Submitted:
29 May 2024
Posted:
30 May 2024
You are already at the latest version
Abstract
Although the neurofilament light chain (NfL) is used as a biomarker for neurodegenerative decline, its use in surgery- and anaesthesia-induced acute cognitive dysfunction remains controversial. We aimed to synthesise the evidence to explore the potential of NfL as an established biomarker for perioperative neurocognitive disorders (PND). We systematically searched the PubMed, EMBASE, MEDLINE, Cochrane Library electronic databases, and Cochrane Central Registry of Clinical Trials. Our results show that CSF NfL levels positively correlated with blood NfL levels (r = 0.63; 95% confidence interval [CI], 0.42-0.77). The pooled standardised mean difference (SMD) showed a significantly higher preoperative CSF NfL levels (SMD = 0.27; 95% CI, 0.07-0.47) and both pre- and postoperative blood NfL levels (SMD = 0.53, 95% CI, 0.40-0.66 and SMD = 0.58, 95% CI, 0.43-0.73) in the postoperative delirium (POD) group. Postoperative blood NfL levels were significantly elevated in both POD group (SMD = 0.49; 95% CI, 0.34-0.64) and no-POD group (SMD = 0.67; 95% CI, 0.53-0.81). Our meta-analysis indicates that NfL may serve as a potential biomarker for POD, and elevated preoperative blood NfL levels could be a risk factor for POD. Further studies are needed to confirm the association of CSF/blood NfL levels with other PND types.
Keywords:
perioperative neurocognitive disorders
; postoperative delirium
; neurofilament light chain
; biomarker
; meta-analysis
1. Introduction
Postoperative cognitive dysfunction (POCD), a cognitive change that occurs following anaesthesia and surgery, has been widely studied for several decades [1,2]. However, due to the lack of unified clinical diagnostic criteria, relevant clinical management and research findings have not been widely acknowledged in related disciplines and fields [3]. POCD was/is an outcome defined by a decreased performance in one or more neuropsychological test usually from a battery of tests. POCD has no subjective or functional component, unlike perioperative neurocognitive disorders (PND) which aligns with Diagnostic and Statistical Manual of Mental Disorders (DSM) V criteria for cognitive disorders. In 2018, a multispecialty working group recommended the use of PND as an overarching term for cognitive impairment identified in the preoperative or postoperative period, including pre-existing cognitive impairment, postoperative delirium (POD), delayed neurocognitive recovery (DNR), and POCD [4]. This clinical nomenclature aims to offer a more precise management of PND, thereby enhancing the consistency of standards for prediction, diagnosis, and treatment.
The prognosis and diagnosis of PND still rely on complex neuropsychological measurements as insufficient evidence supports the use of any biomarker as the sole risk or disease marker for PND [5,6]. Predicting which patients will experience adverse cognitive events during surgery remains challenging [7]. Blood biomarkers of neuronal injury can provide insights into the importance of preoperative vulnerability and perioperative neuronal injury in the pathogenesis of PND [8,9]. With emerging evidence suggesting that neuronal injury plays a role in the pathophysiology of PND, the fluid biomarkers of neuronal injury have been increasingly studied [10,11]. With the development of ultrasensitive immunoassays, additional markers of neuronal injury measurable in the blood have emerged and are under investigation [12]. Neurofilament light chain (NfL) is a structural filament protein of the neuronal cytoskeleton that is released into the cerebrospinal fluid (CSF) and blood following axonal damage [13]. It is a sensitive marker for neuroaxonal injury, increasing shortly after and corresponding to the intensity of the brain insult or disease activity, with a strong correlation between CSF and blood in patients with various brain disorders [14,15,16].
Observational studies have suggested that blood NfL concentrations increase following traumatic brain injury [17] and perioperative ischaemic brain injury [18], and are higher in patients with chronic neurological diseases [19]. Unlike neurodegenerative diseases, PND demonstrate a more acute response to neurodegeneration, neuroinflammation, and neuronal injury due to surgery and anaesthesia, rather than chronic neurodegeneration [20]. Changes in CSF/blood NfL levels have also been observed in response to surgery and anaesthesia, suggesting a potential association between NfL and PND as measured by biomarkers during the perioperative period [21].
Recent studies have found that elevated CSF/blood NfL levels are associated with postoperative cognitive changes [22,23]. However, these results have been inconsistent, with opposing results observed under similar experimental conditions and designs [22,24]. Consequently, we performed a meta-analysis of the relationship between CSF/blood NfL levels and PND to determine the predictive and diagnostic value of NfL for this condition and summarise the correlation between NfL levels in CSF and blood in surgical patients based on existing studies. We aimed to provide evidence that NfL in blood could serve as a biomarker for incident PND.
2. Materials and Methods
The study protocol is registered in the PROSPERO database (CRD42024516907). All analyses were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the Cochrane Handbook for Systematic Reviews of Interventions [25].
2.1. Data Sources and Search Strategy
This meta-analysis focused on published studies investigating CSF/blood NfL levels and PND. Two independent reviewers searched the PubMed, EMBASE, MEDLINE, Cochrane Library electronic databases, and Cochrane Central Registry of Clinical Trials up to March 2024. The search terms combined text words and medical subject headings (MeSH) terms.
In PubMed, we used the search syntax: ((“neurofilament protein light”[MeSH Terms]) OR (“Neurofilament Light Chain”[Title/Abstract]) OR (“Neurofilament Light”[Title/Abstract]) OR (“NF-L polypeptide”[Title/Abstract]) OR (“NEFL protein”[Title/Abstract]) OR (“NEFL polypeptide”[Title/Abstract]) OR (“NF-L protein” [Title/Abstract]) OR (“light neurofilament protein”[Title/Abstract]) OR (“neurofilament light polypeptide”[Title/Abstract]) OR (“NEFL protein, human”[Title/Abstract]) OR (“NF68 protein, human”[Title/Abstract]) OR (“Neurofilament triplet L protein, human”[Title/Abstract]) OR (“neurofilament, light polypeptide 68kDa protein, human”[Title/Abstract]) OR (“CMT1F protein, human”[Title/Abstract]) OR (“CMT2E protein, human”[Title/Abstract])) AND ((perioperative neurocognitive disorders[MeSH Terms]) OR (pre-existing cognitive impairment[MeSH Terms]) OR (postoperative delirium [MeSH Terms]) OR (delayed neurocognitive recovery[MeSH Terms]) OR (postoperative cognitive dysfunction[MeSH Terms])), and the finalised PubMed database search strategy was adapted to fit the syntax and subject heading specifications of other databases. All relevant articles and abstracts were reviewed. In addition, references cited within relevant reviews were retrieved manually, and only full articles were searched.
2.2. Eligibility Criteria
Observational studies, such as cohort, case-control, and cross-sectional studies, were included. The original studies measured CSF/blood NfL levels in subjects with and without PND.
The inclusion criteria were as follows: 1) studies including PND subjects and no-PND control subjects; 2) human subjects; and 3) used standardized PND screening tools or diagnostic assessments.
Studies were excluded if: 1) case reports, review articles, or duplicate publications; 2) studies without outcome data; 3) the trials did not group the results according to PND status; and 4) they were not published in English.
2.3. Study Selection
Study selection was completed by two independent reviewers by screening the abstracts and titles of all included papers from the literature search. They removed duplicates and examined all references for their relevance based on their abstracts. Subsequently, accessed full-text articles and further screened them against the specific inclusion and exclusion criteria. All screenings were independently performed by two investigators, and disagreements were resolved by consensus or by a third reviewer.
2.4. Data Extraction
Three independent evaluators examined each of the retrieved articles. Disagreements between the reviewers were resolved by consensus. The following quantitative data were extracted from the included studies: means and standard deviations (SDs) of NfL and sample sizes of PND cases and controls. For studies that only reported the median, minimum, and maximum values and/or the interquartile ranges (IQRs), the means and SDs were estimated from these quantities using the formulae proposed by Wan and colleagues [26]. If the data were presented in a format in which the mean and SD were not extractable, these measures were requested from the corresponding author of the publication. When the mean (SD) value of biomarker levels could not be provided by the authors, but data were available in the articles in graph format, values were extracted using Engauge Digitiser software 11.3, an open-source software that can extract digital data from a graph to transform the information in the curves.
2.5. Quality Score Evaluation
Three authors independently assessed the quality of the included studies using the Newcastle–Ottawa Scale (NOS) which was used to assess the risk of bias by determining the quality of the observational studies selected using two independent scales (for cohort and case-control studies) [27]. The scale consists of items divided into three domains: selection, comparison, and exposure (case-control studies) or outcome (cohort studies). Scores of 0–3 were classified as low quality, 4–6 as medium quality, and 7–9 as high quality.
2.6. Statistical Analysis
The meta-analysis was performed using STATA version 16 (StataCorp LP), by two reviewers. For continuous variables, we assessed the available data by pooling them to estimate the mean difference using a random effects model, along with a 95% confidence interval (CI) and prediction intervals. We extracted Pearson’s correlation coefficients (r) and Spearman’s correlation coefficients (rs) from each study and conducted a meta-analysis of the correlation between CSF and blood NfL levels. WPS software transformed the correlation coefficient [r = 2sin(rsπ/6)] [28]. After converting r into Fisher’s Z and standard error (SE), the final effect size was calculated as the pooled r value and 95% CI. Odds ratios (ORs) of the included studies were combined using a random effects model. Sensitivity analyses were performed using a leave-one-out approach to assess the impact of each study on the overall estimated effect size. Between-study heterogeneity was estimated using the I2 statistic. We assessed the potential for small study bias by conducting Egger’s test.
3. Results
3.1. Study Selection
We identified 1891 studies, with 1489 studies remaining after removing duplicates. After screening the titles and abstracts, 624 studies were found to be potentially eligible. Finally, 12 studies [22,24,29,30,31,32,33,34,35,36,37,38] were selected based on the exclusion criteria (Figure 1). All reviewers agreed to include these 12 papers.
3.2. Study Characteristics
The demographic and clinical characteristics of the included studies are presented in Table 1. Nine studies [22,24,29,30,31,32,33,34,35] involved patients with POD, three studies [36,37,38] focused on patients with POCD, and one study considered patients with pre-existing cognitive impairment [36]. CSF NfL detection was reported in six studies [24,29,35,36,37,38], whereas four studies [24,29,35,37] discussed the correlation between CSF and blood NfL levels. Furthermore, five studies [24,31,32,33,34] examined preoperative blood NfL levels as a risk factor for subsequent POD and presented the results as odds ratios (ORs) and 95% confidence intervals (CIs).
3.3. Methodological Quality
The Newcastle-Ottawa Scale (NOS) was used to assess the quality of the case-control and cohort studies, covering three quality parameters (selection, comparability, and exposure/outcome). Quality scores ranged from 6 to 9 for case-control studies and 7 to 9 for cohort studies. The mean NOS score was 6.83 (SD = 1.73), indicating that the articles were of moderate quality (Table 2).
3.4. Results of Pooled Analysis
Pooled analyses of data from four trials that mentioned CSF NfL levels demonstrated a significant positive correlation with blood NfL levels, with a pooled effect size z = 0.73 (95% CI, 0.45–1.02) and the pooled r-value = 0.63 (95% CI, 0.42–0.77), with a significant heterogeneity (I2 = 79.7%, P < 0.001) (Figure 2).
Subgroup analysis revealed that the preoperative CSF NfL levels were significantly higher only in the POD group (SMD = 0.27; 95% CI, 0.07–0.47) with low heterogeneity (I2 = 0.0%, P = 0.912) rather than in pre-existing cognitive impairment and POCD groups (Figure 3a). Subgroup analysis also revealed that regardless of whether it was before or after surgery, blood NfL levels in the POD group were higher than in the no-POD group (SMD = 0.53; 95% CI, 0.40–0.66) with low heterogeneity (I2 = 53.0%, P = 0.059) and (SMD = 0.58; 95% CI, 0.43–0.73) with low heterogeneity (I2 = 0.0%, P = 0.903), respectively (Figure 3b). Additional subgroup analyses showed that postoperative blood NfL levels increased significantly in both the cardiac surgery and non-cardiac surgery groups, as well as in the general anaesthesia and spinal anaesthesia groups (Supplementary Figure S1). Further subgroup analysis demonstrated that, the blood NfL levels increased significantly after surgery in the POD group (SMD = 0.49; 95% CI, 0.34–0.64) with low heterogeneity (I2 = 2.7%, P = 0.391), as well as in the no-POD group (SMD = 0.67; 95% CI, 0.53–0.81) with low heterogeneity (I2 = 0.0%, P = 0.759) (Figure 3c).
Moreover, pooling 5 studies revealed that an increase in preoperative blood NfL level was associated with a higher risk of POD (OR = 1.75; 95% CI, 1.01–3.01) with substantial heterogeneity (I2 = 73.9%, P<0.001) (Figure 4).
3.5. Reporting Biases
The Egger’s regression test did not show any evidence of publication bias (Supplementary Table S1).
3.6. Sensitivity Analysis
Sensitivity analysis was also conducted for this meta-analysis. After removing one study at a time and calculating the combined weighted mean differences (WMD) for the remaining studies, it was demonstrated that no single study significantly affected the overall meta-analysis results. This observation indicated that the findings were reliable and statistically stable (Supplementary Figure S2).
4. Discussion
We conducted a systematic review of case-control and prospective cohort studies to compare NfL levels in the CSF and blood in patients with and without PND, both pre- and postoperation. First, blood NfL levels demonstrated a significant positive correlation with CSF NfL levels, supporting the use of NfL as a blood biomarker in future PND studies. Second, the integrated data revealed significant elevations in preoperative CSF NfL levels and pre- and postoperative blood NfL levels in patients with POD compared with controls, highlighting the potential of NfL as a biomarker of POD. Lastly, we found that the preoperative elevation of blood NfL levels was a risk factor for POD, which could assist in the identification of high-risk patients. Therefore, pre- and postoperative testing of blood NfL levels may play an important role in perioperative risk stratification, even when cognitive impairment is not detected.
NfL is a structural filament protein of the neuronal cytoskeleton and is highly expressed in myelinated large-calibre axons [13]. Under normal conditions, it is released at a constant low rate from axons, although this rate increases with age [39]. Recent studies have indicated that NfL is abnormally released into the CSF and blood following damage to various central nervous system neurons [40]. The exact mechanism is not fully understood, but it likely involves the disruption of cell membrane integrity and an increase in blood-brain barrier permeability [41,42]. Neurodegeneration, neurocognitive decline, and neuronal loss associated with Alzheimer’s disease (AD) correlate with increased CSF/plasma NfL levels [43]. Plasma NfL has recently been considered a diagnostic and prognostic biomarker for the preclinical stages of AD [44]. Patients who subsequently develop PND have pre-existing brain vulnerability secondary to prodromal neurodegenerative changes [30]. PND appear to increase the risk of developing new-onset dementia and exacerbate the long-term trajectory of existing dementia, and can be monitored using biofluid markers of neurodegeneration [30,45]. Consequently, an increasing number of studies have expanded the role of NfL in the prediction and as a biomarker for PND.
Acute changes in the NfL have also been observed in response to surgery and anaesthesia. Evered et al. reported an acute response to neuronal injury due to surgery and anaesthesia, with a significant and sequential increase in NfL plasma concentration up to 48 h postoperatively [46]. Halaas et al. identified an association between preoperative NfL levels and POD [29]. However, Casey et al. found no such association [23,24]. Their study included a small sample size, which limited their ability to establish whether NfL in blood is a reliable biomarker. In contrast, the current analysis included 12 articles that examined a larger patient population. A series of meta-analyses and subgroup analyses were performed to confirm the conclusions reported here, indicating that blood NfL levels may reflect axonal degeneration and could be employed as a biomarker of POD.
Ideally, as our primary outcome, we sought to utilise NfL in the blood as a biomarker for PND, since lumbar punctures are invasive procedures that are only clinically required for a minor subset of patients with PND [47]. Thus, using blood levels avoids the invasiveness of CSF sampling, which has limited clinical applications. NfL is released upon axonal injury and is soluble in both the CSF and blood [48]. Animal studies have suggested that NfL is a reliable biomarker of the severity of neuronal apoptosis [49]. NfL can be measured in the CSF using enzyme-linked immunosorbent assay (ELISA), which involves antibody-antigen interactions [50]. With the development of ultrasensitive immunoassays, quantification of NfL concentrations and detection of longitudinal changes in plasma-specific NfL levels have been achieved [23]. Consistent with the results of previous studies on various diseases [15,16], our meta-analysis found that blood NfL levels exhibited a significant positive correlation with CSF NfL levels in surgical patients. This finding forms the basis for demonstrating the effectiveness of blood NfL levels as a biomarker of PND.
The pooled analysis of preoperative CSF NfL levels revealed no significant differences between patients with and without PND. Based on the clinical classification and nomenclature of PND [4], subgroup analysis demonstrated that preoperative CSF NfL levels were significantly higher in the POD group than in those with preexisting cognitive impairment or POCD. This result is not absolute, as the included studies were limited, and future research incorporating more relevant studies is needed to confirm these findings. Consequently, the naming and classification of PND are essential and beneficial for biomarker research. We strongly agree that a formal classification is critical for patients with spontaneous postoperative cognitive complaints. Unifying the development of cognitive dysfunction symptoms after procedures facilitates a better understanding of the relationship between surgical anaesthesia, biomarkers, and cognitive disorders, ensuring consistency and accuracy in the results [50].
In this analysis, owing to the limitations of the existing research, we did not find relevant studies investigating blood NfL levels in patients with preexisting cognitive impairment and DNR, except for POD. Only one study reported blood NfL levels in patients with POCD, which precludes the possibility of a meta-analysis [7]. A major gap identified in our project involved nine studies that measured pre- and postoperative blood NfL levels in patients with and without POD. Pooled analysis revealed that, regardless of whether it was before or after surgery, the blood NfL levels in the POD group were higher than those in the non-POD group. These results may help address two main diagnostic shortcomings in perioperative patients with POD. First, preoperative identification of patients at high risk of developing postoperative delirium is crucial. Current tools for POD prediction have proven to be insufficient. Second, early detection of POD during the postoperative phase is essential. The identification of patients at high risk of POD could enable clinical personnel to conduct closer POD screening and monitoring and, if necessary, initiate early treatment. This consideration is crucial because POD duration is associated with impaired outcomes.
Previous studies have mainly focused on neuroinflammation and biomarkers that may be elevated after surgery, with few studies evaluating whether preoperative biomarkers of brain vulnerability contribute to postoperative cognitive events [15,21,51,52]. Among the biomarkers of neurodegeneration, NfL has been strongly proposed for detecting neuronal injury or loss before the onset of the clinical symptoms of AD, cognitive dysfunction, and brain atrophy [43,44]. Conflicting results have emerged from studies investigating the association between preoperative biomarkers and POD, which may be attributed to small sample sizes, heterogeneous biomarkers, and different methods of statistical analysis [21,22,24,53]. In this meta-analysis, we pooled the results of five studies and determined that elevated preoperative blood NfL levels were a risk factor for POD. However, owing to the limited number of studies, further high-quality clinical studies with larger patient groups are required to verify these results.
Additionally, our results indicated that postoperative blood NfL levels were higher than preoperative blood NfL levels in the subgroups of POD and non-POD, cardiac surgery and non-cardiac surgery, and general anaesthesia and spinal anaesthesia. Nonetheless, anaesthesia and surgery are believed to affect the central nervous system through a fully reversible mechanism that is harmless to nerve cells [54]. Evidence of neurological sequelae following these procedures challenges this belief and suggests the need to reassess theories of anaesthetic action mechanisms or the response of the central nervous system to surgery [55]. The mechanism underlying POD development is poorly understood, however, dysregulated inflammation and neuronal injury are emerging as key features of perioperative neurocognitive disorders in clinical studies [56,57,58]. With vascular and neuronal injuries, various injured biomolecules may be released into the CSF and blood via the leaky blood-brain barrier [59]. Axonal integrity and transport are directly associated with cognitive decline and neurodegeneration [60]. Our findings suggest that NfL, a structural component of axons, could be a promising tool for the early prediction of POD and as a biomarker of POD. If confirmed, this could provide a novel perspective on the pathogenesis of POD.
Notably, NfL has a strong age-related correlation, whereas old age is an independent risk factor for PND [61]. Consequently, an increase in preoperative blood NfL levels is associated with the development of POD and may provide insights into brain susceptibility [62]. The patients included in this study were aged 65 or older; further exploration regarding NfL levels in younger patients with PND is required. Many studies that evaluated changes in NfL following surgery had limited sampling, typically evaluating only one or two postoperative days in this meta-analysis, and employed heterogeneous statistical analyses. It remains unclear whether these biomarker changes are temporary or whether post-surgery biomarker alterations are associated with long-term consequences. As a potential biomarker for PND, future research should ideally focus on NfL levels as a predictor, diagnostic tool, and recovery evaluation measure for PND.
This meta-analysis had several limitations. First, it has the inherent limitations of all meta-analyses of observational studies. As random allocation cannot be achieved, the influence of confounding variables may not be fully evaluated. Second, we employed basic inequalities and approximations to estimate the mean and variance of such trials. Simulated data manipulation of the derived medians and SD should be interpreted with caution. Third, the sample sizes of the included studies were relatively small, and the total number of cases was limited. Fourth, some observational studies have not been registered in clinical trial databases, preventing the determination of the scope of unpublished literature and the elimination of potential biased effects in research and outcome levels. Finally, this study primarily relies on research published in English, which may introduce bias from literature published in other languages.
5. Conclusions
This meta-analysis provides evidence that blood NfL levels could potentially serve as a biomarker for POD, with elevated preoperative NfL levels appearing to be a risk factor for POD. To further understand the significance of elevated NfL levels in CSF or blood in PND, future studies with larger samples and more diverse participants will help elucidate this promising area of investigation.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Forest plots of pooled data for exploratory subgroups. (a) Studies on the changes in pre- and postoperative blood NfL levels in cardiac surgery and non-cardiac surgery groups. (b) Studies on the changes in pre- and postoperative blood NfL levels in general anaesthesia and spinal anaesthesia groups. NfL, neurofilament light chain; CI, confidence interval.; Figure S2: Sensitivity analysis of each pooled analysis. Table S1: Egger’s test results for publication and selective reporting bias.
Author Contributions
conception of research idea: HL; design of the review and completion of search strategy: FC, ZXW, QC; supervision of data analysis and interpretation: HL; data extraction: DKZ, ZXW, FC; data analysis and interpretation: QC, FC; quality score evaluation: DKZ, ZXW, QC; literature review: FC; drafting of the manuscript: FC, DKZ; critical review and revision of the manuscript: HL, ZXW; all authors reviewed the manuscript and gave final approval to the published version.
Funding
This research was supported by grants from National Natural Science Foundation of China (grant numbers: 82171265), Beijing, China.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We are grateful to the authors of the included trials, some of whom provided additional data for this systematic review and meta-analysis.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Moller, J.T.; Cluitmans, P.; Rasmussen, L.S.; Houx, P.; Rasmussen, H.; Canet, J.; Rabbitt, P.; Jolles, J.; Larsen, K.; Hanning, C.D. et al. Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International Study of Post-Operative Cognitive Dysfunction. Lancet 1998, 351, 857-861. [CrossRef]
- Steinmetz, J.; Christensen, K.B.; Lund, T.; Lohse, N.; Rasmussen, L.S. Long-term consequences of postoperative cognitive dysfunction. Anesthesiology 2009, 110, 548-555. [CrossRef]
- Needham, M.J.; Webb, C.E.; Bryden, D.C. Postoperative cognitive dysfunction and dementia: what we need to know and do. Br. J. Anaesth. 2017, 119, i115-i125. [CrossRef]
- Evered, L.; Silbert, B.; Knopman, D.S.; Scott, D.A.; DeKosky, S.T.; Rasmussen, L.S.; Oh, E.S.; Crosby, G.; Berger, M.; Eckenhoff, R.G. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Br. J. Anaesth. 2018, 121, 1005-1012. [CrossRef]
- Liu, J.; Huang, K.; Zhu, B.; Zhou, B.; Ahmad, H.A.; Liu, L.; Wu, X. Neuropsychological Tests in Post-operative Cognitive Dysfunction: Methods and Applications. Front. Psychol. 2021, 12, 684307. [CrossRef]
- Borchers, F.; Spies, C.D.; Feinkohl, I.; Brockhaus, W.R.; Kraft, A.; Kozma, P.; Fislage, M.; Kühn, S.; Ionescu, C.; Speidel, S. et al. Methodology of measuring postoperative cognitive dysfunction: a systematic review. Br. J. Anaesth. 2021, 126, 1119-1127. [CrossRef]
- Wiberg, S.; Holmgaard, F.; Zetterberg, H.; Nilsson, J.C.; Kjaergaard, J.; Wanscher, M.; Langkilde, A.R.; Hassager, C.; Rasmussen, L.S.; Blennow, K. et al. Biomarkers of Cerebral Injury for Prediction of Postoperative Cognitive Dysfunction in Patients Undergoing Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2022, 36, 125-132. [CrossRef]
- Evered, L.; Atkins, K.; Silbert, B.; Scott, D.A. Acute peri-operative neurocognitive disorders: a narrative review. Anaesthesia 2022, 77 Suppl 1, 34-42. [CrossRef]
- Lin, X.; Chen, Y.; Zhang, P.; Chen, G.; Zhou, Y.; Yu, X. The potential mechanism of postoperative cognitive dysfunction in older people. Exp. Gerontol. 2020, 130, 110791. [CrossRef]
- Berger, M.; Browndyke, J.N.; Cooter, W.M.; Nobuhara, C.; Reese, M.; Acker, L.; Bullock, W.M.; Colin, B.J.; Devinney, M.J.; Moretti, E.W. et al. Postoperative changes in cognition and cerebrospinal fluid neurodegenerative disease biomarkers. Ann. Clin. Transl. Neurol. 2022, 9, 155-170. [CrossRef]
- Larsen, J.R.; Kobborg, T.; Shahim, P.; Blennow, K.; Rasmussen, L.S.; Zetterberg, H. Serum-neuroproteins, near-infrared spectroscopy, and cognitive outcome after beach-chair shoulder surgery: Observational cohort study analyses. Acta Anaesthesiol. Scand. 2021, 65, 26-33. [CrossRef]
- Osborn, K.E.; Khan, O.A.; Kresge, H.A.; Bown, C.W.; Liu, D.; Moore, E.E.; Gifford, K.A.; Acosta, L.; Bell, S.P.; Hohman, T.J. et al. Cerebrospinal fluid and plasma neurofilament light relate to abnormal cognition. Alzheimers Dement.-Diagn. Assess. Dis. Monit. 2019, 11, 700-709. [CrossRef]
- Lambertsen, K.L.; Soares, C.B.; Gaist, D.; Nielsen, H.H. Neurofilaments: The C-Reactive Protein of Neurology. Brain Sci. 2020, 10. [CrossRef]
- Gaetani, L.; Blennow, K.; Calabresi, P.; Di Filippo, M.; Parnetti, L.; Zetterberg, H. Neurofilament light chain as a biomarker in neurological disorders. J. Neurol. Neurosurg. Psychiatry. 2019, 90, 870-881. [CrossRef]
- Mielke, M.M.; Syrjanen, J.A.; Blennow, K.; Zetterberg, H.; Vemuri, P.; Skoog, I.; Machulda, M.M.; Kremers, W.K.; Knopman, D.S.; Jack, C.J. et al. Plasma and CSF neurofilament light: Relation to longitudinal neuroimaging and cognitive measures. Neurology 2019, 93, e252-e260. [CrossRef]
- Osborn, K.E.; Khan, O.A.; Kresge, H.A.; Bown, C.W.; Liu, D.; Moore, E.E.; Gifford, K.A.; Acosta, L.; Bell, S.P.; Hohman, T.J. et al. Cerebrospinal fluid and plasma neurofilament light relate to abnormal cognition. Alzheimers Dement.-Diagn. Assess. Dis. Monit. 2019, 11, 700-709. [CrossRef]
- Shahim, P.; Politis, A.; van der Merwe, A.; Moore, B.; Chou, Y.Y.; Pham, D.L.; Butman, J.A.; Diaz-Arrastia, R.; Gill, J.M.; Brody, D.L. et al. Neurofilament light as a biomarker in traumatic brain injury. Neurology 2020, 95, e610-e622. [CrossRef]
- Taylor, J.; Eisenmenger, L.; Lindroth, H.; Booth, J.; Mohanty, R.; Nair, V.; Parker, M.; Kunkel, D.; Rivera, C.; Casey, C. et al. Perioperative ischaemic brain injury and plasma neurofilament light: a secondary analysis of two prospective cohort studies. Br. J. Anaesth. 2023, 130, e361-e369. [CrossRef]
- Gaetani, L.; Blennow, K.; Calabresi, P.; Di Filippo, M.; Parnetti, L.; Zetterberg, H. Neurofilament light chain as a biomarker in neurological disorders. J. Neurol. Neurosurg. Psychiatry. 2019, 90, 870-881. [CrossRef]
- Rudolph, J.L.; Marcantonio, E.R. Review articles: postoperative delirium: acute change with long-term implications. Anesth. Analg. 2011, 112, 1202-1211. [CrossRef]
- Casey, C.P.; Lindroth, H.; Mohanty, R.; Farahbakhsh, Z.; Ballweg, T.; Twadell, S.; Miller, S.; Krause, B.; Prabhakaran, V.; Blennow, K. et al. Postoperative delirium is associated with increased plasma neurofilament light. Brain. 2020, 143, 47-54. [CrossRef]
- Saller, T.; Petzold, A.; Zetterberg, H.; Kuhle, J.; Chappell, D.; von Dossow, V.; Klawitter, F.; Schurholz, T.; Hagl, C.; Reuter, D.A. et al. A case series on the value of tau and neurofilament protein levels to predict and detect delirium in cardiac surgery patients. Biomed. Pap-Olomouc 2019, 163, 241-246. [CrossRef]
- Alifier, M.; Olsson, B.; Andreasson, U.; Cullen, N.C.; Czyżewska, J.; Jakubów, P.; Sieśkiewicz, A.; Stasiak-Barmuta, A.; Hirnle, T.; Kornhuber, J. et al. Cardiac Surgery is Associated with Biomarker Evidence of Neuronal Damage. J. Alzheimers Dis. 2020, 74, 1211-1220. [CrossRef]
- Fong, T.G.; Vasunilashorn, S.M.; Kivisäkk, P.; Metzger, E.D.; Schmitt, E.M.; Marcantonio, E.R.; Jones, R.N.; Shanes, H.T.; Arnold, S.E.; Inouye, S.K. et al. Biomarkers of neurodegeneration and neural injury as potential predictors for delirium. Int. J. Geriatr. Psychiatry 2024, 39, e6044. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021, 372, n71. [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [CrossRef]
- Fagundes, M.A.; Silva, A.; Fernandes, G.A.; Curado, M.P. Dietary Polyphenol Intake and Gastric Cancer: A Systematic Review and Meta-Analysis. Cancers 2022, 14. [CrossRef]
- Pripp, A.H. [Pearson’s or Spearman’s correlation coefficients]. Tidsskr. Nor. Laegeforen. 2018, 138. [CrossRef]
- Halaas, N.B.; Blennow, K.; Idland, A.V.; Wyller, T.B.; Ræder, J.; Frihagen, F.; Staff, A.C.; Zetterberg, H.; Watne, L.O. Neurofilament Light in Serum and Cerebrospinal Fluid of Hip Fracture Patients with Delirium. Dement. Geriatr. Cogn. Disord. 2018, 46, 346-357. [CrossRef]
- Leung, J.M.; Rojas, J.C.; Tang, C.; Chan, B.; Lario-Lago, A.; Boxer, A.L.; Do, Q.; Kramer, J.H.; Du Z; Du P et al. Presence of Preoperative Neurodegeneration Biofluid Markers in Patients with Postoperative Delirium. Anesthesiology 2023, 139, 432-443. [CrossRef]
- Fong, T.G.; Vasunilashorn, S.M.; Ngo, L.; Libermann, T.A.; Dillon, S.T.; Schmitt, E.M.; Pascual-Leone, A.; Arnold, S.E.; Jones, R.N.; Marcantonio, E.R. et al. Association of Plasma Neurofilament Light with Postoperative Delirium. Ann. Neurol. 2020, 88, 984-994. [CrossRef]
- Liu, X.; Wang, Y.; Wu, J.; Ye, C.; Ma, D.; Wang, E. Emergence delirium and postoperative delirium associated with high plasma NfL and GFAP: an observational study. Front. Med. 2023, 10, 1107369. [CrossRef]
- Brown, C.H.; Kim, A.S.; Yanek, L.; Lewis, A.; Mandal, K.; Le L; Tian, J.; Neufeld, K.J.; Hogue, C.; Moghekar, A. Association of perioperative plasma concentration of neurofilament light with delirium after cardiac surgery: a nested observational study. Br. J. Anaesth. 2024, 132, 312-319. [CrossRef]
- Khalifa, C.; Robert, A.; Cappe, M.; Lemaire, G.; Tircoveanu, R.; Dehon, V.; Ivanoiu, A.; Piérard, S.; de Kerchove, L.; Jacobs, S.A. et al. Serum Neurofilament Light and Postoperative Delirium in Cardiac Surgery: A Preplanned Secondary Analysis of a Prospective Observational Study. Anesthesiology 2024, 140, 950-962. [CrossRef]
- Parker, M.; White, M.; Casey, C.; Kunkel, D.; Bo, A.; Blennow, K.; Zetterberg, H.; Pearce, R.A.; Lennertz, R.; Sanders, R.D. Cohort Analysis of the Association of Delirium Severity With Cerebrospinal Fluid Amyloid-Tau-Neurodegeneration Pathologies. J. Gerontol. Ser. A.-Biol. Sci. Med. Sci. 2022, 77, 494-501. [CrossRef]
- Evered, L.; Silbert, B.; Scott, D.A.; Ames, D.; Maruff, P.; Blennow, K. Cerebrospinal Fluid Biomarker for Alzheimer Disease Predicts Postoperative Cognitive Dysfunction. Anesthesiology 2016, 124, 353-361. [CrossRef]
- Danielson, M.; Wiklund, A.; Granath, F.; Blennow, K.; Mkrtchian, S.; Nellgård, B.; Oras, J.; Fagerlund, M.J.; Granström, A.; Schening, A. et al. Association between cerebrospinal fluid biomarkers of neuronal injury or amyloidosis and cognitive decline after major surgery. Br. J. Anaesth. 2021, 126, 467-476. [CrossRef]
- Zhang, X.; Fu, Q. [Correlation of cerebrospinal fluid amyloid β-protein 42 and neurofilament light protein levels with postoperative neurocognitive dysfunction in elderly patients]. Nan Fang Yi Ke Da Xue Xue Bao 2021, 41, 574-578. [CrossRef]
- Yuan, A.; Rao, M.V.; Veeranna; Nixon, R.A. Neurofilaments and Neurofilament Proteins in Health and Disease. Cold Spring Harbor Perspect. Biol. 2017, 9. [CrossRef]
- Luigetti, M.; Primiano, G.; Basile, V.; Vitali, F.; Pignalosa, S.; Romano, A.; Sabino, A.; Marino, M.; Di Santo, R.; Ciasca, G. et al. Serum Neurofilament and Free Light Chain Levels in Patients Undergoing Treatment for Chronic Inflammatory Demyelinating Polyneuropathy. Int. J. Mol. Sci. 2024, 25. [CrossRef]
- Hughes, C.G.; Pandharipande, P.P.; Thompson, J.L.; Chandrasekhar, R.; Ware, L.B.; Ely, E.W.; Girard, T.D. Endothelial Activation and Blood-Brain Barrier Injury as Risk Factors for Delirium in Critically Ill Patients. Crit. Care Med. 2016, 44, e809-e817. [CrossRef]
- Fan, Z.; Liu, X.; Liu, J.; Chen, C.; Zhou, M. Neurofilament Light Chain as a Potential Biomarker in Plasma for Alzheimer’s Disease and Mild Cognitive Impairment: A Systematic Review and a Meta-Analysis. J. Integr. Neurosci. 2023, 22, 85. [CrossRef]
- Leuzy, A.; Mattsson-Carlgren, N.; Palmqvist, S.; Janelidze, S.; Dage, J.L.; Hansson, O. Blood-based biomarkers for Alzheimer’s disease. EMBO Mol. Med. 2022, 14, e14408. [CrossRef]
- Chatterjee, P.; Pedrini, S.; Ashton, N.J.; Tegg, M.; Goozee, K.; Singh, A.K.; Karikari, T.K.; Simrén, J.; Vanmechelen, E.; Armstrong, N.J. et al. Diagnostic and prognostic plasma biomarkers for preclinical Alzheimer’s disease. Alzheimers. Dement. 2022, 18, 1141-1154. [CrossRef]
- Krogseth, M.; Watne, L.O.; Juliebø, V.; Skovlund, E.; Engedal, K.; Frihagen, F.; Wyller, T.B. Delirium is a risk factor for further cognitive decline in cognitively impaired hip fracture patients. Arch. Gerontol. Geriatr. 2016, 64, 38-44. [CrossRef]
- Evered, L.; Silbert, B.; Scott, D.A.; Zetterberg, H.; Blennow, K. Association of Changes in Plasma Neurofilament Light and Tau Levels With Anesthesia and Surgery: Results From the CAPACITY and ARCADIAN Studies. JAMA Neurol. 2018, 75, 542-547. [CrossRef]
- Barro, C.; Chitnis, T.; Weiner, H.L. Blood neurofilament light: a critical review of its application to neurologic disease. Ann. Clin. Transl. Neurol. 2020, 7, 2508-2523. [CrossRef]
- Andersson, E.; Janelidze, S.; Lampinen, B.; Nilsson, M.; Leuzy, A.; Stomrud, E.; Blennow, K.; Zetterberg, H.; Hansson, O. Blood and cerebrospinal fluid neurofilament light differentially detect neurodegeneration in early Alzheimer’s disease. Neurobiol. Aging 2020, 95, 143-153. [CrossRef]
- Liu, S.; Zhang, Z.; Shi, S.; Meng, Y.; Zhang, X.; Lei, Q.; Li, Z. NREM sleep loss increases neurofilament light chain levels in APP/PS1 and C57BL/6 J mice. Sleep Breath. 2023, 27, 1495-1504. [CrossRef]
- Narayanan, S.; Shanker, A.; Khera, T.; Subramaniam, B. Neurofilament light: a narrative review on biomarker utility. Fac Rev 2021, 10, 46. [CrossRef]
- Alves, R.L.; Cardoso, B.; Ramos, I.; Oliveira, B.; Dos, S.M.; de Miranda, A.S.; de Almeida, T.; Vieira, M.; Machado, F.S.; Ferreira, A.J. et al. Physical training improves exercise tolerance, cardiac function and promotes changes in neurotrophins levels in chagasic mice. Life Sci. 2019, 232, 116629. [CrossRef]
- Cata, J.P.; Abdelmalak, B.; Farag, E. Neurological biomarkers in the perioperative period. Br. J. Anaesth. 2011, 107, 844-858. [CrossRef]
- McKay, T.B.; Rhee, J.; Colon, K.; Adelsberger, K.; Turco, I.; Mueller, A.; Qu, J.; Akeju, O. Preliminary Study of Serum Biomarkers Associated With Delirium After Major Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2022, 36, 118-124. [CrossRef]
- Deiner, S.; Baxter, M.G.; Mincer, J.S.; Sano, M.; Hall, J.; Mohammed, I.; O’Bryant, S.; Zetterberg, H.; Blennow, K.; Eckenhoff, R. Human plasma biomarker responses to inhalational general anaesthesia without surgery. Br. J. Anaesth. 2020, 125, 282-290. [CrossRef]
- Vutskits, L.; Xie, Z. Lasting impact of general anaesthesia on the brain: mechanisms and relevance. Nat. Rev. Neurosci. 2016, 17, 705-717. [CrossRef]
- Luo, A.; Yan, J.; Tang, X.; Zhao, Y.; Zhou, B.; Li, S. Postoperative cognitive dysfunction in the aged: the collision of neuroinflammaging with perioperative neuroinflammation. Inflammopharmacology 2019, 27, 27-37. [CrossRef]
- Lin, X.; Chen, Y.; Zhang, P.; Chen, G.; Zhou, Y.; Yu, X. The potential mechanism of postoperative cognitive dysfunction in older people. Exp. Gerontol. 2020, 130, 110791. [CrossRef]
- Xiao, J.Y.; Xiong, B.R.; Zhang, W.; Zhou, W.C.; Yang, H.; Gao, F.; Xiang, H.B.; Manyande, A.; Tian, X.B.; Tian, Y.K. PGE2-EP3 signaling exacerbates hippocampus-dependent cognitive impairment after laparotomy by reducing expression levels of hippocampal synaptic plasticity-related proteins in aged mice. CNS Neurosci. Ther. 2018, 24, 917-929. [CrossRef]
- Zhang, S.; Dong, H.; Zhang, X.; Li, N.; Sun, J.; Qian, Y. Cerebral mast cells contribute to postoperative cognitive dysfunction by promoting blood brain barrier disruption. Behav. Brain Res. 2016, 298, 158-166. [CrossRef]
- Teipel, S.J.; Stahl, R.; Dietrich, O.; Schoenberg, S.O.; Perneczky, R.; Bokde, A.L.; Reiser, M.F.; Möller, H.J.; Hampel, H. Multivariate network analysis of fiber tract integrity in Alzheimer’s disease. Neuroimage 2007, 34, 985-995. [CrossRef]
- Becher, R.D.; Vander, W.B.; Leo-Summers, L.; Desai, M.M.; Gill, T.M. The Incidence and Cumulative Risk of Major Surgery in Older Persons in the United States. Ann. Surg. 2023, 277, 87-92. [CrossRef]
- Strøm, C.; Rasmussen, L.S.; Sieber, F.E. Should general anaesthesia be avoided in the elderly? Anaesthesia 2014, 69 Suppl 1, 35-44. [CrossRef]
Figure 1.
Flow diagram of selection of eligible studies.
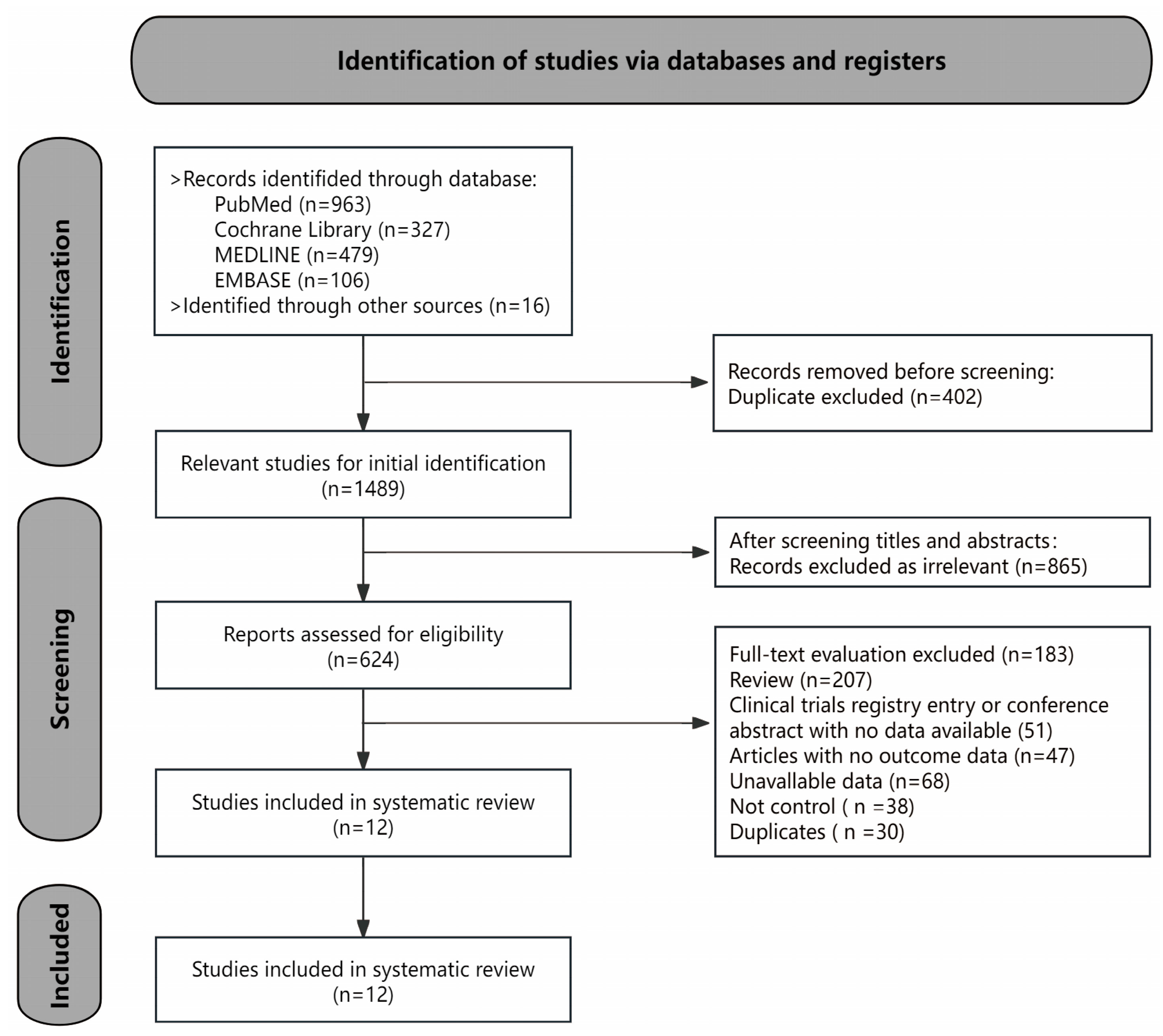
Figure 2.
Forest plot for the correlation (a pooled effect size z) between CSF and blood NfL levels. NfL, neurofilament light chain; CSF, cerebrospinal fluid; CI, confidence interval.
Figure 2.
Forest plot for the correlation (a pooled effect size z) between CSF and blood NfL levels. NfL, neurofilament light chain; CSF, cerebrospinal fluid; CI, confidence interval.
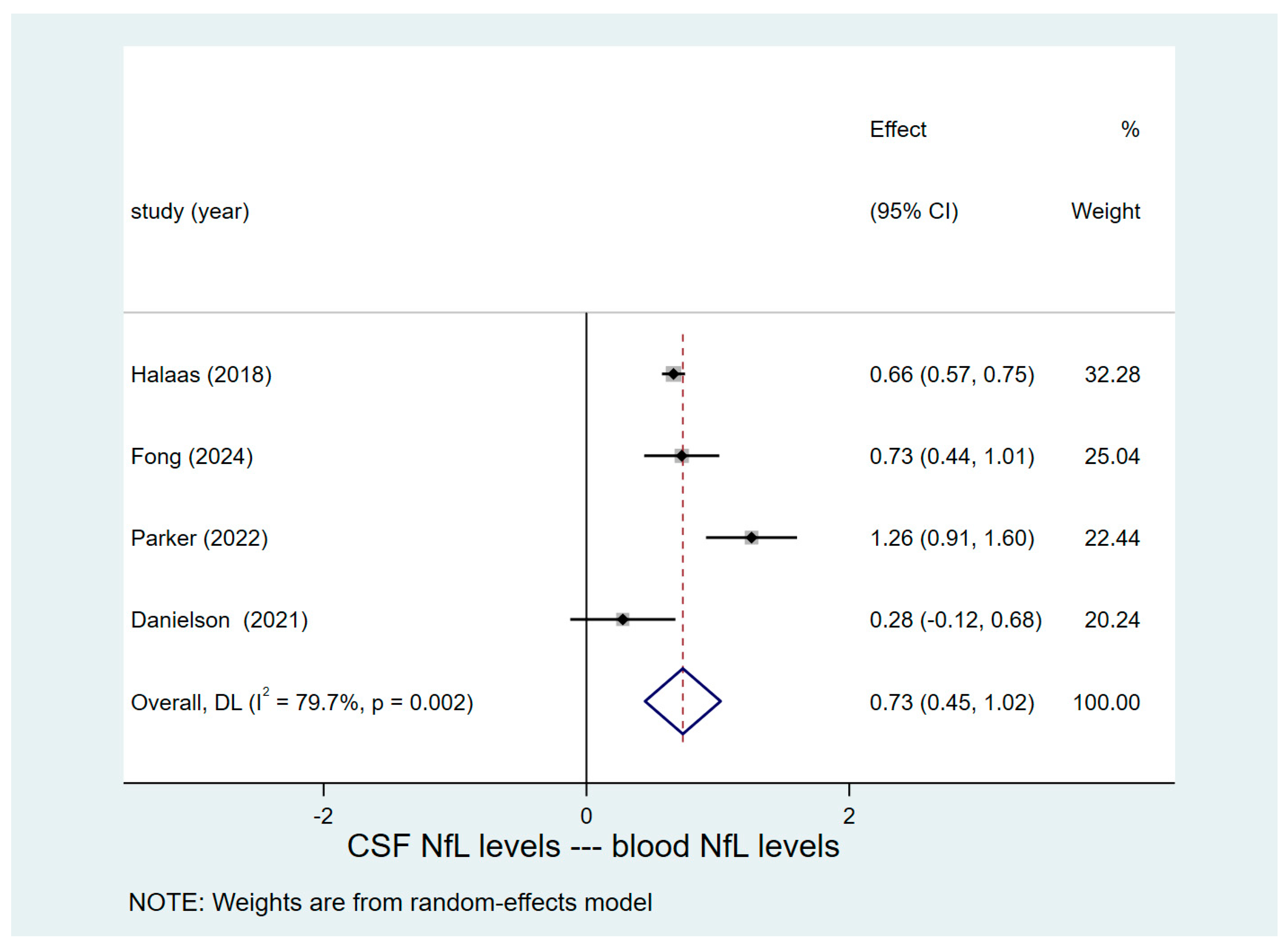
Figure 3.
Forest plots of pooled data for the exploratory subgroups. (a) Studies on different preoperative CSF NfL levels in pre-existing cognitive impairment, POD, and POCD groups. (b) Studies on the changes in pre- and postoperative blood NfL levels in POD and no-POD groups. (c) Studies on the differences in pre- and postoperative blood NfL levels between POD and no-POD groups. NfL, neurofilament light chain; CSF, cerebrospinal fluid; POD, postoperative delirium; POCD, postoperative cognitive dysfunction; PND, perioperative neurocognitive disorders; CI, confidence interval.
Figure 3.
Forest plots of pooled data for the exploratory subgroups. (a) Studies on different preoperative CSF NfL levels in pre-existing cognitive impairment, POD, and POCD groups. (b) Studies on the changes in pre- and postoperative blood NfL levels in POD and no-POD groups. (c) Studies on the differences in pre- and postoperative blood NfL levels between POD and no-POD groups. NfL, neurofilament light chain; CSF, cerebrospinal fluid; POD, postoperative delirium; POCD, postoperative cognitive dysfunction; PND, perioperative neurocognitive disorders; CI, confidence interval.
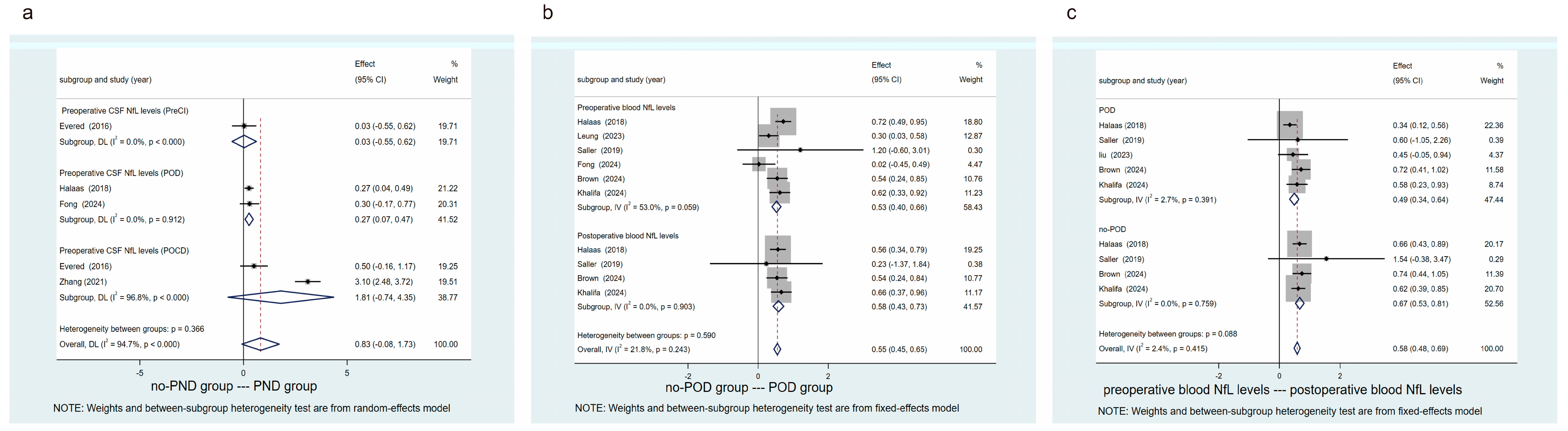
Figure 4.
Forest plot of pooled data for the impact of preoperative blood NfL levels on the risk of POD. NfL, neurofilament light chain; POD, postoperative delirium; OR, odds ratio; CI, confidence interval.
Figure 4.
Forest plot of pooled data for the impact of preoperative blood NfL levels on the risk of POD. NfL, neurofilament light chain; POD, postoperative delirium; OR, odds ratio; CI, confidence interval.
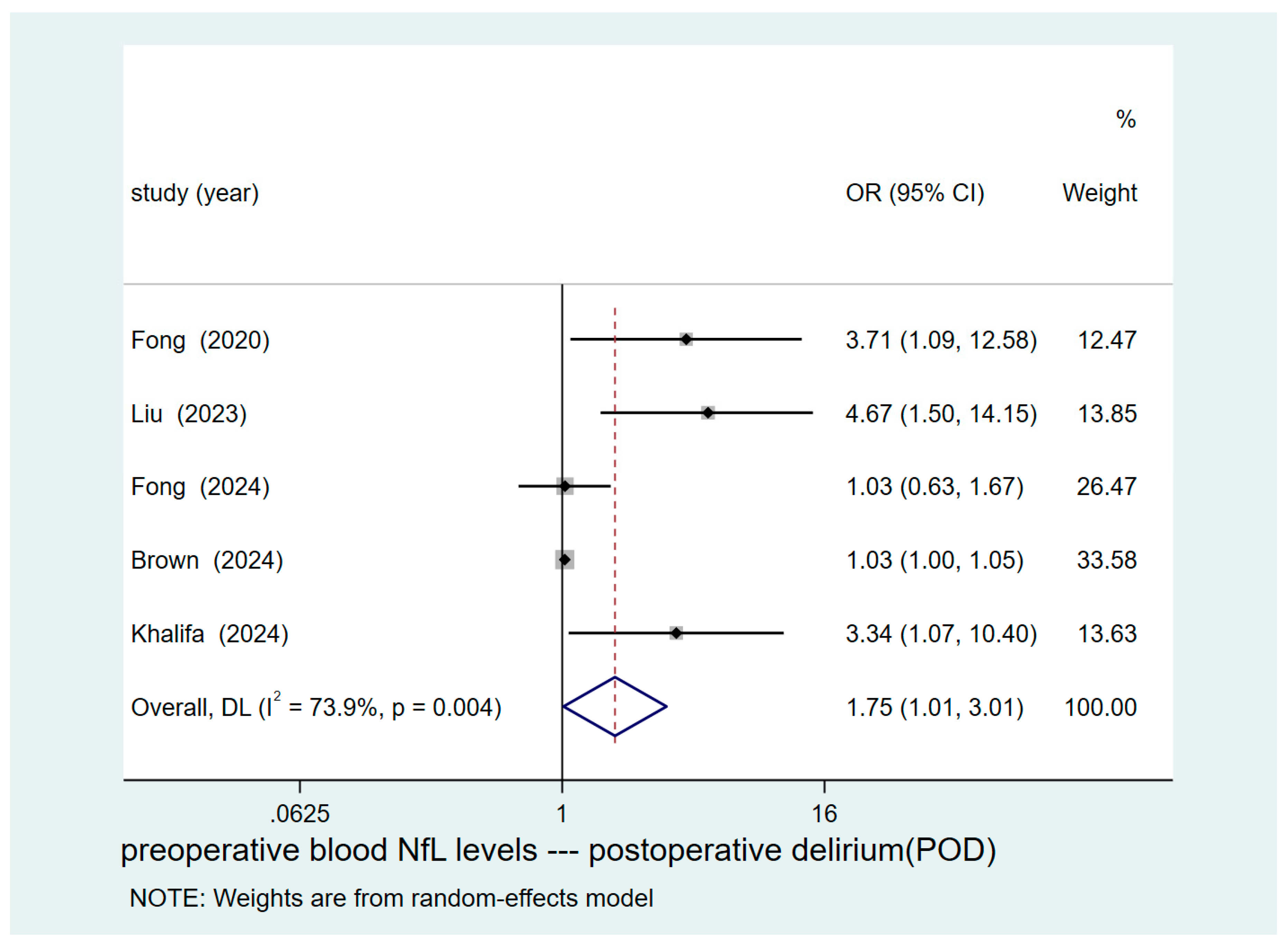

Table 1.
Basic characteristics of the included studies.
| Study | Contry | Surgery | Anesthesia | Sample Size (Male/Female) |
Age Range | Study Design | Diagnostic Criteria or Method |
No. of PNDs/no-PNDs |
Biomarker Measured |
|---|---|---|---|---|---|---|---|---|---|
| Halaas 2018 [29] |
China |
Hip fracture |
SA |
77/237 | 85 (79–79) | Case-control | CAM | POD/no-POD (162/152) |
CSF-NfL(Pre-Op) sNfL(Pre-Op/Post-Op1) |
| Leung 2023 [30] |
USA |
Noncardiac surgery |
GA |
73/131 | 72.91±5.82 | Case-control | CAM | POD/no-POD (102/102) |
pNfL(Pre-Op/Post-Op1) |
| Fong 2020 [31] |
USA |
Elective surgery |
GA |
52/56 | 77±5 | Prospective cohort | CAM | POD/no-POD (54/54) |
pNfL(Pre-Op/Post-Op2) |
| Saller 2019 [22] |
Germany |
Cardiac surgery |
GA |
6(Male) | 76±5 | Case-control | CAM-ICU | POD/no-POD (3/3) |
pNfL(Pre-Op) |
| Liu 2023 [32] |
China |
Elective surgery |
GA |
36/28 | POD (69.22±5.00) no-POD (70.31±3.82) |
Case-control | CAM | POD/no-POD (32/32) |
pNfL(Pre-Op/Post-Op1) |
| Fong 2024 [24] |
USA |
Elective surgery |
GA |
14/56 | 74.7±6.9 | Case-control | CAM | POD/no-POD (35/35) |
CSF-NfL(Pre-Op) pNfL(Pre-Op) |
| Brown 2024 [33] |
USA |
Cardiac surgery |
GA |
131/44 | 70.5(7.6) | Prospective cohort | CAM/CAM-ICU | POD/no-POD (78/97) |
pNfL(Pre-Op/Post-Op1) |
| Khalifa 2024 [34] |
Belgium |
Cardiac surgery |
GA |
180/40 | POD (74 [64, 79]) no-POD (67 [59, 74]) |
Prospective cohort | CAM/CAM-ICU | POD/no-POD (65/155) |
pNfL(Pre-Op/Post-Op1) |
| Parker 2022 [35] |
USA |
Thoracic vascular surgery |
GA |
18/13 | POD (68.5 [61.5-73]) no-POD (72 [67-77]) |
Prospective cohort | CAM-ICU | POD/no-POD (22/9) |
CSF-NfL(Pre-Op) sNfL(Pre-Op) |
| Evered 2016 [36] |
Australia |
Total hip replacement | Combined SA and GA |
19/40 | 70.4±7 | Prospective cohort | ISPOCD test battery | POCD/no-POCD (15/44) |
CSF-NfL(Pre-Op) |
| Danielson 2021 [37] |
Sweden |
Knee or hip replacement |
SA |
9/18 | POCD (71 [65-76]) no-POCD (68 [65-71]) |
Prospective cohort | ISPOCD test battery | POCD/no-POCD (6/21) |
CSF-NfL(Pre-Op) sNfL(Pre-Op) |
| Zhang 2021 [38] |
China |
Knee or hip replacement |
SA |
50/40 | POCD (68.2±4.3) no-POCD (68.9±4.0) |
Prospective cohort | ISPOCD test battery | POCD/no-POCD (38/52) |
CSF-NfL(Pre-Op) |
Note: USA, United States of America; GA, General anesthesia; SA, Spinal anesthesia; POD, postoperative delirium; POCD, postoperative cognitive dysfunction; sNfL, serum neurofilament light chain; pNfL, plasma neurofilament light chain; CSF, cerebrospinal fluid; Pre-Op, preoperative; Post-Op1, postoperative one day; Post-Op2, postoperative two days; CAM, confusion assessment method; CAM-ICU, the confusion assessment method for the intensive care unit; MMSE, mini-mental state examination; ISPOCD, international study of postoperative cognitive dysfunction.
Table 2.
Risk-of-bias assessment using the Newcastle-Ottawa Scale (NOS).
|
Study |
Study design |
Selection | Comparability | Exposure/Outcome | Scores | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | ||||||
| Halaas 2018 [29] | Case-control | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | ☆ | 7 | |||
| Leung 2023 [30] | Case-control | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9 | |||
| Fong 2020 [31] | Prospective cohort | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | ☆ | 7 | |||
| Saller 2019 [22] | Case-control | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | ☆ | 0 | 6 | |||
| Liu 2023 [32] | Case-control | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | ☆ | 7 | |||
| Fong 2024 [24] | Case-control | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 8 | |||
| Brown 2024 [33] | Prospective cohort | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | 0 | 0 | 7 | |||
| Khalifa 2024 [34] | Prospective cohort | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | 7 | |||
| Parker 2022 [35] | Prospective cohort | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | 0 | ☆ | 6 | |||
| Evered 2016 [36] | Prospective cohort | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | ☆ | 0 | 6 | |||
| Danielson 2021 [37] | Prospective cohort | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | ☆ | 7 | |||
| Zhang 2021 [38] | Prospective cohort | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 0 | 0 | 6 | |||
Note: NOS- Case control Studies, (1) Is the case definition adequate? (2) Representativeness of the case. (3) Selection of controls. (4) Definition of controls. (5) Comparability of cases and controls on the basis of design or analysis. (6) Ascertainment of exposure. (7) Same method of ascertainment for cases and controls. (8) Non-response rate. NOS- Cohort studies, (1) Representativeness of the exposed cohort. (2) Selection of the non-exposed cohort. (3) Ascertainment of exposure. (4) Demonstration that outcome of interest was not present at start of study/before ascertainment of exposure. (5) Comparability of cohorts on the basis of the design or analysis. (6) Assessment of outcome. (7) Was follow-up long enough for outcomes to occur. (8) Adequacy of follow up of cohorts.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



