Submitted:
21 May 2024
Posted:
22 May 2024
You are already at the latest version
Abstract
Purpose: Data on Eosinophilic esophagitis in Israel is sparse. We appraised the clinical, endoscopic, and histological characteristics of 50 Israeli adults with EoE.
Methods: Medical records of 50 adult patients with established diagnoses of EoE who were referred to our center from 2020 until 2023 at Bnai Zion Medical Center, Haifa, Israel, were reviewed.
Results: Fifty patients with EoE were included, the mean age at diagnosis was 34±9.5 years. The sex ratio of males to females was approximately 2:1 with 34 males (68%) and 16 females (32%). Twenty-two of the 50 patients had a history of allergic diseases, Symptoms at diagnosis were as follows: Dysphagia was the primary presenting symptom observed (n=25, 50%), followed by food impaction (n=17, 34%) and GERD-like symptoms (n=14, 28%). Less frequent symptoms included vomiting, nausea, and chest pain. The most common endoscopic findings were normal mucosa (n=21, 42%) followed by Trachealization (n=17, 34%), esophagitis (n=7, 14%), and exudates (n=5, 10%). 66% of the subjects were initially treated with proton-pump inhibitors (PPIs). Nine patients (18%) were asymptomatic without any treatment. The remaining eight patients (16%) were given topical steroids. Clinical and histological resolution was detected in 50% of the patients who underwent a second EGD after 6–8 weeks of PPI.
Conclusion: Our current study depicts the clinical features of adult patients with EoE in north Israel. This is the first demographic study in Israel that defines the clinical, endoscopic, and histological manifestations of EoE in the adult population.
Keywords:
eosinophilic esophagitis
; esophagus
; proton pump inhibitors
1. Introduction
Eosinophilic esophagitis (EoE) is a chronic inflammatory disease of the esophagus which is characterized by esophageal dysfunction symptoms and eosinophilic infiltrate of the esophageal mucosa with more than 15 eosinophils per high power field (HPF) [1]. The incidence and prevalence of EoE have constantly raised over time, over the past two decades, EoE has become more diagnosed disease in the context of esophageal symptoms, mainly in western countries [2]. The pattern of the onset of the disease consist of two-stages; with a first occurrence in childhood, and a second peak in the third and fourth decade of life with an average age of 38 years [1,3]. Nowadays, it is considered the second most common cause of chronic esophagitis and dysphagia (after GERD which is the leading cause on the list) [4].
The exact pathogenesis of the disease is yet to be fully understood, however studies show that it consists of a combined interaction between genetic factors and environmental ones [5].
Presently, there are no studies that assess the clinical characteristics of EoE in Israel. We would like to share our data of 50 cases of adult subjects diagnosed with EoE in the last five years (February 2019 to February 2023) at our center in Haifa, north Israel.
2. Materials and Methods
2.1. Study Design and Subjects
We performed a retrospective study of patients evaluated from 2019 to 2023 by the Esophageal Gastrointestinal disease clinic at the Gastroenterology Department at Bnai Zion Medical Center in Haifa, Israel. Data were extrapolated from medical records of adult subjects with the diagnosis of Eosinophilic Esophagitis. Diagnosis of EoE was based on histopathology finding of more than 15 eosinophils per high power field (HPF) taken from esophageal biopsies. Fifty patients older than 18 years of age were found. In each subject; personal history of atopic background, symptomatic manifestations, endoscopic and histological findings were obtained.
2.2. Statistical Analysis
After collecting medical records, the data were analyzed to evaluate the spectrum of the disease fpr each patient, from clinical, endoscopic and initial treatment protocols. Data were stored in Microsoft Office Excel 2013 (Microsoft, Redmond, WA, USA), and the variables were calculated using SPSS program version 23 (IBM Co., Armonk, NY, USA).
3. Results
3.1. Clinical Characteristics
Fifty patients with EoE were included in the study, and the mean age at diagnosis was 34±9.5 years. The sex ratio of males to females was approximately 2:1 with 34 males (68%) and 16 females (32%).
Twenty two patients with EoE had a history of allergic diseases, including allergic rhinitis in 22% (n=11), atopic dermatitis in 6% (n=3), food allergy in 12% (n=6), and asthma in 12% (n=6).
Symptoms at diagnosis were as follows: Dysphagia was the prominent presenting symptom (n=25, 50%), followed by food impaction (n=17, 34%) and GERD like symptoms (n=14, 28%). Less frequent symptoms included vomiting, nausea, and chest pain. (Figure 1)
3.2. Endoscopic Findings
The main endoscopic finding were normal mucosa (n=21, 42%) followed by Trachealization (n=17, 34%), esophagitis (n=7, 14%), and white exudates (n=5, 10%). Furrows, crepe paper esophagus, and edema were found in one case each (Figure 2). Biopsies were taken from upper and lower esophagus, ranging from four to six biopsy pieces.
3.3. Initial Treatment
Thirty three patients (66%) were treated with proton-pump inhibitors (PPIs) at the time of diagnosis. About 50% of them had a clinical and histologic remission (Figure 3). Since the six-food elimination diet was not efficient enough in the adult population, it was not mostly chosen as a first line treatment option. Initially, nine patients (18%) were asymptomatic without any treatment. The other eight sujects (16%) were given topical steroids in the form of Budesonide oral gel (Budesonide 1 mg to be swallowed once a day, avoid food or drink for at least an hour after it) which was later on, since 2021, converted to Budesonide orodispersible tablets (Jorveza). None of the patients had treatment-related adverse even.
4. Discussion
Eosinophilic esophagitis is an emerging disease affecting both the pediatric and adult population. Israeli data on EoE is scarse, however, emerging reports on EoE from Israel postulate that it is not uncommon, probably underdiagnosed due lack of awareness. Worldwide, over the past years, it has become an increasingly diagnosed disease in the context of esophageal symptoms. There are various hypotheses that have tried to explain the increase in incidence. One of them is the increase in awareness of the disease, in addition to the increasing number in the volume of the Esophagogastroduodenoscopy (EGD) examinations that have been added in the last two decades [6,7,8], In spite the above, two studies have shown that both the prevalence and the cumulative incidence of EoE increased more than the rate of annual endoscopies during the observation period in accordance with a real increase in the prevalence and incidence of the disease [9,10].
In our demographic study, the sex difference was prominent with male to female ratio equals to 2:1, showing that males were more affected. This fact is familiar, since males are known to have a higher prevalence than females among both children and adults. In previous studies, the ratio between men and women ranged from 2.5:1 to 3:1 [11], comparable with our ratio. This gender risk is attributed to the hereditary differences between the sexes in the Cytokin receptor-like factor 2 gene which encodes for the Thymic Stromal Lymphopoietin receptor [12].
Clinical presentation relies on the patient’s self-report symptoms associated with esophageal dysfunction, and it can take a long time to reach a diagnosis of EoE. The most prominent presenting symptom was Dysphagia, followed by food impaction, GERD like symptoms and vomiting. This wide range may be explained by symptoms presenting as an acute onset, such as in the case of food bolus impaction, and at other times, the presentation might be more chronically and subtle.
Despite the fact that there is no pathognomonic endoscopic finding consistent with EoE, EGD is usually the first step procedure in the management of a patient with dysphagia for solids [13], there are endoscopic findings that are characterized with EoE, the most common of which are longitudinal furrows, white exudates, narrowings and strictures, Tracheization and rings, edema and crepe paper mucosa [14]. These findings can usually be present in a random combination in any given patient.
In our study, the most common endoscopic features were Normal mucosa (42%), Tracheization (34%), esophagitis (14%) and white exudates (10%). The normal mucosa appearance in most of the cases observed in our study accentuates the concern of regularly performing esophageal biopsies when performing EGD.
Since EoE is a chronic, progressive disease, the treatment also is a long-life treatment to prevent the complications of the disease and its main therapeutic goal controlling the symptoms and reducing the inflammatory process of the esophagus [15]. Nowadays, there are several different treatment options available for EoE: diet treatment, pharmacological treatment and finally, endoscopic dilatation. It should be noted that either diet or pharmacological treatment may serve as a primary treatment option as published in the therapeutic algorithm in the guidelines of the European Society of Gastroenterology UEG [16]. However, the choice should take into account the phenotype of the disease (inflammatory or fibrostenotic/obstructive), the patient's clinical background, preferences, side effects, and the physician's experience. Pharmacologic treatments currently usuable for EoE include PPIs, swallowed steroids and the very new biologic drug Dupilumab; a monoclonal antibody against IL4 and IL13, which is newly approved as second line treatment option in persistent patients [17]. We yet do not have any practical experience regarding prescribing this drug.
Nowadays, PPIs are the first-line treatment option usually offered to patients with EoE, as in our study, most of the patients received PPI as the initial treatment. The efficacy of PPIs in inducing remission appears to be related to two mechanisms: the first is by reducing acid reflux into the esophagus, leading to healing the mucosal barrier, which in turn prevents exposure to environmental allergens [18]. Additionally, they decrease the levels of Eotaxin-3, a pro-inflammatory cytokine produced by Th2 cells involved in recruiting Eosinophils to the esophageal mucosa [19].
PPI’s considered effective and safe, studies show clinical and histological remission in up to 50% of patients with EoE [20], and in everyday practice, they are one of the most common first line treatment options available, especially for the adult population in particular.
Corticosteroids are known for its anti-inflammatory effect and reduction of esophageal constriction and improving the integrity of the esophageal barrier with the outer lumen.
Topical viscous formulations and dispersible tablet formulations are considered optimal delivery methods. Budesonide gel injections (BUDESON GEL) was the first followed in the recent years by an orodispersible tablets of budesonide (JORVEZA), which currently represent a convenient and available option for local steroid treatment.
JORVEZA has been evaluated in multiple placebo-controlled trials and found out to be effective in inducing clinical and histological response when administered at an induction dose of 1 mg twice daily for 12 weeks [21]. Followed by an extension trial of 204 patients with EoE, a maintenance dose of 1 mg per day was administered also proved its effectiveness for 48 weeks in 75% of the subjects [22]. Despite these impressive results, in our study, PPIs were the most frequently prescribed first line treatment probably due to our lack of experience back then with the newly introduced Jorveza back then during the study period.
5. Conclusion
Our study describes the demographic characteristics of the adult population with EoE in north Israel. To the best of our knowledge, it is the first study in Israel that describes the clinical, endoscopic, and histological manifestations of EoE. Our population findings were comparable to those of other studies. Most patients in this study showed good clinical response to PPI treatment. A population-based, multi-center study with long-term follow-up is warranted to estimate the prevalence and incidence of EoE in Israel.
Informed Consent Statement
Patient has given informed consent for publication of images. No identifying information is included.
Conflicts of Interest
All authors report no conflict of interest.
References
- Liacouras, C.A.; Furuta, G.T.; Hirano, I.; Atkins, D.; Attwood, S.E.; Bonis, P.A.; Burks, A.W.; Chehade, M.; Collins, M.H.; Dellon, E.S.; et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J. Allergy Clin. Immunol. 2011, 128, 3–20.e6. [CrossRef]
- Dellon, E.S.; Hirano, I. Epidemiology and Natural History of Eosinophilic Esophagitis. Gastroenterology 2018, 154, 319–+. [CrossRef]
- Weiss, A.; Iorio, N.; Schey, R. Esophageal motility in eosinophilic esophagitis. 2015, 80, 205–213. [CrossRef]
- Arias, Á.; Perezmartinez, I.; Tenias, J.M.; Lucendo, A.J. Systematic review with meta-analysis: the incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Aliment. Pharmacol. Ther. 2016, 43, 3–15. [CrossRef]
- Alexander, E.S.; Martin, L.J.; Collins, M.H.; Kottyan, L.C.; Sucharew, H.; He, H.; Mukkada, V.A.; Succop, P.A.; Abonia, J.P.; Foote, H.; et al. Twin and family studies reveal strong environmental and weaker genetic cues explaining heritability of eosinophilic esophagitis. J. Allergy Clin. Immunol. 2014, 134, 1084–1092.e1. [CrossRef]
- Mahesh VN, Holloway RH, Nguyen NQ. Changing epidemiology offood bolus impaction: is eosinophilic esophagitis to blame? J. Gastroenterol. Hepatol.2013;28: 963–6.8.
- Dellon ES. Epidemiology of eosinophilic esophagitis.Gastroenterol.Clin. North Am.2014;43: 201–18.9.
- Ali MA, Lam-Himlin D, Voltaggio L. Eosinophilic esophagitis: aclinical, endoscopic, and histopathologic review.Gastrointest. Endosc.2012;76: 1224–37.
- Straumann A, Spichtin HP, Grize L, Bucher KA, Beglinger C, Simon HU. Natural history of primary eosinophilic esophagitis: a follow-up of30 adult patients for up to 11.5 years.Gastroenterology2003;125:1660–9.11.
- Giriens B, Yan P, Safroneeva E, Zwahlen M et al Escalating incidence of eosinophilic esophagitis in Canton of Vaud, Switzerland, 1993-2013: a population-based study. Allergy. 2015 Dec;70(12):1633-9.
- Lucendo, A.J.; Molina-Infante, J.; Arias, Á.; Von Arnim, U.; Bredenoord, A.J.; Bussmann, C.; Dias, J.A.; Bove, M.; González-Cervera, J.; Larsson, H.; et al. Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United Eur. Gastroenterol. J. 2017, 5, 335–358. [CrossRef]
- Davis, B.P. Pathophysiology of Eosinophilic Esophagitis. Clin. Rev. Allergy Immunol. 2018, 55, 19–42. [CrossRef]
- Varadarajulu S, Eloubeidi MA, Patel RS et al (2005) The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc 61:804–808.
- Remedios M, Campbell C, Jones DM, Kerlin P (2006) Eosinophilic esophagitis in adults: clinical, endoscopic, histologic findings, and response to treatment with fluticasone propionate. Gastrointest Endosc 63:3–12.
- Dellon ES, Liacouras CA, Molina-Infante J, Furuta GT. Et al Updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis: Proceedings of the AGREE Conference. Gastroenterology. 2018 Oct;155(4):1022-1033.e10.
- Lucendo, AJ, Molina-Infante, J, Arias, A, et al Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J 2017; 5: 335–358.
- Dellon ES, Rothenberg ME, Collins MH, et al Dupilumab in Adults and Adolescents with Eosinophilic Esophagitis. N Engl J Med. 2022 Dec 22;387(25):2317-2330.
- Van Rhijn, BD, Weijenborg, PW, Verheij, J, et al Proton pump inhibitors partially restore mucosal integrity in patients with proton pump inhibitor-responsive esophageal eosinophilia but not eosinophilic esophagitis. Clin Gastroenterol Hepatol 2014; 12: 1815–1823.e2.
- Cheng, E, Zhang, X, Huo, X, et al Omeprazole blocks eotaxin-3 expression by oesophageal squamous cells from patients with eosinophilic oesophagitis and GORD. Gut 2013; 62: 824–832.
- Laserna-Mendieta, EJ, Casabona, S, Savarino, E, et al Efficacy of therapy for eosinophilic esophagitis in real-world practice. Clin Gastroenterol Hepatol 2020; 18: 2903-2911.e4.
- Lucendo, A.J.; Miehlke, S.; Schlag, C.; Vieth, M.; von Arnim, U.; Molina-Infante, J.; Hartmann, D.; Bredenoord, A.J.; de Los Rios, C.C.; Schubert, S.; et al. Efficacy of Budesonide Orodispersible Tablets as Induction Therapy for Eosinophilic Esophagitis in a Randomized Placebo-Controlled Trial. Gastroenterology 2019, 157, 74–86.e15. [CrossRef]
- Straumann, A.; Lucendo, A.J.; Miehlke, S.; Vieth, M.; Schlag, C.; Biedermann, L.; Vaquero, C.S.; de Los Rios, C.C.; Schmoecker, C.; Madisch, A.; et al. Budesonide Orodispersible Tablets Maintain Remission in a Randomized, Placebo-Controlled Trial of Patients With Eosinophilic Esophagitis. Gastroenterology 2020, 159, 1672–1685.e5. [CrossRef]
Figure 1.
Presenting symptoms distribution of patients with EoE; Dysphagia is the most common presenting symptom affecting 50% of the patients, followed by food impaction, GERD like symptoms and vomiting.
Figure 1.
Presenting symptoms distribution of patients with EoE; Dysphagia is the most common presenting symptom affecting 50% of the patients, followed by food impaction, GERD like symptoms and vomiting.
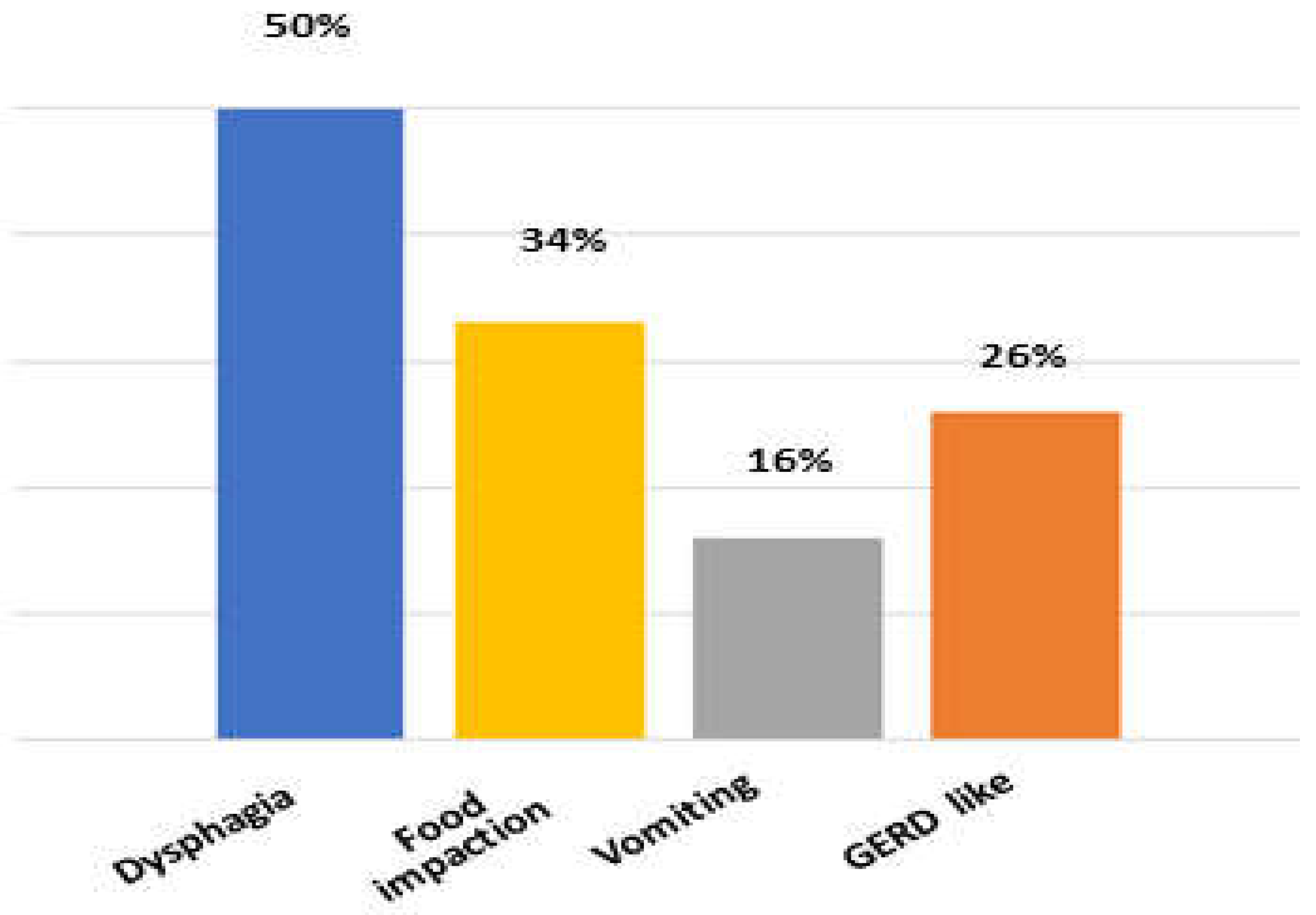
Figure 2.
Pie chart display of endoscopic findings at presentation of patients with EoE., Normal appearance mucosa was observed in 42% of the patients, followed by Trachealization, Esophagitis and white exudates.
Figure 2.
Pie chart display of endoscopic findings at presentation of patients with EoE., Normal appearance mucosa was observed in 42% of the patients, followed by Trachealization, Esophagitis and white exudates.
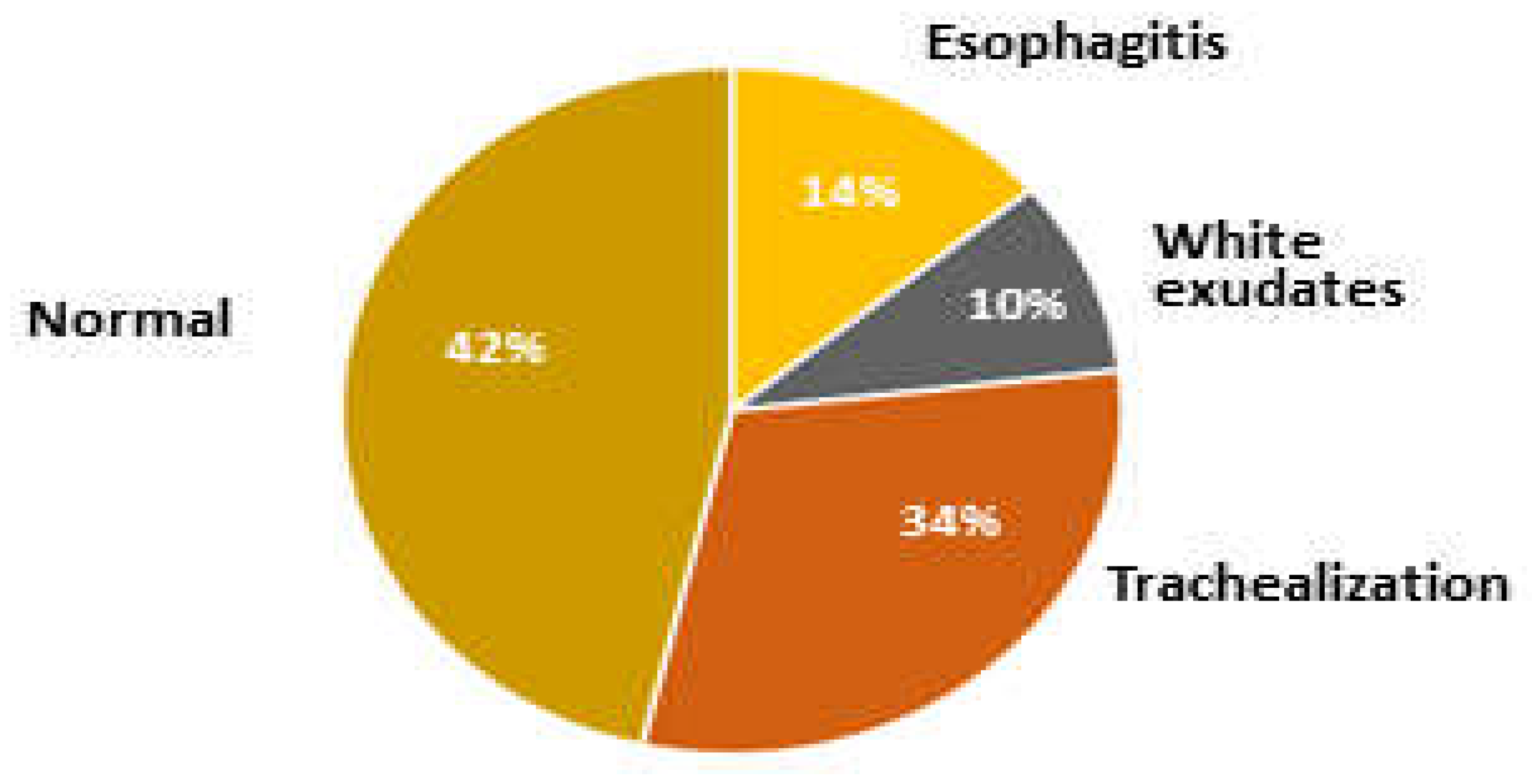
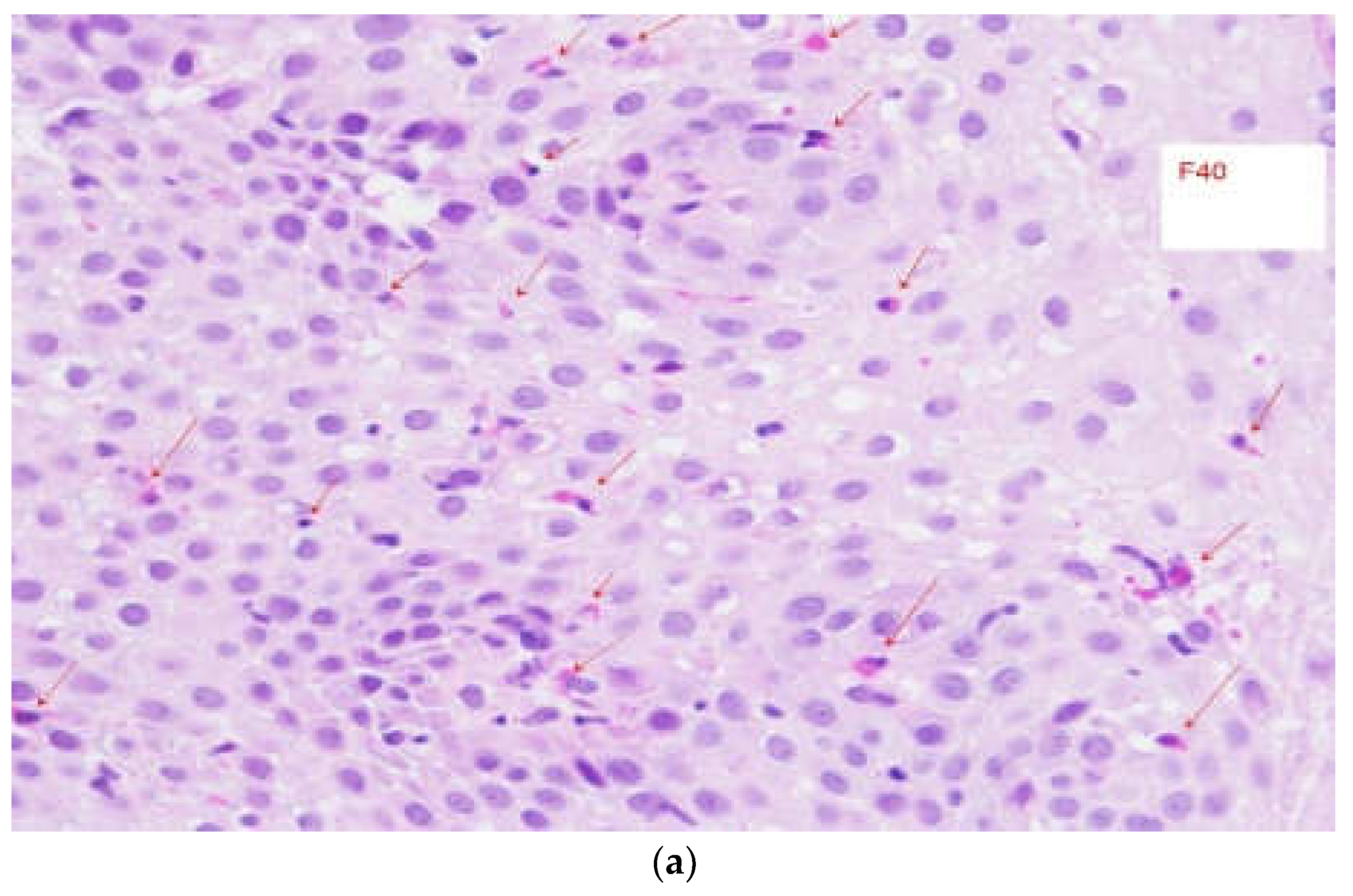
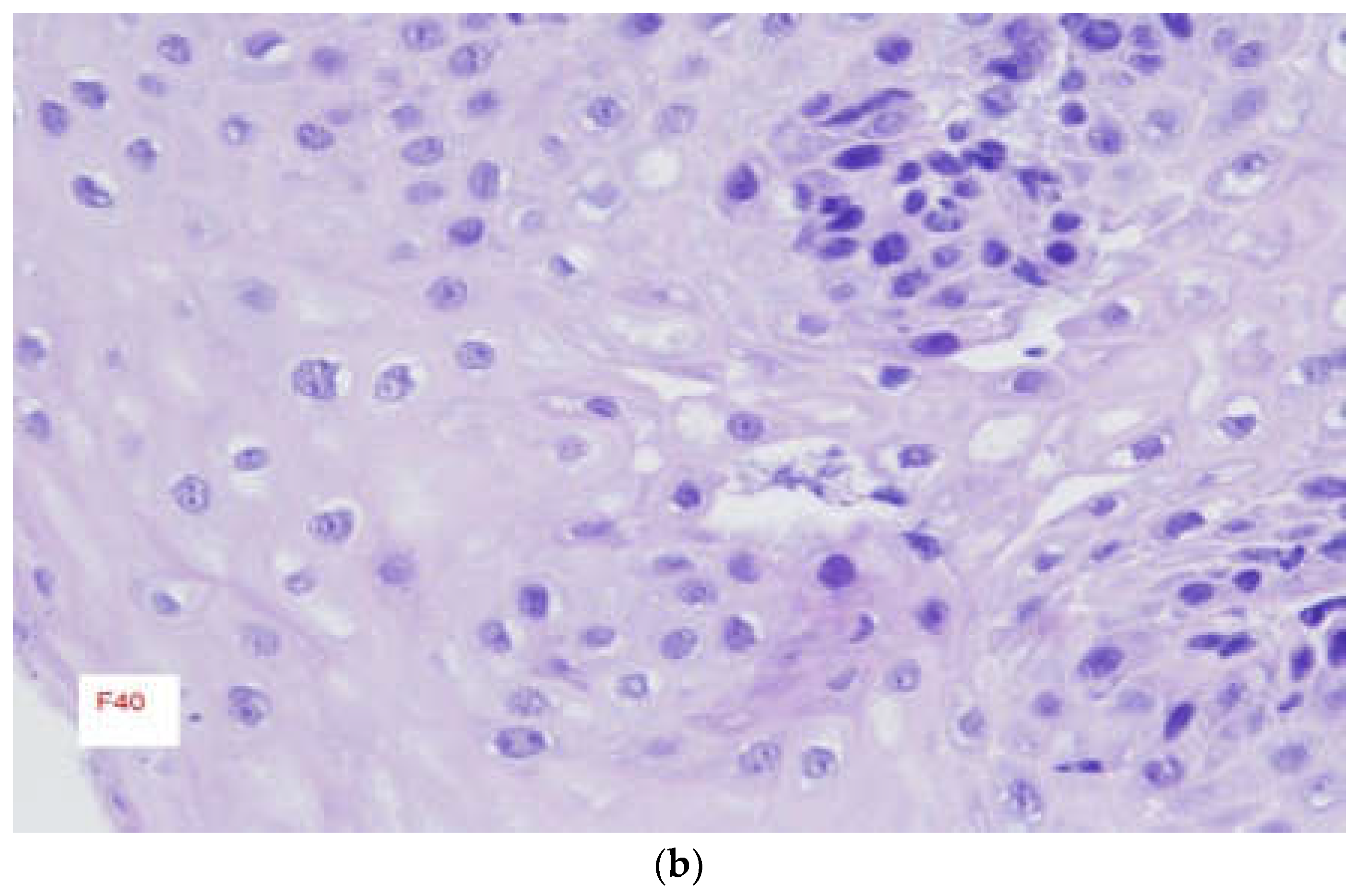
Figure 3.
Microscopic slides of esophageal biopsies with H&E stain of patient treated with Esomeprazol; Slide before treatment with PPI showing infiltration of numerous Eosinophils throughout the mucosa (red arrows) at magnification level of X40 (Figure 3a), another Slide after treatment of PPI for 12 weeks showing no Eosinophils throughout the mucosa at magnification level of X40 (Figure 3b).
Figure 3.
Microscopic slides of esophageal biopsies with H&E stain of patient treated with Esomeprazol; Slide before treatment with PPI showing infiltration of numerous Eosinophils throughout the mucosa (red arrows) at magnification level of X40 (Figure 3a), another Slide after treatment of PPI for 12 weeks showing no Eosinophils throughout the mucosa at magnification level of X40 (Figure 3b).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



