
Submitted:
19 May 2024
Posted:
20 May 2024
You are already at the latest version
Abstract
Asthma is a significant public health concern. This study identified the provinces with the highest morbidity and mortality rates due to asthma among the working-age population (15-69 years) in the Republic of Ecuador. The secondary objective was to explain the possible differences attribut-able to occupational exposure. This nationwide ecological and exploratory study was conducted in 24 provinces between 2016 and 2019. Government databases were used as sources of infor-mation. Standardized rates were calculated for codes the J45 and J46. The hospitalization mor-bidity rate for asthma decreased from 6.51 to 5.76 cases per 100,000 working-age population, and the mortality rate has consistently been low and stable from 0.14 to 0.15 deaths per 100,000 working-age population. Geographic differences between the provinces were evident. The risk of hospitalization and death due to asthma was higher in the Pacific coast (five provinces) and the Andean region (two provinces). The high rates observed in provinces with greater agricultural and industrial development could be the main determinants of national heterogeneity and could act as occupational risk factors. The contribution of occupational hazards in each province should be examined in depth through ad hoc studies. These findings provide valuable information for creating public policies aimed at promoting and safeguarding the respiratory health of the popu-lation, particularly that of workers.
Keywords:
asthma
; working-age population
; geographic differences
; respiratory diseases
; public health
1. Introduction
Asthma is a non-communicable disease characterized by narrowing of the airways and can affect individuals of all age groups [1,2]. The global prevalence of asthma has increased significantly in recent decades, while mortality rates have decreased. In 2019, an estimated 262 million people were affected by asthma, resulting in 455,000 deaths [3]. Consequently, asthma is considered a major global public health issue because of its reduced quality of life and premature death [4].
Although the age at which asthma develops can vary, it is commonly observed in young adults, who are part of the labor-productive population. In this context, when directly linked to work-related activities, it can be considered an occupational health issue [5,6]. Occupational asthma can be triggered by exposure to various factors in the workplace, such as chemical and biological agents that act as sensitizing and irritating substances [7]. Certain economic sectors and geographical areas may also have a higher likelihood of developing occupation-related diseases among in the working population.
For example, this issue has been identified among workers in both industrial and agricultural settings [8]. It is crucial to emphasize that socioeconomic factors, lifestyles of people in each location, and access to healthcare can affect the early detection and subsequent treatment of the condition [9]. Consequently, the examination of asthma disparities between different regions of the same country is particularly interesting [10], as it could provide valuable information for the creation of public policies aimed at safeguarding and promoting the health of the population, particularly workers [11].
In the Republic of Ecuador (hereafter referred to as "Ecuador"), there is a lack of studies on the morbidity and mortality rates of asthma in working-age population, particularly when disaggregated by territory. Another gap in knowledge regarding this issue is the lack of reporting of occupational diseases among workers affiliated with the social security system [12]. Between 2016 and 2019, the only years for which records were available, 64 cases of occupational asthma were reported in Ecuador. Pichincha accounted for 35.9% of the cases, whereas Guayas accounted for 28.1%, making them the provinces with the highest concentrations (see Supplementary Table S1). There is likely to be an undisclosed reality in the other provinces of the country.
This study aimed to identify the Ecuadorian provinces with the highest rates of morbidity and mortality due to asthma among the working-age population and to examine any potential geographic differences with respect to environmental factors, particularly occupational risks.
2. Materials and Methods
2.1. Context and Population
Ecuador, situated in northern South America, covers an approximate area of 256,370 km2 and is known for its rich cultural diversity and significant climatic variation owing to its geography. With approximately 17.3 million inhabitants in 2019, the urban areas of the provinces of Pichincha (with the capital Quito) and Guayas comprise a significant proportion of the population (43.4%). The service sector is predominant in most of the provinces. However, it is worth mentioning mining and oil extraction in the provinces of the Amazon Region and agricultural-related activities in the interior (Andean Region) and Pacific coast.
The working-age population in this study was between 15 and 69 years. This age group substantially contributes to the economy. In this country, the working-age population totals 11.9 million persons, representing 68.8% of the entire population (2019), with 51% being women and 49% being men.
2.2. Design, Data Sources and Statistical Analysis
A comprehensive ecological and longitudinal study was conducted across 24 provinces, extending to the Galapagos Islands, using the administrative records of hospital care and medical certificates of death from 2016 to 2019. Information was obtained from the Statistical Register of Hospital Beds and Emergencies, which records the number of individuals treated within the Integrated Public Health Network, and the General Defunction Register, which documents the causes of death based on the International Classification of Diseases (ICD-10). Both sources underwent statistical quality control before being published on the Web (Open Access Database). Codes J45 [asthma: predominantly allergic asthma (J45.0), nonallergic asthma (J45.1), mixed asthma (J45.8) and unspecified (J45.9)] and J46 (status asthmaticus) were selected. These codes have been used in previous studies to quantify the number of deaths and work-related asthma diseases resulting from exposure to hazardous chemicals as well as air, water, and soil pollution in occupational environments [12,14].
For the data extraction, the province of residence was considered, assuming that it was also a place of work. Foreign residents (nine diagnosed cases and no deaths) were excluded from the analysis. From 2016 to 2019, 2,786 patients were diagnosed and 64 individuals died.
The estimated annual rates of asthma morbidity and mortality are expressed for the selected codes per 100,000 person-years. To compare the provinces and control for the effect of population composition, standardized rates (ASR) and their corresponding confidence intervals (95%CI) were calculated using the direct method, considering the Ecuadorian population standard for defined ages of 15 to 69 years. The denominator used for the ASR was obtained from the population projections of the National Institute of Statistics and Censuses (see Supplementary Table S2).
Owing to the limited duration of the four-year period in question, linear regression analysis was used to show statistically significant changes in the Slopes of the ASR (increasing or decreasing). Finally, a quadrant chart was used to illustrate the average asthma mortality and morbidity rates for each province. The findings were examined to provide potential explanations for working conditions at the provincial level.
3. Results
The hospitalization morbidity rate for asthma in Ecuador decreased from 6.51 to 5.76 cases per 100,000 working-age population between 2016 and 2019. However, no significant reduction was observed (slope = − 0.28, p = 0.122). The asthma mortality rate has been low and consistently stable (slope = 0.01, p = 0.599), with values ranging between 0.14 and 0.15 deaths per 100,000 working-age population.
3.1. Morbidity by Provinces
Table 1 presents the prevalence and annual rates of hospital morbidity for asthma among the working-age population across the 24 provinces of the national territory. The provinces with the highest average prevalence were Pichincha (19.7%), Guayas (18.2%) and Manabí (10.4%).
Nonetheless, when calculating the ASR, eight provinces reported higher morbidity rates for asthma than the national average (7.82 cases per 100,000 inhabitants). The most significant provinces in the Amazon Region are Zamora Chinchipe, Morona Santiago, Sucumbíos, and Loja in the Andean Region. According to the statistical analysis, El Oro province decreased from 9.68 (95% CI, 7.03-12.99) to 55.76 (95% CI, 3.83-8.33) cases per 100,000 working-age population (Slope = –1. 34, p = 0.018), while Chimborazo province increased from 5.72 (95% CI, 3.38-9.04) to 9.35 (95% CI, 6.35-13.28) cases per 100,000 working-age population (Slope = 1.17, p = 0.008).
3.2. Mortality by Provinces
Regarding asthma mortality, during the study period, some provinces did not report any cases, whereas others only reported cases in some years. Table 2 shows only those provinces that reported asthma-related deaths over the consecutive years.
Guayas (29.8%) and Manabí (24.3%) had the highest average number of asthma-related deaths due to asthma. The province of Los Ríos, located in the Pacific Region, was distinguished by its high mortality rate from asthma, which remained above the national average throughout the period (0.36 deaths per 100,000 working-age population). The province of Esmeraldas was notable for its significant increase between 2017 and 2018, although no cases were reported in the following year.
3.3. Identification of the Provinces with the Highest Morbidity and Mortality
The use of individual rates alone is insufficient for identifying the most problematic provinces. In line with our approach, we used a quadrant chart to classify the provinces based on their combined morbidity and mortality ASRs. This classification was only applied to provinces that had reported cases for more than two consecutive years, as depicted in Figure 1.
4. Discussion
The outcomes of the current investigation reveal disparities that contrast with global patterns in the prevalence of asthma morbidity and mortality [4] and challenge those documented in other settings [15]. In our study, we observed a decrease in the morbidity rate and an increase in the mortality rate in the age range of 15–69 years. Distinctions between the provinces of Ecuador were evident from 2016 to 2019.
As mentioned at the beginning of the study, such differences may be due to a variety of determining factors specific to each region [10], even within the peculiarities of each territory of our country. Considering the complexity of establishing more specific causal relationships and the lack of further information, we provide reasonable considerations that could explain the differences observed between the provinces identified in this exploratory study. To this end, we addressed two blocks focused on climate and environmental factors, as well as, with particular interest, those possible exposures to specific occupational risks present in the working conditions by the economic activity of each province that could have been the cause of the development of occupational asthma.
4.1. Environmental and Geoclimatic Factors
Several studies have associated the development of asthma with mold and fungal exposure in the home environment [16,17]. In relation to the above quadrant (Figure 1), the provinces of Esmeraldas, Manabí, and El Oro (including Guayas) are located in the coastal region of the country and are characterized by a humid tropical climate with an average annual temperature ranging between 24-31 °C, as well as rainy seasons from December to April-May. It can be assumed that these climatic particularities increased the likelihood of hospital care during certain seasons. In contrast, a significant association between low temperature and asthma has been demonstrated [18]. In addition (Figure 4), the provinces of Azuay are located in the Andes Mountains, and because of their altitude (more than 2,500 feet above the mean sea level), temperatures can decrease to 6 °C.
Furthermore, it is important to note that different studies have found that asthma is more prevalent in urban areas of regions with a higher population density and consequent exposure to environmental pollution [6,19]. In our study, Guayas and Pichincha were the two most populous and industrialized provinces in the country, especially in the city of Guayaquil (Guayas).
4.2. Attributable Occupational Factors
Asthma is a complex disease that can be diagnosed and affected by several factors. In particular, the labor risk of each economic activity plays a key role. The Azuay and Guayas provinces have the largest number of enterprises in the industrial sector. It has been widely demonstrated that workers exposed to chemical agents have a higher prevalence and risk of developing occupational asthma induced by both sensitizers and irritants [6,7]. Additionally, agro-industrial activities predominated in the provinces of El Oro and Los Ríos (in addition to Guayas). Similarly, exposure to insecticides, fungicides, and herbicides can cause asthma in working-age population [9].
In our study, Orellana (increase in morbidity from 2.46 in 2016 to 6.83 in 2019) and Santa Elena (increase in morbidity from 3.49 in 2016 to 5.25 in 2019) were not among the provinces with the highest morbi-mortality from asthma; they stand out as the only provinces that have shown increases in morbidity rates. Notably, these provinces had two oil refineries. It is presumed that exposure (environmental and occupational) to chemicals used during the refining processes could influence this fact [20]. The province of Esmeraldas, which has the second highest mortality rate and the largest refinery in the country, would leave less uncertainty.
Finally, the province of Manabí (Manta city), has experienced remarkable urban developments in recent years. It is plausible that the high morbidity from asthma may also be due to inhalation of wood, silica, asbestos, and solvents, as well as exposure to welding smoke among construction workers [21].
4.3. Opportunities for Respiratory Health Promotion
This study had some limitations that must be considered. First, the use of secondary sources of information restricted more rigorous analyses to identifying the most affected economic sectors and occupations. This information would have been useful for identifying the most vulnerable workers [8]. Although the quality of administrative records has improved in recent years, it is possible that there is an important diagnosis exists in this context [15]. Furthermore, it is important to note that we did not find a correlation between the standardized rates of morbidity and asthma mortality in the identified provinces.
This finding suggests a need to counteract future research hypotheses that help explain it. These limitations do not alter the findings in terms of geographical heterogeneity or the behavior of the observed trends. This study provides insights into the importance of this respiratory disease and provides the first approach to the current situation in the country for the working-age population [22,23]. Additionally, our results provide a breakdown analysis by provincial unit and updated knowledge from previous research [24].
5. Conclusions
In conclusion, this study makes a noteworthy contribution by highlighting the insufficient understanding of asthma among working-age groups in Ecuador at a regional level. Environmental factors, including climatic conditions and pollution, together with occupational exposure, particularly in the industrial and agro-industrial sectors, play important roles in the prevalence of asthma. Geographic identification in provinces with high morbimortality should be considered a priority for the implementation of prevention and respiratory health promotion programs [25]. Currently, there is an urgent need to slow the normal decline with aging or in response to common or occupational exposures as an essential part of any primary prevention initiative. Nevertheless, additional research is required to better understand this issue better.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Occupational asthma cases in the Republic of Ecuador, 2016–2019; Table S2: Average percentage distribution of the working-age population (15-69 years) by provinces of the Republic of Ecuador, 2016–2019.
Author Contributions
Conceptualization: A.R.G.G. and D.M.; Data curation: A.R.G.G., A.L.C.P. and D.M.; Formal analysis: A.R.G.G.; Methodology: A.R.G.G. and D.M.; Writing—original draft: A.R.G.G.; Writing—review and editing: A.R.G.G., A.L.C.P., D.M. and D.D.G. All authors have read and agreed to the published version of the manuscript.
Funding
This work was conducted within the framework of the research program of the Ecuadorian Observatory of Occupational Safety and Health of the Espiritu Santo University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All studies in our study are included in the Supplementary Materials.
Conflicts of Interest
All authors declare no conflicts of interest.
References
- Mims, J.W. Asthma: definitions and pathophysiology. Int. Forum Allergy Rhinol. 2015, 5 Suppl 1, S2–S6. [Google Scholar] [CrossRef]
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Asthma. Available online: https://www.who.int/news-room/fact-sheets/detail/asthma#:~:text=Asthma%20affected%20an%20estimated%20262,help%20to%20reduce%20asthma%20symptoms (accessed on 5 June 2023).
- Vlaski, E.; Stavrikj, K.; Kimovska, M.; Cholakovska, V.C.; Lawson, J.A. Divergent trends in the prevalence of asthma-like symptoms and asthma in a developing country: three repeated surveys between 2002 and 2016. Allergol. Immunopathol. 2020, 48, 475–483. [Google Scholar] [CrossRef]
- Pralong, J.A.; Cartier, A. Review of Diagnostic Challenges in Occupational Asthma. Curr. Allergy Asthma Rep. 2017, 17, 1. [Google Scholar] [CrossRef]
- Tiotiu, A.I.; Novakova, S.; Labor, M.; Emelyanov, A.; Mihaicuta, S.; Novakova, P.; Nedeva, D. Progress in Occupational Asthma. Int. J. Environ. Res. Public Heal. 2020, 17, 4553. [Google Scholar] [CrossRef]
- Del Roio, L.C.; Mizutani, R.F.; Pinto, R.C.; Terra-Filho, M.; Santos, U.P. Work-related asthma. J. Bras. Pneumol. 2021, 47, e20200577. [Google Scholar] [CrossRef]
- Laditka, J.N.; Laditka, S.B.; Arif, A.A.; Hoyle, J.N. Work-related asthma in the USA: nationally representative estimates with extended follow-up. Occup. Environ. Med. 2020, 77, 617–622. [Google Scholar] [CrossRef]
- Kenyon, N.J.; Morrissey, B.M.; Schivo, M.; Albertson, T.E. Occupational Asthma. Clin. Rev. Allergy Immunol. 2011, 43, 3–13. [Google Scholar] [CrossRef]
- Wang, Z.; Li, Y.; Gao, Y.; Fu, Y.; Lin, J.; Lei, X.; Zheng, J.; Jiang, M. Global, regional, and national burden of asthma and its attributable risk factors from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Respir. Res. 2023, 24, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pega, F.; Al-Emam, R.; Cao, B.; Davis, C.; Edwards, S.; Gagliardi, D.; Fassa, A.G.; Hassan, M.; Hosseinpoor, A.R.; Iavicoli, S.; et al. New global indicator for workers’ health: mortality rate from diseases attributable to selected occupational risk factors. Bull. World Heal. Organ. 2023, 101, 418–430. [Google Scholar] [CrossRef] [PubMed]
- García, A.R.G. Seguridad y salud en el trabajo en Ecuador [Safety and Health at Work in Ecuador]. Arch Prev Riesgos Labor. 2021; 24, 232–239. [Google Scholar] [CrossRef]
- Lindström, I.; Lantto, J.; Karvala, K.; Soini, S.; Ylinen, K.; Suojalehto, H.; Suuronen, K. Occupations and exposure events in acute and subacute irritant-induced asthma. Occup. Environ. Med. 2021, 78, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Sejbaek, C.S.; Flachs, E.M.; Carøe, T.K.; Meye, H.W.; Frederiksen, M.; Frydendall, K.B.; Wolkoff, P.; Clausen, P.A.; Hougaard, K.S.; Schlünssen, V. Professional cleaning and risk of asthma – a Danish nationwide register-based study. Scand. J. Work. Environ. Heal. 2021, 48, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Enilari, O.; Sinha, S. The Global Impact of Asthma in Adult Populations. Ann. Glob. Heal. 2019, 85, 2. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, S.; Shima, M.; Yoda, Y.; Oka, K.; Kurosaka, F.; Shimizu, S.; Takahashi, H.; Nakatani, Y.; Nishikawa, J.; Fujiwara, K.; et al. Association of ambient air pollution and meteorological factors with primary care visits at night due to asthma attack. Environ. Heal. Prev. Med. 2013, 18, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Dutta, S.; Podder, S.; Mondal, P.; Laha, A.; Saha, N.C.; Moitra, S.; Saha, G.K. Sensitivity to House Dust Mites Allergens with Atopic Asthma and Its Relationship with CD14 C(-159T) Polymorphism in Patients of West Bengal, India. J. Med Èntomol. 2018, 55, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Son, J.-Y.; Bell, M.L.; Lee, J.-T. The impact of heat, cold, and heat waves on hospital admissions in eight cities in Korea. Int. J. Biometeorol. 2014, 58, 1893–1903. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [PubMed]
- Lantto, J.; Suojalehto, H.; Karvala, K.; Remes, J.; Soini, S.; Suuronen, K.; Lindström, I. Clinical Characteristics of Irritant-Induced Occupational Asthma. J. Allergy Clin. Immunol. Pr. 2022, 10, 1554–1561. [Google Scholar] [CrossRef]
- Holtjer, J.C.; Bloemsma, L.D.; Beijers, R.J.; Cornelissen, M.E.; Hilvering, B.; Houweling, L.; Vermeulen, R.C.; Downward, G.S.; der Zee, A.-H.M.-V. Identifying risk factors for COPD and adult-onset asthma: an umbrella review. Eur. Respir. Rev. 2023, 32, 230009. [Google Scholar] [CrossRef]
- Benavides, F.G.; Vives, A.; Zimmerman, M.; Silva-Peñaherrera, M. Exceso de mortalidad en población en edad de trabajar en nueve países de Latinoamérica, año 2020 [Excess mortality in 2020 in the working-age population of nine Latin American countries. Excesso de mortalidade na população em idade ativa em nove países da América Latina no ano de 2020]. Rev Panam Salud Publica. 2022, 46, e75. [Google Scholar] [CrossRef]
- Shen, X.; Liang, J.; Cao, J.; Wang, Z. How Population Aging Affects Industrial Structure Upgrading: Evidence from China. Int. J. Environ. Res. Public Heal. 2022, 19, 16093. [Google Scholar] [CrossRef]
- Cabrera, A.; Rodriguez, A.; Romero-Sandoval, N.; Barba, S.; Cooper, P.J. Trends in hospital admissions and mortality rates for asthma in Ecuador: a joinpoint regression analysis of data from 2000 to 2018. BMJ Open Respir. Res. 2021, 8, e000773. [Google Scholar] [CrossRef]
- Camargo, C.A.; Budinger, G.R.S.; Escobar, G.J.; Hansel, N.N.; Hanson, C.K.; Huffnagle, G.B.; Buist, A.S. Promotion of Lung Health: NHLBI Workshop on the Primary Prevention of Chronic Lung Diseases. Ann. Am. Thorac. Soc. 2014, 11 (Suppl 3), S125–S138. [Google Scholar] [CrossRef]
Figure 1.
Identification of the provinces with the highest morbidity and mortality due to asthma in Ecuador during the period 2016 to 2019.
Figure 1.
Identification of the provinces with the highest morbidity and mortality due to asthma in Ecuador during the period 2016 to 2019.
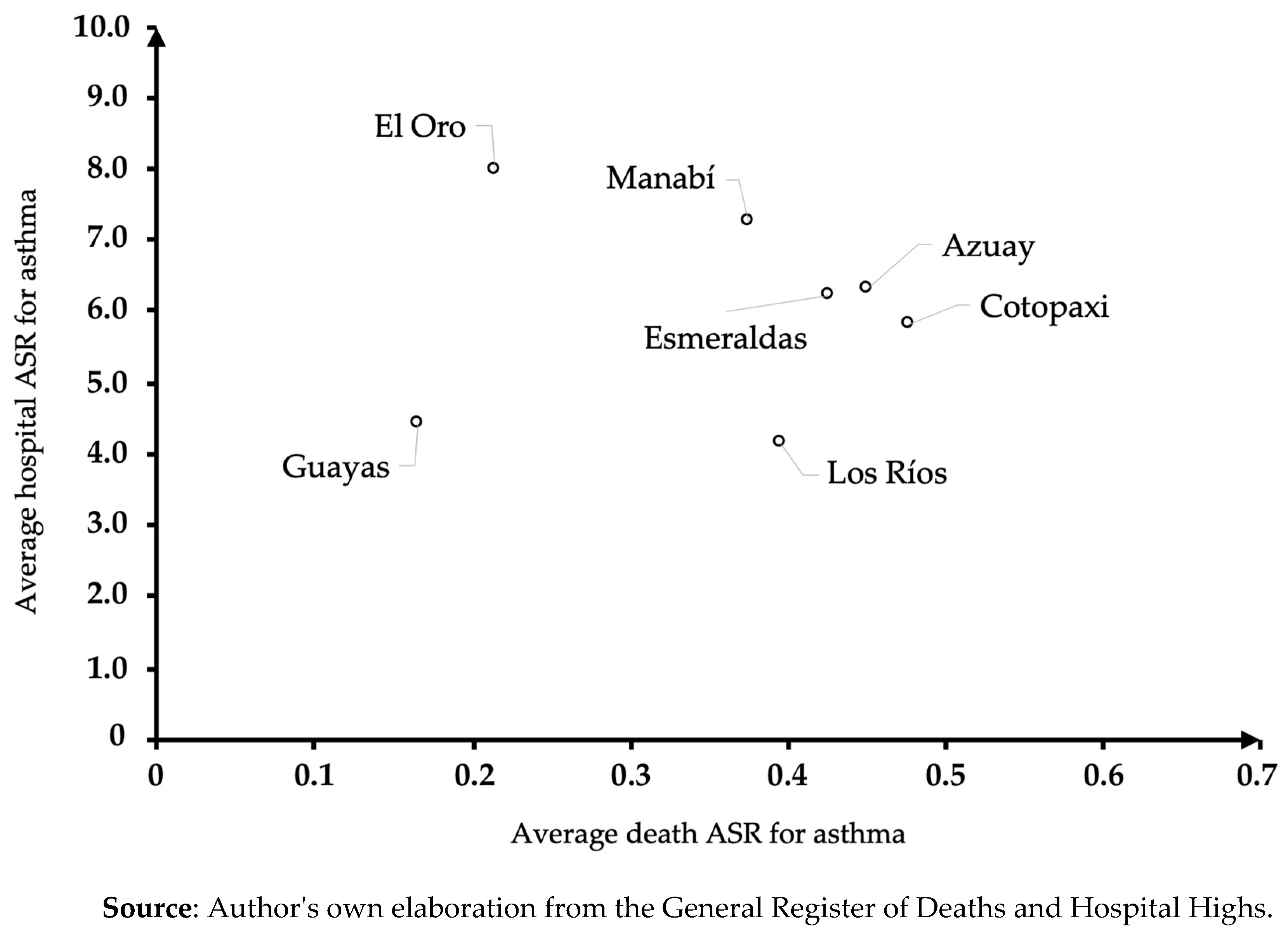

Table 1.
Prevalence and Asthma morbidity rates in working-age population by province in Ecuador during the period 2016 to 2019.
Table 1.
Prevalence and Asthma morbidity rates in working-age population by province in Ecuador during the period 2016 to 2019.
| 2016 (N=702) | 2017 (N=735) | 2018 (N=691) | 2019 (N=658) | Slope | p | |||||||||||||||||
| Province | %a | Crude | ASR (95% CI) | %a | Crude | ASR (95% CI) | %a | Crude | ASR (95% CI) | %a | Crude | ASR (95% CI) | ||||||||||
| Azuay | 4,7 | 6,09 | 6,18 | (4,25–8,68) | 4,6 | 6,13 | 6,12 | (4,24-8,55) | 5,4 | 6,52 | 6,51 | (4,58-8,97) | 5,8 | 6,55 | 6,50 | (4,60–8,93) | 0.13 | 0.156 | ||||
| Bolívar | 1,3 | 7,56 | 7,38 | (3,36–14,04) | 1,1 | 6,64 | 7,09 | (3,04-14,00) | 1,3 | 7,37 | 7,70 | (3,5-14,7) | 1,5 | 8,09 | 8,43 | (4,03–15,52) | 0.38 | 0.158 | ||||
| Cañar | 1,1 | 4,93 | 5,17 | (2,22–10,19) | 1,0 | 4,22 | 4,06 | (1,62-8,39) | 1,0 | 4,12 | 4,31 | (1,72-8,89) | 2,0 | 7,48 | 7,83 | (4,15–13,41) | 0.82 | 0.384 | ||||
| Carchi | - | 0,4 | 2,51 | 2,37 | (0,48-6,94) | 1,6 | 9,09 | 8,85 | (4,41-15,85) | 0,5 | 2,45 | 2,38 | (0,48–6,95) | 1.36 | 0.538 | |||||||
| Cotopaxi | 3,0 | 7,38 | 7,54 | (4,66–11,52) | 1,6 | 4,14 | 4,10 | (2,11-7,16) | 2,3 | 5,41 | 5,60 | (3,20-9,09) | 2,7 | 5,98 | 6,14 | (3,63–9,71) | –0.27 | 0.755 | ||||
| Chimborazo | 2,6 | 5,65 | 5,72 | (3,38-9,04) | 3,0 | 6,81 | 6,90 | (4,32-10,45) | 3,6 | 7,62 | 7,74 | (5,01-11,43) | 4,7 | 9,31 | 9,35 | (6,35–13,28) | 1.17 | 0.008 | ||||
| El Oro | 6,3 | 9,69 | 9,68 | (7,03-12,99) | 5,7 | 9,08 | 9,08 | (6,54-12,27) | 5,1 | 7,43 | 7,40 | (5,10-10,30) | 4,3 | 5,84 | 5,76 | (3,83–8,33) | –1.34 | 0.018 | ||||
| Esmeraldas | 3,0 | 5,74 | 5,92 | (3,66-9,05) | 3,0 | 5,88 | 6,23 | (3,90-9,43) | 3,8 | 6,81 | 7,00 | (4,60-10,30) | 3,3 | 5,64 | 5,80 | (3,63–8,79) | 0.04 | 0.895 | ||||
| Galápagos | 0,4 | 14,72 | 15,99 | (3,15-46,87) | 0,3 | 9,58 | 10,05 | (1,07-36,44) | 0,1 | 4,68 | 4,38 | (0,06-24,38) | 0,2 | 4,57 | 4,42 | (0,06–24,58) | –4.04 | 0.058 | ||||
| Guayas | 16,5 | 4,17 | 4,17 | (3,44-5,00) | 18,9 | 4,91 | 4,88 | (4,10-5,76) | 17,5 | 4,19 | 4,20 | (3,48-5,02) | 19,9 | 4,46 | 4,45 | (3,72–5,28) | 0.02 | 0.937 | ||||
| Imbabura | 2,1 | 5,18 | 5,19 | (2,90-8,56) | 2,6 | 6,43 | 6,50 | (3,91-10,15) | 1,4 | 3,32 | 3,30 | (1,60-6,15) | 2,4 | 5,20 | 5,19 | (2,97–8,43) | –0.32 | 0.686 | ||||
| Loja | 6,7 | 14,90 | 14,75 | (10,83-19,62) | 10,2 | 23,39 | 23,72 | (18,65-29,74) | 5,6 | 11,97 | 12,10 | (8,63-16,61) | 3,3 | 6,65 | 6,75 | (4,23–10,22) | –3.56 | 0.351 | ||||
| Los Ríos | 2,3 | 2,87 | 2,88 | (1,65-4,68) | 3,9 | 5,10 | 5,12 | (3,42-7,35) | 4,5 | 5,36 | 5,38 | (3,66-7,64) | 2,9 | 3,22 | 3,24 | (1,95-5,06) | 0.13 | 0.865 | ||||
| Manabí | 14,0 | 10,03 | 9,97 | (8,10-12,16) | 8,3 | 6,15 | 6,10 | (4,67-7,84) | 10,1 | 6,95 | 6,96 | (5,42-8,79) | 9,3 | 5,97 | 6,00 | (4,59-7,71) | –1.11 | 0.233 | ||||
| Morona Santiago | 3,3 | 22,55 | 23,57 | (14,79-35,56) | 3,8 | 26,51 | 28,33 | (18,66-41,16) | 2,5 | 15,55 | 15,96 | (9,18-25,70) | 1,2 | 7,07 | 7,72 | (3,25-15,34) | –5.99 | 0.143 | ||||
| Napo | 0,6 | 5,47 | 6,07 | (1,59-15,62) | 0,4 | 3,99 | 3,84 | (0,73-11,32) | 0,7 | 6,45 | 7,23 | (2,31-16,90) | 0,5 | 3,76 | 4,02 | (0,80-11,78) | –0.28 | 0.783 | ||||
| Orellana | 0,3 | 2,24 | 2,46 | (0,26-8,95) | 0,5 | 4,39 | 4,19 | (1,13-10,73) | 0,9 | 6,46 | 7,19 | (2,58-15,75) | 0,9 | 6,33 | 6,83 | (2,45-14,95) | 1.61 | 0.074 | ||||
| Pastaza | 0,6 | 6,37 | 6,61 | (1,70-17,10) | 0,3 | 3,07 | 3,19 | (0,31-11,67) | 0,1 | 1,48 | 1,83 | (0,02-10,17) | 0,8 | 7,16 | 7,74 | (2,46-18,12) | 0.20 | 0.906 | ||||
| Pichincha | 20,8 | 7,14 | 7,07 | (5,97-8,32) | 18,1 | 6,36 | 6,29 | (5,26-7,45) | 18,7 | 6,04 | 5,95 | (4,97-7,07) | 21,3 | 6,42 | 6,31 | (5,31-7,45) | –0.26 | 0.285 | ||||
| Santa Elena | 1,1 | 3,47 | 3,49 | (1,50-6,88) | 2,2 | 6,76 | 6,67 | (3,81-10,83) | 2,0 | 5,76 | 5,60 | (3,06-9,39) | 2,0 | 5,21 | 5,25 | (2,79-8,98) | 0.42 | 0.589 | ||||
| Santo Domingo T. | 1,0 | 2,55 | 2,54 | (1,01-5,24) | 1,1 | 2,84 | 2,78 | (1,20-5,48) | 2,0 | 4,85 | 5,00 | (2,73-8,39) | 2,1 | 4,73 | 4,85 | (2,65-8,15) | 0.91 | 0.100 | ||||
| Sucumbíos | 2,3 | 12,08 | 12,41 | (7,06-20,19) | 2,0 | 10,98 | 11,85 | (6,60-19,59) | 2,0 | 9,95 | 10,47 | (5,69-17,61) | 1,1 | 4,83 | 5,33 | (2,12-10,99) | –2.26 | 0.095 | ||||
| Tungurahua | 4,4 | 8,25 | 8,16 | (5,55-11,59) | 4,2 | 8,12 | 7,98 | (5,42-11,33) | 4,6 | 8,25 | 8,14 | (5,57-11,49) | 5,9 | 9,90 | 9,71 | (6,90-13,28) | 0.48 | 0.236 | ||||
| Zamora Chinchipe | 1,7 | 18,41 | 19,57 | (10,02-34,31) | 2,7 | 29,78 | 31,91 | (19,40-49,39) | 3,0 | 30,36 | 32,25 | (19,86-49,43) | 1,5 | 14,04 | 13,78 | (6,51-25,48) | –1.70 | 0.761 | ||||
| Ecuador | 25,2 | 6,51 | 26,38 | 6,68 | 24,8 | 6,16 | 23,62 | 5,76 | –0.28 | 0.122 | ||||||||||||
ASR, age-standardized rate. Source: Author's own elaboration from the Hospital Highs.
Table 2.
Prevalence and Asthma mortality rates in working-age population by province in Ecuador during the period 2016 to 2019.
Table 2.
Prevalence and Asthma mortality rates in working-age population by province in Ecuador during the period 2016 to 2019.
| 2016 (N=15) | 2017 (N=10) | 2018 (N=22) | 2019 (N=17) | Slope | p | |||||||||||||||||
| Province | %a | Crude | ASR (95% CI) | %a | Crude | ASR (95% CI) | %a | Crude | ASR (95% CI) | %a | Crude | ASR (95% CI) | ||||||||||
| Azuay | - | - | 13,6 | 0,53 | 0,57 | (0,11-1,65) | 11,8 | 0,34 | 0,33 | (0,04-1,19) | 0.15 | 0.660 | ||||||||||
| Cotopaxi | 6,7 | 0,35 | 0,36 | (0,005-2,00) | - | 9,1 | 0,68 | 0,72 | (0,08-2,60) | 5,9 | 0,33 | 0,35 | (0,005-1,97) | 0.07 | 0.697 | |||||||
| El Oro | 6,7 | 0,22 | 0,22 | (0,003-1,20) | - | 4,5 | 0,21 | 0,21 | (0,003-1,18) | 5,9 | 0,21 | 0,21 | (0,003-1,16) | 0.02 | 0.782 | |||||||
| Esmeraldas | - | 10,0 | 0,27 | 0,29 | (0,004-1,60) | 9,1 | 0,52 | 0,56 | (0,06-2,01) | - | 0.28 | 0.013 | ||||||||||
| Guayas | 40,0 | 0,22 | 0,21 | (0,08-0,46) | 20,0 | 0,07 | 0,07 | (0,01-0,25) | 18,2 | 0,14 | 0,14 | (0,04-0,35) | 41,2 | 0,24 | 0,24 | (0,10-0,50) | 0.02 | 0.728 | ||||
| Los Ríos | 13,3 | 0,36 | 0,36 | (0,04-1,31) | 30,0 | 0,53 | 0,52 | (0,11-1,53) | 9,1 | 0,35 | 0,35 | (0,04-1,27) | 11,8 | 0,34 | 0,35 | (0,04-1,25) | –0.02 | 0.691 | ||||
| Manabí | 26,7 | 0,41 | 0,41 | (0,11-1,06) | 30,0 | 0,30 | 0,30 | (0,06-0,88) | 22,7 | 0,50 | 0,50 | (0,16-1,16) | 17,6 | 0,29 | 0,29 | (0,06-0,85) | –0.02 | 0.792 | ||||
| Ecuador | 23,44 | 0,14 | 15,63 | 0,09 | 34,38 | 0,20 | 26,56 | 0,15 | 0.01 | 0.599 | ||||||||||||
ASR, age-standardized rate. No deaths occurred in the following provinces: Bolívar, Cañar, Carchi, Chimborazo, Galápagos, Morona Santiago, Napo, Orellana, Pastaza, Santo Domingo, Sucumbíos, Tungurahua, and Zamora Chinchipe. Provinces with death records in a single year. Imbabura reported a total of 10.0% of deaths in 2017, with a crude death rate of 0.34 and an ASR of 0.35 (95% CI, 0.005–1.94 ) per 100,000 working-age population. Loja reported a total of 9.1% of deaths in 2018, with a crude death rate of 0.61 and an ASR of 0.61 (95% CI, 0.07–2.19) per 100,000 working-age population. Santa Elena reported a total of 5.9% of deaths in 2019, with a crude death rate of 0.40 and an ASR of 0.42 (95% CI, 0.01–2.33) per 100,000 working-age population. In 2016 and 2018, 6.7% of deaths, a crude death rate of 0.05, and an ASR of 0. 05 (95% CI, 0.001–0.26) per 100,000 working-age population and 4.5% of deaths, a crude death rate of 0.05, and an ASR of 0. 05 (95% CI, 0.001–0.25) per 100,000 working-age population. Source: Author's own elaboration from the General Register of Deaths.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



