Submitted:
23 May 2024
Posted:
24 May 2024
You are already at the latest version
Abstract
Background: Alzheimer's Disease (AD) is a progressive and incurable condition that prompts the exploration of interventions to slow its advancement and enhance the quality of life. The cortical brain waves could have a role in the process of executive function deterioration, increasing dementia symptoms. Objective: To interrogate the effects of physical exercise, and non-invasive brain stimulation, both in electrophysiological behavior of the brain, the executive functions, and dementia symptoms in older adults with AD. Methods: One hundred and sixteen older adults were grouped (n=22 each): GAE (AD, PMED+NIBS), GCP (AD, PMED), GCN (AD, NIBS), GCS (control, no intervention). Binaural beats were used as a non-invasive brain stimulation, physical exercise, or both, were applied during 16 weeks. Pre/post measurements included Alpha Band, and SMR Rhythms, executive functions, and dementia symptoms. Results: GCS showed no significant changes (p>0.05). GCN and GCS slightly enhanced inhibitory control (p>0.05) and working memory (p>0.05). In contrast, GCP and GAE improved executive function (p
Keywords:
Short-term memory
; Electroencephalography
; Executive Function
; Alzheimer’s disease
; Brain Ageing
; Working Memory
1. Introduction
No human brain disorder has received more attention in recent years than Alzheimer's disease (AD) [1]. Several neurobiological effects occur in the context of brain sensory and psychiatric disorders [2]. AD shows a very high prevalence of degenerative and progressive dementia [3], which is projected to increase four-fold by 2050 [4]. Neurodegeneration is often associated with cognitive problems, the most common of which are learning, cognition, and memory problems [5]. Often, cognitive dysfunction such as working memory dysfunction is the main behavioral symptom in older adults [6], and there is a lack of cures as only palliative measures and medications are used in most cases, suggesting an urgent need an alternative.
The pathophysiology of the disease is characterized by a reduction in cerebral cortex choline acetyltransferase, a number of neurotransmitters and neuromodulators, their synthetizing enzymes and the neuronal morphology that produces them [1]. Reduced production of brain-derived neurotrophic factor (BDNF), and increased production of phosphorylated TAU protein (p-TAU) together the beta Amyloid modifications (β-Amy) are the most prominent neural features of AD [7,8]. Biologically, neuron/axon death in AD is due to hyperphosphorylation of TAU protein [9]. Several manuscripts have shown that exercise attenuates TAU pathogenesis in a mouse model of Alzheimer's disease-like tau pathology [10]. TAU protein is often overexpressed in neurodegenerative diseases, including Alzheimer's disease [11] and used as a marker of severity [12], however, the biochemical parameters is not the central point of this manuscript.
Another important key of the brain function is his electrophysiological behavior [13]. In this sense different brain waves have important relationships with many brain functions as the Alpha band with the cognition [13], and the sensorimotor rhythm (SMR) with the motricity [14]. Due to this, the investigation of the brain wave behavior could be crucial to explain in part the effect of many actions against the degenerative effects of the AD.
However, data suggest that physical activity is one of the few effective interventions for neurodegenerative diseases and other cognition- and memory-related problems, including AD [15], and data suggest that physical activity is one of the few effective interventions for neurodegenerative diseases and other cognition- and memory-related problems, including AD. In addition, many studies reported that physical activity can counteract the neurobiological effects of Alzheimer's disease. For example, reduced functional decline in the hippocampus [16], and improved mitochondrial health in the brain [17], both associated with improvements in many functional aspects of the brain as his electrophysiology, astrocyte remodeling in the long-term exercise exposition [18], and, specifically our manuscript, evidence for beneficial neuroplastic effects is both related to morphological aspects of the cortex [19]. Nonetheless, obtained important cognitive benefits from resistance training, justifying the use of this type of exercise in our study [19].
Noninvasive brain stimulation (NIBS) is another form of cognitive therapy that has received attention recently [20,21]. This approach has shown promise in the treatment of AD and Parkinson's disease [22], other types of mental disorders [23], and a variety of problems associated with memory and cognition [24]. Although studies examining the effects of resistance training (PMED) and even NIBS have shown some efficacy in AD, the results of combining PMED and NIBS as an intervention in the treatment of AD have not been evaluated [20,21].
Since the independent application of either NIBS or physical exercise has revealed positive results in memory-related, cognitive, and mental illness treatment [25], the likelihood of these methods being more effective if applied in combination is relatively high, therefore, the main objective is to exam the effects of physical exercise, non-invasive brain stimulation, both in electrophysiological behavior of the brain, the executive functions, dementia symptoms.
2. Methods
2.1. Participants
The universe of recruiting was composed by 1096 elderly patients with Alzheimer's and Parkinson's from the Vila Vicentina Community Center (CTIV), the Elderly Support Center of the University of Pará (UEPA), the Senior Living Center (CCI) and SESC Porto Velho, Brazil. Syndrome and other psychiatric diseases, only one hundred and sixteen elderly patients met all the inclusion and exclusion criteria for participation in this study.
Diagnosis of dementia is made over a period of weeks by a multidisciplinary team consisting of a general practitioner, a psychiatrist, a psychologist and a nurse in all living national neuro communication parameters The National Institute for Disability Research (NINCDS) Recruitment Center works until completion of the Participation Diagnosis. About this study, the Mini-Mental State Examination (MMSE) [26,27] was used for an objective measurement before and after the intervention program.
2.2. Procedures for Inclusion and Exclusion
Nurses trained in caring for patients with mental illness and other types of exacerbating illnesses referred older patients to the study. The diagnosis of AD follows the NINCDS [28]. This diagnosis was made by the medical or human services department of the Brazilian health system. Furthermore, previously used questionnaires confirmed the identity of these elderly patients and highlighted the characteristics of their dementia symptoms.
To be included in this study of Alzheimer's patients, subjects had to score 9 to 10 on the Edmonton Frailty Scale (EFS) [27,29]. In addition, all study participants were between the ages of 65 and 80, had an MMSE score of 11 or higher, participated substantially in an exercise program, and had physician clearance to participate in program intervention level exercise.
Volunteers were not eligible if they had depression or a clinically acceptable diagnosis of severe sensory deficits or neurologic disease syndromes. Patients who are unable to complete the research tasks due to physical limitations, patients who cannot recognize the content of the research tasks, patients who do not understand their participation in the research, and patients who do not agree to sign the informed consent form are considered unqualified. After the selection process was complete, 116 older adults [29], all with AD constituted the final sample and were randomized into four groups (n= 29 each). The first group was named as the experimental group, AD (GAE) received PMED plus NIBS, AD received only PMED (GCP) positive control, AD received only NIBS (GCN) positive control, and sedentary negative control (GCS) did not intervene. It must be said that all laboratory and statistical procedures were blinded.
Then, after the raw data is collected and sent for statistical processing, field researchers are no longer exposed to the data, so they cannot see the results from an individual or global perspective. This ensures that they do not know individual or collective results until they are statistically processed. An independent statistician was commissioned to process the data. This procedure was chosen to avoid bias and to provide a high level of confidence in the results.
2.3. Sample Characteristics
Population demographic profiles were defined using the following variables: (1) baseline mental state (MMSE), (2) gender, (3) age, (4) income, (5) social income, (6) marital status, (7th) education and (8) time to take medication for illness. Overall, distributions were similar between the three groups for almost the entire population profile. As there were no significant differences among most of these variables, statistical checks for normality of distribution were performed only between age and baseline mental status, the only variables showing significant differences between groups. For this review, the Mann-Whitney test was adjusted for p ≤ 0.05. Table 1 shows the descriptive characteristics of the study participants and the means of all measures, including age, MMSE and between-group comparisons.
2.4. Non-Invasive Brain Stimulation Protocol (NIBS)
The auditory signal synthesizer delivered stimuli at a frequency of 8-12 hertz (Hz) in a binaural firing configuration. The modulator instrument is an Orion brand manufactured by Touch Technology® (Toronto, Canada). The system works by providing brainwave modulation, thereby promoting better attention and increased capacity for mental processing [21,44]. Each step of stimulation lasted 20 minutes, and the stimulation was repeated 3 times a week throughout the ten-week intervention period, for a total of 30 sessions.
2.5. Physical Exercise Protocols (PMED)
The entire program consists of 60 minutes per class, of which 40 minutes are dedicated to physical activity, divided into 5 minutes warm-up, 30 minutes core physics and 5 minutes technical cool down. Participants start in a sitting position and then have to move to different standing positions and vice versa. The core part of the PMED program, followed by a warm-up session, includes exercises for lower body, abdominal, upper body strength and resistance, balance, and overall motor coordination; Intensity plays out in circles. To this extent, if any of the subjects felt tired or uncomfortable, they could stop and rest. While the exercise is self-regulating, all the exercise stimulation is designed to wear yourself out. If the subject required rest, we assumed the exercise was at the highest intensity level, thus allowing us to assume that the exercise program was progressive and characterized by high intensity.
Finally, the relaxation part involves practicing breathing exercises and internalizing the mind, such as those suggested by Eastern techniques such as tai chi or yoga. Resistance training was performed at up to 70% intensity, and muscle strength was determined by a hypothetical repetition-maximum protocol from the American College of Sports Medicine (ACSM) [45], followed by a simple percentage calculation. In summary, for the stress test, all selected exercises were performed at standard intensity until concentric failure. New loads were then performed until the subject reached concentric failure at 20 repetitions. Then set the exercise to 12 repetitions. Strength is recalculated every two weeks using this same method. The equation is: [20 reps at standard load * (percent work) = reps]. All intervention program was performed during 16 weeks.
The exercise intensity was controlled by the maximum heart rate reached in the end of each fourth exercise set of on-by-one exercise during the exercise session every in the Friday. The assessment was done across the Finger Oximeter G-Tech. The exercise intensity was corrected even when necessary to keep ~70% of the maximum heart rate. Additionally, the evolution in the charge was recorded. Finally, the blood lactate was acquired in the same moment that the heart rate frequency in the counter lateral finger and measured using the Accu Check Lactometer.
2.6. Cognitive and Dementia Symptoms Assessments
2.6.1. Memory
2.6.1.1. Digit Span
The Digit Span Test (DST) [30] involves testing short-term memory by verifying working memory operations. The test addresses the functional aspects of memory based on a person's ability to repeat a series of items (which can be letters, numbers, or words) in the correct order to assess the person's memory. The test features memorizing a series of numbers and/or words, with the sequence increasing in length with each correct answer. The DST application is reliable, well-validated, and cross-validated [31], showing that it is one of the most applicable tests for examining working memory function.
2.6.1.2. Short Term Memory Part of the Montreal Cognitive Assessment (MoCA)
The MoCA consists of one page, covering the cognitive domains of executive function and visuospatial abilities, naming, short-term memory, attention and working memory, language, concentration, verbal abstraction, and orientation. It can be carried out within 10 minutes, with a maximum score of 30 indicating no errors were made. Here, only the fifth domain of this cognitive scale, the Short-Term Memory. The Short-Term Memory Part of the Montreal Cognitive Assessment is calculated by adding the number of words remembered in free delayed recall, category-cued recall, and multiple choice–cued recall multiplied by 3, 2 and 1, respectively, with a score ranging from 0 to 15. The examiner administers a memory test by reading a list of 5 words at a rate of one per second.
Additionally, the sessions in regards the assessment of the memory of the Literacy Independent Cognitive Assessment (LICA) and the Mini Mental State Exam were used.
2.6.2. Inhibitory Control
2.6.2.1. Simple and Complex Reaction Time
The stimulus was presented in the same size of the hand and was called as “Simple Reaction Time (SRT). However, in the second, the stimulus was presented in counter lateral side of the domain hand, producing an interference in the answer and called as “Complex Reaction Time (CRP). We performed five executions for acclimatization and more 50 for assessment.
2.6.2.2. Stroop Test
For the third cognitive assessment, the inhibitory control assessment, part of the Stroop test was adapted to a two-choice motor reaction time task format previously used by our group [33,34]. For this assessment, subjects had to press a computer button as soon as a light (stimulus) appeared on either side of the computer screen. Final averages were calculated for five of each part of the 30 trials. There is scientific evidence that reaction time is an important component of human functioning and mental health, especially in older adults [35,36]. Furthermore, several studies analyzing this factor have shown that older adults can significantly improve their responses to such tests through regular practice [37,38,39,40]. Additionally, an electronic reaction time test was used in two versions. First, the simple reaction time, with the computer-gaming reaction test designed to evaluate the reaction time to frontal visual stimuli. The testing was carried out with dominant hands, five executions for acclimatization and more 50 for assessment. The instructions were, when the red box turns green, click as quickly as you can.
2.6.3. Mental Flexibility
2.6.3.1. Trail Making Test to Assess the Mental Flexibility
The Trail Making Test consists of two parts, each with 25 circles spread across a sheet of paper. In Part A, the circles are numbered from 1 to 25, and the individual is tasked with connecting them sequentially. Part B includes both numbers (1 to 13) and letters (A to L), requiring the participant to connect them alternately in an ascending pattern (e.g., 1-A-2-B-3-C). The goal is to complete the trails as quickly as possible without lifting the pen or pencil. Errors are noted and corrected immediately, with correction time factored into the overall completion time. If both parts are not completed within five minutes, the test is discontinued. The procedure involves providing the patient with the test sheet and a writing implement, demonstrating the task, timing the completion of both parts, and recording the results. Scores are reported in seconds, with higher scores indicating greater impairment.
2.7. Cognitive Screening and Dementia Symptoms
2.7.1. Mini Mental State Exam (M.M.S.E.)
The MMSE has been validated in Brazil and its content is divided into seven categories. Each category is designed to assess a specific cognitive function, with scores ranging from 0 to 30; higher scores indicate better cognitive function. Considering the influence of educational factors, values of 18 (average educational level) and 26 (high educational level) are generally defined as critical values [21,32].
2.7.2. Montreal Cognitive Assessment (MoCA)
The MoCA consists of one page, covering the cognitive domains of executive function and visuospatial abilities, naming, short-term memory, attention and working memory, language, concentration, verbal abstraction, and orientation. It can be carried out within 10 minutes, with a maximum score of 30 indicating no errors were made. Scores were corrected for low education according to instructions, by adding one point to the total score of patients with 12 years of education or less. The original suggested cutoff for the diagnosis of CI was a score of (below) 26 (less than 26).
2.7.3. Literacy Independent Cognitive Assessment (LICA)
The LICA in its finalized form presents a 300-point examination, comprising 13 distinct assessments targeting memory, visuospatial acuity, executive function, attention, linguistic prowess, and computational skills. The narrative recall segment entails immediate recollection, delayed retrieval approximately 20 minutes later, and subsequent recognition. Meanwhile, the word recall segment incorporates three successive learning trials featuring ten nouns each, followed by immediate recall, a recall trial after a 20-minute interval, and recognition. Assessing visuospatial prowess and memory involves replicating and identifying ten stick formation images, derived from adaptations of the Stick Pattern Reversal Test. Evaluation of executive functions encompasses the Digit Stroop test and a task gauging fluency in animal naming. Attention, concentration, and working memory are scrutinized through forward and backward repetition tapping exercises involving nine Corsi blocks. Modifications to the arrangement of the blocks on the board and the tapping sequences were made in line with adjustments to Corsi's original block-tapping paradigm. Language assessment entails a fifteen-item confrontation naming challenge encompassing animals, fruits, and vegetables, alongside the previously mentioned fluency task. The Color and Object Recognition Test (CORT) underwent alterations derived from semantic comprehension assessments concerning the visual morphology and hues of various objects. Lastly, computational aptitude is subject to evaluation.
2.8. Brain Wave Patterns Assessment
The assessment of the brain's electrical activity is performed using an EEG, which records activity at specific points in the brain's cortex in real time. The EEG used was produced by Neurotec do Brazil® model Neuromap EQSA260 (São Paulo, Brazil). All cranial points evaluated were selected according to the international system recommended by the Brazilian Neurophysiological Society [41]. The instrument's terminals are secured in such a way that it is grounded to avoid any type of electrical interference during data collection (DA Silva et al, 2016).
The focus here is on alpha-band assessment of the frontal cortex and verification of SMR rhythms in sensorimotor areas. This is due to the relationship between alpha bands on frontal lobe structures recorded primarily by C3 and C4 electrodes and cognition according to Jasper's International System 10-20 [41]. A major interest related to SMR rhythm is the function of this specific region.
Data were processed using Brain Vision Analyzer Software® (version 2.0, Brain Products, Gilching, Germany). First, the data is down sampled to 250 Hz. ECG pulse artifacts were measured using Allen et al. [42]. In a nutshell, intervals are automatically scored based on repeating patterns, intervals are calculated, and their average is subtracted. After the ECG risk model was created, the ECG trace data was removed. Filter the data using high-pass and low-pass filters (0.5 to 70 Hz each) and apply a notch filter at 50 Hz. Using visual data leakage removes possible interference in the channel and any interpolation of such interference to the eye, which is often identified as a target for finding data distortions. Re-reference the EEG signal to a standard reference point by the arithmetic mean of the electrophysiological activity at the peak power of F3, F4, C4, and CZ. Extraction is performed using a sophisticated demodulation technique that correlates to EEG temporal traces in the full alpha band (8-12 Hz), lower (8-10 Hz) and upper (10-12 Hz). Data were extracted individually and exported to MATLAB® (Mathworks, Sherborn, MA, USA) to build statistical models. These programs were previously published by Brueggen et al., [43].
2.9. Study Type and Research Ethics
The study is clinical, randomized, experimental in nature and underwent an ethical assessment by Platform Brazil according to the National Health Council decision CNS 466/12 for approval according to the CAAE Helsinki without declaration. Registration number 2066823 was issued thereafter. In accordance with the ethical principles similar to the law, all volunteers and their legal representatives signed a free informed consent form before participating in this study as volunteers after eliminating their doubts about this study.
2.10. Statistical Procedures
Before recruiting participants, sample size and power calculations were performed based on changes in working memory performance significance and dementia symptoms among the four groups most critical to the null hypothesis. The distribution does not follow a common standard deviation (p>0.05). A sample size of 14 subjects per group was required to obtain at least 80% power to detect mean differences between groups. The actual performance is 91.3%. The method of power calculation was previously described [46].
Statistical analysis followed three distinct phases. First, we used the Kolmogorov-Smirnov test (Dallal-Wilkinson-Lille value of p) to determine data normality, which turned out to be parametric (p> 0.05). Data are descriptively plotted against the mean and standard deviation of the scores. Second, after ascertaining the normality of the data distribution, according to the results obtained in the preliminary results received by older people, the Kruskal-Walli’s test with DUNN's post hoc or the Two Way ANOVA with Tukey’s Post Hoc test both set up at 5% of significance was used to identify the within-group and between-group possible difference. All statistical procedures were performed in GraphPad Prims 9.1.
Finally, the effect size for each intervention type was calculated using Cohen's ʄ-test for three or more interactions and for two interactions using Cohen's d-test. For this test, calculated differences between one score set and another (ʄ²) between 0.02 and 0.14 are described as small effects; and ʄ² between 0.15 and 0.34 are described as moderate effects, values > 0.35 ʄ² is considered a large effect. According to Cohen's results, d is between 0.20 and 0.39 for small effects, between 0.40 and 0.79 for medium effects, and 0.80 or greater for large effects.
3. Results
3.1. The Group Displayed a Homogenous Distribution of Age, Marital Status, and Formal Instruction
The groups displayed a homogeneous distribution concerning age, marital status, and formal education. Most patients were in the 65 to 70 age group, with similar distributions across marital status and other demographic variables. Patients were predominantly in the 65 to 70 age group (30 years; 50.0%), followed by the 71 to 75 age group (11 years; 36.6%) and 76 years or older (8 years; 13.3%). Regarding marital status, more than half of the participants were married (41; 67.83%), followed by divorced (10; 16.6%) or widowed (9; 15.0%). Other demographic variables also showed similar distributions across groups (Table 2).
3.2. The Exercise Control Showed no Difference Between the Training of the Groups
The heart rate control showed no difference between GCP and GAE (p>0.0001), however, both reached the planed cardiac frequency. The lactate level, collected exactly in the same time of the cardiac frequency display homogeneity of intensity between GCP and GAE without differences (p>0.0001). Finally, the charge progression exhibits a comparable implementation of the intensity from the sixth week. However, between GCP and GAE exhibit with no differences between them (p>0.05). In conjunct, this data shown homogeneity of the training intensity and evolution during the exercise program intervention. The Figure 1 dysplay the physical exercise control.
The combination of NIBS plus PMED display a synergic effect on the cognition a dementia of older adults with Alzheimer’s disease.
The GAE, subjected to the combination of NIBS and PMED, showed significant improvements in working memory, outperforming the other groups. The observed effects indicate a significant difference between GCP and GAE, suggesting that the combined intervention had a more substantial impact on working memory and in the short term memory. In terms of group comparisons, GAE showed differences across all groups (p < 0.05), with a large effect size between GCP and GAE (d = 0.92 and 0.95, respectively).
The GAE group exhibited notable improvements in inhibitory control compared to the other groups, indicating positive effects from the combined intervention on this cognitive function. Suppressed control data for GCS showed no significant change after the intervention. GCN scores also showed no difference (p > 0.05). However, GCP and GAE both showed significant differences after the intervention (p < 0.05). Between-group analyses indicated no differences in GCN, GCP, and GCS (p > 0.05), GCP versus GCN (p < 0.05), and GAE versus GCN and GCP (p < 0.05). Effect size tests showed a small effect for GCN and GCP (ʄ² = 0.012 and 0.014, respectively), while GAE showed a large effect (ʄ² = 0.77).
There was a significant reduction in dementia symptoms in the GAE group compared to the other groups, indicating the effectiveness of the combined intervention in improving overall dementia symptoms. In terms of dementia status, GCS showed no significant change after the intervention. GCN also showed no significant difference (p > 0.05). However, GCP and GAE both showed significant improvements (p < 0.05). Comparisons between groups showed differences between GCP and GAE compared to all other groups (p < 0.05), with GAE showing significant differences compared to GCP (p < 0.05). Cohen's test indicated large effect sizes for GCP and GAE (d = 0.73 and 0.94, respectively). The Figure 2 display the data related the gocnition and demantia symptomns.
3.3. The NIBS, and PMED Interventions Both Enhanced the Alpha Brain Wave and SMR Rhythm in the Pre-Frontal Area
GAE showed a significant increase in alpha wave activity after the intervention, suggesting a positive effect of the combination of NIBS and PMED. The observed effects were particularly pronounced compared to the control groups. The alpha band of GCS showed 8.69±0.47 mV at baseline and 8.83±0.46 mV after intervention (p> 0.05). GCP showed 8.65 ± 0.51 mV at baseline and 8.71±0.52 mV after intervention (p> 0.05). However, GCN changed from 8.52±0.46 mV at baseline to 13.45±1.54 mV after intervention, and GAE changed from 8.38±0.39 mV at baseline to 34.81±4, 25 mV after intervention, with significant differences (p<0.0001). Regarding the effect size between groups associated with the alpha band, Cohen's d shows a small effect for GCN (d=0.27) and a large effect for GAE (d=0.97).
All groups undergoing NIBS and PMED demonstrated significant increases in SMR rhythm, indicating positive neurophysiological modulations associated with the intervention. Again, the GAE group stood out with more expressive effects. For SMR rhythms, GCS was 12.60±0.54 mV at baseline and 12.71±0.62 mV after intervention, no difference (p> 0.05). However, GCN increased from 12.94±0.58 mV at baseline to 15.21±0.57 mV after intervention, GCP showed 13.06±0.75 mV at baseline and 15.78±1.83 mV after intervention, and finally GAE increased from 12.69±0.42 mV at baseline All of these modifications were significantly different (p< 0.0001) to 15.24±0.49 mV post-intervention. Regarding effect sizes between groups, GCP, GCN, and GAE showed moderate effects (ʄ² = 0.017; 0.033 and 0.028, respectively). The Figure 3 displays the brain wave paterns.
4. Discussion
We present the results of a 16-week intervention of physical training (PMED) combined with non-invasive brain stimulation (NIBS) in patients with Alzheimer’s Disease. Overall, individuals in the target intervention group outperform the individuals who received only physical exercise, or non-invasive brain stimulation. Furthermore, to explain possible mechanisms underlying the observed behaviors, we assessed brainwave parameters related to AD, cognition, and dementia symptoms. In this trial, the intervention proved beneficial for the primary outcome (dementia symptoms and cognition) and the secondary outcome (Brain wave) in those individuals who received the full intervention. This finding is consistent with our previous study in different groups, as frail elderly [47].
Previously, we demonstrated that the combination of NIBS with PMED was able to improve the cognition concomitantly the modulation of the brain waves of older people with mental and physical frailty [47]. Here only the combined intervention (PMED plus NIBS) improved working memory, which is the most evident impairment of Alzheimer’s disease [47]. These results suggest that it is possible to apply this approach to combat the neurobiological impairments of Alzheimer's disease, as was done here.
For the demographic characteristics of the volunteers, age, and education presented a very even distribution, suggesting that this distribution did not negatively affect the results. In fact, the data presented in Table 1 suggest that demographics do not affect the results. For WM, GAE, and GCP showed significant improvements within and between groups in the post-intervention test (Fig. 1A); however, greater gains were obtained in GAE. No improvement was seen in the other two groups. Given that GCPs and GAEs received the same exercise regimen, these results partially support the evidence that physical activity can improve WM in AD patients [32]. While this is true, exercise associated with NIBS was more effective as GCN received NIBS but did not show improvement in WM. Nonetheless, other previous studies have shown that physical activity can improve working memory [63,64].
Here we demonstrate that the physical exercise was very well controlled and the markers used displayed the same results along 16-weeks of intervention. The increased intensity was comparable between both. In conjunct, this results suggests that the physical exercise wasn’t an intervenient factor in this work, and, the NIBS was the difference in intervention between GCP and GAE.
Physical activity has benefits in various aspects of cognition, such as executive function, working memory, and learning, and may stimulate structural and functional plasticity in the brain [48]. Previous studies have shown that regular physical activity can reduce neurological risk factors such as dementia [49], Parkinson's disease [50], frailty [51], and AD [52], which improve the quality of life [53]. Increased expression, secretion and downstream signalling of neurotrophic factors (BDNF, VEGF, IGF-1), reduced inflammation [54], and cardiovascular improvement, such as reduced arterial stiffness and lowered blood pressure [55,56,57,58], and cardiovascular improvement, such as reduced arterial stiffness and lowered blood pressure [57,59] are some of the mechanisms that could explain exercise-induced neuroplasticity. Taken together, all of these effects can contribute to the development of positive brain health, as shown in numerous studies [60,61,62].
Another fact has to do with the type of exercise regime implemented. For example, we use moderate-volume, and intensity resistance exercises. This choice was made for the safety of our older volunteers, but on the other hand, studies have shown that WM is very sensitive to training intensity [34,65,66].
In regards the primary outcomes, the duration of the intervention proposed was sufficient to produce the expected changes in WM for these groups. For GCP, and GAE this time frame was sufficient to show significant gains of the same variables in the post-intervention test, highlighting the additional effect of the NIBS procedure on the same training schedule for GCN and GAE, suggesting that non-invasive brain stimulation may enhance WM.
In consonance to the results related to working memory, which is the more important clinic symptom of the initial Alzheimer’s disease, GCN, GCP and GAE improved their performance on a post-intervention test assessing inhibitory control, however, GCN improved only in Complex Reaction Time test. The mental flexibility, only was affected in exercised group, but, as observed in regards the WM, the NIBS increased the exercise effect. The results about the GCP and GAE were expected, especially given that most participants initially exhibited dementia symptoms at levels of severe cognitive deficits. These results confirm other works showing the power of exercise to improve inhibitory control[67,68,69,70]. Also, there is one more thing to consider about these big improvements reported here. For example, inhibitory control, and mental flexibility are considered part of the overall cognitive system and represents a partial benefit of the interventions proposed here, as evidenced by current literature [34,67].
The MMSE indicates dementia status in each group. Compared with the scores defining the risk cut point for severe cognitive impairment, the only group that changed from moderate to low likelihood was GAE. Even at the lower limit of GAE scores, the other three groups remained in positions indicating a moderate likelihood of dementia with high cognitive impairment. None of the groups achieved this risk-free status for dementia, however, GCP and GAE groups had benefits from respective interventions to minimize them. Observations of inhibitory control, working memory, and mental flexibility, suggest well-known improvements in cognitive function, especially through motor regulation, which is almost always impaired in AD [52,71].
A comparative analysis of the effects of the two types of interventions on the three cognitive variables examined here showed that the GAE outperformed the other groups almost exclusively with respect to the NIBS procedure. This became apparent in tests of working memory, inhibitory function, and mental flexibility where GAE showed the most pronounced difference compared to the other groups. The impact of this type of PMED on WM is not new, and has been shown before [20,21,50,61], but with the addiction of NIBS the effect of the exercise was improved.
The secondary outcome is related to then electrophysiological activity of the brain. Gather specific observations of the frontal, prefrontal, and sensorimotor areas for their relationship to higher cognitive functions, and motor skills integrated through the intervention, both of which play a role in one factor and often impaired during dementia. Comparing them with the mean EEG of cortical regions activated by alpha waves and SMR rhythms allowed verification of changes in the activation patterns of these regions associated with each intervention type.
First, alpha wave showed an increase in absolute power output after GAE interventions. Given that these groups underwent PMED, the highest alpha-band patterns obtained by GAE were due to the additive effect of the NIBS procedure, as previously shown by our group [21,50,72] and other authors [73,74,75]. However, if it is related to exercise, it is reasonable to be certain that there is a potential synergistic effect due to the strongest activation of this wave in the brains of GAE subjects, who showed higher activity in this region, with a significant impact on neurophysiological craving in older adults tends to exhibit lower alpha during neurological damage caused by Alzheimer's disease [76]. Indeed, brain activation in response to physical activity has previously been shown to mediate in relation to learning and motor function [73,75], as a modulatory effect related to learning, and motricity [21,44,50] and cognition [67,77] were previously described.
Second, regarding the SMR rhythm patterns of GCP, and GAE, it can be seen that the effect after the intervention was different for all groups, as the sensorimotor areas were now more active post-test compared to pre-test. SMR rhythmic activation patterns through relevant cortical points were modified for GCP, and GAE in the post-intervention assessment. For GCP, the spectrum associated with SMR rhythms showed high activation in regions of both hemispheres (P3 and P4). These results may be related to the improvement in inhibitory control and, when combined with the alpha-band power output observed in the C3 and C4 electrodes, confirm that the improvement in brain activation may be related to the cognitive and motor improvements observed here.
These changes benefited all three groups, with effects consistent with their performance on tests assessing abilities related to the cognitive variables studied here. Thus, the superior performance of the GAE over the other groups, especially in the assessment of cognition, reflects the optimal intervention facilitated by the combination of the NIBS procedure and the PMED procedure.
What does this article add? Results associated with GAE seemed consistently more valid and beneficial than those associated with GCP, and these groups accepted either protocol used. This suggests that the combination of NIBS plus PMED, rather than alone, has been shown to improve cognitive function and brain activity in the older adults who participated in this study. The fact that the combined effect can be interpreted as an additive result of each protocol relative to the other is supported by the expansion of the effect size indicated in the Coen’s test results. Therefore, we can consider our results very promising as they identify an emerging tool that can be used as a potential adjunct in the treatment of certain neurobiological impairments caused by AD.
Although our study is quite important in terms of its results, it has some limitations. First, the sample size of the study was relatively small, although other studies of such special populations have used smaller sample sizes in each group. Second, we cannot tightly control the use of medications that may affect cortical neuromodulation, such as general anxiolytics and sedatives, because information about them is "truncated" by many older adults with AD. Third, the investigation of the BDNF, phosphorylated-TAU, and β-Amyloid can explain and give support to our results. In addition, anti-inflammatory drugs can alter the organic inflammatory state normally associated with higher levels of BDNF and thus alter the biochemical regulation of the brain. If properly controlled, these limitations can increase the ability to enable other studies using the same protocol used here.
Addressing the critical aspects of personalization and time efficiency is an advantage. The challenge of adhering to recommended exercise durations due to time constraints can be overcome through personalized programs with flexible timing. HIIT, known for its effectiveness and time efficiency, emerges as a solution for such scenarios. Introducing this time-efficient exercise method to frail individuals holds promise for efficiently enhancing cardiac or cognitive health in the elderly.
5. Conclusions
Our primary findings suggest that an intervention approach comprising PMED and NIBS improves the cognition, and alleviates the dementia symptoms in older adults with early-stage Alzheimer's disease. Furthermore, these enhancements may be linked to improved neurological function in the studied older adults. Finally, the statistical effect sizes of PMED and NIBS applied to enhance cognitive and brain activity functions revealed synergistic effects, suggesting counteraction of AD's pathological effects on certain central nervous system functions.
Acknowledgements
The authors would like to thank to all participants, to SESI, and to Convivence Older Center in Porto Velho, Rondônia, Brazil.
Funding
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), through the Grant/Award Number: 062/2016 and process number 0011.331.0025-00.62/2014 from The Fundação Rondônia de Amparo ao Desenvolvimento das Ações Científicas e Tecnológicas e à Pesquisa do Estado de Rondônia (FAPERO).
References
- Raskin J, Cummings J, Hardy J, Schuh K, Dean R. Neurobiology of Alzheimer’s Disease: Integrated Molecular, Physiological, Anatomical, Biomarker, and Cognitive Dimensions. Curr Alzheimer Res. 2015. [CrossRef]
- Curcio C-L, Wu YY, Vafaei A, Barbosa JF de S, Guerra R, Guralnik J; et al. A Regression Tree for Identifying Risk Factors for Fear of Falling: The International Mobility in Aging Study (IMIAS). The Journals of Gerontology: Series A. 2019. [CrossRef]
- Lee J, Kim Y, Liu T, Hwang YJ, Hyeon SJ, Im H; et al. SIRT3 deregulation is linked to mitochondrial dysfunction in Alzheimer’s disease. Aging Cell. 2018. [CrossRef]
- Kumar A, Tsao JW. Alzheimer Disease: REVUE. StatPearls. 2018.
- Kochhann R, Wilson MA. Introduction: Special issue on neuropsychology of aging. Psychol Neurosci. 2019. [CrossRef]
- Lilamand M, Raynaud-Simon A. Prevalence and consequences of frailty. Pratiques en Nutrition. 2018;14: 13–14. [CrossRef]
- Elliott E, Atlas R, Lange A, Ginzburg I. Brain-derived neurotrophic factor induces a rapid dephosphorylation of tau protein through a PI-3Kinase signalling mechanism. European Journal of Neuroscience. 2005. [CrossRef]
- Hausner L, Frölich L. Antidementia Drug Therapy of Alzheimer’s Dementia: Status 2018 and Outlook. Deutsche Medizinische Wochenschrift. 2019. [CrossRef]
- Van Slegtenhorst M, Lewis J, Hutton M. The molecular genetics of the tauopathies. Experimental Gerontology. 2000. [CrossRef]
- Belarbi K, Burnouf S, Fernandez-Gomez FJ, Laurent C, Lestavel S, Figeac M; et al. Beneficial effects of exercise in a transgenic mouse model of Alzheimer’s disease-like Tau pathology. Neurobiol Dis. 2011;43: 486–494. [CrossRef]
- Scheltens P, Blennow K, Breteler MMB, de Strooper B, Frisoni GB, Salloway S; et al. Alzheimer’s disease. The Lancet. 2016. [CrossRef]
- Yang CC, Chiu MJ, Chen TF, Chang HL, Liu BH, Yang SY. Assay of plasma phosphorylated tau protein (threonine 181) and total tau protein in early-stage Alzheimer’s disease. Journal of Alzheimer’s Disease. 2018;61: 1323–1332. [CrossRef]
- Cruceanu VD, Rotarescu VS. Alpha brainwave entrainment as a cognitive performance activator. Cognition, Brain, Behavior. 2013.
- Reichert JL, Kober SE, Neuper C, Wood G. Resting-state sensorimotor rhythm (SMR) power predicts the ability to up-regulate SMR in an EEG-instrumental conditioning paradigm. Clinical Neurophysiology. 2015. [CrossRef]
- Du Z, Li Y, Li J, Zhou C, Li F, Yang X. Physical activity can improve cognition in patients with alzheimer’s disease: A systematic review and meta-analysis of randomized controlled trials. Clinical Interventions in Aging. 2018. [CrossRef]
- Intlekofer KA, Cotman CW. Exercise counteracts declining hippocampal function in aging and Alzheimer’s disease. Neurobiol Dis. 2013;57: 47–55. [CrossRef]
- Bernardo T, Marques-Aleixo I, Beleza J, Oliveira P, Ascensão A, Magalhães J. PHYSICAL EXERCISE AND BRAIN MITOCHONDRIAL FITNESS : THE POSSIBLE ROLE AGAINST ALZHEIMER ’ S DISEASE. Brain Pathology. 2016;26: 648–663.
- Belaya I, Ivanova M, Sorvari A, Ilicic M, Loppi S, Koivisto H; et al. Astrocyte remodeling in the beneficial effects of long-term voluntary exercise in Alzheimer’s disease. J Neuroinflammation. 2020;17: 1–19. [CrossRef]
- Chow ZS, Moreland AT, Macpherson H, Teo WP. The Central Mechanisms of Resistance Training and Its Effects on Cognitive Function. Sports Medicine. 2021;51: 2483–2506. [CrossRef]
- Xu Y, Qiu Z, Zhu J, Liu J, Wu J, Tao J; et al. The modulation effect of non-invasive brain stimulation on cognitive function in patients with mild cognitive impairment: A systematic review and meta-analysis of randomized controlled trials 11 Medical and Health Sciences 1103 Clinical Sciences 11 Medica. BMC Neurosci. 2019. [CrossRef]
- Calomeni MR, Furtado da Silva V, Velasques BB, Feijó OG, Bittencourt JM, Ribeiro de Souza e Silva AP. Modulatory Effect of Association of Brain Stimulation by Light and Binaural Beats in Specific Brain Waves. Clinical Practice & Epidemiology in Mental Health. 2017;13: 134–144. [CrossRef]
- Brabenec L, Klobusiakova P, Barton M, Mekyska J, Galaz Z, Zvoncak V; et al. Non-invasive stimulation of the auditory feedback area for improved articulation in Parkinson’s disease. Parkinsonism Relat Disord. 2019. [CrossRef]
- Luber B, Deng Z De. Application of non-invasive brain stimulation in psychophysiology. Handbook of Psychophysiology, Fourth Edition. 2016. [CrossRef]
- Dinkelbach L, Brambilla M, Manenti R, Brem AK. Non-invasive brain stimulation in Parkinson’s disease: Exploiting crossroads of cognition and mood. Neuroscience and Biobehavioral Reviews. 2017. [CrossRef]
- Padala KP, Padala PR, Lensing SY, Dennis RA, Bopp MM, Roberson PK; et al. Home-Based Exercise Program Improves Balance and Fear of Falling in Community-Dwelling Older Adults with Mild Alzheimer’s Disease: A Pilot Study. Journal of Alzheimer’s Disease. 2017. [CrossRef]
- Bertolucci PH, Brucki SM, Campacci SR, Juliano Y. The Mini-Mental State Examination in a general population: Impact of educational status. Arq Neuropsiquiatr. 1994;52: 1–7. [CrossRef]
- Fabrício-Wehbe SCC, Schiaveto FV, Vendrusculo TRP, Haas VJ, Dantas RAS, Rodrigues RAP. Cross-cultural adaptation and validity of the “Edmonton Frail Scale - EFS” in a Brazilian elderly sample. Rev Lat Am Enfermagem. 2009. [CrossRef]
- Dubois B, Feldman HH, Jacova C, DeKosky ST, Barberger-Gateau P, Cummings J; et al. Research criteria for the diagnosis of Alzheimer’s disease: Revising the NINCDS-ADRDA criteria. Lancet Neurology. 2007;6: 734–746. [CrossRef]
- Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale [4]. Age and Ageing. 2006. pp. 526–529. [CrossRef]
- Reisberg D, Rappaport I, O’Shaughnessy M. Limits of working memory: The digit digit-span. J Exp Psychol Learn Mem Cogn. 1984;10: 203–221. [CrossRef]
- Wambach D, Lamar M, Swenson R, Penney DL, Kaplan E, Libon DJ. Digit Span. Encyclopedia of Clinical Neuropsychology. 2011. pp. 844–849. [CrossRef]
- Okamura H, Otani M, Shimoyama N, Fujii T. Combined Exercise and Cognitive Training System for Dementia Patients: A Randomized Controlled Trial. Dement Geriatr Cogn Disord. 2018. [CrossRef]
- Tsukamoto H, Takenaka S, Suga T, Tanaka D, Takeuchi T, Hamaoka T; et al. Effect of exercise intensity and duration on postexercise executive function. Med Sci Sports Exerc. 2017. [CrossRef]
- Souza TR, Campos PF, Almeida M, Faria VM, Silveira Chaves B, Faria WM; et al. Exercício progressivo de curtíssima duração possui potente efeito sobre a memória de trabalho, controle inibitório e motricidade fina de adultos jovens sedentários. / Progressive exercise of very short duration has a potent effect on working memory, inhib. Motricidade. 2019;15: 154–163.
- Sun F, Norman IJ, While AE. Physical activity in older people: A systematic review. BMC Public Health. 2013. [CrossRef]
- Forbes D, Thiessen EJ, Blake CM, Forbes SS, Forbes S. Exercise programs for people with dementia. Sao Paulo Medical Journal. 2014. [CrossRef]
- Blazer DG, Yaffe K, Karlawish J. Cognitive aging: A report from the Institute of Medicine. JAMA - Journal of the American Medical Association. 2015. [CrossRef]
- Tam A, Luedke AC, Walsh JJ, Fernandez-Ruiz J, Garcia A. Effects of reaction time variability and age on brain activity during Stroop task performance. Brain Imaging Behav. 2015. [CrossRef]
- Lord SR, Delbaere K, Sturnieks DL. Aging. Handbook of Clinical Neurology. 2018. [CrossRef]
- Hultsch DF, MacDonald SWS, Dixon RA. Variability in reaction time performance of younger and older adults. Journals of Gerontology - Series B Psychological Sciences and Social Sciences. 2002. [CrossRef]
- Jasper H. The ten twenty electrode system of the international federation. Electroencephalogr Clin Neurophysiol. 1958.
- Allen PJ, Josephs O, Turner R. A method for removing imaging artifact from continuous EEG recorded during functional MRI. Neuroimage. 2000. [CrossRef]
- Brueggen K, Fiala C, Berger C, Ochmann S, Babiloni C, Teipel SJ. Early changes in alpha band power and DMN BOLD activity in Alzheimer’s disease: A simultaneous resting state EEG-fMRI study. Front Aging Neurosci. 2017. [CrossRef]
- Furtado V, Calomeni MR, Alkmim R, Nunes M, Elias C, Martins GP; et al. Brain stimulation used as biofeedback in neuronal activation of the temporal lobe area in autistic children. 2016; 632–637. [CrossRef]
- Communications S, Kraemer WJ, Adams K, Cafarelli E, Dudley GA, Dooly C; et al. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2002. [CrossRef]
- Wedell-Neergaard A-S, Lehrskov LL, Christensen RH, Pedersen BK, Ellingsgard H, Krogh-Madsen R. Exercise-Induced Changes in Visceral Adipose Tissue Mass Are Regulated by IL-6 Signaling: A Randomized Controlled Trial. Cell Metab. 2019;29: 844–855.
- Silva VF da, Silva DAS, Martins PC, Calomeni MR, Freire I de A, Militão AG; et al. Effect of physical exercise and noninvasive brain stimulation on cognition and dementia of elderly people with frailty : A randomized study. International Journal Imaging System and Technology. 2022;1: 1–12. [CrossRef]
- Sexton CE, Betts JF, Demnitz N, Dawes H, Ebmeier KP, Johansen-Berg H. A systematic review of MRI studies examining the relationship between physical fitness and activity and the white matter of the ageing brain. Neuroimage. 2016. [CrossRef]
- Mrcpuk CC, Mrcpuk BS. Exercise – Cognition Interaction: Neuroscience Perspectives. Ment Health Phys Act. 2017;12: 1. [CrossRef]
- Silva VF da, Calomeni MR, Nunes RAM, Pimentel CE, Martins GP, Oliveira P da CA; et al. Brain stimulation used as biofeedback in neuronal activation of the temporal lobe area in autistic children. Arq Neuropsiquiatr. 2016. [CrossRef]
- Furtado da Silva V, Simões KM, de Freire IA, Cárdenas RN, O Gonçalvez LG, Borges CJ; et al. Quality of Life, Cognitive Impairment, Treatment, and Physical Exercise in Patients with Parkinson’s Disease: A Review. Journal of Exercise Physiology. 2017;20. Available: https://www.asep.org/asep/asep/JEPonlineOCTOBER_5_2017_Valentim-Silva.pdf.
- Macpherson H, Teo WP, Schneider LA, Smith AE. A life-long approach to physical activity for brain health. Front Aging Neurosci. 2017. [CrossRef]
- Chittrakul J, Siviroj P, Sungkarat S, Sapbamrer R. Multi-system physical exercise intervention for fall prevention and quality of life in pre-frail older adults: A randomized controlled trial. Int J Environ Res Public Health. 2020;17: 1–13. [CrossRef]
- Kawanishi N, Yano H, Mizokami T, Takahashi M, Oyanagi E, Suzuki K. Exercise training attenuates hepatic inflammation, fibrosis and macrophage infiltration during diet induced-obesity in mice. Brain Behav Immun. 2012;26: 931–941. [CrossRef]
- Boer PH, Moss SJ. Effect of continuous aerobic vs. interval training on selected anthropometrical, physiological and functional parameters of adults with Down syndrome. Journal of Intellectual Disability Research. 2016. [CrossRef]
- Braga JC, de Freitas RE, dos Santos KM, Pontes da Silva R, Mota da Silva J, Junior AL; et al. Twelve Weeks of High-Intense Interval Training Enhance the Neuromuscular and Cardiorespiratory Performance of Elderly. Open Sports Sci J. 2020;13: 42–48. [CrossRef]
- Louzada Júnior A, Mota da Silva J, Furtado da Silva V, Clodoaldo Melo Castro A, Eufrásio de Freitas R, Braga Cavalcante J; et al. Multimodal HIIT is More Efficient Than Moderate Continuous Training for Management of Body Composition, Lipid Profile and Glucose Metabolism in the Diabetic Elderly. Int J Morphol. 2020;38: 392–399.
- Silva VF da, Castro ACM, Freitas RE de, Braga JC, Santos KM dos, Albuquerque APA; et al. EIGHT WEEKS OF HIGHINTENSITY INTERVAL TRAINING IMPROVE HAEMATOLOGICAL HEALTH AND DECREASE BLOOD PRESSURE IN SLIGHTLYHYPERTENSIVE ELDERLY. 2018.
- Ringseis R, Eder K, Mooren FC, Krüger K. Metabolic signals and innate immune activation in obesity and exercise. Exercise Immunology Review. 2015. pp. 58–68.
- Baburamani AA, Patkee PA, Arichi T, Rutherford MA. New approaches to studying early brain development in Down syndrome. Developmental Medicine and Child Neurology. 2019. [CrossRef]
- Birba A, Ibáñez A, Sedeño L, Ferrari J, García AM, Zimerman M. Non-invasive brain stimulation: A new strategy in mild cognitive impairment? Frontiers in Aging Neuroscience. 2017. [CrossRef]
- Calverley TA, Ogoh S, Marley CJ, Steggall M, Marchi N, Brassard P; et al. HIITing the brain with exercise: Mechanisms, consequences and practical recommendations. Journal of Physiology. 2020;598: 2513–2530. [CrossRef]
- Liu-Ambrose T, Nagamatsu LS, Graf P, Beattie BL, Ashe MC, Handy TC. Resistance Training and Executive Functions: A 12-Month Randomised Controlled Trial. Arch Intern Med. 2010;170: 170–178. [CrossRef]
- Tsai CL, Pan CY, Chen FC, Wang CH, Chou FY. Effects of acute aerobic exercise on a task-switching protocol and brain-derived neurotrophic factor concentrations in young adults with different levels of cardiorespiratory fitness. Exp Physiol. 2016. [CrossRef]
- de Greeff JW, Bosker RJ, Oosterlaan J, Visscher C, Hartman E. Effects of physical activity on executive functions, attention and academic performance in preadolescent children: A meta-analysis. Journal of Science and Medicine in Sport. 2018. [CrossRef]
- Kelling NJ, Corso GM. The effect of spatial working memory capacity on ball flight perception. Journal of Human Sport and Exercise. 2018. [CrossRef]
- Crush EA, Loprinzi PD. Dose-Response Effects of Exercise Duration and Recovery on Cognitive Functioning. Percept Mot Skills. 2017. [CrossRef]
- Diamond A. Executive Functions. Annu Rev Psychol. 2013;64: 135–68. [CrossRef]
- Collins P, Roberts AC, Dias R, Everitt BJ, Robbins TW. Perseveration and strategy in a novel spatial self-ordered sequencing task for nonhuman primates: Effects of excitotoxic lesions and dopamine depletions of the prefrontal cortex. J Cogn Neurosci. 1998. [CrossRef]
- Lima RF, Da Silva VF, De Oliveira GL, De Oliveira TAP, Filho JF, Mendonça JGR; et al. Practicing karate may improves executive functions of 8-11-year-old schoolchildren. Journal of Physical Education and Sport. 2017;17. [CrossRef]
- Baker LD, Frank LL, Foster-Schubert K, Green PS, Wilkinson CW, McTiernan A; et al. Effects of aerobic exercise on mild cognitive impairment: A controlled trial. Arch Neurol. 2010. [CrossRef]
- Calomeni MR, Rocha JAMDS, da Silva APR, Ribeiro LHB, Marques L, Siza MAF; et al. Brain stimulation used as biofeedback training for recovery of motor functions deteriorated by stroke. Arq Neuropsiquiatr. 2013. [CrossRef]
- Tsuchimoto S, Shibusawa S, Mizuguchi N, Kato K, Ebata H, Liu M; et al. Resting-State Fluctuations of EEG Sensorimotor Rhythm Reflect BOLD Activities in the Pericentral Areas: A Simultaneous EEG-fMRI Study. Front Hum Neurosci. 2017. [CrossRef]
- Moraes H, Ferreira C, Deslandes A, Cagy M, Pompeu F, Ribeiro P; et al. Beta and alpha electroencephalographic activity changes after acute exercise. Arq Neuropsiquiatr. 2007;65: 637–641.
- Chung JW, Ofori E, Misra G, Hess CW, Vaillancourt DE. Beta-band activity and connectivity in sensorimotor and parietal cortex are important for accurate motor performance. Neuroimage. 2017. [CrossRef]
- Fahimi G, Tabatabaei SM, Fahimi E, Rajebi H. Index of theta/alpha ratio of the quantitative electroencephalogram in Alzheimer’s disease: A case-control study. Acta Med Iran. 2017.
- Silva VF da, Matsuura C. Efeitos da prática regular de atividade física sobre o estado cognitivo e a prevenção de quedas em idosos. Fitness & Performance Journal. 2002. [CrossRef]
- O’Connell NE, Wand BM, Marston L, Spencer S, Desouza LH. Non-invasive brain stimulation techniques for chronic pain. Cochrane Database of Systematic Reviews. 2014. [CrossRef]
- Hallett M. Transcranial Magnetic Stimulation: A Primer. Neuron. 2007. [CrossRef]
- Lourenco M V., Frozza RL, de Freitas GB, Zhang H, Kincheski GC, Ribeiro FC; et al. Exercise-linked FNDC5/irisin rescues synaptic plasticity and memory defects in Alzheimer’s models. Nat Med. 2019. [CrossRef]
- Tsai CL, Chen FC, Pan CY, Wang CH, Huang TH, Chen TC. Impact of acute aerobic exercise and cardiorespiratory fitness on visuospatial attention performance and serum BDNF levels. Psychoneuroendocrinology. 2014. [CrossRef]
Figure 1.
Exercise Control. One hundred and sixteen older adults were grouped (n=22 each): GAE (AD, PMED+NIBS), GCP (AD, PMED), GCN (AD, NIBS), GCS (control, no intervention). The ANOVA TWO WAY with Tukey’s Post Hoc Test set up at 5% was used.
Figure 1.
Exercise Control. One hundred and sixteen older adults were grouped (n=22 each): GAE (AD, PMED+NIBS), GCP (AD, PMED), GCN (AD, NIBS), GCS (control, no intervention). The ANOVA TWO WAY with Tukey’s Post Hoc Test set up at 5% was used.
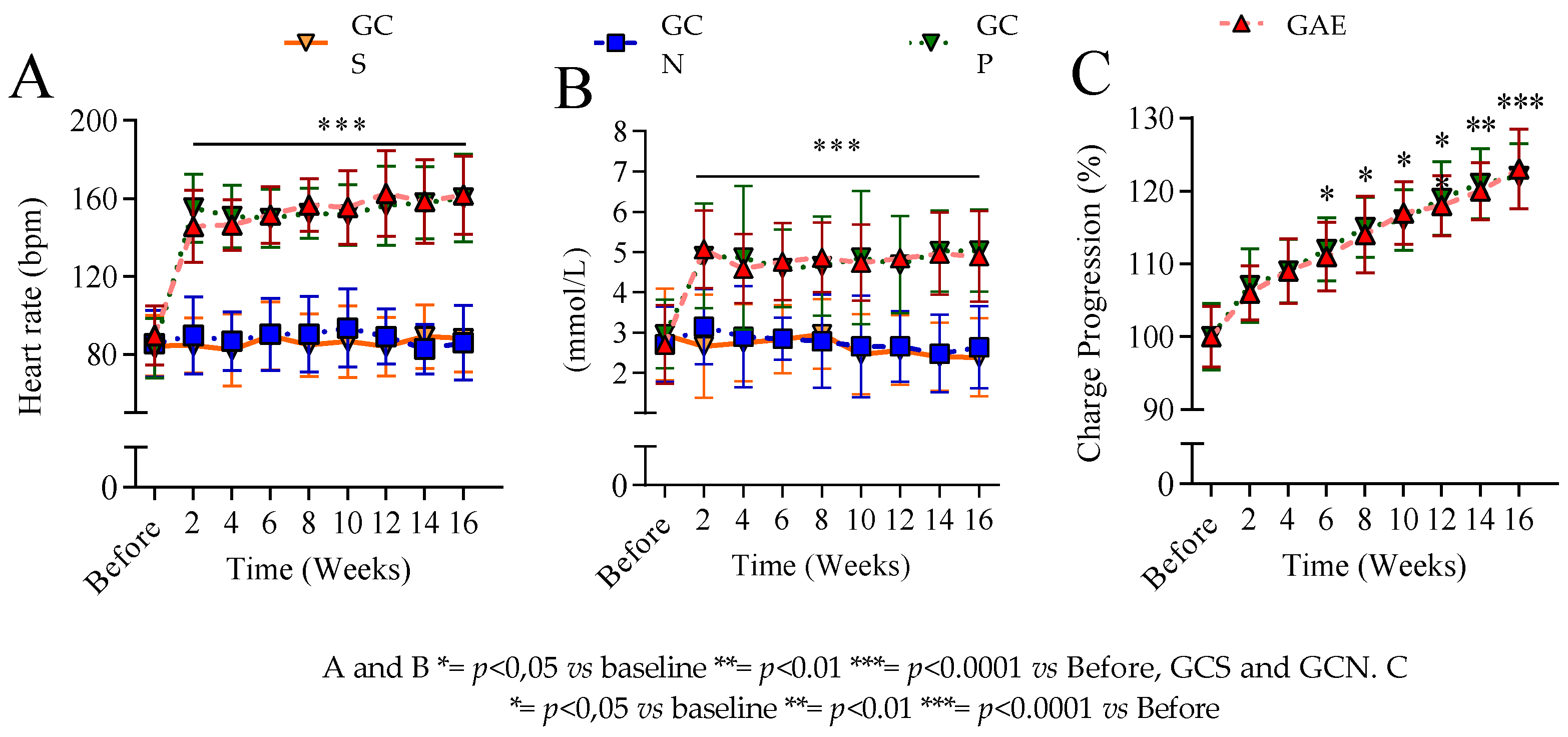
Figure 2.
Mental parameters. One hundred and sixteen older adults were grouped (n=22 each): GAE (AD, PMED+NIBS), GCP (AD, PMED), GCN (AD, NIBS), GCS (control, no intervention). The ANOVA TWO WAY with Tukey’s Post Hoc Test set up at 5% was used.
Figure 2.
Mental parameters. One hundred and sixteen older adults were grouped (n=22 each): GAE (AD, PMED+NIBS), GCP (AD, PMED), GCN (AD, NIBS), GCS (control, no intervention). The ANOVA TWO WAY with Tukey’s Post Hoc Test set up at 5% was used.
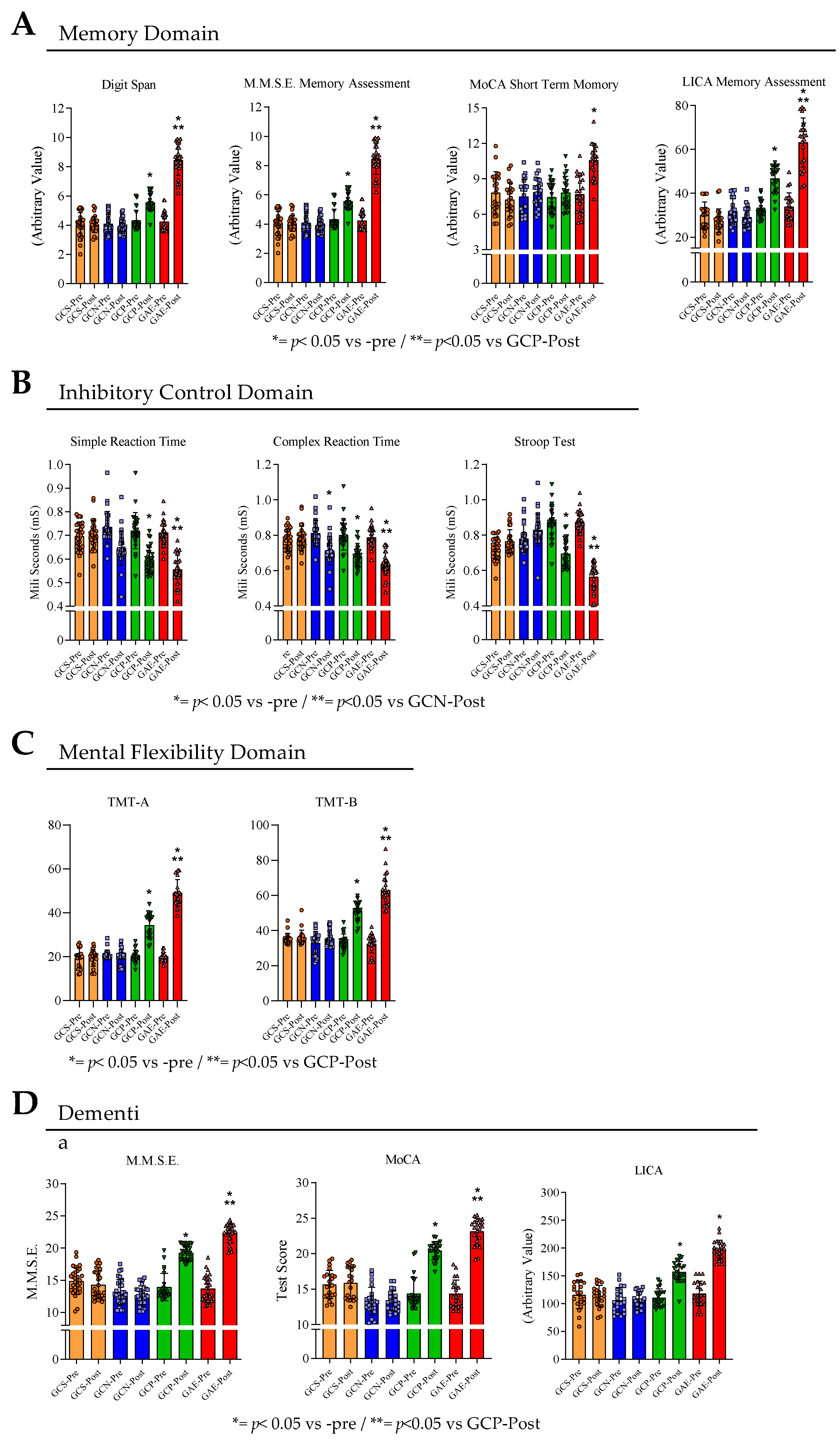
Figure 3.
Electrophysiological brainwave. One hundred and sixteen older adults were grouped (n=22 each): GAE (AD, PMED+NIBS), GCP (AD, PMED), GCN (AD, NIBS), GCS (control, no intervention). The ANOVA TWO WAY with Tukey’s Post Hoc Test set up at 5% was used.
Figure 3.
Electrophysiological brainwave. One hundred and sixteen older adults were grouped (n=22 each): GAE (AD, PMED+NIBS), GCP (AD, PMED), GCN (AD, NIBS), GCS (control, no intervention). The ANOVA TWO WAY with Tukey’s Post Hoc Test set up at 5% was used.
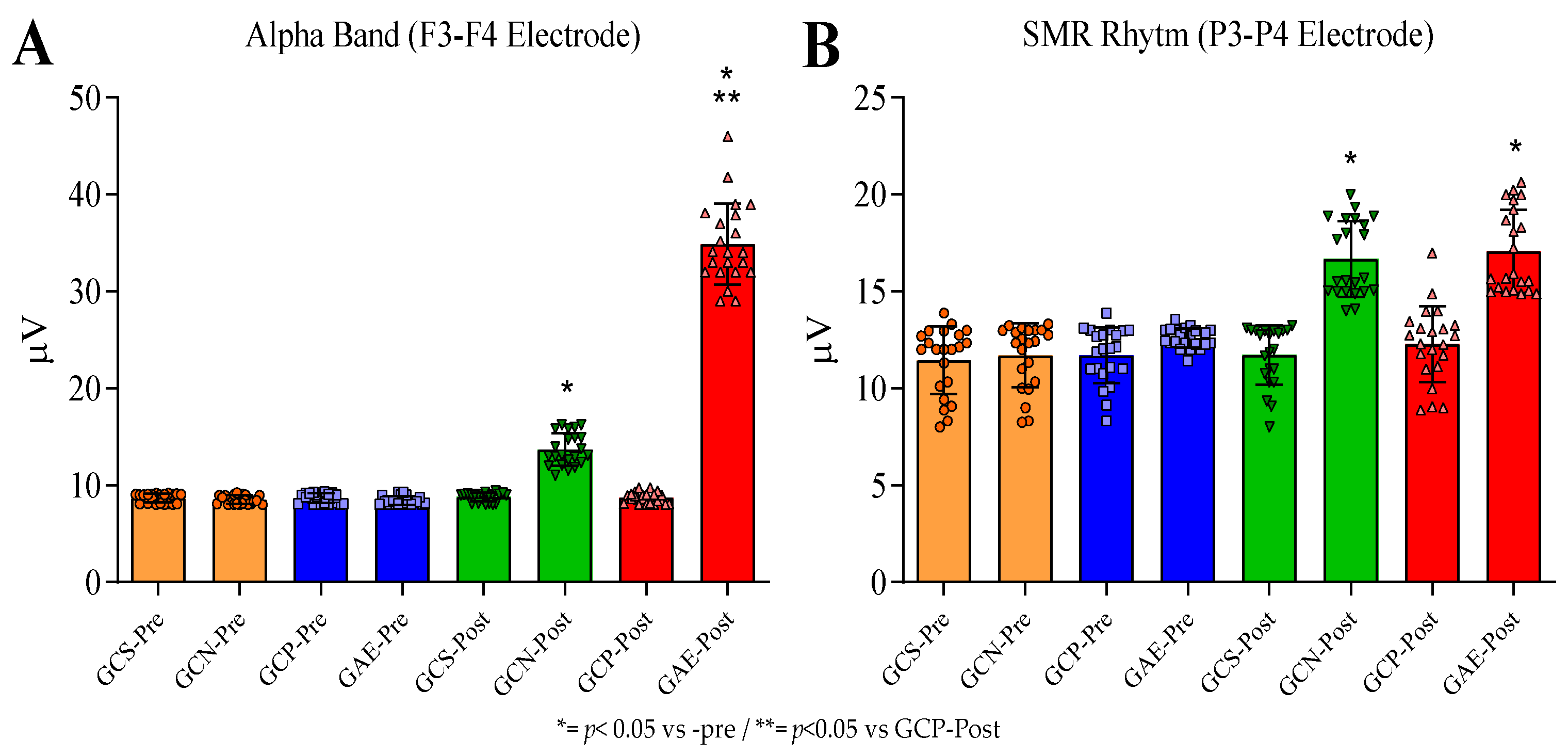

Table 1.
Descriptive Characterization of the study participants.
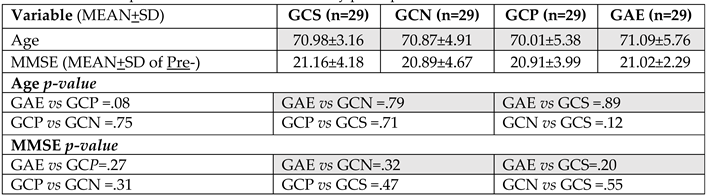
Legend: The volunteers of the GAE (n=29, experimental group with AD subjected to PMED plus NIBS), GCP (n= 29, positive control with AD receiving only PMED), GCN (n=29, positive control with AD that was receiving only NIBS), and GCS (n=29, negative sedentary control kept with no interventions) groups were submitted to the Mini-Mental State Exam (MMSE) test as part of the inclusion and exclusion methodology. The results are described herein. The Mann-Whitney test was used with a significance of 5%. Note SD= Standard Deviation).
Table 2.
Demographic distribution of the sample.
| Variables | GCS | GCN | GCP | GAE | |
|---|---|---|---|---|---|
| Number of individuals in each group | |||||
| Age (Years) | 65-70 71-75 76 > |
18 08 03 |
19 06 04 |
18 05 06 |
20 05 04 |
| Sex | Men Women |
16 13 |
15 14 |
18 11 |
16 13 |
| Marital Status | Divorced Married Widowed |
14 14 01 |
12 15 02 |
16 10 03 |
15 13 01 |
| Educational Level | High School complete> High School incomplete > College complete > |
19 07 03 |
18 10 01 |
17 08 04 |
17 09 03 |
| Social Income | Minimum Wage or < 1-2 Minimum wage(s) 2-4 Minimum Wages 5 > minimum wage |
09 11 03 06 |
07 10 05 07 |
08 07 06 08 |
07 09 08 05 |
| Duration of the disease | 1 year or less 1 year or more 2 years > |
- - - |
15 07 07 |
13 08 08 |
14 09 06 |
Legend: The volunteers of the GAE (n=29, experimental group with AD subjected to PMED plus NIBS), GCP (n=29, positive control with AD receiving only PMED), GCN (n=29, positive control with AD that was receiving only NIBS), and GCS (n=29, negative sedentary control kept with no interventions) groups were submitted to the MMSE test as part of the inclusion and exclusion methodology. The combination of the NIBS plus PMED enhanced working memory function, and inhibitory control, and decreased the symptoms of dementia.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



