
Submitted:
17 May 2024
Posted:
20 May 2024
You are already at the latest version
Abstract
D-dimer testing in combination with clinical assessment is commonly used to diagnose suspected DVT and pulmonary embolism. However, as D-dimer levels are physiologically higher in elderly patients, this test loses clinical specificity in the setting of geriatric patients. The aim of our study was to investigate the changes in D-dimer levels with age and the specificity of the D-dimer test in the diagnosis of pulmonary embolism. 1617 elderly patients consecutively admitted to the Geriatric Emergency Care Department of the INRCA-IRCCS hospital between January 2013 and February 2014 and for whom D-dimer results were available were included. The D-dimer immunoturbidimetric assay was performed on a cs-2100i Sysmex Siemens using a conventional cut-off level of 500 µg/L. The median D-dimer level was 1200 [550-2990] µg/L FEU, and the percentage of patients with D-dimer levels below the conventional cut-off was only 22.1%. As expected, there was a significant age-related increase in D-dimer, even when sex was considered, and a significant decrease in the specificity of D-dimer assay with age. The most established use of D-dimer testing is in the diagnosis of deep vein thrombosis or pulmonary embolism. Our study confirms the need for an age-adjusted cut-off for D-dimer testing in geriatric patients.
Keywords:
D‐dimer
; pulmonary embolism
; specificity
; aging
1. Introduction
Venous thromboembolism (VTE) is a relatively common condition that includes deep vein thrombosis (DVT) and pulmonary embolism (PE) or both. The variety of symptoms and findings can mask the clinical signs and cause the condition to go unnoticed. Particularly in the elderly, VTE is difficult to diagnose because of the presence of comorbidities that can mask it and sometimes lead to a fatal outcome [1,2,3,4]. Due to the difficulty of diagnosis for PE, few data on the epidemiology of this disease are currently available. In Italy, the incidence of PE ranges from 30 to 80 new cases per year per 100000 people and the age-standardized annual PE- related mortality rates are 2.8/100000 women and 2.5/100000 men [5,6]. Mostly, the majority of preventable deaths from DVT and PE are due to missed or delayed diagnosis than to failure of treatment [7,8]. Further, about 30% of patients with DVT and/or PE will develop a recurrence within 10 years. Because the specificity of clinical and physical examination in the diagnosis is low, and the risk of overdiagnosis/underdiagnosis is high, it is necessary to use diagnostic tests to support the examination. The main tests used for the diagnosis are arterial blood gas, D-dimer (DD) test, electrocardiogram, chest radiography, echocardiography, computed tomography angiography (CTA), pulmonary angiography, magnetic resonance imaging, and ventilation perfusion scintigraphy. The use of D-dimer measurement as biochemical-screening test to exclude suspected VTE is well documented [9,10,11,12]. Moreover, abnormal D-dimer after discontinuation of anticoagulation has demonstrated to be associated with high risk of recurrence [13,14], thus adding new clinical value for this measurement. The introduction of algorithms that combine clinical suspicion, D-dimer testing and diagnostic imaging has led to a more accurate approach to diagnosing VTE [15,16]. D-dimer is the degradation product of fibrin and it possesses a high sensitivity (about 99%) for DVT and PE, but, unfortunately, a low specificity (between 10 and 40%), as it is very high also in other situations, like inflammation, infections, cancer, necrosis, surgery, immobilization, disseminated intravascular coagulation (DIC), burns, stroke, Congestive Heart Failure (CHF), liver disease, kidney disease and not last aging. Conversely, it is estimated that, with a cut-off value of 500 µg/L FEU, DD has 100% negative predictive value. Therefore, in patients with low clinical probability, the assessment of DD could be useful to rule out the presence of pulmonary embolism [17,18]. If this claim is applicable to a young patient, the same cannot be said in the case of very old patients, because in this case a similar cut-off level is surely too low. The challenge is that DD level increases with age and its specificity for VTE strongly decreases in elderly patients due to the presence of comorbidities. This leads to an increase in false positives and unnecessary testing for patients, resulting in increased costs and burdensome testing. Although the frequency of VTE is higher in hospitalized patients due to the larger prevalence of prothrombotic risk factors [19,20], VTE may also occur in outpatients; thus, the Emergency Department (ED) becomes the ordinary health-care setting where these patients are referred to. The diagnosis of PE in elderly patients is particularly difficult, because they usually presented almost all the secondary risk factors for PE, i.e., obesity, hypertension, smoking, cancer, ictus, immobilization etc. In this type of patients, the concomitant presence of all these factors makes the diagnosis much more difficult and challenging for physicians. As D-dimer levels are physiologically higher in elderly patients, D-dimer test loses clinical specificity. Alternatively to the classical cut-off level of 500 µg/L FEU, to improve the clinical specificity of D-dimer, other cut-off levels have been proposed: i.e an age adjusted DD cut-off level [ADC = (patient’s age x 0.01)µg/ml] [21,22], a fixed cut-off value of 750 µg/L in patients aged 60 years and older who were referred to secondary care with symptoms of DVT [23] and a cut-off value of 1000 µg/L for those aged >60 years, using the Vidas D-dimer assay [24,25]. It became challenging to perform the right diagnosis in patients who were admitted to the Geriatric Emergency Care Department (GECD) with suspected VTE and who had concomitantly a wide spectrum of comorbidities associated with increased DD levels. An appropriate pre-test clinical probability stratification of VTE risk becomes essential, using universally validated algorithms [16]. Along with a clinical evaluation and radiographic examinations (ECG, chest ray, EGA), DD could be a very useful test in the diagnosis of VTE. The aim of our study was to investigate in a community of very old people how DD levels change during aging and if a different cut-off level of DD could be proposed for very old people suspected to have PE.
2. Methods
2.1. Study Design and D-Dimer Assay
This retrospective study was composed of one-thousand-and-six-hundreds-seventeen patients (962 females and 655 males), with an age range of 21-103 years, and used administrative data from the Geriatric Emergency Care Department (GECD) of the INRCA hospital over approximately 12 months (between January 2013 and February 2014) and for which results of D-dimer test were available.
Patients with a negative test result and a low pretest clinical probability (PTP), according to Wells rules [15], underwent no further diagnostic testing and were not treated with anticoagulants. All patients with a positive D-dimer test result or a high PTP underwent diagnostic imaging.
For PE, on the basis of ventilation-perfusion lung scan showing a high-probability pattern or CTPA or angiography showing segmental or more proximal intraluminal defects. 176 patients suspected to have pulmonary embolism underwent computed tomography angiography (CTA) and/or to scintigraphy. Of these 176 patients, only 42 (2.6%) were effectively affected.
Plasma samples were collected at the initial visit and testing was performed immediately using the D-dimer assay available. The DD immunoturbidimetric assay was performed on cs-2100i Sysmex Siemens, which has been demonstrated to reach a sensitivity of 98,8%, a specificity of 34,2% and a negative predictive value of 98,7, using a conventional cut-off level of 500 µg/L FEU. A value of less than 500 µg/L FEU was regarded as a negative result.
2.2. Statistical Analyses
Patients were analysed in total and grouped into six age categories: <=50, 51-60, 61-70, 71-80, 81-90 and >=91 years of age. Baseline patient characteristics were described using the number (percentage) for categorical variables and the median [IQR] according to distribution for quantitative non-normal variables. To assess the normal distribution of the data, a Kolmogorov-Smirnov test was performed. Chi square test was used to determine differences between proportions of categorical variables. The sensitivity, specificity and predictive value of DD measurement were analysed in the total sample and in each age category. Receiver operating characteristic (ROC) curves analysis and areas under the curve (AUC) were generated for patients in the total and six age groups. The ROC curve is used to calculate the AUC as a measure of the diagnostic accuracy. To test the differences between groups for non-normal variables the non-parametric Kruskal Wallis Test was used. All tests were two-sided, and significance was set at p<0.05. All the statistical analyses were performed using IBM SPSS (IBM Corp, Armonk, NY, USA) version 27.0.
3. Results
3.1. General Characteristics of the Patients
Demographic and anamnestic data, biochemical and hematological variables of the studied population were summarized in Table 1. Enrolled patients had a median age of 85 [IQR, 80-89], with females significantly older than males. The median level [IQR] of D-dimer was 1200 [550-2990] µg/L FEU with not significantly difference in levels between males and females. This D-dimer median level was more than double of the conventional cut-off level (500 µg/L FEU). Indeed, the percentage of patients with D-dimer concentrations below the above-mentioned conventional cut-off value was only 22,1% (358 patients, data not shown). As reported in Table 1, only 42 patients (2.6%) out of 1617 were effectively affected by pulmonary embolism, with no difference in the proportion by gender. Among the other biochemical parameters considered, only hemoglobin, platelets, C-reactive protein, BUN and creatinine resulted statistically different between males and females.
3.2. D-Dimer Levels during Aging
To deeply investigate the relationship between D-dimer and age, we divided our sample in six age classes (<=50, 51-60, 61-70, 71-80, 81-90 and >=91 years of age). The distribution of our patients, also considering sex, in these six age classes was reported in Table 2. The majority of the recruited sample belong to the last three age classes and the 81-90 years class was the most numerous. A statistically significant higher presence of females was found in the last class, i.e., >= 91 years of age (p<0.05). This was not surprisingly since it is well known that extremely long-lived people are represented predominantly by women [26]. It is well known that DD concentration rises with age; so, we investigated, in our sample, the relationship between age and DD assays. A significant age-related increase of D-dimer mean values was found (p<0.01), also when gender was considered (Figure 1).
3.3. D-Dimer Levels and Pulmonary Embolism
Table 3 reported the D-dimer median values among patients with and without pulmonary embolisms, also considering gender. For all the cases considered, patients with pulmonary embolism showed significantly higher median levels of D-dimer in respect to patients without PE (p<0.01). We also investigated the possible correlations between D-dimer and some biochemical variables considered in this study (i.e., WBC, CRP and eGFR). The results were reported in Table 4. Significantly higher median D-dimer levels were found for patients with white blood cells higher than 9000, C-reactive protein levels above 0.5 mg/dL and for patients with an eGFR<=30 ml/min.
3.4. Sensitivity and Specificity of D-Dimer Assay at Different Cut-Offs
To determine the sensitivity and the specificity of D-dimer testing in the whole sample, we considered three cut-off levels: the conventional cut-off level (500 µg/L FEU), the ADC cut-off level and a proposed cut-off level of 1050 µg/L FEU, higher in respect to the conventional (500 µg/L FEU), because took into consideration the increase of D-dimer testing with age (Table 5, Figure 2 and Figure 3).
The diagnostic performance of D dimer was then assessed using ROC curve analysis. As shown in Figure 2, with a fixed value of 100% of sensitivity, for all the patients, an increase from about 23% to 46% in the specificity using the proposed cut-off level of 1050 µg/L FEU instead of the conventional cut-off of 500 µg/L FEU was observed. This implied the recovery of 377 patients considered as false positives for PE.
The specificity was calculated for the last four age groups (61-70, 71-80, 81-90, and >=91 years of age). A marked decrease in specificity can be observed as age increases for all the three cut-offs considered, while maintaining a 100% sensitivity (Table 5).
In particular, for a conventional cut-off level of 500 µg/L FEU, the assay specificity was 65,5% in those aged 61-70 years old, but fell to 9,9% in patients over 90 years old.
Interestingly, a substantial increase in the specificity in the last four age classes with an ADC cut-off level of D-dimer (from 72.6% of the 61-70 years class to 28.2% of the over 90 years) and/or with a proposed 1050 µg/L FEU cut-off level (from 76.2% of the 61-70 years class to 30.4% of the over 90 years) was observed (Table 5). Hence, the use of a cut-off value of 1050 µg/L FEU, instead of the conventional (500 µg/L FEU) and/or the age-adjusted cut-off value, demonstrated an increase in the efficiency without a diminution of safety (i.e., the risk to have false negative patients).
In Figure 3, the ROC curves analysis of D dimer demonstrated that a cut-off of 1050 µg/L FEU showed a better specificity in respect to a 500 µg/L FEU cut off in all the groups considered, always assuming a 100% of sensitivity.
4. Discussion
The conventional cut-off of 500 µg/L FEU for D-dimer testing has been consistently used for ruled out the presence of DVT and/or PE. Several decision-making reference levels have been proposed to exclude this pathology; while this discussion can be applied in young subjects, the issue becomes more complicated and the boundary much less clear in the case of very elderly subjects where an elevated D-dimer level can be found even in subjects without deep vein thrombosis or pulmonary embolism. The issue of the reduction in specificity of the D-dimer test for the exclusion of DVT or PE as patients’age depends on the complex aging phenotype, characterized by increased proinflammatory and procoagulant processes, as well as by increased biomarkers of organ failure [27]. These biomarkers, i.e., troponin or NT-proBNP, that are used in clinical diagnostics, in the setting of geriatric patients could have high sensitivity but poor specificity. DD is often elevated in elderly subjects, presumably in relation to lower mobility and/or atherosclerotic processes. Anticoagulant therapy, either with heparin or oral anticoagulants, reduces fibrin formation and deposition and thus D-dimer levels. In fact, in our case, using the conventional cut-off of 500 µg/L FEU, the proportion of patients with abnormal DD findings is 78%. Clearly, this percentage is too high and it is not plausible that all of these patients have DVT and/or PE. Likely, these high values of DD depend on other causes rather than DVT and/or PE. Frequently, only a minority of patients with a positive DD (>500 µg/L FEU) are finally diagnosed with DVT and PE. In a progressively aging population, this problem is not negligible, and its resolution would greatly reduce the number of false positives and the number of costly invasive and often unnecessary diagnostic investigations for the patient. In addition, if we apply the ADC formula, the percentage of patients with a pathological level of DD does not change significantly. The use of differential thresholds according to patient’s age can significantly improve the overall performance of the examination, and this approach therefore seems preferable in clinical practice because it increases the proportion of elderly patients in whom a VTE can be definitively ruled out (decrease of false positives). In our case, the 377 false-positive patients (with a DD value between 500 and 1050) were “unnecessarily” subjected to a complex and costly diagnostic procedure that could have been avoided with the use of a higher threshold. As also demonstrated in this paper, D dimer levels increase significantly with age, independently of sex and the presence of PE. Our results are in line with several papers that have shown an increase in D-dimer with age, not only for events related to venous thromboembolism, but also for different reasons (infections, neoplasms, immobilization, DIC, stroke, heart failure, renal disease, thrombolytic therapy etc...) [21,22,23,24,25]. The peculiarity of our study is that only few papers have considered DD in a such elderly patient population (74% of patients are over 80 years of age) [22,28,29]. In a paper of Righini et al., the authors sought to understand the influence of age in the cost-effectiveness of therapeutic strategies for PE diagnosis and have finalized that its cost-saving utilize DD only in patients younger than 80 years old. The same authors, however, considered using DD in patients older than 80 years when the risk of imaging (radiation/contrast exposure with CTPA) is high due to impaired renal function [30]. As reported in the paper of Haas FJ et al., it is recommended to raise the cut-off value with the increasing of age, when the discrepancy between specificity and AUC of the ROC curve is too high (i.e., low specificity vs high AUC) [23]. Accordingly, we have proposed a higher cut-off for elderly patients (1050 µg/L FEU) which allows us to decrease the number of false positives. Finding an appropriate DD cut-off for the elderly population is urgently needed, as avoiding unnecessary and often invasive testing in frail individuals remains an unmet clinical need.
5. Conclusions
Our study confirmed that D dimer level increases with age in both sexes, regardless of the real presence of PE, and it confirmed that the specificity of this test decreases sharply with age. The proposed cut-off of 1050 µg/L FEU certainly increases the specificity of the DD test in respect to the conventional cut-off of 500 µg/L FEU (30.4 vs 9.9 in patients older than 90 years of age); however, it still remains a low specificity that raises doubts about the real diagnostic usefulness of DD assay in very elderly patients. Surely, with elderly patients at low risk for VTE on the basis of clinical signs and symptoms, the risk of having DD results above the cut-off remaining still high and DD became a potential confounding factor.
Limitations
Our study presents some limitations; first, our patients are all patients referred to a Geriatric Emergency Care Department (GECD) suspected to have a pulmonary embolism and not inpatients who developed PE during a hospital stay. Further, we do not have any information about follow-up and so we do not know if patients with high levels of DD developed PE.
Importantly, the diagnosis of PE is highly dependent on physician’s assessment, which can influence the final diagnosis and is unlikely to be consistent and standardised across hospitals. This is particularly true also for the DD assay that is entirely “method-specific” and cannot permit the comparison of results obtained with other tests.
Author Contributions
Conceptualization, FM (Francesca Marchegiani) and RG; Methodology, FM (Fausto Moroni), SA, AC, FS, SC, EP and AE; Formal analysis, FM (Francesca Marchegiani); Writing-original draft preparation, FM (Francesca Marchegiani), RG, FO, and ADP; Writing-review and editing, FO and JS; Supervision, FO and ADP. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were not required for this study because of the retrospective and daily clinical practice nature of the project. Clinical decisions were therefore not influenced by the manner in which we obtained the necessary information. All data used were anonymised.
Informed Consent Statement
The study was waved due to the retrospective study based on historical patient data.
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| [ADC] | age adjusted DD cut-off level |
| AUC | areas under the curve |
| BUN | Blood Urea Nitrogen |
| CHF | Congestive Heart Failure |
| CRP | C-reactive Protein |
| CTA | computed tomography angiography |
| DD | D-dimer |
| DIC | disseminated intravascular coagulation |
| DVT | deep vein thrombosis |
| ED | Emergency Department |
| eGFR | Estimated Glomerular Filtration Rate |
| GECD | Geriatric Emergency Care Department |
| HgB | Hemoglobin |
| PE | pulmonary embolism |
| PTP | pretest clinical probability |
| RBC | red blood cell |
| ROC | receiver operating characteristic |
| VTE | Venous thromboembolism |
| WBC | White blood cell |
References
- Ho, K.M.; Litton, E. Venous thromboembolism prophylaxis in hospitalized elderly patients: Time to consider a ‘MUST’ strategy. J Geriatr Cardiol. 2011, 8, 114–120f. [Google Scholar] [CrossRef] [PubMed]
- Raskob, G.E.; Angchaisuksiri, P.; Blanco, A.N.; Buller, H.; Gallus, A.; Hunt, B.J.; Hylek, E.M.; Kakkar, A.; Konstantinides, S.V.; McCumber, M.; Ozaki, Y.; Wendelboe, A.; Weitz, J.I. ISTH Steering Committee for World Thrombosis Day. Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol. 2014; 34, 2363–2371. [Google Scholar] [CrossRef]
- Rogowska, M.; Thornton, M.; Creese, B.; Velayudhan, L.; Aarsland, D.; Ballard, C.; Tsamakis, K.; Stewart, R.; Mueller, C. Implications of Adverse Outcomes Associated with Antipsychotics in Older Patients with Dementia: A 2011-2022 Update. Drugs Aging 2023, 40, 21–32. [Google Scholar] [CrossRef] [PubMed]
- van Rossum, A.B.; van Houwelingen, H.C.; Kieft, G.J.; Pattynama, P.M. Prevalence of deep vein thrombosis in suspected and proven pulmonary embolism: a meta-analysis. Br J Radiol. 1998, 71, 1260–1265. [Google Scholar] [CrossRef] [PubMed]
- Valerio, L.; Zuin, M.; Mahmoudpour, S.H.; Zuliani, G.; Zonzin, P.; Barco, S.; Roncon, L. Aggiornamento sui dati relativi alla mortalità da embolia polmonare in Italia (2003-2015). [An update on pulmonary embolism-related mortality in Italy (2003-2015)]. G Ital Cardiol. (Rome), 2020; 21, 639–646. [Google Scholar] [CrossRef]
- Ageno, W.; Squizzato, A.; Garcia, D.; Imberti, D. Epidemiology and risk factors of venous thromboembolism. Semin Thromb Hemost. 2006, 32, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Raja, A.S.; Greenberg, J.O.; Qaseem, A.; Denberg, T.D.; Fitterman, N.; Schuur, J.D. Clinical Guidelines Committee of the American College of Physicians. Evaluation of Patients With Suspected Acute Pulmonary Embolism: Best Practice Advice From the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2015; 163, 701–711. [Google Scholar] [CrossRef]
- Fedullo, P.F.; Tapson, V.F. Clinical practice. The evaluation of suspected pulmonary embolism. N Engl J Med. 2003, 349, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Bates, S.M. D-dimer assays in diagnosis and management of thrombotic and bleeding disorders. Semin Thromb Hemost. 2012, 38, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Cervellin, G.; Casagranda, I.; Morelli, B.; Testa, S.; Tripodi, A. D-dimer testing for suspected venous thromboembolism in the emergency department. Consensus document of AcEMC, CISMEL, SIBioC, and SIMeL. Clin Chem Lab Med. 2014; 52, 621–628. [Google Scholar] [CrossRef]
- Crawford, F.; Andras, A.; Welch, K.; Sheares, K.; Keeling, D.; Chappell, F.M. D-dimer test for excluding the diagnosis of pulmonary embolism. Cochrane Database Syst Rev. 2016, 2016, CD010864. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; Kucher, N.; Lang, I.M.; Lankeit, M.; Lorusso, R.; Mazzolai, L.; Meneveau, N.; Ní Áinle, F.; Prandoni, P.; Pruszczyk, P.; Righini, M.; Torbicki, A.; Van Belle, E.; Zamorano, J.L. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020; 41, 543–603. [Google Scholar] [CrossRef]
- Wang, J.; Tacey, M.; Ho, P. Retrospective review of D-dimer testing for venous thrombosis recurrence risk stratification: is this a useful test in the real world? J Thromb Thrombolysis 2020, 49, 562–571. [Google Scholar] [CrossRef]
- Douketis, J.; Tosetto, A.; Marcucci, M.; Baglin, T.; Cushman, M.; Eichinger, S.; Palareti, G.; Poli, D.; Tait, R.C.; Iorio, A. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Ann Intern Med. 2010, 153, 523–531. [Google Scholar] [CrossRef]
- Wells, P.S.; Anderson, D.R.; Rodger, M.; Stiell, I.; Dreyer, J.F.; Barnes, D.; Forgie, M.; Kovacs, G.; Ward, J.; Kovacs, M.J. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and D-dimer. Ann Int Med. 2001, 135, 98–107. [Google Scholar] [CrossRef]
- Shen, J.H.; Chen, H.L.; Chen, J.R.; Xing, J.L.; Gu, P.; Zhu, B.F. Comparison of the Wells score with the revised Geneva score for assessing suspected pulmonary embolism: a systematic review and meta-analysis. J Thromb Thrombolysis, 2016; 41, 482–492. [Google Scholar] [CrossRef]
- Favresse, J.; Lippi, G.; Roy, P.M.; Chatelain, B.; Jacqmin, H.; Ten Cate, H.; Mullier, F. D-dimer: Preanalytical, analytical, postanalytical variables, and clinical applications. Crit Rev Clin Lab Sci. 2018, 55, 548–577. [Google Scholar] [CrossRef] [PubMed]
- Talon, L.; Fourneyron, V.; Trapani, A.; Pereira, B.; Sinegre, T.; Lebreton, A. Analytical performance of a new immunoturbidimetric D-dimer assay and comparison with available assays. Res Pract Thromb Haemost. 2022, 6, e12660. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Franchini, M. Pathogenesis of venous thromboembolism: When the cup runneth over. Semin Thromb Hemost. 2008, 34, 747–761. [Google Scholar] [CrossRef] [PubMed]
- Cushman, M. Epidemiology and risk factors for venous thrombosis. Semin Hematol. 2007, 44, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Righini, M.; Van Es, J.; Den Exter, P.L.; Roy, P.M.; Verschuren, F.; Ghuysen, A.; Rutschmann, O.T.; Sanchez, O.; Jaffrelot, M.; Trinh-Duc, A.; Le Gall, C.; Moustafa, F.; Principe, A.; Van Houten, A.A.; Ten Wolde, M.; Douma, R.A.; Hazelaar, G.; Erkens, P.M.; Van Kralingen, K.W.; Grootenboers, M.J.; Durian, M.F.; Cheung, Y.W.; Meyer, G.; Bounameaux, H.; Huisman, M.V.; Kamphuisen, P.W.; Le Gal, G. Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: the ADJUST-PE study. JAMA. 2014, 311, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Douma, R.A.; Tan, M.; Schutgens, R.E.; Bates, S.M.; Perrier, A.; Legnani, C.; Biesma, D.H.; Ginsberg, J.S.; Bounameaux, H.; Palareti, G.; Carrier, M.; Mol, G.C.; Le Gal, G.; Kamphuisen, P.W.; Righini, M. Using an age-dependent D-dimer cut-off value increases the number of older patients in whom deep vein thrombosis can be safely excluded. Haematologica. 2012, 97, 1507–1513. [Google Scholar] [CrossRef]
- Haas, F.J.; Schutgens, R.E.; Biesma, D.H. An age-adapted approach for the use of D-dimers in the exclusion of deep venous thrombosis. Am J Hematol. 2009, 84, 488–491. [Google Scholar] [CrossRef] [PubMed]
- Harper, P.L.; Theakston, E.; Ahmed, J.; Ockelford, P. D-dimer concentration increases with age reducing the clinical value of the D-dimer assay in the elderly. Intern Med J. 2007, 37, 607–613. [Google Scholar] [CrossRef]
- Belo, L.; Valente, M.J.; Rocha, S.; Coimbra, S.; Catarino, C.; Lousa, I.; Bronze-da-Rocha, E.; Rocha-Pereira, P.; Sameiro-Faria, M.D.; Oliveira, J.G.; Madureira, J.; Fernandes, J.C.; Miranda, V.; Nunes, J.P.L.; Santos-Silva, A. Age-Related Changes in Clinical and Analytical Variables in Chronic Hemodialyzed Patients. Int J Mol Sci. 2024, 25, 3325. [Google Scholar] [CrossRef]
- Candore, G.; Balistreri, C.R.; Listì, F.; Grimaldi, M.P.; Vasto, S.; Colonna-Romano, G.; Franceschi, C.; Lio, D.; Caselli, G.; Caruso, C. Immunogenetics, gender, and longevity. Ann N Y Acad Sci. 2006, 1089, 516–537. [Google Scholar] [CrossRef]
- Kale, S.S.; Yende, S. Effects of Aging on Inflammation and Hemostasis through the Continuum of Critical Illness. Aging Dis. 2011, 2, 501–511. [Google Scholar] [PubMed]
- Dutton, J.; Dachsel, M.; Crane, R. Can the use of an age-adjusted D-dimer cut-off value help in our diagnosis of suspected pulmonary embolism? Clin Med (Lond). 2018, 18, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Nobes, J.; Messow, C.M.; Khan, M.; Hrobar, P.; Isles, C. Age-adjusted D-dimer excludes pulmonary embolism and reduces unnecessary radiation exposure in older adults: retrospective study. Postgrad Med J. 2017, 93, 93,420–424. [Google Scholar] [CrossRef] [PubMed]
- Righini, M.; Nendaz, M.; Le Gal, G.; Bounameaux, H.; Perrier, A. Influence of age on the cost-effectiveness of diagnostic strategies for suspected pulmonary embolism. J Thromb Haemost. 2007, 5, 1869–1877. [Google Scholar] [CrossRef]
Figure 1.
D-dimer levels during aging between sexes.
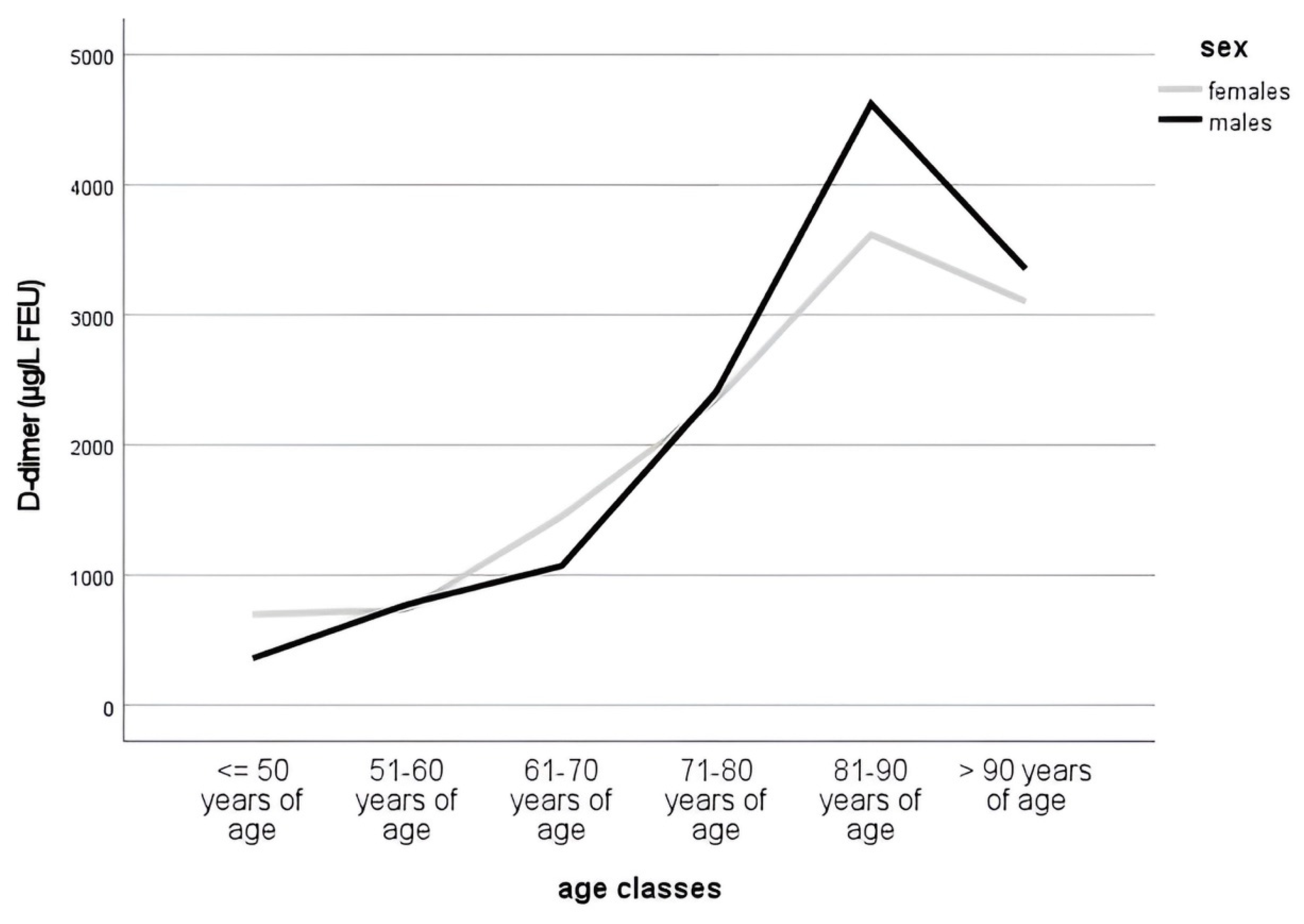
Figure 2.
Receiver operator curve (ROC) of D-dimer results and pulmonary embolism in all patients. The point at which the cut-off value equals 500 µg/L FEU and 1050 µg/L FEU are marked by arrow.
Figure 2.
Receiver operator curve (ROC) of D-dimer results and pulmonary embolism in all patients. The point at which the cut-off value equals 500 µg/L FEU and 1050 µg/L FEU are marked by arrow.
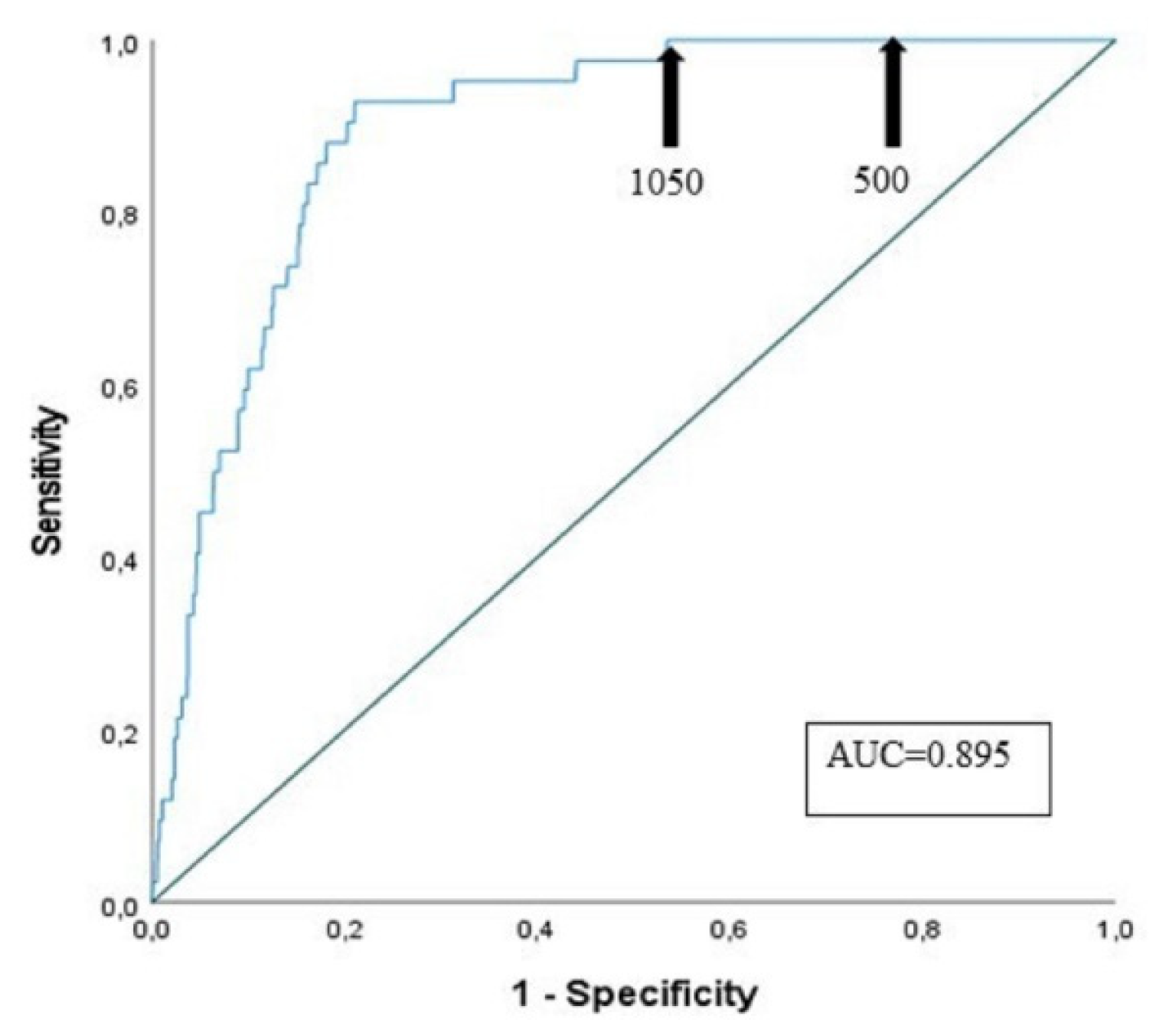
Figure 3.
Receiver operator curves (ROC) of D-dimer results for age groups (A) 61-70 years, (B) 71-80 years, (C) 81-90 years, and (D) >= 91 years. The point at which the cut-off value equals 500 µg/L FEU and 1050 µg/L FEU are marked by arrow.
Figure 3.
Receiver operator curves (ROC) of D-dimer results for age groups (A) 61-70 years, (B) 71-80 years, (C) 81-90 years, and (D) >= 91 years. The point at which the cut-off value equals 500 µg/L FEU and 1050 µg/L FEU are marked by arrow.
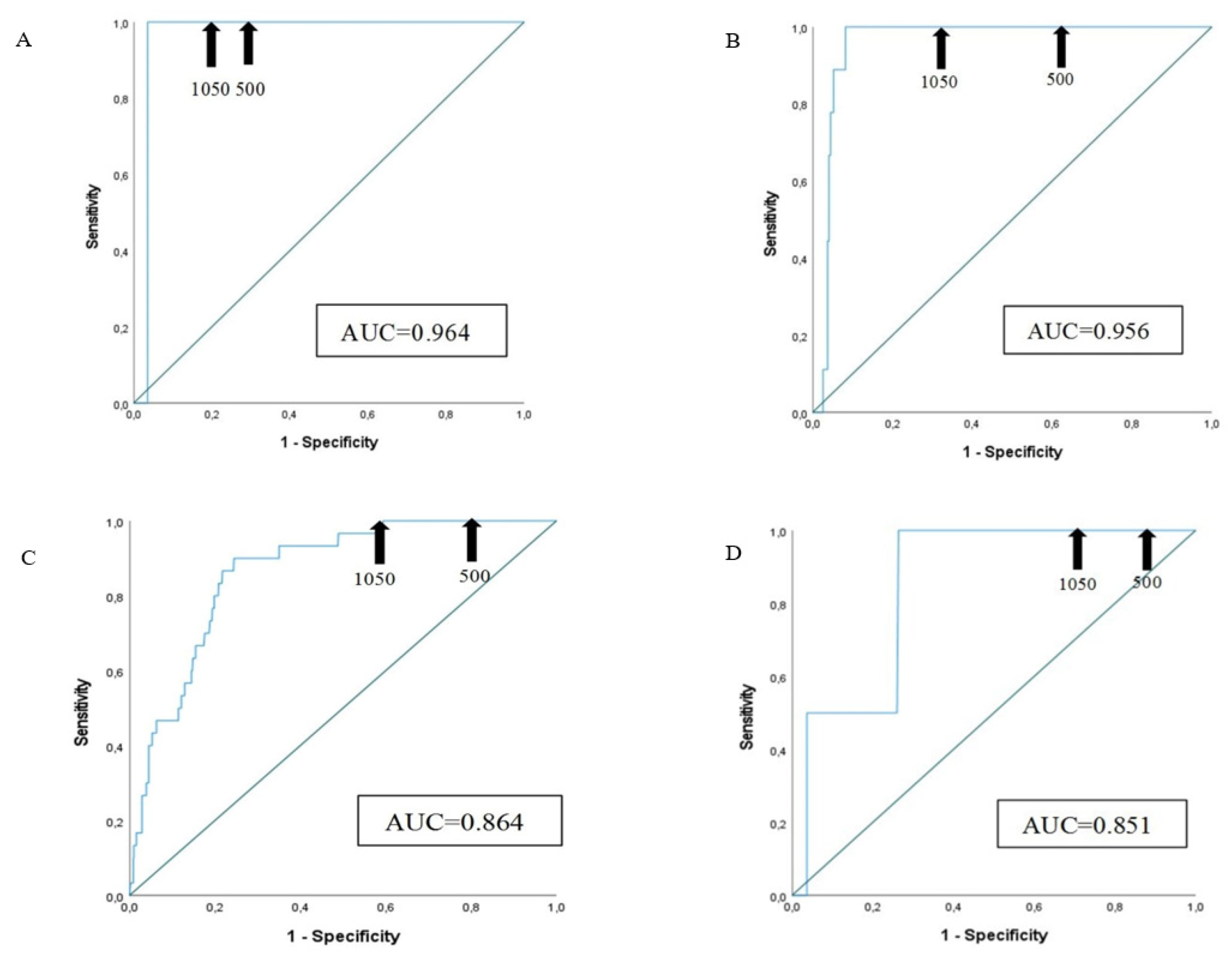

Table 1.
Description of clinical and biochemical characteristics of the patients.
| All n=1617 |
Males n=655 |
Females n=962 |
P | |
|---|---|---|---|---|
| Age (yrs) | 85 [80-89] | 84 [80-88] | 85 [81-90] | ≤0.01 |
| D-dimer (µg/L FEU) | 1200 [550-2990] | 1180 [510-3160] | 1205 [580-2870] | 0.765 |
| Pulmonary embolism (Yes/No) | 42/1575 | 14/641 | 28/934 | 0.337 |
| WBC x 103/µL | 8.4 [6.6-11.2] | 8.4 [6.6-11.2] | 8.40 [6.60-11.29] | 0.677 |
| RBC x 106/µL | 4.21 [3.76-4.60] | 4.21 [3.74-4.65] | 4.20 [3.77-4.57] | 0.559 |
| HgB (g/dL) | 12.5 [11.1-13.7] | 12.9 [11.2-14.1] | 12.3 [11.1-13.4] | ≤0.01 |
| Platelets x 103/µL | 215.0 [171.0-268.7] | 198.0 [159.5-242.0] | 228 [182-281] | ≤0.01 |
| Sodium (mmol/L) | 137 [134-139] | 136 [134-139] | 137 [133-139] | 0.750 |
| Potassium (mmol/L) | 4.0 [3.7-4.4] | 4.1 [3.8-4.4] | 4.0 [3.7-4.4] | 0.056 |
| C-reactive protein (mg/dL) | 2.91 [0.59-8.39] | 3.61 [0.81-8.77] | 2.05 [0.50-8.13] | 0.047 |
| BUN (mg/dL) | 48 [36-75] | 53 [38-80] | 46 [35-71] | ≤0.01 |
| Creatinine (mg/dL) | 1.1 [0.8-1.5] | 1.2 [0.9-1.7] | 1.0 [0.8-1.3] | ≤0.01 |
| eGFR (mL/min) | 54 [36-75] | 55 [36-76] | 53 [35-73] | 0.423 |
Data are median [IQR] for continuous non normal variables; eGFR: estimated Glomerular Filtration Rate; Kruskal Wallis Test per le differenze di significatività tra maschi e femmine; BUN= blood urea nitrogen.
Table 2.
Distribution of patients, also considering sex, in six age classes.
| Age classes | All n=1617 |
Males n=655 |
Females n=962 |
|---|---|---|---|
| <= 50 years n (%) | 30 (1.9) | 14 (2.1) | 16 (1.7) |
| 51-60 years n (%) | 29 (1.8) | 12 (1.8) | 17 (1.8) |
| 61-70 years n (%) | 85 (5.3) | 47 (7.2) | 38 (4.0) |
| 71-80 years n (%) | 277 (17.1) | 128 (19.5) | 149 (15.5) |
| 81-90 years n (%) | 921 (57) | 374 (57.1) | 547 (56.9) |
| >= 91 years n (%) | 275 (17) | 80 (12.2)* | 195 (20.3)* |
*The distribution is statistically significant different.
Table 3.
D-dimer values and pulmonary embolism.
|
All median [IQR] |
Males median [IQR] |
Females median [IQR] |
|
| Pulmonary embolism (yes) |
8910 [4195-15817.5] | 14970 [6440-21612.5] | 5830 [4142.5-13202.5] |
| Pulmonary embolism (no) |
1160 [550-2740] | 1160 [505-2975] | 1180 [560-2615] |
| P | ≤0.01 | ≤0.01 | ≤0.01 |
Table 4.
Correlation of D-dimer levels and WBC, PCR and eGFR.
|
D-dimer levels median [IQR] |
P |
|
| WBC<= 9 | 950 [450-2110] | ≤0.01 |
| WBC> 9 | 1700 [740-4050] | |
| PCR<= 0.5 | 800 [460-1990] | ≤0.01 |
| PCR> 0.5 | 2030 [950-4592.5] | |
| eGFR<= 30 | 2030 [930-4300] | ≤0.01 |
| eGFR> 30 | 1090 [510-2550] |
Table 5.
Sensitivity and specificity of D-dimer test in the six age classes.
| Age classes | Patients (n of PE) |
Sensitivity (%) | Specificity (%) Cut-off 500 µg/L FEU |
Specificity (%) Cut-off ADC= (patient’s agex0.01) µg/L FEU |
Specificity (%) Cut-off (1050 µg/L FEU) |
|---|---|---|---|---|---|
| <= 50 years | 30 (0) | - | - |
- | - |
| 51-60 years | 29 (0) | - | - |
- | - |
| 61-70 years | 85 (1) | 100.0 | 65.5 | 72.6 | 76.2 |
| 71-80 years | 277 (9) | 100.0 | 33.6 | 51.5 | 64.2 |
| 81-90 years | 921 (30) | 100.0 | 16.3 | 34.0 | 40.6 |
| >= 91 years | 275 (2) | 100.0 | 9.9 | 28.2 | 30.4 |
PE=Pulmonary embolism.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



