
Submitted:
27 May 2024
Posted:
28 May 2024
You are already at the latest version
Abstract
From the existing millions of fungal species only a few cause disease. In this study, we investigated invasive fungal infections in the head and neck over a 19-year period (2005 to 2024) at a large academic healthcare system. Among 413 cases, 336 were noninvasive, and 77 were invasive. The highest incidence of invasive infections occurred in the sinonasal cavities, with a 15-fold difference compared to other sites. Most infections affected adults over 40 years old. The most common organisms were Mucorales (51%), hyaline molds (29%), and Candida (11%). Risk factors included malignancy, transplant, diabetes, and illicit drug use. Mortality was high in patients with malignancy and/or transplant. Infections affecting the mandible were usually a complication of osteoradionecrosis and were associated with coinfection of Candida and Actinomyces. At other sites, infections were rare and were usually the result of penetrating injuries or immunosuppression. Treatment typically involved a combination of antifungals and surgical procedures.
Keywords:
Invasive fungal infection
; head and neck infections
; risk factors
; prognostic factors
; treatment outcome
1. Introduction
The number of fungal species is estimated at 2.2 to 3.8 million worldwide, however of these only about 120,000 have been scientifically classified [1], and only 19 are considered “priority pathogens” by the World Health Organization [2]. Superficial fungal infections affecting the skin and mucosae are bothersome but not life-threatening. By contrast, invasive infections are associated with necrosis or tumor-forming granulomatous reactions that can lead to significant tissue damage or mass effect and be potentially life-threatening depending on their extent and/or location, especially in individuals with weakened immune systems. Of the several million fungal species, the few causing invasive mycoses are Candida, Aspergillus, Mucoromycetes, Cryptococcus, Pneumocystis, Histoplasma, Coccidioides and Blastomyces. The incidence of invasive fungal disease has been rising; recent assessments show that globally, every year more than 150 million people suffer from serious infections and more than 1.6 million die of invasive mycoses [3]. The rise in the burden of invasive fungal disease has been attributed to: 1) Persistence of large populations affected by HIV/AIDS in Africa, 2) Expansion of immunosuppressive therapies worldwide, 3) Global emergence of multi-drugs resistant fungi, 4) Lack of rapid and sensitive diagnostics for early recognition and accurate diagnosis of aggressive fungal infections, 5) Restricted availability of antifungal susceptibility testing and 6) Limited availability of antifungal agents. Despite modest recent progress in diagnosing and treating invasive fungal disease, the mortality rate remains high [4].
Invasive fungal infections of the head and neck (H&N) comprise a heterogenous group of diseases with diverse clinical presentations, treatment, and prognosis. Available literature mostly describes involvement of the sinonasal passages in immunocompromised patients, which is associated with a high mortality rate of ~ 50% [5]. Timely diagnosis followed by surgical intervention, systemic antifungal therapy, and restoration of immune function, when possible, are crucial for improving clinical outcomes [6]. Literature involving other H&N sites, such as oral cavity, pharynx, larynx, orbit, or base of skull, is sparse and limited to case reports. In this study, we reviewed 413 cases of fungal infection at different H&N sites from a large tertiary University Hospital System. The clinical presentation, imaging studies and pathologic findings were summarized and analyzed.
2. Materials and Methods
After IRB approval (IRB protocol # 10391) a natural language search of the pathology database of Indiana University School of Medicine for nasal/paranasal sinus, ear/mastoid, oral cavity, oropharynx/esophagus, base of skull and orbit fungal infections for the period 2005-2024 was performed. For the cohort at the site with the largest number of invasive cases additional data was extracted from the electronic medical records, including demographic information, risk factors, extent of disease, treatments received, and outcome. Descriptive statistics on the extracted data were performed using IBM SPSS Statistics for Windows, Version 28.0. (2021 Armonk, NY: IBM Corp.).
3. Results
413 cases of fungal infections at different H&N sites were found, including 336 non-invasive and 77 invasive cases (Table 1). The ratio of non-invasive to invasive cases varied markedly by site, being the highest at the oropharynx/esophagus and lowest at the ear/mastoid (Table 1). The most common site of invasive fungal infections was the sinonasal cavities by a ratio of ≥ 15:1 compared to the other sites. This cohort with fungal invasive sinonasal infections consisted of 45 cases, 31 males, 14 females for a M:F ratio of 2.2. Mean age was 51.2 yrs. (range 7-91). Only 7% of the cases affected children/adolescents <18 yrs., 20% affected young patients between 18 and 40 yrs., and the majority (73%) affected adults >40 yrs. Although cultures were collected in all the cases, final identification of the fungal organism was done by morphology alone in 18 (40%) due to no growth, and by culture in 27 (60%). A single organism was identified in 40 (89%) and >1 fungus in 5 (11%). The most common fungi were from the order Mucorales: 51%, of which Mucor sp. was the most common (64%), followed by hyaline molds: 29%, of which Aspergillus was the most common (88%) (Figure 1), and Candida: 11% (Table 2). On clinical and radiological evaluation only 12 cases (27%) had invasive infections limited to the sinonasal cavities, while the majority 33 (73%) had infections extending into the surrounding tissues, most commonly the orbit (42%) (Table 3, Figure 2).
Four recurring risk factors: malignancy (23/51%), transplant (13/29%), diabetes mellitus (18/40%) and illicit drug use (5/11%), alone or in combination, were present in most (42/93%) cases. In the few patients (3/7%) without these risk factors, the invasive infection was due to a skin laceration (n=1) and pre-existing allergic fungal sinusitis (n=2).
Overall mortality in the cohort was 53%. Of the 24 deaths, 18 (75%) were secondary to the fungal infection, and 6 (25%) were due to the underlying disease. The distribution of risk factors in the cohort and corresponding outcomes is summarized in Table 4. The most prevalent individual risk factors were malignancy (27%) and diabetes mellitus (24%). Mortality rates among these groups were 75% and 27%, respectively. The most common concurrent risk factors were malignancy and transplantation (18%); mortality in this group was the highest at 87.5%. There were no deaths in the group exposed to illicit drug only (7%). In this group, there were 2 marijuana users, and 3 patients with concurrent use of amphetamines and opioids.
Evaluation for statistically significant correlations between the identified risk factors and the outcome death was performed using both Pearson’s Chi-squared test and Fisher’s exact tests since the sample was of intermediate size. Odds ratios were calculated to determine the strength of association between the identified risk factors and the outcome death. The results of these tests are summarized in Table 5. Highly significant correlations between malignancy (p < 0.001) and transplant (p < 0.009) and death were found, with odds ratios (OR) of 16 for malignancy and an OR=8 for transplant. There was no statistical correlation between diabetes mellitus and illicit drug use and mortality.
The therapies received are summarized in Table 6. Most patients (89%) had surgery including resections of sinonasal and facial tissues (maxillectomy, orbitotomy, exenterations) and endoscopic debridement. A third (33%) of the patients had multiple/repeated surgical procedures. In 5 (11%) patients with dismal prognosis due to the extent of disease, only biopsies were performed before transitioning to palliative care. In 3 of these 5 patients, antifungals were not started; all the remaining patients (42/93%) received antifungal agents in combination or sequentially.
The most used antifungals were triazoles (78%) followed by liposomal amphotericin B (60%). Among the triazoles, voriconazole was the most used (40%), followed by posaconazole and isavuconazonium (26% each). Micafungin (7%) and topical terbinafine (4%) were added only in a few patients.
There were only 8 cases of invasive fungal infection involving the mandibular bone. In all these cases the causative organism was Candida (Figure 3). In 7 (88%) cases the infection was a complication of osteoradionecrosis and was associated with Actinomycosis. In a single case (12%) the infection was associated with a dental implant.
There were only 2 cases of blastomycosis, a cutaneous infection of the nose and an infection of the external ear and post-auricular skin. In both cases a penetrating skin injury preceded the infection. A single case of invasive cutaneous cryptococcosis affecting the ear occurred in a 32-year-old male with active HIV/AIDS infection. A single case of histoplasmosis was identified. It affected the larynx of a 73 y.o. man who was an active hunter and was receiving a tumor necrosis factor inhibitor for Crohn’s disease (Figure 4).
4. Discussion
We have compiled a 19-year experience with fungal infections of the H&N at a large tertiary University Hospital System. At skin and mucosal sites in the H&N our study expectedly showed that non-invasive cases far outnumbered invasive infections. However, the ratio of non-invasive to invasive cases varied markedly by site: in the oral cavity, oropharynx/esophagus the ratio was high > 29:1, while at the other sites such as the larynx (5:1), nasal/paranasal cavities (4.5:1) and in the ear/mastoid (2:1) it was low. This variation aligns with the frequency of commensal, asymptomatic and symptomatic infections at these different sites and underscores the inherent efficacy of barrier function across different epithelia, with skin being more protective than squamous mucosa and respiratory mucosa.
Sinonasal infections accounted for most of the invasive infections of the H&N by a ratio of ≥ 15:1 compared to the other sites, explaining why the majority of the existing literature refers to sinonasal infections. In these cases, extension of the infection beyond the sinonasal cavities was present in 73% of the cases and accounted for most of the orbital and base of skull infections. These results are similar to those reported in systematic reviews of this subject [5], however they are likely influenced by referral bias since serious fungal infections require treatment at tertiary centers with large H&N surgical teams able to handle these complex cases [6]. In our cohort one third of the patients required multiple procedures, including neurosurgical interventions. The most common organisms were Mucorales and hyaline molds; among these groups Mucor sp. and Aspergillus sp. were the most common organisms. Although specific identification of the organism by culture was attempted in all cases, in 40% of the cases morphologic examination alone was enough for guiding therapy, and specifically requested by infectious disease specialists if an identification had been deferred to culture in the original pathology report. This indicates that pathologists should always provide a presumptive morphologic identification, that can be fine tuned after the results of cultures or PCR become available.
Although fungi are less common causes of infection of the ocular tissues than bacteria and viruses, they are worldwide pathogens involved in infections of the eye, eye adnexa and the orbit [7,8,9]. The fungi causing oculo-orbital and H&N infections in general are ubiquitous, however, characteristic geographical distributions exist. Coccidioides immitis is endemic in the southwestern United States (US), northwestern and central Mexico, Venezuela, and the Gran Chaco Plain of South America. Blastomyces dermatitidis, occurs most frequently in the southeastern US. Histoplasma capsulatum is endemic to the Ohio and Mississippi River valleys and the Appalachian Mountains in the US. Histoplasma duboisii is endemic in Nigeria.
Fungal endophthalmitis usually follows accidental penetrating trauma, especially wood and less commonly, it is due to extension of infection from the cornea, eyelid margin, conjunctiva, or lacrimal system. Ophthalmic surgeries can lead to contamination with eyelid or conjunctival sac flora, or contaminated irrigating solutions. Keratoplasty with contaminated donor storage media may also cause invasive fungal infections.
Endogenous fungal endophthalmitis is an infrequent but serious complication of systemic mycoses. The most frequent culprit is Candida, affecting mainly individuals with systemic debilitating diseases, such as the acquired immunodeficiency syndrome (AIDS), chemotherapy, immunosuppressive therapy, intravenous catheterization, and illicit intravenous drug abuse [10,11].
The main orbital fungal infections, zygomycosis (most commonly Mucorales) and aspergillosis, are typically extensions from the paranasal sinuses. Diabetic ketoacidosis predisposes to zygomycosis, whereas allergic fungal sinusitis may precede orbital aspergillosis. The principal predisposing factor in mycotic infections of the lacrimal drainage apparatus is partial or complete blockage of that system.
Zygomycetes are ubiquitous in soil and vegetable matter around the world. The airborne spores enter the body through the respiratory tract. In the nose and paranasal sinuses, the fungus may proliferate, penetrate blood vessels, and spread by vascular and direct extension to the orbit [12,13]. Vascular invasion leads to thrombosing vasculitis and infarction of the surrounding tissues [14]. Several Zygomycetes but most commonly Rhizopus, cause the clinical syndrome of cerebrorhinoorbital phycomycosis, a highly lethal disease. In adults, 50% of affected patients have poorly controlled diabetes [14], however, the infection can occur in patients with mild or unrecognized diabetes [15] and occasionally in healthy individuals [16]. Also, alcoholic cirrhosis, ulcerative colitis, hematolymphoid and somatic malignancies and their therapy, extensive burns and deferoxamine therapy [17,18]. In some cases, fungi from the Entomophthorales species cause the syndrome, leading to characteristic dark, gangrenous lesions in the periorbital skin, nasal mucosa, or palate.
In children, the infection is often a sequel to severe diarrhea with dehydration and metabolic acidosis. Rarely, healthy children may be affected [19].
Thrombosis of the ophthalmic and/ or central retinal artery may result in extensive infarction of intraocular structures. Orbital cellulitis, with involvement of the optic nerve and the nerves that pass through the sphenoidal fissure (orbital apex syndrome) [20] are usually associated with fatal cerebral involvement [21].
In zygomycosis the organisms are typically located deep within the lesions, necessitating deep biopsies for histologic diagnosis. In tissue sections, 30-50 μm wide nonseptate branching hyphae are found. A unique feature of this fungi is that they can be easily identified in hematoxylin and eosin-stained tissue sections, which typically show tissue infarction with a minimal cellular response [22].
In our cohort 94% of the patients had one or more of 4 risk factors: malignancy, transplant, diabetes mellitus and illicit drug use. The first 3 have an established association with an impaired immune system [23,24], and the last one an association with increased exposure to contaminated substances [25,26]. In the 3 cases without these risk factors a skin laceration was identified as the port of entry of the infection, and in the 2 remaining cases the infections originated from fungal sinusitis. Fungal infection-associated mortality had a highly significant association with malignancy and transplant, but not with diabetes and illicit drug use. In our cohort, the odds ratio of dying of infection for malignancy and transplant were 16 and 8, respectively. Fatal infections are commonly associated with severe immunosuppression [24] In our cohort, 83% of patients had hematologic malignancies, and 17% had somatic malignancies. Among those with a history of transplant, 69% underwent bone marrow transplantation, while the remaining 31% received solid organ transplants. Notably, patients with hematologic diseases undergoing bone marrow transplants are particularly susceptible to fatal infections due to the profound immunosuppression affecting both cellular and humoral immune responses. Severe neutropenia is the primary risk factor for Aspergillus infections [24], while Mucor infections are associated with neutropenia and diabetes mellitus [23]. These two organisms accounted for most of the infections in our study. The overall mortality rate in our cohort was 53%, consistent with rates reported in literature reviews [5,6].
While most invasive infections of the H&N represented extension of sinonasal disease into the orbit, facial soft tissues and base of skull, involvement of the mandible, which comprised 10% of invasive infections, was primarily due to extension of oral candidiasis into areas of osteoradionecrosis and was frequently associated with Actinomyces. This association had also been reported in a previous study [27].
Invasive infections affecting the ear, oral cavity, and larynx were exceedingly rare in our study. These infections were associated with specific risk factors, including penetrating injuries, hematologic malignancies, immunosuppressive medications, and HIV/AIDS. A large series of laryngeal fungal infections in Vietnam (n=48) revealed that Aspergillus was the most common causative organism, followed by Candida [28]. Notably, all patients in this series were immunocompetent, 44% were smokers, and the infections were attributed to environmental exposure.
Literature on invasive fungal infections of the oral cavity and the ear is limited and primarily based on literature reviews. In both locations, Aspergillus and Candida are consistently cited as the most common organisms, particularly affecting immunocompromised individuals [28,29,30]. In our case series, 97% (86 out of 89) of oral cavity fungal infection were non-invasive and caused by Candida colonization. All three patients with invasive infections were immunocompromised: two with hematopoietic malignancy and one with somatic malignancy. Among the patients diagnosed with ear/mastoid infection, three out of ten presented with invasive disease. One of these patients was HIV-positive, while the other was immunocompetent and had a history of environmental exposure. The medical history of the third patient was unavailable in our electronic medical system.
Invasive mycoses in the sinonasal tract are managed with aggressive surgical debridement and systemic antifungal treatment. Pre-surgical cranial and sinus computerized tomography or magnetic resonance imaging are strongly recommended to assess the disease extent and guide treatment plan [31]. Resection should be repeated as needed. Skiada, A, et al. showed that surgical treatment decreased the risk of death caused by Zygomycosis by 79% [32]. Liposomal Amphotericin B combined with surgery provided the best chance of recovery in this study. In our cohort, 89% of patients had surgical intervention and about one third had more than one procedure. Triazoles were the most used antifungals followed by Amphotericin B. Follow-up imaging at 6-12 weeks intervals after surgery is recommended to evaluate patients’ response and determine the duration of therapy [33]. Post-surgical anti-fungal therapy can be continued until signs and symptoms have resolved and radiologic improvement is evident. For Mucormycosis, treatment duration is usually prolonged to 6-12 months [33]. Addressing underlying risk factors or reducing immunosuppression should be attempted if feasible, for example, control glucose level in diabetic patients or granulocytes infusion in neutropenic patients.
5. Conclusions
We have compiled our 19-year experience with invasive fungal infections of the H&N at a large tertiary academic health system. Invasive sinonasal infections were 15 times more common than any other site. Orbital infections, the second most common site, represented an extension of sinonasal infections. These infections were mostly caused by Aspergillus and Mucor and affected patients with one or several of the following risk factors: malignancy, transplant, diabetes mellitus, and illicit drug use. Mortality in our cohort was primarily associated with malignancy and transplant. The third most common site was the mandible. At this site, infections occurred as a complication of osteoradionecrosis and were caused by coinfection of Candida and Actinomyces. At other H&N sites, infections were exceedingly rare and associated with clearly identifiable risk factors: penetrating injuries, environmental exposures, and immunosuppression. Treatment of invasive fungal infections requires the combination of surgical debridement and antifungals. Despite recent advances in antifungal therapies, mortality remains high (>50%) for immunocompromised patients with advanced infections.
Author Contributions
Conceptualization, TH, HM; methodology, TH, HM; formal analysis, TH, RB, HM; writing—original draft preparation, TH, RB, HM; writing—review and editing, TH, RB, HM; supervision & project administration, HM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Indiana University School of Medicine, IRB protocol # 10391, 2/9/2022. .
Informed Consent Statement
Patient consent was waived because this is a minimal risk retrospective study dealing with aggregated deidentified data.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The Department of Pathology and Laboratory Medicine of Indiana University School of Medicine provided support for this study. .
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hawksworth, D.L.; Lücking, R. , “Fungal Diversity Revisited: 2.2 to 3.8 Million Species,” Microbiol Spectr, vol. 5, no. 4, 2017. [CrossRef]
- Burki, T. , “WHO publish fungal priority pathogens list,” Lancet Microbe, vol. 4, no. 2, 2023. [CrossRef]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. , “Global and multi-national prevalence of fungal diseases—estimate precision,” Journal of Fungi, vol. 3, no. 4. 2017. [CrossRef]
- Firacative, C. , “Invasive fungal disease in humans: Are we aware of the real impact?,” Mem Inst Oswaldo Cruz, vol. 115, no. 9, 2020. [CrossRef]
- Turner, J.H.; Soudry, E.; Nayak, J.V.; Hwang, P.H. , “Survival outcomes in acute invasive fungal sinusitis: A systematic review and quantitative synthesis of published evidence,” Laryngoscope, vol. 123, no. 5, 2013. [CrossRef]
- Roland, L.T. et al., “Diagnosis, Prognosticators, and Management of Acute Invasive Fungal Rhinosinusitis: Multidisciplinary Consensus Statement and Evidence-Based Review with Recommendations,” Int Forum Allergy Rhinol, 2023. [CrossRef]
- “Mycosis of the eye and its adnexa.,” Developments in ophthalmology, vol. 32. 1999.
- Klotz, S.A.; Penn, C.C.; Negvesky, G.J.; Butrus, S.I. , “Fungal and Parasitic Infections of the Eye,” Clin Microbiol Rev, vol. 13, no. 4, 2000. [CrossRef]
- Thomas, P.A. , “Current Perspectives on Ophthalmic Mycoses,” Clinical Microbiology Reviews, vol. 16, no. 4. 2003. [CrossRef]
- Coskuncan, N.M. et al., “The Eye in Bone Marrow Transplantation: VI. Retinal Complications,” Archives of Ophthalmology, vol. 112, no. 3, 1994. [CrossRef]
- Diamond, R.D. , “The growing problem of mycoses in patients infected with the human immunodeficiency virus,” Reviews of Infectious Diseases, vol. 13, no. 3. 1991. [CrossRef]
- Ribes, J.A.; Vanover-Sams, C.L.; Baker, D.J. , “Zygomycetes in human disease,” Clinical Microbiology Reviews, vol. 13, no. 2. 2000. [CrossRef]
- STRAATSMA, B.R.; ZIMMERMAN, L.E.; GASS, J.D. , “Phycomycosis. A clinicopathologic study of fifty-one cases.,” Lab Invest, vol. 11, 1962.
- Gass, J.D.M. , “Ocular Manifestations of Acute Mucormycosis,” Archives of Ophthalmology, vol. 65, no. 2, 1961. [CrossRef]
- Baum, J.L. , “Rhino-orbital mucormycosis. Occurring in an otherwise apparently healthy individual,” Am J Ophthalmol, vol. 63, no. 2, 1967. [CrossRef]
- Yohai, R.A.; Bullock, J.D.; Aziz, A.A.; Markert, R.J. , “Survival factors in rhino-orbital-cerebral mucormycosis,” Survey of Ophthalmology, vol. 39, no. 1. 1994. [CrossRef]
- Daly, A.L.; Velazquez, L.A.; Bradley, S.F.; Kauffman, C.A. , “Mucormycosis: association with deferoxamine therapy,” Am J Med, vol. 87, no. 4, 1989. [CrossRef]
- Morriss, F.H.; Spock, A. , “Intracranial Aneurysm Secondary to Mycotic Orbital and Sinus Infection: Report of a Case Implicating Penicillium as an Opportunistic Fungus,” American Journal of Diseases of Children, vol. 119, no. 4, 1970. [CrossRef]
- Hale, L.M. , “Orbital-Cerebral Phycomycosis: Report of a Case and a Review of the Disease in Infants,” Archives of Ophthalmology, vol. 86, no. 1, 1971. [CrossRef]
- Hedges, T.R.; Leung, L.S.E. , “Parasellar and orbital apex syndrome caused by aspergillosis,” Neurology, vol. 26, no. 2, 1976. [CrossRef]
- Sponsler, T.A.; Sassani, J.W.; Johnson, L.N.; Towfighi, J. , “Ocular invasion in mucormycosis,” Survey of Ophthalmology, vol. 36, no. 5. 1992. [CrossRef]
- Schwartz, J.N.; Donnelly, E.H.; Klintworth, G.K. , “Ocular and orbital phycomycosis,” Survey of Ophthalmology, vol. 22, no. 1. 1977. [CrossRef]
- Skiada, A.; Pavleas, I.; Drogari-Apiranthitou, M. , “Epidemiology and diagnosis of mucormycosis: An update,” Journal of Fungi, vol. 6, no. 4. 2020. [CrossRef]
- Parody, R.; Martino, R.; Sánchez, F.; Subirá, M.; Hidalgo, A.; Sierra, J. , “Predicting survival in adults with invasive aspergillosis during therapy for hematological malignancies or after hematopoietic stem cell transplantation: Single-center analysis and validation of the Seattle, French, and Strasbourg prognostic indexes,” Am J Hematol, vol. 84, no. 9, 2009. [CrossRef]
- Benedict, K.; Thompson, G.R.; Jackson, B.R. , “Cannabis use and fungal infections in a commercially insured population, United States, 2016,” Emerg Infect Dis, vol. 26, no. 6, 2020. [CrossRef]
- Hartnett, K.P. et al., “Bacterial and Fungal Infections in Persons Who Inject Drugs — Western New York, 2017,” MMWR Morb Mortal Wkly Rep, vol. 68, no. 26, 2019. [CrossRef]
- Hamilton, J.D.; Lai, S.Y.; Ginsberg, L.E. , “Superimposed infection in mandibular osteoradionecrosis: Diagnosis and outcomes,” J Comput Assist Tomogr, vol. 36, no. 6, 2012. [CrossRef]
- Trang, P.T.L.; Thi, D.D.; Son, N.T. , “Clinical symptoms, endoscopic imaging and stroboscopic imaging in patients with laryngeal fungal infection : An evaluation in 48 patients,” Biomedical Research and Therapy, vol. 7, no. 9, 2020. [CrossRef]
- Telles, D.R.; Karki, N.; Marshall, M.W. , “Oral Fungal Infections: Diagnosis and Management,” Dental Clinics of North America, vol. 61, no. 2. 2017. [CrossRef]
- Bojanović, M. et al., “Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review,” Journal of Fungi, vol. 9, no. 6. 2023. [CrossRef]
- Cornely, O.A. et al., “Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium,” The Lancet Infectious Diseases, vol. 19, no. 12. 2019. [CrossRef]
- Skiada, A. et al., “Zygomycosis in Europe: Analysis of 230 cases accrued by the registry of the European Confederation of Medical Mycology (ECMM) Working Group on Zygomycosis between 2005 and 2007,” Clinical Microbiology and Infection, vol. 17, no. 12, 2011. [CrossRef]
- Patterson, T.F. et al., “Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the infectious diseases society of America,” Clinical Infectious Diseases, vol. 63, no. 4. 2016. [CrossRef]
Figure 1.
A-C: Mucormycosis. H&E (A) and GMS stain (B) show numerous fungal hyphae invading necrotic tissues and vascular walls (angioinvasion). (C) Nonseptate thick fungal hyphae with irregular branching points associated with acute osteomyelitis and osteonecrosis. D-F: Aspergillosis. H&E (D) and GMS stain (E) show acute angle or dichotomous branching, septate hyphae invading bone. H&E (F) Fungal hyphae invading vascular spaces. .
Figure 1.
A-C: Mucormycosis. H&E (A) and GMS stain (B) show numerous fungal hyphae invading necrotic tissues and vascular walls (angioinvasion). (C) Nonseptate thick fungal hyphae with irregular branching points associated with acute osteomyelitis and osteonecrosis. D-F: Aspergillosis. H&E (D) and GMS stain (E) show acute angle or dichotomous branching, septate hyphae invading bone. H&E (F) Fungal hyphae invading vascular spaces. .
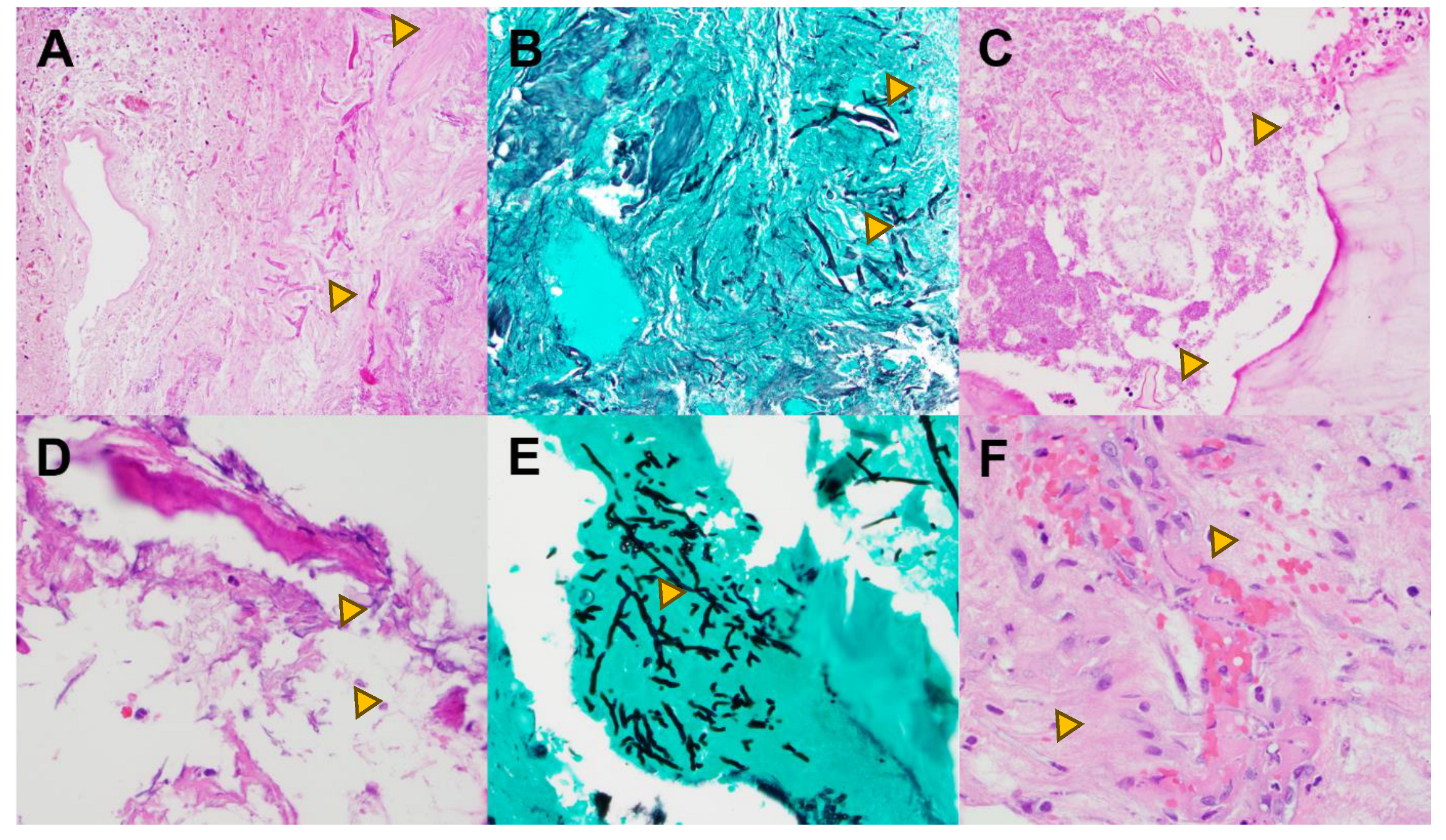
Figure 2.
Magnetic resonance imaging, invasive fungal sinusitis with orbital and base of skull involvement A. Axial image showing left sphenoid sinus mucosal thickening with internal fluid and erosion of the base of skull (arrowheads). B. Axial image showing left-sided proptosis and edema in the soft tissues (arrows) extending from the ocular globe to the orbital apex and cavernous sinus. C. Axial T2-weighted image showing edema of the intraorbital optic nerve (arrow heads). D. Coronal T2-weighted image showing extensive edema in the posterior orbit (arrows) involving soft tissues, the optic canal, vessels and oculomotor nerves. .
Figure 2.
Magnetic resonance imaging, invasive fungal sinusitis with orbital and base of skull involvement A. Axial image showing left sphenoid sinus mucosal thickening with internal fluid and erosion of the base of skull (arrowheads). B. Axial image showing left-sided proptosis and edema in the soft tissues (arrows) extending from the ocular globe to the orbital apex and cavernous sinus. C. Axial T2-weighted image showing edema of the intraorbital optic nerve (arrow heads). D. Coronal T2-weighted image showing extensive edema in the posterior orbit (arrows) involving soft tissues, the optic canal, vessels and oculomotor nerves. .
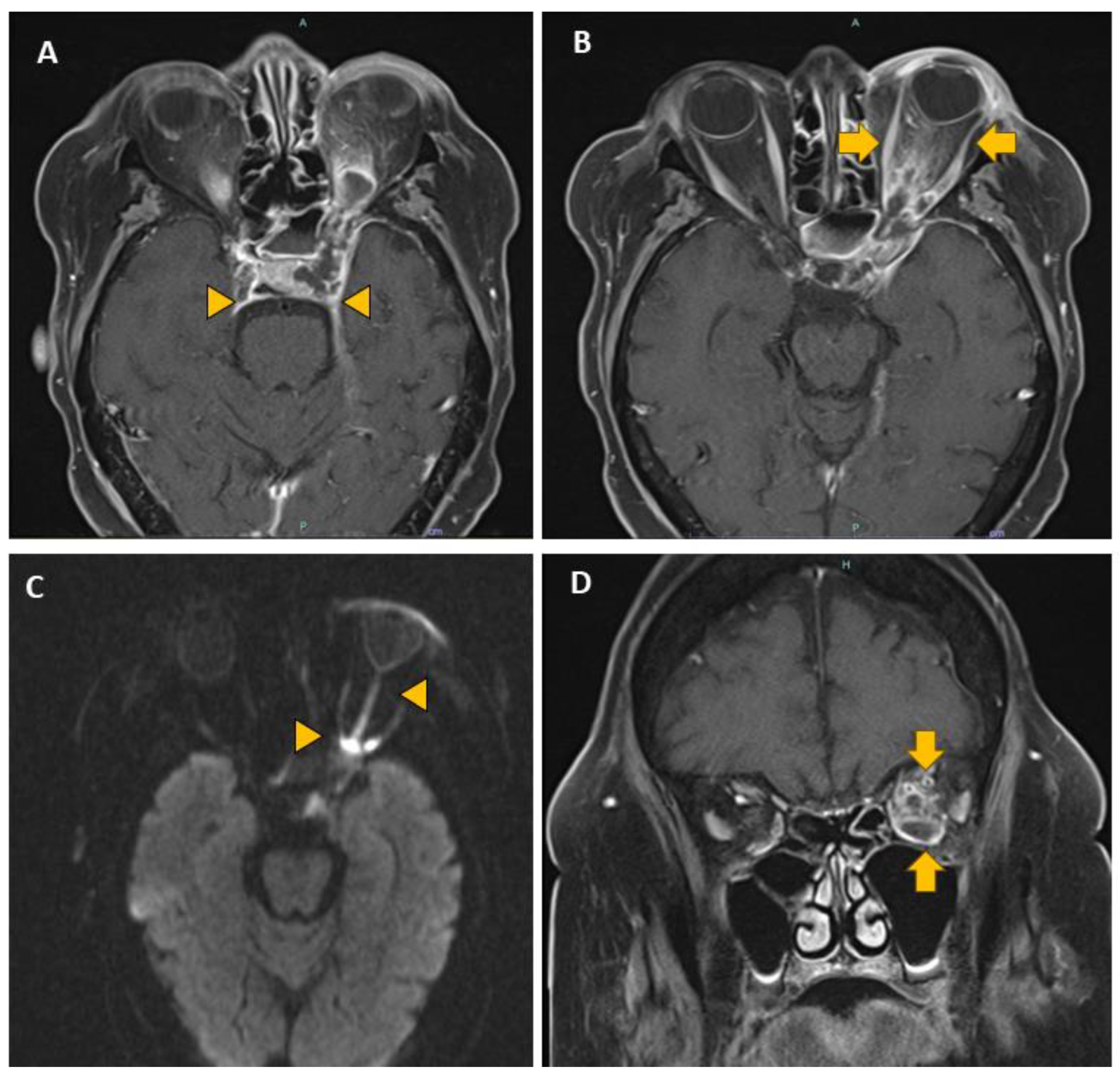
Figure 3.
A-C: Candidiasis. (A) H&E, lower magnification shows Candida (arrowhead) and Actinomyces (arrow) coinfection complicating a case of osteoradionecrosis. (B) H&E, higher magnification and (C) GMS demonstrate characteristic “spaghetti and meatballs” yeasts and fungal hyphae. D-F: Curvularia. (D) H&E, lower and (E) higher magnifications show poorly formed granulomas with numerous multinucleated giant cells (arrowhead) involving sinonasal mucosa. (F) GMS stain highlights septate hyphae. A PCR assay confirmed Curvularia species. .
Figure 3.
A-C: Candidiasis. (A) H&E, lower magnification shows Candida (arrowhead) and Actinomyces (arrow) coinfection complicating a case of osteoradionecrosis. (B) H&E, higher magnification and (C) GMS demonstrate characteristic “spaghetti and meatballs” yeasts and fungal hyphae. D-F: Curvularia. (D) H&E, lower and (E) higher magnifications show poorly formed granulomas with numerous multinucleated giant cells (arrowhead) involving sinonasal mucosa. (F) GMS stain highlights septate hyphae. A PCR assay confirmed Curvularia species. .
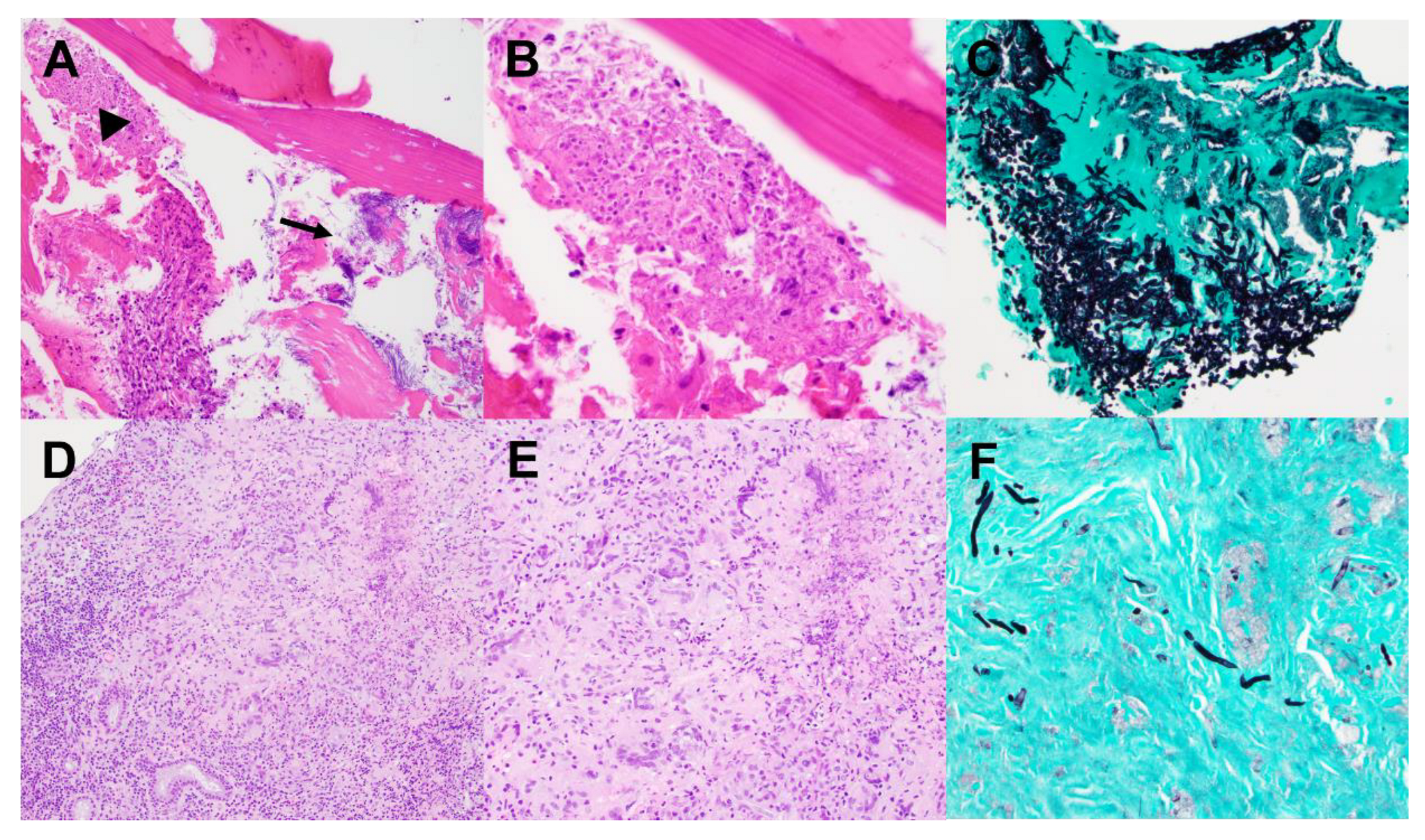
Figure 4.
A-B: Blastomycosis. (A) H&E, lower magnification shows abundant mixed inflammatory cells in the dermis. (B) GMS stain reveals large budding yeasts. C-D: Cryptococcosis. (C) H&E slide demonstrates numerous foamy histiocytes and rare eosinophils in dermis. (D) Mucicarmine stain highlights the cryptococcal capsule. E-F: Histoplasmosis. (E) Extensive non-necrotizing granulomatous inflammation involving the epiglottis. GMS highlights scattered histoplasma yeasts (arrow). .
Figure 4.
A-B: Blastomycosis. (A) H&E, lower magnification shows abundant mixed inflammatory cells in the dermis. (B) GMS stain reveals large budding yeasts. C-D: Cryptococcosis. (C) H&E slide demonstrates numerous foamy histiocytes and rare eosinophils in dermis. (D) Mucicarmine stain highlights the cryptococcal capsule. E-F: Histoplasmosis. (E) Extensive non-necrotizing granulomatous inflammation involving the epiglottis. GMS highlights scattered histoplasma yeasts (arrow). .
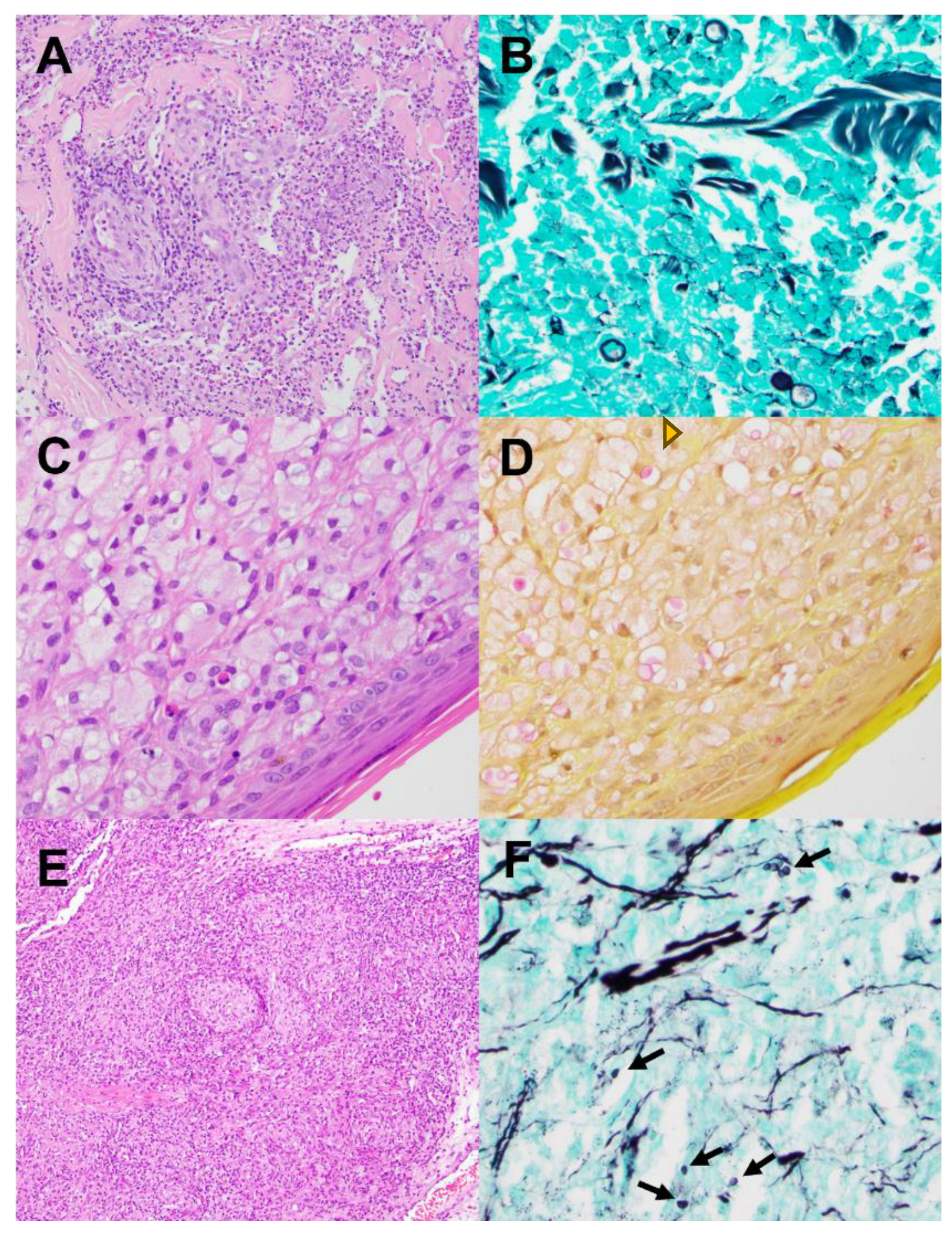

Table 1.
Fungal infections of the H&N in the IUSM pathology database for the period 2005-2024.
| Invasive (Inv) | Non-invasive (Non-inv) | Ratio Non-Inv : Inv | |||
|---|---|---|---|---|---|
| Site | n | % | n | % | |
| Sinonasal | 45 | 58.4 | 203 | 60.4 | 4.5 |
| Ear/mastoid | 3 | 3.9 | 7 | 2.1 | 2.3 |
| Larynx | 2 | 2.6 | 10 | 3.0 | 5 |
| Oral cavity | 3 | 3.9 | 86 | 25.6 | 28.3 |
| Oropharynx/esophagus | 0 | 0 | 30 | 8.9 | >30 |
| Base of skull | 2 | 2.6 | - | - | - |
| Orbit | 14 | 18.2 | - | - | - |
| Mandible | 8 | 10.4 | - | - | - |
Table 2.
Fungus identification in invasive sinonasal infections.
| Morphology | Genus/species | n (%) | N (%) |
|---|---|---|---|
| Mucorales | Mucor sp. Rhizopus sp. Rhizomucor sp. Sincephalastrum racemosum |
18 (64) 5 (18) 4 (14) 1 (4) |
28 (51) |
| Hyaline molds | Aspergillus (various species) Fusarium sp. Scedosporium sp. |
14 (88) 1 (6) 1 (6) |
16 (29) |
| Candida | C. albicans C. parasilopsis C. glabrata C. dubliniensis C. sp. |
2 (33) 1 (17) 1 (17) 1 (17) 1 (17) |
6 (11) |
| Dematiaceous | Curvularia Dematiaceous sp. |
1 (50) 1 (50) |
2 (4) |
| Others | Blastomyces dermatitides Kluyveromyces marxianus Mycelia sterilia |
1 (33) 1 (33) 1 (33) |
3 (6) |
Table 3.
Extent of invasive sinonasal infections.
| Extension | n | % |
|---|---|---|
| Sinonasal only | 12 | 27 |
| Beyond sinonasal | 33 | 73 |
| Extrasinonasal extension | ||
| Orbit | 19 | 42 |
| Intracranial | 5 | 11 |
| Base of skull | 5 | 11 |
| Facial soft tissue | 3 | 7 |
| Palate | 3 | 7 |
| Nasopharynx | 2 | 4 |
| Oropharynx | 1 | 2 |
Table 4.
Frequency of risk factors and death outcome in invasive sinonasal infections.
| Risk Factor | Subgroup n (%) | n (%) | Dead n (%) |
All Risk Factors | n (%) | Dead n (%) |
|---|---|---|---|---|---|---|
| Malignancy | Hematolymphoid 19 (83) Somatic 4 (17) |
23 (51) | 19 (83) | Malignancy only Malign. + transplant Malignancy + DM Malignancy + Drugs Malign. + transpl.+ DM Transplant only Transplant + DM Transplant + Drugs DM only DM + Drugs Drugs only |
12 (27) 8 (18) 1 (2) 0 2 (4) 1 (2) 2 (4) 0 11 (24) 2 (4) 3 (7) |
9 (75) 7 (87.5) 1 (100) 0 2 (100) 1 (100) 1 (50) 0 3 (27.3) 1 (50) 0 |
| Transplant | Bone marrow 9 (69) Pancreas & kidney 1 (8) Pancreas 1 (8) Kidney 1 (8) Liver 1 (8) |
13 (29) | 11 (85) | |||
| Diabetes mellitus (DM) | Type 1 5 (28) Type 2 13 (72) |
18 (40) | 7 (39) | |||
| Illicit Drug | Marijuana 2 (40) Methamphetamines 3 (60) Opioids* 3 (60) |
5 (11) | 1 (20) | |||
| None | - | 3 (7) | 0 |
* Percentage reflects concurrent use of illicit drugs.
Table 5.
Significance/strength of association between risk factors and outcome death.
| Risk Factor | Pearson Chi2 test (2-sided) |
Fisher’s exact test (2-sided) |
Odds Ratio | 95% Confidence Interval |
|---|---|---|---|---|
| Malignancy | < 0.001*** | < 0.001*** | 16.150 | 3.718 - 70.142* |
| Transplant | 0.007** | 0.009** | 8.038 | 1.523 - 42.430* |
| Diabetes mellitus | 0.113 | 0.138 | 0.374 | 0.110 - 1.278 |
| Illicit Drug | 0.113 | 0.169 | 0.185 | 0.019 - 1.805 |
Table 6.
Treatment for invasive sinonasal fungal infections.
| Therapy | n | % |
|---|---|---|
| Surgery | 40 | 89 |
| Multiple surgeries | 15 | 33 |
| Biopsy only | 5 | 11 |
| No antifungals | 3 | 7 |
| Amphotericin B | 27 | 60 |
| Triazoles | 35 | 78 |
| Voriconazole (40%) | 14 | 31 |
| Itraconazole (3%) | 1 | 2 |
| Posaconazole (26%) | 9 | 20 |
| Isavuconazonium (26%) | 9 | 20 |
| Fluconazole (6%) | 2 | 4 |
| Micafungin | 3 | 7 |
| Terbinafine | 2 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



