
Submitted:
27 May 2024
Posted:
28 May 2024
You are already at the latest version
Abstract
Antimicrobial resistance (AMR) is a public health problem exacerbated by the overuse and misuse of antibiotics and an inadequate capacity of laboratories to conduct AMR surveillance. This study assessed the capacity of laboratories in seven faith-based hospitals to conduct bacteriology, AMR testing and surveillance in Zambia. This multi-facility, cross-sectional exploratory study was conducted from February 2024 to April 2024. We collected and analysed data using the self-scoring Laboratory Assessment of Antibiotic Resistance Testing Capacity (LAARC) tool. This study found an overall score of 39%, indicating a low capacity of laboratories to conduct AMR surveillance. The highest capacity score was 47%, while the lowest was 25%. Only one hospital had full capacity (100%) to utilise a Laboratory Information System (LIS). Three hospitals had good capacity to perform data management with scores of 83%, 85%, and 95%. Only one hospital had full capacity (100%) to process specimens, and only one hospital had good safety requirements for a microbiology laboratory, with a score of 89%. This study demonstrates that all the assessed hospitals have a low capacity to conduct AMR surveillance. Therefore, there is an urgent need to strengthen the microbiology capacity of laboratories to enhance surveillance in faith-based hospitals in Zambia.
Keywords:
antimicrobial resistance
; bacteriology
; laboratory capacity
; surveillance
; Zambia
1. Introduction
Antimicrobial resistance (AMR) occurs when bacteria, viruses, fungi, and parasites do not respond to antimicrobial drugs in animals or humans, thereby allowing the organism to survive in the host despite exposure to sufficient doses [1,2,3]. Antimicrobial resistance (AMR) has been spreading extensively worldwide and remains a serious threat to public health globally [4,5]. The effects of AMR cut across health, environmental and economic paradigms, making its impact more pronounced [6,7,8]. This phenomenon has been worsened by a lack of surveillance and diagnostic systems, especially in low-income settings, where large quantities of antimicrobial agents are used [9,10,11]. With the problem expected to escalate, it is estimated that there will be 10 million deaths per year globally due to AMR [1,12].
The deficiency in laboratory capacity and systems to conduct AMR surveillance has been linked to many factors, including lack of funding, inadequate training of healthcare personnel, lack of training in antimicrobial stewardship (AMS), shortages of laboratory consumables, and a lack of necessary laboratory equipment [13]. Consequently, some laboratories in low-resource settings face challenges regarding infrastructure, technical issues, and behavioural change in implementing clinical bacteriology testing [14]. Additionally, evidence has shown that the role of laboratories in the surveillance of AMR is affected by the absence of antibiograms, a lack of quality management systems, a lack of proficiency testing, lack of guidelines and standard operating procedures (SOPs), among other challenges [6,14,15,16,17]. A study that was done at a teaching hospital in Ghana highlighted the importance of cumulative antibiograms in AMS programmes after its communication to clinicians and subsequent monitoring influenced prescribing indicators [18].
Strengthening laboratory surveillance of AMR is essential to address escalating drug-resistant infections [19,20,21]. Studies have shown an improvement in AMR surveillance after improving the capacity of laboratory testing [6,10,22]. Additionally, laboratory findings help clinicians to make decisions regarding the treatment of particular infections [13,23,24]. This promotes the principles of diagnostic stewardship through which laboratories contribute to the appropriate diagnosis and treatment of infections [25,26,27,28]. Hence, through diagnostic stewardship, antimicrobials are prescribed based on the right test, to the right patient, which prompts the right action, leading to efficient use of resources, improved use of antimicrobials, and a reduction in AMR [25,26,29]. However, there are some concerns about clinicians underutilizing clinical microbiology laboratory data when making clinical decisions [30]. Substantial investment has to be made to improve laboratory capacity to conduct AMR surveillance, especially in low-income and middle-income countries (LMICs), which have the highest burden of diseases [31,32].
Addressing AMR requires systematic instigation and implementation of AMS programs in healthcare facilities [33,34,35]. Through AMS programs, laboratory staff can be educated and trained in good laboratory practices that aim to promote the generation of high-quality and reliable test data, reduction in antimicrobial use, and reduction in AMR [18,36,37,38]. AMS programs can facilitate education and capacity building among laboratory scientists, leading to enhanced antimicrobial susceptibility testing (AST), enhanced culture and susceptibility reports, accurate rapid diagnostic testing, and improved alert and surveillance systems [39]. Furthermore, collaborations that foster action-oriented and multidisciplinary facility AMS programs can lead to the successful implementation of AMS activities [40,41]. Notably, AMS interventions lead to improved prescribing practices of antimicrobials and lead to improved patient outcomes [42,43,44,45,46].
Zambia is a country in the sub-Saharan African (SSA) region with a reportedly high burden of infectious diseases [47,48,49]. Consequently, the presence of drug-resistant pathogens in healthcare facilities has been reported in several studies [50,51,52,53,54,55,56,57,58]. The Antimicrobial Resistance Coordinating Committee (AMRCC) hosted at the Zambia National Public Health Institute (ZNPHI) has been promoting the establishment and strengthening of AMR surveillance across the country [59,60]. The ZNPHI has supported One Health AMR surveillance through the 2019 Zambia Integrated Surveillance Framework for Antimicrobial Resistance [59]. However, there is a paucity of information on the capacities of laboratories to conduct AMR surveillance in Zambia. Therefore, this study assessed the capacity to conduct bacteriology, AMR testing and surveillance in seven faith-based hospitals in the Zambia to contribute to available data on the subject. It was envisaged that the findings of this assessment would be used to strengthen AMR surveillance in faith-based hospital-affiliated laboratories in Zambia.
2. Results
This study enrolled seven faith-based hospitals in five provinces of Zambia. All the seven hospitals surveyed had physical laboratory infrastructure. However, they all scored below 50% regarding their ability to conduct basic medical bacteriology and capacity to test for AMR, indicating low capacity to conduct AMR surveillance (Figure 1). The overall score was 39%.
This study found that an average score of 41% was obtained for all the assessed indicators thereby demonstrating the low capacity of hospitals to conduct medical bacteriology and AMR testing (Figure 2). The hospitals scored low (0-48%) in 10 indicators while moderate (51-74%) in four indicators (Figure 2). Low scores (0-48%) were recorded by the assessed laboratories in 10 indicators while moderate scores (51-74%) in four indicators were recorded (Figure 2). The highest average score was 74% on data management with only St. Francis Mission Hospital (SFMH), (Macha Mission Hospital (MaMH), and Chikankata Mission Hospital (CMH) having performed well. All the surveyed hospitals scored 0% in quality control of ASTs (Figure 2). Only CMH performed well regarding the safety audit. Finally, only MMH had full capacity to run LIS and to conduct identification quality control (Figure 2). Individual facility scores are also shown in the Supplementary Material (S1).
3. Discussion
This study was a situation analysis involving a baseline assessment of the capacity of laboratories to conduct medical bacteriology, AMR testing and surveillance in faith-based hospitals in Zambia. We found that all seven faith-based hospitals exhibited limited capacity to conduct AMR surveillance, with an overall score of 39%. Additionally, an average score of 41% was recorded based on the indicators that were assessed. Despite having physical laboratory infrastructure across all seven hospitals, only three had good capacity to perform data management, only one hospital had a well-functioning LIS, and only one hospital met the safety standards required of a microbiology laboratory. Therefore, our findings demonstrated a strong need to strengthen the capacity of laboratories to perform bacteriology, AMR testing and surveillance.
Our study found a low capacity of faith-based hospital-affiliated laboratories to conduct medical bacteriology, AMR testing, and implementation of laboratory-based AMR surveillance in Zambia. Our findings are evidenced by the low overall score regarding the indicators used in assessing the capacity of laboratories to test for AMR and perform all bacteriological processes. These findings align with those reported in other studies [6,61,62]. A recent study conducted in Zambia in secondary and tertiary hospitals found an overall capacity of 52%, with the highest-scoring hospital having scored 63% and the lowest having scored 38% [63]. Another study in Burkina Faso found that an overall capacity to conduct AMR surveillance was 40% across 18 laboratories, with the highest laboratory scoring 58% and the lowest 26%, indicating a low capacity to conduct QMS and AMR surveillance [64]. The low capacity of laboratories to conduct bacteriological tests and AMR testing affects the surveillance of AMR. This problem affects many African countries [65]. In Africa, the lack of capacity of laboratories to conduct most microbiology tests affects the validity, usefulness, and trustworthiness of data generated from the surveillance systems [66].
The present study found that none of the surveyed laboratories had full capacity to test for AMR due to challenges including sub-optimum laboratory conditions, equipment unavailability, lack calibration and maintenance, inconsistent or lack of temperature monitoring, lack of an autoclave and inconsistent or absent inventory management. Our findings resonate with another study conducted in Ethiopia where, despite the availability of laboratories, there was a lack of basic equipment and consumables to conduct AMR testing [6]. Another study in Kenya reported similar findings where nearly one-third of the healthcare facilities examined did not offer bacterial culture testing, and only a meagre 16.9% conducted AST [61]. This was due to poor access to LIS, low participation in external quality assessment programs for cultures, severe infrastructural gaps and lack of equipment [61]. In Rwanda, critical gaps in equipment and supplies were found in district hospitals, similar to those found in our study [67]. Our findings and those reported in other African countries conform with earlier findings that there is a lack of proper reliable, cost-effective and easy-to-use AMR diagnostic tools, particularly in routine diagnostic laboratories [65,68]. Additionally, there are few reports of major testing gaps for AMR in other regions with currently available data comprehensively describing AMR trends [69]. These differences could be attributed to differences in the setup and development of healthcare systems, particularly those in the African region severely impacted by financial constraints and infrastructural challenges.
Our study revealed that only Mwandi Mission Hospital had full LIS capacity to run electronic data management systems. The rest of the surveyed hospitals could not run LIS, demonstrating a critical disadvantage in the processing and storage of information. Our findings corroborate those reported in Kenya, where most laboratories scored low on the LIS component of the indicators [61]. Evidence has shown that LIS is generally poor in most LMICs, affecting AMR surveillance [32]. Studies have reported that laboratories need to develop and implement their LIS to reduce identification errors, improve data security and protection, and promote the efficiency reported of results [70,71,72].
The current study found that only three hospitals, including Chikankata, St. Francis, and Macha Mission Hospitals had good data management capacity and scored well in patient and specimen identification, specimen requisition forms, order entry, culture observations, AST data reporting, data backup and security, and AMR data sharing. Hence, most hospitals in this study could not perform good data management. These findings were also echoed in a study in Ethiopia, where data capture and transmission challenges were cited as common problems in implementing AMR surveillance work [73]. Additionally, a comprehensive review underscored the necessity for prompt intervention to address the issues related to data infrastructure and financial stability [74]. This is crucial to maintain the effectiveness and sustainability of surveillance initiatives. Moreover, it has been established that data systems for AMR surveillance are essential for fostering unified public health measures and guaranteeing the distribution of sufficient feedback [74]. Our findings agree with a previous study done in Nepal, where data generated from facilities was inconsistent, incomplete and delayed, thereby causing challenges in data transmitted to the national level for action [22]. In contrast, a study in Ethiopia described effective data management after deliberate efforts to establish a surveillance system [75]. These differences could be due to an absence of systems for capturing AMR data.
Our study found that all the surveyed hospitals could not perform quality assurance, including the basics of the quality management system (QMS), staff competency assessments, troubleshooting mechanisms and external QA. Implementation of QMS dictates that health facilities align themselves to national and international requirements of quality assurance which eventually enables a culture of quality in all sectors of healthcare [17]. A study among 18 laboratories in Burkina Faso also reported a low performance of laboratories to conduct QMS and external QA [64]. Not surprisingly, our study found that all the surveyed hospitals could not perform media QC, identification QC, and AST QC. Similarly, a study in Togo had findings in which the AST QC was very low [76]. In contrast to our findings, a study conducted in Burkina Faso found that most (76.5%) facilities had a good capacity to conduct AST QC [64]. In keeping with the findings from the Burkina Faso study [64], a study conducted in Kenya reported good performances (≥80%) in QA and a score of 81.1% in AST QC was reported [61]. Intriguingly, evidence has shown that the implementation of QMS in laboratories enhances patient safety [77].
All the surveyed hospitals in the current study did not have the full capacity to implement bacteriological identification methods. The methods used were not supported by SOPs, protocols and flow charts. These findings are worrying because the lack of proper identification of microorganisms affects the management, treatment and control of infections [78]. The lack of SOPs, protocols, and flow charts has also been reported in other countries, especially in low-resource settings [14,16,17]. The implementation of clinical bacteriology improves patient management, provides valuable surveillance for local antibiotic treatment guidelines and supports the containment of AMR as well as the prevention and control of hospital-acquired infections [14]. Additionally, SOPs provide instructions on how to isolate and identify pathogens, assign bacteria to a specific group, interpretation of results, and recommend panels of antibiotics for AST for a particular pathogen [16,79]. Hence, gaps in basic identification methods and a lack of SOPs negatively affect the process of bacteriology. There is an urgent need to strengthen laboratory detection of pathogens through the strengthening of laboratory capacity to conduct bacteriology [78]. Therefore, the need for SOPs in bacteriological processes must be emphasized in maintaining the accuracy, consistency, and quality of data [79].
Our study revealed that none of the seven hospitals had the full capacity to perform maintenance of discs and strips, inoculum preparation, incubation, reading and interpreting results and breakpoints standards. Hence, this deficiency highlights the potential problems associated with adhering to the established guidelines provided by the Clinical and Laboratory Standards Institute (CLSI) and/or the European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints and AST expert rules for the priority pathogens. These challenges are mostly seen in LMIC where securing the supply chain and investing in adapted equipment, diagnostics, and reagents adapted to the environmental, logistic, and financial challenges is difficult to sustain [80]. In addition, none of the seven hospitals in the present study had the full capacity to perform specimen collection, transport, management, and processing of blood, urine, and stool cultures. Many studies have documented challenges in conducting routine bacteriological diagnostics and subsequent AST, mainly in low- and middle-income countries [13,69,73,75,81].
Our study found that only Chikankata Mission Hospital had a good capacity for the safety requirements of a microbiology laboratory that must be involved in AMR testing and surveillance. Zimba Mission Hospital was at borderline (79%) to attain good capacity regarding safety audits in the microbiology laboratory. Poor safety standards in laboratories have the potential to put laboratory workers at increased risk of contracting laboratory-acquired infections [82]. The challenges in biosafety and biosecurity have been documented in other countries, outlining the lack of safety assurance leading to unsafe handling of infectious materials in the laboratory [83,84]. Ultimately, this affected the implementation of AMR programs in health facilities and laboratories [85,86]. Our findings and those reported in other studies indicate the need to conduct frequent assessments and monitoring of biosafety and biosecurity in laboratories [87]. Hence, there is a critical need to strengthen biorisk management in laboratories to reduce and tackle infections [82,88].
We found that none of the seven assessed laboratories had an antibiogram. The absence of antibiograms creates a huge gap in promoting targeted antimicrobial treatment. Due to the absence of antibiograms in health institutions, it is not feasible to evaluate the extent of pathogen resistance to antimicrobials. Notably, the use of antibiograms enhances the rational use of antimicrobials and promotes AMS [18,89]. Additionally, antibiograms are used to detect and monitor current patterns in AMR [90]. Consequently, the lack of antibiograms in clinical laboratories can have substantial implications for patient treatment and public health. The significance of antibiograms in the presence of significant AMR in Gram-negative bacteria was underscored, focusing on their role in directing antibiotic treatment and managing multi-drug resistant organisms [91]. Notably, antibiograms are essential in enhancing AMS, infection control, and rational antimicrobial therapy [18,92]. A study in Ghana highlighted the importance of antibiograms’ ability to support empirical clinical decision-making and enhance infection prevention highlighting their value in laboratories [93].
The gaps identified in our study demonstrate the need to develop strategies that should be used to improve the surveillance of AMR in Zambia. In addition, none of the surveyed hospitals had an AMS committee to champion heightened AMR surveillance. Therefore, we believe setting up AMS teams is critical to improving the surveillance of AMR, similar to earlier publications [20,94,95,96,97,98,99,100]. Additionally, AMS and surveillance programs can help in capacity building and mentorship of laboratory personnel regarding microbiology and AMR surveillance [39]. Strengthening laboratory capacity to monitor and conduct AMR surveillance potentially reduces the development and spread of AMR [101,102,103].
We are aware that our study had limitations. First, this was a cross-sectional study relying on self-reporting by respondents and is prone to recall biases. Second, this study was conducted in faith-based hospitals. Hence, generalisation of the findings must be made with caution as the findings may not reflect what is obtained in public and private hospitals. Consequently, the study findings may not represent all the faith-based hospitals in Zambia as the study was done in five out of ten provinces in Zambia. However, our findings are vital and can be used to identify opportunities and gaps that can be leveraged on to strengthen AMR surveillance in faith-based hospitals in Zambia. Additionally, as a starting point to strengthen AMR testing and surveillance in the surveyed hospitals, the presence of a physical laboratory infrastructure in all seven hospitals is very cardinal.
4. Materials and Methods
4.1. Study Design, Period, and Setting
We conducted a cross-sectional exploratory study in seven faith-based hospitals in Zambia from February 2024 to April 2024. The hospitals are located in five different provinces as follows: Chikankata Mission Hospital (CMH) in the Chikankata District, Macha Mission Hospital (MaMH) in the Choma District, Zimba Mission Hospital (ZMH) in the Zimba District of the Southern Province; Mwandi Mission Hospital (MMH) in Mwandi District of the Western Province; St. Francis Mission Hospital (SFMH) in Katete District of the Eastern Province; St. Dominic’s Mission Hospital (SDMH) in Ndola District of the Copperbelt Province; and Mukinge Mission Hospital (MuMH) in Kasempa District of the Northwestern Province. These faith-based hospitals were chosen because they provide medical and surgical services to many Zambian people, largely in remote places (Figure 3). Additionally, the sites were chosen because they are under the ambit of the Churches Health Association of Zambia (CHAZ), which will strengthen the microbiology activities of these hospitals to help scale up their capacity to conduct bacteriology, AMR testing and surveillance. In our study, a faith-based hospital was defined as a hospital that is supported by or affiliated with a Christian religious group such as Catholics, Anglicans, Presbyterians, and Protestants.
4.2. Sample Size and Sampling Technique
We selected seven faith-based hospitals using the purposive sampling method to conduct a baseline assessment study on the capacity of laboratories to conduct basic medical bacteriology, AMR testing and surveillance. Purposive sampling has been used in studies similar to the current study because it helps collect comprehensive, specific information based on the study objectives [62,104]. We purposefully selected four key informants working in the microbiology section of the laboratory in the surveyed hospitals. This gave us a total of 28 key informants across the seven hospitals. The key informants included the laboratory manager, the quality control officer, and bench personnel.
4.3. Data Collection
Data were collected using a Microsoft Excel sheet version of the self-scoring Laboratory Assessment of Antibiotic Resistance Testing Capacity (LAARC) questionnaire [105]. The tool is validated and recommended by the Centers for Disease Control and Prevention (CDC) to be used for evaluating laboratories proficient in conducting bacteriologic techniques and other related quality processes that require accurate and reliable AMR detection and reporting [105]. The LAARC questionnaire has 15 modules, each containing 3 to 10 indicators. Additionally, each indicator contains closed-ended questions to which laboratory personnel respond [105].
The 15 modules include Module 0, called General (laboratory demographics, test menu and workload, ST/AMR workload and methods, laboratory staff education and training, QMS mentoring programs, and accreditation and certification); Module 1: Facility (laboratory facility, general equipment availability, media preparation equipment availability, equipment calibration records, thermometers, temperature and atmosphere monitoring, autoclave management, instrument availability and maintenance, and inventory and stock outs); Module 2: Laboratory Information System (LIS) (demographic data fields, specimen data fields, culture observation data fields, AST data fields, reports and data transfer capabilities, and interface connectivity); Module 3: Data Management (patient and specimen identification, specimen requisition form, order entry, culture observations, AST results reporting, data backup and security, and AMR data sharing); Module 4: Quality Assurance (QA) (quality structure/basics, laboratory staff education/training/competency, troubleshooting, problem solving, and route cause analyses, and external quality assessment (EQA); Module 5: Media Quality Control (QC Media) (media preparation SOPs, general media preparation, distilled/deionized water preparation, routine media QC, Mueller Hinton media preparation and QC, and blood culture bottles preparation and QC); Module 6: Identification QC (QC ID) (gram stain QC and reagent labeling and storage, QC of individual biochemical methods, QC of enteric serology, QC of commercial ID kids and automated ID systems); Module 7: Antimicrobial Sensitivity Testing QC (QC AST) (routine AST references strains, special AST reference strains, QC of disc diffusion methods, QC of gradient strip AST methods, and QC of automated AST systems); Module 8: Specimen (specimen management, specimen rejection, blood specimen collection and transportation, urine collection specimen and transportation, and stool specimen collection and transportation); Module 9: Processing (blood culture processing, manual blood culture systems, urine culture, stool cultures for Salmonella and Shigella); Module 10: Identification methods and Standard Operating Procedures; Module 11: Basic AST (antibiotic disc and gradient strips maintenance, inoculum preparation, inoculum/incubation, reading AST results, interpreting AST results, and breakpoints standards; Module 12: AST expert rules (expert rules for Salmonella, gram negatives and beta-lactams breakpoints, phenotypic ESBL testing, phenotypic carbapenamase testing, colistin testing, expert rules for Staphylococcus aureus, general considerations and expert rules for Streptococcus pneumoniae, inducible clindamycin resistance testing, and expert rules for cerebrospinal fluid); Module 13: AST policy (AST panels, cumulative antibiograms, and AST policy); and Module 14: Safety (biosafety equipment, personal protective equipment, biosafety behaviours, and biosafety documentation and training) [105].
A summary of the findings was prepared and the main findings were shared with the hospital management and laboratory staff. The data collection team paid a courtesy call to the hospital management and explained the purpose of the assessment. After that, the team visited the laboratory and interacted with laboratory staff regarding the purpose of their visit. The team toured the laboratory and reviewed documents including SOPs. The questionnaire was administered for two days (approximately eight hours per day) per facility by four data collectors, including two public health experts and two clinical microbiology experts. Since the facilities are sparsely distributed, data collection was done for 18 days, taking into consideration the travel days.
4.4. Data Analysis
The LAARC tool is a self-scoring tool; therefore, the data were entered into the LAARC tool for initial scoring based on each indicator. The minimum score was 0% and the maximum score was 100%. Low capacity to conduct basic medical bacteriology and test for AMR scored from 0-49%, moderate capacity was scored 50-79%, whereas good capacity was scored 80-100% [105]. All the charts were developed using Microsoft Excel version 2013. The overall scores for the hospitals were generated average was calculated to produce the overall capacity of the laboratory to conduct AMR surveillance. For the assessed indicators, the scores were aggregated for all hospitals and an average score was produced to indicate the capacity of laboratories to perform activities under that indicator. Scores of 0-49% meant that the laboratory needed significant improvement in conducting the activities under such indicators. Scores of 50-79% meant that some improvement was required, while scores of 80% and above were satisfactory.
5. Conclusions
This study demonstrates that the assessed hospitals had low capacity regarding testing and surveillance of AMR. The presence of a physical laboratory in all seven hospitals is very important to setting up and implementing AMR testing and surveillance. There is a need to strengthen all seven laboratories in the areas of laboratory conditions, equipment, LIS, data management, quality control, specimen collection and handling, pathogen identification methods, conducting of AST, and safety standards. These improvements could in turn improve diagnostic stewardship and patient outcomes. Additionally, this strategy can be extended to other laboratories across the country.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Microsoft Word Document S1.
Author Contributions
Conceptualization, DMS and SM; methodology, SM; software, SM; validation, DMS, SM, JS, JYC, JBM and KS; formal analysis, SM and JC; investigation, DMS, SM, MHK, MK (Mapeesho Kamayani), BY, and A.M.; resources, DMS and KS; data curation, DMS, SM, and KS; writing—original draft preparation, DMS and SM; writing—review and editing, DMS, SM, MK (Maisa Kasanga), VD, MHK, MK (Mapeesho Kamayani), JS, BY, CBK, RN, AM., FC, MN, BS, LM, JYC, JBM, RC and KS; visualization, DMS, SM, MK (Maisa Kasanga), VD, MHK, MK (Mapeesho Kamayani), JS, BY, CBK, RN, AM, FC, MN, BS, LM, JYC, JBM, RC and KS; supervision, DMS, SM, JC, JBM, RC and KS; project administration, DMS, SM and KS; funding acquisition, DMS and KS. All authors have read and agreed to the submitted version of the manuscript.
Funding
This research did not receive any external funding.
Institutional Review Board Statement
We obtained ethical approval from the Tropical Diseases Research Centre (TDRC) Ethics Committee with a protocol ID number TRC/C4/09/2023. All key informants were informed about the purpose of the study, and they provided informed and written consent to participate. Participation in this study was voluntary. Finally, we obtained clearance from the hospital management to collect data from the key informants and to check the performance of their laboratories in conducting bacteriology and AMR testing. This research was conducted ethically regarding privacy, confidentiality and respect for autonomy.
Informed Consent Statement
Written and Informed consent to conduct the interviews was obtained from the key informants. Additionally, written and informed consent to publish the findings of the study was obtained from the hospital management and the research participants.
Data Availability Statement
The data supporting the reported results can be made available on request from the corresponding author.
Acknowledgments
We are grateful to the Institutional Management across the seven hospitals for accepting our request to collect data from the institution.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tang, K.W.K.; Millar, B.C.; Moore, J.E. Antimicrobial Resistance (AMR). Br. J. Biomed. Sci. 2023, 80, 11387.
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and Economic Impact of Antibiotic Resistance in Developing Countries: A Systematic Review and Meta-Analysis. PLoS One 2017, 12, e0189621. [CrossRef]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [CrossRef]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial Resistance: A Global Multifaceted Phenomenon. Pathog. Glob. Health 2015, 109, 309. [CrossRef]
- Llor, C.; Bjerrum, L. Antimicrobial Resistance: Risk Associated with Antibiotic Overuse and Initiatives to Reduce the Problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [CrossRef]
- Beyene, A.M.; Andualem, T.; Dagnaw, G.G.; Getahun, M.; LeJeune, J.; Ferreira, J.P. Situational Analysis of Antimicrobial Resistance, Laboratory Capacities, Surveillance Systems and Containment Activities in Ethiopia: A New and One Health Approach. One Heal. 2023, 16, 100527. [CrossRef]
- Shrestha, P.; Cooper, B.S.; Coast, J.; Oppong, R.; Do Thi Thuy, N.; Phodha, T.; Celhay, O.; Guerin, P.J.; Wertheim, H.; Lubell, Y. Enumerating the Economic Cost of Antimicrobial Resistance per Antibiotic Consumed to Inform the Evaluation of Interventions Affecting Their Use. Antimicrob. Resist. Infect. Control 2018, 7, 98. [CrossRef]
- Aa, J.; Ab, U.; Cd, U. Upaganlawar AB, et Al. Impact of Antimicrobial Resistance in Health and Economic Outcomes: A Review. Adv. Pharmacol. Clin. Trials 2024, 9, 000234. [CrossRef]
- Matee, M.; Mshana, S.E.; Mtebe, M.; Komba, E.V.; Moremi, N.; Lutamwa, J.; Kapona, O.; Sekamatte, M.; Mboera, L.E.G. Mapping and Gap Analysis on Antimicrobial Resistance Surveillance Systems in Kenya, Tanzania, Uganda and Zambia. Bull. Natl. Res. Cent. 2023, 47, 12. [CrossRef]
- Trollip, A.; Gadde, R.; Datema, T.; Gatwechi, K.; Oskam, L.; Katz, Z.; Whitelaw, A.; Kinyanjui, P.; Njukeng, P.; Wendifraw, D.A.; et al. Implementation of a Customised Antimicrobial Resistance Laboratory Scorecard in Cameroon Ethiopia and Kenya. Afr. J. Lab. Med. 2022, 11, 1476. [CrossRef]
- Sartorius, B.; Gray, A.P.; Davis Weaver, N.; Robles Aguilar, G.; Swetschinski, L.R.; Ikuta, K.S.; Mestrovic, T.; Chung, E.; Wool, E.E.; Han, C.; et al. The Burden of Bacterial Antimicrobial Resistance in the WHO African Region in 2019: A Cross-Country Systematic Analysis. Lancet Glob. Heal. 2024, 12, e201–e216. [CrossRef]
- de Kraker, M.E.A.; Stewardson, A.J.; Harbarth, S. Will 10 Million People Die a Year Due to Antimicrobial Resistance by 2050? PLoS Med. 2016, 13, e1002184. [CrossRef]
- Malania, L.; Wagenaar, I.; Karatuna, O.; Tambic Andrasevic, A.; Tsereteli, D.; Baidauri, M.; Imnadze, P.; Nahrgang, S.; Ruesen, C. Setting up Laboratory-Based Antimicrobial Resistance Surveillance in Low- and Middle-Income Countries: Lessons Learned from Georgia. Clin. Microbiol. Infect. 2021, 27, 1409–1413.
- Ombelet, S.; Ronat, J.B.; Walsh, T.; Yansouni, C.P.; Cox, J.; Vlieghe, E.; Martiny, D.; Semret, M.; Vandenberg, O.; Jacobs, J.; et al. Clinical Bacteriology in Low-Resource Settings: Today’s Solutions. Lancet Infect. Dis. 2018, 18, e248–e258. [CrossRef]
- Mathew, P.; Ranjalkar, J.; Chandy, S.J. Challenges in Implementing Antimicrobial Stewardship Programmes at Secondary Level Hospitals in India: An Exploratory Study. Front. Public Heal. 2020, 8, 493904. [CrossRef]
- Karah, N.; Rafei, R.; Elamin, W.; Ghazy, A.; Abbara, A.; Hamze, M.; Uhlin, B.E. Guideline for Urine Culture and Biochemical Identification of Bacterial Urinary Pathogens in Low-Resource Settings. Diagnostics 2020, 10. [CrossRef]
- Barbé, B.; Yansouni, C.P.; Affolabi, D.; Jacobs, J. Implementation of Quality Management for Clinical Bacteriology in Low-Resource Settings. Clin. Microbiol. Infect. 2017, 23, 426–433. [CrossRef]
- Dakorah, M.P.; Agyare, E.; Acolatse, J.E.E.; Akafity, G.; Stelling, J.; Chalker, V.J.; Spiller, O.B.; Aidoo, N.B.; Kumi-Ansah, F.; Azumah, D.; et al. Utilising Cumulative Antibiogram Data to Enhance Antibiotic Stewardship Capacity in the Cape Coast Teaching Hospital, Ghana. Antimicrob. Resist. Infect. Control 2022, 11, 122. [CrossRef]
- Tornimbene, B.; Eremin, S.; Abednego, R.; Abualas, E.O.; Boutiba, I.; Egwuenu, A.; Fuller, W.; Gahimbare, L.; Githii, S.; Kasambara, W.; et al. Global Antimicrobial Resistance and Use Surveillance System on the African Continent: Early Implementation 2017–2019. Afr. J. Lab. Med. 2022, 11, 1–11. [CrossRef]
- Mudenda, S.; Chabalenge, B.; Daka, V.; Mfune, R.L.; Salachi, K.I.; Mohamed, S.; Mufwambi, W.; Kasanga, M.; Matafwali, S.K. Global Strategies to Combat Antimicrobial Resistance: A One Health Perspective. Pharmacol. Pharm. 2023, 14, 271–328. [CrossRef]
- Jacobs, J.; Hardy, L.; Semret, M.; Lunguya, O.; Phe, T.; Affolabi, D.; Yansouni, C.; Vandenberg, O. Diagnostic Bacteriology in District Hospitals in Sub-Saharan Africa: At the Forefront of the Containment of Antimicrobial Resistance. Front. Med. 2019, 6, 20. [CrossRef]
- Yadav, S.K.; Shrestha, L.; Acharya, J.; Gompo, T.R.; Chapagain, S.; Jha, R. Integrative Digital Tools to Strengthen Data Management for Antimicrobial Resistance Surveillance in the “One Health” Domain in Nepal. Trop. Med. Infect. Dis. 2023, 8. [CrossRef]
- Cantón, R. Role of Microbiology Laboratory in Infectious Disease Surveillance, Alert and Response. Clin. Microbiol. Infect. Suppl. 2005, 11, 3–8. [CrossRef]
- Perovic, O.; Schultsz, C. Stepwise Approach for Implementation of Antimicrobial Resistance Surveillance in Africa. Afr. J. Lab. Med. 2016, 5, 482. [CrossRef]
- Fabre, V.; Davis, A.; Diekema, D.J.; Granwehr, B.; Hayden, M.K.; Lowe, C.F.; Pfeiffer, C.D.; Sick-Samuels, A.C.; Sullivan, K. V.; Van Schooneveld, T.C.; et al. Principles of Diagnostic Stewardship: A Practical Guide from the Society for Healthcare Epidemiology of America Diagnostic Stewardship Task Force. Infect. Control Hosp. Epidemiol. 2023, 44, 178–185. [CrossRef]
- Morgan, D.J.; Malani, P.; Diekema, D.J. Diagnostic Stewardship - Leveraging the Laboratory to Improve Antimicrobial Use. JAMA - J. Am. Med. Assoc. 2017, 318, 607–608. [CrossRef]
- Dik, J.H.; Poelman, R.; Friedrich, A.W.; Niesters, H.G.M.; Rossen, J.W.A.; Sinha, B. Integrated Stewardship Model Comprising Antimicrobial, Infection Prevention, and Diagnostic Stewardship (AID Stewardship). J. Clin. Microbiol. 2017, 55, 3306–3307. [CrossRef]
- Patel, R.; Fang, F.C. Diagnostic Stewardship: Opportunity for a Laboratory-Infectious Diseases Partnership. Clin. Infect. Dis. 2018, 67, 799–801. [CrossRef]
- Dik, J.W.H.; Poelman, R.; Friedrich, A.W.; Panday, P.N.; Lo-Ten-Foe, J.R.; Assen, S. Van; Van Gemert-Pijnen, J.E.W.C.; Niesters, H.G.M.; Hendrix, R.; Sinha, B. An Integrated Stewardship Model: Antimicrobial, Infection Prevention and Diagnostic (AID). Future Microbiol. 2016, 11, 93–102. [CrossRef]
- Iregbu, K.C.; Osuagwu, C.S.; Umeokonkwo, C.D.; Fowotade, A.A.; Ola-Bello, O.I.; Nwajiobi-Princewill, P.I.; Taiwo, S.S.; Olayinka, A.T.; Oduyebo, O.O. Underutilization of the Clinical Microbiology Laboratory by Physicians in Nigeria. African J. Clin. Exp. Microbiol. 2019, 21, 53–59. [CrossRef]
- Yansouni, C.P.; Seifu, D.; Libman, M.; Alemayehu, T.; Gizaw, S.; Johansen, Ø.H.; Abebe, W.; Amogne, W.; Semret, M. A Feasible Laboratory-Strengthening Intervention Yielding a Sustainable Clinical Bacteriology Sector to Support Antimicrobial Stewardship in a Large Referral Hospital in Ethiopia. Front. Public Heal. 2020, 8, 258. [CrossRef]
- Turner, P.; Rupali, P.; Opintan, J.A.; Jaoko, W.; Feasey, N.A.; Peacock, S.J.; Ashley, E.A. Laboratory Informatics Capacity for Effective Antimicrobial Resistance Surveillance in Resource-Limited Settings. Lancet Infect. Dis. 2021, 21, e170–e174.
- Khadse, S.N.; Ugemuge, S.; Singh, C. Impact of Antimicrobial Stewardship on Reducing Antimicrobial Resistance. Cureus 2023, 15, e49935. [CrossRef]
- Agyare, E.; Acolatse, J.E.E.; Dakorah, M.P.; Akafity, G.; Chalker, V.J.; Spiller, O.B.; Schneider, K.A.; Yevutsey, S.; Aidoo, N.B.; Blankson, S.; et al. Antimicrobial Stewardship Capacity and Antibiotic Utilisation Practices in the Cape Coast Teaching Hospital, Ghana: A Point Prevalence Survey Study. PLoS One 2024, 19, e0297626. [CrossRef]
- Mudenda, S.; Chabalenge, B.; Daka, V.; Jere, E.; Sefah, I.; Wesangula, E.; Yamba, K.; Nyamupachitu, J.; Mugenyi, N.; Mustafa, Z.U.; et al. Knowledge, Awareness and Practices of Healthcare Workers Regarding Antimicrobial Use, Resistance and Stewardship in Zambia: A Multi-Facility Cross-Sectional Study. JAC-Antimicrobial Resist. 2024, 6, dlae076. [CrossRef]
- Gebretekle, G.B.; Mariam, D.H.; Abebe, W.; Amogne, W.; Tenna, A.; Fenta, T.G.; Libman, M.; Yansouni, C.P.; Semret, M. Opportunities and Barriers to Implementing Antibiotic Stewardship in Low and Middle-Income Countries: Lessons from a Mixed-Methods Study in a Tertiary Care Hospital in Ethiopia. PLoS One 2018, 13, e0208447. [CrossRef]
- Watson, K.J.; Trautner, B.; Russo, H.; Phe, K.; Lasco, T.; Pipkins, T.; Lembcke, B.; Al Mohajer, M. Using Clinical Decision Support to Improve Urine Culture Diagnostic Stewardship, Antimicrobial Stewardship, and Financial Cost: A Multicenter Experience. Infect. Control Hosp. Epidemiol. 2020, 41, 564–570. [CrossRef]
- Langford, B.J.; Seah, J.; Chan, A.; Downing, M.; Johnstone, J.; Matukas, L.M. Antimicrobial Stewardship in the Microbiology Laboratory: Impact of Selective Susceptibility Reporting on Ciprofloxacin Utilization and Susceptibility of Gram-Negative Isolates to Ciprofloxacin in a Hospital Setting. J. Clin. Microbiol. 2016, 54, 2343–2347. [CrossRef]
- Morency-Potvin, P.; Schwartz, D.N.; Weinstein, R.A. Antimicrobial Stewardship: How the Microbiology Laboratory Can Right the Ship. Clin. Microbiol. Rev. 2017, 30, 381–407. [CrossRef]
- O. Popoola, O. Implementing Antimicrobial Stewardship in Various Healthcare Settings. In Antimicrobial Stewardship [Working Title]; IntechOpen, 2023; pp. 1–22 ISBN 978-1-83769-091-6.
- Bhowmick, T.; Kirn, T.J.; Hetherington, F.; Takavarasha, S.; Sandhu, S.S.; Gandhi, S.; Narayanan, N.; Weinstein, M.P. Collaboration between an Antimicrobial Stewardship Team and the Microbiology Laboratory Can Shorten Time to Directed Antibiotic Therapy for Methicillin-Susceptible Staphylococcal Bacteremia and to Discontinuation of Antibiotics for Coagulase-Negative Stap. Diagn. Microbiol. Infect. Dis. 2018, 92, 214–219. [CrossRef]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; Mcneil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients. Cochrane Database Syst. Rev. 2017, 2017, CD003543. [CrossRef]
- Steinberg, D.I. Review: Interventions Improve Hospital Antibiotic Prescribing and Reduce Hospital Stay but Do Not Affect Mortality. Ann. Intern. Med. 2017, 166, JC59. [CrossRef]
- Valderrama-Rios, M.C.; Álvarez-Moreno, C.A.; Cortes, J.A. Interventions to Improve Antibiotic Use in Hospitals with Different Levels of Complexity in Colombia: Findings from a Before-and-After Study and Suggestions for the Future. Antibiotics 2023, 12, 867. [CrossRef]
- Crayton, E.; Richardson, M.; Fuller, C.; Smith, C.; Liu, S.; Forbes, G.; Anderson, N.; Shallcross, L.; Michie, S.; Hayward, A.; et al. Interventions to Improve Appropriate Antibiotic Prescribing in Long-Term Care Facilities: A Systematic Review. BMC Geriatr. 2020, 20, 237. [CrossRef]
- Gruber, M.M.; Weber, A.; Jung, J.; Strehlau, A.; Tsilimparis, N.; Draenert, R. The Impact of Antibiotic Stewardship Interventions and Patient Related Factors on Antibiotic Prescribing in a Vascular Surgical Department. Infection 2024, 52, 83–91. [CrossRef]
- Loevinsohn, G.; Hardick, J.; Sinywimaanzi, P.; Fenstermacher, K.Z.J.; Shaw-Saliba, K.; Monze, M.; Gaydos, C.A.; Rothman, R.E.; Pekosz, A.; Thuma, P.E.; et al. Respiratory Pathogen Diversity and Co-Infections in Rural Zambia. Int. J. Infect. Dis. 2021, 102, 291–298. [CrossRef]
- Fwoloshi, S.; Hines, J.Z.; Barradas, D.T.; Yingst, S.; Siwingwa, M.; Chirwa, L.; Zulu, J.E.; Banda, D.; Wolkon, A.; Nikoi, K.I.; et al. Prevalence of Severe Acute Respiratory Syndrome Coronavirus 2 Among Healthcare Workers-Zambia, July 2020. Clin. Infect. Dis. 2021, 73, e1321–e1328. [CrossRef]
- Lungu, P.; Kasapo, C.; Mihova, R.; Chimzizi, R.; Sikazwe, L.; Banda, I.; Mucheleng’anga, L.A.; Chanda-Kapata, P.; Kapata, N.; Zumla, A.; et al. A 10-Year Review of TB Notifications and Mortality Trends Using a Joint Point Analysis in Zambia - a High TB Burden Country. Int. J. Infect. Dis. 2022, 124, S30–S40. [CrossRef]
- Yamba, K.; Lukwesa-Musyani, C.; Samutela, M.T.; Kapesa, C.; Hang’ombe, M.B.; Mpabalwani, E.; Hachaambwa, L.; Fwoloshi, S.; Chanda, R.; Mpundu, M.; et al. Phenotypic and Genotypic Antibiotic Susceptibility Profiles of Gram-Negative Bacteria Isolated from Bloodstream Infections at a Referral Hospital, Lusaka, Zambia. PLOS Glob. Public Heal. 2023, 3, e0001414. [CrossRef]
- Mwansa, T.N.; Kamvuma, K.; Mulemena, J.A.; Phiri, C.N.; Chanda, W. Antibiotic Susceptibility Patterns of Pathogens Isolated from Laboratory Specimens at Livingstone Central Hospital in Zambia. PLOS Glob. Public Heal. 2022, 2, e0000623. [CrossRef]
- Bumbangi, F.N.; Llarena, A.-K.; Skjerve, E.; Hang’ombe, B.M.; Mpundu, P.; Mudenda, S.; Mutombo, P.B.; Muma, J.B. Evidence of Community-Wide Spread of Multi-Drug Resistant Escherichia Coli in Young Children in Lusaka and Ndola Districts, Zambia. Microorganisms 2022, 10, 1684. [CrossRef]
- Kasanga, M.; Mudenda, S.; Siyanga, M.; Chileshe, M.; Mwiikisa, M.J.; Kasanga, M.; Solochi, B.B.; Gondwe, T.; Kantenga, T.; L Shibemba, A.; et al. Antimicrobial Susceptibility Patterns of Bacteria That Commonly Cause Bacteremia at a Tertiary Hospital in Zambia. Future Microbiol. 2020, 15, 1735–1745. [CrossRef]
- Kasanga, M.; Kwenda, G.; Wu, J.; Kasanga, M.; Mwikisa, M.J.; Chanda, R.; Mupila, Z.; Yankonde, B.; Sikazwe, M.; Mwila, E.; et al. Antimicrobial Resistance Patterns and Risk Factors Associated with ESBL-Producing and MDR Escherichia Coli in Hospital and Environmental Settings in Lusaka, Zambia: Implications for One Health, Antimicrobial Stewardship and Surveillance Systems. Microorganisms 2023, 11, 1951. [CrossRef]
- Yamba, K.; Mudenda, S.; Mpabalwani, E.; Mainda, G.; Mukuma, M.; Samutela, M.T.; Lukwesa, C.; Chizimu, J.; Kaluba, C.K.; Mutalange, M.; et al. Antibiotic Prescribing Patterns and Carriage of Antibiotic-Resistant Escherichia Coli and Enterococcus Species in Healthy Individuals from Selected Communities in Lusaka and Ndola Districts, Zambia. JAC-Antimicrobial Resist. 2024, 6, dlae027. [CrossRef]
- Shawa, M.; Paudel, A.; Chambaro, H.; Kamboyi, H.; Nakazwe, R.; Alutuli, L.; Zorigt, T.; Sinyawa, T.; Samutela, M.; Chizimu, J.; et al. Trends, Patterns and Relationship of Antimicrobial Use and Resistance in Bacterial Isolates Tested between 2015–2020 in a National Referral Hospital of Zambia. PLoS One 2024, 19, e0302053. [CrossRef]
- Chileshe, C.; Shawa, M.; Phiri, N.; Ndebe, J.; Khumalo, C.S.; Nakajima, C.; Kajihara, M.; Higashi, H.; Sawa, H.; Suzuki, Y.; et al. Detection of Extended-Spectrum Beta-Lactamase (ESBL)-Producing Enterobacteriaceae from Diseased Broiler Chickens in Lusaka District, Zambia. Antibiotics 2024, 13, 259. [CrossRef]
- Kasanga, M.; Shempela, D.M.; Daka, V.; Mwikisa, M.J.; Sikalima, J.; Chanda, D.; Mudenda, S. Antimicrobial Resistance Profiles of Escherichia Coli Isolated from Clinical and Environmental Samples: Findings and Implications. JAC-Antimicrobial Resist. 2024, 6, dlae061. [CrossRef]
- 2020; 59. Republic of Zambia AMRCC Zambia’s Integrated Antimicrobial Resistance Surveillance Framework; 2020;
- 2017; 60. Government of the Republic of Zambia Multi-Sectoral National Action Plan on Antimicrobial Resistance; 2017;
- Moirongo, R.M.; Aglanu, L.M.; Lamshöft, M.; Adero, B.O.; Yator, S.; Anyona, S.; May, J.; Lorenz, E.; Eibach, D. Laboratory-Based Surveillance of Antimicrobial Resistance in Regions of Kenya: An Assessment of Capacities, Practices, and Barriers by Means of Multi-Facility Survey. Front. Public Heal. 2022, 10, 1003178. [CrossRef]
- Mao, S.; Soputhy, C.; Lay, S.; Jacobs, J.; Ku, G.M.; Chau, D.; Chhea, C.; Ir, P. The Barriers and Facilitators of Implementing a National Laboratory-Based AMR Surveillance System in Cambodia: Key Informants’ Perspectives and Assessments of Microbiology Laboratories. Front. Public Heal. 2023, 11, 1332423. [CrossRef]
- Yamba, K.; Chizimu, J.Y.; Mudenda, S.; Lukwesa, C.; Chanda, R.; Nakazwe, R.; Simunyola, B.; Shawa, M.; Kalungia, A.C.; Chanda, D.; et al. Assessment of Antimicrobial Resistance Laboratory-Based Surveillance Capacity of Hospitals in Zambia: Findings and Implications for System Strengthening. J. Hosp. Infect. 2024, 148, 129–137. [CrossRef]
- Zongo, E.; Dama, E.; Yenyetou, D.; Muhigwa, M.; Nikiema, A.; Dahourou, G.A.; Ouedraogo, A.S. On-Site Evaluation as External Quality Assessment of Microbiology Laboratories Involved in Sentinel Laboratory-Based Antimicrobial Resistance Surveillance Network in Burkina Faso. Antimicrob. Resist. Infect. Control 2024, 13, 3. [CrossRef]
- Musa, K.; Okoliegbe, I.; Abdalaziz, T.; Aboushady, A.T.; Stelling, J.; Gould, I.M. Laboratory Surveillance, Quality Management, and Its Role in Addressing Antimicrobial Resistance in Africa: A Narrative Review. Antibiotics 2023, 12, 1313.
- Okolie, O.J.; Igwe, U.; Ismail, S.U.; Ighodalo, U.L.; Adukwu, E.C. Systematic Review of Surveillance Systems for AMR in Africa. J. Antimicrob. Chemother. 2023, 78, 31–51. [CrossRef]
- Umutesi, G.; Velin, L.; Muwanguzi, M.; Faktor, K.; Mugabo, C.; Rukundo, G.; Rucogoza, A.; Yankurije, M.; Mazimpaka, C.; Gatete, J.D.D.; et al. Strengthening Antimicrobial Resistance Diagnostic Capacity in Rural Rwanda: A Feasibility Assessment. Ann. Glob. Heal. 2021, 87, 1–13. [CrossRef]
- Gulumbe, B.H.; Haruna, U.A.; Almazan, J.; Ibrahim, I.H.; Faggo, A.A.; Bazata, A.Y. Combating the Menace of Antimicrobial Resistance in Africa: A Review on Stewardship, Surveillance and Diagnostic Strategies. Biol. Proced. Online 2022, 24, 19.
- Gajic, I.; Kabic, J.; Kekic, D.; Jovicevic, M.; Milenkovic, M.; Mitic Culafic, D.; Trudic, A.; Ranin, L.; Opavski, N. Antimicrobial Susceptibility Testing: A Comprehensive Review of Currently Used Methods. Antibiotics 2022, 11, 427. [CrossRef]
- Mtonga, T.M.; Choonara, F.E.; Espino, J.U.; Kachaje, C.; Kapundi, K.; Mengezi, T.E.; Mumba, S.L.; Douglas, G.P. Design and Implementation of a Clinical Laboratory Information System in a Low-Resource Setting. Afr. J. Lab. Med. 2019, 8, 2225–2002. [CrossRef]
- Lukić, V. Laboratory Information System-Where Are We Today? J. Med. Biochem. 2017, 36, 220–224. [CrossRef]
- Kammergruber, R.; Durner, J. Laboratory Information System and Necessary Improvements in Function and Programming. J. Lab. Med. 2018, 42, 277–287. [CrossRef]
- Ibrahim, R.A.; Teshale, A.M.; Dinku, S.F.; Abera, N.A.; Negeri, A.A.; Desta, F.G.; Seyum, E.T.; Gemeda, A.W.; Keficho, W.M. Antimicrobial Resistance Surveillance in Ethiopia: Implementation Experiences and Lessons Learned. Afr. J. Lab. Med. 2018, 7, 2225–2002. [CrossRef]
- Do, P.C.; Assefa, Y.A.; Batikawai, S.M.; Reid, S.A. Strengthening Antimicrobial Resistance Surveillance Systems: A Scoping Review. BMC Infect. Dis. 2023, 23, 593. [CrossRef]
- Hazim, C.; Abubeker Ibrahim, R.; Westercamp, M.; Belete, G.A.; Amare Kibret, B.; Kanter, T.; Yimer, G.; Adem, T.S.; Stevenson, K.B.; Urrego, M.; et al. Establishment of a Sentinel Laboratory-Based Antimicrobial Resistance Surveillance Network in Ethiopia. Heal. Secur. 2018, 16, S30–S36. [CrossRef]
- Katawa, G.; Adziyno Agbemanyole, K.; Nguepou Tchopba, C.; Ataba, E.; Oukoé Amessoudji, M.; Adjoa Ameyapoh, H.; Edlom Tchadié, P.; Fagdéba Bara, D.; Karou, D.; Ameyapoh, Y. Antimicrobial Susceptibility Testing: Evaluation of the Conformity of 3 Medical Bacteriology Laboratories of Togo According to EUCAST/CA-SFM Guidelines. J. Appl. Biosci. 2021, 162, 16795–16803. [CrossRef]
- Allen, L.C. Role of a Quality Management System in Improving Patient Safety - Laboratory Aspects. Clin. Biochem. 2013, 46, 1187–1193. [CrossRef]
- Owusu, M.; Nkrumah, B.; Acheampong, G.; Mensah, E.K.; Komei, A.A.K.; Sroda, F.K.; David, S.; Emery, S.; Robinson, L.M.; Asante, K.; et al. Improved Detection of Microbiological Pathogens: Role of Partner and Non-Governmental Organizations. BMC Infect. Dis. 2021, 21, 303. [CrossRef]
- Barbé, B.; Verdonck, K.; Mukendi, D.; Lejon, V.; Lilo Kalo, J.R.; Alirol, E.; Gillet, P.; Horié, N.; Ravinetto, R.; Bottieau, E.; et al. The Art of Writing and Implementing Standard Operating Procedures (SOPs) for Laboratories in Low-Resource Settings: Review of Guidelines and Best Practices. PLoS Negl. Trop. Dis. 2016, 10, e0005053. [CrossRef]
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Hardcastle, T.C.; Haque, M.; Lugova, H.; Dhingra, S.; Sharma, P.; Islam, S.; et al. Surveillance of Antimicrobial Resistance in Low- and Middle-Income Countries: A Scattered Picture. Antimicrob. Resist. Infect. Control 2021, 10, 63.
- Chaplain, D.; Asutaku, B. Ben; Mona, M.; Bulafu, D.; Aruhomukama, D. The Need to Improve Antimicrobial Susceptibility Testing Capacity in Ugandan Health Facilities: Insights from a Surveillance Primer. Antimicrob. Resist. Infect. Control 2022, 11, 23. [CrossRef]
- Peng, H.; Bilal, M.; Iqbal, H.M.N. Improved Biosafety and Biosecurity Measures and/or Strategies to Tackle Laboratory-Acquired Infections and Related Risks. Int. J. Environ. Res. Public Health 2018, 15, 2697. [CrossRef]
- Sodjinou, V.D.; Ayelo, P.A.; Achade, A.G.A.; Affolabi, D.; Ouendo, D.E.M. Assessment of the Biosafety and Biosecurity in the Reference Veterinary Laboratory of Parakou in Benin. Trop. Med. Infect. Dis. 2021, 6, 146. [CrossRef]
- Mouillé, B.; Dauphin, G.; Wiersma, L.; Blacksell, S.D.; Claes, F.; Kalpravidh, W.; Kabore, Y.; Hietala, S. A Tool for Assessment of Animal Health Laboratory Safety and Biosecurity: The Safety Module of the Food and Agriculture Organization’s Laboratory Mapping Tool. Trop. Med. Infect. Dis. 2018, 3, 33. [CrossRef]
- Rutebemberwa, E.; Aku, F.Y.; Al Zein, E.I.K.; Bellali, H. Reasons for and Barriers to Biosafety and Biosecurity Training in Health-Related Organizations in Africa, Middle East and Central Asia: Findings from GIBACHT Training Needs Assessments 2018-2019. Pan Afr. Med. J. 2020, 37, 1–14. [CrossRef]
- Odetokun, I.A.; Jagun-Jubril, A.T.; Onoja, B.A.; Wungak, Y.S.; Raufu, I.A.; Chen, J.C. Status of Laboratory Biosafety and Biosecurity in Veterinary Research Facilities in Nigeria. Saf. Health Work 2017, 8, 49–58. [CrossRef]
- Orelle, A.; Nikiema, A.; Zakaryan, A.; Albetkova, A.A.; Keita, M.S.; Rayfield, M.A.; Peruski, L.F.; Pierson, A. A Multilingual Tool for Standardized Laboratory Biosafety and Biosecurity Assessment and Monitoring. Heal. Secur. 2022, 20, 488–496. [CrossRef]
- Dama, E.; Orelle, A.; Nikiema, A.; Mandingar, P.D.; Naby, A.; Bationo, G.B.; Kéita, M.S.; Pierson, A.; Sawadogo, C.; Koné, R.G. Strengthening Biorisk Management Capacities in Burkina Faso: Contribution of the Global Health Security Agenda. Heal. Secur. 2022, 20, 479–487. [CrossRef]
- Klinker, K.P.; Hidayat, L.K.; DeRyke, C.A.; DePestel, D.D.; Motyl, M.; Bauer, K.A. Antimicrobial Stewardship and Antibiograms: Importance of Moving beyond Traditional Antibiograms. Ther. Adv. Infect. Dis. 2021, 8, 20499361211011372. [CrossRef]
- Var, S.K.; Hadi, R.; Khardori, N.M. Evaluation of Regional Antibiograms to Monitor Antimicrobial Resistance in Hampton Roads, Virginia. Ann. Clin. Microbiol. Antimicrob. 2015, 14, 22. [CrossRef]
- Roth, B.M.; Laps, A.; Yamba, K.; Heil, E.L.; Johnson, J.K.; Stafford, K.; Hachaambwa, L.M.; Kalumbi, M.; Mulenga, L.; Patel, D.M.; et al. Antibiogram Development in the Setting of a High Frequency of Multi-Drug Resistant Organisms at University Teaching Hospital, Lusaka, Zambia. Antibiotics 2021, 10, 782. [CrossRef]
- Darboe, S.; Mirasol, R.; Adejuyigbe, B.; Muhammad, A.K.; Nadjm, B.; De St. Maurice, A.; Dogan, T.L.; Ceesay, B.; Umukoro, S.; Okomo, U.; et al. Using an Antibiogram Profile to Improve Infection Control and Rational Antimicrobial Therapy in an Urban Hospital in The Gambia, Strategies and Lessons for Low- and Middle-Income Countries. Antibiotics 2023, 12, 790. [CrossRef]
- Truong, W.R.; Hidayat, L.; Bolaris, M.A.; Nguyen, L.; Yamaki, J. The Antibiogram: Key Considerations for Its Development and Utilization. JAC-Antimicrobial Resist. 2021, 3, dlab060. [CrossRef]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C. What Is Antimicrobial Stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798.
- Mendelson, M.; Morris, A.M.; Thursky, K.; Pulcini, C. How to Start an Antimicrobial Stewardship Programme in a Hospital. Clin. Microbiol. Infect. 2020, 26, 447–453. [CrossRef]
- Shamseddine, J.; Sadeq, A.; Yousuf, K.; Abukhater, R.; Yahya, L.O.; Espil, M.A.; Hassan, M.E.; Fadl, R.E.; Ahmed, R.T.E.; Elkonaissi, I.; et al. Impact of Antimicrobial Stewardship Interventions on Days of Therapy and Guideline Adherence: A Comparative Point-Prevalence Survey Assessment. Front. Trop. Dis. 2023, 3, 1050344. [CrossRef]
- Chukwu, E.E.; Abuh, D.; Idigbe, I.E.; Osuolale, K.A.; Chuka-Ebene, V.; Awoderu, O.; Audu, R.A.; Ogunsola, F.T. Implementation of Antimicrobial Stewardship Programs: A Study of Prescribers’ Perspective of Facilitators and Barriers. PLoS One 2024, 19, e0297472. [CrossRef]
- Tahoon, M.A.; Khalil, M.M.; Hammad, E.; Morad, W.S.; Awad, S.M.; Ezzat, S. The Effect of Educational Intervention on Healthcare Providers’ Knowledge, Attitude, & Practice towards Antimicrobial Stewardship Program at, National Liver Institute, Egypt. Egypt. Liver J. 2020, 10, 5. [CrossRef]
- Al-Omari, A.; Al Mutair, A.; Alhumaid, S.; Salih, S.; Alanazi, A.; Albarsan, H.; Abourayan, M.; Al Subaie, M. The Impact of Antimicrobial Stewardship Program Implementation at Four Tertiary Private Hospitals: Results of a Five-Years Pre-Post Analysis. Antimicrob. Resist. Infect. Control 2020, 9, 95. [CrossRef]
- Siachalinga, L.; Mufwambi, W.; Lee, I.-H. Impact of Antimicrobial Stewardship Interventions to Improve Antibiotic Prescribing for Hospital Inpatients in Africa: A Systematic Review and Meta-Analysis. J. Hosp. Infect. 2022, 129, 124–143.
- Cui, Y.; Liu, J.; Zhang, X. Effects of Laboratory Capabilities on Combating Antimicrobial Resistance, 2013–2016: A Static Model Panel Data Analysis. J. Glob. Antimicrob. Resist. 2019, 19, 116–121. [CrossRef]
- Eliopoulos, G.M.; Schwaber, M.J.; Carmeli, Y. An Ongoing National Intervention to Contain the Spread of Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2014, 58, 697–703. [CrossRef]
- Lesho, E.P.; Waterman, P.E.; Chukwuma, U.; McAuliffe, K.; Neumann, C.; Julius, M.D.; Crouch, H.; Chandrasekera, R.; English, J.F.; Clifford, R.J.; et al. The Antimicrobial Resistance Monitoring and Research (ARMoR) Program: The US Department of Defense Response to Escalating Antimicrobial Resistance. Clin. Infect. Dis. 2014, 59, 390–397. [CrossRef]
- Goddard, L.; Wozniak, T.M. Antimicrobial Resistance Surveillance to Support Decision-Making in a High-Prevalence Region: An Evaluation. Front. Trop. Dis. 2021, 2, 772491. [CrossRef]
- Centers for Disease Control and Prevention Laboratory Assessment of Antibiotic Resistance Testing Capacity. Centers Dis. Control Prev. 2020, 1–91.
Figure 1.
Overall capacity to conduct bacteriology, testing for antimicrobial resistance and surveillance among faith-based hospitals in Zambia.
Figure 1.
Overall capacity to conduct bacteriology, testing for antimicrobial resistance and surveillance among faith-based hospitals in Zambia.
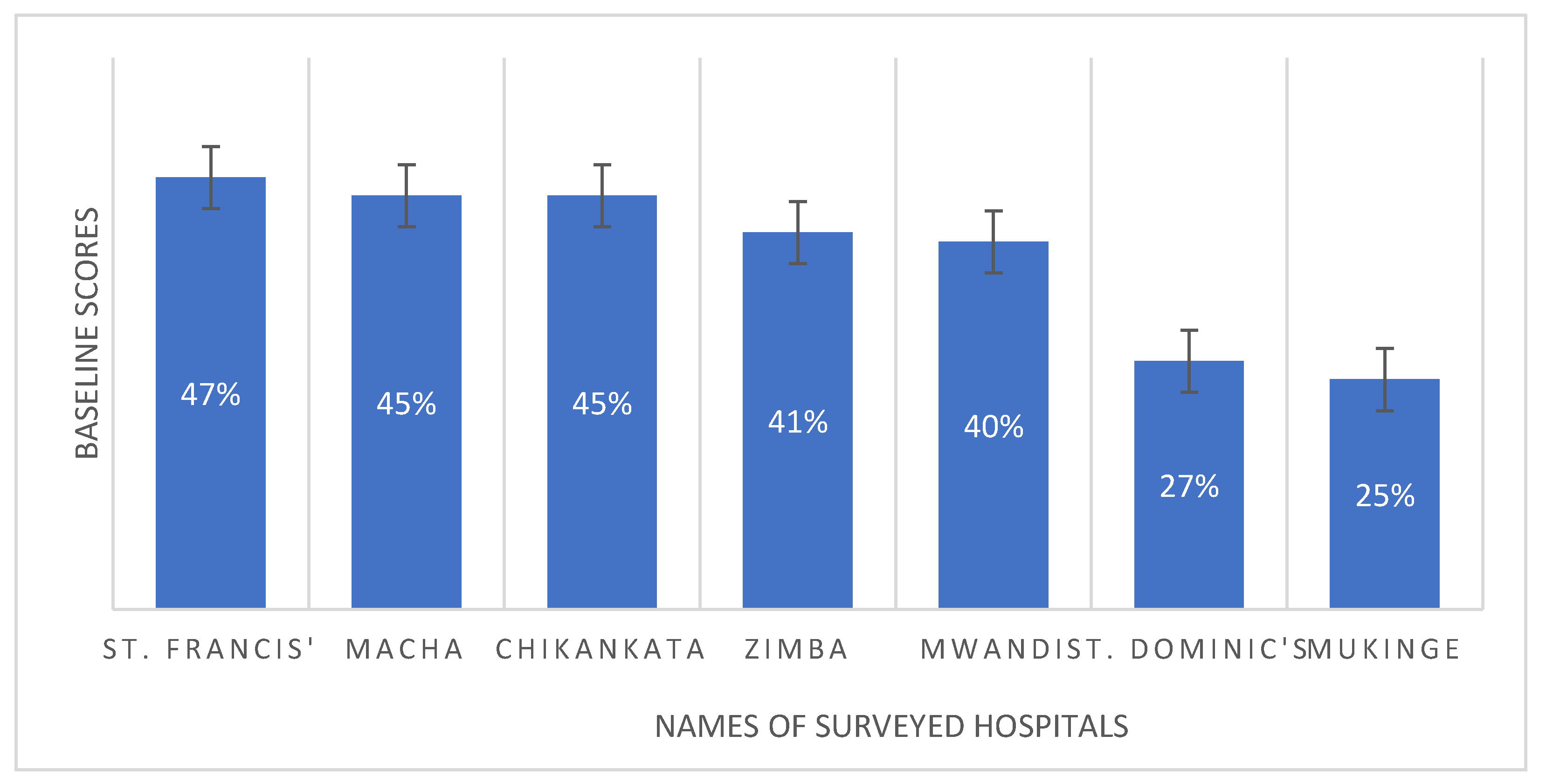
Figure 2.
Baseline scores of hospitals regarding their capacity to conduct basic medical bacteriology and AMR testing based on the assessed indicators. Note: ZMH = Zimba Mission Hospital, SFMH = St. Francis Mission Hospital, MMH = Macha Mission Hospital, CMH = Chikankata Mission Hospital, MMH = Mwandi Mission Hospital, MuMH = Mukinge Mission Hospital, and SDMH = St. Dominic’s Mission Hospital.
Figure 2.
Baseline scores of hospitals regarding their capacity to conduct basic medical bacteriology and AMR testing based on the assessed indicators. Note: ZMH = Zimba Mission Hospital, SFMH = St. Francis Mission Hospital, MMH = Macha Mission Hospital, CMH = Chikankata Mission Hospital, MMH = Mwandi Mission Hospital, MuMH = Mukinge Mission Hospital, and SDMH = St. Dominic’s Mission Hospital.
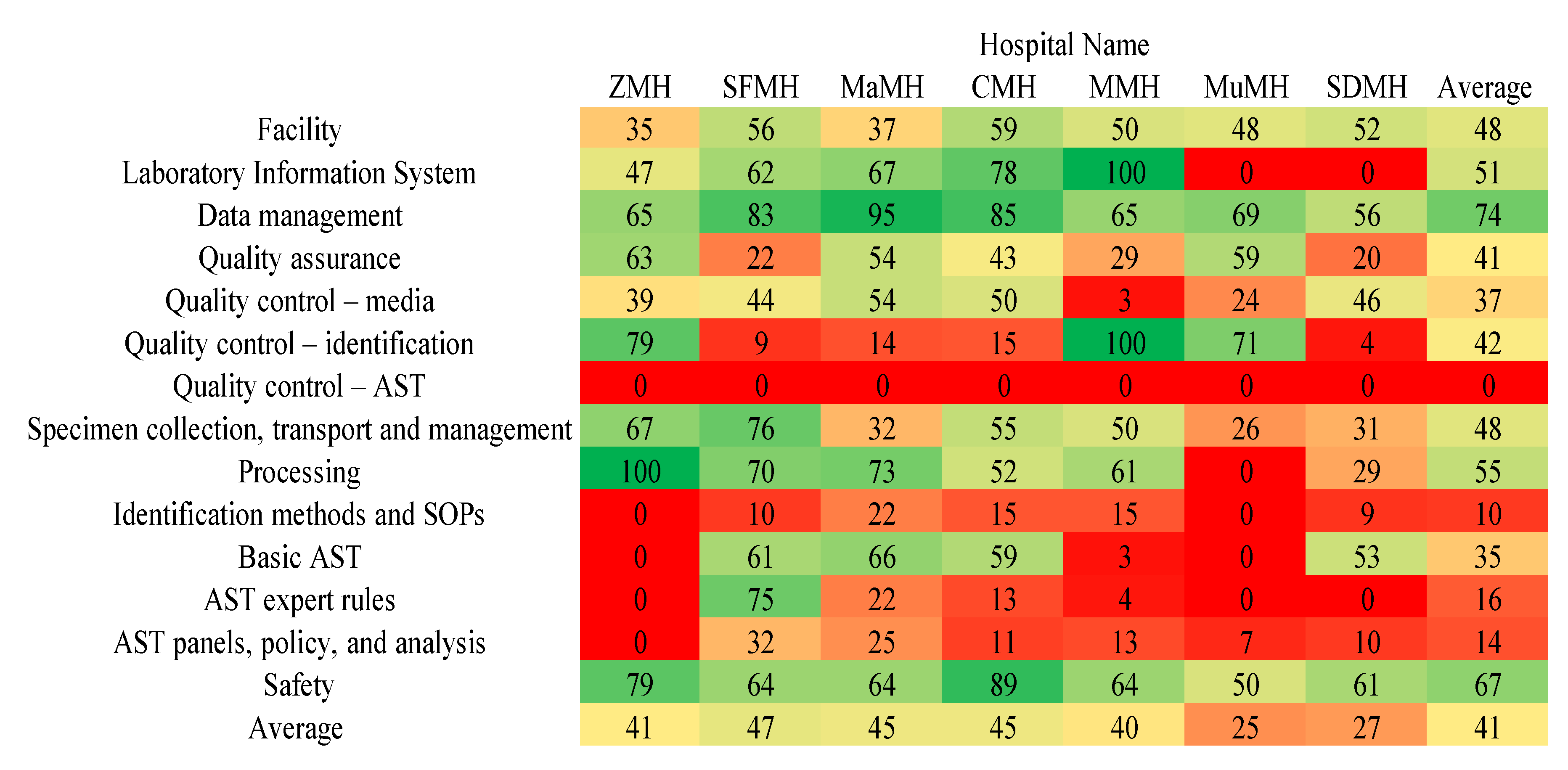
Figure 3.
Map of Zambia showing the location of faith-based health facilities included in the baseline assessment study.
Figure 3.
Map of Zambia showing the location of faith-based health facilities included in the baseline assessment study.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



