
Submitted:
30 May 2024
Posted:
30 May 2024
You are already at the latest version
Abstract
The accurate identification of bacterial infections is critical for effective treatment in intensive care units (ICUs), yet current diagnostic methods face limitations in sensitivity and specificity, along-side cost and accessibility issues. Consequently, there's a pressing need for a marker that is economically feasible, rapid, and reliable. Presepsin (PSP), also known as soluble CD14 subtype (sCD14-ST), has emerged as a promising biomarker for early sepsis diagnosis. PSP, derived from soluble CD14, reflects the activation of monocytes/macrophages in response to bacterial infec-tions. It has shown potential as a marker of cellular immune response activation against patho-gens, with plasma concentrations increasing during bacterial infections and decreasing post-antibiotic treatment. Unlike traditional markers such as procalcitonin (PCT) and C-reactive protein (CRP), PSP specifically indicates monocyte/macrophage activation in bacterial infections. While limited studies in critical illness have explored PSP's role in sepsis, its diagnostic accuracy varies with threshold values, impacting sensitivity and specificity. Recent meta-analyses suggest PSP's diagnostic potential for sepsis, yet its standalone effectiveness in ICU infection management remains uncertain. This review provides a comprehensive overview of PSP's utility in ICU set-tings, including its diagnostic accuracy, prognostic value, therapeutic implications, challenges, and future directions.
Keywords:
presepsin
; sepsis
; critical care patients
1. Introduction
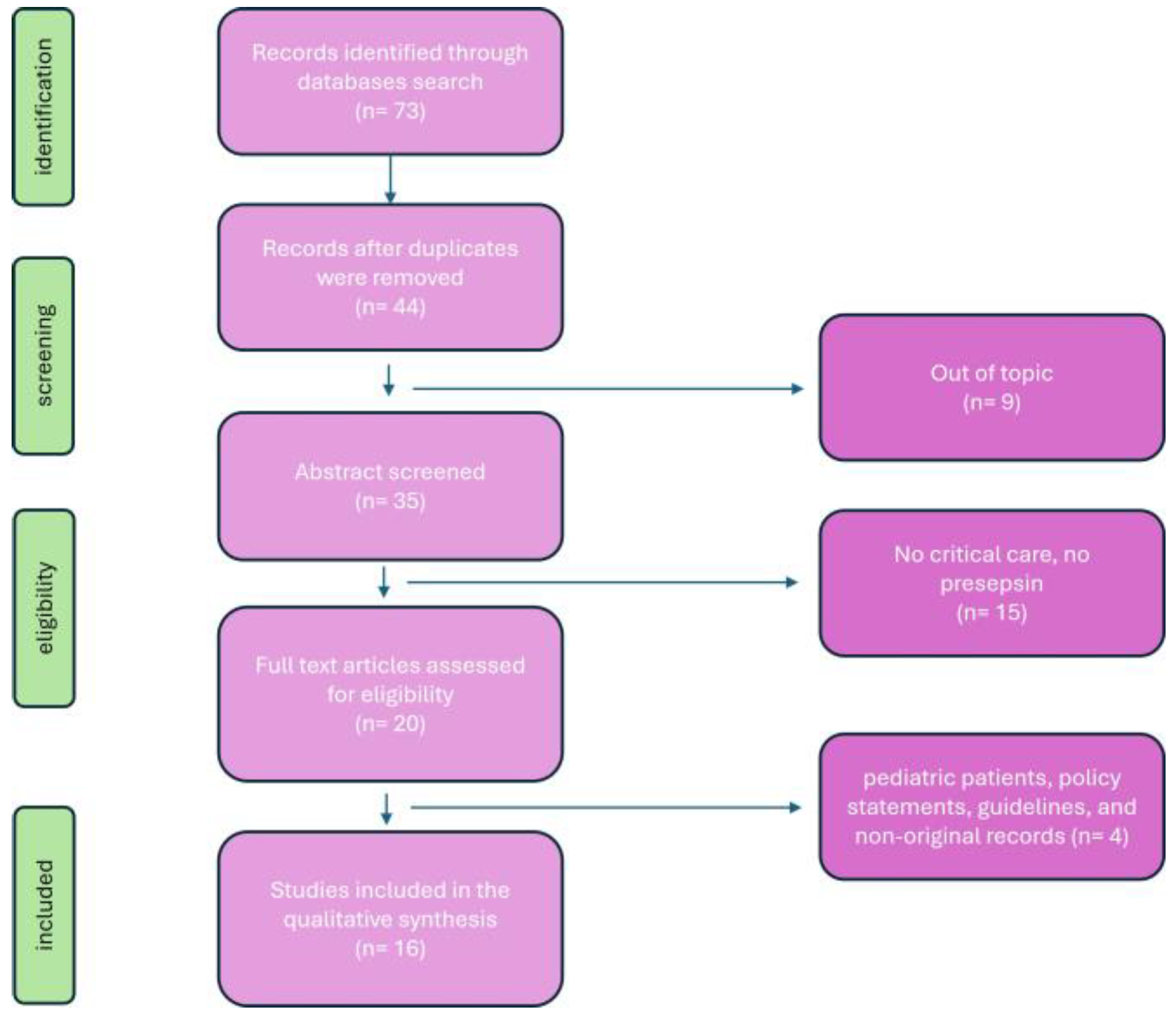
The accurate identification of bacterial infection is crucial for effective treatment and control of infectious diseases, but its recognition is often challenging as signs and symptoms overlap with other inflammatory disorders [1]. Current diagnostic approaches in intensive care unit (ICU) rely on microbiological culture, biochemical methods, and molecular techniques [2]. However, there is still no gold standard as these methods have significant limitations in sensitivity and specificity, and their implementation often requires expensive technologies and equipment, which may not be accessible to all laboratories [3]. Therefore, there is an urgent need for a marker that is economically feasible, rapid, simple, reliable, specific, and sensitive for the diagnosis of infection [4,5]. Presepsin (PSP), also known as soluble CD14 subtype (sCD14-ST) [6], is a promising biomarker that has garnered interest for its potential role in the early diagnosis and management of sepsis in ICU [7]. CD14 belongs to the Toll-like receptor (TLR) family, playing a significant role in identifying ligands from both gram-positive and gram-negative bacteria, thereby stimulating the inflammatory response [8]. CD14 exists in two forms: one anchored to the membrane (mCD14) of monocytes/macrophages, and the other soluble (sCD14) found in plasma [9]. In plasma, sCD14 is cleaved by cathepsin D into a small fragment, known as PSP. Plasma concentrations of PSP have shown an increase in response to bacterial infections and a decrease after antibiotic treatment [10]. Therefore, this molecule can be considered a marker of cellular immune response activation against pathogens. PSP secretion has also been associated with monocyte phagocytosis, suggesting that it could be measured in healthy, non-infected individuals [11]. Unlike traditional markers such as procalcitonin (PCT) and C-reactive protein (CRP), PSP specifically reflects the activation of monocytes/macrophages in response to bacterial infections [12]. Within the context of critical illness, limited studies have explored PSP in sepsis, revealing that the accuracy of PSP determination relies on the chosen threshold value. For instance, with a threshold set at 600 ng/mL, sensitivity reached 70.3%, and specificity was 81.3% [13]. However, when a higher threshold (> 860 ng/mL) was used, sensitivity improved to 71.4%, albeit at the cost of reduced specificity to 63.8%. A recent meta-analysis highlighted the diagnostic potential of PSP for sepsis, indicating high sensitivity and specificity [14]. Nevertheless, it is not yet shown whether PSP alone can effectively be used as an infection marker in the ICU. This review aims to provide a detailed overview of PSP’s utility in ICU settings, encompassing its diagnostic accuracy, prognostic value, therapeutic implications, challenges, and future directions. A review of literature was conducted to evaluate published articles documenting perioperative ultrasound diaphragm evaluation ("population") and the presence or development of DD ("outcome"). Six databases were searched: PubMed (1996–present), Embase (1974–present), Scopus (2004–present), SpringerLink (1950–present), Ovid Emcare (1995–present), and Google Scholar (2004–present). The search utilized keywords such as " presepsin", "presepsin in critical care", "sepsi and presepsin", "diagnostic presepsin", "prognostic presepsin" across these selected databases. Two authors (PF and PMU) retrieved full texts of relevant articles. All related titles and abstracts were reviewed, and full versions were obtained. Exclusion criteria included studies involving pediatric patients, policy statements, and guidelines. The quality of the retrieved articles was assessed through careful evaluation of their methodology, sample size, study design, and relevance to the topic of presepsin (Figure 1).
2.1.1. Immunobiology of Presepsin
CD14 is a membrane glycoprotein encoded by chromosome 5q and was first described in 1990 [15]. It serves as the receptor for lipopolysaccharide (LPS)-LPS-binding protein complexes, primarily found on monocytes/macrophages and, to a lesser extent, on neutrophil leukocytes [16]. Activation of tyrosine kinases and mitogen-activated protein kinases leads to the transcription of inflammation genes and the release of cytokines [17]. Subsequent activation of the secondary inflammatory cascade and acquired immunity further stimulates macrophages, neutrophils, and endothelial cells to release numerous other cytokines and synthesize adhesion molecules [18]. This can lead to an intense systemic inflammatory response with activation of coagulation and fibrinolysis mechanisms. The result of these defensive mechanisms can sometimes be disproportionate and counterproductive, resulting in serious syndromes such as systemic inflammatory response syndrome (SIRS), septic shock, disseminated intravascular coagulation, and multiorgan dysfunction [19]. In addition to the membrane-bound form of phagocytes, CD14 also exists in a soluble form, derived from secretion or cleavage by plasma proteases [20]. It plays a role in mediating the immune response to LPS in cells typically indicated as CD14-negative, such as endothelial and epithelial cells [21]. Other authors hypothesize that soluble forms of CD14 may modulate the innate response to bacterial endotoxins by transferring lipopolysaccharides from monocyte membranes to plasma lipoproteins [22]. Clinical studies on sCD14 show that the plasma concentration of these molecules significantly increase in septic patients, and this increase is related to the severity of the condition [23]. The soluble CD14 subtype is the N-terminal fragment of sCD14 derived from the antibacterial phagocytic activity of monocytes-macrophages and has been identified as a reliable marker of ongoing infectious processes in sepsis [24]. The metabolism and excretion of PSP are influenced by renal function, therefore special attention is needed in interpreting values in the presence of chronic renal failure [25]. Specifically, PSP concentration was higher in patients undergoing hemodialysis, hence a different threshold should be considered in these patients [26]. PSP concentrations are known to rise with age, necessitating careful consideration when assessing elderly patients [27]. Additionally, newborn, children and adolescent’s PSP values require particular attention [28]. Moreover, PSP levels can be influenced by the translocation of intestinal microbial flora [29,30]. Given that PSP is excreted through both the kidneys and the hepatobiliary system, elevated concentrations may be detectable [31]. These observations highlight the necessity of establishing adapted cut-off values for specific populations and conditions.
2.1.2. Diagnostic Utility of Presepsin
PSP demonstrates rapid kinetics, with elevated levels detectable within a few hours of infection onset [32]. Its ability to distinguish between septic and non-septic systemic inflammatory conditions makes it a valuable tool for early sepsis detection, although limited research has explored its utility in critically ill patients. Moreover, the interpretation and cutoff of presepsin should be carefully evaluated in critically ill patients, as they often simultaneously present multiple organ dysfunctions. Godnic et al [33] utilized a cut-off of 413 ng/L to diagnose bacterial infections in ICU patients. They found that PSP showed a higher area under the curve (AUC) compared to PCT, although it was lower than CRP. In another study including ICU patients, PSP demonstrated a good accuracy in predicting sepsis, with sensitivity and specificity values of 84.6% and 62.5%, respectively [34]. Notably, these findings were significantly associated with the APACHE II score. Sargentini et al [30] demonstrated that while PSP can effectively distinguish between septic and non-septic patients in the ICU, it is inferior in performance compared to PCT. The ALBIOS trial [13] observed that individuals infected with Gram-negative bacterial infections exhibited higher PSP levels compared to those with Gram-positive infections. Additionally, patients with bacterial infections, as figured out by site or blood culture, demonstrated significantly elevated PSP concentrations compared to individuals with negative culture results or those for whom no culture data were available. Endo et al [35] obtained contrasting results, showing no significant difference between Gram-positive and Gram-negative bacterial infections, and no significant disparities in PSP levels between the blood culture-positive and culture-negative groups. Currently, there are limited meta-analyses on the diagnostic efficiency of PSP compared to these biomarkers. A recent study [36] compared PSP with PCT for early sepsis diagnosis in critically ill patients and concluded that both markers have similar efficacy, suggesting their combined use. The study enrolled more than a thousand patients with confirmed infection and critical illnesses such as acute respiratory distress syndrome and sepsis. The diagnostic accuracy for detecting infection was found to be comparable between PCT and PSP, with sensitivity values of 0.80 and 0.84, and specificity values of 0.75 and 0.73, respectively. Both biomarkers proved to be valuable for the early diagnosis of sepsis and the reduction of mortality in critically ill adults. Similarly, a multicenter prospective study indicated that PSP is more closely associated with SOFA and APACHE scores than PCT in the clinical assessment of patients in emergency departments and ICU [37]. PSP was assessed as a prospective biomarker for bacterial infection decline among critical care patients [38]. In cases of clinical recurrence of sepsis, PSP levels remained elevated, while PCT levels normalized during the transient remission phase. The presence of persistently high PSP levels may serve as an indicator for clinicians to consider continuation of antibiotic therapy in patients with sepsis. Overall, despite these conflicting results, we can summarize that the efficiency of presepsin depends on the considered cutoff value. The variations in reported cutoff values across studies may be attributed to the heterogeneity of clinical settings, the sepsis criteria employed (pre- or post-Sepsis-3), study design (prospective vs. retrospective), comorbidities, or the type of sample used (plasma vs. whole blood vs. serum) for presepsin measurement.
2.1.3. Prognostic Value of Presepsin
The possibility of having early prognostic information in patients with suspected sepsis admitted to ICU could provide fundamental data that meet the clinical need for management and therapeutic differentiation based on risk stratification of major events and therefore prognosis. A few studies showed how patients with sepsis and septic shock who present high levels of PSP upon admission have a significantly higher probability of death at 30 days [39]. Hence, circulating PSP concentrations at admission may be used to stratify the risk of mortality. For instance, PSP concentrations on day 2 and day 7 post-admission were fund to be independently correlated not only with ICU mortality but also with short-term (28 days) and long-term (90 days) post-admission mortality [13]. Interestingly, the SOFA score was the only clinical variable associated with mortality in a multivariate analysis model that included procalcitonin. When procalcitonin was replaced with PSP in the model, the SOFA score was no longer significantly associated with mortality. The potential prognostic use of PSP determination appears to be a promising tool, albeit poorly evaluated in ICU. PSP was included in a population previously investigated [40] to assess the effectiveness of combing procalcitonin with a clinical score, the Multidimensional Prognostic Index (MPI), in stratifying the risk of one-month mortality [41]. Upon admission, both PCT and PSP were measured. The results indicated that while MPI effectively stratifies mortality risk upon admission nor did the median values of PCT and PSP. Consequently, these biomarkers did not demonstrate significant prognostic efficacy. However, only PSP adds prognostic value when measured in association with MPI in stratifying intermediate-risk patients compared to low-risk patients. The data from this study are consistent with recent literature in critical setting in which the prognostic value of PSP in stratifying short-term mortality risk in patients with pneumonia has been confirmed [42]. In this report, in more than hundred ICU patients the authors showed that PSP and PCT were significantly higher in septic than in non-septic patients. Moreover, in half of the patients, PSP capability to diagnose pneumoniae was significantly better than PCT. Jovanovic et al [43] investigated the prognostic significance of PSP for ventilator-associated pneumonia (VAP) and sepsis in critically injured patients necessitating mechanical ventilation. Their research revealed that PSP levels were notably elevated in patients who developed VAP. Moreover, PSP levels were significantly higher in patients diagnosed with sepsis compared to those with either VAP or SIRS. Zaho et al [44] found that PSP is an independent predictor of in-hospital mortality in a cohort of ARDS patients. Similar results have been described in other categories of critically ill patients, such as patients undergoing cardiac surgery, patients with cirrhosis, neonates with suspected sepsis, and patients with acute renal failure. In a separate analysis from the ALBIOS trial [45], which enrolled patients with severe sepsis or septic shock in ICUs, PSP levels were independently associated with both the number and severity of organ dysfunctions or failures, as well as with coagulation disorders and ICU mortality. Of note is the observation that not only admission biomarker values but also changes in concentration during monitoring seemed to provide interesting prognostic information that differentiates PSP from PCT. Indeed, not only PSP concentrations were significantly higher in patients who die, but in this group, they remained consistently elevated during monitoring. In this type of combined biomarker application that provides additional rather than mutually exclusive information, PCT and PSP determinations should be placed both in patients with suspected sepsis and in patients diagnosed with sepsis/septic shock: the physio-pathological complexity of the disease calls for a biochemical approach combined with a specific added value to clinical assessment. Then, Xiao et al [46] assessed the prognostic impact of PSP in sepsis. Their findings indicated that using PSP to guide antibiotic therapy did not adversely affect 28-day and 90-day survival rates. This approach appeared to outperform other conventional infection-related biomarkers like PCT. Enguix-Armada et al [47] investigated the prognostic potential of CRP, PCT, and mid-regional pro-adrenomedullin, along with PSP, measured within the initial 24 hours of ICU admission. They examined 28-day mortality and length of ICU stay as outcome variables. However, the authors did not find any prognostic value associated with PSP measured during the first 24 hours. In the study by Brodska et al [48] which included 30 consecutive patients admitted for sepsis to the mixed medical-surgical ICU, contrasting results were observed. Specifically, the study found that PSP did not demonstrate superior performance compared to traditional biomarkers such as PCT, CRP, and lactate in predicting mortality among critically ill patients with sepsis and SIRS. Koh et al [49] assessed the efficacy of PSP as a biomarker for predicting in-hospital mortality in 153 patients with sepsis or septic shock admitted to the ICU. While PSP values were elevated in the non-survivor group compared to the survivor group, the ROC analysis revealed poor performance of PSP in prognosticating sepsis outcomes. PSP levels exceeding 1176 pg/ml exhibited a sensitivity of 66.7% and specificity of 61.1% in predicting in-hospital mortality. In summary, several studies conducted in critical care settings comparing the diagnostic and prognostic efficacy of PSP with CRP and/or PCT have produced solid results. PSP demonstrates a performance that generally aligns with that of PCT and appears to be a valuable parameter associated with patient outcomes.
2.1.4. Therapeutic Implications
Current guidelines recommend initiating antibiotic therapy within one hour of sepsis diagnosis [2]. However, the duration of antibiotic treatment often depends on the physician’s judgment and may vary based on treatment protocols [50], leading in some cases to prolonged antibiotic use. Extended administration of antibiotics not only results in significant costs but also increases the risk of complications, mortality, and prolonged hospitalization [51,52]. PSP-guided therapy has shown promise in optimizing antibiotic use and guiding early interventions in septic patients [53]. However, this potential role has not been thoroughly investigated in the critical care setting. The ALBIOS sub-study suggested that PSP might offer valuable guidance for therapy in sepsis. Masson et al [45] investigated the potential of PSP as a biomarker in sepsis, discovering that PSP levels tended to rise in patients with positive microbiology and inappropriate antibiotic therapy. Growing evidence supports the potentially beneficial approaches of PSP-guided antibiotic escalation and de-escalation. Xiao et al [46] conducted a multicenter prospective cohort study aiming to investigate the utility of PSP in guiding physicians in the decision to continue or discontinue antibiotics for septic patients. The primary objective was to assess whether a PSP-based strategy would be linked to a reduction in antibiotic duration among septic patients, measured by the number of antibiotic-free days within a 28-day period or the duration until the initiation of the first antibiotic course. The authors showed that among patients with sepsis, employing a PSP-based antibiotic prescription strategy was linked with notable reductions in antibiotic treatment duration, ICU or hospital length of stay, and hospitalization costs. Importantly, these reductions occurred without any increase in mortality, recurrent infection rates, or risk of worsening organ failure. This targeted approach to therapy has the potential to improve patient outcomes while minimizing antibiotic overuse and associated complications.
3.1. Presepsin and COVID-19
In December 2019 a new zoonosis named COVID-19, caused by the new Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-CoV-2) appeared in China. The disease, characterized by clinical manifestations similar to ARDS, provoked a terrible pandemia from 2020, with an elevated numbers of critical patients that rapidly overcrowded the ICUs all over the world. The WHO updated at the 17 March 2024 the number of deaths at 7.040.264 [54]. Zaninotto at al [55] described a first case series of patients in whom PSP were dosed. The authors in few patients formulated these observations: 1) PSP were higher in patients who died; 2) PSP showed a statistically significant but poor correlation with CRP and PCT; 3) PSP levels were related to ICU LOS. From these first observations, PSP demonstrated a possible role in providing diagnostic and prognostic information in COVID-19 patients, even if the disease was caused by viral and not by bacterial pathogen. Generally, PSP values do not increase in patients with viral infections. Some years before COVID-19 outspread, Ozlem Demirpence [56] described an increase in PSP in patients affected by Crimean-Congo hemorrhagic fever; the PSP levels were related to disease severity. The authors speculated that elevated PSP levels are likely associated with macrophage activation also in a non-bacterial disease. Some years later, after COVID-19 outspread, high PSP levels were detected even in the mild COVID-19 [57]. Yamazaky et al [58] speculated that SARS-CoV-2 can directly infect monocytes to reduce CD14+/CD16- classical monocytes and increase CD14+/CD16+ intermediate monocytes, which have an increased phagocytic function, resulting in the release of cytokines including PSP in the early stage of the disease. On the other hand, the typical clinical presentation of COVID-19 was similar to ARDS, and Zhao and colleagues [44] described how PSP were considerably increased in patients with ARDS independently from the etiology, but patients with sepsis-related ARDS had notably higher plasma PSP levels than patients with non-sepsis-related ARDS. Following the first observation cited above, several studies investigated the role of PSP as a diagnostic and a prognostic tool in COVID-19 patients. Assal and colleagues [59] found that PSP levels were significantly elevated in patients presenting with severe COVID-19, and levels above 775 pg/ml was significantly associated with in-hospital mortality (sensitivity 73% and specificity 80%). They postulated that elevated PSP level indicates poor outcomes and should alert the physicians in making decisions regarding intensive care monitoring and further interventions. The same results were described by Kocyigit et al [60] that found that PSP levels were significantly higher in patients with SARS-CoV-2. Moreover, there was a significant correlation between PSP and disease severity. Lippi and colleagues [61] published the results of a pooled analysis of six studies with a total of 420 COVID-19 patients, whom 173 (41.2%) with a critical form of disease. They found that PSP levels were increased by 2.74-fold in COVID-19 patients with severe illness compared to those without. Guarino et al [62] published a meta-analysis of data from 707 patients from 15 studies, and they found that the pooled mean difference of PSP levels between high- and low-severity COVID-19 patients was 441.70 pg/ml (95%CI: 150.40–732.99 pg/ml). In another interesting study published by Dell’Aquila and colleagues [63], in a population of COVID-19 patients with acute respiratory failure in an emergency department, PSP was accurate predictor of 30-day mortality. PSP achieved a sensitivity of 54% and a specificity of 92% for a cut-off value of 871 pg/mL. The AUC for the ROC curve was 0.85. The authors proposed that PSP high specificity could help the early identification of patients who could benefit from more intensive care as soon as they enter the emergency department. Fukui et al [64] in a cohort oh 201 patients showed the high prognostic value of PSP in non-severe COVID 19 patients, suggesting that PSP might be a highly sensitive indicator of immunological reactions against infectious antigens in the early stage of COVID 19 infection, and might predict subsequent disease evolution. Different studies proposed a combination of clinical and biochemical markers of inflammation to better detect patients affected by COVID-19 with poor prognosis underlining how high PSP levels in the first 7 days of hospital stay was a good biomarker of poor prognosis [65,66,67,68]. More accurately, Yamazaky et al [58] evaluated PSP values at multiple time points as well as the change in values after admission for patients with COVID-19. The authors observed an elevation in PSP values in non survivors over time; however, these elevations were not observed in survivors. Moreover, some non-survivor patients with COVID-19 showed renal dysfunction, so the authors adjusted PSP for renal failure, and significant differences in PSP values remained. These data indicated that PSP might be used as predictive markers, apart from renal function. In summary, PSP could be a useful tool in diagnosis and prognostication in COVID-19. The PSP levels and trend correlated to the severity and the evolution of the disease, so high PSP level should alert the physicians in making decisions regarding intensive care monitoring and further interventions.
Figure 2.
The mechanism of presepsin production.
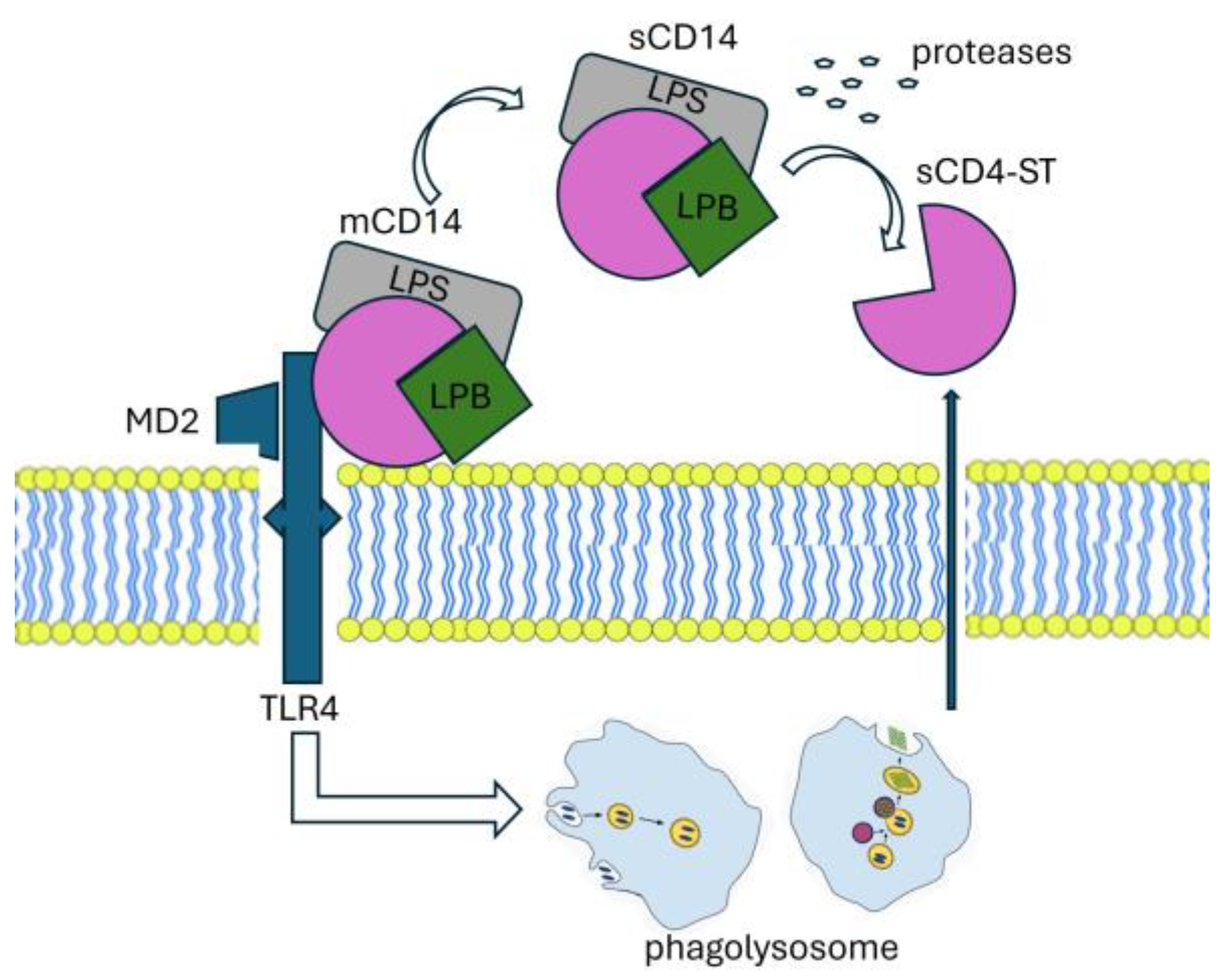
The production mechanism of presepsin involves various molecular players. CD14, found in two forms - membrane-bound (mCD14) and soluble (sCD14), interacts with a complex resulting in lipopolysaccharide (LPS) and lipoprotein binding protein (LBP). This complex, along with Toll-like receptor 4 (TLR4) and MD2, is internalized into a phagolysosome. Within this compartment, enzymatic processing facilitated by cathepsin D leads to the cleavage of CD14, resulting in the release of a small soluble peptide fragment known as soluble CD14 subtype (sCD14-ST), or presepsin. This presepsin fragment is subsequently released into the bloodstream via proteolysis and exocytosis. LBP: Lipoprotein Binding Protein, LPS: lipopolysaccharide, TLR4: Toll-like receptor, MD2:co-protein of TLR4.

Table 1.
Principal investigation on Presepsin in critical care setting.
| Study | Patients |
Design | Main Findings |
|---|---|---|---|
| Masson et al [45] |
100 ICU patients; severe sepsis or septic shock |
Multicenter RTC |
PSP, measured at day 1, was higher in non-survivors than in survivors. The evolution of PSP levels over time was significantly different in survivors compared to non-survivors; PSP concentrations on day 2 and day 7 post-admission were independently correlated with 28 days and 90 days post-admission mortality. |
| Endo et al [37] | 103 ICU patients; sepsis or septic shock | Multicenter prospective study | PSP decreased on days 3 and 7 after ICU admission in survivors. PSP was more closely associated with SOFA and APACHE scores than PCT. |
| Endo et al [35] | 207 ICU patients; suspected sepsis | Multicenter prospective study | PSP does not differ between patients with Gram-positive vs Gram-negative bacterial infections. The sensitivity for discrimination of bacterial and nonbacterial infectious diseases of blood culture was 35.4 % vs PSP was 91.9 %. |
| Godnic et al [33] | 47 ICU patients | Comparative study three groups: SIRS, sepsis, septic shock |
bacterial infection showed statistical significance in PSP, CRP not in PCT. The severity of diagnosed SIRS was significantly associated only with PCT. Values of PCT were the only ones to predict SIRS severity and could distinguish between sepsis and severe sepsis or septic shock. |
| Liu et al [69] | 859 hospitalized patients; SIRS | Single-center prospective observational study | PSP increased with sepsis severity. PSP demonstrated effectiveness in predicting sepsis (sensitivity and specificity 84.6% and 62.5%). PSP in septic were higher in non-survivors than in survivors at 28 days. |
| Sargentini et al [30] |
21 ICU patients | Single-center, prospective observational study | ROC for the sepsis diagnosis was 0.945 PCT vs 0.756 for PSP. While PSP could effectively distinguish between septic and non-septic patients in the ICU, its performance was inferior compared to PCT. |
| Sargentini et al [38] |
64 ICU patients | Single-center prospective observational study | PSP levels remained elevated in recurrent septic patients, while PCT levels normalized during the transient remission phase. The presence of persistently high PSP levels may serve as an indicator for clinicians to consider continuation of antibiotic therapy in patients with sepsis. |
| Carpio et al [39] | 246 patients included | Single-center, prospective observational study. SIRS and/or sepsis vs healthy | PSP were significantly different in patients with SIRS, sepsis, severe sepsis, and septic shock and showed strong association with 30-day mortality. Combination of PSP with MEDS score improved the performance for outcome prediction. PSP values in the course of the disease were statistically different between non-survivors and survivors. |
| Klouche et al [42] | 144 ICU patients | Observational prospective study | PSP and PCT were significantly higher in septic than in non-septic patients. The prognostic value of PSP in stratifying short-term mortality risk in patients with pneumonia has been confirmed. In the patients admitted for acute respiratory failure, the accuracy of PSP to diagnose sCAP was significantly better than PCT. |
| Zaho et al [44] |
225 ARDS patients | Multicenter prospective cohort trial sepsis-related ARDS vs non-sepsis-related ARDS | PSP was found to be an independent predictor of in-hospital mortality in sepsis-related ARDS. Patients with sepsis-related ARDS had higher PSP levels than patients with non-sepsis-related ARDS. ROC PSP (0.81) was significantly greater than that of PCT (0.62). Among patients with sepsis-related ARDS, PSP levels were significantly higher in non-survivors than in survivors. |
| Xiao et al [46] | 656 patients | Multicenter prospective cohort trial |
PSP to guide antibiotic therapy-> not adversely affect 28-day and 90-day survival rates. Patients in the PSP group also had significantly more days without antibiotics than those in the control group. |
| Brodska et al [48] |
60 ICU patients | Single-center observational prospective | PSP did not correlate with SOFA on day 1. PSP did not demonstrate superior performance compared to traditional biomarkers such as PCT, CRP, and lactate in predicting mortality among critically ill patients with sepsis and SIRS. |
| Koh et al [49] | 153 patient’s septic and septic shock | Retrospective cohort survival vs non-survival |
PSP values elevated in non-survivor vs survivor group. PSP levels exceeding 1176 pg/ml exhibited a sensitivity of 66.7% and specificity of 61.1% in predicting in-hospital mortality. |
| Yu et al [53] |
109 patients | Monocentric observational prospective Survival vs non survival |
PSP levels in the survival group decreased persistently, while they rose gradually in the non-survival group. |
| Masson et al [45] | 997 patients; severe sepsis/septic shock | Multicenter randomized trial | PSP concentration at admission was associated with SOFA score. PSP levels tended to decrease in patients with negative blood cultures and in those with positive blood cultures and appropriate antibiotic therapy, while raised in patients with positive microbiology and inappropriate antibiotic therapy. |
| Kondo et al [36] |
3012 patients |
Meta-analysis |
no differences in both pooled sensitivities and specificities between PCT and PSP (0.80 vs 0.84, and 0.75 vs 0.73). Both biomarkers proved to be valuable for the early diagnosis of sepsis and the reduction of mortality in critically ill adults. |
4. Conclusions
PSP has the potential to significantly improve patient outcomes in critical care settings by enabling earlier diagnosis and initiation of appropriate treatment for sepsis. Ongoing clinical trials investigated its effectiveness in various critical illness scenarios, including the diagnosing sepsis in patients with suspected infection, the guiding antibiotic treatment decisions, and the monitoring treatment response and predicting patient outcomes. However, further research is needed to further elucidate PSP's clinical utility, refine its diagnostic and prognostic capabilities, and optimize its integration into sepsis management protocols in the ICU.
Author Contributions
L.F., F.P., G.S, S.P., V.R., and A.P. Conceptualization, L.F, G.S., F.P., S.P. and A.G..; methodology, S.P.,V.R. G.S..; software, G.S.; formal analysis, M.U.; investigation, P.F.., M.G. and A.M..; data curation, P.F., M.G..; writing—original draft preparation, P.F., M.G., G.S., M.U.; writing—review and editing, G.S., P.F., M.U., A.P.; supervision, A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
not applicable.
Informed Consent Statement
not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wang, H.; Zhang, W.; Tang, Y.-W. Clinical Microbiology in Detection and Identification of Emerging Microbial Pathogens: Past, Present and Future. Emerg Microbes Infect 11, 2579–2589. [CrossRef]
- Dellinger, R.P.; Rhodes, A.; Evans, L.; Alhazzani, W.; Beale, R.; Jaeschke, R.; Machado, F.R.; Masur, H.; Osborn, T.; Parker, M.M.; et al. Surviving Sepsis Campaign. Crit Care Med 2023, 51, 431–444. [Google Scholar] [CrossRef] [PubMed]
- Peri, A.M.; Stewart, A.; Hume, A.; Irwin, A.; Harris, P.N.A. New Microbiological Techniques for the Diagnosis of Bacterial Infections and Sepsis in ICU Including Point of Care. Curr Infect Dis Rep 2021, 23, 12. [Google Scholar] [CrossRef] [PubMed]
- Burillo, A.; Bouza, E. Use of Rapid Diagnostic Techniques in ICU Patients with Infections. BMC Infect Dis 2014, 14, 593. [Google Scholar] [CrossRef] [PubMed]
- Heilmann, E.; Gregoriano, C.; Schuetz, P. Biomarkers of Infection: Are They Useful in the ICU? Semin Respir Crit Care Med 2019, 40, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Marazzi, M.G.; Randelli, F.; Brioschi, M.; Drago, L.; Romanò, C.L.; Banfi, G.; Massaccesi, L.; Crapanzano, C.; Morelli, F.; Corsi Romanelli, M.M.; et al. Presepsin: A Potential Biomarker of PJI? A Comparative Analysis with Known and New Infection Biomarkers. Int J Immunopathol Pharmacol 2018, 31, 394632017749356. [Google Scholar] [CrossRef] [PubMed]
- Aliu-Bejta, A.; Atelj, A.; Kurshumliu, M.; Dreshaj, S.; Baršić, B. Presepsin Values as Markers of Severity of Sepsis. Int J Infect Dis 2020, 95, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ciesielska, A.; Matyjek, M.; Kwiatkowska, K. TLR4 and CD14 Trafficking and Its Influence on LPS-Induced pro-Inflammatory Signaling. Cell Mol Life Sci 2021, 78, 1233–1261. [Google Scholar] [CrossRef] [PubMed]
- Funda, D.P.; Tučková, L.; Farré, M.A.; Iwase, T.; Moro, I.; Tlaskalová-Hogenová, H. CD14 Is Expressed and Released as Soluble CD14 by Human Intestinal Epithelial Cells In Vitro: Lipopolysaccharide Activation of Epithelial Cells Revisited. Infect Immun 2001, 69, 3772–3781. [Google Scholar] [CrossRef] [PubMed]
- Galliera, E.; Massaccesi, L.; Vecchi, E. de; Banfi, G.; Romanelli, M.M.C. Clinical Application of Presepsin as Diagnostic Biomarker of Infection: Overview and Updates. Clinical Chemistry and Laboratory Medicine (CCLM) 2020, 58, 11–17. [Google Scholar] [CrossRef]
- Ikegame, A.; Kondo, A.; Kitaguchi, K.; Sasa, K.; Miyoshi, M. Presepsin Production in Monocyte/Macrophage-Mediated Phagocytosis of Neutrophil Extracellular Traps. Sci Rep 2022, 12, 5978. [Google Scholar] [CrossRef]
- Maddaloni, C.; De Rose, D.U.; Santisi, A.; Martini, L.; Caoci, S.; Bersani, I.; Ronchetti, M.P.; Auriti, C. The Emerging Role of Presepsin (P-SEP) in the Diagnosis of Sepsis in the Critically Ill Infant: A Literature Review. International Journal of Molecular Sciences 2021, 22, 12154. [Google Scholar] [CrossRef]
- Masson, S.; Caironi, P.; Spanuth, E.; Thomae, R.; Panigada, M.; Sangiorgi, G.; Fumagalli, R.; Mauri, T.; Isgrò, S.; Fanizza, C.; et al. Presepsin (Soluble CD14 Subtype) and Procalcitonin Levels for Mortality Prediction in Sepsis: Data from the Albumin Italian Outcome Sepsis Trial. Crit Care 2014, 18, R6. [Google Scholar] [CrossRef]
- Wu, J.; Hu, L.; Zhang, G.; Wu, F.; He, T. Accuracy of Presepsin in Sepsis Diagnosis: A Systematic Review and Meta-Analysis. PLoS One 2015, 10, e0133057. [Google Scholar] [CrossRef] [PubMed]
- Beekhuizen, H.; Blokland, I.; Corsèl-van Tilburg, A.J.; Koning, F.; van Furth, R. CD14 Contributes to the Adherence of Human Monocytes to Cytokine-Stimulated Endothelial Cells. J Immunol 1991, 147, 3761–3767. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.D.; Ramos, R.A.; Tobias, P.S.; Ulevitch, R.J.; Mathison, J.C. CD14, a Receptor for Complexes of Lipopolysaccharide (LPS) and LPS Binding Protein. Science 1990, 249, 1431–1433. [Google Scholar] [CrossRef] [PubMed]
- Hamidzadeh, K.; Christensen, S.M.; Dalby, E.; Chandrasekaran, P.; Mosser, D.M. Macrophages and the Recovery from Acute and Chronic Inflammation. Annu Rev Physiol 2017, 79, 567–592. [Google Scholar] [CrossRef] [PubMed]
- Megha, KB.; Joseph, X.; Akhil, V.; Mohanan, PV. Cascade of Immune Mechanism and Consequences of Inflammatory Disorders. Phytomedicine 2021, 91, 153712. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, A. Cascade System Activation in Shock. Acta Anaesthesiol Scand Suppl 1993, 98, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Grunwald, U.; Krüger, C.; Westermann, J.; Lukowsky, A.; Ehlers, M.; Schütt, C. An Enzyme-Linked Immunosorbent Assay for the Quantification of Solubilized CD14 in Biological Fluids. J Immunol Methods 1992, 155, 225–232. [Google Scholar] [CrossRef]
- Frey, E.A.; Miller, D.S.; Jahr, T.G.; Sundan, A.; Bazil, V.; Espevik, T.; Finlay, B.B.; Wright, S.D. Soluble CD14 Participates in the Response of Cells to Lipopolysaccharide. J Exp Med 1992, 176, 1665–1671. [Google Scholar] [CrossRef]
- Kitchens, R.L.; Thompson, P.A.; Viriyakosol, S.; O’Keefe, G.E.; Munford, R.S. Plasma CD14 Decreases Monocyte Responses to LPS by Transferring Cell-Bound LPS to Plasma Lipoproteins. J Clin Invest 2001, 108, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Brunialti, M.K.C.; Martins, P.S.; Barbosa de Carvalho, H.; Machado, F.R.; Barbosa, L.M.; Salomao, R. TLR2, TLR4, CD14, CD11B, and CD11C Expressions on Monocytes Surface and Cytokine Production in Patients with Sepsis, Severe Sepsis, and Septic Shock. Shock 2006, 25, 351–357. [Google Scholar] [CrossRef]
- Shirakawa, K.; Naitou, K.; Hirose, J.; Takahashi, T.; Furusako, S. Presepsin (sCD14-ST): Development and Evaluation of One-Step ELISA with a New Standard That Is Similar to the Form of Presepsin in Septic Patients. Clin Chem Lab Med 2011, 49, 937–939. [Google Scholar] [CrossRef]
- Miyoshi, M.; Inoue, Y.; Nishioka, M.; Ikegame, A.; Nakao, T.; Kishi, S.; Doi, T.; Nagai, K. Clinical Evaluation of Presepsin Considering Renal Function. PLoS One 2019, 14, e0215791. [Google Scholar] [CrossRef] [PubMed]
- Dragoş, D.; Ghenu, M.I.; Timofte, D.; Balcangiu-Stroescu, A.-E.; Ionescu, D.; Manea, M.M. The Cutoff Value of Presepsin for Diagnosing Sepsis Increases with Kidney Dysfunction, a Cross-Sectional Observational Study. Medicine (Baltimore) 2023, 102, e32620. [Google Scholar] [CrossRef]
- Wang, S.; Ruan, W.-Q.; Yu, Z.; Zhao, X.; Chen, Z.-X.; Li, Q. Validity of Presepsin for the Diagnosis and Prognosis of Sepsis in Elderly Patients Admitted to the Intensive Care Unit. Minerva Anestesiol 2020, 86, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Capossela, L.; Margiotta, G.; Ferretti, S.; Curatola, A.; Bertolaso, C.; Pansini, V.; Di Sarno, L.; Gatto, A. Presepsin as a Diagnostic Marker of Sepsis in Children and Adolescents: A Short Critical Update. Acta Biomed 2023, 94, e2023062. [Google Scholar] [CrossRef]
- Marascio, N.; Scarlata, G.G.M.; Romeo, F.; Cicino, C.; Trecarichi, E.M.; Quirino, A.; Torti, C.; Matera, G.; Russo, A. The Role of Gut Microbiota in the Clinical Outcome of Septic Patients: State of the Art and Future Perspectives. Int J Mol Sci 2023, 24, 9307. [Google Scholar] [CrossRef]
- Sargentini, V.; Ceccarelli, G.; D’Alessandro, M.; Collepardo, D.; Morelli, A.; D’Egidio, A.; Mariotti, S.; Nicoletti, A.M.; Evangelista, B.; D’Ettorre, G.; et al. Presepsin as a Potential Marker for Bacterial Infection Relapse in Critical Care Patients. A Preliminary Study. Clin Chem Lab Med 2015, 53, 567–573. [Google Scholar] [CrossRef]
- Xiao, H.-L.; Wang, G.-X.; Wang, Y.; Tan, Z.-M.; Zhou, J.; Yu, H.; Xie, M.-R.; Li, C.-S. Dynamic Blood Presepsin Levels Are Associated with Severity and Outcome of Acute Pancreatitis: A Prospective Cohort Study. World J Gastroenterol 2022, 28, 5203–5216. [Google Scholar] [CrossRef]
- Ali, F.T.; Ali, M.A.M.; Elnakeeb, M.M.; Bendary, H.N.M. Presepsin Is an Early Monitoring Biomarker for Predicting Clinical Outcome in Patients with Sepsis. Clin Chim Acta 2016, 460, 93–101. [Google Scholar] [CrossRef]
- Godnic, M.; Stubljar, D.; Skvarc, M.; Jukic, T. Diagnostic and Prognostic Value of sCD14-ST--Presepsin for Patients Admitted to Hospital Intensive Care Unit (ICU). Wien Klin Wochenschr 2015, 127, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Chen, Y.-X.; Yin, Q.; Zhao, Y.-Z.; Li, C.-S. Diagnostic Value and Prognostic Evaluation of Presepsin for Sepsis in an Emergency Department. Crit Care 2013, 17, R244. [Google Scholar] [CrossRef]
- Endo, S.; Suzuki, Y.; Takahashi, G.; Shozushima, T.; Ishikura, H.; Murai, A.; Nishida, T.; Irie, Y.; Miura, M.; Iguchi, H.; et al. Usefulness of Presepsin in the Diagnosis of Sepsis in a Multicenter Prospective Study. J Infect Chemother 2012, 18, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Umemura, Y.; Hayashida, K.; Hara, Y.; Aihara, M.; Yamakawa, K. Diagnostic Value of Procalcitonin and Presepsin for Sepsis in Critically Ill Adult Patients: A Systematic Review and Meta-Analysis. J Intensive Care 2019, 7, 22. [Google Scholar] [CrossRef]
- Endo, S.; Suzuki, Y.; Takahashi, G.; Shozushima, T.; Ishikura, H.; Murai, A.; Nishida, T.; Irie, Y.; Miura, M.; Iguchi, H.; et al. Presepsin as a Powerful Monitoring Tool for the Prognosis and Treatment of Sepsis: A Multicenter Prospective Study. J Infect Chemother 2014, 20, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Sargentini, V.; Collepardo, D.; D Alessandro, M.; Petralito, G.; Ceccarelli, G.; Alessandri, F.; Piciocchi, A.; Angeloni, A.; Venditti, M.; Bachetoni, A. Role of Biomarkers in Adult Sepsis and Their Application for a Good Laboratory Practice: A Pilot Study. J Biol Regul Homeost Agents 2017, 31, 1147–1154. [Google Scholar] [PubMed]
- Carpio, R.; Zapata, J.; Spanuth, E.; Hess, G. Utility of Presepsin (sCD14-ST) as a Diagnostic and Prognostic Marker of Sepsis in the Emergency Department. Clin Chim Acta 2015, 450, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; Rengo, F.; Marchionni, N.; Sancarlo, D.; Fontana, A.; Panza, F.; Ferrucci, L. ; FIRI-SIGG Study Group Comparing the Prognostic Accuracy for All-Cause Mortality of Frailty Instruments: A Multicentre 1-Year Follow-up in Hospitalized Older Patients. PLoS One 2012, 7, e29090. [Google Scholar] [CrossRef]
- Pilotto, A.; Dini, S.; Daragjati, J.; Miolo, M.; Mion, M.M.; Fontana, A.; Storto, M.L.; Zaninotto, M.; Cella, A.; Carraro, P.; et al. Combined Use of the Multidimensional Prognostic Index (MPI) and Procalcitonin Serum Levels in Predicting 1-Month Mortality Risk in Older Patients Hospitalized with Community-Acquired Pneumonia (CAP): A Prospective Study. Aging Clin Exp Res 2018, 30, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Klouche, K.; Cristol, J.P.; Devin, J.; Gilles, V.; Kuster, N.; Larcher, R.; Amigues, L.; Corne, P.; Jonquet, O.; Dupuy, A.M. Diagnostic and Prognostic Value of Soluble CD14 Subtype (Presepsin) for Sepsis and Community-Acquired Pneumonia in ICU Patients. Ann Intensive Care 2016, 6, 59. [Google Scholar] [CrossRef] [PubMed]
- Jovanovic, B.; Djuric, O.; Denic, L.; Isakovic, A.; Doklestić, K.; Stankovic, S.; Vidičević, S.; Palibrk, I.; Samardzic, J.; Bumbasirevic, V. Prognostic Value of Soluble CD14-ST (Presepsin) in Diagnosis of Ventilator-Associated Pneumonia and Sepsis in Trauma Patients. Vojnosanitetski pregled 2017, 75, 27–27. [Google Scholar] [CrossRef]
- Zhao, J.; Tan, Y.; Wang, L.; Shi, Y. Discriminatory Ability and Prognostic Evaluation of Presepsin for Sepsis-Related Acute Respiratory Distress Syndrome. Sci Rep 2020, 10, 9114. [Google Scholar] [CrossRef] [PubMed]
- Masson, S.; Caironi, P.; Fanizza, C.; Thomae, R.; Bernasconi, R.; Noto, A.; Oggioni, R.; Pasetti, G.S.; Romero, M.; Tognoni, G.; et al. Circulating Presepsin (Soluble CD14 Subtype) as a Marker of Host Response in Patients with Severe Sepsis or Septic Shock: Data from the Multicenter, Randomized ALBIOS Trial. Intensive Care Med 2015, 41, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Wang, G.; Wang, Y.; Tan, Z.; Sun, X.; Zhou, J.; Duan, M.; Zhi, D.; Tang, Z.; Hang, C.; et al. Potential Value of Presepsin Guidance in Shortening Antibiotic Therapy in Septic Patients: A Multicenter, Prospective Cohort Trial. Shock 2022, 57, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Enguix-Armada, A.; Escobar-Conesa, R.; García-De La Torre, A.; De La Torre-Prados, M.V. Usefulness of Several Biomarkers in the Management of Septic Patients: C-Reactive Protein, Procalcitonin, Presepsin and Mid-Regional pro-Adrenomedullin. Clin Chem Lab Med 2016, 54, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Brodska, H.; Valenta, J.; Pelinkova, K.; Stach, Z.; Sachl, R.; Balik, M.; Zima, T.; Drabek, T. Diagnostic and Prognostic Value of Presepsin vs. Established Biomarkers in Critically Ill Patients with Sepsis or Systemic Inflammatory Response Syndrome. Clin Chem Lab Med 2018, 56, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.S.; Kim, Y.J.; Kang, D.H.; Lee, J.E.; Lee, S.-I. Usefulness of Presepsin in Predicting the Prognosis of Patients with Sepsis or Septic Shock: A Retrospective Cohort Study. Yeungnam Univ J Med 2021, 38, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, J.; Rhee, C.; Klompas, M. A Critical Analysis of the Literature on Time-to-Antibiotics in Suspected Sepsis. J Infect Dis 2020, 222, S110–S118. [Google Scholar] [CrossRef]
- Cortegiani, A.; Antonelli, M.; Falcone, M.; Giarratano, A.; Girardis, M.; Leone, M.; Pea, F.; Stefani, S.; Viaggi, B.; Viale, P. Rationale and Clinical Application of Antimicrobial Stewardship Principles in the Intensive Care Unit: A Multidisciplinary Statement. J Anesth Analg Crit Care 2023, 3, 11. [Google Scholar] [CrossRef]
- Llor, C.; Bjerrum, L. Antimicrobial Resistance: Risk Associated with Antibiotic Overuse and Initiatives to Reduce the Problem. Ther Adv Drug Saf 2014, 5, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Qi, Z.; Hang, C.; Fang, Y.; Shao, R.; Li, C. Evaluating the Value of Dynamic Procalcitonin and Presepsin Measurements for Patients with Severe Sepsis. Am J Emerg Med 2017, 35, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Aikebaier, S. COVID-19, New Challenges to Human Safety: A Global Review. Front Public Health 2024, 12, 1371238. [Google Scholar] [CrossRef] [PubMed]
- Zaninotto, M.; Mion, M.M.; Cosma, C.; Rinaldi, D.; Plebani, M. Presepsin in Risk Stratification of SARS-CoV-2 Patients. Clin Chim Acta 2020, 507, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Demirpençe, Ö.; Doğan, H.O.; Erşan, S.; Şahin, M.; Şahin, H.; Bakır, M. Presepsin Levels of Patients with Crimean-Congo Hemorrhagic Fever. Jpn J Infect Dis 2016, 69, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Karacaer, C.; Sert, H.; Demirci, T.; Varım, C.; Kaya, G.; Genc, A.B.; Ergenc, D.C.H.; Ergenc, Z.; Yaylacı, S.; Nalbant, A.; et al. The Significance of a Novel Inflammatory Biomarker, Presepsin, in Predicting Disease Prognosis in Patients with COVID-19. Eur Rev Med Pharmacol Sci 2022, 26, 8612–8619. [Google Scholar] [CrossRef]
- Yamazaki, A.; Nukui, Y.; Kameda, T.; Saito, R.; Koda, Y.; Ichimura, N.; Tohda, S.; Ohkawa, R. Variation in Presepsin and Thrombomodulin Levels for Predicting COVID-19 Mortality. Sci Rep 2023, 13, 21493. [Google Scholar] [CrossRef] [PubMed]
- Assal, H.H.; Abdelrahman, S.M.; Abdelbasset, M.A.; Abdelaziz, M.; Sabry, I.M.; Shaban, M.M. Presepsin as a Novel Biomarker in Predicting In-Hospital Mortality in Patients With COVID-19 Pneumonia. Int J Infect Dis 2022, 118, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Kocyigit, A.; Sogut, O.; Durmus, E.; Kanimdan, E.; Guler, E.M.; Kaplan, O.; Yenigun, V.B.; Eren, C.; Ozman, Z.; Yasar, O. Circulating Furin, IL-6, and Presepsin Levels and Disease Severity in SARS-CoV-2-Infected Patients. Sci Prog 2021, 104, 368504211026119. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Henry, B.M. Presepsin Value Predicts the Risk of Developing Severe/Critical COVID-19 Illness: Results of a Pooled Analysis. Clin Chem Lab Med 2022, 60, e1–e3. [Google Scholar] [CrossRef]
- Guarino, M.; Perna, B.; Maritati, M.; Remelli, F.; Trevisan, C.; Spampinato, M.D.; Costanzini, A.; Volpato, S.; Contini, C.; De Giorgio, R. Presepsin Levels and COVID-19 Severity: A Systematic Review and Meta-Analysis. Clin Exp Med 2023, 23, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, P.; Raimondo, P.; Orso, D.; De Luca, P.; Pozzessere, P.; Parisi, C.V.; Bove, T.; Vetrugno, L.; Grasso, S.; Procacci, V. A Simple Prognostic Score Based on Troponin and Presepsin for COVID-19 Patients Admitted to the Emergency Department: A Single-Center Pilot Study. Acta Biomed 2021, 92, e2021233. [Google Scholar] [CrossRef] [PubMed]
- Fukui, S.; Ikeda, K.; Kobayashi, M.; Nishida, K.; Yamada, K.; Horie, S.; Shimada, Y.; Miki, H.; Goto, H.; Hayashi, K.; et al. Predictive Prognostic Biomarkers in Patients with COVID-19 Infection. Mol Med Rep 2023, 27, 15. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Hur, M.; Kim, H.; Lee, C.H.; Lee, J.H.; Kim, H.W.; Nam, M. Prognostic Utility of Procalcitonin, Presepsin, and the VACO Index for Predicting 30-Day Mortality in Hospitalized COVID-19 Patients. Ann Lab Med 2022, 42, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Lee, H.; Lee, S.H.; Jo, S.J.; Lee, J.; Lim, J. Usefulness of Monocyte Distribution Width and Presepsin for Early Assessment of Disease Severity in COVID-19 Patients. Medicine (Baltimore) 2022, 101, e29592. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, N.; Matsuyama, S.; Matsuoka, M.; Kitamura, I.; Miyashita, K.; Kitagawa, Y.; Imai, K.; Ogawa, K.; Maeda, T.; Saito, Y.; et al. Serum Stratifin and Presepsin as Candidate Biomarkers for Early Detection of COVID-19 Disease Progression. J Pharmacol Sci 2022, 150, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Ishikura, H.; Maruyama, J.; Nakashio, M.; Hoshino, K.; Morimoto, S.; Izutani, Y.; Noake, J.; Yamagaito, T.; Yoshida, M.; Kitamura, T.; et al. Daily Combined Measurement of Platelet Count and Presepsin Concentration Can Predict In-Hospital Death of Patients with Severe Coronavirus Disease 2019 (COVID-19). Int J Hematol 2023, 117, 845–855. [Google Scholar] [CrossRef]
- Liu, B.; Yin, Q.; Chen, Y.-X.; Zhao, Y.-Z.; Li, C.-S. Role of Presepsin (sCD14-ST) and the CURB65 Scoring System in Predicting Severity and Outcome of Community-Acquired Pneumonia in an Emergency Department. Respir Med 2014, 108, 1204–1213. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of search strategy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



