Submitted:
20 May 2024
Posted:
21 May 2024
You are already at the latest version
Abstract
Despite global efforts to improve vaccination coverage, the number of zero dose and under immunized children has increased in the African continent, particularly in Nigeria where more than 2.3 million unvaccinated children currently reside, making it the country with highest number of unvaccinated children on the African continent. It is thus imperative to identity barriers and facilitators of immunization in Nigeria with a view to formulate and design targeted interventions that can effectively bridge the immunization gap in Nigeria. In this review, we systematically mapped and summarized existing literature and data on key barriers to vaccine uptake, and facilitators influencing immunization practices in Nigeria. The electronic databases were systematically searched and articles that reported determinants of routine immunization uptake in Nigeria from inception of the databases up till October 2023 were included. The eligible articles were evaluated using a set of pre-defined criteria and the extracted data were analysed and visualized. This scoping review identified barriers spanning logistical, socio-economic, cultural, and healthcare system-related aspects, highlighting the need for a multi-pronged approach to address these challenges. While considerable progress has been made over the years, persistent barriers like distance between area of residence of caregivers and immunization centers, vaccine shortages, poor interpersonal relationship between healthcare workers and caregivers and cultural/religious influences persist. Lastly, collaborative efforts among stakeholders and communities remain paramount in ensuring improved routine immunization coverage across the Nigeria’s diverse socio-cultural landscape.
Keywords:
Immunization
; Barriers
; Facilitators
; Scoping Review
; Nigeria
1. Introduction
Immunization is a critical and cost-effective public health interventions that has emerged as the indisputable cornerstone of global public health, effectively reducing morbidity and mortality from vaccine-preventable diseases [1]. As high as over four million deaths annually have been prevented by careful implementation of childhood immunization program around the world [1]. In recognition of the importance of childhood vaccines in public health, the World Health Organisation (WHO) in 1974 established the Expanded Programme on Immunisation (EPI) to ensure that all children have access to four recommended vaccines. This alongside other vaccines and doses constituted the routine immunization programme. Through immunization, the world has made significant progress in successfully reducing childhood diseases, especially under-five deaths since 1990, from 12.6 million to 5.4 million in 2017 [2].
Despite the proven benefits of immunization, challenges persist in ensuring that vaccines reach all individuals, particularly in resource-constrained settings [3]. Globally, while the number of zero-dose children has improved from 18.1 in 2021 to 14.3 million in 2022, this is not yet back to pre-pandemic level of 12.9 million [4]. According to 2022 estimates from the United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO), Nigeria holds a large share of burden of zero dose and under immunized children, with an estimated over 2.3 million [4]. Nigeria alongside Ethiopia, the Democratic Republic of the Congo, Angola, and Guinea collectively accounts for the highest burden of missed dose and zero dose children in Africa [5,6].
Nigeria has aligned with the global momentum on immunization equity and developed the three-year national strategic plan to optimize routine immunization with a goal to reduce zero dose children to less than 10% of the target cohort by 2024 (National Strategic Plan to Optimize Routine Immunization in Nigeria (2021-2024)). In a concerted push to bolster immunization coverage, the National Primary Health Care Development Agency (NPHCDA) took decisive action by declaring a state of emergency on routine immunization. This initiative led to the establishment of the National Emergency Routine Immunization Coordination Centre (NERICC). Collaborative efforts with developmental partners such as GAVI, USAIDS, among others, have resulted in considerable progress. Penta-3 coverage, for instance, has increased from 33% in 2016 to a commendable 54% by 2022 [4]. Nevertheless, challenges persist in achieving optimal immunization coverage, with rates still currently below the WHO target.
A number of factors including economic and political terrain serve as substantial barriers impeding the achievement of high and equitable immunization rates in Nigeria [7]. These barriers include, but are not limited to hesitancy and resistance by parents fuelled mainly by rumours about the safety of vaccines and partly by religious and cultural considerations [8,9]. Socioeconomic status of the parents, accessibility to healthcare, maternal education and area of residence in the country are other factors that have been identified to contribute to vaccine resistance [8,9].
As we confront the realities of vaccine-preventable diseases, understanding the specific landscape of immunization in Nigeria is of paramount importance. While several attempts have been made to summarise findings of various studies on determinants of childhood immunization, the studies were mostly limited in scope and contextual specificity [7]. To date, there has been no comprehensive review documenting regional variations in factors affecting immunization uptake in Nigeria. To overcome these challenges, a comprehensive examination of literature is required to understand both the obstacles impeding immunization coverage and the strategies that have facilitated progress over time. Such an assessment is fundamental to crafting targeted interventions and policies to strengthen immunization programs, reduce health disparities, and improve public health outcomes. The primary objective of this scoping review is to summarize existing literature and data on barriers and facilitators of immunization in Nigeria. Through a rigorous analysis of existing literature, we aim to delineate the factors that contribute to the current state of immunization in Nigeria, identify regional differences in immunization determinants and recommend appropriate measures to address the identified challenges. This scoping review is a component of a broader study entitled 'Closing the Immunization Gap: Enhancing Routine Immunization in Nigeria by Reaching Zero Dose and Under-Immunized Children in Marginalized Communities'. The study is based on a competitive grant awarded by Gavi to the Consortium of the African Field Epidemiology Network (AFENET)/Africa Health Budget Network (AHBN) as Country Learning Hub Partners for Immunization Equity in Nigeria (055-2022-Gavi-RFP).
2. Materials and Methods
2.1. Review Approach
The review was conducted in accordance with the published updated methodological guidance for the conduct of scoping reviews by the Joanna Briggs Institute (JBI) and Arksey and O’Malley [10,11]. Evidence synthesis and reporting was guided by the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for Scoping Reviews (PRISMA-ScR) checklist [12].
2.2. Research Questions
This scoping review attempts to answer the following fundamental questions:
- What are the facilitators influencing routine vaccination uptake in Nigeria?
- What are the specific barriers contributing to missed and zero doses children in Nigeria's vaccination programs?
- What variations exist at state and regional levels regarding barriers and facilitators of vaccination uptake in Nigeria?
2.3. Search Strategy and Study Selection
A systemic search of electronic databases comprising Google scholar, PubMed, Web of Science, EMBASE and AJOL (African Journals Online) was conducted on 28th of August 2023 and repeated on the 5th of October 2023. The search covers articles published in peer reviewed English language journals from database inception up to October 2023, targeting studies on determinants (barriers and facilitators) of immunization among human subjects in Nigeria. The search query employed Boolean operators to combine key concepts including "Immunization" or "Vaccination" or "Vaccines," "BCG vaccine" or "Bacillus Calmette-Guérin vaccine" "DTP vaccine" or "Diphtheria Tetanus Pertussis vaccine" or "Polio vaccine" OR "Pol" or “Polio Containing Vaccines” or “PCV” or “Rotavirus” or "Measles-Containing Vaccines" or "MCV” and “Facilitators” or “Drivers" or “Coverage" or "“Challenges" or “Barriers” and "Nigeria" or "Nigerian," or “"Abia" or "Adamawa" or "Akwa Ibom" or "Anambra" or "Bauchi" or "Bayelsa" or "Benue" or "Borno" or "Cross River" or "Delta" or "Ebonyi" or "Edo" or "Ekiti" or "Enugu" or "Gombe" or "Imo" or "Jigawa" or "Kaduna" or "Kano" or "Katsina" or "Kebbi" or "Kogi" or "Kwara" or "Lagos" or "Nasarawa" or "Niger" or "Ogun" or "Ondo" or "Osun" or "Oyo" or "Plateau" or "Rivers" or "Sokoto" or "Taraba" or "Yobe" or "Zamfara" or "The Federal Capital Territory" or "FCT" or "Abuja”. The synonyms and alternative terms of the keywords were searched to ensure comprehensive coverage of the topic.
In addition, a manual search of the bibliographies of the identified articles was performed to ensure no relevant article was inadvertently missed. The search was further supplemented with grey literatures and report on the same topic through a snowball approach with government, partners and funders working in the immunization space in Nigeria.
2.4. Study Selection
2.4.1. Inclusion Criteria
The retrieved articles were examined critically and included in the study if they met following criteria:
a) Original research articles focused on childhood vaccines and routine immunization in Nigeria
b) Focus on at least a factor facilitating or hindering vaccine uptake,
c) Studies in which qualitative, quantitative, or mixed methods were used and
d) Written or published in English Language and from the onset of the database till October 2023.
2.4.2. Exclusion Criteria
Studies conducted outside Nigeria or not related to barriers or drivers of immunization were excluded. Also, review articles, thesis and dissertations, editorials, letters to editor, commentary or opinion or perspective articles were excluded. The summary of the study selection criteria is presented in Table 1.
For the purpose of this review, we defined childhood immunization as all routine vaccines recommended by the NPHCDA for children under two (2) years of age in Nigeria. This includes Bacillus Calmette-Guérin (BCG) vaccine, Diphtheria, Tetanus, Pertussis (DTP) containing vaccine, Polio vaccines (Pol), and Measles-Containing Vaccines (MCV). The SPIDER framework (Table 2) was employed to systematically assess and evaluate the characteristics of included studies.
2.5. Study Identification
The retrieved references from databases were imported into an online systematic review management tool, Covidence. The duplicate references were removed, and the remaining records were screened first by title and abstract, independently by two reviewers to ensure accuracy. Disagreement among the reviewer’s during screening was resolved by consensus or involvement of a third reviewer when there were differences of opinion. This was followed by a stage of double independent screening in which full text of the articles that scaled through the first screening process were retrieved and imported into Covidence and screened. A double independent screening was used to ensure that the eligibility criteria were strictly followed.
2.6. Data Extraction
Key data were carefully extracted from the included studies into a data collection template predesigned and previously piloted for this scoping review in Covidence. The following data were obtained from each study: the first author's name, publication year, aim of study, study population (caregivers, opinion influencers, healthcare workers), study location (state and geopolitical zone), vaccination assessed (DTP, polio, childhood vaccines in general), study design, number of participants and relevant key findings related to immunization barriers and facilitators. Authors of articles with incomplete metadata were contacted by E-mail for supplementary information.
The framework proposed by Bedford et al. [13] which categorises factors influencing childhood vaccination uptake into three levels (Caregiver-related (individual) factors, Health systems-factors and government policy and Community/Social context) was adopted for this study.
2.7. Data Analysis
The characteristics of the study such as the year of publication, study location, type and number of participants were summarized using basic descriptive statistics (frequency and percentages). The major findings from each of the included studies were tabulated. The identified barriers and drivers were mapped into the three conceptual themes. The identified factors were delineated according to the Nigerian six geopolitical zones.
2.8. Ethical Consideration
The Study is part of a larger study implemented by the learning hub that was approved by the National Health Research Ethics Committee of Nigeria (NHREC) with NHREC Protocol Number: NHREC/01/01/2007-31/08/2023 and NHREC Approval Number: NHREC/01/01/2007-11/09/202.
3. Results
3.1. Study Selection and Inclusion Process
Our database search yielded 7044 potentially relevant references from Scopus, PubMed, Google scholar and AJOL. An additional 14 documents were obtained from various stakeholders working in the Nigerian immunization space. Of these, 3568 references were identified and removed as duplicates and an additional 3122 references removed as irrelevant during title and abstract screening. Of the remaining 368 studies considered of interest and assessed for full-text eligibility, 7 studies were inaccessible, and 251 studies were excluded for various reasons. Overall, 110 studies were included and used for evidence synthesis and mapping [8,9,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120]. The summary of study selection is presented in a PRISMA flow chart (Figure 1).
3.2. Characteristics of Included Studies
The characteristics of the included studies are summarised in Table 3.
A large proportion of studies (n= 26) targeted participants residing in all states of the federation. Some other studies concentrating on selected states (n= 11), either exclusively within the northern regions or spanning across both the northern and southern regions. The qualitative research approach (n =61) was the most frequently adopted study type. Data collection methods across all studies included questionnaire (n=32), analysis of secondary data (n =33), focus group discussions (n =7) and interviews (n =18). Most of the data analysed in studies involving analysis of secondary data were from Nigerian Demographic and Health Surveys (NDHS), Integrated Disease Surveillance and Response (IDSR), Multiple Indicator Cluster Survey (MICS), Post-Campaign Coverage Surveys (PCCS), Immunization Clinic Records, among others.
While vaccines included in the routine childhood immunization was the focus of most of the studies (n=89), few studies focused on specific childhood vaccines (Table 3).
This scoping review presented result of data involving a combined 271, 273 participants, comprising caregivers, community influencers and immunization implementing stakeholders.
3.3 Facilitators of Routine Immunization in Nigeria
3.3.1. Caregiver-Related Drivers
A total of 29 facilitators or drivers of childhood vaccines were recognised from the included studies. Of all the factors identified in various studies, maternal education of at least secondary education or higher was the most frequently mentioned (n=19) drivers of childhood immunization followed by delivery in a healthcare facility with skilled birth attendants (n=14). Moreover, maternal socio-economic status measured as high household wealth (n=10) and maternal age (≥ 20 years) at childbirth (n=9) were also mentioned in the literature (Figure 2).
Across all studies, cultural and religious factors (n=9) emerged prominently, alongside positive social support (n=8). Trust in healthcare providers (n=3), maternal discretion in vaccination decision-making without husband's consent (n=4), being married (n=1), and maintaining a monogamous family structure (n=1) were also identified as also playing significant roles in driving immunization uptake. The provision of non-financial incentives such as providing free transportation service to caregivers of vaccine eligible children (n=3) was also highlighted as another positive motivators.
3.3.2. Health-System Related Drivers
Adequate vaccine supply (n=2) and presence of a skilled healthcare workforce (n=3) were identified primarily as key elements of health-system related drivers. Additionally, timely immunization reminder systems and strong health information systems played were also vital. Furthermore, supportive government policies emerged as a facilitator of immunization (n=3). Vaccination at private health facilities was also identified (n=1), emphasizing their significance in the health system's role in promoting childhood immunization (Figure 3).
3.3.3. Community/Social Context Related Drivers
We identified five (5) drivers of immunization related to community/social context. Notably, community engagement and social mobilization (n=16). Residence in highbrow areas (n=2) and living in urban centres (n=6) emerged as noteworthy drivers. The presence of vaccine advocates in the community (n=3) and putting adequate security protection in place via engagement of security personnel (n=1) have also been reported (Figure 4).
3.4. Barriers of Routine Immunization in Nigeria
3.4.1. Caregiver-Related Barriers
Among the recognized caregiver-related barriers, the fear of side effects of immunization (n=20) and misinformation (n=19) emerged as prominent concerns affecting caregivers' decisions regarding childhood immunization. Furthermore, cultural, or religious beliefs (n=17) and lack of awareness about immunization schedule (n=19) were key factors shaping caregivers' perceptions and behaviours. Socioeconomic barriers were also evident, with low household wealth (n=17) and low or no maternal education (n=20) playing pivotal roles in vaccine uptake. Logistical challenges (n=29) posed by factors such as access to healthcare services, place of immunization, and cost of transportation to access immunization, further hindered caregivers' ability to access vaccines for their children (Figure 5).
3.4.2. Health System-Related Barriers
Among the health system-related barriers, vaccine shortages (n=20) emerged as the most prominent issue, significantly affecting vaccine accessibility. Poor interpersonal communication between healthcare workers and caregivers (n=13) further hinders effective immunization delivery. Healthcare workforce shortages (n=10) and lengthy queues at health facilities (n=8) contribute to service limitations. Inadequate access to healthcare (n=6) and weak supply chain management (n=5) compounded these challenges. Additionally, poor health information infrastructure (n=4), the cost of vaccination (n=3), and issues related to vaccine governance (n=3) serve as additional hurdles in the vaccination process (Figure 4).
3.4.3. Community/Social Context Related Barriers
Residency in rural or urban slum areas (n=14) and regional disparities with most authors reporting residency in northern and south-south regions of the country as prominent social barriers to immunization. Additionally, ethnicity (n=8) with authors reporting high vaccine hesitancy or refusal among Hausa/Fulani ethnic groups compared to Yoruba and Igbos and cultural or religious beliefs (n=6) playing substantial roles. Challenges from insurgency, conflict, and insecurity (n=6), along with high vaccine hesitancy or refusal among internally displaced individuals and migrants (n=4), were also noted. Distrust in the healthcare system, female-headed households, low literacy rates in communities, and lack of social support were additional barriers impacting childhood immunization.
3.5. Regional Insights into Childhood Immunization Dynamics in Nigeria
Our analysis revealed distinct regional variations in factors influencing immunization practices across Nigeria’s six geopolitical zones. Among studies conducted in a single state, majority were conducted in the south- west region (n= 21), followed by north-west region (n=17). Twelve of the studies were conducted in southeast while 10 and 9 studies each were conducted in the south-south and northeastern regions.
In the North-Eastern Zone, peer influence (n=1), robust reminder systems (n=2) and provision of additional security personnel bolstered acceptance and significantly supported adherence. Provision of financial incentive to health facilities based on vaccination performance was reported as a significant motivator in this region. In the North-Western region, caregivers were motivated by perceived vaccine benefits, fear of non-immunization consequences, and a perception that vaccinating one’s child makes one a good parent. Also, residents of urban and highbrow areas in northwest region tends to comply fully with immunization schedule. Health literacy and ANC visit were uniquely observed as major driving factors in this region. Additionally, the influence of community influencers such as religious and traditional rulers were noted, and their engagement and mobilization as vaccines advocates significantly improves immunization uptake in the region. Similar to the North-West, factors like knowledge, perceived benefits, and trust in healthcare providers were predominant drivers of immunization uptake in North-Central zone. Maternal autonomy in decision-making (n=1), health literacy (n=1), and fear of non-immunization consequences (n=1) played crucial roles in driving immunization practice in South-Eastern Zone.
South-South zone was unique for its strong peer influence (n=2) and widespread use of reminder systems like WhatsApp and SMS. Higher maternal education levels (n=3) were notable. Maternal autonomy (n=2), peer influence (n=2) alongside Health card usage (n=1), high maternal education (n=6), and the belief that vaccination defines responsible parenting (n=1) correlates with higher immunization uptake in the South-Western zone. Additionally, availability of vaccines and skilled health care workforce at immunization sites together with supportive government policies and provision of non-financial incentives were reported to be instrumental in driving immunization uptake in this region (Figure 2).
4. Discussion
In Nigeria, understanding the factors that influence immunization uptake and hesitancy is paramount as the country is currently home to highest number of missed dose children on the African continent. The review elucidates on these factors from the perspectives of both caregivers and immunization service providers. The reports of different studies summarized in this review revealed a multitude of interrelated and multi-layered challenges faced by caregivers in accessing immunization services in Nigeria.
The long distance between caregivers' homes and immunization centres stands out as the most frequently reported impediment to routine immunization uptake. Studies in Kenya, Ethiopia and Mozambique have similarly reported that children whose caregivers travelled shorter distances to health facilities for immunization were more likely to be fully vaccinated [121,122]. Despite initiatives like the 'Reaching Every Ward' policy by the Nigerian government, an adaptations of the WHO's 'Reaching Every District' strategy [123], more comprehensive efforts are needed to ensure the availability and easy accessibility of routine immunization services to the broader populace. Moreover, the scheduling of immunization campaigns on specific days like Mondays [83] or during market days [24], or during the rainy season [8,90] further exacerbates these accessibility challenges. This timing often conflicts with caregivers' work schedule, and further adding logistical strain and hindering their ability to prioritize vaccination schedules. In line with the finding of this study, inconvenient timing has also been identified as major hindrance to optimum immunization uptake in sub-Saharan Africa [122]. Gaining insights into caregivers' schedules via community feedback and adopting flexible immunization campaign strategies would markedly improve accessibility by aligning immunization schedules with caregivers' routines.
The finding that children of educated and employed mothers exhibited higher rates of complete vaccination aligns with report of a recent study [124]. This has been potentially attributed to better access to immunization information and a deeper understanding of its importance. Additionally, these mothers might be better able to afford and cover indirect costs associated with accessing immunization services. Promoting women's education through adult and nomadic education programs and creating opportunities for mothers to engage in gainful employment could significantly bolster immunization uptake in Nigeria.
Furthermore, the reviewed studies frequently cited instances of male heads of households refusing immunization [81]. Even when not explicitly expressed, their refusal to cover indirect costs and provide necessary support might prevent intending mothers from vaccinating their children. This refusal is more prevalent in north-western and north central states, where conservative Hausa/Fulani ethnic groups, largely comprising husband-headed households with husbands as the primary decision-makers, are predominant. This is a key equity and gender issue as prioritized by Gavi 5.0 guideline and it has also been identified as key barrier in other sub-Saharan Africa countries [122]. Empowering women financially and specifically engaging males during immunization mobilization becomes crucial in addressing this issue.
The finding that children of caregivers from wealthy households and highbrow areas of the society were likely to be fully vaccinated than children of mothers with low household wealth or resident of urban slum or rural areas concurs with several other reports [5,125]. This may be attributed to inequalities in terms of ability to access healthcare services including immunization services between poor and wealthy households as children from impoverished parents may face challenges in reaching health facilities and may also have difficulties covering indirect cost of immunization. In addition, they may not be able to afford interference with their daily business activities to access immunization services.
Certain cultural practices, such as the masquerades and 'oro' rites in southern Nigeria, were reported to impede caregivers' access to immunization services [8]. To mitigate such barriers, proactive measures such as scheduling around cultural festivities should be taken during the planning of immunization campaigns, to ensure maximum participation and accessibility for caregivers. Furthermore, a significant disparity was observed in the immunization rates among children based on the religious affiliation of their caregivers. Children under the care of Christian caregivers, particularly within the Catholic faith, exhibited higher rates of complete immunization compared to children whose caregivers identified with the Islamic faith [68,80]. This discrepancy could be attributed to religion inspired concern about vaccine safety and an enduring impact of a religious campaign against immunization, stemming from the botched Pfizer vaccine in the 1990s in Kano state [55]. This incident triggered a widespread boycott of immunization services, particularly within the Muslim-dominated northern region of Nigeria. The recurrent mention of religion's influence on routine immunization uptake in Nigeria aligns with similar reports from neighbouring countries like Ghana [126]. Efforts should therefore be directed towards fostering community engagement, building trust, and conducting tailored awareness campaigns within religious communities to dispel myths, address concerns, and promote the importance of immunization for overall community health.
The impact of cultural gender sensitivity on immunization uptake was notably observed, especially in conservative northern regions where male heads of households may object to male vaccinators accessing their household for vaccination purposes during outreach campaigns [29]. Similar sensitivities have been identified in culturally sensitive areas like Bangladesh [127]. Deploying dedicated teams of female vaccinators and female community influencers is imperative to bolster acceptance and accessibility.
Misinformation surrounding immunization and concerns about potential side effects were consistently also highlighted across several studies as significant barriers to achieving effective immunization uptake. For instance, at the turn of millennium, there was widespread and prolonged beliefs in the Muslim dominated north and supported by influencer religious organisations that vaccines were deliberately contaminated with anti-fertility drugs and HIV virus in order to depopulate the north [128,129]. Similarly, people in other countries like France have expressed low confidence in vaccine, often fuelled by circulating rumours questioning vaccine safety [130]. Therefore, proactive measures aimed at dispelling myths and allaying fears surrounding immunization are essential to foster trust and encourage higher vaccination rates.
Within the spectrum of healthcare system-related barriers, shortage of vaccines emerged as the most frequently cited barrier, signifying a persistent gap in the consistent availability of vaccines despite multifaceted efforts by stakeholders. Moreover, the prominence of poor interpersonal communication, healthcare workforce shortages, and lengthy queues at immunization centres highlights the multifaceted nature of barriers hindering routine immunization uptake. These factors collectively underscore the need for comprehensive solutions, spanning from targeted training programs to alleviate communication gaps among healthcare providers to strategic workforce planning initiatives aimed at mitigating staffing shortages.
Among the community/social context, resident in rural areas or in urban slum [31,47,110], residing in northern or south-south regions of the country [80], belonging to Hausa/Fulani or Kanuri ethnic groups [80,86,94], conflict affected [46,102] , displacement and migration [82] were the most frequently reported barriers. The regional discrepancies in immunization uptake are not unexpected as each of the Nigeria’s six geopolitical zones have varying socio-economic, cultural, and demographic development which may in turn influence health seeking behaviours including immunization practice. Northern regions in particular are economically disadvantaged regions with spectre of conflicts and armed insurgency and home to the highest number of uneducated individuals in the country [131]. Additionally, rural areas and urban slums face impediments in accessing healthcare services due to infrastructure deficit hampering vaccine delivery and coverage.
The general insecurity exemplified by Boko-haram insurgency in north-eastern states of Borno and Yobe [46,76,102] and unabated armed conflict between herdsmen and farmers on land and grazing paths in Benue states [70] often leads to population displacement and migration, and consequently significant disruption of immunization efforts. In the north-western states particularly Sokoto, Kebbi and Zamfara axis, armed banditry typifies by mass kidnapping, robbery along major highways, cattle rustling, and disruption of socio-economic activities by ethnic militias has resulted in internal displacement of thousands of people and missed communities [132]. The insecurity has recently extended into the south-eastern states where the armed wing of Indigenous People of Biafra has been enforcing a mandatory Monday sit-at-home order with attendant impact on vaccination coverage. The finding of severe negative impact of conflict on vaccination uptake in this study aligns with a report of multinational study where similarly conflicts and insecurity was reported to be associated with sudden drops in national and sub-national immunisation coverage e [133]. The hard-to-reach conflict affected regions should be prioritized during outreach campaigns and heightened security measures should be put in place to safeguard routine immunization personnel and give confidence to the targeted populace.
5. Conclusions
This review underscores the multifaceted challenges hindering routine immunization uptake in Nigeria and the variation in factors and gaps in evidence by region. The identified barriers span logistical, socio-economic, cultural, and healthcare system-related aspects, highlighting the need for a multi-pronged approach to address these challenges. While considerable progress has been made over the years, persistent barriers like distance between area of residence of caregivers and immunization centres, vaccine shortages, poor interpersonal relationship between healthcare workers and caregivers and cultural/religious influences persist. Collaborative efforts among stakeholders and communities remain paramount in ensuring improved routine immunization coverage across the diverse socio-cultural landscape of Nigeria.
6. Future Directions
We aimed to present these findings to immunization stakeholders in Nigeria and to further prioritized and implement mitigation measures on lessons from this review so that a concerted effort will be done to address these factors in line with the mandate of the Gavi led Zero Dose Learning Hub implemented by the AFENET/AHBN consortium. It is the vision of the Zero Dose Learning Hub through the rapid assessment, implementation research, and other activities to go much deeper in to understanding these barriers for under-represented states and to understand how ZD children may face multiple deprivations and the interacting effects of multiple barriers or enablers.
7. Limitations
This review on childhood immunization in Nigeria highlights identified drivers, barriers, variations, and gaps at the sub-national level particularly. We acknowledge the potential influence of investigator perspectives and limited data availability on their scope. It is important to note that additional potentially significant barriers relating to ZD children and missed communities may exist beyond the current identified list Further research and data collection are crucial to gain a comprehensive understanding of the full spectrum of challenges. Moreover, the dynamic nature of immunization programs underscores the potential for the review to not fully capture the latest developments or practice changes that may have occurred recently like the focus on 100 LGAs to identify and reach ZD children and the recent introduction of the human papilloma virus vaccine in Nigeria and its associated challenges.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. The Data Extraction Table has been provided as a supplement (S-1).
Author Contributions
Conceptualization: Y.M.: H.W.R, G.C.C., H.W., A.O., M.W., B.U., M.K., N.E.W. and P.N., methodology: Y.M., H.W., A.O., M.M., N.A., I.H., M.T., M.W. and B.U., ; software: A.A, A.O., validation: A.O.A., Y.Y., I.W.B., S.E., A.Y., R.G., M.K. and N.E.W.; formal analysis: Y.M., A.O., H.W., A.A, B.D.L., T.B.B., L.S.M., O.F., O.P., A.M.G. and M.U., resources: I.W.B., S.E., A.Y., R.G., H.W.R., G.C.C., N.V., T.F., N.M., Y.Y. and P.N., ; data curation: A.O., A.A., B.D.L., T.B.B., L.S.M., O.F., O.P., A.M.G. and M.U.; writing—original draft preparation: Y.M., A.O.A., M.W., B.U., A.O., M.M., N.A., I.H. and M.T., writing—review and editing: M.K., N.E.W., Y.Y., P.N., N.V., T.F., N.M, H.W.R. and G.C.C. ; visualization: I.W.B., A.O., S.E., A.Y., R.G., M.M., N.A., I.H. and M.T.,; supervision: N.V., T.F., N.M., H.W.R and P.N.; project administration: Y.M., M.K., N.E.W., P.N., P.N.; funding acquisition: M.K., N.E.W., P.N., G.C.C., and H.W.R. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by Gavi - The Vaccine Alliance, based on a competitive grant awarded to the Consortium of the African Field Epidemiology Network (AFENET)/Africa Health Budget Network (AHBN) as Country Learning Hub Partners for Immunization Equity in Nigeria (055-2022-Gavi-RFP) through the Zero Dose Learning Hub (ZDLH) project in Nigeria.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of NATIONAL HEALTH RESEARCH ETHICS COMMITTEE. The Study is part of a larger study implemented by the learning hub that was ap-proved by the National Health Research Ethics Committee of Nigeria (NHREC) with NHREC Protocol Number: NHREC/01/01/2007-31/08/2023 and NHREC Approval Number: NHREC/01/01/2007-11/09/202.
Informed Consent Statement
Not applicable.
Acknowledgments
This is to acknowledge all immunization stakeholders within and outside Nigeria that supported this review by the provision of relevant reports, documents, and guidance to this review.
Conflicts of Interest
The authors declare no conflicts of interest. All authors (including the funders) provided technical support in the design of the study; collection, analyses, interpretation of data; writing of the manuscript; and in the decision to publish the results.
References
- WHO. Immunization. WHO Reg Off Afr 2023. https://www.afro.who.int/health-topics/immunization (accessed September 23, 2023).
- Unicef undefined. Levels and trends in child mortality report 2017 2017.
- Yamey G, Garcia P, Hassan F, Mao W, McDade KK, Pai M, et al. It is not too late to achieve global covid-19 vaccine equity. BMJ 2022;376:e070650. [CrossRef]
- WHO/UNICEF. Progress and Challenges with achieving Universal Immunization Coverage: 2022 Estimates of National Immunization coverage. 2022.
- Hosseinpoor AR, Bergen N, Schlotheuber A, Gacic-Dobo M, Hansen PM, Senouci K, et al. State of inequality in diphtheria-tetanus-pertussis immunisation coverage in low-income and middle-income countries: a multicountry study of household health surveys. Lancet Glob Health 2016;4:e617–26. [CrossRef]
- Khetsuriani N, Mosina L, Van Damme P, Mozalevskis A, Datta S, Tohme RA. Progress Toward Hepatitis B Control - World Health Organization European Region, 2016-2019. MMWR Morb Mortal Wkly Rep 2021;70:1029–35. [CrossRef]
- Mahachi K, Kessels J, Boateng K, Jean Baptiste AE, Mitula P, Ekeman E, et al. Zero- or missed-dose children in Nigeria: Contributing factors and interventions to overcome immunization service delivery challenges. Vaccine 2022;40:5433–44. [CrossRef]
- Akwataghibe NN, Ogunsola EA, Broerse JEW, Popoola OA, Agbo AI, Dieleman MA. Exploring Factors Influencing Immunization Utilization in Nigeria—A Mixed Methods Study. Front Public Health 2019;7.
- Ataguba JE, Ojo KO, Ichoku HE. Explaining socio-economic inequalities in immunization coverage in Nigeria. Health Policy Plan 2016;31:1212–24.
- Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth 2020;18:2119. [CrossRef]
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005;8:19–32. [CrossRef]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018;169:467–73. [CrossRef]
- Bedford H, Attwell K, Danchin M, Marshall H, Corben P, Leask J. Vaccine hesitancy, refusal and access barriers: The need for clarity in terminology. Vaccine 2018;36:6556–8. [CrossRef]
- Olaniyan A, Isiguzo C, Hawk M. The Socioecological Model as a framework for exploring factors influencing childhood immunization uptake in Lagos state, Nigeria. BMC Public Health 2021;21:867. [CrossRef]
- Omoleke SA, Tadesse MG. A pilot study of routine immunization data quality in Bunza Local Government area: causes and possible remedies. Pan Afr Med J 2017;27. [CrossRef]
- Abad N, Uba BV, Patel P, Barau DN, Ugochukwu O, Aliyu N, et al. A rapid qualitative assessment of barriers associated with demand and uptake of health facility-based childhood immunizations and recommendations to improve immunization service delivery in Sokoto State, Northwest Nigeria, 2017. Pan Afr Med J 2021;40:10. [CrossRef]
- Odinaka. Acceptance of mobile phone short message service for childhood immunisation reminders by Nigerian mothers n.d. https://www.phmj.org/article.asp?issn=0795-3038;year=2018;volume=12;issue=3;spage=127;epage=130;aulast=Odinaka (accessed October 5, 2023).
- Michael CA, Team OCMCS, Ashenafi S, Team OCMCS, Ogbuanu IU, Team OCMCS, et al. An evaluation of community perspectives and contributing factors to missed children during an oral polio vaccination campaign–Katsina State, Nigeria. J Infect Dis 2014;210:S131–5.
- Uwaibi N, Erah F. Assessment of healthcare worker’s implementation of childhood routine immunization in primary healthcare centers in Edo State, Nigeria: A mixed method survey. Ann Clin Biomed Res 2021;2. [CrossRef]
- Danjuma SD, Ibrahim AI, Shehu NY, Diala MU, Pam CV, Ogbodo CO. At-birth vaccination timeliness: An analysis of inborns in the highlands of Jos, North-Central Nigeria. Niger Postgrad Med J 2020;27:209–14. [CrossRef]
- Ekhaguere OA, Oluwafemi RO, Badejoko B, Oyeneyin LO, Butali A, Lowenthal ED, et al. Automated phone call and text reminders for childhood immunisations (PRIMM): a randomised controlled trial in Nigeria. BMJ Glob Health 2019;4:e001232. [CrossRef]
- Akaba GO, Dirisu O, Okunade KS, Adams E, Ohioghame J, Obikeze OO, et al. Barriers and facilitators of access to maternal, newborn and child health services during the first wave of COVID-19 pandemic in Nigeria: findings from a qualitative study. BMC Health Serv Res 2022;22:611. [CrossRef]
- Freeland C, Kanu F, Mohammed Y, Nwokoro UU, Sandhu H, Ikwe H, et al. Barriers and facilitators to hepatitis B birth dose vaccination: Perspectives from healthcare providers and pregnant women accessing antenatal care in Nigeria. PLOS Glob Public Health 2023;3:e0001332.
- Olaniyan A, Isiguzo C, Agbomeji S, Akinlade-Omeni O, Ifie B, Hawk M. Barriers, facilitators, and recommendations for childhood immunisation in Nigeria: perspectives from caregivers, community leaders, and healthcare workers. Pan Afr Med J 2022;43.
- Nasiru S-G, Aliyu GG, Gasasira A, Aliyu MH, Zubair M, Mandawari SU, et al. Breaking community barriers to polio vaccination in northern Nigeria: the impact of a grass roots mobilization campaign (Majigi). Pathog Glob Health 2012;106:166–71. [CrossRef]
- Adekunle L. Child immunization—What are the impediments for reaching desired goals in a transitional society? Soc Sci Med Part Med Psychol Med Sociol 1978;12:353–7. [CrossRef]
- McGavin ZA, Wagner AL, Carlson BF, Power LE, Eboreime E, Boulton ML. Childhood full and under-vaccination in Nigeria, 2013. Vaccine 2018;36:7294–9. [CrossRef]
- Uthman OA, Adedokun ST, Olukade T, Watson S, Adetokunboh O, Adeniran A, et al. Children who have received no routine polio vaccines in Nigeria: Who are they and where do they live? Hum Vaccines Immunother 2017;13:2111–22. [CrossRef]
- Babalola S. COMMUNITY AND SYSTEMIC FACTORS AFFECTING THE UPTAKE OF IMMUNISATION IN NIGERIA: A QUALITATIVE STUDY IN FIVE STATES 2023.
- McArthur-Lloyd A, McKenzie A, Findley SE, Green C, Adamu F. Community Engagement, Routine Immunization, and the Polio Legacy in Northern Nigeria. Glob Health Commun 2016;2:1–10. [CrossRef]
- Itimi K, Dienye PO, Ordinioha B. Community participation and childhood immunization coverage: a comparative study of rural and urban communities of Bayelsa State, south-south Nigeria. Niger Med J J Niger Med Assoc 2012;53:21.
- Nalley JC, Maduka O. Completeness and timeliness of immunization among children aged 12 to 23 months in South-South Nigeria. J Community Med Prim Health Care 2019;31:22–31. [CrossRef]
- Onyeneho N, Igwe I, I’Aronu N, Okoye U. Compliance With Regimens of Existing Vaccines in Orumba North Local Government Area of Anambra State, Nigeria. Int Q Community Health Educ 2015;35:120–32. [CrossRef]
- Duru JI, Usman S, Adeosun O, Stamidis KV, Bologna L. Contributions of volunteer community mobilizers to polio eradication in Nigeria: the experiences of non-governmental and civil society organizations. Am J Trop Med Hyg 2019;101:74.
- Kawakatsu Y, Adesina AO, Kadoi N, Aiga H. Cost-effectiveness of SMS appointment reminders in increasing vaccination uptake in Lagos, Nigeria: a multi-centered randomized controlled trial. Vaccine 2020;38:6600–8.
- Nwangwu CC, Chike AE, Eucharia Ijeoma IO. Cross-sectional Survey on Parental Perception and Attitude on Measles Vaccine: Low Hospital Measles Case Presentation in Rural Area in Enugu Nigeria. J Clin Diagn Res 2021;15.
- Obi-Jeff C, Garcia C, Onuoha O, Adewumi F, David W, Bamiduro T, et al. Designing an SMS reminder intervention to improve vaccination uptake in Northern Nigeria: a qualitative study. BMC Health Serv Res 2021;21:844. [CrossRef]
- Konwea PE, David FA, Ogunsile SE. Determinants of compliance with child immunization among mothers of children under five years of age in Ekiti State, Nigeria. J Health Res 2018;32:229–36. [CrossRef]
- Alhassan NH, Hamza AM, Bala U, Kaugama BM. Determinants of Immunization Coverage in Children 12-23 Months in Miga Local Government Area, Jigawa State Nigeria. South Am J Public Health 2016:1–13.
- Gidado S, Nguku P, Biya O, Waziri N, Mohammed A, Nsubuga P. Determinants of routine immunization coverage in Bungudu, Zamfara state, northern Nigeria, may 2010. Pan Afr Med J. 2014; 18 n.d.
- Babalola S. Determinants of the Uptake of the Full Dose of Diphtheria–Pertussis–Tetanus Vaccines (DPT3) in Northern Nigeria: A Multilevel Analysis. Matern Child Health J 2009;13:550–8. [CrossRef]
- Fatiregun AA, Etukiren EE. Determinants of uptake of third doses of oral polio and DTP vaccines in the Ibadan North Local Government Area of Nigeria. Int Health 2014;6:213–24.
- Olumuyiwa O Odusanya. Determinants of vaccination coverage in rural Nigeria | BMC Public Health | Full Text n.d. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-8-381 (accessed October 14, 2023).
- Sato R. Differential determinants and reasons for the non-and partial vaccination of children among Nigerian caregivers. Vaccine 2020;38:63–9.
- IPSOS. Drivers And Barriers To Uptake And Completion Of Early Years Vaccination: Early Insights n.d.
- Sato R. Effect of armed conflict on vaccination: evidence from the Boko haram insurgency in northeastern Nigeria. Confl Health 2019;13:49. [CrossRef]
- Balogun FM, Bamidele OS, Bamgboye EA. Effect of intensive training in improving older women’s knowledge and support for infant vaccination in Nigerian urban slums: a before-and-after intervention study. BMC Public Health 2021;21:266. [CrossRef]
- Brown VB, Oluwatosin OA, Akinyemi JO, Adeyemo AA. Effects of Community Health Nurse-Led Intervention on Childhood Routine Immunization Completion in Primary Health Care Centers in Ibadan, Nigeria. J Community Health 2016;41:265–73. [CrossRef]
- Dougherty L, Abdulkarim M, Ahmed A, Cherima Y, Ladan A, Abdu S, et al. Engaging traditional barbers to identify and refer newborns for routine immunization services in Sokoto, Nigeria: a mixed methods evaluation. Int J Public Health 2020;65:1785–95. [CrossRef]
- Afolabi RF, Salawu MM, Gbadebo BM, Salawu AT, Fagbamigbe AF, Adebowale AS. Ethnicity as a cultural factor influencing complete vaccination among children aged 12-23 months in Nigeria. Hum Vaccines Immunother 2021;17:2008–17. [CrossRef]
- Fagbamigbe AF, Lawal TV, Atoloye KA. Evaluating the performance of different Bayesian count models in modelling childhood vaccine uptake among children aged 12–23 months in Nigeria. BMC Public Health 2023;23:1197. [CrossRef]
- Balogun FM, Omotade OO. Facilitators and barriers of healthcare workers’ recommendation of HPV vaccine for adolescents in Nigeria: views through the lens of theoretical domains framework. BMC Health Serv Res 2022;22:824. [CrossRef]
- Taiwo L, Idris S, Abubakar A, Nguku P, Nsubuga P, Gidado S, et al. Factors affecting access to information on routine immunization among mothers of under 5 children in Kaduna State Nigeria, 2015. Pan Afr Med J 2017;27.
- Oku A, Oyo-Ita A, Glenton C, Fretheim A, Eteng G, Ames H, et al. Factors affecting the implementation of childhood vaccination communication strategies in Nigeria: a qualitative study. BMC Public Health 2017;17:1–12.
- Ghani NA, Dalhatu S, Adam MF, Ghazalli FSM. Factors Associated with Polio Immunization Resistivityin Kano State, Nigeria. Env Sci 2015.
- Sadoh AE, Sadoh WE, Uduebor J, Ekpebe P, Iguodala O. Factors contributing to delay in commencement of immunization in Nigerian infants. Tanzan J Health Res 2013;15.
- Rahji FatimaR. Factors Influencing Compliance with Immunization Regimen among Mothers in Ibadan, Nigeria. IOSR J Nurs Health Sci 2013;2:01–9. [CrossRef]
- Antai D. Gender inequities, relationship power, and childhood immunization uptake in Nigeria: a population-based cross-sectional study. Int J Infect Dis 2012;16:e136–45.
- Tobin-West CI, Alex-Hart BA. Identifying Barriers and Sustainable Solution to Childhood Immunization in Khana Local Government Area of Rivers State, Nigeria. Int Q Community Health Educ 2012;32:149–58. [CrossRef]
- Adedire EB, Ajayi I, Fawole OI, Ajumobi O, Kasasa S, Wasswa P, et al. Immunisation coverage and its determinants among children aged 12-23 months in Atakumosa-west district, Osun State Nigeria: a cross-sectional study. BMC Public Health 2016;16:905. [CrossRef]
- Fajola A, Chidozie B. Immunization Completion Rates in a Cottage Hospital in the Niger Delta Area of Nigeria 2018;Volume 8:51–3.
- Nkwogu L, Shuaib F, Braka F, Mkanda P, Banda R, Korir C, et al. Impact of engaging security personnel on access and polio immunization outcomes in security-inaccessible areas in Borno state, Nigeria. BMC Public Health 2018;18:1311. [CrossRef]
- Walker J-A, Hashim Y, Oranye N. Impact of Muslim opinion leaders’ training of healthcare providers on the uptake of MNCH services in Northern Nigeria. Glob Public Health 2019;14:200–13. [CrossRef]
- Gooding E, Spiliotopoulou E, Yadav P. Impact of vaccine stockouts on immunization coverage in Nigeria. Vaccine 2019;37:5104–10.
- Obi-Jeff C, Garcia C, Adewumi F, Bamiduro T, David W, Labrique A, et al. Implementing SMS reminders for routine immunization in Northern Nigeria: a qualitative evaluation using the RE-AIM framework. BMC Public Health 2022;22:2370. [CrossRef]
- Yau IB, Mustapha MZ, Nwaze E, Nobila O, Maigoro A, Abdullah A, et al. Improving the timeliness and completeness of childhood vaccination through color-coded bracelets: a pilot study among Fulani tribe populations in Nigeria. J Public Health Afr 2023.
- Adedokun ST, Uthman OA, Adekanmbi VT, Wiysonge CS. Incomplete childhood immunization in Nigeria: a multilevel analysis of individual and contextual factors. BMC Public Health 2017;17:236. [CrossRef]
- Oleribe O, V K, A A-O, Sd T-R. Individual and socioeconomic factors associated with childhood immunization coverage in Nigeria. Pan Afr Med J 2017;26. [CrossRef]
- Adeiga A, Omilabu SA, Audu RA, Sanni FA, Lakehinde GF, Balogun O, et al. Infant immunization coverage in difficult-to-reach area of Lagos metropolis. Afr J Clin Exp Microbiol 2005;6:227–31. [CrossRef]
- Korave J, Bawa S, Ageda B, Ucho A, Bem-Bura DM, Onimisi A, et al. Internal displacement; an impediment to the successful implementation of planned measles supplemental activities in Nigeria, a case study of Benue State. Vaccine 2021;39:C76–81.
- Limaye RJ, Sara AB, Siddique AR, Vivas C, Malik S, Omonoju K. Interpersonal and community influences affecting childhood vaccination decision-making among Nigerian caregivers: Perceptions among frontline workers in Nigeria. J Child Health Care 2019;23:403–14. [CrossRef]
- Umoke PCI, Umoke M, Nwalieji CA, Igwe FO, Umoke UG, Onwe RN, et al. Investigating Factors Associated with Immunization Incompletion of Children Under Five in Ebonyi State, Southeast Nigeria: Implication for Policy Dialogue. Glob Pediatr Health 2021;8:2333794X2199100. [CrossRef]
- Sibeudu FT, Uzochukwu BSC, Onwujekwe OE. Investigating socio-economic inequity in access to and expenditures on routine immunization services in Anambra state. BMC Res Notes 2017;10:78. [CrossRef]
- Mangal TD, Aylward RB, Mwanza M, Gasasira A, Abanida E, Pate MA, et al. Key issues in the persistence of poliomyelitis in Nigeria: a case-control study. Lancet Glob Health 2014;2:e90–7.
- Adegbenro CA, Olowookere SA, Fehintola FO, Adegbenro PA, Orioke OT. Knowledge about and preventive practices against neonatal tetanus among young Nigerian women. Tzu-Chi Med J 2019;31:154.
- M Shuaibu F, Birukila G, Usman S, Mohammed A, Galway M, Corkum M, et al. Mass immunization with inactivated polio vaccine in conflict zones – Experience from Borno and Yobe States, North-Eastern Nigeria. J Public Health Policy 2016;37:36–50. [CrossRef]
- Fatiregun AA, Okoro AO. Maternal determinants of complete child immunization among children aged 12–23 months in a southern district of Nigeria. Vaccine 2012;30:730–6. [CrossRef]
- Okenwa UJ, Dairo MD, Bamgboye E, Ajumobi O. Maternal knowledge and infant uptake of valid hepatitis B vaccine birth dose at routine immunization clinics in Enugu State – Nigeria. Vaccine 2020;38:2734–40. [CrossRef]
- Okenwa UJ, Dairo MD, Uba B, Ajumobi O. Maternal reasons for non-receipt of valid Hepatitis B birth dose among mother-infant pairs attending routine immunization clinics, South-east, Nigeria. Vaccine 2019;37:6894–9.
- Chidiebere ODI, Uchenna E, Kenechi OS. Maternal sociodemographic factors that influence full child immunisation uptake in Nigeria. South Afr J Child Health 2014;8:138–42.
- Okafor IP, Chukwudi CL, Igwilo UU, Ogunnowo BE. “Men are the head of the family, the dominant head”: A mixed method study of male involvement in maternal and child health in a patriarchal setting, Western Nigeria. PLOS ONE 2022;17:e0276059. [CrossRef]
- Antai D. Migration and child immunization in Nigeria: individual- and community-level contexts. BMC Public Health 2010;10:116. [CrossRef]
- Fatiregun AA, Lochlainn LN, Kaboré L, Dosumu M, Isere E, Olaoye I, et al. Missed opportunities for vaccination among children aged 0–23 months visiting health facilities in a southwest State of Nigeria, December 2019. PLOS ONE 2021;16:e0252798. [CrossRef]
- MRITE. Momentum Routine Immunization Transformation and Equity : Baseline Assessment of Routine Immunization Services Performance. n.d.
- Adegboye OA, Kotze D, Adegboye OA. Multi-year trend analysis of childhood immunization uptake and coverage in Nigeria. J Biosoc Sci 2014;46:225–39.
- Aheto JMK, Pannell O, Dotse-Gborgbortsi W, Trimner MK, Tatem AJ, Rhoda DA, et al. Multilevel analysis of predictors of multiple indicators of childhood vaccination in Nigeria. Plos One 2022;17:e0269066.
- Oladepo O, Dipeolu IO, Oladunni O. Nigerian rural mothers’ knowledge of routine childhood immunizations and attitudes about use of reminder text messages for promoting timely completion. J Public Health Policy 2019;40:459–77. [CrossRef]
- Obanewa OA. Optimising childhood immunisation in Nigeria. phd. University of Southampton, 2019.
- Oku A, A O-I, C G, A F, H A, A M, et al. Perceptions and experiences of childhood vaccination communication strategies among caregivers and health workers in Nigeria: A qualitative study. PloS One 2017;12. [CrossRef]
- Etokidem A, Nkpoyen F, Ekanem C, Mpama E, Isika A. Potential barriers to and facilitators of civil society organization engagement in increasing immunization coverage in Odukpani Local Government Area of Cross River State, Nigeria: an implementation research. Health Res Policy Syst 2021;19:1–12.
- Ogbuabor DC, Chime AC. Prevalence and predictors of vaccine hesitancy among expectant mothers in Enugu metropolis, South-east Nigeria. J Public Health Policy 2021;42:222–35. [CrossRef]
- Victoria TO, Ogunleye A, Abubakar MA, Abacha M, Okijiola SO, Adediji PO. Routine Immunization Compliance among Nursing Mothers in Ibadan North East Local Government, Oyo State, Nigeria. Eur J Mod Med Pract 2023;3:82–93.
- Gunnala R, Ogbuanu IU, Adegoke OJ, Scobie HM, Uba BV, Wannemuehler KA, et al. Routine Vaccination Coverage in Northern Nigeria: Results from 40 District-Level Cluster Surveys, 2014-2015. PLOS ONE 2016;11:e0167835. [CrossRef]
- Antai D. Rural-urban inequities in childhood immunisation in Nigeria: The role of community contexts. Afr J Prim Health Care Fam Med 2011;3:1–8.
- Nwokocha EE, Obioma C. Social and cultural factors influencing immunization of children in rural Abia State, Nigeria. Int J Child Youth Fam Stud 2016;7:404–22.
- Monguno AK. Socio cultural and geographical determinants of child immunisation in Borno State, Nigeria. J Public Health Afr 2013;4.
- Oluwatosin OA. Socio-demographic factors associated with childhood immunization uptake in Akinyele Local Government Area, Oyo State, Nigeria. Afr J Med Med Sci 2012;41:161–7.
- Ilusanya T, Oladosun M. Socio-Economic Factors Influencing Health Behavior of Women and Immunization Status of Children in Nigeria. 2017.
- Okoro JC, Ojinnaka NC, Ikefuna AN, Onyenwe NE. Sociodemographic influences on immunization of children with chronic neurological disorders in Enugu, Nigeria. Trials Vaccinol 2015;4:9–13.
- Lawal TV, Atoloye KA, Adebowale AS, Fagbamigbe AF. Spatio-temporal analysis of childhood vaccine uptake in Nigeria: a hierarchical Bayesian Zero-inflated Poisson approach. BMC Pediatr 2023;23:493. [CrossRef]
- Korir C, Shuaib F, Adamu U, Bawa S, Musa A, Bashir A, et al. Targeting the last polio sanctuaries with Directly Observed Oral Polio Vaccination (DOPV) in northern Nigeria, (2014–2016). BMC Public Health 2018;18:1314. [CrossRef]
- Babakura B, Nomhwange T, Baptiste AEJ, Dede O, Taiwo L, Abba S, et al. The challenges of insecurity on implementing vaccination campaign and its effect on measles elimination and control efforts: A case study of 2017/18 measles campaign in Borno state, Nigeria q 2021.
- Sato R, Belel A. The effect of performance-based financing on child vaccinations in northern Nigeria. Vaccine 2020;38:2209–15.
- Anichukwu OI, Asamoah BO. The impact of maternal health care utilisation on routine immunisation coverage of children in Nigeria: a cross-sectional study. BMJ Open 2019;9:e026324.
- Sato R. The impacts of quantity and quality of health clinics on health behaviors and outcomes in Nigeria: analysis of health clinic census data. BMC Health Serv Res 2019;19:377. [CrossRef]
- Oluwadare C. The Social Determinants of Routine Immunisation in Ekiti State of Nigeria. Stud Ethno-Med 2009;3:49–56. [CrossRef]
- Masresha B, Nwankwo O, Bawa S, Igbu T, Oteri J, Tafida H, et al. The use of WhatsApp group messaging in the coordination of measles supplemental immunization activity in Cross Rivers State, Nigeria, 2018. Pan Afr Med J 2020;35.
- Adeyanju GC, Sprengholz P, Betsch C. Understanding drivers of vaccine hesitancy among pregnant women in Nigeria: A longitudinal study. Npj Vaccines 2022;7:96.
- Taylor S, Khan M, Muhammad A, Akpala O, van Strien M, Morry C, et al. Understanding vaccine hesitancy in polio eradication in northern Nigeria. Vaccine 2017;35:6438–43.
- Ijarotimi IT, Fatiregun AA, Adebiyi OA, Ilesanmi OS, Ajumobi O. Urban–rural differences in immunisation status and associated demographic factors among children 12-59 months in a southwestern state, Nigeria. PLoS One 2018;13:e0206086.
- Ozawa S, Wonodi C, Babalola O, Ismail T, Bridges J. Using best-worst scaling to rank factors affecting vaccination demand in northern Nigeria. Vaccine 2017;35:6429–37. [CrossRef]
- Akwataghibe NN, Ogunsola EA, Popoola OA, Agbo AI, Dieleman MA. Using participatory action research to improve immunization utilization in areas with pockets of unimmunized children in Nigeria. Health Res Policy Syst 2021;19:88. [CrossRef]
- Adamu AA, Uthman OA, Gadanya MA, Cooper S, Wiysonge CS. Using the theoretical domains framework to explore reasons for missed opportunities for vaccination among children in Kano, Nigeria: a qualitative study in the pre-implementation phase of a collaborative quality improvement project. Expert Rev Vaccines 2019;18:847–57. [CrossRef]
- Tagbo BN, Eke CB, Omotowo BI, Onwuasigwe CN, Onyeka EB, Mildred UO. Vaccination Coverage and Its Determinants in Children Aged 11 - 23 Months in an Urban District of Nigeria. World J Vaccines 2014;04:175–83. [CrossRef]
- Ignis IO, Tomini S. Vaccination Coverage: Vaccine-Related Determinants & Anthropometric Measures in Children Resident in a Rural Community in Nigeria. Curr Drug Saf 2022;17:199–210. [CrossRef]
- Obi-Jeff C, Rakhshani NS, Bello-Malabu JI, Nwangwu C, Nwaononiwu E, Eboreime E, et al. Vaccine indicator and reminder band to improve demand for vaccination in Northern Nigeria: A qualitative evaluation of implementation outcomes. Vaccine 2020;38:4191–9.
- Murele B, Vaz R, Gasasira A, Mkanda P, Erbeto T, Okeibunor J. Vaccine perception among acceptors and non-acceptors in Sokoto State, Nigeria. Vaccine 2014;32:3323–7. [CrossRef]
- Olorunsaiye CZ, Degge H. Variations in the Uptake of Routine Immunization in Nigeria: Examining Determinants of Inequitable Access. Glob Health Commun 2016;2:19–29. [CrossRef]
- Cockcroft A, Usman MU, Nyamucherera OF, Emori H, Duke B, Umar NA, et al. Why children are not vaccinated against measles: a cross-sectional study in two Nigerian States. Arch Public Health 2014;72:48. [CrossRef]
- Musa A, Mkanda P, Manneh F, Korir C, Warigon C, Gali E, et al. Youth group engagement in noncompliant communities during supplemental immunization activities in Kaduna, Nigeria, in 2014. J Infect Dis 2016;213:S91–5.
- Galadima AN, Zulkefli NAM, Said SM, Ahmad N. Factors influencing childhood immunisation uptake in Africa: a systematic review. BMC Public Health 2021;21:1475. [CrossRef]
- Bangura JB, Xiao S, Qiu D, Ouyang F, Chen L. Barriers to childhood immunization in sub-Saharan Africa: A systematic review. BMC Public Health 2020;20:1108. [CrossRef]
- Nigeria: Making Reaching Every District Operational n.d.
- Amoah A, Issaka J, Ayebeng C, Okyere J. Influence of women empowerment on childhood (12–23 months) immunization coverage: Recent evidence from 17 sub-Saharan African countries. Trop Med Health 2023;51:63. [CrossRef]
- Kalaij AGI, Sugiyanto M, Ilham AF. Factors Associated With Vaccination Compliance in Southeast Asian Children: A Systematic Review. Asia Pac J Public Health 2021;33:479–88. [CrossRef]
- Anokye R, Acheampong E, Budu-Ainooson A, Edusei AK, Okyere P, Dogbe J, et al. Socio-demographic determinants of childhood immunization incompletion in Koforidua, Ghana. BMC Res Notes 2018;11:656. [CrossRef]
- Jalloh MF, Bennett SD, Alam D, Kouta P, Lourenço D, Alamgir M, et al. Rapid behavioral assessment of barriers and opportunities to improve vaccination coverage among displaced Rohingyas in Bangladesh, January 2018. Vaccine 2019;37:833–8. [CrossRef]
- Yahya M. Polio vaccines—“no thank you!” barriers to polio eradication in Northern Nigeria. Afr Aff 2007;106:185–204. [CrossRef]
- Raufu A. Polio vaccine plans may run into problems in Nigeria. BMJ 2003;327:380. [CrossRef]
- Larson HJ, Figueiredo A de, Xiahong Z, Schulz WS, Verger P, Johnston IG, et al. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. eBioMedicine 2016;12:295–301. [CrossRef]
- Demographic and Health Survey 2018 n.d.
- Ojo JS, Oyewole S, Aina F. Forces of Terror: Armed Banditry and Insecurity in North-west Nigeria. Democr Secur 2023;19:319–46. [CrossRef]
- Grundy J, Biggs B-A. The impact of conflict on immunisation coverage in 16 countries. Int J Health Policy Manag 2019;8:211.
Figure 1.
Selection of articles for inclusion.
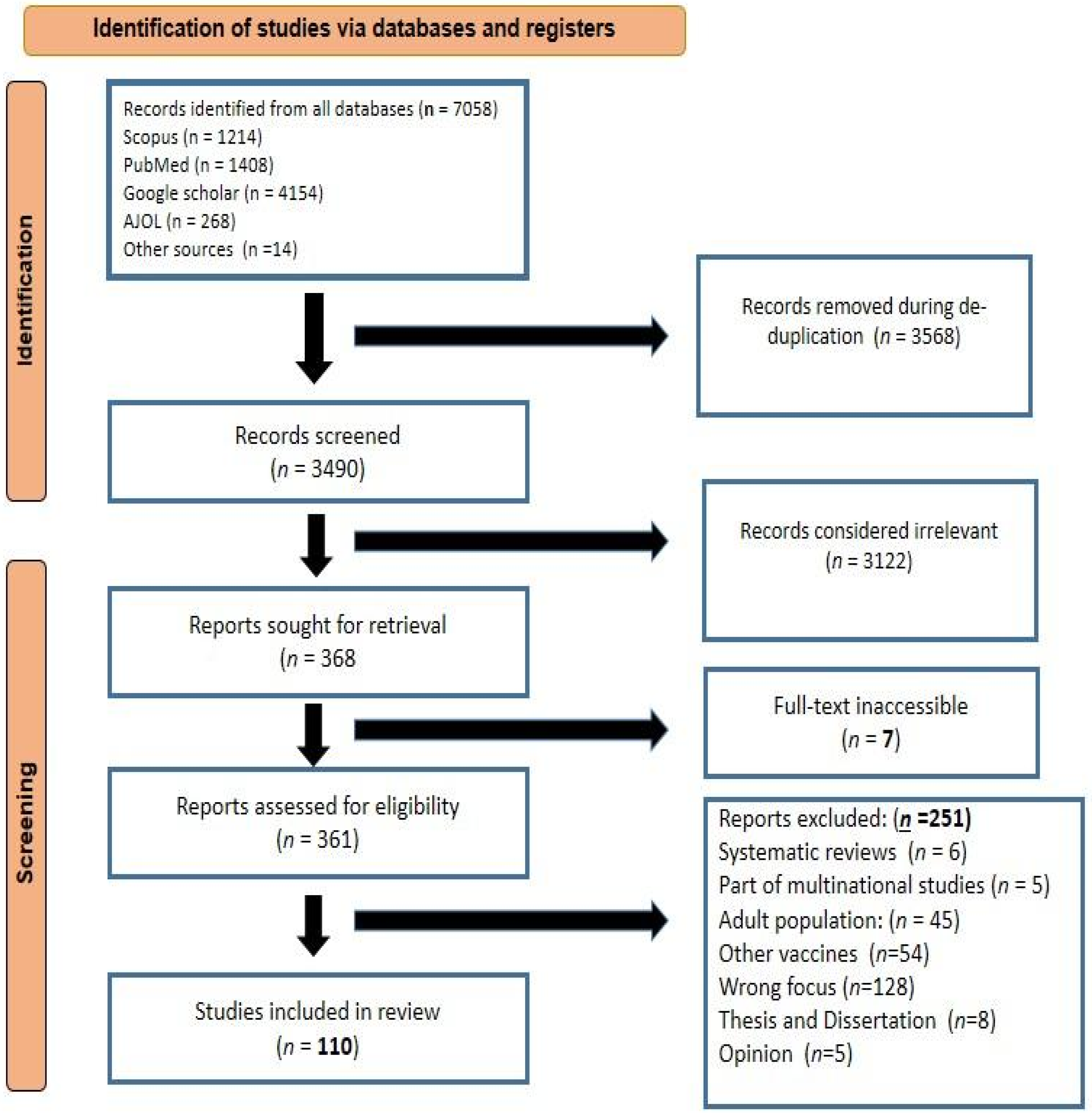
Figure 2.
Caregiver-related facilitators.
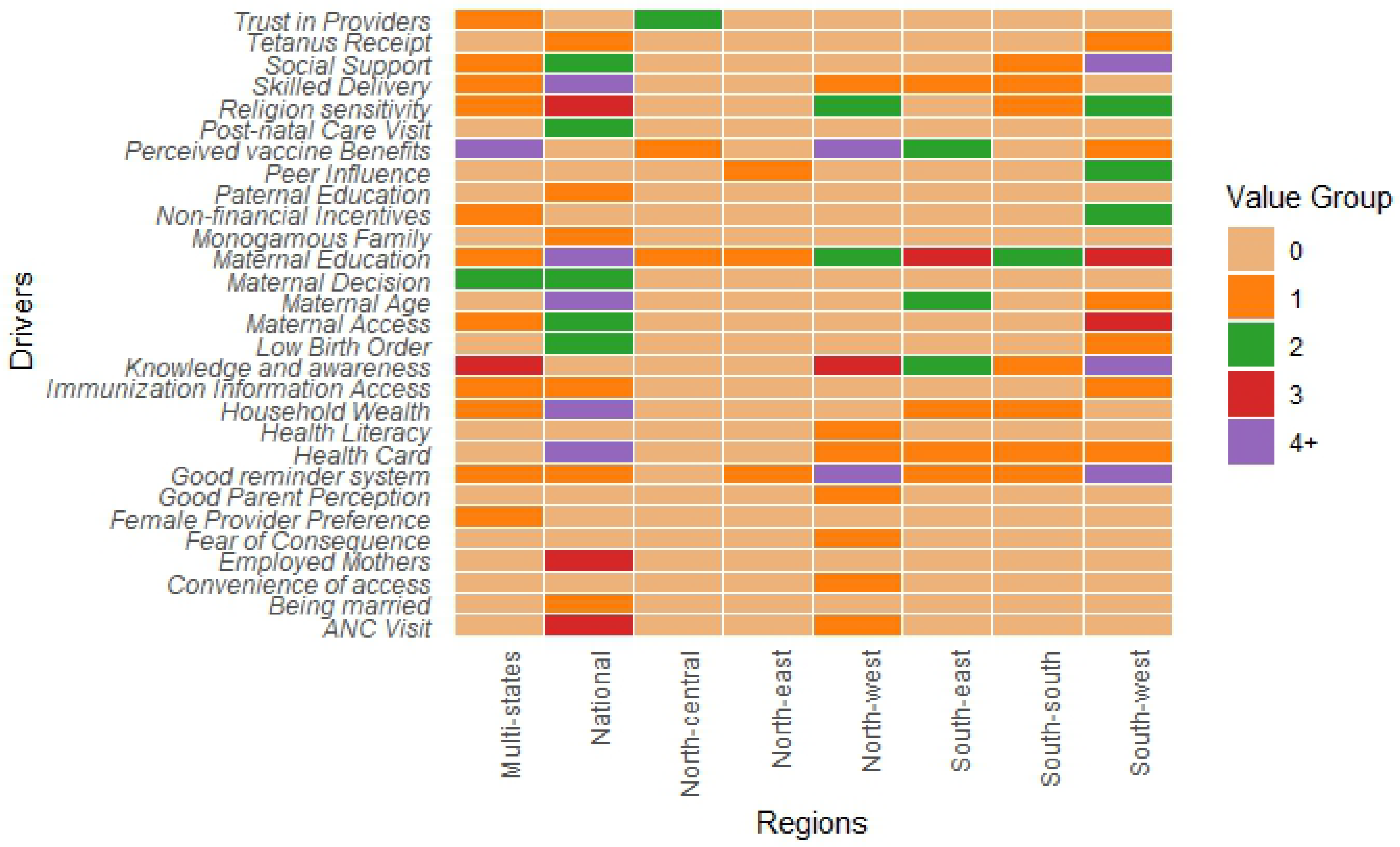
Figure 3.
Health system-related facilitators and barriers .
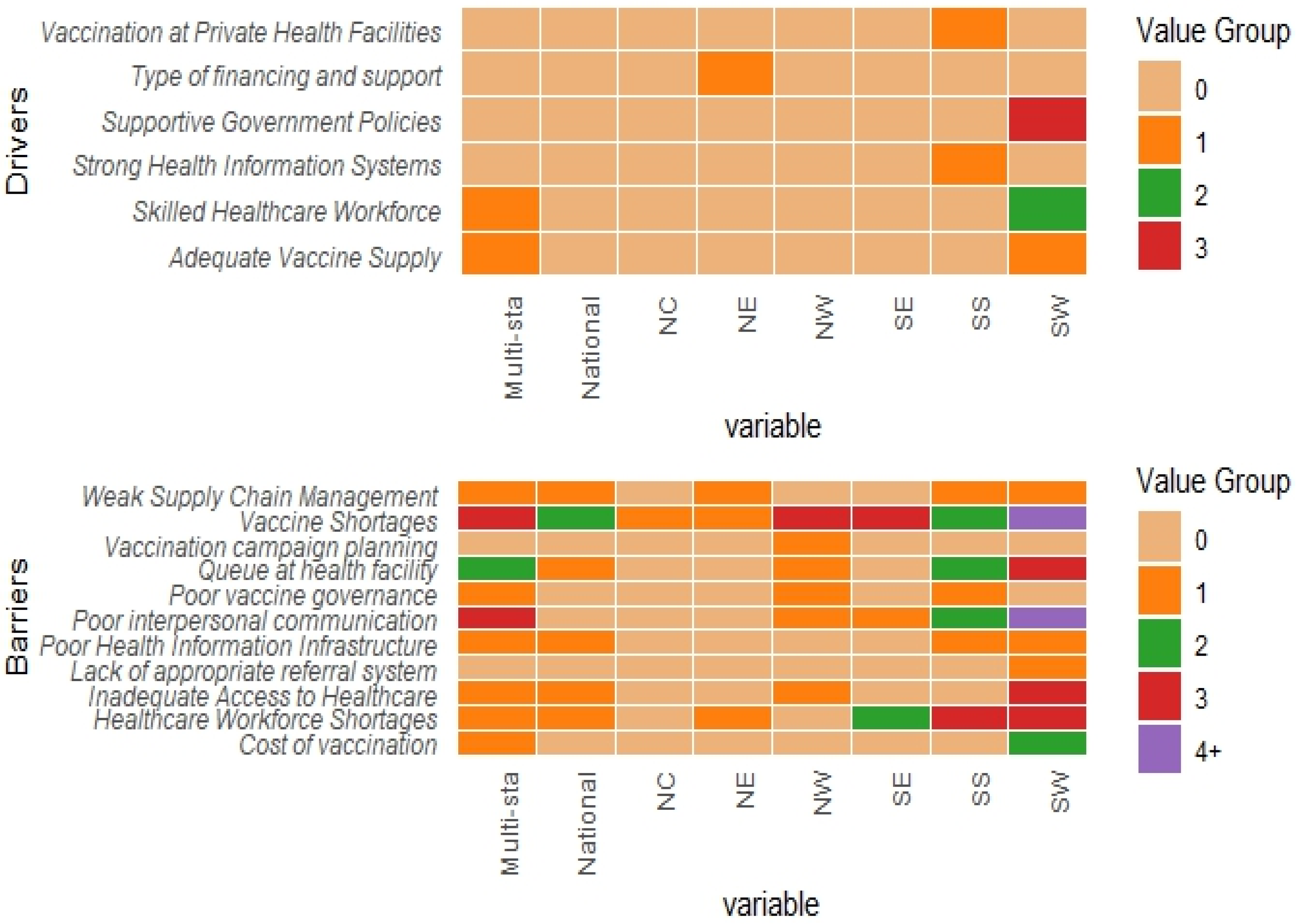
Figure 4.
Social/Community related facilitators and barriers .
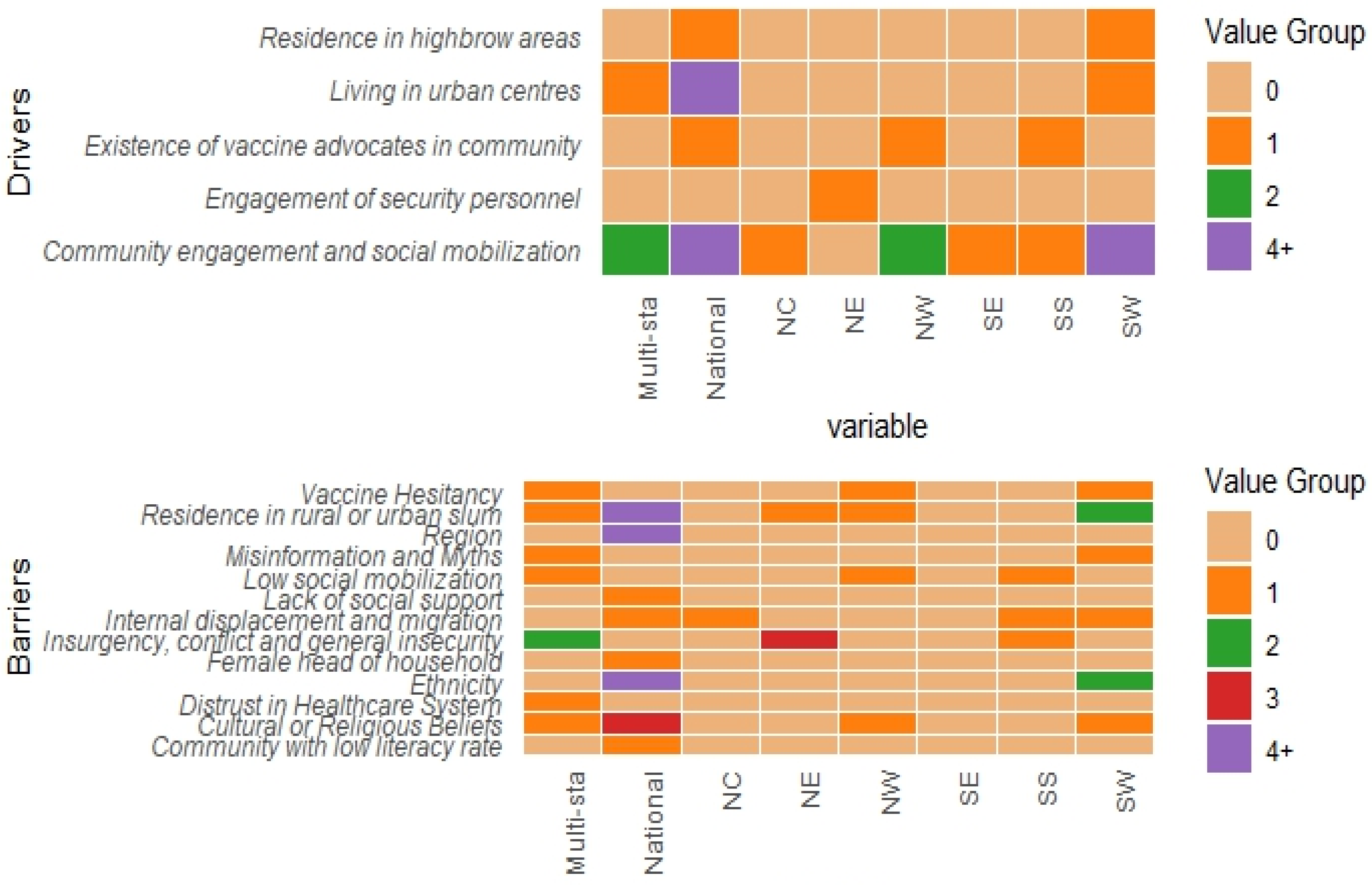
Figure 5.
Caregiver-related barriers.
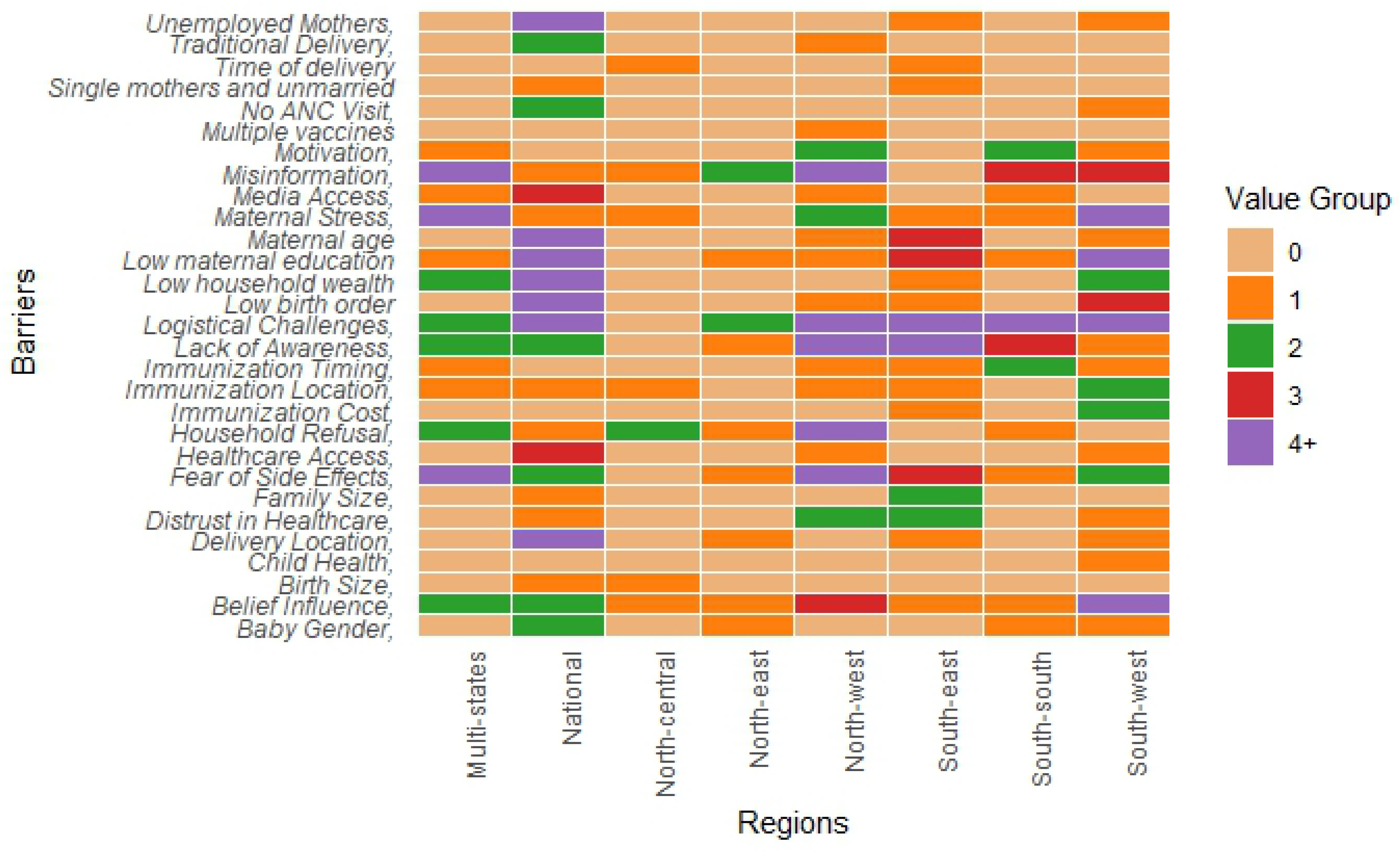

Table 1.
Summary of study selection criteria.
| Selection criteria | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Year of publication | All articles published from inception of the databases to 2023 | Articles published outside this period. |
| Type of publication | Peer review articles, grey literature and specific unpublished reports from stakeholders involved in vaccine administration and policy in Nigeria | Preprints, Thesis and dissertations and other publications that have not been peer reviewed. |
| Language | English | All other languages |
| Issue | Determinants of childhood vaccine uptake | Drivers and facilitators of COVID-19, influenza vaccines and other vaccines not included in the NPHDA routine immunization schedule as at October 2023 |
Table 2.
SPIDER framework for accessing studies.
| Sample | Under 2 children eligible for routine immunization in accordance to the NPHCDA recommendations, their caregivers including their parents and healthcare workers administering vaccine and providing necessary logistics and administrative responsibilities. |
| Phenomenon of interest | Routine vaccination recommended by the NPHCDA |
| Design | This includes primary studies employing exploratory, observational, or experimental study designs |
| Evaluation | Behaviours towards vaccination |
| Research type | This is mainly qualitative or mixed methods |
Table 3.
Characteristics of included studies.
| Characteristics | Number of studies (%), n=110 | References |
|---|---|---|
| Publication period | ||
| Before 1990 | 1 (0.9%) | [1] |
| Between 1990 and 2010 | 5 (4.5%) | [2,3,4,5,6] |
| After 2010 | 104 (94.5%) | [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109] |
| Geographical Regions | ||
| Multi-states | 11 (10.0 %) | [35,46,67,74,77,83,91,98,108] |
| National | 26 (23.6 %) | [2,5,15,19,20,22,26,34,40,41,42,46,50,56,59,60,65,71,75,76,78,84,88,90,94,107] |
| North-Central | 4 (3.6 %) | [13,61,62,97] |
| North-East | 9(8.2 %) | [16,34,54,58,86,92,93,95] |
| North-West | 17 (15.5 %) | [8,9,11,18,29,31,32,39,45,47,55,57,100,102,105,106,109] |
| South-East | 12 (10.9 %) | [10,25,28,63,64,68,69,70,89,103] |
| South-South | 10 (17.3 %) | [3,12,23,24,48,51,53,80,96,104] |
| South-West | 21 (19.1 %) | [1,4,6,7,14,17,27,30,33,37,38,43,44,49,52,72,73,82,87,99,101] |
| Research approach | ||
| Mixed Method | 44 (40.0 %) | [1,2,5,12,13,16,19,20,21,26,31,34,35,38,39,40,42,43,44,46,50,52,53,54,56,71,72,73,74,75,76,78,83,84,85,86,90,92,94,95,101,107,109] |
| Qualitative | 61 (55.5 %) | [1,3,4,6,7,8,9,10,14,15,17,18,22,23,24,25,27,28,29,30,32,33,34,35,37,41,45,46,47,48,49,51,55,57,58,60,61,62,63,64,65,67,68,69,70,77,80,81,82,87,89,91,92,93,96,97,98,99,100,102,103,104,105,106] |
| Quantitative | 5 (4.5 %) | [35,41,47,60,65] |
| Data collection methods | ||
| Combination of methods | 12 (10.9 %) | [9,35,43,73,74,83,101] |
| Analysis of secondary data | 33 (30.0 %) | [2,5,18,19,20,34,36,40,41,42,50,53,54,56,59,60,65,71,75,76,84,86,88,90,92,94,96,107,109,110,111] |
| Focus Groups | 7 (6.4 %) | [12,17,21,57,62,80,102] |
| Interviews | 18 (16.4 %) | [1,3,4,6,15,17,35,48,51,61,68,97,98,103,105,106,108] |
| Observation | 6 (5.5 %) | [14,22,27,37,58,91] |
| Questionnaire and household surveys | 34 (306 %) | [8,10,11,13,23,24,25,28,30,31,32,33,34,38,39,45,47,49,52,55,63,64,67,69,70,77,81,82,85,89,99,104] [87,100] |
| Vaccines assessed | ||
| Routine immunization | 89 (80.9 %) | [1,3,4,5,6,7,8,9,10,12,13,14,15,17,19,21,23,24,26,29,30,31,32,34,35,37,38,39,40,41,42,43,45,46,47,48,49,50,51,52,53,55,56,57,58,60,62,63,64,67,68,71,72,73,74,75,76,77,79,80,81,82,83,84,85,86,87,88,89,90,93,94,95,96,97,99,100,101,102,104,105,106,107,110,111] |
| Diphtheria, Tetanus, and Pertussis (DTaP) Vaccine | 2 (1.8 %) | [2,33] |
| Diphtheria, Tetanus, and Pertussis (DTaP) Vaccine; Polio Vaccine | 1 (0.9 %) | [33] |
| Hepatitis B Vaccine | 3 (2.7 %) | [16,69,70] |
| Measles, Mumps, and Rubella (MMR) Vaccine | 5 (4.5 %) | [28,61,92,108] |
| Polio Vaccine | 10 (9.1 %) | [11,20,22,54,65,91,98,103,109,112] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



