
Submitted:
31 May 2024
Posted:
04 June 2024
You are already at the latest version
Abstract
(1) Background : When placing implants in the maxillary posterior region with insufficient alveolar bone, a maxillary sinus elevation is necessary. Autogenous bone, though biologically ideal, poses risks and discomfort due to donor site harvesting. Block-type autogenous tooth bone graft material, made from the patient’s own extracted tooth, offers similar biological stability without these drawbacks; (2) Methods : This study observed the progress of 19 implant patients who were treated with maxillary sinus elevation procedures using block-type autogenous tooth bone graft material at the Daegu Catholic University Medical Center. Extracted teeth were processed into demineralized tooth block bone. After elevating the sinus membrane, implants and the tooth bone graft material were placed in the space, and the bony window was repositioned. Postoperative evaluations through clinical observation and radiographic imaging assessed sinus membrane elevation, alveolar bone height increase, and implant osseointegration; (3) Results : Results showed proportional increases in alveolar bone height to the graft material size, with long-term stability. No postoperative complications occurred, even with sinus membrane perforation, and implants remained stable; (4) Conclusions : The study concludes that maxillary sinus lifts using block-type autogenous tooth bone graft material provide excellent bone induction and biocompatibility, making it a highly beneficial method for both dentists and patients.
Keywords:
sinus augmentation
; tooth bone graft
; dental implant
1. Introduction
The restoration of partially edentulous and edentulous areas using dental implants has been widely applied since Branemark discovered the phenomenon of osseointegration and is now regarded as the most ideal treatment method for reconstructing lost teeth [1]. Although the success rate of implants has gradually increased with advancing technology, there are still instances of implant failure. Particularly, when placing implants in the posterior maxilla, challenging situations such as thin and low alveolar ridges, poor bone quality, or increased pneumatization of the maxillary sinus exist [2,3,4].
For these reasons, removable dentures have long been used as a traditional and successful treatment option with predictable outcomes for patients who have lost their maxillary molars. In the case of removable dentures, natural teeth or implants in the anterior region are used as surveyed crowns, and the posterior extension area is covered by traditional removable partial dentures. These removable dentures can be provided at a low cost, do not require additional surgical procedures, and are reversible, making them a less burdensome option. However, they do have disadvantages in terms of patient satisfaction, such as lower masticatory efficiency and psychological comfort compared to fixed prostheses [5].
Thanks to recent advancements in implant technology, placing implants in the maxillary molar area has also become easier. Unsuccessful implant surgery in the molar part of maxilla has been related to unsatisfactory residual bone height, ridge width, and disadvantageous bone quality [6,7,8]. Such problems have been overcome by augmenting the bone height through maxillary sinus augmentation [9,10,11]. Variety of maxillary sinus augmentation surgeries have been operated for restoration of the posterior maxilla with simultaneous or delayed placement of dental implants.
The lateral approach is a routinely used procedure in maxillary sinus augmentation, particularly when the initial alveolar ridge highness is not high enough to get initial stability of simultaneously placed implant [9,10,11]. In the case of lateral approach technique, sinus membrane (Schneiderian membrane) was elevated, and powdered bone graft materials were conventionally used to fill the new space under the elevated sinus membrane [8]. Various bone graft materials have been utilized to pack the space of the maxillary sinus. For example, autogenous bone, allogenous bone, xenogenous bone, synthetic bone, demineralized autogenous teeth and a combination of various materials [12,13,14].
However, sticking points which are related to graft materials are still exist. For example, unexpected resorption, limited amounts and required donor sites of autogenous bone, nonability of alloplastic materials to bone development, and slow resorption speed of xenograft materials [15,16,17].
In addition, a large amount of bone is needed to fill maxillary sinus. An average of 5–6 cc of autograft bone is needed for one sinus cavity and an average of 2–3 cc of combination graft bone material is needed. As a solution of these problems, some studies have verified bone formation using the patient’s own blood or platelet-rich plasma (PRP) to fill the space without graft materials [18,19,20]. Therefore, we concentrated on demineralized tooth block bone to solve the problems associated with the other sinus bone grafts.
Recently, the use of tooth graft material has raised in alveolar bone and sinus augmentation. Demineralized autogenous teeth can be a great bone graft material [16,21]. Demineralized autogenous tooth graft materials were made from extracted teeth, such as freshly extracted third molars, and teeth which are extracted because of periodontic or endodontic disease. In previous experimental studies, human teeth have been turned out to be biocompatible materials that exhibited both osteoinductive and osteoconductive characteristics [22]. However, the disadvantage of tooth graft material is the limited amount available for sinus graft. To solve this problem, block type rather than a power type tooth bone can have advantage of space maintenance [23].
This retrospective study evaluated the use of autogenous demineralized tooth block bone in sinus augmentation by lateral approach with a residual bone height of less than 6 mm.
2. Materials and Methods
2.1. Patient Selection
This clinical retrospective study population comprised 18 patients from April 2017 to October 2022 and was approved by the local university ethics committee. Data were obtained from the dental-treatment records of the patients of the Department of Dentistry, Daegu Catholic University Hospital, Daegu, Republic of Korea (IRB No. CR-22-174-L). All patients were notified about the process of the treatment and signed the consent form about the surgery.
Before patient selection, each patient’s medical history was carefully screened, and the patient who had disease which affects bone metabolism were ruled out. Smokers were notified that smoking could weaken the quality of sinus augmentation and reduce the success rate of implants. But they were not ruled out from the study. All subjects had no contraindication for surgical procedures. The surgery was done at partial or complete edentulous premolar and molar part in maxilla with same surgical procedure.
Implant mobility was the criterion for removal of implant, and the removal was determined as implant failure. The survival rate of implant was estimated by measuring the time passed from implant placement to the last follow-up visit or implant removal. For the radiographic analysis, preoperative examinations were done.
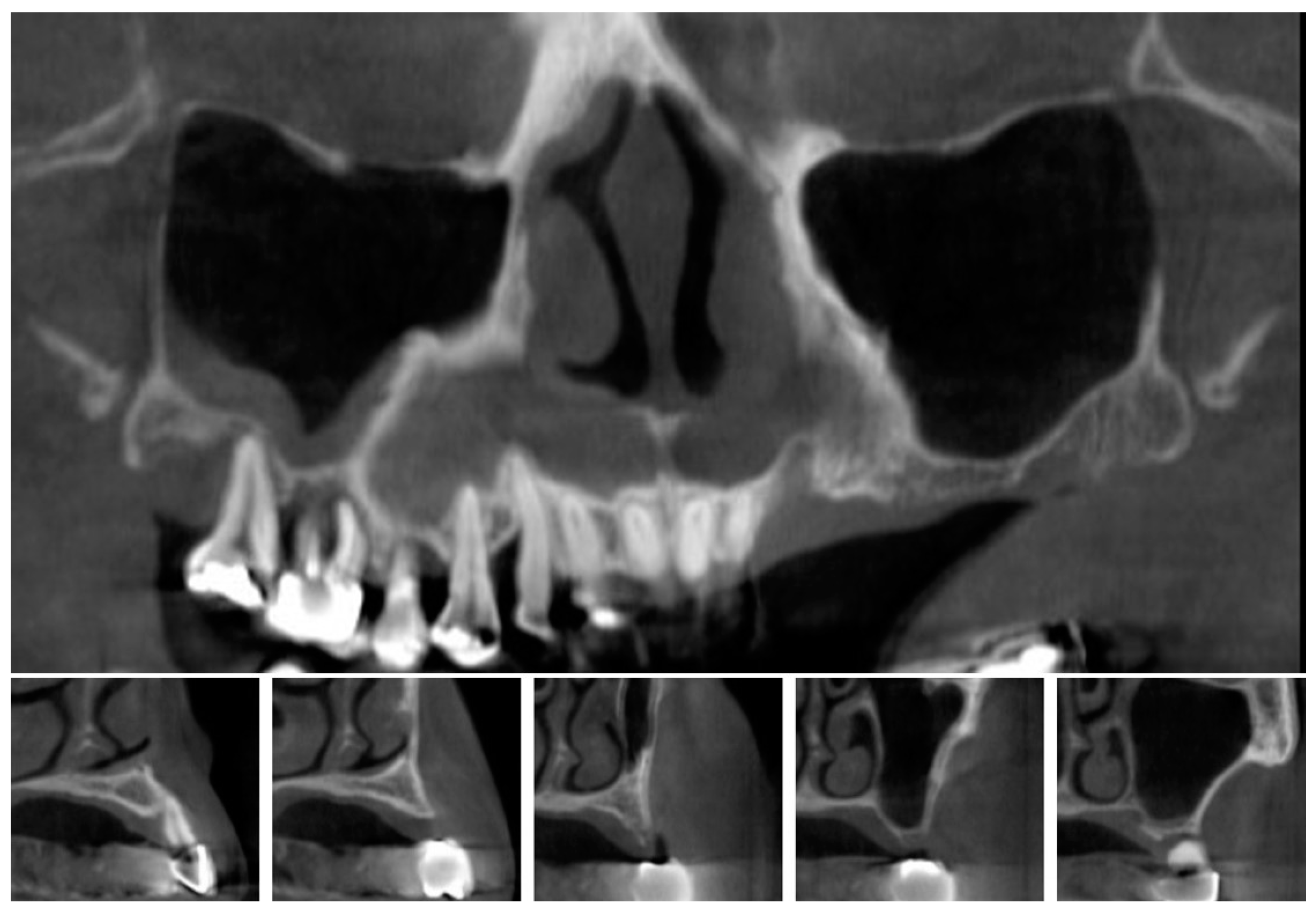
Panoramic radiograph and dental cone beam computed tomographic scans (Combi, Pointnix Co, Seoul, Korea and i-Cat, Imaging Sciences, Hatifield, USA) were taken to estimate preoperative sinus conditions and residual bone heights and later to assess postoperative bone gain (Figure 1).
With these software programs, we could check the residual bone height in millimeters. The width of maxillary sinus was measured at the widest point of the sinus cavity. Because of the reason that elevated sinus membrane goes down when there is no tenting material, amount of membrane elevation was measured from the base of the sinus floor to the top of the grafted tooth block bone.
Figure 1.
Preoperative panoramic CBCT images (subject number 19): (A) Panoramic image of CBCT scan reveals unfavorable bone height on the upper posterior edentulous ridge due to pneumatization of left maxillary sinus; (B) The cross-section images of CBCT show severe bone resorption.
Figure 1.
Preoperative panoramic CBCT images (subject number 19): (A) Panoramic image of CBCT scan reveals unfavorable bone height on the upper posterior edentulous ridge due to pneumatization of left maxillary sinus; (B) The cross-section images of CBCT show severe bone resorption.
2.2. Preparation of Osteoinductive Tooth Block Bone
A hopeless tooth is extracted carefully and processed into demineralized tooth block bone by following technique. Soft tissue attached to tooth, decay, calculus, or composite restorations were removed with a rotary bur. the tooth is divided into halves along its long axis with a disk while irrigating with sufficient coolant. Pulp attached to teeth is removed with a rotary bur. All procedures were done with saline irrigation to prevent denaturalization of the proteins in teeth by heat. 0.5 mm wide micro-holes are created at 5-6 mm intervals in each dentin block using a small round bur, allowing for the infiltration of blood into the tooth block bone (Figure 2).
The perforated dentin blocks were sterilized with sterilization reagent (peracetic acid ethanol solution) in a device to undergo vacuum compression and ultrasonic vibration. (VacuaSonic System, CosmoBioMedicare Co., Seoul, Korea). After sterilization of perforated dentin blocks, they are demineralized for 60 minutes using 0.6N hydrochloride under vacuum compression and ultrasonic vibration in a vacuum-ultrasonic device. The demineralized tooth blocks then are consecutively washed again with phosphate buffered saline (PBS), and distilled water in the same device (Figure 3 and Figure 4).
2.3. Surgical Protocol
All patients received the same pharmacologic protocol of prophylactic oral antibiotics. Prophylactic oral antibiotics, Amoxicillin sodium (Augmentin; Ilsung pharmaceutical, Seoul, Korea) 500mg 3 times a day was prescribed routinely, from 1 day before the procedure to 7 days after the procedure. Prior to sinus grafting, 20-60CC of patient’s venous blood was taken from the patient’s forearm. The blood was collected in two non-coated vacutainers and first centrifuged at 2400-2700 rpm using specific centrifuge (Medifuge, Silfradent srl, Sofia, Italy) for 2 minutes to obtain autologous fibrin glue, which will make sticky bone by Sohn et. al. [6] Upper layer shown on non-coated vacutainer after centrifugation was mixed with biomaterials to make sticky bone grafts. While the non-coated vacutainers were centrifuged, patient’s venous blood was collected in four to six glass coated vacutainers were centrifuged for 12 minutes using the same centrifuge to make concentrated growth factors (CGF) fibrin blocks.
Surgery was performed under local maxillary block anesthesia using 2% lidocaine with 1:100,000 epinephrine. Maxillary sinus floor elevation via the lateral approach was completed on all patients. The full thickness of the mucoperiosteal flap was elevated to expose the lateral wall of the maxillary sinus. The piezoelectric saw, with a thin blade (S-Saw, Bukboo Dental Co., Daegu, Korea), connected to piezoelectric device (Surgybone®, Silfradent srl, Sofia, Italy), was used with copious saline irrigation to create the replaceable osteoinductive bony window (ROBW) at the lateral wall of the maxillary sinus.
The anterior vertical osteotomy was made 2-3 mm distal to the anterior vertical wall of the maxillary sinus and the distal osteotomy was made approximately 20 mm away from the anterior vertical osteotomy. The height of the vertical osteotomy was approximately 8-10 mm. The anterior and inferior osteotomy lines were created perpendicular to the inner surface of the maxillary sinus lateral wall. Subsequently, superior and posterior osteotomies perpendicular to the sinus wall were performed. This osteotomy design enabled the precise replacement of the bony window as a barrier over the inserted fibrin-rich block in the maxillary sinus (Figure 5-A).
The bony window was carefully detached to expose the sinus membrane. Using a flat blunt-edged sinus elevator, the sinus membrane was meticulously dissected from the sinus floor walls. This dissection continued until reaching the anterior and medial walls of the sinus cavity. The height of the exposed medial wall was parallel to the superior osteotomy line of the lateral window.
After elevating the sinus membrane, a one-step, undersized osteotomy was conducted to achieve initial stability of the implants at operation sites with low bone height. Following the placement of implants, one or two tooth blocks were positioned over the implant apex (Figure 5-B). Two to six pieces of fibrin-rich blocks containing concentrated growth factors (CGF) were inserted into the newly formed space beneath the tooth block bone to accelerate bone regeneration (Figure 5-C). The ROBW was repositioned to prevent soft tissue sinus cavity ingrowths and to promote new bone formation from the lateral wall of the maxillary sinus (Figure 5-D).
In cases where the width of the alveolar bone is insufficient, a procedure for alveolar bone augmentation using tooth bone or other bone substitutes was performed (Figure 6-A). After collagen barrier was covered over the bone graft (Figure 6-B), flaps were sutured by Polytetrafluoroethylene sutures (Cytoplast; Osteogenics Biomedical, Lubbock, TX) with continuous locking suture technique and interrupt suture technique to get passive primary closure (Figure 6-C, 6-D).
Patients were instructed not to blow their noses for two weeks after surgery and to cough or sneeze with an open mouth. The sutures were removed 10 days post-operatively. Plain panoramic radiographs and cone-beam computed tomograms were made immediately after surgery (Figure 7). A healing period of 5 to 8 months was allowed for new bone consolidation and the osseointegaration of implants. Plain panoramic radiograms and dental cone-beam computed tomograms were obtained to assess the new bone formation around the implants before the implants were uncovered (Figure 8).
The prosthetic procedure for the implants was conducted. After a provisional loading period of three months, the final full-zirconia restoration was delivered to the patient (Figure 9). A follow-up examination was conducted for an average of 53.2 months for all patients after prosthesis placement, and no complications were observed (Figure 10).
3. Results
3.1. Clinical Results
Clinical results are tabulated in Table 1. A total of 19 patients (11 male and 8 female) with a mean age of 53.9 agreed to be registered in this study, and no one failed to come during the follow up period. Sinus augmentation was done at both maxillary sinus in 1 patient and 1 side in 18 patients. 20 sinus membrane elevation procedures were performed, and 27 implants were placed simultaneously.
Except for temporary swelling on operation site, there was no serious complications in any of the patients during the follow up period. There was no symptoms and signs of infection or maxillary sinus disease neither.
During sinus membrane elevation, Sinus membrane perforation (less than 3mm) was occurred in 3 cases. Absorbable collagen (CollaTape; Zimmer Dental, Carlsbad, CA) was used to manage these perforations. The overall survival rate of the implants was 100%. No implants had mobile state until the end of the study. So, we could see that the sinus membrane perforations were not associated with clinical results. All patients were followed over 2 years after prosthesis placement, and no complications were observed.
3.2. Radiographic Results
Radiographic results are tabulated in Table 2. The width of maxillary sinus was measured at the widest point of the sinus cavity. Because of the reason that elevated sinus membrane goes down when there is no tenting material, amount of membrane elevation was measured from the base of the sinus floor to the top of the grafted tooth block bones.
The preoperative residual bone height varied from 1.0 to 6.0 mm (SD 3.67 ± 1.49). The range of the maxillary sinus width varied from 12 to 25 mm (SD 18.84 ± 4.15). Postoperative cone-beam computed tomographic scans revealed the sinus filled with venous blood and voids under the elevated sinus membrane. Until the end of the study, in all cases, infection signs in the maxillary sinus were not found in the radiographic images. Also, obvious increase in alveolar bone height and new bone formation with good continuity was found in the radiographic images. In all the cases, newly formed maxillary sinus floor was observed around the implants. Marginal bone loss around the implants were not observed in any cases. Correlation between residual bone height and increment of bone height were not found. Also, correlation between maxillary sinus width and increment of bone height were not found. But amount of membrane elevation and new bone formation showed positive correlation.
4. Discussion
When performing implant surgery at thin maxillary alveolar ridge area, it is important to do the sinus augmentation and implantation at the same time. Because, with this way, we can get stable volume of the grafted sinus, minimize operation times, shorten the total healing period, minimize the surgery fee.
A conventional sinus augmentation technique is the lateral approach that use powder type graft materials from various bone. This technique enables the surgeon to get direct approach to the sinus floor. Also, this technique is quite predictable and simple [16]. However, with this technique, large amount of graft material is needed and if graft materials go through the sinus membrane, it may cause a maxillary sinusitis [18,24].
Some studies reported the success of sinus augmentation by using PRP and peripheral blood without any bone graft. Pinchasov et al. reviewed the scientific literature that researched on new bone formation in the sinus augmentation without using any bone graft material from 1993 to 2013 [25]. 19 studies were reviewed in total. This study showed that the preoperative alveolar bone height was more than the average of 5 mm, and the increase of bone height ranged from 4.5 to 8.2 mm. Furthermore, space maintaining devices were used to improve the increase of bone height. For example, hollow hydroxyapatite space maintainer and titanium bone fixation instruments were used.
Xu et al. reported that bulk of the new bone in the augmented sinus disappeared 10 weeks after sinus augmentation by using blood clots, without using any bone graft material [26]. The augmented height remarkably shortened from 2 to 10 weeks. This is because of the increased positive air pressure in sinus cavity which facilitates the pneumatization of the sinus. The authors proposed that the blood clots might not bear the positive air pressure.
To prevent resorption of the grafted material due to the positive air pressure, xenogenous bone graft material has been used in the sinus augmentation. Until a certain period of time after the surgery, the augmented height was actually stable [15,26]. These findings suggested that the xenograft particles endured air pressure which induces osteoclastic bone resorption [26]. However, the xenogenous bone graft material seems to be slow resorbable or even non resorbable up to 6 years, as proved by clinical biopsies [27,28]. Non resorbable graft materials will not change into new bone and functionally adjust to the nearby bone.
This study was conducted to find the alternative of these disadvantageous methods. We tried to use patient’s extracted tooth for sinus augmentation. Because of the reason that the extracted tooth is an autogenous graft, there was no donor site complication. We made the extracted tooth into autogenous demineralized tooth block bones.
Demineralized autogenous tooth ring and block bone grafts provide a beneficial solid space maker that overcomes several drawbacks of autogenous ring and block bone grafts, aiding in vertical augmentation of the extraction socket and ridge defect. Dentin is known to have similar inorganic and organic components to alveolar bone [22]. Tooth bone has been utilized in the form of particulate or block bone or ring bone with and without demineralization for ridge augmentation [29,30,31]. Autogenous undemineralized dentin block implanted in host bone grafts were replaced gradually by newly formed bone and showed a structural and biological potential as alternative to autogenous block graft [32]. However, undemineralized dentin block demonstrates poor osteoinductive potential in non-osteogenic area [33]. Demineralization of the dentin block bone is known to have an important effect in bone regeneration [34]. Demineralization increases the number of exposed dentinal tubules, enlarges dentinal tubules to expose osteoinductive proteins, and decreases the crystallinity of dentin to allow replacement resorption [35,36,37]. When teeth bones are utilized in block or ring forms, demineralization and micro-perforation of the teeth bones are necessary. Demineralized and micro-perforated dentin block induced fastest and highest bone formation than undemineralized and non-perforated dentin blocks [38,39]. Demineralized dentin block, as a three-dimensional scaffold, has been observed to be well incorporated with alveolar bone, with volume largely maintained and minor bone loss, after an average of 44 months of follow-up [40].
By this autogenous demineralized tooth block technique, small amount of bone graft material was needed compared to the conventional techniques. Autogenous demineralized tooth block bone requires only one molar for one sinus augmentation. Also, surgical procedure became simple because only tooth blocks need to be inserted into the maxillary sinus. Because the tooth block bones are made by extracted tooth, it is more cost saving than ready-made bone graft material. In addition, our data showed that the autogenous demineralized tooth block bone contributed to the maintenance of the space by bearing the sinus air pressure.
An ideal characteristic of graft material for sinus augmentation is biologic safety, osteoinduction capability and space maintenance while preventing sinus pneumatization. Autogenous demineralized tooth block bone for sinus augmentation provided the space maintenance to prevent pneumatization. In addition, some studies reported that autogenous demineralized teeth stimulated osteogenesis [16,22,41]. This is because, demineralized tooth is rich in growth factors, such as transforming growth factor-beta (TGF-beta), fibroblast growth factor (FGF), bone morphogenetic proteins (BMP), platelet-derived growth factor (PDGF) and epidermal growth factor (EGF) [21,42].
In many lateral approach cases, lateral window is made by grinding the lateral wall of sinus cavity, and after bone graft procedure, grinded bone was covered by resorbable or non-resorbable membrane. In this study, we made lateral window with precise osteotomy technique and detached it. After bone graft procedure, we repositioned it. By this technique, bony window not only prevented soft tissue invade into the grafted site, but also acted as osteoinductive substance for accelerating new bone formation in the sinus. Moreover, the cost to purchase the membranes and the operation time to stabilize the membrane could be saved.
Precise osteotomy is essential to reposition the bony window in the right place. This is possible by the thin blade saw tip which combined with the piezoelectric device. The precisely created osteotomy line protects the replaceable bony window from falling to the sinus cavity. The use of the piezoelectric device has many advantages. It has more favorable new bone formation speed than other osteotomy devices, direct visibility over whole operation site, precise bone cutting and soft tissue protection ability which prevents the artery damage.
5. Conclusions
Through clinical and radiographic results, this retrospective study shows that using only demineralized tooth block bones allowed successful sinus bone grafts without inflammatory reaction, damage of donor site, manufactured graft materials. This study clearly showed that using demineralized tooth block bone in sinus augmentation can elicit a favorable prognosis. Therefore, it has been shown to have advantages for both patients and clinicians.
Author Contributions
Conceptualization, H.C. and D.-S.S.; methodology, D.-S.S.; software, H.C.; validation, H.C.; formal analysis, H.C.; investigation, H.C.; resources, H.C.; writing—original draft preparation, H.C.; writing—review and editing, D.-S.S.; visualization, H.C.; supervision, H.C.; project administration, D.-S.S.; funding acquisition, H.C. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by research grants from Daegu Catholic University in 2022.
Institutional Review Board Statement
The study was approved by the Animal Care and Use Committee at Catholic University Medical Center of Daegu (Approval IRB No. CR-22-174-L).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Le Guéhennec L, Soueidan A, Layrolle P, Amouriq Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent Mater J. 2007;23:844-854.
- Misch CE. Maxillary sinus augmentation for endosteal implants: organized alternative treatment plans. Int J Oral Implantol. 1987;4:49–58.
- Smiler DG, Johnson PW, Lozada JL, Misch C, Rosenlicht JL, Tatum OH, Wagner JR. Sinus lift grafts and endosseous implants: Treatment of the atrophic posterior maxilla. Dent Clin North Am. 1992;36:151–186.
- Chanavaz M. Maxillary sinus: anatomy, physiology, surgery, and bone grafting related to implantology--eleven years of surgical experience (1979-1990). J Oral Implantol. 1990;16:199–209.
- Thomason JM, Heydecke G, Feine JS, et al. How do patients perceive the benefit of reconstructive dentistry with regard to oral health-related quality of life and patient satisfaction? A systemic review. Clin Oral Implants Res. 2007; 18: 168-188.
- Sohn DS, Heo JU, Kwak DH, Kim DE, Kim JM, Moon JW, Lee JH, Park IS. Bone regeneration in the maxillary sinus using an autologous fibrin-rich block with concentrated growth factors alone. Implant Dent. 2011;20:389–395.
- Jaffin RA, Berman CL. The excessive loss of Branemark fixtures in type IV bone: a 5-year analysis. J Periodontol. 1991;62:2–4.
- Boyne PJ. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613–616.
- Tatum Jr H. Maxillary and sinus implant reconstructions. Dent Clin North Am. 1986;30:207–229.
- Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants. 2007;22 Suppl:49-70.
- Adell R, Lekholm U, Gröndahl K, Brånemark P-I, Lindström J, Jacobsson M. Reconstruction of severely resorbed edentulous maxillae using osseointegrated fixtures in immediate autogenous bone grafts. Int J Oral Maxillofac Implants. 1990;5.
- Klijn RJ, Meijer GJ, Bronkhorst EM, Jansen JA. A meta-analysis of histomorphometric results and graft healing time of various biomaterials compared to autologous bone used as sinus floor augmentation material in humans. Tissue Eng Part B Rev. 2010;16:493–507.
- Schlegel KA, Fichtner G, Schultze-Mosgau S, Wiltfang J. Histologic findings in sinus augmentation with autogenous bone chips versus a bovine bone substitute. Int J Oral Maxillofac Implants. 2003;18.
- Lee EY, Kim KW. A double layers technique for maxillary sinus augmentation with demineralized and mineralized bone graft materials. Maxillofac Plast Reconstr Surg. 2009;31:46–52.
- Hatano N, Shimizu Y, Ooya K. A clinical long-term radiographic evaluation of graft height changes after maxillary sinus floor augmentation with a 2: 1 autogenous bone/xenograft mixture and simultaneous placement of dental implants. Clin Oral Implants Res. 2004;15:339–345.
- Kim YK, Lee J, Yun JY, Yun PY, Um IW. Comparison of autogenous tooth bone graft and synthetic bone graft materials used for bone resorption around implants after crestal approach sinus lifting: a retrospective study. J Periodontal Implant Sci. 2014;44:216–221.
- Iezzi G, Degidi M, Piattelli A, Mangano C, Scarano A, Shibli JA, Perrotti V. Comparative histological results of different biomaterials used in sinus augmentation procedures: a human study at 6 months. Clin Oral Implants Res. 2012;23:1369–1376.
- Chen TW, Chang HS, Leung KW, Lai YL, Kao SY. Implant placement immediately after the lateral approach of the trap door window procedure to create a maxillary sinus lift without bone grafting: a 2-year retrospective evaluation of 47 implants in 33 patients. J Oral Maxillofac Surg. 2007;65:2324–2328.
- Mazor Z, Peleg M, Garg AK, Luboshitz J. Platelet-rich plasma for bone graft enhancement in sinus floor augmentation with simultaneous implant placement: patient series study. Implant Dent. 2004;13:65–72.
- Moon JW, Shin HI, Jung JK. New bone formation in the maxillary sinus using peripheral venous blood alone. J Oral Maxillofac Surg. 2011;69:2357–2367.
- Urist MR, Huo YK, Brownell AG, Hohl WM, Buyske J, Lietze A, Tempst P, Hunkapiller M, DeLange RJ. Purification of bovine bone morphogenetic protein by hydroxyapatite chromatography. Proc Natl Acad Sci U S A. 1984;81:371–375.
- Yeomans JD, Urist MR. Bone induction by decalcified dentine implanted into oral, osseous and muscle tissues. Arch Oral Biol. 1967;12:999-1008.
- Kim ES, Kang JY, Kim JJ, Kim KW, Lee EY. Space maintenance in autogenous fresh demineralized tooth blocks with platelet-rich plasma for maxillary sinus bone formation: a prospective study. Springerplus. 2016;5:274.
- Peleg M, Garg AK, Misch CM, Mazor Z. Maxillary sinus and ridge augmentations using a surface-derived autogenous bone graft. J Oral Maxillofac Surg. 2004;62:1535–1544.
- Pinchasov G, Juodzbalys G. Graft-free sinus augmentation procedure: a literature review. J Oral Maxillofac Res. 2014;5.
- Xu H, Shimizu Y, Ooya K. Histomorphometric study of the stability of newly formed bone after elevation of the floor of the maxillary sinus. Br J Oral Maxillofac Surg. 2005;43:493–499.
- Schlegel AK, Donath K. BIO-OSS--a resorbable bone substitute? J Long Term Eff Med Implants. 1998;8:201–209.
- Hallman M, Cederlund A, Lindskog S, Lundgren S, Sennerby L. A clinical histologic study of bovine hydroxyapatite in combination with autogenous bone and fibrin glue for maxillary sinus floor augmentation: results after 6 to 8 months of healing. Clin Oral Implants Res. 2001;12:135–143.
- Kim YK, Lee J, Um IW, Kim KW, Murata M, Akazawa T, et al. Tooth-derived bone graft material. J Korean Assoc Oral Maxillofac Surg. 2013;39(3):103-111.
- Lee KH, Kim YK, Cho WJ, Um IW, Murata M, Mitsugi M. Autogenous tooth bone graft block for sinus augmentation with simultaneous implant installation: a technical note. J Korean Assoc Oral Maxillofac Surg. 2015;41(5):284-289.
- Schwarz F, Golubovic V, Becker K, Mihatovic I. Extracted tooth roots used for lateral alveolar ridge augmentation: a proof-of-concept study. J Clin Periodontol. 2016;43(4):345–353.
- Becker K, Drescher D, Hönscheid R, Golubovic V, Mihatovic I, Schwarz F. Biomechanical, micro-computed tomographic and immunohistochemical analysis of early osseous integration at titanium implants placed following lateral ridge augmentation using extracted tooth roots. Clin Oral Implants Res. 2017; 28(3):334-340.
- Asfour A, Farzad P, Andersson L, Joseph B, Dahlin C. Host tissue reactions of non-demineralized autogenic and xenogenic dentin blocks implanted in a non-osteogenic environment. An experimental study in rabbits. Dent Traumatol. 2014;30(3):198-203.
- Park SM, Kim DH, Pang EK. Bone formation of demineralized human dentin block graft with different demineralization time: In vitro and in vivo study. J Craniomaxillofac Surg. 2017;45(6):903-912.
- Urist MR. Bone histogenesis and morphogenesis in implants of demineralized enamel and dentin. J Oral Surg.1971;29:88-102.
- Bang G. Induction of heterotopic bone formation by demineralized dentin in guinea pigs: antigenicity of the dentin matrix. J Oral Pathol.1972;1:172-185.
- Bang G. Induction of heterotopic bone formation by demineralized dentin: an experimental model in guinea pigs. Scand J Dent Res.1973;81:240-250.
- Kabir MA, Murata M, Akazawa T, Kusano K, Yamada K, Ito M. Evaluation of perforated demineralized dentin scaffold on bone regeneration in critical-size sheep iliac defects. Clin Oral Implants Res. 2017;28(11):e227-e235.
- Moon YS, Sohn DS, Kim G, Park IS. Comparative histomorphometric evaluation of bone regeneration with different preparations of xenogeneic tooth block bone. Int J Oral Maxillofac Implants. 2019;34(6):1413-1422.
- Kim YK, Pang KM, Yun PY, Leem DH, Um IW. Long-term follow-up of autogenous tooth bone graft blocks with dental implants. Clin Case Rep. 2017;8;5(2):108-118.
- Lee EY, Kim ES, Kim KW. Scanning electron microscopy and energy dispersive X-ray spectroscopy studies on processed tooth graft material by vacuum-ultrasonic acceleration. Maxillofac Plast Reconstr Surg. 2014;36:103.
- Gomes MF, Abreu PP de, Morosolli ARC, Araújo MM, Goulart M das GV. Densitometric analysis of the autogenous demineralized dentin matrix on the dental socket wound healing process in humans. Braz Oral Res. 2006;20:324–330.
Figure 2.
Demineralized and microperforated tooth blocks for maxillary sinus bone grafting.
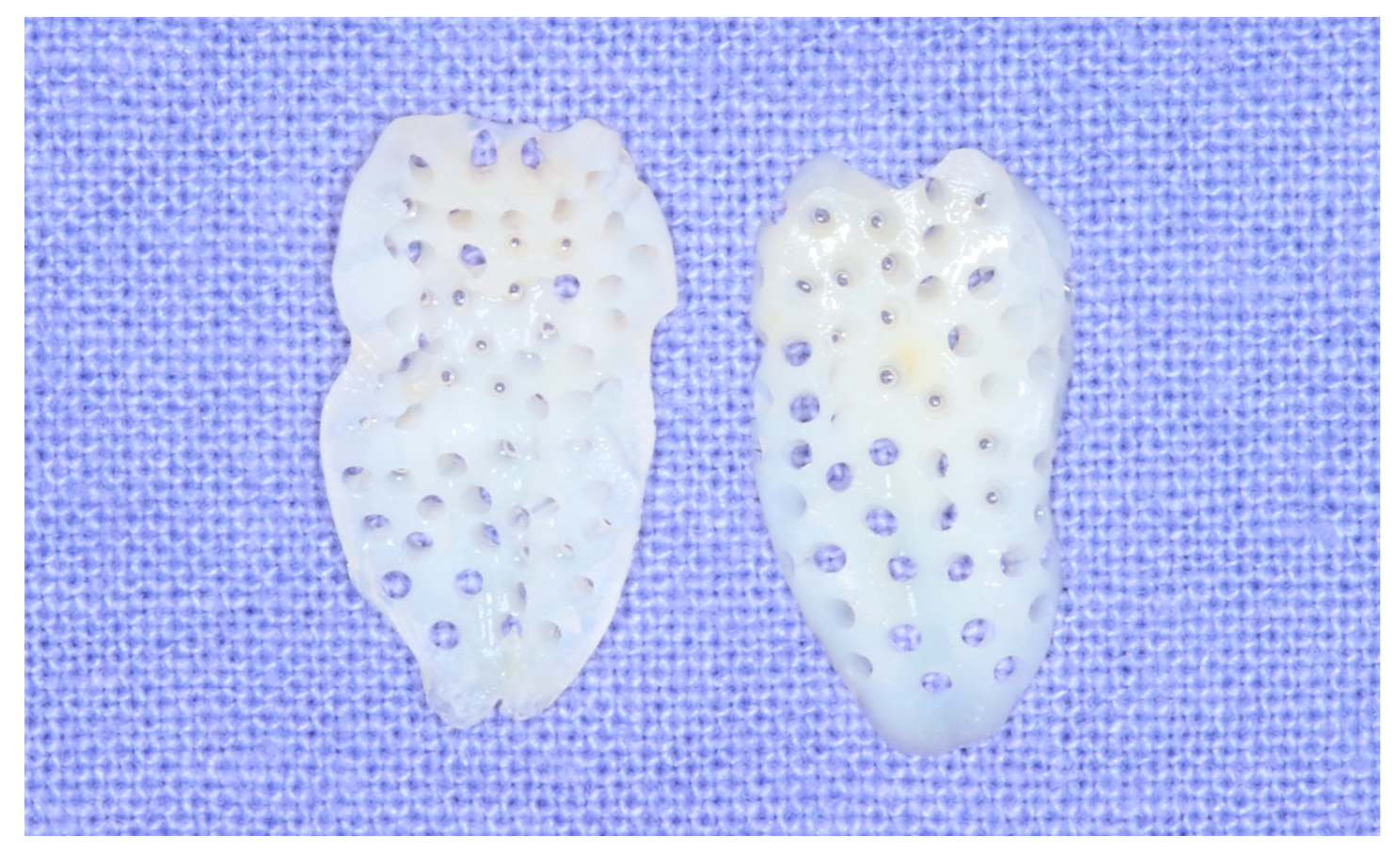
Figure 3.
SEM (Scanning Electron Microscope) images of undemineralized dentin show dentinal tubules blocked with hydroxyapatites. Consequently, diverse osteoinductive proteins are released with a delay.
Figure 3.
SEM (Scanning Electron Microscope) images of undemineralized dentin show dentinal tubules blocked with hydroxyapatites. Consequently, diverse osteoinductive proteins are released with a delay.
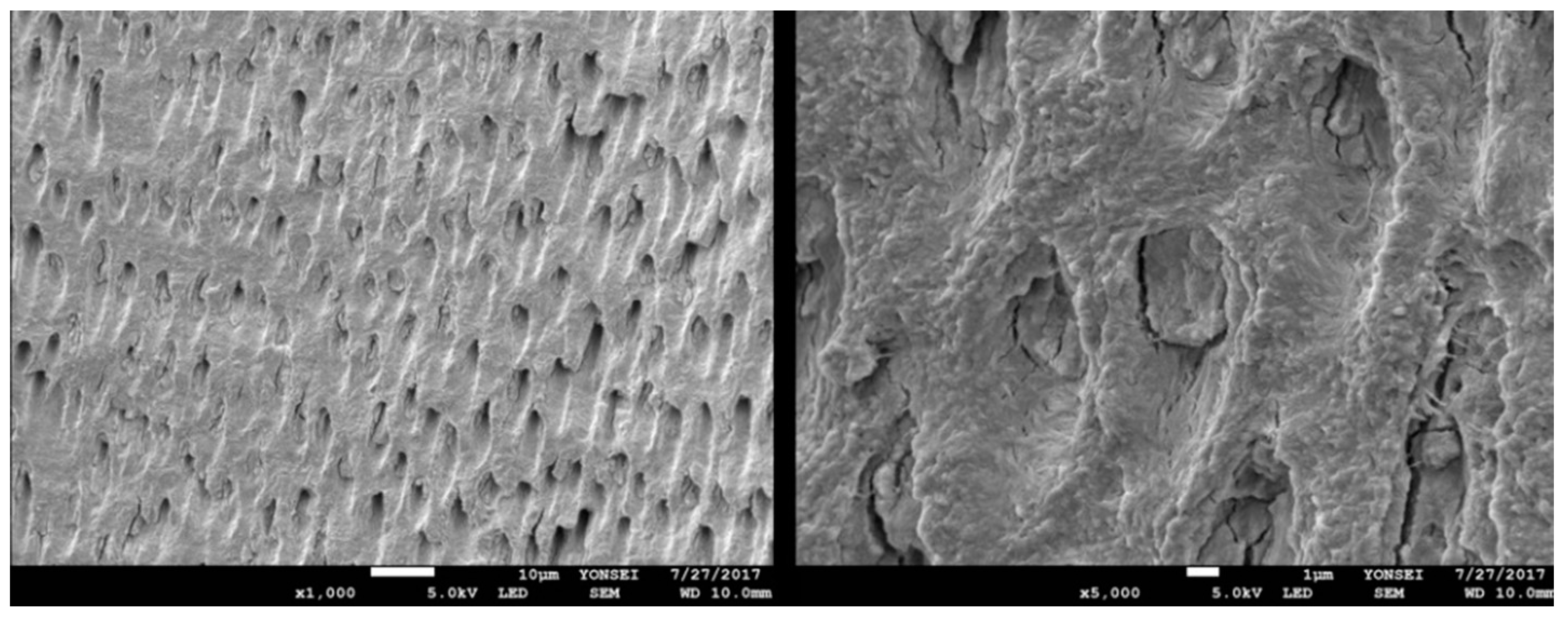
Figure 4.
SEM images of demineralized dentin. Dentinal tubules are enlarged, allowing for rapid proteins release, thereby promoting bone regeneration. Type I collagen fibers are also exposed, providing a scaffold for bone mineralization.
Figure 4.
SEM images of demineralized dentin. Dentinal tubules are enlarged, allowing for rapid proteins release, thereby promoting bone regeneration. Type I collagen fibers are also exposed, providing a scaffold for bone mineralization.
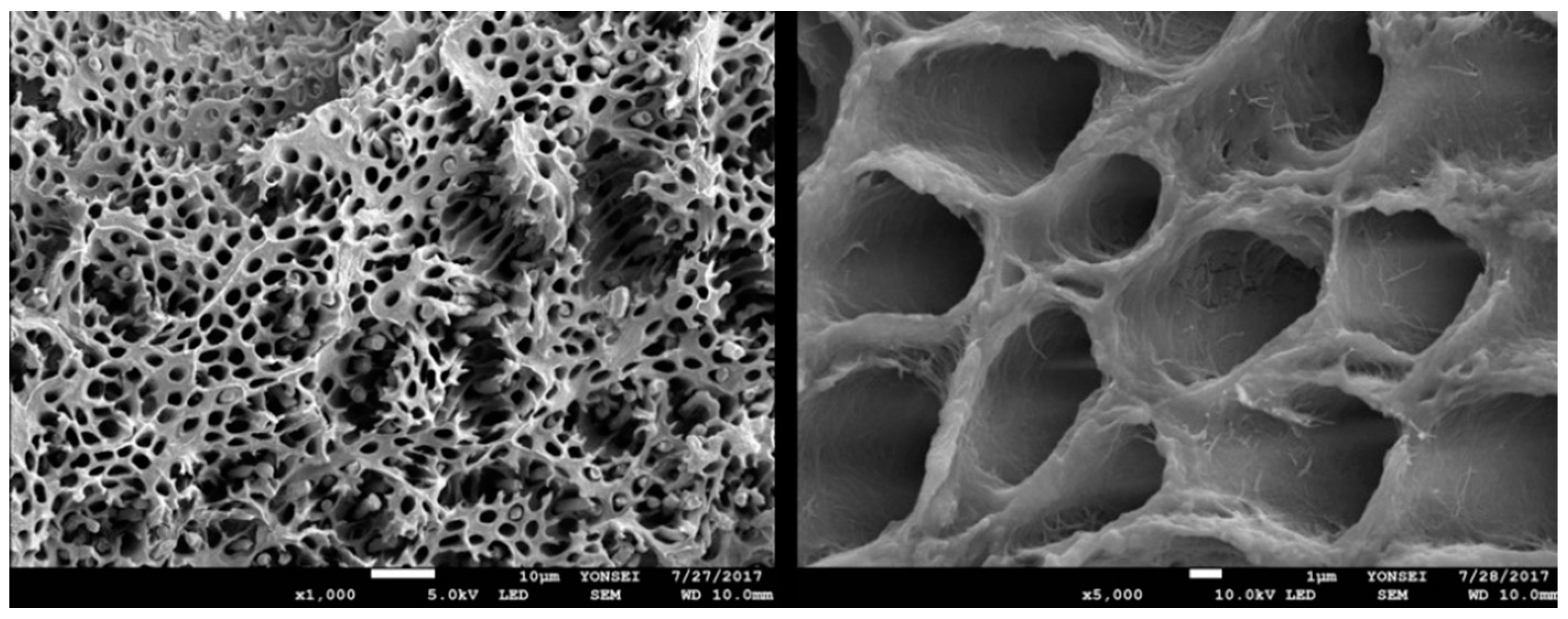
Figure 5.
Surgical procedure of sinus augmentation using demineralized tooth block bones: (A) Replaceable osteoinductive bony window (ROBW) was prepared by using piezoelectric device to expose and elevate the maxillary sinus mucosa; (B) Implants were placed with good stability after under-osteotomy with two tooth block bones placed over implant apex. Note severe horizontal bone deficiency around implants; (C) Fibrin-rich CGF blocks were placed in the sinus to accelerate bone regeneration; (D) ROBW was repositioned to exclude soft tissue ingrowth into maxillary sinus.
Figure 5.
Surgical procedure of sinus augmentation using demineralized tooth block bones: (A) Replaceable osteoinductive bony window (ROBW) was prepared by using piezoelectric device to expose and elevate the maxillary sinus mucosa; (B) Implants were placed with good stability after under-osteotomy with two tooth block bones placed over implant apex. Note severe horizontal bone deficiency around implants; (C) Fibrin-rich CGF blocks were placed in the sinus to accelerate bone regeneration; (D) ROBW was repositioned to exclude soft tissue ingrowth into maxillary sinus.
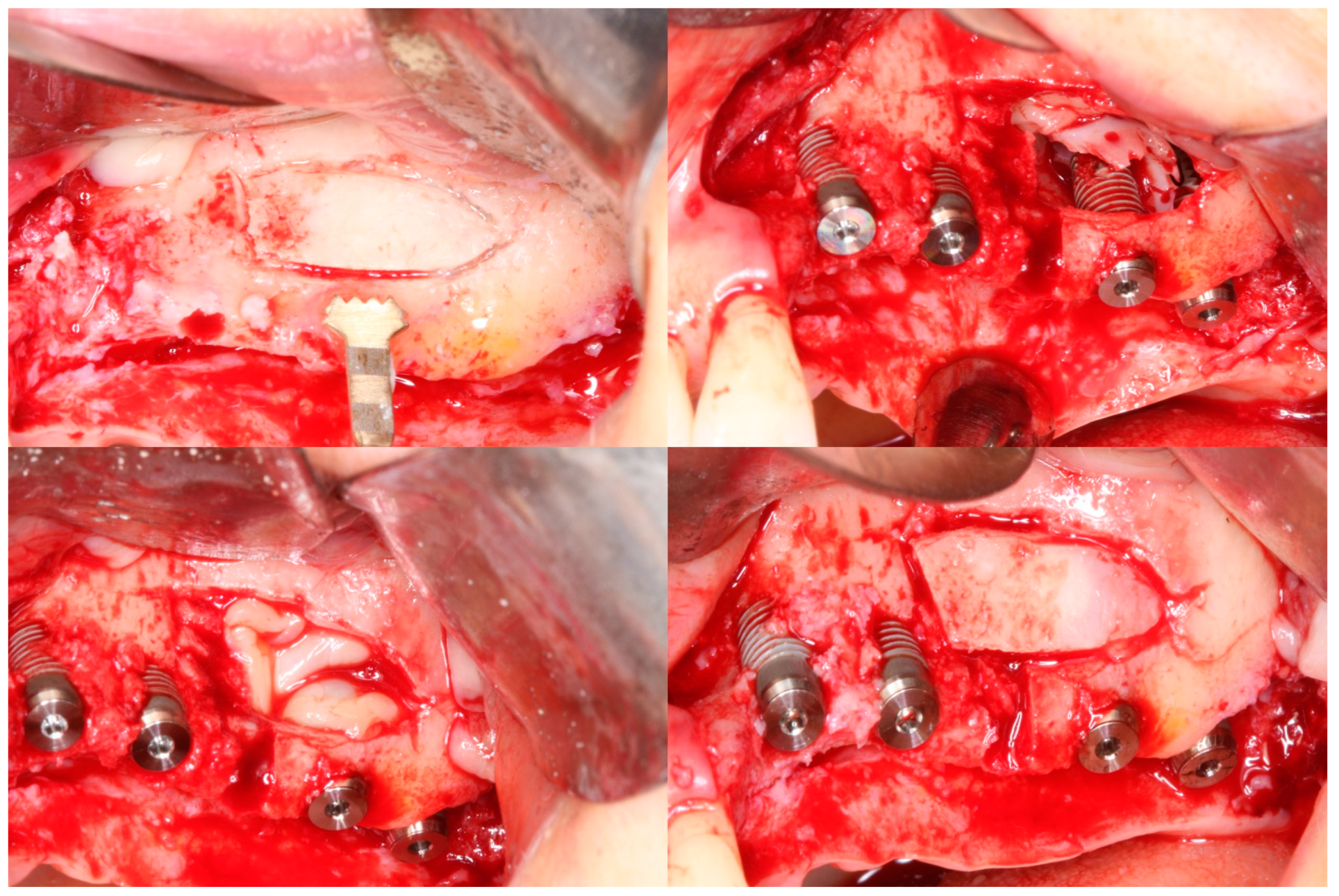
Figure 6.
(A) After grafting sticky tooth bone powder onto the buccal and palatal defects of the alveolar bone, a tooth block was transplanted onto the buccal side and secured with a mini screw. Simultaneously, a tooth block bone was inserted beneath the palatal mucosa on the palatal side; (B) A collagen barrier was covered over the bone graft; (C) Tension free primary closure was achieved; (D) Postoperative periapical radiograph.
Figure 6.
(A) After grafting sticky tooth bone powder onto the buccal and palatal defects of the alveolar bone, a tooth block was transplanted onto the buccal side and secured with a mini screw. Simultaneously, a tooth block bone was inserted beneath the palatal mucosa on the palatal side; (B) A collagen barrier was covered over the bone graft; (C) Tension free primary closure was achieved; (D) Postoperative periapical radiograph.
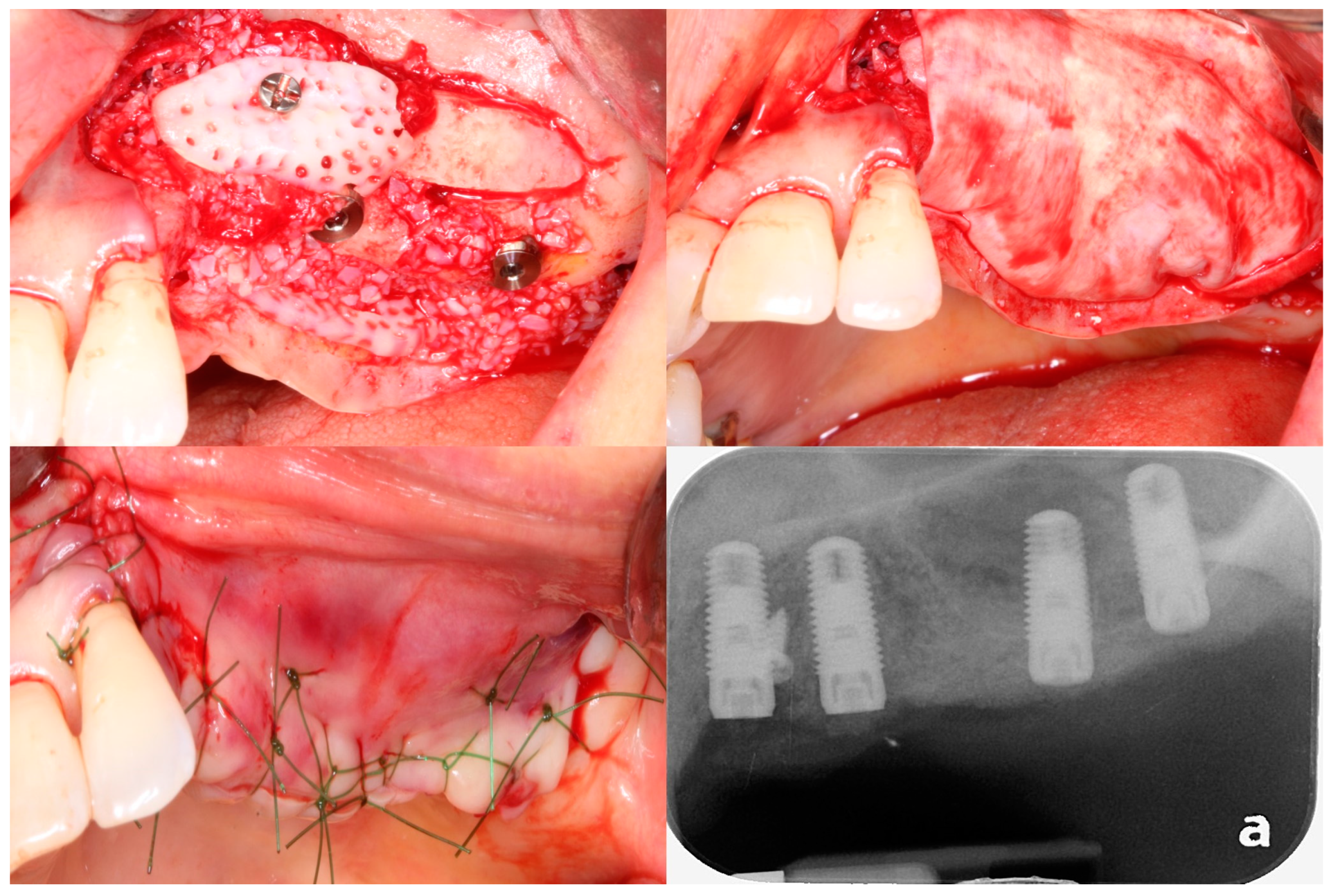
Figure 7.
Postoperative panoramic CBCT images: (A) Panoramic image of CBCT scans reveals elevated sinus mucosa; (B) Cross-sectional images of CBCT scans reveals tooth blocks under the elelvated sinus mucosa.
Figure 7.
Postoperative panoramic CBCT images: (A) Panoramic image of CBCT scans reveals elevated sinus mucosa; (B) Cross-sectional images of CBCT scans reveals tooth blocks under the elelvated sinus mucosa.
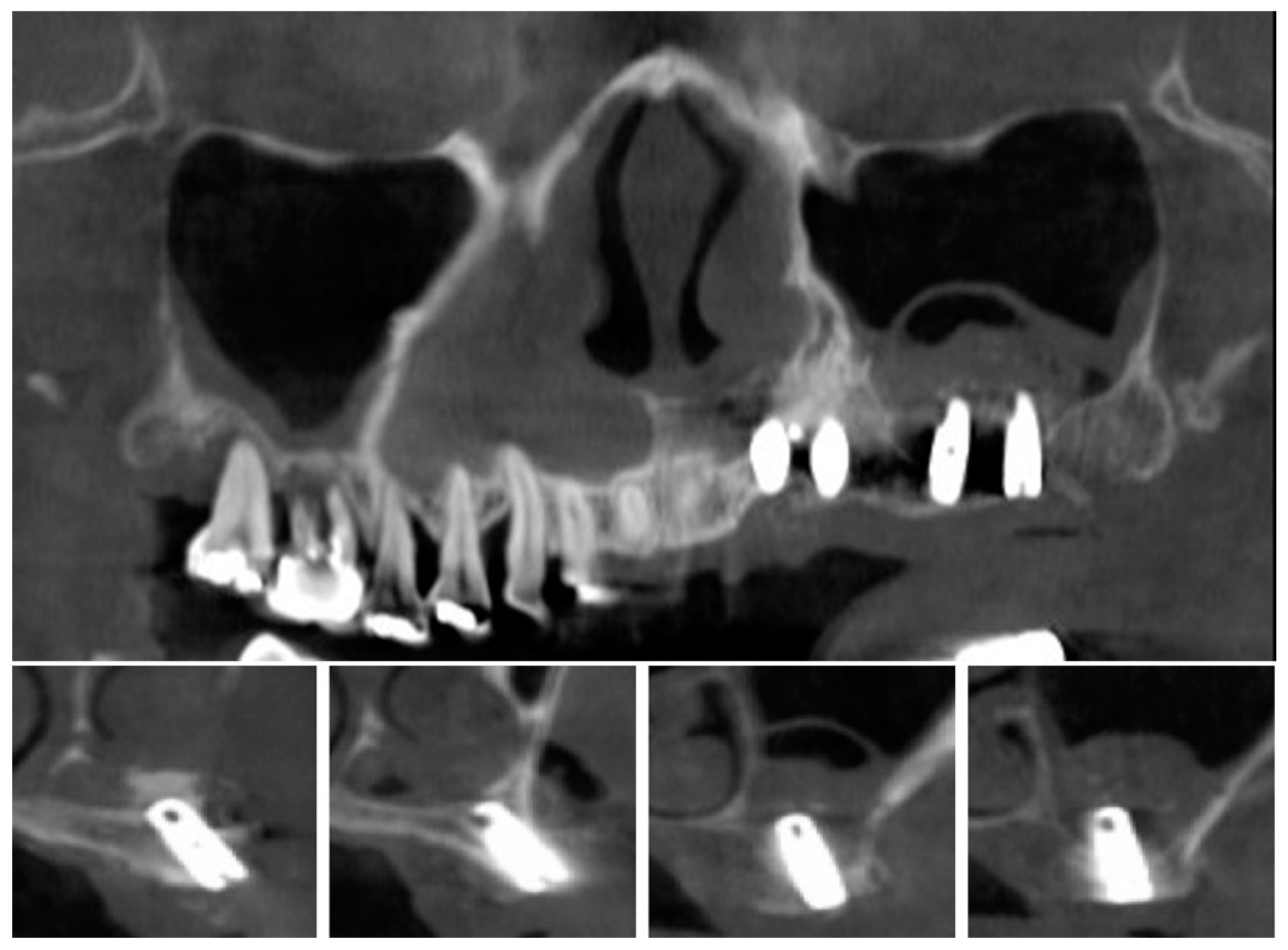
Figure 8.
CBCT scans after 5 months of healing: (A) Panoramic image shows augmented maxillary sinus; (B) Cross-sectional images shows favorably augmented alveolar ridge and maxillary sinus.
Figure 8.
CBCT scans after 5 months of healing: (A) Panoramic image shows augmented maxillary sinus; (B) Cross-sectional images shows favorably augmented alveolar ridge and maxillary sinus.
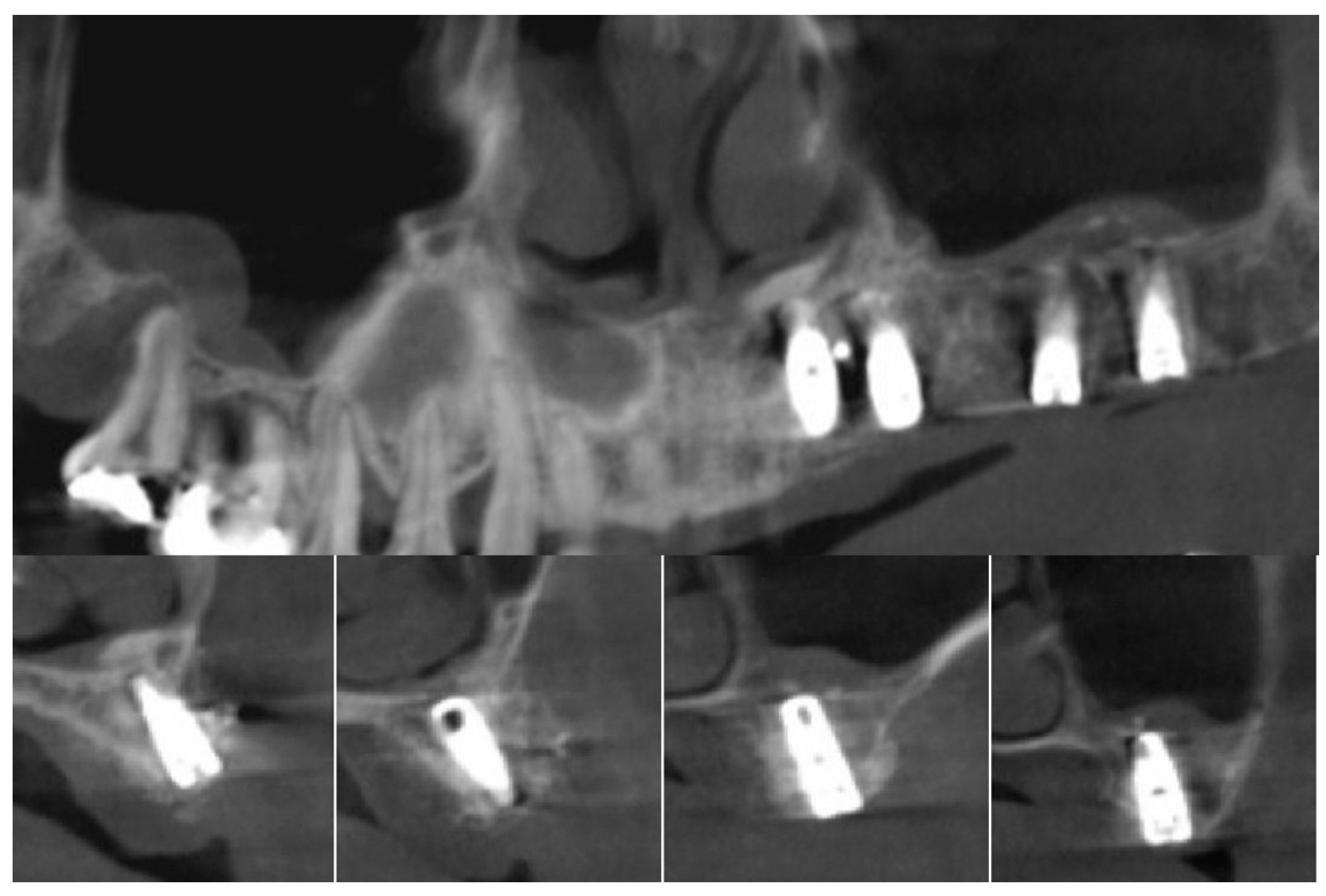
Figure 9.
Delivery of final implant zirconia prosthesis: (A) Intraoral photograph; (B) Periapical radiograph.
Figure 9.
Delivery of final implant zirconia prosthesis: (A) Intraoral photograph; (B) Periapical radiograph.
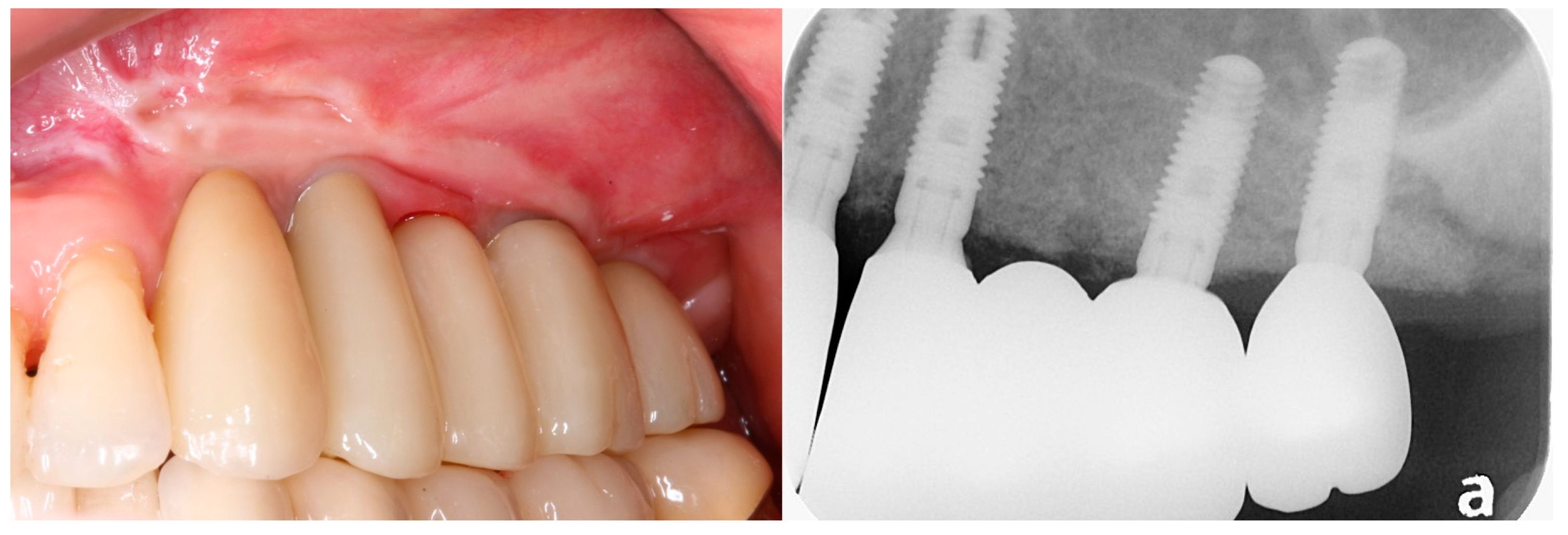
Figure 10.
5-years follow up examination: (A) Intraoral photograph; (B) Periapical radiograph.
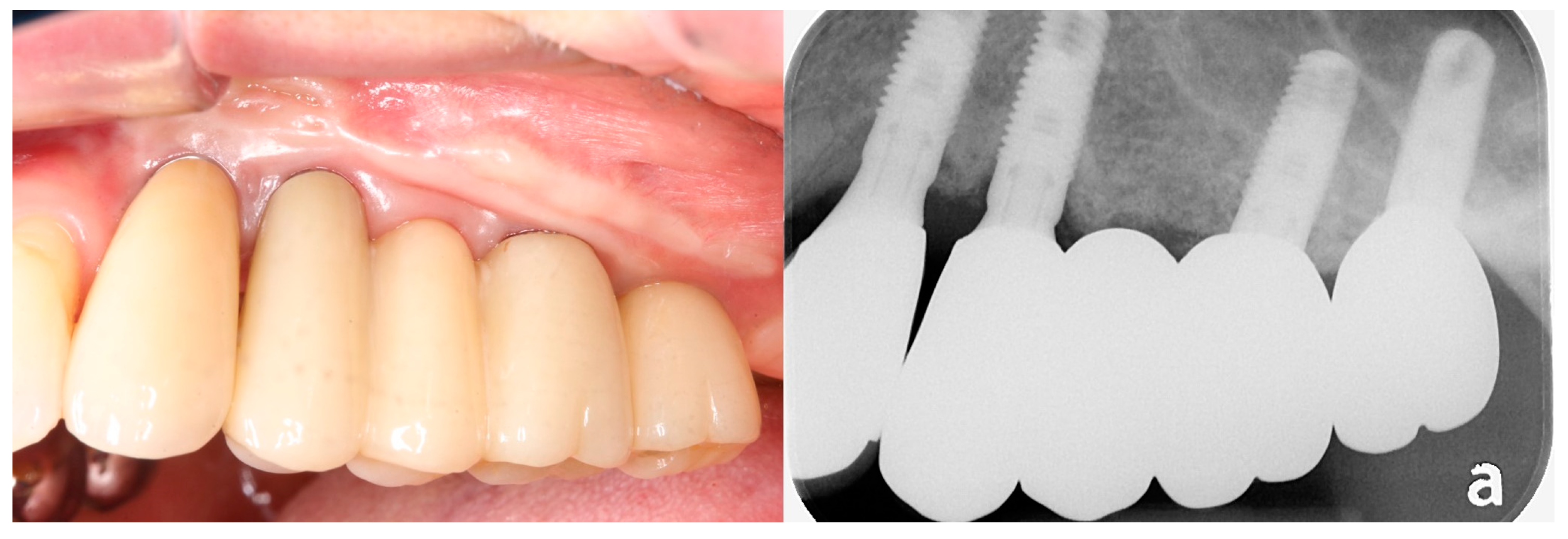

Table 1.
Table 1. Patient characteristics and clinical findings.
| Subject | Sex/Age | Region | Failed site | Sinus membrane perforation | Months to second stage surgery | Months in function | ||
| 1 | M/50 | #16 | - | No | 4 | 58 | ||
| 2 | M/46 | #26 | - | No | 6 | 42 | ||
| 3 | F/50 | #27 | - | Yes | 4.5 | 60 | ||
| 4 | M/46 | #14,15,16,17 | - | No | 7 | 51 | ||
| 5 | M/59 | #26,27 | - | No | 5 | 50 | ||
| 6 | F/57 | #26 | - | No | 5 | 48 | ||
| 7 | F/52 | #17 | - | Yes | 10 | 50 | ||
| 8 | F/52 | #27 | - | No | 5.5 | 55 | ||
| 9 | M/65 | #16 | - | Yes | 6.5 | 54 | ||
| 10 | M/50 | #16,26 | - | No | 7.5 | 59 | ||
| 11 | F/58 | #26,27 | - | No | 7.5 | 52 | ||
| 12 | F/47 | #27 | - | No | 4 | 58 | ||
| 13 | M/64 | #16 | - | No | 3 | 50 | ||
| 14 | M/75 | #26 | - | No | 6 | 60 | ||
| 15 | F/54 | #16 | - | No | 10 | 46 | ||
| 16 | M/45 | #17 | - | No | 3.5 | 49 | ||
| 17 | M/52 | #26,27 | - | No | 5 | 53 | ||
| 18 | M/45 | #27 | - | No | 10.5 | 54 | ||
| 19 | F/57 | #26,27 | - | No | 5 | 61 | ||
Table 2.
Radiographic assessment about maxillary sinus and alveolar crest.
| Subject | Region |
Preoperative bone height (mm) |
Maxillary sinus width (mm) |
Amount of sinus membrane elevation (mm) |
Bone height at the end of the study (mm) |
Increment of bone height (mm) |
| 1 | #16 | 5 | 12 | 18 | 14 | 9 |
| 2 | #26 | 3 | 18 | 17 | 13 | 10 |
| 3 | #27 | 5 | 16 | 16 | 14 | 9 |
| 4 | #14,15,16,17 | 5,3,5,5 | 22 | 15,18,14,16 | 15,16,14,14 | 10,13,9,8 |
| 5 | #26,27 | 4,4 | 16 | 16,16 | 15,12 | 11,8 |
| 6 | #26 | 6 | 16 | 18 | 20 | 14 |
| 7 | #17 | 2 | 24 | 16 | 15 | 13 |
| 8 | #27 | 2 | 22 | 19 | 18 | 16 |
| 9 | #16 | 2 | 22 | 16 | 14 | 12 |
| 10 | #16,26 | 3,3 | 23 | 23,20 | 20,22 | 17,19 |
| 11 | #26,27 | 3,2 | 24 | 19,18 | 20,16 | 17,14 |
| 12 | #27 | 4 | 22 | 16 | 15 | 11 |
| 13 | #16 | 5 | 12 | 14 | 14 | 9 |
| 14 | #26 | 4 | 16 | 12 | 12 | 8 |
| 15 | #16 | 1 | 20 | 22 | 18 | 17 |
| 16 | #17 | 5 | 13 | 17 | 20 | 15 |
| 17 | #26,27 | 6,6 | 15 | 10,11 | 15,16 | 9,10 |
| 18 | #27 | 3 | 25 | 12 | 14 | 11 |
| 19 | #26,27 | 1,2 | 20 | 21 | 14,14 | 13,12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



