The presynaptic inhibitory neurotransmitters and receptors are painted in grey. The therapeutic effect of new antipsychotic drugs, namely the TAAR1 agonist ulataront and the M1 and M4 receptor agonist xanomeline combined with trospium, cariprazine (Car), brexipiprazole (Brex) and lumateperone (Lum) are included in the figure.
5. Phase III Clinical Studies
The recently developed second-generation antipsychotic drugs such as cariprazine, brexipiprazole, lumateperone, the non-antidopaminergic antipsychotic drugs such as TAAR1 agonists, and the combination of the M1 and M4 receptor agonist xanomeline with trospium, underwent all phase 3 clinical studies. In a phase 3b randomized, double-blind clinical study, cariprazine was compared to risperidone in the treatment of predominant negative schizophrenia symptoms. 227 patients were included in the cariprazine group, and 229 patients belonged to the risperidone group. The treatment was continued for 26 weeks. Cariprazine improved PANSS (Positive and Negative Schizophrenia Syndrome Scale) better than risperidone, above all negative schizophrenia symptoms [45]. A 3 to 8-week pivotal study about the effect of cariprazine on cognitive function was performed, including the Cognitive Drug Research System attention battery. An improvement of cognitive functions in power of attention was observed when 3 mg cariprazine was administered, but not for 6 mg cariprazine. An improvement in continuity of attention was observed with 3 and 6 mg cariprazine [46].
In a retrospective, observational study in Japan, the discontinuation rate was compared in a cohort of 978 patients treated with brexipiprazole and 4898 patients treated with other atypical antipsychotics, for example aripiprazole, olanzapine, quetiapine or risperidone. Patients treated with brexipiprazole were less likely to discontinue the treatment than patients treated with the above mentioned atypical antipsychotics. Consequently, brexipiprazole might contribute to continue antipsychotic treatment [47]. Brexipiprazole, examined in clinical studies, ameliorated positive and negative schizophrenia symptoms, besides depressive and manic and cognitive symptoms [21,22].
In a randomized, placebo-controlled clinical study, 450 patients were enrolled and were treated in a short-term treatment with lumateperone or with placebo. After treatment, the PANSS and the Clinical Global Impression-Severity of Illness (CGI-S) scores were determined. Both scores were improved in comparison to placebo, and no motor, cardiovascular nor endocrine adverse effects were seen [48].
The TAAR1 agonist ulataront has been examined in phase 3 clinical trials, and it improved positive and negative schizophrenia symptoms. Besides, it ameliorated cognitive functions, however an acute schizophrenia exacerbation has been reported as an adverse effect. It did not cause movement disturbances, nor did it raise prolactin levels [27,28].
M1 and M4 subreceptors stimulation in schizophrenia might be a new pharmacological strategy, because a reduced muscarinic cholinergic activity decreased cognitive function and caused negative schizophrenia symptoms [13]. Positive allosteric modulators of M1 and M4 receptors exerted antipsychotic activities in amphetamine- and MK 801-induced hyperlocomotion tasks in animal experiments [13]. Emraclidine, a positive allosteric modulator of the M4 receptor, and xanomeline, combined with trospium were examined in a phase 3 clinical trial. Both compounds improved positive and negative schizophrenia symptoms, as well as depressive and manic and cognitive symptoms [29].
6. Discussion
Schizophrenia and schizoaffective disorder are generally treated with second-generation antipsychotic drugs, which are mostly D2 and 5-HT2A receptor antagonists. These drugs improve positive schizophrenia symptoms very well; however, they treat negative schizophrenia symptoms to a small extent, nor do they improve cognitive functions. Movement disturbances, i.e., EPS still occur, and raised prolactin levels are often seen. The antipsychotic drug clozapine does not alter movement, nor does it raise prolactin levels, as a consequence of a different mechanism of action. Another question that should be answered in long-term clinical studies, is whether the new antipsychotic drugs are secure in preventing rehospitalization of schizophrenia patients, after psychotic symptoms get worse. Genetic techniques should also be applied to choose the appropriate antipsychotic drug, the SNP’s of some important risk genes for schizophrenia should be examined and might be correlated with an improved therapeutic effect of a specific antipsychotic drug. Thus, an antipsychotic drug with a higher therapeutic effect could be selected. Some second-generation antipsychotic drugs such as cariprazine, brexipiprazole and lumateperone have a partial agonism at dopaminergic and serotonergic receptors. In phase 3 clinical studies, it was found that these new drugs better treat positive and negative schizophrenia symptoms, and above all cognitive functions. The discontinuation rate was better than with other second-generation antipsychotic drugs. Some new antipsychotic drugs have been reported, which do not have an antagonism at dopaminergic receptors. The TAAR1 ulataront stimulates TAAR1 receptors and stabilizes the monoamine neurotransmission. In phase 3 clinical trials, it improved positive and negative schizophrenia symptoms, it ameliorated cognitive functions and ameliorated affective symptoms. It did not cause movement disturbances, nor did it raise prolactin levels. An acute schizophrenia exacerbation can occur as an adverse effect. New promising antipsychotic drugs are the M4 and M1 receptor agonist xanomeline, in combination with trospium, and the positive M4 receptor allosteric modulator emraclidine. These drugs exert antipsychotic effects, which can be explained by the neural networks involved in schizophrenia. M1 and M4 muscarinic cholinergic neurons and D2 dopaminergic neurons exert an interaction upon each other in the prefrontal cortex. A stimulation of M1 and M4 receptors leads to antagonism at D2 dopaminergic neurons. Besides, it improves cognitive functions. In phase 3 clinical studies, these new drugs improved positive and negative schizophrenia symptoms well, they improved cognitive functions, and ameliorated depressive and manic symptoms. The occurrence of movement disturbances and endocrine and cardiovascular adverse effects were largely reduced. The approval of xanomeline by FDA is expected in September 2024.
7. Conclusion and Future Perspectives
In order to compare the therapeutic effects of widely used second-generation antipsychotic drugs with novel antipsychotic drugs, more clinical trials should be performed. In these clinical studies, PANSS score should be determined, above all that regarding the negative schizophrenia symptoms. Besides, cognitive functions should be evaluated by an assessment. The results might give a hint to replace the second-generation antipsychotic drugs by novel antipsychotic drugs.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Werner, F.M.; Coveñas, R. Classical neurotransmitters and neuropeptides involved in schizoaffective disorder: Focus on prophylactic medication; Bentham Science Publishers: Sharjah, 2016. [Google Scholar]
- Correll, C.U.; Arango, C.; Fagerlund, B.; Galderisi, S.; Kas, M.J.; Leucht, S. Identification and treatment of individuals with childhood onset and early-onset schizophrenia. Eur Neuropsychopharmacol. 2024, 82, 57–71. [Google Scholar] [CrossRef]
- Phawa, M.; Sleem, A.; Elsayed, O.H.; Good, M.E.; El Mallakh, R.S. New antipsychotic medications in the last decade. Curr. Psychiatry Rep. 2021, 23, 87. [Google Scholar]
- Werner, F.M.; Coveñas, R. Updated neural networks in schizophrenia and novel antipsychotic drugs. Clin. Neurophysiol. 2023, 148, e1–e7. [Google Scholar] [CrossRef]
- de Bartolomeis, A.; Ciccarelli, M.; Velucci, L.; Fornaro, M.; Iasevoli, V.; Barone, A. Update on novel antipsychotics and pharmcological strategies for treatment-resistant schizophrenia. Expert Opin Pharmacother 2022, 23, 2035–2035. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Abi-Dargham, A.; Howes, O. Emerging treatments in schizophrenia. J. Clin. Psychiat. 2022, 83, SU21024IP1. [Google Scholar] [CrossRef] [PubMed]
- Mauri, M.C.; Paletta, S.; Di Pace, C.; Reggiori, A.; Cirnigliaro, G.; Valli, I.; Altamura, A.C. Clinical pharmacokinetics of atypical antipsychotics: An update. Clin. Pharmacokinet. 2019, 58, 1219–1220. [Google Scholar] [CrossRef] [PubMed]
- Werner, F.M.; Coveñas, R. Safety of antipsychotic drugs: Focus on therapeutic and adverse effects. Expert Opin. Drug Saf. 2014, 13, 1031–1042. [Google Scholar] [CrossRef]
- Orzelska-Górka, J.; Mikulska, J.; Wiszniewska, A.; Biala, G. New atypical antipsychotics in the treatment of schizophrenia and depression. Int J Mol Sci. 2022, 23, 10624. [Google Scholar] [CrossRef] [PubMed]
- Mohr, P.; Masopust, J.; Kopecek, M. Dopamine receptor partial agonists: Do they differ in their clinical efficacy? Front. Psychiatry 2022, 12, 781946. [Google Scholar] [CrossRef]
- Wu, H.; Siafis, S.; Hamza, T.; Schneider-Thoma, J.; Davis, J.M.; Salanti, G.; Leucht, S. Antipsychotic-induced weight gain: Dose-response meta-analysis of randomized controlled trials. Schizophr. Bull. 2022, 48, 643–654. [Google Scholar] [CrossRef]
- Schneider-Thoma, J.; Chalkou, K.; Dörries, C.; Bighelli, I.; Ceraso, A.; Huhn, M.; Siafis, S.; Davis, J.M.; Cipriani, A.; Furukawa, T.A.; et al. Comparative efficacy and tolerability of 32 oral and injectable long-acting antipsychotics for the maintenance treatment of adults with schizophrenia: A systematic review and network meta-analysis. Lancet 2022, 399, 824–836. [Google Scholar] [CrossRef] [PubMed]
- Dean, B.; Scarr, E. Muscarinic M1 and M4 receptors: Hypothesis driven drug development for schizophrenia. Psychiatry Res. 2020, 288, 112989. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.C.; Tsai, S.-J. New targets for schizophrenia treatment beyond the dopamine hypothesis. Int. J. Mol. Sci. 2017, 17, 1689. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, M.L.R.; Hermann, L.E.; Brown, S.; Jones, P.G.; Shao, L.; Hewitt, M.C.; Campbell, J.E.; Dedic, N.; Hopkins, S.C.; Koblan, K.S.; et al. Ulotaront: A TAAR1 agonist for the treatment of schizophrenia. ACS Med. Chem. Lett. 2022, 13, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Caccia, S.; Invernizzi, R.W.; Nobili, A.; Pasina, L. A new generation of antipsychotics: Pharmacology and clinical utility of cariprazine in schizophrenia. Ther. Clin. Risk Manag. 2013, 9, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Werner, F.M.; Coveñas, R. New developments in the management of schizophrenia and bipolar disorder: Potential use of cariprazine. Ther. Clin. Risk Manag. 2015, 11, 1657–1661. [Google Scholar] [PubMed]
- Laszlovsky, I.; Barbassy, A.; Nemeth, G. Cariprazine, a broad-spectrum antipsychotic for the treatment of schizophrenia: Pharmacology, efficacy and safety. Adv. Ther. 2021, 38, 3652–3673. [Google Scholar] [CrossRef] [PubMed]
- Mohr, P.; Masopust, J.; Kopecek, M. Dopamine receptor partial agonists: Do they differ in their clinical efficacy? Front. Psychiatry 2022, 12, 781946. [Google Scholar] [CrossRef] [PubMed]
- Grossberg, G.T.; Kohegyi, E.; Mergel, V.; Josiassen, M.K.; Meulier, D.; Hobart, M.; Slomkowski, M.; Baker, A.R.; McQuade, R.D.; Cummings, J.L. Efficacy and safety of brexipiprazole for the treatment of agitation in Alzheimer’s dementia: Two 12-week, randomized, double-blind, placebo-controlled trials. Am. J. Geriatr. Psychiatry 2020, 28, 383–400. [Google Scholar] [CrossRef]
- Ishigooka, J.; Iwashita, S.; Igashi, K.; Liew, E.L.; Tadori, Y. Pharmacokinetics and safety of brexipiprazole following multiple-dose administration to Japanese patients with schizophrenia. J. Clin. Pharmacol. 2018, 58, 74–80. [Google Scholar] [CrossRef]
- Greig, S.L. Brexipiprazole: First global approval. Drugs 2015, 75, 1687–1697. [Google Scholar] [CrossRef] [PubMed]
- Edinoff, A.; Wu, N.; de Boisblanc, C.; Feltner, C.O.; Norder, M.; Tzoneva, V.; Kaye, A.M.; Cornett, E.M.; Kaye, A.D.; Viswanath, O.; et al. Lumateperone for the treatment of schizophrenia. Psychopharmacol. Bull. 2020, 50, 32–59. [Google Scholar] [PubMed]
- Werner, F.M.; Coveñas, R. The novel antipsychotic drug cariprazine and cognition enhancing drugs: Indications for their use as the add-on therapy in schizophrenia. Curr. Pharm. Des. 2021, 27, 4033–4038. [Google Scholar] [CrossRef] [PubMed]
- Blair, H.A. Lumateperone: First approval. Drugs 2020, 80, 417–423. [Google Scholar] [CrossRef]
- Snyder, G.L.; Vanover, K.E.; Davis, R.E.; Li, P.; Fienberg, A.; Mates, S. A review of the pharmacology and clinical profile of lumateperone for the treatment of schizophrenia. Adv. Pharmacol. 2021, 90, 253–276. [Google Scholar] [PubMed]
- Dodd, S.; Carvalho, A.F.; Puri, B.K.; Maes, M.; Bertolasci, C.C.; Morris, B.; Berk, M. Trace amine-associated receptor 1 (TAAR1): A new drug target for psychiatry? Neurosci. Biobehav. Rev. 2021, 120, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Koblan, K.S.; Kent, J.; Hopkins, S.C.; Krystal, J.H.; Cheng, H.; Goldman, R.; Loebel, A. A non-D2-receptor-binding drug for the treatment of schizophrenia. N. Eng. J. Med. 2020, 382, 1497–1506. [Google Scholar] [CrossRef] [PubMed]
- Dean, B. Muscarinic M1 and M4 receptor agonists for schizophrenia: Promising candidates for the therapeutic arsenal. Expert Opin. Investig. Drugs 2023, 32, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Kaul, I.; Sawchak, S.; Correll, C.U.; Kakar, R.; Breier, A.; Zhu, A.; Miller, A.C.; Paul, S.M.; Brannan, S.K. Efficacy and safety of the muscarinic receptor agonist KarXT (xanomeline-trospium) in schizophrenia (EMERGENT-2) in the USA: Results from a randomised, double-blind, placebo-controlled, flexible-dose phase 3 trial. Lancet 2024, 403, 160–170. [Google Scholar] [CrossRef]
- Jones, C.K.; Byun, N.; Bubser, M. Muscarinic and nicotinic acetylcholine receptor agonists and allosteric modulators for the treatment of schizophrenia. Neuropsychopharmacology 2012, 37, 16–42. [Google Scholar] [CrossRef]
- Jones, C.K.; Eberle, E.L.; Shaw, D.B.; McKinzie, D.L.; Shannon, H.E. Pharmacologic interactions between the muscarinic cholinergic and dopaminergic systems in the modulation of prepulse inhibition in rats. J. Pharmacol. Exp. Ther. 2005, 312, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, M.; Wess, J.; Fulton, B.S.; Fink-Jensen, A.; Caine, S.B. Modulation of prepulse inhibition through both M1 and M 4 muscarinic receptors in mice. Psychopharmacology (Berlin) 2010, 208, 401–416. [Google Scholar] [CrossRef] [PubMed]
- Thorn, C.A.; Popiolek, M.; Stark, E.; Edgerton, J.R. Effects of M1 and M4 activation on excitatory synaptic transmission in CA1. Hippocampus 2017, 27, 794–810. [Google Scholar] [CrossRef] [PubMed]
- Crook, J.M.; Tomaskovic-Crook, E.; Copolov, D.L.; Dean, B. Decreased muscarinic receptor binding in subjects with schizophrenia: A study of the human hippocampal formation. Biol. Psychiatry 2000, 48, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Werner, F.; Coveñas, R. New, not anti-dopaminergic antipsychotic drugs in the treatment of schizophrenia, M4 or M1 receptor agonists and TAAR1 agonists. Clin. Neurophysiol. 2024, 159, e1–e54. [Google Scholar] [CrossRef]
- Krystal, J.H.; Kane, J.M.; Correll, C.U.; Walling, D.P.; Leoni, M.; Duvvuri, S.; Patel, S.; Chang, I.; Iredale, P.; Frohlich, L.; et al. Emraclidine, a novel positive allosteric modulator of cholinergic M4 receptors, for the treatment of schizophrenia: A two-part, randomised, double-blind, placebo-controlled, phase 1b trial. Lancet 2022, 400, 2210–2220. [Google Scholar] [CrossRef] [PubMed]
- Corponi, F.; Fabri, C.; Bitter, I.; Montgomery, S.; Vieta, E.; Kapser, S.; Pallanti, S.; Serretti, A. Novel antipsychotics specificity profile: A clinically oriented review of lurasidone, brexpiprazole, cariprazine and lumateperone. Eur Neuropsychopharmacol. 2019, 29, 971–985. [Google Scholar] [CrossRef] [PubMed]
- Citrome, L. Activating and Sedating Adverse Effects of Second-Generation Antipsychotics in the Treatment of Schizophrenia and Major Depressive Disorder: Absolute Risk Increase and Number Needed to Harm. J Clin Psychopharmacol 2017, 37, 138–147. [Google Scholar] [CrossRef]
- Barmann, R.; Mujumder, P.; Doifode, T.; Kablinger, A. Newer antipsychotics: Brexpiprazole, cariprazine, and lumateperone: A pledge or another unkept promise? World J Psychiatry 2021, 11, 1228–1238. [Google Scholar] [CrossRef]
- Edinoff, A.; Ruoff, M.F.; Ghaffar, Y.T.; Rezayev, A.; Jani, T.; Kaye, A.M.; Cornett, E.M.; Kaye, A.D.; Viswanath, O.; Urits, I. Carprazine to treat Schizophrenia and Bipolar Disorder in Adults. Psychopharmacol Bull 2020, 50, 83–117. [Google Scholar]
- Breier, A.; Brannan, S.K.; Braun, S.M.; Miller, A.C. Evidence of trospium’s ability to mitigate cholinergic adverse events related to xanomeline: Phase 1 study results. Psychopharmacology (Berl). 2023, 240, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.K.O.; Noetzel, M.J.; De Lorme, K.C.; Jukubík, J.; Dolezal, V. Pharmacological evaluation of the long-term effects of xanomeline on the M(1) muscarinic acetylcholine receptor. PLoS ONE 2010, 5, e15722. [Google Scholar] [CrossRef] [PubMed]
- Russel, K.J.; Ingram, S.M.; Teal, L.B.; Linsley, C.W.; Jones, C.K. M1/M4-Preferring Muscarinic Cholinergic Receptor Agonist Xanomeline Reverses Wake and Arousal Deficits in Nonpathologically Aged Mice. ACS Chem. Neurosci. 2023, 14, 435–457. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, G.; Laszlovszky, I.; Czobor, P.; Szalai, E.; Szatmari, B.; Harsanyi, J.; Barabassy, A.; Debelle, M.; Durgam, S.; Bitter, I.; et al. Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: A randomised, double-blind, controlled trial. Lancet 2017, 389, 1103–1113. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Daniel, D.G.; Vieta, E.; Laszlovszky, I.; Goetgebeur, P.J.; Earley, W.R.; Patel, M.D. The efficacy of cariprazine on cognition: A post hoc analysis from phase II/III clinical trials in bipolar mania, bipolar depression, and schizophrenia. CNS Spectr. 2023, 28, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Hishimoto, A.; Yasui-Furukori, N.; Sekine, D.; Matsukawa, M.; Yamada, S. Treatment discontinuation among patients with schizophrenia treated with brexpiprazole and other oral atypical antipsychotics in Japan: A retrospective observational study. Adv. Ther. 2022, 39, 4299–4314. [Google Scholar] [CrossRef]
- Correll, C.U.; Davis, R.E.; Weingart, M.; Saillard, J.; O’Gorman, C.; Kane, J.M.; Lieberman, J.A.; Tamminga, C.A.; Mates, S.; Vanover, K.E. Efficacy and safety of lumateperone for treatment of schizophrenia. A ramomized clinical trial. JAMA Psychiatry 2020, 77, 349–358. [Google Scholar] [CrossRef]
Figure 1.
Mechanisms of action of novel antipsychotic drugs in the brain centers involved in schizophrenia.
Figure 1.
Mechanisms of action of novel antipsychotic drugs in the brain centers involved in schizophrenia.
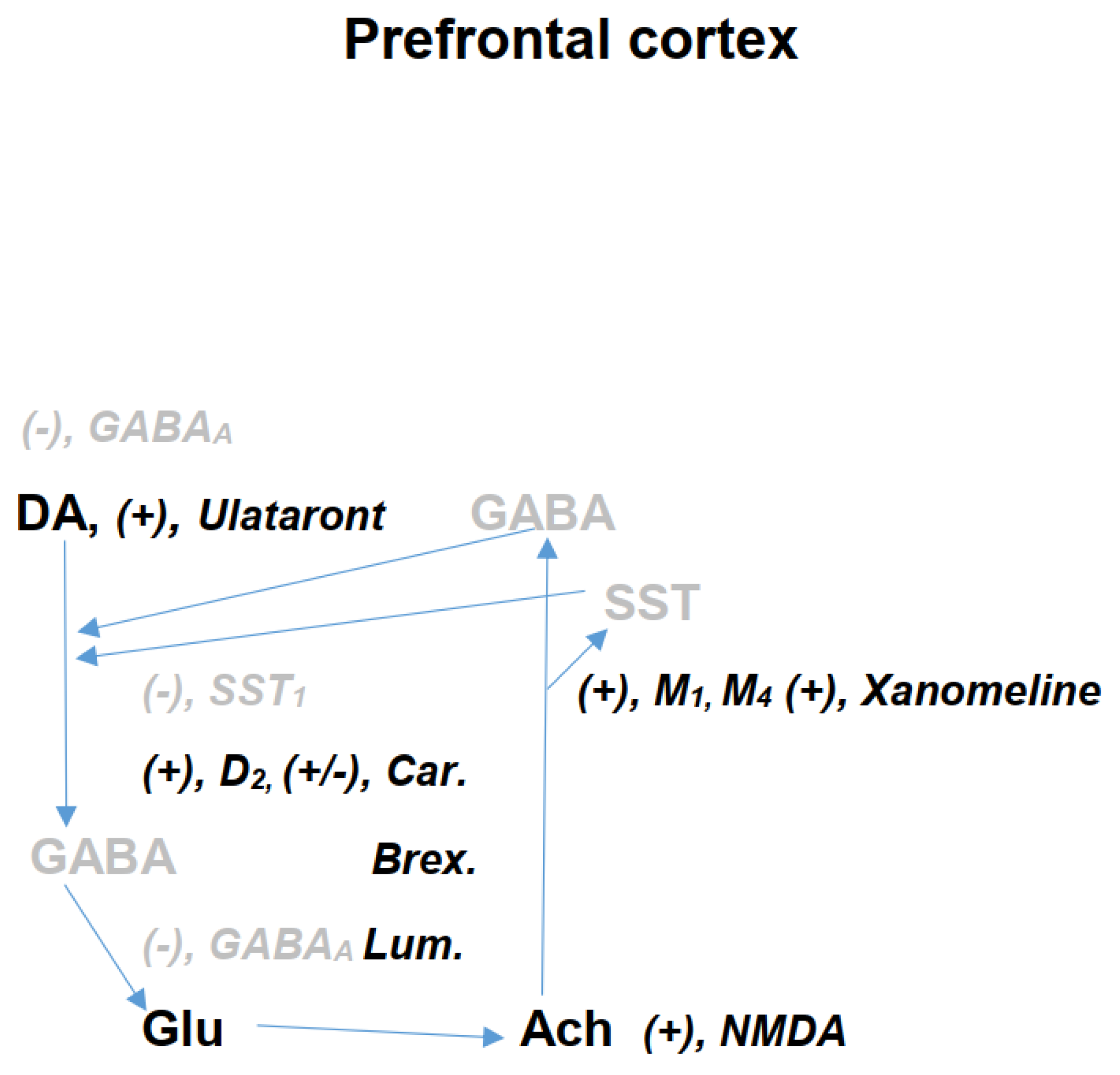
Table 2.
Therapeutic effects of second- and third-generation antipsychotic drugs.
| Second-generation antipsychotic drugs | |
| Criterium | 2nd generation antipsychotic drugs |
| Therapeutic effect on disorder symptoms | Good therapeutic effect on positive schizophrenia symptoms |
| Therapeutic effect on negative schizophrenia symptoms | Reduced therapeutic effect on negative schizophrenia symptoms |
| Therapeutic effect on cognitive symptoms | No therapeutic effect on cognitive symptoms |
| References | 5 - 36 |
| Mechanism of action of 3rd generation antipsychotic drugs | |
| Antipsychotic drug | Mechanism of action |
| Cariprazine | Partial agonism at D2 and D3 receptors and an agonism at 5-HT1A receptors |
| Brexipiprazole | Partial agonism at D2 receptors and an agonism at 5-HT1A receptors |
| Lumateperone | Partial agonism at D2 and 5-HT2A receptors, blocks serotonin reuptake and interfers with the glutamate neurotransmission |
| Lumataront | Agonism at TAAR1 receptors and 5-HT1A receptors |
| Xanomeline | Agonism at M4 and M1 receptors, which interacts with a D2 receptor blockade |
| Therapeutic and adverse effects of 3rd generation antipsychotic drugs | |
| Therapeutic effects on positive schizophrenia symptoms | Improves well. |
| Therapeutic effects on negative schizophrenia symptoms | Improves well. |
| Therapeutic effects on cognitive symptoms | Exerts a good therapeutic effect. |
| Movement disturbances | Very reduced |
| Metabolic and cardiac adverse effects | Very rarely and very reduced |
| References | 5 - 37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



