
Submitted:
30 May 2024
Posted:
03 June 2024
You are already at the latest version
Abstract
Background: The goal of this study was to evaluate the effect of Extracorporeal Membrane Oxygenator (ECMO) on mortality in patients with cardiogenic shock excluding Impella and IABP use. Method: The large Nationwide Inpatient Sample (NIS) database was utilized to study any association between the use of ECMO in adults over age of 18 on mortality and complications with a diagnosis of cardiogenic shocks. Results: ICD-10 codes for ECMO, and cardiogenic shock for available years 2016-2020 were utilized. A total of 796,585 (age 66.5±14.4) patients had a diagnosis of cardiogenic shock excluding Impella. 13,160 (age 53.7±15.4) were treated with ECMO without IABP. Total inpatient mortality without any device was 32.7%. It was 47.9% with ECMO. Using multivariate analysis adjusting for 47 variables such as age, gender, race, lactic acidosis, three-vessel intervention, left main myocardial infarction, cardiomyopathy, systolic heart failure, acute ST-elevation myocardial infarction, peripheral vascular disease, chronic renal disease, etc., ECMO utilization remained highly associated with mortality (OR: 1.78, CI: 1.6-1.9, p<0.001). Evaluating teaching hospitals only revealed similar findings. Major complications were also high in ECMO cohort. Conclusion: In patients with cardiogenic shock, the use of ECMO was associated with the high in hospital mortality regardless of comorbid condition, high-risk futures, or type of hospital.
Keywords:
MCS
; mechanical circulatory support
; ECMO/IABP/Tandem/Impella
; CS - Shock
; Cardiogenic
; shock
; cardiac assist device
; artificial heart
; IABP
; Impella
; cardiac arrest
Introduction
Cardiogenic shock, a devastating clinical consequence of acute myocardial infarction (AMI) and the primary contributor to post-MI mortality, occurs in approximately 5-15% of patients experiencing AMI due to deleterious effects of severe ischemia on left ventricular function [1,2]. It is characterized as systolic blood pressure below 90 mm Hg for 30 minutes or using inotropic agents to keep systolic blood pressure over 90 mm Hg and existing end-organ damage with subsequent diminished tissue perfusion and increased cardiac filling pressures [3]. Managing such conditions may sometimes require Mechanical circulatory support (MCS) such as ECMO (extra-corporeal membrane oxygenation), IABP (intra-aortic balloon pump), and Impella (an axial flow pump), to ensure hemodynamic support and boost myocardial function as a temporary bridging option [4]. Nevertheless, consensus is lacking regarding the beneficial effects of ECMO on mortality following cardiogenic shock with inconclusive data available.
Currently, trends in the use of MCDs in the last ten years in the USA show an upward trend in the use of Impella and ECMO [5]. The first trial comparing the efficacy of IABP with standard treatment (IABP-SHOCK II trial) demonstrated no significant difference in the rate of 30-day mortality post-MI complicated by cardiogenic shock [6]. Furthermore, in a recent 6-year follow-up study conducted on this trial, there were no statistically significant differences observed in terms of mortality, recurrent myocardial infarction, stroke, repeat revascularization, or rehospitalization for cardiac reasons between the groups [7]. Interestingly, as recent data has shown the efficacy of IABP in 30-day and 1-year mortality reduction following cardiogenic shock, given the incongruity within the data and the importance of the subsequent analysis in IABP Shock II follow-up, several guidelines have adjusted the recommended class for the use of IABP in cardiogenic shock in ACS patients to a lower category. The European Society of Cardiology (ESC) and European Association for Cardio-Thoracic Surgery (EACTS) guidelines have revised the recommended classification moving from a Class I to a Class III B recommendation (indicating not recommended for routine use in cardiogenic shock due to ACS). Similarly, the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) guidelines have downgraded it to a Class IIb B recommendation. (Weak/Usefulness or unknown/unclear/uncertain) [8,9,10,11]. While a recent meta-analysis, consisting of data from more than 10 thousand patients, has shown improved mortality reduction outcomes with IABP over ECMO and Impella, no reasonable grounds seem to exist for explaining this reclassification by guidelines [12]. We recently presented our data comparing Impella and intra-aortic balloon pumps (IABP) in patients with cardiogenic shock revealing highest mortality with the use of Impella and lowest mortality with IABP [13].
VA. ECMO (veno-arterial ECMO), is another option for treating cardiogenic shock in patients following AMI. VA-ECMO employs a centrifugal flow pump, membrane oxygenator, and cannulas for venous inflow and arterial outflow [4,13]. Additional ports may be utilized for ultrafiltration and hemodialysis. Deoxygenated blood from a central vein passes through the membrane oxygenator, adjusting pCO2, pO2, and pH, before being reintroduced into systemic circulation via the pump. Cardiac support can reach up to 6–7 L/min [14,15]. Cannulation options include central placement in the right atrium and ascending aorta for physiological circulation, primarily for post-cardiotomy patients, and peripheral approaches such as femoral-femoral or upper extremity arteries, allowing for retrograde or anterograde perfusion [16,17]. Continuous monitoring of hemodynamics and blood gases is crucial post-ECMO initiation, with targets for flow, mean arterial pressure, and oxygen saturation aimed to promote myocardial recovery and organ function [18,19].
In a recent meta-analysis, VA-ECMO demonstrated no decrease in the 30-day mortality rate when compared to medical therapy in individuals experiencing infarct-related cardiogenic shock. Moreover, there was an observed rise in instances of major bleeding and vascular complications [20]. This meta-analysis only included 567 patients which does not seem to add ample evidence to the literature. While data from NIS revealed an uptrend in the use of ECMO and a downtrend in the use of IABP in patients with cardiogenic shock and ACS, there remains uncertainty regarding the efficacy of ECMO and its comparison to IABP in mortality reduction [21].
A thorough examination of a large cohort is imperative to establish more conclusive evidence regarding the comparative mortality outcomes associated with the use of ECMO. Utilizing a retrospective analysis of data from the Nationwide Inpatient Sample (NIS) database among adult patients, we sought to achieve the largest possible sample size for a study of this nature.
Methods
Data Source
The dataset employed in this research, known as the Nationwide Inpatient Sample (NIS), was formulated by the Agency for Healthcare Research and Quality (AHRQ) as a component of the Healthcare Cost and Utilization Project (HCUP). This database is de-identified, falls under the exemption from Institutional Review Board (IRB) approval, and is accessible to researchers and policymakers for the examination of nationwide patterns in healthcare utilization and results. The NIS encompasses details on both primary and secondary diagnoses and procedures, discharge vital status, and demographic information from almost one-fifth of all community hospitals in the United States.
Sample Selection
This retrospective analysis included individuals aged 18 and above who were discharged from a Nationwide Inpatient Sample (NIS) hospital between 2016 and 2020. Inclusion criteria involved specific International Classification of Diseases, Tenth Revision, and Clinical Modification (ICD-10-CM) codes: Cardiogenic Shock (R57.0), To mitigate the impact of confounding variables, a multivariate analysis was conducted, adjusting for 47 factors, including age, gender, race, and various comorbidities. The considered comorbidities encompassed conditions such as smoking, diabetes mellitus (250), chronic kidney disease, Peripheral Vascular Diseases, Cardiomyopathy, Systolic Heart Failure, PCI Three Vessel, Left main STEMI, STEMI, Anterior Wall STEMI, Cachexia, Morbid Obesity, Obesity, Chronic Liver Disease, Atrial Fibrillation/Flutter, COPD, ALL Valvular Heart Disease, History of Stroke, Acute Lactic Acidosis, Cardiac Arrest, Mechanical Ventilation, Renal Replacement Therapy, Heart Failure, Presence of Aortocoronary Bypass Graft, Right Ventricular Infarction, and Rotational Atherectomy (see Table 1). Comorbidities exhibiting significant p values were included in the multivariate analysis for further adjustment. Additionally, we scrutinized outcome data, making comparisons between teaching hospitals and rural facilities.
Statistical Analysis
Patient demographic, clinical, and hospital characteristics are presented as percentages in the tables. Odds ratios and corresponding 95% confidence intervals are computed for continuous variables and proportions, while categorical variables have associated 95% confidence intervals. Temporal trends were evaluated using Chi-squared analysis for categorical outcomes and univariate linear regression for continuous variables. Multivariable logistic regression was employed to determine the odds of binary clinical outcomes concerning patient and hospital characteristics, as well as the odds of clinical outcomes over time. All analyses incorporated population discharge weights. All p-values are two-sided, and a significance level of p<0.05 was adopted. The analysis was conducted using STATA 17 (Stata Corporation, College Station, TX). Cardiogenic shock occurrence and in-hospital mortality rates were computed annually to examine trends (2016-2020) and collectively for the final analysis.
Results
Mortality
In this retrospective analysis conducted from 2016-2020 using ICD-10 codes for ECMO, IABP, and cardiogenic shock, a comprehensive examination of 796,585 patients (mean age 66.5±14.4) with a diagnosis of cardiogenic shock, excluding Impella use, was conducted. Among this cohort, 13,160 patients (mean age 53.7±15.4) were treated with ECMO alone. The complete demographics of the patients are available in Table 1. The overall inpatient mortality rate for patients without mechanical circulatory support devices was 32.7%. Notably, mortality rate varied among the different treatment groups with a high mortality rate of 47.9% for those treated with ECMO (Figure 1).
Multivariate and Subgroup Analysis
A multivariate analysis was done, adjusting for a robust set of 47 variables, including age, gender, race, lactic acidosis, three-vessel intervention, left main myocardial infarction, cardiomyopathy, systolic heart failure, acute ST-elevation myocardial infarction, peripheral vascular disease, chronic renal disease, among others. Upon adjustment, ECMO utilization remained significantly associated with the highest mortality (OR: 1.78, CI: 1.6-1.9, p<0.001), underscoring the considerable impact of ECMO on patient outcomes. (Table 2).
Complications
Beyond mortality outcomes, an analysis of major complications revealed a higher incidence in the ECMO cohort (Table 3) including increased pericardial effusion (OR=2.19(1.84-2.60), p<0.001), cardiac tamponade (OR=3.40(2.80-4.13), p<0.001), acute posthemorrhagic anemia (OR=2.93(2.65-3.23), p<0.001), hemolytic anemia (OR=6.92(3.08-15.56), p<0.001), disseminated intravascular coagulation (OR=6.07(5.13-7.19), p<0.001), cardiac perforation (OR=2.58(1.94-3.44), p<0.001), procedural bleeding (OR=11.63(6.60-20.49), p<0.001), intraoperative cardiac functional disturbances (OR=4.04(2.66-6.14), p<0.001) and acute postprocedural respiratory failure (OR=1.23(1.03-1.48), p=0.02).
Discussion
Our retrospective study found that ECMO was associated with the highest inpatient all-cause mortality in patients with cardiogenic shock (47.9%). Additionally, a mortality rate of 32.7% was observed when no device was used.
Various studies have reported different mortality rates of ECMO in patients with cardiogenic shock. Overall the results have been virtually heterogenous and the in-hospital mortality rate ranged from 40% to 60 % [22,23,24,25,26,27]. Recent clinical trials comparing the efficacy of VA-ECMO and optimal medical treatment demonstrated that using ECMO in patients with cardiogenic shock did not improve early and long-term mortality [28,29]. Additionally, a recent meta-analysis comparing the efficacy of ECMO compared to medical treatment revealed no mortality benefit from ECMO use in 30 days, however, long-term results looked in favor of ECMO use [30]. Similarly, our study showed ECMO is associated with the highest mortality. ECMO patients likely had much worse underlying conditions that we could not capture in our database and adjust for it. For example, patients requiring ECMO usually are very hypoxic and not only require mechanical support but also external oxygenation making them much sicker than common patients with cardiogenic shock. Higher complications associated with the use of ECMO including bleeding, thromboembolic events, infections, and neurologic and vascular complications could also contribute to higher mortality found in our study [31,32,33]. These complications emphasize the importance of considering both efficacy and safety profiles when evaluating mechanical circulatory support devices in the context of cardiogenic shock.
In our multivariate analysis adjusting for 47 variables, including age, gender, race, lactic acidosis, three-vessel intervention, left main myocardial infarction, cardiomyopathy, systolic heart failure, acute ST-elevation myocardial infarction, peripheral vascular disease, chronic renal disease, etc., ECMO use remained associated with the highest mortality (OR: 1.78, CI: 1.6-1.9, p<0.001). This aligns with a recent meta-analysis of 10,985 patients concluding that IABP outperforms both Impella and ECMO in improving mortality [12]. The contrast between our results and recent guideline adjustments by the European Society of Cardiology (ESC), European Association for Cardio-Thoracic Surgery (EACTS), American College of Cardiology Foundation (ACCF), and the American Heart Association (AHA) prompts questions about the rationale behind downgrading device use [8,9,34]. Our data underscores the need to reconsider recent guideline changes, given their substantial impact on clinical practice and patient outcomes. The difference between guidelines and our study highlights the need for continuous scrutiny and updates. This ensures that guidelines accurately reflect the latest evidence.
Other MCDs could also be used in the setting of cardiogenic shock. Previous data showed that in a cohort of patients with cardiogenic shock, the highest mortality was with the use of impella(40.7%) while the lowest was with the use of IABP (25.1%) compared to no device use(34.2%). However, a recent clinical trial comparing a microaxial flow pump (Impella CP) plus medical therapy to medical therapy alone, showed that microaxial flow pump reduced the risk of mortality in 180 days (HR=0.74; 95% [CI], 0.55 to 0.99) but was associated with a higher risk of complications [35].
With recent advances in the use of MCDs especially ECMO, the high mortality rate with the use of ECMO is still concerning. Although ECMO is a feasible option in patients with cardiogenic shock and rapidly deteriorating conditions, several factors could be considered in its use. First, it is imperative to recognize that ECMO serves solely as a bridging strategy to definitive treatment, and its implementation should not be expedited until thorough consideration of all potential complications. Secondly, recent studies have proposed models for predicting outcomes and selecting patients for ECMO use. Prior to ECMO initiation, factors predictive of adverse outcomes include advanced age, female gender, elevated body mass index, alongside indicators of heightened illness severity such as renal, hepatic, or neurological impairment, prolonged mechanical ventilation, increased lactate levels, and diminished prothrombin activity [36,37]. Notably, the PRECISE score has been able to predict in-hospital mortality with a sensitivity of 89% in patients with cardiogenic shock requiring VA-ECMO [38]. Ultimately, the consideration of these factors becomes paramount in the clinical decision-making process regarding the initiation of ECMO support. This offers a chance to identify patients who are most likely to derive significant advantages from such intervention.
Conclusion
Our study showed ECMO is associated with very high mortality despite adjustment for 47 variables in patients with cardiogenic shock. It is very likely that ECMO patients had much worse underlying condition that we could not capture in our database and adjust for it. For example, patients requiring ECMO usually are very hypoxic that requires not only mechanical support but also external oxygenation making them being much sicker than common patients with cardiogenic shock. Higher complications associated with the use of ECMO including bleeding, thromboembolic events, infections, and neurologic and vascular complications could also contributed to higher mortality found in our study. These findings underscore the critical importance of the making correct selection between different cardiac support devices in managing cardiogenic shock patients.
Limitations
First of all, the retrospective and non-randomized nature of our study might undermine the generalizability of our results. Although a multivariable adjustment was utilized for our analysis, there might have been unmeasured variables that were not taken into account. We employed ICD-10 coding, acknowledging its inherent limitations in providing precise diagnosis. Moreover, it is challenging to evaluate the rationale behind clinicians' decision-making processes regarding the selection of ECMO or no device in each patient. In fact, it could not be ruled out that the patients receiving ECMO were sicker in nature. The complexities involved in understanding the factors influencing such choices, including patient-specific considerations and clinical judgment, remain beyond the scope of our current analysis.
Conflict of Interest:
Authors report no financial relationships or conflicts of interest regarding the content herein.
Funding
None.
References
- Goldberg RJ, Samad NA, Yarzebski J, Gurwitz J, Bigelow C, Gore JM. Temporal trends in cardiogenic shock complicating acute myocardial infarction. N Engl J Med. 1999;340(15):1162-8.
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation. 2009;119(9):1211-9.
- Vahdatpour C, Collins D, Goldberg S. Cardiogenic Shock. J Am Heart Assoc. 2019;8(8):e011991.
- Telukuntla KS, Estep JD. Acute Mechanical Circulatory Support for Cardiogenic Shock. Methodist Debakey Cardiovasc J. 2020;16(1):27-35.
- Malik A, Basu T, VanAken G, Aggarwal V, Lee R, Abdul-Aziz A, et al. National Trends for Temporary Mechanical Circulatory Support Utilization in Patients With Cardiogenic Shock From Decompensated Chronic Heart Failure: Incidence, Predictors, Outcomes, and Cost. Journal of the Society for Cardiovascular Angiography & Interventions. 2023;2(6, Part B):101177.
- Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med. 2012;367(14):1287-96.
- Thiele H, Zeymer U, Thelemann N, Neumann FJ, Hausleiter J, Abdel-Wahab M, et al. Intraaortic Balloon Pump in Cardiogenic Shock Complicating Acute Myocardial Infarction: Long-Term 6-Year Outcome of the Randomized IABP-SHOCK II Trial. Circulation. 2019;139(3):395-403. [CrossRef]
- Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165.
- Tehrani BN, Truesdell AG, Psotka MA, Rosner C, Singh R, Sinha SS, et al. A Standardized and Comprehensive Approach to the Management of Cardiogenic Shock. JACC Heart Fail. 2020;8(11):879-91.
- Yuan S, He J, Cai Z, Zhang R, Song C, Qiao Z, et al. Intra-aortic balloon pump in cardiogenic shock: A propensity score matching analysis. Catheter Cardiovasc Interv. 2022;99 Suppl 1:1456-64. [CrossRef]
- Zein R, Patel C, Mercado-Alamo A, Schreiber T, Kaki A. A Review of the Impella Devices. Interv Cardiol. 2022;17:e05.
- Zhang Q, Han Y, Sun S, Zhang C, Liu H, Wang B, et al. Mortality in cardiogenic shock patients receiving mechanical circulatory support: a network meta-analysis. BMC Cardiovasc Disord. 2022;22(1):48.
- Rao P, Khalpey Z, Smith R, Burkhoff D, Kociol RD. Venoarterial Extracorporeal Membrane Oxygenation for Cardiogenic Shock and Cardiac Arrest. Circ Heart Fail. 2018;11(9):e004905.
- Burkhoff D, Sayer G, Doshi D, Uriel N. Hemodynamics of Mechanical Circulatory Support. Journal of the American College of Cardiology. 2015;66(23):2663-74. [CrossRef]
- Tsangaris A, Alexy T, Kalra R, Kosmopoulos M, Elliott A, Bartos JA, et al. Overview of Veno-Arterial Extracorporeal Membrane Oxygenation (VA-ECMO) Support for the Management of Cardiogenic Shock. Front Cardiovasc Med. 2021;8:686558.
- Piechura LM, Coppolino A, Mody GN, Rinewalt DE, Keshk M, Ogawa M, et al. Left ventricle unloading strategies in ECMO: A single-center experience. J Card Surg. 2020;35(7):1514-24.
- Shen J, Tse JR, Chan F, Fleischmann D. CT Angiography of Venoarterial Extracorporeal Membrane Oxygenation. Radiographics. 2022;42(1):23-37.
- Keebler ME, Haddad EV, Choi CW, McGrane S, Zalawadiya S, Schlendorf KH, et al. Venoarterial Extracorporeal Membrane Oxygenation in Cardiogenic Shock. JACC: Heart Failure. 2018;6(6):503-16.
- Richardson AC, Tonna JE, Nanjayya V, Nixon P, Abrams DC, Raman L, et al. Extracorporeal Cardiopulmonary Resuscitation in Adults. Interim Guideline Consensus Statement From the Extracorporeal Life Support Organization. ASAIO Journal. 2021;67(3):221-8.
- Zeymer U, Freund A, Hochadel M, Ostadal P, Belohlavek J, Rokyta R, et al. Venoarterial extracorporeal membrane oxygenation in patients with infarct-related cardiogenic shock: an individual patient data meta-analysis of randomised trials. Lancet. 2023;402(10410):1338-46. [CrossRef]
- Shah M, Patnaik S, Patel B, Ram P, Garg L, Agarwal M, et al. Trends in mechanical circulatory support use and hospital mortality among patients with acute myocardial infarction and non-infarction related cardiogenic shock in the United States. Clin Res Cardiol. 2018;107(4):287-303.
- El Sibai R, Bachir R, El Sayed M. Outcomes in Cardiogenic Shock Patients with Extracorporeal Membrane Oxygenation Use: A Matched Cohort Study in Hospitals across the United States. BioMed Research International. 2018;2018:2428648.
- García-Gigorro R, Renes-Carreño E, Pérez-Vela JL, Marín-Mateos H, Gutiérrez J, Corrés-Peiretti MA, et al. Mechanical support with venoarterial extracorporeal membrane oxygenation (ECMO-VA): Short-term and long-term prognosis after a successful weaning. Med Intensiva. 2017;41(9):513-22.
- Koerner MM, Harper MD, Gordon CK, Horstmanshof D, Long JW, Sasevich MJ, et al. Adult cardiac veno-arterial extracorporeal life support (VA-ECMO): prevention and management of acute complications. Ann Cardiothorac Surg. 2019;8(1):66-75.
- Krasivskyi I, Ivanov B, Vehrenberg J, Eghbalzadeh K, Gerfer S, Gaisendrees C, et al. Sex-Related Differences in Short-Term Outcomes after Mobile VA-ECMO Implantation: Five-Year Experience of an ECMO Retrieval Program. Life (Basel). 2022;12(11).
- Pang S, Miao G, Zhao X. Effects and safety of extracorporeal membrane oxygenation in the treatment of patients with ST-segment elevation myocardial infarction and cardiogenic shock: A systematic review and meta-analysis. Front Cardiovasc Med. 2022;9:963002.
- Senoner T, Treml B, Breitkopf R, Oezpeker UC, Innerhofer N, Eckhardt C, et al. ECMO in Myocardial Infarction-Associated Cardiogenic Shock: Blood Biomarkers as Predictors of Mortality. Diagnostics. 2023;13(24):3683.
- Ostadal P, Rokyta R, Karasek J, Kruger A, Vondrakova D, Janotka M, et al. Extracorporeal Membrane Oxygenation in the Therapy of Cardiogenic Shock: Results of the ECMO-CS Randomized Clinical Trial. Circulation. 2023;147(6):454-64.
- Thiele H, Zeymer U, Akin I, Behnes M, Rassaf T, Mahabadi AA, et al. Extracorporeal Life Support in Infarct-Related Cardiogenic Shock. N Engl J Med. 2023;389(14):1286-97.
- Paddock S, Meng J, Johnson N, Chattopadhyay R, Tsampasian V, Vassiliou V. The impact of extracorporeal membrane oxygenation on mortality in patients with cardiogenic shock post-acute myocardial infarction: a systematic review and meta-analysis. Eur Heart J Open. 2024;4(1):oeae003.
- Burgos LM, Seoane L, Diez M, Baro Vila RC, Furmento JF, Vrancic M, et al. Multiparameters associated to successful weaning from VA ECMO in adult patients with cardiogenic shock or cardiac arrest: Systematic review and meta-analysis. Ann Card Anaesth. 2023;26(1):4-11.
- Henry TD, Yannopoulos D, van Diepen S. Extracorporeal Membrane Oxygenation for Cardiogenic Shock: When to Open the Parachute? Circulation. 2023;147(6):465-8.
- Lo Coco V, Lorusso R, Raffa GM, Malvindi PG, Pilato M, Martucci G, et al. Clinical complications during veno-arterial extracorporeal membrane oxigenation in post-cardiotomy and non post-cardiotomy shock: still the achille's heel. J Thorac Dis. 2018;10(12):6993-7004.
- Geller BJ, Sinha SS, Kapur NK, Bakitas M, Balsam LB, Chikwe J, et al. Escalating and De-escalating Temporary Mechanical Circulatory Support in Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2022;146(6):e50-e68.
- Møller JE, Engstrøm T, Jensen LO, Eiskjær H, Mangner N, Polzin A, et al. Microaxial Flow Pump or Standard Care in Infarct-Related Cardiogenic Shock. New England Journal of Medicine. 2024;390(15):1382-93.
- Hajjar LA, Teboul JL. Mechanical Circulatory Support Devices for Cardiogenic Shock: State of the Art. Crit Care. 2019;23(1):76.
- Ouweneel DM, Schotborgh JV, Limpens J, Sjauw KD, Engström AE, Lagrand WK, et al. Extracorporeal life support during cardiac arrest and cardiogenic shock: a systematic review and meta-analysis. Intensive Care Med. 2016;42(12):1922-34.
- Jeong JH, Kook H, Lee SH, Joo HJ, Park JH, Hong SJ, et al. Prediction of In-Hospital Mortality for Ischemic Cardiogenic Shock Requiring Venoarterial Extracorporeal Membrane Oxygenation. J Am Heart Assoc. 2024;13(4):e032701.
Figure 1.
Mortality trends over years with ECMO.
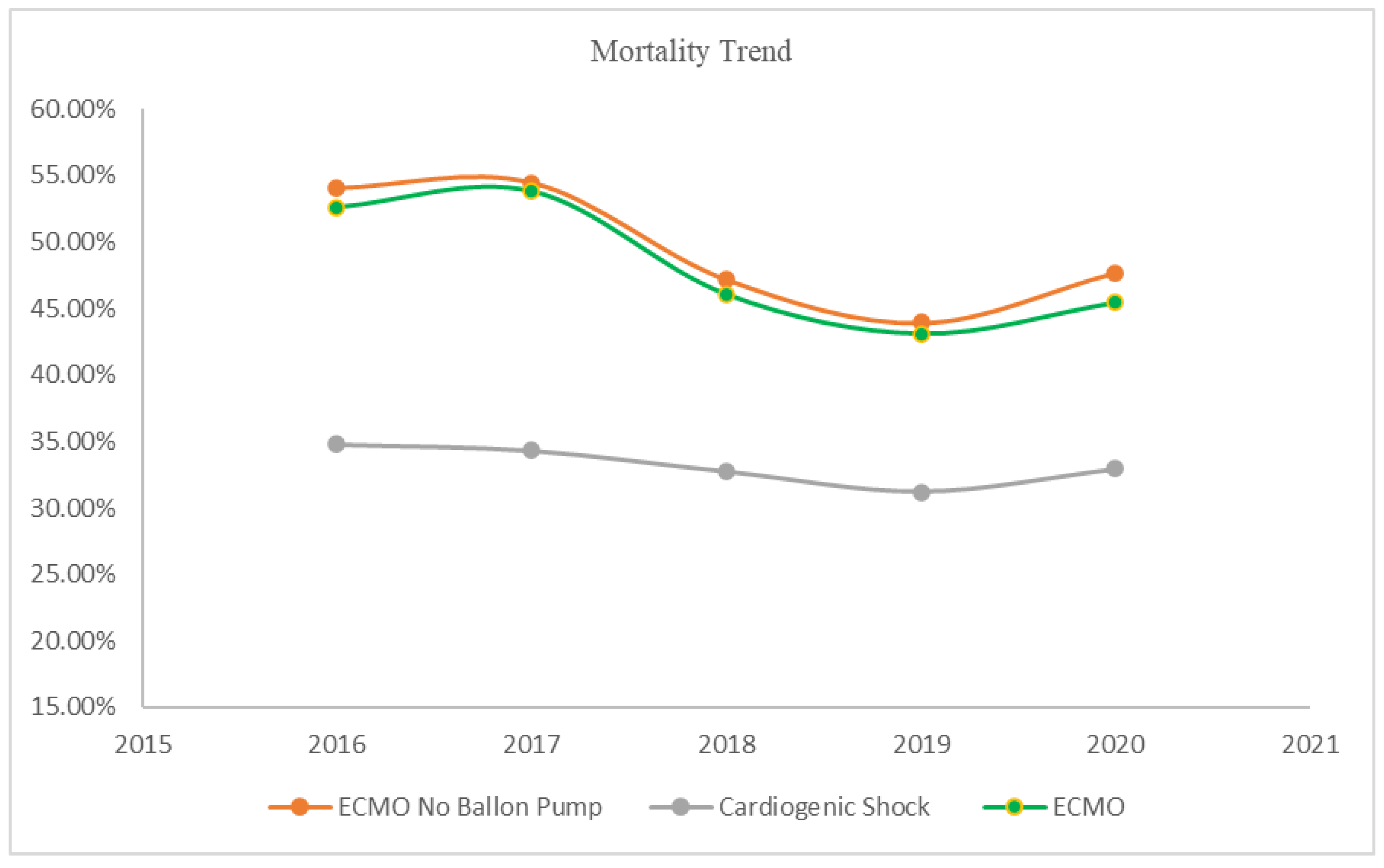

Table 1.
Baseline characteristics of patients with cardiogenic shock.
| Cardiogenic Shock | No ECMO | ECMO | ECMO No Balloon Pump | p-value | |
|---|---|---|---|---|---|
| Age N(Mean±SD) | 796,585(66.57±14.40) | 779,225(66.83±14.28) | 17,360(54.87±15.40) | 13,160(53.72±15.43) | <0.001 |
| Mortality | 33.07% | 32.74% | 47.91% | 49.05% | <0.001 |
| Gender % | <0.001 | ||||
| Male | 62.00% | 61.91% | 66.16% | 64.29% | |
| Female | 38.00% | 38.09% | 33.84% | 35.71% | |
| Race % | <0.001 | ||||
| White | 67.40% | 67.46% | 64.27% | 63.34% | |
| Black | 16.40% | 16.39% | 17.01% | 17.80% | |
| Hipanic | 8.99% | 9.00% | 8.74% | 8.80% | |
| Asian/Pac Isl | 3.32% | 3.31% | 3.70% | 3.58% | |
| Native-American | 0.67% | 0.67% | 0.91% | 1.07% | |
| Others | 3.22% | 3.17% | 5.37% | 5.41% | |
| Smoking | 23.11% | 23.30% | 14.92% | 15.05% | <0.001 |
| Peripheral Vascular Diseases | 5.27% | 5.31% | 3.08% | 2.96% | <0.001 |
| Cardiomyopathy | 41.98% | 42.17% | 33.41% | 29.86% | <0.001 |
| Diabetes | 39.48% | 39.77% | 26.56% | 25.87% | <0.001 |
| CKD | 39.78% | 40.15% | 22.96% | 21.39% | <0.001 |
| Systolic Heart Failure | 52.81% | 52.93% | 47.35% | 43.84% | <0.001 |
| PCI Three Vessel | 0.56% | 0.55% | 1.18% | 0.80% | <0.001 |
| Left main STEMI | 0.12% | 0.11% | 0.52% | 0.46% | 0.56 |
| STEMI | 20.46% | 20.42% | 22.09% | 18.73% | <0.001 |
| Non-STEMI | 18.35% | 18.52% | 10.92% | 9.19% | <0.001 |
| Anterior Wall STEMI | 5.89% | 5.82% | 9.27% | 7.56% | <0.001 |
| History of MI | 12.03% | 12.17% | 5.88% | 5.32% | <0.001 |
| Cachexia | 2.62% | 2.64% | 1.84% | 1.98% | 0.005 |
| Morbid Obesity | 8.29% | 8.27% | 8.99% | 9.80% | <0.001 |
| Obesity | 8.42% | 8.42% | 8.24% | 8.13% | <0.001 |
| Chronic Liver Disease | 19.18% | 18.74% | 38.88% | 39.06% | <0.001 |
| Atrial Fibrillation/Flutter | 43.54% | 43.76% | 33.87% | 32.60% | <0.001 |
| COPD | 23.46% | 23.73% | 11.18% | 11.06% | <0.001 |
| ALL Valvular Heart Disease | 22.73% | 22.88% | 20.54% | 18.35% | <0.001 |
| History of Stroke | 2.02% | 2.05% | 0.86% | 0.80% | 0.006 |
| Acute Lactic Acidosis | 36.93% | 36.68% | 48.30% | 48.44% | <0.001 |
| Cardiac Arrest | 9.57% | 9.49% | 13.10% | 13.34% | <0.001 |
| Mechanical Ventilation | 45.96% | 45.47% | 68.23% | 69.83% | <0.001 |
| Renal Replacement Therapy | 12.41% | 12.11% | 26.04% | 26.75% | <0.001 |
| Heart Failure | 70.37% | 70.44% | 67.25% | 64.67% | <0.001 |
| Presence of Coronary Angioplasty & Graft | 9.17% | 9.22% | 6.94% | 6.00% | <0.001 |
| Presence of Aortocoronary Bypass Graft | 7.83% | 7.91% | 4.35% | 4.48% | 0.1 |
| Presence of Cardiac Pacemaker | 3.14% | 3.18% | 1.24% | 1.03% | 0.04 |
| Prosthetic Heart Valve | 2.72% | 2.73% | 2.42% | 2.51% | <0.001 |
| Presence of Automatic (implantable) Cardiac Defibrillator | 8.27% | 8.37% | 4.03% | 3.76% | 0.002 |
| Coronary Angioplasty Status | 1.04% | 1.04% | 0.86% | 0.80% | 0.24 |
| Right Ventricular Infarction | 1.35% | 1.34% | 1.73% | 1.14% | <0.001 |
| Rotational Atherectomy | 0.10% | 0.10% | 0.14% | 0.11% | 0.09 |
Table 2.
Mortality is very high with the use of ECMO regardless of any subgroup.
| Mortality | ECMO No Balloon Pump | Risk ratio (CI) | p-value |
|---|---|---|---|
| Age<50 | 41.24% | 2.73 (2.40-3.11) | <0.001 |
| Age>=50 | 53.48% | 2.11 (2.00-2.22) | |
| Male | 48.23% | 2.12 (2.00-2.25) | <0.001 |
| Female | 50.53% | 1.81 (1.68-1.95) | |
| Diabetes | 52.72% | 2.07 (1.91-2.24) | 0.73 |
| No Diabetes | 47.77% | 2.03 (1.92-2.15) | |
| STEMI | 54.56% | 1.95 (1.79-2.12) | 0.009 |
| No STEMI | 47.78% | 2.24 (2.11-2.37) | |
| Non-STEMI | 50.83% | 2.20 (1.92-2.51) | 0.13 |
| No Non-STEMI | 48.87% | 1.97 (1.87-2.07) | |
| Left main STEMI | 66.67% | 2.94 (1.73-5.02) | 0.16 |
| No Left main STEMI | 48.97% | 2.01 (1.92-2.10) | |
| Anterior Wall STEMI | 51.76% | 2.04 (1.76-2.35) | 0.95 |
| No Anterior Wall STEMI | 48.83% | 2.03 (1.93-2.13) | |
| PCI Three Vessel | 47.62% | 1.92 (1.19-3.10) | 0.84 |
| No PCI Three Vessel | 49.06% | 2.01 (1.92-2.11) | |
| Cardiac Arrest | 56.13% | 1.15 (1.04-1.28) | <0.001 |
| No Cardiac Arrest | 47.96% | 2.17 (2.07-2.29) | |
| Acute Lactic Acidosis | 56.47% | 1.44 (1.36-1.53) | <0.001 |
| No Acute Lactic Acidosis | 42.08% | 2.37 (2.21-2.55) | |
| Peripheral Vascular Diseases | 57.69% | 1.95 (1.58-2.41) | 0.74 |
| No Peripheral Vascular Diseases | 48.79% | 2.03 (1.93-2.12) | |
| Obesity | 52.34% | 2.59 (2.22-3.01) | <0.001 |
| No Obesity | 48.76% | 1.96 (1.87-2.06) | |
| Smoking | 50.76% | 2.13 (1.91-2.38) | 0.24 |
| No Smoking | 48.75% | 1.99 (1.89-2.09) | |
| Hypertension | 50.51% | 2.12 (2.00-2.25) | <0.001 |
| No Hypertension | 47.22% | 1.80 (1.66-1.94) |
Table 3.
Complications in patients with ECMO vs IABP.
| Complications | Balloon Pump No ECMO | ECMO No Balloon Pump | p-value | Odds Ratio (C.I) |
|---|---|---|---|---|
| Pericardial Effusion | 3.72% | 7.79% | <0.001 | 2.19(1.84-2.60) |
| Cardiac Tamponade | 1.90% | 6.19% | <0.001 | 3.40(2.80-4.13) |
| Postprocedural Acute Kidney Failure | 0.42% | 0.34% | 0.59 | 0.81(0.39-1.71) |
| Acute Posthemorrhagic Anemia | 28.90% | 54.33% | <0.001 | 2.93(2.65-3.23) |
| Acquired Hemolytic Anemia | 0.07% | 0.49% | <0.001 | 6.92(3.08-15.56) |
| Postprocedural Hemorrhage | 0.96% | 5.09% | <0.001 | 5.55(4.42-6.97) |
| Acute Postprocedural Respiratory Failure | 4.49% | 5.47% | 0.02 | 1.23(1.03-1.48) |
| Disseminated Intravascular Coagulation | 1.58% | 8.89% | <0.001 | 6.07(5.13-7.19) |
| Cardiac Perforation (Accidental puncture and laceration of a circulatory system organ) | 0.87% | 2.20% | <0.001 | 2.58(1.94-3.44) |
| Procedural Bleeding | 0.10% | 1.18% | <0.001 | 11.63(6.60-20.49) |
| Intraoperative Cardiac Functional Disturbances | 0.33% | 1.33% | <0.001 | 4.04(2.66-6.14) |
| Postprocedural Cerebrovascular Infarction | 0.07% | 0.15% | 0.18 | 2.12(0.70-6.45) |
| Amputation of limb | 0.06% | 0.15% | 0.09 | 2.70(0.86-8.49) |
| Hemopericardium as current complication following acute myocardial infarction | 0.11% | 0.04% | 0.29 | 0.34(0.05-2.49) |
| Ventricular septal defect as current complication following acute myocardial infarction | 0.65% | 0.61% | 0.82 | 0.94(0.56-1.59) |
| Rupture of cardiac wall without hemopericardium as current complication following acute myocardial infarction | 0.15% | 0.11% | 0.66 | 0.77(0.23-2.52) |
| Rupture of chordae tendineae as current complication following acute myocardial infarction | 0.32% | 0.46% | 0.27 | 1.42(0.76-2.63) |
| Other current complications following acute myocardial infarction | 0.09% | 0.08% | 0.8 | 0.82(0.19-3.56) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



